Embed Size (px)
Citation preview
What actually happens in a
Pediatric Dental Office?
EstherYang,DDSApril7,2018
• Chief of ServiceDepartment of Dental SurgeryTexas Children’s Hospital• Adjunct Clinical Assistant Professor Department of Pediatric Dentistry UT School of Dentistry at Houston
NoDisclosures
• NeitherI,normembersofmyimmediatefamily,haveanyfinancialrelationshipswithcommercialentitiesthatmayberelevanttothispresentation.
April 9, 2018 Baylor College of Medicine 2
Disclaimers
• TheopinionsexpressedinthispresentationarethoseofthespeakerandnotnecessarilythoseoftheTexasChildren’sHospital.
• Theopinionsexpressedinthiscourseshouldnotbeconstructedasadvicetocareforspecificpatients.
April 9, 2018 Baylor College of Medicine 3
CourseObjectives
– CollaboratewithDentalprovidertointegratehealthcareneeds.
– Identifyspecialconsiderationssuchas:labvalues,medications,andantibioticprophylaxis
– Assessingdentalemergencies.
April 9, 2018 Baylor College of Medicine 4
Dental Home
• The American Academy of Pediatric Dentistry indicates that an establishment of a Dental Home no later than 12 months of age.
GatheringinformationanddevelopingaplanwithHealthcareprovider• Identifydentaltreatmentneeds• Assesspediatricpatientcompliance.• Identifybesttreatmentmodalityforpatients.• Identifymedicalstatusandcommunicatewith
primarycareprovider• HistoryandPhysical,medicalclearances.
April 9, 2018 Baylor College of Medicine 6
Typical Pediatric Patients
• Definitely Positive• Interest in Dental
procedures• Good Rapport with
Dentist
• Definitely Negative• Refusal of treatment• Forceful crying• Fearfulness
PatientCompliance
April 9, 2018 Baylor College of Medicine 8

What is our GOAL?
• TO MAKE OUR PEDIATRIC PATIENTS AND THEIR PARENTS AS COMFORTABLE AS POSSIBLE!
• Childlife Specialist, behavior therapist
Basic Behavior GuidanceTell Show Do

Voice Control

Non-verbal communication
Positive Reinforcement
Advanced Behavior Guidance
1. Protective Stabilization2. Nitrous Oxide3. Sedation4. General Anesthesia
Protective Stabilization(Papoose Board)

Protective Stabilization
• Parent places child in papoose• Parent present during treatment• Dentist removes patient from papoose at end of procedure• Consent from parent• Used as behavior as management• Social stigma of papoose• Indications:
– Emergency– Previously cooperative and became uncooperative mid treatment– Uncooperative with limited treatment unable to undergo
sedation– Sedated patient with untoward movements
Nitrous Oxide … Laughing Gas
Nitrous Oxide :Pros/Cons
• Pros: Anxiolysis, Analgesic, Decrease Gag Reflex, Increase tolerance for longer appointments, potentiate effects of sedatives, Favorable parental and patient acceptance
• Cons: Nausea, vomiting, diffusion hypoxia, lack of potency, dependant on psychological reassurance, interference of nasal hood with injection in maxillary region, ability to breath through nose
Nitrous Oxide: Contraindication
• Some chronic obstructive pulmonary diseases• Severe emotional disturbances (Cleft Lip &
Palate) drug-related dependencies• First trimester of pregnancy• Treatment with Bleomycin sulfate• Methylenetetrahydrofolate (MTHFR)
reductase deficiency• Vitamin B12 (Cobalamin) deficiency• Acute Otitis Media
Oral Sedation Sedation vs. Screamation
• Demerol, Phenergan, Nitrous Oxide, & 2% Lidocaine w/1:100,000 epinephrine
• Demerol, Hydroxyzine, Nitrous Oxide & 2% Lidocaine w/1:100,000 epinephrine
• Chloral Hydrate, Nitrous Oxide & 2% Lidocaine w/1:100,000 epinephrine
• Versed, Nitrous Oxide & 2% Lidocaine w/1:100,000 epinephrine
Sedation:Pros/Cons
• Pros:•Patient does not “remember” the event.•“less traumatizing”•Financial•Availability
• Cons:• Still need papoose board• Need to carefully monitor due to increased risk• Parents in vs out of room• Costs• Predictability varies• Treatment amount
General Anesthesia
• Pros:• Can perform all treatments in one visit• Cooperation
• Cons:• Long waiting time• Increased risks• Costs
HistoryandPhysicalMedicalclearances.
• Types of Procedures:
– Oral Sedation: ASA I and ASA II
– IV Sedation: ASA I and and ASA II
• Dental Anesthesiologist or MD anesthesiologist
– General Anesthesia
• Unclear medical history from parents
• How well controlled are they?
– Asthma, Cardiac, Cancer, Sickle Cell Anemia,
Muscular dystrophy
– Airway
– Immunocompromised
– Post-operative issuesApril 9, 2018 Baylor College of Medicine 23
AntibioticProphylaxis• CardiacCondition• CompromisedImmunity• Shunts,Indwellingvascularcatheters,medicaldevices
• Prostheticjoints– nolongersupported
April 9, 2018 Baylor College of Medicine 24
• DentalTreatment– Dentalproceduresthatinvolvemanipulationofgingivaltissueortheperiapicalregionoftheteethororalmucosa
– Possibleincreasedbacteremiaduringprocedure
– Extractions,scaling,invasivedentalprocedures
April 9, 2018 Baylor College of Medicine 25
Cardiac Conditions
• Prosthetic cardiac valve or prosthetic material used for cardiac valve repair
• Previous infective endocarditis• Congenital Heart Disease (CHD)• Cardiac Transplantation recipients who
develop cardiac valvulopathy.
April 9, 2018 Baylor College of Medicine 26
Congenital Heart Disease (CHD)
– Unrepaired cyanotic CHD, including palliative shunts and conduits.
– Completely repaired congenital heart defect with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first six months after the procedure
– Repaired CHD with residual defects at the site or adjacent to the site of prosthetic patch or prosthetic device
April 9, 2018 Baylor College of Medicine 27
Compromised Immunity
• Immunosuppresionsecondaryto:– HIV– Severecombinedimmunodeficiency– Neutropenia– Cancerchemotherapy– Hematopoieticstemcellorsolidorgantransplantation
• SickleCellAnemia• Diabetes• Chronicsteroiduse
April 9, 2018 Baylor College of Medicine 28
Shunts,Indwellingvascularcatheters,medicaldevices
• Nonvalvular devices, catheters, cardiovascular implantable electronic devices only at time of placement
• Shunts: – Vascular access
• ventriculoatrial, ventriculocardiac, and ventriculovenus shunts.
– Not ventriculoperiotoneal shunts
April 9, 2018 Baylor College of Medicine 29
April 9, 2018 Baylor College of Medicine 30
AHAGuidelinesforInfectiveEndocarditisProphylaxis:
Give30min-1hourpriortodentaltreatment.Amoxicillin50mg/kg,maximum2,000mgClindamycin20mg/kg,maximum600mg
• Patient requires antibiotic prophylaxis– Patient will be getting dental treatment in OR.
Should I prescribe them antibiotics prior?– Referring the patient to your office for
consultation because they have cavities. Should I prescribe them antibiotics prior?
April 9, 2018 Baylor College of Medicine 31
LaboratoryValues• AbsoluteNeutrophilCountsandImmunocompromised– >2000antibioticprophylaxisnotnecessary– 1,000-2,000:Clinicaljudgement– <1,000:Antibioticnecessary– <500:Emergenttreatmentneeds.
• Plateletsandbleedingrisk– >75,000– 40,000-75,000Increasedbleeding,possibletransfusionneeded
– <40,000Transfusionneeded,Emergenttreatmentonly
April 9, 2018 Baylor College of Medicine 32

April 9, 2018 Baylor College of Medicine 33
Dental Emergencies
• Active Dental Infection• Dental Trauma
April 9, 2018 Baylor College of Medicine 34
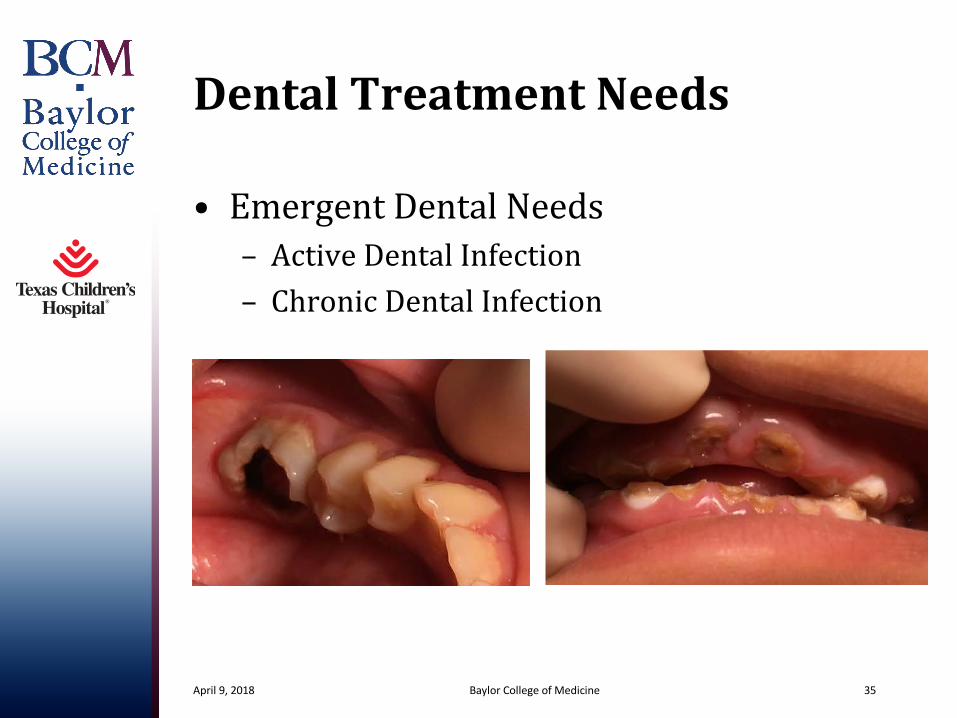
DentalTreatmentNeeds
• EmergentDentalNeeds– ActiveDentalInfection– ChronicDentalInfection
April 9, 2018 Baylor College of Medicine 35
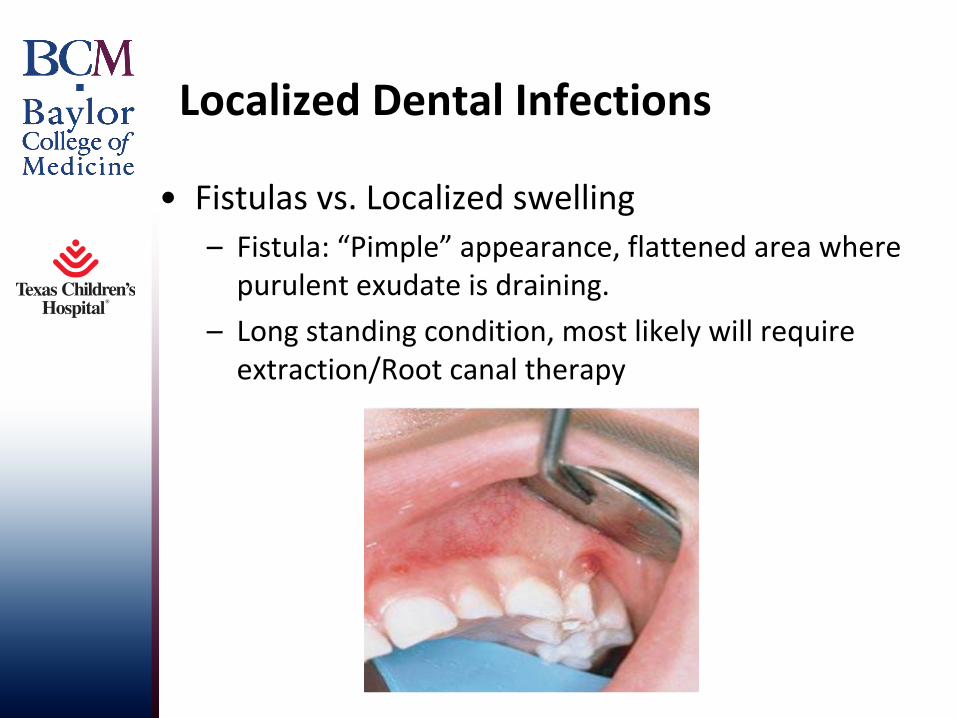
Localized Dental Infections
• Fistulas vs. Localized swelling– Fistula: “Pimple” appearance, flattened area where
purulent exudate is draining.– Long standing condition, most likely will require
extraction/Root canal therapy
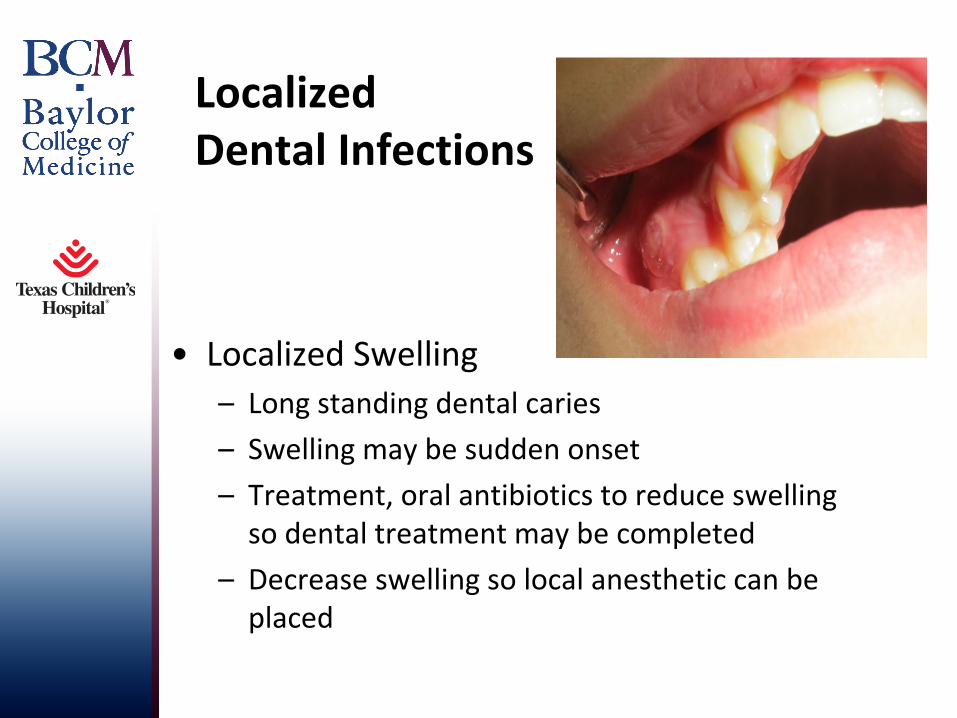
Localized Dental Infections
• Localized Swelling– Long standing dental caries– Swelling may be sudden onset– Treatment, oral antibiotics to reduce swelling
so dental treatment may be completed– Decrease swelling so local anesthetic can be
placed
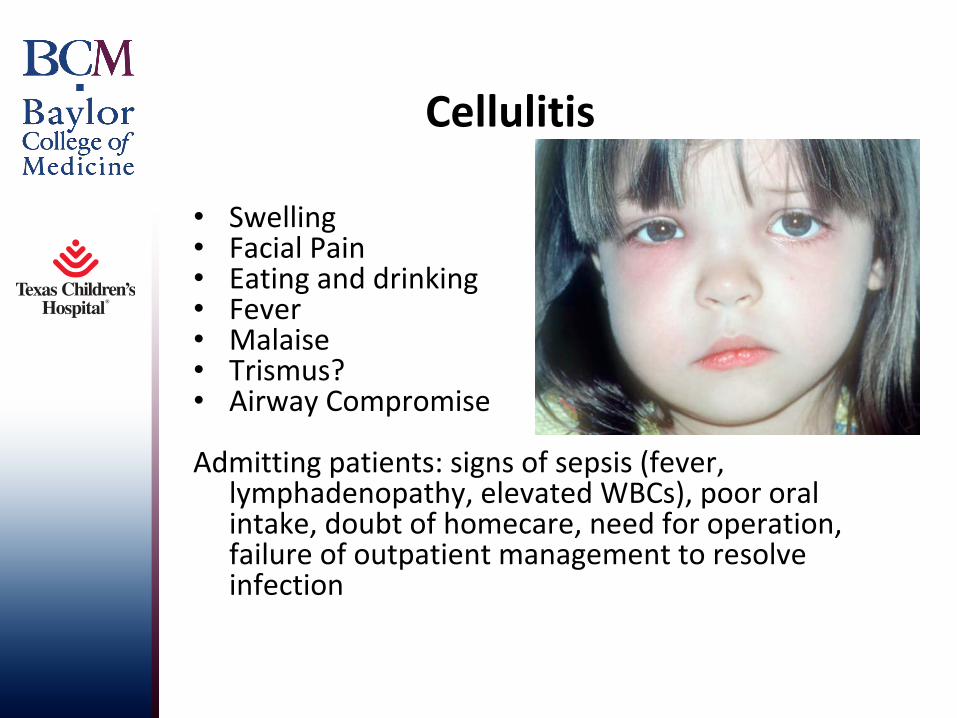
Cellulitis
• Swelling• Facial Pain• Eating and drinking• Fever• Malaise• Trismus?• Airway Compromise
Admitting patients: signs of sepsis (fever, lymphadenopathy, elevated WBCs), poor oral intake, doubt of homecare, need for operation, failure of outpatient management to resolve infection
Erythema, right at midline, unilateral
Trismus, Limited opening
EmergentDentalNeedsAirwayConcerns
April 9, 2018 Baylor College of Medicine 40
§ Antibiotics § IV Antibiotics vs I&D
§ Pen VK, Clindamycin, Unasyn§ May require admission § Removal of source of infection§ Surgical intervention§ Active infection, difficulty with local
anesthesia
Orofacial Trauma
• Assessment• Dental Effects• Soft Tissue• Hard Tissue

Orofacial Injury Assessment
• Review health history• Assess
systemic/neurological effects
• Evaluate tetanus immunization
• Be alert to potential child abuse
(Cameron, Angus C.. Handbook of Pediatric Dentistry, 2nd Edition. C.V. Mosby, 2003.)
Tetanus
Clinical Examination
• Facial and neck palpation
• Intraoral examination• Primary site• Knee to knee position.
– Under the age of 3 years old
• Parents help stabilize the patient
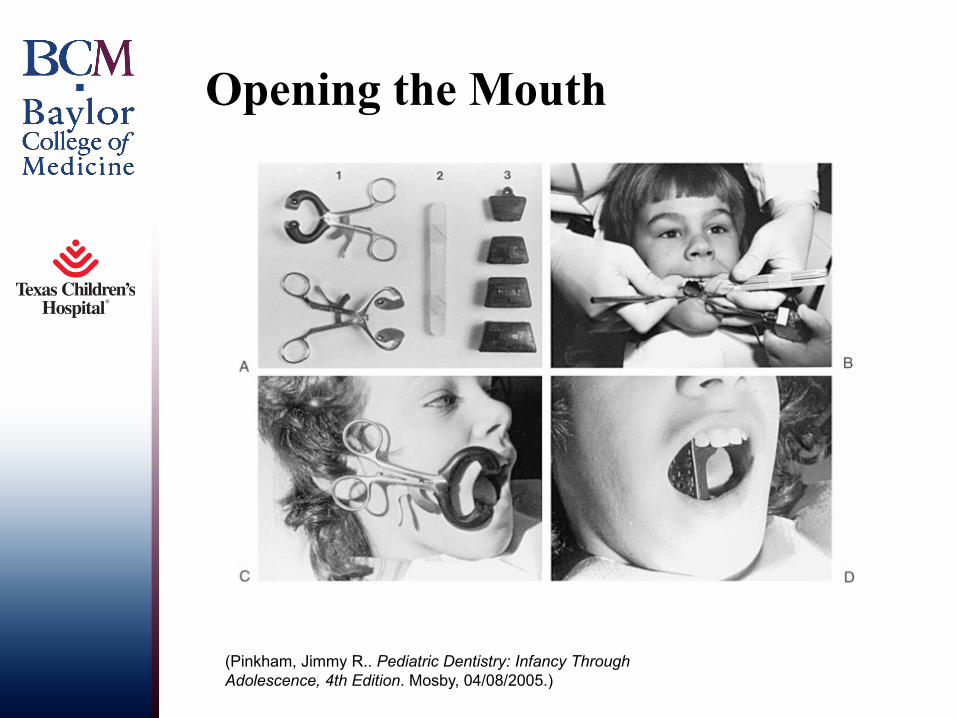
Opening the Mouth
(Pinkham, Jimmy R.. Pediatric Dentistry: Infancy Through Adolescence, 4th Edition. Mosby, 04/08/2005.)
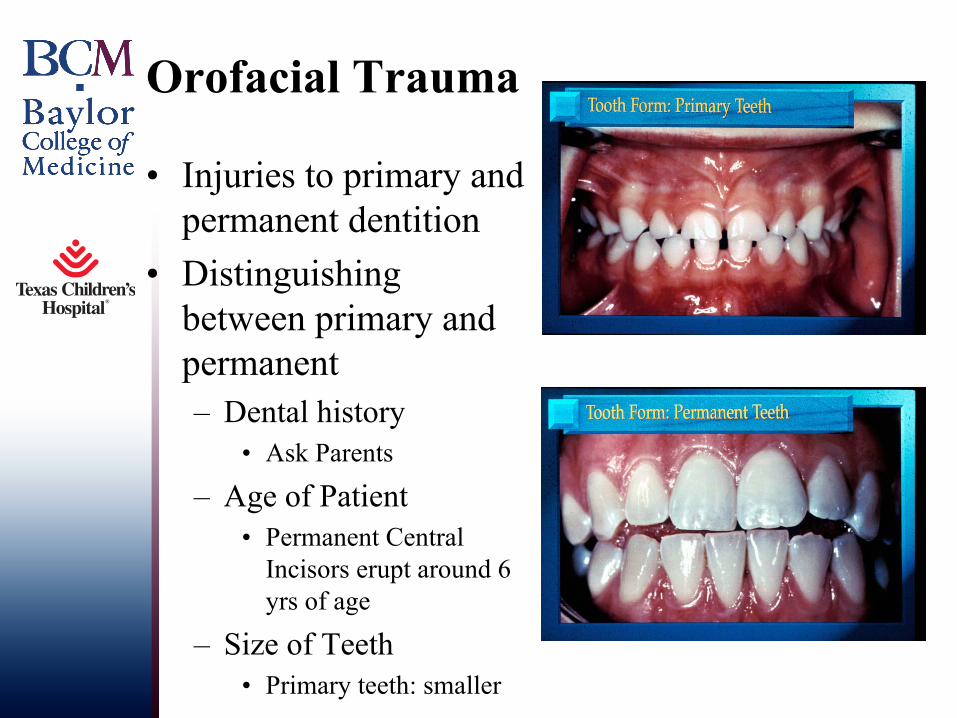
Orofacial Trauma
• Injuries to primary and permanent dentition
• Distinguishing between primary and permanent– Dental history
• Ask Parents
– Age of Patient• Permanent Central
Incisors erupt around 6 yrs of age
– Size of Teeth• Primary teeth: smaller
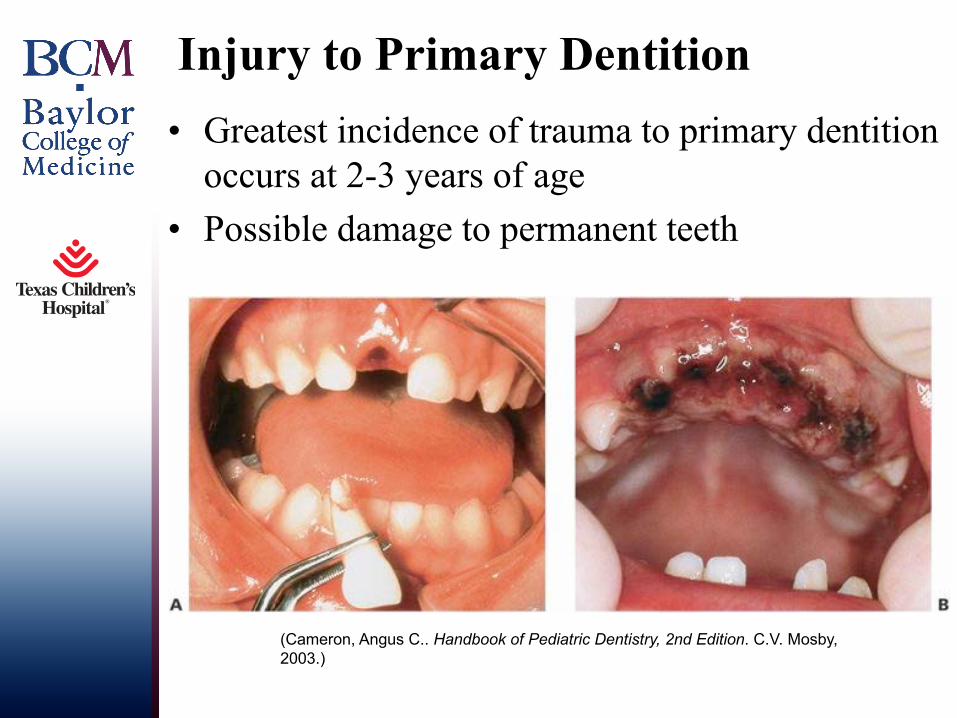
Injury to Primary Dentition• Greatest incidence of trauma to primary dentition
occurs at 2-3 years of age• Possible damage to permanent teeth
(Cameron, Angus C.. Handbook of Pediatric Dentistry, 2nd Edition. C.V. Mosby, 2003.)
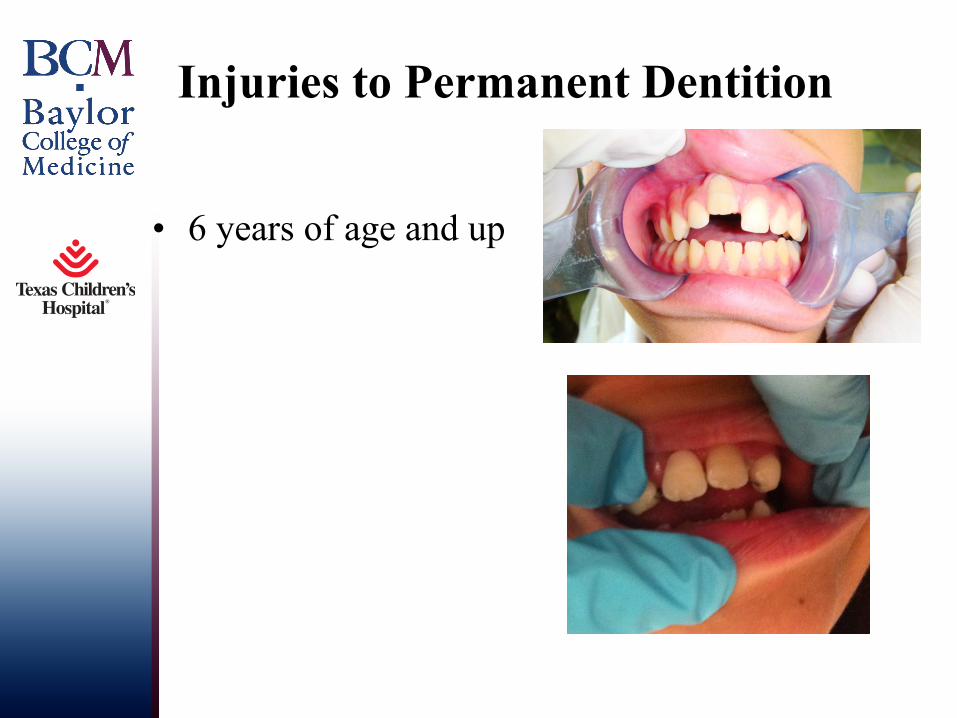
Injuries to Permanent Dentition
• 6 years of age and up
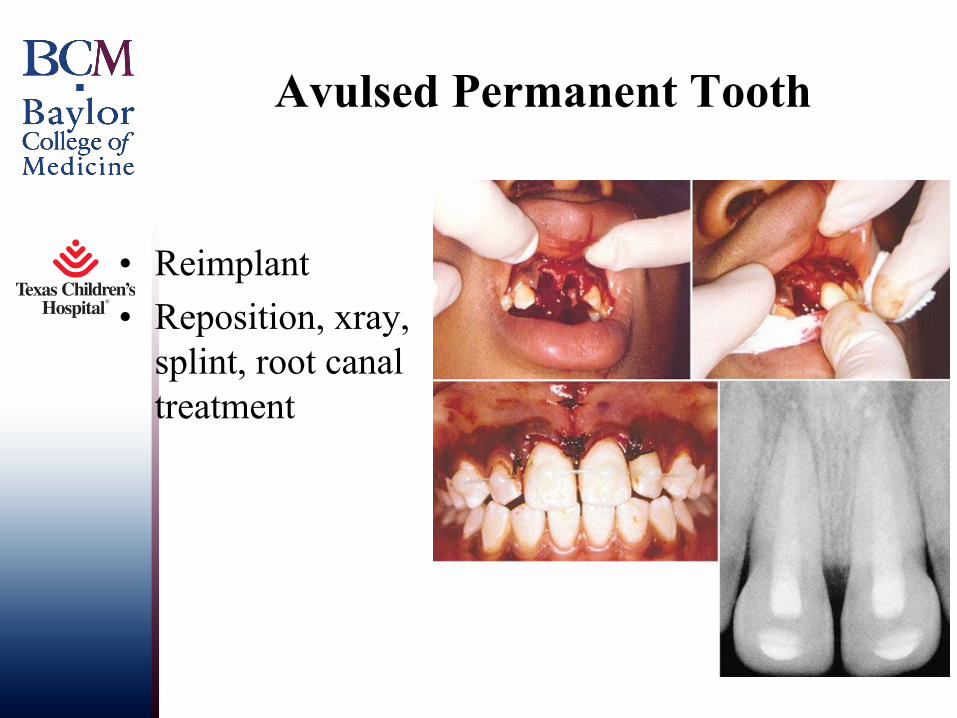
Avulsed Permanent Tooth
• Reimplant• Reposition, xray,
splint, root canal treatment
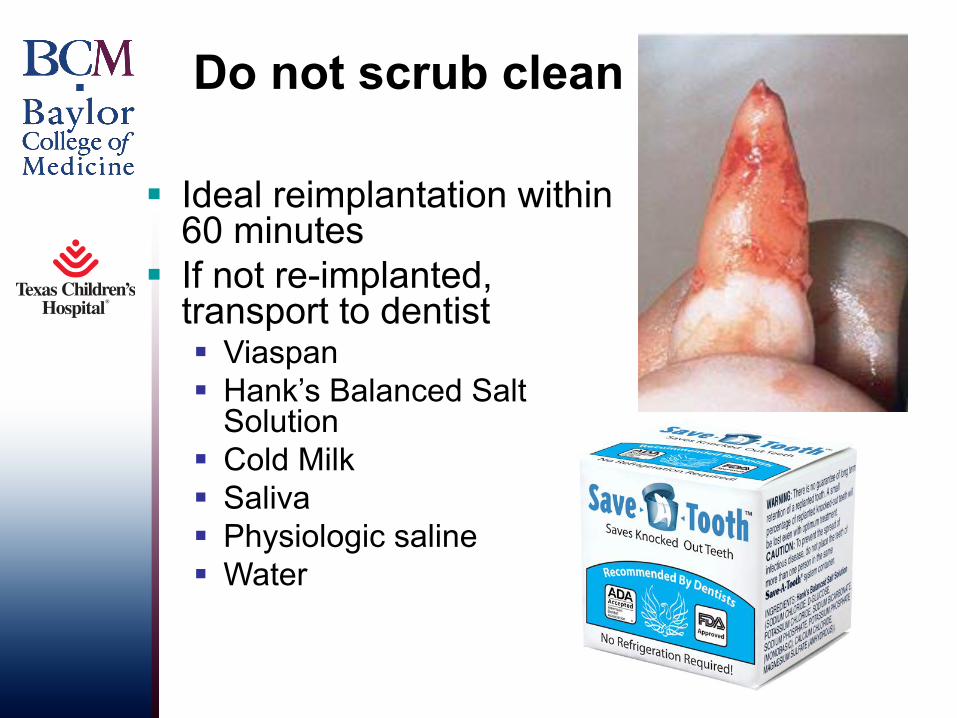
Do not scrub clean
§ Ideal reimplantation within 60 minutes
§ If not re-implanted, transport to dentist § Viaspan§ Hank’s Balanced Salt
Solution§ Cold Milk§ Saliva § Physiologic saline§ Water
Bloody Tooth
Wet Tooth
Steps for you to take initially
• Transport medium• Antibiotics• Chlorhexidine rinse• Tetanus Vaccination
Follow-Up Care
Regular private pediatric dentistGreater Houston Dental Society: after hours
directory281-540-9393Operator sorts dentist by zip code
TCH Affiliated Dentistshttp://www.texaschildrens.org/Locate/Find-a-Doctor/ Under Dental Specialty Tab~30 private pediatric dentist
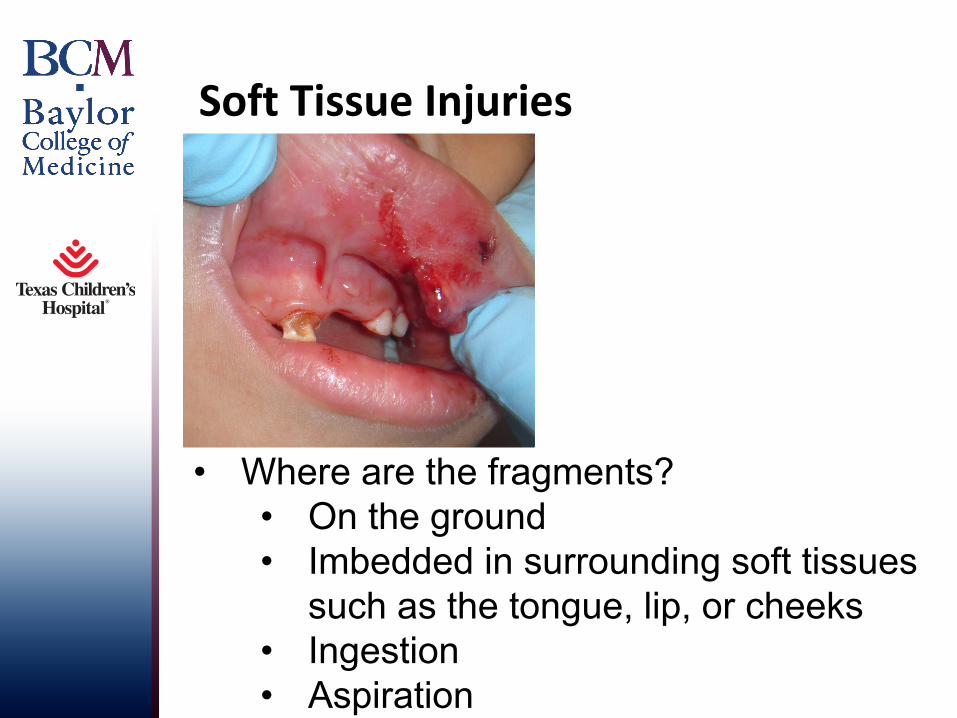
Soft Tissue Injuries
• Where are the fragments?• On the ground• Imbedded in surrounding soft tissues
such as the tongue, lip, or cheeks• Ingestion• Aspiration
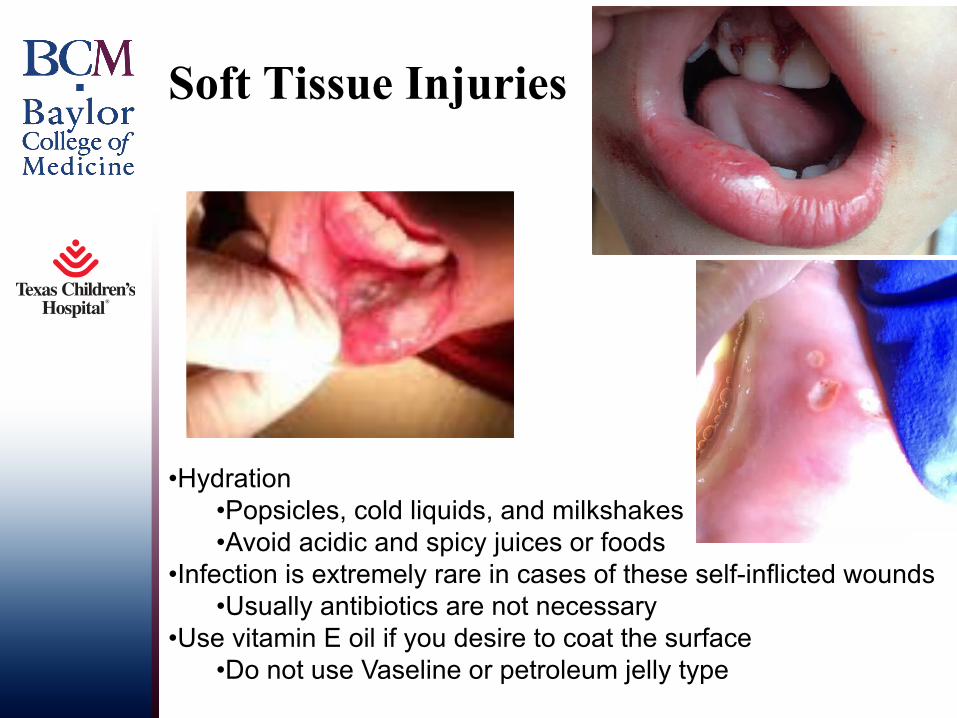
Soft Tissue Injuries
.
•Hydration•Popsicles, cold liquids, and milkshakes•Avoid acidic and spicy juices or foods
•Infection is extremely rare in cases of these self-inflicted wounds •Usually antibiotics are not necessary
•Use vitamin E oil if you desire to coat the surface •Do not use Vaseline or petroleum jelly type
NewDevelopments
• SilverDiamineFluoride– Kills pathogenic organisms– Hardens softened dentin making it more acid
and abrasion resistant– Does not stain sound dentin or enamel– Stabilize caries on uncooperative child
April 9, 2018 Baylor College of Medicine 56
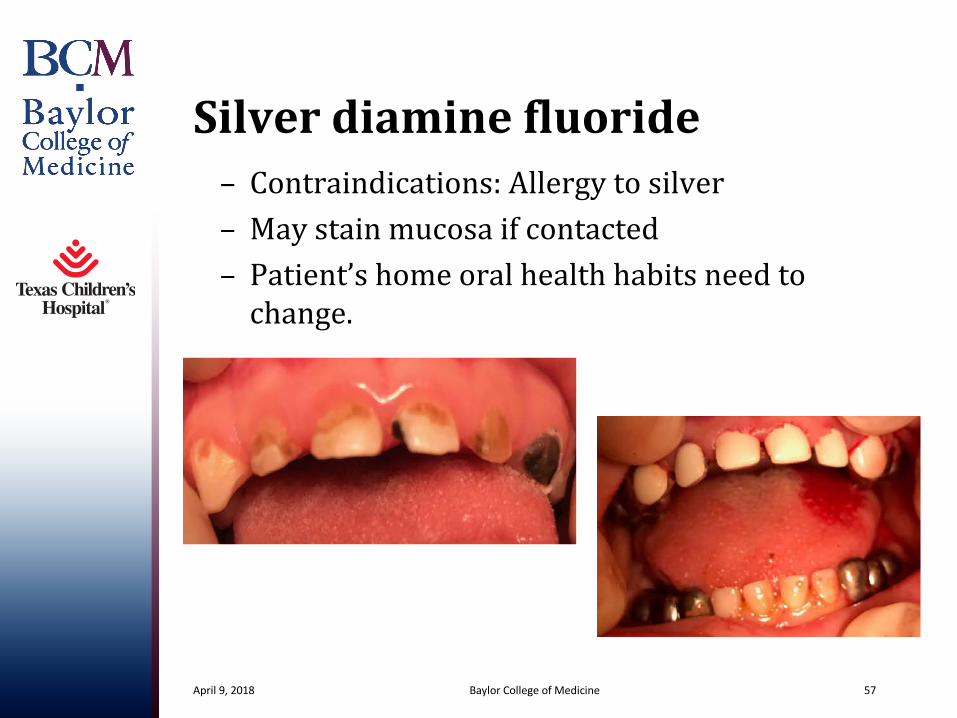
Silverdiaminefluoride– Contraindications:Allergytosilver– Maystainmucosaifcontacted– Patient’shomeoralhealthhabitsneedtochange.
April 9, 2018 Baylor College of Medicine 57
TCH Dental Clinic• Medical Compromised
– Patients needing dental treatment prior to:• Transplants• Cardiac surgery• Chemotherapy• Radiation treatment
• Special Needs Clinic– Autistic– Down’s – Cerebral Palsy – Cleft Lip and Palate
HelpfulWebsites
PreventionofInfectiveEndocarditisbyAHAhttps://www.heart.org/idc/groups/heart-public/@wcm/@hcm/documents/downloadable/ucm_307684.pdf
American Academy of Pediatric Dentistryhttp://www.aapd.org/policies/
Thankyouforyourtimeandattention
April 9, 2018 Baylor College of Medicine 59
• Questions?
April 9, 2018 Baylor College of Medicine 60