Embed Size (px)
Citation preview
ecraielg
wtentipe
c
SMFM Clinical Opinion www.AJOG.org
Evaluation and management of severe preeclampsiabefore 34 weeks’ gestation
Publications Committee, Society for Maternal-Fetal Medicine, with the assistance of Baha M. Sibai, MDtac(aaipdftpdgaept
coo
IntroductionPreeclampsia is a multisystem disorderthat can manifest clinically with hyper-tension and proteinuria with or with-out accompanying symptoms, abnormalmaternal laboratory test results, intra-uterine growth restriction, or reducedamniotic fluid volume.1 The incidence ofsevere preeclampsia ranges from 0.6-1.2%of pregnancies in Western countries.2-5
Preeclampsia �37 weeks’ and severe pre-clampsia �34 weeks’ gestation compli-ates 0.6-1.5% and 0.3% of pregnancies,espectively.3,6 The likelihood of severend preterm preeclampsia is substantiallyncreased in women with a history of pre-clampsia, and in those with diabetes mel-itus, chronic hypertension, or a multifetalestation.1,3,7-10 Published reports use
differing criteria for the diagnoses ofpreeclampsia, severe and superimposedpreeclampsia, and HELLP (hemolysis, ele-vated liver enzymes, low platelets) syn-drome. Commonly used definitions arepresented in the Table.11-14 For women
ith preexisting hypertension or pro-einuria, the diagnosis of severe pre-clampsia can be more difficult, butew-onset severe hypertension or pro-
einuria, or development of other clin-cal or laboratory findings of severereeclampsia are suggestive of pre-clampsia in this setting.
Severe preeclampsia occurring preterman result in both acute1,2,4,7-10 and long-
From the Society for Maternal-FetalMedicine, Washington, DC (PublicationsCommittee); and Division of Maternal FetalMedicine, Department of Obstetrics andGynecology, Clinical Perinatal Research,University of Cincinnati College ofMedicine, Cincinnati, OH (Dr Sibai).
Received July 1, 2011; accepted July 7, 2011.
Reprints not available from the authors.
0002-9378/free© 2011 Published by Mosby, Inc.
doi: 10.1016/j.ajog.2011.07.017erm complications for both the mothernd her newborn.15,16 Maternal compli-ations of severe preeclampsia (Table)as well as myocardial infarction, stroke,cute respiratory distress syndrome, co-gulopathy, severe renal failure, retinalnjury) occur more commonly in theresence of preexistent medical disor-ers, and with acute maternal organ dys-
unction related to preeclampsia.10,17 Ma-ernal morbidities rarely persist after severereeclampsia, although cardiovascularisease later in life is more common re-ardless of clinical presentation.15,16 Fetalnd newborn complications of severe pre-clampsia result from exposure to utero-lacental insufficiency and/or from pre-erm birth.1,10
Historically, women with severe pre-eclampsia have had delivery initiated upondiagnosis in order to limit maternal com-
OBJECTIVE: We sought to review the risksevere preeclampsia remote from term, anmanagement, maternal and fetal evaluationMETHODS: Studies were identified throughpeer-reviewed articles published in the EnDecember 2010. Additionally, the Cochrastudies identified through review of the aboto identify relevant articles. Where reliableauthorities were used.RESULTS AND RECOMMENDATIONS: Pustudies regarding management of severe prsuggest that expectant management of selebut that delivery is often required for worseare not candidates for expectant managemeedema, disseminated intravascular coagulabnormal fetal testing, HELLP syndrome, orFor women with severe preeclampsia beforhas been associated with frequent maternanewborn. Expectant management of a seleoccurring �34 weeks’ gestation may impin-hospital maternal and fetal surveillance.
Key words: expectant management, fetal gpreeclampsia
plications from worsening disease.1,12 The
SEPTEMBER 2011 Am
linical course of severe preeclampsia isften characterized by progressive deteri-ration if delivery is not pursued.10,17
However, some have challenged the viewthat all patients with severe preeclampsiamust be delivered expeditiously.7 Thefirst attempts at expectant managementwere aimed at providing brief pregnancyprolongation to allow for antenatal corti-costeroid administration, but the potentialfor longer expectant management was en-tertained because some patients remainedstable or improved during initial observa-tion. Further study has shown that me-dian latency with expectant manage-ment ranges from 7–14 days.18
In this report, the risks and benefits ofexpectant management of severe pre-eclampsia remote from term are re-viewed, and recommendations regard-ing expectant management, maternal
nd benefits of expectant management ofo provide recommendations for expectanteatment, and indications for delivery.arch of the MEDLINE database for relevant
sh language from January 1980 throughLibrary, guidelines by organizations, andocuments and review articles were utilizedwere not available, opinions of respected
hed randomized trials and observationallampsia occurring �34 weeks of gestationd patients can improve neonatal outcomesg maternal or fetal condition. Patients whoinclude women with eclampsia, pulmonaryn, renal insufficiency, abruptio placentae,rsistent symptoms of severe preeclampsia.e limit of viability, expectant managementorbidity with minimal or no benefits to theroup of women with severe preeclampsia
e newborn outcomes but requires careful
th restriction, HELLP syndrome, severe
s ad t, tr
a segli
neve ddata
bliseeccteninnt
atiopee thl mct grov
row
and fetal evaluation, and indications
erican Journal of Obstetrics & Gynecology 191

mpeptcrdtawrc.mrP(fbnmptstmae
SMFM Clinical Opinion www.AJOG.org
for delivery are offered. For the pur-pose of this document, expectant man-agement is defined as any attempt todelay delivery for antenatal corticoste-roid administration or longer.
What are the benefits and risks ofexpectant management of severepreeclampsia <34 weeks’ gestation?Randomized trialsOnly 2 randomized trials of delivery vs ex-pectant management of preterm severepreeclampsia have been published.19,20
Odendaal et al19 studied 38 womenwith severe preeclampsia between 28-34weeks’ gestation age and whose fetal
TABLEDiagnostic criteria for preeclampsipreeclampsia, and HELLP syndrom
➢ PreeclampsiaŒ Blood pressure �140 mm Hg or �90 m
in woman with previously normal bloodexcretion �0.3 g protein in 24-h urine
➢ Severe preeclampsia (�1 of following criteŒ Blood pressure �160 mm Hg systolic o
least 6 h apart while patient is on bed rŒ Proteinuria �5 g in 24-h urine specime
least 4 h apartŒ Oliguria �500 mL in 24 hŒ Cerebral or visual symptomsŒ Pulmonary edema or cyanosisŒ Epigastric or right upper quadrant painŒ Impaired liver functionŒ ThrombocytopeniaŒ Fetal growth restriction
➢ Superimposed preeclampsia (�1 of followŒ New-onset proteinuria �0.3 g protein inŒ If hypertension and proteinuria present
� Sudden increase in proteinuria if bot�20 wk’ gestation
� Sudden increase in hypertension in wwell controlled
� Thrombocytopenia (platelet count �� Increase in alanine aminotransferase
levelsWomen with chronic hypertension who devepigastric pain also may have superimpose
➢ HELLP syndrome (differing diagnostic critecriteria follow)Œ Sibai et al13 (each of following required
(1) Hemolysis on peripheral smear, lact�1.2 mg/dL
(2) Aspartate aminotransferase �70 U/(3) Platelet count �100,000 cells/mm3
Œ Martin et al14 (each of following require(1) Lactate dehydrogenase �600 U/L(2) Aspartate aminotransferase or alani(3) Platelet count �150,000 cells/mm3
...................................................................................................................
SMFM. Severe preeclampsia. Am J Obstet Gynecol 2011.
weight was estimated to be between 650- v
192 American Journal of Obstetrics & Gynecology
1500 g. Eighteen women received ante-natal corticosteroids for fetal maturationand were then treated expectantly, withdelivery only for specific maternal or fetalindications. Another 20 patients were as-signed to receive antenatal corticosteroidswith planned delivery after 48 hours. La-tency to delivery (7.1 vs 1.3 days; P � .05)and gestational age at delivery (223 vs 221days; P � .05) were both greater with ex-pectant management while total neona-tal complications were reduced (33% vs75%; P � .05) compared with planneddelivery.
Sibai et al20 studied 95 women with se-
severe-14
Hg diastolic that occurs �20 wk’ gestationssure plus proteinuria defined as urinarycimenis required)110 mm Hg diastolic on 2 occasions at
3� on 2 random urine samples collected at
criteria is required)oman with hypertension �20 wk’ gestation0 wk’ gestationpertension and proteinuria are present
an whose hypertension has previously been
,000 cells/mm3)aspartate aminotransferase to abnormal
p persistent headache, scotoma, orreeclampsiaave been reported, 2 commonly used
dehydrogenase �600 U/L, or total bilirubin
minotransferase �40 IU/L
..................................................................................................................
ere preeclampsia and no concurrent
SEPTEMBER 2011
edical (eg, renal disease, insulin-de-endent diabetes, connective tissue dis-ase) or obstetric (eg, vaginal bleeding,remature rupture of membranes, mul-ifetal gestation, preterm labor) compli-ations at 28-32 weeks’ gestation. Thoseandomized to expectant managementelivered at a more advanced gesta-ional age (32.9 vs 30.8 weeks; P � .01),nd had newborns with higher birth-eights (1622 vs 1233 g; P � .01) who
equired less frequent neonatal intensiveare unit admission (76% vs 100%; P �01). Newborns from the expectantly
anaged group had less frequent respi-atory distress syndrome (22.4% vs 50%;� .002) and necrotizing enterocolitis
0% vs 10.9%; P � .02), but were morerequently small for gestational age atirth (30.1 vs 10.9; P � .04). There wereo cases of maternal eclampsia or pul-onary edema in either trial. Abruptio
lacentae was similar in frequency be-ween the randomized groups in bothtudies, but was more common in bothhe expectantly and nonexpectantly
anaged groups from the Odendaal etl19 trial (22% vs 15%) than in the Sibait al20 study (4.1% vs 4.3%). HELLP syn-
drome complicated only 2 expectantlymanaged cases and 1 aggressively man-aged case in the latter study (4.1% vs2.1%).
Two additional randomized trialsevaluated therapeutic interventions dur-ing expectant management. Fenakel etal21 described 49 women with severe pre-eclampsia at 26-36 weeks who were ran-domly assigned to receive either sublingualand oral nifedipine or intravenous and oralhydralazine treatments for severe hyper-tension during expectant management.Those assigned to nifedipine therapy deliv-ered more frequently at �36 weeks, wereless frequently diagnosed with acute fetaldistress, and their infants had a shortermean duration of neonatal intensive careunit stay than those assigned to hydral-azine therapy (P � .01 for each). How-ever, mean gestational age at delivery(34.6 vs 33.6 weeks; P � .20) and preg-nancy prolongation (15.5 vs 9.5 days;P � .07) were not improved, and no dif-ferences in the frequencies of “major” or“minor” newborn complications were
a,e11
mpre
speriar �estn �
ingw
�2h hy
om
100or
elod p
ria h
)ate
L
d)
ne a
.........
seen between groups. In multicenter

npe
OOahi
vapta
osmsn(sfdazclttf
pcchmd9n0(
www.AJOG.org SMFM Clinical Opinion
comparison of antihypertensive therapyalone vs antihypertensive therapy plusplasma volume expansion, Ganzevoortet al22 found that volume expansion gave
o additional benefit among women ex-ectantly managed with severe pre-clampsia at 24-33 weeks 6 days.
bservational studiesbservational studies regarding expect-
nt management of severe preeclampsiaave varied in their inclusion criteria and
ndications for delivery.5,7,10,18,23-35 Someincluded only those women who remainedstable after 24-48 hours of observation,while others included women expectantlymanaged from the time of diagnosis. A re-cent systematic review summarized thefrequency of complications related to se-vere preeclampsia remote from term.18
Presented as (median; interquartile range[IQR]), complications of expectant man-agement included: intensive care unit ad-mission (median, 27.6%; IQR, 1.5–52.6),hypotension (median, 17.0%; IQR, 12.0–21.0), HELLP syndrome (median, 11.0%;IQR, 5.3–17.6]), recurrent severe hyper-tension (median, 8.8%; IQR, 3.3–27.5),abruption placentae (median, 5.1%; IQR,2.2– 8.5), pulmonary edema (median,2.9%; IQR, 1.5–52.6), eclampsia (median,1.1%; IQR, 0–2.0), subcapsular liver he-matoma (median, 0.5%; IQR, 0.2–0.7),stroke (median, 0.4%; IQR, 0–3.1), still-birth (median, 2.5%; IQR, 0 –11.3), andneonatal death (median, 7.3%; IQR,5.0 –10.7). Small for gestational age in-fants were common (median, 36.8%;IQR, 20.5–53.8) after expectant manage-ment. Delivery for fetal (46%) or maternal(40%) indications was similarly frequent.
In summary, expectant managementof severe preeclampsia occurring �34weeks’ gestation aimed at increasing ges-tational age at delivery and birth weight,and decreasing neonatal complicationsis appropriate in selected cases, but care-ful in-hospital maternal and fetal sur-veillance are recommended.
What is the initial evaluation andmanagement of severe preeclampsia<34 completed weeks’ gestation?Women with suspected severe pre-eclampsia should be hospitalized to con-
firm the diagnosis, evaluate maternal sand fetal condition, and monitor forrapid progression of the disease. Duringthis initial assessment, intravenous mag-nesium sulfate seizure prophylaxis hasbeen suggested by some, and may beconsidered. Continuous fetal heart rateand uterine contraction monitoring areinitiated if there is an intention to inter-vene for fetal benefit. Maternal assess-ment should include evaluation of vitalsigns and physical examination with spe-cific attention for signs of preeclampsiaand its complications. Laboratory testsshould include at least a complete bloodcell count with platelet count, serum cre-atinine, and liver enzymes (aspartateaminotransferase, alanine aminotrans-ferase). Urinary protein or urinary totalprotein/creatinine ratio, to confirm thepresence of significant proteinuria, areoften evaluated from a random urinesample. However, because these tests donot reliably exclude significant protein-uria or accurately quantitate the amountof proteinuria, 24-hour urine collectionand analysis should generally be per-formed. Coagulation studies includingserum fibrinogen, prothrombin time,and partial thrombin time, and evaluationfor hemolysis (peripheral smear, serumbilirubin and/or lactate dehydrogenase)should be considered if the platelet count is�100,000/mm3, if liver enzymes are ele-ated, or if there are findings suggestive ofbruptio placentae. Ultrasound should beerformed to evaluate for fetal presenta-ion, evidence of growth restriction,nd/or oligohydramnios.
Women with persistent symptomsf severe preeclampsia, uncontrollableevere hypertension, eclampsia, pul-
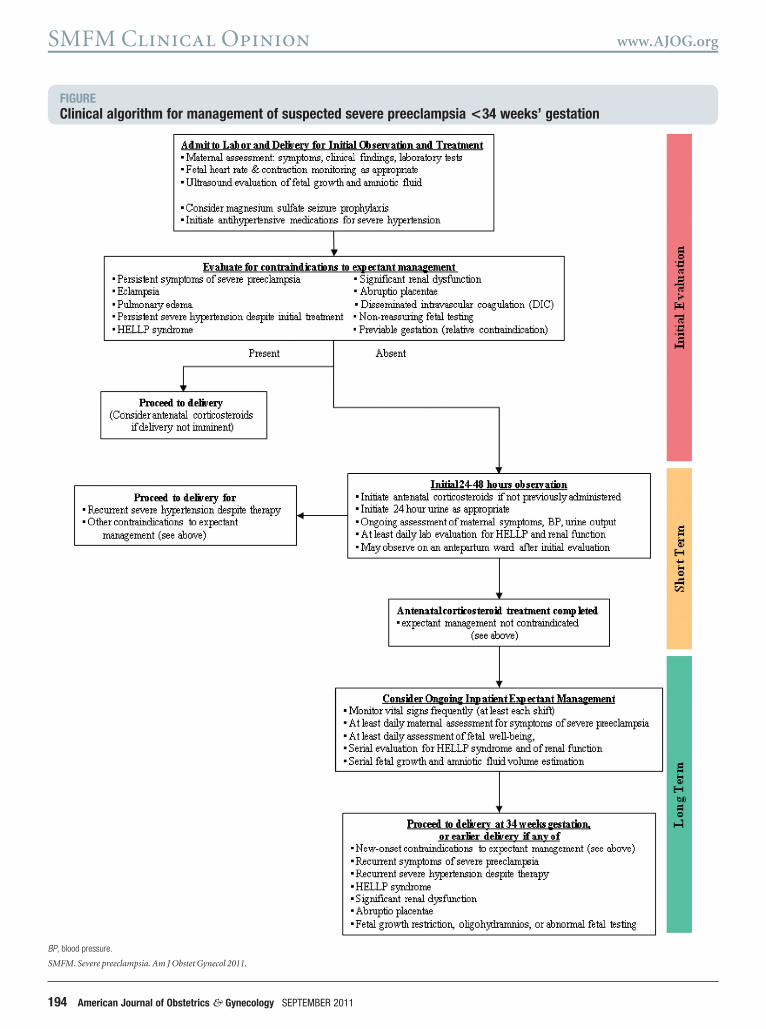
onary edema, abruptio placentae, dis-eminated intravascular coagulation, sig-ificant and new-onset renal dysfunctionserum creatinine �1.5 mg/dL), HELLPyndrome, and those who have abnormaletal surveillance results should typically beelivered (vaginal or cesarean delivery asppropriate) after initial maternal stabili-ation (Figure).10 The remainder may beandidates for short-term pregnancy pro-ongation to achieve the benefits of antena-al corticosteroid treatment, or for ex-ended pregnancy prolongation to allowetal growth and maturation. While data
pecific to expectantly managed severeSEPTEMBER 2011 Am
reeclampsia are limited, randomizedontrolled trials involving pregnanciesomplicated by hypertension syndromesave found antenatal corticosteroid treat-ent to result in less frequent respiratory
istress syndrome (risk ratio [RR], 0.50;5% confidence interval [CI], 0.35–0.72),eonatal death (RR, 0.50; 95% CI, 0.29–.87), and intraventricular hemorrhageRR, 0.38; 95% CI, 0.17–0.87).36 In a sin-
gle placebo-controlled study of weeklybetamethasone for women with severepreeclampsia between 26-34 weeks’ gesta-tion, treatment (mean exposure 1.7 doses)reduced the frequencies of respiratory dis-tress syndrome (RR, 0.53; 95% CI, 0.35–0.82) and intraventricular hemorrhage(RR, 0.35; 95% CI, 0.15–0.86), amongother complications.37 In this study, therewere 2 maternal deaths among 218pregnancies.
If not previously given, and if it is an-ticipated that there will be time for fetalbenefit from this intervention, antenatalcorticosteroid administration shouldbe considered regardless of a plan forexpectant management. Those who de-velop new-onset contraindications toexpectant management before or aftercompletion of antenatal corticosteroidtreatment should be delivered (Figure).If the maternal and fetal conditions re-main stable during initial inpatient mon-itoring, continued expectant manage-ment of women �34 weeks’ gestationalage is appropriate. Continuous fetalmonitoring, and magnesium sulfate sei-zure prophylaxis if initiated, can be dis-continued. Women with suspected fetalgrowth restriction and/or oligohydram-nios are not typically considered to becandidates for expectant managementbeyond completion of antenatal cortico-steroid therapy due to the increased riskof adverse outcomes including perinataldeath.5,17,20,22,26 Management in thesecases should be individualized and basedon the severity of fetal growth restriction,the presence of coexisting oligohydram-nios, and results of fetal surveillance. Forthe remaining women, the potential ma-ternal risks and perinatal benefits of con-tinued expectant management after an-tenatal corticosteroid treatment shouldbe determined after consideration of
clinical factors such as gestational age,erican Journal of Obstetrics & Gynecology 193
SMFM Clinical Opinion www.AJOG.org
FIGUREClinical algorithm for management of suspected severe preeclampsia <34 weeks’ gestation
BP, blood pressure.
SMFM. Severe preeclampsia. Am J Obstet Gynecol 2011.
194 American Journal of Obstetrics & Gynecology SEPTEMBER 2011

esumcmgttu
spp(hledtttcp
ddt
gef7(r4cls3s15f(d
www.AJOG.org SMFM Clinical Opinion
maternal status, and likelihood of signif-icant pregnancy prolongation.
Because of the potential for rapid deteri-oration of the maternal and/or fetal con-dition during expectant managementof severe preeclampsia, such womenare optimally cared for in a hospitalwith services capable of managing compli-cated obstetric cases and preterm new-borns.10 Maternal evaluation should in-clude monitoring of blood pressure, urineoutput, and signs or symptoms of concern(persistent headache, visual changes, epi-gastric pain, abdominal tenderness, orvaginal bleeding). The frequency and na-ture of fetal monitoring should be basedon gestational age and fetal status. Dur-ing initial expectant management, atleast daily assessment of the completeblood cell count with platelet count, aswell as liver and renal functions can helpidentify those in whom the disease isprogressing and requires delivery. Eval-uation of maternal coagulation parame-ters is not typically necessary. The fre-quency of subsequent laboratory testingcan be determined based on the severity ofillness and disease progression. Uric acidlevels and changes in urinary protein con-centrations do not reliably predict adversematernal or perinatal outcomes and there-fore serial measurement offers little clinicalbenefit.38-41 Depending on the duration ofxpectant management, follow-up ultra-ound examination for fetal growth eval-ation and amniotic fluid volume esti-ation should also be performed. If
ontraindications to expectant manage-ent are not encountered by 34 weeks of
estation, delivery should be initiated athat time because of the ongoing risks tohe mother and fetal risks during contin-ed expectant management.
Should severe proteinuria alterthe approach to managementof severe preeclampsia?The presence of severe proteinuria inwomen with severe preeclampsia under-going expectant management is not as-sociated with worse outcomes. In onestudy of 42 expectantly managed womenwith severe proteinuria (defined as �5g/24 h), significant pregnancy prolonga-tion occurred, maternal complications
were not increased, and resolution of re- snal dysfunction occurred in all womenby 3 months after delivery.23 A secondtudy categorized women with severereeclampsia according to the severity ofroteinuria as mild (�5 g/24 h), severe5-9.9 g/24 h), or massive (�10 g/24).41 No differences in the rates of ec-
ampsia, abruptio placentae, pulmonarydema, HELLP syndrome, neonataleath, or neonatal morbidity were iden-ified between these groups. Althoughhe amount of proteinuria increases overime with expectant management, thishange is not predictive of pregnancyrolongation or perinatal outcomes.39
On the basis of these data, severe pro-teinuria alone and the degree of changein proteinuria should not be consideredcriteria to avoid or terminate expectantmanagement.
Should expectant managementbe offered when HELLPsyndrome is present?Women with HELLP syndrome havebeen excluded from most publishedstudies of expectantly managed pretermsevere preeclampsia as these abnormali-ties are generally considered to be indi-cations for delivery.10,19,20 Further, the
iagnostic criteria used for HELLP syn-rome have varied between publica-ions.42 In a systematic review of 12 stud-
ies, Magee et al18 evaluated the frequencyof complications that can occur when ex-pectant management is undertaken in thesetting of HELLP syndrome �34 weeks’estation. Median [IQR] latency to deliv-ry was 5.8 days [0.8–10.3] and delivery foretal indication was common (median,0.8%; IQR, 53.9–89.0). Complicationsmedian [interquartile range]) includedecurrent severe hypertension (median,6.2%; IQR, 33.6–58.8), abruptio pla-entae (median, 5.1%; IQR, 3.3–6.4), ec-ampsia (median, 0.8%; IQR, 0 – 4.9),ubcapsular liver hematoma (median,.1%; IQR, 1.6 – 4.7), stroke (6.3%),tillbirth (median, 10.5%; IQR, 3.4 –9.1), and neonatal death (median,.5%; IQR, 4.3– 8.9). Delivery of a smallor gestational age infant was common56.3%). Maternal death has also occurreduring expectant management of HELLP
yndrome.43SEPTEMBER 2011 Am
A recent metaanalysis of 11 trials eval-uated the impact of antenatal maternalcorticosteroid treatment on perinataloutcomes during expectant manage-ment of HELLP.44 This systematic re-view found improved maternal plateletcounts when corticosteroids are given,but there was no evidence of improve-ments in maternal mortality, severe ma-ternal morbidities, or perinatal/infantdeaths.
Given current evidence of brief latencyand maternal risk without demonstratedfetal benefits, women with HELLP syn-drome should not typically be managedexpectantly, and vaginal or cesarean de-livery should be pursued as appropriate.Antenatal corticosteroid administrationmay be given concurrently, if it is antic-ipated that there will be adequate timefor fetal benefit from treatment, but therisk of surgical complications in the settingof thrombocytopenia should be consid-ered. If delivery is delayed for antenatalcorticosteroid administration (eg, for pa-tients with incomplete findings of HELLPsyndrome), magnesium sulfate seizureprophylaxis should be continued and con-tinuous fetal monitoring should be per-formed because of the potential for ec-lampsia and fetal death. Delivery should bepursued if the maternal or fetal conditionworsens, or upon completion of thistreatment.5,10,20,21,27
Should expectant managementbe offered when fetal growthrestriction is suspected?While no prospective trials have evalu-ated the benefits and risks of expectantmanagement when fetal growth restric-tion is suspected in the setting of pretermsevere preeclampsia, 2 retrospective obser-vational studies have described outcomesfor such pregnancies.22,26 In one study ofvolume expansion during expectant man-agement of severe preeclampsia, thosewith suspected fetal growth restriction(defined as ultrasound estimated weight�10th percentile or abdominal circumfer-ence �5th percentile) had a median preg-nancy prolongation of 7 days, and the fre-quency of adverse outcome (perinataldeath, chronic lung disease, grade �3 in-traventricular hemorrhage, or grade �2
periventricular leukomalacia) for thiserican Journal of Obstetrics & Gynecology 195

sswwbwtmwTetseegstTai
lhamrad(ha�g
pomsei
ttam
tctmcm
dediprtmudadilt�3
SMFM Clinical Opinion www.AJOG.org
group was similar to the overall cohort.22 Aecond study compared 14 women withevere preeclampsia and estimated fetaleight �10th percentile with 33 womenithout fetal growth restriction.26 Onlyrief pregnancy prolongation (3.1 days)as seen with expectant management, and
he incidences of abruption and neonatalorbidities were similar between thoseith or without fetal growth restriction.hese investigators recommended deliv-ry after antenatal corticosteroid adminis-ration in such cases. While publishedtudies fail to demonstrate benefits fromxpectant management of severe pre-clampsia with concurrent suspected fetalrowth restriction, the number of subjectstudied is small and there is a wide spec-rum of severity of fetal growth restriction.he decision regarding expectant man-gement of these patients should bendividualized.
Should severe preeclampsiaoccurring before the limit of viabilitybe treated expectantly?Severe preeclampsia that develops near theimit of fetal viability is associated with aigh likelihood of perinatal morbiditiesnd mortality, regardless of expectantanagement.5,7,8,31,33,45-50 However, data
egarding outcomes with expectant man-gement categorized by gestational week atiagnosis are limited. Survival rates of 0/340%), 4/22 (18.2%), and 15/26 (57.7%)ave been reported after expectant man-gement of severe preeclampsia initiated23 weeks’, at 23 weeks’, and at 24 weeks’
estation, respectively.5,31,49,50 Other re-ports have also suggested rare survival withexpectant management of severe pre-eclampsia�23-24 weeks’ gestation.7,48 Ex-
licit counseling regarding the likelihoodf poor perinatal outcomes with expectantanagement should be provided. Delivery
hould be considered when severe pre-clampsia occurs before the limit of viabil-ty (Figure).5,7,10,31,48-50
What is the role of antihypertensivetherapy during expectantmanagement?In women with severe preeclampsia,control of maternal blood pressure isnecessary to decrease the risks of acute
hypertension (eg, maternal cerebrovas-196 American Journal of Obstetrics & Gynecology
cular accident, myocardial ischemia),but a dramatic decrease may also impairuteroplacental perfusion. Antihyperten-sive medications should be considered ifsystolic blood pressure remains persis-tently �160 mm Hg, or if diastolic bloodpressure persists �110 mm Hg.10 Oncereated, the target range should be a sys-olic blood pressure of 140-155 mm Hgnd a diastolic blood pressure of 90-105m Hg.Although parenteral antihypertensive
herapy may be needed initially for acuteontrol of blood pressure, oral medica-ions can be utilized as expectant manage-
ent is continued. Oral labetalol andalcium channel blockers have been com-only used.10 One approach is to begin an
initial regimen of labetalol at 200 mg orallyevery 12 hours, and increase the dose up to800 mg orally every 8-12 hours as needed(maximum total 2400 mg/d). If the maxi-mum dose is inadequate to achieve the de-sired blood pressure goal, then short-act-ing oral nifedipine can be added at aninitial dose of 10 mg orally every 6 hoursand increased as needed up to 20 mg every4 hours (40-120 mg/d). An alternativeregimen is a long-acting preparation of ni-fedipine (up to 30-60 mg/d). Follow-ing initial control ofsevere hypertension,blood pressure should be measured at leastevery 6-8 hours. If there is recurrent persis-tent severe hypertension despite adequateoral or intravenous antihypertensive ther-apy, delivery should be pursued after ma-ternal stabilization.
What strategies are available for fetalassessment during expectantmanagement?No randomized trials have identified anoptimal method of fetal assessment dur-ing expectant management of severe pre-eclampsia, however there is agreementthat fetal testing is indicated if the preg-nancy is considered viable.5,19-33 Non-stress testing (NST) is recommended,but the optimal frequency of testing andthe additional value of biophysical pro-file testing have not been determined.One approach for fetal surveillance in-volves at least daily NSTs, with biophysi-cal profile testing performed should a non-reactive NST result be encountered.
Follow-up fetal growth evaluation andSEPTEMBER 2011
amniotic fluid volume estimation shouldalso be performed. If fetal growth restric-tion is suspected, and expectant man-agement is undertaken, then incorpo-ration of Doppler blood flow studiesinto an individualized managementscheme is appropriate.
What are the indications for deliveryafter expectant management?In the published studies of preterm se-vere preeclampsia managed expectantly,delivery has typically been pursued at ap-proximately 34 completed weeks’ gesta-tion. However, deterioration of maternaland/or fetal conditions prior to this ges-tational age is the most common reasonfor delivery.18 Maternal indications for
elivery are delineated in Figure. Deliv-ry should also be considered for womeneclining or noncompliant to ongoing
npatient observation; those developingersistent epigastric or right upper quad-ant pain, nausea, or vomiting; and forhose who develop preterm labor or pre-
ature rupture of membranes (Fig-re).5,11,12,19,20,26-33 When delivery is in-icated, vaginal delivery can often beccomplished, but this is less likely withecreasing gestational age. With labor
nduction, the likelihood of cesarean de-ivery increases with decreasing gesta-ional age in this setting (range, 93–97%
28 weeks’, 53–65% at 28-32 weeks’, and1–38% at 32-34 weeks’ gestation).51-54
RECOMMENDATIONS
Levels I and II evidence,level A recommendation1. Expectant management of severe pre-
eclampsia remote from term is appro-priate in selected cases, and is associatedwith pregnancy prolongation and im-proved newborn outcomes.
Levels II and III evidence,level B recommendation2. Women with persistent symptoms of
severe preeclampsia, uncontrollable se-vere hypertension, eclampsia, pulmo-nary edema, abruptio placentae, dis-seminated intravascular coagulation,significant and new-onset renal dys-function, and those who have abnor-
mal fetal surveillance results, should
Ll3
Ll4
Ll5
Ll6
Ll7
Ll8
www.AJOG.org SMFM Clinical Opinion
typically be delivered after initial mater-nal stabilization.
evel I evidence,evel A recommendation. If not previously given, and if it is an-
ticipated that there will be time for fe-tal benefit from this intervention be-fore delivery, antenatal corticosteroidadministration should be consideredregardless of a plan for expectantmanagement.
evel III evidence,evel C recommendation. Because of the ongoing risks to the
mother and fetal risks during contin-ued expectant management, deliveryfor severe preeclampsia should be un-dertaken at 34 weeks’ gestation forthose who remain pregnant to this ges-
Quality of evidence
The quality of evidence for each includedarticle was evaluated according to thecategories outlined by the USPreventative Services Task Force:
I Properly powered and conductedrandomized controlled trial; well-conducted systematic review ormetaanalysis of homogeneous ran-domized controlled trials.
.........................................................................................................
II-1 Well-designed controlled trial withoutrandomization.
.........................................................................................................
II-2 Well-designed cohort or case-controlanalytic study.
.........................................................................................................
II-3 Multiple time series with or withoutthe intervention; dramatic resultsfrom uncontrolled experiments.
.........................................................................................................
III Opinions of respected authorities,based on clinical experience; descrip-tive studies or case reports; reports ofexpert committees.
Recommendations are gradedin the following categories:
Level AThe recommendation is based on good andconsistent scientific evidence.
Level BThe recommendation is based on limited orinconsistent scientific evidence.
Level CThe recommendation is based on expertopinion or consensus.
tational age.
evel II evidence,evel A recommendation. Severe proteinuria alone and the de-
gree of change in proteinuria shouldnot be considered criteria to avoid orterminate expectant management.
evels I and II evidence,evel A recommendation. Women with HELLP syndrome should
not typically be managed expectantly.Vaginal or cesarean delivery shouldbe pursued as appropriate.
evel II and III evidence,evel B recommendation. The decision regarding expectant man-
agement of severe preeclampsia withconcurrent suspected fetal growth re-striction should be individualized.
evels I and II evidence,evel B recommendation. Explicit counseling regarding the po-
tential maternal risks should be pro-vided and delivery should be consid-ered when severe preeclampsia occursbefore the limit of viability. f
This opinion was developed by the PublicationsCommittee of the Society for Maternal-FetalMedicine with the assistance of Baha M. Sibai,MD, and was approved by the executive com-mittee of the society on June 30, 2011. Dr Sibaiand each member of the publications commit-tee (Brian Mercer, MD [Chair], Vincenzo Ber-ghella, MD, Sean Blackwell, MD, Joshua Copel,MD, William Grobman, MD, MBA, Cynthia Gy-amfi, MD, Donna Johnson, MD, Sarah Kilpat-rick, MD, PhD, George Macones, MD, GeorgeSaade, MD, Hyagriv Simhan, MD, Lynn Simp-son, MD, Joanne Stone, MD, Michael Varner,MD, Ms Deborah Gardner) have submitted aconflict of interest disclosure delineating per-sonal, professional, and/or business intereststhat might be perceived as a real or potentialconflict of interest in relation to this publication.
REFERENCES1. Sibai B, Dekker G, Kupfermic M. Preeclamp-sia. Lancet 2005;365:785-99. Level III.2. Kuklina EV, Aya C, Callaghan WM. Hyperten-sive disorders and severe obstetric morbidity inthe United States. Obstet Gynecol 2009;113:1299-306. Level II-3.3. Catov JM, Ness RB, Kip KE, Olsen J. Risk ofearly or severe preeclampsia related to preex-isting conditions. Int J Epidemiol 2007;36:412-9. Level II-3.4. Zhang J, Meikle S, Trumble A. Severe mater-
nal morbidity associated with hypertensive dis-SEPTEMBER 2011 Am
orders in pregnancy in the United States.Hypertens Pregnancy 2003;22:203-12. LevelII-3.5. Haddad B, Deis S, Goffinet F, Daniel BJ, Ca-brol D, Sibai BM. Maternal and perinatal out-comes during expectant management of 239severe preeclamptic women between 24 and33 weeks’ gestation. Am J Obstet Gynecol2004;190:1590-5. Level II-2.6. Gupta LM, Gaston L, Chauhan SP. Detec-tion of fetal growth restriction with pretermsevere preeclampsia: experience at two ter-tiary centers. Am J Perinatol 2008;25:247-9.Level II-3.7. Sibai BM, Akl S, Fairlie F, Moretti M. A proto-col for managing severe preeclampsia in thesecond trimester. Am J Obstet Gynecol 1990;163:733-8. Level II-2.8. Visser W, Wallenburg HCS. Maternal andperinatal outcome of temporizing managementin 254 consecutive patients with severe pre-eclampsia remote from term. Eur J Obstet Gy-necol Reprod Biol 1995;63:147-54. Level II-2.9. Vigil-DeGarcia P, Montufar-Rueda C, Ruiz J.Expectant management of severe preeclamp-sia between 24 and 34 weeks’ gestation. Eur JObstet Gynecol Reprod Biol 2003;107:24-7.Level II-2.10. Sibai BM, Barton JR. Expectant manage-ment of severe preeclampsia remote from term:patient selection, treatment, and delivery indi-cations. Am J Obstet Gynecol 2007;196:514e1-9. Level II-2.11. Report of the National High Blood PressureEducation Program. Working group report onhigh blood pressure in pregnancy. Am J ObstetGynecol 2000;183:S1-22. Level III.12. American College of Obstetricians and Gy-necologists. Diagnosis and management ofpreeclampsia and eclampsia: ACOG practicebulletin no. 33. Obstet Gynecol 2002;99:159-67. Level III.13. Sibai BM, Ramadan MK, Usta I, Salama M,Mercer BM, Friedman SA. Maternal morbidityand mortality in 442 pregnancies with hemoly-sis, elevated liver enzymes, and low platelets(HELLP syndrome). Am J Obstet Gynecol1993;169:1000-6. Level III.14. Martin JN Jr, Blake PG, Perry KG, McCaulJF, Hess LW, Martin RW. The natural history ofHELLP syndrome: patterns of disease progres-sion and regression. Am J Obstet Gynecol1991;164:1500-9. Level III.15. Magnussen EB, Vatlen LJ, Lund-Nilsen TI,et al. Pregnancy cardiovascular risk factors aspredictors of preeclampsia: population basedcohort study. BMJ 2007;335:978-81. LevelII-2.16. Lykke A, Langoff-Ross J, Sibai BM, et al.Hypertensive pregnancy disorders and subse-quent cardiovascular morbidity and type 2 dia-betes mellitus in the mother. Hypertension2009;53:944-51. Level II-2.17. Schiff E, Friedman SA, Sibai BM. Conser-vative management of severe preeclampsia re-mote from term. Obstet Gynecol 1994;84:
626-30. Level III.erican Journal of Obstetrics & Gynecology 197

ataI3efE13pvp3Nawn3rwb3sts3acr3ice14UaI4ecG4meO4AdpHs
4DldR4ae84am14ptn4WpbrB4Csw25EsM5dlA5ebO5epM5ieeO
SMFM Clinical Opinion www.AJOG.org
18. Magee LA, Yong PJ, Espinosa V, Côté AM,Chen I, von Dadelszen P. Expectant manage-ment of severe preeclampsia remote from term:a structured systematic review. HypertensPregnancy 2009;28:312-47. Level I.19. Odendaal HJ, Pattinson RC, Bam R, GroveD, Kotze TJ. Aggressive or expectant manage-ment for patients with severe preeclampsia be-tween 28-34 weeks’ gestation: a randomizedcontrolled trial. Obstet Gynecol 1990;76:1070-5. Level I.20. Sibai BM, Mercer BM, Schiff E, FriedmanSA. Aggressive versus expectant managementof severe preeclampsia at 28 to 32 weeks’ ges-tation: a randomized controlled trial. Am J Ob-stet Gynecol 1994;171:818-22. Level I.21. Fenakel K, Kenakel G, Appleman Z, et al.Nifedipine in treatment of severe preeclampsia.Obstet Gynecol 1991;77:331-7. Level I.22. Ganzevoort W, Rep A, Bousel GJ, et al. Arandomized controlled trial comparing two tem-porizing management strategies, one with andone without plasma volume expansion, for se-vere preeclampsia. BJOG 2005;112:1358-68.Level I.23. Chua S, Redman CW. Prognosis for pre-eclampsia complicated by 5 g or more of pro-teinuria in 24 hours. Eur J Obstet Gynecol Re-prod Biol 1992;43:9-12. Level II-3.24. Olah KS, Redman WG, Gee H. Manage-ment of severe, early pre-eclampsia: is conser-vative management justified? Eur J Obstet Gy-necol Reprod Biol 1993;51:175-80. Level II-2.25. van Pampus MG, Wolf H, Westenberg SM,der Post V, Bonsel GJ, Treffers PE. Maternaland perinatal outcome after expectant manage-ment of HELLP syndrome compared with pre-eclampsia without HELLP syndrome. Eur J Ob-stet Gynecol Reprod Biol 1998;76:31-6. LevelII-2.26. Chammas MF, Nguyen TM, Li MA, Nuway-hid BS, Castro LC. Expectant management ofsevere preterm preeclampsia: is intrauterinegrowth restriction an indication for immediatedelivery? Am J Obstet Gynecol 2000;183:853-8. Level II-3.27. Hall DR, Odendaal HJ, Steyn DW, Grove D.Expectant management of early onset, severepreeclampsia; maternal outcome. Br J ObstetGynaecol 2000;107:1252-7. Level II-3.28. Hall DR, Odendaal HJ, Kristen GF, Smith J,Grove D. Expectant management of early onset,severe preeclampsia: perinatal outcome. Br J Ob-stet Gynaecol 2000;107:1258-64. Level II-3.29. Shear RM, Rinfret D, Leduc L. Should weoffer expectant management in cases of severepreterm preeclampsia with fetal growth restric-tion? Am J Obstet Gynecol 2005;192:1119-25.Level II-3.30. Oettle C, Hall D, Roux A, Grove D. Earlyonset severe preeclampsia: expectant man-agement at a secondary hospital in close asso-ciation with a tertiary institution. BJOG 2005;
112:84-8. Level II-3. L198 American Journal of Obstetrics & Gynecology
31. Bombrys AE, Barton JR, Nowacki E, HabliM, Sibai BM. Expectant management of severepreeclampsia at �27 weeks’ gestation: mater-nal and perinatal outcomes according to gesta-tional age by weeks at onset of expectant man-agement. Am J Obstet Gynecol 2008;199:247.e1-6. Level II-2.32. Bombrys AE, Barton JR, Habli M, Sibai BM.Expectant management of severe preeclamp-sia at 270/7-336/7 weeks’ gestation: maternalnd perinatal outcomes according to gesta-ional age by weeks at onset of expectant man-gement. Am J Perinatol 2009;26:441-6. Level
I-3.3. Hall DR, Grove D, Carstens E. Early-pre-clampsia: what proportion of women qualifyor expectant management and if not, why not?ur J Obstet Gynecol Reprod Biol 2006;128:69-74. Level II-3.4. Sarsam DS, Shamden M, Al Wazan R. Ex-ectant versus aggressive management in se-ere preeclampsia remote from term. Singa-ore Med J 2008;49:698-703. Level II-1.5. Abdel-Hady el-S, Fawzy M, El-Negeri M,ezar M, Ragab A, Helal AS. Is expectant man-gement of early-onset severe preeclampsiaorthwhile in low-resource settings? Arch Gy-ecol Obstet 2010;282:23-7. Level II-2.6. Roberts D, Dalziel SR. Antenatal corticoste-oids for accelerating fetal lung maturation foromen at risk of preterm birth. Cochrane Data-ase Syst Rev 2006;3:CD004454. Level I.7. Amorim MM, Santos LC, Faundes A. Cortico-teroid therapy for prevention of respiratory dis-ress syndrome in severe preeclampsia. Am J Ob-tet Gynecol 1999;180:1283-8. Level I.8. Thangaratinam S, Ismail KMK, Sharp S, etl. Accuracy of serum uric acid in predictingomplications of pre-eclampsia: a systematiceview. BJOG 2006;113:369-78. Level I.9. Schiff E, Friedman SA, Kao L, Sibai BM. The
mportance of urinary protein excretion duringonservative management of severe pre-clampsia. Am J Obstet Gynecol 1996;175:313-6. Level II-3.0. Hall DR, Odendaal HJ, Stein DW, Grive D.rinary protein excretion and expectant man-gement of early onset, severe preeclampsia.
nt J Gynaecol Obstet 2002;77:1-6. Level II-3.1. Newman MG, Robichaux AG, Stedman CM,t al. Perinatal outcomes in preeclampsia that isomplicated by massive proteinuria. Am J Obstetynecol 2003;188:264-8. Level II-3.2. Sibai BM. Diagnosis, controversies, andanagement of the syndrome of hemolysis, el-
vated liver enzymes, and low platelet count.bstet Gynecol 2004;103:981-91. Level II-2.3. van Runnard Heimel PJ, Huisjes AJM, Fraux, Koopman C, Bots ML, Bruinse HW. A ran-omized placebo-controlled trial of prolongedrednisolone administration to patients withELLP syndrome remote from term. Eur J Ob-tet Gynecol Reprod Biol 2006;128:187-93.
evel I.SEPTEMBER 2011
4. Woudstra DM, Chandra S, Hofmeyr GJ,owswell T. Corticosteroids for HELLP (hemo-
ysis, elevated liver enzymes, low platelets) syn-rome in pregnancy. Cochrane Database Systev 2010;9:CD008148. Level I.5. Moodley J, Koranteng SA, Rout C. Expect-nt management of early onset of severe pre-clampsia in Durban. S Afr Med J 1993;3:584-7. Level II-3.6. Hall DR, Odendaal HJ, Steyn DW. Expect-nt management of severe pre-eclampsia in theid-trimester. Eur J Obstet Gynecol 2001;96:68-72. Level II-3.7. Jenkins SM, Head BB, Hauth JC. Severereeclampsia at �25 weeks of gestation: ma-ernal and neonatal outcomes. Am J Obstet Gy-ecol 2002;186:790-5. Level II-3.8. Gaugler-Senden IPM, Huijssoon AG, Visser, Steegers EAP, deGroot CJM. Maternal and
erinatal outcome of preeclampsia with onsetefore 24 weeks’ gestation: audit in a tertiaryeferral center. Eur J Obstet Gynecol Reprodiol 2006;128:216-21. Level II-3.9. Budden A, Wilkinson L, Buksh MJ, Mc-owan L. Pregnancy outcome in women pre-enting with pre-eclampsia at less than 25eeks’ gestation. Aust N Z J Obstet Gynaecol006;46:407-12. Level II-3.0. Sezik M, Ozkaya O, Sezik HT, Yapar EG.xpectant management of severe preeclamp-ia presenting before 25 weeks of gestation.ed Sci Monit 2007;13:523-7. Level II-3.1. Nassar AH, Adra AA, Chakhtoura N, Bey-oun S. Severe preeclampsia remote from term:
abor induction or elective cesarean delivery?m J Obstet Gynecol 1998;179:1210-3. Level III.2. Alexander JM, Bloom SL, McIntire DD, Lev-no KJ. Severe preeclampsia and the very-lowirth weight infant: is induction of labor harmful?bstet Gynecol 1999;93:485-8. Level III.3. Blackwell SC, Redman ME, Tomlinson M,t al. Labor induction for the preterm severere-eclamptic patient: is it worth the effort? Jatern Fetal Med 2001;10:305-11. Level III.4. Alanis MC, Robinson CJ, Hulsey TC, Ebel-
ng M, Johnson DJ. Early-onset severe pre-clampsia: induction of labor vs elective cesar-an delivery and neonatal outcomes. Am Jbstet Gynecol 2008;199:262.e1-6. Level II-3.
The practice of medicine continues toevolve, and individual circumstances willvary. This opinion reflects informationavailable at the time of its submission forpublication and is neither designed norintended to establish an exclusive stan-dard of perinatal care. This publication isnot expected to reflect the opinions of allmembers of the Society for Maternal-Fetal Medicine.





























