Embed Size (px)
Citation preview

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Bioterrorism Bioterrorism PreparednessPreparedness
European Masters in Disaster European Masters in Disaster Medicine Medicine
Arona, ItalyArona, Italy27 April 200427 April 2004
Eric K. Noji, MD, MPHDepartment of Homeland Security
Washington, D.C.

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
““A bioterrorism attack anywhere in the A bioterrorism attack anywhere in the
world is inevitable in the 21world is inevitable in the 21stst century.” century.”
Anthony Fauci, Director, NIAIDAnthony Fauci, Director, NIAID
Clinical Infectious Diseases 2001;32:678Clinical Infectious Diseases 2001;32:678

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Increasing Global TravelIncreasing Global Travel Rapid access to large Rapid access to large
populationspopulations Poor global security & Poor global security &
awarenessawareness
...create the potential for simultaneous ...create the potential for simultaneous creation of large numbers of casualtiescreation of large numbers of casualties
ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
• Limited prior experience in CBRN type response except for naturally occurring infectious disease outbreaks, for example – Cholera/Lassa fever/Ebola virus.
• Evacuation only strategy.
• Limited numbers of adequately trained staff, equipment, procedural knowledge.
Global Preparedness

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
HistoryHistory CBRN Agents have been CBRN Agents have been
used on unprotected civil used on unprotected civil populations on many populations on many occasionsoccasions
Some of the locations Some of the locations where the local population where the local population had no defense werehad no defense were• EthiopiaEthiopia• IraqIraq• AfghanistanAfghanistan• LaosLaos• JapanJapan
CDCCenters for Disease Control
and Prevention

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
CBRNE AgentsCBRNE AgentsConventional Conventional (Explosive)(Explosive)
ChemicalChemical Biological / Biological / RadoilogicRadoilogic
OnsetOnset InstantInstant RapidRapid Often DelayedOften Delayed
SourceSource ObviousObvious ObviousObvious Often covertOften covert
First Victim First Victim EncounterEncounter
PrehospitalPrehospital PrehospitalPrehospital HospitalHospital
ContainmentContainment EasyEasy Relatively EasyRelatively Easy DifficultDifficult
Decon HelpfulDecon Helpful Usually NotUsually Not YesYes Usually Not*Usually Not*
ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Sources of Agents for Sources of Agents for Terrorism UseTerrorism Use
World Directory of Collections of World Directory of Collections of Cultures and MicroorganismsCultures and Microorganisms• 453 worldwide repositories in 67 nations453 worldwide repositories in 67 nations• 54 ship/sell anthrax54 ship/sell anthrax• 18 ship/sell plague18 ship/sell plague
International black-market sales International black-market sales associated with governmental associated with governmental programsprograms

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
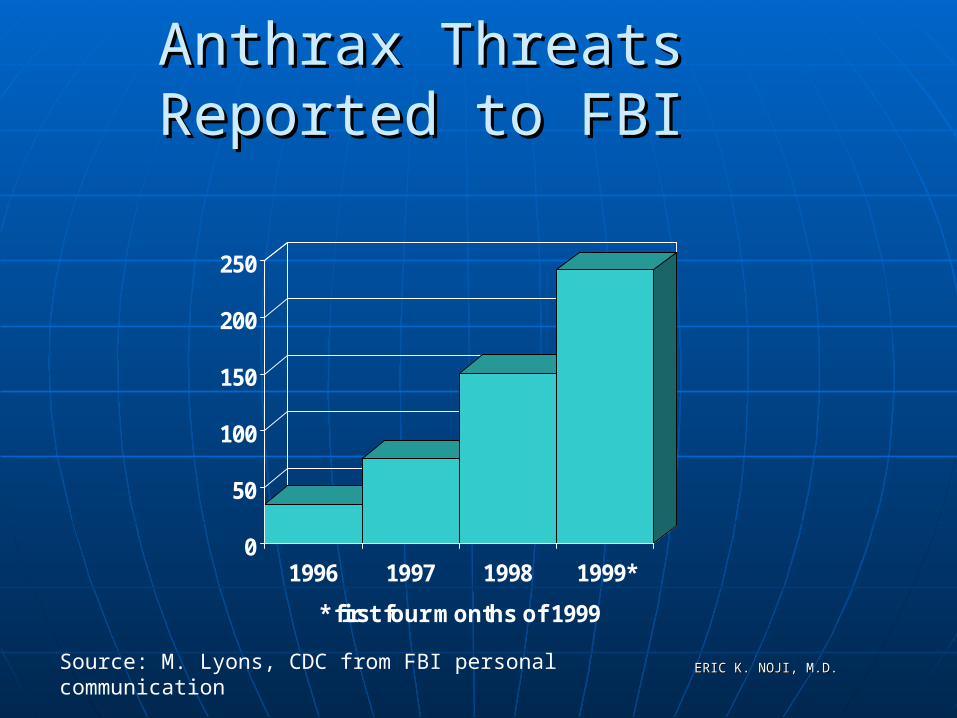
Anthrax Threats Reported to Anthrax Threats Reported to FBIFBI
0
50
100
150
200
250
1996 1997 1998 1999*
* first four months of 1999
Source: M. Lyons, CDC from FBI personal communication

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Biological AgentsBiological Agents• CDC/WHO list of high-likelihood potential bio-terrorist CDC/WHO list of high-likelihood potential bio-terrorist
agentsagents• Prioritized according to: Prioritized according to:
• Ease of disseminationEase of dissemination• TransmissibilityTransmissibility• MortalityMortality• Public health impactPublic health impact• Potential to cause fear and social disruptionPotential to cause fear and social disruption• Need for special preparednessNeed for special preparedness

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Biological AgentsBiological Agents
Category ACategory A• SmallpoxSmallpox• AnthraxAnthrax• PlaguePlague• BotulismBotulism• TularemiaTularemia• Viral Hemorrhagic FeversViral Hemorrhagic Fevers
Ebola, Marburg, Lassa, Argentine HFEbola, Marburg, Lassa, Argentine HF
ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
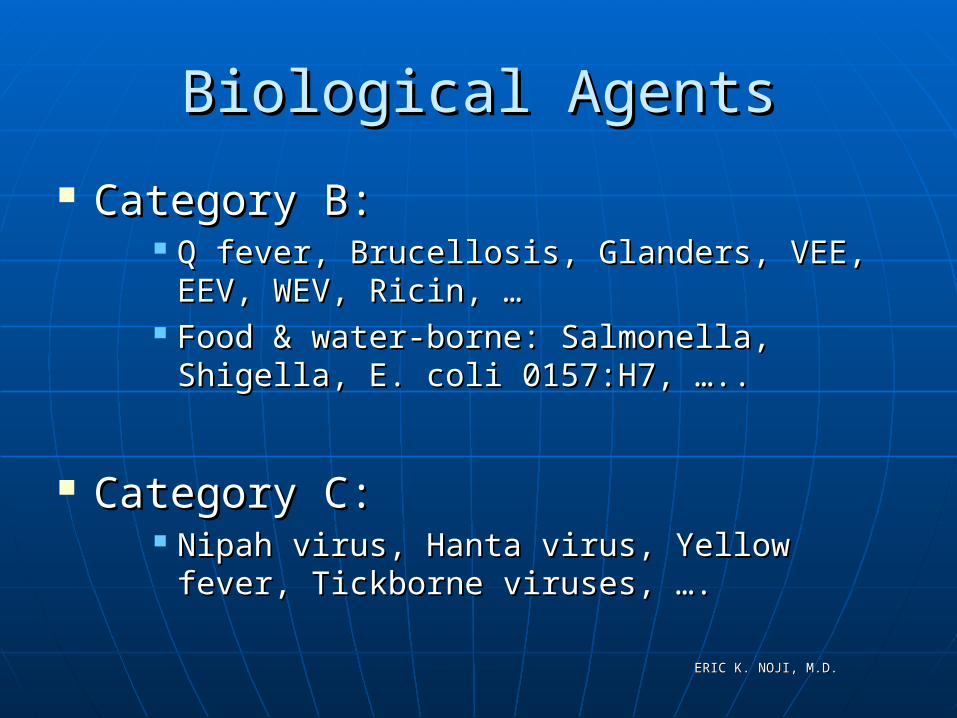
Biological AgentsBiological Agents
Category B:Category B: Q fever, Brucellosis, Glanders, VEE, EEV, Q fever, Brucellosis, Glanders, VEE, EEV,
WEV, Ricin, …WEV, Ricin, … Food & water-borne: Salmonella, Shigella, E. Food & water-borne: Salmonella, Shigella, E.
coli 0157:H7, …..coli 0157:H7, …..
Category C:Category C: Nipah virus, Hanta virus, Yellow fever, Nipah virus, Hanta virus, Yellow fever,
Tickborne viruses, ….Tickborne viruses, ….
ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
DiagnosisDiagnosis
-Diagnosis difficult given diseases have been seen by few living clinicians
-Abnormal presentations of classical diseases may be present due to super infection
-Diagnosis critical for epidemiological monitoring
-Accurate data required for potential future prosecution of war crimes
-Psychogenic overlay may cloud the diagnostic process

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Biological AgentsBiological Agents
Syndrome RecognitionSyndrome Recognition• Most bio-terrorist agents initially induce an Most bio-terrorist agents initially induce an
influenza-like prodrome, including fever, influenza-like prodrome, including fever, chills, myalgias, or malaisechills, myalgias, or malaise
• One of four syndromic patterns then follow:One of four syndromic patterns then follow: Rapidly progressive pneumoniaRapidly progressive pneumonia Fever with rashFever with rash Fever with altered mental statusFever with altered mental status Bloody diarrheaBloody diarrhea

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Small Pox (Variola major virus)Small Pox (Variola major virus)
Transmitted primarily by aerosol Transmitted primarily by aerosol route, contaminated clothes & linensroute, contaminated clothes & linens
Highly communicableHighly communicable Vaccine can lessen the severity of Vaccine can lessen the severity of
disease if given within 4 days of disease if given within 4 days of exposureexposure

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Epidemiological Pattern of Epidemiological Pattern of Smallpox WeaponSmallpox Weapon
New foci of secondary infection
“Contaminated” zone
“Infected” zone
Zone of initialexplosion

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Small PoxSmall Pox
30% case fatality rate if untreated30% case fatality rate if untreated One of four biological agents thought One of four biological agents thought
to be most likely used by terroriststo be most likely used by terrorists Incubation 7-17 daysIncubation 7-17 days Prodrome of high fever, malaise, Prodrome of high fever, malaise,
vomiting, headache, myalgiasvomiting, headache, myalgias 2-3 days later get rash beginning on 2-3 days later get rash beginning on
face, hands, forearms face, hands, forearms

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Small PoxSmall Pox
Patients infectious until all scabs are Patients infectious until all scabs are shedshed
No treatment, but animal studies No treatment, but animal studies show promise for cidofovirshow promise for cidofovir

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Smallpox Infected People Smallpox Infected People DisperseDisperse
Infected board flights to thirty eight US citiesInfected board flights to thirty eight US cities

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Anthrax (bacillus Anthracis)Anthrax (bacillus Anthracis)
Inhalational, gastrointestinal, cutaneousInhalational, gastrointestinal, cutaneous NOTNOT communicable communicable (except maybe cutaneous)(except maybe cutaneous)
Vaccine not available for civilian useVaccine not available for civilian use 20%-80% mortality20%-80% mortality

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Anthrax: InhalationalAnthrax: Inhalational
Inhalation of sporesInhalation of spores Incubation: 1 to 43 days Incubation: 1 to 43 days Initial symptoms (2-5 d) Initial symptoms (2-5 d)
• Fever, cough, myalgia, malaiseFever, cough, myalgia, malaise Terminal symptoms (1-2d )Terminal symptoms (1-2d )
• High fever, dyspnea, cyanosisHigh fever, dyspnea, cyanosis• Hemorrhagic Hemorrhagic
mediastinitis/effusionmediastinitis/effusion• Rapid progression shock/deathRapid progression shock/death
Mortality rate in 1957 ~ Mortality rate in 1957 ~ 100% despite Rx 100% despite Rx CDC

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Anthrax: CutaneousAnthrax: Cutaneous
Most common form Most common form (95%)(95%)
Inoculation of spores Inoculation of spores under skinunder skin
Incubation: hours to 7 Incubation: hours to 7 daysdays
Small papule --> ulcer Small papule --> ulcer surrounded by vesicles surrounded by vesicles (24-28h)(24-28h)
Painless eschar with Painless eschar with edemaedema
Death 20% untreated; Death 20% untreated; rare treated rare treated USAMRICD

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
AnthraxAnthrax
Resistant to heat, UV, drying, many Resistant to heat, UV, drying, many disinfectantsdisinfectants
Incubation 2-6 daysIncubation 2-6 days Biphasic illness Biphasic illness
• nonspecific flu-like symptomsnonspecific flu-like symptoms• High fever, SOB, chest and abdominal High fever, SOB, chest and abdominal
painpain• Sore throat, runny noseSore throat, runny noseNOTNOT associated associated

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
AnthraxAnthrax
Treatment – multi-drug antibioticsTreatment – multi-drug antibiotics Prophylaxis – single drug for 60 daysProphylaxis – single drug for 60 days

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Pneumonic PlaguePneumonic Plague
Caused by infection with Yersinia Caused by infection with Yersinia PestisPestis
Pneumonic form will occur after Pneumonic form will occur after intentional aerosol deliveryintentional aerosol delivery
Incubation period of 1-7 daysIncubation period of 1-7 days

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Pneumonic PlaguePneumonic Plague
Symptoms:Symptoms:• Fever, malaise, fatigue, cough, SOBFever, malaise, fatigue, cough, SOB
Signs:Signs:• Classic finding of production of bloody Classic finding of production of bloody
sputum in a previously healthy patientsputum in a previously healthy patient
Treatment: AntibioticsTreatment: Antibiotics

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Detection & surveillanceDetection & surveillance
Rapid laboratory diagnosisRapid laboratory diagnosis
Epidemiologic investigationsEpidemiologic investigations
Implementation of control Implementation of control measuresmeasures
Public Health ResponsePublic Health Responseto Bioterrorismto Bioterrorism

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Bioterrorism SurveillanceBioterrorism Surveillance
Early, rapid recognition of unusual Early, rapid recognition of unusual clinical syndromes or deathsclinical syndromes or deaths
Early rapid recognition of increase Early rapid recognition of increase above “expected levels” of common above “expected levels” of common syndromes, diseases, or deathsyndromes, diseases, or death

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Clues to Possible Bioterrorism Clues to Possible Bioterrorism II
Single case caused by an uncommon agentSingle case caused by an uncommon agent Large number of ill persons with similar disease, Large number of ill persons with similar disease,
syndrome, or deathssyndrome, or deaths Large number of unexplained disease, syndrome, or Large number of unexplained disease, syndrome, or
deathdeath Unusual illness in a populationUnusual illness in a population Higher morbidity & mortality than expected with a Higher morbidity & mortality than expected with a
common disease or syndromecommon disease or syndrome Multiple disease entities coexisting in the same patientMultiple disease entities coexisting in the same patient Disease with an unusual geographic or seasonal Disease with an unusual geographic or seasonal
distributiondistribution
ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Clues to Possible Bioterrorism II Clues to Possible Bioterrorism II
Multiple atypical presentations of disease agentsMultiple atypical presentations of disease agents Similar genetic type of agent from distinct sourcesSimilar genetic type of agent from distinct sources Unusual, atypical, genetically engineered, or Unusual, atypical, genetically engineered, or
antiquated antiquated strainstrain Endemic disease with unexplained increased Endemic disease with unexplained increased
incidenceincidence Simultaneous clusters of similar illness in con-Simultaneous clusters of similar illness in con-
contiguous areascontiguous areas Atypical aerosol, food, or water transmission Atypical aerosol, food, or water transmission Ill persons presenting during the same timeIll persons presenting during the same time Concurrent animal diseaseConcurrent animal disease

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Bioterrorism: Bioterrorism: Potential Data SourcesPotential Data Sources
LaboratoriesLaboratories Infectious diseaseInfectious disease SpecialistsSpecialists HospitalsHospitals Physician’s officesPhysician’s offices Poison control Poison control
centerscenters
Medical Medical ExaminersExaminers
Death CertificatesDeath Certificates Police/Fire Police/Fire
departmentsdepartments Other “first Other “first
responders”responders” Pharmacy dataPharmacy data

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Syndrome SurveillanceSyndrome Surveillance
• The monitoring of illnesses based upon a The monitoring of illnesses based upon a constellation of symptoms and/or constellation of symptoms and/or findingsfindings
• Provides an “early warning system” for Provides an “early warning system” for outbreaks, emerging pathogensoutbreaks, emerging pathogens
• Highly sensitive, seasonal specificity Highly sensitive, seasonal specificity varies varies

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Examples of Syndromes Examples of Syndromes for Surveillancefor Surveillance
• Unexplained death w/ history of feverUnexplained death w/ history of fever• Meningitis, encephalitis or unexplained acute Meningitis, encephalitis or unexplained acute
encephalopathy/deliriumencephalopathy/delirium• Botulism-like syndrome (cranial nerve impairment Botulism-like syndrome (cranial nerve impairment
and weakness)and weakness)• Rash and feverRash and fever• Non-pneumonia respiratory tract infection w/ feverNon-pneumonia respiratory tract infection w/ fever• Diarrhea/GastroenteritisDiarrhea/Gastroenteritis• PneumoniaPneumonia• Sepsis or non-traumatic shockSepsis or non-traumatic shock
ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Information System Functions Needed for Information System Functions Needed for Bioterrorism Preparedness and ResponseBioterrorism Preparedness and Response PREPAREDNESS REQUIRES THAT ALL PREPAREDNESS REQUIRES THAT ALL
PARTNERS--LOCAL, STATE, & FEDERAL PARTNERS--LOCAL, STATE, & FEDERAL ARE PART OF SYSTEMSARE PART OF SYSTEMS
Surveillance data analysis--event detection Surveillance data analysis--event detection & management& management
Notification—rapid alerting Notification—rapid alerting Communications –information, not dataCommunications –information, not data Knowledge managementKnowledge management
ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
The Immediate Future The Immediate Future 2003 – 20102003 – 2010
A Revolution in A Revolution in biotechnology, genomics biotechnology, genomics and proteomics that will and proteomics that will affect all human beingsaffect all human beings

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
TODAY’S SITUATIONTODAY’S SITUATION
Many hospitals on trauma diversion with Many hospitals on trauma diversion with nono major incidents going on major incidents going on
Not economically viable for hospitals to Not economically viable for hospitals to maintain surge capacity, or even to focus maintain surge capacity, or even to focus on treating sick and injured (hospitals on treating sick and injured (hospitals lose lose money treating the truly sick)money treating the truly sick)
Public health infrastructure is beyond Public health infrastructure is beyond simple band-aid fixessimple band-aid fixes
Military health system (including VA) is not Military health system (including VA) is not effectively integrated or usedeffectively integrated or used

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Provide More Health System Provide More Health System Surge CapacitySurge Capacity
Health care cost control has Health care cost control has systematically eliminated reserve systematically eliminated reserve capacity from the system.capacity from the system.
Need to rethink how much surge Need to rethink how much surge capacity is needed for emergencies.capacity is needed for emergencies.
Need to re-assess adequacy and Need to re-assess adequacy and geographic extent of mutual aid geographic extent of mutual aid agreements.agreements.
What mobile resources can the federal What mobile resources can the federal and state governments and state governments truly truly provide?provide?
Also need plans to tap unconventional Also need plans to tap unconventional resources if disasters strike – e.g., sites resources if disasters strike – e.g., sites for emergency care, inventories of for emergency care, inventories of health care workers.health care workers.

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Summary:Summary:Priority Preparedness ActivitiesPriority Preparedness Activities
State & local preparedness planningState & local preparedness planning Surveillance and epidemiologySurveillance and epidemiology Outbreak verificationOutbreak verification Laboratory capacity for biologic & Laboratory capacity for biologic &
chemical agentschemical agents Health information & communication Health information & communication
systemssystems TrainingTraining Establish key liaisonsEstablish key liaisons

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
Bottom LineBottom Line
Early, rapid recognition of unusual Early, rapid recognition of unusual clinical syndromes or deathsclinical syndromes or deaths
Early rapid recognition of increase Early rapid recognition of increase above “expected levels” of common above “expected levels” of common syndromes, diseases, or deathsyndromes, diseases, or death

ERIC K. NOJI, M.D.ERIC K. NOJI, M.D.
… … Life Has Changed for us allLife Has Changed for us all