Embed Size (px)
Citation preview
Evaluating the GERD Patient – Minimum to Maximum
Blair A. Jobe, MD
Professor of Surgery
Department of Surgery
University of Pittsburgh
Pittsburgh, Pennsylvania
Failure of Antireflux Surgery
“It is well recognized that inadequate or inaccurate preoperative evaluation can be a major contributor to a poor outcome following antireflux surgery”
Gastrointest Endoscopy Clin N Am 2005;15:347
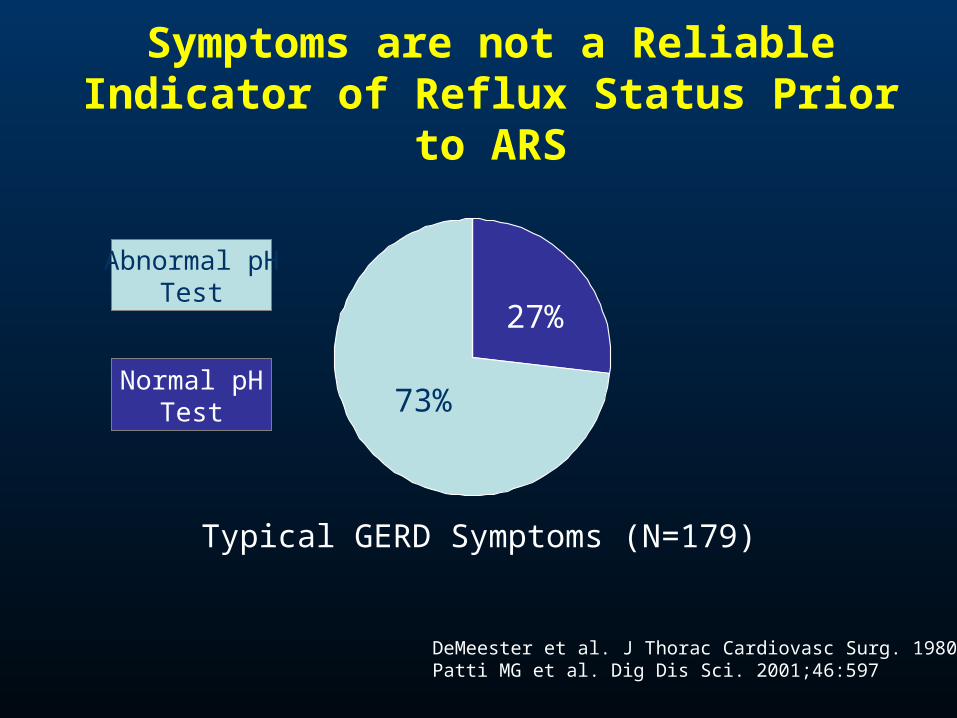
Symptoms are not a Reliable Indicator of Reflux Status Prior to ARS
DeMeester et al. J Thorac Cardiovasc Surg. 1980;79:656Patti MG et al. Dig Dis Sci. 2001;46:597
73%
27%
Typical GERD Symptoms (N=179)
Normal pHTest
Abnormal pHTest
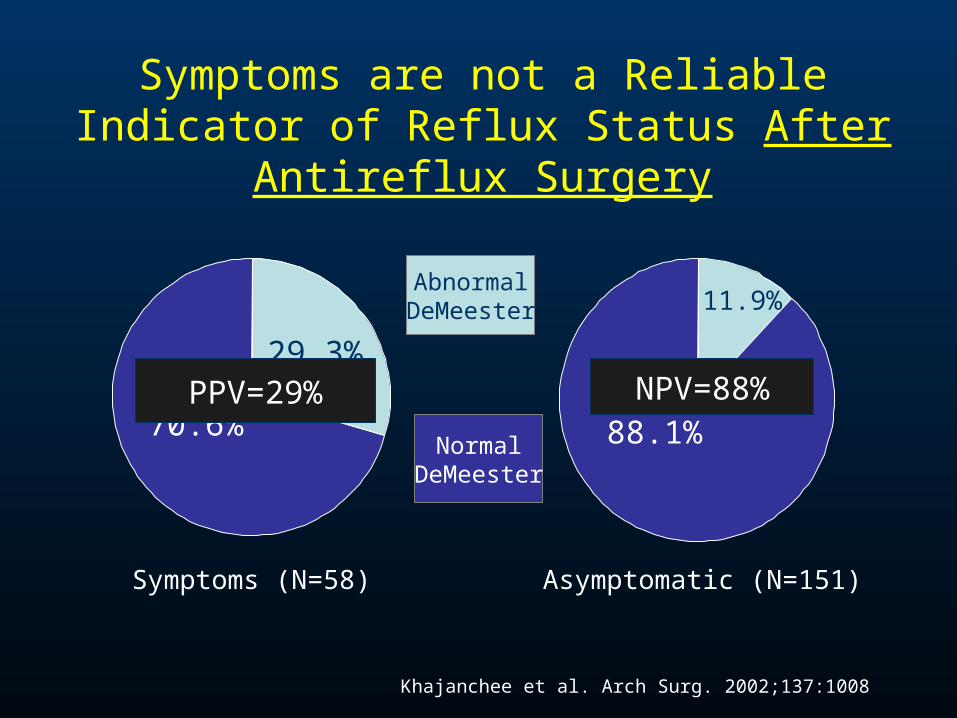
Symptoms are not a Reliable Indicator of Reflux Status After Antireflux Surgery
Symptoms (N=58) Asymptomatic (N=151)
29.3%
70.6%
11.9%
88.1%
AbnormalDeMeester
NormalDeMeester
Khajanchee et al. Arch Surg. 2002;137:1008
PPV=29% NPV=88%
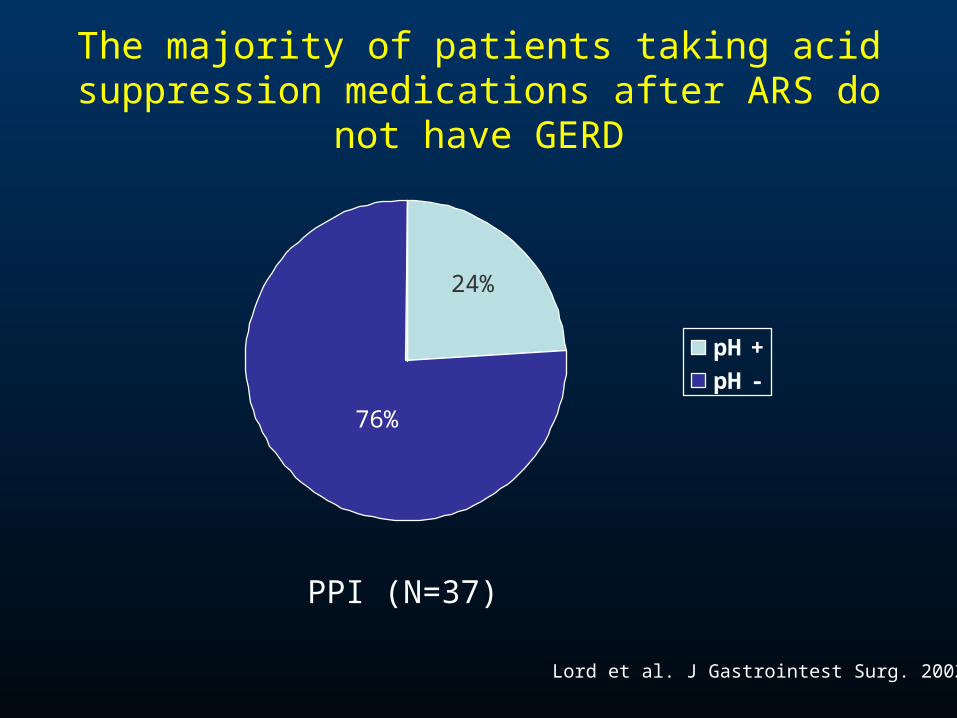
The majority of patients taking acid suppression medications after ARS do not have GERD
PPI (N=37)
Lord et al. J Gastrointest Surg. 2002;6:3
pH +
pH -
76%
24%
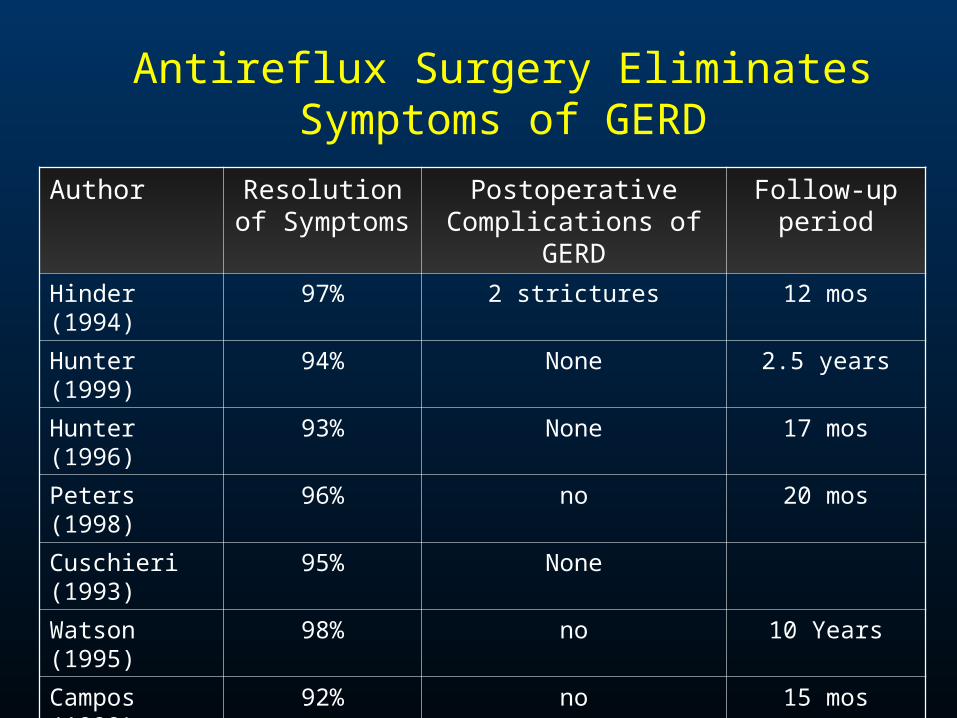
Antireflux Surgery Eliminates Symptoms of GERD
Author Resolution of Symptoms
Postoperative Complications of GERD
Follow-up period
Hinder (1994) 97% 2 strictures 12 mos
Hunter (1999) 94% None 2.5 years
Hunter (1996) 93% None 17 mos
Peters (1998) 96% no 20 mos
Cuschieri (1993)
95% None
Watson (1995) 98% no 10 Years
Campos (1999) 92% no 15 mos
Lundell
(2001)
95% Minimal esophagitis 5 Years
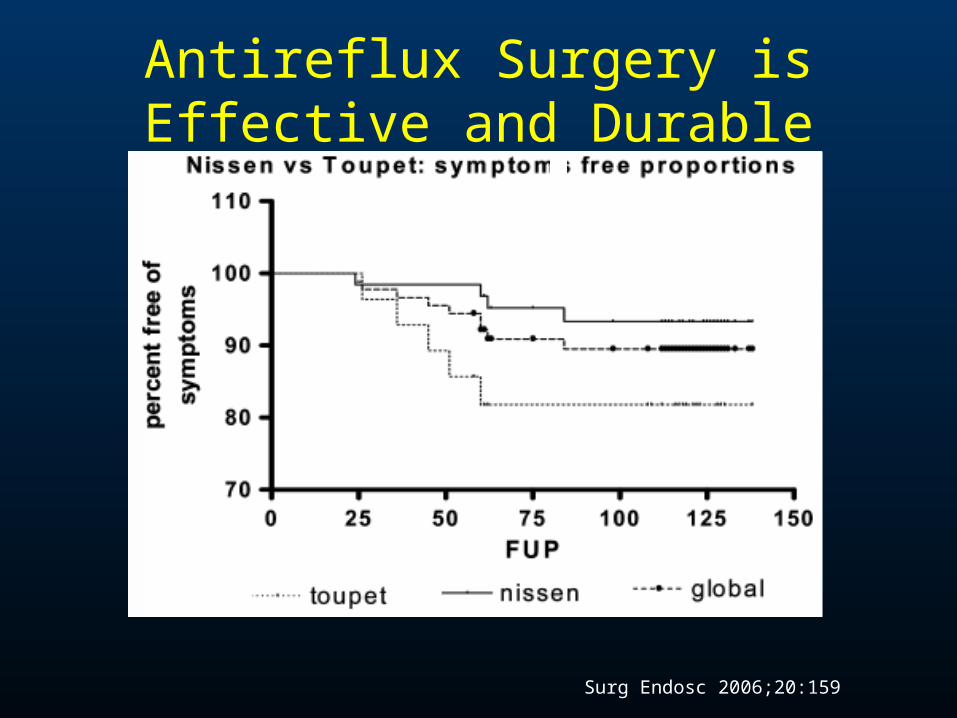
Antireflux Surgery is Effective and Durable
Surg Endosc 2006;20:159
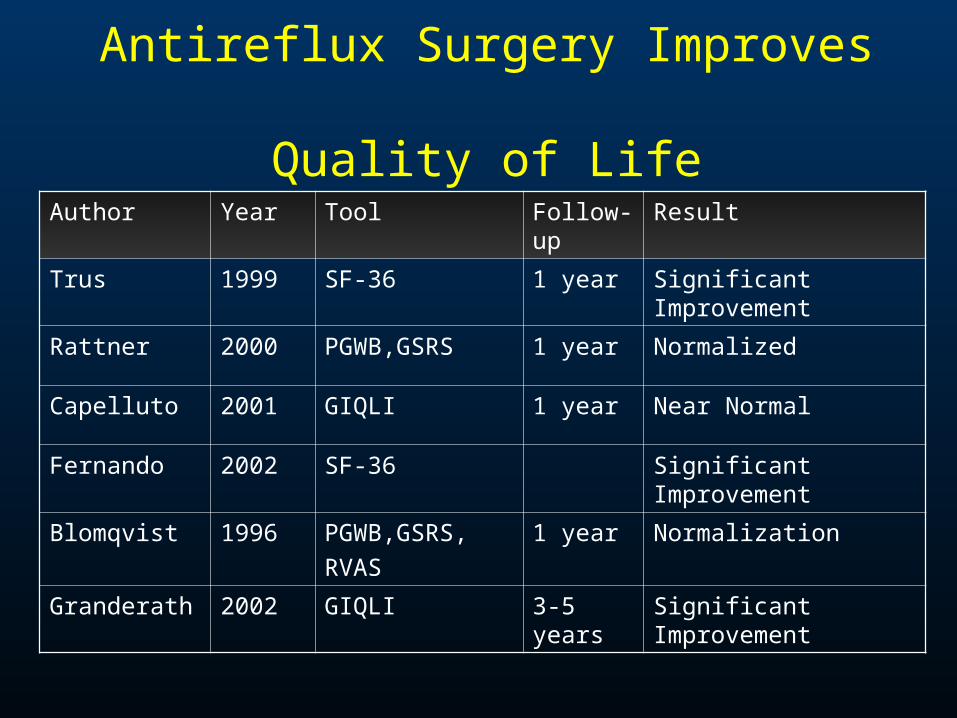
Antireflux Surgery Improves Quality of Life
Author Year Tool Follow-up
Result
Trus 1999 SF-36 1 year Significant Improvement
Rattner 2000 PGWB,GSRS 1 year Normalized
Capelluto 2001 GIQLI 1 year Near Normal
Fernando 2002 SF-36 Significant Improvement
Blomqvist 1996 PGWB,GSRS,
RVAS
1 year Normalization
Granderath 2002 GIQLI 3-5 years Significant Improvement
Success in Antireflux Surgery:What is Essential?
1. Patient Selection
2. Patient Selection
3. Patient Selection
4. Surgeon Training
5. Procedure Tailoring– Wrap type, length, tightness
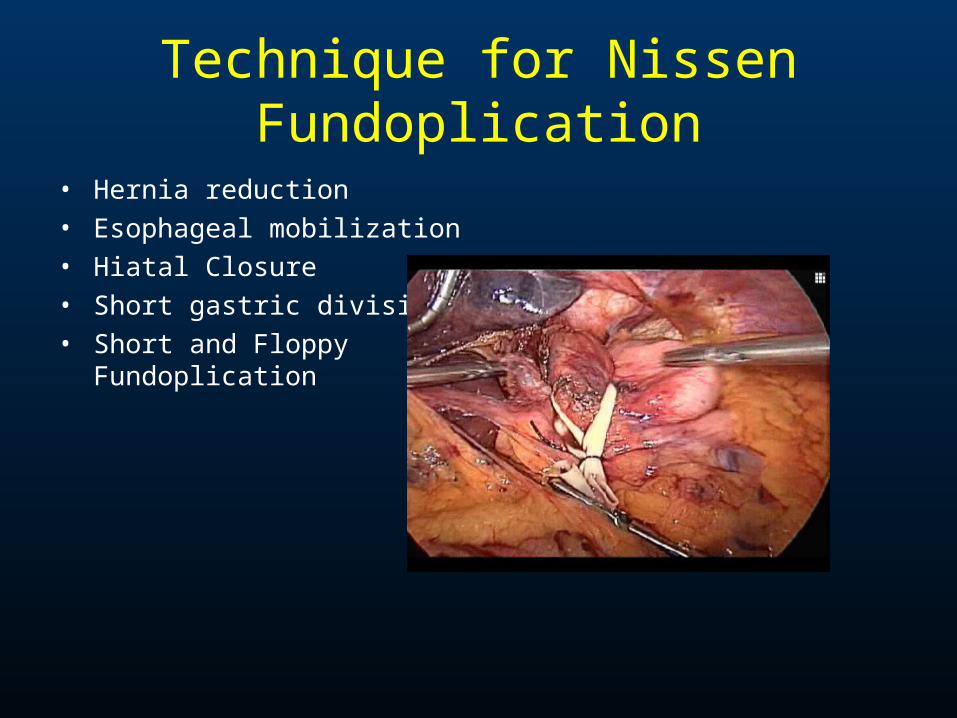
Technique for Nissen Fundoplication
• Hernia reduction• Esophageal mobilization• Hiatal Closure• Short gastric division• Short and Floppy
Fundoplication
Goals in Workup• Query GERD-related symptoms• Assess co-morbid conditions as they
relate to surgery• Objectify GERD• Identify anatomic abnormalities• Identify functional abnormalities• Set expectations with patient• Pick procedure (complete fundoplication)
Gastrointest Endoscopy Clin N Am 2005;15:347
The History and Expectation Setting
• Typical vs. atypical symptoms• R/O non-GERD causes of atypical symptoms• Primary and secondary symptoms• Response to medical therapy• Associated symptoms
– Bloating, emesis, nausea
• Eating disorder• Counsel patient as to the probability of success
The Quiver• Esophagram• Upper Endoscopy• Manometry
– High resolution
• pH testing– Catheter-based– “Wireless”
• Impedance– pH or Manometry
• Gastric Emptying• Esophageal Emptying
Video Esophagram (Required)
• Dynamic imaging of entire organ– Contour– Obstructive lesions– Some functional
information
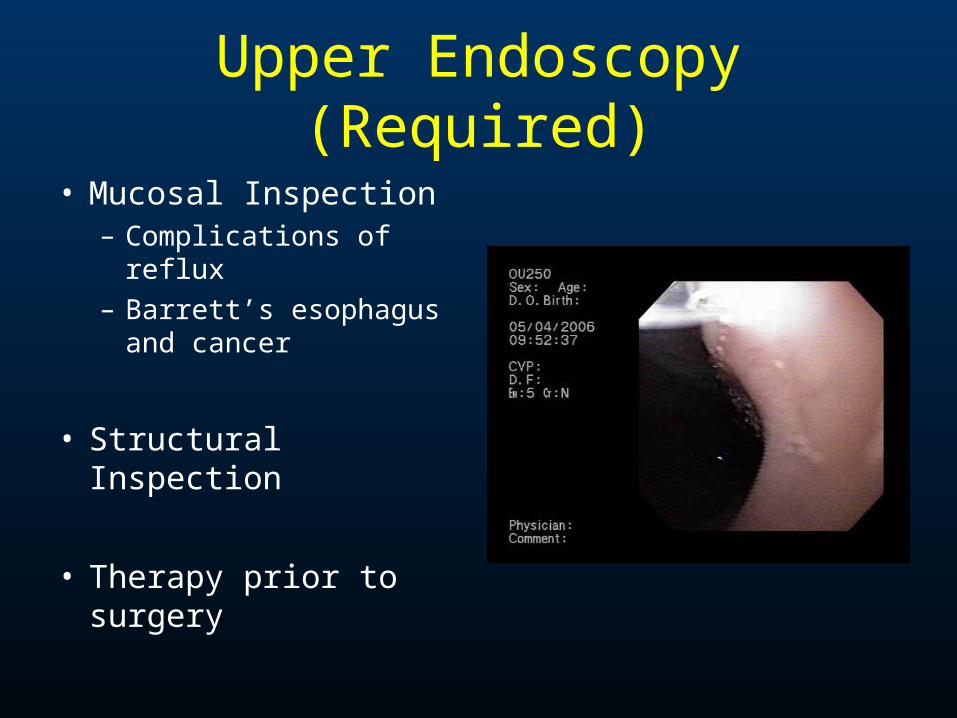
Upper Endoscopy (Required)
• Mucosal Inspection– Complications of reflux– Barrett’s esophagus
and cancer
• Structural Inspection
• Therapy prior to surgery
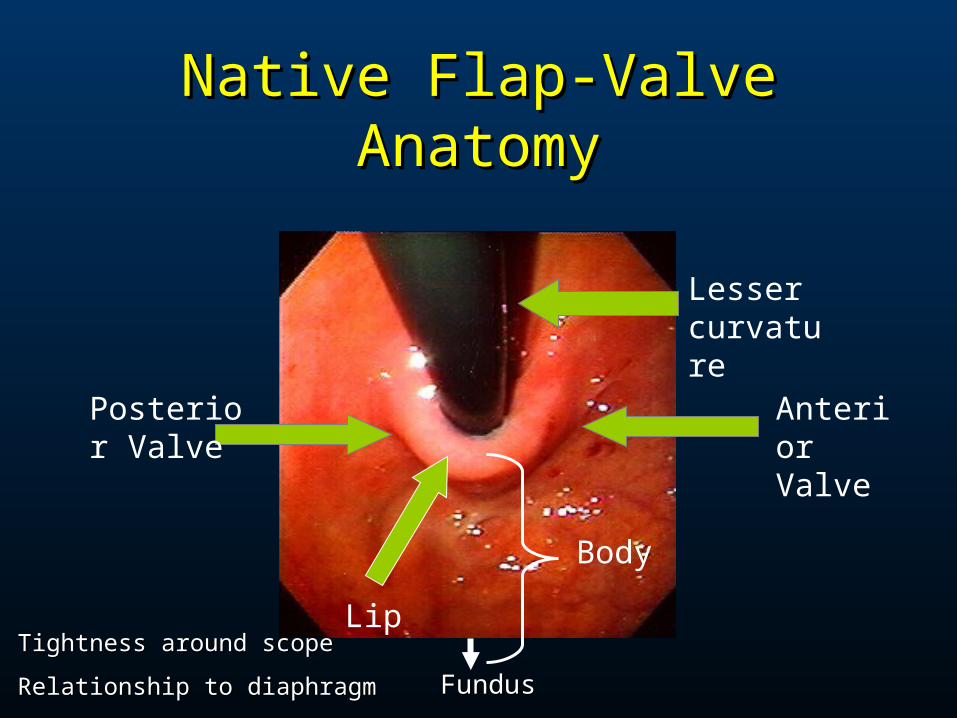
Native Flap-Valve AnatomyNative Flap-Valve Anatomy
Lesser curvature
Anterior Valve
Body
Lip
Posterior Valve
Tightness around scope Tightness around scope
Relationship to diaphragmRelationship to diaphragm FundusFundus
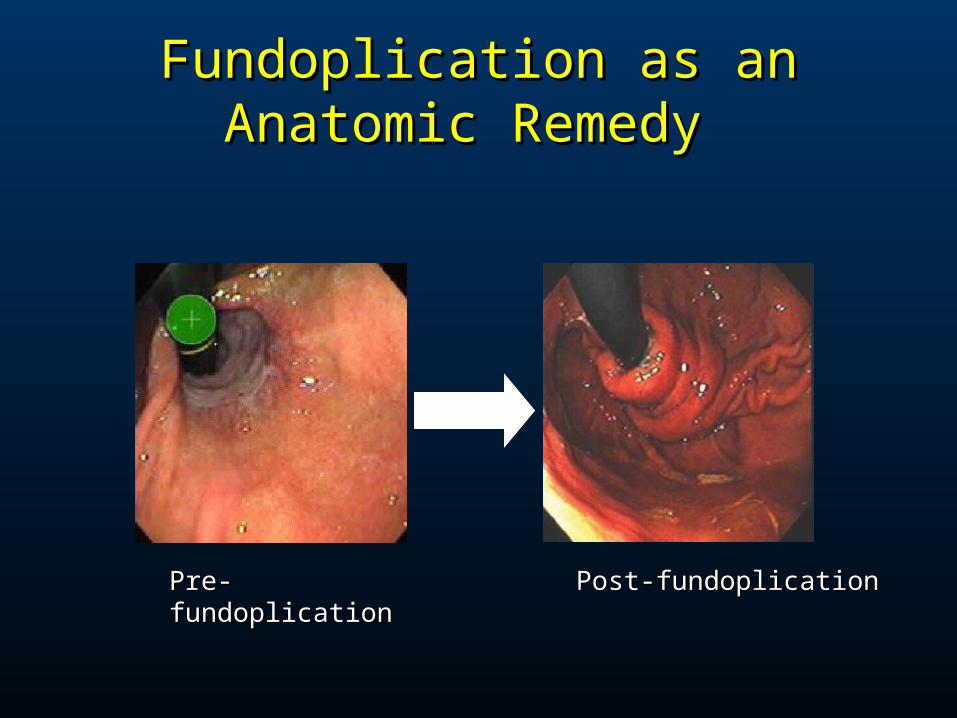
Fundoplication as an Anatomic Fundoplication as an Anatomic Remedy Remedy
Pre-fundoplicationPre-fundoplication Post-fundoplicationPost-fundoplication
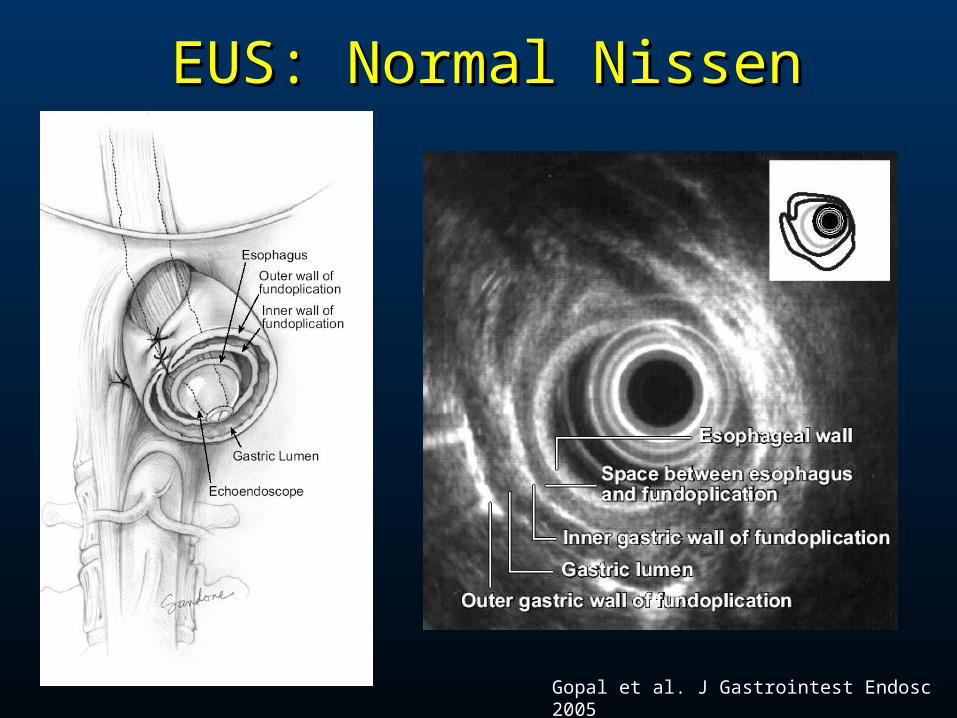
EUS: Normal NissenEUS: Normal Nissen
Gopal et al. J Gastrointest Endosc 2005Gopal et al. J Gastrointest Endosc 2005
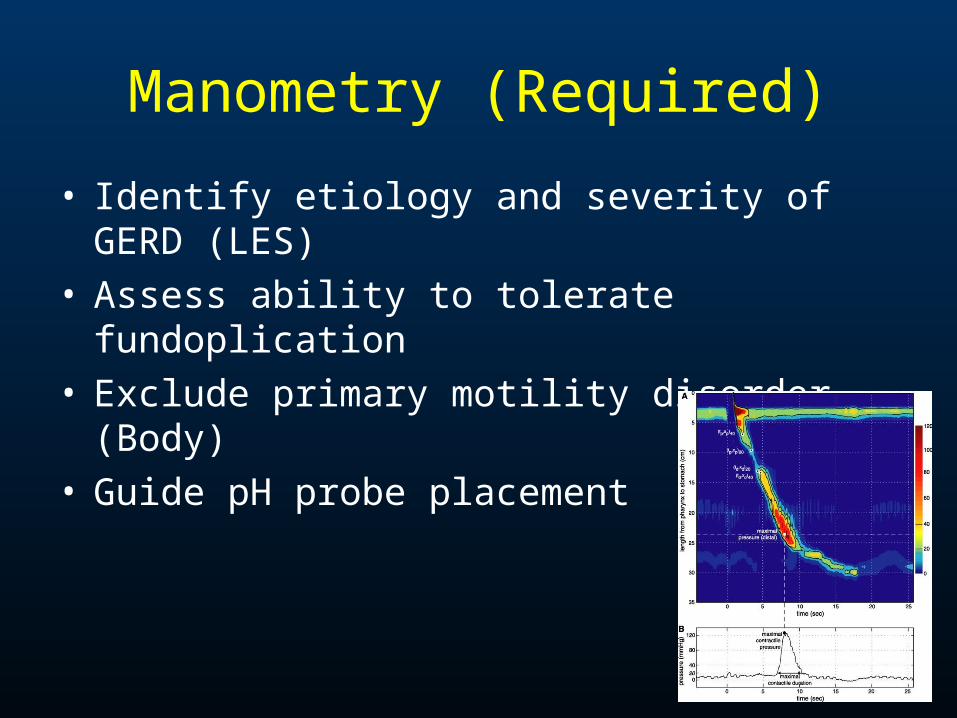
Manometry (Required)
• Identify etiology and severity of GERD (LES)• Assess ability to tolerate fundoplication• Exclude primary motility disorder (Body)• Guide pH probe placement
24-Hour pH Testing (Required)
• Detects esophageal acid exposure
• Correlate symptoms with reflux episodes
• ? Tailor fundoplication
• Considered the “gold standard” for making diagnosis
Potential Pitfalls with pH Testing
• Wrong position
• “Good day”
• Acidic foods
• Atrophic gastritis
• Sensitive esophagus
• Achalasia
• Poor sensitivity in LPR
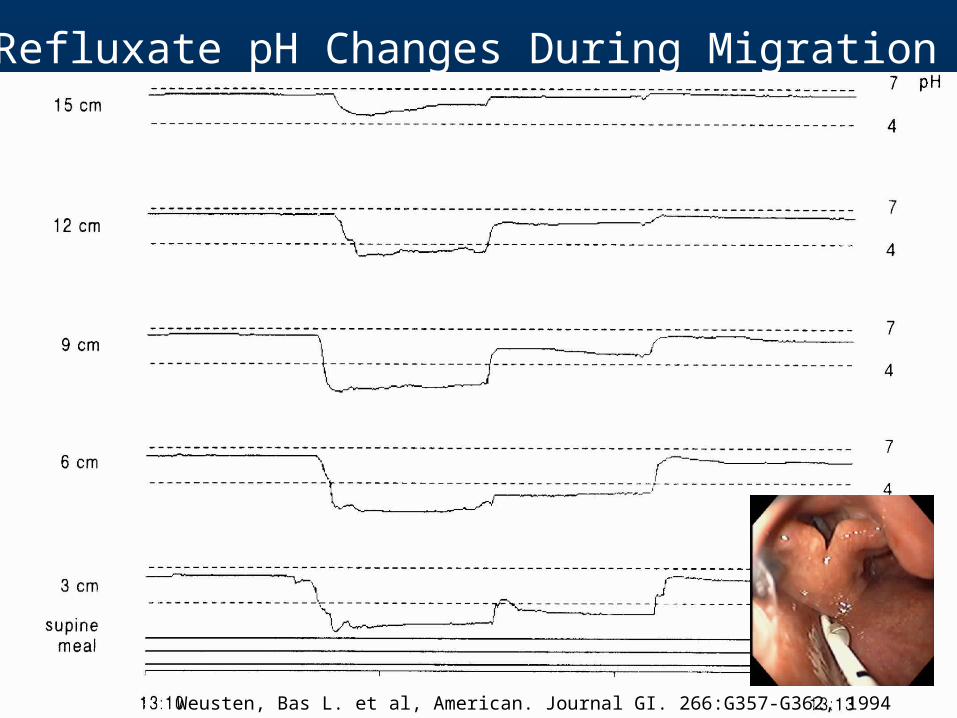
Refluxate pH Changes During Migration
Weusten, Bas L. et al, American. Journal GI. 266:G357-G362, 1994
How Do You Select the Correct Patient with GERD?
The Three Most Important Factors which Predict the Likelihood of Success
• Abnormal 24-hour pH score
• Typical primary symptom
• Clinical response to PPI
J Gastrointest Surg 1999;3:292
Situations in which ARS may be Applied
• Typical GERD
• NERD
• PEH
• Achalasia
• Primary, Secondary, Tertiary Failure
• Asthma and other Extraesophageal Sxs
• Atypical
Pitfall #1Missed Achalasia
•Perform manometry on everyone
•Think of this with re-dos
•Read your own tracings
•Be suspicious–Positive pH–Esophagitis
Pitfall #2Eating Disorder
•History
•Physical–Finger nails–Dentition–Body habitus may be normal
•Esophagitis with normal manometry or pH
•Index of suspicion
Pitfall #3Functional Dyspepsia
•History and physical
•Don’t mistake for GERD
•Listen to your objective evidence
•Order more tests
•If uncertain, refer for second opinion
Pitfall #4Structural Gastric Outlet
Obstruction
•Be suspicious with normal LES physiology and abnormal pH
•Bloating, nausea
•NSAID use or prior treatment for H. pylori
•EGD
Pitfall #5: Occult GERD-Pitfall #5: Occult GERD-Proving Association with Proving Association with
Extraesophageal SymptomsExtraesophageal Symptoms
1) Gastric juice, of either acid or alkaline pH, can cause damage to the 1) Gastric juice, of either acid or alkaline pH, can cause damage to the laryngeal or airway mucosalaryngeal or airway mucosa
2) Airway desquamation is followed by mucosal regeneration over 3-7 2) Airway desquamation is followed by mucosal regeneration over 3-7 daysdays
3) Microaspiration can be asymptomatic and occur with a normal 24 3) Microaspiration can be asymptomatic and occur with a normal 24 hour pH scorehour pH score
4) Symptoms can occur with only distal esophageal acid exposure4) Symptoms can occur with only distal esophageal acid exposure
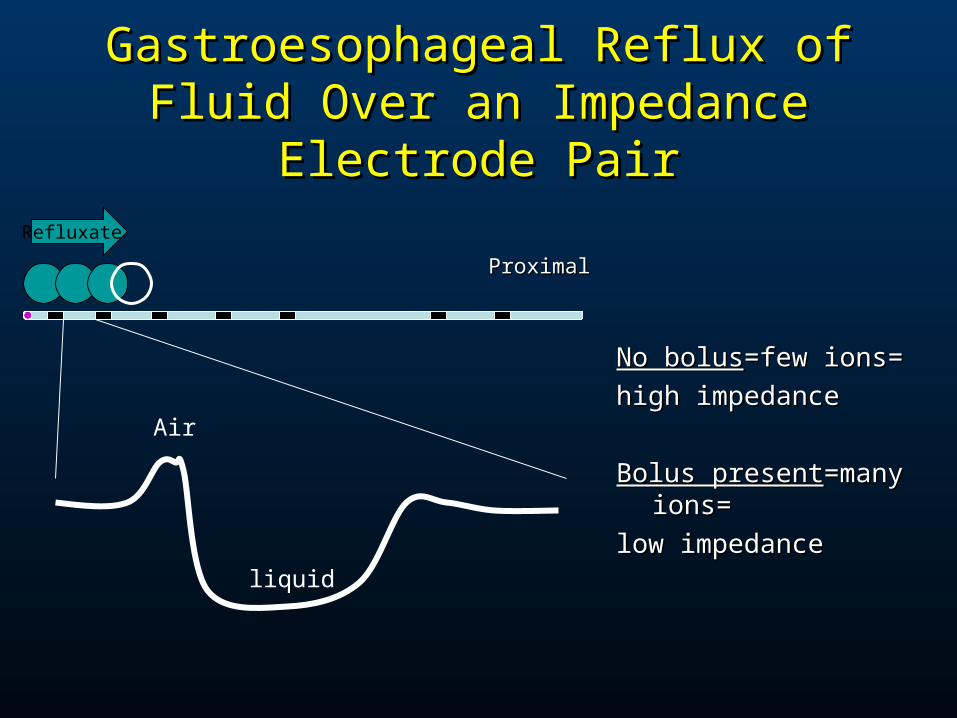
Gastroesophageal Reflux of Fluid Gastroesophageal Reflux of Fluid Over an Impedance Electrode PairOver an Impedance Electrode Pair
No bolusNo bolus=few ions==few ions=
high impedancehigh impedance
Bolus presentBolus present=many ions==many ions=
low impedancelow impedance
Air
liquid
Refluxate
ProximalProximal
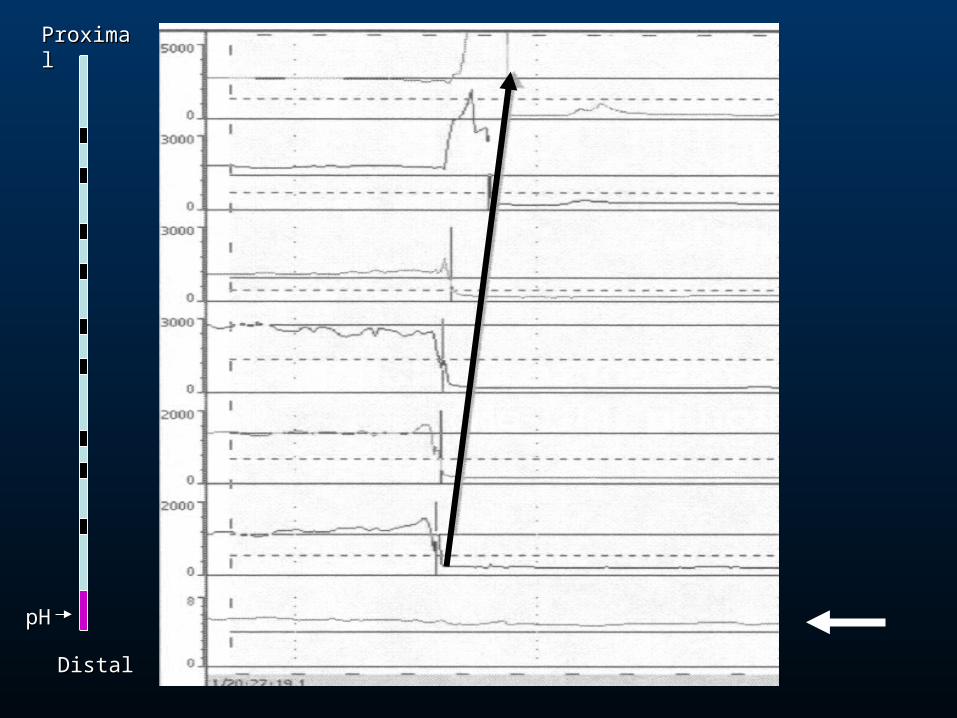
pHpH
ProximalProximal
DistalDistal
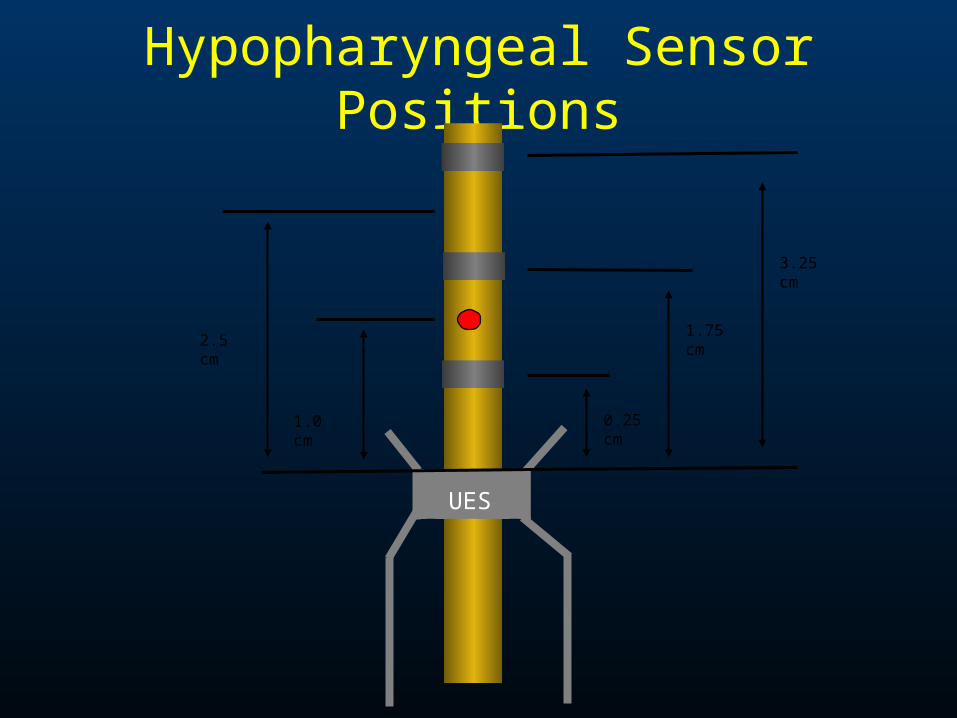
Hypopharyngeal Sensor Positions
0.25 cm
1.75 cm
3.25 cm
1.0 cm
UES
2.5 cm
Mr. EMr. E
•75 year old male 75 year old male •non-smoker non-smoker •17 months of non-productive cough and dysphonia17 months of non-productive cough and dysphonia
–Worse when supine and after mealsWorse when supine and after meals–Mild HB symptoms and no regurgitationMild HB symptoms and no regurgitation
•History of post-nasal dripHistory of post-nasal drip•Two episodes of pneumonia in last yearTwo episodes of pneumonia in last year•No history of AsthmaNo history of Asthma•Does not take ACE inhibitorsDoes not take ACE inhibitors
Mr. EMr. E
•Physical ExamPhysical Exam–Fit appearingFit appearing–VSSVSS–normalnormal
CXRCXR
“PPI Test”
Omeprazole 40mg bid for 4mosOmeprazole 40mg bid for 4mos– Mild subjective improvement in Mild subjective improvement in
hoarseness but cough is samehoarseness but cough is same
– Chronic throat clearingChronic throat clearing
– GERD symptoms resolvedGERD symptoms resolved
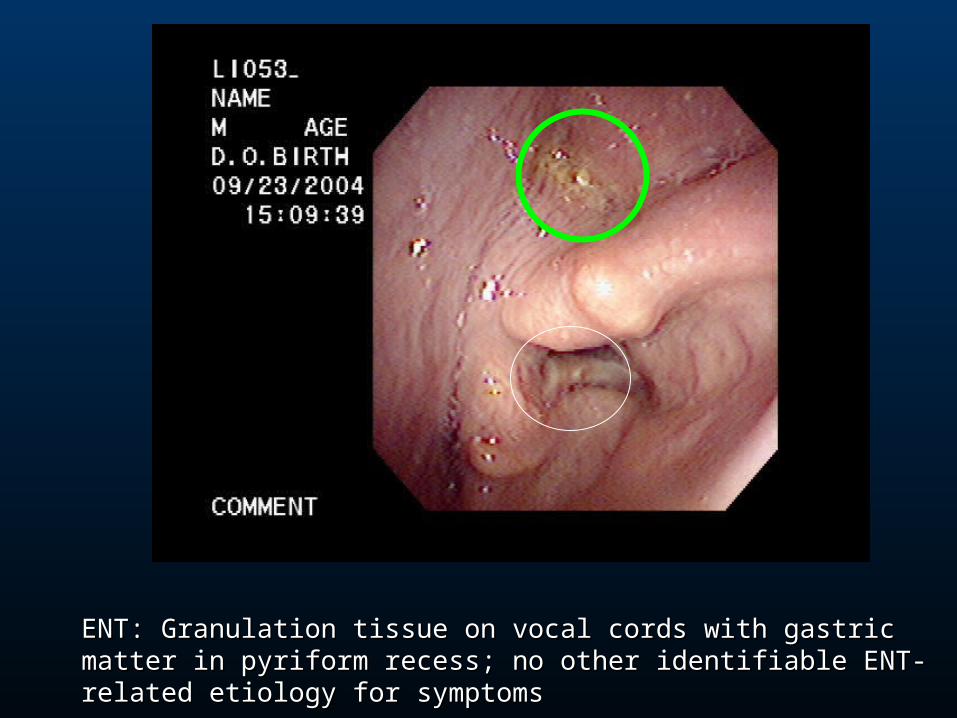
ENT: Granulation tissue on vocal cords with gastric matter in pyriform recess; ENT: Granulation tissue on vocal cords with gastric matter in pyriform recess; no other identifiable ENT-related etiology for symptomsno other identifiable ENT-related etiology for symptoms
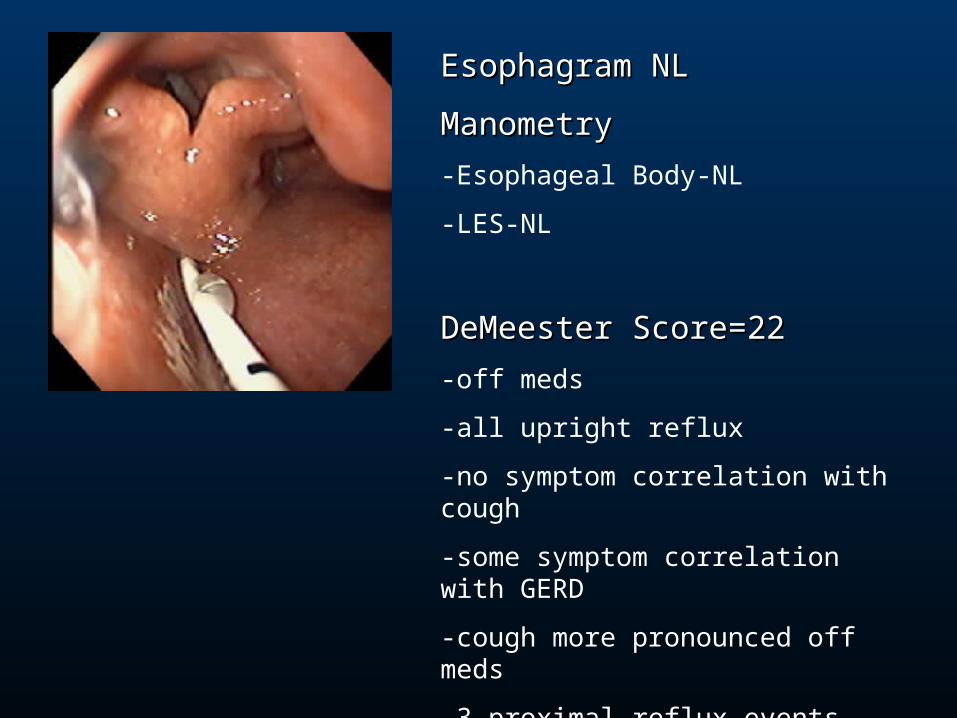
Esophagram NLEsophagram NL
ManometryManometry
-Esophageal Body-NL
-LES-NL
DeMeester Score=22DeMeester Score=22
-off meds
-all upright reflux
-no symptom correlation with cough
-some symptom correlation with GERD
-cough more pronounced off meds
-3 proximal reflux events
Upper EndoscopyUpper Endoscopy
No esophagitis
No hiatal hernia
Slightly varigated squamocolumnar junction
-less than 2 cm
Biopsy obtainedBarrett’s esophagus without dysplasia
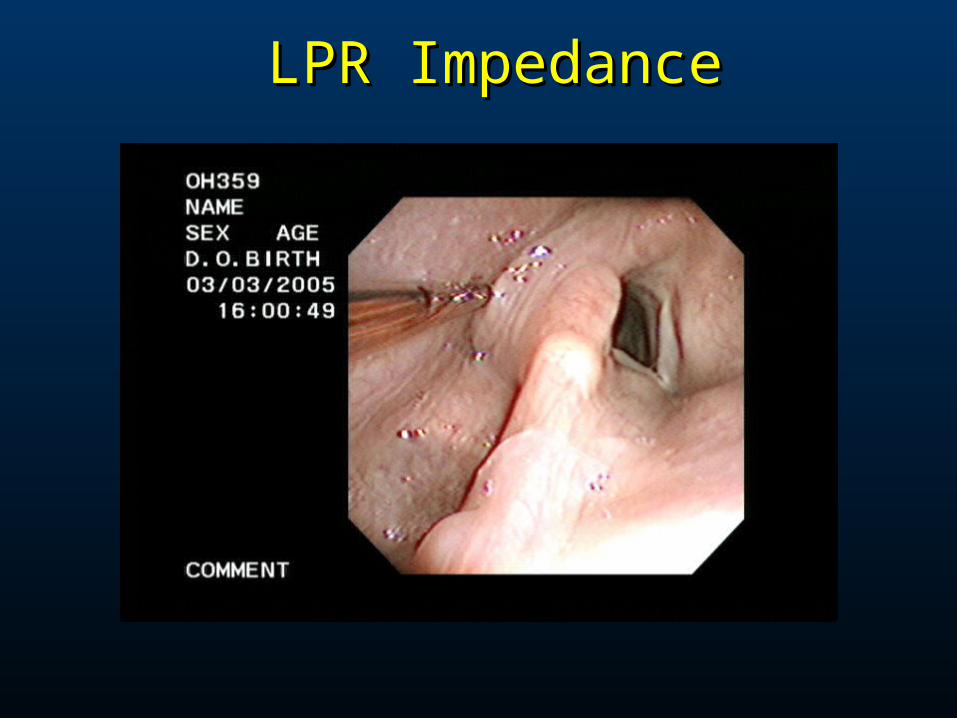
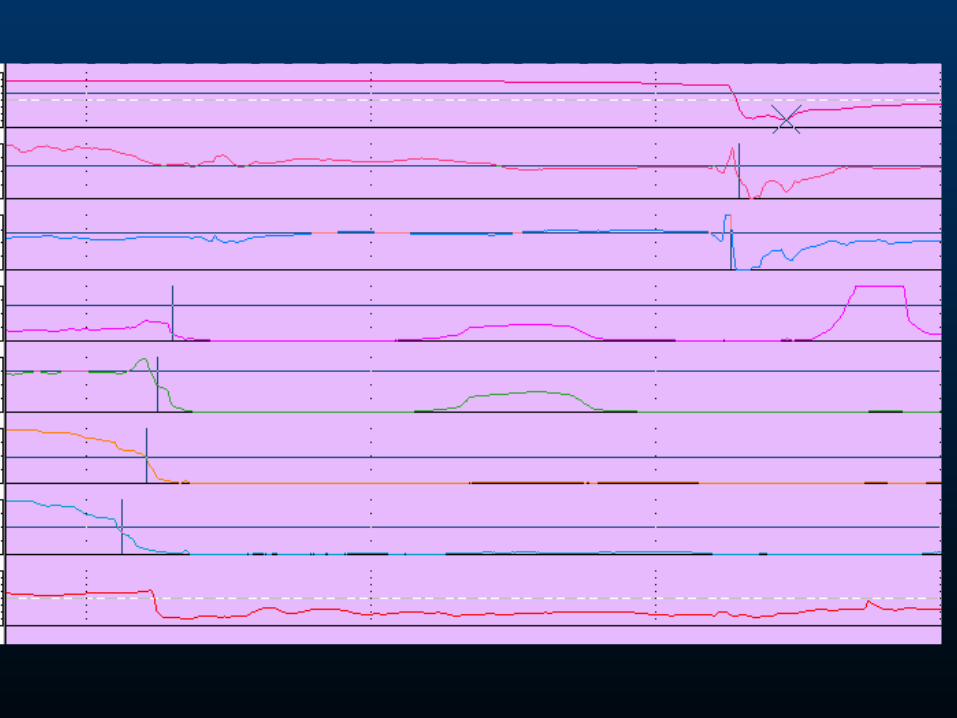
LPR ImpedanceLPR Impedance
“Wisdom and understanding can only become the possession of individual men (and women) by traveling the old road of observation, attention, perseverance, and industry”
-Samuel Smiles

LETS VOTELETS VOTE
• Nissen Fundoplication after lengthy Nissen Fundoplication after lengthy informed consent?informed consent?
• Increase PPI therapy?Increase PPI therapy?
• Promotility Agent?Promotility Agent?
• Antihistamines, beta-2 agonists, Antihistamines, beta-2 agonists, corticosteroidscorticosteroids
• Other TestsOther Tests
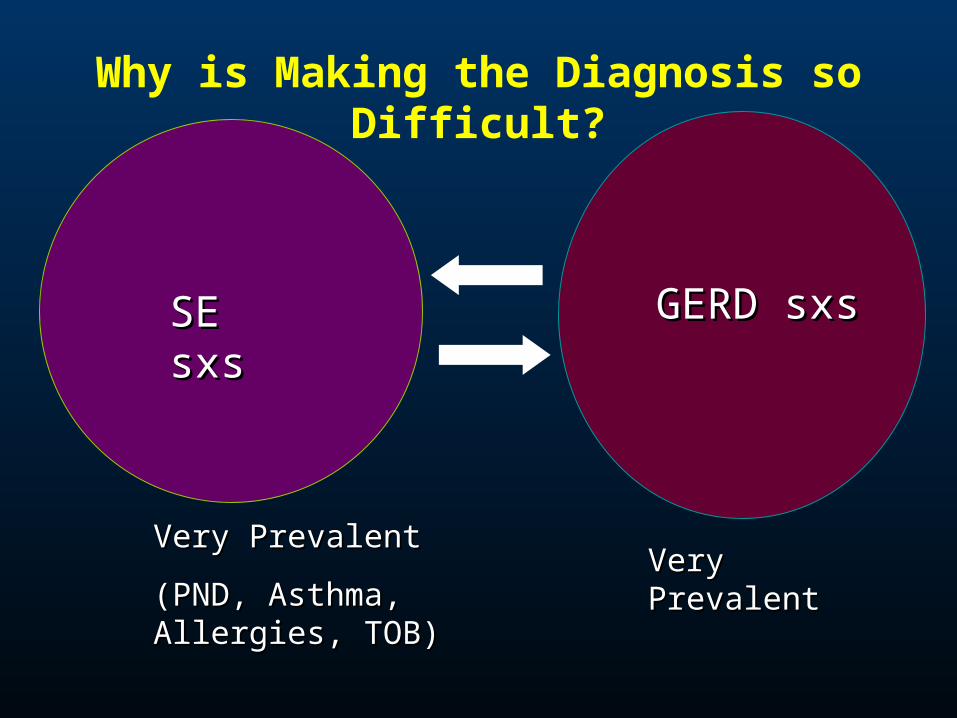
SE sxsSE sxs GERD sxsGERD sxs
Very PrevalentVery Prevalent
(PND, Asthma, Allergies, (PND, Asthma, Allergies, TOB)TOB)
Very PrevalentVery Prevalent
Why is Making the Diagnosis so Difficult?