Embed Size (px)
Citation preview

Evaluation and Medical Management of
Neuroendocrine Tumors Encountered
During Endoscopy or Abdominal
Imaging
8th Annual Symposium on “Gastrointestinal Cancers: An update on
advances in diagnosis and management”
Session II: Commonly Encountered NETs of the Gut
Lowell Anthony, M.D., F.A.C.P.
Professor of Medicine
LSUHSC New Orleans
Ritz Carlton Hotel
St. Louis, MO
September 12th, 2009

Questions
Is further work-up for systemic disease needed in all
patients with neuroendocrine tumors of the gut?
What kind of further evaluation is needed if the gut
lesion is:
– Carcinoid tumor?
– Gastrinoma?
– Non-functioning NE tumor?
How to evaluate patients with serum hypergastrinemia
– What to do if no gastrin producing lesion is identifiable?
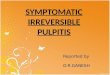
Carcinoid Tumors Are Most
Common (50% of all NETs)
Digestive
system
Bronchopulmonary
system
Other
%Other
Colon
and
Rectum
Small
Intestine
Stomach
2.3
28
28.5
4.6
1. Modlin IM et al. A 5-decade analysis of 13,715 carcinoid tumours. Cancer 2003;97:934-59.
Duodenum –3
Jejunum – 2
Ileum – 15
NOS – 8
Other – 0.5
Colon, except
the appendix – 9
Appendix – 5
Rectum – 14
NOS=not otherwise specified
28%
8%64%

0.00
1.00
2.00
3.00
4.00
5.00
6.00
1973
1974
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
Year
An
nu
al
in
cid
en
ce
pe
r 1
00 0
00
Incidence of neuroendocrine tumors
Incidence Of Neuroendocrine Tumors
Over Time – Analysis Of The SEER
Database (1973–2004)
1. Yao JC et al. One hundred years after "Carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol
2008;26(18):3063–72.
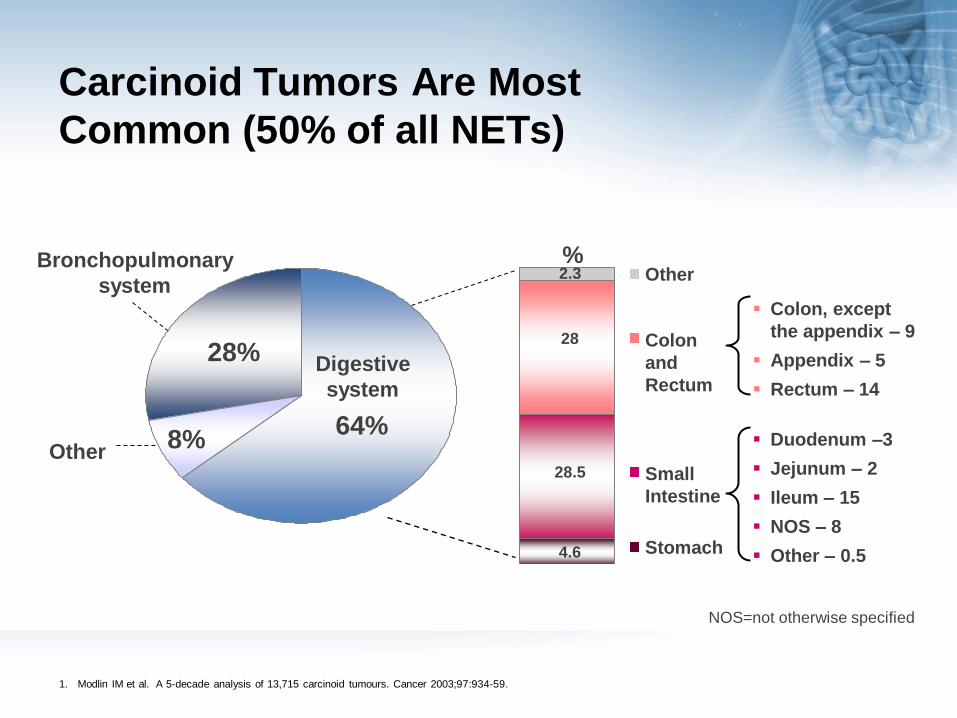
Prevalence of NETs
1. American Cancer Society. Cancer Reference Information. Cancer Prevalence: How Many People Have Cancer? © 2008 American Cancer Society Inc. Available at
http://www.cancer.org/docroot/CRI/content/CRI_2_6x_Cancer_Prevalence_How_Many_People_Have_Cancer.asp?sitearea=&level=. Accessed November 2008.
2. Yao JC et al. One hundred years after "Carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 2008;
26(18): 3063–72.
0
0.2
0.4
0.6
0.8
1
1.2
Colon & Rectum Neuroendocrine Stomach Pancreas Esophagus Hepatobiliary
103,312cases
100,000
1,100,000
1,200,000
1,168,000 cases
65,836 cases
32,353cases
28,664 cases 21,427
cases
NETs: 2004/2005 US Prevalence
29-year limited duration prevalence analyses based on SEER1,2

6
Carcinoid syndrome – causes and
symptoms
Carcinoid heart disease
Diarrhea
Vasodilation/bronchoconstriction
Flushing
Hypersecretion of biogenic amines and peptides e.g. serotonin, tachykinin

Carcinoid Syndrome – Symptom
Overview

Work-up for Carcinoid Tumors Encountered
During Endoscopy or Abdominal Imaging
Additional work-up for carcinoid tumors includes:1,2,3
Gastric Appendix Small bowel Colon Rectal
Endoscopy / A.I.
Serum Gastrin
EUS
A / P CT / MRI
SRS for patients
with normal gastrin
or syndrome sx
B12 level if
hypergastrinemic
With syndrome sx:
serotonin, 5-HIAA,
histamine, VIP
Laparoscopy /
Laparotomy / A.I.
A / P CT / MRI
For tumors > 2
cm or syndrome
present:
- SRS
- 5-HIAA, CGA
Endoscopy / Enteroscopy
/ CLN / Video endoscopy /
A.I.
A / P CT – consider triple
phase helical imaging /
MRI
GI series with SBFT as
indicated
Enteroclysis (optional)
SRS
5-HIAA, CGA
Echocardiography (with
inc 5-HIAA)
Colonoscopy / A.I.
SRS
A / P CT –
consider triple
phase helical
imaging / MRI
5-HIAA, CGA
Colonoscopy /
Sigmoidscopy / A.I.
EUS
A / P CT – consider
triple phase helical
imaging / MRI
With syndrome sx:
- SRS
- 5-HIAA, CGA
• If negative SRS and
+CT/MRI: FDG-PET
1. The NCCN Guideline Neuroendocrine Tumors. Clinical Practice Guidelines in Oncology (Version 2.2006). © 2006 National Comprehensive Cancer Network, Inc. Available at
http://www.nccn.org. Accessed Nov 07 2008. To view the most recent and complete version of the guideline, go online to www.nccn.org.
2. Jensen RT et al. Well-Differentiated Duodenal Tumor/Carcinoma (Excluding Carcinomas) [ENETS guidelines]. Neuroendocrinology 2006;84:165-172
3. Personal experience, Lowell Anthony.
A.I. = abdominal imaging

Work-up for Less Encountered NETs During
Endoscopy or Abdominal Imaging
Additional work-up for carcinoid tumors includes:1
Esophageal Liver Gall Bladder Extra-Hepatic
Biliary Ducts
Ampullary
Endoscopy / A.I.
EUS
Well-differentiated:
- SRS
- 5-HIAA, CGA
Poorly-
differentiated:
- FDG-PET
Laparoscopy /
Laparotomy / A.I.
A / P CT – triple-
phase helical / MRI
SRS
5-HIAA, CGA
Echocardiography
(inc 5-HIAA)
A.I.
A / P CT - triple-phase
helical / MRI / US
SRS
5-HIAA, CGA
ERCP / A.I.
A / P CT - triple-
phase helical / MRI
/ US
SRS
5-HIAA, CGA
Endoscopy / ERCP /
A.I.
A / P CT - triple-
phase helical / MRI /
EUS
SRS
5-HIAA, CGA
1. Personal suggestions, Lowell Anthony

Stains and Laboratory Studies Used
in the Work-Up of NETs Encountered at
Endoscopy or Abdominal Imaging There is a range of stains
recommended for the work-up of NETs, including:1-4
– Basic stains for diagnosis:
• Chromogranin A
– Qualitative vs quantitative
• Synaptophysin
– Qualitative vs quantitative
• Cytokeratin
Low vs intermediate vs high grade
– # of mitotic cells / 10 HPFs
– Ki-67
There is a range of hormone-related studies recommended for the work-up of NETs, including:1-4
– Carcinoid
• 5-HIAA (24 h urine)
• Chromogranin A
– Gastrinoma
• Gastrin
• Secretin
• Calcium
1. The NCCN Guideline Neuroendocrine Tumors. Clinical Practice Guidelines in Oncology (Version 2.2006). © 2006 National Comprehensive Cancer Network, Inc.
Available at http://www.nccn.org. Accessed Nov 07 2008. To view the most recent and complete version of the guideline, go online to www.nccn.org.
2. Falconi M et al. Well-Differentiated Pancreatic Nonfunctioning Tumors/Carcinoma. Neuroendocrinology 2006;84:196–211
3. Jensen RT et al. Gastrinoma (Duodenal and Pancreatic). Neuroendocrinology 2006;84:173–182
4. Steinmuller T et al. Consensus Guidelines for the Management of Patients with Liver Metastases from Digestive (Neuro)endocrine Tumors: Foregut, Midgut,
Hindgut, and Unknown Primary. Neuroendocrinology 2008;87:47–62

Pathology of NETs
Role of Biologic Markers:
Chromogranin A (CgA)

Carcinoid Syndrome Specific Marker:
5-hydroxyindoleacetic Acid (5-HIAA)
Serotonin-Rich Foods
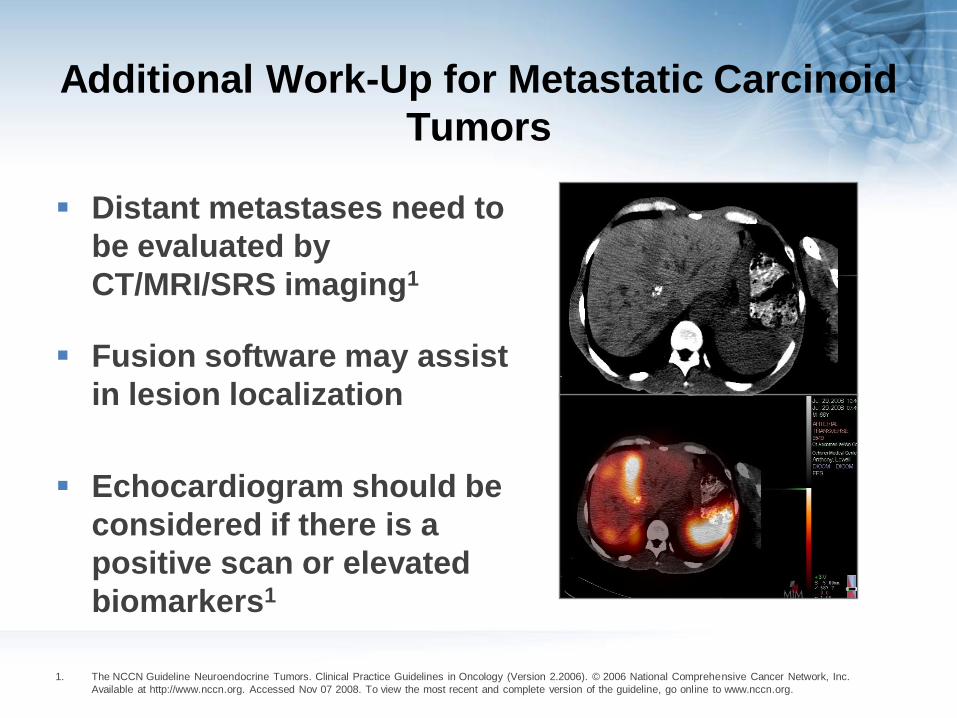
Additional Work-Up for Metastatic Carcinoid
Tumors
Distant metastases need to
be evaluated by
CT/MRI/SRS imaging1
Fusion software may assist
in lesion localization
Echocardiogram should be
considered if there is a
positive scan or elevated
biomarkers1
1. The NCCN Guideline Neuroendocrine Tumors. Clinical Practice Guidelines in Oncology (Version 2.2006). © 2006 National Comprehensive Cancer Network, Inc.
Available at http://www.nccn.org. Accessed Nov 07 2008. To view the most recent and complete version of the guideline, go online to www.nccn.org.

NCCN Treatment Algorithm for
Carcinoid Syndrome
Neuroendocrine Tumors, Clinical Practice Guidelines in Oncology - Version 2.2006, National Comprehensive Cancer Network.Available at: http://www.caringforcarcinoid.org/carcinoid/documents/nccn.pdf – accessed 28 October 2008.
Distant
metastases
Bone
LiverOctreotide d,e 150 mcg SC
TID• If tolerated and
symptomatic response, consider Octreotide LAR initially 20 mg IM monthly, then may gradually increase dose and frequency
OrManage clinical syndrome
as appropriate
Resect
Observe with
markers and
scans every
3-6 mo, or
Clinical trial
If progression, see below
Hepatic regional therapy
(arterial embolization,
chemoembolization,
or other)
or
Chemoembolization
or
Systemic chemotherapy
with doxorubicin/
streptozocin
or
Ablative therapy (RFA,
cryotherapy)
or
Clinical trial
Resect
RT if symptomatic
or
Clinical trial
or
Consider systemic
chemotherapy
with doxorubicin/
streptozocin
or
Interferon
Systemic chemotherapy
with doxorubicin/
streptozocin
or
Interferon
or
Clinical trial
Resect
Asymptomatic
Symptomatic
or
Progression
If liver and
resectable
Extrahepaticorunresectable
Unresectable
Resectable
Unresectable
Resectable
Lung
Somatostatin
Peptide produced by normal cells and certain tumors
Regulates wide variety of physiologic functions
Controls proliferation of normal and tumor cells
Was one of the first targets for NET therapy
1. Guillermet-Guibert J et al. Somatostatin receptors as tools for diagnosis and therapy: molecular aspects. Best Pract Res Clin Gastroenterol 2005;19:535–51

18
sst receptors and NETs
Somatostatin receptors are G-protein-coupled receptors that mediate the inhibition of a large number of secretory processes
Distributed throughout the body and expressed in 80–90% of NETs
Based on their structure and function, somatostatin receptors can be divided into five subtypes, sst1 5
In NETs, sst2, sst5 and sst1 are most frequently expressed, followed by sst4 and sst3
Schmid et al. Mol Cell Endocrinol 2008;286:69–74
19
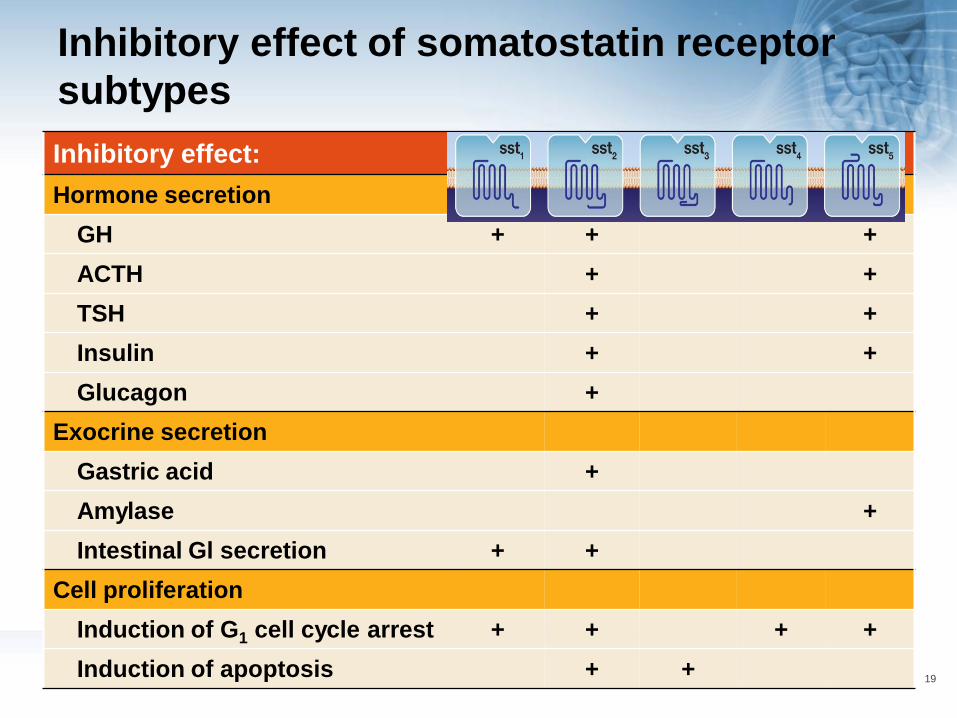
Inhibitory effect of somatostatin receptor
subtypes
Inhibitory effect: sst1 sst2 sst3 sst4 sst5
Hormone secretion
GH + + +
ACTH + +
TSH + +
Insulin + +
Glucagon +
Exocrine secretion
Gastric acid +
Amylase +
Intestinal Gl secretion + +
Cell proliferation
Induction of G1 cell cycle arrest + + + +
Induction of apoptosis + +

Somatostatin Biological Effects
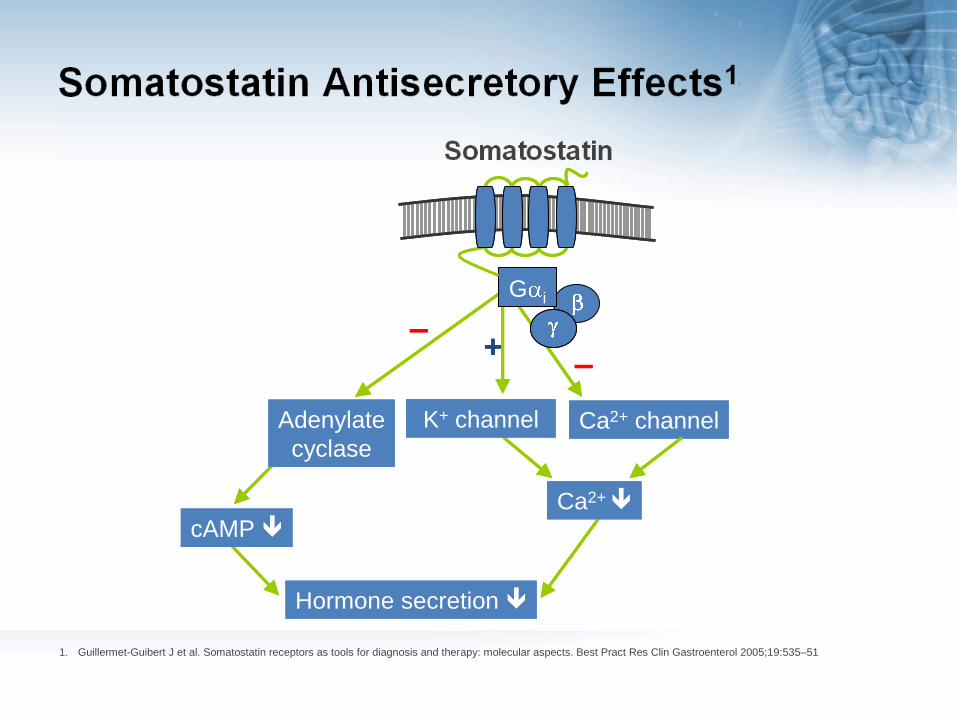
Ca2+ channel
Ca2+
Hormone secretion
–
Ca2+ channelCa2+ channel
Ca2+
Hormone secretion
–
Ca2+ channelAdenylate
cyclase
cAMP
–
Adenylate
cyclase
cAMP
–
K+ channel
+
K+ channel
+
1. Guillermet-Guibert J et al. Somatostatin receptors as tools for diagnosis and therapy: molecular aspects. Best Pract Res Clin Gastroenterol 2005;19:535–51
Somatostatin
G i
Somatostatin Antisecretory Effects1

Somatostatin Antiproliferative Effects

U
23
PROMID – octreotide LAR significantly
increases time to tumor progression
Octreotide LAR vs placebo P=0.000072
HR=0.34 [95% CI: 0.20–0.59]
Octreotide LAR: 42 patients / 26 events
Median 14.3 months [95% CI: 11.0–28.8]
Placebo: 43 patients / 40 events
Median 6.0 months [95% CI: 3.7–9.4]
Time (months)
Pro
po
rtio
n w
ith
ou
t p
rog
res
sio
n
0
0.25
0.5
0.75
1
0 6 12 18 24 30 36 42 48 54 60 66 72 78
Based on the conservative ITT analysis
Arnold R. Presented at ASCO-GI 2009

Treatment Options and Follow-Up
Require Cross Discipline Coordination
Examples of the disciplines involved in the treatment and follow-up of NET
patients1-4
1. Caplin M et al. Carcinoid tumour. Lancet 1998; 352:799-805
2. McStay M K G and Caplin M E. Carcinoid tumour. Minerva Med 2002, 93:389-401
3. The NCCN Guideline Neuroendocrine Tumors. Clinical Practice Guidelines in Oncology (Version 2.2006). © 2006 National Comprehensive Cancer Network, Inc. Available at
http://www.nccn.org. Accessed Nov 07 2008. To view the most recent and complete version of the guideline, go online to www.nccn.org.
4. Steinmuller T et al. Consensus Guidelines for the Management of Patients with Liver Metastases from Digestive (Neuro)endocrine Tumors: Foregut, Midgut, Hindgut, and
Unknown Primary. Neuroendocrinology 2008;87:47–62
Discipline Treatment and follow-up options
Surgery team Endoscopic resection, surgical resection, radical gastric resection, lymph node removal, antrectomy, partial hepatectomy, ablative therapy
Gastroenterology team Esophagogastroduodenoscopy, colonoscopy, ileoscopy
Pathology/histology
team
Biopsy of tumor and adjacent mucosa, follow-up of pathology and histology markers
Endocrinology/oncology
team
Medical therapy, systemic chemotherapy
Radiology/radiotherapy/
nuclear medicine team
Radiotherapy, CT/MRI, SRS, imaging studies as required, chemoembolization, ablative therapy
Nurse team Specialist nurses will interact with the patient on an ongoing basis

Requirements for an Improvement in
NETs Outcomes1
Refinement of universal classification and grading
system
Elucidation of cell biology
Development of cell lines and animal models
Acquisition of genetic information
Identification of serum markers for early diagnosis
Definition of tissue markers to identify tumor origin
Development of molecular pathological profiling to define
prognosis
1. Modlin I M et al. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncology 2008;9(2): p61-72

Requirements for an Improvement in
NETs Outcomes1 (cont’d)
Precise identification of topographic information before
and during surgery
Identification of molecular therapeutic targets
Development of improved (adjuvant) treatment for
residual disease
Establishment of centers of excellence and
multidisciplinary specialty NET clinical teams
Construction of central clinical and tissue database
resources
Government focus on clinical/research funding
1. Modlin I M et al. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncology 2008;9(2): p61-72

Questions
Is further work-up for systemic disease needed in all
patients with neuroendocrine tumors of the gut?
What kind of further evaluation is needed if the gut
lesion is:
– Carcinoid tumor?
– Gastrinoma?
– Non-functioning NE tumor?
How to evaluate patients with serum
hypergastrinemia
– What to do if no gastrin producing lesion is identifiable?











![Interpreting biochemical control response rates with first ... · pasireotide LAR versus octreotide LAR by Colao et al. [19] in patients who were either de novo or had received transsphenoidal](https://img.pdfslide.us/doc/110x75/5f6f75f2ce5a7e1a3a2f4144/interpreting-biochemical-control-response-rates-with-first-pasireotide-lar-versus.jpg)