Embed Size (px)
Citation preview

Dr Upali Weragama MBBS(Pera), MD(Col),
MRCP(UK), MAGA(USA)Consultant Physician
Sri Lanka Police HospitalColombo

• Although substantial reduction in AIDS deaths
• Liver disease emerging as an important non-AIDS related cause of death among HIV infected patients •Accounting for 14-18% of all deaths in this population
•Almost half of deaths among hospitalized HIV infected patients


ClinicianDeranged LFT
Decompensation
ART IncludingImmune
Reconstitution
Biliary Complications Alcohol and
substance abuse





HIV-HCV coinfected individuals treated for HCV who achieve SVR have lower rates of HIV progression and non-liver mortality


Treatment of HIV/HCV coinfection PEG-IFN/ribavirin ( low efficacy adverse events
associated with IFN-based therapy)
availability of HCV direct-acting antivirals (DAAs) ( 5 5 )specially NS A & NS B classes
Daclatasvir plus sofosbuvir , with or without ribavirin
/ safe appropriate antiretroviral drugs – ritonavir, darunavir, atazanavir, lopinavir, efavirenz, rilpivirine, raltegravir, and dolutegravir.

Although HCV-infected patients have a higher incidence of ART-related liver toxicity
may leads to inappropriate ART discontinuation the benefits of ART for HIV treatment are profound
will have beneficial effects on the progression of liver disease in coinfection as improvement in CD4 count may decrease fibrosis progression
therefore, ART should not be withheld inappropriately in the coinfected population




•HIV-infected patients have a lower rate of spontaneous clearance of HBeAg
•increased HBV replication
• higher rate of loss of anti-HBs Ab and reactivation of HBV
•increased progression to cirrhosis, decompensation & HCC
• higher liver-related mortality compared to HBV monoinfected individuals


The decision to initiate HBV treatment depends on whether the patient meets indications to treat either HIV or HBV

Treatment decisions of Chronic Hepatitis BHBe status Age of the patient & comrbiditiesPresence of / significant fibrosis cirrhosis ALT level HBV DNA level

In patients with HIV and HBV coinfection, HBV infection should be treated only in conjunction with HIV infection.
Treatment of HBV infection alone without addressing the HIV infection will lead to emergence of resistant HIV strains

•If there is no indication to treat either infection, the patient should be monitored closely.
• If treatment is indicated for either HIV or HBV, ART should be initiated and should include the combination of tenofovir , emtricitabine and lamivudine (anti-viral agents with dual activity).
•A - . void entecavir mono therapy



Classes of Antiretroviral agents
•Nucleoside reverse transcriptase inhibitors (NRTIs)•Protease inhibitors (PIs)•Nonnucleoside reverse transcriptase inhibitors (NNRTIs)•Fusion inhibitors•CCR5 co-receptor antagonists (entry inhibitors)•HIV integrase strand transfer inhibitors

Direct drug toxicity and/or drug metabolism Hypersensitivity reactions
Mitochondrial toxicity
IRIS (Immune reconstitution inflammatory syndrome)

IRIS describes a collection of inflammatory disorders associated with paradoxical worsening of preexisting infectious processes following initiation of antiretroviral therapy in the setting of successful HIV RNA suppression
previous subclinical and later unmasked by the host's regained capacity to mount an inflammatory response.

The syndrome generally manifests within the first two months of ART initiation and is accompanied by a precipitous decline in HIV RNA and rise in CD4 count.
In patients with HBV & HCV, immune restoration can lead to clinical flares of hepatitis due to the immune response to the virus.





Main adverse effect of the NRTI class - mitochondrial toxicity
The spectrum ranges from nonspecific symptoms to lactic acidosis syndrome with fulminant hepatic failure.

Lactic acidosis syndrome Is manifested by nausea, vomiting and abdominal pain, rapidly progressing to tachypnoea with severe acidosis.
Liver function tests may be modestly elevated in this setting, often with AST greater than ALT.
Late recognition of this syndrome usually is associated with death of the patient.

All NNRTIs except etravirine have the ability to cause some degree of hepatotoxicity.
Delavirdine and efavirenz can increase transaminase levels
nevirapine can cause severe toxicity (the NNRTI most associated with hepatotoxicity)

Protease inhibitors-
asymptomatic hyperbilirubinemia is common with atazanavir and indinavir
does not require discontinuation of therapy in the absence of concomitant elevation in levels of liver transaminases

Chemokine Receptor Antagonists
severe hepatotoxicity has been reported with maraviroc
be cautioned when maraviroc is administered to any patient predisposed to hepatic impairment

Given the large benefit of ART, which clearly outweighs its potential risks for liver toxicity, it is unjustifiable to inappropriately defer antiretroviral therapy.
Clinicians need to educate the patient regarding symptoms and signs of hepatotoxicity, assess risk factors for drug injury, address those factors that can be modified, and be vigilant for the earliest signs of drug injury.



Non-alcoholic fatty liver disease (NAFLD) in HIV-positive patients is associated with HIV specific factors, such as lipodystrophy and the use of antiretroviral therapy (ART), as well as higher risk of insulin resistance.
Traditional risk factors (including obesity, insulin resistance and the metabolic syndrome).
As a consequence, and given the ageing HIV population, NAFLD has been reported in up to 40–60% of HIV-infected individuals.

Causes of non-cirrhotic PHT in HIV
Nodular regenerative hyperplasia strong association with- Didanosine &
Stavudine
Hepatoportal scerosis





A significant proportion of patients with features suggestive of biliary tract disease will be found to have common conditions such as
cholelithiasis benign bile duct strictures periampullary neoplasms
Such readily treatable conditions must be excluded prior to searching for an AIDS-associated diagnosis





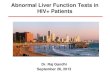
Hepatic safety profile of antiretroviral drugs. RTV, ritonavir (*at full doses, not when used as booster); ddI, didanosine; d4T, stavudine; AZT, zidovudine; ABV, abacavir; TDF, tenofovir; 3TC, lamivudine; FTC, emtricitabine; NVP, nevirapine; EFV, efavirenz; TPV, tipranavir; APV, amprenavir; DRV, darunavir; ATV, atazanavir; LPV, lopinavir; SQV, saquinavir; NFV, nelfinavir; T20, enfuvirtide; NRTI, nucleoside reverse transcriptase inhibitors; NNRTI, nonnucleoside reverse transcriptase inhibitors; PI,
protease inhibitors.


In addition to drug injury, flares in serum transaminase concentrations in a patient with chronic HBV can be related to several different factors, including viral rebound after withdrawal of effective anti-HBV therapy, breakthrough of drug-resistant HBV strains or spontaneous flares of HBV viraemia.[21,27-
29] The clinician must bear this in mind before misinterpreting hepatic flares as drug injury.


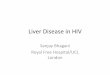
Estimated numbers of Co-infected persons (worldwide)

by the presence of HIV p24 within Kupffer cells and hepatic endothelial cells
HIV messenger RNA within hepatocytes
however, whether HIV itself directly damages the liver?