Embed Size (px)
Citation preview

at SciVerse ScienceDirect
Clinical Nutrition 31 (2012) 630e636
Contents lists available
Clinical Nutrition
journal homepage: http: / /www.elsevier .com/locate/clnu
Original article
Essential trace element status and clinical outcomes in long-term dialysispatients: A two-year prospective observational cohort study
Chih-Yu Yang a,d,e, Ming-Ling Wu b,c,d,e, Yea-Yun Chou a, Szu-Yuan Li a,d, Jou-Fang Deng b,d,Wu-Chang Yang a,d, Yee-Yung Ng a,d,*
aDivision of Nephrology, Department of Medicine, Taipei Veterans General Hospital, Taipei, TaiwanbDivision of Clinical Toxicology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwanc Institute of Environmental and Occupational Health Sciences, National Yang-Ming University, Taipei, Taiwand School of Medicine, National Yang-Ming University, Taipei, Taiwan
a r t i c l e i n f o
Article history:Received 1 April 2011Accepted 17 February 2012
Keywords:Trace elementZincDialysisOutcomeInfectionMortality
* Corresponding author. Division of Nephrology, DeVeterans General Hospital, No. 201, Section 2, Shih-PTel.: þ886 2 2871 2121x2987; fax: þ886 2 2875 7841
E-mail address: [email protected] (Y.-Y. Ng).e Yang C and Wu M contributed equally to this wo
0261-5614/$ e see front matter � 2012 Elsevier Ltd adoi:10.1016/j.clnu.2012.02.008
s u m m a r y
Background & aims: Essential trace elements are involved in many biological processes for normal cellfunction including immunological defense against oxidation and infection. Deficiency of these elementsgenerally leads to illness or even death in the general population. Therefore, we investigated thepredictive values of trace element status on clinical outcomes in dialysis patients, who are more prone totrace element deficiency.Methods: We enrolled 111 prevalent patients on maintenance dialysis from a Taipei tertiary-care referralhospital and measured serum levels of selenium, copper, and zinc. Patients were followed for 2 years oruntil death or withdrawal.Results: Multivariate Cox regression analysis indicated that patients with diabetes mellitus (HR, 2.162[95% CI, 1.105e4.232], p¼ 0.024), prior stroke (HR, 3.876 [95% CI, 1.136e13.221], p¼ 0.030), and zincdeficiency (HR, 0.979 [95% CI, 0.966e0.992], p¼ 0.002) were more likely to be hospitalized for infectiousdiseases. Furthermore, beyond traditional risk factors, such as old age and hypoalbuminemia, multi-variate Cox regression also indicated that lower serum level of zinc independently predicts overallmortality (HR, 0.973 [95% CI, 0.948e0.999], p¼ 0.046).Conclusions: In long-term dialysis patients, the serum level of zinc was an independent predictor offuture hospitalization due to infectious diseases and of overall mortality.
� 2012 Elsevier Ltd and European Society for Clinical Nutrition and Metabolism. All rights reserved.
1. Introduction
Although uremic patients undergoing long-term dialysis mayaccumulate deleterious toxic trace elements, such as arsenic,mercury, lead and cadmium due to the use of contaminated dialysisfluid,1 essential trace element deficiencies such as selenium (Se)and zinc (Zn) are prevalent among dialysis patients.2e4 Deficiencyin trace elements is known to have adverse health effects, and thebiological impact in patients with renal insufficiency is even higherthan in the general population.
partment of Medicine, Taipeiai Road, Taipei 11217, Taiwan..
rk.
nd European Society for Clinical N
Essential trace element status was independently related toimmune status, inflammation, oxidative damage, lymphocytefunction, and granulocyte motility.5e14 For example, at the molec-ular level, Zn is an important co-factor for diverse enzymes,peptides, transcriptional factors, and cytokines that are involved invarious aspects of normal immune responses.6 Meanwhile, Zn isessential for one of the most important free radical scavengers, thecopper zinc form of superoxide dismutase (CuZuSOD, SOD1).Furthermore, a previous study showed that Zn supplementationdecreases the serum level of C-reactive protein (CRP) in dialysispatients.15 Trace elements are essential for the maintenance ofnormal immune system function, so patients with essential traceelement deficiencies are expected to be more susceptible to infec-tious diseases and have worse prognoses. However, very fewstudies have examined the effect of these deficiencies on clinicaloutcomes.1e3,16
Dialysis patients are at risk for essential trace element defi-ciencies and infectious diseases, so we postulated that the poor
utrition and Metabolism. All rights reserved.

C.-Y. Yang et al. / Clinical Nutrition 31 (2012) 630e636 631
immune function of dialysis patients may be partly related to theiressential trace element deficiencies. The aim of this study was toexamine whether essential trace element deficiencies are associ-ated with future infectious diseases or mortality in end-stage renaldisease (ESRD) patients undergoing long-term dialysis.
2. Patients and methods
2.1. Study protocol and subjects
From July 2008 to June 2010, we conducted a prospectiveobservational cohort study at Taipei Veterans General Hospital,a tertiary-care referral hospital. Each subject provided writteninformed consent, and the Institutional Review Board of thisinstitution approved the study. All patients were at least 18 years ofage, had ESRD, and were on maintenance hemodialysis (HD) orperitoneal dialysis (PD) for at least 6 months. We excluded patientswho refused to provide consent, andwho did not agree to the bloodtest for trace elements after an 8-h fasting period. A total of 43 HDpatients and 68 PD patients were enrolled.
At the study entry, all patients underwent measurement ofserum essential trace elements, including Se, copper (Cu), and Zn.Demographic features and clinical parameters, including age,gender, duration of dialysis, body weight index, comorbidities,nutritional supplements, medications, serum biochemical data, andblood cell counts were recorded. The indices of smoking andalcohol consumption were coded as never (0), quit (1), less thanonce weekly (2), more than once weekly (3), and at least once daily(4). The index of the exposure history of heavy metal chemicalswere coded as never (0), less than once weekly (1), more than onceweekly (2). The indices of herbal drug use and vitamin supplementwere coded as at least once daily (1), more than once weekly (2),less than once weekly (3), and never (4).
2.2. Healthy subjects
We also checked the serum levels of essential trace elements in67 healthy subjects with normal renal function. Mean age was 36years and 64% of patients were male. A total of 1 patient (1.5%) haddiabetes mellitus and 7 patients (10.4%) had hypertension amonghealthy subjects.
2.3. Dialysis procedures
HD was performed three times weekly (4 h per session) using1.8-m2 surface area dialyzers with bicarbonate-based dialysateswith calcium at a concentration of 2.5e3.0 mEq/L. PD was providedas continuous ambulatory PD or automated PD. All patients weretreated with recombinant human erythropoietin, with a targethematocrit level of 30e36%. Kt/V of HD patients was 1.67� 0.24,and Kt/V of PD patients was 2.17� 0.40.
2.4. Measurements of serum trace elements
Fasting venous blood specimens were drawn before the mid-week HD session and collected into no additive Vacutainer blood-collecting tubes (BectoneDickinson, Franklin Lakes, New Jersey,USA) according to standard hospital guidelines for venipunctureand sample collection. The serum separator tube specimens wereallowed to clot and thenwere centrifuged for 5 min at 5000 rpm toseparate the serum. Serum samples were stored at the refrigerator(2e8 �C). All samples were well-mixed at room temperature priorto analysis. Each 0.4 mL serum sample was added with 0.4 mLinternal standard and 4 mL 2% nitric acid. The mixture was vortex-mixed and centrifuged for 5 min at 5000 rpm. Serum levels of Se,
Cu, and Zn were determined with an Elan 6100 DRC Plus induc-tively coupled plasma mass spectrometry (Perkin Elmer, Waltham,USA). All the calibrators and samples were placed in the auto-sampler tray. Yttrium was used as internal standard.
2.5. Clinical outcomes
After baseline assessments, all patients were followed for 2years or until death. Patients who received kidney transplantationwere censored at the time of transplantation. Clinical outcomesevaluated were the first episode of infection requiring hospitali-zation and overall mortality. For patients with multiple hospitali-zations for infection, survival analysis in relation to hospitalizationfor infection was limited to the first hospitalization during thefollow-up period. The diagnosis of infectious diseases and thecauses of death were determined by the attending physicians whohad no knowledge of the baseline serum Zn levels. In case of deaththat occurred out of our hospital, family members were inter-viewed by telephone to ascertain the cause and time of death.
2.6. Statistical analysis
Chi-square analysis or Fisher’s exact test was used for compar-ison of categorical variables as appropriate. Continuous variableswere compared by Student’s t-test. Values of the continuous vari-ables are presented as mean and standard deviation, unlessotherwise specified. The Cox proportional hazards model was usedto determine the significance of variables in predicting the primaryend-point. Variables associatedwith clinical outcomes in univariateCox regression analysis with p value less than 0.10 were used formultivariate Cox regression analysis. KaplaneMeier analysis wasused to assess the difference between patients with serum Zn levelsgreater than themedian level (72.2 mg/dL) and those with serum Znlevels less than 72.2 mg/dL in reaching the primary end-point. Thiscomparison was performed by the Log-rank test. The correlationbetween serum Zn and serum albumin was analyzed using linearregression analysis. Because serum levels of albumin and Zn bothreflects nutritional status, we categorized our patients into 4 groupsaccording to their median serum levels of albumin and Zn in orderto further analyze the role of these 2 parameters in the clinicaloutcomes of dialysis patients. We used KaplaneMeier analysis toassess survival differences between these 4 groups. SPSS version15.0 for Windows (SPSS Inc., Chicago, Illinois, USA) was used for allstatistical analyses. All probabilities were two-tailed and a p valueof less than 0.05 was considered statistically significant.
3. Results
3.1. Baseline characteristics of study subjects
Table 1 shows the baseline characteristics of the 111 patientswho were followed for 2 years. Mean age was 58 years, 29% ofpatients were male, and mean duration on dialysis was 6.5 years.Themean serum essential trace element levels were 7.07�2.23 mg/dL (range, 1.48e14.60 mg/dL) for Se, 83.85� 38.14 mg/dL (range,18.59e205.26 mg/dL) for Cu, and 79.26� 33.16 mg/dL (range,16.83e225.71 mg/dL) for Zn, which showed a low normal value ascompared to our institutional reference ranges (7e19 mg/dL for Se,57e125 mg/dL (male) and 61e130 mg/dL (female) for Cu, and61e130 mg/dL for Zn, respectively). A total of 31 patients (28%) haddiabetes mellitus, 82 patients (74%) had hypertension, 26 patients(23%) had hyperlipidemia, 19 patients (17%) had cardiovasculardiseases, and 4 patients (4%) had history of stroke. Compared topatients with serum Zn above themedian value of 72.2 mg/dL, thosewith serum Zn below the medianwere more likely to have diabetes

Table 2Comparison of serum essential trace element levels between dialysis patients(n¼ 111) and healthy subjects (n¼ 67).
Factor Dialysis patients Healthy subjects p Value
Patient number (n) 111 67
Serum levelSelenium (mg/dL) 7.07� 2.23 9.59� 1.32 <0.001Copper (mg/dL) 83.85� 38.14 85.63� 16.48 0.668Zinc (mg/dL) 79.26� 33.16 86.71� 17.19 0.051
Age (year) 58� 15 36� 11 <0.001Male gender (%) 28.8% 64.2% <0.001
Data are expressed as mean� standard deviation.
Table 1Baseline characteristics of dialysis patients with high levels of serum zinc (>72.2 mg/dL) and low levels of serum zinc (�72.2 mg/dL).
Factor Serum zincbelow medianvalue (n¼ 55)
Serum zincabove medianvalue (n¼ 56)
p Value
Serum zinc (mg/dL) 54.3� 13.6 103.8� 28.0 <0.001Age (year) 59� 15 56� 15 0.318Male gender (%) 36.40% 21.40% 0.082Dialysis modality (PD/HD) 60.0%/40.0% 62.5%/37.5% 0.787Dialysis duration (year) 5.8� 5.3 7.1� 5.4 0.194Body mass index (kg/m2) 22.2� 3.5 22.7� 4.5 0.536Smoking index 0.78 0.54 0.292Alcohol index 0.53 0.43 0.549Heavy metal exposure index 1.11 1.11 0.980
ComorbiditiesDiabetes mellitus (%) 43.6 12.5 <0.001Hypertension (%) 76.4 71.4 0.554Hyperlipidemia (%) 18.2 28.6 0.196Cardiovascular disease (%) 21.8 12.5 0.193Prior stroke (%) 3.6 3.6 1.000Malignancy (%) 3.6 7.1 0.679
Nutritional supplementHerbal drug index 3.82 3.88 0.544Multi-vitamin index 3.24 3.16 0.750Vitamin B complex index 2.47 2.52 0.864Folic acid index 2.78 2.93 0.587Vitamin D3 (%) 18.2 16.1 0.768
MedicationsACE inhibitor (%) 25.5 16.1 0.223ARB (%) 40.0 35.7 0.642Statins (%) 9.1 10.7 0.775
Albumin (g/dL) 3.9� 0.3 4.0� 0.3 0.016Calcium (mg/dL) 9.5� 0.6 9.7� 0.9 0.163Phosphate (mg/dL) 4.8� 1.0 5.0� 1.0 0.277Total cholesterol (mg/dL) 184� 38 184� 33 0.984Triglycerides (mg/dL) 180� 104 189� 99 0.621Uric acid (mg/dL) 7.2� 1.3 7.5� 1.6 0.215Bicarbonate (mmol/L) 24.8� 4.2 25.2� 4.8 0.596ALT (U/L) 20.1� 8.0 19.7� 8.7 0.835AST (U/L) 19.6� 8.5 20.0� 8.2 0.813Alk-P (mg/dL) 98.3� 52.6 94.2� 48.5 0.671GGT (mg/dL) 24.6� 25.1 30.5� 41.2 0.361Fasting glucose (mg/dL) 116� 41 101� 24 0.027HbA1c (%) 6.3� 1.2 5.9� 0.9 0.064WBC count (1000 per cumm) 6.96� 2.07 7.30� 1.90 0.376Hemoglobin (g/dL) 10.6� 1.3 10.9� 1.2 0.270Platelet count (1000 per cumm) 217� 79 244� 88 0.094Ferritin (ng/mL) 487.6� 673.8 562.7� 641.3 0.551Transferrin saturation (%) 31.2� 12.8 31.9� 10.6 0.765Intact PTH (pg/mL) 240.4� 316.3 191.8� 203.4 0.341
Data are expressed as mean� standard deviation. Abbreviations: HD, hemodialysis;ACE, angiotensin converting enzyme; ARB, angiotensin receptor blocker; ALT,alanine aminotransferase; AST, aspartate aminotransferase; GGT, g-glutamyl-transpeptidase; Alk-P, alkaline phosphatase; WBC, white blood cell; HbA1c, glyco-sylated hemoglobin; PTH, parathyroid hormone.
C.-Y. Yang et al. / Clinical Nutrition 31 (2012) 630e636632
mellitus (p< 0.001), higher blood glucose (p¼ 0.027), and lowerserum albumin (p¼ 0.016).
3.2. Healthy subjects
The mean serum essential trace element levels of 67 healthysubjects were 9.59�1.32 mg/dL (range, 6.60e13.18 mg/dL) for Se,85.63�16.48 mg/dL (range, 52.35e128.66 mg/dL) for Cu, and86.71�17.19 mg/dL (range, 58.08e136.52 mg/dL) for Zn. Table 2depicts that the serum level of Se was significantly lower(p< 0.001) and Zn was borderline lower (p¼ 0.051) in the dialysispatients than those of the healthy subjects, whereas the serumlevel of Cu was not significantly different between two groups.
3.3. Relationship between serum trace element status and clinicaloutcomes
Table 3 shows the essential trace element status and clinicaloutcomes of our long-term dialysis patients. During the 2 years offollow-up, 37 patients (33%) were hospitalized at least once due toan infectious disease, and 14 patients (13%) died. The averageduration between study entry and first hospitalization due toinfection was 10.8 months, with a range from 0.9 to 21.5 months.The reasons for hospitalization were PD catheter-related infection(12 patients), pneumonia (11 patients), cellulitis or osteomyelitis (8patients), HD access infection (3 patients), biliary tract infection (1patient), polycystic kidney disease cystic infection (1 patient), andurosepsis (1 patient). Causes of death were sepsis (7 patients),cardiovascular events (6 patients), and malignancy (1 patient).Univariate Cox regression analysis indicated that patients withlower serum levels of Se (p¼ 0.026) and Zn (p¼ 0.001) were morelikely to be hospitalized for an infectious disease. In addition, theoverall mortality was higher in patients with lower serum levels ofZn (p¼ 0.038) (Table 3).
3.4. Significant predictors of hospitalization for infection bymultivariate Cox regression analysis
An initial univariate Cox regression analysis of variables signif-icantly associated with hospitalization due to infection (p< 0.10)indicated that dialysis duration, diabetes mellitus, cardiovasculardisease, prior stroke, hypoalbuminemia, hypophosphatemia,hypocholesterolemia, anemia, Se deficiency, and Zn deficiencyincreased this risk. After age, gender, and all these variables wereincluded in amultivariate Cox regression analysis, diabetes mellitus(HR, 2.442 [95% CI, 1.249e4.773], p¼ 0.009), prior stroke (HR, 3.876[95% CI, 1.136e13.221], p¼ 0.030), and Zn deficiency (HR, 0.980[95% CI, 0.967e0.993], p¼ 0.002) were independent predictors ofinfectious diseases requiring hospitalization (Table 4).
3.5. Significant predictors of overall mortality by multivariate Coxregression analysis
As above, an initial univariate Cox regression analysis of vari-ables significantly associated with overall mortality (p< 0.10)indicated that old age, diabetes mellitus, cardiovascular disease,prior stroke, hypoalbuminemia, hypophosphatemia, hypergly-cemia, high glycosylated hemoglobin, and Zn deficiency increasedthis risk. We included gender and all these variables in a multivar-iate Cox regression analysis. The results indicated that old age (HR,1.833 [95% CI, 1.139e2.951] per 10 years, p¼ 0.013), hypo-albuminemia (HR, 0.091 [95% CI, 0.016e0.529], p¼ 0.008), and Zndeficiency (HR, 0.973 [95% CI, 0.948-0.999], p¼ 0.046) were inde-pendent predictors of 2-year mortality (Table 5).

Table 3Univariate Cox regression analysis of essential trace element status and clinical outcomes in dialysis patients.
Factor Hospitalization due to infection 2-Year mortality
HR 95% CI p Value HR 95% CI p Value
Lower Upper Lower Upper
Dialysis modality (HD as reference) 1.406 0.706 2.801 0.332 0.899 0.312 2.591 0.843
Serum levelSelenium (mg/dL) 0.837 0.716 0.979 0.026a 0.878 0.683 1.130 0.314Copper (mg/dL) 0.995 0.986 1.004 0.254 0.995 0.981 1.011 0.555Zinc (mg/dL) 0.980 0.968 0.992 0.001a 0.977 0.956 0.999 0.038a
Age (per 10 years) 1.078 0.864 1.344 0.508 1.699 1.144 2.522 0.009a
Male gender 1.720 0.875 3.384 0.116 2.012 0.698 5.804 0.196Dialysis duration (year) 0.913 0.837 0.996 0.040a 0.895 0.764 1.049 0.172Body mass index (kg/m2) 1.031 0.951 1.118 0.462 1.011 0.879 1.164 0.875Smoking index 1.043 0.817 1.332 0.733 0.833 0.494 1.405 0.493Alcohol index 1.168 0.829 1.647 0.374 1.439 0.882 2.350 0.145Heavy metal exposure index 1.505 0.762 2.973 0.239 0.846 0.190 3.770 0.827
ComorbiditiesDiabetes mellitus (yes/no) 2.867 1.498 5.486 0.001a 6.809 2.133 21.738 0.001a
Hypertension (yes/no) 1.225 0.578 2.596 0.597 2.085 0.466 9.316 0.336Hyperlipidemia (yes/no) 1.309 0.617 2.774 0.483 1.246 0.391 3.975 0.710Cardiovascular disease (yes/no) 2.447 1.207 4.961 0.013a 2.779 0.931 8.297 0.067a
Prior stroke (yes/no) 4.132 1.264 13.510 0.019a 4.300 0.961 19.248 0.056a
Malignancy (yes/no) 0.983 0.236 4.089 0.981 1.401 0.183 10.712 0.745
Nutritional supplementHerbal drug index 0.697 0.423 1.148 0.157 0.772 0.316 1.886 0.570Multi-vitamin index 0.895 0.699 1.145 0.376 0.863 0.585 1.273 0.457Vitamin B complex index 1.134 0.897 1.433 0.293 0.964 0.661 1.407 0.850Folic acid index 1.060 0.841 1.336 0.622 0.942 0.656 1.353 0.747Vitamin D3 (yes/no) 0.530 0.188 1.497 0.231 0.789 0.176 3.524 0.756
MedicationsACE inhibitor (yes/no) 1.303 0.596 2.852 0.507 1.766 0.554 5.636 0.336ARB (yes/no) 1.365 0.715 2.606 0.346 0.894 0.300 2.668 0.841Statins (yes/no) 0.505 0.121 2.100 0.347 0.632 0.083 4.832 0.658
Albumin (g/dL) 0.353 0.130 0.963 0.042a 0.065 0.012 0.348 0.001a
Calcium (mg/dL) 0.962 0.654 1.415 0.844 1.075 0.548 2.111 0.833Phosphate (mg/dL) 0.751 0.535 1.054 0.098a 0.574 0.328 1.002 0.051a
Total cholesterol (mg/dL) 0.991 0.981 1.001 0.069a 0.996 0.981 1.012 0.645Triglycerides (mg/dL) 1.001 0.998 1.004 0.579 1.002 0.998 1.007 0.293Uric acid (mg/dL) 0.900 0.720 1.125 0.356 0.774 0.527 1.139 0.194Bicarbonate (mmol/L) 1.002 0.935 1.073 0.963 1.004 0.895 1.127 0.947ALT (U/L) 0.981 0.940 1.024 0.373 0.942 0.864 1.028 0.179AST (U/L) 0.984 0.942 1.027 0.453 0.981 0.914 1.053 0.599Alk-P (mg/dL) 1.000 0.994 1.007 0.960 1.004 0.995 1.013 0.382GGT (mg/dL) 1.000 0.989 1.012 0.949 1.006 0.994 1.017 0.336Fasting glucose (mg/dL) 1.004 0.995 1.012 0.417 1.012 1.003 1.022 0.013a
HbA1c (%) 1.243 0.952 1.624 0.110 1.564 1.116 2.191 0.009a
WBC count (1000 per cumm) 1.065 0.917 1.238 0.409 0.958 0.726 1.263 0.760Hemoglobin (g/dL) 0.781 0.611 1.000 0.050a 0.827 0.543 1.260 0.377Platelet count (1000 per cumm) 0.997 0.993 1.001 0.153 0.996 0.989 1.004 0.312Ferritin (ng/mL) 1.000 1.000 1.001 0.384 1.000 1.000 1.001 0.411Transferrin saturation (%) 1.002 0.976 1.030 0.868 0.986 0.938 1.035 0.565Intact PTH (pg/mL) 0.999 0.998 1.001 0.414 1.001 0.999 1.002 0.393
Data are expressed as mean� standard deviation. Abbreviations: HR, hazard ratio; CI, confidence interval; HD, hemodialysis; ACE, angiotensin converting enzyme; ARB,angiotensin receptor blocker; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, g-glutamyltranspeptidase; Alk-P, alkaline phosphatase;WBC, white bloodcell; HbA1c, glycosylated hemoglobin; PTH, parathyroid hormone.
a p< 0.10.
C.-Y. Yang et al. / Clinical Nutrition 31 (2012) 630e636 633
3.6. Lower serum Zn levels associated with hospitalization forinfection and overall mortality
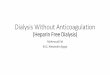
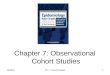
KaplaneMeier estimates show a significantly greater event-freesurvival probability for hospitalization due to infection for patientswith serum Zn greater than 72.2 mg/dL (median value) than forthosewith concentrations less than 72.2 mg/dL (p¼ 0.001; Log-ranktest) (Fig. 1). In addition, patients with serum Zn greater than72.2 mg/dL had a significantly higher overall survival probabilitythan those with concentrations less than 72.2 mg/dL (p¼ 0.027;Log-rank test) (Fig. 2).
3.7. Dialysis patients with both hypoalbuminemia and Zndeficiency were at risk for hospitalization for infection and overallmortality
Finally, we examined the relationship between serum levels ofZn and albumin at patient enrollment. Interestingly, serum Znwas weakly but positively correlated with serum albumin(r¼ 0.204, p¼ 0.032). Furthermore, as mentioned previously, Zn-deficient patients had a significantly higher percentage of hypo-albuminemia than those with high serum Zn level (p¼ 0.016)(Table 3). The median value of serum albumin in our patients was

Table 4Multivariate Cox regression analysis of significant predictors of 2-year hospitaliza-tion due to infection in dialysis patients.a
Factor HR 95% CI p Value
Lower Upper
Diabetes mellitus 2.442 1.249 4.773 0.009Prior stroke 3.876 1.136 13.221 0.030Serum zinc (mg/dL) 0.980 0.967 0.993 0.002
a The model consists age, gender, and variables with p value less than 0.10 inunivariate Cox regression analysis, including dialysis duration, diabetes mellitus,cardiovascular disease, prior stroke, albumin, phosphate, total cholesterol, hemo-globin, selenium, and zinc. Abbreviations: HR, hazard ratio; CI, confidence interval.
Fig. 1. Two-year KaplaneMeier estimate of event-free survival probability for hospi-talization due to infectious diseases in dialysis patients with high levels of serum zinc(>72.2 mg/dL) and low levels of serum zinc (�72.2 mg/dL) (p¼ 0.001; Log-rank test).
C.-Y. Yang et al. / Clinical Nutrition 31 (2012) 630e636634
3.9 g/dL, so patients were categorized as those with albumin above3.9 g/dL and Zn above 72.2 mg/dL (n¼ 32), those with albuminbelow 3.9 g/dL and Zn above 72.2 mg/dL (n¼ 24), those withalbumin above 3.9 g/dL and Zn below 72.2 mg/dL (n¼ 23), and thosewith albumin below 3.9 g/dL and Zn below 72.2 mg/dL (n¼ 32).
KaplaneMeier estimates of event-free survival probability forhospitalization due to infection indicate that patients with bothhypoalbuminemia and Zn deficiency had the worst prognosis, ascompared to those with hypoalbuminemia but normal/high level ofZn (p¼ 0.024; Log-rank test) and those with neither hypo-albuminemia nor Zn deficiency (p< 0.001; Log-rank test) (Fig. 3).As to overall survival probability, KaplaneMeier estimates alsoshow that patients with both hypoalbuminemia and Zn deficiencywere at the greatest risk for mortality, as compared to those withneither hypoalbuminemia nor Zn deficiency (p¼ 0.002; Log-ranktest) (Fig. 4).
4. Discussion
The results of the present study indicate that low levels of serumZn in long-term dialysis patients, but not Se and Cu, is an inde-pendent predictor of future hospitalization for infectious diseaseand for overall mortality. Our data showed that for each 1 mg/dLdecrease in serum level of Zn, there were a 2.0% risk increase inhospitalization for infection and a 2.8% risk increase in mortalityduring the two years of follow-up. Although our study populationwas composed of HD and PD patients, there were no differences inhospitalization for infection and overall mortality between twotreatment modalities (Table 3).
This study further supports the previous reports that Zn defi-ciency is a parameter of malnutrition in dialysis patients.17,18 Inaddition, serum levels of Zn and albumin were found to be inde-pendent predictors of overall survival in dialysis patients. Patientswith both hypoalbuminemia and Zn deficiency were at the greatestrisk for hospitalization for infection and mortality, as comparedwith those with neither hypoalbuminemia nor Zn deficiency.Therefore, serum Zn, combined with albumin, could be used asparameters for the analysis of overall nutritional status of long-
Table 5Multivariate Cox regression analysis of significant predictors of 2-year mortality indialysis patients.a
Factor HR 95% CI p Value
Lower Upper
Age (per 10 years) 1.833 1.139 2.951 0.013Albumin (g/dL) 0.091 0.016 0.529 0.008Serum zinc (mg/dL) 0.973 0.948 0.999 0.046
a The model consists gender and variables with p value less than 0.10 inunivariate Cox regression analysis, including age, diabetes mellitus, cardiovasculardisease, prior stroke, albumin, phosphate, fasting glucose, glycosylated hemoglobin,and zinc. Abbreviations: HR, hazard ratio; CI, confidence interval.
term dialysis patients. This study further underscores the factthat malnutrition is a significant predictor of morbidity andmortality in patients receiving maintenance dialysis.
A multicenter cross-sectional study showed that HD patientswith infections complications had lower serum levels of Zn.16 Ourprospective study further adjusted for various clinical parametersand clearly demonstrated the independently predictive value of Znlevels on future infectious diseases in dialysis patients. This findingwas supported by other reports which suggested that zinc defi-ciency leads to poor immunity in dialysis patients.5e9,13,14
Furthermore, our multivariate Cox regression analysis indicatedthat dialysis patients with serum levels of Zn below 72.2 mg/dLweremore likely to suffer from an infectious disease that requiredhospitalization and had a higher mortality rate. In addition, wefound that Zn deficiency is more prevalent in dialysis patients withdiabetes. This suggests that not only should serum Zn bemonitoredin long-term dialysis patients, patients with low serum Zn shouldbe more aggressively monitored, particularly if they have diabetes.Our study offers a reference value of serum Zn in association withadverse clinical outcomes in dialysis patients.
The effect of supplemental Zn on the clinical outcomes of long-term dialysis patients is not performed in this study, which will bean important issue to investigate in future studies. To the best of ourknowledge, there was no interventional study of zinc supplementon patient outcomes performed in the dialysis population. Never-theless, there was an interventional study of Zn supplementationshowing its survival benefits in cancer patients, in which a daily
Fig. 2. Two-year KaplaneMeier estimate of overall survival probability of dialysispatients with high levels of serum zinc (>72.2 mg/dL) and low levels of serum zinc(�72.2 mg/dL) (p¼ 0.027; Log-rank test).

Fig. 3. Dialysis patients with both hypoalbuminemia and zinc deficiency were at thehighest risk for an infectious disease requiring hospitalization, as compared to hypo-albuminemic patients without zinc deficiency (p¼ 0.024; Log-rank test) and patientswithout hypoalbuminemia and zinc deficiency (p< 0.001; Log-rank test).
C.-Y. Yang et al. / Clinical Nutrition 31 (2012) 630e636 635
dose of 25 mg Zn was used.19 On the other hand, the dosage of Znwas 220 mg per day in a study which demonstrated that Znsupplementation decreases serum CRP in dialysis patients.15
However, the Zn ingredient of multivitamin is around 10 mg pertablet, which is lower than the dose used in the above two studies.Therefore, though a proportion of our patients had taken multivi-tamin, we could not assure its clinical significance on patientoutcomes.
There are some limitations of our study that need considering.First, there are only 3 common essential trace elements that wereused as parameters in this study. Other clinically relevant essentialtrace element such as cobalt (Co) was not included, but Co wasmainly associated with erythropoiesis and there was no evidenceshowing its influences on outcomes in the general population.Second, the enrolled healthy controls were not age-matched.However, the correlation between Zn and aging remains contro-versial.20 Although aging might influence serum levels of Zn,21e23
Fig. 4. Dialysis patients with both hypoalbuminemia and zinc deficiency were at thehighest risk for overall mortality, as compared to patients without hypoalbuminemiaand zinc deficiency (p¼ 0.002; Log-rank test).
there were also numerous evidences showing that Zn levels weresimilar among healthy subjects with different ages.20,24e27 Third,the sample size of our study was relatively small. Nevertheless, thepresent study clearly points out the significance of serum Zn level.
In conclusion, this study found that low serum level of Zn inlong-term dialysis patients was associated with a higher risk ofhospitalization due to infection and overall mortality within twoyears of follow-up. Serum Zn, in addition to serum albumin, can beconsidered to reflect the overall nutritional status of long-termdialysis patients.
Statement of authorship
All authors have made substantial contributions and finalapproval of the conceptions, drafting, and final version. Authorcontributions: Yang C, Wu M, and Ng Y designed research; Yang C,Wu M, Chou Y, Li S, Deng J, Yang W, and Ng Y performed research;Yang C, Li S, and Ng Y analyzed data; and Yang C, Wu M, and Ng Ywrote the paper. All authors read and approved the finalmanuscript.
Conflict of interest
All authors declare no conflict of interest.
Acknowledgments
This study is supported by the grant from Taipei VeteransGeneral Hospital, Taipei, Taiwan (VGH97-07-30A, V98C1-106). Theauthors thank the physicians and nurses for technical assistance,Dr. Sandy Cho for providing valuable suggestions and Englishcorrection, and laboratory staffs for excellent laboratory skills.
References
1. Covic A, Gusbeth-Tatomir P. Trace elements in end-stage renal disease e
unfamiliar territory to be revealed. BMC Nephrol 2009;10:12.2. Rucker D, Thadhani R, Tonelli M. Trace element status in hemodialysis patients.
Semin Dial 2010 Jun 14.3. Tonelli M, Wiebe N, Hemmelgarn B, Klarenbach S, Field C, Manns B, et al. Trace
elements in hemodialysis patients: a systematic review and meta-analysis.BMC Med 2009;7:25.
4. Vanholder R, Cornelis R, Dhondt A, Lameire N. The role of trace elements inuraemic toxicity. Nephrol Dial Transplant 2002;17(Suppl. 2):2e8.
5. Briggs WA, Pedersen MM, Mahajan SK, Sillix DH, Prasad AS, McDonald FD.Lymphocyte and granulocyte function in zinc-treated and zinc-deficienthemodialysis patients. Kidney Int 1982 Jun;21(6):827e32.
6. Bozalioglu S, Ozkan Y, Turan M, Simsek B. Prevalence of zinc deficiency andimmune response in short-term hemodialysis. J Trace Elem Med Biol2005;18(3):243e9.
7. Dvornik S, Cuk M, Racki S, Zaputovic L. Serum zinc concentrations in themaintenance hemodialysis patients. Coll Antropol 2006 Mar;30(1):125e9.
8. Ribeiro RC, Sales VS, Neves FA, Draibe S, Brandao-Neto J. Effects of zinc on cell-mediated immunity in chronic hemodialysis patients. Biol Trace Elem Res 2004Jun;98(3):209e18.
9. Richard MJ, Ducros V, Foret M, Arnaud J, Coudray C, Fusselier M, et al. Reversalof selenium and zinc deficiencies in chronic hemodialysis patients by intra-venous sodium selenite and zinc gluconate supplementation. Time-course ofglutathione peroxidase repletion and lipid peroxidation decrease. Biol TraceElem Res 1993 Nov;39(2e3):149e59.
10. Turan B, Delilbasi E, Dalay N, Sert S, Afrasyap L, Sayal A. Serum selenium andglutathione-peroxidase activities and their interaction with toxic metals indialysis and renal transplantation patients. Biol Trace Elem Res 1992Apr;33:95e102.
11. Zachara BA, Adamowicz A, Trafikowska U, Trafikowska A, Manitius J,Nartowicz E. Selenium and glutathione levels, and glutathione peroxidaseactivities in blood components of uremic patients on hemodialysis supple-mented with selenium and treated with erythropoietin. J Trace Elem Med Biol2001;15(4):201e8.
12. Adamowicz A, Trafikowska U, Trafikowska A, Zachara B, Manitius J. Effect oferythropoietin therapy and selenium supplementation on selected antioxidantparameters in blood of uremic patients on long-term hemodialysis. Med SciMonit 2002 Mar;8(3):CR202e5.

C.-Y. Yang et al. / Clinical Nutrition 31 (2012) 630e636636
13. Allen JI, Korchik W, Kay NE, McClain CJ. Zinc and T-lymphocyte function inhemodialysis patients. Am J Clin Nutr 1982 Sep;36(3):410e5.
14. Guo CH, Wang CL, Chen PC, Yang TC. Linkage of some trace elements,peripheral blood lymphocytes, inflammation, and oxidative stress inpatients undergoing either hemodialysis or peritoneal dialysis. Perit Dial Int2010 Jun 30.
15. Rashidi AA, Salehi M, Piroozmand A, Sagheb MM. Effects of zinc supplemen-tation on serum zinc and C-reactive protein concentrations in hemodialysispatients. J Ren Nutr 2009 Nov;19(6):475e8.
16. Skarupskiene I, Kuzminskis V, Abdrachmanovas O, Ryselis S, Smalinskiene A.Zinc and aluminum concentrations in blood of hemodialysis patients and itsimpact on the frequency of infections. Medicina (Kaunas) 2005;41(Suppl.1):65e8.
17. Chevalier CA, Liepa G, Murphy MD, Suneson J, Vanbeber AD, Gorman MA, et al.The effects of zinc supplementation on serum zinc and cholesterol concen-trations in hemodialysis patients. J Ren Nutr 2002 Jul;12(3):183e9.
18. Mahajan SK, Prasad AS, Rabbani P, Briggs WA, McDonald FD. Zinc deficiency:a reversible complication of uremia. Am J Clin Nutr 1982 Dec;36(6):1177e83.
19. Lin YS, Lin LC, Lin SW. Effects of zinc supplementation on the survival ofpatients who received concomitant chemotherapy and radiotherapy foradvanced nasopharyngeal carcinoma: follow-up of a double-blind randomizedstudy with subgroup analysis. Laryngoscope 2009 Jul;119(7):1348e52.
20. Savarino L, Granchi D, Ciapetti G, Cenni E, Ravaglia G, Forti P, et al. Serumconcentrations of zinc and selenium in elderly people: results in healthynonagenarians/centenarians. Exp Gerontol 2001 Feb;36(2):327e39.
21. Mariani E, Cornacchiola V, Polidori MC, Mangialasche F, Malavolta M,Cecchetti R, et al. Antioxidant enzyme activities in healthy old subjects:influence of age, gender and zinc status: results from the Zincage Project.Biogerontology 2006 Oct;7(5-6):391e8.
22. Sfar S, Jawed A, Braham H, Amor S, Laporte F, Kerkeni A. Zinc, copper andantioxidant enzyme activities in healthy elderly Tunisian subjects. Exp Gerontol2009 Dec;44(12):812e7.
23. Maes M, DeVos N, Wauters A, Demedts P, Maurits VW, Neels H, et al. Inflam-matory markers in younger vs elderly normal volunteers and in patients withAlzheimer’s disease. J Psychiatr Res 1999 Sep;33(5):397e405.
24. Licastro F, Chiricolo M, Morini MC, Capri I, Davis LJ, Conte R, et al. Influence ofage and health on immune functions and trace elements. Gerontology1995;41(4):235e41.
25. Galan P, Viteri FE, Bertrais S, Czernichow S, Faure H, Arnaud J, et al. Serumconcentrations of beta-carotene, vitamins C and E, zinc and selenium areinfluenced by sex, age, diet, smoking status, alcohol consumption and corpu-lence in a general French adult population. Eur J Clin Nutr 2005Oct;59(10):1181e90.
26. Rukgauer M, Klein J, Kruse-Jarres JD. Reference values for the trace elementscopper, manganese, selenium, and zinc in the serum/plasma of children,adolescents, and adults. J Trace Elem Med Biol 1997 Jun;11(2):92e8.
27. Andriollo-Sanchez M, Hininger-Favier I, Meunier N, Toti E, Zaccaria M,Brandolini-Bunlon M, et al. Zinc intake and status in middle-aged and olderEuropean subjects: the ZENITH study. Eur J Clin Nutr 2005 Nov;59(Suppl.2):S37e41.