Embed Size (px)
Citation preview

Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 1 of 18
Inter-group chairpersons
Prof. Dr. Dieter Körholz
(Coordinating chairperson) Universitätsklinikum Giessen und Marburg GmbH; Standort Giessen - Zentrum für Kinderhämatologie und –onkologie
Feulgenstr. 12, 35392 Giessen
Germany
Sponsor
Prof. Dr. W. Hamish Wallace
Royal Hospital for Sick Children, Sciennes Road, Edinburgh EH9 1LF, Scotland, UK.
Prof. Dr. Judith Landman-Parker
Service d’hématologie et d’oncologie pédiatrique Hôpital Trousseau AP-HP Paris, France
Justus-Liebig-University of Giessen
Medizinische Fakultät Rudolf-Buchheim-Str. 6 35392 Giessen Germany
EudraCT number: 2012-004053-88
Date of Version: 2015-09-15
EuroNet-Paediatric Hodgkin’s Lymphoma Group
Second International Inter-Group Study
for Classical Hodgkin’s Lymphoma in Children and Adolescents
Imaging Manual
EuroNet-PHL-C2

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 2 of 18
Table of Contents
1. REFERENCE IMAGING CENTRES .......................................................................................... 3
2. SUMMARY ................................................................................................................................. 3
2.1. DATES OF IMAGING ................................................................................................................. 3
2.2. RECOMMENDED IMAGING OPTIONS FOR IM1, IM2, IM3 AND IMR DEPENDING ON
AVAILABLE IMAGING FACILITIES .......................................................................................... 4
2.3. PET – PATIENT PREPARATION AND ACQUISITION ............................................................ 5
2.4. IMAGE TRANSFER ................................................................................................................... 6
2.5. EVALUATION OF EXAMINATIONS AND REPORTING .......................................................... 6
3. DETAILED INFORMATION ............................................................................................................. 6
3.1. FDG-PET /CT, PET/MRI OR PET EXAMINATIONS ..................................................................... 6
3.2. F-18-FDG DOSAGE AND RADIATION PROTECTION ISSUES ................................................. 6
3.3. ADDITIONAL RECOMMENDATIONS FOR PET .......................................................................... 7
3.4. ADDITIONAL REQUIREMENTS FOR MRI AND CT .................................................................... 8
3.5. IMAGE TRANSFER ....................................................................................................................... 10
3.6. ASSESSMENT OF INVOLMENT AND RESPONSE BY CENTRAL REVIEW BOARD .......... 10
3.6.1. INITIAL STAGING ...................................................................................................................... 10
3.6.1.1. INDEPENDENT LYMPH NODE REGIONS .......................................................................... 11
3.6.1.2. DEFINITION OF INVOLVEMENT .......................................................................................... 12
3.6.1.3. DEFINITION OF BULK – MEASUREMENT OF LARGEST NODAL TUMOR MASS ...... 13
3.6.2. EARLY AND LATE RESPONSE ASSESSMENT (ERA/LRA) ............................................... 14
3.6.2.1. DEFINITION OF RESPONSE GROUPS AT ERA ............................................................... 16
4. REFERENCES ............................................................................................................................... 17

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 3 of 18
1. REFERENCE IMAGING CENTRES
2. SUMMARY
2.1. Dates of imaging
Table 1: Dates of Cross sectional imaging and FDG-PET
Dates Which patients When
Im1 –initial staging all Before start of treatment
Im2 - After 2 OEPA
Early response assessment (ERA)
all Day 14 – 17 after the last dose of prednisone in the second cycle
Im3 - End of ChT
Late response assessment (LRA)
TL-2 or TL-3
only if qPET+ at Im2
Day 14 – 17 after the last dose of prednisone in the last cycle
ImR at diagnosis of relapse or progression
Patients with biopsy confirmed relapse/progression
After relapse is confirmed by biopsy
Reference nuclear physician
Prof. Dr. Regine Kluge
Klinik und Poliklinik für Nuklearmedizin
Universitätsklinikum Leipzig
Liebigstraße 18, D-04103 Leipzig, Germany
Tel.: +49-341- 97 18 031 or 97 18 000,
Fax: +49-341- 97 18 009
Reference Radiologists
Dr. D. Stoevesandt and Prof. Dr. Rolf Peter Spielmann
Universitätsklinikum der Martin-Luther-Universität Halle-Wittenberg
Universitätsklinik und Poliklinik für Diagnostische Radiologie
Ernst-Grube-Straße 40
06120 Halle (Saale), Germany
Tel.: +49-345-5572441
Fax: +49-345-5572157

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 4 of 18
Table 2: Imaging during Follow-up
Diagnostics Year 1 Years 2. + 3. Years 4. + 5.
Chest x-ray 6 months and 12 months after end of treatment
Every four months
Ultrasound neck, abdomen and pelvis
6 months and 9 months after end of treatment
Every four months Every six months
Chest CT in patients with initial lung involvement
3 months and 12 months after end of treatment*
MRI of all initially involved regions
3 months and 12 months after end of treatment*
Please note: FDG-PET is not recommended at regular follow-up visits
2.2. Recommended imaging options for Im1, Im2, Im3 and ImR depending on
available imaging facilities
The following three options - ordered by preference – are allowed according to local
availability.
a) Neck and Torso PET/MRI with i.v. contrast
− Acquisition from skull base to mid thighs. Respiratory triggering is recommended for
chest and abdomen.
− An additional diagnostic quality chest CT in end-inspiration is required at Im1 for
lung evaluation (only if chest-CT was not performed within two (to three) weeks prior
to diagnosis of Hodgkin`s lymphoma).
− In case of lung involvement chest CT in end-inspiration is required also at Im2 (Im3
if applicable).
− At Im1 liver and spleen ultrasound is required.
− At Im1 in case of suspected skeletal involvement an additional bone scintigraphy is
required, if no corresponding CT is performed for the respective region of a PET
positive lesion.

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 5 of 18
b) Neck and Torso PET/CT with i.v. contrast and X-ray-dose optimization protocol
(follow local or national protocols and guidelines)
− Acquisition from skull base to mid thighs
− At Im1 additional diagnostic quality chest CT in end-inspiration is required for lung
evaluation at Im1, preferentially added immediately after end of the whole-body scan
(only if a chest-CT has not been performed within two (to three) weeks prior to
diagnosis of Hodgkin`s lymphoma).
− In case of lung involvement additional CT of the lungs in end-inspiration is added at
Im2 (Im3 if applicable).
− At Im1 liver and spleen ultrasound is required.
− No bone scintigraphy is required.
c) ONLY if A and B are not available: PET/CT (low dose) without contrast (not
recommended!) or PET only
− Acquisition of PET from skull base to mid thighs is required at Im1 and Im2 and for
qPET positive patients also at Im3.
− At Im1 additional diagnostic quality chest CT with i.v. contrast in end-inspiration is
required (only if a chest-CT has not been performed within two (to three) weeks prior
to diagnosis of Hodgkin`s lymphoma). In case of lung involvement additional CT of
the lungs in end-inspiration is added at Im2 (Im3 if applicable).
− At Im1 additional MRI with i.v. contrast of neck, abdomen and pelvis is required. At
Im2 and Im3 additional MRIs are required only for initially involved regions.
− At Im1 liver and spleen ultrasound is required.
− At Im1 in case of suspected skeletal involvement an additional bone scintigraphy is
required, if no corresponding CT is performed for the respective region of a PET
positive lesion.
2.3. PET – Patient preparation and acquisition
a) Premedication with oral non-selective β-blockers is strongly recommended in
patients > 10 years of age and without contraindications.
- One hour prior to FDG-application
- 1mg/kg BW Propranolol, do not exceed 40 mg
- Off-label use requires informed consent

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 6 of 18
b) Acquisition starts 60 ± 10 min p.i. of FDG (essential for qPET evaluation!)
c) Head and spine in neutral position. Position arms up over the head at Im1 if
possible. Identical position of arms at Im1, Im2 and Im3.
2.4. Image reconstruction and transfer
All images (including PET/MRI or PET/CT (, and if applicable CT, MRI or bone scan) for
reference evaluation will be transferred to the central server (Hermes Medical Solutions;
Sweden). Please send data in DICOM format reconstructed with an algorithm according to
EANM Guideline e.g. OSEM (15)
Recommended: Direct transfer from the local centre to the central server. (contact:
[email protected] (Refer to Hodgkin Project) If direct transfer not feasible:
Transfer via CD to study office in Halle (until end of October 2015, afterwards to study office
in Gießen, see address Prof. Körholz), from where images are stored on the central server,
NOTE: This may trigger delays compromising treatment delivery.
2.5. Evaluation of examinations and reporting
All study specific evaluations for staging and response evaluation (see Section 3+4+5
below) are performed at central review. Central review is provided by the EuroNet-PHL
study centre in Gießen/Halle/Leipzig except for Austria (Vienna).
Images are evaluated and reported by the local nuclear physician and radiologist as per local
standard. Local findings are forwarded to the Central review.
3. DETAILED INFORMATION
3.1. FDG-PET /CT, PET/MRI or PET examinations
Please follow the guidelines of the European Association of Nuclear Medicine for F-18-FDG
examinations for patient preparation, data acquisition (1) and image reconstruction (15) .
3.2. F-18-FDG dosage and radiation protection issues
- Don’t exceed F-18-FDG doses as recommended in the EANM dosage card (2-4) and
national reference levels. Please Note: Use the lowest activity appropriate for
your technical setting to achieve good image quality. The value for the "minimum
recommended activity" is reduced to 14 MBq for 3D- and to 26 MBq for 2D-
acquisitions (3).

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 7 of 18
- Please use 3D-acquisition if possible.
- Use PET/MRI (option A) or low-dose PET/CT with i.v. contrast agent (option B)
or – if both entities are not available – combine FDG-PET with MRI imaging
(option C). For detection of lung involvement additional chest CT is required at
Im1 and – in case of lung involvement – also at Im2.
- Use of bone scintigraphy is limited to patients with FDG-PET positive skeletal
lesions and without available CT of these lesions. Please follow the guidelines
for paediatric bone scanning (5) and use Tc-99m-diphosphonate doses as
recommended in the EANM dosage card (4).
- PET is not recommended for routine follow-up.
3.3. Additional recommendations for PET
a) Avoid uptake in brown fat tissue
Enhanced FDG uptake in brown adipose tissue is a problem in children and adolescents.
Since head and neck area and upper mediastinum are frequently involved in Hodgkin’s
lymphoma special care has to be taken to avoid this artificial FDG-uptake. Especially at
Im2 and Im3 residual tumour tissue cannot be adequately evaluated if it is surrounded by
enhanced uptake in brown fat, which may cause unclear or even false-positive interim
PET results (Note: qPET results are essential for the decision on radiotherapy). The
following measures are strongly recommended:
- Keep the patient warm. Please inform parental guardian or the responsible
nurse to keep the patient warm on the way to the PET facility. Please provide a
warm and draught-free room for patient preparation. If necessary, use hot
(unsweetened) tea or blankets.
- Ask the patient to come one hour in advance for application of β-blocker.
- Since glucose uptake of brown fat is stimulated by the sympathetic nervous
system it can be considerably reduced by non-selective β-blockers such as
Propranolol (6-8). We recommend propranolol (oral administration) at a
dose of 1 mg/kg, not exceeding – a maximum of 40 mg one hour before
application of FDG if no contraindications are present and for patients over 10
years of age. (Please note: Propranolol in this indication is off-label use).

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 8 of 18
b) Patient positioning
Please position the patient’s head and spine in a neutral position (Don’t use pillows!).
This is necessary for proper evaluation of the tumour involvement in upper and lower neck
areas at Im1 and for standardization of head and neck positioning for direct slice-by-slice
image comparison at Im2 and Im3.
Please position both arms over the head at Im1 if possible. Please use identical
position of arms at Im1, Im2 and Im3. This is required for the slice-by-slice comparison
of the follow-up images. If for example a patient at Im1 was not able to put the right arm
over the head due to recent axillary biopsy the right arm should be positioned identically
at Im2 and Im3.
c) PET acquisition
Start PET acquisition 60 ± 10 minutes after i.v. application of F-18-FDG. Don’t exceed a
time interval of 50 – 70 (90) minutes. An accurate timing is important since FDG uptake in
tumour lesions increases with time (9) while it is constant in the liver (10) and therefore
qPET values might artificially increase with long intervals.
d) PET reconstruction
The reconstruction algorithm influences the detectability and interpretation, the SUVmax
and SUVpeak of small lesions (16). Please use OSEM reconstruction or other
reconstruction setting as indicated in the EANM guidelines (15, Appendix II). In addition
(not instead of) you are welcome to send PSF/UHD reconstructed images
3.4. . Additional requirements for MRI and CT
PET-CT: Tube current as low as possible
− usage of local body-weight adjusted low dose protocol with i.v. contrast in the
parenchymal phase
− reconstruction FOV adapted to patient size (markedly < 500 mm)
− reconstruction of 5 mm or thinner slices in transversal orientation
− (4mm or thinner if patient < 15 kg)
− additional image reconstruction in 5 mm slices in coronal orientation (if possible
separately for neck, thorax and abdomen)
− in case of spinal involvement additional reconstruction in sagittal image orientation
(3mm or thinner slice thickness).

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 9 of 18
Diagnostic chest-CT:
1. Usage of local dose optimizing protocol with i.v. contrast in inspiration (mAs suggestion
see (11)
2. Recommended use of breast protection shield
3. reconstruction of 5 or thinner mm slices in transversal orientation (4mm or thinner if
patient < 15 kg). Recommended two data sets (“soft tissue” and “sharp” algorithm).
4. additional image reconstruction in 5 mm slices in coronal orientation (alternative:
primary data with slice thickness ≤ 1mm)
Other MRI or CT imaging
1. all images to be sent send as DICOM to the central server (Hermes Med. Sol. Sweden)
– see image transfer
2. local reports send to secured fax number: +49 345 557 2389
Suggestions for MRI-imaging
For whole-body (PET)/MRI we propose as basic sequences T2-weighted inversion
recovery (TIRM) sequences in transversal AND coronal plane and diffusion weighted
sequence (DWI) in a transversal plane. (12).
Regional MRI-imaging
1. Neck: ≤ 5mm (T1-weighted transversal AND coronal, T2--weighted transversal, T2-
weighted inversion recovery (TIRM) coronal AND diffusion imaging transversal)
2. Chest:
a. Body mass < 30 kg use slice thickness ≤ 6 mm
b. Body mass ≥ 30kg use slice thickness. ≤ 8 mm
Gap (< 20% if possible < 10%), (T2 transversal AND coronal (if possible with fat
saturation), T1 transversal with and without i.v. contrast agent, if possible T1 coronal).
ECG and respiratory triggering (or breathhold) is recommended for chest imaging
3. Abdomen:
c. Body mass < 30 kg use slice thickness ≤ 6 mm
d. Body mass ≥ 30kg use slice thickness. ≤ 8 mm

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 10 of 18
Gap < 20% if possible < 10%, (T2 transversal AND coronal, T1 transversal with and without
i.v. contrast agent (dynamic liver imaging if possible) if possible T1 coronal).
Respiratory triggering (or breathhold) is recommended for imaging of the abdomen.
3.5. Image transfer
Decision on stage, treatment level and response is made by central review. Central review is
provided by the EuroNet-PHL study centre in Gießen/Halle/Leipzig (or for patients from
Austria: Vienna).
For the reference reading all images (i.e. all data and all slices) at Im1, Im2, Im3 and ImR
(PET/MRI, PET/CT, PET, MRI, CT, bone scan) have to be transferred in DICOM format to a
central server. This server is operated and technically supported by Hermes Med. Sol.
Stockholm, Sweden.
A data transfer network between most involved clinics was established with support from the
European Union (EAHC funded project “Paediatric Hodgkin Network”). Images can be sent
via:
- Hermes application X-port (program installed on the client PC)
- Hermes application Gold3Upload (program on the server)
- Any sFTP capable software
For all three options a personal account is needed. The data transfer is encrypted and
secured via https. The process is approved by the responsible data safety authority in
Germany (see data protection plan, version 2012-1-27). For organization and technical
support of image transfer contact HERMES Medical Solutions, Skeppsbron 44 1130
Stockholm, Sweden; +46 8 19 03 25; [email protected], refer to ‘’Hodgkin
project“
3.6. Assessment of involvement and response by Central Review Board
3.6.1. Initial staging
Every patient requires a FDG-PET examination before starting any therapy (imaging1 = Im1).
In exceptional emergency cases FDG-PET should be performed as soon as possible after
starting prednisone prephase.
The process described below is done by central review.

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 11 of 18
At central review in the study office at Gießen/Halle/Leipzig (Austria: Vienna) the images are
evaluated in 28 regions (Table 3). During the interdisciplinary tumour board CT or MRI findings
for each region are presented by the radiologist and PET findings by the nuclear physician.
Thereafter, status of each region (involved or not involved) is assessed according to the
definitions described below (see also protocol section). Based on these results, stage is
determined and volume of the largest nodal mass (see below) is measured.
3.6.1.1. Independent Lymph node regions
Please also refer to section 12.2.2 of trial protocol and for a more detailed region description refer to Appendix 1: Definition of independent lymph node regions and extranodal lesions.
Independent lymph node regions are:
- Waldeyer’s ring (left and right)
- cervical (left and right) with sub-regions relevant for irradiation:
o upper neck: above upper margin of the hyoid bone
o lower neck: below upper margin of the hyoid bone above lower margin of
cricoid cartilage
- supraclavicular (left and right) (below lower margin of cricoid cartilage above fossa
jugularis or lateral above Vena subclavia)
- infraclaviular (left and right): (below M. pectoralis major or minor)
- axillar (left and right): lateral of the M. pectoralis major or minor
- lung hilus (left and right): bronchopulmonary lymph nodes
- mediastinum with sub-regions relevant for irradiation:
o upper mediastinum: fossa jugularis to carina
o lower mediastinum: below carina to upper edge of the diaphragm
- supradiaphragmatic (left and right): diaphragmatic recesses (below upper edge of the
diaphragm but still above diaphragm)
- spleen
- splenic hilus
- liver hilus (porta hepatis)
- mesenteric: mesentery or mesocolon
- paraortic:
o upper (above the renal hilus)
o lower (at or below the renal hilus)
- iliac (left and right): below aortic bifurcation to inguinal ligament
- inguinal (left and right): below inguinal ligament

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 12 of 18
3.6.1.2. Definition of involvement
Please also refer to section 12.1 of trial protocol
Lymph node involvement If the largest diameter of a lymph node or a lymph node conglomerate
is smaller than 1 cm the region is considered not involved – independent of the PET result. Small
tumour lesions do not impair therapy results according to previous experience.
− If a lymph node or a lymph node conglomerate has a diameter of 1.0 – 2.0 cm the region
is considered involved only if it is FDG-PET positive.
− If the largest diameter of a lymph node or a lymph node conglomerate exceeds 2.0 cm the
region is considered involved – independent of the PET result.
Waldeyer’s ring
Involvement is defined by clinical assessment preferably by ENT physician. Biopsy is not required.
Spleen involvement
Spleen involvement is assumed if
− focal PET positive lesion are confirmed by CT or MRI or ultrasound
or
− tumour suspicious multiple small focal changes in the spleen structure are detected by
ultrasound – irrespective of the FDG-PET result.
Note: Exclusive spleen involvement without other lymphatic disease is classified as stage I. Assessment of E-lesions
An E-lesion is a per continuum infiltration from a lymph node mass into extra-lymphatic structures or organs (e.g. lung, bone).
Pleura involvement
Involvement of the pleura is assumed if
− an adjacent nodal lesion infiltrates the pleura or chest wall AND
− the infiltrate and/or the adjacent nodal lesion is PET positive
− Note that a pleural effusion is not considered to be an E-lesion,
Pericardial involvement
Pericardial involvement is assumed if
− adjacent nodal lesion infiltrates the pericardium AND

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 13 of 18
− the infiltrate and/or the adjacent nodal lesion is PET positive
− Note that - a pericardial effusion is not considered to be an E-lesion.
Organ involvement
Disseminated organ involvement always implies stage IV.
Lung involvement
Disseminated lung involvement is assumed if
− there are more than two foci >2 mm and <10 mm within the whole lung
or
− at least one intrapulmonary focus has a diameter of ≥10 mm
− (Please note: If all lesions are exclusively on one side of the lung, only this side is involved)
Even if only one additional smaller focus (>2mm) is found on the other side of the lung,
both sides are considered involved). Completely calcified nodules are not considered to
be caused by Hodgkin’s disease.
Liver involvement
Liver involvement is assumed if focal PET positive lesions are confirmed by CT or MRI or ultrasound.
Skeletal involvement
Bone marrow involvement is assumed, if
− More than 2 lymphoma-typical PET-positive lesions are found in skeleton, irrespective
of positivity in CT or MRI (13)
Bone involvement is assumed, if
− a PET positive skeletal lesion is located in spine, pelvis or upper parts of femora or
humeri and shows tumour-typical correlation in CT
(or increased uptake in bone scan if CT is not assessable)
3.6.1.3. Definition of bulk – Measurement of largest nodal tumor mass
Bulk is present if the volume of the largest contiguous lymph node mass is ≥ 200 ml

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 14 of 18
Please note: In the mediastinum the total volume of the initial tumour mass in the upper,
middle and lower mediastinum and both hili and both supradiaphragmatic recesses is
considered contiguous due to the complex anatomic structure.
Volumes are measured in CT or MRI based on the largest perpendicular diameters on
multiplanar reconstruction mode (A*B*C / 2).
3.6.2. Early and Late response assessment (ERA/LRA)
Every patient requires an imaging (= Im2) after the second cycle of OEPA. The PET
examination has to be done at day 14 – 17 after last dose of Prednisone/Prednisolone, which
is day 28 – 31 of the second OEPA.
Im3 for late response assessment is performed only in patients in treatment level TL-2 and TL-
3 with a positive qPET (see below) at Im2.
Response PET examinations are evaluated in direct comparison with the staging PET.
Images have to be co-registered and displayed in corresponding transversal, coronal and
sagittal slices (Hermes Hybrid viewer e.g.). Assessment of PET/MRI or PET/CT examinations
is done by synchronized evaluation of PET images, MRI or CT images and fused images. Use
same camera systems, if possible.
All initially involved regions are systematically checked to detect visibly enhanced FDG uptake
in a residual tumour mass. In all regions with a visibly detectable residual FDG uptake the
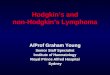
qPET value is determined by:
qPET
For qPET calculation a special software application is used (qPET, Hermes Med. Sol.). The
area with enhanced FDG uptake is labelled. The program automatically outlines the contour
of the volume with enhanced uptake, identifies the voxel with the highest SUV and checks the
surrounding of this voxel to identify the four hottest connected voxels. These four voxels are
highlighted and their mean SUV value is calculated to determine the SUVpeak of the tumour
residuum.

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 15 of 18
Figure 1: Semiautomatic region growing and calculation of SUVpeak
Residuum using qPET software
(Hermes Med. Sol. Sweden
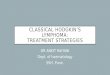
To calculate the SUVmean of the liver a predefined squared box with a volume of 30 ml is
placed in the middle of the liver. In case of focal lesions in the liver the volume of interest has
to be placed outside of these lesions. The mean SUV of this volume is calculated automatically
Figure 2: Semiautomatic calculation of SUVmeanLiver.
A detailed explanation of the qPET method and its use for response evaluation in lymphoma
patients has been published (14).

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 16 of 18
3.6.2.1. Definition of response groups at ERA (LRA)
If no tumour progression is detected, response groups are defined as follows:
Inadequate response (IR)
− Visual Deauville 4+ which corresponds to ERA qPET-positive ≥ 1.3 and/or
− Poor bulk response (volume reduction < 50 %) and/or
− A nodal site has a largest diameter of ≥ 2 cm and is not assessable by qPET due to brown
fatty tissue.
Adequate response (AR)
− No IR criterion is fulfilled
Please Note: At Im3 enhanced residual uptake is considered only in residual tumour masses
≥ 1cm. At LRA the threshold is at visual Deauville 3+ which corresponds to LRA qPET-
positive ≥ 0,95.

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 17 of 18
4. REFERENCES
(1) Stauss J, Franzius C, Pfluger T, Juergens KU, Biassoni L, Begent J, Kluge R, Amthauer H,
Voelker T, Højgaard L, Barrington S, Hain S, Lynch T, Hahn K; European Association of
Nuclear Medicine. Guidelines for 18F-FDG PET and PET-CT imaging in paediatric oncology.
Eur J Nucl Med Mol Imaging 2008;35(8):1581-8
(2) Lassmann M; L. Biassoni; M. Monsieurs; C. Franzius; F. Jacobs; EANM Dosimetry and
Paediatrics Committees.The new EANM paediatric dosage card. Eur J Nucl Med Mol Imaging.
2008;35(9):1748.
(3) Lassmann M, Biassoni L, Monsieurs M, Franzius C; EANM Dosimetry and Paediatrics
Committees.The new EANM paediatric dosage card: additional notes with respect to F-18. Eur
J Nucl Med Mol Imaging. 2008;35(9):1666-8
(4) Lassmann M, Treves ST; EANM/SNMMI Paediatric Dosage Harmonization Working
Group.Paediatric radiopharmaceutical administration: harmonization of the 2007 EANM
paediatric dosage card (version 1.5.2008) and the 2010 North American consensus
guidelines.Eur J Nucl Med Mol Imaging. 2014;41:1036-41
(5) Stauss J, Hahn K, Mann M, De Palma D. Guidelines for paediatric bone scanning with
99mTc-labelled radiopharmaceuticals and 18F-fluoride. Eur J Nucl Med Mol Imaging.
2010;37(8):1621-8.
(6) Agarwal A, Nair N, Baghel NS. A novel approach for reduction of brown fat uptake on FDG
PET. Br J Radiol. 2009;82(980):626-31
(7) Parysow O, Mollerach AM, Jager V, Racioppi S, San Roman J, Gerbaudo VH. Low-dose
oral propranolol could reduce brown adipose tissue F-18 FDG uptake in patients undergoing
PET scans. Clin Nucl Med. 2007;32(5):351-7.
(8) Söderlund V, Larsson SA, Jacobsson H. Reduction of FDG uptake in brown adipose tissue
in clinical patients by a single dose of propranolol. Eur J Nucl Med Mol Imaging.
2007;34(7):1018-22.
(9) Shinya T, Fujii S, Asakura S, Taniguchi T, Yoshio K, Alafate A, Sato S, Yoshino T,
Kanazawa S. Dual-time-point F-18 FDG PET/CT for evaluation in patients with malignant
lymphoma. Ann Nucl Med. Epub 2012 Jun 13

Imaging Manual Confidential
EuroNet-PHL-C2 final 2.0, 2015-09-15 Page 18 of 18
(10) Laffon E, Adhoute X, de Clermont H, Marthan R. Is liver SUV stable over time in ¹⁸F-FDG
PET imaging? J Nucl Med Technol. 2011;39(4):258-63.
(11) Stöver B, Rogalla P. CT examinations in children; Radiologe. 2008 Mar;48(3):243-8.
(12) Hirsch FW, Sattler B, Sorge I, Kurch L, Viehweger A, Ritter L, Werner P, Jochimsen T,
Barthel H, Bierbach U, Till H, Sabri O, Kluge R. PET/MR in children. Initial clinical experience
in paediatric oncology using an integrated PET/MR scanner. Pediatr Radiol. 2013;43:860-75
(13) Purz S, Mauz-Körholz C, Körholz D, Hasenclever D, Krausse A, Sorge I, Ruschke K,
Stiefel M, Amthauer H, Schober O, Kranert WT, Weber WA, Haberkorn U, Hundsdörfer P,
Ehlert K, Becker M, Rössler J, Kulozik AE, Sabri O, Kluge R. [18F]Fluorodeoxyglucose positron
emission tomography for detection of bone marrow involvement in children and adolescents
with Hodgkin's lymphoma. J Clin Oncol. 2011;29:3523-8
(14) Hasenclever D, Kurch L, Mauz-Körholz C, Elsner A, Georgi T, Wallace H, Landman-
Parker J, Moryl-Bujakowska A, Cepelová M, Karlén J, Álvarez Fernández-Teijeiro A,
Attarbaschi A, Fosså A, Pears J, Hraskova A, Bergsträsser E, Beishuizen A, Uyttebroeck A,
Schomerus E, Sabri O, Körholz D, Kluge R. qPET - a quantitative extension of the Deauville
scale to assess response in interim FDG-PET scans in lymphoma. Eur J Nucl Med Mol
Imaging. 2014;41:1301-8
(15) Boellaard R, Delgado-Bolton R, Oyen WJ, Giammarile F, Tatsch K, Eschner W,
Verzijlbergen FJ, Barrington SF, Pike LC, Weber WA, Stroobants S, Delbeke D, Donohoe
KJ, Holbrook S, Graham MM, Testanera G, Hoekstra OS, Zijlstra J, Visser E, Hoekstra CJ,
Pruim J, Willemsen A, Arends B, Kotzerke J, Bockisch A, Beyer T, Chiti A, Krause BJ. Eur J
Nucl Med Mol Imaging. 2015 Feb;42(2):328-54
(16) Kuhnert G, Boellaard R, Sterzer S, Kahraman D, Scheffler M, Wolf J, Dietlein M,
Drzezga A, Kobe C Eur J Nucl Med Mol Imaging. 2015 Aug 18.