Embed Size (px)
Citation preview

thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
1
open access
1National Centre for Epidemiology Carlos III Institute of Health Madrid Spain2Consortium for Biomedical Research in Epidemiology and Public Health (CIBERESP) Madrid Spain3Department of Preventive Medicine and Public Health Faculty of Medicine Complutense University Madrid Spain4National School of Public Health Carlos III Institute of Health 28029 Madrid Spain5National Drug and Alcohol Research Centre University of New South Wales Sidney Australia6Melbourne School of Population and Global Health University of Melbourne Melbourne Australia7Sector Best Practices Knowledge Exchange and Economic Issues European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Lisbon PortugalCorrespondence to G Barrio gbarrioisciiiesAdditional material is published online only To view please visit the journal onlineCite this as BMJ 2017357j1550httpdxdoiorg101136bmjj1550
Accepted 17 March 2017
Mortality risk during and after opioid substitution treatment systematic review and meta-analysis of cohort studiesLuis Sordo123 Gregorio Barrio4 Maria J Bravo12 B Iciar Indave12 Louisa Degenhardt56 Lucas Wiessing7 Marica Ferri7 Roberto Pastor-Barriuso12
ABSTRACTObjeCtiveTo compare the risk for all cause and overdose mortality in people with opioid dependence during and after substitution treatment with methadone or buprenorphine and to characterise trends in risk of mortality after initiation and cessation of treatmentDesignSystematic review and meta-analysisData sOurCesMedline Embase PsycINFO and LILACS to September 2016stuDy seleCtiOnProspective or retrospective cohort studies in people with opioid dependence that reported deaths from all causes or overdose during follow-up periods in and out of opioid substitution treatment with methadone or buprenorphineData extraCtiOn anD synthesisTwo independent reviewers performed data extraction and assessed study quality Mortality rates in and out of treatment were jointly combined across methadone or buprenorphine cohorts by using multivariate random effects meta-analysisresultsThere were 19 eligible cohorts following 122 885 people treated with methadone over 13-139 years and 15 831 people treated with buprenorphine over 11-45 years Pooled all cause mortality rates were 113 and 361 per 1000 person years in and out of methadone treatment (unadjusted out-to-in rate ratio 320 95 confidence interval 265 to 386) and reduced to 43 and 95 in and
out of buprenorphine treatment (220 134 to 361) In pooled trend analysis all cause mortality dropped sharply over the first four weeks of methadone treatment and decreased gradually two weeks after leaving treatment All cause mortality remained stable during induction and remaining time on buprenorphine treatment Overdose mortality evolved similarly with pooled overdose mortality rates of 26 and 127 per 1000 person years in and out of methadone treatment (unadjusted out-to-in rate ratio 480 290 to 796) and 14 and 46 in and out of buprenorphine treatmentCOnClusiOnsRetention in methadone and buprenorphine treatment is associated with substantial reductions in the risk for all cause and overdose mortality in people dependent on opioids The induction phase onto methadone treatment and the time immediately after leaving treatment with both drugs are periods of particularly increased mortality risk which should be dealt with by both public health and clinical strategies to mitigate such risk These findings are potentially important but further research must be conducted to properly account for potential confounding and selection bias in comparisons of mortality risk between opioid substitution treatments as well as throughout periods in and out of each treatment
IntroductionOpioid dependence is a rising drug use disorder with substantial contribution to the global disease burden The absolute number (age standardised prevalence) of people with opioid dependence worldwide increased from 104 million (020) in 1990 to 155 million (022) in 2010 and the disability adjusted years of life lost attributable to opioid dependence rose from 53 million (021 of global disease burden) in 1990 to 92 million (037) in 20101
Opioid substitution treatment either with metha-done or buprenorphine has been shown to be safe and effective in suppressing illicit opioid use2 3 improving physical and mental wellbeing4 5 and reducing all cause and overdose mortality6 Growing evidence however suggests that mortality experience during and after opioid substitution treatment is time varying and differs by type of drug6-10 Methadone a full opioid agonist might pose an excess risk of death from overdose during treatment induction if initial doses are too high or coexist with illicit opioid use6 7 10 Buprenorphine a partial agonist is less effective in retaining patients in treatment3 which seems a major weakness because mortality increases significantly in the period immediately after treatment stops10 11 Nev-ertheless studies of individual cohorts have generally
WhAT IS AlReAdy knoWn on ThIS TopICOpioid substitution treatment is effective in suppressing illicit opioid use and reducing all cause and overdose mortalityGrowing evidence suggests that mortality during and after opioid substitution treatment is time varying and differs by type of drug
WhAT ThIS STudy AddSIn patients using methadone maintenance treatment there are on average 25 fewer deaths1000 person years than in patients who discontinue it Mortality risk among opioid users during treatment is less than a third of that expected in the absence of opioid substitution treatmentBuprenorphine maintenance treatment is probably also effective in reducing mortality in opioid users but quantification of averted deaths requires further studiesThe mortality risk in the induction phase of methadone (first four weeks) is high but seems to decreases substantially during this period with a further stabilisation at around six deaths1000 person years in the remaining time in treatment This did not occur with buprenorphine The mortality risk in the four weeks immediately after cessation of either treatment is high and could exceed 30 deaths1000 person years
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
2
been under-powered to detect potential differences in mortality risk by time interval in and out of treatment and long term large trials comparing the effect of methadone and buprenorphine on all cause and over-dose mortality are hardly feasible3 In this context a systematic review of cohort studies can provide valu-able evidence on the mortality experience of opioid dependent people at different periods of methadone and buprenorphine substitution treatment that could guide clinicians and policymakers in the optimal pro-vision of treatment12
In this systematic review and meta-analysis we syn-thesised results from cohort studies on mortality among patients receiving opioid substitution treatment to obtain pooled estimates of all cause and overdose mor-tality rates during periods in and out of treatment with methadone and buprenorphine evaluate heterogeneity of mortality rates across cohort characteristics and investigate changes in mortality rates over time in and out of treatment particularly within the first weeks after treatment initiation and cessation
Methodssearch strategy and inclusion criteriaWe searched Medline Embase PsycINFO and LILACS by using different combinations of free text and data-base specific index terms related to the topics of opioid dependence opioid substitution treatment mortality and cohort studies Details of the full search strategy are provided in appendix 1 The search was updated to September 2016 with no language restrictions We also searched the Cochrane Database of Systematic Reviews reviewed the reference lists of relevant original papers and reviews screened articles in the PubMed ldquorelated citationsrdquo section searched online for technical reports and monographs and consulted experts and investiga-tors with ongoing studies in opioid dependence We followed the PRISMA statement for reporting system-atic reviews and meta-analyses13
We included cohort studies comparing mortality among people with opioid dependence To be eligible studies had to include follow-up data during and after opioid substitution treatment with methadone or buprenorphine The prespecified exclusion criteria were as follows
bull No data in humansbull No original research (reviews editorials non-re-
search letters protocols)bull Study design other than observational cohort (clini-
cal trials case-control studies cross sectional sur-veys case reports case series qualitative research)
bull Study not focused on people with opioid dependence bull People in prison or recently releasedbull Treatment unknown or other than methadone or
buprenorphine maintenance (methadone detoxifica-tion opioid antagonist therapy therapeutic community)
bull No all cause or overdose mortality as outcome or no deaths over follow-up
bull Insufficient data to compute mortality rates during periods in and out of treatment (number of deaths
and person years broken down by follow-up period in and out of treatment)
For cohorts originating several reports we used data from non-overlapping follow-up periods from each report whenever possible or selected the publication with the longest follow-up
study selection and data extractionTwo investigators independently reviewed the titles and abstracts identified in the search and retrieved articles to determine eligibility and to extract study data Dis-agreements or uncertainties were resolved by consen-sus with an additional investigator
For each eligible study we retrieved information on baseline population characteristics including study location sex and age distribution primary opioid of misuse and prevalence of opioid injection non-opi-oid drug use HIV infection and psychiatric and med-ical comorbidity number of cohort participants entering opioid substitution treatment during the study period (untreated participants and those under other types of treatment were excluded) treatment features including drug type (methadone or buprenor-phine) average daily dose induction method (inpa-tient or ambulatory) and provider (addiction medicine specialist or general practitioner) and main follow-up characteristics including calendar period average length of follow-up from the start of mainte-nance treatment (excluding any previous detoxifica-tion period) loss to follow-up and mortality outcomes We also registered detailed information on the number of deaths person years at risk and mor-tality rates from all causes and overdose during fol-low-up periods in and out of treatment and whenever possible during specific time intervals since treat-ment initiation and cessation Finally we registered information on first and subsequent treatment epi-sodes (table A in appendix 2) and on completeness of treatment (table B in appendix 2)
We specifically designed a quality assessment form based on standardised and extensively used instru-ments the methodology checklist for cohort studies developed by the Scottish Intercollegiate Guidelines Network14 and the checklist for drug related studies developed by the National Drug and Alcohol Research Centre Australia15 The design process based on a thor-ough review of the above sources included the develop-ment of different proposals discussion of their appropriateness and final agreement among the authors The final version comprised separate sections according to the study design and was based on a ldquostar systemrdquo score approach16 including a general appraisal of external and internal validity and of the biases rele-vant to cohort studies plus an ad hoc assessment of reporting for studies on mortality during and after opi-oid substitution treatment (appendix 3)
statistical analysisFor each selected cohort we calculated crude mortality rates from all causes and overdose during periods in
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
3
and out of treatment by dividing the number of deaths registered in each period by the person years contrib-uted by all participants to that period If not explicitly reported we derived the number of person years by treatment period from the available summary statistics on follow-up and treatment retention or the reported mortality rates We computed exact 95 confidence intervals for the underlying mortality rates by assuming a Poisson distribution for the observed number of deaths and fixed person years at risk
Cause specific mortality rates in and out of treatment were jointly combined across all methadone or buprenorphine cohorts by using a bivariate random effects meta-analysis on log transformed mortality rates in both treatment periods17-19 This bivariate meta-ana-lytic approach allowed estimation of not only the pooled mortality rates and 95 confidence intervals in and out of treatment but also the pooled rate difference and rate ratio comparing periods out of and in treatment with confidence intervals that took into account the correlation between rates in both treatment periods
To evaluate whether cause specific mortality rates differed by baseline population characteristics treat-ment delivery and follow-up features of methadone cohorts we included the location (EuropeIsrael North America or Australia) prevalence of opioid injection (lt100 or 100) percentage of men (lt75 or ge75) mean age (lt35 or ge35) average methadone dose (le80 or gt80 mgday) percentage of inpatient induction (0 or gt0) treatment provider (specialist or general practitionermixed) midpoint follow-up period (lt2000 or ge2000) and percentage loss to follow-up (lt10 or ge10) in each methadone cohort as single predictors in separate bivariate random effects meta-regression models on log transformed mortality rates in and out of treatment17 18 We contrasted heterogeneity of pooled mortality rates by these cohort characteristics through likelihood ratio tests comparing nested meta-regression models with and without the predictor fitted through maximum like-lihood The limited number of buprenorphine cohorts precluded a similar heterogeneity analysis across these cohorts
For methadone or buprenorphine cohorts that reported mortality data by time interval in and out of treatment we combined cause specific mortality rates before and after four weeks of treatment initiation and cessation through a multivariate random effects meta-analysis on log transformed mortality rates in these time-by-treatment intervals To obtain pooled trends in all cause mortality risk over time in and out of methadone substitution treatment we fitted a bivariate random effects meta-regression of log transformed rates on a quadratic linear spline function of log time with knot at four weeks20 This quadratic linear spline allowed for a quadratic trend in the first four weeks in and out of treatment and forced the trend to be linear thereafter to avoid implausible shapes at long follow-up times The resulting pooled trends were virtually insensitive to different knot locations at three four or five weeks
We examined the overall heterogeneity in mortality rates across studies as well as the residual heterogene-ity beyond that explained by study level characteristics with the multivariate extension of the Cochran χ2 test and quantified it with the extended I2 statistic18 21 which described the proportion of total variation in study specific mortality rates because of heterogeneity The influence of each study on pooled estimates was evaluated by removal of each individual study from the analysis Publication bias and genuine small study effects were assessed with the extended Egger test allowing for heterogeneity22 23
In all the above multivariate random effects meta-an-alytic models we assumed the correlations within cohorts in the estimated mortality rates to be zero as they were obtained over different follow-up periods in and out of treatment Nevertheless we performed sen-sitivity analyses assuming positive within cohort cor-relations between mortality rates in and out of treatment of 025 050 075 and 095 for all studies and the pooled rates and their standard errors were virtually identical to those obtained under uncorrelated rates within cohorts (changes of minus13 to 16 in pooled rates and minus57 to 76 in standard errors) All models were fitted through restricted maximum likelihood methods with unstructured between cohort covariance matrix with the R package mvmeta (R Foundation for Statistical Computing) The estimated between cohort correlations in the underlying rates in and out of treat-ment were 093 for all cause mortality and 081 for over-dose mortality with no estimation problems in any model regarding between cohort correlations at the boundary of the parameter space of 1
Patient involvementNo patients were involved in setting the research ques-tion or outcome measures nor were they involved in developing plans for design or implementation of the study No patients were asked to advise on interpreta-tion or writing up on results There are no plans to disseminate the results of the research to study partici-pants or the relevant patient community
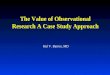
Resultsstudy characteristicsOf the 2033 distinct records identified through the search we selected 19 cohort studies reported in 20 arti-cles6-10 24-38 (two articles27 28 reported different mortality outcomes from the same cohort) that met the inclusion criteria and provided mortality data in people with opi-oid dependence during and after opioid substitution treatment (fig 1 ) Tables 1 and 2 show the main charac-teristics of selected cohorts The studies were published between 1974 and 2016 and were all carried out in high income countries 11 in EuropeIsrael four in North America and four in Australia There were mixed base-line prevalences of opioid injection and HIV infection except four cohorts that enrolled only opioid injectors two of them further restricted to patients positive for HIV All but four cohorts included patients with concur-rent use of non-opioid drugs with limited information
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
4
on psychiatric and medical comorbidities More than 70 of participants were men and the mean age at baseline ranged from 234 to 396 (table 1)
Methadone was prescribed in 18 cohorts including 122 885 participants over the period 1965-2010 and buprenorphine was used in three cohorts including 15 831 participants over 1990-2010 (table 2) The average daily dose ranged from 47 mg to 116 mg of methadone and 10 mg to 12 mg of buprenorphine Treatment was initiated on an ambulatory basis in all recent cohorts and provided by addiction medicine specialists in 11 cohorts and general practitioners or mixed staff in eight cohorts The average follow-up after initiation varied between 13 and 139 years for methadone and 11 and 45 years for buprenorphine with loss to follow-up exceeding 10 in only four cohorts All cause mortality during follow-up periods in and out of treatment was reported in all but two methadone cohorts and over-dose mortality in 11 methadone cohorts and one buprenorphine cohort Most studies were of moderate quality They ranged from 3 to 13 points on a 16 point scale with a median of 8 points
all cause mortality during and after opioid substitution treatmentAll cause mortality rates varied widely across the 16 methadone cohorts (overall I2=98 Plt0001) although rates were consistently higher out of treatment than in treatment (fig 2 ) The pooled all cause mortality rates were 113 and 361 deaths per 1000 person years in and out of methadone treatment respectively with an unadjusted pooled rate difference for periods out and in treatment of 249 deaths (95 confidence interval 136 to 361) per 1000 person years and an unadjusted pooled rate ratio of 320 (265 to 386) In heterogeneity analyses (table 3) the pooled all cause mortality rates in and out of methadone treatment were significantly higher in studies that mostly enrolled opioid injectors who were positive for HIV than in studies including
both injectors and non-injectors and marginally higher in studies conducted in Europe and North America than in Australia
The pooled all cause mortality rates in the three buprenorphine cohorts were 43 and 95 deaths per 1000 person years in and out of treatment respectively (fig 2) The unadjusted pooled rate difference for peri-ods out and in treatment was 52 deaths (95 confi-dence interval minus10 to 114) per 1000 person years and the unadjusted pooled rate ratio was 220 (134 to 361)
After we removed each individual cohort the pooled all cause mortality rates ranged from 106 to 119 deaths per 1000 person years in methadone treatment and from 325 to 391 deaths per 1000 person years out of methadone treatment With buprenorphine treatment these figures were 33 to 56 deaths and 77 to 123 deaths per 1000 person years respectively There was some evidence of small study effects on all cause mortality (P=005) with higher rates in small cohorts that mostly enrolled opioid injectors who were positive for HIV (table 1 and fig 2)
Five methadone cohorts and one buprenorphine cohort reported all cause mortality rate ratios for peri-ods out of and in treatment with various degrees of adjustment for patient demographics severity of drug use treatment delivery and comorbidity (table 4) After adjustment out-to-in rate ratios remained unchanged in two methadone cohorts and increased by 155-355 in the other three methadone cohorts and by 168 in the buprenorphine cohort
Overdose mortality during and after opioid substitution treatmentThe pooled overdose mortality rates across the 11 meth-adone cohorts were 26 and 127 overdose deaths per 1000 person years in and out of methadone treatment respectively (fig 3) with an unadjusted pooled rate dif-ference comparing periods out and in treatment of 100 overdose deaths (95 confidence interval 26 to 174) per 1000 person years and an unadjusted pooled rate ratio of 480 (290 to 796) There was moderate heterogeneity between studies in mortality rates in treatment (I2=66 P=0001) and strong heterogeneity in rates out of treat-ment (I2=97 Plt0001) with significantly higher rates out of treatment among methadone patients in specialist services than in primary care (table 3 ) In the single buprenorphine cohort there were 14 and 46 fatal overdoses per 1000 person years in and out of treatment (fig 3)
After we removed each methadone cohort the pooled overdose mortality rates varied between 24 and 28 fatal overdoses per 1000 person years in methadone treatment and between 106 and 149 fatal overdoses per 1000 person years out of treatment There was no evi-dence of publication bias or other small study effects on overdose mortality (P=014) Adjustment for potential confounders did not produce any change in overdose mortality rate ratios for periods out compared with in treatment in three methadone cohorts but resulted in 258 and 286 larger rate ratios in two other metha-done cohorts (table 4)
Distinct records identied (n=2033) Medline (n=1215) Embase (n=729) PsycINFO (n=486)
Full text articles retrieved and assessed for eligibility (n=328)
Articles included in meta-analysis (n=20)
LILACS (n=182)Other searches (n=102)
Records excluded aer title and abstract review (n=1705) No data in humans (n=120) No original research (n=126) Design other than observational cohort (n=462) Not focused on opioid dependent people (n=997)
Articles excluded (n=308) Imprisoned or recently released population (n=22) Treatment unknown or other than methadone or buprenorphine maintenance (n=133) No all cause or overdose mortality as outcome (n=44) Insucient data to compute mortality rates during follow-up periods in and out of treatment (n=72) Secondary publication (n=37)
Fig 1 | selection process of cohort studies on mortality among people receiving opioid substitution treatment
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
5
all cause mortality by time interval in and out of treatmentSix recent methadone cohorts provided all cause mortal-ity data disaggregated by time interval in and out of treat-ment (fig 4) After we excluded a selective high risk cohort of injectors who were HIV positive and received highly active antiretroviral therapy the pooled all cause mortal-ity rates were 114 and 58 deaths per 1000 person years in the first four weeks and the remaining time on metha-done treatment respectively with an unadjusted pooled rate difference for initial compared with subsequent treat-ment periods of 56 deaths (95 confidence interval minus24 to 136) per 1000 person years and an unadjusted pooled rate ratio of 197 (094 to 410) Similarly the pooled all cause mortality dropped from 321 deaths per 1000 person years in the first four weeks after stopping methadone treatment to 135 deaths per 1000 person years thereafter resulting in an unadjusted pooled rate difference for ini-tial compared with subsequent periods out of treatment of 186 deaths (29 to 343) per 1000 person years and an unadjusted pooled rate ratio of 238 (151 to 374)
In continuous time trend analysis (fig 5) there were significant departures from linearity in trends in all cause mortality risk over time in and out of methadone treatment (P=004) The pooled all cause mortality rates decreased sharply from 374 to 64 deaths per 1000 per-son years throughout the initial four weeks of metha-done treatment and were fairly stable thereafter In contrast after people left methadone treatment the pooled all cause mortality remained high at between 241 and 352 deaths per 1000 person years during the initial two weeks out of treatment and decreased pro-gressively afterwards
In the two buprenorphine cohorts reporting disaggre-gated data the pooled all cause mortality remained equally low at 45 deaths per 1000 person years during and after the first four weeks of buprenorphine treat-ment (fig 4) The pooled all cause mortality however increased to 320 deaths per 1000 person years in the first four weeks after people stopped buprenorphine treatment and reduced thereafter to 109 deaths per 1000 person years with an unadjusted pooled rate dif-ference for initial compared with subsequent periods out of treatment of 212 deaths (95 confidence interval minus59 to 482) per 1000 person years and an unadjusted pooled rate ratio of 294 (134 to 646)
Overdose mortality by time interval in and out of treatmentOnly three methadone cohorts and one buprenorphine cohort reported overdose mortality by time interval (fig 6) The pooled overdose mortality rates were 35 and 20 overdose deaths per 1000 person years in the first four weeks and the rest of time on methadone treatment and 42 and 34 overdose deaths per 1000 person years during and after the first four weeks out of treatment In the single buprenorphine cohort there were 09 and 15 fatal overdoses per 1000 person years before and after the first four weeks on buprenorphine treatment and 108 and 42 fatal overdoses per 1000 person years before and after four weeks out of treatment respectivelyta
ble
1 | b
asel
ine
popu
latio
n ch
arac
teris
tics o
f coh
ort s
tudi
es o
n m
orta
lity r
isk
in p
eopl
e w
ith o
pioi
d de
pend
ence
dur
ing
and
after
opi
oid
subs
titut
ion
treat
men
t
stud
ylo
catio
nPo
pula
tion
Opi
oid
in
ject
ors
()
non-
opio
id
drug
use
()
hiv
po
sitiv
e (
)Ps
ychi
atric
co
mor
bidi
ty (
)M
edic
al
com
orbi
dity
()
Men
()
base
line
mea
n ag
e (y
ears
)M
etha
done
Gear
ing
1974
24Ne
w Yo
rk U
SHe
roin
dep
ende
ntNA
84
00
00
NA79
030
0Cu
shm
an 1
97725
New
York
US
Opio
id d
epen
dent
NANA
00
29
274
730
385
Groumln
blad
h 19
9026
Natio
nwid
e S
wed
enHe
roin
dep
ende
ntNA
00
00
NANA
783
275
Capl
ehor
n 19
9427
1996
28Pa
rram
atta
NSW
Aus
tralia
Hero
in d
epen
dent
NANA
00
NANA
720
234
Fuge
lsta
d 19
9529
Stoc
khol
m S
wed
enHI
V po
sitiv
e in
ject
ing
opio
id d
epen
dent
100
00
010
00
NANA
NA31
8Fu
gels
tad
1998
30St
ockh
olm
Sw
eden
Non
volu
ntar
ily tr
eate
d in
ject
ing
hero
in d
epen
dent
100
00
067
938
698
250
029
3
Bust
er 2
0027
Amst
erda
m N
ethe
rland
sOp
ioid
dep
ende
nt34
7NA
NANA
NA77
032
6Sc
herb
aum
200
231St
ate-
wid
e N
orth
Rhi
ne-W
estp
halia
Ger
man
yIn
ject
ing
opio
id d
epen
dent
100
0NA
NA70
0NA
780
320
Davo
li 2
00732
Natio
nwid
e It
aly
Hero
in d
epen
dent
720
NA8
013
0NA
800
315
Fuge
lsta
d 2
00733
Stoc
khol
m S
wed
enHe
roin
dep
ende
ntNA
00
275
NANA
NA38
2Cl
ause
n 2
00834
Natio
nwid
e N
orw
ayOp
ioid
dep
ende
nt92
5NA
35
NANA
676
396
Dege
nhar
dt 2
0096
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA64
829
6Co
rnis
h 2
0108
Natio
nwid
e U
KOp
ioid
dep
ende
ntNA
NANA
NA17
569
330
1Pe
les
201
035Te
l Avi
v Is
rael
Opio
id d
epen
dent
NA67
58
441
6NA
736
376
Evan
s 2
0159
Stat
e-w
ide
CA
US
Opio
id d
epen
dent
552
219
NA23
119
064
235
3Ki
mbe
r 20
1510
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA65
833
4No
syk
201
536St
ate-
wid
e B
C C
anad
aHA
ART
treat
ed H
IV p
ositi
ve in
ject
ing
opio
id d
epen
dent
100
0NA
100
0NA
333
667
360
Cous
ins
201
637Na
tionw
ide
Irel
and
Opio
id d
epen
dent
NANA
NA22
822
068
730
5bu
pren
orph
ine
Corn
ish
201
08Na
tionw
ide
UK
Opio
id d
epen
dent
NANA
NANA
175
693
301
Reec
e 2
01038
Bris
bane
Que
ensl
and
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA73
030
5Ki
mbe
r 20
1510
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA70
732
5NA
=not
ava
ilabl
e H
AART
=hig
hly a
ctiv
e an
tiret
rovi
ral t
hera
py
Opi
oid
subs
titut
ion
treat
men
t with
eith
er m
etha
done
or b
upre
norp
hine
exc
ept f
or C
laus
en e
t al34
in w
hich
abo
ut 9
3 o
f par
ticip
ants
use
d m
etha
done
and
onl
y 7
use
d bu
pren
orph
ine
durin
g st
udy p
erio
d
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
6
tabl
e 2
| tre
atm
ent d
eliv
ery a
nd fo
llow
-up
feat
ures
of c
ohor
t stu
dies
on
mor
talit
y ris
k in
peo
ple
with
opi
oid
depe
nden
ce d
urin
g an
d aft
er o
pioi
d su
bstit
utio
n tre
atm
ent
stud
yno
of c
ohor
t pa
rtic
ipan
tsdagger
aver
age
Ost
do
se (m
gda
y)in
patie
nt
indu
ctio
n (
)O
st
prov
ider
Follo
w-u
p pe
riod
aver
age
follo
w-u
p (y
ears
)Dagger
loss
to
follo
w-u
p (
)sectM
orta
lity
outc
ome
Qua
lity
scor
epara
Met
hado
neGe
arin
g 19
7424
3000
100
176
Spec
ialis
t19
65-7
25
24
0Al
l cau
ses
ove
rdos
e9
Cush
man
197
72554
710
0NA
Spec
ialis
t19
66-7
53
623
2Al
l cau
ses
ove
rdos
e6
Groumln
blad
h 19
9026
166
7510
00
Spec
ialis
t19
67-8
711
00
0Al
l cau
ses
ove
rdos
e4
Capl
ehor
n 19
9427
1996
2830
511
632
3Sp
ecia
list
1970
-90
139
144
All c
ause
s27
ove
rdos
e286
Fuge
lsta
d 19
9529
135
NA10
00
Spec
ialis
t19
86-9
02
10
0Al
l cau
ses
6Fu
gels
tad
1998
3056
8010
00
Spec
ialis
t19
86-9
34
20
0Al
l cau
ses
6Bu
ster
200
2752
0048
00
Mix
ed19
86-9
85
70
0O
verd
ose
8Sc
herb
aum
200
23124
447
00
Spec
ialis
t19
88-9
65
315
6Al
l cau
ses
ove
rdos
e7
Davo
li 2
00732
5276
NA0
0Sp
ecia
list
1998
-200
11
33
7O
verd
ose
11Fu
gels
tad
200
73367
9NA
100
0Sp
ecia
list
1988
-200
06
96
2Al
l cau
ses
3Cl
ause
n 2
00834
3229
112
00
Mix
ed19
97-2
003
24
00
All c
ause
s o
verd
ose
7De
genh
ardt
200
9631
846
700
0M
ixed
1985
-200
0daggerdagger6
80
0Al
l cau
sesDaggerDagger
12Co
rnis
h 2
0108
4894
500
0GP
1990
-200
519
175
All c
ause
s9
Pele
s 2
01035
613
113
00
Spec
ialis
t19
93-2
008
770
8Al
l cau
ses
ove
rdos
e9
Evan
s 2
0159
32 32
2NA
00
Spec
ialis
t20
06-1
02
35
0Al
l cau
sesDaggerDagger
12Ki
mbe
r 20
1510
26 0
6470
00
Mix
ed20
01-1
05
30
0Al
l cau
ses
ove
rdos
e13
Nosy
k 2
01536
1326
NA0
0GP
1996
-201
04
279
All c
ause
sDaggerDagger13
Cous
ins
201
63769
8372
00
GP20
04-1
04
12
0Al
l cau
ses
ove
rdos
e12
bupr
enor
phin
eCo
rnis
h 2
0108
1373
100
0GP
1990
-200
511
103
All c
ause
s9
Reec
e 2
01038
2518
NA0
0GP
2000
-07
32
12Al
l cau
ses
5Ki
mbe
r 20
1510
11 94
012
00
Mix
ed20
01-1
04
50
0Al
l cau
ses
ove
rdos
e13
NA=n
ot a
vaila
ble
OST
=opi
oid
subs
titut
ion
treat
men
tO
pioi
d su
bstit
utio
n tre
atm
ent w
ith e
ither
met
hado
ne o
r bup
reno
rphi
ne e
xcep
t for
Cla
usen
et a
l34 in
whi
ch a
bout
93
of p
artic
ipan
ts u
sed
met
hado
ne a
nd o
nly 7
u
sed
bupr
enor
phin
e du
ring
stud
y per
iod
daggerPar
ticip
ants
rece
ivin
g op
ioid
sub
stitu
tion
treat
men
t at l
east
onc
e du
ring
stud
y per
iod
Unt
reat
ed p
artic
ipan
ts a
nd th
ose
rece
ivin
g ot
her t
ypes
of t
reat
men
t for
opi
oid
depe
nden
ce (m
etha
done
det
oxifi
catio
n o
pioi
d an
tago
nist
ther
apy
ther
apeu
tic
com
mun
ity) e
xclu
ded
from
met
a-an
alys
is
DaggerAve
rage
follo
w-u
p fro
m s
tart
of o
pioi
d su
bstit
utio
n tre
atm
ent c
ombi
ning
sub
sequ
ent p
erio
ds in
and
out
of t
reat
men
tsectP
erce
ntag
e lo
ss to
follo
w-u
p be
fore
end
of s
tudy
per
iod
or d
eath
If n
ot o
ther
wis
e sp
ecifi
ed c
ompl
ete
case
asc
erta
inm
ent a
ssum
ed fo
r stu
dies
bas
ed o
n po
pula
tion
mor
talit
y reg
istri
es
paraQua
lity a
sses
smen
t sco
re ra
ngin
g fro
m 0
(low
est q
ualit
y) to
16 (h
ighe
st q
ualit
y)
O
verd
ose
mor
talit
y rep
orte
d bu
t not
incl
uded
in m
eta-
anal
ysis
as t
here
wer
e no
ove
rdos
e de
aths
whi
le p
artic
ipan
ts w
ere
in o
pioi
d su
bstit
utio
n tre
atm
ent
daggerdaggerFo
llow
-up
rest
ricte
d to
1985
-200
0 as
sub
sequ
ent 2
001-
06 fo
llow
-up
perio
d ov
erla
pped
with
Kim
ber e
t al10
DaggerDaggerO
verd
ose
mor
talit
y rep
orte
d on
ly fo
r com
bine
d tre
atm
ents
or i
nclu
ded
untre
ated
par
ticip
ants
and
hen
ce n
ot in
clud
ed in
met
a-an
alys
is
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
7
discussionMain findingsOur review suggests that time spent in opioid substitu-tion treatment with methadone is associated with an average reduction of 25 deaths1000 person years (95 confidence interval 14 to 36) The rate in treatment was less than a third of the rate out of treatment with the greatest difference in deaths from overdose The all cause mortality risk during treatment is much higher in the first four weeks than in the remainder of treatment Mortality risk is also higher in the first four weeks after cessation than in the remainder time out of treatment
Based on three cohorts (two from Australia) findings also suggest that opioid substitution treatment with buprenorphine could be associated with a reduction in mortality with a similar risk across all time in treatment (about four deaths1000 person years) consistent with its safety profile39-44 and a risk after cessation higher in the first four weeks than in the remainder of time out of treatment (32 versus 11 deaths1000 person years)
Mortality risk during specific periods in and out of methadone treatmentThe larger relative effect size (as measured by rate ratio) for overdose than non-overdose deaths with metha-done substitution6 11 34 45 is consistent with previous findings although the effect on non-overdose deaths had not been previously reviewed This disparity is
consistent with what would be expected given metha-donersquos effect on reducing use of heroin and other illicit opioids32 34
Our finding that the first four weeks after onset (114 deaths1000 person years) and cessation (3211000 person years) of methadone treatment are the highest risk periods suggests that these are key periods during which to focus efforts for prevention of drug related deaths Moreover within periods of methadone treat-ment there is a swift decline in risk from first to fourth week followed by a stable trend whereas after cessa-tion there is a high but quite stable risk during the first four weeks and a progressive decline afterward This is important because some patients cycle in and out of opioid substitution treatment46-50 and are therefore exposed to repeated periods of high risk for mortality Such changes probably mainly reflect changes in risk of fatal overdose6 32 but this has not been accurately assessed because only two cohorts reported overdose data specifically7 10 The increased risk during the first few weeks of treatment could be explained by an accu-mulation of methadone that exceeds the opioid toler-ance level (the mean elimination half life for methadone is 22 hours)51 as opioid tolerance does not seem to fully protect against respiratory depression52 Psychological factors and concomitant use of other respiratory depressant drugs or cocaine could also play a role7 8 40 53 54
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1994 Fugelstad et al 1995 Fugelstad et al 1998 Scherbaum et al 2002 Fugelstad et al 2007 Clausen et al 2008 Degenhardt et al 2009 Cornish et al 2010 Peles et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine Cornish et al 2010 Reece 2010 Kimber et al 2015Overall
2 5 10 20 50 100 200
11014 474251655161085111975
82427177
181114773354906450
648111 538305129423985
16325 27763691 792
89397911522 648
774031119
8721 936
In treatment
3311701429732740
362279545457
14172741311461303
1510105 73571428852727
84848 12256345 2652061582986247
10751406911
31431 239
Out of treatment
No of deathsperson years
76 (62 to 92)151 (98 to 223)148 (84 to 239)56 (28 to 100)
331 (143 to 651)395 (159 to 814)162 (96 to 255)
230 (181 to 287)140 (112 to 171)
58 (54 to 63)58 (40 to 83)
105 (76 to 142)64 (55 to 75)69 (64 to 75)
224 (180 to 275)51 (42 to 61)
113 (84 to 152)
95 (38 to 195)27 (06 to 78)40 (32 to 49)43 (21 to 89)
In treatment
282 (194 to 396)471 (258 to 791)432 (296 to 610)158 (111 to 219)
1111 (361 to 2593)699 (191 to 1790)814 (445 to 1366)565 (443 to 709)353 (259 to 471)143 (136 to 150)166 (129 to 209)715 (534 to 938)176 (165 to 188)124 (114 to 135)
1302 (1130 to 1493)157 (127 to 191)361 (245 to 533)
133 (64 to 245)58 (41 to 79)
101 (90 to 112)95 (39 to 234)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 2 | all cause mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled all cause mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates during periods in and out of treatment across all methadone or buprenorphine cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
8
tabl
e 3
| Poo
led
all c
ause
and
ove
rdos
e m
orta
lity r
ates
dur
ing
perio
ds in
and
out
of o
pioi
d su
bstit
utio
n tre
atm
ent w
ith m
etha
done
by s
tudy
char
acte
ristic
s
stud
y ch
arac
teris
tic
all c
ause
mor
talit
y ra
te1
000
pers
on y
ears
(95
Ci)
Ove
rdos
e m
orta
lity
rate
100
0 pe
rson
yea
rs (9
5 C
i)
no o
f st
udie
sin
trea
tmen
tO
ut o
f tre
atm
ent
P va
luedagger
i2 (
)Daggerno
of
stud
ies
in tr
eatm
ent
Out
of t
reat
men
tP
valu
edaggeri2 (
)Dagger
Loca
tion
E
urop
eIs
rael
913
9 (9
5 to
20
5)46
6 (2
90
to 74
9)
008
987
31
(24
to 4
0)
133
(59
to 2
98)
013
93
Nor
th A
mer
ica
411
2 (6
4 to
196
)42
3 (2
12 to
84
6)2
23
(14
to 3
8)
205
(44
to 9
45)
A
ustra
lia3
63
(33
to 12
1)14
0 (6
3 to
30
8)2
20
(14
to 2
9)
67
(15
to 2
96)
Opio
id in
ject
ors (
)
lt
100
129
0 (6
9 to
117
)25
8 (1
87
to 3
55)
000
195
102
5 (2
0 to
30
)10
6 (6
1 to
185
)mdash
mdash
100
423
4 (1
42
to 3
85)
109
9 (5
94
to 2
034
)1
mdashsect
mdashsect
Men
()
lt
7511
95
(69
to 13
2)
300
(18
4 to
48
8)0
6798
62
4 (1
8 to
34
)10
6 (4
5 to
24
8)0
7493
ge
753
116
(61
to 2
20)
459
(178
to 11
79)
52
9 (2
0 to
42
)15
8 (6
2 to
40
3)M
ean
age
(yea
rs)
lt
3510
99
(68
to 14
5)
293
(179
to 4
82)
040
988
26
(19
to 3
5)
106
(52
to 2
18)
060
93
ge35
614
0 (8
7 to
22
7)50
3 (2
68
to 9
43)
32
7 (1
5 to
47
)20
5 (6
2 to
676
)Av
erag
e m
etha
done
dos
e (m
gda
y)
le
807
96
(63
to 14
8)
269
(15
5 to
46
5)0
5692
53
1 (2
0 to
46
)10
3 (4
0 to
26
9)0
2293
gt
805
99
(60
to 16
5)
354
(18
5 to
677
)5
25
(16
to 3
9)
170
(65
to 4
49)
Inpa
tient
indu
ctio
n (
)
09
92
(63
to 13
6)
299
(173
to 5
16)
019
987
25
(18
to 3
4)
100
(45
to 2
23)
065
93
gt0
615
4 (9
3 to
25
3)45
9 (2
29
to 9
21)
32
9 (1
7 to
50
)18
4 (5
4 to
62
5)Tr
eatm
ent p
rovi
der
S
peci
alis
t10
134
(92
to 19
5)
465
(28
2 to
765
)0
2698
72
5 (1
7 to
37
)20
8 (1
11 to
38
8)0
0188
G
Pm
ixed
68
6 (5
4 to
137
)24
4 (1
31
to 4
54)
42
4 (1
6 to
36
)5
6 (2
5 to
125
)M
idpo
int f
ollo
w-u
p pe
riod
lt
2000
1012
6 (8
5 to
187
)38
8 (2
28
to 6
61)
058
987
28
(20
to 3
9)
154
(70
to 3
39)
067
93
ge20
006
97
(60
to 15
9)
320
(16
5 to
62
3)4
24
(17
to 3
5)
90
(32
to 2
52)
Loss
to fo
llow
-up
()
lt
1012
119
(83
to 1
70)
383
(23
7 to
619
)0
8198
82
5 (1
9 to
32
)9
8 (5
0 to
195
)0
3393
ge
104
95
(50
to 18
0)
313
(13
5 to
72
3)3
32
(17
to 6
0)
254
(81
to 7
94)
Poo
led
mor
talit
y rat
es a
nd 9
5 c
onfid
ence
inte
rval
s dur
ing
perio
ds in
and
out
of t
reat
men
t by s
tudy
cha
ract
eris
tics e
stim
ated
from
sep
arat
e bi
varia
te ra
ndom
effe
cts m
eta-
regr
essi
on m
odel
s rel
atin
g lo
g tra
nsfo
rmed
rate
s in
both
trea
tmen
t per
iods
w
ith e
ach
stud
y cha
ract
eris
tic
daggerOve
rall
P va
lue
for h
eter
ogen
eity
of p
oole
d m
orta
lity r
ates
acr
oss c
ateg
orie
s of s
tudy
cha
ract
eris
tic a
s obt
aine
d fro
m li
kelih
ood
ratio
test
com
parin
g ne
sted
met
a-re
gres
sion
mod
els w
ith a
nd w
ithou
t stu
dy c
hara
cter
istic
fitte
d vi
a m
axim
um li
kelih
ood
DaggerOve
rall
I2 sta
tistic
for r
esid
ual h
eter
ogen
eity
in s
tudy
spe
cific
mor
talit
y rat
es n
ot e
xpla
ined
by c
orre
spon
ding
stu
dy c
hara
cter
istic
sectP
oole
d m
orta
lity r
ates
not
app
licab
le to
cat
egor
ies w
ith s
ingl
e st
udy
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
9
Although the long half life of methadone could con-tribute to the increase in mortality in the first three to four days after cessation of treatment there was a large increase in mortality across the first four weeks after cessation compared with the treatment period Such increased mortality could be explained by loss of toler-ance to the toxic effects of heroin assuming that many patients return to use6 8 32 47 55 56 and probably also by the use of multiple legal and illicit substances during that period Similar peaks in drug related mortality occur in other situations where opioid tolerance is prob-ably diminished (for example after prison release or hospital discharge57-59 ) Lifestyle factors and comorbid issues such as mental health problems could also increase mortality from other external causes as deaths from suicide and injury are also more common during that period53
Mortality risk during specific periods in and out of buprenorphine treatmentData from three cohorts (two from Australia) suggest that substitution treatment with buprenorphine could reduce all cause mortality although the disparity in mortality rates in periods in and out of treatment did not reach significance Findings also suggest a signifi-cantly increased mortality in the first four weeks after cessation of treatment compared with the remaining time out of treatment (320 versus 1091000 person years) while during the treatment period there was no difference between the first four weeks and the remain-ing time in treatment It is difficult to draw firm conclu-sions because of limited evidence from similar settings 96 of included deaths and 98 of person years came from Australian studies (with 87 and 86 from the study by Kimber and colleagues13)
Comparative effectiveness of buprenorphine and methadone substitution treatmentOther sources of data have suggested that buprenor-phine could be more effective than methadone in reduc-ing mortality especially from overdose39 42 43 Unlike methadone there is a ceiling for respiratory depressant effects of buprenorphine as dose increases and the probability of triggering arrhythmias is lower for buprenorphine than methadone41 44 60 When we com-pared the mortality between periods in and out of treat-ment first within those taking methadone and then within those taking buprenorphine we found a greater reduction in mortality with methadone than with buprenorphine (measured as the rate difference or rate ratio between periods) When we compared mortality between them first within the treatment period and then in the period off treatment we found a signifi-cantly lower mortality with buprenorphine than meth-adone in both periods
Our conclusions must remain tentative until further studies in varied treatment settings and contexts are undertaken to examine this issue Differences in mor-tality might also reflect confounding through differ-ences in characteristics of patients (such as age severity of opioid dependence injecting drug use other ta
ble
4 | C
ohor
t stu
dies
repo
rtin
g al
l cau
se a
nd o
verd
ose
mor
talit
y rat
e ra
tios c
ompa
ring
perio
ds o
ut a
nd in
opi
oid
subs
titut
ion
treat
men
t adj
uste
d fo
r con
foun
ding
stud
y
Conf
ound
ing
fact
ors
all c
ause
mor
talit
yO
verd
ose
mor
talit
y
Patie
nt d
emog
raph
ics
seve
rity
of d
rug
use
trea
tmen
tCo
mor
bidi
tyun
adju
sted
ra
te ra
tioad
just
ed
rate
ratio
Perc
enta
ge
chan
gedagger
unad
just
ed
rate
ratio
adju
sted
ra
te ra
tioPe
rcen
tage
ch
ange
dagger
Met
hado
neBu
ster
200
27Se
x ra
ceTr
eatm
ent m
odal
ity t
ime
sinc
e fir
st tr
eatm
ent
mdashmdash
mdashmdash
087
087
minus03
Davo
li 2
00732
Age
sex
Leng
th o
f her
oin
use
her
oin
inje
ctio
n
prev
ious
ove
rdos
eHI
V p
sych
iatri
c com
orbi
dity
mdashmdash
mdash77
174
3minus3
6
Dege
nhar
dt 2
0096
Age
sex
cal
enda
r yea
rmdash
mdash19
118
8minus1
3mdash
mdashmdash
Corn
ish
201
08Ag
e s
ex c
alen
dar y
ear
mdashM
edic
al c
omor
bidi
ty2
833
2715
5mdash
mdashmdash
Evan
s 2
0159Dagger
Age
sex
rac
e e
duca
tion
em
ploy
men
t cr
imin
ality
hea
lth c
over
age
Prim
ary o
pioi
d fr
eque
ncy a
nd le
ngth
of
opio
id u
se n
on-o
pioi
d dr
ug u
seHI
V h
epat
itis C
tub
ercu
losi
s
disa
bilit
y m
edic
al c
omor
bidi
ty
psyc
hiat
ric c
omor
bidi
ty
273
370
355
351
442
258
Nosy
k 2
01536
DaggerAg
e s
ex r
ace
cal
enda
r yea
r re
gion
No o
f pre
viou
s tre
atm
ent e
piso
des
Tim
e si
nce
HIV
diag
nosi
s C
D4
coun
t AI
DS a
ntire
trovi
ral
ther
apy
med
ical
com
orbi
dity
304
294
minus34
114
147
286
Cous
ins
201
637Ag
e s
exTr
eatm
ent s
uper
visi
on m
etha
done
dos
eM
edic
al c
omor
bidi
ty3
093
6417
816
016
317
bupr
enor
phin
eCo
rnis
h 2
0108
Age
sex
cal
enda
r yea
rmdash
Med
ical
com
orbi
dity
141
164
168
mdashmdash
mdashB
asel
ine
or ti
me
vary
ing
conf
ound
ing
fact
ors u
sed
in a
djus
tmen
tdaggerP
erce
ntag
e ch
ange
in ra
te ra
tio a
fter a
djus
tmen
t for
cor
resp
ondi
ng c
onfo
undi
ng fa
ctor
sDaggerO
verd
ose
mor
talit
y rat
e ra
tios r
epor
ted
com
bini
ng m
etha
done
mai
nten
ance
with
det
oxifi
catio
n (1
14
of p
erso
n ye
ars i
n tre
atm
ent)
in E
vans
et a
l9 an
d in
clud
ing
neve
r tre
ated
par
ticip
ants
(73
3 o
f per
son
year
s out
of t
reat
men
t) in
Nos
yk e
t al36
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
10
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1996 Buster et al 2002 Scherbaum et al 2002 Davoli et al 2007 Clausen et al 2008 Peles et al 2010 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine Kimber et al 2015
2105 5 10 20 50 100
3314 474416557108541792
4218 7476111475751
24645053985
16991 7925422 648
3121 936
In treatment
2111707297
27740192004
2610 983131729998
28130313727
21645 265246247
14331 239
Out of treatment
No of deathsperson years
23 (16 to 32)24 (07 to 62)
64 (26 to 133)22 (06 to 57)22 (16 to 30)
54 (20 to 117)12 (05 to 25)37 (24 to 55)12 (04 to 29)18 (16 to 21)24 (18 to 31)26 (21 to 33)
14 (10 to 20)
In treatment
179 (111 to 274)236 (95 to 486)
365 (240 to 531)95 (57 to 148)24 (16 to 35)
756 (402 to 1292)90 (41 to 171)
215 (143 to 311)179 (95 to 306)
48 (42 to 54)38 (25 to 57)
127 (69 to 234)
46 (39 to 54)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 3 | Overdose mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled overdose mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates during periods in and out of treatment across all methadone cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
Methadone rst four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallMethadone aer four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Cornish et al 2010 Kimber et al 2015OverallBuprenorphine aer four weeks Cornish et al 2010 Kimber et al 2015Overall
21 5 10 20 50 100
9425057465
151950323344
4100153371
554109 033234664
14823 32760488 449
85388010019 277
18192094
66597819 842
In treatment
38189821479
154267335183679113
441181
1472103 838503809
69445 44952843 4301271469545067
788281674
366328629 565
Out of treatment
No of deathsperson years
375 (303 to 459)151 (61 to 311)77 (43 to 127)96 (66 to 135)
mdash44 (25 to 73)
114 (58 to 224)
51 (47 to 55)49 (31 to 74)63 (54 to 74)68 (63 to 74)
mdash52 (42 to 63)58 (50 to 67)
124 (03 to 692)43 (20 to 82)
45 (12 to 168)
91 (33 to 198)39 (31 to 49)45 (32 to 62)
In treatment
200 (142 to 275)438 (271 to 670)576 (489 to 675)191 (133 to 265)
mdash373 (271 to 500)321 (191 to 539)
142 (135 to 149)131 (97 to 173)
153 (141 to 164)122 (111 to 132)
mdash107 (80 to 139)
135 (119 to 153)
800 (322 to 1648)167 (111 to 242)320 (132 to 775)
45 (09 to 132)97 (86 to 109)
109 (85 to 139)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 4 | all cause mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled all cause mortality rates 2009-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except Degenhardt et al6 which reported mortality before and after two weeks of treatment initiation and cessation high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-analysis area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates before and after four weeks in and out of treatment across methadone or buprenorphine cohorts estimated from multivariate random effects meta-analysis on log transformed rates in four time-by-treatment intervals
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
11
drug use comorbidities prison history overdose his-tory patientrsquos preference) characteristics of treatment (such as previous treatment specialisation of the doc-tor who controls the treatment dose provision charac-teristics cointerventions retention or drop outs) or the sociopolitical context in which studies have been conducted For example the initial prognosis might be better in those given buprenorphine than those given methadone (that is fewer comorbid problems less severe opioid dependence)6 8 10 61 though this was not clearly found in a recent US study62
The role of such confounding factors has received almost empirical examination Few details on char-acteristics of patients or treatments were reported in articles included in this meta-analysis to permit a detailed examination of this potential issue (tables 1 and 2 ) so it was not possible to assess the possibil-ity of confounding A sensitivity simulation analysis in the study by Kimber and colleagues however suggested that the lower mortality with buprenor-phine than with methadone during first four weeks of treatment was unlikely to be caused by unmea-sured confounding10
strengths and limitationsThis meta-analysis synthesised evidence from cohort studies published until 2016 on risk of mortality in people who are dependent on opioids during and after opioid substitution treatment separately for buprenor-phine and methadone Mortality changes over time (1st-32th week) during and after methadone are care-fully quantified for the first time
The published studies however had several methodological shortcomings Firstly in the included
Methadone rst four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallMethadone aer four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Kimber et al 2015Buprenorphine aer four weeks Kimber et al 2015
21 505 10 20
9150018334443371
3317 20015188 4495019 277
22094
2919 842
In treatment
2130010183681181
24960020643 430
165067
181674
12529 565
Out of treatment
No of deathsperson years
60 (27 to 114)54 (32 to 85)12 (03 to 30)35 (13 to 95)
19 (13 to 27)17 (14 to 20)26 (19 to 34)20 (15 to 27)
09 (01 to 34)
15 (10 to 21)
In treatment
15 (02 to 56)54 (26 to 100)68 (29 to 134)42 (18 to 99)
25 (16 to 37)47 (41 to 54)32 (18 to 51)34 (23 to 51)
108 (64 to 170)
42 (35 to 50)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 6 | Overdose mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled overdose mortality rates 2002-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except buster et al7 which reported mortality before and after two weeks of treatment initiation and cessation area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates before and after four weeks in and out of treatment across methadone cohorts estimated from multivariate random-effects meta-analysis on log transformed rates in four time-by-treatment intervals
Time since treatment initiation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s In methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Time since treatment cessation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s Out of methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Degenhardt et al 2009Cornish et al 2010Evans et al 2015Kimber et al 2015Cousins et al 2016
Fig 5 | all cause mortality rates by time since treatment initiation and cessation in methadone cohorts and pooled all cause mortality risk trends 2009-16 high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-regression area of each circle is proportional to weight of each time interval in meta-regression Pooled trends in all cause mortality risk (solid lines) and their 95 confidence intervals (shaded regions) over time in and out of methadone treatment were estimated from bivariate random effects meta-regression of log transformed rates on quadratic linear spline function of log time with knot at four weeks
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
12
observational studies the same patients are compared throughout follow-up periods in and out of opioid sub-stitution treatment but these patients leave and re-en-ter treatment in a non-random way and hence there could still be a large potential for confounding in com-parisons of crude mortality risk in and out of treat-ment In some studies with diverse information on patient demographics severity of drug use and comor-bidities measured mostly at baseline (table 3 ) adjust-ment for these potential confounders resulted in similar or even increased out-to-in mortality rate ratios which merely reflects that the above conditions tended to be less prevalent at baseline among patients who later left or were discharged from treatment than those who remained in treatment Nevertheless to obtain an unbiased estimate of the preventive effect of opioid substitution treatment on all cause and overdose mor-tality these and other relevant confounders should be measured every time a patient leaves and resumes treatment Time varying data can then be used to adjust for confounder history in standard regression models or even better to construct inverse probability of treatment weights for marginal structural models63 which properly control for time varying confounders for later treatment that are themselves affected by pre-vious treatment such as severity of drug use and comorbidity Also differential loss to follow-up is a concern in the meta-analysed cohorts as dropouts are more likely to occur in patients at higher risk of death during periods out of treatment thus inducing a selec-tion bias in crude comparisons of out-to-in mortality risk because of informative censoring Marginal struc-tural models with inverse probability of censoring weights can also be used to correct for differential loss to follow-up63 provided that common predictors of death and censoring are measured over time In sum-mary individual cohorts are prone to confounding and selection bias because of differential loss to follow-up but it is hard to assess with the available information the amount and direction of bias projected onto the pooled mortality rate differences and rate ratios between periods in and out of treatment obtained in this meta-analysis
Secondly studies were conducted in high income countries with the follow-up often spread over many calendar years (1965-2010 for methadone and 1990-2010 for buprenorphine) and a highly variable average length of follow-up (ranges 13-158 years and 11-45 years respectively) Studies in low and middle income countries are especially needed
Thirdly by design we have not captured overdose mortality when opioid substitution treatment was obtained on illicit drug markets40 64 Fourthly a delayed record of treatment cessation could have led to some deaths that occurred out of treatment being incorrectly classified as occurring in treatment40 if so this makes our estimated impact of opioid substitution treatment on mortality a conservative one There could similarly be misclassification between overdose and non-over-dose deaths because of inconsistencies in definition of overdose and codification of causes of deaths (for
instance criteria for separating overdose death from intentional poisoning or sudden cardiac death)40 65 again these misclassifications would tend to underesti-mate deaths from overdose
implications for policy and practiceIn many countries the number of deaths attributable to opioid use is substantial66 67 and increasing in some such as the US where deaths from opioid overdose now outnumber gun related deaths in the country68 Over-doses are preventable causes of death warranting wide implementation of preventive interventions Our review has provided evidence that methadone and probably buprenorphine reduce mortality among people depen-dent on opioids making it imperative that further research confirms this using study designs that con-sider a wide range of confounding variables to increase confidence that these effects are causal
It must be borne in mind that there is strong evidence of the efficacy of methadone and buprenorphine on a range of clinical outcomes and these medicines are listed as WHO essential medicines the findings we have presented here provide additional imperatives for their widespread availability Despite this coverage of opioid substitution treatment is low in many countries worldwide69 Policymakers clinicians and those responsible for drug treatment systems should work to ensure the availability of such treatment remove access barriers and promote engagement This means the strategic development of services from a public health perspective which could reduce the social harm associ-ated with opioid use
Our review suggests that some precautions should be taken during and after opioid substitution treatment to increase safety Firstly careful clinical assessment of opioid tolerance before onset of treatment to establish a safe induction dose seems warranted Secondly moni-toring during the induction period is important espe-cially for methadone with clinicians considering adjusting opioid doses monitoring mental and somatic problems and preventing the use of opioids obtained on the illicit drug market64 In addition education of patients about the risk of overdose risk and use of ldquotake homerdquo naloxone70 71 is warranted Buprenorphine induction followed by transition to methadone might also be considered10 72 Retention in opioid substitution treatment reduces risk of exposure to mortality after cessation and also to re-exposure to mortality risk during induction onto methadone so efforts to improve retention are important as a strategy to reduce mortal-ity More generally establishment of mechanisms for information and coordination between healthcare social and legal services and patient counselling while in treatment in addition to more specific overdose pre-vention programmes such as naloxone distribution should be considered
Finally there is a pressing need for new studies on the comparative effectiveness of methadone and buprenorphine in reducing mortality New ran-domised controlled trials are highly unlikely they would be prohibitively expensive and difficult to
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score

doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
2
been under-powered to detect potential differences in mortality risk by time interval in and out of treatment and long term large trials comparing the effect of methadone and buprenorphine on all cause and over-dose mortality are hardly feasible3 In this context a systematic review of cohort studies can provide valu-able evidence on the mortality experience of opioid dependent people at different periods of methadone and buprenorphine substitution treatment that could guide clinicians and policymakers in the optimal pro-vision of treatment12
In this systematic review and meta-analysis we syn-thesised results from cohort studies on mortality among patients receiving opioid substitution treatment to obtain pooled estimates of all cause and overdose mor-tality rates during periods in and out of treatment with methadone and buprenorphine evaluate heterogeneity of mortality rates across cohort characteristics and investigate changes in mortality rates over time in and out of treatment particularly within the first weeks after treatment initiation and cessation
Methodssearch strategy and inclusion criteriaWe searched Medline Embase PsycINFO and LILACS by using different combinations of free text and data-base specific index terms related to the topics of opioid dependence opioid substitution treatment mortality and cohort studies Details of the full search strategy are provided in appendix 1 The search was updated to September 2016 with no language restrictions We also searched the Cochrane Database of Systematic Reviews reviewed the reference lists of relevant original papers and reviews screened articles in the PubMed ldquorelated citationsrdquo section searched online for technical reports and monographs and consulted experts and investiga-tors with ongoing studies in opioid dependence We followed the PRISMA statement for reporting system-atic reviews and meta-analyses13
We included cohort studies comparing mortality among people with opioid dependence To be eligible studies had to include follow-up data during and after opioid substitution treatment with methadone or buprenorphine The prespecified exclusion criteria were as follows
bull No data in humansbull No original research (reviews editorials non-re-
search letters protocols)bull Study design other than observational cohort (clini-
cal trials case-control studies cross sectional sur-veys case reports case series qualitative research)
bull Study not focused on people with opioid dependence bull People in prison or recently releasedbull Treatment unknown or other than methadone or
buprenorphine maintenance (methadone detoxifica-tion opioid antagonist therapy therapeutic community)
bull No all cause or overdose mortality as outcome or no deaths over follow-up
bull Insufficient data to compute mortality rates during periods in and out of treatment (number of deaths
and person years broken down by follow-up period in and out of treatment)
For cohorts originating several reports we used data from non-overlapping follow-up periods from each report whenever possible or selected the publication with the longest follow-up
study selection and data extractionTwo investigators independently reviewed the titles and abstracts identified in the search and retrieved articles to determine eligibility and to extract study data Dis-agreements or uncertainties were resolved by consen-sus with an additional investigator
For each eligible study we retrieved information on baseline population characteristics including study location sex and age distribution primary opioid of misuse and prevalence of opioid injection non-opi-oid drug use HIV infection and psychiatric and med-ical comorbidity number of cohort participants entering opioid substitution treatment during the study period (untreated participants and those under other types of treatment were excluded) treatment features including drug type (methadone or buprenor-phine) average daily dose induction method (inpa-tient or ambulatory) and provider (addiction medicine specialist or general practitioner) and main follow-up characteristics including calendar period average length of follow-up from the start of mainte-nance treatment (excluding any previous detoxifica-tion period) loss to follow-up and mortality outcomes We also registered detailed information on the number of deaths person years at risk and mor-tality rates from all causes and overdose during fol-low-up periods in and out of treatment and whenever possible during specific time intervals since treat-ment initiation and cessation Finally we registered information on first and subsequent treatment epi-sodes (table A in appendix 2) and on completeness of treatment (table B in appendix 2)
We specifically designed a quality assessment form based on standardised and extensively used instru-ments the methodology checklist for cohort studies developed by the Scottish Intercollegiate Guidelines Network14 and the checklist for drug related studies developed by the National Drug and Alcohol Research Centre Australia15 The design process based on a thor-ough review of the above sources included the develop-ment of different proposals discussion of their appropriateness and final agreement among the authors The final version comprised separate sections according to the study design and was based on a ldquostar systemrdquo score approach16 including a general appraisal of external and internal validity and of the biases rele-vant to cohort studies plus an ad hoc assessment of reporting for studies on mortality during and after opi-oid substitution treatment (appendix 3)
statistical analysisFor each selected cohort we calculated crude mortality rates from all causes and overdose during periods in
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
3
and out of treatment by dividing the number of deaths registered in each period by the person years contrib-uted by all participants to that period If not explicitly reported we derived the number of person years by treatment period from the available summary statistics on follow-up and treatment retention or the reported mortality rates We computed exact 95 confidence intervals for the underlying mortality rates by assuming a Poisson distribution for the observed number of deaths and fixed person years at risk
Cause specific mortality rates in and out of treatment were jointly combined across all methadone or buprenorphine cohorts by using a bivariate random effects meta-analysis on log transformed mortality rates in both treatment periods17-19 This bivariate meta-ana-lytic approach allowed estimation of not only the pooled mortality rates and 95 confidence intervals in and out of treatment but also the pooled rate difference and rate ratio comparing periods out of and in treatment with confidence intervals that took into account the correlation between rates in both treatment periods
To evaluate whether cause specific mortality rates differed by baseline population characteristics treat-ment delivery and follow-up features of methadone cohorts we included the location (EuropeIsrael North America or Australia) prevalence of opioid injection (lt100 or 100) percentage of men (lt75 or ge75) mean age (lt35 or ge35) average methadone dose (le80 or gt80 mgday) percentage of inpatient induction (0 or gt0) treatment provider (specialist or general practitionermixed) midpoint follow-up period (lt2000 or ge2000) and percentage loss to follow-up (lt10 or ge10) in each methadone cohort as single predictors in separate bivariate random effects meta-regression models on log transformed mortality rates in and out of treatment17 18 We contrasted heterogeneity of pooled mortality rates by these cohort characteristics through likelihood ratio tests comparing nested meta-regression models with and without the predictor fitted through maximum like-lihood The limited number of buprenorphine cohorts precluded a similar heterogeneity analysis across these cohorts
For methadone or buprenorphine cohorts that reported mortality data by time interval in and out of treatment we combined cause specific mortality rates before and after four weeks of treatment initiation and cessation through a multivariate random effects meta-analysis on log transformed mortality rates in these time-by-treatment intervals To obtain pooled trends in all cause mortality risk over time in and out of methadone substitution treatment we fitted a bivariate random effects meta-regression of log transformed rates on a quadratic linear spline function of log time with knot at four weeks20 This quadratic linear spline allowed for a quadratic trend in the first four weeks in and out of treatment and forced the trend to be linear thereafter to avoid implausible shapes at long follow-up times The resulting pooled trends were virtually insensitive to different knot locations at three four or five weeks
We examined the overall heterogeneity in mortality rates across studies as well as the residual heterogene-ity beyond that explained by study level characteristics with the multivariate extension of the Cochran χ2 test and quantified it with the extended I2 statistic18 21 which described the proportion of total variation in study specific mortality rates because of heterogeneity The influence of each study on pooled estimates was evaluated by removal of each individual study from the analysis Publication bias and genuine small study effects were assessed with the extended Egger test allowing for heterogeneity22 23
In all the above multivariate random effects meta-an-alytic models we assumed the correlations within cohorts in the estimated mortality rates to be zero as they were obtained over different follow-up periods in and out of treatment Nevertheless we performed sen-sitivity analyses assuming positive within cohort cor-relations between mortality rates in and out of treatment of 025 050 075 and 095 for all studies and the pooled rates and their standard errors were virtually identical to those obtained under uncorrelated rates within cohorts (changes of minus13 to 16 in pooled rates and minus57 to 76 in standard errors) All models were fitted through restricted maximum likelihood methods with unstructured between cohort covariance matrix with the R package mvmeta (R Foundation for Statistical Computing) The estimated between cohort correlations in the underlying rates in and out of treat-ment were 093 for all cause mortality and 081 for over-dose mortality with no estimation problems in any model regarding between cohort correlations at the boundary of the parameter space of 1
Patient involvementNo patients were involved in setting the research ques-tion or outcome measures nor were they involved in developing plans for design or implementation of the study No patients were asked to advise on interpreta-tion or writing up on results There are no plans to disseminate the results of the research to study partici-pants or the relevant patient community
Resultsstudy characteristicsOf the 2033 distinct records identified through the search we selected 19 cohort studies reported in 20 arti-cles6-10 24-38 (two articles27 28 reported different mortality outcomes from the same cohort) that met the inclusion criteria and provided mortality data in people with opi-oid dependence during and after opioid substitution treatment (fig 1 ) Tables 1 and 2 show the main charac-teristics of selected cohorts The studies were published between 1974 and 2016 and were all carried out in high income countries 11 in EuropeIsrael four in North America and four in Australia There were mixed base-line prevalences of opioid injection and HIV infection except four cohorts that enrolled only opioid injectors two of them further restricted to patients positive for HIV All but four cohorts included patients with concur-rent use of non-opioid drugs with limited information
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
4
on psychiatric and medical comorbidities More than 70 of participants were men and the mean age at baseline ranged from 234 to 396 (table 1)
Methadone was prescribed in 18 cohorts including 122 885 participants over the period 1965-2010 and buprenorphine was used in three cohorts including 15 831 participants over 1990-2010 (table 2) The average daily dose ranged from 47 mg to 116 mg of methadone and 10 mg to 12 mg of buprenorphine Treatment was initiated on an ambulatory basis in all recent cohorts and provided by addiction medicine specialists in 11 cohorts and general practitioners or mixed staff in eight cohorts The average follow-up after initiation varied between 13 and 139 years for methadone and 11 and 45 years for buprenorphine with loss to follow-up exceeding 10 in only four cohorts All cause mortality during follow-up periods in and out of treatment was reported in all but two methadone cohorts and over-dose mortality in 11 methadone cohorts and one buprenorphine cohort Most studies were of moderate quality They ranged from 3 to 13 points on a 16 point scale with a median of 8 points
all cause mortality during and after opioid substitution treatmentAll cause mortality rates varied widely across the 16 methadone cohorts (overall I2=98 Plt0001) although rates were consistently higher out of treatment than in treatment (fig 2 ) The pooled all cause mortality rates were 113 and 361 deaths per 1000 person years in and out of methadone treatment respectively with an unadjusted pooled rate difference for periods out and in treatment of 249 deaths (95 confidence interval 136 to 361) per 1000 person years and an unadjusted pooled rate ratio of 320 (265 to 386) In heterogeneity analyses (table 3) the pooled all cause mortality rates in and out of methadone treatment were significantly higher in studies that mostly enrolled opioid injectors who were positive for HIV than in studies including
both injectors and non-injectors and marginally higher in studies conducted in Europe and North America than in Australia
The pooled all cause mortality rates in the three buprenorphine cohorts were 43 and 95 deaths per 1000 person years in and out of treatment respectively (fig 2) The unadjusted pooled rate difference for peri-ods out and in treatment was 52 deaths (95 confi-dence interval minus10 to 114) per 1000 person years and the unadjusted pooled rate ratio was 220 (134 to 361)
After we removed each individual cohort the pooled all cause mortality rates ranged from 106 to 119 deaths per 1000 person years in methadone treatment and from 325 to 391 deaths per 1000 person years out of methadone treatment With buprenorphine treatment these figures were 33 to 56 deaths and 77 to 123 deaths per 1000 person years respectively There was some evidence of small study effects on all cause mortality (P=005) with higher rates in small cohorts that mostly enrolled opioid injectors who were positive for HIV (table 1 and fig 2)
Five methadone cohorts and one buprenorphine cohort reported all cause mortality rate ratios for peri-ods out of and in treatment with various degrees of adjustment for patient demographics severity of drug use treatment delivery and comorbidity (table 4) After adjustment out-to-in rate ratios remained unchanged in two methadone cohorts and increased by 155-355 in the other three methadone cohorts and by 168 in the buprenorphine cohort
Overdose mortality during and after opioid substitution treatmentThe pooled overdose mortality rates across the 11 meth-adone cohorts were 26 and 127 overdose deaths per 1000 person years in and out of methadone treatment respectively (fig 3) with an unadjusted pooled rate dif-ference comparing periods out and in treatment of 100 overdose deaths (95 confidence interval 26 to 174) per 1000 person years and an unadjusted pooled rate ratio of 480 (290 to 796) There was moderate heterogeneity between studies in mortality rates in treatment (I2=66 P=0001) and strong heterogeneity in rates out of treat-ment (I2=97 Plt0001) with significantly higher rates out of treatment among methadone patients in specialist services than in primary care (table 3 ) In the single buprenorphine cohort there were 14 and 46 fatal overdoses per 1000 person years in and out of treatment (fig 3)
After we removed each methadone cohort the pooled overdose mortality rates varied between 24 and 28 fatal overdoses per 1000 person years in methadone treatment and between 106 and 149 fatal overdoses per 1000 person years out of treatment There was no evi-dence of publication bias or other small study effects on overdose mortality (P=014) Adjustment for potential confounders did not produce any change in overdose mortality rate ratios for periods out compared with in treatment in three methadone cohorts but resulted in 258 and 286 larger rate ratios in two other metha-done cohorts (table 4)
Distinct records identied (n=2033) Medline (n=1215) Embase (n=729) PsycINFO (n=486)
Full text articles retrieved and assessed for eligibility (n=328)
Articles included in meta-analysis (n=20)
LILACS (n=182)Other searches (n=102)
Records excluded aer title and abstract review (n=1705) No data in humans (n=120) No original research (n=126) Design other than observational cohort (n=462) Not focused on opioid dependent people (n=997)
Articles excluded (n=308) Imprisoned or recently released population (n=22) Treatment unknown or other than methadone or buprenorphine maintenance (n=133) No all cause or overdose mortality as outcome (n=44) Insucient data to compute mortality rates during follow-up periods in and out of treatment (n=72) Secondary publication (n=37)
Fig 1 | selection process of cohort studies on mortality among people receiving opioid substitution treatment
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
5
all cause mortality by time interval in and out of treatmentSix recent methadone cohorts provided all cause mortal-ity data disaggregated by time interval in and out of treat-ment (fig 4) After we excluded a selective high risk cohort of injectors who were HIV positive and received highly active antiretroviral therapy the pooled all cause mortal-ity rates were 114 and 58 deaths per 1000 person years in the first four weeks and the remaining time on metha-done treatment respectively with an unadjusted pooled rate difference for initial compared with subsequent treat-ment periods of 56 deaths (95 confidence interval minus24 to 136) per 1000 person years and an unadjusted pooled rate ratio of 197 (094 to 410) Similarly the pooled all cause mortality dropped from 321 deaths per 1000 person years in the first four weeks after stopping methadone treatment to 135 deaths per 1000 person years thereafter resulting in an unadjusted pooled rate difference for ini-tial compared with subsequent periods out of treatment of 186 deaths (29 to 343) per 1000 person years and an unadjusted pooled rate ratio of 238 (151 to 374)
In continuous time trend analysis (fig 5) there were significant departures from linearity in trends in all cause mortality risk over time in and out of methadone treatment (P=004) The pooled all cause mortality rates decreased sharply from 374 to 64 deaths per 1000 per-son years throughout the initial four weeks of metha-done treatment and were fairly stable thereafter In contrast after people left methadone treatment the pooled all cause mortality remained high at between 241 and 352 deaths per 1000 person years during the initial two weeks out of treatment and decreased pro-gressively afterwards
In the two buprenorphine cohorts reporting disaggre-gated data the pooled all cause mortality remained equally low at 45 deaths per 1000 person years during and after the first four weeks of buprenorphine treat-ment (fig 4) The pooled all cause mortality however increased to 320 deaths per 1000 person years in the first four weeks after people stopped buprenorphine treatment and reduced thereafter to 109 deaths per 1000 person years with an unadjusted pooled rate dif-ference for initial compared with subsequent periods out of treatment of 212 deaths (95 confidence interval minus59 to 482) per 1000 person years and an unadjusted pooled rate ratio of 294 (134 to 646)
Overdose mortality by time interval in and out of treatmentOnly three methadone cohorts and one buprenorphine cohort reported overdose mortality by time interval (fig 6) The pooled overdose mortality rates were 35 and 20 overdose deaths per 1000 person years in the first four weeks and the rest of time on methadone treatment and 42 and 34 overdose deaths per 1000 person years during and after the first four weeks out of treatment In the single buprenorphine cohort there were 09 and 15 fatal overdoses per 1000 person years before and after the first four weeks on buprenorphine treatment and 108 and 42 fatal overdoses per 1000 person years before and after four weeks out of treatment respectivelyta
ble
1 | b
asel
ine
popu
latio
n ch
arac
teris
tics o
f coh
ort s
tudi
es o
n m
orta
lity r
isk
in p
eopl
e w
ith o
pioi
d de
pend
ence
dur
ing
and
after
opi
oid
subs
titut
ion
treat
men
t
stud
ylo
catio
nPo
pula
tion
Opi
oid
in
ject
ors
()
non-
opio
id
drug
use
()
hiv
po
sitiv
e (
)Ps
ychi
atric
co
mor
bidi
ty (
)M
edic
al
com
orbi
dity
()
Men
()
base
line
mea
n ag
e (y
ears
)M
etha
done
Gear
ing
1974
24Ne
w Yo
rk U
SHe
roin
dep
ende
ntNA
84
00
00
NA79
030
0Cu
shm
an 1
97725
New
York
US
Opio
id d
epen
dent
NANA
00
29
274
730
385
Groumln
blad
h 19
9026
Natio
nwid
e S
wed
enHe
roin
dep
ende
ntNA
00
00
NANA
783
275
Capl
ehor
n 19
9427
1996
28Pa
rram
atta
NSW
Aus
tralia
Hero
in d
epen
dent
NANA
00
NANA
720
234
Fuge
lsta
d 19
9529
Stoc
khol
m S
wed
enHI
V po
sitiv
e in
ject
ing
opio
id d
epen
dent
100
00
010
00
NANA
NA31
8Fu
gels
tad
1998
30St
ockh
olm
Sw
eden
Non
volu
ntar
ily tr
eate
d in
ject
ing
hero
in d
epen
dent
100
00
067
938
698
250
029
3
Bust
er 2
0027
Amst
erda
m N
ethe
rland
sOp
ioid
dep
ende
nt34
7NA
NANA
NA77
032
6Sc
herb
aum
200
231St
ate-
wid
e N
orth
Rhi
ne-W
estp
halia
Ger
man
yIn
ject
ing
opio
id d
epen
dent
100
0NA
NA70
0NA
780
320
Davo
li 2
00732
Natio
nwid
e It
aly
Hero
in d
epen
dent
720
NA8
013
0NA
800
315
Fuge
lsta
d 2
00733
Stoc
khol
m S
wed
enHe
roin
dep
ende
ntNA
00
275
NANA
NA38
2Cl
ause
n 2
00834
Natio
nwid
e N
orw
ayOp
ioid
dep
ende
nt92
5NA
35
NANA
676
396
Dege
nhar
dt 2
0096
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA64
829
6Co
rnis
h 2
0108
Natio
nwid
e U
KOp
ioid
dep
ende
ntNA
NANA
NA17
569
330
1Pe
les
201
035Te
l Avi
v Is
rael
Opio
id d
epen
dent
NA67
58
441
6NA
736
376
Evan
s 2
0159
Stat
e-w
ide
CA
US
Opio
id d
epen
dent
552
219
NA23
119
064
235
3Ki
mbe
r 20
1510
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA65
833
4No
syk
201
536St
ate-
wid
e B
C C
anad
aHA
ART
treat
ed H
IV p
ositi
ve in
ject
ing
opio
id d
epen
dent
100
0NA
100
0NA
333
667
360
Cous
ins
201
637Na
tionw
ide
Irel
and
Opio
id d
epen
dent
NANA
NA22
822
068
730
5bu
pren
orph
ine
Corn
ish
201
08Na
tionw
ide
UK
Opio
id d
epen
dent
NANA
NANA
175
693
301
Reec
e 2
01038
Bris
bane
Que
ensl
and
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA73
030
5Ki
mbe
r 20
1510
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA70
732
5NA
=not
ava
ilabl
e H
AART
=hig
hly a
ctiv
e an
tiret
rovi
ral t
hera
py
Opi
oid
subs
titut
ion
treat
men
t with
eith
er m
etha
done
or b
upre
norp
hine
exc
ept f
or C
laus
en e
t al34
in w
hich
abo
ut 9
3 o
f par
ticip
ants
use
d m
etha
done
and
onl
y 7
use
d bu
pren
orph
ine
durin
g st
udy p
erio
d
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
6
tabl
e 2
| tre
atm
ent d
eliv
ery a
nd fo
llow
-up
feat
ures
of c
ohor
t stu
dies
on
mor
talit
y ris
k in
peo
ple
with
opi
oid
depe
nden
ce d
urin
g an
d aft
er o
pioi
d su
bstit
utio
n tre
atm
ent
stud
yno
of c
ohor
t pa
rtic
ipan
tsdagger
aver
age
Ost
do
se (m
gda
y)in
patie
nt
indu
ctio
n (
)O
st
prov
ider
Follo
w-u
p pe
riod
aver
age
follo
w-u
p (y
ears
)Dagger
loss
to
follo
w-u
p (
)sectM
orta
lity
outc
ome
Qua
lity
scor
epara
Met
hado
neGe
arin
g 19
7424
3000
100
176
Spec
ialis
t19
65-7
25
24
0Al
l cau
ses
ove
rdos
e9
Cush
man
197
72554
710
0NA
Spec
ialis
t19
66-7
53
623
2Al
l cau
ses
ove
rdos
e6
Groumln
blad
h 19
9026
166
7510
00
Spec
ialis
t19
67-8
711
00
0Al
l cau
ses
ove
rdos
e4
Capl
ehor
n 19
9427
1996
2830
511
632
3Sp
ecia
list
1970
-90
139
144
All c
ause
s27
ove
rdos
e286
Fuge
lsta
d 19
9529
135
NA10
00
Spec
ialis
t19
86-9
02
10
0Al
l cau
ses
6Fu
gels
tad
1998
3056
8010
00
Spec
ialis
t19
86-9
34
20
0Al
l cau
ses
6Bu
ster
200
2752
0048
00
Mix
ed19
86-9
85
70
0O
verd
ose
8Sc
herb
aum
200
23124
447
00
Spec
ialis
t19
88-9
65
315
6Al
l cau
ses
ove
rdos
e7
Davo
li 2
00732
5276
NA0
0Sp
ecia
list
1998
-200
11
33
7O
verd
ose
11Fu
gels
tad
200
73367
9NA
100
0Sp
ecia
list
1988
-200
06
96
2Al
l cau
ses
3Cl
ause
n 2
00834
3229
112
00
Mix
ed19
97-2
003
24
00
All c
ause
s o
verd
ose
7De
genh
ardt
200
9631
846
700
0M
ixed
1985
-200
0daggerdagger6
80
0Al
l cau
sesDaggerDagger
12Co
rnis
h 2
0108
4894
500
0GP
1990
-200
519
175
All c
ause
s9
Pele
s 2
01035
613
113
00
Spec
ialis
t19
93-2
008
770
8Al
l cau
ses
ove
rdos
e9
Evan
s 2
0159
32 32
2NA
00
Spec
ialis
t20
06-1
02
35
0Al
l cau
sesDaggerDagger
12Ki
mbe
r 20
1510
26 0
6470
00
Mix
ed20
01-1
05
30
0Al
l cau
ses
ove
rdos
e13
Nosy
k 2
01536
1326
NA0
0GP
1996
-201
04
279
All c
ause
sDaggerDagger13
Cous
ins
201
63769
8372
00
GP20
04-1
04
12
0Al
l cau
ses
ove
rdos
e12
bupr
enor
phin
eCo
rnis
h 2
0108
1373
100
0GP
1990
-200
511
103
All c
ause
s9
Reec
e 2
01038
2518
NA0
0GP
2000
-07
32
12Al
l cau
ses
5Ki
mbe
r 20
1510
11 94
012
00
Mix
ed20
01-1
04
50
0Al
l cau
ses
ove
rdos
e13
NA=n
ot a
vaila
ble
OST
=opi
oid
subs
titut
ion
treat
men
tO
pioi
d su
bstit
utio
n tre
atm
ent w
ith e
ither
met
hado
ne o
r bup
reno
rphi
ne e
xcep
t for
Cla
usen
et a
l34 in
whi
ch a
bout
93
of p
artic
ipan
ts u
sed
met
hado
ne a
nd o
nly 7
u
sed
bupr
enor
phin
e du
ring
stud
y per
iod
daggerPar
ticip
ants
rece
ivin
g op
ioid
sub
stitu
tion
treat
men
t at l
east
onc
e du
ring
stud
y per
iod
Unt
reat
ed p
artic
ipan
ts a
nd th
ose
rece
ivin
g ot
her t
ypes
of t
reat
men
t for
opi
oid
depe
nden
ce (m
etha
done
det
oxifi
catio
n o
pioi
d an
tago
nist
ther
apy
ther
apeu
tic
com
mun
ity) e
xclu
ded
from
met
a-an
alys
is
DaggerAve
rage
follo
w-u
p fro
m s
tart
of o
pioi
d su
bstit
utio
n tre
atm
ent c
ombi
ning
sub
sequ
ent p
erio
ds in
and
out
of t
reat
men
tsectP
erce
ntag
e lo
ss to
follo
w-u
p be
fore
end
of s
tudy
per
iod
or d
eath
If n
ot o
ther
wis
e sp
ecifi
ed c
ompl
ete
case
asc
erta
inm
ent a
ssum
ed fo
r stu
dies
bas
ed o
n po
pula
tion
mor
talit
y reg
istri
es
paraQua
lity a
sses
smen
t sco
re ra
ngin
g fro
m 0
(low
est q
ualit
y) to
16 (h
ighe
st q
ualit
y)
O
verd
ose
mor
talit
y rep
orte
d bu
t not
incl
uded
in m
eta-
anal
ysis
as t
here
wer
e no
ove
rdos
e de
aths
whi
le p
artic
ipan
ts w
ere
in o
pioi
d su
bstit
utio
n tre
atm
ent
daggerdaggerFo
llow
-up
rest
ricte
d to
1985
-200
0 as
sub
sequ
ent 2
001-
06 fo
llow
-up
perio
d ov
erla
pped
with
Kim
ber e
t al10
DaggerDaggerO
verd
ose
mor
talit
y rep
orte
d on
ly fo
r com
bine
d tre
atm
ents
or i
nclu
ded
untre
ated
par
ticip
ants
and
hen
ce n
ot in
clud
ed in
met
a-an
alys
is
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
7
discussionMain findingsOur review suggests that time spent in opioid substitu-tion treatment with methadone is associated with an average reduction of 25 deaths1000 person years (95 confidence interval 14 to 36) The rate in treatment was less than a third of the rate out of treatment with the greatest difference in deaths from overdose The all cause mortality risk during treatment is much higher in the first four weeks than in the remainder of treatment Mortality risk is also higher in the first four weeks after cessation than in the remainder time out of treatment
Based on three cohorts (two from Australia) findings also suggest that opioid substitution treatment with buprenorphine could be associated with a reduction in mortality with a similar risk across all time in treatment (about four deaths1000 person years) consistent with its safety profile39-44 and a risk after cessation higher in the first four weeks than in the remainder of time out of treatment (32 versus 11 deaths1000 person years)
Mortality risk during specific periods in and out of methadone treatmentThe larger relative effect size (as measured by rate ratio) for overdose than non-overdose deaths with metha-done substitution6 11 34 45 is consistent with previous findings although the effect on non-overdose deaths had not been previously reviewed This disparity is
consistent with what would be expected given metha-donersquos effect on reducing use of heroin and other illicit opioids32 34
Our finding that the first four weeks after onset (114 deaths1000 person years) and cessation (3211000 person years) of methadone treatment are the highest risk periods suggests that these are key periods during which to focus efforts for prevention of drug related deaths Moreover within periods of methadone treat-ment there is a swift decline in risk from first to fourth week followed by a stable trend whereas after cessa-tion there is a high but quite stable risk during the first four weeks and a progressive decline afterward This is important because some patients cycle in and out of opioid substitution treatment46-50 and are therefore exposed to repeated periods of high risk for mortality Such changes probably mainly reflect changes in risk of fatal overdose6 32 but this has not been accurately assessed because only two cohorts reported overdose data specifically7 10 The increased risk during the first few weeks of treatment could be explained by an accu-mulation of methadone that exceeds the opioid toler-ance level (the mean elimination half life for methadone is 22 hours)51 as opioid tolerance does not seem to fully protect against respiratory depression52 Psychological factors and concomitant use of other respiratory depressant drugs or cocaine could also play a role7 8 40 53 54
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1994 Fugelstad et al 1995 Fugelstad et al 1998 Scherbaum et al 2002 Fugelstad et al 2007 Clausen et al 2008 Degenhardt et al 2009 Cornish et al 2010 Peles et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine Cornish et al 2010 Reece 2010 Kimber et al 2015Overall
2 5 10 20 50 100 200
11014 474251655161085111975
82427177
181114773354906450
648111 538305129423985
16325 27763691 792
89397911522 648
774031119
8721 936
In treatment
3311701429732740
362279545457
14172741311461303
1510105 73571428852727
84848 12256345 2652061582986247
10751406911
31431 239
Out of treatment
No of deathsperson years
76 (62 to 92)151 (98 to 223)148 (84 to 239)56 (28 to 100)
331 (143 to 651)395 (159 to 814)162 (96 to 255)
230 (181 to 287)140 (112 to 171)
58 (54 to 63)58 (40 to 83)
105 (76 to 142)64 (55 to 75)69 (64 to 75)
224 (180 to 275)51 (42 to 61)
113 (84 to 152)
95 (38 to 195)27 (06 to 78)40 (32 to 49)43 (21 to 89)
In treatment
282 (194 to 396)471 (258 to 791)432 (296 to 610)158 (111 to 219)
1111 (361 to 2593)699 (191 to 1790)814 (445 to 1366)565 (443 to 709)353 (259 to 471)143 (136 to 150)166 (129 to 209)715 (534 to 938)176 (165 to 188)124 (114 to 135)
1302 (1130 to 1493)157 (127 to 191)361 (245 to 533)
133 (64 to 245)58 (41 to 79)
101 (90 to 112)95 (39 to 234)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 2 | all cause mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled all cause mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates during periods in and out of treatment across all methadone or buprenorphine cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
8
tabl
e 3
| Poo
led
all c
ause
and
ove
rdos
e m
orta
lity r
ates
dur
ing
perio
ds in
and
out
of o
pioi
d su
bstit
utio
n tre
atm
ent w
ith m
etha
done
by s
tudy
char
acte
ristic
s
stud
y ch
arac
teris
tic
all c
ause
mor
talit
y ra
te1
000
pers
on y
ears
(95
Ci)
Ove
rdos
e m
orta
lity
rate
100
0 pe
rson
yea
rs (9
5 C
i)
no o
f st
udie
sin
trea
tmen
tO
ut o
f tre
atm
ent
P va
luedagger
i2 (
)Daggerno
of
stud
ies
in tr
eatm
ent
Out
of t
reat
men
tP
valu
edaggeri2 (
)Dagger
Loca
tion
E
urop
eIs
rael
913
9 (9
5 to
20
5)46
6 (2
90
to 74
9)
008
987
31
(24
to 4
0)
133
(59
to 2
98)
013
93
Nor
th A
mer
ica
411
2 (6
4 to
196
)42
3 (2
12 to
84
6)2
23
(14
to 3
8)
205
(44
to 9
45)
A
ustra
lia3
63
(33
to 12
1)14
0 (6
3 to
30
8)2
20
(14
to 2
9)
67
(15
to 2
96)
Opio
id in
ject
ors (
)
lt
100
129
0 (6
9 to
117
)25
8 (1
87
to 3
55)
000
195
102
5 (2
0 to
30
)10
6 (6
1 to
185
)mdash
mdash
100
423
4 (1
42
to 3
85)
109
9 (5
94
to 2
034
)1
mdashsect
mdashsect
Men
()
lt
7511
95
(69
to 13
2)
300
(18
4 to
48
8)0
6798
62
4 (1
8 to
34
)10
6 (4
5 to
24
8)0
7493
ge
753
116
(61
to 2
20)
459
(178
to 11
79)
52
9 (2
0 to
42
)15
8 (6
2 to
40
3)M
ean
age
(yea
rs)
lt
3510
99
(68
to 14
5)
293
(179
to 4
82)
040
988
26
(19
to 3
5)
106
(52
to 2
18)
060
93
ge35
614
0 (8
7 to
22
7)50
3 (2
68
to 9
43)
32
7 (1
5 to
47
)20
5 (6
2 to
676
)Av
erag
e m
etha
done
dos
e (m
gda
y)
le
807
96
(63
to 14
8)
269
(15
5 to
46
5)0
5692
53
1 (2
0 to
46
)10
3 (4
0 to
26
9)0
2293
gt
805
99
(60
to 16
5)
354
(18
5 to
677
)5
25
(16
to 3
9)
170
(65
to 4
49)
Inpa
tient
indu
ctio
n (
)
09
92
(63
to 13
6)
299
(173
to 5
16)
019
987
25
(18
to 3
4)
100
(45
to 2
23)
065
93
gt0
615
4 (9
3 to
25
3)45
9 (2
29
to 9
21)
32
9 (1
7 to
50
)18
4 (5
4 to
62
5)Tr
eatm
ent p
rovi
der
S
peci
alis
t10
134
(92
to 19
5)
465
(28
2 to
765
)0
2698
72
5 (1
7 to
37
)20
8 (1
11 to
38
8)0
0188
G
Pm
ixed
68
6 (5
4 to
137
)24
4 (1
31
to 4
54)
42
4 (1
6 to
36
)5
6 (2
5 to
125
)M
idpo
int f
ollo
w-u
p pe
riod
lt
2000
1012
6 (8
5 to
187
)38
8 (2
28
to 6
61)
058
987
28
(20
to 3
9)
154
(70
to 3
39)
067
93
ge20
006
97
(60
to 15
9)
320
(16
5 to
62
3)4
24
(17
to 3
5)
90
(32
to 2
52)
Loss
to fo
llow
-up
()
lt
1012
119
(83
to 1
70)
383
(23
7 to
619
)0
8198
82
5 (1
9 to
32
)9
8 (5
0 to
195
)0
3393
ge
104
95
(50
to 18
0)
313
(13
5 to
72
3)3
32
(17
to 6
0)
254
(81
to 7
94)
Poo
led
mor
talit
y rat
es a
nd 9
5 c
onfid
ence
inte
rval
s dur
ing
perio
ds in
and
out
of t
reat
men
t by s
tudy
cha
ract
eris
tics e
stim
ated
from
sep
arat
e bi
varia
te ra
ndom
effe
cts m
eta-
regr
essi
on m
odel
s rel
atin
g lo
g tra
nsfo
rmed
rate
s in
both
trea
tmen
t per
iods
w
ith e
ach
stud
y cha
ract
eris
tic
daggerOve
rall
P va
lue
for h
eter
ogen
eity
of p
oole
d m
orta
lity r
ates
acr
oss c
ateg
orie
s of s
tudy
cha
ract
eris
tic a
s obt
aine
d fro
m li
kelih
ood
ratio
test
com
parin
g ne
sted
met
a-re
gres
sion
mod
els w
ith a
nd w
ithou
t stu
dy c
hara
cter
istic
fitte
d vi
a m
axim
um li
kelih
ood
DaggerOve
rall
I2 sta
tistic
for r
esid
ual h
eter
ogen
eity
in s
tudy
spe
cific
mor
talit
y rat
es n
ot e
xpla
ined
by c
orre
spon
ding
stu
dy c
hara
cter
istic
sectP
oole
d m
orta
lity r
ates
not
app
licab
le to
cat
egor
ies w
ith s
ingl
e st
udy
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
9
Although the long half life of methadone could con-tribute to the increase in mortality in the first three to four days after cessation of treatment there was a large increase in mortality across the first four weeks after cessation compared with the treatment period Such increased mortality could be explained by loss of toler-ance to the toxic effects of heroin assuming that many patients return to use6 8 32 47 55 56 and probably also by the use of multiple legal and illicit substances during that period Similar peaks in drug related mortality occur in other situations where opioid tolerance is prob-ably diminished (for example after prison release or hospital discharge57-59 ) Lifestyle factors and comorbid issues such as mental health problems could also increase mortality from other external causes as deaths from suicide and injury are also more common during that period53
Mortality risk during specific periods in and out of buprenorphine treatmentData from three cohorts (two from Australia) suggest that substitution treatment with buprenorphine could reduce all cause mortality although the disparity in mortality rates in periods in and out of treatment did not reach significance Findings also suggest a signifi-cantly increased mortality in the first four weeks after cessation of treatment compared with the remaining time out of treatment (320 versus 1091000 person years) while during the treatment period there was no difference between the first four weeks and the remain-ing time in treatment It is difficult to draw firm conclu-sions because of limited evidence from similar settings 96 of included deaths and 98 of person years came from Australian studies (with 87 and 86 from the study by Kimber and colleagues13)
Comparative effectiveness of buprenorphine and methadone substitution treatmentOther sources of data have suggested that buprenor-phine could be more effective than methadone in reduc-ing mortality especially from overdose39 42 43 Unlike methadone there is a ceiling for respiratory depressant effects of buprenorphine as dose increases and the probability of triggering arrhythmias is lower for buprenorphine than methadone41 44 60 When we com-pared the mortality between periods in and out of treat-ment first within those taking methadone and then within those taking buprenorphine we found a greater reduction in mortality with methadone than with buprenorphine (measured as the rate difference or rate ratio between periods) When we compared mortality between them first within the treatment period and then in the period off treatment we found a signifi-cantly lower mortality with buprenorphine than meth-adone in both periods
Our conclusions must remain tentative until further studies in varied treatment settings and contexts are undertaken to examine this issue Differences in mor-tality might also reflect confounding through differ-ences in characteristics of patients (such as age severity of opioid dependence injecting drug use other ta
ble
4 | C
ohor
t stu
dies
repo
rtin
g al
l cau
se a
nd o
verd
ose
mor
talit
y rat
e ra
tios c
ompa
ring
perio
ds o
ut a
nd in
opi
oid
subs
titut
ion
treat
men
t adj
uste
d fo
r con
foun
ding
stud
y
Conf
ound
ing
fact
ors
all c
ause
mor
talit
yO
verd
ose
mor
talit
y
Patie
nt d
emog
raph
ics
seve
rity
of d
rug
use
trea
tmen
tCo
mor
bidi
tyun
adju
sted
ra
te ra
tioad
just
ed
rate
ratio
Perc
enta
ge
chan
gedagger
unad
just
ed
rate
ratio
adju
sted
ra
te ra
tioPe
rcen
tage
ch
ange
dagger
Met
hado
neBu
ster
200
27Se
x ra
ceTr
eatm
ent m
odal
ity t
ime
sinc
e fir
st tr
eatm
ent
mdashmdash
mdashmdash
087
087
minus03
Davo
li 2
00732
Age
sex
Leng
th o
f her
oin
use
her
oin
inje
ctio
n
prev
ious
ove
rdos
eHI
V p
sych
iatri
c com
orbi
dity
mdashmdash
mdash77
174
3minus3
6
Dege
nhar
dt 2
0096
Age
sex
cal
enda
r yea
rmdash
mdash19
118
8minus1
3mdash
mdashmdash
Corn
ish
201
08Ag
e s
ex c
alen
dar y
ear
mdashM
edic
al c
omor
bidi
ty2
833
2715
5mdash
mdashmdash
Evan
s 2
0159Dagger
Age
sex
rac
e e
duca
tion
em
ploy
men
t cr
imin
ality
hea
lth c
over
age
Prim
ary o
pioi
d fr
eque
ncy a
nd le
ngth
of
opio
id u
se n
on-o
pioi
d dr
ug u
seHI
V h
epat
itis C
tub
ercu
losi
s
disa
bilit
y m
edic
al c
omor
bidi
ty
psyc
hiat
ric c
omor
bidi
ty
273
370
355
351
442
258
Nosy
k 2
01536
DaggerAg
e s
ex r
ace
cal
enda
r yea
r re
gion
No o
f pre
viou
s tre
atm
ent e
piso
des
Tim
e si
nce
HIV
diag
nosi
s C
D4
coun
t AI
DS a
ntire
trovi
ral
ther
apy
med
ical
com
orbi
dity
304
294
minus34
114
147
286
Cous
ins
201
637Ag
e s
exTr
eatm
ent s
uper
visi
on m
etha
done
dos
eM
edic
al c
omor
bidi
ty3
093
6417
816
016
317
bupr
enor
phin
eCo
rnis
h 2
0108
Age
sex
cal
enda
r yea
rmdash
Med
ical
com
orbi
dity
141
164
168
mdashmdash
mdashB
asel
ine
or ti
me
vary
ing
conf
ound
ing
fact
ors u
sed
in a
djus
tmen
tdaggerP
erce
ntag
e ch
ange
in ra
te ra
tio a
fter a
djus
tmen
t for
cor
resp
ondi
ng c
onfo
undi
ng fa
ctor
sDaggerO
verd
ose
mor
talit
y rat
e ra
tios r
epor
ted
com
bini
ng m
etha
done
mai
nten
ance
with
det
oxifi
catio
n (1
14
of p
erso
n ye
ars i
n tre
atm
ent)
in E
vans
et a
l9 an
d in
clud
ing
neve
r tre
ated
par
ticip
ants
(73
3 o
f per
son
year
s out
of t
reat
men
t) in
Nos
yk e
t al36
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
10
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1996 Buster et al 2002 Scherbaum et al 2002 Davoli et al 2007 Clausen et al 2008 Peles et al 2010 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine Kimber et al 2015
2105 5 10 20 50 100
3314 474416557108541792
4218 7476111475751
24645053985
16991 7925422 648
3121 936
In treatment
2111707297
27740192004
2610 983131729998
28130313727
21645 265246247
14331 239
Out of treatment
No of deathsperson years
23 (16 to 32)24 (07 to 62)
64 (26 to 133)22 (06 to 57)22 (16 to 30)
54 (20 to 117)12 (05 to 25)37 (24 to 55)12 (04 to 29)18 (16 to 21)24 (18 to 31)26 (21 to 33)
14 (10 to 20)
In treatment
179 (111 to 274)236 (95 to 486)
365 (240 to 531)95 (57 to 148)24 (16 to 35)
756 (402 to 1292)90 (41 to 171)
215 (143 to 311)179 (95 to 306)
48 (42 to 54)38 (25 to 57)
127 (69 to 234)
46 (39 to 54)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 3 | Overdose mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled overdose mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates during periods in and out of treatment across all methadone cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
Methadone rst four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallMethadone aer four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Cornish et al 2010 Kimber et al 2015OverallBuprenorphine aer four weeks Cornish et al 2010 Kimber et al 2015Overall
21 5 10 20 50 100
9425057465
151950323344
4100153371
554109 033234664
14823 32760488 449
85388010019 277
18192094
66597819 842
In treatment
38189821479
154267335183679113
441181
1472103 838503809
69445 44952843 4301271469545067
788281674
366328629 565
Out of treatment
No of deathsperson years
375 (303 to 459)151 (61 to 311)77 (43 to 127)96 (66 to 135)
mdash44 (25 to 73)
114 (58 to 224)
51 (47 to 55)49 (31 to 74)63 (54 to 74)68 (63 to 74)
mdash52 (42 to 63)58 (50 to 67)
124 (03 to 692)43 (20 to 82)
45 (12 to 168)
91 (33 to 198)39 (31 to 49)45 (32 to 62)
In treatment
200 (142 to 275)438 (271 to 670)576 (489 to 675)191 (133 to 265)
mdash373 (271 to 500)321 (191 to 539)
142 (135 to 149)131 (97 to 173)
153 (141 to 164)122 (111 to 132)
mdash107 (80 to 139)
135 (119 to 153)
800 (322 to 1648)167 (111 to 242)320 (132 to 775)
45 (09 to 132)97 (86 to 109)
109 (85 to 139)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 4 | all cause mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled all cause mortality rates 2009-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except Degenhardt et al6 which reported mortality before and after two weeks of treatment initiation and cessation high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-analysis area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates before and after four weeks in and out of treatment across methadone or buprenorphine cohorts estimated from multivariate random effects meta-analysis on log transformed rates in four time-by-treatment intervals
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
11
drug use comorbidities prison history overdose his-tory patientrsquos preference) characteristics of treatment (such as previous treatment specialisation of the doc-tor who controls the treatment dose provision charac-teristics cointerventions retention or drop outs) or the sociopolitical context in which studies have been conducted For example the initial prognosis might be better in those given buprenorphine than those given methadone (that is fewer comorbid problems less severe opioid dependence)6 8 10 61 though this was not clearly found in a recent US study62
The role of such confounding factors has received almost empirical examination Few details on char-acteristics of patients or treatments were reported in articles included in this meta-analysis to permit a detailed examination of this potential issue (tables 1 and 2 ) so it was not possible to assess the possibil-ity of confounding A sensitivity simulation analysis in the study by Kimber and colleagues however suggested that the lower mortality with buprenor-phine than with methadone during first four weeks of treatment was unlikely to be caused by unmea-sured confounding10
strengths and limitationsThis meta-analysis synthesised evidence from cohort studies published until 2016 on risk of mortality in people who are dependent on opioids during and after opioid substitution treatment separately for buprenor-phine and methadone Mortality changes over time (1st-32th week) during and after methadone are care-fully quantified for the first time
The published studies however had several methodological shortcomings Firstly in the included
Methadone rst four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallMethadone aer four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Kimber et al 2015Buprenorphine aer four weeks Kimber et al 2015
21 505 10 20
9150018334443371
3317 20015188 4495019 277
22094
2919 842
In treatment
2130010183681181
24960020643 430
165067
181674
12529 565
Out of treatment
No of deathsperson years
60 (27 to 114)54 (32 to 85)12 (03 to 30)35 (13 to 95)
19 (13 to 27)17 (14 to 20)26 (19 to 34)20 (15 to 27)
09 (01 to 34)
15 (10 to 21)
In treatment
15 (02 to 56)54 (26 to 100)68 (29 to 134)42 (18 to 99)
25 (16 to 37)47 (41 to 54)32 (18 to 51)34 (23 to 51)
108 (64 to 170)
42 (35 to 50)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 6 | Overdose mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled overdose mortality rates 2002-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except buster et al7 which reported mortality before and after two weeks of treatment initiation and cessation area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates before and after four weeks in and out of treatment across methadone cohorts estimated from multivariate random-effects meta-analysis on log transformed rates in four time-by-treatment intervals
Time since treatment initiation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s In methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Time since treatment cessation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s Out of methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Degenhardt et al 2009Cornish et al 2010Evans et al 2015Kimber et al 2015Cousins et al 2016
Fig 5 | all cause mortality rates by time since treatment initiation and cessation in methadone cohorts and pooled all cause mortality risk trends 2009-16 high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-regression area of each circle is proportional to weight of each time interval in meta-regression Pooled trends in all cause mortality risk (solid lines) and their 95 confidence intervals (shaded regions) over time in and out of methadone treatment were estimated from bivariate random effects meta-regression of log transformed rates on quadratic linear spline function of log time with knot at four weeks
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
12
observational studies the same patients are compared throughout follow-up periods in and out of opioid sub-stitution treatment but these patients leave and re-en-ter treatment in a non-random way and hence there could still be a large potential for confounding in com-parisons of crude mortality risk in and out of treat-ment In some studies with diverse information on patient demographics severity of drug use and comor-bidities measured mostly at baseline (table 3 ) adjust-ment for these potential confounders resulted in similar or even increased out-to-in mortality rate ratios which merely reflects that the above conditions tended to be less prevalent at baseline among patients who later left or were discharged from treatment than those who remained in treatment Nevertheless to obtain an unbiased estimate of the preventive effect of opioid substitution treatment on all cause and overdose mor-tality these and other relevant confounders should be measured every time a patient leaves and resumes treatment Time varying data can then be used to adjust for confounder history in standard regression models or even better to construct inverse probability of treatment weights for marginal structural models63 which properly control for time varying confounders for later treatment that are themselves affected by pre-vious treatment such as severity of drug use and comorbidity Also differential loss to follow-up is a concern in the meta-analysed cohorts as dropouts are more likely to occur in patients at higher risk of death during periods out of treatment thus inducing a selec-tion bias in crude comparisons of out-to-in mortality risk because of informative censoring Marginal struc-tural models with inverse probability of censoring weights can also be used to correct for differential loss to follow-up63 provided that common predictors of death and censoring are measured over time In sum-mary individual cohorts are prone to confounding and selection bias because of differential loss to follow-up but it is hard to assess with the available information the amount and direction of bias projected onto the pooled mortality rate differences and rate ratios between periods in and out of treatment obtained in this meta-analysis
Secondly studies were conducted in high income countries with the follow-up often spread over many calendar years (1965-2010 for methadone and 1990-2010 for buprenorphine) and a highly variable average length of follow-up (ranges 13-158 years and 11-45 years respectively) Studies in low and middle income countries are especially needed
Thirdly by design we have not captured overdose mortality when opioid substitution treatment was obtained on illicit drug markets40 64 Fourthly a delayed record of treatment cessation could have led to some deaths that occurred out of treatment being incorrectly classified as occurring in treatment40 if so this makes our estimated impact of opioid substitution treatment on mortality a conservative one There could similarly be misclassification between overdose and non-over-dose deaths because of inconsistencies in definition of overdose and codification of causes of deaths (for
instance criteria for separating overdose death from intentional poisoning or sudden cardiac death)40 65 again these misclassifications would tend to underesti-mate deaths from overdose
implications for policy and practiceIn many countries the number of deaths attributable to opioid use is substantial66 67 and increasing in some such as the US where deaths from opioid overdose now outnumber gun related deaths in the country68 Over-doses are preventable causes of death warranting wide implementation of preventive interventions Our review has provided evidence that methadone and probably buprenorphine reduce mortality among people depen-dent on opioids making it imperative that further research confirms this using study designs that con-sider a wide range of confounding variables to increase confidence that these effects are causal
It must be borne in mind that there is strong evidence of the efficacy of methadone and buprenorphine on a range of clinical outcomes and these medicines are listed as WHO essential medicines the findings we have presented here provide additional imperatives for their widespread availability Despite this coverage of opioid substitution treatment is low in many countries worldwide69 Policymakers clinicians and those responsible for drug treatment systems should work to ensure the availability of such treatment remove access barriers and promote engagement This means the strategic development of services from a public health perspective which could reduce the social harm associ-ated with opioid use
Our review suggests that some precautions should be taken during and after opioid substitution treatment to increase safety Firstly careful clinical assessment of opioid tolerance before onset of treatment to establish a safe induction dose seems warranted Secondly moni-toring during the induction period is important espe-cially for methadone with clinicians considering adjusting opioid doses monitoring mental and somatic problems and preventing the use of opioids obtained on the illicit drug market64 In addition education of patients about the risk of overdose risk and use of ldquotake homerdquo naloxone70 71 is warranted Buprenorphine induction followed by transition to methadone might also be considered10 72 Retention in opioid substitution treatment reduces risk of exposure to mortality after cessation and also to re-exposure to mortality risk during induction onto methadone so efforts to improve retention are important as a strategy to reduce mortal-ity More generally establishment of mechanisms for information and coordination between healthcare social and legal services and patient counselling while in treatment in addition to more specific overdose pre-vention programmes such as naloxone distribution should be considered
Finally there is a pressing need for new studies on the comparative effectiveness of methadone and buprenorphine in reducing mortality New ran-domised controlled trials are highly unlikely they would be prohibitively expensive and difficult to
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score

thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
3
and out of treatment by dividing the number of deaths registered in each period by the person years contrib-uted by all participants to that period If not explicitly reported we derived the number of person years by treatment period from the available summary statistics on follow-up and treatment retention or the reported mortality rates We computed exact 95 confidence intervals for the underlying mortality rates by assuming a Poisson distribution for the observed number of deaths and fixed person years at risk
Cause specific mortality rates in and out of treatment were jointly combined across all methadone or buprenorphine cohorts by using a bivariate random effects meta-analysis on log transformed mortality rates in both treatment periods17-19 This bivariate meta-ana-lytic approach allowed estimation of not only the pooled mortality rates and 95 confidence intervals in and out of treatment but also the pooled rate difference and rate ratio comparing periods out of and in treatment with confidence intervals that took into account the correlation between rates in both treatment periods
To evaluate whether cause specific mortality rates differed by baseline population characteristics treat-ment delivery and follow-up features of methadone cohorts we included the location (EuropeIsrael North America or Australia) prevalence of opioid injection (lt100 or 100) percentage of men (lt75 or ge75) mean age (lt35 or ge35) average methadone dose (le80 or gt80 mgday) percentage of inpatient induction (0 or gt0) treatment provider (specialist or general practitionermixed) midpoint follow-up period (lt2000 or ge2000) and percentage loss to follow-up (lt10 or ge10) in each methadone cohort as single predictors in separate bivariate random effects meta-regression models on log transformed mortality rates in and out of treatment17 18 We contrasted heterogeneity of pooled mortality rates by these cohort characteristics through likelihood ratio tests comparing nested meta-regression models with and without the predictor fitted through maximum like-lihood The limited number of buprenorphine cohorts precluded a similar heterogeneity analysis across these cohorts
For methadone or buprenorphine cohorts that reported mortality data by time interval in and out of treatment we combined cause specific mortality rates before and after four weeks of treatment initiation and cessation through a multivariate random effects meta-analysis on log transformed mortality rates in these time-by-treatment intervals To obtain pooled trends in all cause mortality risk over time in and out of methadone substitution treatment we fitted a bivariate random effects meta-regression of log transformed rates on a quadratic linear spline function of log time with knot at four weeks20 This quadratic linear spline allowed for a quadratic trend in the first four weeks in and out of treatment and forced the trend to be linear thereafter to avoid implausible shapes at long follow-up times The resulting pooled trends were virtually insensitive to different knot locations at three four or five weeks
We examined the overall heterogeneity in mortality rates across studies as well as the residual heterogene-ity beyond that explained by study level characteristics with the multivariate extension of the Cochran χ2 test and quantified it with the extended I2 statistic18 21 which described the proportion of total variation in study specific mortality rates because of heterogeneity The influence of each study on pooled estimates was evaluated by removal of each individual study from the analysis Publication bias and genuine small study effects were assessed with the extended Egger test allowing for heterogeneity22 23
In all the above multivariate random effects meta-an-alytic models we assumed the correlations within cohorts in the estimated mortality rates to be zero as they were obtained over different follow-up periods in and out of treatment Nevertheless we performed sen-sitivity analyses assuming positive within cohort cor-relations between mortality rates in and out of treatment of 025 050 075 and 095 for all studies and the pooled rates and their standard errors were virtually identical to those obtained under uncorrelated rates within cohorts (changes of minus13 to 16 in pooled rates and minus57 to 76 in standard errors) All models were fitted through restricted maximum likelihood methods with unstructured between cohort covariance matrix with the R package mvmeta (R Foundation for Statistical Computing) The estimated between cohort correlations in the underlying rates in and out of treat-ment were 093 for all cause mortality and 081 for over-dose mortality with no estimation problems in any model regarding between cohort correlations at the boundary of the parameter space of 1
Patient involvementNo patients were involved in setting the research ques-tion or outcome measures nor were they involved in developing plans for design or implementation of the study No patients were asked to advise on interpreta-tion or writing up on results There are no plans to disseminate the results of the research to study partici-pants or the relevant patient community
Resultsstudy characteristicsOf the 2033 distinct records identified through the search we selected 19 cohort studies reported in 20 arti-cles6-10 24-38 (two articles27 28 reported different mortality outcomes from the same cohort) that met the inclusion criteria and provided mortality data in people with opi-oid dependence during and after opioid substitution treatment (fig 1 ) Tables 1 and 2 show the main charac-teristics of selected cohorts The studies were published between 1974 and 2016 and were all carried out in high income countries 11 in EuropeIsrael four in North America and four in Australia There were mixed base-line prevalences of opioid injection and HIV infection except four cohorts that enrolled only opioid injectors two of them further restricted to patients positive for HIV All but four cohorts included patients with concur-rent use of non-opioid drugs with limited information
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
4
on psychiatric and medical comorbidities More than 70 of participants were men and the mean age at baseline ranged from 234 to 396 (table 1)
Methadone was prescribed in 18 cohorts including 122 885 participants over the period 1965-2010 and buprenorphine was used in three cohorts including 15 831 participants over 1990-2010 (table 2) The average daily dose ranged from 47 mg to 116 mg of methadone and 10 mg to 12 mg of buprenorphine Treatment was initiated on an ambulatory basis in all recent cohorts and provided by addiction medicine specialists in 11 cohorts and general practitioners or mixed staff in eight cohorts The average follow-up after initiation varied between 13 and 139 years for methadone and 11 and 45 years for buprenorphine with loss to follow-up exceeding 10 in only four cohorts All cause mortality during follow-up periods in and out of treatment was reported in all but two methadone cohorts and over-dose mortality in 11 methadone cohorts and one buprenorphine cohort Most studies were of moderate quality They ranged from 3 to 13 points on a 16 point scale with a median of 8 points
all cause mortality during and after opioid substitution treatmentAll cause mortality rates varied widely across the 16 methadone cohorts (overall I2=98 Plt0001) although rates were consistently higher out of treatment than in treatment (fig 2 ) The pooled all cause mortality rates were 113 and 361 deaths per 1000 person years in and out of methadone treatment respectively with an unadjusted pooled rate difference for periods out and in treatment of 249 deaths (95 confidence interval 136 to 361) per 1000 person years and an unadjusted pooled rate ratio of 320 (265 to 386) In heterogeneity analyses (table 3) the pooled all cause mortality rates in and out of methadone treatment were significantly higher in studies that mostly enrolled opioid injectors who were positive for HIV than in studies including
both injectors and non-injectors and marginally higher in studies conducted in Europe and North America than in Australia
The pooled all cause mortality rates in the three buprenorphine cohorts were 43 and 95 deaths per 1000 person years in and out of treatment respectively (fig 2) The unadjusted pooled rate difference for peri-ods out and in treatment was 52 deaths (95 confi-dence interval minus10 to 114) per 1000 person years and the unadjusted pooled rate ratio was 220 (134 to 361)
After we removed each individual cohort the pooled all cause mortality rates ranged from 106 to 119 deaths per 1000 person years in methadone treatment and from 325 to 391 deaths per 1000 person years out of methadone treatment With buprenorphine treatment these figures were 33 to 56 deaths and 77 to 123 deaths per 1000 person years respectively There was some evidence of small study effects on all cause mortality (P=005) with higher rates in small cohorts that mostly enrolled opioid injectors who were positive for HIV (table 1 and fig 2)
Five methadone cohorts and one buprenorphine cohort reported all cause mortality rate ratios for peri-ods out of and in treatment with various degrees of adjustment for patient demographics severity of drug use treatment delivery and comorbidity (table 4) After adjustment out-to-in rate ratios remained unchanged in two methadone cohorts and increased by 155-355 in the other three methadone cohorts and by 168 in the buprenorphine cohort
Overdose mortality during and after opioid substitution treatmentThe pooled overdose mortality rates across the 11 meth-adone cohorts were 26 and 127 overdose deaths per 1000 person years in and out of methadone treatment respectively (fig 3) with an unadjusted pooled rate dif-ference comparing periods out and in treatment of 100 overdose deaths (95 confidence interval 26 to 174) per 1000 person years and an unadjusted pooled rate ratio of 480 (290 to 796) There was moderate heterogeneity between studies in mortality rates in treatment (I2=66 P=0001) and strong heterogeneity in rates out of treat-ment (I2=97 Plt0001) with significantly higher rates out of treatment among methadone patients in specialist services than in primary care (table 3 ) In the single buprenorphine cohort there were 14 and 46 fatal overdoses per 1000 person years in and out of treatment (fig 3)
After we removed each methadone cohort the pooled overdose mortality rates varied between 24 and 28 fatal overdoses per 1000 person years in methadone treatment and between 106 and 149 fatal overdoses per 1000 person years out of treatment There was no evi-dence of publication bias or other small study effects on overdose mortality (P=014) Adjustment for potential confounders did not produce any change in overdose mortality rate ratios for periods out compared with in treatment in three methadone cohorts but resulted in 258 and 286 larger rate ratios in two other metha-done cohorts (table 4)
Distinct records identied (n=2033) Medline (n=1215) Embase (n=729) PsycINFO (n=486)
Full text articles retrieved and assessed for eligibility (n=328)
Articles included in meta-analysis (n=20)
LILACS (n=182)Other searches (n=102)
Records excluded aer title and abstract review (n=1705) No data in humans (n=120) No original research (n=126) Design other than observational cohort (n=462) Not focused on opioid dependent people (n=997)
Articles excluded (n=308) Imprisoned or recently released population (n=22) Treatment unknown or other than methadone or buprenorphine maintenance (n=133) No all cause or overdose mortality as outcome (n=44) Insucient data to compute mortality rates during follow-up periods in and out of treatment (n=72) Secondary publication (n=37)
Fig 1 | selection process of cohort studies on mortality among people receiving opioid substitution treatment
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
5
all cause mortality by time interval in and out of treatmentSix recent methadone cohorts provided all cause mortal-ity data disaggregated by time interval in and out of treat-ment (fig 4) After we excluded a selective high risk cohort of injectors who were HIV positive and received highly active antiretroviral therapy the pooled all cause mortal-ity rates were 114 and 58 deaths per 1000 person years in the first four weeks and the remaining time on metha-done treatment respectively with an unadjusted pooled rate difference for initial compared with subsequent treat-ment periods of 56 deaths (95 confidence interval minus24 to 136) per 1000 person years and an unadjusted pooled rate ratio of 197 (094 to 410) Similarly the pooled all cause mortality dropped from 321 deaths per 1000 person years in the first four weeks after stopping methadone treatment to 135 deaths per 1000 person years thereafter resulting in an unadjusted pooled rate difference for ini-tial compared with subsequent periods out of treatment of 186 deaths (29 to 343) per 1000 person years and an unadjusted pooled rate ratio of 238 (151 to 374)
In continuous time trend analysis (fig 5) there were significant departures from linearity in trends in all cause mortality risk over time in and out of methadone treatment (P=004) The pooled all cause mortality rates decreased sharply from 374 to 64 deaths per 1000 per-son years throughout the initial four weeks of metha-done treatment and were fairly stable thereafter In contrast after people left methadone treatment the pooled all cause mortality remained high at between 241 and 352 deaths per 1000 person years during the initial two weeks out of treatment and decreased pro-gressively afterwards
In the two buprenorphine cohorts reporting disaggre-gated data the pooled all cause mortality remained equally low at 45 deaths per 1000 person years during and after the first four weeks of buprenorphine treat-ment (fig 4) The pooled all cause mortality however increased to 320 deaths per 1000 person years in the first four weeks after people stopped buprenorphine treatment and reduced thereafter to 109 deaths per 1000 person years with an unadjusted pooled rate dif-ference for initial compared with subsequent periods out of treatment of 212 deaths (95 confidence interval minus59 to 482) per 1000 person years and an unadjusted pooled rate ratio of 294 (134 to 646)
Overdose mortality by time interval in and out of treatmentOnly three methadone cohorts and one buprenorphine cohort reported overdose mortality by time interval (fig 6) The pooled overdose mortality rates were 35 and 20 overdose deaths per 1000 person years in the first four weeks and the rest of time on methadone treatment and 42 and 34 overdose deaths per 1000 person years during and after the first four weeks out of treatment In the single buprenorphine cohort there were 09 and 15 fatal overdoses per 1000 person years before and after the first four weeks on buprenorphine treatment and 108 and 42 fatal overdoses per 1000 person years before and after four weeks out of treatment respectivelyta
ble
1 | b
asel
ine
popu
latio
n ch
arac
teris
tics o
f coh
ort s
tudi
es o
n m
orta
lity r
isk
in p
eopl
e w
ith o
pioi
d de
pend
ence
dur
ing
and
after
opi
oid
subs
titut
ion
treat
men
t
stud
ylo
catio
nPo
pula
tion
Opi
oid
in
ject
ors
()
non-
opio
id
drug
use
()
hiv
po
sitiv
e (
)Ps
ychi
atric
co
mor
bidi
ty (
)M
edic
al
com
orbi
dity
()
Men
()
base
line
mea
n ag
e (y
ears
)M
etha
done
Gear
ing
1974
24Ne
w Yo
rk U
SHe
roin
dep
ende
ntNA
84
00
00
NA79
030
0Cu
shm
an 1
97725
New
York
US
Opio
id d
epen
dent
NANA
00
29
274
730
385
Groumln
blad
h 19
9026
Natio
nwid
e S
wed
enHe
roin
dep
ende
ntNA
00
00
NANA
783
275
Capl
ehor
n 19
9427
1996
28Pa
rram
atta
NSW
Aus
tralia
Hero
in d
epen
dent
NANA
00
NANA
720
234
Fuge
lsta
d 19
9529
Stoc
khol
m S
wed
enHI
V po
sitiv
e in
ject
ing
opio
id d
epen
dent
100
00
010
00
NANA
NA31
8Fu
gels
tad
1998
30St
ockh
olm
Sw
eden
Non
volu
ntar
ily tr
eate
d in
ject
ing
hero
in d
epen
dent
100
00
067
938
698
250
029
3
Bust
er 2
0027
Amst
erda
m N
ethe
rland
sOp
ioid
dep
ende
nt34
7NA
NANA
NA77
032
6Sc
herb
aum
200
231St
ate-
wid
e N
orth
Rhi
ne-W
estp
halia
Ger
man
yIn
ject
ing
opio
id d
epen
dent
100
0NA
NA70
0NA
780
320
Davo
li 2
00732
Natio
nwid
e It
aly
Hero
in d
epen
dent
720
NA8
013
0NA
800
315
Fuge
lsta
d 2
00733
Stoc
khol
m S
wed
enHe
roin
dep
ende
ntNA
00
275
NANA
NA38
2Cl
ause
n 2
00834
Natio
nwid
e N
orw
ayOp
ioid
dep
ende
nt92
5NA
35
NANA
676
396
Dege
nhar
dt 2
0096
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA64
829
6Co
rnis
h 2
0108
Natio
nwid
e U
KOp
ioid
dep
ende
ntNA
NANA
NA17
569
330
1Pe
les
201
035Te
l Avi
v Is
rael
Opio
id d
epen
dent
NA67
58
441
6NA
736
376
Evan
s 2
0159
Stat
e-w
ide
CA
US
Opio
id d
epen
dent
552
219
NA23
119
064
235
3Ki
mbe
r 20
1510
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA65
833
4No
syk
201
536St
ate-
wid
e B
C C
anad
aHA
ART
treat
ed H
IV p
ositi
ve in
ject
ing
opio
id d
epen
dent
100
0NA
100
0NA
333
667
360
Cous
ins
201
637Na
tionw
ide
Irel
and
Opio
id d
epen
dent
NANA
NA22
822
068
730
5bu
pren
orph
ine
Corn
ish
201
08Na
tionw
ide
UK
Opio
id d
epen
dent
NANA
NANA
175
693
301
Reec
e 2
01038
Bris
bane
Que
ensl
and
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA73
030
5Ki
mbe
r 20
1510
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA70
732
5NA
=not
ava
ilabl
e H
AART
=hig
hly a
ctiv
e an
tiret
rovi
ral t
hera
py
Opi
oid
subs
titut
ion
treat
men
t with
eith
er m
etha
done
or b
upre
norp
hine
exc
ept f
or C
laus
en e
t al34
in w
hich
abo
ut 9
3 o
f par
ticip
ants
use
d m
etha
done
and
onl
y 7
use
d bu
pren
orph
ine
durin
g st
udy p
erio
d
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
6
tabl
e 2
| tre
atm
ent d
eliv
ery a
nd fo
llow
-up
feat
ures
of c
ohor
t stu
dies
on
mor
talit
y ris
k in
peo
ple
with
opi
oid
depe
nden
ce d
urin
g an
d aft
er o
pioi
d su
bstit
utio
n tre
atm
ent
stud
yno
of c
ohor
t pa
rtic
ipan
tsdagger
aver
age
Ost
do
se (m
gda
y)in
patie
nt
indu
ctio
n (
)O
st
prov
ider
Follo
w-u
p pe
riod
aver
age
follo
w-u
p (y
ears
)Dagger
loss
to
follo
w-u
p (
)sectM
orta
lity
outc
ome
Qua
lity
scor
epara
Met
hado
neGe
arin
g 19
7424
3000
100
176
Spec
ialis
t19
65-7
25
24
0Al
l cau
ses
ove
rdos
e9
Cush
man
197
72554
710
0NA
Spec
ialis
t19
66-7
53
623
2Al
l cau
ses
ove
rdos
e6
Groumln
blad
h 19
9026
166
7510
00
Spec
ialis
t19
67-8
711
00
0Al
l cau
ses
ove
rdos
e4
Capl
ehor
n 19
9427
1996
2830
511
632
3Sp
ecia
list
1970
-90
139
144
All c
ause
s27
ove
rdos
e286
Fuge
lsta
d 19
9529
135
NA10
00
Spec
ialis
t19
86-9
02
10
0Al
l cau
ses
6Fu
gels
tad
1998
3056
8010
00
Spec
ialis
t19
86-9
34
20
0Al
l cau
ses
6Bu
ster
200
2752
0048
00
Mix
ed19
86-9
85
70
0O
verd
ose
8Sc
herb
aum
200
23124
447
00
Spec
ialis
t19
88-9
65
315
6Al
l cau
ses
ove
rdos
e7
Davo
li 2
00732
5276
NA0
0Sp
ecia
list
1998
-200
11
33
7O
verd
ose
11Fu
gels
tad
200
73367
9NA
100
0Sp
ecia
list
1988
-200
06
96
2Al
l cau
ses
3Cl
ause
n 2
00834
3229
112
00
Mix
ed19
97-2
003
24
00
All c
ause
s o
verd
ose
7De
genh
ardt
200
9631
846
700
0M
ixed
1985
-200
0daggerdagger6
80
0Al
l cau
sesDaggerDagger
12Co
rnis
h 2
0108
4894
500
0GP
1990
-200
519
175
All c
ause
s9
Pele
s 2
01035
613
113
00
Spec
ialis
t19
93-2
008
770
8Al
l cau
ses
ove
rdos
e9
Evan
s 2
0159
32 32
2NA
00
Spec
ialis
t20
06-1
02
35
0Al
l cau
sesDaggerDagger
12Ki
mbe
r 20
1510
26 0
6470
00
Mix
ed20
01-1
05
30
0Al
l cau
ses
ove
rdos
e13
Nosy
k 2
01536
1326
NA0
0GP
1996
-201
04
279
All c
ause
sDaggerDagger13
Cous
ins
201
63769
8372
00
GP20
04-1
04
12
0Al
l cau
ses
ove
rdos
e12
bupr
enor
phin
eCo
rnis
h 2
0108
1373
100
0GP
1990
-200
511
103
All c
ause
s9
Reec
e 2
01038
2518
NA0
0GP
2000
-07
32
12Al
l cau
ses
5Ki
mbe
r 20
1510
11 94
012
00
Mix
ed20
01-1
04
50
0Al
l cau
ses
ove
rdos
e13
NA=n
ot a
vaila
ble
OST
=opi
oid
subs
titut
ion
treat
men
tO
pioi
d su
bstit
utio
n tre
atm
ent w
ith e
ither
met
hado
ne o
r bup
reno
rphi
ne e
xcep
t for
Cla
usen
et a
l34 in
whi
ch a
bout
93
of p
artic
ipan
ts u
sed
met
hado
ne a
nd o
nly 7
u
sed
bupr
enor
phin
e du
ring
stud
y per
iod
daggerPar
ticip
ants
rece
ivin
g op
ioid
sub
stitu
tion
treat
men
t at l
east
onc
e du
ring
stud
y per
iod
Unt
reat
ed p
artic
ipan
ts a
nd th
ose
rece
ivin
g ot
her t
ypes
of t
reat
men
t for
opi
oid
depe
nden
ce (m
etha
done
det
oxifi
catio
n o
pioi
d an
tago
nist
ther
apy
ther
apeu
tic
com
mun
ity) e
xclu
ded
from
met
a-an
alys
is
DaggerAve
rage
follo
w-u
p fro
m s
tart
of o
pioi
d su
bstit
utio
n tre
atm
ent c
ombi
ning
sub
sequ
ent p
erio
ds in
and
out
of t
reat
men
tsectP
erce
ntag
e lo
ss to
follo
w-u
p be
fore
end
of s
tudy
per
iod
or d
eath
If n
ot o
ther
wis
e sp
ecifi
ed c
ompl
ete
case
asc
erta
inm
ent a
ssum
ed fo
r stu
dies
bas
ed o
n po
pula
tion
mor
talit
y reg
istri
es
paraQua
lity a
sses
smen
t sco
re ra
ngin
g fro
m 0
(low
est q
ualit
y) to
16 (h
ighe
st q
ualit
y)
O
verd
ose
mor
talit
y rep
orte
d bu
t not
incl
uded
in m
eta-
anal
ysis
as t
here
wer
e no
ove
rdos
e de
aths
whi
le p
artic
ipan
ts w
ere
in o
pioi
d su
bstit
utio
n tre
atm
ent
daggerdaggerFo
llow
-up
rest
ricte
d to
1985
-200
0 as
sub
sequ
ent 2
001-
06 fo
llow
-up
perio
d ov
erla
pped
with
Kim
ber e
t al10
DaggerDaggerO
verd
ose
mor
talit
y rep
orte
d on
ly fo
r com
bine
d tre
atm
ents
or i
nclu
ded
untre
ated
par
ticip
ants
and
hen
ce n
ot in
clud
ed in
met
a-an
alys
is
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
7
discussionMain findingsOur review suggests that time spent in opioid substitu-tion treatment with methadone is associated with an average reduction of 25 deaths1000 person years (95 confidence interval 14 to 36) The rate in treatment was less than a third of the rate out of treatment with the greatest difference in deaths from overdose The all cause mortality risk during treatment is much higher in the first four weeks than in the remainder of treatment Mortality risk is also higher in the first four weeks after cessation than in the remainder time out of treatment
Based on three cohorts (two from Australia) findings also suggest that opioid substitution treatment with buprenorphine could be associated with a reduction in mortality with a similar risk across all time in treatment (about four deaths1000 person years) consistent with its safety profile39-44 and a risk after cessation higher in the first four weeks than in the remainder of time out of treatment (32 versus 11 deaths1000 person years)
Mortality risk during specific periods in and out of methadone treatmentThe larger relative effect size (as measured by rate ratio) for overdose than non-overdose deaths with metha-done substitution6 11 34 45 is consistent with previous findings although the effect on non-overdose deaths had not been previously reviewed This disparity is
consistent with what would be expected given metha-donersquos effect on reducing use of heroin and other illicit opioids32 34
Our finding that the first four weeks after onset (114 deaths1000 person years) and cessation (3211000 person years) of methadone treatment are the highest risk periods suggests that these are key periods during which to focus efforts for prevention of drug related deaths Moreover within periods of methadone treat-ment there is a swift decline in risk from first to fourth week followed by a stable trend whereas after cessa-tion there is a high but quite stable risk during the first four weeks and a progressive decline afterward This is important because some patients cycle in and out of opioid substitution treatment46-50 and are therefore exposed to repeated periods of high risk for mortality Such changes probably mainly reflect changes in risk of fatal overdose6 32 but this has not been accurately assessed because only two cohorts reported overdose data specifically7 10 The increased risk during the first few weeks of treatment could be explained by an accu-mulation of methadone that exceeds the opioid toler-ance level (the mean elimination half life for methadone is 22 hours)51 as opioid tolerance does not seem to fully protect against respiratory depression52 Psychological factors and concomitant use of other respiratory depressant drugs or cocaine could also play a role7 8 40 53 54
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1994 Fugelstad et al 1995 Fugelstad et al 1998 Scherbaum et al 2002 Fugelstad et al 2007 Clausen et al 2008 Degenhardt et al 2009 Cornish et al 2010 Peles et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine Cornish et al 2010 Reece 2010 Kimber et al 2015Overall
2 5 10 20 50 100 200
11014 474251655161085111975
82427177
181114773354906450
648111 538305129423985
16325 27763691 792
89397911522 648
774031119
8721 936
In treatment
3311701429732740
362279545457
14172741311461303
1510105 73571428852727
84848 12256345 2652061582986247
10751406911
31431 239
Out of treatment
No of deathsperson years
76 (62 to 92)151 (98 to 223)148 (84 to 239)56 (28 to 100)
331 (143 to 651)395 (159 to 814)162 (96 to 255)
230 (181 to 287)140 (112 to 171)
58 (54 to 63)58 (40 to 83)
105 (76 to 142)64 (55 to 75)69 (64 to 75)
224 (180 to 275)51 (42 to 61)
113 (84 to 152)
95 (38 to 195)27 (06 to 78)40 (32 to 49)43 (21 to 89)
In treatment
282 (194 to 396)471 (258 to 791)432 (296 to 610)158 (111 to 219)
1111 (361 to 2593)699 (191 to 1790)814 (445 to 1366)565 (443 to 709)353 (259 to 471)143 (136 to 150)166 (129 to 209)715 (534 to 938)176 (165 to 188)124 (114 to 135)
1302 (1130 to 1493)157 (127 to 191)361 (245 to 533)
133 (64 to 245)58 (41 to 79)
101 (90 to 112)95 (39 to 234)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 2 | all cause mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled all cause mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates during periods in and out of treatment across all methadone or buprenorphine cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
8
tabl
e 3
| Poo
led
all c
ause
and
ove
rdos
e m
orta
lity r
ates
dur
ing
perio
ds in
and
out
of o
pioi
d su
bstit
utio
n tre
atm
ent w
ith m
etha
done
by s
tudy
char
acte
ristic
s
stud
y ch
arac
teris
tic
all c
ause
mor
talit
y ra
te1
000
pers
on y
ears
(95
Ci)
Ove
rdos
e m
orta
lity
rate
100
0 pe
rson
yea
rs (9
5 C
i)
no o
f st
udie
sin
trea
tmen
tO
ut o
f tre
atm
ent
P va
luedagger
i2 (
)Daggerno
of
stud
ies
in tr
eatm
ent
Out
of t
reat
men
tP
valu
edaggeri2 (
)Dagger
Loca
tion
E
urop
eIs
rael
913
9 (9
5 to
20
5)46
6 (2
90
to 74
9)
008
987
31
(24
to 4
0)
133
(59
to 2
98)
013
93
Nor
th A
mer
ica
411
2 (6
4 to
196
)42
3 (2
12 to
84
6)2
23
(14
to 3
8)
205
(44
to 9
45)
A
ustra
lia3
63
(33
to 12
1)14
0 (6
3 to
30
8)2
20
(14
to 2
9)
67
(15
to 2
96)
Opio
id in
ject
ors (
)
lt
100
129
0 (6
9 to
117
)25
8 (1
87
to 3
55)
000
195
102
5 (2
0 to
30
)10
6 (6
1 to
185
)mdash
mdash
100
423
4 (1
42
to 3
85)
109
9 (5
94
to 2
034
)1
mdashsect
mdashsect
Men
()
lt
7511
95
(69
to 13
2)
300
(18
4 to
48
8)0
6798
62
4 (1
8 to
34
)10
6 (4
5 to
24
8)0
7493
ge
753
116
(61
to 2
20)
459
(178
to 11
79)
52
9 (2
0 to
42
)15
8 (6
2 to
40
3)M
ean
age
(yea
rs)
lt
3510
99
(68
to 14
5)
293
(179
to 4
82)
040
988
26
(19
to 3
5)
106
(52
to 2
18)
060
93
ge35
614
0 (8
7 to
22
7)50
3 (2
68
to 9
43)
32
7 (1
5 to
47
)20
5 (6
2 to
676
)Av
erag
e m
etha
done
dos
e (m
gda
y)
le
807
96
(63
to 14
8)
269
(15
5 to
46
5)0
5692
53
1 (2
0 to
46
)10
3 (4
0 to
26
9)0
2293
gt
805
99
(60
to 16
5)
354
(18
5 to
677
)5
25
(16
to 3
9)
170
(65
to 4
49)
Inpa
tient
indu
ctio
n (
)
09
92
(63
to 13
6)
299
(173
to 5
16)
019
987
25
(18
to 3
4)
100
(45
to 2
23)
065
93
gt0
615
4 (9
3 to
25
3)45
9 (2
29
to 9
21)
32
9 (1
7 to
50
)18
4 (5
4 to
62
5)Tr
eatm
ent p
rovi
der
S
peci
alis
t10
134
(92
to 19
5)
465
(28
2 to
765
)0
2698
72
5 (1
7 to
37
)20
8 (1
11 to
38
8)0
0188
G
Pm
ixed
68
6 (5
4 to
137
)24
4 (1
31
to 4
54)
42
4 (1
6 to
36
)5
6 (2
5 to
125
)M
idpo
int f
ollo
w-u
p pe
riod
lt
2000
1012
6 (8
5 to
187
)38
8 (2
28
to 6
61)
058
987
28
(20
to 3
9)
154
(70
to 3
39)
067
93
ge20
006
97
(60
to 15
9)
320
(16
5 to
62
3)4
24
(17
to 3
5)
90
(32
to 2
52)
Loss
to fo
llow
-up
()
lt
1012
119
(83
to 1
70)
383
(23
7 to
619
)0
8198
82
5 (1
9 to
32
)9
8 (5
0 to
195
)0
3393
ge
104
95
(50
to 18
0)
313
(13
5 to
72
3)3
32
(17
to 6
0)
254
(81
to 7
94)
Poo
led
mor
talit
y rat
es a
nd 9
5 c
onfid
ence
inte
rval
s dur
ing
perio
ds in
and
out
of t
reat
men
t by s
tudy
cha
ract
eris
tics e
stim
ated
from
sep
arat
e bi
varia
te ra
ndom
effe
cts m
eta-
regr
essi
on m
odel
s rel
atin
g lo
g tra
nsfo
rmed
rate
s in
both
trea
tmen
t per
iods
w
ith e
ach
stud
y cha
ract
eris
tic
daggerOve
rall
P va
lue
for h
eter
ogen
eity
of p
oole
d m
orta
lity r
ates
acr
oss c
ateg
orie
s of s
tudy
cha
ract
eris
tic a
s obt
aine
d fro
m li
kelih
ood
ratio
test
com
parin
g ne
sted
met
a-re
gres
sion
mod
els w
ith a
nd w
ithou
t stu
dy c
hara
cter
istic
fitte
d vi
a m
axim
um li
kelih
ood
DaggerOve
rall
I2 sta
tistic
for r
esid
ual h
eter
ogen
eity
in s
tudy
spe
cific
mor
talit
y rat
es n
ot e
xpla
ined
by c
orre
spon
ding
stu
dy c
hara
cter
istic
sectP
oole
d m
orta
lity r
ates
not
app
licab
le to
cat
egor
ies w
ith s
ingl
e st
udy
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
9
Although the long half life of methadone could con-tribute to the increase in mortality in the first three to four days after cessation of treatment there was a large increase in mortality across the first four weeks after cessation compared with the treatment period Such increased mortality could be explained by loss of toler-ance to the toxic effects of heroin assuming that many patients return to use6 8 32 47 55 56 and probably also by the use of multiple legal and illicit substances during that period Similar peaks in drug related mortality occur in other situations where opioid tolerance is prob-ably diminished (for example after prison release or hospital discharge57-59 ) Lifestyle factors and comorbid issues such as mental health problems could also increase mortality from other external causes as deaths from suicide and injury are also more common during that period53
Mortality risk during specific periods in and out of buprenorphine treatmentData from three cohorts (two from Australia) suggest that substitution treatment with buprenorphine could reduce all cause mortality although the disparity in mortality rates in periods in and out of treatment did not reach significance Findings also suggest a signifi-cantly increased mortality in the first four weeks after cessation of treatment compared with the remaining time out of treatment (320 versus 1091000 person years) while during the treatment period there was no difference between the first four weeks and the remain-ing time in treatment It is difficult to draw firm conclu-sions because of limited evidence from similar settings 96 of included deaths and 98 of person years came from Australian studies (with 87 and 86 from the study by Kimber and colleagues13)
Comparative effectiveness of buprenorphine and methadone substitution treatmentOther sources of data have suggested that buprenor-phine could be more effective than methadone in reduc-ing mortality especially from overdose39 42 43 Unlike methadone there is a ceiling for respiratory depressant effects of buprenorphine as dose increases and the probability of triggering arrhythmias is lower for buprenorphine than methadone41 44 60 When we com-pared the mortality between periods in and out of treat-ment first within those taking methadone and then within those taking buprenorphine we found a greater reduction in mortality with methadone than with buprenorphine (measured as the rate difference or rate ratio between periods) When we compared mortality between them first within the treatment period and then in the period off treatment we found a signifi-cantly lower mortality with buprenorphine than meth-adone in both periods
Our conclusions must remain tentative until further studies in varied treatment settings and contexts are undertaken to examine this issue Differences in mor-tality might also reflect confounding through differ-ences in characteristics of patients (such as age severity of opioid dependence injecting drug use other ta
ble
4 | C
ohor
t stu
dies
repo
rtin
g al
l cau
se a
nd o
verd
ose
mor
talit
y rat
e ra
tios c
ompa
ring
perio
ds o
ut a
nd in
opi
oid
subs
titut
ion
treat
men
t adj
uste
d fo
r con
foun
ding
stud
y
Conf
ound
ing
fact
ors
all c
ause
mor
talit
yO
verd
ose
mor
talit
y
Patie
nt d
emog
raph
ics
seve
rity
of d
rug
use
trea
tmen
tCo
mor
bidi
tyun
adju
sted
ra
te ra
tioad
just
ed
rate
ratio
Perc
enta
ge
chan
gedagger
unad
just
ed
rate
ratio
adju
sted
ra
te ra
tioPe
rcen
tage
ch
ange
dagger
Met
hado
neBu
ster
200
27Se
x ra
ceTr
eatm
ent m
odal
ity t
ime
sinc
e fir
st tr
eatm
ent
mdashmdash
mdashmdash
087
087
minus03
Davo
li 2
00732
Age
sex
Leng
th o
f her
oin
use
her
oin
inje
ctio
n
prev
ious
ove
rdos
eHI
V p
sych
iatri
c com
orbi
dity
mdashmdash
mdash77
174
3minus3
6
Dege
nhar
dt 2
0096
Age
sex
cal
enda
r yea
rmdash
mdash19
118
8minus1
3mdash
mdashmdash
Corn
ish
201
08Ag
e s
ex c
alen
dar y
ear
mdashM
edic
al c
omor
bidi
ty2
833
2715
5mdash
mdashmdash
Evan
s 2
0159Dagger
Age
sex
rac
e e
duca
tion
em
ploy
men
t cr
imin
ality
hea
lth c
over
age
Prim
ary o
pioi
d fr
eque
ncy a
nd le
ngth
of
opio
id u
se n
on-o
pioi
d dr
ug u
seHI
V h
epat
itis C
tub
ercu
losi
s
disa
bilit
y m
edic
al c
omor
bidi
ty
psyc
hiat
ric c
omor
bidi
ty
273
370
355
351
442
258
Nosy
k 2
01536
DaggerAg
e s
ex r
ace
cal
enda
r yea
r re
gion
No o
f pre
viou
s tre
atm
ent e
piso
des
Tim
e si
nce
HIV
diag
nosi
s C
D4
coun
t AI
DS a
ntire
trovi
ral
ther
apy
med
ical
com
orbi
dity
304
294
minus34
114
147
286
Cous
ins
201
637Ag
e s
exTr
eatm
ent s
uper
visi
on m
etha
done
dos
eM
edic
al c
omor
bidi
ty3
093
6417
816
016
317
bupr
enor
phin
eCo
rnis
h 2
0108
Age
sex
cal
enda
r yea
rmdash
Med
ical
com
orbi
dity
141
164
168
mdashmdash
mdashB
asel
ine
or ti
me
vary
ing
conf
ound
ing
fact
ors u
sed
in a
djus
tmen
tdaggerP
erce
ntag
e ch
ange
in ra
te ra
tio a
fter a
djus
tmen
t for
cor
resp
ondi
ng c
onfo
undi
ng fa
ctor
sDaggerO
verd
ose
mor
talit
y rat
e ra
tios r
epor
ted
com
bini
ng m
etha
done
mai
nten
ance
with
det
oxifi
catio
n (1
14
of p
erso
n ye
ars i
n tre
atm
ent)
in E
vans
et a
l9 an
d in
clud
ing
neve
r tre
ated
par
ticip
ants
(73
3 o
f per
son
year
s out
of t
reat
men
t) in
Nos
yk e
t al36
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
10
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1996 Buster et al 2002 Scherbaum et al 2002 Davoli et al 2007 Clausen et al 2008 Peles et al 2010 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine Kimber et al 2015
2105 5 10 20 50 100
3314 474416557108541792
4218 7476111475751
24645053985
16991 7925422 648
3121 936
In treatment
2111707297
27740192004
2610 983131729998
28130313727
21645 265246247
14331 239
Out of treatment
No of deathsperson years
23 (16 to 32)24 (07 to 62)
64 (26 to 133)22 (06 to 57)22 (16 to 30)
54 (20 to 117)12 (05 to 25)37 (24 to 55)12 (04 to 29)18 (16 to 21)24 (18 to 31)26 (21 to 33)
14 (10 to 20)
In treatment
179 (111 to 274)236 (95 to 486)
365 (240 to 531)95 (57 to 148)24 (16 to 35)
756 (402 to 1292)90 (41 to 171)
215 (143 to 311)179 (95 to 306)
48 (42 to 54)38 (25 to 57)
127 (69 to 234)
46 (39 to 54)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 3 | Overdose mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled overdose mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates during periods in and out of treatment across all methadone cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
Methadone rst four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallMethadone aer four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Cornish et al 2010 Kimber et al 2015OverallBuprenorphine aer four weeks Cornish et al 2010 Kimber et al 2015Overall
21 5 10 20 50 100
9425057465
151950323344
4100153371
554109 033234664
14823 32760488 449
85388010019 277
18192094
66597819 842
In treatment
38189821479
154267335183679113
441181
1472103 838503809
69445 44952843 4301271469545067
788281674
366328629 565
Out of treatment
No of deathsperson years
375 (303 to 459)151 (61 to 311)77 (43 to 127)96 (66 to 135)
mdash44 (25 to 73)
114 (58 to 224)
51 (47 to 55)49 (31 to 74)63 (54 to 74)68 (63 to 74)
mdash52 (42 to 63)58 (50 to 67)
124 (03 to 692)43 (20 to 82)
45 (12 to 168)
91 (33 to 198)39 (31 to 49)45 (32 to 62)
In treatment
200 (142 to 275)438 (271 to 670)576 (489 to 675)191 (133 to 265)
mdash373 (271 to 500)321 (191 to 539)
142 (135 to 149)131 (97 to 173)
153 (141 to 164)122 (111 to 132)
mdash107 (80 to 139)
135 (119 to 153)
800 (322 to 1648)167 (111 to 242)320 (132 to 775)
45 (09 to 132)97 (86 to 109)
109 (85 to 139)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 4 | all cause mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled all cause mortality rates 2009-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except Degenhardt et al6 which reported mortality before and after two weeks of treatment initiation and cessation high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-analysis area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates before and after four weeks in and out of treatment across methadone or buprenorphine cohorts estimated from multivariate random effects meta-analysis on log transformed rates in four time-by-treatment intervals
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
11
drug use comorbidities prison history overdose his-tory patientrsquos preference) characteristics of treatment (such as previous treatment specialisation of the doc-tor who controls the treatment dose provision charac-teristics cointerventions retention or drop outs) or the sociopolitical context in which studies have been conducted For example the initial prognosis might be better in those given buprenorphine than those given methadone (that is fewer comorbid problems less severe opioid dependence)6 8 10 61 though this was not clearly found in a recent US study62
The role of such confounding factors has received almost empirical examination Few details on char-acteristics of patients or treatments were reported in articles included in this meta-analysis to permit a detailed examination of this potential issue (tables 1 and 2 ) so it was not possible to assess the possibil-ity of confounding A sensitivity simulation analysis in the study by Kimber and colleagues however suggested that the lower mortality with buprenor-phine than with methadone during first four weeks of treatment was unlikely to be caused by unmea-sured confounding10
strengths and limitationsThis meta-analysis synthesised evidence from cohort studies published until 2016 on risk of mortality in people who are dependent on opioids during and after opioid substitution treatment separately for buprenor-phine and methadone Mortality changes over time (1st-32th week) during and after methadone are care-fully quantified for the first time
The published studies however had several methodological shortcomings Firstly in the included
Methadone rst four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallMethadone aer four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Kimber et al 2015Buprenorphine aer four weeks Kimber et al 2015
21 505 10 20
9150018334443371
3317 20015188 4495019 277
22094
2919 842
In treatment
2130010183681181
24960020643 430
165067
181674
12529 565
Out of treatment
No of deathsperson years
60 (27 to 114)54 (32 to 85)12 (03 to 30)35 (13 to 95)
19 (13 to 27)17 (14 to 20)26 (19 to 34)20 (15 to 27)
09 (01 to 34)
15 (10 to 21)
In treatment
15 (02 to 56)54 (26 to 100)68 (29 to 134)42 (18 to 99)
25 (16 to 37)47 (41 to 54)32 (18 to 51)34 (23 to 51)
108 (64 to 170)
42 (35 to 50)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 6 | Overdose mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled overdose mortality rates 2002-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except buster et al7 which reported mortality before and after two weeks of treatment initiation and cessation area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates before and after four weeks in and out of treatment across methadone cohorts estimated from multivariate random-effects meta-analysis on log transformed rates in four time-by-treatment intervals
Time since treatment initiation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s In methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Time since treatment cessation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s Out of methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Degenhardt et al 2009Cornish et al 2010Evans et al 2015Kimber et al 2015Cousins et al 2016
Fig 5 | all cause mortality rates by time since treatment initiation and cessation in methadone cohorts and pooled all cause mortality risk trends 2009-16 high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-regression area of each circle is proportional to weight of each time interval in meta-regression Pooled trends in all cause mortality risk (solid lines) and their 95 confidence intervals (shaded regions) over time in and out of methadone treatment were estimated from bivariate random effects meta-regression of log transformed rates on quadratic linear spline function of log time with knot at four weeks
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
12
observational studies the same patients are compared throughout follow-up periods in and out of opioid sub-stitution treatment but these patients leave and re-en-ter treatment in a non-random way and hence there could still be a large potential for confounding in com-parisons of crude mortality risk in and out of treat-ment In some studies with diverse information on patient demographics severity of drug use and comor-bidities measured mostly at baseline (table 3 ) adjust-ment for these potential confounders resulted in similar or even increased out-to-in mortality rate ratios which merely reflects that the above conditions tended to be less prevalent at baseline among patients who later left or were discharged from treatment than those who remained in treatment Nevertheless to obtain an unbiased estimate of the preventive effect of opioid substitution treatment on all cause and overdose mor-tality these and other relevant confounders should be measured every time a patient leaves and resumes treatment Time varying data can then be used to adjust for confounder history in standard regression models or even better to construct inverse probability of treatment weights for marginal structural models63 which properly control for time varying confounders for later treatment that are themselves affected by pre-vious treatment such as severity of drug use and comorbidity Also differential loss to follow-up is a concern in the meta-analysed cohorts as dropouts are more likely to occur in patients at higher risk of death during periods out of treatment thus inducing a selec-tion bias in crude comparisons of out-to-in mortality risk because of informative censoring Marginal struc-tural models with inverse probability of censoring weights can also be used to correct for differential loss to follow-up63 provided that common predictors of death and censoring are measured over time In sum-mary individual cohorts are prone to confounding and selection bias because of differential loss to follow-up but it is hard to assess with the available information the amount and direction of bias projected onto the pooled mortality rate differences and rate ratios between periods in and out of treatment obtained in this meta-analysis
Secondly studies were conducted in high income countries with the follow-up often spread over many calendar years (1965-2010 for methadone and 1990-2010 for buprenorphine) and a highly variable average length of follow-up (ranges 13-158 years and 11-45 years respectively) Studies in low and middle income countries are especially needed
Thirdly by design we have not captured overdose mortality when opioid substitution treatment was obtained on illicit drug markets40 64 Fourthly a delayed record of treatment cessation could have led to some deaths that occurred out of treatment being incorrectly classified as occurring in treatment40 if so this makes our estimated impact of opioid substitution treatment on mortality a conservative one There could similarly be misclassification between overdose and non-over-dose deaths because of inconsistencies in definition of overdose and codification of causes of deaths (for
instance criteria for separating overdose death from intentional poisoning or sudden cardiac death)40 65 again these misclassifications would tend to underesti-mate deaths from overdose
implications for policy and practiceIn many countries the number of deaths attributable to opioid use is substantial66 67 and increasing in some such as the US where deaths from opioid overdose now outnumber gun related deaths in the country68 Over-doses are preventable causes of death warranting wide implementation of preventive interventions Our review has provided evidence that methadone and probably buprenorphine reduce mortality among people depen-dent on opioids making it imperative that further research confirms this using study designs that con-sider a wide range of confounding variables to increase confidence that these effects are causal
It must be borne in mind that there is strong evidence of the efficacy of methadone and buprenorphine on a range of clinical outcomes and these medicines are listed as WHO essential medicines the findings we have presented here provide additional imperatives for their widespread availability Despite this coverage of opioid substitution treatment is low in many countries worldwide69 Policymakers clinicians and those responsible for drug treatment systems should work to ensure the availability of such treatment remove access barriers and promote engagement This means the strategic development of services from a public health perspective which could reduce the social harm associ-ated with opioid use
Our review suggests that some precautions should be taken during and after opioid substitution treatment to increase safety Firstly careful clinical assessment of opioid tolerance before onset of treatment to establish a safe induction dose seems warranted Secondly moni-toring during the induction period is important espe-cially for methadone with clinicians considering adjusting opioid doses monitoring mental and somatic problems and preventing the use of opioids obtained on the illicit drug market64 In addition education of patients about the risk of overdose risk and use of ldquotake homerdquo naloxone70 71 is warranted Buprenorphine induction followed by transition to methadone might also be considered10 72 Retention in opioid substitution treatment reduces risk of exposure to mortality after cessation and also to re-exposure to mortality risk during induction onto methadone so efforts to improve retention are important as a strategy to reduce mortal-ity More generally establishment of mechanisms for information and coordination between healthcare social and legal services and patient counselling while in treatment in addition to more specific overdose pre-vention programmes such as naloxone distribution should be considered
Finally there is a pressing need for new studies on the comparative effectiveness of methadone and buprenorphine in reducing mortality New ran-domised controlled trials are highly unlikely they would be prohibitively expensive and difficult to
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score

doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
4
on psychiatric and medical comorbidities More than 70 of participants were men and the mean age at baseline ranged from 234 to 396 (table 1)
Methadone was prescribed in 18 cohorts including 122 885 participants over the period 1965-2010 and buprenorphine was used in three cohorts including 15 831 participants over 1990-2010 (table 2) The average daily dose ranged from 47 mg to 116 mg of methadone and 10 mg to 12 mg of buprenorphine Treatment was initiated on an ambulatory basis in all recent cohorts and provided by addiction medicine specialists in 11 cohorts and general practitioners or mixed staff in eight cohorts The average follow-up after initiation varied between 13 and 139 years for methadone and 11 and 45 years for buprenorphine with loss to follow-up exceeding 10 in only four cohorts All cause mortality during follow-up periods in and out of treatment was reported in all but two methadone cohorts and over-dose mortality in 11 methadone cohorts and one buprenorphine cohort Most studies were of moderate quality They ranged from 3 to 13 points on a 16 point scale with a median of 8 points
all cause mortality during and after opioid substitution treatmentAll cause mortality rates varied widely across the 16 methadone cohorts (overall I2=98 Plt0001) although rates were consistently higher out of treatment than in treatment (fig 2 ) The pooled all cause mortality rates were 113 and 361 deaths per 1000 person years in and out of methadone treatment respectively with an unadjusted pooled rate difference for periods out and in treatment of 249 deaths (95 confidence interval 136 to 361) per 1000 person years and an unadjusted pooled rate ratio of 320 (265 to 386) In heterogeneity analyses (table 3) the pooled all cause mortality rates in and out of methadone treatment were significantly higher in studies that mostly enrolled opioid injectors who were positive for HIV than in studies including
both injectors and non-injectors and marginally higher in studies conducted in Europe and North America than in Australia
The pooled all cause mortality rates in the three buprenorphine cohorts were 43 and 95 deaths per 1000 person years in and out of treatment respectively (fig 2) The unadjusted pooled rate difference for peri-ods out and in treatment was 52 deaths (95 confi-dence interval minus10 to 114) per 1000 person years and the unadjusted pooled rate ratio was 220 (134 to 361)
After we removed each individual cohort the pooled all cause mortality rates ranged from 106 to 119 deaths per 1000 person years in methadone treatment and from 325 to 391 deaths per 1000 person years out of methadone treatment With buprenorphine treatment these figures were 33 to 56 deaths and 77 to 123 deaths per 1000 person years respectively There was some evidence of small study effects on all cause mortality (P=005) with higher rates in small cohorts that mostly enrolled opioid injectors who were positive for HIV (table 1 and fig 2)
Five methadone cohorts and one buprenorphine cohort reported all cause mortality rate ratios for peri-ods out of and in treatment with various degrees of adjustment for patient demographics severity of drug use treatment delivery and comorbidity (table 4) After adjustment out-to-in rate ratios remained unchanged in two methadone cohorts and increased by 155-355 in the other three methadone cohorts and by 168 in the buprenorphine cohort
Overdose mortality during and after opioid substitution treatmentThe pooled overdose mortality rates across the 11 meth-adone cohorts were 26 and 127 overdose deaths per 1000 person years in and out of methadone treatment respectively (fig 3) with an unadjusted pooled rate dif-ference comparing periods out and in treatment of 100 overdose deaths (95 confidence interval 26 to 174) per 1000 person years and an unadjusted pooled rate ratio of 480 (290 to 796) There was moderate heterogeneity between studies in mortality rates in treatment (I2=66 P=0001) and strong heterogeneity in rates out of treat-ment (I2=97 Plt0001) with significantly higher rates out of treatment among methadone patients in specialist services than in primary care (table 3 ) In the single buprenorphine cohort there were 14 and 46 fatal overdoses per 1000 person years in and out of treatment (fig 3)
After we removed each methadone cohort the pooled overdose mortality rates varied between 24 and 28 fatal overdoses per 1000 person years in methadone treatment and between 106 and 149 fatal overdoses per 1000 person years out of treatment There was no evi-dence of publication bias or other small study effects on overdose mortality (P=014) Adjustment for potential confounders did not produce any change in overdose mortality rate ratios for periods out compared with in treatment in three methadone cohorts but resulted in 258 and 286 larger rate ratios in two other metha-done cohorts (table 4)
Distinct records identied (n=2033) Medline (n=1215) Embase (n=729) PsycINFO (n=486)
Full text articles retrieved and assessed for eligibility (n=328)
Articles included in meta-analysis (n=20)
LILACS (n=182)Other searches (n=102)
Records excluded aer title and abstract review (n=1705) No data in humans (n=120) No original research (n=126) Design other than observational cohort (n=462) Not focused on opioid dependent people (n=997)
Articles excluded (n=308) Imprisoned or recently released population (n=22) Treatment unknown or other than methadone or buprenorphine maintenance (n=133) No all cause or overdose mortality as outcome (n=44) Insucient data to compute mortality rates during follow-up periods in and out of treatment (n=72) Secondary publication (n=37)
Fig 1 | selection process of cohort studies on mortality among people receiving opioid substitution treatment
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
5
all cause mortality by time interval in and out of treatmentSix recent methadone cohorts provided all cause mortal-ity data disaggregated by time interval in and out of treat-ment (fig 4) After we excluded a selective high risk cohort of injectors who were HIV positive and received highly active antiretroviral therapy the pooled all cause mortal-ity rates were 114 and 58 deaths per 1000 person years in the first four weeks and the remaining time on metha-done treatment respectively with an unadjusted pooled rate difference for initial compared with subsequent treat-ment periods of 56 deaths (95 confidence interval minus24 to 136) per 1000 person years and an unadjusted pooled rate ratio of 197 (094 to 410) Similarly the pooled all cause mortality dropped from 321 deaths per 1000 person years in the first four weeks after stopping methadone treatment to 135 deaths per 1000 person years thereafter resulting in an unadjusted pooled rate difference for ini-tial compared with subsequent periods out of treatment of 186 deaths (29 to 343) per 1000 person years and an unadjusted pooled rate ratio of 238 (151 to 374)
In continuous time trend analysis (fig 5) there were significant departures from linearity in trends in all cause mortality risk over time in and out of methadone treatment (P=004) The pooled all cause mortality rates decreased sharply from 374 to 64 deaths per 1000 per-son years throughout the initial four weeks of metha-done treatment and were fairly stable thereafter In contrast after people left methadone treatment the pooled all cause mortality remained high at between 241 and 352 deaths per 1000 person years during the initial two weeks out of treatment and decreased pro-gressively afterwards
In the two buprenorphine cohorts reporting disaggre-gated data the pooled all cause mortality remained equally low at 45 deaths per 1000 person years during and after the first four weeks of buprenorphine treat-ment (fig 4) The pooled all cause mortality however increased to 320 deaths per 1000 person years in the first four weeks after people stopped buprenorphine treatment and reduced thereafter to 109 deaths per 1000 person years with an unadjusted pooled rate dif-ference for initial compared with subsequent periods out of treatment of 212 deaths (95 confidence interval minus59 to 482) per 1000 person years and an unadjusted pooled rate ratio of 294 (134 to 646)
Overdose mortality by time interval in and out of treatmentOnly three methadone cohorts and one buprenorphine cohort reported overdose mortality by time interval (fig 6) The pooled overdose mortality rates were 35 and 20 overdose deaths per 1000 person years in the first four weeks and the rest of time on methadone treatment and 42 and 34 overdose deaths per 1000 person years during and after the first four weeks out of treatment In the single buprenorphine cohort there were 09 and 15 fatal overdoses per 1000 person years before and after the first four weeks on buprenorphine treatment and 108 and 42 fatal overdoses per 1000 person years before and after four weeks out of treatment respectivelyta
ble
1 | b
asel
ine
popu
latio
n ch
arac
teris
tics o
f coh
ort s
tudi
es o
n m
orta
lity r
isk
in p
eopl
e w
ith o
pioi
d de
pend
ence
dur
ing
and
after
opi
oid
subs
titut
ion
treat
men
t
stud
ylo
catio
nPo
pula
tion
Opi
oid
in
ject
ors
()
non-
opio
id
drug
use
()
hiv
po
sitiv
e (
)Ps
ychi
atric
co
mor
bidi
ty (
)M
edic
al
com
orbi
dity
()
Men
()
base
line
mea
n ag
e (y
ears
)M
etha
done
Gear
ing
1974
24Ne
w Yo
rk U
SHe
roin
dep
ende
ntNA
84
00
00
NA79
030
0Cu
shm
an 1
97725
New
York
US
Opio
id d
epen
dent
NANA
00
29
274
730
385
Groumln
blad
h 19
9026
Natio
nwid
e S
wed
enHe
roin
dep
ende
ntNA
00
00
NANA
783
275
Capl
ehor
n 19
9427
1996
28Pa
rram
atta
NSW
Aus
tralia
Hero
in d
epen
dent
NANA
00
NANA
720
234
Fuge
lsta
d 19
9529
Stoc
khol
m S
wed
enHI
V po
sitiv
e in
ject
ing
opio
id d
epen
dent
100
00
010
00
NANA
NA31
8Fu
gels
tad
1998
30St
ockh
olm
Sw
eden
Non
volu
ntar
ily tr
eate
d in
ject
ing
hero
in d
epen
dent
100
00
067
938
698
250
029
3
Bust
er 2
0027
Amst
erda
m N
ethe
rland
sOp
ioid
dep
ende
nt34
7NA
NANA
NA77
032
6Sc
herb
aum
200
231St
ate-
wid
e N
orth
Rhi
ne-W
estp
halia
Ger
man
yIn
ject
ing
opio
id d
epen
dent
100
0NA
NA70
0NA
780
320
Davo
li 2
00732
Natio
nwid
e It
aly
Hero
in d
epen
dent
720
NA8
013
0NA
800
315
Fuge
lsta
d 2
00733
Stoc
khol
m S
wed
enHe
roin
dep
ende
ntNA
00
275
NANA
NA38
2Cl
ause
n 2
00834
Natio
nwid
e N
orw
ayOp
ioid
dep
ende
nt92
5NA
35
NANA
676
396
Dege
nhar
dt 2
0096
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA64
829
6Co
rnis
h 2
0108
Natio
nwid
e U
KOp
ioid
dep
ende
ntNA
NANA
NA17
569
330
1Pe
les
201
035Te
l Avi
v Is
rael
Opio
id d
epen
dent
NA67
58
441
6NA
736
376
Evan
s 2
0159
Stat
e-w
ide
CA
US
Opio
id d
epen
dent
552
219
NA23
119
064
235
3Ki
mbe
r 20
1510
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA65
833
4No
syk
201
536St
ate-
wid
e B
C C
anad
aHA
ART
treat
ed H
IV p
ositi
ve in
ject
ing
opio
id d
epen
dent
100
0NA
100
0NA
333
667
360
Cous
ins
201
637Na
tionw
ide
Irel
and
Opio
id d
epen
dent
NANA
NA22
822
068
730
5bu
pren
orph
ine
Corn
ish
201
08Na
tionw
ide
UK
Opio
id d
epen
dent
NANA
NANA
175
693
301
Reec
e 2
01038
Bris
bane
Que
ensl
and
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA73
030
5Ki
mbe
r 20
1510
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA70
732
5NA
=not
ava
ilabl
e H
AART
=hig
hly a
ctiv
e an
tiret
rovi
ral t
hera
py
Opi
oid
subs
titut
ion
treat
men
t with
eith
er m
etha
done
or b
upre
norp
hine
exc
ept f
or C
laus
en e
t al34
in w
hich
abo
ut 9
3 o
f par
ticip
ants
use
d m
etha
done
and
onl
y 7
use
d bu
pren
orph
ine
durin
g st
udy p
erio
d
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
6
tabl
e 2
| tre
atm
ent d
eliv
ery a
nd fo
llow
-up
feat
ures
of c
ohor
t stu
dies
on
mor
talit
y ris
k in
peo
ple
with
opi
oid
depe
nden
ce d
urin
g an
d aft
er o
pioi
d su
bstit
utio
n tre
atm
ent
stud
yno
of c
ohor
t pa
rtic
ipan
tsdagger
aver
age
Ost
do
se (m
gda
y)in
patie
nt
indu
ctio
n (
)O
st
prov
ider
Follo
w-u
p pe
riod
aver
age
follo
w-u
p (y
ears
)Dagger
loss
to
follo
w-u
p (
)sectM
orta
lity
outc
ome
Qua
lity
scor
epara
Met
hado
neGe
arin
g 19
7424
3000
100
176
Spec
ialis
t19
65-7
25
24
0Al
l cau
ses
ove
rdos
e9
Cush
man
197
72554
710
0NA
Spec
ialis
t19
66-7
53
623
2Al
l cau
ses
ove
rdos
e6
Groumln
blad
h 19
9026
166
7510
00
Spec
ialis
t19
67-8
711
00
0Al
l cau
ses
ove
rdos
e4
Capl
ehor
n 19
9427
1996
2830
511
632
3Sp
ecia
list
1970
-90
139
144
All c
ause
s27
ove
rdos
e286
Fuge
lsta
d 19
9529
135
NA10
00
Spec
ialis
t19
86-9
02
10
0Al
l cau
ses
6Fu
gels
tad
1998
3056
8010
00
Spec
ialis
t19
86-9
34
20
0Al
l cau
ses
6Bu
ster
200
2752
0048
00
Mix
ed19
86-9
85
70
0O
verd
ose
8Sc
herb
aum
200
23124
447
00
Spec
ialis
t19
88-9
65
315
6Al
l cau
ses
ove
rdos
e7
Davo
li 2
00732
5276
NA0
0Sp
ecia
list
1998
-200
11
33
7O
verd
ose
11Fu
gels
tad
200
73367
9NA
100
0Sp
ecia
list
1988
-200
06
96
2Al
l cau
ses
3Cl
ause
n 2
00834
3229
112
00
Mix
ed19
97-2
003
24
00
All c
ause
s o
verd
ose
7De
genh
ardt
200
9631
846
700
0M
ixed
1985
-200
0daggerdagger6
80
0Al
l cau
sesDaggerDagger
12Co
rnis
h 2
0108
4894
500
0GP
1990
-200
519
175
All c
ause
s9
Pele
s 2
01035
613
113
00
Spec
ialis
t19
93-2
008
770
8Al
l cau
ses
ove
rdos
e9
Evan
s 2
0159
32 32
2NA
00
Spec
ialis
t20
06-1
02
35
0Al
l cau
sesDaggerDagger
12Ki
mbe
r 20
1510
26 0
6470
00
Mix
ed20
01-1
05
30
0Al
l cau
ses
ove
rdos
e13
Nosy
k 2
01536
1326
NA0
0GP
1996
-201
04
279
All c
ause
sDaggerDagger13
Cous
ins
201
63769
8372
00
GP20
04-1
04
12
0Al
l cau
ses
ove
rdos
e12
bupr
enor
phin
eCo
rnis
h 2
0108
1373
100
0GP
1990
-200
511
103
All c
ause
s9
Reec
e 2
01038
2518
NA0
0GP
2000
-07
32
12Al
l cau
ses
5Ki
mbe
r 20
1510
11 94
012
00
Mix
ed20
01-1
04
50
0Al
l cau
ses
ove
rdos
e13
NA=n
ot a
vaila
ble
OST
=opi
oid
subs
titut
ion
treat
men
tO
pioi
d su
bstit
utio
n tre
atm
ent w
ith e
ither
met
hado
ne o
r bup
reno
rphi
ne e
xcep
t for
Cla
usen
et a
l34 in
whi
ch a
bout
93
of p
artic
ipan
ts u
sed
met
hado
ne a
nd o
nly 7
u
sed
bupr
enor
phin
e du
ring
stud
y per
iod
daggerPar
ticip
ants
rece
ivin
g op
ioid
sub
stitu
tion
treat
men
t at l
east
onc
e du
ring
stud
y per
iod
Unt
reat
ed p
artic
ipan
ts a
nd th
ose
rece
ivin
g ot
her t
ypes
of t
reat
men
t for
opi
oid
depe
nden
ce (m
etha
done
det
oxifi
catio
n o
pioi
d an
tago
nist
ther
apy
ther
apeu
tic
com
mun
ity) e
xclu
ded
from
met
a-an
alys
is
DaggerAve
rage
follo
w-u
p fro
m s
tart
of o
pioi
d su
bstit
utio
n tre
atm
ent c
ombi
ning
sub
sequ
ent p
erio
ds in
and
out
of t
reat
men
tsectP
erce
ntag
e lo
ss to
follo
w-u
p be
fore
end
of s
tudy
per
iod
or d
eath
If n
ot o
ther
wis
e sp
ecifi
ed c
ompl
ete
case
asc
erta
inm
ent a
ssum
ed fo
r stu
dies
bas
ed o
n po
pula
tion
mor
talit
y reg
istri
es
paraQua
lity a
sses
smen
t sco
re ra
ngin
g fro
m 0
(low
est q
ualit
y) to
16 (h
ighe
st q
ualit
y)
O
verd
ose
mor
talit
y rep
orte
d bu
t not
incl
uded
in m
eta-
anal
ysis
as t
here
wer
e no
ove
rdos
e de
aths
whi
le p
artic
ipan
ts w
ere
in o
pioi
d su
bstit
utio
n tre
atm
ent
daggerdaggerFo
llow
-up
rest
ricte
d to
1985
-200
0 as
sub
sequ
ent 2
001-
06 fo
llow
-up
perio
d ov
erla
pped
with
Kim
ber e
t al10
DaggerDaggerO
verd
ose
mor
talit
y rep
orte
d on
ly fo
r com
bine
d tre
atm
ents
or i
nclu
ded
untre
ated
par
ticip
ants
and
hen
ce n
ot in
clud
ed in
met
a-an
alys
is
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
7
discussionMain findingsOur review suggests that time spent in opioid substitu-tion treatment with methadone is associated with an average reduction of 25 deaths1000 person years (95 confidence interval 14 to 36) The rate in treatment was less than a third of the rate out of treatment with the greatest difference in deaths from overdose The all cause mortality risk during treatment is much higher in the first four weeks than in the remainder of treatment Mortality risk is also higher in the first four weeks after cessation than in the remainder time out of treatment
Based on three cohorts (two from Australia) findings also suggest that opioid substitution treatment with buprenorphine could be associated with a reduction in mortality with a similar risk across all time in treatment (about four deaths1000 person years) consistent with its safety profile39-44 and a risk after cessation higher in the first four weeks than in the remainder of time out of treatment (32 versus 11 deaths1000 person years)
Mortality risk during specific periods in and out of methadone treatmentThe larger relative effect size (as measured by rate ratio) for overdose than non-overdose deaths with metha-done substitution6 11 34 45 is consistent with previous findings although the effect on non-overdose deaths had not been previously reviewed This disparity is
consistent with what would be expected given metha-donersquos effect on reducing use of heroin and other illicit opioids32 34
Our finding that the first four weeks after onset (114 deaths1000 person years) and cessation (3211000 person years) of methadone treatment are the highest risk periods suggests that these are key periods during which to focus efforts for prevention of drug related deaths Moreover within periods of methadone treat-ment there is a swift decline in risk from first to fourth week followed by a stable trend whereas after cessa-tion there is a high but quite stable risk during the first four weeks and a progressive decline afterward This is important because some patients cycle in and out of opioid substitution treatment46-50 and are therefore exposed to repeated periods of high risk for mortality Such changes probably mainly reflect changes in risk of fatal overdose6 32 but this has not been accurately assessed because only two cohorts reported overdose data specifically7 10 The increased risk during the first few weeks of treatment could be explained by an accu-mulation of methadone that exceeds the opioid toler-ance level (the mean elimination half life for methadone is 22 hours)51 as opioid tolerance does not seem to fully protect against respiratory depression52 Psychological factors and concomitant use of other respiratory depressant drugs or cocaine could also play a role7 8 40 53 54
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1994 Fugelstad et al 1995 Fugelstad et al 1998 Scherbaum et al 2002 Fugelstad et al 2007 Clausen et al 2008 Degenhardt et al 2009 Cornish et al 2010 Peles et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine Cornish et al 2010 Reece 2010 Kimber et al 2015Overall
2 5 10 20 50 100 200
11014 474251655161085111975
82427177
181114773354906450
648111 538305129423985
16325 27763691 792
89397911522 648
774031119
8721 936
In treatment
3311701429732740
362279545457
14172741311461303
1510105 73571428852727
84848 12256345 2652061582986247
10751406911
31431 239
Out of treatment
No of deathsperson years
76 (62 to 92)151 (98 to 223)148 (84 to 239)56 (28 to 100)
331 (143 to 651)395 (159 to 814)162 (96 to 255)
230 (181 to 287)140 (112 to 171)
58 (54 to 63)58 (40 to 83)
105 (76 to 142)64 (55 to 75)69 (64 to 75)
224 (180 to 275)51 (42 to 61)
113 (84 to 152)
95 (38 to 195)27 (06 to 78)40 (32 to 49)43 (21 to 89)
In treatment
282 (194 to 396)471 (258 to 791)432 (296 to 610)158 (111 to 219)
1111 (361 to 2593)699 (191 to 1790)814 (445 to 1366)565 (443 to 709)353 (259 to 471)143 (136 to 150)166 (129 to 209)715 (534 to 938)176 (165 to 188)124 (114 to 135)
1302 (1130 to 1493)157 (127 to 191)361 (245 to 533)
133 (64 to 245)58 (41 to 79)
101 (90 to 112)95 (39 to 234)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 2 | all cause mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled all cause mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates during periods in and out of treatment across all methadone or buprenorphine cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
8
tabl
e 3
| Poo
led
all c
ause
and
ove
rdos
e m
orta
lity r
ates
dur
ing
perio
ds in
and
out
of o
pioi
d su
bstit
utio
n tre
atm
ent w
ith m
etha
done
by s
tudy
char
acte
ristic
s
stud
y ch
arac
teris
tic
all c
ause
mor
talit
y ra
te1
000
pers
on y
ears
(95
Ci)
Ove
rdos
e m
orta
lity
rate
100
0 pe
rson
yea
rs (9
5 C
i)
no o
f st
udie
sin
trea
tmen
tO
ut o
f tre
atm
ent
P va
luedagger
i2 (
)Daggerno
of
stud
ies
in tr
eatm
ent
Out
of t
reat
men
tP
valu
edaggeri2 (
)Dagger
Loca
tion
E
urop
eIs
rael
913
9 (9
5 to
20
5)46
6 (2
90
to 74
9)
008
987
31
(24
to 4
0)
133
(59
to 2
98)
013
93
Nor
th A
mer
ica
411
2 (6
4 to
196
)42
3 (2
12 to
84
6)2
23
(14
to 3
8)
205
(44
to 9
45)
A
ustra
lia3
63
(33
to 12
1)14
0 (6
3 to
30
8)2
20
(14
to 2
9)
67
(15
to 2
96)
Opio
id in
ject
ors (
)
lt
100
129
0 (6
9 to
117
)25
8 (1
87
to 3
55)
000
195
102
5 (2
0 to
30
)10
6 (6
1 to
185
)mdash
mdash
100
423
4 (1
42
to 3
85)
109
9 (5
94
to 2
034
)1
mdashsect
mdashsect
Men
()
lt
7511
95
(69
to 13
2)
300
(18
4 to
48
8)0
6798
62
4 (1
8 to
34
)10
6 (4
5 to
24
8)0
7493
ge
753
116
(61
to 2
20)
459
(178
to 11
79)
52
9 (2
0 to
42
)15
8 (6
2 to
40
3)M
ean
age
(yea
rs)
lt
3510
99
(68
to 14
5)
293
(179
to 4
82)
040
988
26
(19
to 3
5)
106
(52
to 2
18)
060
93
ge35
614
0 (8
7 to
22
7)50
3 (2
68
to 9
43)
32
7 (1
5 to
47
)20
5 (6
2 to
676
)Av
erag
e m
etha
done
dos
e (m
gda
y)
le
807
96
(63
to 14
8)
269
(15
5 to
46
5)0
5692
53
1 (2
0 to
46
)10
3 (4
0 to
26
9)0
2293
gt
805
99
(60
to 16
5)
354
(18
5 to
677
)5
25
(16
to 3
9)
170
(65
to 4
49)
Inpa
tient
indu
ctio
n (
)
09
92
(63
to 13
6)
299
(173
to 5
16)
019
987
25
(18
to 3
4)
100
(45
to 2
23)
065
93
gt0
615
4 (9
3 to
25
3)45
9 (2
29
to 9
21)
32
9 (1
7 to
50
)18
4 (5
4 to
62
5)Tr
eatm
ent p
rovi
der
S
peci
alis
t10
134
(92
to 19
5)
465
(28
2 to
765
)0
2698
72
5 (1
7 to
37
)20
8 (1
11 to
38
8)0
0188
G
Pm
ixed
68
6 (5
4 to
137
)24
4 (1
31
to 4
54)
42
4 (1
6 to
36
)5
6 (2
5 to
125
)M
idpo
int f
ollo
w-u
p pe
riod
lt
2000
1012
6 (8
5 to
187
)38
8 (2
28
to 6
61)
058
987
28
(20
to 3
9)
154
(70
to 3
39)
067
93
ge20
006
97
(60
to 15
9)
320
(16
5 to
62
3)4
24
(17
to 3
5)
90
(32
to 2
52)
Loss
to fo
llow
-up
()
lt
1012
119
(83
to 1
70)
383
(23
7 to
619
)0
8198
82
5 (1
9 to
32
)9
8 (5
0 to
195
)0
3393
ge
104
95
(50
to 18
0)
313
(13
5 to
72
3)3
32
(17
to 6
0)
254
(81
to 7
94)
Poo
led
mor
talit
y rat
es a
nd 9
5 c
onfid
ence
inte
rval
s dur
ing
perio
ds in
and
out
of t
reat
men
t by s
tudy
cha
ract
eris
tics e
stim
ated
from
sep
arat
e bi
varia
te ra
ndom
effe
cts m
eta-
regr
essi
on m
odel
s rel
atin
g lo
g tra
nsfo
rmed
rate
s in
both
trea
tmen
t per
iods
w
ith e
ach
stud
y cha
ract
eris
tic
daggerOve
rall
P va
lue
for h
eter
ogen
eity
of p
oole
d m
orta
lity r
ates
acr
oss c
ateg
orie
s of s
tudy
cha
ract
eris
tic a
s obt
aine
d fro
m li
kelih
ood
ratio
test
com
parin
g ne
sted
met
a-re
gres
sion
mod
els w
ith a
nd w
ithou
t stu
dy c
hara
cter
istic
fitte
d vi
a m
axim
um li
kelih
ood
DaggerOve
rall
I2 sta
tistic
for r
esid
ual h
eter
ogen
eity
in s
tudy
spe
cific
mor
talit
y rat
es n
ot e
xpla
ined
by c
orre
spon
ding
stu
dy c
hara
cter
istic
sectP
oole
d m
orta
lity r
ates
not
app
licab
le to
cat
egor
ies w
ith s
ingl
e st
udy
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
9
Although the long half life of methadone could con-tribute to the increase in mortality in the first three to four days after cessation of treatment there was a large increase in mortality across the first four weeks after cessation compared with the treatment period Such increased mortality could be explained by loss of toler-ance to the toxic effects of heroin assuming that many patients return to use6 8 32 47 55 56 and probably also by the use of multiple legal and illicit substances during that period Similar peaks in drug related mortality occur in other situations where opioid tolerance is prob-ably diminished (for example after prison release or hospital discharge57-59 ) Lifestyle factors and comorbid issues such as mental health problems could also increase mortality from other external causes as deaths from suicide and injury are also more common during that period53
Mortality risk during specific periods in and out of buprenorphine treatmentData from three cohorts (two from Australia) suggest that substitution treatment with buprenorphine could reduce all cause mortality although the disparity in mortality rates in periods in and out of treatment did not reach significance Findings also suggest a signifi-cantly increased mortality in the first four weeks after cessation of treatment compared with the remaining time out of treatment (320 versus 1091000 person years) while during the treatment period there was no difference between the first four weeks and the remain-ing time in treatment It is difficult to draw firm conclu-sions because of limited evidence from similar settings 96 of included deaths and 98 of person years came from Australian studies (with 87 and 86 from the study by Kimber and colleagues13)
Comparative effectiveness of buprenorphine and methadone substitution treatmentOther sources of data have suggested that buprenor-phine could be more effective than methadone in reduc-ing mortality especially from overdose39 42 43 Unlike methadone there is a ceiling for respiratory depressant effects of buprenorphine as dose increases and the probability of triggering arrhythmias is lower for buprenorphine than methadone41 44 60 When we com-pared the mortality between periods in and out of treat-ment first within those taking methadone and then within those taking buprenorphine we found a greater reduction in mortality with methadone than with buprenorphine (measured as the rate difference or rate ratio between periods) When we compared mortality between them first within the treatment period and then in the period off treatment we found a signifi-cantly lower mortality with buprenorphine than meth-adone in both periods
Our conclusions must remain tentative until further studies in varied treatment settings and contexts are undertaken to examine this issue Differences in mor-tality might also reflect confounding through differ-ences in characteristics of patients (such as age severity of opioid dependence injecting drug use other ta
ble
4 | C
ohor
t stu
dies
repo
rtin
g al
l cau
se a
nd o
verd
ose
mor
talit
y rat
e ra
tios c
ompa
ring
perio
ds o
ut a
nd in
opi
oid
subs
titut
ion
treat
men
t adj
uste
d fo
r con
foun
ding
stud
y
Conf
ound
ing
fact
ors
all c
ause
mor
talit
yO
verd
ose
mor
talit
y
Patie
nt d
emog
raph
ics
seve
rity
of d
rug
use
trea
tmen
tCo
mor
bidi
tyun
adju
sted
ra
te ra
tioad
just
ed
rate
ratio
Perc
enta
ge
chan
gedagger
unad
just
ed
rate
ratio
adju
sted
ra
te ra
tioPe
rcen
tage
ch
ange
dagger
Met
hado
neBu
ster
200
27Se
x ra
ceTr
eatm
ent m
odal
ity t
ime
sinc
e fir
st tr
eatm
ent
mdashmdash
mdashmdash
087
087
minus03
Davo
li 2
00732
Age
sex
Leng
th o
f her
oin
use
her
oin
inje
ctio
n
prev
ious
ove
rdos
eHI
V p
sych
iatri
c com
orbi
dity
mdashmdash
mdash77
174
3minus3
6
Dege
nhar
dt 2
0096
Age
sex
cal
enda
r yea
rmdash
mdash19
118
8minus1
3mdash
mdashmdash
Corn
ish
201
08Ag
e s
ex c
alen
dar y
ear
mdashM
edic
al c
omor
bidi
ty2
833
2715
5mdash
mdashmdash
Evan
s 2
0159Dagger
Age
sex
rac
e e
duca
tion
em
ploy
men
t cr
imin
ality
hea
lth c
over
age
Prim
ary o
pioi
d fr
eque
ncy a
nd le
ngth
of
opio
id u
se n
on-o
pioi
d dr
ug u
seHI
V h
epat
itis C
tub
ercu
losi
s
disa
bilit
y m
edic
al c
omor
bidi
ty
psyc
hiat
ric c
omor
bidi
ty
273
370
355
351
442
258
Nosy
k 2
01536
DaggerAg
e s
ex r
ace
cal
enda
r yea
r re
gion
No o
f pre
viou
s tre
atm
ent e
piso
des
Tim
e si
nce
HIV
diag
nosi
s C
D4
coun
t AI
DS a
ntire
trovi
ral
ther
apy
med
ical
com
orbi
dity
304
294
minus34
114
147
286
Cous
ins
201
637Ag
e s
exTr
eatm
ent s
uper
visi
on m
etha
done
dos
eM
edic
al c
omor
bidi
ty3
093
6417
816
016
317
bupr
enor
phin
eCo
rnis
h 2
0108
Age
sex
cal
enda
r yea
rmdash
Med
ical
com
orbi
dity
141
164
168
mdashmdash
mdashB
asel
ine
or ti
me
vary
ing
conf
ound
ing
fact
ors u
sed
in a
djus
tmen
tdaggerP
erce
ntag
e ch
ange
in ra
te ra
tio a
fter a
djus
tmen
t for
cor
resp
ondi
ng c
onfo
undi
ng fa
ctor
sDaggerO
verd
ose
mor
talit
y rat
e ra
tios r
epor
ted
com
bini
ng m
etha
done
mai
nten
ance
with
det
oxifi
catio
n (1
14
of p
erso
n ye
ars i
n tre
atm
ent)
in E
vans
et a
l9 an
d in
clud
ing
neve
r tre
ated
par
ticip
ants
(73
3 o
f per
son
year
s out
of t
reat
men
t) in
Nos
yk e
t al36
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
10
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1996 Buster et al 2002 Scherbaum et al 2002 Davoli et al 2007 Clausen et al 2008 Peles et al 2010 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine Kimber et al 2015
2105 5 10 20 50 100
3314 474416557108541792
4218 7476111475751
24645053985
16991 7925422 648
3121 936
In treatment
2111707297
27740192004
2610 983131729998
28130313727
21645 265246247
14331 239
Out of treatment
No of deathsperson years
23 (16 to 32)24 (07 to 62)
64 (26 to 133)22 (06 to 57)22 (16 to 30)
54 (20 to 117)12 (05 to 25)37 (24 to 55)12 (04 to 29)18 (16 to 21)24 (18 to 31)26 (21 to 33)
14 (10 to 20)
In treatment
179 (111 to 274)236 (95 to 486)
365 (240 to 531)95 (57 to 148)24 (16 to 35)
756 (402 to 1292)90 (41 to 171)
215 (143 to 311)179 (95 to 306)
48 (42 to 54)38 (25 to 57)
127 (69 to 234)
46 (39 to 54)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 3 | Overdose mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled overdose mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates during periods in and out of treatment across all methadone cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
Methadone rst four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallMethadone aer four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Cornish et al 2010 Kimber et al 2015OverallBuprenorphine aer four weeks Cornish et al 2010 Kimber et al 2015Overall
21 5 10 20 50 100
9425057465
151950323344
4100153371
554109 033234664
14823 32760488 449
85388010019 277
18192094
66597819 842
In treatment
38189821479
154267335183679113
441181
1472103 838503809
69445 44952843 4301271469545067
788281674
366328629 565
Out of treatment
No of deathsperson years
375 (303 to 459)151 (61 to 311)77 (43 to 127)96 (66 to 135)
mdash44 (25 to 73)
114 (58 to 224)
51 (47 to 55)49 (31 to 74)63 (54 to 74)68 (63 to 74)
mdash52 (42 to 63)58 (50 to 67)
124 (03 to 692)43 (20 to 82)
45 (12 to 168)
91 (33 to 198)39 (31 to 49)45 (32 to 62)
In treatment
200 (142 to 275)438 (271 to 670)576 (489 to 675)191 (133 to 265)
mdash373 (271 to 500)321 (191 to 539)
142 (135 to 149)131 (97 to 173)
153 (141 to 164)122 (111 to 132)
mdash107 (80 to 139)
135 (119 to 153)
800 (322 to 1648)167 (111 to 242)320 (132 to 775)
45 (09 to 132)97 (86 to 109)
109 (85 to 139)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 4 | all cause mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled all cause mortality rates 2009-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except Degenhardt et al6 which reported mortality before and after two weeks of treatment initiation and cessation high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-analysis area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates before and after four weeks in and out of treatment across methadone or buprenorphine cohorts estimated from multivariate random effects meta-analysis on log transformed rates in four time-by-treatment intervals
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
11
drug use comorbidities prison history overdose his-tory patientrsquos preference) characteristics of treatment (such as previous treatment specialisation of the doc-tor who controls the treatment dose provision charac-teristics cointerventions retention or drop outs) or the sociopolitical context in which studies have been conducted For example the initial prognosis might be better in those given buprenorphine than those given methadone (that is fewer comorbid problems less severe opioid dependence)6 8 10 61 though this was not clearly found in a recent US study62
The role of such confounding factors has received almost empirical examination Few details on char-acteristics of patients or treatments were reported in articles included in this meta-analysis to permit a detailed examination of this potential issue (tables 1 and 2 ) so it was not possible to assess the possibil-ity of confounding A sensitivity simulation analysis in the study by Kimber and colleagues however suggested that the lower mortality with buprenor-phine than with methadone during first four weeks of treatment was unlikely to be caused by unmea-sured confounding10
strengths and limitationsThis meta-analysis synthesised evidence from cohort studies published until 2016 on risk of mortality in people who are dependent on opioids during and after opioid substitution treatment separately for buprenor-phine and methadone Mortality changes over time (1st-32th week) during and after methadone are care-fully quantified for the first time
The published studies however had several methodological shortcomings Firstly in the included
Methadone rst four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallMethadone aer four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Kimber et al 2015Buprenorphine aer four weeks Kimber et al 2015
21 505 10 20
9150018334443371
3317 20015188 4495019 277
22094
2919 842
In treatment
2130010183681181
24960020643 430
165067
181674
12529 565
Out of treatment
No of deathsperson years
60 (27 to 114)54 (32 to 85)12 (03 to 30)35 (13 to 95)
19 (13 to 27)17 (14 to 20)26 (19 to 34)20 (15 to 27)
09 (01 to 34)
15 (10 to 21)
In treatment
15 (02 to 56)54 (26 to 100)68 (29 to 134)42 (18 to 99)
25 (16 to 37)47 (41 to 54)32 (18 to 51)34 (23 to 51)
108 (64 to 170)
42 (35 to 50)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 6 | Overdose mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled overdose mortality rates 2002-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except buster et al7 which reported mortality before and after two weeks of treatment initiation and cessation area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates before and after four weeks in and out of treatment across methadone cohorts estimated from multivariate random-effects meta-analysis on log transformed rates in four time-by-treatment intervals
Time since treatment initiation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s In methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Time since treatment cessation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s Out of methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Degenhardt et al 2009Cornish et al 2010Evans et al 2015Kimber et al 2015Cousins et al 2016
Fig 5 | all cause mortality rates by time since treatment initiation and cessation in methadone cohorts and pooled all cause mortality risk trends 2009-16 high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-regression area of each circle is proportional to weight of each time interval in meta-regression Pooled trends in all cause mortality risk (solid lines) and their 95 confidence intervals (shaded regions) over time in and out of methadone treatment were estimated from bivariate random effects meta-regression of log transformed rates on quadratic linear spline function of log time with knot at four weeks
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
12
observational studies the same patients are compared throughout follow-up periods in and out of opioid sub-stitution treatment but these patients leave and re-en-ter treatment in a non-random way and hence there could still be a large potential for confounding in com-parisons of crude mortality risk in and out of treat-ment In some studies with diverse information on patient demographics severity of drug use and comor-bidities measured mostly at baseline (table 3 ) adjust-ment for these potential confounders resulted in similar or even increased out-to-in mortality rate ratios which merely reflects that the above conditions tended to be less prevalent at baseline among patients who later left or were discharged from treatment than those who remained in treatment Nevertheless to obtain an unbiased estimate of the preventive effect of opioid substitution treatment on all cause and overdose mor-tality these and other relevant confounders should be measured every time a patient leaves and resumes treatment Time varying data can then be used to adjust for confounder history in standard regression models or even better to construct inverse probability of treatment weights for marginal structural models63 which properly control for time varying confounders for later treatment that are themselves affected by pre-vious treatment such as severity of drug use and comorbidity Also differential loss to follow-up is a concern in the meta-analysed cohorts as dropouts are more likely to occur in patients at higher risk of death during periods out of treatment thus inducing a selec-tion bias in crude comparisons of out-to-in mortality risk because of informative censoring Marginal struc-tural models with inverse probability of censoring weights can also be used to correct for differential loss to follow-up63 provided that common predictors of death and censoring are measured over time In sum-mary individual cohorts are prone to confounding and selection bias because of differential loss to follow-up but it is hard to assess with the available information the amount and direction of bias projected onto the pooled mortality rate differences and rate ratios between periods in and out of treatment obtained in this meta-analysis
Secondly studies were conducted in high income countries with the follow-up often spread over many calendar years (1965-2010 for methadone and 1990-2010 for buprenorphine) and a highly variable average length of follow-up (ranges 13-158 years and 11-45 years respectively) Studies in low and middle income countries are especially needed
Thirdly by design we have not captured overdose mortality when opioid substitution treatment was obtained on illicit drug markets40 64 Fourthly a delayed record of treatment cessation could have led to some deaths that occurred out of treatment being incorrectly classified as occurring in treatment40 if so this makes our estimated impact of opioid substitution treatment on mortality a conservative one There could similarly be misclassification between overdose and non-over-dose deaths because of inconsistencies in definition of overdose and codification of causes of deaths (for
instance criteria for separating overdose death from intentional poisoning or sudden cardiac death)40 65 again these misclassifications would tend to underesti-mate deaths from overdose
implications for policy and practiceIn many countries the number of deaths attributable to opioid use is substantial66 67 and increasing in some such as the US where deaths from opioid overdose now outnumber gun related deaths in the country68 Over-doses are preventable causes of death warranting wide implementation of preventive interventions Our review has provided evidence that methadone and probably buprenorphine reduce mortality among people depen-dent on opioids making it imperative that further research confirms this using study designs that con-sider a wide range of confounding variables to increase confidence that these effects are causal
It must be borne in mind that there is strong evidence of the efficacy of methadone and buprenorphine on a range of clinical outcomes and these medicines are listed as WHO essential medicines the findings we have presented here provide additional imperatives for their widespread availability Despite this coverage of opioid substitution treatment is low in many countries worldwide69 Policymakers clinicians and those responsible for drug treatment systems should work to ensure the availability of such treatment remove access barriers and promote engagement This means the strategic development of services from a public health perspective which could reduce the social harm associ-ated with opioid use
Our review suggests that some precautions should be taken during and after opioid substitution treatment to increase safety Firstly careful clinical assessment of opioid tolerance before onset of treatment to establish a safe induction dose seems warranted Secondly moni-toring during the induction period is important espe-cially for methadone with clinicians considering adjusting opioid doses monitoring mental and somatic problems and preventing the use of opioids obtained on the illicit drug market64 In addition education of patients about the risk of overdose risk and use of ldquotake homerdquo naloxone70 71 is warranted Buprenorphine induction followed by transition to methadone might also be considered10 72 Retention in opioid substitution treatment reduces risk of exposure to mortality after cessation and also to re-exposure to mortality risk during induction onto methadone so efforts to improve retention are important as a strategy to reduce mortal-ity More generally establishment of mechanisms for information and coordination between healthcare social and legal services and patient counselling while in treatment in addition to more specific overdose pre-vention programmes such as naloxone distribution should be considered
Finally there is a pressing need for new studies on the comparative effectiveness of methadone and buprenorphine in reducing mortality New ran-domised controlled trials are highly unlikely they would be prohibitively expensive and difficult to
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score
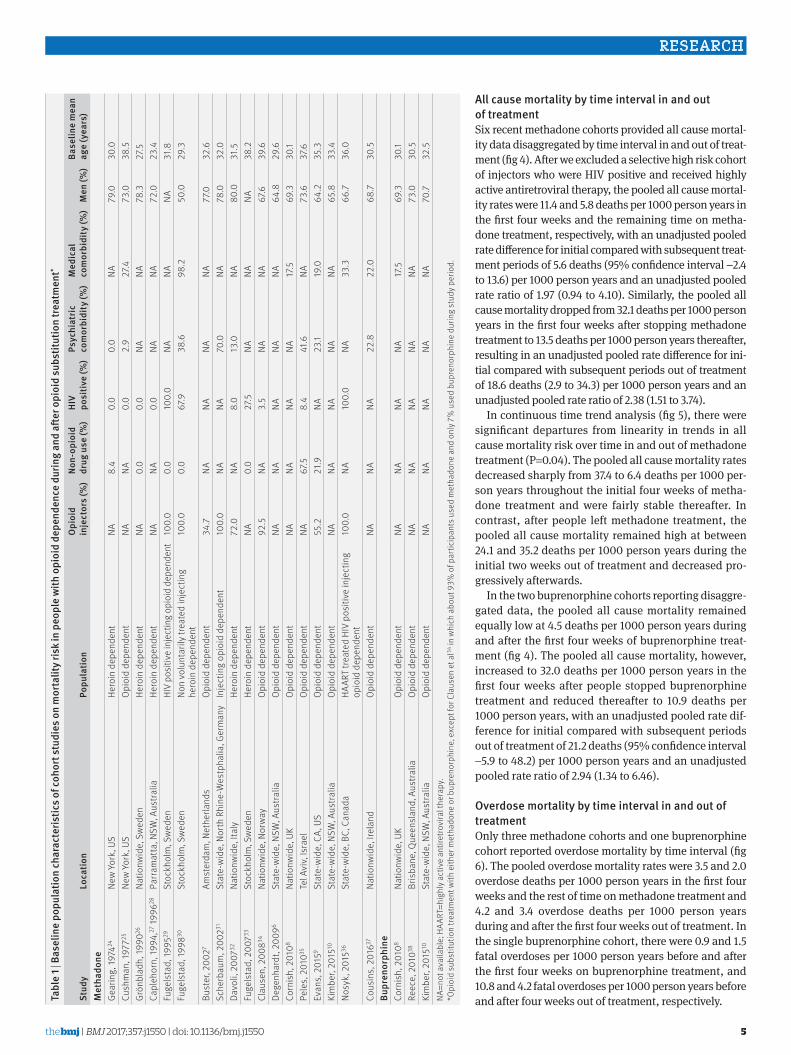
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
5
all cause mortality by time interval in and out of treatmentSix recent methadone cohorts provided all cause mortal-ity data disaggregated by time interval in and out of treat-ment (fig 4) After we excluded a selective high risk cohort of injectors who were HIV positive and received highly active antiretroviral therapy the pooled all cause mortal-ity rates were 114 and 58 deaths per 1000 person years in the first four weeks and the remaining time on metha-done treatment respectively with an unadjusted pooled rate difference for initial compared with subsequent treat-ment periods of 56 deaths (95 confidence interval minus24 to 136) per 1000 person years and an unadjusted pooled rate ratio of 197 (094 to 410) Similarly the pooled all cause mortality dropped from 321 deaths per 1000 person years in the first four weeks after stopping methadone treatment to 135 deaths per 1000 person years thereafter resulting in an unadjusted pooled rate difference for ini-tial compared with subsequent periods out of treatment of 186 deaths (29 to 343) per 1000 person years and an unadjusted pooled rate ratio of 238 (151 to 374)
In continuous time trend analysis (fig 5) there were significant departures from linearity in trends in all cause mortality risk over time in and out of methadone treatment (P=004) The pooled all cause mortality rates decreased sharply from 374 to 64 deaths per 1000 per-son years throughout the initial four weeks of metha-done treatment and were fairly stable thereafter In contrast after people left methadone treatment the pooled all cause mortality remained high at between 241 and 352 deaths per 1000 person years during the initial two weeks out of treatment and decreased pro-gressively afterwards
In the two buprenorphine cohorts reporting disaggre-gated data the pooled all cause mortality remained equally low at 45 deaths per 1000 person years during and after the first four weeks of buprenorphine treat-ment (fig 4) The pooled all cause mortality however increased to 320 deaths per 1000 person years in the first four weeks after people stopped buprenorphine treatment and reduced thereafter to 109 deaths per 1000 person years with an unadjusted pooled rate dif-ference for initial compared with subsequent periods out of treatment of 212 deaths (95 confidence interval minus59 to 482) per 1000 person years and an unadjusted pooled rate ratio of 294 (134 to 646)
Overdose mortality by time interval in and out of treatmentOnly three methadone cohorts and one buprenorphine cohort reported overdose mortality by time interval (fig 6) The pooled overdose mortality rates were 35 and 20 overdose deaths per 1000 person years in the first four weeks and the rest of time on methadone treatment and 42 and 34 overdose deaths per 1000 person years during and after the first four weeks out of treatment In the single buprenorphine cohort there were 09 and 15 fatal overdoses per 1000 person years before and after the first four weeks on buprenorphine treatment and 108 and 42 fatal overdoses per 1000 person years before and after four weeks out of treatment respectivelyta
ble
1 | b
asel
ine
popu
latio
n ch
arac
teris
tics o
f coh
ort s
tudi
es o
n m
orta
lity r
isk
in p
eopl
e w
ith o
pioi
d de
pend
ence
dur
ing
and
after
opi
oid
subs
titut
ion
treat
men
t
stud
ylo
catio
nPo
pula
tion
Opi
oid
in
ject
ors
()
non-
opio
id
drug
use
()
hiv
po
sitiv
e (
)Ps
ychi
atric
co
mor
bidi
ty (
)M
edic
al
com
orbi
dity
()
Men
()
base
line
mea
n ag
e (y
ears
)M
etha
done
Gear
ing
1974
24Ne
w Yo
rk U
SHe
roin
dep
ende
ntNA
84
00
00
NA79
030
0Cu
shm
an 1
97725
New
York
US
Opio
id d
epen
dent
NANA
00
29
274
730
385
Groumln
blad
h 19
9026
Natio
nwid
e S
wed
enHe
roin
dep
ende
ntNA
00
00
NANA
783
275
Capl
ehor
n 19
9427
1996
28Pa
rram
atta
NSW
Aus
tralia
Hero
in d
epen
dent
NANA
00
NANA
720
234
Fuge
lsta
d 19
9529
Stoc
khol
m S
wed
enHI
V po
sitiv
e in
ject
ing
opio
id d
epen
dent
100
00
010
00
NANA
NA31
8Fu
gels
tad
1998
30St
ockh
olm
Sw
eden
Non
volu
ntar
ily tr
eate
d in
ject
ing
hero
in d
epen
dent
100
00
067
938
698
250
029
3
Bust
er 2
0027
Amst
erda
m N
ethe
rland
sOp
ioid
dep
ende
nt34
7NA
NANA
NA77
032
6Sc
herb
aum
200
231St
ate-
wid
e N
orth
Rhi
ne-W
estp
halia
Ger
man
yIn
ject
ing
opio
id d
epen
dent
100
0NA
NA70
0NA
780
320
Davo
li 2
00732
Natio
nwid
e It
aly
Hero
in d
epen
dent
720
NA8
013
0NA
800
315
Fuge
lsta
d 2
00733
Stoc
khol
m S
wed
enHe
roin
dep
ende
ntNA
00
275
NANA
NA38
2Cl
ause
n 2
00834
Natio
nwid
e N
orw
ayOp
ioid
dep
ende
nt92
5NA
35
NANA
676
396
Dege
nhar
dt 2
0096
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA64
829
6Co
rnis
h 2
0108
Natio
nwid
e U
KOp
ioid
dep
ende
ntNA
NANA
NA17
569
330
1Pe
les
201
035Te
l Avi
v Is
rael
Opio
id d
epen
dent
NA67
58
441
6NA
736
376
Evan
s 2
0159
Stat
e-w
ide
CA
US
Opio
id d
epen
dent
552
219
NA23
119
064
235
3Ki
mbe
r 20
1510
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA65
833
4No
syk
201
536St
ate-
wid
e B
C C
anad
aHA
ART
treat
ed H
IV p
ositi
ve in
ject
ing
opio
id d
epen
dent
100
0NA
100
0NA
333
667
360
Cous
ins
201
637Na
tionw
ide
Irel
and
Opio
id d
epen
dent
NANA
NA22
822
068
730
5bu
pren
orph
ine
Corn
ish
201
08Na
tionw
ide
UK
Opio
id d
epen
dent
NANA
NANA
175
693
301
Reec
e 2
01038
Bris
bane
Que
ensl
and
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA73
030
5Ki
mbe
r 20
1510
Stat
e-w
ide
NSW
Aus
tralia
Opio
id d
epen
dent
NANA
NANA
NA70
732
5NA
=not
ava
ilabl
e H
AART
=hig
hly a
ctiv
e an
tiret
rovi
ral t
hera
py
Opi
oid
subs
titut
ion
treat
men
t with
eith
er m
etha
done
or b
upre
norp
hine
exc
ept f
or C
laus
en e
t al34
in w
hich
abo
ut 9
3 o
f par
ticip
ants
use
d m
etha
done
and
onl
y 7
use
d bu
pren
orph
ine
durin
g st
udy p
erio
d
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
6
tabl
e 2
| tre
atm
ent d
eliv
ery a
nd fo
llow
-up
feat
ures
of c
ohor
t stu
dies
on
mor
talit
y ris
k in
peo
ple
with
opi
oid
depe
nden
ce d
urin
g an
d aft
er o
pioi
d su
bstit
utio
n tre
atm
ent
stud
yno
of c
ohor
t pa
rtic
ipan
tsdagger
aver
age
Ost
do
se (m
gda
y)in
patie
nt
indu
ctio
n (
)O
st
prov
ider
Follo
w-u
p pe
riod
aver
age
follo
w-u
p (y
ears
)Dagger
loss
to
follo
w-u
p (
)sectM
orta
lity
outc
ome
Qua
lity
scor
epara
Met
hado
neGe
arin
g 19
7424
3000
100
176
Spec
ialis
t19
65-7
25
24
0Al
l cau
ses
ove
rdos
e9
Cush
man
197
72554
710
0NA
Spec
ialis
t19
66-7
53
623
2Al
l cau
ses
ove
rdos
e6
Groumln
blad
h 19
9026
166
7510
00
Spec
ialis
t19
67-8
711
00
0Al
l cau
ses
ove
rdos
e4
Capl
ehor
n 19
9427
1996
2830
511
632
3Sp
ecia
list
1970
-90
139
144
All c
ause
s27
ove
rdos
e286
Fuge
lsta
d 19
9529
135
NA10
00
Spec
ialis
t19
86-9
02
10
0Al
l cau
ses
6Fu
gels
tad
1998
3056
8010
00
Spec
ialis
t19
86-9
34
20
0Al
l cau
ses
6Bu
ster
200
2752
0048
00
Mix
ed19
86-9
85
70
0O
verd
ose
8Sc
herb
aum
200
23124
447
00
Spec
ialis
t19
88-9
65
315
6Al
l cau
ses
ove
rdos
e7
Davo
li 2
00732
5276
NA0
0Sp
ecia
list
1998
-200
11
33
7O
verd
ose
11Fu
gels
tad
200
73367
9NA
100
0Sp
ecia
list
1988
-200
06
96
2Al
l cau
ses
3Cl
ause
n 2
00834
3229
112
00
Mix
ed19
97-2
003
24
00
All c
ause
s o
verd
ose
7De
genh
ardt
200
9631
846
700
0M
ixed
1985
-200
0daggerdagger6
80
0Al
l cau
sesDaggerDagger
12Co
rnis
h 2
0108
4894
500
0GP
1990
-200
519
175
All c
ause
s9
Pele
s 2
01035
613
113
00
Spec
ialis
t19
93-2
008
770
8Al
l cau
ses
ove
rdos
e9
Evan
s 2
0159
32 32
2NA
00
Spec
ialis
t20
06-1
02
35
0Al
l cau
sesDaggerDagger
12Ki
mbe
r 20
1510
26 0
6470
00
Mix
ed20
01-1
05
30
0Al
l cau
ses
ove
rdos
e13
Nosy
k 2
01536
1326
NA0
0GP
1996
-201
04
279
All c
ause
sDaggerDagger13
Cous
ins
201
63769
8372
00
GP20
04-1
04
12
0Al
l cau
ses
ove
rdos
e12
bupr
enor
phin
eCo
rnis
h 2
0108
1373
100
0GP
1990
-200
511
103
All c
ause
s9
Reec
e 2
01038
2518
NA0
0GP
2000
-07
32
12Al
l cau
ses
5Ki
mbe
r 20
1510
11 94
012
00
Mix
ed20
01-1
04
50
0Al
l cau
ses
ove
rdos
e13
NA=n
ot a
vaila
ble
OST
=opi
oid
subs
titut
ion
treat
men
tO
pioi
d su
bstit
utio
n tre
atm
ent w
ith e
ither
met
hado
ne o
r bup
reno
rphi
ne e
xcep
t for
Cla
usen
et a
l34 in
whi
ch a
bout
93
of p
artic
ipan
ts u
sed
met
hado
ne a
nd o
nly 7
u
sed
bupr
enor
phin
e du
ring
stud
y per
iod
daggerPar
ticip
ants
rece
ivin
g op
ioid
sub
stitu
tion
treat
men
t at l
east
onc
e du
ring
stud
y per
iod
Unt
reat
ed p
artic
ipan
ts a
nd th
ose
rece
ivin
g ot
her t
ypes
of t
reat
men
t for
opi
oid
depe
nden
ce (m
etha
done
det
oxifi
catio
n o
pioi
d an
tago
nist
ther
apy
ther
apeu
tic
com
mun
ity) e
xclu
ded
from
met
a-an
alys
is
DaggerAve
rage
follo
w-u
p fro
m s
tart
of o
pioi
d su
bstit
utio
n tre
atm
ent c
ombi
ning
sub
sequ
ent p
erio
ds in
and
out
of t
reat
men
tsectP
erce
ntag
e lo
ss to
follo
w-u
p be
fore
end
of s
tudy
per
iod
or d
eath
If n
ot o
ther
wis
e sp
ecifi
ed c
ompl
ete
case
asc
erta
inm
ent a
ssum
ed fo
r stu
dies
bas
ed o
n po
pula
tion
mor
talit
y reg
istri
es
paraQua
lity a
sses
smen
t sco
re ra
ngin
g fro
m 0
(low
est q
ualit
y) to
16 (h
ighe
st q
ualit
y)
O
verd
ose
mor
talit
y rep
orte
d bu
t not
incl
uded
in m
eta-
anal
ysis
as t
here
wer
e no
ove
rdos
e de
aths
whi
le p
artic
ipan
ts w
ere
in o
pioi
d su
bstit
utio
n tre
atm
ent
daggerdaggerFo
llow
-up
rest
ricte
d to
1985
-200
0 as
sub
sequ
ent 2
001-
06 fo
llow
-up
perio
d ov
erla
pped
with
Kim
ber e
t al10
DaggerDaggerO
verd
ose
mor
talit
y rep
orte
d on
ly fo
r com
bine
d tre
atm
ents
or i
nclu
ded
untre
ated
par
ticip
ants
and
hen
ce n
ot in
clud
ed in
met
a-an
alys
is
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
7
discussionMain findingsOur review suggests that time spent in opioid substitu-tion treatment with methadone is associated with an average reduction of 25 deaths1000 person years (95 confidence interval 14 to 36) The rate in treatment was less than a third of the rate out of treatment with the greatest difference in deaths from overdose The all cause mortality risk during treatment is much higher in the first four weeks than in the remainder of treatment Mortality risk is also higher in the first four weeks after cessation than in the remainder time out of treatment
Based on three cohorts (two from Australia) findings also suggest that opioid substitution treatment with buprenorphine could be associated with a reduction in mortality with a similar risk across all time in treatment (about four deaths1000 person years) consistent with its safety profile39-44 and a risk after cessation higher in the first four weeks than in the remainder of time out of treatment (32 versus 11 deaths1000 person years)
Mortality risk during specific periods in and out of methadone treatmentThe larger relative effect size (as measured by rate ratio) for overdose than non-overdose deaths with metha-done substitution6 11 34 45 is consistent with previous findings although the effect on non-overdose deaths had not been previously reviewed This disparity is
consistent with what would be expected given metha-donersquos effect on reducing use of heroin and other illicit opioids32 34
Our finding that the first four weeks after onset (114 deaths1000 person years) and cessation (3211000 person years) of methadone treatment are the highest risk periods suggests that these are key periods during which to focus efforts for prevention of drug related deaths Moreover within periods of methadone treat-ment there is a swift decline in risk from first to fourth week followed by a stable trend whereas after cessa-tion there is a high but quite stable risk during the first four weeks and a progressive decline afterward This is important because some patients cycle in and out of opioid substitution treatment46-50 and are therefore exposed to repeated periods of high risk for mortality Such changes probably mainly reflect changes in risk of fatal overdose6 32 but this has not been accurately assessed because only two cohorts reported overdose data specifically7 10 The increased risk during the first few weeks of treatment could be explained by an accu-mulation of methadone that exceeds the opioid toler-ance level (the mean elimination half life for methadone is 22 hours)51 as opioid tolerance does not seem to fully protect against respiratory depression52 Psychological factors and concomitant use of other respiratory depressant drugs or cocaine could also play a role7 8 40 53 54
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1994 Fugelstad et al 1995 Fugelstad et al 1998 Scherbaum et al 2002 Fugelstad et al 2007 Clausen et al 2008 Degenhardt et al 2009 Cornish et al 2010 Peles et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine Cornish et al 2010 Reece 2010 Kimber et al 2015Overall
2 5 10 20 50 100 200
11014 474251655161085111975
82427177
181114773354906450
648111 538305129423985
16325 27763691 792
89397911522 648
774031119
8721 936
In treatment
3311701429732740
362279545457
14172741311461303
1510105 73571428852727
84848 12256345 2652061582986247
10751406911
31431 239
Out of treatment
No of deathsperson years
76 (62 to 92)151 (98 to 223)148 (84 to 239)56 (28 to 100)
331 (143 to 651)395 (159 to 814)162 (96 to 255)
230 (181 to 287)140 (112 to 171)
58 (54 to 63)58 (40 to 83)
105 (76 to 142)64 (55 to 75)69 (64 to 75)
224 (180 to 275)51 (42 to 61)
113 (84 to 152)
95 (38 to 195)27 (06 to 78)40 (32 to 49)43 (21 to 89)
In treatment
282 (194 to 396)471 (258 to 791)432 (296 to 610)158 (111 to 219)
1111 (361 to 2593)699 (191 to 1790)814 (445 to 1366)565 (443 to 709)353 (259 to 471)143 (136 to 150)166 (129 to 209)715 (534 to 938)176 (165 to 188)124 (114 to 135)
1302 (1130 to 1493)157 (127 to 191)361 (245 to 533)
133 (64 to 245)58 (41 to 79)
101 (90 to 112)95 (39 to 234)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 2 | all cause mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled all cause mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates during periods in and out of treatment across all methadone or buprenorphine cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
8
tabl
e 3
| Poo
led
all c
ause
and
ove
rdos
e m
orta
lity r
ates
dur
ing
perio
ds in
and
out
of o
pioi
d su
bstit
utio
n tre
atm
ent w
ith m
etha
done
by s
tudy
char
acte
ristic
s
stud
y ch
arac
teris
tic
all c
ause
mor
talit
y ra
te1
000
pers
on y
ears
(95
Ci)
Ove
rdos
e m
orta
lity
rate
100
0 pe
rson
yea
rs (9
5 C
i)
no o
f st
udie
sin
trea
tmen
tO
ut o
f tre
atm
ent
P va
luedagger
i2 (
)Daggerno
of
stud
ies
in tr
eatm
ent
Out
of t
reat
men
tP
valu
edaggeri2 (
)Dagger
Loca
tion
E
urop
eIs
rael
913
9 (9
5 to
20
5)46
6 (2
90
to 74
9)
008
987
31
(24
to 4
0)
133
(59
to 2
98)
013
93
Nor
th A
mer
ica
411
2 (6
4 to
196
)42
3 (2
12 to
84
6)2
23
(14
to 3
8)
205
(44
to 9
45)
A
ustra
lia3
63
(33
to 12
1)14
0 (6
3 to
30
8)2
20
(14
to 2
9)
67
(15
to 2
96)
Opio
id in
ject
ors (
)
lt
100
129
0 (6
9 to
117
)25
8 (1
87
to 3
55)
000
195
102
5 (2
0 to
30
)10
6 (6
1 to
185
)mdash
mdash
100
423
4 (1
42
to 3
85)
109
9 (5
94
to 2
034
)1
mdashsect
mdashsect
Men
()
lt
7511
95
(69
to 13
2)
300
(18
4 to
48
8)0
6798
62
4 (1
8 to
34
)10
6 (4
5 to
24
8)0
7493
ge
753
116
(61
to 2
20)
459
(178
to 11
79)
52
9 (2
0 to
42
)15
8 (6
2 to
40
3)M
ean
age
(yea
rs)
lt
3510
99
(68
to 14
5)
293
(179
to 4
82)
040
988
26
(19
to 3
5)
106
(52
to 2
18)
060
93
ge35
614
0 (8
7 to
22
7)50
3 (2
68
to 9
43)
32
7 (1
5 to
47
)20
5 (6
2 to
676
)Av
erag
e m
etha
done
dos
e (m
gda
y)
le
807
96
(63
to 14
8)
269
(15
5 to
46
5)0
5692
53
1 (2
0 to
46
)10
3 (4
0 to
26
9)0
2293
gt
805
99
(60
to 16
5)
354
(18
5 to
677
)5
25
(16
to 3
9)
170
(65
to 4
49)
Inpa
tient
indu
ctio
n (
)
09
92
(63
to 13
6)
299
(173
to 5
16)
019
987
25
(18
to 3
4)
100
(45
to 2
23)
065
93
gt0
615
4 (9
3 to
25
3)45
9 (2
29
to 9
21)
32
9 (1
7 to
50
)18
4 (5
4 to
62
5)Tr
eatm
ent p
rovi
der
S
peci
alis
t10
134
(92
to 19
5)
465
(28
2 to
765
)0
2698
72
5 (1
7 to
37
)20
8 (1
11 to
38
8)0
0188
G
Pm
ixed
68
6 (5
4 to
137
)24
4 (1
31
to 4
54)
42
4 (1
6 to
36
)5
6 (2
5 to
125
)M
idpo
int f
ollo
w-u
p pe
riod
lt
2000
1012
6 (8
5 to
187
)38
8 (2
28
to 6
61)
058
987
28
(20
to 3
9)
154
(70
to 3
39)
067
93
ge20
006
97
(60
to 15
9)
320
(16
5 to
62
3)4
24
(17
to 3
5)
90
(32
to 2
52)
Loss
to fo
llow
-up
()
lt
1012
119
(83
to 1
70)
383
(23
7 to
619
)0
8198
82
5 (1
9 to
32
)9
8 (5
0 to
195
)0
3393
ge
104
95
(50
to 18
0)
313
(13
5 to
72
3)3
32
(17
to 6
0)
254
(81
to 7
94)
Poo
led
mor
talit
y rat
es a
nd 9
5 c
onfid
ence
inte
rval
s dur
ing
perio
ds in
and
out
of t
reat
men
t by s
tudy
cha
ract
eris
tics e
stim
ated
from
sep
arat
e bi
varia
te ra
ndom
effe
cts m
eta-
regr
essi
on m
odel
s rel
atin
g lo
g tra
nsfo
rmed
rate
s in
both
trea
tmen
t per
iods
w
ith e
ach
stud
y cha
ract
eris
tic
daggerOve
rall
P va
lue
for h
eter
ogen
eity
of p
oole
d m
orta
lity r
ates
acr
oss c
ateg
orie
s of s
tudy
cha
ract
eris
tic a
s obt
aine
d fro
m li
kelih
ood
ratio
test
com
parin
g ne
sted
met
a-re
gres
sion
mod
els w
ith a
nd w
ithou
t stu
dy c
hara
cter
istic
fitte
d vi
a m
axim
um li
kelih
ood
DaggerOve
rall
I2 sta
tistic
for r
esid
ual h
eter
ogen
eity
in s
tudy
spe
cific
mor
talit
y rat
es n
ot e
xpla
ined
by c
orre
spon
ding
stu
dy c
hara
cter
istic
sectP
oole
d m
orta
lity r
ates
not
app
licab
le to
cat
egor
ies w
ith s
ingl
e st
udy
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
9
Although the long half life of methadone could con-tribute to the increase in mortality in the first three to four days after cessation of treatment there was a large increase in mortality across the first four weeks after cessation compared with the treatment period Such increased mortality could be explained by loss of toler-ance to the toxic effects of heroin assuming that many patients return to use6 8 32 47 55 56 and probably also by the use of multiple legal and illicit substances during that period Similar peaks in drug related mortality occur in other situations where opioid tolerance is prob-ably diminished (for example after prison release or hospital discharge57-59 ) Lifestyle factors and comorbid issues such as mental health problems could also increase mortality from other external causes as deaths from suicide and injury are also more common during that period53
Mortality risk during specific periods in and out of buprenorphine treatmentData from three cohorts (two from Australia) suggest that substitution treatment with buprenorphine could reduce all cause mortality although the disparity in mortality rates in periods in and out of treatment did not reach significance Findings also suggest a signifi-cantly increased mortality in the first four weeks after cessation of treatment compared with the remaining time out of treatment (320 versus 1091000 person years) while during the treatment period there was no difference between the first four weeks and the remain-ing time in treatment It is difficult to draw firm conclu-sions because of limited evidence from similar settings 96 of included deaths and 98 of person years came from Australian studies (with 87 and 86 from the study by Kimber and colleagues13)
Comparative effectiveness of buprenorphine and methadone substitution treatmentOther sources of data have suggested that buprenor-phine could be more effective than methadone in reduc-ing mortality especially from overdose39 42 43 Unlike methadone there is a ceiling for respiratory depressant effects of buprenorphine as dose increases and the probability of triggering arrhythmias is lower for buprenorphine than methadone41 44 60 When we com-pared the mortality between periods in and out of treat-ment first within those taking methadone and then within those taking buprenorphine we found a greater reduction in mortality with methadone than with buprenorphine (measured as the rate difference or rate ratio between periods) When we compared mortality between them first within the treatment period and then in the period off treatment we found a signifi-cantly lower mortality with buprenorphine than meth-adone in both periods
Our conclusions must remain tentative until further studies in varied treatment settings and contexts are undertaken to examine this issue Differences in mor-tality might also reflect confounding through differ-ences in characteristics of patients (such as age severity of opioid dependence injecting drug use other ta
ble
4 | C
ohor
t stu
dies
repo
rtin
g al
l cau
se a
nd o
verd
ose
mor
talit
y rat
e ra
tios c
ompa
ring
perio
ds o
ut a
nd in
opi
oid
subs
titut
ion
treat
men
t adj
uste
d fo
r con
foun
ding
stud
y
Conf
ound
ing
fact
ors
all c
ause
mor
talit
yO
verd
ose
mor
talit
y
Patie
nt d
emog
raph
ics
seve
rity
of d
rug
use
trea
tmen
tCo
mor
bidi
tyun
adju
sted
ra
te ra
tioad
just
ed
rate
ratio
Perc
enta
ge
chan
gedagger
unad
just
ed
rate
ratio
adju
sted
ra
te ra
tioPe
rcen
tage
ch
ange
dagger
Met
hado
neBu
ster
200
27Se
x ra
ceTr
eatm
ent m
odal
ity t
ime
sinc
e fir
st tr
eatm
ent
mdashmdash
mdashmdash
087
087
minus03
Davo
li 2
00732
Age
sex
Leng
th o
f her
oin
use
her
oin
inje
ctio
n
prev
ious
ove
rdos
eHI
V p
sych
iatri
c com
orbi
dity
mdashmdash
mdash77
174
3minus3
6
Dege
nhar
dt 2
0096
Age
sex
cal
enda
r yea
rmdash
mdash19
118
8minus1
3mdash
mdashmdash
Corn
ish
201
08Ag
e s
ex c
alen
dar y
ear
mdashM
edic
al c
omor
bidi
ty2
833
2715
5mdash
mdashmdash
Evan
s 2
0159Dagger
Age
sex
rac
e e
duca
tion
em
ploy
men
t cr
imin
ality
hea
lth c
over
age
Prim
ary o
pioi
d fr
eque
ncy a
nd le
ngth
of
opio
id u
se n
on-o
pioi
d dr
ug u
seHI
V h
epat
itis C
tub
ercu
losi
s
disa
bilit
y m
edic
al c
omor
bidi
ty
psyc
hiat
ric c
omor
bidi
ty
273
370
355
351
442
258
Nosy
k 2
01536
DaggerAg
e s
ex r
ace
cal
enda
r yea
r re
gion
No o
f pre
viou
s tre
atm
ent e
piso
des
Tim
e si
nce
HIV
diag
nosi
s C
D4
coun
t AI
DS a
ntire
trovi
ral
ther
apy
med
ical
com
orbi
dity
304
294
minus34
114
147
286
Cous
ins
201
637Ag
e s
exTr
eatm
ent s
uper
visi
on m
etha
done
dos
eM
edic
al c
omor
bidi
ty3
093
6417
816
016
317
bupr
enor
phin
eCo
rnis
h 2
0108
Age
sex
cal
enda
r yea
rmdash
Med
ical
com
orbi
dity
141
164
168
mdashmdash
mdashB
asel
ine
or ti
me
vary
ing
conf
ound
ing
fact
ors u
sed
in a
djus
tmen
tdaggerP
erce
ntag
e ch
ange
in ra
te ra
tio a
fter a
djus
tmen
t for
cor
resp
ondi
ng c
onfo
undi
ng fa
ctor
sDaggerO
verd
ose
mor
talit
y rat
e ra
tios r
epor
ted
com
bini
ng m
etha
done
mai
nten
ance
with
det
oxifi
catio
n (1
14
of p
erso
n ye
ars i
n tre
atm
ent)
in E
vans
et a
l9 an
d in
clud
ing
neve
r tre
ated
par
ticip
ants
(73
3 o
f per
son
year
s out
of t
reat
men
t) in
Nos
yk e
t al36
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
10
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1996 Buster et al 2002 Scherbaum et al 2002 Davoli et al 2007 Clausen et al 2008 Peles et al 2010 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine Kimber et al 2015
2105 5 10 20 50 100
3314 474416557108541792
4218 7476111475751
24645053985
16991 7925422 648
3121 936
In treatment
2111707297
27740192004
2610 983131729998
28130313727
21645 265246247
14331 239
Out of treatment
No of deathsperson years
23 (16 to 32)24 (07 to 62)
64 (26 to 133)22 (06 to 57)22 (16 to 30)
54 (20 to 117)12 (05 to 25)37 (24 to 55)12 (04 to 29)18 (16 to 21)24 (18 to 31)26 (21 to 33)
14 (10 to 20)
In treatment
179 (111 to 274)236 (95 to 486)
365 (240 to 531)95 (57 to 148)24 (16 to 35)
756 (402 to 1292)90 (41 to 171)
215 (143 to 311)179 (95 to 306)
48 (42 to 54)38 (25 to 57)
127 (69 to 234)
46 (39 to 54)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 3 | Overdose mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled overdose mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates during periods in and out of treatment across all methadone cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
Methadone rst four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallMethadone aer four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Cornish et al 2010 Kimber et al 2015OverallBuprenorphine aer four weeks Cornish et al 2010 Kimber et al 2015Overall
21 5 10 20 50 100
9425057465
151950323344
4100153371
554109 033234664
14823 32760488 449
85388010019 277
18192094
66597819 842
In treatment
38189821479
154267335183679113
441181
1472103 838503809
69445 44952843 4301271469545067
788281674
366328629 565
Out of treatment
No of deathsperson years
375 (303 to 459)151 (61 to 311)77 (43 to 127)96 (66 to 135)
mdash44 (25 to 73)
114 (58 to 224)
51 (47 to 55)49 (31 to 74)63 (54 to 74)68 (63 to 74)
mdash52 (42 to 63)58 (50 to 67)
124 (03 to 692)43 (20 to 82)
45 (12 to 168)
91 (33 to 198)39 (31 to 49)45 (32 to 62)
In treatment
200 (142 to 275)438 (271 to 670)576 (489 to 675)191 (133 to 265)
mdash373 (271 to 500)321 (191 to 539)
142 (135 to 149)131 (97 to 173)
153 (141 to 164)122 (111 to 132)
mdash107 (80 to 139)
135 (119 to 153)
800 (322 to 1648)167 (111 to 242)320 (132 to 775)
45 (09 to 132)97 (86 to 109)
109 (85 to 139)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 4 | all cause mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled all cause mortality rates 2009-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except Degenhardt et al6 which reported mortality before and after two weeks of treatment initiation and cessation high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-analysis area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates before and after four weeks in and out of treatment across methadone or buprenorphine cohorts estimated from multivariate random effects meta-analysis on log transformed rates in four time-by-treatment intervals
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
11
drug use comorbidities prison history overdose his-tory patientrsquos preference) characteristics of treatment (such as previous treatment specialisation of the doc-tor who controls the treatment dose provision charac-teristics cointerventions retention or drop outs) or the sociopolitical context in which studies have been conducted For example the initial prognosis might be better in those given buprenorphine than those given methadone (that is fewer comorbid problems less severe opioid dependence)6 8 10 61 though this was not clearly found in a recent US study62
The role of such confounding factors has received almost empirical examination Few details on char-acteristics of patients or treatments were reported in articles included in this meta-analysis to permit a detailed examination of this potential issue (tables 1 and 2 ) so it was not possible to assess the possibil-ity of confounding A sensitivity simulation analysis in the study by Kimber and colleagues however suggested that the lower mortality with buprenor-phine than with methadone during first four weeks of treatment was unlikely to be caused by unmea-sured confounding10
strengths and limitationsThis meta-analysis synthesised evidence from cohort studies published until 2016 on risk of mortality in people who are dependent on opioids during and after opioid substitution treatment separately for buprenor-phine and methadone Mortality changes over time (1st-32th week) during and after methadone are care-fully quantified for the first time
The published studies however had several methodological shortcomings Firstly in the included
Methadone rst four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallMethadone aer four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Kimber et al 2015Buprenorphine aer four weeks Kimber et al 2015
21 505 10 20
9150018334443371
3317 20015188 4495019 277
22094
2919 842
In treatment
2130010183681181
24960020643 430
165067
181674
12529 565
Out of treatment
No of deathsperson years
60 (27 to 114)54 (32 to 85)12 (03 to 30)35 (13 to 95)
19 (13 to 27)17 (14 to 20)26 (19 to 34)20 (15 to 27)
09 (01 to 34)
15 (10 to 21)
In treatment
15 (02 to 56)54 (26 to 100)68 (29 to 134)42 (18 to 99)
25 (16 to 37)47 (41 to 54)32 (18 to 51)34 (23 to 51)
108 (64 to 170)
42 (35 to 50)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 6 | Overdose mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled overdose mortality rates 2002-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except buster et al7 which reported mortality before and after two weeks of treatment initiation and cessation area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates before and after four weeks in and out of treatment across methadone cohorts estimated from multivariate random-effects meta-analysis on log transformed rates in four time-by-treatment intervals
Time since treatment initiation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s In methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Time since treatment cessation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s Out of methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Degenhardt et al 2009Cornish et al 2010Evans et al 2015Kimber et al 2015Cousins et al 2016
Fig 5 | all cause mortality rates by time since treatment initiation and cessation in methadone cohorts and pooled all cause mortality risk trends 2009-16 high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-regression area of each circle is proportional to weight of each time interval in meta-regression Pooled trends in all cause mortality risk (solid lines) and their 95 confidence intervals (shaded regions) over time in and out of methadone treatment were estimated from bivariate random effects meta-regression of log transformed rates on quadratic linear spline function of log time with knot at four weeks
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
12
observational studies the same patients are compared throughout follow-up periods in and out of opioid sub-stitution treatment but these patients leave and re-en-ter treatment in a non-random way and hence there could still be a large potential for confounding in com-parisons of crude mortality risk in and out of treat-ment In some studies with diverse information on patient demographics severity of drug use and comor-bidities measured mostly at baseline (table 3 ) adjust-ment for these potential confounders resulted in similar or even increased out-to-in mortality rate ratios which merely reflects that the above conditions tended to be less prevalent at baseline among patients who later left or were discharged from treatment than those who remained in treatment Nevertheless to obtain an unbiased estimate of the preventive effect of opioid substitution treatment on all cause and overdose mor-tality these and other relevant confounders should be measured every time a patient leaves and resumes treatment Time varying data can then be used to adjust for confounder history in standard regression models or even better to construct inverse probability of treatment weights for marginal structural models63 which properly control for time varying confounders for later treatment that are themselves affected by pre-vious treatment such as severity of drug use and comorbidity Also differential loss to follow-up is a concern in the meta-analysed cohorts as dropouts are more likely to occur in patients at higher risk of death during periods out of treatment thus inducing a selec-tion bias in crude comparisons of out-to-in mortality risk because of informative censoring Marginal struc-tural models with inverse probability of censoring weights can also be used to correct for differential loss to follow-up63 provided that common predictors of death and censoring are measured over time In sum-mary individual cohorts are prone to confounding and selection bias because of differential loss to follow-up but it is hard to assess with the available information the amount and direction of bias projected onto the pooled mortality rate differences and rate ratios between periods in and out of treatment obtained in this meta-analysis
Secondly studies were conducted in high income countries with the follow-up often spread over many calendar years (1965-2010 for methadone and 1990-2010 for buprenorphine) and a highly variable average length of follow-up (ranges 13-158 years and 11-45 years respectively) Studies in low and middle income countries are especially needed
Thirdly by design we have not captured overdose mortality when opioid substitution treatment was obtained on illicit drug markets40 64 Fourthly a delayed record of treatment cessation could have led to some deaths that occurred out of treatment being incorrectly classified as occurring in treatment40 if so this makes our estimated impact of opioid substitution treatment on mortality a conservative one There could similarly be misclassification between overdose and non-over-dose deaths because of inconsistencies in definition of overdose and codification of causes of deaths (for
instance criteria for separating overdose death from intentional poisoning or sudden cardiac death)40 65 again these misclassifications would tend to underesti-mate deaths from overdose
implications for policy and practiceIn many countries the number of deaths attributable to opioid use is substantial66 67 and increasing in some such as the US where deaths from opioid overdose now outnumber gun related deaths in the country68 Over-doses are preventable causes of death warranting wide implementation of preventive interventions Our review has provided evidence that methadone and probably buprenorphine reduce mortality among people depen-dent on opioids making it imperative that further research confirms this using study designs that con-sider a wide range of confounding variables to increase confidence that these effects are causal
It must be borne in mind that there is strong evidence of the efficacy of methadone and buprenorphine on a range of clinical outcomes and these medicines are listed as WHO essential medicines the findings we have presented here provide additional imperatives for their widespread availability Despite this coverage of opioid substitution treatment is low in many countries worldwide69 Policymakers clinicians and those responsible for drug treatment systems should work to ensure the availability of such treatment remove access barriers and promote engagement This means the strategic development of services from a public health perspective which could reduce the social harm associ-ated with opioid use
Our review suggests that some precautions should be taken during and after opioid substitution treatment to increase safety Firstly careful clinical assessment of opioid tolerance before onset of treatment to establish a safe induction dose seems warranted Secondly moni-toring during the induction period is important espe-cially for methadone with clinicians considering adjusting opioid doses monitoring mental and somatic problems and preventing the use of opioids obtained on the illicit drug market64 In addition education of patients about the risk of overdose risk and use of ldquotake homerdquo naloxone70 71 is warranted Buprenorphine induction followed by transition to methadone might also be considered10 72 Retention in opioid substitution treatment reduces risk of exposure to mortality after cessation and also to re-exposure to mortality risk during induction onto methadone so efforts to improve retention are important as a strategy to reduce mortal-ity More generally establishment of mechanisms for information and coordination between healthcare social and legal services and patient counselling while in treatment in addition to more specific overdose pre-vention programmes such as naloxone distribution should be considered
Finally there is a pressing need for new studies on the comparative effectiveness of methadone and buprenorphine in reducing mortality New ran-domised controlled trials are highly unlikely they would be prohibitively expensive and difficult to
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score

doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
6
tabl
e 2
| tre
atm
ent d
eliv
ery a
nd fo
llow
-up
feat
ures
of c
ohor
t stu
dies
on
mor
talit
y ris
k in
peo
ple
with
opi
oid
depe
nden
ce d
urin
g an
d aft
er o
pioi
d su
bstit
utio
n tre
atm
ent
stud
yno
of c
ohor
t pa
rtic
ipan
tsdagger
aver
age
Ost
do
se (m
gda
y)in
patie
nt
indu
ctio
n (
)O
st
prov
ider
Follo
w-u
p pe
riod
aver
age
follo
w-u
p (y
ears
)Dagger
loss
to
follo
w-u
p (
)sectM
orta
lity
outc
ome
Qua
lity
scor
epara
Met
hado
neGe
arin
g 19
7424
3000
100
176
Spec
ialis
t19
65-7
25
24
0Al
l cau
ses
ove
rdos
e9
Cush
man
197
72554
710
0NA
Spec
ialis
t19
66-7
53
623
2Al
l cau
ses
ove
rdos
e6
Groumln
blad
h 19
9026
166
7510
00
Spec
ialis
t19
67-8
711
00
0Al
l cau
ses
ove
rdos
e4
Capl
ehor
n 19
9427
1996
2830
511
632
3Sp
ecia
list
1970
-90
139
144
All c
ause
s27
ove
rdos
e286
Fuge
lsta
d 19
9529
135
NA10
00
Spec
ialis
t19
86-9
02
10
0Al
l cau
ses
6Fu
gels
tad
1998
3056
8010
00
Spec
ialis
t19
86-9
34
20
0Al
l cau
ses
6Bu
ster
200
2752
0048
00
Mix
ed19
86-9
85
70
0O
verd
ose
8Sc
herb
aum
200
23124
447
00
Spec
ialis
t19
88-9
65
315
6Al
l cau
ses
ove
rdos
e7
Davo
li 2
00732
5276
NA0
0Sp
ecia
list
1998
-200
11
33
7O
verd
ose
11Fu
gels
tad
200
73367
9NA
100
0Sp
ecia
list
1988
-200
06
96
2Al
l cau
ses
3Cl
ause
n 2
00834
3229
112
00
Mix
ed19
97-2
003
24
00
All c
ause
s o
verd
ose
7De
genh
ardt
200
9631
846
700
0M
ixed
1985
-200
0daggerdagger6
80
0Al
l cau
sesDaggerDagger
12Co
rnis
h 2
0108
4894
500
0GP
1990
-200
519
175
All c
ause
s9
Pele
s 2
01035
613
113
00
Spec
ialis
t19
93-2
008
770
8Al
l cau
ses
ove
rdos
e9
Evan
s 2
0159
32 32
2NA
00
Spec
ialis
t20
06-1
02
35
0Al
l cau
sesDaggerDagger
12Ki
mbe
r 20
1510
26 0
6470
00
Mix
ed20
01-1
05
30
0Al
l cau
ses
ove
rdos
e13
Nosy
k 2
01536
1326
NA0
0GP
1996
-201
04
279
All c
ause
sDaggerDagger13
Cous
ins
201
63769
8372
00
GP20
04-1
04
12
0Al
l cau
ses
ove
rdos
e12
bupr
enor
phin
eCo
rnis
h 2
0108
1373
100
0GP
1990
-200
511
103
All c
ause
s9
Reec
e 2
01038
2518
NA0
0GP
2000
-07
32
12Al
l cau
ses
5Ki
mbe
r 20
1510
11 94
012
00
Mix
ed20
01-1
04
50
0Al
l cau
ses
ove
rdos
e13
NA=n
ot a
vaila
ble
OST
=opi
oid
subs
titut
ion
treat
men
tO
pioi
d su
bstit
utio
n tre
atm
ent w
ith e
ither
met
hado
ne o
r bup
reno
rphi
ne e
xcep
t for
Cla
usen
et a
l34 in
whi
ch a
bout
93
of p
artic
ipan
ts u
sed
met
hado
ne a
nd o
nly 7
u
sed
bupr
enor
phin
e du
ring
stud
y per
iod
daggerPar
ticip
ants
rece
ivin
g op
ioid
sub
stitu
tion
treat
men
t at l
east
onc
e du
ring
stud
y per
iod
Unt
reat
ed p
artic
ipan
ts a
nd th
ose
rece
ivin
g ot
her t
ypes
of t
reat
men
t for
opi
oid
depe
nden
ce (m
etha
done
det
oxifi
catio
n o
pioi
d an
tago
nist
ther
apy
ther
apeu
tic
com
mun
ity) e
xclu
ded
from
met
a-an
alys
is
DaggerAve
rage
follo
w-u
p fro
m s
tart
of o
pioi
d su
bstit
utio
n tre
atm
ent c
ombi
ning
sub
sequ
ent p
erio
ds in
and
out
of t
reat
men
tsectP
erce
ntag
e lo
ss to
follo
w-u
p be
fore
end
of s
tudy
per
iod
or d
eath
If n
ot o
ther
wis
e sp
ecifi
ed c
ompl
ete
case
asc
erta
inm
ent a
ssum
ed fo
r stu
dies
bas
ed o
n po
pula
tion
mor
talit
y reg
istri
es
paraQua
lity a
sses
smen
t sco
re ra
ngin
g fro
m 0
(low
est q
ualit
y) to
16 (h
ighe
st q
ualit
y)
O
verd
ose
mor
talit
y rep
orte
d bu
t not
incl
uded
in m
eta-
anal
ysis
as t
here
wer
e no
ove
rdos
e de
aths
whi
le p
artic
ipan
ts w
ere
in o
pioi
d su
bstit
utio
n tre
atm
ent
daggerdaggerFo
llow
-up
rest
ricte
d to
1985
-200
0 as
sub
sequ
ent 2
001-
06 fo
llow
-up
perio
d ov
erla
pped
with
Kim
ber e
t al10
DaggerDaggerO
verd
ose
mor
talit
y rep
orte
d on
ly fo
r com
bine
d tre
atm
ents
or i
nclu
ded
untre
ated
par
ticip
ants
and
hen
ce n
ot in
clud
ed in
met
a-an
alys
is
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
7
discussionMain findingsOur review suggests that time spent in opioid substitu-tion treatment with methadone is associated with an average reduction of 25 deaths1000 person years (95 confidence interval 14 to 36) The rate in treatment was less than a third of the rate out of treatment with the greatest difference in deaths from overdose The all cause mortality risk during treatment is much higher in the first four weeks than in the remainder of treatment Mortality risk is also higher in the first four weeks after cessation than in the remainder time out of treatment
Based on three cohorts (two from Australia) findings also suggest that opioid substitution treatment with buprenorphine could be associated with a reduction in mortality with a similar risk across all time in treatment (about four deaths1000 person years) consistent with its safety profile39-44 and a risk after cessation higher in the first four weeks than in the remainder of time out of treatment (32 versus 11 deaths1000 person years)
Mortality risk during specific periods in and out of methadone treatmentThe larger relative effect size (as measured by rate ratio) for overdose than non-overdose deaths with metha-done substitution6 11 34 45 is consistent with previous findings although the effect on non-overdose deaths had not been previously reviewed This disparity is
consistent with what would be expected given metha-donersquos effect on reducing use of heroin and other illicit opioids32 34
Our finding that the first four weeks after onset (114 deaths1000 person years) and cessation (3211000 person years) of methadone treatment are the highest risk periods suggests that these are key periods during which to focus efforts for prevention of drug related deaths Moreover within periods of methadone treat-ment there is a swift decline in risk from first to fourth week followed by a stable trend whereas after cessa-tion there is a high but quite stable risk during the first four weeks and a progressive decline afterward This is important because some patients cycle in and out of opioid substitution treatment46-50 and are therefore exposed to repeated periods of high risk for mortality Such changes probably mainly reflect changes in risk of fatal overdose6 32 but this has not been accurately assessed because only two cohorts reported overdose data specifically7 10 The increased risk during the first few weeks of treatment could be explained by an accu-mulation of methadone that exceeds the opioid toler-ance level (the mean elimination half life for methadone is 22 hours)51 as opioid tolerance does not seem to fully protect against respiratory depression52 Psychological factors and concomitant use of other respiratory depressant drugs or cocaine could also play a role7 8 40 53 54
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1994 Fugelstad et al 1995 Fugelstad et al 1998 Scherbaum et al 2002 Fugelstad et al 2007 Clausen et al 2008 Degenhardt et al 2009 Cornish et al 2010 Peles et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine Cornish et al 2010 Reece 2010 Kimber et al 2015Overall
2 5 10 20 50 100 200
11014 474251655161085111975
82427177
181114773354906450
648111 538305129423985
16325 27763691 792
89397911522 648
774031119
8721 936
In treatment
3311701429732740
362279545457
14172741311461303
1510105 73571428852727
84848 12256345 2652061582986247
10751406911
31431 239
Out of treatment
No of deathsperson years
76 (62 to 92)151 (98 to 223)148 (84 to 239)56 (28 to 100)
331 (143 to 651)395 (159 to 814)162 (96 to 255)
230 (181 to 287)140 (112 to 171)
58 (54 to 63)58 (40 to 83)
105 (76 to 142)64 (55 to 75)69 (64 to 75)
224 (180 to 275)51 (42 to 61)
113 (84 to 152)
95 (38 to 195)27 (06 to 78)40 (32 to 49)43 (21 to 89)
In treatment
282 (194 to 396)471 (258 to 791)432 (296 to 610)158 (111 to 219)
1111 (361 to 2593)699 (191 to 1790)814 (445 to 1366)565 (443 to 709)353 (259 to 471)143 (136 to 150)166 (129 to 209)715 (534 to 938)176 (165 to 188)124 (114 to 135)
1302 (1130 to 1493)157 (127 to 191)361 (245 to 533)
133 (64 to 245)58 (41 to 79)
101 (90 to 112)95 (39 to 234)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 2 | all cause mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled all cause mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates during periods in and out of treatment across all methadone or buprenorphine cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
8
tabl
e 3
| Poo
led
all c
ause
and
ove
rdos
e m
orta
lity r
ates
dur
ing
perio
ds in
and
out
of o
pioi
d su
bstit
utio
n tre
atm
ent w
ith m
etha
done
by s
tudy
char
acte
ristic
s
stud
y ch
arac
teris
tic
all c
ause
mor
talit
y ra
te1
000
pers
on y
ears
(95
Ci)
Ove
rdos
e m
orta
lity
rate
100
0 pe
rson
yea
rs (9
5 C
i)
no o
f st
udie
sin
trea
tmen
tO
ut o
f tre
atm
ent
P va
luedagger
i2 (
)Daggerno
of
stud
ies
in tr
eatm
ent
Out
of t
reat
men
tP
valu
edaggeri2 (
)Dagger
Loca
tion
E
urop
eIs
rael
913
9 (9
5 to
20
5)46
6 (2
90
to 74
9)
008
987
31
(24
to 4
0)
133
(59
to 2
98)
013
93
Nor
th A
mer
ica
411
2 (6
4 to
196
)42
3 (2
12 to
84
6)2
23
(14
to 3
8)
205
(44
to 9
45)
A
ustra
lia3
63
(33
to 12
1)14
0 (6
3 to
30
8)2
20
(14
to 2
9)
67
(15
to 2
96)
Opio
id in
ject
ors (
)
lt
100
129
0 (6
9 to
117
)25
8 (1
87
to 3
55)
000
195
102
5 (2
0 to
30
)10
6 (6
1 to
185
)mdash
mdash
100
423
4 (1
42
to 3
85)
109
9 (5
94
to 2
034
)1
mdashsect
mdashsect
Men
()
lt
7511
95
(69
to 13
2)
300
(18
4 to
48
8)0
6798
62
4 (1
8 to
34
)10
6 (4
5 to
24
8)0
7493
ge
753
116
(61
to 2
20)
459
(178
to 11
79)
52
9 (2
0 to
42
)15
8 (6
2 to
40
3)M
ean
age
(yea
rs)
lt
3510
99
(68
to 14
5)
293
(179
to 4
82)
040
988
26
(19
to 3
5)
106
(52
to 2
18)
060
93
ge35
614
0 (8
7 to
22
7)50
3 (2
68
to 9
43)
32
7 (1
5 to
47
)20
5 (6
2 to
676
)Av
erag
e m
etha
done
dos
e (m
gda
y)
le
807
96
(63
to 14
8)
269
(15
5 to
46
5)0
5692
53
1 (2
0 to
46
)10
3 (4
0 to
26
9)0
2293
gt
805
99
(60
to 16
5)
354
(18
5 to
677
)5
25
(16
to 3
9)
170
(65
to 4
49)
Inpa
tient
indu
ctio
n (
)
09
92
(63
to 13
6)
299
(173
to 5
16)
019
987
25
(18
to 3
4)
100
(45
to 2
23)
065
93
gt0
615
4 (9
3 to
25
3)45
9 (2
29
to 9
21)
32
9 (1
7 to
50
)18
4 (5
4 to
62
5)Tr
eatm
ent p
rovi
der
S
peci
alis
t10
134
(92
to 19
5)
465
(28
2 to
765
)0
2698
72
5 (1
7 to
37
)20
8 (1
11 to
38
8)0
0188
G
Pm
ixed
68
6 (5
4 to
137
)24
4 (1
31
to 4
54)
42
4 (1
6 to
36
)5
6 (2
5 to
125
)M
idpo
int f
ollo
w-u
p pe
riod
lt
2000
1012
6 (8
5 to
187
)38
8 (2
28
to 6
61)
058
987
28
(20
to 3
9)
154
(70
to 3
39)
067
93
ge20
006
97
(60
to 15
9)
320
(16
5 to
62
3)4
24
(17
to 3
5)
90
(32
to 2
52)
Loss
to fo
llow
-up
()
lt
1012
119
(83
to 1
70)
383
(23
7 to
619
)0
8198
82
5 (1
9 to
32
)9
8 (5
0 to
195
)0
3393
ge
104
95
(50
to 18
0)
313
(13
5 to
72
3)3
32
(17
to 6
0)
254
(81
to 7
94)
Poo
led
mor
talit
y rat
es a
nd 9
5 c
onfid
ence
inte
rval
s dur
ing
perio
ds in
and
out
of t
reat
men
t by s
tudy
cha
ract
eris
tics e
stim
ated
from
sep
arat
e bi
varia
te ra
ndom
effe
cts m
eta-
regr
essi
on m
odel
s rel
atin
g lo
g tra
nsfo
rmed
rate
s in
both
trea
tmen
t per
iods
w
ith e
ach
stud
y cha
ract
eris
tic
daggerOve
rall
P va
lue
for h
eter
ogen
eity
of p
oole
d m
orta
lity r
ates
acr
oss c
ateg
orie
s of s
tudy
cha
ract
eris
tic a
s obt
aine
d fro
m li
kelih
ood
ratio
test
com
parin
g ne
sted
met
a-re
gres
sion
mod
els w
ith a
nd w
ithou
t stu
dy c
hara
cter
istic
fitte
d vi
a m
axim
um li
kelih
ood
DaggerOve
rall
I2 sta
tistic
for r
esid
ual h
eter
ogen
eity
in s
tudy
spe
cific
mor
talit
y rat
es n
ot e
xpla
ined
by c
orre
spon
ding
stu
dy c
hara
cter
istic
sectP
oole
d m
orta
lity r
ates
not
app
licab
le to
cat
egor
ies w
ith s
ingl
e st
udy
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
9
Although the long half life of methadone could con-tribute to the increase in mortality in the first three to four days after cessation of treatment there was a large increase in mortality across the first four weeks after cessation compared with the treatment period Such increased mortality could be explained by loss of toler-ance to the toxic effects of heroin assuming that many patients return to use6 8 32 47 55 56 and probably also by the use of multiple legal and illicit substances during that period Similar peaks in drug related mortality occur in other situations where opioid tolerance is prob-ably diminished (for example after prison release or hospital discharge57-59 ) Lifestyle factors and comorbid issues such as mental health problems could also increase mortality from other external causes as deaths from suicide and injury are also more common during that period53
Mortality risk during specific periods in and out of buprenorphine treatmentData from three cohorts (two from Australia) suggest that substitution treatment with buprenorphine could reduce all cause mortality although the disparity in mortality rates in periods in and out of treatment did not reach significance Findings also suggest a signifi-cantly increased mortality in the first four weeks after cessation of treatment compared with the remaining time out of treatment (320 versus 1091000 person years) while during the treatment period there was no difference between the first four weeks and the remain-ing time in treatment It is difficult to draw firm conclu-sions because of limited evidence from similar settings 96 of included deaths and 98 of person years came from Australian studies (with 87 and 86 from the study by Kimber and colleagues13)
Comparative effectiveness of buprenorphine and methadone substitution treatmentOther sources of data have suggested that buprenor-phine could be more effective than methadone in reduc-ing mortality especially from overdose39 42 43 Unlike methadone there is a ceiling for respiratory depressant effects of buprenorphine as dose increases and the probability of triggering arrhythmias is lower for buprenorphine than methadone41 44 60 When we com-pared the mortality between periods in and out of treat-ment first within those taking methadone and then within those taking buprenorphine we found a greater reduction in mortality with methadone than with buprenorphine (measured as the rate difference or rate ratio between periods) When we compared mortality between them first within the treatment period and then in the period off treatment we found a signifi-cantly lower mortality with buprenorphine than meth-adone in both periods
Our conclusions must remain tentative until further studies in varied treatment settings and contexts are undertaken to examine this issue Differences in mor-tality might also reflect confounding through differ-ences in characteristics of patients (such as age severity of opioid dependence injecting drug use other ta
ble
4 | C
ohor
t stu
dies
repo
rtin
g al
l cau
se a
nd o
verd
ose
mor
talit
y rat
e ra
tios c
ompa
ring
perio
ds o
ut a
nd in
opi
oid
subs
titut
ion
treat
men
t adj
uste
d fo
r con
foun
ding
stud
y
Conf
ound
ing
fact
ors
all c
ause
mor
talit
yO
verd
ose
mor
talit
y
Patie
nt d
emog
raph
ics
seve
rity
of d
rug
use
trea
tmen
tCo
mor
bidi
tyun
adju
sted
ra
te ra
tioad
just
ed
rate
ratio
Perc
enta
ge
chan
gedagger
unad
just
ed
rate
ratio
adju
sted
ra
te ra
tioPe
rcen
tage
ch
ange
dagger
Met
hado
neBu
ster
200
27Se
x ra
ceTr
eatm
ent m
odal
ity t
ime
sinc
e fir
st tr
eatm
ent
mdashmdash
mdashmdash
087
087
minus03
Davo
li 2
00732
Age
sex
Leng
th o
f her
oin
use
her
oin
inje
ctio
n
prev
ious
ove
rdos
eHI
V p
sych
iatri
c com
orbi
dity
mdashmdash
mdash77
174
3minus3
6
Dege
nhar
dt 2
0096
Age
sex
cal
enda
r yea
rmdash
mdash19
118
8minus1
3mdash
mdashmdash
Corn
ish
201
08Ag
e s
ex c
alen
dar y
ear
mdashM
edic
al c
omor
bidi
ty2
833
2715
5mdash
mdashmdash
Evan
s 2
0159Dagger
Age
sex
rac
e e
duca
tion
em
ploy
men
t cr
imin
ality
hea
lth c
over
age
Prim
ary o
pioi
d fr
eque
ncy a
nd le
ngth
of
opio
id u
se n
on-o
pioi
d dr
ug u
seHI
V h
epat
itis C
tub
ercu
losi
s
disa
bilit
y m
edic
al c
omor
bidi
ty
psyc
hiat
ric c
omor
bidi
ty
273
370
355
351
442
258
Nosy
k 2
01536
DaggerAg
e s
ex r
ace
cal
enda
r yea
r re
gion
No o
f pre
viou
s tre
atm
ent e
piso
des
Tim
e si
nce
HIV
diag
nosi
s C
D4
coun
t AI
DS a
ntire
trovi
ral
ther
apy
med
ical
com
orbi
dity
304
294
minus34
114
147
286
Cous
ins
201
637Ag
e s
exTr
eatm
ent s
uper
visi
on m
etha
done
dos
eM
edic
al c
omor
bidi
ty3
093
6417
816
016
317
bupr
enor
phin
eCo
rnis
h 2
0108
Age
sex
cal
enda
r yea
rmdash
Med
ical
com
orbi
dity
141
164
168
mdashmdash
mdashB
asel
ine
or ti
me
vary
ing
conf
ound
ing
fact
ors u
sed
in a
djus
tmen
tdaggerP
erce
ntag
e ch
ange
in ra
te ra
tio a
fter a
djus
tmen
t for
cor
resp
ondi
ng c
onfo
undi
ng fa
ctor
sDaggerO
verd
ose
mor
talit
y rat
e ra
tios r
epor
ted
com
bini
ng m
etha
done
mai
nten
ance
with
det
oxifi
catio
n (1
14
of p
erso
n ye
ars i
n tre
atm
ent)
in E
vans
et a
l9 an
d in
clud
ing
neve
r tre
ated
par
ticip
ants
(73
3 o
f per
son
year
s out
of t
reat
men
t) in
Nos
yk e
t al36
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
10
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1996 Buster et al 2002 Scherbaum et al 2002 Davoli et al 2007 Clausen et al 2008 Peles et al 2010 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine Kimber et al 2015
2105 5 10 20 50 100
3314 474416557108541792
4218 7476111475751
24645053985
16991 7925422 648
3121 936
In treatment
2111707297
27740192004
2610 983131729998
28130313727
21645 265246247
14331 239
Out of treatment
No of deathsperson years
23 (16 to 32)24 (07 to 62)
64 (26 to 133)22 (06 to 57)22 (16 to 30)
54 (20 to 117)12 (05 to 25)37 (24 to 55)12 (04 to 29)18 (16 to 21)24 (18 to 31)26 (21 to 33)
14 (10 to 20)
In treatment
179 (111 to 274)236 (95 to 486)
365 (240 to 531)95 (57 to 148)24 (16 to 35)
756 (402 to 1292)90 (41 to 171)
215 (143 to 311)179 (95 to 306)
48 (42 to 54)38 (25 to 57)
127 (69 to 234)
46 (39 to 54)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 3 | Overdose mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled overdose mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates during periods in and out of treatment across all methadone cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
Methadone rst four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallMethadone aer four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Cornish et al 2010 Kimber et al 2015OverallBuprenorphine aer four weeks Cornish et al 2010 Kimber et al 2015Overall
21 5 10 20 50 100
9425057465
151950323344
4100153371
554109 033234664
14823 32760488 449
85388010019 277
18192094
66597819 842
In treatment
38189821479
154267335183679113
441181
1472103 838503809
69445 44952843 4301271469545067
788281674
366328629 565
Out of treatment
No of deathsperson years
375 (303 to 459)151 (61 to 311)77 (43 to 127)96 (66 to 135)
mdash44 (25 to 73)
114 (58 to 224)
51 (47 to 55)49 (31 to 74)63 (54 to 74)68 (63 to 74)
mdash52 (42 to 63)58 (50 to 67)
124 (03 to 692)43 (20 to 82)
45 (12 to 168)
91 (33 to 198)39 (31 to 49)45 (32 to 62)
In treatment
200 (142 to 275)438 (271 to 670)576 (489 to 675)191 (133 to 265)
mdash373 (271 to 500)321 (191 to 539)
142 (135 to 149)131 (97 to 173)
153 (141 to 164)122 (111 to 132)
mdash107 (80 to 139)
135 (119 to 153)
800 (322 to 1648)167 (111 to 242)320 (132 to 775)
45 (09 to 132)97 (86 to 109)
109 (85 to 139)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 4 | all cause mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled all cause mortality rates 2009-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except Degenhardt et al6 which reported mortality before and after two weeks of treatment initiation and cessation high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-analysis area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates before and after four weeks in and out of treatment across methadone or buprenorphine cohorts estimated from multivariate random effects meta-analysis on log transformed rates in four time-by-treatment intervals
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
11
drug use comorbidities prison history overdose his-tory patientrsquos preference) characteristics of treatment (such as previous treatment specialisation of the doc-tor who controls the treatment dose provision charac-teristics cointerventions retention or drop outs) or the sociopolitical context in which studies have been conducted For example the initial prognosis might be better in those given buprenorphine than those given methadone (that is fewer comorbid problems less severe opioid dependence)6 8 10 61 though this was not clearly found in a recent US study62
The role of such confounding factors has received almost empirical examination Few details on char-acteristics of patients or treatments were reported in articles included in this meta-analysis to permit a detailed examination of this potential issue (tables 1 and 2 ) so it was not possible to assess the possibil-ity of confounding A sensitivity simulation analysis in the study by Kimber and colleagues however suggested that the lower mortality with buprenor-phine than with methadone during first four weeks of treatment was unlikely to be caused by unmea-sured confounding10
strengths and limitationsThis meta-analysis synthesised evidence from cohort studies published until 2016 on risk of mortality in people who are dependent on opioids during and after opioid substitution treatment separately for buprenor-phine and methadone Mortality changes over time (1st-32th week) during and after methadone are care-fully quantified for the first time
The published studies however had several methodological shortcomings Firstly in the included
Methadone rst four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallMethadone aer four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Kimber et al 2015Buprenorphine aer four weeks Kimber et al 2015
21 505 10 20
9150018334443371
3317 20015188 4495019 277
22094
2919 842
In treatment
2130010183681181
24960020643 430
165067
181674
12529 565
Out of treatment
No of deathsperson years
60 (27 to 114)54 (32 to 85)12 (03 to 30)35 (13 to 95)
19 (13 to 27)17 (14 to 20)26 (19 to 34)20 (15 to 27)
09 (01 to 34)
15 (10 to 21)
In treatment
15 (02 to 56)54 (26 to 100)68 (29 to 134)42 (18 to 99)
25 (16 to 37)47 (41 to 54)32 (18 to 51)34 (23 to 51)
108 (64 to 170)
42 (35 to 50)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 6 | Overdose mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled overdose mortality rates 2002-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except buster et al7 which reported mortality before and after two weeks of treatment initiation and cessation area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates before and after four weeks in and out of treatment across methadone cohorts estimated from multivariate random-effects meta-analysis on log transformed rates in four time-by-treatment intervals
Time since treatment initiation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s In methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Time since treatment cessation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s Out of methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Degenhardt et al 2009Cornish et al 2010Evans et al 2015Kimber et al 2015Cousins et al 2016
Fig 5 | all cause mortality rates by time since treatment initiation and cessation in methadone cohorts and pooled all cause mortality risk trends 2009-16 high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-regression area of each circle is proportional to weight of each time interval in meta-regression Pooled trends in all cause mortality risk (solid lines) and their 95 confidence intervals (shaded regions) over time in and out of methadone treatment were estimated from bivariate random effects meta-regression of log transformed rates on quadratic linear spline function of log time with knot at four weeks
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
12
observational studies the same patients are compared throughout follow-up periods in and out of opioid sub-stitution treatment but these patients leave and re-en-ter treatment in a non-random way and hence there could still be a large potential for confounding in com-parisons of crude mortality risk in and out of treat-ment In some studies with diverse information on patient demographics severity of drug use and comor-bidities measured mostly at baseline (table 3 ) adjust-ment for these potential confounders resulted in similar or even increased out-to-in mortality rate ratios which merely reflects that the above conditions tended to be less prevalent at baseline among patients who later left or were discharged from treatment than those who remained in treatment Nevertheless to obtain an unbiased estimate of the preventive effect of opioid substitution treatment on all cause and overdose mor-tality these and other relevant confounders should be measured every time a patient leaves and resumes treatment Time varying data can then be used to adjust for confounder history in standard regression models or even better to construct inverse probability of treatment weights for marginal structural models63 which properly control for time varying confounders for later treatment that are themselves affected by pre-vious treatment such as severity of drug use and comorbidity Also differential loss to follow-up is a concern in the meta-analysed cohorts as dropouts are more likely to occur in patients at higher risk of death during periods out of treatment thus inducing a selec-tion bias in crude comparisons of out-to-in mortality risk because of informative censoring Marginal struc-tural models with inverse probability of censoring weights can also be used to correct for differential loss to follow-up63 provided that common predictors of death and censoring are measured over time In sum-mary individual cohorts are prone to confounding and selection bias because of differential loss to follow-up but it is hard to assess with the available information the amount and direction of bias projected onto the pooled mortality rate differences and rate ratios between periods in and out of treatment obtained in this meta-analysis
Secondly studies were conducted in high income countries with the follow-up often spread over many calendar years (1965-2010 for methadone and 1990-2010 for buprenorphine) and a highly variable average length of follow-up (ranges 13-158 years and 11-45 years respectively) Studies in low and middle income countries are especially needed
Thirdly by design we have not captured overdose mortality when opioid substitution treatment was obtained on illicit drug markets40 64 Fourthly a delayed record of treatment cessation could have led to some deaths that occurred out of treatment being incorrectly classified as occurring in treatment40 if so this makes our estimated impact of opioid substitution treatment on mortality a conservative one There could similarly be misclassification between overdose and non-over-dose deaths because of inconsistencies in definition of overdose and codification of causes of deaths (for
instance criteria for separating overdose death from intentional poisoning or sudden cardiac death)40 65 again these misclassifications would tend to underesti-mate deaths from overdose
implications for policy and practiceIn many countries the number of deaths attributable to opioid use is substantial66 67 and increasing in some such as the US where deaths from opioid overdose now outnumber gun related deaths in the country68 Over-doses are preventable causes of death warranting wide implementation of preventive interventions Our review has provided evidence that methadone and probably buprenorphine reduce mortality among people depen-dent on opioids making it imperative that further research confirms this using study designs that con-sider a wide range of confounding variables to increase confidence that these effects are causal
It must be borne in mind that there is strong evidence of the efficacy of methadone and buprenorphine on a range of clinical outcomes and these medicines are listed as WHO essential medicines the findings we have presented here provide additional imperatives for their widespread availability Despite this coverage of opioid substitution treatment is low in many countries worldwide69 Policymakers clinicians and those responsible for drug treatment systems should work to ensure the availability of such treatment remove access barriers and promote engagement This means the strategic development of services from a public health perspective which could reduce the social harm associ-ated with opioid use
Our review suggests that some precautions should be taken during and after opioid substitution treatment to increase safety Firstly careful clinical assessment of opioid tolerance before onset of treatment to establish a safe induction dose seems warranted Secondly moni-toring during the induction period is important espe-cially for methadone with clinicians considering adjusting opioid doses monitoring mental and somatic problems and preventing the use of opioids obtained on the illicit drug market64 In addition education of patients about the risk of overdose risk and use of ldquotake homerdquo naloxone70 71 is warranted Buprenorphine induction followed by transition to methadone might also be considered10 72 Retention in opioid substitution treatment reduces risk of exposure to mortality after cessation and also to re-exposure to mortality risk during induction onto methadone so efforts to improve retention are important as a strategy to reduce mortal-ity More generally establishment of mechanisms for information and coordination between healthcare social and legal services and patient counselling while in treatment in addition to more specific overdose pre-vention programmes such as naloxone distribution should be considered
Finally there is a pressing need for new studies on the comparative effectiveness of methadone and buprenorphine in reducing mortality New ran-domised controlled trials are highly unlikely they would be prohibitively expensive and difficult to
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score

thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
7
discussionMain findingsOur review suggests that time spent in opioid substitu-tion treatment with methadone is associated with an average reduction of 25 deaths1000 person years (95 confidence interval 14 to 36) The rate in treatment was less than a third of the rate out of treatment with the greatest difference in deaths from overdose The all cause mortality risk during treatment is much higher in the first four weeks than in the remainder of treatment Mortality risk is also higher in the first four weeks after cessation than in the remainder time out of treatment
Based on three cohorts (two from Australia) findings also suggest that opioid substitution treatment with buprenorphine could be associated with a reduction in mortality with a similar risk across all time in treatment (about four deaths1000 person years) consistent with its safety profile39-44 and a risk after cessation higher in the first four weeks than in the remainder of time out of treatment (32 versus 11 deaths1000 person years)
Mortality risk during specific periods in and out of methadone treatmentThe larger relative effect size (as measured by rate ratio) for overdose than non-overdose deaths with metha-done substitution6 11 34 45 is consistent with previous findings although the effect on non-overdose deaths had not been previously reviewed This disparity is
consistent with what would be expected given metha-donersquos effect on reducing use of heroin and other illicit opioids32 34
Our finding that the first four weeks after onset (114 deaths1000 person years) and cessation (3211000 person years) of methadone treatment are the highest risk periods suggests that these are key periods during which to focus efforts for prevention of drug related deaths Moreover within periods of methadone treat-ment there is a swift decline in risk from first to fourth week followed by a stable trend whereas after cessa-tion there is a high but quite stable risk during the first four weeks and a progressive decline afterward This is important because some patients cycle in and out of opioid substitution treatment46-50 and are therefore exposed to repeated periods of high risk for mortality Such changes probably mainly reflect changes in risk of fatal overdose6 32 but this has not been accurately assessed because only two cohorts reported overdose data specifically7 10 The increased risk during the first few weeks of treatment could be explained by an accu-mulation of methadone that exceeds the opioid toler-ance level (the mean elimination half life for methadone is 22 hours)51 as opioid tolerance does not seem to fully protect against respiratory depression52 Psychological factors and concomitant use of other respiratory depressant drugs or cocaine could also play a role7 8 40 53 54
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1994 Fugelstad et al 1995 Fugelstad et al 1998 Scherbaum et al 2002 Fugelstad et al 2007 Clausen et al 2008 Degenhardt et al 2009 Cornish et al 2010 Peles et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine Cornish et al 2010 Reece 2010 Kimber et al 2015Overall
2 5 10 20 50 100 200
11014 474251655161085111975
82427177
181114773354906450
648111 538305129423985
16325 27763691 792
89397911522 648
774031119
8721 936
In treatment
3311701429732740
362279545457
14172741311461303
1510105 73571428852727
84848 12256345 2652061582986247
10751406911
31431 239
Out of treatment
No of deathsperson years
76 (62 to 92)151 (98 to 223)148 (84 to 239)56 (28 to 100)
331 (143 to 651)395 (159 to 814)162 (96 to 255)
230 (181 to 287)140 (112 to 171)
58 (54 to 63)58 (40 to 83)
105 (76 to 142)64 (55 to 75)69 (64 to 75)
224 (180 to 275)51 (42 to 61)
113 (84 to 152)
95 (38 to 195)27 (06 to 78)40 (32 to 49)43 (21 to 89)
In treatment
282 (194 to 396)471 (258 to 791)432 (296 to 610)158 (111 to 219)
1111 (361 to 2593)699 (191 to 1790)814 (445 to 1366)565 (443 to 709)353 (259 to 471)143 (136 to 150)166 (129 to 209)715 (534 to 938)176 (165 to 188)124 (114 to 135)
1302 (1130 to 1493)157 (127 to 191)361 (245 to 533)
133 (64 to 245)58 (41 to 79)
101 (90 to 112)95 (39 to 234)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 2 | all cause mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled all cause mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates during periods in and out of treatment across all methadone or buprenorphine cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
8
tabl
e 3
| Poo
led
all c
ause
and
ove
rdos
e m
orta
lity r
ates
dur
ing
perio
ds in
and
out
of o
pioi
d su
bstit
utio
n tre
atm
ent w
ith m
etha
done
by s
tudy
char
acte
ristic
s
stud
y ch
arac
teris
tic
all c
ause
mor
talit
y ra
te1
000
pers
on y
ears
(95
Ci)
Ove
rdos
e m
orta
lity
rate
100
0 pe
rson
yea
rs (9
5 C
i)
no o
f st
udie
sin
trea
tmen
tO
ut o
f tre
atm
ent
P va
luedagger
i2 (
)Daggerno
of
stud
ies
in tr
eatm
ent
Out
of t
reat
men
tP
valu
edaggeri2 (
)Dagger
Loca
tion
E
urop
eIs
rael
913
9 (9
5 to
20
5)46
6 (2
90
to 74
9)
008
987
31
(24
to 4
0)
133
(59
to 2
98)
013
93
Nor
th A
mer
ica
411
2 (6
4 to
196
)42
3 (2
12 to
84
6)2
23
(14
to 3
8)
205
(44
to 9
45)
A
ustra
lia3
63
(33
to 12
1)14
0 (6
3 to
30
8)2
20
(14
to 2
9)
67
(15
to 2
96)
Opio
id in
ject
ors (
)
lt
100
129
0 (6
9 to
117
)25
8 (1
87
to 3
55)
000
195
102
5 (2
0 to
30
)10
6 (6
1 to
185
)mdash
mdash
100
423
4 (1
42
to 3
85)
109
9 (5
94
to 2
034
)1
mdashsect
mdashsect
Men
()
lt
7511
95
(69
to 13
2)
300
(18
4 to
48
8)0
6798
62
4 (1
8 to
34
)10
6 (4
5 to
24
8)0
7493
ge
753
116
(61
to 2
20)
459
(178
to 11
79)
52
9 (2
0 to
42
)15
8 (6
2 to
40
3)M
ean
age
(yea
rs)
lt
3510
99
(68
to 14
5)
293
(179
to 4
82)
040
988
26
(19
to 3
5)
106
(52
to 2
18)
060
93
ge35
614
0 (8
7 to
22
7)50
3 (2
68
to 9
43)
32
7 (1
5 to
47
)20
5 (6
2 to
676
)Av
erag
e m
etha
done
dos
e (m
gda
y)
le
807
96
(63
to 14
8)
269
(15
5 to
46
5)0
5692
53
1 (2
0 to
46
)10
3 (4
0 to
26
9)0
2293
gt
805
99
(60
to 16
5)
354
(18
5 to
677
)5
25
(16
to 3
9)
170
(65
to 4
49)
Inpa
tient
indu
ctio
n (
)
09
92
(63
to 13
6)
299
(173
to 5
16)
019
987
25
(18
to 3
4)
100
(45
to 2
23)
065
93
gt0
615
4 (9
3 to
25
3)45
9 (2
29
to 9
21)
32
9 (1
7 to
50
)18
4 (5
4 to
62
5)Tr
eatm
ent p
rovi
der
S
peci
alis
t10
134
(92
to 19
5)
465
(28
2 to
765
)0
2698
72
5 (1
7 to
37
)20
8 (1
11 to
38
8)0
0188
G
Pm
ixed
68
6 (5
4 to
137
)24
4 (1
31
to 4
54)
42
4 (1
6 to
36
)5
6 (2
5 to
125
)M
idpo
int f
ollo
w-u
p pe
riod
lt
2000
1012
6 (8
5 to
187
)38
8 (2
28
to 6
61)
058
987
28
(20
to 3
9)
154
(70
to 3
39)
067
93
ge20
006
97
(60
to 15
9)
320
(16
5 to
62
3)4
24
(17
to 3
5)
90
(32
to 2
52)
Loss
to fo
llow
-up
()
lt
1012
119
(83
to 1
70)
383
(23
7 to
619
)0
8198
82
5 (1
9 to
32
)9
8 (5
0 to
195
)0
3393
ge
104
95
(50
to 18
0)
313
(13
5 to
72
3)3
32
(17
to 6
0)
254
(81
to 7
94)
Poo
led
mor
talit
y rat
es a
nd 9
5 c
onfid
ence
inte
rval
s dur
ing
perio
ds in
and
out
of t
reat
men
t by s
tudy
cha
ract
eris
tics e
stim
ated
from
sep
arat
e bi
varia
te ra
ndom
effe
cts m
eta-
regr
essi
on m
odel
s rel
atin
g lo
g tra
nsfo
rmed
rate
s in
both
trea
tmen
t per
iods
w
ith e
ach
stud
y cha
ract
eris
tic
daggerOve
rall
P va
lue
for h
eter
ogen
eity
of p
oole
d m
orta
lity r
ates
acr
oss c
ateg
orie
s of s
tudy
cha
ract
eris
tic a
s obt
aine
d fro
m li
kelih
ood
ratio
test
com
parin
g ne
sted
met
a-re
gres
sion
mod
els w
ith a
nd w
ithou
t stu
dy c
hara
cter
istic
fitte
d vi
a m
axim
um li
kelih
ood
DaggerOve
rall
I2 sta
tistic
for r
esid
ual h
eter
ogen
eity
in s
tudy
spe
cific
mor
talit
y rat
es n
ot e
xpla
ined
by c
orre
spon
ding
stu
dy c
hara
cter
istic
sectP
oole
d m
orta
lity r
ates
not
app
licab
le to
cat
egor
ies w
ith s
ingl
e st
udy
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
9
Although the long half life of methadone could con-tribute to the increase in mortality in the first three to four days after cessation of treatment there was a large increase in mortality across the first four weeks after cessation compared with the treatment period Such increased mortality could be explained by loss of toler-ance to the toxic effects of heroin assuming that many patients return to use6 8 32 47 55 56 and probably also by the use of multiple legal and illicit substances during that period Similar peaks in drug related mortality occur in other situations where opioid tolerance is prob-ably diminished (for example after prison release or hospital discharge57-59 ) Lifestyle factors and comorbid issues such as mental health problems could also increase mortality from other external causes as deaths from suicide and injury are also more common during that period53
Mortality risk during specific periods in and out of buprenorphine treatmentData from three cohorts (two from Australia) suggest that substitution treatment with buprenorphine could reduce all cause mortality although the disparity in mortality rates in periods in and out of treatment did not reach significance Findings also suggest a signifi-cantly increased mortality in the first four weeks after cessation of treatment compared with the remaining time out of treatment (320 versus 1091000 person years) while during the treatment period there was no difference between the first four weeks and the remain-ing time in treatment It is difficult to draw firm conclu-sions because of limited evidence from similar settings 96 of included deaths and 98 of person years came from Australian studies (with 87 and 86 from the study by Kimber and colleagues13)
Comparative effectiveness of buprenorphine and methadone substitution treatmentOther sources of data have suggested that buprenor-phine could be more effective than methadone in reduc-ing mortality especially from overdose39 42 43 Unlike methadone there is a ceiling for respiratory depressant effects of buprenorphine as dose increases and the probability of triggering arrhythmias is lower for buprenorphine than methadone41 44 60 When we com-pared the mortality between periods in and out of treat-ment first within those taking methadone and then within those taking buprenorphine we found a greater reduction in mortality with methadone than with buprenorphine (measured as the rate difference or rate ratio between periods) When we compared mortality between them first within the treatment period and then in the period off treatment we found a signifi-cantly lower mortality with buprenorphine than meth-adone in both periods
Our conclusions must remain tentative until further studies in varied treatment settings and contexts are undertaken to examine this issue Differences in mor-tality might also reflect confounding through differ-ences in characteristics of patients (such as age severity of opioid dependence injecting drug use other ta
ble
4 | C
ohor
t stu
dies
repo
rtin
g al
l cau
se a
nd o
verd
ose
mor
talit
y rat
e ra
tios c
ompa
ring
perio
ds o
ut a
nd in
opi
oid
subs
titut
ion
treat
men
t adj
uste
d fo
r con
foun
ding
stud
y
Conf
ound
ing
fact
ors
all c
ause
mor
talit
yO
verd
ose
mor
talit
y
Patie
nt d
emog
raph
ics
seve
rity
of d
rug
use
trea
tmen
tCo
mor
bidi
tyun
adju
sted
ra
te ra
tioad
just
ed
rate
ratio
Perc
enta
ge
chan
gedagger
unad
just
ed
rate
ratio
adju
sted
ra
te ra
tioPe
rcen
tage
ch
ange
dagger
Met
hado
neBu
ster
200
27Se
x ra
ceTr
eatm
ent m
odal
ity t
ime
sinc
e fir
st tr
eatm
ent
mdashmdash
mdashmdash
087
087
minus03
Davo
li 2
00732
Age
sex
Leng
th o
f her
oin
use
her
oin
inje
ctio
n
prev
ious
ove
rdos
eHI
V p
sych
iatri
c com
orbi
dity
mdashmdash
mdash77
174
3minus3
6
Dege
nhar
dt 2
0096
Age
sex
cal
enda
r yea
rmdash
mdash19
118
8minus1
3mdash
mdashmdash
Corn
ish
201
08Ag
e s
ex c
alen
dar y
ear
mdashM
edic
al c
omor
bidi
ty2
833
2715
5mdash
mdashmdash
Evan
s 2
0159Dagger
Age
sex
rac
e e
duca
tion
em
ploy
men
t cr
imin
ality
hea
lth c
over
age
Prim
ary o
pioi
d fr
eque
ncy a
nd le
ngth
of
opio
id u
se n
on-o
pioi
d dr
ug u
seHI
V h
epat
itis C
tub
ercu
losi
s
disa
bilit
y m
edic
al c
omor
bidi
ty
psyc
hiat
ric c
omor
bidi
ty
273
370
355
351
442
258
Nosy
k 2
01536
DaggerAg
e s
ex r
ace
cal
enda
r yea
r re
gion
No o
f pre
viou
s tre
atm
ent e
piso
des
Tim
e si
nce
HIV
diag
nosi
s C
D4
coun
t AI
DS a
ntire
trovi
ral
ther
apy
med
ical
com
orbi
dity
304
294
minus34
114
147
286
Cous
ins
201
637Ag
e s
exTr
eatm
ent s
uper
visi
on m
etha
done
dos
eM
edic
al c
omor
bidi
ty3
093
6417
816
016
317
bupr
enor
phin
eCo
rnis
h 2
0108
Age
sex
cal
enda
r yea
rmdash
Med
ical
com
orbi
dity
141
164
168
mdashmdash
mdashB
asel
ine
or ti
me
vary
ing
conf
ound
ing
fact
ors u
sed
in a
djus
tmen
tdaggerP
erce
ntag
e ch
ange
in ra
te ra
tio a
fter a
djus
tmen
t for
cor
resp
ondi
ng c
onfo
undi
ng fa
ctor
sDaggerO
verd
ose
mor
talit
y rat
e ra
tios r
epor
ted
com
bini
ng m
etha
done
mai
nten
ance
with
det
oxifi
catio
n (1
14
of p
erso
n ye
ars i
n tre
atm
ent)
in E
vans
et a
l9 an
d in
clud
ing
neve
r tre
ated
par
ticip
ants
(73
3 o
f per
son
year
s out
of t
reat
men
t) in
Nos
yk e
t al36
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
10
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1996 Buster et al 2002 Scherbaum et al 2002 Davoli et al 2007 Clausen et al 2008 Peles et al 2010 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine Kimber et al 2015
2105 5 10 20 50 100
3314 474416557108541792
4218 7476111475751
24645053985
16991 7925422 648
3121 936
In treatment
2111707297
27740192004
2610 983131729998
28130313727
21645 265246247
14331 239
Out of treatment
No of deathsperson years
23 (16 to 32)24 (07 to 62)
64 (26 to 133)22 (06 to 57)22 (16 to 30)
54 (20 to 117)12 (05 to 25)37 (24 to 55)12 (04 to 29)18 (16 to 21)24 (18 to 31)26 (21 to 33)
14 (10 to 20)
In treatment
179 (111 to 274)236 (95 to 486)
365 (240 to 531)95 (57 to 148)24 (16 to 35)
756 (402 to 1292)90 (41 to 171)
215 (143 to 311)179 (95 to 306)
48 (42 to 54)38 (25 to 57)
127 (69 to 234)
46 (39 to 54)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 3 | Overdose mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled overdose mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates during periods in and out of treatment across all methadone cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
Methadone rst four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallMethadone aer four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Cornish et al 2010 Kimber et al 2015OverallBuprenorphine aer four weeks Cornish et al 2010 Kimber et al 2015Overall
21 5 10 20 50 100
9425057465
151950323344
4100153371
554109 033234664
14823 32760488 449
85388010019 277
18192094
66597819 842
In treatment
38189821479
154267335183679113
441181
1472103 838503809
69445 44952843 4301271469545067
788281674
366328629 565
Out of treatment
No of deathsperson years
375 (303 to 459)151 (61 to 311)77 (43 to 127)96 (66 to 135)
mdash44 (25 to 73)
114 (58 to 224)
51 (47 to 55)49 (31 to 74)63 (54 to 74)68 (63 to 74)
mdash52 (42 to 63)58 (50 to 67)
124 (03 to 692)43 (20 to 82)
45 (12 to 168)
91 (33 to 198)39 (31 to 49)45 (32 to 62)
In treatment
200 (142 to 275)438 (271 to 670)576 (489 to 675)191 (133 to 265)
mdash373 (271 to 500)321 (191 to 539)
142 (135 to 149)131 (97 to 173)
153 (141 to 164)122 (111 to 132)
mdash107 (80 to 139)
135 (119 to 153)
800 (322 to 1648)167 (111 to 242)320 (132 to 775)
45 (09 to 132)97 (86 to 109)
109 (85 to 139)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 4 | all cause mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled all cause mortality rates 2009-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except Degenhardt et al6 which reported mortality before and after two weeks of treatment initiation and cessation high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-analysis area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates before and after four weeks in and out of treatment across methadone or buprenorphine cohorts estimated from multivariate random effects meta-analysis on log transformed rates in four time-by-treatment intervals
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
11
drug use comorbidities prison history overdose his-tory patientrsquos preference) characteristics of treatment (such as previous treatment specialisation of the doc-tor who controls the treatment dose provision charac-teristics cointerventions retention or drop outs) or the sociopolitical context in which studies have been conducted For example the initial prognosis might be better in those given buprenorphine than those given methadone (that is fewer comorbid problems less severe opioid dependence)6 8 10 61 though this was not clearly found in a recent US study62
The role of such confounding factors has received almost empirical examination Few details on char-acteristics of patients or treatments were reported in articles included in this meta-analysis to permit a detailed examination of this potential issue (tables 1 and 2 ) so it was not possible to assess the possibil-ity of confounding A sensitivity simulation analysis in the study by Kimber and colleagues however suggested that the lower mortality with buprenor-phine than with methadone during first four weeks of treatment was unlikely to be caused by unmea-sured confounding10
strengths and limitationsThis meta-analysis synthesised evidence from cohort studies published until 2016 on risk of mortality in people who are dependent on opioids during and after opioid substitution treatment separately for buprenor-phine and methadone Mortality changes over time (1st-32th week) during and after methadone are care-fully quantified for the first time
The published studies however had several methodological shortcomings Firstly in the included
Methadone rst four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallMethadone aer four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Kimber et al 2015Buprenorphine aer four weeks Kimber et al 2015
21 505 10 20
9150018334443371
3317 20015188 4495019 277
22094
2919 842
In treatment
2130010183681181
24960020643 430
165067
181674
12529 565
Out of treatment
No of deathsperson years
60 (27 to 114)54 (32 to 85)12 (03 to 30)35 (13 to 95)
19 (13 to 27)17 (14 to 20)26 (19 to 34)20 (15 to 27)
09 (01 to 34)
15 (10 to 21)
In treatment
15 (02 to 56)54 (26 to 100)68 (29 to 134)42 (18 to 99)
25 (16 to 37)47 (41 to 54)32 (18 to 51)34 (23 to 51)
108 (64 to 170)
42 (35 to 50)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 6 | Overdose mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled overdose mortality rates 2002-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except buster et al7 which reported mortality before and after two weeks of treatment initiation and cessation area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates before and after four weeks in and out of treatment across methadone cohorts estimated from multivariate random-effects meta-analysis on log transformed rates in four time-by-treatment intervals
Time since treatment initiation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s In methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Time since treatment cessation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s Out of methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Degenhardt et al 2009Cornish et al 2010Evans et al 2015Kimber et al 2015Cousins et al 2016
Fig 5 | all cause mortality rates by time since treatment initiation and cessation in methadone cohorts and pooled all cause mortality risk trends 2009-16 high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-regression area of each circle is proportional to weight of each time interval in meta-regression Pooled trends in all cause mortality risk (solid lines) and their 95 confidence intervals (shaded regions) over time in and out of methadone treatment were estimated from bivariate random effects meta-regression of log transformed rates on quadratic linear spline function of log time with knot at four weeks
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
12
observational studies the same patients are compared throughout follow-up periods in and out of opioid sub-stitution treatment but these patients leave and re-en-ter treatment in a non-random way and hence there could still be a large potential for confounding in com-parisons of crude mortality risk in and out of treat-ment In some studies with diverse information on patient demographics severity of drug use and comor-bidities measured mostly at baseline (table 3 ) adjust-ment for these potential confounders resulted in similar or even increased out-to-in mortality rate ratios which merely reflects that the above conditions tended to be less prevalent at baseline among patients who later left or were discharged from treatment than those who remained in treatment Nevertheless to obtain an unbiased estimate of the preventive effect of opioid substitution treatment on all cause and overdose mor-tality these and other relevant confounders should be measured every time a patient leaves and resumes treatment Time varying data can then be used to adjust for confounder history in standard regression models or even better to construct inverse probability of treatment weights for marginal structural models63 which properly control for time varying confounders for later treatment that are themselves affected by pre-vious treatment such as severity of drug use and comorbidity Also differential loss to follow-up is a concern in the meta-analysed cohorts as dropouts are more likely to occur in patients at higher risk of death during periods out of treatment thus inducing a selec-tion bias in crude comparisons of out-to-in mortality risk because of informative censoring Marginal struc-tural models with inverse probability of censoring weights can also be used to correct for differential loss to follow-up63 provided that common predictors of death and censoring are measured over time In sum-mary individual cohorts are prone to confounding and selection bias because of differential loss to follow-up but it is hard to assess with the available information the amount and direction of bias projected onto the pooled mortality rate differences and rate ratios between periods in and out of treatment obtained in this meta-analysis
Secondly studies were conducted in high income countries with the follow-up often spread over many calendar years (1965-2010 for methadone and 1990-2010 for buprenorphine) and a highly variable average length of follow-up (ranges 13-158 years and 11-45 years respectively) Studies in low and middle income countries are especially needed
Thirdly by design we have not captured overdose mortality when opioid substitution treatment was obtained on illicit drug markets40 64 Fourthly a delayed record of treatment cessation could have led to some deaths that occurred out of treatment being incorrectly classified as occurring in treatment40 if so this makes our estimated impact of opioid substitution treatment on mortality a conservative one There could similarly be misclassification between overdose and non-over-dose deaths because of inconsistencies in definition of overdose and codification of causes of deaths (for
instance criteria for separating overdose death from intentional poisoning or sudden cardiac death)40 65 again these misclassifications would tend to underesti-mate deaths from overdose
implications for policy and practiceIn many countries the number of deaths attributable to opioid use is substantial66 67 and increasing in some such as the US where deaths from opioid overdose now outnumber gun related deaths in the country68 Over-doses are preventable causes of death warranting wide implementation of preventive interventions Our review has provided evidence that methadone and probably buprenorphine reduce mortality among people depen-dent on opioids making it imperative that further research confirms this using study designs that con-sider a wide range of confounding variables to increase confidence that these effects are causal
It must be borne in mind that there is strong evidence of the efficacy of methadone and buprenorphine on a range of clinical outcomes and these medicines are listed as WHO essential medicines the findings we have presented here provide additional imperatives for their widespread availability Despite this coverage of opioid substitution treatment is low in many countries worldwide69 Policymakers clinicians and those responsible for drug treatment systems should work to ensure the availability of such treatment remove access barriers and promote engagement This means the strategic development of services from a public health perspective which could reduce the social harm associ-ated with opioid use
Our review suggests that some precautions should be taken during and after opioid substitution treatment to increase safety Firstly careful clinical assessment of opioid tolerance before onset of treatment to establish a safe induction dose seems warranted Secondly moni-toring during the induction period is important espe-cially for methadone with clinicians considering adjusting opioid doses monitoring mental and somatic problems and preventing the use of opioids obtained on the illicit drug market64 In addition education of patients about the risk of overdose risk and use of ldquotake homerdquo naloxone70 71 is warranted Buprenorphine induction followed by transition to methadone might also be considered10 72 Retention in opioid substitution treatment reduces risk of exposure to mortality after cessation and also to re-exposure to mortality risk during induction onto methadone so efforts to improve retention are important as a strategy to reduce mortal-ity More generally establishment of mechanisms for information and coordination between healthcare social and legal services and patient counselling while in treatment in addition to more specific overdose pre-vention programmes such as naloxone distribution should be considered
Finally there is a pressing need for new studies on the comparative effectiveness of methadone and buprenorphine in reducing mortality New ran-domised controlled trials are highly unlikely they would be prohibitively expensive and difficult to
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
8
tabl
e 3
| Poo
led
all c
ause
and
ove
rdos
e m
orta
lity r
ates
dur
ing
perio
ds in
and
out
of o
pioi
d su
bstit
utio
n tre
atm
ent w
ith m
etha
done
by s
tudy
char
acte
ristic
s
stud
y ch
arac
teris
tic
all c
ause
mor
talit
y ra
te1
000
pers
on y
ears
(95
Ci)
Ove
rdos
e m
orta
lity
rate
100
0 pe
rson
yea
rs (9
5 C
i)
no o
f st
udie
sin
trea
tmen
tO
ut o
f tre
atm
ent
P va
luedagger
i2 (
)Daggerno
of
stud
ies
in tr
eatm
ent
Out
of t
reat
men
tP
valu
edaggeri2 (
)Dagger
Loca
tion
E
urop
eIs
rael
913
9 (9
5 to
20
5)46
6 (2
90
to 74
9)
008
987
31
(24
to 4
0)
133
(59
to 2
98)
013
93
Nor
th A
mer
ica
411
2 (6
4 to
196
)42
3 (2
12 to
84
6)2
23
(14
to 3
8)
205
(44
to 9
45)
A
ustra
lia3
63
(33
to 12
1)14
0 (6
3 to
30
8)2
20
(14
to 2
9)
67
(15
to 2
96)
Opio
id in
ject
ors (
)
lt
100
129
0 (6
9 to
117
)25
8 (1
87
to 3
55)
000
195
102
5 (2
0 to
30
)10
6 (6
1 to
185
)mdash
mdash
100
423
4 (1
42
to 3
85)
109
9 (5
94
to 2
034
)1
mdashsect
mdashsect
Men
()
lt
7511
95
(69
to 13
2)
300
(18
4 to
48
8)0
6798
62
4 (1
8 to
34
)10
6 (4
5 to
24
8)0
7493
ge
753
116
(61
to 2
20)
459
(178
to 11
79)
52
9 (2
0 to
42
)15
8 (6
2 to
40
3)M
ean
age
(yea
rs)
lt
3510
99
(68
to 14
5)
293
(179
to 4
82)
040
988
26
(19
to 3
5)
106
(52
to 2
18)
060
93
ge35
614
0 (8
7 to
22
7)50
3 (2
68
to 9
43)
32
7 (1
5 to
47
)20
5 (6
2 to
676
)Av
erag
e m
etha
done
dos
e (m
gda
y)
le
807
96
(63
to 14
8)
269
(15
5 to
46
5)0
5692
53
1 (2
0 to
46
)10
3 (4
0 to
26
9)0
2293
gt
805
99
(60
to 16
5)
354
(18
5 to
677
)5
25
(16
to 3
9)
170
(65
to 4
49)
Inpa
tient
indu
ctio
n (
)
09
92
(63
to 13
6)
299
(173
to 5
16)
019
987
25
(18
to 3
4)
100
(45
to 2
23)
065
93
gt0
615
4 (9
3 to
25
3)45
9 (2
29
to 9
21)
32
9 (1
7 to
50
)18
4 (5
4 to
62
5)Tr
eatm
ent p
rovi
der
S
peci
alis
t10
134
(92
to 19
5)
465
(28
2 to
765
)0
2698
72
5 (1
7 to
37
)20
8 (1
11 to
38
8)0
0188
G
Pm
ixed
68
6 (5
4 to
137
)24
4 (1
31
to 4
54)
42
4 (1
6 to
36
)5
6 (2
5 to
125
)M
idpo
int f
ollo
w-u
p pe
riod
lt
2000
1012
6 (8
5 to
187
)38
8 (2
28
to 6
61)
058
987
28
(20
to 3
9)
154
(70
to 3
39)
067
93
ge20
006
97
(60
to 15
9)
320
(16
5 to
62
3)4
24
(17
to 3
5)
90
(32
to 2
52)
Loss
to fo
llow
-up
()
lt
1012
119
(83
to 1
70)
383
(23
7 to
619
)0
8198
82
5 (1
9 to
32
)9
8 (5
0 to
195
)0
3393
ge
104
95
(50
to 18
0)
313
(13
5 to
72
3)3
32
(17
to 6
0)
254
(81
to 7
94)
Poo
led
mor
talit
y rat
es a
nd 9
5 c
onfid
ence
inte
rval
s dur
ing
perio
ds in
and
out
of t
reat
men
t by s
tudy
cha
ract
eris
tics e
stim
ated
from
sep
arat
e bi
varia
te ra
ndom
effe
cts m
eta-
regr
essi
on m
odel
s rel
atin
g lo
g tra
nsfo
rmed
rate
s in
both
trea
tmen
t per
iods
w
ith e
ach
stud
y cha
ract
eris
tic
daggerOve
rall
P va
lue
for h
eter
ogen
eity
of p
oole
d m
orta
lity r
ates
acr
oss c
ateg
orie
s of s
tudy
cha
ract
eris
tic a
s obt
aine
d fro
m li
kelih
ood
ratio
test
com
parin
g ne
sted
met
a-re
gres
sion
mod
els w
ith a
nd w
ithou
t stu
dy c
hara
cter
istic
fitte
d vi
a m
axim
um li
kelih
ood
DaggerOve
rall
I2 sta
tistic
for r
esid
ual h
eter
ogen
eity
in s
tudy
spe
cific
mor
talit
y rat
es n
ot e
xpla
ined
by c
orre
spon
ding
stu
dy c
hara
cter
istic
sectP
oole
d m
orta
lity r
ates
not
app
licab
le to
cat
egor
ies w
ith s
ingl
e st
udy
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
9
Although the long half life of methadone could con-tribute to the increase in mortality in the first three to four days after cessation of treatment there was a large increase in mortality across the first four weeks after cessation compared with the treatment period Such increased mortality could be explained by loss of toler-ance to the toxic effects of heroin assuming that many patients return to use6 8 32 47 55 56 and probably also by the use of multiple legal and illicit substances during that period Similar peaks in drug related mortality occur in other situations where opioid tolerance is prob-ably diminished (for example after prison release or hospital discharge57-59 ) Lifestyle factors and comorbid issues such as mental health problems could also increase mortality from other external causes as deaths from suicide and injury are also more common during that period53
Mortality risk during specific periods in and out of buprenorphine treatmentData from three cohorts (two from Australia) suggest that substitution treatment with buprenorphine could reduce all cause mortality although the disparity in mortality rates in periods in and out of treatment did not reach significance Findings also suggest a signifi-cantly increased mortality in the first four weeks after cessation of treatment compared with the remaining time out of treatment (320 versus 1091000 person years) while during the treatment period there was no difference between the first four weeks and the remain-ing time in treatment It is difficult to draw firm conclu-sions because of limited evidence from similar settings 96 of included deaths and 98 of person years came from Australian studies (with 87 and 86 from the study by Kimber and colleagues13)
Comparative effectiveness of buprenorphine and methadone substitution treatmentOther sources of data have suggested that buprenor-phine could be more effective than methadone in reduc-ing mortality especially from overdose39 42 43 Unlike methadone there is a ceiling for respiratory depressant effects of buprenorphine as dose increases and the probability of triggering arrhythmias is lower for buprenorphine than methadone41 44 60 When we com-pared the mortality between periods in and out of treat-ment first within those taking methadone and then within those taking buprenorphine we found a greater reduction in mortality with methadone than with buprenorphine (measured as the rate difference or rate ratio between periods) When we compared mortality between them first within the treatment period and then in the period off treatment we found a signifi-cantly lower mortality with buprenorphine than meth-adone in both periods
Our conclusions must remain tentative until further studies in varied treatment settings and contexts are undertaken to examine this issue Differences in mor-tality might also reflect confounding through differ-ences in characteristics of patients (such as age severity of opioid dependence injecting drug use other ta
ble
4 | C
ohor
t stu
dies
repo
rtin
g al
l cau
se a
nd o
verd
ose
mor
talit
y rat
e ra
tios c
ompa
ring
perio
ds o
ut a
nd in
opi
oid
subs
titut
ion
treat
men
t adj
uste
d fo
r con
foun
ding
stud
y
Conf
ound
ing
fact
ors
all c
ause
mor
talit
yO
verd
ose
mor
talit
y
Patie
nt d
emog
raph
ics
seve
rity
of d
rug
use
trea
tmen
tCo
mor
bidi
tyun
adju
sted
ra
te ra
tioad
just
ed
rate
ratio
Perc
enta
ge
chan
gedagger
unad
just
ed
rate
ratio
adju
sted
ra
te ra
tioPe
rcen
tage
ch
ange
dagger
Met
hado
neBu
ster
200
27Se
x ra
ceTr
eatm
ent m
odal
ity t
ime
sinc
e fir
st tr
eatm
ent
mdashmdash
mdashmdash
087
087
minus03
Davo
li 2
00732
Age
sex
Leng
th o
f her
oin
use
her
oin
inje
ctio
n
prev
ious
ove
rdos
eHI
V p
sych
iatri
c com
orbi
dity
mdashmdash
mdash77
174
3minus3
6
Dege
nhar
dt 2
0096
Age
sex
cal
enda
r yea
rmdash
mdash19
118
8minus1
3mdash
mdashmdash
Corn
ish
201
08Ag
e s
ex c
alen
dar y
ear
mdashM
edic
al c
omor
bidi
ty2
833
2715
5mdash
mdashmdash
Evan
s 2
0159Dagger
Age
sex
rac
e e
duca
tion
em
ploy
men
t cr
imin
ality
hea
lth c
over
age
Prim
ary o
pioi
d fr
eque
ncy a
nd le
ngth
of
opio
id u
se n
on-o
pioi
d dr
ug u
seHI
V h
epat
itis C
tub
ercu
losi
s
disa
bilit
y m
edic
al c
omor
bidi
ty
psyc
hiat
ric c
omor
bidi
ty
273
370
355
351
442
258
Nosy
k 2
01536
DaggerAg
e s
ex r
ace
cal
enda
r yea
r re
gion
No o
f pre
viou
s tre
atm
ent e
piso
des
Tim
e si
nce
HIV
diag
nosi
s C
D4
coun
t AI
DS a
ntire
trovi
ral
ther
apy
med
ical
com
orbi
dity
304
294
minus34
114
147
286
Cous
ins
201
637Ag
e s
exTr
eatm
ent s
uper
visi
on m
etha
done
dos
eM
edic
al c
omor
bidi
ty3
093
6417
816
016
317
bupr
enor
phin
eCo
rnis
h 2
0108
Age
sex
cal
enda
r yea
rmdash
Med
ical
com
orbi
dity
141
164
168
mdashmdash
mdashB
asel
ine
or ti
me
vary
ing
conf
ound
ing
fact
ors u
sed
in a
djus
tmen
tdaggerP
erce
ntag
e ch
ange
in ra
te ra
tio a
fter a
djus
tmen
t for
cor
resp
ondi
ng c
onfo
undi
ng fa
ctor
sDaggerO
verd
ose
mor
talit
y rat
e ra
tios r
epor
ted
com
bini
ng m
etha
done
mai
nten
ance
with
det
oxifi
catio
n (1
14
of p
erso
n ye
ars i
n tre
atm
ent)
in E
vans
et a
l9 an
d in
clud
ing
neve
r tre
ated
par
ticip
ants
(73
3 o
f per
son
year
s out
of t
reat
men
t) in
Nos
yk e
t al36
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
10
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1996 Buster et al 2002 Scherbaum et al 2002 Davoli et al 2007 Clausen et al 2008 Peles et al 2010 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine Kimber et al 2015
2105 5 10 20 50 100
3314 474416557108541792
4218 7476111475751
24645053985
16991 7925422 648
3121 936
In treatment
2111707297
27740192004
2610 983131729998
28130313727
21645 265246247
14331 239
Out of treatment
No of deathsperson years
23 (16 to 32)24 (07 to 62)
64 (26 to 133)22 (06 to 57)22 (16 to 30)
54 (20 to 117)12 (05 to 25)37 (24 to 55)12 (04 to 29)18 (16 to 21)24 (18 to 31)26 (21 to 33)
14 (10 to 20)
In treatment
179 (111 to 274)236 (95 to 486)
365 (240 to 531)95 (57 to 148)24 (16 to 35)
756 (402 to 1292)90 (41 to 171)
215 (143 to 311)179 (95 to 306)
48 (42 to 54)38 (25 to 57)
127 (69 to 234)
46 (39 to 54)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 3 | Overdose mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled overdose mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates during periods in and out of treatment across all methadone cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
Methadone rst four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallMethadone aer four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Cornish et al 2010 Kimber et al 2015OverallBuprenorphine aer four weeks Cornish et al 2010 Kimber et al 2015Overall
21 5 10 20 50 100
9425057465
151950323344
4100153371
554109 033234664
14823 32760488 449
85388010019 277
18192094
66597819 842
In treatment
38189821479
154267335183679113
441181
1472103 838503809
69445 44952843 4301271469545067
788281674
366328629 565
Out of treatment
No of deathsperson years
375 (303 to 459)151 (61 to 311)77 (43 to 127)96 (66 to 135)
mdash44 (25 to 73)
114 (58 to 224)
51 (47 to 55)49 (31 to 74)63 (54 to 74)68 (63 to 74)
mdash52 (42 to 63)58 (50 to 67)
124 (03 to 692)43 (20 to 82)
45 (12 to 168)
91 (33 to 198)39 (31 to 49)45 (32 to 62)
In treatment
200 (142 to 275)438 (271 to 670)576 (489 to 675)191 (133 to 265)
mdash373 (271 to 500)321 (191 to 539)
142 (135 to 149)131 (97 to 173)
153 (141 to 164)122 (111 to 132)
mdash107 (80 to 139)
135 (119 to 153)
800 (322 to 1648)167 (111 to 242)320 (132 to 775)
45 (09 to 132)97 (86 to 109)
109 (85 to 139)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 4 | all cause mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled all cause mortality rates 2009-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except Degenhardt et al6 which reported mortality before and after two weeks of treatment initiation and cessation high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-analysis area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates before and after four weeks in and out of treatment across methadone or buprenorphine cohorts estimated from multivariate random effects meta-analysis on log transformed rates in four time-by-treatment intervals
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
11
drug use comorbidities prison history overdose his-tory patientrsquos preference) characteristics of treatment (such as previous treatment specialisation of the doc-tor who controls the treatment dose provision charac-teristics cointerventions retention or drop outs) or the sociopolitical context in which studies have been conducted For example the initial prognosis might be better in those given buprenorphine than those given methadone (that is fewer comorbid problems less severe opioid dependence)6 8 10 61 though this was not clearly found in a recent US study62
The role of such confounding factors has received almost empirical examination Few details on char-acteristics of patients or treatments were reported in articles included in this meta-analysis to permit a detailed examination of this potential issue (tables 1 and 2 ) so it was not possible to assess the possibil-ity of confounding A sensitivity simulation analysis in the study by Kimber and colleagues however suggested that the lower mortality with buprenor-phine than with methadone during first four weeks of treatment was unlikely to be caused by unmea-sured confounding10
strengths and limitationsThis meta-analysis synthesised evidence from cohort studies published until 2016 on risk of mortality in people who are dependent on opioids during and after opioid substitution treatment separately for buprenor-phine and methadone Mortality changes over time (1st-32th week) during and after methadone are care-fully quantified for the first time
The published studies however had several methodological shortcomings Firstly in the included
Methadone rst four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallMethadone aer four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Kimber et al 2015Buprenorphine aer four weeks Kimber et al 2015
21 505 10 20
9150018334443371
3317 20015188 4495019 277
22094
2919 842
In treatment
2130010183681181
24960020643 430
165067
181674
12529 565
Out of treatment
No of deathsperson years
60 (27 to 114)54 (32 to 85)12 (03 to 30)35 (13 to 95)
19 (13 to 27)17 (14 to 20)26 (19 to 34)20 (15 to 27)
09 (01 to 34)
15 (10 to 21)
In treatment
15 (02 to 56)54 (26 to 100)68 (29 to 134)42 (18 to 99)
25 (16 to 37)47 (41 to 54)32 (18 to 51)34 (23 to 51)
108 (64 to 170)
42 (35 to 50)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 6 | Overdose mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled overdose mortality rates 2002-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except buster et al7 which reported mortality before and after two weeks of treatment initiation and cessation area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates before and after four weeks in and out of treatment across methadone cohorts estimated from multivariate random-effects meta-analysis on log transformed rates in four time-by-treatment intervals
Time since treatment initiation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s In methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Time since treatment cessation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s Out of methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Degenhardt et al 2009Cornish et al 2010Evans et al 2015Kimber et al 2015Cousins et al 2016
Fig 5 | all cause mortality rates by time since treatment initiation and cessation in methadone cohorts and pooled all cause mortality risk trends 2009-16 high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-regression area of each circle is proportional to weight of each time interval in meta-regression Pooled trends in all cause mortality risk (solid lines) and their 95 confidence intervals (shaded regions) over time in and out of methadone treatment were estimated from bivariate random effects meta-regression of log transformed rates on quadratic linear spline function of log time with knot at four weeks
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
12
observational studies the same patients are compared throughout follow-up periods in and out of opioid sub-stitution treatment but these patients leave and re-en-ter treatment in a non-random way and hence there could still be a large potential for confounding in com-parisons of crude mortality risk in and out of treat-ment In some studies with diverse information on patient demographics severity of drug use and comor-bidities measured mostly at baseline (table 3 ) adjust-ment for these potential confounders resulted in similar or even increased out-to-in mortality rate ratios which merely reflects that the above conditions tended to be less prevalent at baseline among patients who later left or were discharged from treatment than those who remained in treatment Nevertheless to obtain an unbiased estimate of the preventive effect of opioid substitution treatment on all cause and overdose mor-tality these and other relevant confounders should be measured every time a patient leaves and resumes treatment Time varying data can then be used to adjust for confounder history in standard regression models or even better to construct inverse probability of treatment weights for marginal structural models63 which properly control for time varying confounders for later treatment that are themselves affected by pre-vious treatment such as severity of drug use and comorbidity Also differential loss to follow-up is a concern in the meta-analysed cohorts as dropouts are more likely to occur in patients at higher risk of death during periods out of treatment thus inducing a selec-tion bias in crude comparisons of out-to-in mortality risk because of informative censoring Marginal struc-tural models with inverse probability of censoring weights can also be used to correct for differential loss to follow-up63 provided that common predictors of death and censoring are measured over time In sum-mary individual cohorts are prone to confounding and selection bias because of differential loss to follow-up but it is hard to assess with the available information the amount and direction of bias projected onto the pooled mortality rate differences and rate ratios between periods in and out of treatment obtained in this meta-analysis
Secondly studies were conducted in high income countries with the follow-up often spread over many calendar years (1965-2010 for methadone and 1990-2010 for buprenorphine) and a highly variable average length of follow-up (ranges 13-158 years and 11-45 years respectively) Studies in low and middle income countries are especially needed
Thirdly by design we have not captured overdose mortality when opioid substitution treatment was obtained on illicit drug markets40 64 Fourthly a delayed record of treatment cessation could have led to some deaths that occurred out of treatment being incorrectly classified as occurring in treatment40 if so this makes our estimated impact of opioid substitution treatment on mortality a conservative one There could similarly be misclassification between overdose and non-over-dose deaths because of inconsistencies in definition of overdose and codification of causes of deaths (for
instance criteria for separating overdose death from intentional poisoning or sudden cardiac death)40 65 again these misclassifications would tend to underesti-mate deaths from overdose
implications for policy and practiceIn many countries the number of deaths attributable to opioid use is substantial66 67 and increasing in some such as the US where deaths from opioid overdose now outnumber gun related deaths in the country68 Over-doses are preventable causes of death warranting wide implementation of preventive interventions Our review has provided evidence that methadone and probably buprenorphine reduce mortality among people depen-dent on opioids making it imperative that further research confirms this using study designs that con-sider a wide range of confounding variables to increase confidence that these effects are causal
It must be borne in mind that there is strong evidence of the efficacy of methadone and buprenorphine on a range of clinical outcomes and these medicines are listed as WHO essential medicines the findings we have presented here provide additional imperatives for their widespread availability Despite this coverage of opioid substitution treatment is low in many countries worldwide69 Policymakers clinicians and those responsible for drug treatment systems should work to ensure the availability of such treatment remove access barriers and promote engagement This means the strategic development of services from a public health perspective which could reduce the social harm associ-ated with opioid use
Our review suggests that some precautions should be taken during and after opioid substitution treatment to increase safety Firstly careful clinical assessment of opioid tolerance before onset of treatment to establish a safe induction dose seems warranted Secondly moni-toring during the induction period is important espe-cially for methadone with clinicians considering adjusting opioid doses monitoring mental and somatic problems and preventing the use of opioids obtained on the illicit drug market64 In addition education of patients about the risk of overdose risk and use of ldquotake homerdquo naloxone70 71 is warranted Buprenorphine induction followed by transition to methadone might also be considered10 72 Retention in opioid substitution treatment reduces risk of exposure to mortality after cessation and also to re-exposure to mortality risk during induction onto methadone so efforts to improve retention are important as a strategy to reduce mortal-ity More generally establishment of mechanisms for information and coordination between healthcare social and legal services and patient counselling while in treatment in addition to more specific overdose pre-vention programmes such as naloxone distribution should be considered
Finally there is a pressing need for new studies on the comparative effectiveness of methadone and buprenorphine in reducing mortality New ran-domised controlled trials are highly unlikely they would be prohibitively expensive and difficult to
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score

thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
9
Although the long half life of methadone could con-tribute to the increase in mortality in the first three to four days after cessation of treatment there was a large increase in mortality across the first four weeks after cessation compared with the treatment period Such increased mortality could be explained by loss of toler-ance to the toxic effects of heroin assuming that many patients return to use6 8 32 47 55 56 and probably also by the use of multiple legal and illicit substances during that period Similar peaks in drug related mortality occur in other situations where opioid tolerance is prob-ably diminished (for example after prison release or hospital discharge57-59 ) Lifestyle factors and comorbid issues such as mental health problems could also increase mortality from other external causes as deaths from suicide and injury are also more common during that period53
Mortality risk during specific periods in and out of buprenorphine treatmentData from three cohorts (two from Australia) suggest that substitution treatment with buprenorphine could reduce all cause mortality although the disparity in mortality rates in periods in and out of treatment did not reach significance Findings also suggest a signifi-cantly increased mortality in the first four weeks after cessation of treatment compared with the remaining time out of treatment (320 versus 1091000 person years) while during the treatment period there was no difference between the first four weeks and the remain-ing time in treatment It is difficult to draw firm conclu-sions because of limited evidence from similar settings 96 of included deaths and 98 of person years came from Australian studies (with 87 and 86 from the study by Kimber and colleagues13)
Comparative effectiveness of buprenorphine and methadone substitution treatmentOther sources of data have suggested that buprenor-phine could be more effective than methadone in reduc-ing mortality especially from overdose39 42 43 Unlike methadone there is a ceiling for respiratory depressant effects of buprenorphine as dose increases and the probability of triggering arrhythmias is lower for buprenorphine than methadone41 44 60 When we com-pared the mortality between periods in and out of treat-ment first within those taking methadone and then within those taking buprenorphine we found a greater reduction in mortality with methadone than with buprenorphine (measured as the rate difference or rate ratio between periods) When we compared mortality between them first within the treatment period and then in the period off treatment we found a signifi-cantly lower mortality with buprenorphine than meth-adone in both periods
Our conclusions must remain tentative until further studies in varied treatment settings and contexts are undertaken to examine this issue Differences in mor-tality might also reflect confounding through differ-ences in characteristics of patients (such as age severity of opioid dependence injecting drug use other ta
ble
4 | C
ohor
t stu
dies
repo
rtin
g al
l cau
se a
nd o
verd
ose
mor
talit
y rat
e ra
tios c
ompa
ring
perio
ds o
ut a
nd in
opi
oid
subs
titut
ion
treat
men
t adj
uste
d fo
r con
foun
ding
stud
y
Conf
ound
ing
fact
ors
all c
ause
mor
talit
yO
verd
ose
mor
talit
y
Patie
nt d
emog
raph
ics
seve
rity
of d
rug
use
trea
tmen
tCo
mor
bidi
tyun
adju
sted
ra
te ra
tioad
just
ed
rate
ratio
Perc
enta
ge
chan
gedagger
unad
just
ed
rate
ratio
adju
sted
ra
te ra
tioPe
rcen
tage
ch
ange
dagger
Met
hado
neBu
ster
200
27Se
x ra
ceTr
eatm
ent m
odal
ity t
ime
sinc
e fir
st tr
eatm
ent
mdashmdash
mdashmdash
087
087
minus03
Davo
li 2
00732
Age
sex
Leng
th o
f her
oin
use
her
oin
inje
ctio
n
prev
ious
ove
rdos
eHI
V p
sych
iatri
c com
orbi
dity
mdashmdash
mdash77
174
3minus3
6
Dege
nhar
dt 2
0096
Age
sex
cal
enda
r yea
rmdash
mdash19
118
8minus1
3mdash
mdashmdash
Corn
ish
201
08Ag
e s
ex c
alen
dar y
ear
mdashM
edic
al c
omor
bidi
ty2
833
2715
5mdash
mdashmdash
Evan
s 2
0159Dagger
Age
sex
rac
e e
duca
tion
em
ploy
men
t cr
imin
ality
hea
lth c
over
age
Prim
ary o
pioi
d fr
eque
ncy a
nd le
ngth
of
opio
id u
se n
on-o
pioi
d dr
ug u
seHI
V h
epat
itis C
tub
ercu
losi
s
disa
bilit
y m
edic
al c
omor
bidi
ty
psyc
hiat
ric c
omor
bidi
ty
273
370
355
351
442
258
Nosy
k 2
01536
DaggerAg
e s
ex r
ace
cal
enda
r yea
r re
gion
No o
f pre
viou
s tre
atm
ent e
piso
des
Tim
e si
nce
HIV
diag
nosi
s C
D4
coun
t AI
DS a
ntire
trovi
ral
ther
apy
med
ical
com
orbi
dity
304
294
minus34
114
147
286
Cous
ins
201
637Ag
e s
exTr
eatm
ent s
uper
visi
on m
etha
done
dos
eM
edic
al c
omor
bidi
ty3
093
6417
816
016
317
bupr
enor
phin
eCo
rnis
h 2
0108
Age
sex
cal
enda
r yea
rmdash
Med
ical
com
orbi
dity
141
164
168
mdashmdash
mdashB
asel
ine
or ti
me
vary
ing
conf
ound
ing
fact
ors u
sed
in a
djus
tmen
tdaggerP
erce
ntag
e ch
ange
in ra
te ra
tio a
fter a
djus
tmen
t for
cor
resp
ondi
ng c
onfo
undi
ng fa
ctor
sDaggerO
verd
ose
mor
talit
y rat
e ra
tios r
epor
ted
com
bini
ng m
etha
done
mai
nten
ance
with
det
oxifi
catio
n (1
14
of p
erso
n ye
ars i
n tre
atm
ent)
in E
vans
et a
l9 an
d in
clud
ing
neve
r tre
ated
par
ticip
ants
(73
3 o
f per
son
year
s out
of t
reat
men
t) in
Nos
yk e
t al36
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
10
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1996 Buster et al 2002 Scherbaum et al 2002 Davoli et al 2007 Clausen et al 2008 Peles et al 2010 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine Kimber et al 2015
2105 5 10 20 50 100
3314 474416557108541792
4218 7476111475751
24645053985
16991 7925422 648
3121 936
In treatment
2111707297
27740192004
2610 983131729998
28130313727
21645 265246247
14331 239
Out of treatment
No of deathsperson years
23 (16 to 32)24 (07 to 62)
64 (26 to 133)22 (06 to 57)22 (16 to 30)
54 (20 to 117)12 (05 to 25)37 (24 to 55)12 (04 to 29)18 (16 to 21)24 (18 to 31)26 (21 to 33)
14 (10 to 20)
In treatment
179 (111 to 274)236 (95 to 486)
365 (240 to 531)95 (57 to 148)24 (16 to 35)
756 (402 to 1292)90 (41 to 171)
215 (143 to 311)179 (95 to 306)
48 (42 to 54)38 (25 to 57)
127 (69 to 234)
46 (39 to 54)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 3 | Overdose mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled overdose mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates during periods in and out of treatment across all methadone cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
Methadone rst four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallMethadone aer four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Cornish et al 2010 Kimber et al 2015OverallBuprenorphine aer four weeks Cornish et al 2010 Kimber et al 2015Overall
21 5 10 20 50 100
9425057465
151950323344
4100153371
554109 033234664
14823 32760488 449
85388010019 277
18192094
66597819 842
In treatment
38189821479
154267335183679113
441181
1472103 838503809
69445 44952843 4301271469545067
788281674
366328629 565
Out of treatment
No of deathsperson years
375 (303 to 459)151 (61 to 311)77 (43 to 127)96 (66 to 135)
mdash44 (25 to 73)
114 (58 to 224)
51 (47 to 55)49 (31 to 74)63 (54 to 74)68 (63 to 74)
mdash52 (42 to 63)58 (50 to 67)
124 (03 to 692)43 (20 to 82)
45 (12 to 168)
91 (33 to 198)39 (31 to 49)45 (32 to 62)
In treatment
200 (142 to 275)438 (271 to 670)576 (489 to 675)191 (133 to 265)
mdash373 (271 to 500)321 (191 to 539)
142 (135 to 149)131 (97 to 173)
153 (141 to 164)122 (111 to 132)
mdash107 (80 to 139)
135 (119 to 153)
800 (322 to 1648)167 (111 to 242)320 (132 to 775)
45 (09 to 132)97 (86 to 109)
109 (85 to 139)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 4 | all cause mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled all cause mortality rates 2009-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except Degenhardt et al6 which reported mortality before and after two weeks of treatment initiation and cessation high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-analysis area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates before and after four weeks in and out of treatment across methadone or buprenorphine cohorts estimated from multivariate random effects meta-analysis on log transformed rates in four time-by-treatment intervals
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
11
drug use comorbidities prison history overdose his-tory patientrsquos preference) characteristics of treatment (such as previous treatment specialisation of the doc-tor who controls the treatment dose provision charac-teristics cointerventions retention or drop outs) or the sociopolitical context in which studies have been conducted For example the initial prognosis might be better in those given buprenorphine than those given methadone (that is fewer comorbid problems less severe opioid dependence)6 8 10 61 though this was not clearly found in a recent US study62
The role of such confounding factors has received almost empirical examination Few details on char-acteristics of patients or treatments were reported in articles included in this meta-analysis to permit a detailed examination of this potential issue (tables 1 and 2 ) so it was not possible to assess the possibil-ity of confounding A sensitivity simulation analysis in the study by Kimber and colleagues however suggested that the lower mortality with buprenor-phine than with methadone during first four weeks of treatment was unlikely to be caused by unmea-sured confounding10
strengths and limitationsThis meta-analysis synthesised evidence from cohort studies published until 2016 on risk of mortality in people who are dependent on opioids during and after opioid substitution treatment separately for buprenor-phine and methadone Mortality changes over time (1st-32th week) during and after methadone are care-fully quantified for the first time
The published studies however had several methodological shortcomings Firstly in the included
Methadone rst four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallMethadone aer four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Kimber et al 2015Buprenorphine aer four weeks Kimber et al 2015
21 505 10 20
9150018334443371
3317 20015188 4495019 277
22094
2919 842
In treatment
2130010183681181
24960020643 430
165067
181674
12529 565
Out of treatment
No of deathsperson years
60 (27 to 114)54 (32 to 85)12 (03 to 30)35 (13 to 95)
19 (13 to 27)17 (14 to 20)26 (19 to 34)20 (15 to 27)
09 (01 to 34)
15 (10 to 21)
In treatment
15 (02 to 56)54 (26 to 100)68 (29 to 134)42 (18 to 99)
25 (16 to 37)47 (41 to 54)32 (18 to 51)34 (23 to 51)
108 (64 to 170)
42 (35 to 50)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 6 | Overdose mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled overdose mortality rates 2002-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except buster et al7 which reported mortality before and after two weeks of treatment initiation and cessation area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates before and after four weeks in and out of treatment across methadone cohorts estimated from multivariate random-effects meta-analysis on log transformed rates in four time-by-treatment intervals
Time since treatment initiation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s In methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Time since treatment cessation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s Out of methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Degenhardt et al 2009Cornish et al 2010Evans et al 2015Kimber et al 2015Cousins et al 2016
Fig 5 | all cause mortality rates by time since treatment initiation and cessation in methadone cohorts and pooled all cause mortality risk trends 2009-16 high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-regression area of each circle is proportional to weight of each time interval in meta-regression Pooled trends in all cause mortality risk (solid lines) and their 95 confidence intervals (shaded regions) over time in and out of methadone treatment were estimated from bivariate random effects meta-regression of log transformed rates on quadratic linear spline function of log time with knot at four weeks
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
12
observational studies the same patients are compared throughout follow-up periods in and out of opioid sub-stitution treatment but these patients leave and re-en-ter treatment in a non-random way and hence there could still be a large potential for confounding in com-parisons of crude mortality risk in and out of treat-ment In some studies with diverse information on patient demographics severity of drug use and comor-bidities measured mostly at baseline (table 3 ) adjust-ment for these potential confounders resulted in similar or even increased out-to-in mortality rate ratios which merely reflects that the above conditions tended to be less prevalent at baseline among patients who later left or were discharged from treatment than those who remained in treatment Nevertheless to obtain an unbiased estimate of the preventive effect of opioid substitution treatment on all cause and overdose mor-tality these and other relevant confounders should be measured every time a patient leaves and resumes treatment Time varying data can then be used to adjust for confounder history in standard regression models or even better to construct inverse probability of treatment weights for marginal structural models63 which properly control for time varying confounders for later treatment that are themselves affected by pre-vious treatment such as severity of drug use and comorbidity Also differential loss to follow-up is a concern in the meta-analysed cohorts as dropouts are more likely to occur in patients at higher risk of death during periods out of treatment thus inducing a selec-tion bias in crude comparisons of out-to-in mortality risk because of informative censoring Marginal struc-tural models with inverse probability of censoring weights can also be used to correct for differential loss to follow-up63 provided that common predictors of death and censoring are measured over time In sum-mary individual cohorts are prone to confounding and selection bias because of differential loss to follow-up but it is hard to assess with the available information the amount and direction of bias projected onto the pooled mortality rate differences and rate ratios between periods in and out of treatment obtained in this meta-analysis
Secondly studies were conducted in high income countries with the follow-up often spread over many calendar years (1965-2010 for methadone and 1990-2010 for buprenorphine) and a highly variable average length of follow-up (ranges 13-158 years and 11-45 years respectively) Studies in low and middle income countries are especially needed
Thirdly by design we have not captured overdose mortality when opioid substitution treatment was obtained on illicit drug markets40 64 Fourthly a delayed record of treatment cessation could have led to some deaths that occurred out of treatment being incorrectly classified as occurring in treatment40 if so this makes our estimated impact of opioid substitution treatment on mortality a conservative one There could similarly be misclassification between overdose and non-over-dose deaths because of inconsistencies in definition of overdose and codification of causes of deaths (for
instance criteria for separating overdose death from intentional poisoning or sudden cardiac death)40 65 again these misclassifications would tend to underesti-mate deaths from overdose
implications for policy and practiceIn many countries the number of deaths attributable to opioid use is substantial66 67 and increasing in some such as the US where deaths from opioid overdose now outnumber gun related deaths in the country68 Over-doses are preventable causes of death warranting wide implementation of preventive interventions Our review has provided evidence that methadone and probably buprenorphine reduce mortality among people depen-dent on opioids making it imperative that further research confirms this using study designs that con-sider a wide range of confounding variables to increase confidence that these effects are causal
It must be borne in mind that there is strong evidence of the efficacy of methadone and buprenorphine on a range of clinical outcomes and these medicines are listed as WHO essential medicines the findings we have presented here provide additional imperatives for their widespread availability Despite this coverage of opioid substitution treatment is low in many countries worldwide69 Policymakers clinicians and those responsible for drug treatment systems should work to ensure the availability of such treatment remove access barriers and promote engagement This means the strategic development of services from a public health perspective which could reduce the social harm associ-ated with opioid use
Our review suggests that some precautions should be taken during and after opioid substitution treatment to increase safety Firstly careful clinical assessment of opioid tolerance before onset of treatment to establish a safe induction dose seems warranted Secondly moni-toring during the induction period is important espe-cially for methadone with clinicians considering adjusting opioid doses monitoring mental and somatic problems and preventing the use of opioids obtained on the illicit drug market64 In addition education of patients about the risk of overdose risk and use of ldquotake homerdquo naloxone70 71 is warranted Buprenorphine induction followed by transition to methadone might also be considered10 72 Retention in opioid substitution treatment reduces risk of exposure to mortality after cessation and also to re-exposure to mortality risk during induction onto methadone so efforts to improve retention are important as a strategy to reduce mortal-ity More generally establishment of mechanisms for information and coordination between healthcare social and legal services and patient counselling while in treatment in addition to more specific overdose pre-vention programmes such as naloxone distribution should be considered
Finally there is a pressing need for new studies on the comparative effectiveness of methadone and buprenorphine in reducing mortality New ran-domised controlled trials are highly unlikely they would be prohibitively expensive and difficult to
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score

doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
10
Methadone Gearing et al 1974 Cushman 1977 Groumlnbladh et al 1990 Caplehorn et al 1996 Buster et al 2002 Scherbaum et al 2002 Davoli et al 2007 Clausen et al 2008 Peles et al 2010 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine Kimber et al 2015
2105 5 10 20 50 100
3314 474416557108541792
4218 7476111475751
24645053985
16991 7925422 648
3121 936
In treatment
2111707297
27740192004
2610 983131729998
28130313727
21645 265246247
14331 239
Out of treatment
No of deathsperson years
23 (16 to 32)24 (07 to 62)
64 (26 to 133)22 (06 to 57)22 (16 to 30)
54 (20 to 117)12 (05 to 25)37 (24 to 55)12 (04 to 29)18 (16 to 21)24 (18 to 31)26 (21 to 33)
14 (10 to 20)
In treatment
179 (111 to 274)236 (95 to 486)
365 (240 to 531)95 (57 to 148)24 (16 to 35)
756 (402 to 1292)90 (41 to 171)
215 (143 to 311)179 (95 to 306)
48 (42 to 54)38 (25 to 57)
127 (69 to 234)
46 (39 to 54)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 3 | Overdose mortality rates in and out of opioid substitution treatment with methadone or buprenorphine and overall pooled overdose mortality rates 1974-2016 area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates during periods in and out of treatment across all methadone cohorts estimated from bivariate random effects meta-analysis on log transformed rates in both treatment periods
Methadone rst four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallMethadone aer four weeks Degenhardt et al 2009 Cornish et al 2010 Evans et al 2015 Kimber et al 2015 Nosyk et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Cornish et al 2010 Kimber et al 2015OverallBuprenorphine aer four weeks Cornish et al 2010 Kimber et al 2015Overall
21 5 10 20 50 100
9425057465
151950323344
4100153371
554109 033234664
14823 32760488 449
85388010019 277
18192094
66597819 842
In treatment
38189821479
154267335183679113
441181
1472103 838503809
69445 44952843 4301271469545067
788281674
366328629 565
Out of treatment
No of deathsperson years
375 (303 to 459)151 (61 to 311)77 (43 to 127)96 (66 to 135)
mdash44 (25 to 73)
114 (58 to 224)
51 (47 to 55)49 (31 to 74)63 (54 to 74)68 (63 to 74)
mdash52 (42 to 63)58 (50 to 67)
124 (03 to 692)43 (20 to 82)
45 (12 to 168)
91 (33 to 198)39 (31 to 49)45 (32 to 62)
In treatment
200 (142 to 275)438 (271 to 670)576 (489 to 675)191 (133 to 265)
mdash373 (271 to 500)321 (191 to 539)
142 (135 to 149)131 (97 to 173)
153 (141 to 164)122 (111 to 132)
mdash107 (80 to 139)
135 (119 to 153)
800 (322 to 1648)167 (111 to 242)320 (132 to 775)
45 (09 to 132)97 (86 to 109)
109 (85 to 139)
Out of treatment
All cause mortality rate1000 person years (95 CI)
All cause mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 4 | all cause mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled all cause mortality rates 2009-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except Degenhardt et al6 which reported mortality before and after two weeks of treatment initiation and cessation high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-analysis area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled all cause mortality rates before and after four weeks in and out of treatment across methadone or buprenorphine cohorts estimated from multivariate random effects meta-analysis on log transformed rates in four time-by-treatment intervals
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
11
drug use comorbidities prison history overdose his-tory patientrsquos preference) characteristics of treatment (such as previous treatment specialisation of the doc-tor who controls the treatment dose provision charac-teristics cointerventions retention or drop outs) or the sociopolitical context in which studies have been conducted For example the initial prognosis might be better in those given buprenorphine than those given methadone (that is fewer comorbid problems less severe opioid dependence)6 8 10 61 though this was not clearly found in a recent US study62
The role of such confounding factors has received almost empirical examination Few details on char-acteristics of patients or treatments were reported in articles included in this meta-analysis to permit a detailed examination of this potential issue (tables 1 and 2 ) so it was not possible to assess the possibil-ity of confounding A sensitivity simulation analysis in the study by Kimber and colleagues however suggested that the lower mortality with buprenor-phine than with methadone during first four weeks of treatment was unlikely to be caused by unmea-sured confounding10
strengths and limitationsThis meta-analysis synthesised evidence from cohort studies published until 2016 on risk of mortality in people who are dependent on opioids during and after opioid substitution treatment separately for buprenor-phine and methadone Mortality changes over time (1st-32th week) during and after methadone are care-fully quantified for the first time
The published studies however had several methodological shortcomings Firstly in the included
Methadone rst four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallMethadone aer four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Kimber et al 2015Buprenorphine aer four weeks Kimber et al 2015
21 505 10 20
9150018334443371
3317 20015188 4495019 277
22094
2919 842
In treatment
2130010183681181
24960020643 430
165067
181674
12529 565
Out of treatment
No of deathsperson years
60 (27 to 114)54 (32 to 85)12 (03 to 30)35 (13 to 95)
19 (13 to 27)17 (14 to 20)26 (19 to 34)20 (15 to 27)
09 (01 to 34)
15 (10 to 21)
In treatment
15 (02 to 56)54 (26 to 100)68 (29 to 134)42 (18 to 99)
25 (16 to 37)47 (41 to 54)32 (18 to 51)34 (23 to 51)
108 (64 to 170)
42 (35 to 50)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 6 | Overdose mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled overdose mortality rates 2002-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except buster et al7 which reported mortality before and after two weeks of treatment initiation and cessation area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates before and after four weeks in and out of treatment across methadone cohorts estimated from multivariate random-effects meta-analysis on log transformed rates in four time-by-treatment intervals
Time since treatment initiation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s In methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Time since treatment cessation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s Out of methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Degenhardt et al 2009Cornish et al 2010Evans et al 2015Kimber et al 2015Cousins et al 2016
Fig 5 | all cause mortality rates by time since treatment initiation and cessation in methadone cohorts and pooled all cause mortality risk trends 2009-16 high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-regression area of each circle is proportional to weight of each time interval in meta-regression Pooled trends in all cause mortality risk (solid lines) and their 95 confidence intervals (shaded regions) over time in and out of methadone treatment were estimated from bivariate random effects meta-regression of log transformed rates on quadratic linear spline function of log time with knot at four weeks
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
12
observational studies the same patients are compared throughout follow-up periods in and out of opioid sub-stitution treatment but these patients leave and re-en-ter treatment in a non-random way and hence there could still be a large potential for confounding in com-parisons of crude mortality risk in and out of treat-ment In some studies with diverse information on patient demographics severity of drug use and comor-bidities measured mostly at baseline (table 3 ) adjust-ment for these potential confounders resulted in similar or even increased out-to-in mortality rate ratios which merely reflects that the above conditions tended to be less prevalent at baseline among patients who later left or were discharged from treatment than those who remained in treatment Nevertheless to obtain an unbiased estimate of the preventive effect of opioid substitution treatment on all cause and overdose mor-tality these and other relevant confounders should be measured every time a patient leaves and resumes treatment Time varying data can then be used to adjust for confounder history in standard regression models or even better to construct inverse probability of treatment weights for marginal structural models63 which properly control for time varying confounders for later treatment that are themselves affected by pre-vious treatment such as severity of drug use and comorbidity Also differential loss to follow-up is a concern in the meta-analysed cohorts as dropouts are more likely to occur in patients at higher risk of death during periods out of treatment thus inducing a selec-tion bias in crude comparisons of out-to-in mortality risk because of informative censoring Marginal struc-tural models with inverse probability of censoring weights can also be used to correct for differential loss to follow-up63 provided that common predictors of death and censoring are measured over time In sum-mary individual cohorts are prone to confounding and selection bias because of differential loss to follow-up but it is hard to assess with the available information the amount and direction of bias projected onto the pooled mortality rate differences and rate ratios between periods in and out of treatment obtained in this meta-analysis
Secondly studies were conducted in high income countries with the follow-up often spread over many calendar years (1965-2010 for methadone and 1990-2010 for buprenorphine) and a highly variable average length of follow-up (ranges 13-158 years and 11-45 years respectively) Studies in low and middle income countries are especially needed
Thirdly by design we have not captured overdose mortality when opioid substitution treatment was obtained on illicit drug markets40 64 Fourthly a delayed record of treatment cessation could have led to some deaths that occurred out of treatment being incorrectly classified as occurring in treatment40 if so this makes our estimated impact of opioid substitution treatment on mortality a conservative one There could similarly be misclassification between overdose and non-over-dose deaths because of inconsistencies in definition of overdose and codification of causes of deaths (for
instance criteria for separating overdose death from intentional poisoning or sudden cardiac death)40 65 again these misclassifications would tend to underesti-mate deaths from overdose
implications for policy and practiceIn many countries the number of deaths attributable to opioid use is substantial66 67 and increasing in some such as the US where deaths from opioid overdose now outnumber gun related deaths in the country68 Over-doses are preventable causes of death warranting wide implementation of preventive interventions Our review has provided evidence that methadone and probably buprenorphine reduce mortality among people depen-dent on opioids making it imperative that further research confirms this using study designs that con-sider a wide range of confounding variables to increase confidence that these effects are causal
It must be borne in mind that there is strong evidence of the efficacy of methadone and buprenorphine on a range of clinical outcomes and these medicines are listed as WHO essential medicines the findings we have presented here provide additional imperatives for their widespread availability Despite this coverage of opioid substitution treatment is low in many countries worldwide69 Policymakers clinicians and those responsible for drug treatment systems should work to ensure the availability of such treatment remove access barriers and promote engagement This means the strategic development of services from a public health perspective which could reduce the social harm associ-ated with opioid use
Our review suggests that some precautions should be taken during and after opioid substitution treatment to increase safety Firstly careful clinical assessment of opioid tolerance before onset of treatment to establish a safe induction dose seems warranted Secondly moni-toring during the induction period is important espe-cially for methadone with clinicians considering adjusting opioid doses monitoring mental and somatic problems and preventing the use of opioids obtained on the illicit drug market64 In addition education of patients about the risk of overdose risk and use of ldquotake homerdquo naloxone70 71 is warranted Buprenorphine induction followed by transition to methadone might also be considered10 72 Retention in opioid substitution treatment reduces risk of exposure to mortality after cessation and also to re-exposure to mortality risk during induction onto methadone so efforts to improve retention are important as a strategy to reduce mortal-ity More generally establishment of mechanisms for information and coordination between healthcare social and legal services and patient counselling while in treatment in addition to more specific overdose pre-vention programmes such as naloxone distribution should be considered
Finally there is a pressing need for new studies on the comparative effectiveness of methadone and buprenorphine in reducing mortality New ran-domised controlled trials are highly unlikely they would be prohibitively expensive and difficult to
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score

thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
11
drug use comorbidities prison history overdose his-tory patientrsquos preference) characteristics of treatment (such as previous treatment specialisation of the doc-tor who controls the treatment dose provision charac-teristics cointerventions retention or drop outs) or the sociopolitical context in which studies have been conducted For example the initial prognosis might be better in those given buprenorphine than those given methadone (that is fewer comorbid problems less severe opioid dependence)6 8 10 61 though this was not clearly found in a recent US study62
The role of such confounding factors has received almost empirical examination Few details on char-acteristics of patients or treatments were reported in articles included in this meta-analysis to permit a detailed examination of this potential issue (tables 1 and 2 ) so it was not possible to assess the possibil-ity of confounding A sensitivity simulation analysis in the study by Kimber and colleagues however suggested that the lower mortality with buprenor-phine than with methadone during first four weeks of treatment was unlikely to be caused by unmea-sured confounding10
strengths and limitationsThis meta-analysis synthesised evidence from cohort studies published until 2016 on risk of mortality in people who are dependent on opioids during and after opioid substitution treatment separately for buprenor-phine and methadone Mortality changes over time (1st-32th week) during and after methadone are care-fully quantified for the first time
The published studies however had several methodological shortcomings Firstly in the included
Methadone rst four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallMethadone aer four weeks Buster et al 2002 Kimber et al 2015 Cousins et al 2016OverallBuprenorphine rst four weeks Kimber et al 2015Buprenorphine aer four weeks Kimber et al 2015
21 505 10 20
9150018334443371
3317 20015188 4495019 277
22094
2919 842
In treatment
2130010183681181
24960020643 430
165067
181674
12529 565
Out of treatment
No of deathsperson years
60 (27 to 114)54 (32 to 85)12 (03 to 30)35 (13 to 95)
19 (13 to 27)17 (14 to 20)26 (19 to 34)20 (15 to 27)
09 (01 to 34)
15 (10 to 21)
In treatment
15 (02 to 56)54 (26 to 100)68 (29 to 134)42 (18 to 99)
25 (16 to 37)47 (41 to 54)32 (18 to 51)34 (23 to 51)
108 (64 to 170)
42 (35 to 50)
Out of treatment
Overdose mortality rate1000 person years (95 CI)
Overdose mortality rate1000 person years (95 CI)
In treatment Out of treatment
Fig 6 | Overdose mortality rates by time interval in and out of opioid substitution treatment with methadone or buprenorphine and pooled overdose mortality rates 2002-16 Mortality data were disaggregated into first four weeks and remaining follow-up in and out of treatment in all cohort studies except buster et al7 which reported mortality before and after two weeks of treatment initiation and cessation area of each square is proportional to study weight in meta-analysis horizontal lines represent exact 95 confidence intervals based on Poisson distribution Diamonds represent pooled overdose mortality rates before and after four weeks in and out of treatment across methadone cohorts estimated from multivariate random-effects meta-analysis on log transformed rates in four time-by-treatment intervals
Time since treatment initiation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s In methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Time since treatment cessation (weeks)
All c
ause
mor
talit
y ra
te
1000
per
son
year
s Out of methadone treatment
05 1 2 4 8 16 32
5
10
20
50
100
Degenhardt et al 2009Cornish et al 2010Evans et al 2015Kimber et al 2015Cousins et al 2016
Fig 5 | all cause mortality rates by time since treatment initiation and cessation in methadone cohorts and pooled all cause mortality risk trends 2009-16 high risk cohort of nosyk et al36 (injectors positive for hiv receiving highly active antiretroviral therapy) was excluded from meta-regression area of each circle is proportional to weight of each time interval in meta-regression Pooled trends in all cause mortality risk (solid lines) and their 95 confidence intervals (shaded regions) over time in and out of methadone treatment were estimated from bivariate random effects meta-regression of log transformed rates on quadratic linear spline function of log time with knot at four weeks
doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
12
observational studies the same patients are compared throughout follow-up periods in and out of opioid sub-stitution treatment but these patients leave and re-en-ter treatment in a non-random way and hence there could still be a large potential for confounding in com-parisons of crude mortality risk in and out of treat-ment In some studies with diverse information on patient demographics severity of drug use and comor-bidities measured mostly at baseline (table 3 ) adjust-ment for these potential confounders resulted in similar or even increased out-to-in mortality rate ratios which merely reflects that the above conditions tended to be less prevalent at baseline among patients who later left or were discharged from treatment than those who remained in treatment Nevertheless to obtain an unbiased estimate of the preventive effect of opioid substitution treatment on all cause and overdose mor-tality these and other relevant confounders should be measured every time a patient leaves and resumes treatment Time varying data can then be used to adjust for confounder history in standard regression models or even better to construct inverse probability of treatment weights for marginal structural models63 which properly control for time varying confounders for later treatment that are themselves affected by pre-vious treatment such as severity of drug use and comorbidity Also differential loss to follow-up is a concern in the meta-analysed cohorts as dropouts are more likely to occur in patients at higher risk of death during periods out of treatment thus inducing a selec-tion bias in crude comparisons of out-to-in mortality risk because of informative censoring Marginal struc-tural models with inverse probability of censoring weights can also be used to correct for differential loss to follow-up63 provided that common predictors of death and censoring are measured over time In sum-mary individual cohorts are prone to confounding and selection bias because of differential loss to follow-up but it is hard to assess with the available information the amount and direction of bias projected onto the pooled mortality rate differences and rate ratios between periods in and out of treatment obtained in this meta-analysis
Secondly studies were conducted in high income countries with the follow-up often spread over many calendar years (1965-2010 for methadone and 1990-2010 for buprenorphine) and a highly variable average length of follow-up (ranges 13-158 years and 11-45 years respectively) Studies in low and middle income countries are especially needed
Thirdly by design we have not captured overdose mortality when opioid substitution treatment was obtained on illicit drug markets40 64 Fourthly a delayed record of treatment cessation could have led to some deaths that occurred out of treatment being incorrectly classified as occurring in treatment40 if so this makes our estimated impact of opioid substitution treatment on mortality a conservative one There could similarly be misclassification between overdose and non-over-dose deaths because of inconsistencies in definition of overdose and codification of causes of deaths (for
instance criteria for separating overdose death from intentional poisoning or sudden cardiac death)40 65 again these misclassifications would tend to underesti-mate deaths from overdose
implications for policy and practiceIn many countries the number of deaths attributable to opioid use is substantial66 67 and increasing in some such as the US where deaths from opioid overdose now outnumber gun related deaths in the country68 Over-doses are preventable causes of death warranting wide implementation of preventive interventions Our review has provided evidence that methadone and probably buprenorphine reduce mortality among people depen-dent on opioids making it imperative that further research confirms this using study designs that con-sider a wide range of confounding variables to increase confidence that these effects are causal
It must be borne in mind that there is strong evidence of the efficacy of methadone and buprenorphine on a range of clinical outcomes and these medicines are listed as WHO essential medicines the findings we have presented here provide additional imperatives for their widespread availability Despite this coverage of opioid substitution treatment is low in many countries worldwide69 Policymakers clinicians and those responsible for drug treatment systems should work to ensure the availability of such treatment remove access barriers and promote engagement This means the strategic development of services from a public health perspective which could reduce the social harm associ-ated with opioid use
Our review suggests that some precautions should be taken during and after opioid substitution treatment to increase safety Firstly careful clinical assessment of opioid tolerance before onset of treatment to establish a safe induction dose seems warranted Secondly moni-toring during the induction period is important espe-cially for methadone with clinicians considering adjusting opioid doses monitoring mental and somatic problems and preventing the use of opioids obtained on the illicit drug market64 In addition education of patients about the risk of overdose risk and use of ldquotake homerdquo naloxone70 71 is warranted Buprenorphine induction followed by transition to methadone might also be considered10 72 Retention in opioid substitution treatment reduces risk of exposure to mortality after cessation and also to re-exposure to mortality risk during induction onto methadone so efforts to improve retention are important as a strategy to reduce mortal-ity More generally establishment of mechanisms for information and coordination between healthcare social and legal services and patient counselling while in treatment in addition to more specific overdose pre-vention programmes such as naloxone distribution should be considered
Finally there is a pressing need for new studies on the comparative effectiveness of methadone and buprenorphine in reducing mortality New ran-domised controlled trials are highly unlikely they would be prohibitively expensive and difficult to
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score

doi 101136bmjj1550 | BMJ 2017357j1550 | thethinspbmj
RESEARCH
12
observational studies the same patients are compared throughout follow-up periods in and out of opioid sub-stitution treatment but these patients leave and re-en-ter treatment in a non-random way and hence there could still be a large potential for confounding in com-parisons of crude mortality risk in and out of treat-ment In some studies with diverse information on patient demographics severity of drug use and comor-bidities measured mostly at baseline (table 3 ) adjust-ment for these potential confounders resulted in similar or even increased out-to-in mortality rate ratios which merely reflects that the above conditions tended to be less prevalent at baseline among patients who later left or were discharged from treatment than those who remained in treatment Nevertheless to obtain an unbiased estimate of the preventive effect of opioid substitution treatment on all cause and overdose mor-tality these and other relevant confounders should be measured every time a patient leaves and resumes treatment Time varying data can then be used to adjust for confounder history in standard regression models or even better to construct inverse probability of treatment weights for marginal structural models63 which properly control for time varying confounders for later treatment that are themselves affected by pre-vious treatment such as severity of drug use and comorbidity Also differential loss to follow-up is a concern in the meta-analysed cohorts as dropouts are more likely to occur in patients at higher risk of death during periods out of treatment thus inducing a selec-tion bias in crude comparisons of out-to-in mortality risk because of informative censoring Marginal struc-tural models with inverse probability of censoring weights can also be used to correct for differential loss to follow-up63 provided that common predictors of death and censoring are measured over time In sum-mary individual cohorts are prone to confounding and selection bias because of differential loss to follow-up but it is hard to assess with the available information the amount and direction of bias projected onto the pooled mortality rate differences and rate ratios between periods in and out of treatment obtained in this meta-analysis
Secondly studies were conducted in high income countries with the follow-up often spread over many calendar years (1965-2010 for methadone and 1990-2010 for buprenorphine) and a highly variable average length of follow-up (ranges 13-158 years and 11-45 years respectively) Studies in low and middle income countries are especially needed
Thirdly by design we have not captured overdose mortality when opioid substitution treatment was obtained on illicit drug markets40 64 Fourthly a delayed record of treatment cessation could have led to some deaths that occurred out of treatment being incorrectly classified as occurring in treatment40 if so this makes our estimated impact of opioid substitution treatment on mortality a conservative one There could similarly be misclassification between overdose and non-over-dose deaths because of inconsistencies in definition of overdose and codification of causes of deaths (for
instance criteria for separating overdose death from intentional poisoning or sudden cardiac death)40 65 again these misclassifications would tend to underesti-mate deaths from overdose
implications for policy and practiceIn many countries the number of deaths attributable to opioid use is substantial66 67 and increasing in some such as the US where deaths from opioid overdose now outnumber gun related deaths in the country68 Over-doses are preventable causes of death warranting wide implementation of preventive interventions Our review has provided evidence that methadone and probably buprenorphine reduce mortality among people depen-dent on opioids making it imperative that further research confirms this using study designs that con-sider a wide range of confounding variables to increase confidence that these effects are causal
It must be borne in mind that there is strong evidence of the efficacy of methadone and buprenorphine on a range of clinical outcomes and these medicines are listed as WHO essential medicines the findings we have presented here provide additional imperatives for their widespread availability Despite this coverage of opioid substitution treatment is low in many countries worldwide69 Policymakers clinicians and those responsible for drug treatment systems should work to ensure the availability of such treatment remove access barriers and promote engagement This means the strategic development of services from a public health perspective which could reduce the social harm associ-ated with opioid use
Our review suggests that some precautions should be taken during and after opioid substitution treatment to increase safety Firstly careful clinical assessment of opioid tolerance before onset of treatment to establish a safe induction dose seems warranted Secondly moni-toring during the induction period is important espe-cially for methadone with clinicians considering adjusting opioid doses monitoring mental and somatic problems and preventing the use of opioids obtained on the illicit drug market64 In addition education of patients about the risk of overdose risk and use of ldquotake homerdquo naloxone70 71 is warranted Buprenorphine induction followed by transition to methadone might also be considered10 72 Retention in opioid substitution treatment reduces risk of exposure to mortality after cessation and also to re-exposure to mortality risk during induction onto methadone so efforts to improve retention are important as a strategy to reduce mortal-ity More generally establishment of mechanisms for information and coordination between healthcare social and legal services and patient counselling while in treatment in addition to more specific overdose pre-vention programmes such as naloxone distribution should be considered
Finally there is a pressing need for new studies on the comparative effectiveness of methadone and buprenorphine in reducing mortality New ran-domised controlled trials are highly unlikely they would be prohibitively expensive and difficult to
thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score

thethinspbmj | BMJ 2017357j1550 | doi 101136bmjj1550
RESEARCH
13
implement A more pragmatic solution is to conduct cohort studies in multiple countries including both methadone and buprenorphine patients with hetero-geneous characteristics and sufficient information on potential confounders These studies could focus on the relation between time in treatment and risks after interruption of treatment to identify a minimum requirement for treatment duration to observe reduc-tions in mortality riskContributors LS GB MJB BII MF and RP-B were involved in the conception and design of the review LS GB and BII developed the search strategy and performed study selection LS and RP-B extracted data from included studies LS GB and RP-B were involved in the data analysis LS GB MJB LD LW MF and RP-B were involved in the interpretation and discussion of results LS GB MJB and RP-B drafted the manuscript and BII LD LW and MF contributed to the drafting of the review All authors approved the final version of the article RP-B is the guarantorFunding This work was partially supported by the ISCIII Network on Addictive Disorders (Networks for Cooperative Research in Health from the Carlos III Institute of Health) (grant No RD1600170013 and RD1200280018) and by the EMCDDA in the context of the activities related to identification promotion and monitor of best practicesCompeting interests All authors have completed the ICMJE uniform disclosure form at httpwwwicmjeorgcoi_disclosurepdf and declare LD has received grants from Reckitt BenckiserIndivior and grants from Mundipharma outside the submitted work No further support from any organisation for the submitted work no other financial relationships with any organisation that might have an interest in the submitted work in the previous three years no other relationships or activities that could appear to have influenced the submitted workEthical approval Not requiredTransparency The lead author affirms that the manuscript is an honest accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been disclosedData sharing No additional data availableThis is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 40) license which permits others to distribute remix adapt build upon this work non-commercially and license their derivative works on different terms provided the original work is properly cited and the use is non-commercial See httpcreativecommonsorglicensesby-nc401 Degenhardt L Charlson F Mathers B et al The global
epidemiology and burden of opioid dependence results from the global burden of disease 2010 study Addiction 20141091320-33 doi101111add12551
2 Mattick RP Breen C Kimber J Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev 2009(3)CD002209
3 Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev 20142CD002207
4 Lawrinson P Ali R Buavirat A et al Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIVAIDS Addiction 20081031484-92 doi101111j1360-0443200802249x
5 Ward J Hall W Mattick RP Role of maintenance treatment in opioid dependence Lancet 1999353221-6 doi101016S0140-6736(98)05356-2
6 Degenhardt L Randall D Hall W Law M Butler T Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years risk factors and lives saved Drug Alcohol Depend 20091059-15 doi101016jdrugalcdep200905021
7 Buster MC van Brussel GH van den Brink W An increase in overdose mortality during the first 2 weeks after entering or re-entering methadone treatment in Amsterdam Addiction 200297993-1001 doi101046j1360-0443200200179x
8 Cornish R Macleod J Strang J Vickerman P Hickman M Risk of death during and after opiate substitution treatment in primary care prospective observational study in UK General Practice Research Database BMJ 2010341c5475 doi101136bmjc5475
9 Evans E Li L Min J et al Mortality among individuals accessing pharmacological treatment for opioid dependence in California 2006-10 Addiction 2015110996-1005 doi101111add12863
10 Kimber J Larney S Hickman M Randall D Degenhardt L Mortality risk of opioid substitution therapy with methadone versus buprenorphine a retrospective cohort study Lancet Psychiatry 20152901-8 doi101016S2215-0366(15)00366-1
11 Degenhardt L Bucello C Mathers B et al Mortality among regular or dependent users of heroin and other opioids a systematic review and meta-analysis of cohort studies Addiction 201110632-51 doi101111j1360-0443201003140x
12 Hickman M Macleod J Degenhardt L Commentary on Cousins et al (2016) Accumulating evidence on risk of mortality on and off opioid substitution treatment Addiction 201611183-4 doi101111add13185
13 Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement BMJ 2009339b2535 doi101136bmjb2535
14 Scottish Intercollegiate Guidelines Network (SIGN) SIGN 50 a guidelines developersrsquo handbook 2014 Edinburgh Scottish Intercollegiate Guidelines Network (SIGN)
15 Degenhardt L Calabria B Nelson P et al and Global Burden of Disease Mental Disorders and Illicit Drug Use Expert group Methodology used in a systematic review of evidence on the prevalence of amphetamine use and dependence 2009 Sydney National Drug and Alcohol Research Centre University of NSW Illicit drugs discussion paper No13
16 Wells G Shea B OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses In 3rd Symposium on Systematic Reviews Beyondthe Basics Improving Quality and Impact Oxford UK 2013
17 Berkey CS Hoaglin DC Antczak-Bouckoms A Mosteller F Colditz GA Meta-analysis of multiple outcomes by regression with random effects Stat Med 1998172537-50 doi101002(SICI)1097-0258(19981130)1722lt2537AID-SIM953gt30CO2-C
18 Gasparrini A Armstrong B Kenward MG Multivariate meta-analysis for non-linear and other multi-parameter associations Stat Med 2012313821-39 doi101002sim5471
19 Jackson D Riley R White IR Multivariate meta-analysis potential and promise Stat Med 2011302481-98 doi101002sim4247
20 Greenland S Dose-response and trend analysis in epidemiology alternatives to categorical analysis Epidemiology 19956356-65 doi10109700001648-199507000-00005
21 Jackson D White IR Riley RD Quantifying the impact of between-study heterogeneity in multivariate meta-analyses Stat Med 2012313805-20 doi101002sim5453
22 Egger M Davey Smith G Schneider M Minder C Bias in meta-analysis detected by a simple graphical test BMJ 1997315629-34 doi101136bmj3157109629
23 Thompson SG Sharp SJ Explaining heterogeneity in meta-analysis a comparison of methods Stat Med 1999182693-708 doi101002(SICI)1097-0258(19991030)1820lt2693AID-SIM235gt30CO2-V
24 Gearing FR Schweitzer MD An epidemiologic evaluation of long-term methadone maintenance treatment for heroin addiction Am J Epidemiol 1974100101-12 doi101093oxfordjournalsajea112012
25 Cushman P Jr Ten years of methadone maintenance treatment some clinical observations Am J Drug Alcohol Abuse 19774543-53 doi10310900952997709007010
26 Groumlnbladh L Ohlund LS Gunne LM Mortality in heroin addiction impact of methadone treatment Acta Psychiatr Scand 199082223-7 doi101111j1600-04471990tb03057x
27 Caplehorn JR Dalton MS Cluff MC Petrenas AM Retention in methadone maintenance and heroin addictsrsquo risk of death Addiction 199489203-9 doi101111j1360-04431994tb00879x
28 Caplehorn JR Dalton MS Haldar F Petrenas AM Nisbet JG Methadone maintenance and addictsrsquo risk of fatal heroin overdose Subst Use Misuse 199631177-96 doi10310910826089609045806
29 Fugelstad A Rajs J Boumlttiger M Gerhardsson de Verdier M Mortality among HIV-infected intravenous drug addicts in Stockholm in relation to methadone treatment Addiction 199590711-6 doi101111j1360-04431995tb02209x
30 Fugelstad A Agren G Romelsjouml A Changes in mortality arrests and hospitalizations in nonvoluntarily treated heroin addicts in relation to methadone treatment Subst Use Misuse 1998332803-17 doi10310910826089809059352
31 Scherbaum N Specka M Hauptmann G Gastpar M [Does maintenance treatment reduce the mortality rate of opioid addicts] Fortschr Neurol Psychiatr 200270455-61 doi101055s-2002-33758
32 Davoli M Bargagli AM Perucci CA et al VEdeTTE Study Group Risk of fatal overdose during and after specialist drug treatment the VEdeTTE study a national multi-site prospective cohort study Addiction 20071021954-9 doi101111j1360-0443200702025x
33 Fugelstad A Stenbacka M Leifman A Nylander M Thiblin I Methadone maintenance treatment the balance between life-saving treatment and fatal poisonings Addiction 2007102406-12 doi101111j1360-0443200601714x
RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score

RESEARCH
No commercial reuse See rights and reprints httpwwwbmjcompermissions Subscribe httpwwwbmjcomsubscribe
34 Clausen T Anchersen K Waal H Mortality prior to during and after opioid maintenance treatment (OMT) a national prospective cross-registry study Drug Alcohol Depend 200894151-7 doi101016jdrugalcdep200711003
35 Peles E Schreiber S Adelson M 15-Year survival and retention of patients in a general hospital-affiliated methadone maintenance treatment (MMT) center in Israel Drug Alcohol Depend 2010107141-8 doi101016jdrugalcdep200909013
36 Nosyk B Min JE Evans E et al The Effects of Opioid Substitution Treatment and Highly Active Antiretroviral Therapy on the Cause-Specific Risk of Mortality Among HIV-Positive People Who Inject Drugs Clin Infect Dis 2015611157-65 doi101093cidciv476
37 Cousins G Boland F Courtney B Barry J Lyons S Fahey T Risk of mortality on and off methadone substitution treatment in primary care a national cohort study Addiction 201611173-82 doi101111add13087
38 Reece AS Favorable mortality profile of naltrexone implants for opiate addiction J Addict Dis 20102930-50 doi10108010550880903435988
39 Auriacombe M Franques P Tignol J Deaths attributable to methadone vs buprenorphine in France JAMA 200128545 doi101001jama285139
40 Bell J Trinh L Butler B Randall D Rubin G Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment Addiction 20091041193-200 doi101111j1360-0443200902627x
41 Kleber HD Pharmacologic treatments for opioid dependence detoxification and maintenance options Dialogues Clin Neurosci 20079455-70
42 Pirnay S Borron SW Giudicelli CP Tourneau J Baud FJ Ricordel I A critical review of the causes of death among post-mortem toxicological investigations analysis of 34 buprenorphine-associated and 35 methadone-associated deaths Addiction 200499978-88 doi101111j1360-0443200400790x
43 Soyka M Apelt SM Lieb M Wittchen HU One-year mortality rates of patients receiving methadone and buprenorphine maintenance therapy a nationally representative cohort study in 2694 patients J Clin Psychopharmacol 200626657-60 doi10109701jcp00002455619903649
44 Thomas CP Fullerton CA Kim M et al Medication-assisted treatment with buprenorphine assessing the evidence Psychiatr Serv 201465158-70 doi101176appips201300256
45 Brugal MT Domingo-Salvany A Puig R Barrio G Garciacutea de Olalla P de la Fuente L Evaluating the impact of methadone maintenance programmes on mortality due to overdose and aids in a cohort of heroin users in Spain Addiction 2005100981-9 doi101111j1360-0443200501089x
46 Bell J Burrell T Indig D Gilmour S Cycling in and out of treatment participation in methadone treatment in NSW 1990-2002 Drug Alcohol Depend 20068155-61 doi101016jdrugalcdep200505010
47 Cousins G Teljeur C Motterlini N McCowan C Dimitrov BD Fahey T Risk of drug-related mortality during periods of transition in methadone maintenance treatment a cohort study J Subst Abuse Treat 201141252-60 doi101016jjsat201105001
48 Hser YI Evans E Grella C Ling W Anglin D Long-term course of opioid addiction Harv Rev Psychiatry 20152376-89 doi101097HRP0000000000000052
49 Nordt C Vogel M Duumlrsteler KM Stohler R Herdener M A comprehensive model of treatment participation in chronic disease allowed prediction of opioid substitution treatment participation in Zurich 1992-2012 J Clin Epidemiol 2015681346-54 doi101016jjclinepi201505002
50 Teesson M Marel C Darke S et al Long-term mortality remission criminality and psychiatric comorbidity of heroin dependence 11-year findings from the Australian Treatment Outcome Study Addiction 2015110986-93 doi101111add12860
51 Eap CB Buclin T Baumann P Interindividual variability of the clinical pharmacokinetics of methadone implications for the treatment of opioid dependence Clin Pharmacokinet 2002411153-93 doi10216500003088-200241140-00003
52 Jolley CJ Bell J Rafferty GF Moxham J Strang J Understanding heroin overdose a study of the acute respiratory depressant effects of injected pharmaceutical heroin PLoS One 201510e0140995 doi101371journalpone0140995
53 McCowan C Kidd B Fahey T Factors associated with mortality in Scottish patients receiving methadone in primary care retrospective cohort study BMJ 2009338b2225 doi101136bmjb2225
54 Yokell MA Zaller ND Green TC Rich JD Buprenorphine and buprenorphinenaloxone diversion misuse and illicit use an international review Curr Drug Abuse Rev 2011428-41 doi1021741874473711104010028
55 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Mortality realted to drug use in Europe Public Health Implications EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union Selected Issues 2011
56 White JM Irvine RJ Mechanisms of fatal opioid overdose Addiction 199994961-72 doi101046j1360-044319999479612x
57 Binswanger IA Blatchford PJ Mueller SR Stern MF Mortality after prison release opioid overdose and other causes of death risk factors and time trends from 1999 to 2009 Ann Intern Med 2013159592-600 doi1073260003-4819-159-9-201311050-00005
58 Merrall EL Kariminia A Binswanger IA et al Meta-analysis of drug-related deaths soon after release from prison Addiction 20101051545-54 doi101111j1360-0443201002990x
59 Merrall EL Bird SM Hutchinson SJ A record-linkage study of drug-related death and suicide after hospital discharge among drug-treatment clients in Scotland 1996-2006 Addiction 2013108377-84 doi101111j1360-0443201204066x
60 Bell JR Butler B Lawrance A Batey R Salmelainen P Comparing overdose mortality associated with methadone and buprenorphine treatment Drug Alcohol Depend 200910473-7 doi101016jdrugalcdep200903020
61 Brogly SB Saia KA Walley AY Du HM Sebastiani P Prenatal buprenorphine versus methadone exposure and neonatal outcomes systematic review and meta-analysis Am J Epidemiol 2014180673-86 doi101093ajekwu190
62 Manhapra A Quinones L Rosenheck R Characteristics of veterans receiving buprenorphine vs methadone for opioid use disorder nationally in the Veterans Health Administration Drug Alcohol Depend 201616082-9 doi101016jdrugalcdep201512035
63 Robins JM Hernaacuten MA Brumback B Marginal structural models and causal inference in epidemiology Epidemiology 200011550-60 doi10109700001648-200009000-00011
64 Rhodes T Hedrich D Strategies to prevent diversion of opioid substitution treatment medicationsEuropean Monitoring Centre for Drugs and Drug Addiction 2016
65 Gossop M Stewart D Treacy S Marsden J A prospective study of mortality among drug misusers during a 4-year period after seeking treatment Addiction 20029739-47 doi101046j1360-0443200200079x
66 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2015 Trends and developments EMCDDA (European Monitoring Centre for Drugs and Drug Addiction)Publications Office of the European Union EMCDDA Papers 2015
67 United Nations Office on Drugs and Crime World Drug Report 2015 2015 United Nations publication Sales No E 14XI7
68 Rudd RA Seth P David F Scholl L Increases in Drug and Opioid-Involved Overdose Deaths - United States 2010-2015 MMWR Morb Mortal Wkly Rep 2016651445-52 doi1015585mmwrmm655051e1
69 Mathers BM Degenhardt L Ali H et al 2009 Reference Group to the UN on HIV and Injecting Drug Use HIV prevention treatment and care services for people who inject drugs a systematic review of global regional and national coverage Lancet 20103751014-28 doi101016S0140-6736(10)60232-2
70 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Preventing overdose deaths in Europe 2015 Lisbon European Monitoring Centre for Drugs and Drug Addiction (EMCDDA)
71 Zador D Sunjic S Deaths in methadone maintenance treatment in New South Wales Australia 1990-1995 Addiction 20009577-84 doi101046j1360-04432000951778x
72 Kakko J Groumlnbladh L Svanborg KD et al A stepped care strategy using buprenorphine and methadone versus conventional methadone maintenance in heroin dependence a randomized controlled trial Am J Psychiatry 2007164797-803 doi101176ajp20071645797
Appendix 1 SearchesAppendix 2 Supplementary tables A and BAppendix 3 Quality score