Embed Size (px)
Citation preview
+ MODEL
Journal of the Formosan Medical Association (2016) xx, 1e11
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.jfma-onl ine.com
REVIEW ARTICLE
Establishment of a renal supportive careprogram: Experience from a ruralcommunity hospital in Taiwan
Chia-Ter Chao a,b,j, Hung-Bin Tsai c,j, Chih-Yuan Shih a,Su-Hsuan Hsu a, Yu-Chien Hung a, Chun-Fu Lai d,Ruey-Hsiuang Ueng e, Ding-Cheng Chan f,g, Juey-Jen Hwang a,h,Sheng-Jean Huang i,*
a Department of Medicine, National Taiwan University Hospital Jin-Shan Branch, New Taipei City,Taiwanb Graduate Institute of Toxicology, College of Medicine, National Taiwan University, Taipei, Taiwanc Department of Traumatology, National Taiwan University Hospital, Taipei, Taiwand Division of Nephrology, Department of Internal Medicine, National Taiwan University Hospital,Taipei, Taiwane Department of Nursing, National Taiwan University Hospital Jin-Shan Branch, New Taipei City,Taiwanf Department of Geriatrics and Gerontology, National Taiwan University Hospital, Taipei, Taiwang Department of Internal Medicine, National Taiwan University Hospital Chu-Tung Branch, Hsin-ChuCounty, Taiwanh Division of Cardiology, Department of Internal Medicine, National Taiwan University Hospital, Taipei,Taiwani Taipei City Hospital, Taipei, Taiwan
Received 10 September 2015; received in revised form 11 November 2015; accepted 10 December 2015
KEYWORDSchronic kidneydisease;
end-stage renaldisease;
hospice;palliative care;renal supportive care
Conflicts of interest: The authors h* Corresponding author. Taipei CityE-mail address: [email protected]
j Dr Chia-Ter Chao and Dr Hung-Bin
Please cite this article in press as: Chhospital in Taiwan, Journal of the Fo
http://dx.doi.org/10.1016/j.jfma.2010929-6646/Copyright ª 2016, Formosa
Renal supportive care (RSC) denotes a care program dedicated for patients with acute, chronic
renal failure, and end-stage renal disease (ESRD), aiming to offer maximal symptom relief and
optimize patients’ quality of life. The uncertainty of prognosis for patients with chronic kidney
disease and ESRD, the sociocultural issues inherent to the Taiwanese society, and the void of
structured and practical RSC pathway, contributes to the underrecognition and poor utilization
of RSC. Taiwanese patients rarely receive information regarding RSC as part of a standardized
care and are not commonly offered this option. In National Taiwan University Hospital Jinshan
branch, we started a RSC subprogram, supported by the community-based palliative/hospice
ave no conflicts of interest relevant to this article.Hospital, Number 145, Zhengzhou Road, Datong District, Taipei City 10341, Taiwan..tw (S.-J. Huang).Tsai contributed equally to this article.
ao C-T, et al., Establishment of a renal supportive care program: Experience from a rural communityrmosan Medical Association (2016), http://dx.doi.org/10.1016/j.jfma.2015.12.009
5.12.009n Medical Association. Published by Elsevier Taiwan LLC. All rights reserved.

2 C.-T. Chao et al.
+ MODEL
Please cite this article in press as: Chhospital in Taiwan, Journal of the Fo
care main program. We focused on understanding the need and providing the choice of RSC tosuitable candidates. A three-step and four-phase protocol was designed and implemented toidentify appropriate patients and to enhance the applicability of the RSC. We harnessed familyvisit and home-based family meeting as a vehicle to understand the patients’ preferences, todiscover what ESRD patients and their family value most, and to introduce the option of RSC. Inthe current review, we described our pilot experience of establishing a RSC program in Taiwan,and discuss its potential advantage.Copyright ª 2016, Formosan Medical Association. Published by Elsevier Taiwan LLC. All rightsreserved.
Introduction
The prevalence of chronic kidney disease (CKD) is esti-mated at 7% among persons who are in their thirties orolder, increasing to 23e36% among the elderly.1 Thehealthcare cost of patients with CKD and end-stage renaldisease (ESRD) confers significant burden to the existinghealthcare system; administrative data disclose that caringfor ESRD patients is responsible for nearly 2% of allhealthcare expenditure.2 Apart from its economicalimpact, the presence of CKD/ESRD and their predecessor,acute kidney injury (AKI), all increase the risk of adversepatients outcomes but can be partially ameliorated bymultidisciplinary CKD care.3,4
Other than the hard endpoints including hospitalizationrates and survival, patient-reported outcomes (PROs) inpatients with CKD/ESRD have drawn increasing attention.PROs, including health-related quality of life (HRQoL),symptom-scoring indices, and self-rated health status, aredefined as measurements based on reports coming directlyfrom patients without the amendment or interpretation bythe clinicians.5 Components of PROs and subjective symp-toms of CKD/ESRD patients have already been validated asfactors strongly associated with patient survival and renaloutcomes.6 In addition, assessment of PROs potentially im-proves patient care, enhances our understanding of patientpreferences, and most important of all, aids in the decision-making processes of patients and physicians.7,8 Moreover,existing treatments proven to provide survival benefits inCKD/ESRD patients might not offer similar improvement inPROs. Patients with ESRD, unlike those with failure of othervital organs, enjoy reasonable life expectancy beyond years,thanks to the advancement in renal replacement therapies;nonetheless, they are particularly prone to suffer fromadverse symptomatology over their lives after dialysis initi-ation.9 Therefore, for ESRD patients, PROs emerge asimportant outcomes alternative to patient survival. Weigh-ing the importance of survival against PROs becomes animportant issue during the care of CKD/ESRD patients.
Dilemma of CKD/ESRD patients: pros and consof dialysis
The course of dialysis, including hemodialysis and perito-neal dialysis, is often fraught with discomfort of differentseverities.9,10 The accessibility and convenience of main-tenance dialysis significantly prolongs the survival amongESRD patients. However, this extension in life is not without
ao C-T, et al., Establishment of armosan Medical Association (2016
cost; ESRD patients frequently have complex comorbiditiesand high symptom burdens. Local studies identify that35e70% of ESRD patient have comorbid hypertension, dia-betes mellitus, or heart failure, all of which potentiallycompromise their functional status.11,12 A U.S. studyrevealed that patients in their seventies commencing renalreplacement therapies have an estimated 1- and 5-yearsurvival of 50% and 15%, compared to 75% and 35% in dial-ysis patients without age specifications, whereas in Taiwan,the number could lie somewhere between 70e80% and40e50%, respectively.13,14 Among their dialysis career,studies from Western countries reported that an average of71% suffer from fatigue, whereas 50% are plagued by uremicpruritus, constipation, anorexia, and pain from multiplesites; in Taiwan, cross-sectional studies similarly reportedthat fatigue, dry mouth, and muscular weakness occur inmore than 50% of dialysis patients.10,15 Intradialytic hypo-tension is particularly common in these vulnerable pa-tients.16 Consequently, the reduction of discomfortassumes higher priority than maintaining their lives, atleast for some of these patients. Physicians caring forelderly with advanced CKD/ESRD should balance betweentraditional therapeutic goals (renal and overall survival)and the PROs (QoL, symptom severity) at the same time.
Trajectories of survival in elderly patients withCKD/ESRD
The dilemma in choosing the best therapies for elderly CKD/ESRD patients also stems from the ambiguity in estimatingtheir prognosis. The trajectories to death differ betweenESRD and other terminal illnesses. From the clinicians’perspective, the clinical courses of patients with renal failurecould be rather indolent compared to those of the other dis-eases, and the “turning point” of the rapid involution towardmortality might be obscure.17 From patients’ view, they alsoreport that “an unexpected turn occurs when they developESRD from diabetic nephropathy.”18 It is no wonder that themixed feelings frommultimorbidity, diverse symptomatology,and an uncertainty about their lives frequently promptsthese elderly to forgo or discontinue their dialysis carrier.
Renal palliative care/renal supportive care inTaiwan: why?
Palliative care for advanced CKD and ESRD patients, orrenal supportive care (RSC), provides multifaceted assis-tance to suitable candidates that value quality more than
renal supportive care program: Experience from a rural community), http://dx.doi.org/10.1016/j.jfma.2015.12.009

Renal supportive care in Taiwan 3
+ MODEL
quantity of their lives; alternatively, managing PROs as-sumes priority over survival for these patients. Discomfortreported by ESRD patients arises partially from dialysis perse, and the interruption or discontinuation of such therapycould potentially improve their QoL.19 Palliative care,recognized as “both patient- and family-centered carethat optimizes QoL by anticipating, preventing, andtreating suffering,” becomes increasingly important whendisease cure seems unattainable.20 This is particularly truefor the comorbidity-ridden ESRD patients, for whom dial-ysis undoubtedly prolongs their lives but does not improveor even worsens the PROs.21,22 In fact, dialysis withdrawalis currently the second to third common cause of mortalityamong ESRD patients from developed countries (around3.5 case per 100 patient-year), and there are guidelines orpositional statements from professional societies, detail-ing the why, who, and how to implement RSC(Figure 1).23,24 By contrast, the spread and adoption of RSCin Asian countries has been slow, including Taiwan. TheDialysis Outcomes and Practice Patterns Study found thatin Japan, the rate of dialysis withdrawal is significantlylower than that in Western countries.25 Although theintroduction of hospice/palliative care in Taiwan began25 years ago, the expansion of the hospice/palliative careto cover ESRD patients began only after 2010 (Figure 2).The first expert meeting on domestic palliative care modelin ESRD patients reached preliminary consensus, but de-tails on selecting the appropriate enrollees were highlydebated, in light of the cultural issues among Taiwanesepeople and other concerns.26 Currently, the government,the academic societies, the clinicians, and the patientgroups are exerting concerted efforts to increase thefeasibility of RSC in Taiwan. However, much more is stillneeded along the path.
Figure 1 The diagram illustrating the recommended potentialprofessional societies of United States (left circle) and Australia/Nthe subpopulation that both guidelines recognize to be suitable forcomorbidity index; FSZ functional status; RSCZ renal supportive
Please cite this article in press as: Chao C-T, et al., Establishment of a rhospital in Taiwan, Journal of the Formosan Medical Association (2016
Prior to establishing the domestic RSCpathway, we could.?
The importance of RSC in appropriate candidates cannot beoverstated, as PROs frequently outweigh patient survivalamong the preferences of advanced CKD/ESRD patients,especially the elderly ones. We have recognized threeimportant issues that need to be considered when evalu-ating the applicability of a RSC pathwaydthat is, theruraleurban differences, the uncertainty in prognosis esti-mation for aged renal patients, and the inherent sociocul-tural issues in Taiwan.
Ruraleurban differences
Differences in several aspects exist between rural andurban residents with CKD/ESRD, as geographic separationhas been found to negatively influence clinical outcomes.Studies identified that residential locations could impactthe accessibility to predialysis care, whereas facilityproperties as well as patient educational levels are alloutcome determinants in CKD/ESRD patients.27 Ourexperience concurs that an incrementally inverse rela-tionship exists between the distance to dialysis facilitiesand serum albumin/hemoglobin levels in chronic dialysispatients.28 The potential mediators of this associationinclude the healthcare accessibility, the timeliness ofmedical events recognition, or the literacy for healthknowledge. Judging from this, a domestic RSC programmight have different penetration rates between rural andurban areas.
Critical knowledge gaps can exist between rural andurban residents regarding RSC. The unfamiliarity with RSC
candidates for receiving RSC among different guidelines fromew Zealand (right circle). The central ellipsoid area representsreceiving RSC. ACPZ advanced care planning; CCIZ Charlsoncare; SQZ surprise question.
enal supportive care program: Experience from a rural community), http://dx.doi.org/10.1016/j.jfma.2015.12.009

Figure 2 Timelines depicting the temporal trend of palliative/hospice care program establishment and the Taiwan NHI reim-bursement schemes change. ESRDZ end-stage renal disease; MVZmechanical ventilation; NHIZ National Health Insurance;TSNZ Taiwan Society of Nephrology.
4 C.-T. Chao et al.
+ MODEL
among medical students, primary care physicians, generalinternists, and laypersons might lead to misunderstandingwhen medical communication takes place.29 Interdisci-plinary effort is often required to facilitate discussionsabout end-of-life (EOL) care in a need-oriented way,30 butdedicated specialists including psychologists and socialworkers are frequently lacking in rural areas. The patient/physician ratio is also higher in the geographically remoteregions, reducing the time each physician can spend ininterview or family meeting. Finally, its takes longer timefor older and noncancer terminal patients to understandthe option of RSC than for younger ones, which occupies alower percentage of the rural population.30 Both localstudies and those from other countries found that decision-making processes are often suboptimal in older andnoncancerous patients being hospitalized.31,32 Aging pa-tients are frequently impaired in their communicativeability owing to the visual and auditory dysfunction,requiring proxies for assistance in decision-making. Infer-ring their true wishes poses another challenge if we want tosuccessfully establish a domestic RSC program.33
Despite the abovementioned concerns, there are advan-tages for starting an RSC program in rural areas. In ourexperience, rural residents maintain a better relationshipwith their primary care physicians owing to a deep-rootedacquaintance. Rural Taiwanese patients, especially those ofadvanced age, tend to completely rely on physicians tomakerecommendations on treatment options, with little personalinput. Furthermore, we also found that rural elderly patientsplace more emphasis on their symptom burden than on theduration of survival, compared to their urban counterparts.These features should be factored into consideration prior toimplementing the RSC program in different areas.
Please cite this article in press as: Chao C-T, et al., Establishment of ahospital in Taiwan, Journal of the Formosan Medical Association (2016
Prognosis estimation
To accurately estimate the duration of survival as possiblein advanced CKD/ESRD patients is the cornerstone for allRSC programs; such estimation provides suitable candidateswith a reasonable expectation of their life span, based onwhich medical decisions can be made. Domestic studiesidentified that terminally ill patients with inaccurateprognostic awareness are more likely to be undecided uponinvasive life-sustaining treatments.34 Existing RSC guide-lines suggest different prognosis-estimation formulae,23,24
and the core variables include age, comorbidity, nutri-tional status, and functional levels, aided by the “surprisequestion.” Modified Charlson score, prognostic scores byCouchoud et al35 and Cohen et al36 are the most commontools for prognosis prediction in predialysis and chronicdialysis patients. However, none of these formulae derivefrom a predominantly Asian population, and the accuracyamong Taiwanese patients is unknown. Consequently, adomestic prognosis-estimation formula in patients withadvanced CKD/ESRD would be beneficial. Kan et al37 haveconducted a pilot study on this issue by designing a newcomorbidity index system for elderly dialysis patients, usingTaiwan National Health Insurance database analysis. How-ever, more studies are needed to validate its utility, andmodification of this formula with the incorporation of othervariables would be anticipated in the future.
Sociocultural issue in Taiwanese society
The discussions surrounding EOL care is frequently avoidedconsciously or subconsciously in Taiwan.26,32,33 Family
renal supportive care program: Experience from a rural community), http://dx.doi.org/10.1016/j.jfma.2015.12.009

Renal supportive care in Taiwan 5
+ MODEL
members may regard physicianepatient discussions on EOLcare as taboos that will bring bad luck to their sick rela-tives. The responsibility of medical decision-making oftenfalls on the patients’ bloodlines or spouses, called “Family-centered decision-making model.”26 Domestic studies re-ported that among a large cohort of oncology patients, only22.6% signed their own Do-Not-Resuscitate (DNR) orders,and 67.6% of the DNR forms signed by patients wereincomplete, compared to 81.7% by their surrogate(s).38 Thisexemplifies the phenomenon that in Taiwan, disclosure ofthe terminal status is potentially unpleasant for familymembers or sometimes for patients; in response, medicaldecision-making is often accomplished by patients’ surro-gates.39 For patients with advanced CKD/ESRD, the unde-termined prognosis and the family-centered model mightprompt physicians to avoid telling the truth to patients,potentially interfering with the implementation of the RSCprogram.
Implementation of RSC in Taiwan: how?
A successful RSC program can potentially relieve patientsuffering, enhance both patient and family satisfaction,and ultimately reduce unnecessary healthcare spending.40
However, in Taiwan, very few have addressed the issue ofsuccessfully implementing a domestic RSC program.
National Taiwan University Hospital Jinshan branch(NTUH-JS) is a community hospital in the rural outskirt ofNew Taipei City.28 Supported by its main branch, a tertiaryreferral center, NTUH-JS has initiated a community-basedpalliative/hospice care program since 2012, with anoutreach RSC subprogram aiming to offer the best con-servative management for rural residents covered byNTUH-JS medical service. We will briefly overview our 4-year experience in advancing the RSC subprogram in thefollowing section, from how to recognize potential candi-dates, to the three-step/four-phase care structures weprovided.
Identification of appropriate candidates for RSC
Who will benefit the most from RSC has been the center ofdebate in the literature. Most clinicians agree that fullyinformed patients with decision-making capacity and whenmaking voluntary choices about refusing dialysis orrequesting to discontinue dialysis are suitable candidates;those with previous explicit expressions of such wills in theform of advance directives, or with properly appointedsurrogates, would also be candidates for RSC. However,apart from these commonalities, significant disparitiesemerge in the indications of RSC between countries(Figure 1). For example, the U.S. version places moreemphasis on neurological and extrarenal conditions,whereas the Australian/New Zealand version providesphenotype-based descriptions of suitable candidates. InTaiwan, a formal consensus has not been unanimouslyreached, but adaptations of criteria for RSC candidatesfrom other countries have been recommended.
To deal with this controversy, we adapted a hospice/palliative need assessment form (Table 1) from the StMary’s Medical Center Palliative Care Screening Tool. Our
Please cite this article in press as: Chao C-T, et al., Establishment of a rhospital in Taiwan, Journal of the Formosan Medical Association (2016
form includes five categories: the main diagnosis with life-threatening impact, the comorbidities, the current func-tional status (Eastern Co-operative Oncology Group scale),the miscellaneous conditions, and the surprise question. Allthe chronic dialysis patients in NTUH-JS dialysis unitsreceived a formal assessment using this form, and thosewith scores higher than 5 were offered the choice ofentering into our RSC subprogram. Interfacility palliativecare coordination between NTUH-JS, NTUH main branch,and primary care clinics also exists to maximize patientidentification and recruitment (Figure 3).
Step one: home-based family visit
After the identification of suitable RSC candidates, weconducted family visits (FVs) for all of them on an annualbasis. There are several advantages offered by FVs forchronic dialysis patients; first, psychosocial factors,including the health interference of social activities, thedissatisfaction with family and staffs, and the sense ofisolation occur in more than one-half of ESRD patients,correlating significantly with their QoL.41,42 FV has beenfound to improve the communication between familymembers and patients, and ameliorate patients’ psycho-logical suffering.43,44 We found that patient satisfactionimproved significantly after our FVs, and the rapportgained during FVs could be helpful in arranging subsequentfamily meetings and EOL discussions. Second, EOL careinvolves the designation of the preferred place of death,and a domestic study found that 67% of the patients’ familymembers chose home as the preferred place of death.45 Ina rural and mountainous area where NTUH-JS is located,FVs can help physicians estimate the transport time be-tween the patient residences and the dialysis units, if thepatients wish to receive RSC in hospital-based settings.Finally, FVs enable physicians to understand more thor-oughly the symptom burdens of these patients. ESRD pa-tients, despite their diverse symptomatology, often fail todisclose in detail how they feel to physicians or other staffmembers in the dialysis units. Consequently, an opportu-nity to walk into patients’ lives increases the willingness ofphysicians to show more empathy, facilitating the subse-quent introduction of the RSC concept.
Step two: home-based family meeting in an openatmosphere
Self-reported knowledge of renal palliative care is pooramong CKD and ESRD patients, and only 12e22% of patientsunderstand the meaning and implications of palliative/hospice care.40,46 Even in developed countries, more than90% of CKD and ESRD patients are unaware of their illnesstrajectories, despite the fact that most participants wish toknow their medical conditions and prognosis.46 Further-more, 80% of CKD/ESRD patients rely on nephrologists forobtaining health information, and 66e70% feel comfortablein EOL discussions with their family members. These find-ings point out the importance of involving family membersand nephrologists in a successful RSC program.
Home-based palliative care is often used in clinicalsettings, but home-based family meeting for RSC is rarely
enal supportive care program: Experience from a rural community), http://dx.doi.org/10.1016/j.jfma.2015.12.009

Table 1 National Taiwan University Hospital Jinshan branch hospice/palliative care assessment form.
Abbreviations: ARDS, adult respiratory distress syndrome; Cat, Category; COPD, chronic obstructive pulmonary disease; MOF,multi-organ failure.
+ MODEL
Please cite this article in press as: Chao C-T, et al., Establishment of a renal supportive care program: Experience from a rural communityhospital in Taiwan, Journal of the Formosan Medical Association (2016), http://dx.doi.org/10.1016/j.jfma.2015.12.009

Figure 3 The geographic location of NTUH-JS hospital and the residential sites of dialysis patients covered by NTUH-JS. NTUH-JSZ National Taiwan University Hospital Jinshan branch.
Renal supportive care in Taiwan 7
+ MODEL
attempted. ESRD patients prefer more privacy during EOLdiscussions in a separate room during dialysis or in an in-dividual clinic, compared to those held in dialysis units.46
In Taiwan, dialysis units are less spacious than those inother countries, and patient could easily overhear thewords from others during the talk. Lack of privacy could bea critical but under-ecognized factor in determiningwhether an EOL discussion will succeed. In our home-basedRSC program, we test the feasibility for nephrologists toshare prognostic and EOL information with candidates attheir home, where patients are expectedly more relaxedand open-minded.
The location in which the EOL discussion takes place isimportant. Literature suggests that the hospital settinglikely plays a role in influencing patients’ perceptions.47
Although counseling held in individual clinics is more pref-erable than in dialysis units, patients facing the disclosureof a poor prognosis tend to be emotionally unstable. In suchcases, a familiar space, along with the presence of theirloved ones, could ease their uneasiness, reducing the ten-sion that might emerge without proper environmentalsetup. In addition, nephrologists can provide recommen-dations for home preparation if RSC is deemed appropriate.
An open atmosphere is also required for a successful EOLdiscussion. Traditionally, family meetings involve schedulesset in advance with all parties. Although meetings arrangedaccording to standardized protocols can decrease tension,the lack of flexibility in such circumstances might deferdecision-making by patients or family members during theEOL talk.30 The privacy and sense of ease offered by home-based family meeting could reduce the conflict andenhance the patients/family’s willingness to consider allpossible scenarios, even the worse ones.
Please cite this article in press as: Chao C-T, et al., Establishment of a rhospital in Taiwan, Journal of the Formosan Medical Association (2016
Step three: postdecision EOL care
Decision phaseOnce the patients or their proxies decide upon receiving RSC,patients then enter into the first of the four stages of EOLcare for renal patients (Figure 4). The four stagesdthe de-cision, the stabilization, the near-death, and the bereave-ment phasesdeach contain different goals of care. In thedecision phase, the content of RSC will be explained indetail, along with prognosis estimation and conflict resolu-tion, all of which take several rounds of family meetings toachieve. Informed consent will be sought if patients arecompetent, assisted by folk communicators and/or villageheads; otherwise, a patient proxy, supported by familymembers, will be designated after family meetings. We willalso inquire about the acceptability of DNR, and explainabout the pros and cons of aggressive resuscitation. Ne-phrologists, patients, and their family members will reach aconclusion on the appropriate timing of RSC implementation(dialysis withdrawal or withhold). Finally, advanced careplanning constitutes another important issue in this phase.
Stabilization phaseThe stabilization phase is a symptom-free period lastingfrom days to as long as weeks after RSC is initiated(Figure 4). Symptoms of cutis, respiratory, or gastrointes-tinal tract are reduced to a minimal level with optimallyadjusted medications. Oral intake or intravenous fluid canbe given ad libitum, according to patients’ wishes andtolerability. This phase offers time and opportunity forrenal patients to do what they have been longing for buthave never accomplished before, assisted by family mem-bers and dedicated staff members.
enal supportive care program: Experience from a rural community), http://dx.doi.org/10.1016/j.jfma.2015.12.009
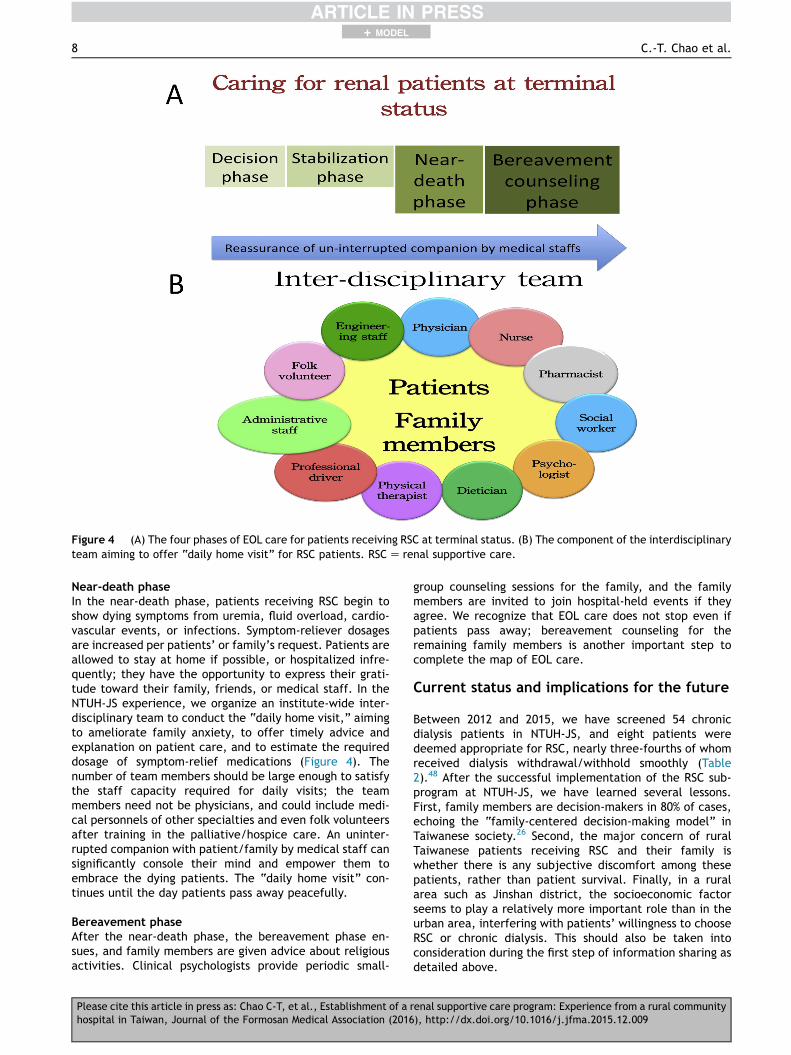
Figure 4 (A) The four phases of EOL care for patients receiving RSC at terminal status. (B) The component of the interdisciplinaryteam aiming to offer “daily home visit” for RSC patients. RSCZ renal supportive care.
8 C.-T. Chao et al.
+ MODEL
Near-death phaseIn the near-death phase, patients receiving RSC begin toshow dying symptoms from uremia, fluid overload, cardio-vascular events, or infections. Symptom-reliever dosagesare increased per patients’ or family’s request. Patients areallowed to stay at home if possible, or hospitalized infre-quently; they have the opportunity to express their grati-tude toward their family, friends, or medical staff. In theNTUH-JS experience, we organize an institute-wide inter-disciplinary team to conduct the “daily home visit,” aimingto ameliorate family anxiety, to offer timely advice andexplanation on patient care, and to estimate the requireddosage of symptom-relief medications (Figure 4). Thenumber of team members should be large enough to satisfythe staff capacity required for daily visits; the teammembers need not be physicians, and could include medi-cal personnels of other specialties and even folk volunteersafter training in the palliative/hospice care. An uninter-rupted companion with patient/family by medical staff cansignificantly console their mind and empower them toembrace the dying patients. The “daily home visit” con-tinues until the day patients pass away peacefully.
Bereavement phaseAfter the near-death phase, the bereavement phase en-sues, and family members are given advice about religiousactivities. Clinical psychologists provide periodic small-
Please cite this article in press as: Chao C-T, et al., Establishment of ahospital in Taiwan, Journal of the Formosan Medical Association (2016
group counseling sessions for the family, and the familymembers are invited to join hospital-held events if theyagree. We recognize that EOL care does not stop even ifpatients pass away; bereavement counseling for theremaining family members is another important step tocomplete the map of EOL care.
Current status and implications for the future
Between 2012 and 2015, we have screened 54 chronicdialysis patients in NTUH-JS, and eight patients weredeemed appropriate for RSC, nearly three-fourths of whomreceived dialysis withdrawal/withhold smoothly (Table2).48 After the successful implementation of the RSC sub-program at NTUH-JS, we have learned several lessons.First, family members are decision-makers in 80% of cases,echoing the “family-centered decision-making model” inTaiwanese society.26 Second, the major concern of ruralTaiwanese patients receiving RSC and their family iswhether there is any subjective discomfort among thesepatients, rather than patient survival. Finally, in a ruralarea such as Jinshan district, the socioeconomic factorseems to play a relatively more important role than in theurban area, interfering with patients’ willingness to chooseRSC or chronic dialysis. This should also be taken intoconsideration during the first step of information sharing asdetailed above.
renal supportive care program: Experience from a rural community), http://dx.doi.org/10.1016/j.jfma.2015.12.009

Table 2 Selected patients received renal supportive care in NTUH Jinshan branch.
Age(y)
Sex Religion Clinicalscenario
Dialysisvintage
Decision maker RSC settings Survivalduration a
Main issues of concern bypatients or family members
Case 1 75 F Taoism CKD stage 5D 3 y Family members Community-based 7 d 1. Repeated hospitaliza-tions with deconditioning
2. SepsisCase 2 80 F Taoism CKD stage 5 Not yet Patient Community-based 3 d (from
discharge)1. Subjective discomfort2. Balancing between avail-
ability of long-term careand the burden on herfamily
Case 3 90 F Taoism Acute on CKD(stage IIIb)
Not yet Family members Community-based 4 d (fromdiagnosis)
1. Subjective discomfort
Case 4 77 F Taoism CKD stage 5D 10 y Family members Community-based 7 d 1. Subjective discomfort2. Severe functional
limitation3. Poor survival from
advanced esophagealcancer
Case 5 55 M None CKD stage 5D 2 y Patient andFamilymembers
Community-based 3 d 1. Subjective discomfort2. Poor survival from gastric
cancer with multiplemetastases
CKDZ chronic kidney disease; NTUHZ National Taiwan University Hospital.Note. From “Incorporating palliative care into the dialysis unit affects patterns near the end of life,” by C.F. Lai, S.H. Hsu and S.J.Huang, 2015, Mayo Clin Proc, 90, p. 1307e9. Copyright 2015, Elsevier Inc. Partly adapted with permission.
a After dialysis withdrawal or withhold.
Renal supportive care in Taiwan 9
+ MODEL
By contrast, we have encountered difficulty in explainingprognostic information for those who are elderly, have loweducational levels, and are less cognitively competent. Theprognostic models recommended by different professionalsocieties can be too complicated for rural residents to un-derstand. We are currently investigating whether we couldintroduce the concept of frailty into our RSC program.49
Frailty denotes a phenotype of age-associated physical andfunctional decline in the elderly, and the prevalence offrailty in CKD/ESRDpatients is high. The presence of frailty inCKD/ESRD patients is associated with cardiovascular eventsand poor outcomes.50,51 The frequent coexistence of frailtyand CKD/ESRD might be an important hinge that we can levywhen explaining prognosis, because frailty is often explicit inappearance. However, further research is still needed.
Conclusion
Initiating a successful RSC program is often thought to bedifficult in Taiwanese society, and the complex socioculturalinherent issue is an important concern. Through the three-step and four-phase RSC infrastructure, we attempt toconfront this dilemma and the progress is fair so far.Although the case number is still low, we believe a widerapplication of our approach could improve the feasibility ofRSC in Taiwan.
Author contributions
CTC, HBT, and SJH are responsible for conception anddesign of this study; CTC, HBT, CYS, SHH, YCH, CFL, and
Please cite this article in press as: Chao C-T, et al., Establishment of a rhospital in Taiwan, Journal of the Formosan Medical Association (2016
RHU are responsible for acquisition of data; CTC, HBT, DCC,JJH, and SJH are responsible for analysis and data inter-pretation; CTC, HBT, and SJH drafted and revised themanuscript. All authors read the manuscript and approvedthe submission of this manuscript.
Acknowledgments
We are grateful to all the NTUH-JS staff members andvolunteers for assisting in RSC subprogram preparation andimplementations.
References
1. Zhang Q-L, Rothenbacher D. Prevalence of chronic kidneydisease in population-based studies: systematic review. BMCPublic Health 2008;8:117.
2. De Vecchi AF, Dratwa M, Wiedemann ME. Healthcare systemsand end-stage renal disease (ESRD) therapiesdan internationalreview: costs and reimbursement/funding of ESRD therapies.Nephrol Dial Transplant 1999;14:31e41.
3. Wouters OJ, O’Donoghue DJ, Ritchie J, Kanavos PG, Narva AS.Early chronic kidney disease: diagnosis, management andmodels of care. Nat Rev Nephrol 2015;11:491e502.
4. Chao CT, Tsai HB, Wu CY, Lin YF, Hsu NC, Chen JS, et al. Theseverity of initial acute kidney injury at admission of geriatricpatients significantly correlates with subsequent in-hospitalcomplications. Sci Rep 2015;5:13925.
5. Perrone RD, Joel Coons S, Cavanaugh K, Finkelstein F,Meyer KB. Patient-reported outcomes in clinical trials of CKD-related therapies: report of a symposium sponsored by the
enal supportive care program: Experience from a rural community), http://dx.doi.org/10.1016/j.jfma.2015.12.009

10 C.-T. Chao et al.
+ MODEL
National Kidney Foundation and the US Food and Drug Admin-istration. Am J Kidney Dis 2013;62:1046e57.
6. Tsai Y-C, Hung C-C, Hwang S-J, Wang S-L, Hsiao S-M, Lin M-Y,et al. Quality of life predicts risks of end-stage renal diseaseand mortality in patients with chronic kidney disease. NephrolDial Transplant 2010;25:1621e6.
7. Cavanaugh KL. Prioritizing patient-centered care imple-mentation and research for patients with kidney disease.Semin Dial 2015;28:131e40.
8. Robinson-Cohen C, Hall YN, Katz R, Rivara MB, de Boer IH,Kestenbaum BR, et al. Self-rated health and adverse events inCKD. Clin J Am Soc Nephrol 2014;9:2044e51.
9. Lee BO, Lin CC, Chaboyer W, Chiang CL, Hung CC. The fatigueexperience of haemodialysis patients in Taiwan. J Clin Nurs2007;16:407e13.
10. Yu IC, Huang JY, Tsai YF. Symptom cluster among hemodialysispatients in Taiwan. Appl Nurs Res 2012;25:190e6.
11. Chao CT, Lee SY, Yang WS, Yen CJ, Chiang CK, Huang JW, et al.Serum vitamin D levels are positively associated with varicellazoster immunity in chronic dialysis patients. Sci Rep 2014;4:7371.
12. Yang CW, Tzeng NS, Yin YJ, Li CH, Chen HA, Chiu SH, et al.Angiotensin receptor blockers decrease the risk of majoradverse cardiovascular events in patients with end-stage renaldisease on maintenance dialysis: a nationwide matched-cohortstudy. PLoS One 2015;10:e0140633.
13. Kurella M, Covinsky KE, Collins AJ, Chertow GM. Octogenariansand nonagenarians starting dialysis in the United States. AnnIntern Med 2007;146:177e83.
14. Ministry of Health and Welfare and National Health ResearchInstitute. 2014 Annual Report on Kidney Disease in Taiwan.2015. p. 38.
15. Murtagh FEM, Addington-Hall J, Higginson IJ. The prevalence ofsymptoms in end-stage renal disease: a systematic review. AdvChronic Kidney Dis 2007;14:82e99.
16. Chao CT, Huang JW, Yen CJ. Intradialytic hypotension andcardiac remodeling: a vicious cycle. Biomed Res Int 2015;2015:724147.
17. Murtagh FEM, Sheerin NS, Addington-Hall J, Higginson IJ. Tra-jectories of illness in stage 5 chronic kidney disease: a longi-tudinal study of patient symptoms and concerns in the last yearof life. Clin J Am Soc Nephrol 2011;6:1580e90.
18. Yu IC, Tsai YF. From silence to storm e patient illness trajec-tory from diabetes diagnosis to haemodialysis in Taiwan: aqualitative study of patients’ perceptions. J Adv Nurs 2013;69:1943e52.
19. Peng YS, Chiang CK, Hung KY, Chang CH, Lin CY, Yang CS, et al.Comparison of self-reported health-related quality of life be-tween Taiwan hemodialysis and peritoneal dialysis patients: amulti-center collaborative study. Qual Life Res 2011;20:399e405.
20. Grubbs V, Moss AH, Cohen LM, Fischer MJ, Germain MJ,Jassal SV, et al. A palliative approach to dialysis care: apatient-centered transition to the end of life. Clin J Am SocNephrol 2014;9:2203e9.
21. Chao CT, Wu VC, Lai CF, Shiao CC, Huang TM, Wu PC, et al.Advanced age affects the outcome-predictive power of RIFLEclassification in geriatric patients with acute kidney injury.Kidney Int 2012;82:920e7.
22. Chao CT, Lin YF, Tsai HB, Wu VC, Ko WJ. Acute kidney injurynetwork staging in geriatric postoperative acute kidney injurypatients: shortcomings and improvements. J Am Coll Surg2013;217:240e50.
23. Moss AH. Revised dialysis clinical practice guideline promotesmore iformed decision-making. Clin J Am Soc Nephrol 2010;5:2380e3.
24. Brown MA, Crail SM, Masterson R, Foote C, Robins J, Katz I,et al. ANZSN Renal Supportive Care Guidelines 2013.Nephrology 2013;18:401e54.
Please cite this article in press as: Chao C-T, et al., Establishment of ahospital in Taiwan, Journal of the Formosan Medical Association (2016
25. Robinson B, Zhang J, Morgenstern H, Bradbury BD, Ng LJ,McCullough K, et al. World-wide, mortality is a high risk soonafter initiation of hemodialysis. Kidney Int 2014;85:158e65.
26. Lai C-F, Tsai H-B, Hsu S-H, Chiang C-K, Huang J-W, Huang S-J.Withdrawal from long-term hemodialysis in patients with end-stage renal disease in Taiwan. J Formos Med Assoc 2013;112:589e99.
27. McClellan WM, Wasse H, McClellan AC, Kipp A, Waller LA,Rocco MV. Treatment center and geographic variability in pre-ESRD care associate with increased mortality. J Am SocNephrol 2009;20:1078e85.
28. Chao C-T, Lai C-F, Huang J-W, Chiang C-K, Huang S-J. Associ-ation of increased travel distance to dialysis units with the riskof anemia in rural chronic hemodialysis elderly. Hemodial Int2015;19:44e53.
29. Shih CY, Hu WY, Lee YT, Yao CA, Chen CY, Chiu TY. Effect of acompassion-focused training program in palliative care edu-cation for medical students. Am J Hosp Palliat Care 2013;30:114e20.
30. Galushko M, Romotzky V, Voltz R. Challenges in end-of-lifecommunication. Curr Opin Support Palliat Care 2012;6:355e64.
31. Chambaere K, Bilsen J, Cohen J, Onwuteaka-Philipsen BD,Mortier F, Deliens L. Trends in medical end-of-life decisionmaking in Flanders, Belgium 1998e2001e2007. Med DecisMaking 2011;31:500e10.
32. Huang HL, Chiu TY, Lee YT, Yao CA, Chen CY, Hu WY. Familyexperience with difficulty decisions in end-of-life care. Psy-chooncology 2012;21:785e91.
33. Tang ST, Liu TW, Liu LN, Chiu CF, Hsieh RK, Tsai CM. Phys-icianepatient end-of-life care discussions: correlates andassociations with end-of-life preferences of cancer patientse a cross-sectional survey study. Palliat Med 2014;28:1222e30.
34. Tang ST, Wen FH, Hsieh CH, Chou WC, Chang WC, Chen JS,et al. Preferences for life-sustaining treatments and associa-tions with accurate prognostic awareness and depressivesymptoms in terminally ill cancer patients’ last yeat of life. JPain Symptom Manage 2016;51:41e51.
35. Couchoud C, Labeeuw M, Moranne O, Allot V, Esnault V,Frimat L, et al. A clinical score to predict 6-month prognosis inelderly patients starting dialysis for end-stage renal disease.Nephrol Dial Transplant 2009;24:1553e61.
36. Cohen LM, Ruthazer R, Moss AH, Germain MJ. Predicting six-month mortality for patients who are on maintenance hemo-dialysis. Clin J Am Soc Nephrol 2010;5:72e9.
37. Kan W-C, Wang J-J, Wang S-Y, Sun Y-M, Hung C-Y, Chu C-C,et al. The new comorbidity index for predicting survival inelderly dialysis patients: a long-term population-based study.PLoS ONE 2013;8:e68748.
38. Wen K-Y, Lin Y-C, Cheng J-F, Chou P-C, Wei C-H, Chen Y-F,et al. Insights into Chinese perspectives on do-not-resuscitate(DNR) orders from an examination of DNR order formcompleteness for cancer patients. Support Care Cancer 2013;21:2593e8.
39. Cheng SY, Suh SY, Morita T, Oyama Y, Chiu TY, Koh SJ, et al.Cross-cultural study on behaviors when death is approaching inEast Asian countries: what are the physician-perceived com-mon beliefs and practices? Medicine 2015;94:e1573.
40. Hung YS, Chen CH, Yeh KY, Chang H, Huang YC, Chang CL, et al.Potential benefits of palliative care for polysymptomatic pa-tients with late-stage nonmalignant disease in Taiwan. J For-mos Med Assoc 2013;112:406e15.
41. Yang YJ, Huang JW, Peng YS, Chiang SS, Yang CS, Yang CC,et al. Quality of sleep and psychosocial factors for patientsundergoing peritoneal dialysis. Perit Dial Int 2007;27:675e80.
42. Kao TW, Lai MS, Tsai TJ, Jan CF, Chie WC, Chen WY. Economic,social, and psychological factors associated with health-related
renal supportive care program: Experience from a rural community), http://dx.doi.org/10.1016/j.jfma.2015.12.009

Renal supportive care in Taiwan 11
+ MODEL
quality of life of chronic hemodialysis patients in northernTaiwan: a multicenter study. Artif Organs 2009;33:61e8.
43. McCallion P, Toseland RW, Freeman K. An evaluation of afamily visit education program. J Am Geriatr Soc 1999;47:203e14.
44. Lin J, Hsiao CT, Gien R, Pai JY, Zeng SH. Perceived servicequality, perceived value, overall satisfaction and happiness ofoutlook for long-term care institution residents. Health Expect2014;17:311e20.
45. Shih C-Y, Hu W-Y, Cheng S-Y, Yao C-A, Chen C-Y, Lin Y-C, et al.Patient preferences versus family physicians’ perceptionsregarding the place of end-of-life care and death: a nationwidestudy in Taiwan. J Palliat Med 2015;18:625e30.
46. Davison SN. End-of-life care peferences and needs: percep-tions of patients with chronic kidney disease. Clin J Am SocNephrol 2010;5:195e204.
47. Osborn TR, Curtis JR, Nielsen EL, Back AL, Shannon SE,Engelberg RA. Identifying elements of ICU care that families
Please cite this article in press as: Chao C-T, et al., Establishment of a rhospital in Taiwan, Journal of the Formosan Medical Association (2016
report as important but unsatisfactory: decision-making, con-trol, and ICU atmosphere. Chest 2012;142:1185e92.
48. Lai CF, Hsu SH, Huang SJ. Incorporating palliative care into thedialysis unit affects patterns near the end of life. Mayo ClinProc 2015;90:1307e9.
49. Chao C-T, Hsu Y-H, Chang P-Y, He Y-T, Ueng R-S, Lai C-F, et al.Simple self-report FRAIL scale might be more closely associ-ated with dialysis complications than other frailty screeninginstruments in rural chronic dialysis patients. Nephrology 2015;20:321e8.
50. Alfaadhel TA, Soroka SD, Kiberd BA, Landry D, Moorhouse P,Tennankore KK. Frailty and mortality in dialysis: evaluation ofa clinical frailty scale. Clin J Am Soc Nephrol 2015;10:832e40.
51. Chao CT, Huang JW. Frailty severity is significantly associatedwith electrocardiographic QRS duration in chronic dialysis pa-tients. Peer J 2015;3:e1354.
enal supportive care program: Experience from a rural community), http://dx.doi.org/10.1016/j.jfma.2015.12.009