Embed Size (px)
Citation preview
MEDICAL CANNABIS
Dr. Michael Verbora, MBA, MD, CCFPMedical Director, Canabo Medical CorpPhysician Lead, Toronto, Cannabinoid Medical ClinicFocused Designated Practice in Pain Management
October 19, 2017
Introduction – Dr. Michael Verbora
Education
Honours Bachelor Science (Biochemistry) 2008 – University of Windsor
Masters of Business Administration 2009 – Odette School of Business
Medical Doctorate 2013 – Schulich School of Medicine & Dentistry, University of Western Ontario
Family Medicine Residency 2015 – Toronto Western Hospital, University of Toronto
Experience
Cannabinoid Medical Clinic (2015 – present) – Lead Physician, Toronto
Canabo Medical Corporation (2017 – present) - Medical Director
Completed many cannabis focused IME’s in the past
DisclosureI have a financial interest in Canabo Medical Corp. which operates clinics across Canada for referred patient consultations on cannabinoid therapy.
I have received speaking honorariums from LPs, Canabo, RIDM, International Organizations
My presentation today is based on medical research and first hand experience as a cannabinoid medical doctor who has treated over 2000 patients with medical cannabis in the past two years
AgendaPatient Case
About Cannabis
Medical Evidence
Methods of Consumption
Risks/Benefits of Medical Cannabis
Canadian Cannabis LP System
Script and Clinic Operations
Case Review
Insurance Considerations

PATIENT CASE
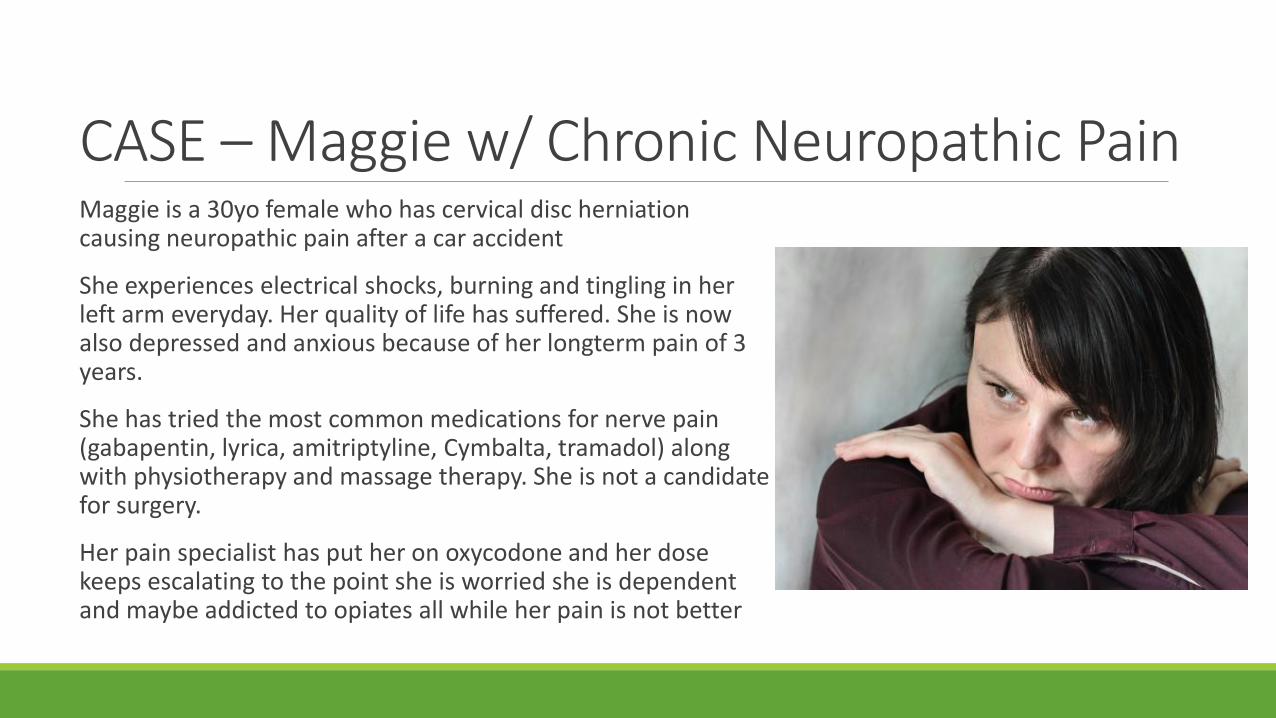
CASE – Maggie w/ Chronic Neuropathic PainMaggie is a 30yo female who has cervical disc herniation causing neuropathic pain after a car accident
She experiences electrical shocks, burning and tingling in her left arm everyday. Her quality of life has suffered. She is now also depressed and anxious because of her longterm pain of 3 years.
She has tried the most common medications for nerve pain (gabapentin, lyrica, amitriptyline, Cymbalta, tramadol) along with physiotherapy and massage therapy. She is not a candidate for surgery.
Her pain specialist has put her on oxycodone and her dose keeps escalating to the point she is worried she is dependent and maybe addicted to opiates all while her pain is not better
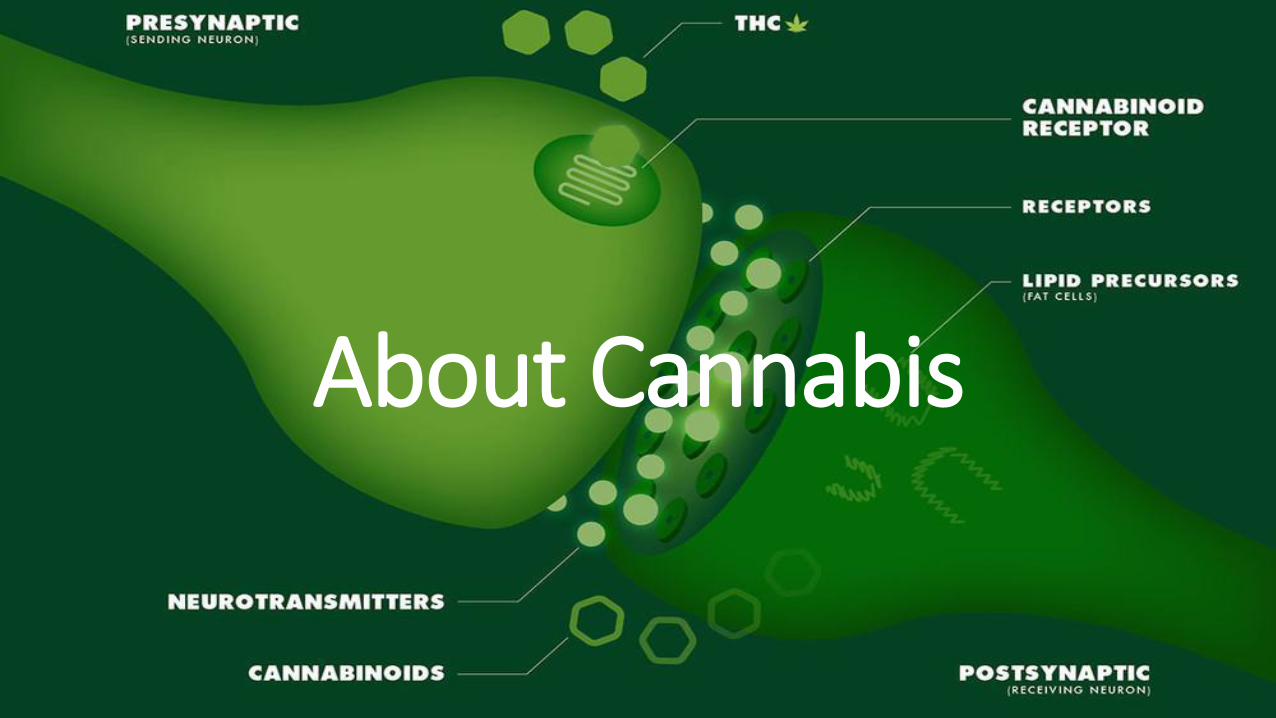
About Cannabis
DEFINITIONS
• Cannabinoids are a class of compounds that act on cannabinoid receptors in the human body
• Endocannabinoids are cannabinoids that are naturally produced in the body (endogenous)
• Phytocannabinoids are cannabinoids produced by the cannabis plan
• Synthetic cannabinoids are laboratory-synthesized compounds that bind to cannabinoid receptors
• Some are used as pharmaceuticals (e.g. Nabilone)
• Some are used as street drugs (e.g “Spice” and “K2”)
Background Information on CannabisThe body makes it’s own cannabis molecules (endocannabinoids)
The endocannabinoid system in the human body is responsible for regulating many bodily functions: immune function, sleep, pain perception, appetite, bone development, memory, cardiovascular function, digestion and more
When people run and feel euphoric, part of this is the body making cannabinoid molecules
You cannot survive without an endocannabinoid system
Cannabis augments our bodies system
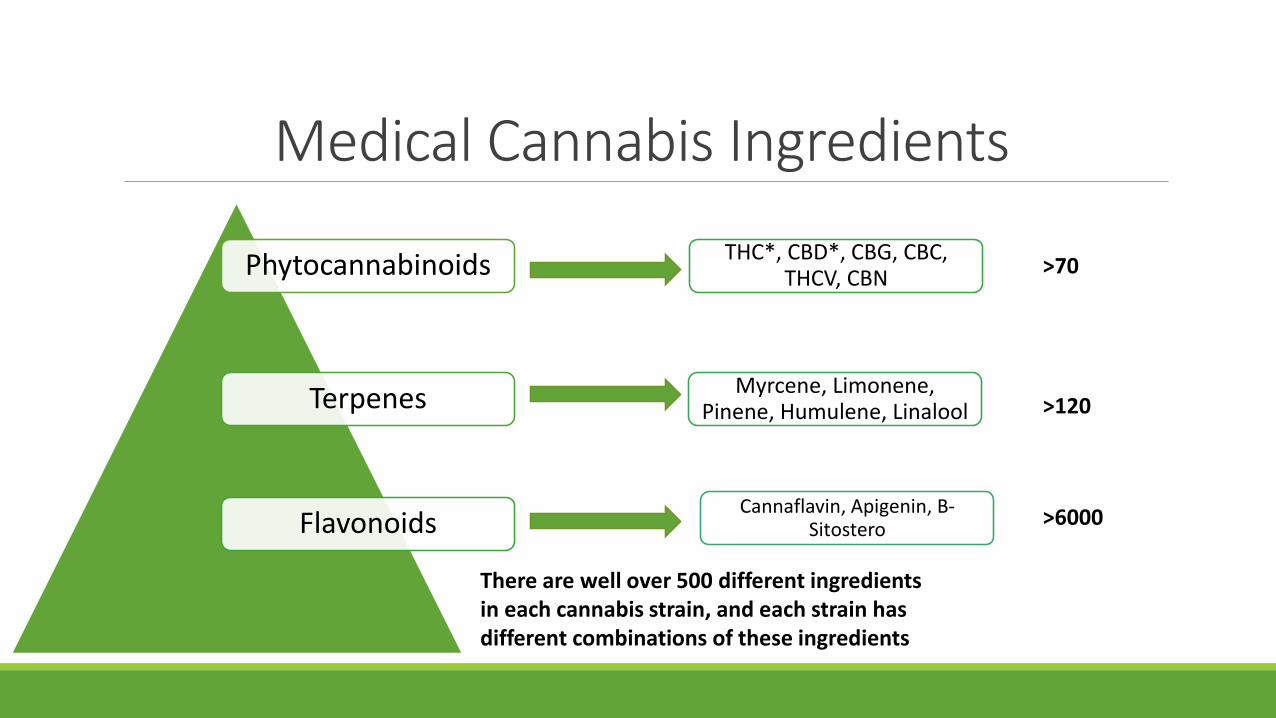
Medical Cannabis Ingredients
Phytocannabinoids
Terpenes
Flavonoids
THC*, CBD*, CBG, CBC, THCV, CBN
Myrcene, Limonene, Pinene, Humulene, Linalool
Cannaflavin, Apigenin, B-Sitostero
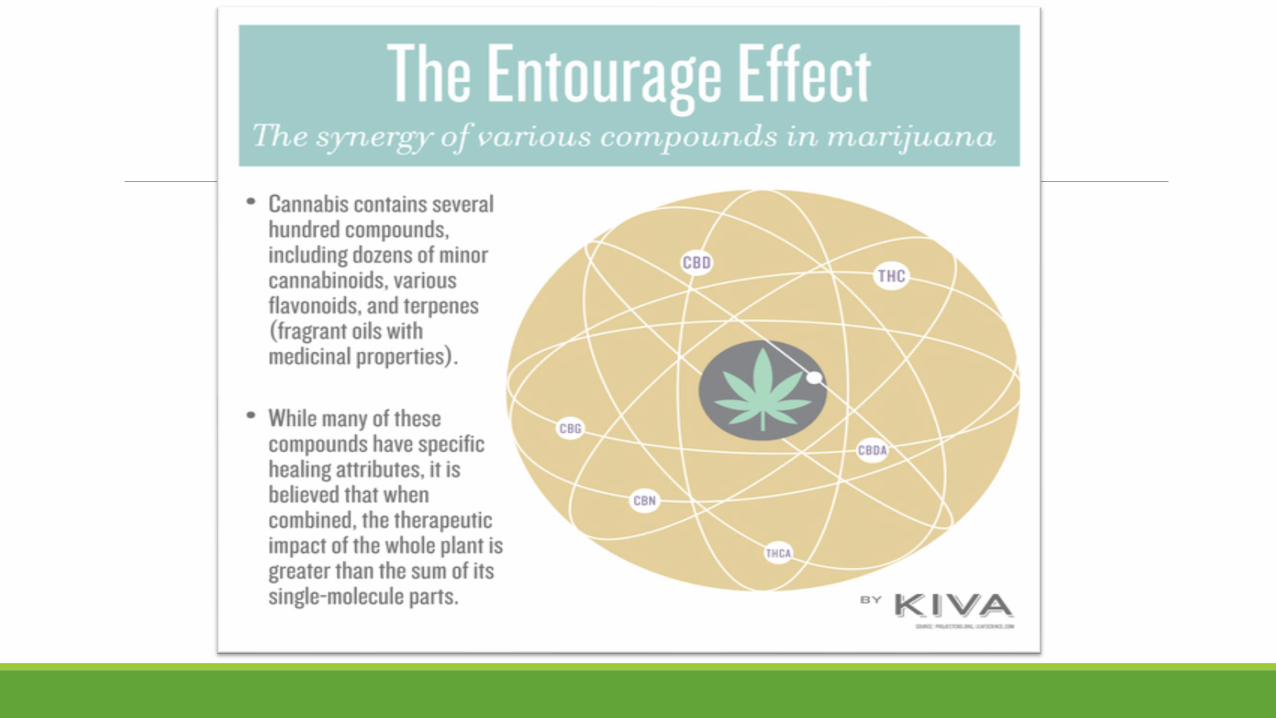
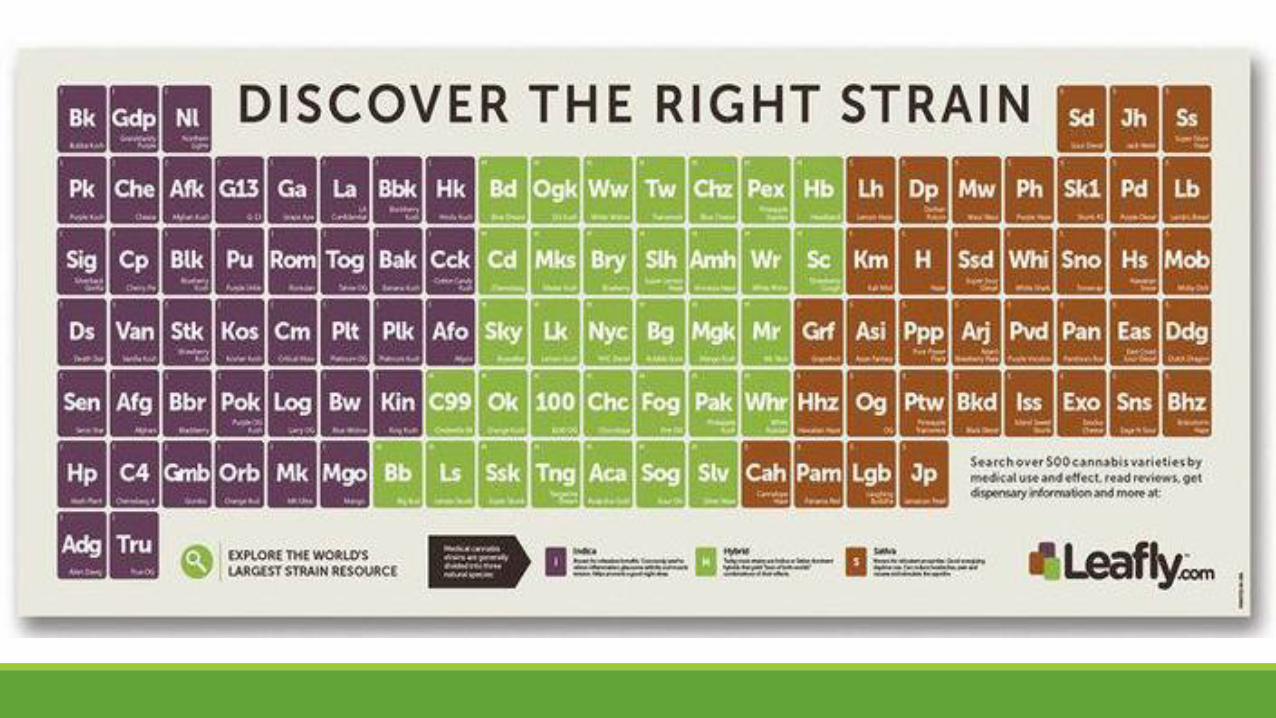
There are well over 500 different ingredients in each cannabis strain, and each strain has different combinations of these ingredients
>70
>120
>6000
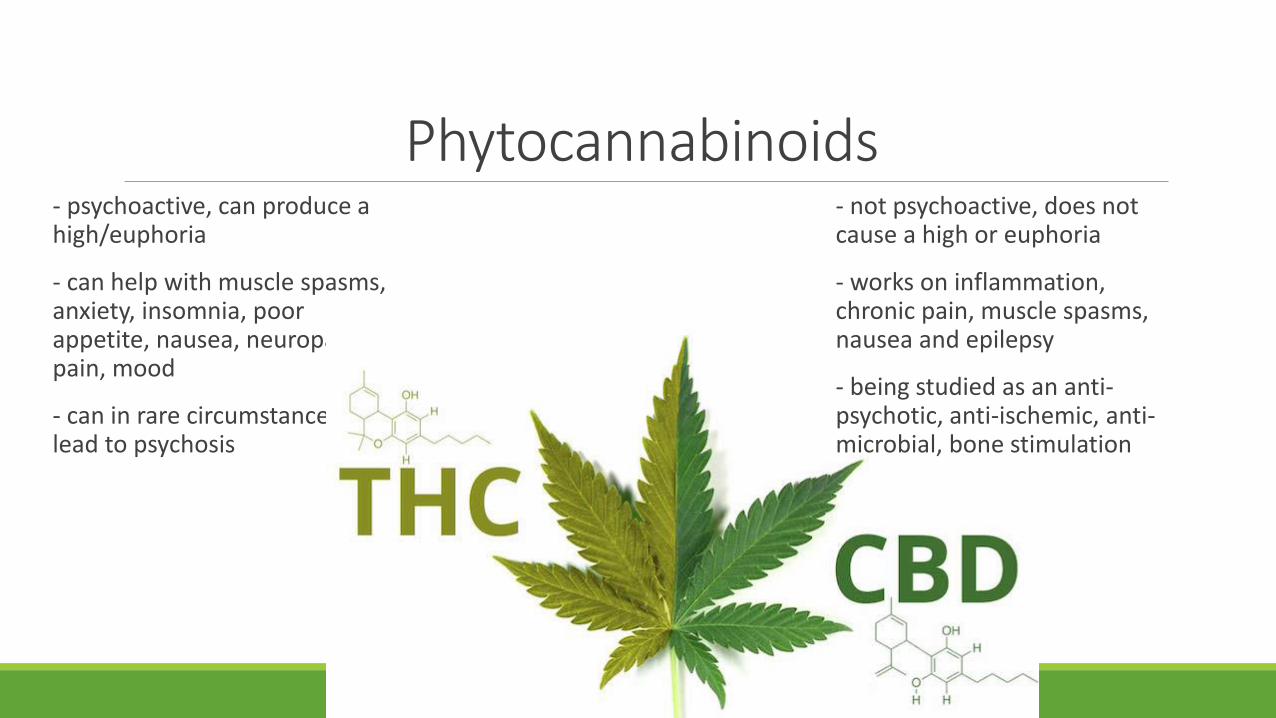
Phytocannabinoids- psychoactive, can produce a high/euphoria
- can help with muscle spasms, anxiety, insomnia, poor appetite, nausea, neuropathic pain, mood
- can in rare circumstances lead to psychosis
- not psychoactive, does not cause a high or euphoria
- works on inflammation, chronic pain, muscle spasms, nausea and epilepsy
- being studied as an anti-psychotic, anti-ischemic, anti-microbial, bone stimulation
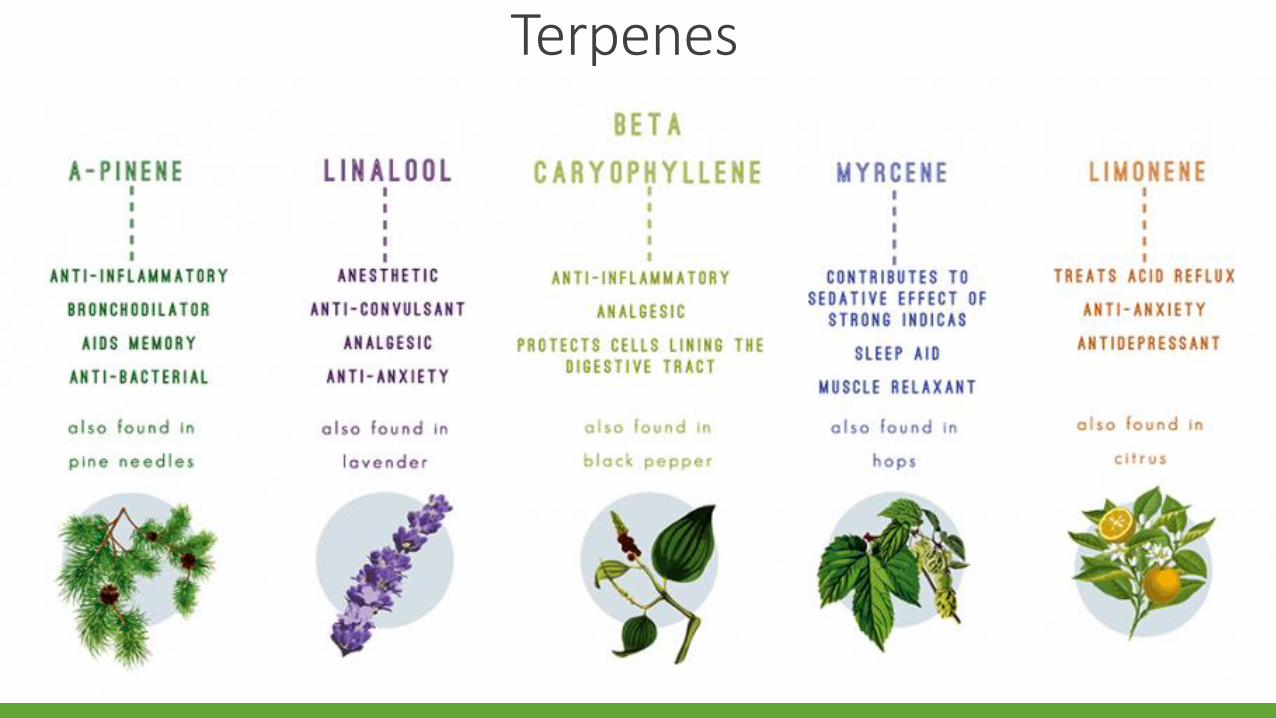
Terpenes
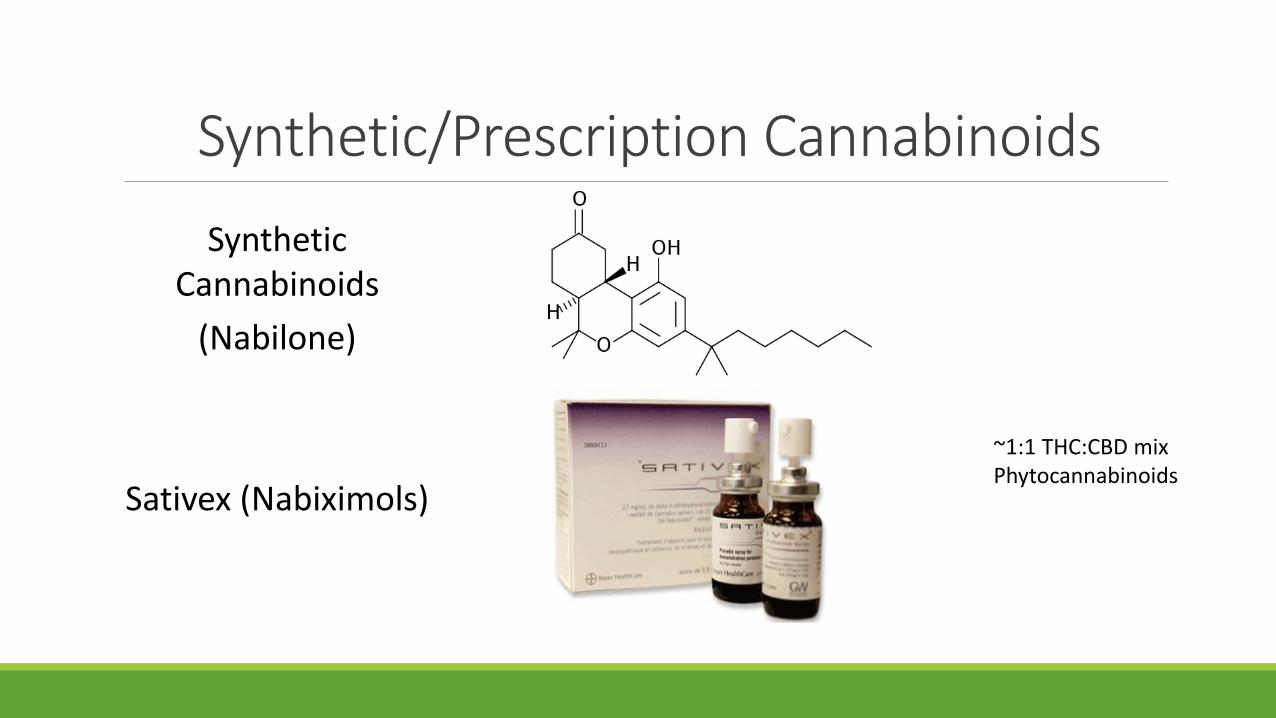
Synthetic/Prescription Cannabinoids
Synthetic Cannabinoids
(Nabilone)
Sativex (Nabiximols)
~1:1 THC:CBD mixPhytocannabinoids
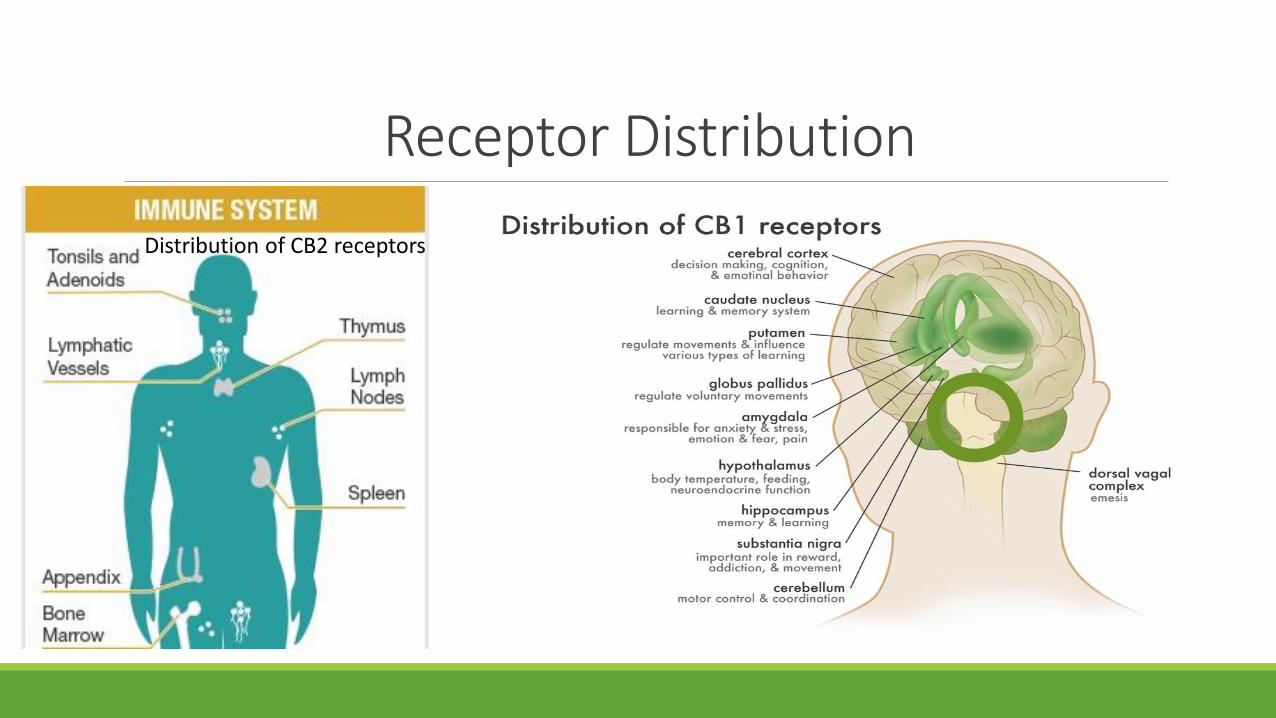
Receptor Distribution
Distribution of CB2 receptors
MEDICAL EVIDENCE
Difficulties with Cannabis Evidence - BIASACCESS BIAS - Schedule 1 drug in many countries means access to cannabis is restricted, limited by drug agencies and political organizations. Very low THC is often studied and very little studies on CBD. Does not reflect true cannabis in marketplace/streets.
RESEARCH BIAS - Scanning the literature demonstrates that 90% or more of cannabis research was to prove a NEGATIVE outcome. Positive outcome studies in the past often did not receive funding or approval.
SELECTION BIAS – Many of the harms reported in studies are conducted on recreational users, not medicinal users. Wrong population.
CONFIRMATION BIAS – Many have been told cannabis is a drug, not a medicine and have a hard time reevaluating evidence through unbiased lens.
National Academies Press (2017)Recently published 400 page document (US State Sponsored Data)
Team made up of experts in: mental health, epidemiology, public and population health, reproductive and fetal health, and cannabinoid biology
Reviewed epidemiological, and clinical trial data on therapeutic effects of cannabis, including health outcomes, as well as data from systematic reviews and primary literature since 1999
Research & EvidenceConclusions:
Substantial evidence that adults with chronic pain had a clinically significant reduction in pain symptoms compared with control patients
Patients with multiple sclerosis-related spasticity, short-term use of oral cannabinoid products improved spasticity symptoms
In adults with chemotherapy-induced nausea and vomiting oral cannabinoids are effective at alleviating symptoms
We still need high quality trials to support additional uses. Researchers need access to proper cannabis strains and potency. Positive outcomes need to be researched.
Research & EvidenceConclusions (negatives):
Smoking cannabis (while in theory is bad) demonstrated limited evidence to an association in worsening lung function
There is no evidence to conclude smoking cannabis leads to increased cancer risks of lung, head and neck
Smoking cannabis in pregnancy leads to lower birth weight
Heavy cannabis use in adolescence is related to impairments in academic achievement and education, employment and income and social relations
Cannabis use before driving increases risk of MVA
Use of cannabis is associated with psychoses (in patients with risk factors and heavy cannabis users). There is no causal relationship evidence.
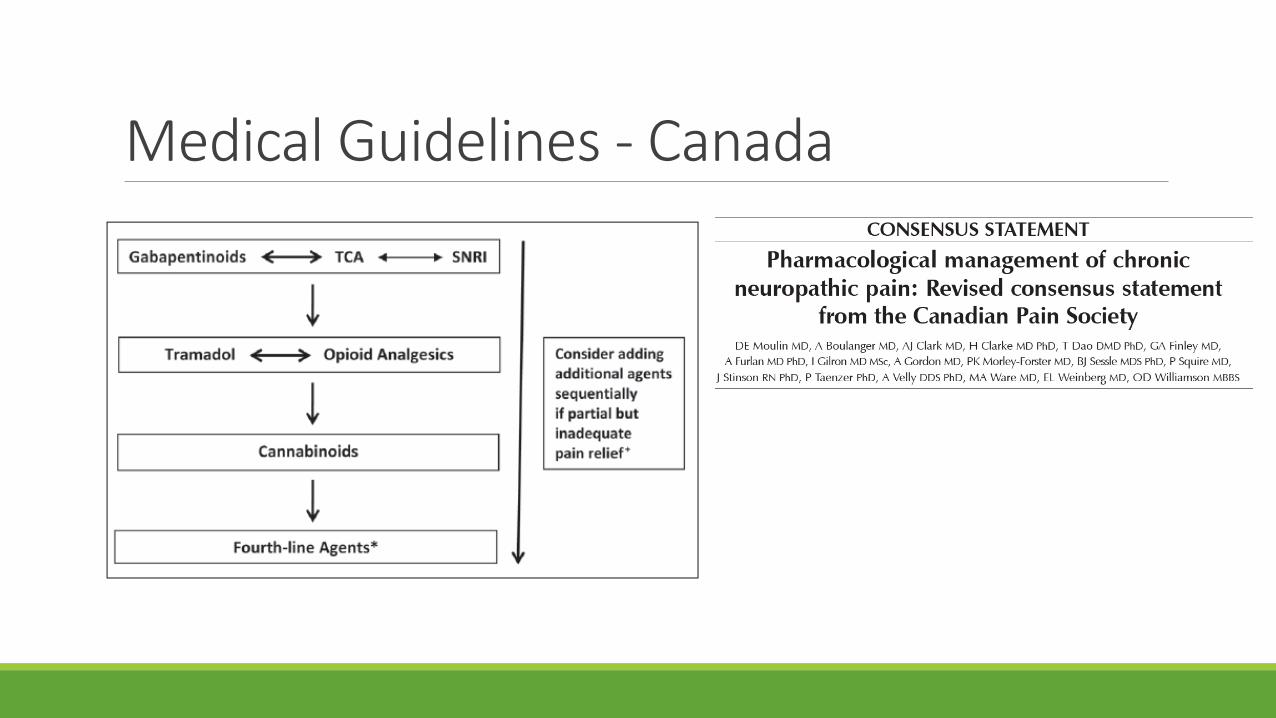
Medical Guidelines - Canada

Methods of Consumption
Delivery Methods
▪ Raw (“Juicing”)
▪ Ingestion (“Edibles”)
▪ Smoking (“Joint/Bong/Pipe”)
▪ Vaporizing
▪ Sublingual (“Tinctures”)
▪ Topical
Routes of Delivery
LUNGS GUT
Inhalation
▪ Diffusion into alveolar capillaries and then enters in the bloodstream
▪ Maximal onset occurs at 10-30 min and last 2-3 hours
▪ Metabolism occurs in the lung, liver, brain
▪ Rapid dose delivery
▪ Bioavailability factors (breath holding, duration, depth of inhalation) ~20%
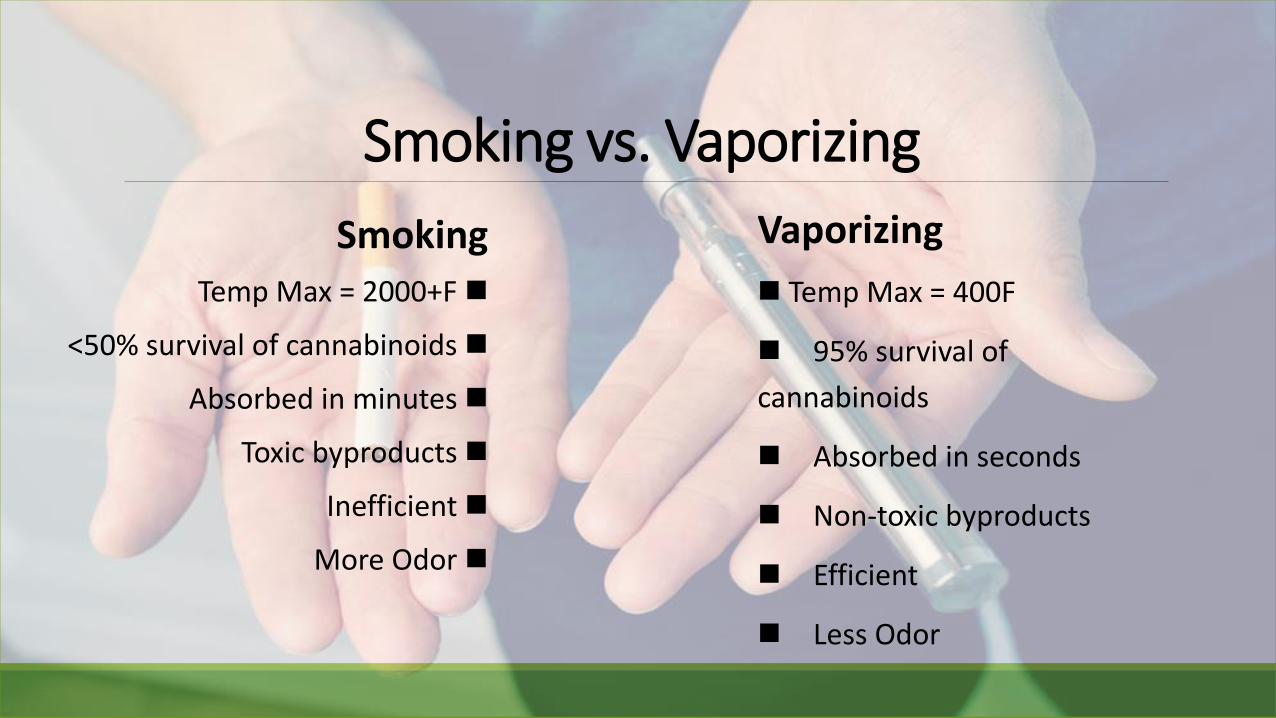
Smoking vs. Vaporizing
Smoking
Temp Max = 2000+F
<50% survival of cannabinoids
Absorbed in minutes
Toxic byproducts
Inefficient
More Odor
Vaporizing
Temp Max = 400F
95% survival of
cannabinoids
Absorbed in seconds
Non-toxic byproducts
Efficient
Less Odor
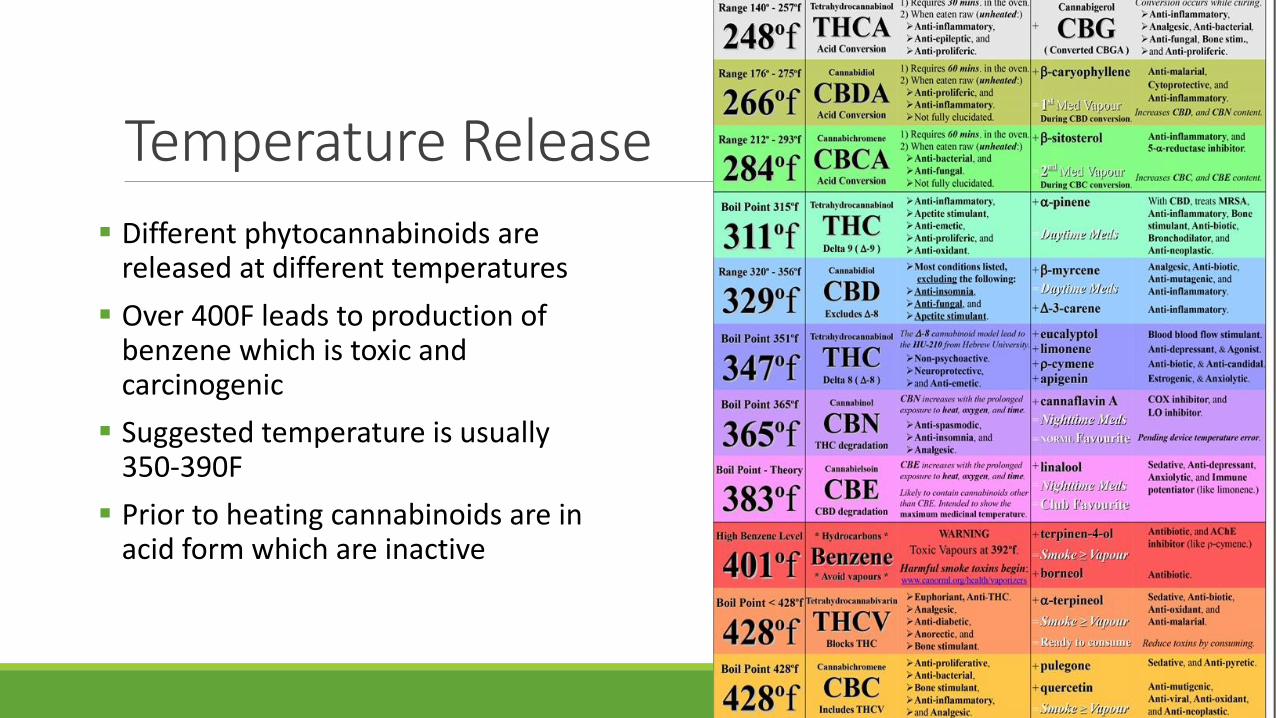
Temperature Release
▪ Different phytocannabinoids are released at different temperatures
▪ Over 400F leads to production of benzene which is toxic and carcinogenic
▪ Suggested temperature is usually 350-390F
▪ Prior to heating cannabinoids are in acid form which are inactive
Ingestion▪ Metabolized in the liver and turned into 11-hydroxy THC
via CYP450 (CYP3A4, CYP2C9, CYP2C19), CBD undergoes conversion to 7-OH CBD, 6OH-CBD
▪ Activated prior to ingestion by heating (decarboxylation)
▪ Increase in sedation or euphoria
▪ Variables to consider (High intra/inter-patient variability)
▪ Other food ingested/gastric contents
▪ Individual variation in metabolism rates
▪ Frequency of use
▪ Onset can be anywhere from 30 min to 2 hours and can last 5-8 hours
▪ Extensive liver metabolism reduces bioavailability ~13%
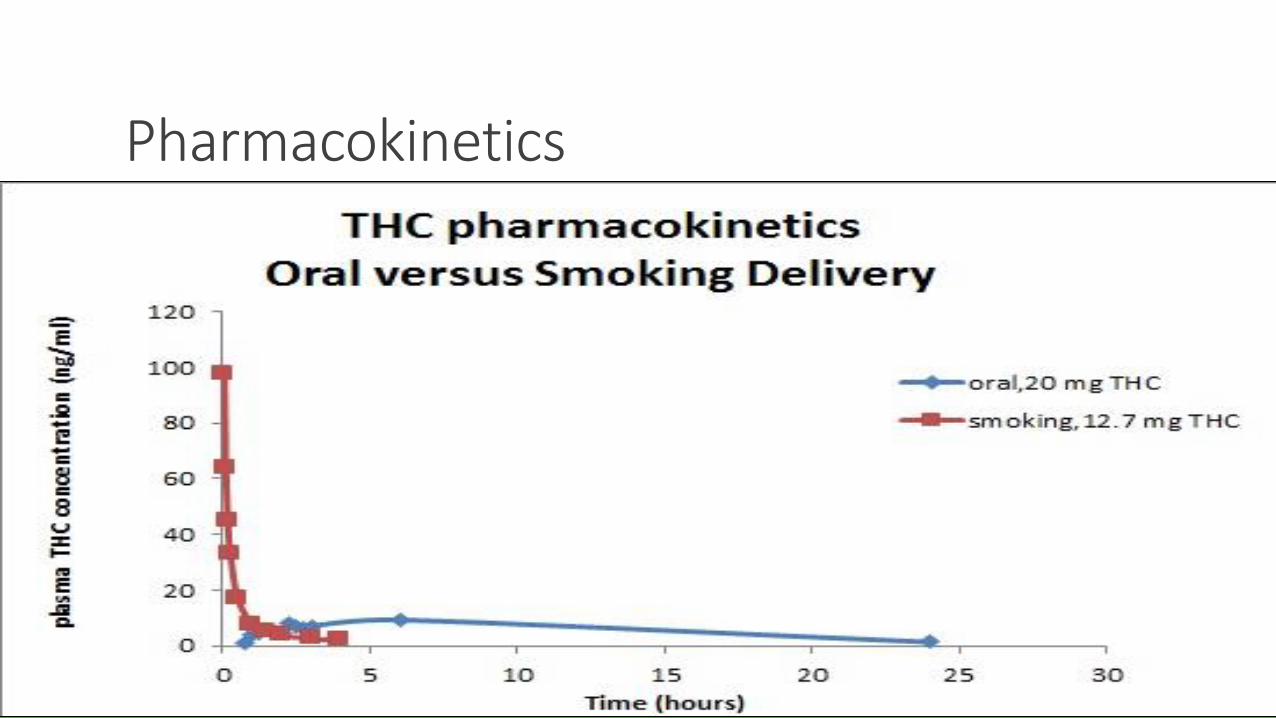
Pharmacokinetics

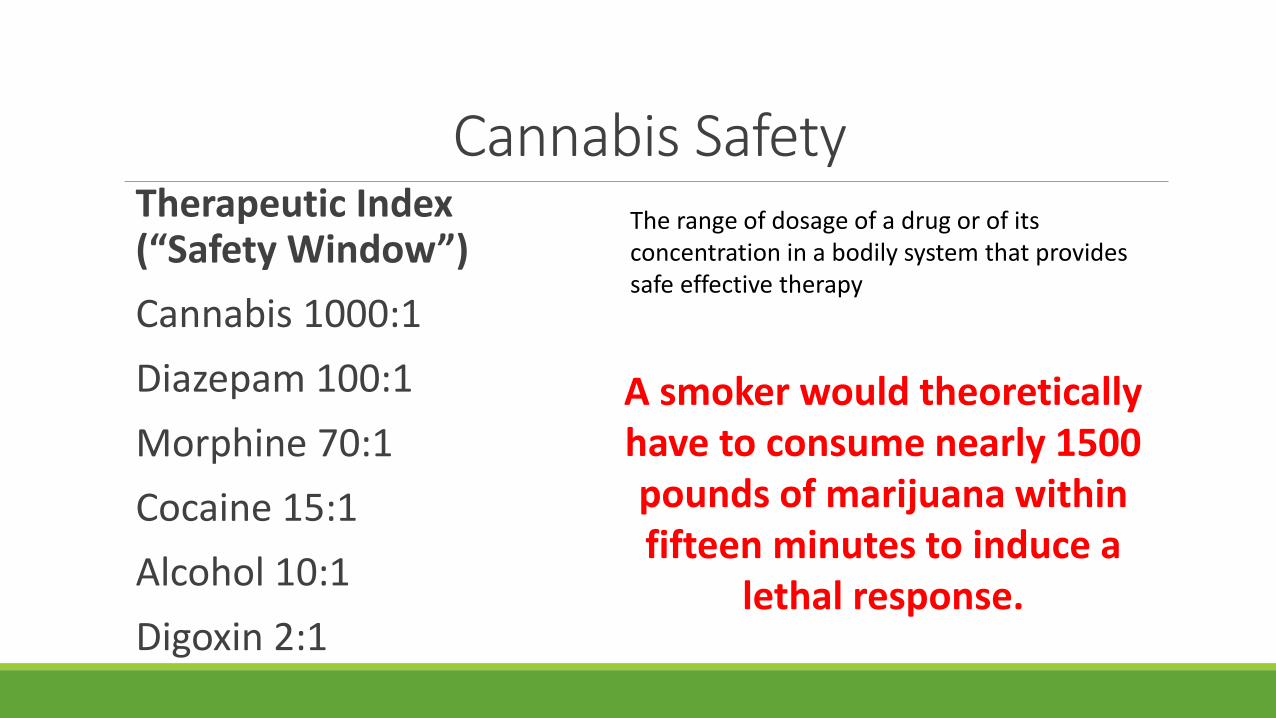
Cannabis SafetyTherapeutic Index (“Safety Window”)
Cannabis 1000:1
Diazepam 100:1
Morphine 70:1
Cocaine 15:1
Alcohol 10:1
Digoxin 2:1
A smoker would theoretically have to consume nearly 1500 pounds of marijuana within fifteen minutes to induce a
lethal response.
The range of dosage of a drug or of its concentration in a bodily system that provides safe effective therapy
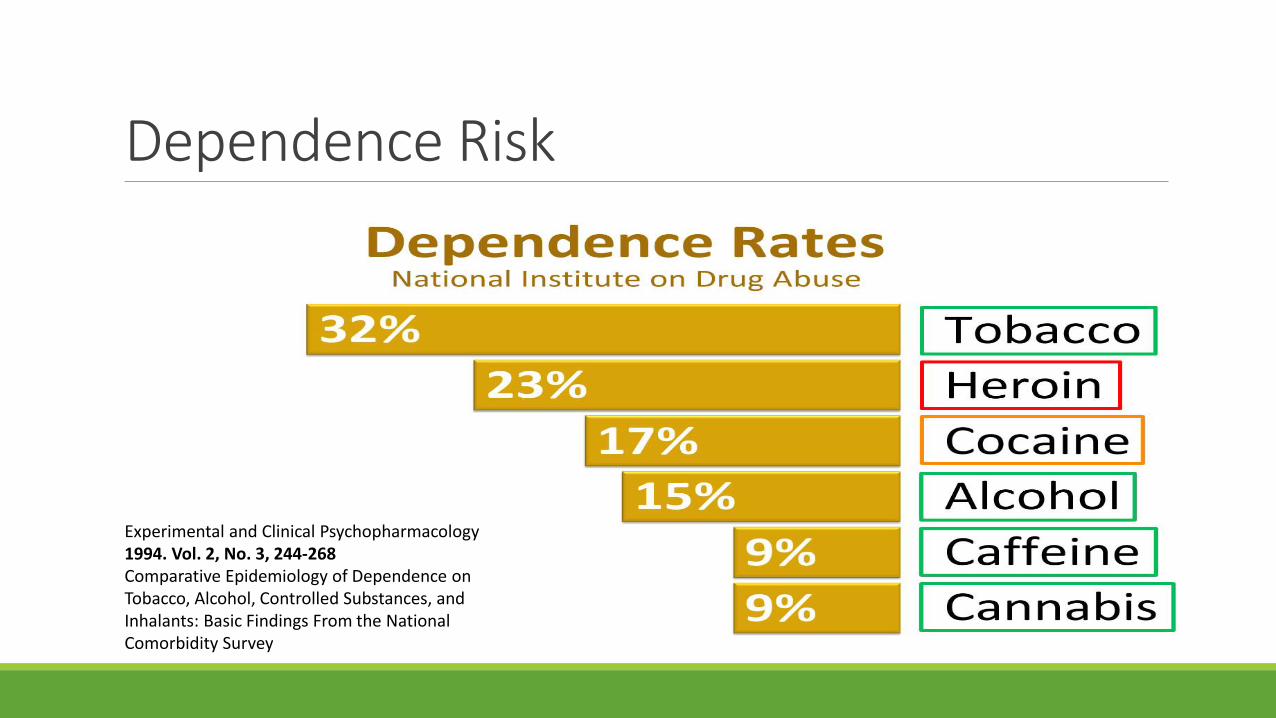
Dependence Risk
Experimental and Clinical Psychopharmacology 1994. Vol. 2, No. 3, 244-268 Comparative Epidemiology of Dependence on Tobacco, Alcohol, Controlled Substances, and Inhalants: Basic Findings From the National Comorbidity Survey
Cannabis Side EffectsCOMMON SIDE EFFECTS
• Drowsiness, Dizziness, Dry Mouth, Tachycardia (THC Induced)
• Euphoria/High (THC Induced, Inhaled>Oral)
LESS COMMON
• Nausea/Vomiting (THC Oral Consumption high dose)
• Paranoia/Anxiety (High THC, inhaled, Sativa dominant strains)
• Mild Amnesia (THC, inhaled, short-term memory)
RARE SIDE EFFECTS
• Hallucination/Psychosis/Paranoid Delusions (High THC, inhaled, FH risks or existing severe mental
health), NNH 1:23,000*
• Cannabinoid Hyper-emesis Syndrome (Chronic, excessive recreational use of THC)
• Depression/Anxiety (Heavy recreational cannabis use in those under 25 years of age)

MEDICAL CANNABISCANADIAN SYSTEM
Canadian Licensed Producer System
Company develops facilities, security, growing team, management team, capital funding
Government inspects, evaluates, reviews companies and then grants license
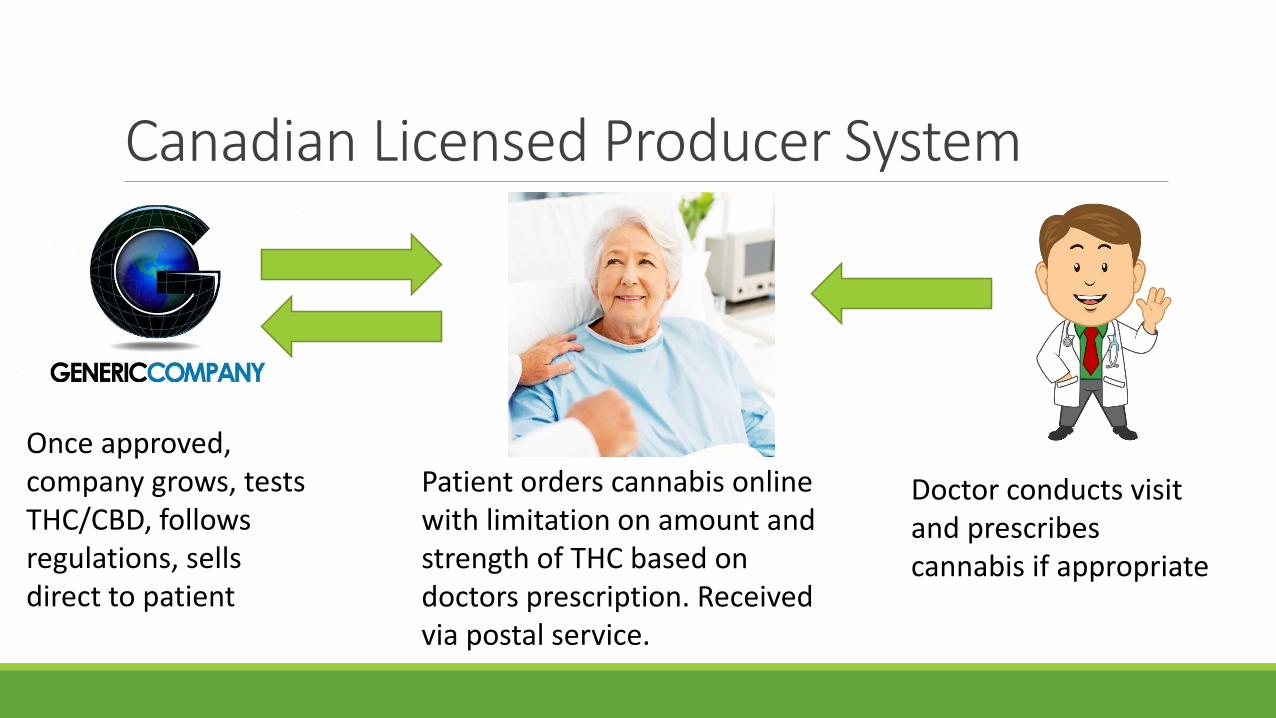
Canadian Licensed Producer System
Once approved, company grows, tests THC/CBD, follows regulations, sells direct to patient
Patient orders cannabis online with limitation on amount and strength of THC based on doctors prescription. Received via postal service.
Doctor conducts visit and prescribes cannabis if appropriate

Available Products
Future products: inhalers, creams/topicals, patches, capsules
Scripts and Clinic Operations
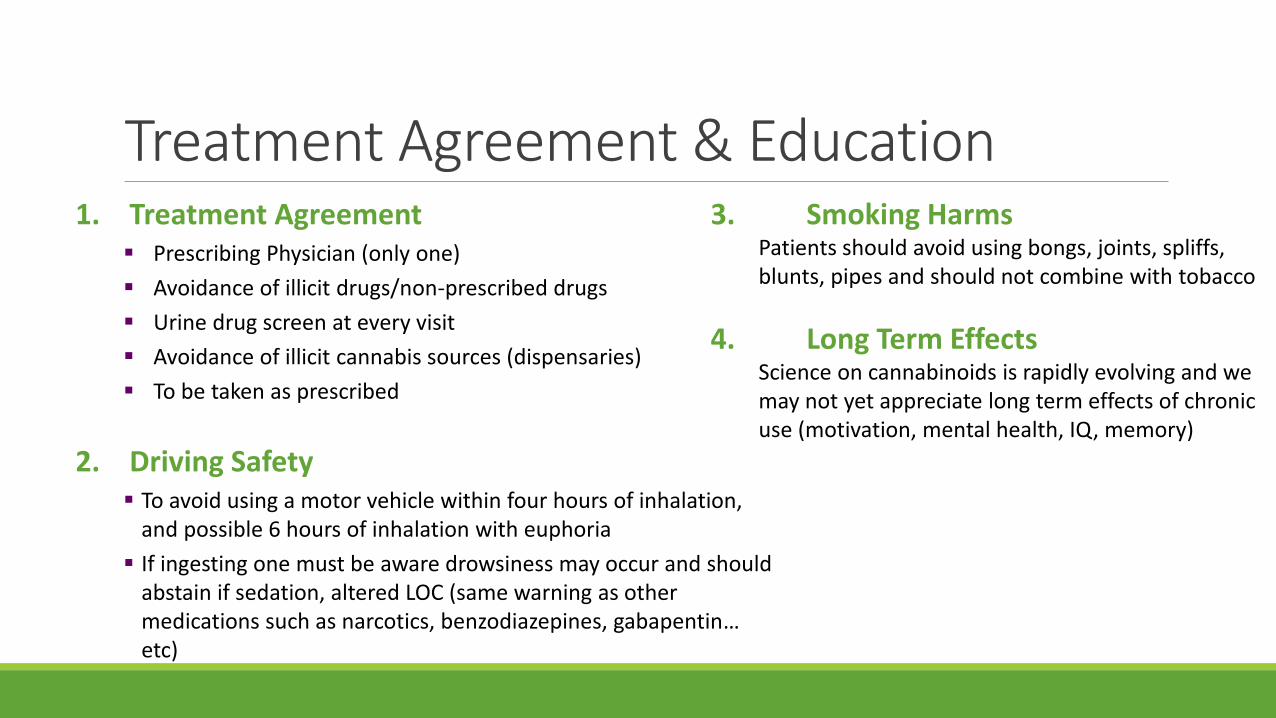
Treatment Agreement & Education1. Treatment Agreement
▪ Prescribing Physician (only one)
▪ Avoidance of illicit drugs/non-prescribed drugs
▪ Urine drug screen at every visit
▪ Avoidance of illicit cannabis sources (dispensaries)
▪ To be taken as prescribed
2. Driving Safety▪ To avoid using a motor vehicle within four hours of inhalation,
and possible 6 hours of inhalation with euphoria
▪ If ingesting one must be aware drowsiness may occur and should abstain if sedation, altered LOC (same warning as other medications such as narcotics, benzodiazepines, gabapentin…etc)
3. Smoking HarmsPatients should avoid using bongs, joints, spliffs, blunts, pipes and should not combine with tobacco
4. Long Term EffectsScience on cannabinoids is rapidly evolving and we may not yet appreciate long term effects of chronic use (motivation, mental health, IQ, memory)
Documentation RequiredFollowing Documents are required for a legal prescription in Canada:
✓MD signed prescription✓Amount to be used daily, THC limit
and duration of prescription✓Licensed Producer Form
(downloadable form online)

PATIENT CASE
CASE – Maggie w/ Chronic Neuropathic PainMaggie was started on CBD cannabis in the day and THC cannabis at night vaporized
At her first visit she reported she was feeling 25% better (less pain) and she lowered her opiates by 10%. We increased her THC strength and CBD strength.
At her second visit she reported she was 50% better, and lower her opiates by 50%. She also lost thirty pounds and her depression and anxiety was getting better. We moved some of her inhaled cannabis to oral cannabis oils (ingested).
At her third visit she was 80% better, she was now off her opiates completely. She has lost 70lbs. She is carrying her 2 year old daughter for the first time in her life. She often wonders without cannabis what her life would have turned out to be.

Employer Considerations
Medical Cannabis and Insurance/EmployersMedical Cannabis consumption continues to rise
Medical cannabis is similar to other prescription drugs that have the potential to impair and employee’s ability to perform their duties and responsibilities
Employers have a legal duty to accommodate those returning to work on medical cannabis
Workplace Safety needs to be considered when patients are using ANY potentially cognitive impairing drug, cannabis included
There is no scientific test available today to confirm impairment. One must rely on physical presentation to diagnose impairment
The right to use cannabis does not entitle employees to be impaired at work or inflict harm/danger on tehmselves/others
Accommodation Considerations• Does the disability require a leave of absence?
• Is it a short-term or long-term disability (prognosis)?
• Is consumption of Cannabis at work needed? Frequency?
• How is the Cannabis consumed?
• Can it be used after work hours only?
• Does the employee hold a safety sensitive role?
• Can they confirm their registration with an LP?
Medical Information (Confirm)• Seek information from physician about workplace restrictions
• Confirm ability to work unimpaired
• Onus is on Employer to do medical due diligence
• Employer may want to conduct an IME with a qualified expert to confirm the above
Undue Hardship•Duty to accommodate has limits (ie. Undue Hardship for employer)
◦ Under the Canadian Human Rights Act, an employer or service provider can claim undue hardship when adjustments to a policy, practice, by-law or building would cost too much, or create risks to health or safety
◦ There is no precise legal definition of undue hardship or a standard formula for determining undue hardship. Each situation should be viewed as unique and assessed individually
◦ It is not enough for an employer to claim undue hardship based on an assumption or opinion, or by simply saying there is some cost. To prove undue hardship, the employer will have to provide evidence as to the nature and extent of the hardship
Accommodation Options• Reassign employee to different role or re-bundle duties
• Remove safety sensitive duties
• Allow longer breaks and/or flexible schedule or use leave time
• Allow employee to work from home
• Be collaborative/creative
Employer Cannabis Policies• If internal drug policy not in place, now is the time (recreational cannabis coming 2018)
• Recreational cannabis should be treated like any other controlled substance (eg. Alcohol)
• If policy in place should be clarified to ensure employees understand legalization of cannabis does not change anything when it comes to the workplace
• Employers must ensure safety of employees and they have a right to enforce zero-tolerance policy against intoxication or impairment at work
• Good Policies establish:• The priority of a safe workplace;
• The shared responsibility for acceptable conduct;
• Consequences of non-compliance
• The communication protocol for empl0uyees needing information or answers to questions
• Specific section dedicated to medical cannabis
Legal Canadian Cases in Cannabis• French v. Selkin Logging
• Wilson v. Transparent Glazing Systems
• Old v. Ridge County Contracting
• IBEW Local 1620 v. Lower Churchill Transmission Construction Employers Association
• Calgary (City) v. CUPE
Prescribing Pattern ConsiderationsIn my experience there is limited expertise in prescribing cannabinoids, individual practitioners prescribing in their current practice have limited experience/knowledge
Cannabis is still a last line therapy and other medical therapies should be trialed prior to using medical cannabis
In my experience I often see patients being prescribed cannabis far too early in their treatment plan, IME from cannabinoid experts can help clarify whether cannabis is appropriately or inappropriately being prescribed
Cannabinoid Medical Clinic has expertise in prescribing cannabinoids with over 30,000 patients to date across the country
THANK YOU