-
7/31/2019 Estetica en Ortodoncia
1/14
O r i g i n a l a r t i c l e
Dental Press J. Orthod.118 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
Aesthetics in Orthodontics: Six horizontalsmile linesCarlos
Alexandre Cmara*
Introduction: Smile analysis is an important stage or the
diagnosis, planning, treatment andprognosis o any dental treatment
involving aesthetic objectives. The evaluation o the in-trinsic
characteristics o the smile is a necessary procedure to achieve
consistent orm inorthodontic treatments, which in turn makes it
necessary to recognize the components and
actors that a ect these characteristics.Objective: The objective
o this work is to present six horizontal smile lines and their
importance in obtaining the desired results in
orthodontictreatments.Conclusion: The analysis o the six horizontal
smile lines acilitates the under-standing o the intrinsic
characteristics that inter ere in the aesthetics o the mouth.
Moreover,a harmonization o these lines gives each pro essional a
higher possibility o success in theirtreatments that include
aesthetic objectives.
Abstract
Keywords: Orthodontics. Aesthetics in Orthodontics. Dental
aesthetics. Mouth aesthetics. Smile.
* Specialist in Orthodontics (FO-UERJ). Certifed member o the
Brazilian Board o Orthodontics and Facial Orthopedics (BBO).
INTRODUCTIONObtaining a beauti ul smile is always the
main objective o any aesthetic dental treatment.A ter all, it is
the beauty o the smile that willmake the di erence between an
acceptable orpleasing aesthetic result or any given
treatment.Nevertheless, in spite o its importance, the in-trinsic
characteristics o the smile are little dis-cussed. Much is said o
the clinical consequenceso dental procedures on the smile, but its
in-
trinsic characteristics are not widely evaluated.These
characteristics can sometimes be alteredand sometimes not, as they
are integral parts o the individual. As such, the eld o dentistry
has
no reach over these characteristics, and can onlymake
evaluations o them.
Evaluating beauty is always subjective. How-ever, we need
adequate tools to overcome thechallenge o this subjectivity. In
orthodontics, it is not enough only to recognize what is inter
er-ing with the smileit requires a diagnosis o what is not normal,
in order to establish a treatment plan. Just as in unctional
problems, in which we
ollow conducts that lead us to a diagnosis o the
anomalies, aesthetic problems also require param-eters so we can
nd the de ects. When searchingor the visualization o problems,
several rules and
assumptions are created, leading sometimes to an
-
7/31/2019 Estetica en Ortodoncia
2/14
Cmara CA
Dental Press J. Orthod.119 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
underestimation o de ects or an overvaluing o rules, creating
paradigms that are not supportedby proven scienti c data. The very
essence o aes-thetic dentistry, which involves artistic
criteria,contributes to this act. The use o simple and re-liable
mechanisms can improve the possibilities o success, i not eliminate
per ormance errors.
There are some tools that can be used or that purpose. The
Diagram o Facial Aesthetic Re er-ences (DFAR) is an auxiliary
diagnostic tool that is well suited to that purpose. The diagram
con-sists o six rames that surround the maxillary in-cisors and
canines; their limits are speci c to each
aesthetic re erence. The unction o the DFAR isto give an exact
idea o the positioning and ratiosbetween teeth, as well as their
relationship withthe gum and lips.5 Originally conceived to aidin
the visualization o maxillary anterior teeth,DFAR, when aided by
additional data, makes it possible to objectively evaluate the
smile, acili-tating the aesthetic diagnosis and prognosis. Thus,the
objective o this work will be to present thenew characteristics o
DFAR and its role in thesix horizontal smile lines, which in turn
assist
the diagnosis, treatment and prognosis o mouthaesthetics.
DIAGRAM OF FACIAL AESTHETICREFERENCES - DFAR (new
characteristics)
The Diagram o Facial Aesthetic Re erences(DFAR) was created to
acilitate the visualiza-
tion o maxillary anterior teeth, by suggestingwhat needs to be
created or achieved with thoseteeth, aiming or the best possible
dental aesthet-ics. The objective o the diagram is to give anexact
idea o the positioning and ratios betweenteeth, as well as their
relationship with the gumand lips in rontal view. As previously
mentioned,the diagram consists o six rames that surroundthe
maxillary incisors and canines; their limits arespeci c to each
dental re erence. Each rame sur-rounds its respective tooth,
observing its limits(Fig 1). Although these rames can serve as re
er-ences in the di erent observation planes, DFAR is
evaluated at a 90
view rom the rontal planeinother words, perpendicular to it. Its
use acilitatesthe planning and visualization o the best aesthet-ic
positioning o anterior teeth, and its objective isto provide data
that can assist the reorganizationand restructuring o those teeth,
whenever theyneed to be repositioned and/or restored.
However,although the original conception o DFAR is use-
ul to assist in the evaluation o mouth aesthet-ics, a ew re
erences o dental, gingival and labialstructures can be added to its
ormat, improving
and acilitating the visualization o the smile.In its original
ormat, DFAR makes re erence
to the gingival apexes, which are most apical land-marks o the
gingival contour. The present reeval-uation will add the locations
o the extremities o gingival papillae (papillary tips) and
emphasizethe contact points (Fig 2).
FIGURE 1 - Diagram o Facial Aesthetic Re erences (DFAR). FIGURE
2 - DFAR with new re erence points: contact points and
gingivalpapillary tips.
-
7/31/2019 Estetica en Ortodoncia
3/14
Aesthetics in Orthodontics: Six horizontal smile lines
Dental Press J. Orthod.120 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
The union o these points will orm lines that give evaluative re
erences in the analysis o thesmile. As such, DFAR will
intrinsically have ourlines, ormed by the ollowing structures (Fig
3):
Cervical linegingival apexes. Papillary linepapillary tips.
Contact points linecontact points. Incisal lineincisal edges
(incisal line).The relationship o the papillary line with
the contact points line will create a band namedconnector band,
in a re erence to the concept o dental connectors.19 This band,
ormed by thetwo lines (papillary and contact points), added
to the cervical and incisal lines, will provide thehorizontal
dental re erences o the smile in arontal view.
The other two lines that make up the groupo horizontal smile
lines are the upper lip lineand lower lip line. These lines, along
with thedental and gingival lines, compose the group o six
horizontal smile lines (Fig 4).
CERVICAL LINEThe cervical or gingival line is ormed rom
the union o the apexes o the canines, maxil-lary lateral and
central incisors. As the most api-cal point o the gingival contour,
the apex in
maxillary teeth is usually located distal to thelong axis o the
tooth. However, this rule doesnot always apply to the maxillary
lateral inci-sors. On those teeth, the gingival limit may
becentered on the long axis. Because the apexeso the maxillary
canines are most o ten higherthan the lateral incisors and about
the same levelas the central incisors, the cervical line attains
aconvex aspect in relation to the occlusal plane.That would be the
ideal orm o the cervical line. When the lateral incisors are
positioned moreapical, at the same height as the canines andcentral
incisors, the line becomes plain. When
the gingival contour o the canines is below thelateral incisors,
the line ormed will be concave(Figs 5 to 7). The concave cervical
line is the least pleasing among the three possibilities.
There will be situations in which the heightso the anterior
teeth will be asymmetrical, lead-ing to the ormation o an
asymmetrical cervicalline (Fig 8). It should be clear that the
positiono the gingival apexes can vary widely betweenteeth and each
individual will have a uniquelyshaped cervical line, making it
practically impos-
sible to characterize all the possibilities. The no-menclature
used or the cervical line (plain, con-cave, and convex) serves only
as an evaluation
FIGURE 3 - Aesthetic re erence lines: Cervical Line (A);
Papillary Line(B); Contact Points Line (C); Incisal Line (d ).
A
B
C
D
FIGURE 4 - The six horizontal smile lines. Cervical Line (A);
Papillary Line(B); Contact Points Line (C); Incisal Line (d );
Upper Lip Line (e ); LowerLip Line (F).
-
7/31/2019 Estetica en Ortodoncia
4/14
Cmara CA
Dental Press J. Orthod.121 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
re erence. The variation in the cervical height o teeth will
depend on the periodontal conditionso each tooth, as well as on
tooth size, tipping,eruption pattern, and occlusal plane
tipping.
INCISAL LINEThe incisal line ollows the edges o anterior
maxillary teeth. The ideal is that in young pa-tients the
incisal edges o the central incisors bebelow the edges o the
lateral incisors and ca-nines in a rontal view. In that con
guration, the
orm o the incisal line resembles the outlineo a deep plate (Fig
9). A change in the posi-
tioning o the incisal edges modi es that gure. When the incisal
edge o the central incisors areno longer below the lateral
incisors, the outlinewill change, becoming known as shallow
plate,or depending on the relation, an inverted plate.
In general, the con guration o the incisal lineis related to the
patients age. Over time, thereis wear o the central incisors,
leading to thesechanges. However, it is not only
wear-relatedchanges that a ect the outline o the incisal line.
FIGURE 6 - Plain orm o the cervical line. FIGURE 7 - Concave orm
o the cervical line.
FIGURE 5 - Convex orm o the cervical line.
FIGURE 8 - Asymmetrical cervical line. FIGURE 9 - Incisal line
in the orm o a deep plate.
-
7/31/2019 Estetica en Ortodoncia
5/14
Aesthetics in Orthodontics: Six horizontal smile lines
Dental Press J. Orthod.122 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
As with the cervical line, tooth size, tipping,eruption
patterns, and occlusal plane tipping canalso alter the outline. The
most utilized termwhen the incisal line orms an inverted plateis
inverted smile. The line becomes concave inrelation to the rontal
occlusal plane, giving anaged and anti-aesthetic appearance. The
classi -cation o the incisal line may also use the nomen-clature
concave (inverted plate), plain (shal-low plate) and convex (deep
plate). Other
requently used terms to describe the incisal lineare the smile
arch,25 incisal curvature6 andseagull wing.16
CONTACT POINTS LINEThe contact between anterior maxillary
teeth
is done in a descending ashion, starting rom thecanine. The
contact between the canine and lat-eral incisor is positioned
higher than the contact between the lateral and central incisors;
the con-tact between the central incisors is even lower.The contact
points should be narrow, unlessthere is a discrepancy in the
mesio-distal diam-eter o the crown.2 The position o the contact
between teeth is related to tooth position andorm.16 As such,
the line that unites these points
will be parallel to the incisal line, whenever thereis no
discrepancy between the sizes, shapes andangles o anterior teeth.
Although there is a con-tact point whenever a tooth touches
another, theideal is when that contact happens in an areabroader
than a single point, orming a connect-ing space. Connecting spaces
are areas in whichteeth appear to touch. As will be seen urtheron,
this act has a positive infuence on dentalaesthetics. For practical
purposes, whenever thedental contact takes place over an area
instead o in a single point, we consider the most apical siteas the
re erence or the contact point (Fig 10).
PAPILLARY LINEThe papillary line is ormed by the tips o the
gingival papillae located between the canines and
lateral incisors, and between the maxillary lateral
incisors and central incisors. There are no studiesthat have
evaluated the standard height or thisrelationship. In other words,
there is no de nitiono an ideal model or the relationship
betweenthe heights o the papillae. Nevertheless, based onworks that
evaluated the ideal height o the cen-tral incisors and the
relationship between the pap-illary tips and the position and size
o teeth,13,27 it can be presumed that an ideal line would
beparallel to the line ormed by the contact points.According to the
work o Kurt and Kokich,13 thepapilla in the central incisors lls
hal the size o those teeth, under normal conditions. As such, it
would be expected that the same pattern wouldbe repeated or the
lateral incisors and canines.Given that the lateral incisors are
smaller than thecentral incisors and the papilla should ll hal
theheight o their crowns, the position o the papillabetween the
central and lateral incisor should bein an apical aspect in
relation to that o the centralincisors, as well as to the papilla o
the lateral inci-sor and canine (Fig 11).
Connector bandThe location where anterior teeth appear to
touch is named a connecting space. As previouslymentioned, there
is a di erence between a con-necting space and a contact point.
Contact pointsare small areas in which teeth touch. Connect-ing
spaces are larger, broader, and can be de ned
FIGURE 10 - Contact points line. This line should have a certain
parallel-ism with the incisal line.
-
7/31/2019 Estetica en Ortodoncia
6/14
Cmara CA
Dental Press J. Orthod.123 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
as zones in which two adjacent teeth appear totouch. The best
aesthetic relationship o anteriorteeth is one that ollows the
50-40-30 rule orthe connecting space.19 This rule establishes that
the connecting space between the central inci-sors should be 50% o
the size o those teeth. Theideal connecting space between the
central andlateral incisor is 40% o the length o the
centralincisors, and the connecting space between thelateral
incisor and the canine is 30% o the samere erence. Although the re
erence points to de-termine the connecting space were not de nedby
Morley and Eubank,19 these re erences can becreated rom the contact
points and the gingivalpapilla. There ore, whenever there are no
dark spaces or diastemas between two teeth, with thespace lled by
the gingival papilla, the area o theconnecting spaces will be
delimited by the papil-lary tips and the contact points. As such,
usingthe papillary line and the contact points line as
re erence, we will have a band named connec-tor band. The gure o
this band resembles theshape o a hang glider (Fig 12). Small
changesin this band can make a di erence in dental aes-thetics.
Dental remodeling can increase or de-crease the connecting space,
resulting in an im-proved con guration o the area (Fig 13).
Clinical ApplicationThe clinical evaluation o DFAR with the
our lines and connector band will permit the useo a checklist
that will be able to detect errors intooth positions and their
relationship to the gin-giva. By observing the orm o each line, a
plancan be drawn ocusing on correcting the de ects,harmonizing the
lines, and later evaluating theachieved results. This evaluation
acilitates thediagnosis and makes it easier and more practical
or all pro essionals who treat aesthetic problemsto detect
problems (Fig 14).
FIGURE 11 - Papillary line. It consists o the tips o gingival
papillae. FIGURE 12 - Connector band. This band is delimited by the
contact pointsline and papillary line. The fgure o the band
resembles the shape o ahang glider.
FIGURE 13 - Un avorable ratio o the connector band
30-40-30-40-30 (A). A simple re-contour with the addition o
composite resin between the centralincisors led to the ormation o a
avorable connector band: 30-40-50-40-30 ( B).
A B
-
7/31/2019 Estetica en Ortodoncia
7/14
Aesthetics in Orthodontics: Six horizontal smile lines
Dental Press J. Orthod.124 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
Lip analysisIn addition to teeth, DFAR also involves the
lips. A ter the labial evaluation, the six horizon-tal smile
lines are ound in addition to the ourdento-gingival lines, there
are the upper and low-er lip lines. Both the upper and lower lips
havea marked e ect on the beauty o the smile. In-dividually, each
lip will infuence the dentolabialensemble, and together they will
create guresthat will determine the visible tooth exposure.The lip
separation that occurs during smiling willpermit the exposure o
dental and gingival struc-tures. This separation can be called
labial unveil-ing, as it will be this unveiling that will give
thedental work a chance to be shown (Fig 15). Labialunveiling is
what makes possible the evaluationo the relationship between the
white (teeth) andpink (gums) aesthetics, and their relationship
withthe lips. The three-dimensional relationship thesestructures
have with one another is what willcause the e ect o beauty or
not.
This concept is essential, as it leads to the needto know a
series o actors that infuence that un-veiling. The greater or
lesser tooth exposure willbe infuenced by labial unveiling and all
intrinsic
actors to it, such as its ormation, stages, phasesand lip
involvement. As such, be ore we beginevaluating the upper and lower
lip lines, we willpresent the actors that a ect the smile.
Smile formationThe smile can be de ned as a change in acial
expression that involves a sparkle in the eyes, anupper
curvature in the corners o the lips, no soundemission, and less
distortion o muscle orms thanwith a laugh.12 It begins at the
commissure andextends laterally; the lips may initially remain
incontact, except in people who do not eature pas-sive lip seal or
have a short upper lip. As the smileexpands, the lips separate, the
commissures curveupwards, and the teeth are exposed. The
maxil-laries are separated, and a dark space develops be-tween
upper and lower teeth, known as negativespace.18 During smiling,
upper lip height is dimin-ished, and the width o the mouth is
increased by23% to 28% compared to the lip at rest.26
FIGURE 14 - CHECKLIST Cervical line: concave (accentuated) and
asymmetrical. Incisal line: inverted deep plate orm (concave) and
asymmetrical.Connector band: 30% (13/12) 20% (12/11) 40% (11/21)
20% (21-22) 20% (22/23) (A). CHECKLIST Cervical line: concave
(slight) and symmetrical.Incisal line: deep plate orm (convex) and
symmetrical. Connector band: 30% (13/12) 35% (12/11) 40% (11/21)
35% (21/22) 30% (22/23) (B).
FIGURE 15 - Labial unveiling.
dentAl exposition AreA
A B
-
7/31/2019 Estetica en Ortodoncia
8/14
Cmara CA
Dental Press J. Orthod.125 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
The symmetry o muscle activity should not be overestimated. In
normal people, individualvariability o motor unction is observed
be-tween di erent sides o the same individual.Combined
measurements, both o skin mobilityand muscle activity, indicate
that there is an av-erage asymmetry o 64% between the sides o the
human ace.4
Stages of the smileIn smile analysis, its stages should be
observed.
There are two stages in smile ormation: the rst (voluntary
smile) elevates the upper lip towards
the nasolabial groove through the contraction o the elevator
muscles that originate in this grooveand are inserted in the lip.
The medial bundles el-evate the lip in the area o the anterior
teeth, andthe lateral bundles act on the area o the poste-rior
teeth. The lip then nd meets resistance dueto the adipose tissue in
the cheeks. The secondstage (spontaneous smile) begins with
higherelevation, both in the lip and in the nasolabialgroove, under
the action o three muscle groups:the elevator o the upper lip,
originating in the
in raorbital area; the zygomatic major muscleand the upper bers
o the buccinator muscle.23
The appearance o hal -shut eyes should accom-pany the nal stage
and represents the contrac-tion o the periocular musculature
(orbicularmuscles o the eyes), in order to support themaximum
elevation o the upper lip through thenasolabial old. The hal -shut
look that accompa-nies the smile is a muscular trigger o the
acethat activates the centers in the temporal anteriorarea o the
brain, which regulates the productiono pleasant emotions. There
ore, without this nalaction o semi-closure o the eyes, the
noticeablehappy smile is probably a alse smile, without joy
rom the person who gives it 9 (Fig 16).
Phases of the smileIn addition to the stages, the smile also
ol-
lows phases. These phases are three old: the rst is named the
initial peak phase, which corre-sponds to the period in which the
lips depart
rom a neutral position until the position o maximum lip
contraction during the spontane-ous smile. During this phase, mouth
width isincreased and lip height is reduced, the commis-sures move
upwards and sideways in the same
ratio, with great individual variability in the di-rection o the
movement o these points. It is
FIGURE 16 - Resting position (A). First stage o the smile Social
smile ( B). Second stage o the smile Spontaneous smile. Notice that
in this stage thepatients eyes are hal -shut. ( C).
A B C
-
7/31/2019 Estetica en Ortodoncia
9/14
Aesthetics in Orthodontics: Six horizontal smile lines
Dental Press J. Orthod.126 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
the shortest phase o the cycle, lasting on aver-age less than
0.5 second. The second phase is lipsupport. It is during this phase
that the smileis dependent on stimulus. The duration o thisphase is
quite variable and depends on individualvolition. The last phase is
the decline, in whichthe lips close again. The duration o this
phaseis usually longer than the initial peak phase, but as with the
support phase, it is not possible tomeasure its duration because it
is subject to astimulus. In evaluating the smile cycle, it canbe
observed that the only reproducible phase isthe initial one. Unlike
the other phases, which
can be infuenced by individual volition, thepeak phase depends
only on the initial stimu-lus that causes the smile, although its
duration isextremely brie .26 This hinders the collection o static
images, such as photographs, as it is practi-cally impossible to
record the maximum smileobtained during the rst phase. That is why
sev-eral authors advise against evaluating the smileusing
photographic images, recommending in-stead that video images be
taken.1,24
Stimulating and recording the smileAlthough 18 types o smiles
have been re-
corded,9 the smile that directly interests the eldo dentistry is
the one that expresses joy. Thisis the smile type known as
Duchenne, in whichthere is a contraction o the orbicular
muscula-ture o the eyes combined with traction o thecorner o the
lip by the zygomatic major muscle;among the di erent types o
smiles, it is the onethat best demonstrates satis action or
happiness.It is the spontaneous smile.9 As such, the smilethat
expresses pleasure is the type that pro es-sionals seek to record.
For that type o record,a stimulus is necessary. In this case, the
stimu-lus becomes a problem, as what is unny to oneperson is not so
to another. The di culty in ob-taining photographs that represent
the patientsnatural smile in clinical practice was observed
byRigsbee et al,22 who reported that the interac-
tion o the photographing pro essional and thepatient should not
be underestimated, and sug-gested the use o phrases to obtain the
picture. This method is also recommended by Zachris-son30, who
suggests the use o the word cheeseto stimulate the exposure o the
incisors dur-ing smiling. For records o the resting position,the
author recommended that teeth be slightlyapart, and that perioral
so t tissues and the man-dibular position be relaxed.30 Although
the useo phrases can be use ul, the best way to obtaina smile is
through comic stimulus. The use o videos, photographs, or even the
pro essionals
comic ability can be used to provoke the stimu-lus. What is
important is that the stimulus causesa smile that expresses
pleasure. For evaluationsthat involve the relationship between the
teethand upper lip, it is recommended, in spite o possible
questioning, that the patient pronouncethe sound o the letter e in
an uninhibited andexaggerated manner. This causes the
maximumelevation o the upper lip.21
Recording the smile is another problem. Theideal is that static
(photographs) and moving
(video) records be made. In the static records,image gathering
should include close-up shotsin rontal, sagittal, and oblique
planes. For themoving records, video should be recorded anduploaded
to a computer, and the best image se-lected.24,25 During the
evaluation, pre erence canbe given to the social or spontaneous
smile withmaximum elevation o the upper lip. What isimportant is
that the initial record be the sameas the nal record, so that di
erences can beevaluated without inter erence rom the di er-ent
stages. In other words, i the rst record wasmade in stage 1, so
should the nal record.
UPPER LIP LINEThe upper lip line represents the lower edge
o the lip, and dictates the exposure o upperteeth. Not only
anterior teeth have their expo-sure limited by this line, but
posterior teeth as
-
7/31/2019 Estetica en Ortodoncia
10/14
Cmara CA
Dental Press J. Orthod.127 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
well. Several authors recommend that duringsmiling, the position
o the lower edge o the up-per lip should coincide with the gingival
edge o the maxillary central incisor.14,15,17 However, oth-er
authors consider that a smile could be aesthet-ically acceptable
with exposure o up to 2 mmo gingival tissue.3,10,30This di erence
in opinionsleads to inadequate and con using concepts that do not
help the standardization o smile classi -cations. Although the
simplest way to classi y thesmile lineusing the relationship
between themaxillary incisors and the upper lipis throughheight
(low, medium, and high), the description
o the parameters is still inadequate. For example,the classi
cation o smile heights as described byTjan et al29 used by Dong et
al,8 regards as highany smile in which the crown o the
maxillarycentral incisor is totally exposed. There ore, asmile with
a band o gingival tissue only 1 mmthick would receive the same
classi cation as asmile with, or instance, 5 mm o gingival
tissueexposure. The same can be said o the classi ca-tion described
by Teo,28 which classi es as Class Iall smiles in which the buccal
sur ace o the inci-
sor is totally exposed, regardless o the amount o visible
gingival tissue. Likewise, the classi cationo a smile when the
upper lip does not exposethe maxillary incisors is also con using
in the de-scriptions by some authors.3,11 In the Goldstein11 classi
cation,a smile eaturing the upper lip cov-ering only 1 mm o the
crown o the maxillarycentral incisor will receive the same classi
ca-tion as another smile with the upper lip coveringmore than hal
or even the entire crown o themaxillary central incisor.
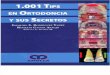
As previously mentioned, the ideal is or theheight o the smile
line to be classi ed using asre erence the relationship between the
loweredge o the upper lip and the gingival edge o the maxillary
central incisor. However, a 2 mmlimit should be established above
and below thegingival edge, thus instituting the three classeso
smile height: high, medium, and low (Fig 17).
As such, a positive aspect is that, with a 4 mmdi erence, the di
erentiation o high and lowsmilesthe smile types that lead patients
to seek treatmentis clinically acilitated.21 Moreover,a numeric di
erentiation is created among theheights, making it easier to
measure their clas-si cation.
Smile height is infuenced by age and gender.The older the
individual, the greater is the ten-dency or a low-type smile.7 This
piece o in or-mation is clinically relevant, as high smiles tendto
become medium smiles with age, and lowsmiles become even lower over
time. In other
words, there is a possibility o sel -correction orgingival
smiles over time, which is not true orlow smiles.
Gender also seems to infuence smile height.Although not many
studies exist on the subject,the work o Puppin21 shows that there
is a greatertendency or women to show medium (55.9%)and high
(37.7%) smile lines, while men eaturemedium (54%) and low (23.8%)
smile lines.These ndings are similar to the values ound inthe work
o Peck, Peck and Kataja,20 who also ob-
served that medium (52.2%) and high (32.5%)smiles are more
common in women and that me-dium (48%) and low (33%) smiles prevail
in men.
The smile line can be regarded as a determin-ing actor in the
evaluation o mouth aesthetics.
FIGURE 17 - High smile (A); medium smile (B); low smile (C).
Ahigh smile
Bmedium smile
Clow smile
-
7/31/2019 Estetica en Ortodoncia
11/14
Aesthetics in Orthodontics: Six horizontal smile lines
Dental Press J. Orthod.128 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
The aesthetic results o orthodontic treatmentsalways maintain a
strong relationship to this line.It is not uncommon or the
conclusion o orth-odontic treatments to be compromised by thesmile
line. Either high or low smiles can com-promise the results. This
is perhaps the great challenge o contemporary orthodontics in
itssearch or excellence. The integration betweenthe di erent
dentistry specialties will need to beexpanded also to the medical
elds that can posi-tively inter ere in the solution o mouth
aesthet-ic problems that are compromised by the nega-tive infuence
o the smile line, in particular the
upper lip line. Medical and dental interventionsthat are able to
correct a negative labial infuenceare always welcome. This
integrated approach bypro essional teams will bring new
possibilities o better results, expanding treatment options,
andperhaps creating a higher demand or the solu-tion o problems
involving mouth, acial anddental aesthetics.
LOWER LIP LINEAlthough the lower lip line is less studied
than the upper lip line, it is no less important. It consists o
the group ormed by the upper andlower lips that will produce labial
unveiling.
In general, it is the shape o the lower lip andthe incisal edges
o maxillary and mandibulartips that create a pleasing or unpleasing
smile en-semble.25 What is important is that the maxillaryincisal
plane and the shape o the lower lip retaina harmonious
relationship.30 That harmony isrepresented in the parallelism o the
arch ormedthe incisal edges o maxillary teeth with the up-per edge
o the lower lip.
There should be harmony between the cur-vature o the incisal
edge o anterior maxillaryteeth with the curvature o the upper edge
o the lower lip during voluntary smiling.11 This re-lationship
between the incisal edges o caninesand maxillary incisors with the
lower lip is calledthe smile arch.10,24 The ideal is or the
curvature
o incisal edges to be parallel to the lower lip andthe incisal
edges slightly apart or so tly touch-ing the lip. However, this is
only possible whenthe lower lip creates a natural curvature, with
thecorners o the mouth turned upwards, and incisaledges ollow that
curvature. In other words, inorder to achieve a pleasing e ect, it
is necessarythat dental and labial structures be symmetrical.In
case the lips or teeth limit the parallelism be-tween them, the
smile arch will not be possible.Labial asymmetry is also a limiting
actor or thisharmony between teeth and lip.
As previously mentioned, the ideal is that the
line ormed by the incisal edges o anterior teethcreates the orm
o a deep plate, in which thecentral incisors are positioned more in
erior tothe lateral incisors and canines, and are in har-mony with
the other smile lines5 (Fig 18).
This con guration varies with age. As age ad-vances, the deep
plate orm is altered, givingway to a new shallow plate or inverted
plate
orm. That is, the line that contours the incisaledge becomes
plainer or more concave. The wearin the incisal edges creates these
new orms over
time. Knowledge o these characteristics createsthe possibility o
rejuvenating or aging a smile. Achange in the plate orms can make
this e ect possible5 (Fig 19).
FIGURE 18 - The vertical positioning o the maxillary incisors
and caninesorms a curvature; the line that contours this
relationship resembles the
fgure o a deep plate.
m a ch
-
7/31/2019 Estetica en Ortodoncia
12/14
Cmara CA
Dental Press J. Orthod.129 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
It should be clear that the ideal relationshipo parallelism
between maxillary teeth and low-er lip is dictated by the lip. The
contraction pat-tern o the lower lips and their relationship
withteeth are much less uni orm than those o theupper lips. Whereas
in the relationship betweenthe upper lip and maxillary teeth it is
possibleto establish three de ned positions with regardto the smile
line (high, medium, and low), thesame is not possible with the
lower lip. Thesmiles own dynamics complicate this evalua-tion. The
possibility o an individual opening hismouth wider or not makes a
standardized evalu-
ation more di cult. Maxillary teeth may occa-sionally touch the
lower lip (contact position),remain apart (non-contact position),
or else becovered by the lip (covered position).10 Thissituation
can vary among individuals or even inthe same person depending on
mouth opening.The muscle contractions o the lower lip alsoalter
this relationship. Muscles such as the riso-rius, mentalis,
triangularis and quadratus o thelower lip are responsible or the
contraction o the lower lip and its greater or lesser
participa-
tion during smiling inter eres in labial contrac-tion and
symmetry.23 Variations in the contrac-tion and intensity o muscle
groups play an im-portant role in the creation o di erent
smiles.
Vigorous contractions pull down the lower lip,increasing tooth
exposure. Individuals with in-tense contractions o the lower lip
tend to alsoexpose their lower teeth (Fig 20).
This situation requires attention, as the needsand possibilities
o the aesthetic treatment change perspective, because the
evaluation isusually made o the relationship between thelips and
maxillary teeth, and not the ull arch.Seeking parallelism between
the incisal line andthe lower lip (smile arch) is totally un
easible,showing us that establishing aesthetic rules andobjectives
by taking the lower lip in consider-
ation does not allow standardizations. Anothersituation that
also creates di culties in obtain-ing the smile arch is when the
lower lip con-tracts in an inverted ashion; the contraction o the
lower lip is greater in the area o the caninesthan in the area o
the incisors, possibly due togreater action by the risorius muscle.
When theupper lip also contracts in the same manner, theappearance
o mirroring is created betweenthe lips. This lower lip contour is
usually ac-companied by a low smile line and the gure
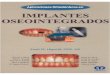
ormed by the lips resembles the in nity symbol( ). (Fig 21).
This in nity-type smile gure in-dicates an un avorable prognosis or
mouth aes-thetic treatments.
FIGURE 19 - The vertical repositioning o the maxillary incisors
and canines, a ter an ortho-surgical treatment eaturing maxillary
impaction and rotation,resulted in an improved relationship between
the incisal edges o the maxillary anterior teeth and the lower lip,
creating the deep plate fgure. Thisconvex line gives a more
pleasing and jovial aesthetic aspect ( A, B).
A B
-
7/31/2019 Estetica en Ortodoncia
13/14
Aesthetics in Orthodontics: Six horizontal smile lines
Dental Press J. Orthod.130 v. 15, no. 1, p. 118-131, Jan./Feb.
2010
CONCLUSIONKnowledge o the intrinsic characteristics o
the smile helps in the aesthetic perception o it.Being able to
evaluate the smile o each patient assures the pro essional o the
possibility o see-ing what needs to be done, what can be done,
andwhat should be accepted. In other words, beingable to interpret
the nuances o a smile gives eachorthodontist the opportunity to act
in a consciousmanner in the mouth aesthetic treatment o
theirpatients, allowing the diagnosis to be integratedwith the
prognosis and giving a realistic outlook o the results than can be
obtained. In that per-spective, the six horizontal smile lines meet
thispurpose, as the analysis o these lines acilitates
theunderstanding o the intrinsic characteristics o thesmile and
gives each pro essional a better look intotheir chances or success.
Nevertheless, we knowthat observing the six lines is not enough to
evalu-ate a smile. Several other actors also need to betaken in
consideration. Buccal corridor, number o exposed teeth during
smiling, rontal, oblique andpro le acial analyses, relationship
between restingand speech positions and the smile are some
actorsthat should also be observed in order to achievea better
diagnosis o mouth aesthetics. Althoughthese components were not
examined in this work,
they should not be ignored, as, along with the sixlines, they
can allow a complete observation o thesmile, acilitating its
understanding and treatment possibilities.
ACKNOWLEDGEMENTSAdilson Torreo, Adilson Torreo Filho, Aldino
Puppin, Isana lvares, Jonas Capelli Jr., MarcoAntnio Almeida,
Vera Cosendey.
FIGURE 21 - Mirroring o lower lip and upper lip orms. Notice
that thearea o the lower lip (yellow arrow) is closer to the upper
lip than thelateral areas (white arrows). The fgure ormed by the
lips resembles theinfnity symbol ( ).
FIGURE 20 - Excessive contraction o the lower lip, completely
exposing the mandibular incisors.
Submitted: March 2009Revised and accepted: December 2009
-
7/31/2019 Estetica en Ortodoncia
14/14
Cmara CA
131 v 15 no 1 p 118 131 Jan /Feb 2010
1. Ackerman MB, Ackerman JL. Smile analysis and design in
the
digital era. J Clin Orthod. 2002 Apr;36(4):221-36.2. Andrews LF.
Straight-Wire: the concept and appliance. SanDiego: Wells;
1989.
3. Arnet GW, Bergman RT. Facial keys to orthodontic diagno-sis
and treatment planning. Part I. Am J Orthod Dento acialOrthop. 1993
Apr;103(4):299-312.
4. Burres SA. Facial biomechanics: the standards o normal.
Laryn-goscope. 1985 Jun;95(6):708-14.
5. Cmara CALP. Esttica em Ortodontia: diagramas de re eren-cias
estticas dentrias (DRED) e Faciais (DREF). Rev DentalPress Ortod
Ortop Facial. 2006 nov/dez;11(6):130-56.
6. Chiche G, Pinault A. Artistic and scienti c principles
appliedto esthetic dentistry. In: Chiche G, Pinault. A. Esthetics o
anterior xed prosthodontics. St. Louis: Quintessence; 1994.p.
13-32.
7. Cosendey V L. Avaliao do relacionamento entre o lbiosuperior
e incisivos durante a ala e o sorriso. [dissertao].Rio de Janeiro
(RJ): Universidade do Estado do Rio de Janei-
ro; 2008.8. Dong J, Jin T, Cho H, Oh S. The esthetics o the
smile: a reviewo some recent studies. Int J Prosthod. 1984
Jan;12(1):16-24.
9. Ekman P, Davidson RJ, Friesen WV. The Duchenne smile:
emo-tion expression and brain physiology II. J Pers Soc
Psychol.1990 Feb;58(2):342-53.
10. Fowler P. Orthodontics and orthognatic surgery in the
combi-nated treatment o an excessive gummy smile. New ZealandDent
J. 1999 Jun;95:53-4.
11. Goldstein RE. Esttica em Odontologia. Rio de Janeiro:
Ed.Guanabara Koogan; 1980.
12. Grove PB. Websters third new international dictionary o the
English language. Spring ield: G and C Merriam Com-pany; 1961.
13. Kurth JR, Kokich VG. Open gingival embrasures a ter
orth-odontic treatment in adults: prevalence and etiology. Am
JOrthod Dento acial Orthop. 2001 Aug;120(2):116-23.
14. Legan HL, Burstone CJ. So t tissue cephalometric analysis
ororthognatic surgery. J Oral Surg. 1980 Oct;38(10):744-51.
15. Levine RA, McGuire M. The diagnosis and treatment o the
gummy smile. Compend Contin Educ Dent. 1997Aug;18(8):757-62, 764;
quiz 766.
16. Magne P, Belser U. Restauraes adesivas de porcelana nadentio
anterior. Uma abordagem biomimtica. So Paulo:Quintessence;
2003.
REFERENCES
17. Marckley RJ. An evaluation o smiles be ore and a ter
orth-
odontic treatment. Angle Orthod. 1993 Fall;63(3):183-9.18.
Mathews TG. The anatomy o a smile. J Prosthet Dent.
1978Feb;39(2):128-34.
19. Morley J, Eubank J. Macro esthetic elements o smile design.
JAm Dent Assoc. 2001 Jan;132(1):39-45.
20. Peck S, Peck L, Kataja M. Some vertical lineaments o lip
position. Am J Orthod Dento acial Orthop.
1992Jun;101(6):519-24.
21. Puppin FA. Avaliao quantitativa de medidas dento-
aciaisrelacionadas altura da linha do sorriso. [dissertao]. Rio
deJaneiro (RJ): Universidade do Estado do Rio de Janeiro; 2002.
22. Rigsbee OH 3rd, Sperry TP, BeGole EA. The infuence o acialon
smile characteristics. Int J Adult Orthodon Orthognath
Surg.1988;3(4):233-9.
23. Rubin LR. The anatomy o a smile: its importance in
thetreatment o acial paralysis. Plast Reconstr Surg.
1974Apr;53(4):384-7.
24. Sarver DM, Ackerman MB. Dynamic smile visualization and
quanti cation: Part 1. Evolution o the concept and
dynamicrecords or smile capture. Am J Orthod Dento acial
Orthop.2003 Jul;124(1):4-12.
25. Sarver DM. The importance o incisor positioning in the
es-thetic smile: smile arc. Am J Orthod Dento acial Orthop.
2001Aug;120(2):98-111.
26. Tarantili VV, Halazonetis DJ, Spyropoulos MN. The
spontane-ous smile in dynamic motion. Am J Orthod Dento acial
Orthop.2005 Jul;128(1):8-15.
27. Tarnow DP, Magner AW, Fletcher P. The e ect o the
distancerom the contact point to the crest o bone on the
presence
or absence o the interproximal dental papilla. J
Periodontol.1992 Dec;63(12):995-6.
28. Teo CS. An evaluation o the smiling lip line. Singapore Dent
J.1981 May;6(1):27-30.
29. Tjan AH, Miller GD, The JG. Some esthetics actors in a
smile. JProsthet Dent. 1984 Jan;51(1)24-8.
30. Zachrisson BU. Esthetic actors involved in anterior
toothdisplay and smile: vertical dimension. J Clin
Orthod.1998;32(7):432-45.
Contact addressCarlos Alexandre CmaraRua Joaquim Fagundes 597,
TirolCEP: 59.022-500 Natal / RNE-mail:
[email protected]