Embed Size (px)
Citation preview

LITHUANIAN UNIVERSITY OF HEALTH SCIENCES
VETERINARY ACADEMY
Faculty of Veterinary Medicine
Disa M. Stattin
Equine Calcaneal Bursitis; diagnostics, treatment and
outcome
MASTER THESES
Integrated Studies of Veterinary Medicine
Supervisor: Lekt. DVM. Giedrė Vokietytė-Vilėniškė
KAUNAS 2019
2
THE WORK WAS DONE IN THE DEPARTMENT OF LARGE ANIMAL SURGERY CONFIRMATION OF THE INDEPENDENCE OF DONE WORK
I confirm that the presented Master Theses “Equine Calcaneal Bursitis; Diagnostics, Treatment and Outcome’’
1. has been done by me;
2. has not been used in any other Lithuanian or foreign university;
3. I have not used any other sources not indicated in the work and I present the complete list of
the used literature.
Disa M. Stattin (date) (author’s name, surname) (signature)
CONFIRMATION ABOUT RESPONSIBILITY FOR CORRECTNESS OF THE LITHUANIAN LANGUAGE IN THE DONE WORK
I confirm the correctness of the Lithuanian language in the done work.
Disa M. Stattin (date) (author’s name, surname) (signature)
CONCLUSION OF THE SUPERVISOR REGARDING DEFENCE OF THE MASTER
THESES
(date) (supervisor’s name, surname) (signature)
THE MASTER THESES HAVE BEEN APPROVED IN THE DEPARTMENT/CLINIC
(date of approbation) (name, surname of the manager of
department/clinic) (signature)
Reviewers of the Master Theses
1)
2) (name, surname) (signatures)
Evaluation of defence commission of the Master Theses:
(date) (name, surname of the secretary of the defence
commission) (signature)

3
TABLE OF CONTENTS
SUMMARY..................................................................................................................................................4SANTRAUKA..............................................................................................................................................5ABBREVIATIONS.....................................................................................................................................6INTRODUCTION.......................................................................................................................................7
Objective...................................................................................................................................................................7Aim............................................................................................................................................................................7Tasks..........................................................................................................................................................................71. LITERATURE REVIEW................................................................................................................................8
1.1. General clinical anatomy of the tarsal region of the horse................................................................................81.2. Calcaneal bursae in the horse...................................................................................................................................111.3. Bursitis.............................................................................................................................................................................111.3.1. Etiopathogenesis.......................................................................................................................................................111.3.2. Synoviocentesis........................................................................................................................................................12
2. SURGICAL APPROACH OVERVIEW....................................................................................................132.1. Endoscopic surgical approach comparisons.......................................................................................................132.2. Treatment........................................................................................................................................................................15
3. METHODOLOGY..........................................................................................................................................163.1. Case selection................................................................................................................................................................163.1.1. Case descriptions......................................................................................................................................................17
4. RESULTS..........................................................................................................................................................254.1. Case results....................................................................................................................................................................254.1.1. Endoscopic approaches used in the study........................................................................................................264.1.2. Synoviocentesis results..........................................................................................................................................304.1.3. Statistics of diagnostic codes................................................................................................................................344.1.4. Final results................................................................................................................................................................35
5. DISCUSSION...................................................................................................................................................36CONCLUSIONS........................................................................................................................................39
Conclusion of tasks..............................................................................................................................................................39RECOMMENDATION...........................................................................................................................40ACKNOWLEDGEMENT.......................................................................................................................41LITERATURE LIST................................................................................................................................42ANNEX 1.....................................................................................................................................................44

4
SUMMARY
Equine Calcaneal Bursitis; Diagnostics, Treatment and Outcome
Disa Stattin
Master Theses
Not many studies have been done regarding the tarsal bursae, its diagnostics and treatment. The
literature review section includes articles of calcaneal bursitis as well as the more prominent and
highly studied navicular bursa. In this study 16 horses with calcaneal bursitis were examined and
treated with bursoscopy. Horses were diagnosed by ultrasound and synoviocentesis, and
radiography was done to identify bone injuries. The nomenclature of the calcaneal bursae is
described differently in a range of literatures, in this study the calcaneal bursae is referred to as the
bursae in the tarsal region; the subcutaneous calcaneal bursa (SCB), the intertendinous calcaneal
bursa (ICB), the gastrocnemius calcaneal bursa (GCB) and the cunean calcaneal bursa (CCB).
Synovia, synovial fluids, and the lining of the bursa can get inflamed and irritated due to trauma
with or without penetrating wounds. The bursal lining gets thickened, and the synovial fluid gets
more viscous at the inflammation site, causing pain and lameness.
Key words: Bursitis, Bursoscopy, Synoviocentesis, Intertendinous calcaneal bursa (ICB),
Subcutaneous calcaneal bursa (SCB), Gastrocnemius calcaneal bursa (GCB)

5
SANTRAUKA
Arklių kalkanalinis bursitas; diagnozavimas, gydymas ir baigtis
Disa Stattin
Magistro baigiamasis darbas
Studijų apie tarzalinių bursų tyrimus, jų diagnozavimą ir gydymą yra atlikta nedaug. Literatūros
apžvalgoje yra apžvelgiami moksliniai straipsniai apie kalkanalinį bursitą, taip pat apie dažniau
pasitaikančią ir labiau išstudijuotą navikuliarinę bursą. Šiame darbe buvo ištirta 16 arklių, kuriems
nustatytas kalkanalinis bursitas ir gydyti naudojant bursoskopiją. Arkliai buvo tiriami naudojant
ultragarsą ir sinovijos centezę, rentgenologinis tyrimas atliktas siekiant nustatyti sužalojimus.
Kalkanalinio bursito terminas literatūroje apibrėžiamas įvairiai. Šiame darbe kalkanalinė bursa yra
apibrėžiama kaip bursa tarzalinėje srityje; poodinė kalkanalinė bursa (SCB), intertendinous
kalkanalinė bursa (ICB), gastrocnemius kalkanalinė bursa (GCB) ir cunean kalkanalinė bursa
(CCB). Sinovijos, sinovijos skysčių ir bursos pamušalų uždegimas gali kilti esant traumoms kai yra
atviros arba uždaros žaizdos..Uždegimo vietoje bursos pamušalas sustorėja, o sinovijos skysčiai
tampa klampūs dėl ko atsiranda skausmas ir lameness.
Raktažodžiai: bursitas, bursoskopija, sinovijos centezė, intertendinous kalkanalinė bursa (ICB),
poodinė kalkanalinė bursa (SCB), gastrocnemius kalkanalinė bursa (GCB)

6
ABBREVIATIONS
ICB: Intertendinous Calcaneal Bursa
SCB: Subcutaneous Calcaneal Bursa
GCB: Gastrocnemius Calcaneal Bursa
CCB: Cunean Calcaneal Bursa
GT: Gastrocnemius Tendon
CT: Cunean Tendon
SDFT: Superficial Digital Flexor Tendon
DDFT: Deep Digital Flexor Tendon
A-RILP: Antibiotic perfused Regional Intravenous Limb Perfusion
RILP: Regional Intravenous Limb Perfusion
LH: Left Hind (Limb)
RH: Right Hind (Limb)
BH: Both Hind (Limbs)
IB: Intra bursae
PO: Per Os
IV: Intravenously
IM: Intramuscular
US: Ultrasound
NSAID: Non-Steroidal Anti-Inflammatory Drugs

7
INTRODUCTION
Depending on the severity of the bursitis, its infection type, and the health status of the horse
together with the realistic thoughts of owners and their future with the horse, a treatment program is
discussed. Bursitis of the tarsal regional bursas occurs often in correlation to trauma whereas a
puncture wound into the bursa can cause a septic process. All cases in the study (septic and aseptic)
were treated with bursoscopy in form of diagnostic means and treatment by lavage and debridement
of the bursae. 87,5% of cases in the study had a penetrating wound into bursae whereas 12,5% of
them had a septic process with microorganisms in the luminal cavity of the bursae. All cases except
one was treated with IB injection and/or A-RILP together with systemic antibiotic treatment. The
standard endoscopic approach used in the study was a proximal and/or distal approach to the
insertion sites of retinaculum of the SDFT. The proximal end of calcaneus encounters an enlarged
osseous structure and has minimal soft tissue protection, causing an increased risk of injuries to the
bone. The tendons attaching to the tuber calcanei has by that, also less protection, that is one reason
why there are two main bursae located in the calcaneal region (SCB and ICB). A septic process of
the bursae interior structures might also affect the tendons and ligaments coursing through its
synovial structure.
Objective The objective of this study was to describe the clinical presentation, diagnostic features,
response to medical and endoscopic treatment and long‐term outcome of horses with
bursitis.
Aim The aim of this study was to evaluate the outcome and treatment for cases with bursitis.
Tasks 1. To find percentage of bursitis cases treated with bursoscopy (endoscopy) that came
back to their previous training form.
2. Ascertain techniques of treatment for aseptic versus septic bursitis, their outcome
and prognosis
3. To find out the most common placement of portals into bursae.
4. To find out anatomic communication between bursae.
5. To find out most common bacterial flora in septic bursitis.
6. Ascertain differences in comparison of A-RILP and IB injections.
7. To find out if direct approach with the endoscope is better than transtechal approach
due to the transition of a membrane.

8
1. LITERATURE REVIEW
1.1. General clinical anatomy of the tarsal region of the horse
The tarsal region also called the hock is situated distal to the tibia and proximal to the cannon bone
of the distal hoof of the hind limb. The tarsal or hock joint is a ginglymus joint; with the tarsocrural
joint being a cochlear joint. This composite, uniaxial joint has a one-way momentum that only
moves over one axis, craniocaudal. (1) Joints are synovial fluid filled gaps between bones that make
movement possible, the synovial fluid acts as lubrication for the bones as they move against each
other. The tarsal region is made up out of the tarsocrural joint that attaches cochlea of tibia with
trochlea of talus, talus also attaches to calcaneus via talocalcaneal joint. Talus and calcaneus creates
the first/proximal row of bones in the tarsal region, they attaches to the central tarsal and 4th tarsal
bone via proximal intertarsal joint. The distal intertarsal joint is situated between central tarsal bone
and 1st to 3rd tarsal bones. The tarsometatarsal joint is situated between the 1st to 4th tarsal bones and
2nd to 4th metatarsal bones. Intertarsal joints are vertical joints situated between the tarsal bones. (2)
The tarsal bones stick together by the articulations described above and ligaments coursing from
bone to bone and tendons cursing from muscles to bone. The interosseous ligament follows
metatarsal bone 3 (MTB-III), and the deep digital flexor tendon (DDFT) courses over all the way to
the distal hoof and to the last phalanx. The superficial digital flexor tendon (SDFT) courses over the
DDFT from femur to tuber calcanei and down to the second phalanx of the distal foot.
1. Tarsocrural/tibiotarsal joint
2. Talocalcaneal joint
3. Proximal intertarsal joint
4. Distal intertarsal joint
5. Tarsometatarsal joint
Fig. 1.1. Schematic drawing of the hock joint of the horse

9
Bursas are anatomically similar to joint capsules by their inner synovial membrane and outer
fibrous layer. They are different in structures where the bone surfaces for bursas are covered with
fibrocartilage rather than hyaline cartilage as it is for joints. Bursas are situated at places where
tendons courses over bone, they work as a cushion to prevent friction of the tendon against the bony
surface, like tendon sheaths they work to promote the gliding motion of tendons. An example is the
intertendinous calcaneal bursa (ICB) that lies between calcaneus and SDFT. (3)
Several bursas are located in the plantaroproximal aspect of tuber calcanei, including: the potential
subcutaneous bursa (SCB), where the presence of a true bursa is debatable and is, in some articles
considered a ’’fake bursa’’ because of the upcoming of the bursa is often associated to trauma
rather than genetics in some cases. (4) The SCB develops superficial to the superficial digital flexor
tendon (SDFT). The intertendinous calcaneal bursa (ICB), also called subtendinous calcanean bursa
is located between the SDFT and gastrocnemius tendon (GT). Another bursa is situated dorsally to
the insertion of the GT on tuber calcanei and is by its position named gastrocnemius calcaneal bursa
(GCB)(5)(6) The GCB often communicates with ICB.(7)(8) On the medial aspect of the tarsus triangled
between tibia, calcaneus and talus is the cunean calcaneal bursa (CCB) situated, where the cunean
tendon (CT) courses over the surface where tarsal bone 1 and 2 fuses. The small CCB is said to be
of clinical importance.(9)
Bursas are located in different places in the tarsal region were tendons courses over bone, they do
not surround the tendinous structure like tendon sheaths do, as they are only located on one side of
the tendon. SDFT has bursae on each side of its most prominent section where it courses over tuber
cancanei. As seen in Figure 1.2 the superficial SCB (B), situated above the SDFT (dark blue), and
the ICB (C) situated below the same tendon as it courses over bone (tuber calcanei of calcaneus).
As shown in the picture the ICB is at least double the size of the smaller SCB. GT (red) courses
behind ICB, and attaches at tuber calcanei, it is sandwiched between ICB (C) and the GCB (D),
these bursae often communicates.(10) Behind GCB in the lateral view of the bone a branch of DDFT,
the Lateral DFT is situated (pink)(11)(12) In the medial aspect of the tarsal region lateral to the bone,
the CCB (A) is situated as the CT (green) courses over bone in a horizontal aspect where tarsal
bone 1 and 2 fuses. Letters and numbers for Fig 1.2 are described in Table 1.3 and 1.4.

10
Fig 1.2. Schematic drawing of bursas, tendons and tendon sheaths
Letter Name of bursae
A Cunean calcaneal bursa
B Subcutaneous calcaneal bursa
C Intertendinous calcaneal bursa
D Gastrocnemius calcaneal bursa
Number Name of bone
1 Tibia
2 Talus
3 Central tb
4 3rd tb
5 3rd mt
6 Tuber calcanei
7 Calcaneus
8 4th tb
9 4th mt
10 1st & 2nd tb
11 2nd mt
Table 1.3. Translating of schematic drawing of bones shown in Fig 1.2.
Table 1.4. Translating of schematic drawing of bursae shown in Fig 1.2.

11
1.2. Calcaneal bursae in the horse
In the anatomical study of Post et al. (2007) a communication between the ICB and the GCB was
confirmed in the study. The result was based on emersion of synovial fluid from the GCB,
following water injection of the ICB. Latex was injected into the ICB, and emersion of latex was
confirmed from the GCB.(10) The study identified a communication on the medial aspect in all 18
(100%) limbs in the study, and a lateral communicative aspect in limbs between the ICB and GCB.
In more than one third (39%) of the 18 limbs a communication between SCB and ICB was
identified, and therefore also the GCB. As the study inflicts the ICB and GCB is to be considered as
one synovial structure due to the communicating compartments, this hence that synoviocentesis in a
septic calcaneal bursitis could be considered in the GCB as well as for the ICB.(12)(10) Diagnostic
tools for bursitis used are endoscopy, ultrasonography and radiography. (4) (13) (14)
1.3. Bursitis
1.3.1. Etiopathogenesis
Wounds to the tarsal region due to trauma are commonly seen in cases with bursitis of the calcaneal
bursas. Tendon tears and ligament raptures can be examined during diagnostic procedures of the
bursae by endoscopy and ultrasonography. Commonly seen in equine practice are mares in heat,
which kicks against the surrounding walls causing trauma or crapped hock that results in
inflammation of the SCB. If the trauma caused a penetrating wound into the bursal lumen there are
large chances of infection to occur in the bursa. The infection can become chronic if not taken care
of by correct means as endoscopy and antibiotic treatment. In a study by Richardson et al. (1986)
bacterial cultures was examined from 9 horses with navicular bursitis. (16) The results of the 9 horses
tested for bacterial growth in the navicular bursae showed bacterial growth of Streptococcus
zooepidemicus, Proteus spp., Pseudomonas aeroginosa, Enteric gram-negative rods, Escherechia
coli or was without any bacterial growth.(16)

12
Sensitivity testing for the infected cases of navicular bursitis showed positive for Gentamicin,
Kanamycin, Amikacin, Trumethoprim/sulfamethoxazole, Carbenicillin, Tobramycin, Tetracycline,
Chloramphenicol and Aampicillin. All Streptococcus spp. was considered sensitive to penicillin at
the clinic where the study was done. The antibiotics used were Penicillin G for Proteus spp,
Pseudomonas aeroginosa, Enteric gram-negative rods, Streptococcus aeroginosa and Escherechia
coli. Penicillin G was used together with Trimethoprim/sulfamethoxazole for 5 cases and alone for
the horse with no bacterial growth. In total 34 horses out of 38 received antibiotics (one or more in
combinations) in the study. In the study the horses were hospitalized for 1-708 days (mean 44,8
days). (16)
1.3.2. Synoviocentesis
A synoviocentesis is applied to measure the synovial fluids in synovial structures to rule out
inflammation or infection in the luminal cavity. Infection in synovial structures in horses is a
potential threat to the athletic function of the horse, as the infection can cause intraluminal
structures to break down. If the wound penetrating the cavity is large enough, causing a drainage of
the effused fluid, the lameness may not show until the wound granulates and the draining stops,
imprisoning the fluid inside the cavity causing a out pouching of the area due to the distension of
the fluid filling the cavity, causing the lameness due to pain.(17)
In the procedure of synoviocentesis the area should be aseptic and the procedure should be done
with precision not to cause infection or injuries of the membrane. Normal synovial fluid is light
yellow in color and viscous but does not clot, it has a cell count of ≤0,5x109 cells/L while a infected
or inflamed synovia has synovial fluid which is yellow to red-brownish in color and has low
viscosity with a cell count of >20x109 cells/L with some variations. In normal synovia the
Neutrophil percentage is around <10 %, a increased percentage of the neutrophil count indicates on
synovitis. Synovitis cases can include a neutrophil cell count in percentage up to ≥85 % in some
cases.(17)
The viscosity of the synovial fluid is created by polymerized hyaluronic acid that binds the fluid,
creating the viscosity. If taking a drop of synovial fluids between two fingers the normal synovial
fluid stretches 2-4cm before breaking, if synovitis is present these polymerized hyaluronic acid
bonds breaks earlier. In normal synovial fluids the mononuclear cells together with neutrophils is
around 10% of the total cell count, which increases to ≥90% in septic cases.(18)
13
2. SURGICAL APPROACH OVERVIEW
2.1. Endoscopic surgical approach comparisons There are two mostly used approaches in the endoscopic vision of the bursae; direct or transtechal
approach. Other articles have described modified approaches to bursas of cadavers, and in all
articles observed for the study, the authors agree on the fact that an endoscopic visualization is
necessary for the treatment process and diagnostics of bursitis. In a study where two approaches
into the navicular bursa by an endoscope through a single portal in 16 cadavers, a modified
straightforward approach allowed near-complete examination of the navicular bursa with minimal
iatrogenic damage to the intrabursal structures.(19) The study was based on two original reports
whereas the first had synoviocentesis as the main diagnostic technique as well as bursoscopy. The
authors agree that the most appropriate approach of treatment is a surgical exploration and
debridement of the bursae together with regional perfusion of antimicrobial drugs. (14) In the second
article, radiography was used as the main diagnostic approach for endoscopy of the bursae and its
pathological findings. 17 cadavers front limbs was used in the study. A podotrochlear bursa
endoscopy was used to identify abnormalities associated with podotrochleosis, the endoscopical
approach was done on the ipsilateral side of the bursa which was described in the report as a
difficult portal to observe the bursal linings. Podotrochlear endoscopical approach to the bursa
could assist in the identification of podotrochleosis pathological changes within the bursa hence the
author. (20) Transtechal approach has been described in navicular bursas by dissection through the
distal part of the distopalmar recess of the DDFT sheath. A single ipsilateral portal was done that
created a vision of the whole navicular bursa and allowed free movement of the endoscope. The
results support earlier studies where the modified approach of the portal increased the access to the
bursa. (21)(19)

14
In a study by Ingle-Fehr et al (1998) an endoscopic diagnostic approach was done to the calcaneal
bursa of 12 cadavers and 2 adult horses with a direct approach that enabled a complete assessment
of the bursal cavity through a single portal on the plantar medial or plantar lateral aspect distally to
the bursa below the attachment of the SDFT. Positioning of the horse on the operation table was
discussable due to the easier positioning of the lateral recumbence while the dorsal recumbence
allowed access to both aspects of the bursa, medial and lateral. The GT was used as a landmark for
the proximal aspect of the ICB as it attaches to tuber cancanei of calcaneus. By this approach no
damage was done to the SDFT as evaluated during gross dissection of the bursa. The use of an
endoscope to the bursa for diagnostic approach provided a direct observation of the whole bursa,
and with a single endoscopic portal.(13) The study by Ingle-Fehr and Baxter (1998) is also described
as the main surgical approach in the literature of the book ’’Diagnostic and surgical arthroscopy in
the horse’’ that refers to the article when describing the insertion of the instrument in the standard
approach to the bursae. The endoscope is inserted between the SDFT and the plantar ligament (PL)
in a distal to medial or lateral approach to the retinacular insertion of the SDFT. A portal is created
distal to the retinaculum into the bursa medial or lateral to the retinaculum distally. The approach
enables a thorough full view of the bursa through one portal. The approach could, as mentioned be a
lateral approach or a medial approach called ’’standard approaches’’. Depending on circumstances
for the specific bursa, eg. Wounds, different approaches can be made in a proximal or distal
approach to the retinaculum. That may be ipsilateral or contralateral to the endoscope.(22)
Fig. 2.1. Lateral approach with endoscope (brown)

15
2.2. Treatment
After diagnostically observed the bursitis to evaluate the possibility of inflammation and/or
infection of the bursa, the treatment plan can be done for the individual horse. Regional intravenous
(saphenous vein) limb perfusion (RILP) together with endoscopic lavage of the bursae was used as
treatment reported by Wright et al. (1999) for treatment of contaminated and infected bursae, in all
recorded articles one method of treatment was done by endoscopy.(14)(11) (23) (12) Median of the
horses hospitalized was 16 days with a mean of 17 days and the interval of 7-40 days following
surgery. 10 horses returned to their previous training form, 2 were euthanized due to persistent
lameness. Synoviocentesis was performed as the main diagnostic technique, and endoscopic
treatment resulted in a shorter hospitalization period. In a report by Richardson et al. (1986), a study
of 38 horses with puncture wounds into the navicular bursa was examined. The age of the horses
ranged from 3 months to 20 years of age, with a mean age of 8,3 years. Treatment was done by
debridement and endoscopy of the bursae. 15 horses needed a repeated surgical treatment. 34 horses
received antibiotic treatment in form of penicillin G, Trimethoprim/sulfamethoxazole, Kanamycin,
Gentamicin, Streptomycin, and Oxacillin some with combinations.(16) It does not say in the report
how the antibiotics were administrated (per os (PO), intravenoursly (IV), intrabursal (IB)). The
mean hospitalized period for the horses were 44,8 days, septic cases had a bad prognosis. The
author recommends the use of penicillin G and Aminoglycoside as an initial therapy before the
sensitivity test results are available. 12 (31,6%) of the horses in the study had a satisfactory
outcome.(16) (14)

16
3. METHODOLOGY
3.1. Case selection
16 cases with bursitis treated with bursoscopy between the years of 2016 and 2018 at UDS in
Uppsala, was used for the study to enable an understanding of endoscopic techniques of bursae in
the tarsal region, how to diagnose the pathology its prognosis, diagnostics, treatment and outcome
of endoscopic surgery due to bursitis. Cases were observed during pre- and post-surgery for
observation of the treatment plan; owners were contacted years/months after the surgery for a
follow-up. Synovial samples from the bursa was tested for most cases, and its parameters was
observed for a indication of severeness of the bursitis, observation of choice of treatment plan
depending on the synovial tests was used as guidance.
RLP is done in the saphenous vein of the hind limb to assemble the antibiotics in the tarsal region.
The procedure is done by placement of a tourniquet on the hind limb to compress the saphenous
vein to a stasis. The vein is then locally sedated with lidocaine or carbocaine before gentamicin or
amikacin is injected into the vein during a period of time. In the IB injection, a dose of gentamicin
is directly administrated into the bursa and the accumulation of the antibiotics assembles in the
closed cavity of the pouch. The techniques were used together in most cases.
Diagnostic codes for the pathology of relevance was selected:
MB412: Bursitis (acute)
MB71: Trauma to synovial structures (tendon sheath and bursae)
MB422: Bursitis (chronic)
These codes were sent to insurance companies whereas statistics was sustained from one company
‘’Sveland djurförsäkringar’’ (translated into Sveland animal insurance company). The insurance
company replied that the statistics of cases with the diagnostic codes MB412, MB71 and MB422,
from the years of 2017 and 2018 show less than 1% out of all injury enquiries they receive in
equine medicine, which concludes that these diagnostic codes (MB412, MB71 and MB422) are
uncommon. The results of the statistics only shows if the horse got euthanized or got a continuous
treatment by veterinarian, and not the specific question of potential athletic training form post
surgery. The statistics is shown in Annex 1, used as an elective interest in the diagnostic codes.

17
3.1.1. Case descriptions
All 16 cases (named from A to P) their diagnostics, treatment, synovial test results and outcome are
described in the following section below. All cases were treated with Geepenil (bensylpencillin
natrium/Penicillin G), Gentaject (Gentamicin) and Flunixin (NSAID) systemically. Variation was
done in the matter of A-RILP and/or IB injections with either Biklin (Amikacin) or Gentaject
(Gentamicin). During A-RILP a concentration of lidocaine or procaine was first administrated IV
into the saphenous vein of the hind limb before start of the infusion. The horses stayed hospitalised
for 3 to 18 days (mean 9,5 days) post surgery. All cases got a sterile bandage post surgery and got
sterile bandage change throughout the hospitalization. Horses with an insufficient vaccination status
of the tetanus vaccine, got a vaccination if a penetrating wound into the bursae was present.
Case A:
Diagnostics:
Wound in plantaroproximal aspect of the calcaneus. Effusion of fluids in the ICB causing distension seed in
both lateral and medial aspect of the proximal calcaneal region and lateral, medial and dorsal to the SDFT
and distal attachment of the GT. No distension of the SCB or other structures (tendons, ligaments) is seen in
the ultrasound. Osteitis is suspected by x-ray.
Treatment and surgical approach:
Calcaneal inter- and subtendinous approach with standard distolateral and proximomedial portals. Amikacin
was administraded IB right after the surgery and portals were closed. RILP with lidocaine+gentaject
(gentamicin) was done. Geepenil (bensylpenicillinnatrium/Penicillin G)+Gentaject (gentamicin) and flunixin
was administrated IV during the hospitalization.
Synovial test results:
Synoviocentesis of ICB with high cell count: Leucocytes 1090 10e6/L, Neutrophils 66%, Lymphocytes 14%,
mononuclear cells 20%.

18
Case B:
Diagnostics:
Wound plantaromedial calcaneus. No skeletal damage seen in x-ray.
Treatment and surgical approach:
Surgery 1: Standard distolateral portal to ICB, penetration observed in the middle third of the bursa.
Additional portal proxomedially to lavage GCB, torn fibers of SDFT is debrided. Drain placed distally. RILP
with gentamicin was done and Gentaject (gentamicin) + Geepenil (bensylpenicillinnatrium/penicillin G) was
administrated IV.
Surgery 2: ICB accessed from the wound. Purulent material in SCB was debrided and an additional portal
proximomedially was made to lavage GCB. Double layer support bandage was applied sterile for support.
Ceftiofur+gentamicin IB. Complications after 6 days, horse came back to clinic. Euthanasia due to bad
prognosis and economics.
Synovial test results:
Synoviocentesis of ICB, 2% eosinophils, Leukocytes 21000 10e6/L, Neutrophils 87%, Lymphocytes 4%,
mononuclear cells 7%. A second synoviocentesis was sent to the lab, but the answer was not received, it was
probably septic due to the outcome (euthanasia).
Case C:
Diagnostics:
Wound plantarolateral aspect of calcaneus.
Treatment and surgical approach:
Standard distolateral and medial portals to ICB and additional portals proximolaterally to GCB, the bursae
was lavage with 5L saline. SCB debridement. Drain distally placed. ICB injected with gentamicin, portal
closed. Geepenil, gentaject, flunixin IV. RILP with gentamicin.
Synovial test results: -

19
Case D:
Diagnostics:
Wound proximal and dital to calcaneus. Effusion of ICB seen medially to the bone in ultrasound and osteitis
evaluated by radiography.
Treatment and surgical approach:
Surgery 1: Standard portals to ICB, injection with gentamicin IB.
Surgery 2: Previous portals opened, partial synovectomy performed but not possible to remove all pannus
from proliferative villi, bursae were lavaged with 40L RA. Laterodistal portal left open for drainage rest was
closed. RILP with amikacin. Enrofloxacin was considered as anticiotic change due to worsened condition of
the horse, but euthanasia was done in the end due to pad prognosis.
Synovial test results:
Purulent inflammation seen in ICB with particles inside macrophages (phagocytised), actinobacillus
susceptible for gentamicin was evaluated as bacterial flora. Leukocytes 36160 10e6/L, Neutrophils 87%,
Lymphocytes 1%, mononuclear cells 12%. On the second synovial test Staphylococcus aureus and a non-
specific coagulative-negative bacteria was observed. Septic synovitis.
Case E:
Diagnostics:
Wound plantarolateral calcaneus.
Treatment and surgical approach:
Gentamicin to ICB injected IB and sterile bandage. Standard portals to ICB and GCB done for endoscopic
diagnostics. Split lesion of SDFT communicating with the wound, injury debrided. Drain placed laterodistal
to wound. RILP with gentamicin, gentamicin injected IB portals closed. Geepenil
(bensylpencillinnatrium/Penicillin G)+gentaject (Gentamicin)+flunixin administrated IV.
Synovial test results:
No bacterial growth in ICB.

20
Case F:
Diagnostics:
Wound horizontal on lateral view of calcaneus. Thickening surrounding the plantaroproximal aspect of the
calcaneus and along the plantar aspect of calcaneus, no skeletal abnormalities was seen in radiography.
Treatment and surgical approach:
Got tetanus vaccination. Standard proximodistal lateromedial portals into ICB, lavage. RILP with
gentamicin, drain distally to wound. Gentamicin IB. Geepenil+gentaject+flunixin.:
Synovial test results
Leukocytes slightly increased but the test was too small for instrumental measurement. Neutrophils 63%,
Lymphocytes 22%, mononuclear cells 14%.
Case G:
Diagnostics:
A horizontal wound distally to tuber calcanei, no skeletal abnormalities.
Treatment and surgical approach:
Biklin (Amikacin) IB ICB/SCB, gentamicin+geepenil (Bensinpenicillinnatrium/Penicillin G). Bursoscopy
was done through wound over distolateral pouch of ICB. Standard medial and lateral approach, plantar
ligament rupture. Lavage of bursa and application of drain, closure of portals, biklin (amikacin) was
administrated IB in ICB. Suspected communication with GCB. Bandage. RILP with gentaject (gentamicin).
Geepenil (bensynpenicillinnatrium/Penicillin G)+flunixin.
Synovial test results:
Leukocytes 156300 10e6/L, Neutrophils 91%, Lymphocytes 0%, mononuclear cells 9%. No
microorganisms. Synovitis.
Case H:
Diagnostics:
No wound. UL+X-ray, no effusion shown in UL, necrotic bone defect seen in x-ray, osteomyelit.
Treatment and surgical approach:
Bursoscopy with standard distolateral and medial portals to ICB and instrument portal in the proximal lateral
bursa (GCB), no tendon damage examined with endoscope. Bursae medicated with amikacin and portals
closed. Geepenil (Bensylpenicillinnatrium/Penicillin G), flunixin, RILP with gentamicin and placement of a
sterile bandage.
Synovial test results: -
21
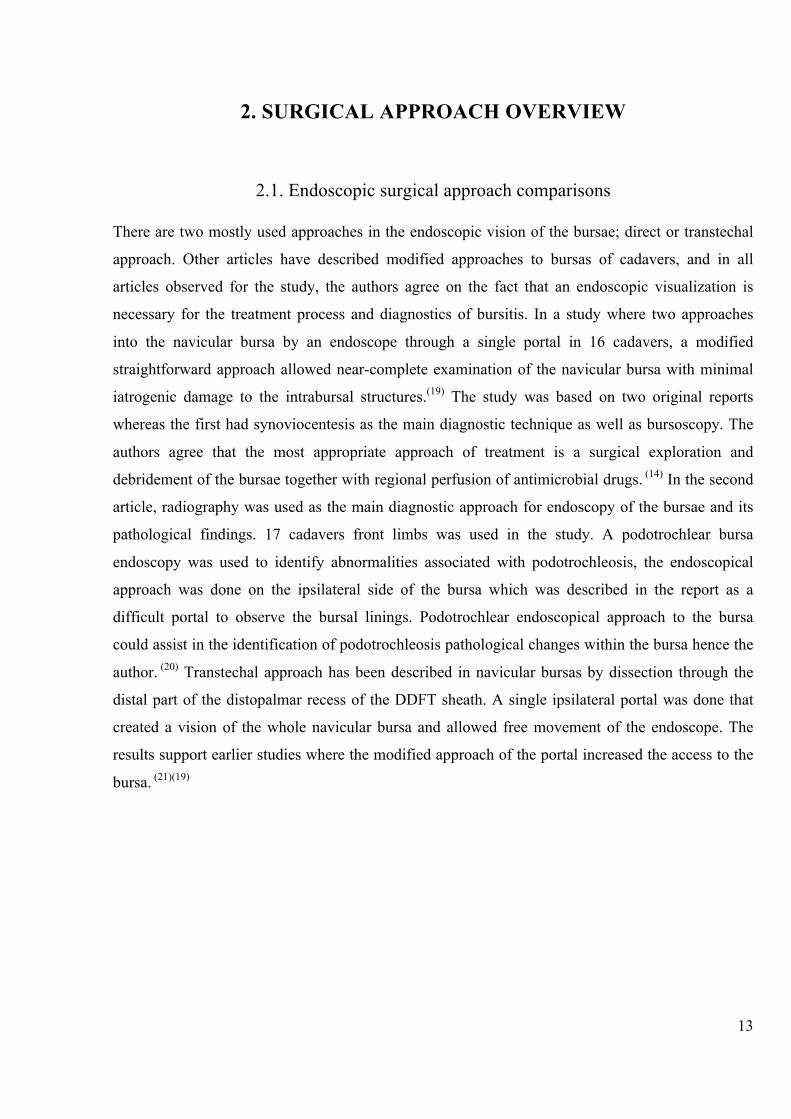
Case I:
Diagnostics:
Ventrical wound laterocaudal, distally to tuber calcanei, no skeletal changes seen in x-ray.
Treatment and surgical approach:
Geepenil (Bensylpenicillinnatrium/Penicillin G), gentamicin and flunixin IV. A perfusion from wound to
ICB was seen plantarolaterally. Proximal mediolateral and distomedial and lateral portals to ICB and GCB.
Portals closed. Sterile bandage. RILP with gentamycin. IB injection with gentamicin.
Synovial test results: -
Case J:
Diagnostics:
No wound, effusion of ICB/GCB can be seen. US show echoic fluids in bursae and X-ray shows small defect
in skeleton.
Treatment and surgical approach:
Two lateral and three medial portals into ICB and GCB, severe synovitis and a granuloma can be debrided.
Lavage of bursae and IB injection of gentamycin together with morphine. Sterile bandage.
Synovial test results:
Leukocytes 640 10e6/L, Neutrophiles 10%, Lymphocytes 29%, mononuclear cells 61%. No synovitis.
Case K:
Diagnostics:
Wound at tip of calcaneus, no signs of osteomyelitis or sequester on x-ray. Split of SDFT could be seen in
US as well as bursitis in GCB and ICB.
Treatment and surgical approach:
Geepenil (bensylpencillinnatrium/Penicillin G), flunixin IV. ICB sampled for HemoCue 1,7x10^9 cells/L.
Distension of ICB via GCB no communication to SCB. Proximolateral and medial portals to ICB, split
injury to SDFT, lavage of bursae and injection IB with gentamicin. Portals closed.
Synovial test results:
3% eosinophils, erythrocytes 11g/L, Leukocytes 1190 10e6/L, Neutrophils 20%, Lymphocytes 22%,
mononuclear cells 55%.
22
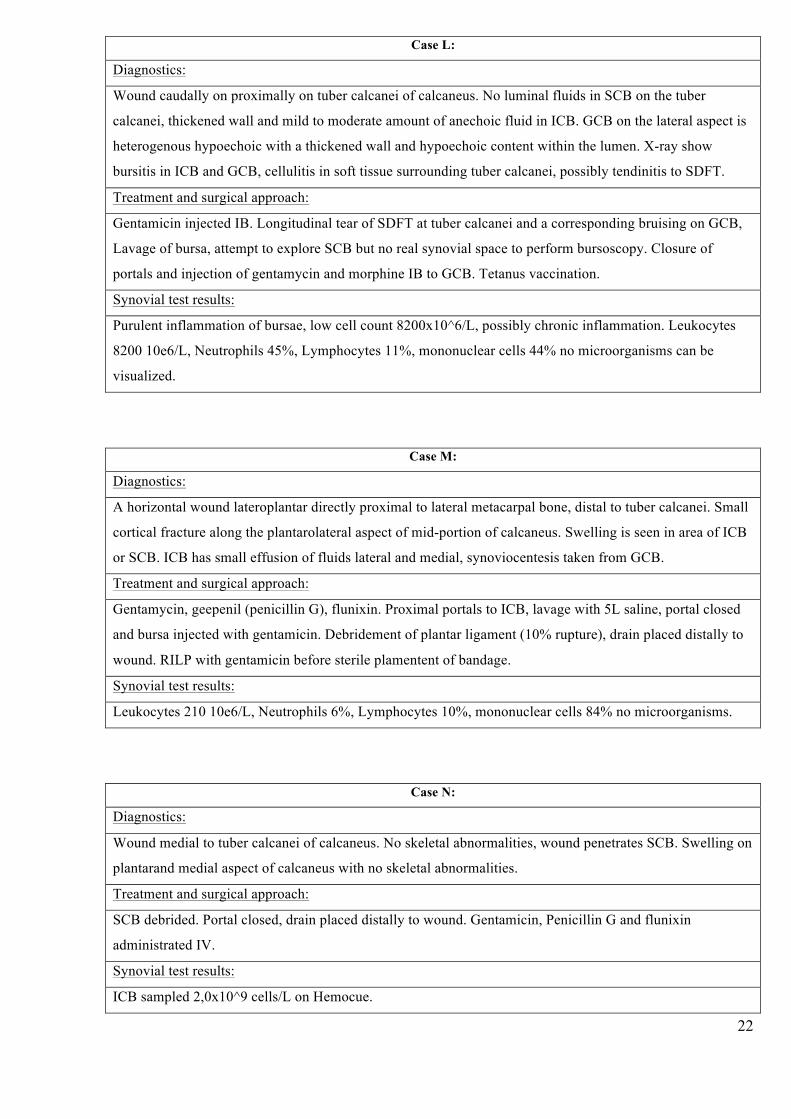
Case L:
Diagnostics:
Wound caudally on proximally on tuber calcanei of calcaneus. No luminal fluids in SCB on the tuber
calcanei, thickened wall and mild to moderate amount of anechoic fluid in ICB. GCB on the lateral aspect is
heterogenous hypoechoic with a thickened wall and hypoechoic content within the lumen. X-ray show
bursitis in ICB and GCB, cellulitis in soft tissue surrounding tuber calcanei, possibly tendinitis to SDFT.
Treatment and surgical approach:
Gentamicin injected IB. Longitudinal tear of SDFT at tuber calcanei and a corresponding bruising on GCB,
Lavage of bursa, attempt to explore SCB but no real synovial space to perform bursoscopy. Closure of
portals and injection of gentamycin and morphine IB to GCB. Tetanus vaccination.
Synovial test results:
Purulent inflammation of bursae, low cell count 8200x10^6/L, possibly chronic inflammation. Leukocytes
8200 10e6/L, Neutrophils 45%, Lymphocytes 11%, mononuclear cells 44% no microorganisms can be
visualized.
Case M:
Diagnostics:
A horizontal wound lateroplantar directly proximal to lateral metacarpal bone, distal to tuber calcanei. Small
cortical fracture along the plantarolateral aspect of mid-portion of calcaneus. Swelling is seen in area of ICB
or SCB. ICB has small effusion of fluids lateral and medial, synoviocentesis taken from GCB.
Treatment and surgical approach:
Gentamycin, geepenil (penicillin G), flunixin. Proximal portals to ICB, lavage with 5L saline, portal closed
and bursa injected with gentamicin. Debridement of plantar ligament (10% rupture), drain placed distally to
wound. RILP with gentamicin before sterile plamentent of bandage.
Synovial test results:
Leukocytes 210 10e6/L, Neutrophils 6%, Lymphocytes 10%, mononuclear cells 84% no microorganisms.
Case N:
Diagnostics:
Wound medial to tuber calcanei of calcaneus. No skeletal abnormalities, wound penetrates SCB. Swelling on
plantarand medial aspect of calcaneus with no skeletal abnormalities.
Treatment and surgical approach:
SCB debrided. Portal closed, drain placed distally to wound. Gentamicin, Penicillin G and flunixin
administrated IV.
Synovial test results:
ICB sampled 2,0x10^9 cells/L on Hemocue.

23
Case O:
Diagnostics:
Wound bilateral on BH. LH horizontal wound distal to calcaneus, RH similar wound but more proximal. No
skeletal injuries bilateral.
Treatment and surgical approach:
Geepenil (bensylpenicillinnatrium), gentamicin, flunixin IV.
Surgery 1: 24-06-18
LH: Synoviocentesis. Wound involving the laterodistal pocket of ICB and therefore used as a portal.
Standard portals to the ICB bursa. Severe contamination with hair inbedded in the bone, injury to plantar
ligament, mild amount of fibrin. Debrided with shaver. Drain placed distally to wound, sterile bandage.
RH: Synoviocentesis. Standard portals to ICB mild injury to synovia is seen in lateral aspect of wound,
debrided with shaver. Drain placed distally to the wound, portals closed, bursa injected with gentamicin.
Sterile bandage. LH: RILP with gentamicin, RH: IB inj with gentamicin. (LH worse condition). Bilateral IB
injection with gentamicin.
Surgery 2: 29-06-18
LH: Distomedial portal open and wound is still involving ICB, lateral aspect of wound reopened. Standard
portals to the ICB. Distomedial portal extended for drainage of the bursa. Previous drainportal from the
wound left open for drainage. Proximal portals closed and sterile bandage applied. RILP with amikacin.
RH: Reopened previous portals. Below lateral apect of wound a mild injury to the synovia could be seen as
previously towards the calcaneus. Synovioectomy and debridement of fibrin done, distolateral portal
enlarged for draining portal from the bursa. Previous drain portal left open for drainage. sterile bandage.
Due to non-responsive to Geepenil(bensylpenicillinnatrium/Penicilling G), gentaject (gentamicin), a change
to enrofloxacine is done together with geepenil (bensylpenicillinnatrium/Penicillin G). (enrofloxacin in RILP
is not done due to high venous irritant), cannot make IB injection due to drainage. Bad prognosis, 40-50%
highly estimated. RILP biklin (amikacin)+carbocaine BH.
Synovial test results:
First synoviocentesis: 25-06-18
LH ICB synoviocentesis purulent inflammation Leukocytes 138800 10e6/L, Neutrophils 93%, Lymphocytes
0%, mononuclear cells 7%.
RH ICB synviocentesis staphylococcus can be seen in form of a septic purulent inflammation. Leukocytes
429000 10e6/L, Neutrophils 96%, Lymphocytes 0%, mononuclear cells 4%.
Mixed bacterial flora bilateral bursae.
Second synoviocentesis: 28-06-18
LH ICB synoviocentesis: Leukocytes 236100 10e6/L, Neutrophils 96%, Lymphocytes 0%, mononuclear
cells 4%
RH ICB synoviocentesis: Leukocytes 45710 10e6/L, Neutrophils 98%, Lymphocytes 1%, mononuclear cells
1%. No microorganisms can be seen today.
24
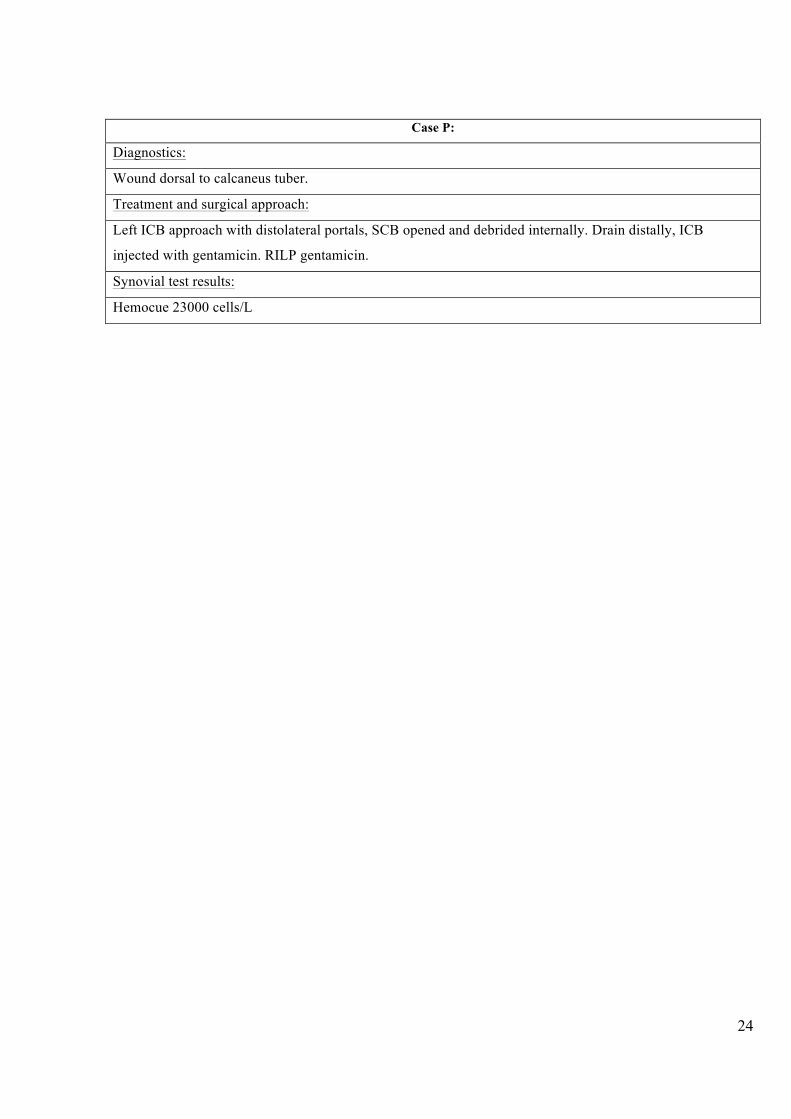
Case P:
Diagnostics:
Wound dorsal to calcaneus tuber.
Treatment and surgical approach:
Left ICB approach with distolateral portals, SCB opened and debrided internally. Drain distally, ICB
injected with gentamicin. RILP gentamicin.
Synovial test results:
Hemocue 23000 cells/L

25
4. RESULTS
4.1. Case results All cases were treated with endoscopy and selected as surgical emergencies due to inflammation of
a synovial structure. A sterile bandage was applied for all cases. Intravenous treatment was
performed in form of Flunixin (NSAID), Geepenil (bensylpencinillnatrium/penicillin G), and
Gentaject (gentamicin). Septic cases were treated more aggressively with IB injections and A-RILP,
and a change in antibiotics into to a stronger type to manage the infection (Enrofloxacin) occurred
in one septic case with a bacterial infection.
Out of the 16 horses that were observed in this study, 4 (25%) of them had septic bursitis, whereas 3
(20%) of these septic cases needed a second operation. 50% cases with septic bursitis had a positive
microbial lab result. And the remaining 12 (75%) cases had aseptic bursitis.
Fig 4.1. Pie chart of 16 cases with different types of bursitis in percentage
12%
75%
13%
Typesofbursitiscasesinpercentage
Septicbursitis Asepticbursitis Bacterialbursitis n=16n=12n=2n=2

26
Out of the 16 cases in the study 10 (63%) cases were treated both with IB injections and A-RILP, 3
(19%) cases was treated with RILP only, and 2 (12%) cases was treated only with IB injections and
1 (6%) cases got only systemic treatment. Differences between septic and aseptic antibiotic
treatment was not of significant matter. The bursae most often treated were the ICB in both septic
and aseptic cases.
Fig 4.2. Pie chart showing treatment methods differences for 16 cases with bursitis.
4.1.1. Endoscopic approaches used in the study Direct approach to the bursa was done in all cases of the study. The standard approach to bursae in
the tarsal region was done by a direct approach lateral or dorsally with the horse in a dorsal
recumbency. The scope was inserted below the retinacular insertion of the SDFT, laterally or
dorsally and via one portal, the ICB could be visualized completely, why no other approach was
used.
19%
12%
63%
6%
Percentageoftreatmentapplicationofantibiotics
A-RILP IBinj A-RILP+INinj Systemiconlyn=16n=3 n=2 n=1n=10

27
Bursas examined were the ICB, GCB and SCB, in the study no approach was done to the CCB. A
hypothesis may be that the CCB is well protected due to the fact that it is situated on the medial side
of the bone, some studies discusses about the ability of a lameness due to inflammation of the CCB
is even possible. In studies observed in chapter 2, a communication between ICB and GCB has
been studied between the bursas and most articles describe the interaction between them. In this
study the ICB and GCB was interacting and both were debrided during endoscopy in 9 (56%) cases.
ICB GCB ICB+GCB SCB ICB+SCB ICB+GCB+SCB
Bursaeapproachedbyendoscopy 4 1 7 1 1 2
4
1
7
1 1
2
012345678
Timesofapproach
Bursaeapproached
Bursaeapproachedbyendoscopyn=16
Table 4.3. Prevalence of different bursae diagnosed with endoscopy, regarding communication of bursae.

28
The endoscopic approach made in this study of 16 horses with calcaneal bursitis the standard
approach to the bursae was done in all 16 (100%) cases with variations due to placement of
penetrating wounds used as portals. The portals were done in one or more places of the tarsal region
in different cases due to re-surgeries or penetrating wounds. The proximal and/or distal
(mediodistal/distomedial) approach was done in 6 cases, and a variation of the distolateral approach
(n=6), proximomedial (n=5), proximolateral (n=2), proximodistal (n=1), medial (n=4), lateral (=1),
laterodistal (n=1) and lateromedial (n=3).
Fig 4.4. Chart that shows types and number of direct endoscopic approaches.
6 6
5
2
1
4
1 1
3
0
1
2
3
4
5
6
7
Numberofapproaches
Typesofapproaches
TypesofendoscopicapproachIB nofhorses=16nofapproaches=29

29
Surgery was done to ICB in 87% cases, to GCB in 31% cases and to SCB in 21% cases. In the cases
that involved GCB the ICB was involved as well in 93% of cases, indicating on communication
between the bursae in all except one case. 87% of cases had a wound in the calcaneal region
whereas 2 (12,5%) cases with a wound had a septic process with microorganism growth. In a
follow-up of the 16 cases 2 (12,5%) were euthanized after the procedure (case B and D), while 14
(87,5%) cases was sound including one case of septic bacterial bursitis (case O).
Fig 4.5. Pie chart that shows percentage of approaches with ensocope into bursae, note that CCB was not approached.
48%
31%
21%
0%
EndoscopicsurgeryIB
ICB GCB SCB CCBn=16
n=14 n=9 n=6 n=0

30
Horses were 4-22 years (mean 10 years) at the time of the procedure (bursoscopy). The study
included horses of different origin and athletic form: trotter (n=2), ponies (n=3), riding horses
(n=11). Out of these 16 cases the genders were distributed as geldings (n=6), mares (n=10). The
horses had been lame for 0-28 days (mean of 4,5 days) days prior to examination. And horses
stayed hospitalised for 3 to 18 days (mean 9,5 days) post surgery.
4.1.2. Synoviocentesis results
Out of the 16 cases in the study 80% of all cases did synoviocentesis to estimate the cell count of
synovial fluids in the bursae. Synovial fluids were tested with Hemocue in 3 cases, while 77% was
sent to the lab for further investigation. 2 cases got tested for synoviocentesis but the results could
not be estimated.

31
Due to the 2 times bilateral testing of Case O, a median result was estimated. With statistical
significants between means (P=0,013;P<0,05) showing the significants between septic (>20x109 to
>30x109 cells/L) and aseptic (≤0,5x109 cells/L) bursitis.
0,109
21
36,16
156,3
0,64
1,19
8,2
0,21
2
212,402
0,00023
0,0001 5
CaseA
CaseB
CaseD
CaseG
CaseJ
CaseK
CaseL
CaseM
CaseN
CaseO
CaseP
cells10e9/L Thousands
Casegroups
LeukocytesinsynovialNluids10e9/L
CaseA CaseB CaseD CaseG CaseJ CaseK
CaseL CaseM CaseN CaseO CaseP
P=0,013n=11
Table 4.6. Case results from Leukocyte cell count in value of 10e9/L. above 20x10e9/L shows synovitis.

32
Neutrophils percent count in normal synovia is <10 %, while in a synovitis it can be up to ≥85 %.
The other granulocytes percentage was not further investigated due to lack of studies studying their
normal values in bursitis. With statistical significants between means (P=0,014;P<0,05) for
synovitis, septic synovitis and aseptic synovitis results, septic cases are calculated from 85%.
66%
87% 87%
63%
91%
10%
20%
45%
6%
96%
0%5%10%15%20%25%30%35%40%45%50%55%60%65%70%75%80%85%90%95%100%
CaseA CaseB CaseD CaseF CaseG CaseJ CaseK CaseL CaseM CaseO
Peercentage
Casegroups
neutrophilsinsynovialNluids P=0,014n=11
Table 4.7. Comparison of neutrophils in synovia of different bursae, severe septic cases reach above the blue line (85%).

33
In the study, 100% of cases were treated with a direct approach to the bursa. The most common
portals were placed in a proximal lateral or medial direction to the bursae. The communication
between ICB and GCB were observed in most cases where the bursae was involved with synovitis.
Septic cases in the study were 25% in total where 12,5% of cases had bacterial flora intraluminar in
form of: Actinobacillus, Streptococcus aureus, and an unspecific mixed bacterial culture growth.
Due to the low caseload, a bacterial culture investigation could not be estimated. In one case (Case
O) a stronger antibiotics was used in form of Enrofloxacine, and in one case (Case D) it was
considered treatment but the horse was euthanized.
50% cases with septic bursitis were euthanized after surgery due to complications and bad
prognosis; the remaining 2 (50%) cases with septic bursitis came back to full athletic training form.
The 12 horses that were aseptic 100% came back to some type of training form. The most common
complications were relapse of lameness and pain of the tarsal region due to effusion of fluid in the
bursa.
Fig 4.8. Chart that shows how many cases with septic or aseptic bursitis came back to their previous training form.
2 2
12
0
Backtotraining Euthanized0
2
4
6
8
10
12
14
Outcomeofseptic/asepticcases
Numberofcases
Septic/Asepticcasesoutcome
Septiccases
Asepticcases
n=16
75%
12,5%12,5%

34
4.1.3. Statistics of diagnostic codes
Chart of diagnostic codes from an insurance company in Sweden evaluates the diagnostic codes
prone to the study, the outcomes presented as treatment (meaning that the horse got a continuous
veterinary treatment of the pathology) or euthanasia. Horse type refers to the type of horse that had
the diagnostic code, a sport horse used for riding, eventing etc., trotter or pony. Explanation of the
diagnostic codes:
MB412: Bursitis (acute)
MB71: Trauma to synovial structures (tendon sheath or bursae)
MB422: Bursitis (chronic)
In the total 83 (100%) cases, the diagnostic code MB71 encountered 67 (80,7%) cases, while codes
MB412 and MB422 encountered 8 (9,6%) cases each. Code MB71 consisted of 23 geldings, 7
stallions and 37 mares. Out of these 67 cases for the code MB71 4 (6%) cases were euthanized. For
the code MB412 the 8 cases consisted of 0 geldings, 2 stallions and 6 mares. Out of these 8 cases
for the code MB412, 2 (25%) cases were euthanized. The code MB422 had 8 cases in total whereas
0 was geldings, 0 were stallions and all 8 cases were mares, out of these 8 cases, 2 (25%) were
euthanized. Table seen in Annex 1.

35
4.1.4. Final results
Comparisons Total number of cases Septic bursitis Aseptic bursitis
Cases affected
with septic or
aseptic bursitis.
n=16 (25%) cases
n=4
(75%) cases
n=12
Outcome (Back to athletic
training or
euthanasia)
n=16 (12,5%) euthanasia
n=2
(12,5%) back to training
n=2
(0%) euthanasia
n=0
(75%) back to training
n=12
Endoscopic
approach
n=16 Direct approach Direct approach
Treatment n=16 Systemic+RILP+IB inj Systemic+RILP/IB inj
Synoviocentesis
results
n=16 Highly increased
neutrophil+leukocyte cell
count
Normal/slightly increased
neutrophil+leukocyte cell
count
Bacterial sepsis n=16 Bacterial influenced
n=2
Bacterial influenced
n=0
Wound or no
wound
n=16 Wound (100%)
n=4
No wound
n=0
Wound (83%)
n=10
No wound (17%)
n=2 Table 4.9. Comparisons of results done from septic versus aseptic bursitis in different perspectives.

36
5. DISCUSSION
In the study a large percentage (87,5%) of cases came back to their original training form after the
surgery. As seen in the results, the prognosis of aseptic bursitis is of high satisfactory outcome
while the septic cases has a lower satisfactory outcome and needs a more aggressive treatment.
Some changes could be seen in the treatment of septic and aseptic cases of bursitis, whereas the
aseptic cases could be treated systemically only, while septic cases were treated more aggressively,
especially the bacterial affected cases.
As seen in the results of the study 87.5% of cases came back to some type of training after the
surgery, and 12,5% of cases was euthanized due to bad prognosis. 50% of the eutanasal cases had a
septic bacterial process in the ICB, which is the largest bursa compared in the study, the prognosis
was bad and the owners did not want to exceed with stronger antibiotics. The second case with a
septic bacterial bursitis came back to full training form, this makes a 50/50 chance of the cases in
this study to come back to their previous training form from a secondary bacterial infection
infiltrating the bursae. As stated from Sveland insurance company, the cases of bursitis only
encounter (less than) 1% of all cases they receive each year, whereas out of the 83 cases 9% cases
were euthanized and 74% got veterinary care. In the study of Richardson et al (1986), (31,5%) of
horses with navicular bursitis had satisfactory outcome and in the study of Wright et al (1999) 10
(38%) horses came back to previous training form and 2 were euthanized due to persistent
lameness.
All cases were seen as emergency surgeries and treatment was done immediately in form of
systemic treatment (Gentamicin, Penicillin G and Flunixin), as well as A-RILP and IB injections
with amikacin or gentamicin. All cases were treated surgically by endoscopy in form of lavage and
debridement of the bursa; non-depending on if the specific case was septic or aseptic. One case was
treated systemically only; this single case was aseptic without a wound or complications. The cases
with a bacterial sepsis IB were treated more aggressively and required a longer convalescence
period and treatment plan before coming back to the post-traumatic training form. A-RILP and
endoscopy was used as treatment as reported by Wright et al. (1999) for treatment of contaminated
and infected bursae.

37
The arthurs of Wright et al (1999), E. S. Post et al (2007), Whitcomb et al (2006) and Tomlinson JE
et al (2003) recommends endoscopy for treatment of bursitis. In Richardson et al (1999) the horses
received antibiotic treatment in form of penicillin G, gentamicin and kanamycin and other.
Hyaluran was injected IB before closure of portals. Hyaluran acid is used for arthritis cases due to
the similarity of the fluids to synovial fluids, which lubricates the joint. It was not used in this
study, whereas morphine was used as pain relief for the bursae.
The most common endoscopic approach for bursas is the direct or transtechal approach, a direct
approach was used for all 16 (100%) cases in the study. The direct approach is described in most
articles to be the preferred approach due to less damage to surrounded tissues. In most cases a
medial or lateral approach was done to reach the ICB and GCB, by entering below the retinaculum
of the SDFT. In studies reflected from Chapter 2, the most common approach to the calcaneal
bursas where, as in this study, the direct approaches. For the navicular bursa however, a transtechal
approach was used through the DDFT to access the bursa in some cases. In this study seen in the
results of chapter 4, direct proximal medial or lateral approach to the bursae was used.
In the cases approached with the endoscope in this study a communication between the ICB and
GCB were described in more than 50% of cases (56.25%). A communication between the GCB and
ICB has been described in the studies of Sack W. O and Ferraglio (1978) and E. S. Post et al (2010
and 2007). The communication between the bursas differs a bit from the lateral and medial aspects.
Due to this highly suspected communication, the GCB can be used as a site for synoviocentesis for
ICB as said in E. S. Post et al (2007) and Tomlindon JE (2003) studies. This study concurred with
reviewed articles that communications between the bursas is possible, why synoviocentesis should
be received from a smaller bursa (GCB) when the larger ICB is infected as well would make sense
in some cases where the ICB is difficult to reach, why testing of the GCB could be done as an
option due to the communication.
In the study, cases with a septic bacterial infection IB, both encountered the ICB; the flora was
actinobaccillus and streptococcus for one case and a mixed bacterial growth in the other. The later
was treated with enrofloxacin and came back to training, while the other was euthanized. In the
study of Richardson et al (1986), the IB bacterial growth were aerobic and a wound was present as
for the cases in this study. The bacteria’s were Streptococcus, Pseudomonas, Proteus, Escherechia
and mixed a flora of bacteriae.
38
Discussion on however common bacterial infection IB is difficult due to the low caseload. Even
tough a high caseload had a wound penetrating the bursae only 25% of cases had a septic process
whereas 50% of these had a bacterial infection. This indicates on the fact that a bacterial infection
might be uncommon even if a penetrating wound into the bursae is present.
Aseptic cases were differentiated by the upcoming of a wound. In cases without a wound, the
prognosis was better without complications and the outcome were preferable. Septic cases were
treated more aggressively, but all cases were treated with endoscopy and systemic treatment. Cases
with infected synovia went through an invasive surgery with debridement with or without
synovectomy, and excessive amounts of lavage. The treatment program was longer for those cases
with infected synovia, and aggressive antibiotic treatment was done in form of RILP and/or IB
injections together with systemic antibiotic treatment.
In the study only direct approach of the endoscope to the bursae was done, this due to the placement
of wounds and the preference of the surgeon and also due to fewer invasions to surrounding tissues.
In cases with tendon tears, the approach could be a bit different due to debridement of these. In the
study of Smith et al (2007) and Haupt et al (2010) a transtechal approach to the navicular bursa was
done in the fact that a dissection through the distal part of the distopalmar recess of the DDFT
sheath was done to reach the bursa. In Inger Fehr and Baxter (1998) direct approach to the calcaneal
bursas was done without damage to the SDFT.

39
CONCLUSIONS
Conclusion of tasks
1. In thestudya largepercentage(87,5%)ofcasescameback to theiroriginal training
formafter surgery.As seen in the results, theprognosisofasepticbursitis isofhigh
satisfactory outcome while the septic cases had a lower satisfactory outcome and
neededmoreaggressivetreatment.
2. Some changes couldbe seen in the treatment of septic and aseptic cases of bursitis,
whereastheasepticcasescouldbetreatedsystemicallyonly,whilesepticcaseswere
treatedmoreaggressively,especiallythebacterialinfluencedcases.
3. Inthestudy,all16casesweretreatedwithadirectapproachtothebursa.Themost
commonportalswereplacedinaproximallateralormedialdirectiontothebursae.A
transtechalapproachcouldbedoneincaseswerethepenetratingwoundwasusedas
aportal,andthiswoundpenetratesthroughanytissueormembrane.
4. Acommunicationbetween ICBandGCBwereobserved in56%of caseswhereboth
bursaswereinvolvedwithsynovitis.
5. Inthestudy,12,5%ofcaseshadabacterialsepsisIBwithaninfectionofactinobacillus,
streptococcusandmixedbacterialgrowth.
6. Cases with septic bursitis had worse prognosis but with aggressive treatment the
outcome could be satisfactory. Septic bursitic cases had more complications and
neededlongerhospitalizedperiod,andanaggressivetreatmentprogramtogetherwith
a longer convalescence period than aseptic cases. But 50% of horses with septic
bursitiscamebacktofullathletictrainingform.
7. Differentiations between the antibiotic treatment applications of septic VS aseptic
bursitis were done due to the severeness of the synovitis. The IB injection is more
precise and gives a higher concentration of the antibiotics directly into the luminal
cavityofthebursae.

40
RECOMMENDATION
As the results and conclusion refers to, an endoscopic approach should be applied in the treatment
of septic and aseptic bursitis and the pathology should be considered a surgical emergency for the
best outcome possible. Septic cases needs to be treated more aggressively than aseptic bursitis, and
cases with presence of a penetrating wound should be considered septic, but a synoviocentesis is
preferable to be used as differentiation and to estimate prognosis.

41
ACKNOWLEDGEMENT
This study is based on one especially interesting case where both hind limbs were infected in the
ICB bilateral, the prognosis was very bad due to the innervation of two endoscopic surgeries and a
mixed bacterial growth bilateral together with an extreme case of hair contamination intra luminal
in ICB bilaterally. The case had touch many hearts as a raise of money for the cause was done to
enable a second operation for the horse, which came back to full athletic training form after the
procedure. This case was very interesting and I am privileged to have been assisting in both
surgeries of the case and to have been able to do a follow up of the case and to happily announce
the full recovery of the case in the end. I want to thank all nurses working in the operation room of
UDS equine clinic in Uppsala, Sweden and their talented surgeons. The help of my supervisor
Giedrė Vokietytė-Vilėniškė, DVM and lector in equine anatomy and osteopathy completed the
study.

42
LITERATURE LIST
1. König, Liebich. Veterinary anatomy of domestic mammals. Veterinary anatomy of domestic mammals. Munich : Schattauer, 2014, s. 254. 2. MJ, Shively. Correct anatomic nomenclature for the joint of equine tarsus. Equine sports medicine program and department of anatomy and physiology , Auburn university. Auburn : John Schumancher, Ray Wilhite, 2012. PhD thesis. 3. Kathryn A. Seabaugh, DVM, MS, Diplomate ACVS and ACVSMR and Gary M. Baxter, VMD, MS, Diplomate ACVS. Veterian Key. Veterian Key. [Online] den 05 09 2017. [Citat: den 31 08 2019.] Veteriankey.com. 4. Post EM, Singer ER, Clegg PD. Retrospective study of 24 cases of septic calcaneal bursitis in the horse. u.o. : Equine vet J, 2010. ss. 662-668, PhD Thesis. 5. Traumatic subcutaneous calcaneal bursitis (crapped hock) in the horse. Riley, Van Pelt and. u.o. : J. Am. Vet. med. Ass, 1968, ss. 1176-1180. 6. Sisson, S. and Grossman, J.D. The muscles of the leg and foot. [bokförf.] S. sisson and J.D Grossman. The anatomy of domestic animals. Philadelphia : W.B. Saunders Co., 1974, ss. 364-370. 7. Clinically important structures of the equine hock. Sack W.O and Ferraglio, S. 1978, ss. 172, 277-280. 8. retrospective study of 24 cases of septic calcanean bursitis i the horse. Post, E.M., Singer, E.R, Clegg P.D. 2010, Equine veterinary journal, ss. 662-668. 9. treatment and prognosis of cunean tendon bursitis-tarsitis of standardbred horses. A.A., Gabriel. 1979, J Am vet assoc, ss. 175, 1086-1088. 10. An anatomic study of the calcaneal bursae in the horse. POST. EM, Singer, Glegg. 2007, ss. 6-8. 11. —.Post, E.M., Singer, E.R. and Clegg. 2007, Vet surg J, ss. 224, 264-270. 12. Computed tomographic anatomy of the equine tarsus. Tomlinson JE, Redding WR, Berry C. 2003, Vet radiol ultrasound, ss. 44, 174-178. 13. Endoscopy of the calcaneal bursa in horses. Ingle-Fehr, J.E and Baxter, G.M. 1998, Veterinary surgery, ss. 661-567. 14. endoscopy of the navicular bursae: a new technique for the treatment of contaminated and septic bursae. WRIGHT, I.M, PHILLIPS, T.J and WALMSLEY, J.P. 1999, Equine veterinary journal, ss. 31(1) 5-11. 15. VB, Reef. Musculoskeletal ultrasonography. Equine diagnostic ultrasound. Philadelphia : W.W. Saunders, 1998, ss. 39-186.
43
16. puncture wounds of the avicular bursa in 38 horses a retrospective study. RICHARDSON, G.L, O'BRIEN, T.R, PASCOE, J.R, and MEAGHER, D.M. 1986, veterinary surgery, ss. 156-160. 17. Susann Adehed, Karin Bergström, Kerstin Bergvall, Viveca Båverud, Anna Kendall, Christina Greko, Gittan Gröndahl, Carina Ingvast Larsson, Mads Kristoffersen, Oskar Nilsson, Lena Malmgren, Kristina Odensvik, John Pringle, Mia Riihimäki, Lena Ström. Riktlinjer för användning av antibiotika inom hästsjukvård. Uppsala : Sveriges veterinärmedicinska sällskap, 2013. Policies. 18. Forsyth, Sandra. Equine synovial fluid analysis. SVS laboratories. New Zealand : VetScript, 2018. Analysis. 19. Navicular bursoscopy in the horse: A comparative study. Haupt, J.L and Caron, J.P. 2010, Veterinary surgery, no-no, ss. 742-747. 20. Podotrochlear bursa endoscopy in the horse: A cadaver study. Cruz, A.M, Pharr, J.W, Bailey, J.V, Barber, S.M and Fretz. 2001, Veterinary surgery, ss. 539-545. 21. Endoscopic assessment and treatment of lesions of the deep digital flexor tendon in the navicular bursae of 20 lame horses. SMITH, M.R.W., WRIGHT, I.M., and SMITH. 2007, Equine veterinary journal, ss. 18-24. 22. C. Wayne Mcllwraith, Alan J. Nixon, Ian M. Wright, Dr. K. Josef Boening. Diagnostic and surgical arthroscopy in the horse. Diagnostic and surgical arthroscopy in the horse. Toronto : mosby elsevier, 2005, ss. 409-426, 437. 23. Results. Whitcomb, Mary Beth. 2006, Ultrasonography of the equine tarsus, ss. 26-29. 24. Bassage 2, L.H, Ross, M.W. Diagnostic anelgesia. [bokförf.] Dyson, S.J M.W. Ross. Diagnosis and management of lameness in the horse. Philadelphia : Saunders, 2003, ss. 93-124. 25. Wissdorf, H., Hertsch, B,. Keller, H, Stadtbäumer, G. Beckenglidemaße: Hintermittelfuß-, Tarsal- und Knieberich. [bokförf.] Gerhards H, Huskamp, B,. Deegen, E. H. Wissdorf. 2 ed. Anatomie und Propädeutik des Pferdes. Hannover : Verlag M. u. H. Scharper Alfeld, 2002, ss. 528, 546, 570. 26. Osteomyelitis of the calcaneus in horses: 28 cases. MacDonald MG, Honnas CM, Meagher DM. 1989, J Am Vet Med Assic, ss. 194:1317-1327, .

44
ANNEX 1
Diagnose code Outcome Gender Horse Type Calendar Year Year at trauma
MB71 Treatment Mare Sport horse 2017 8
MB71 Treatment Gelding Sport horse 2018 15
MB71 Treatment Mare Sport horse 2018 15
MB71 Treatment Mare Sport horse 2018 15
MB71 Euthanasia Gelding Trotter 2017 4
MB71 Treatment Mare Sport horse 2018 6
MB71 Treatment Mare Sport horse 2018 6
MB71 Treatment Mare Pony 2017 14
MB71 Treatment Mare Pony 2017 14
MB71 Treatment Mare Pony 2017 14
MB71 Treatment Mare Pony 2017 14
MB71 Treatment Mare Sport horse 2017 0
MB71 Treatment Mare Sport horse 2017 0
MB71 Treatment Mare Sport horse 2017 0
MB71 Treatment Gelding Pony 2018 11
MB71 Treatment Gelding Pony 2018 11
MB71 Treatment Gelding Pony 2018 14
MB71 Treatment Mare Sport horse 2018 5
MB71 Euthanasia Gelding Trotter 2018 6
MB71 Euthanasia Mare Sport horse 2018 4
MB71 Treatment Mare Sport horse 2018 4
MB71 Treatment Mare Sport horse 2018 4
MB71 Treatment Gelding Sport horse 2018 10
MB71 Treatment Stallion Sport horse 2018 18
MB71 Treatment Mare Sport horse 2018 19
MB71 Treatment Gelding Sport horse 2018 16
MB71 Treatment Mare Sport horse 2018 10
MB71 Treatment Stallion Sport horse 2017 8
MB71 Treatment Gelding Sport horse 2017 13
MB71 Treatment Gelding Sport horse 2018 13
MB71 Euthanasia Gelding Trotter 2018 11
MB71 Treatment Mare Pony 2017 15
MB71 Treatment Mare Sport horse 2017 19
MB71 Treatment Mare Sport horse 2017 19
MB71 Treatment Mare Sport horse 2017 19
MB71 Treatment Mare Sport horse 2018 20
MB71 Treatment Mare Sport horse 2017 19

45
MB71 Treatment Mare Sport horse 2017 21
MB71 Treatment Stallion Sport horse 2018 6
MB71 Treatment Gelding Sport horse 2018 11
MB71 Treatment Gelding Sport horse 2018 12
MB71 Treatment Gelding Sport horse 2018 12
MB71 Treatment Gelding Pony 2018 19
MB71 Treatment Gelding Pony 2018 19
MB71 Treatment Mare Sport horse 2017 4
MB71 Treatment Mare Sport horse 2017 8
MB71 Treatment Mare Sport horse 2017 8
MB71 Treatment Mare Sport horse 2017 8
MB71 Treatment Gelding Sport horse 2017 8
MB71 Treatment Gelding Sport horse 2018 8
MB71 Treatment Gelding Sport horse 2017 7
MB71 Treatment Mare Trotter 2018 2
MB71 Treatment Mare Sport horse 2018 10
MB71 Treatment Mare Sport horse 2018 10
MB71 Treatment Mare Sport horse 2018 10
MB71 Treatment Mare Sport horse 2018 10
MB71 Treatment Stallion Sport horse 2018 3
MB71 Treatment Stallion Sport horse 2018 3
MB71 Treatment Stallion Sport horse 2018 3
MB71 Treatment Stallion Sport horse 2018 3
MB71 Treatment Gelding Sport horse 2017 16
MB71 Treatment Mare Pony 2018 12
MB71 Treatment Gelding Sport horse 2017 13
MB71 Treatment Gelding Sport horse 2018 6
MB71 Treatment Gelding Sport horse 2017 9
MB71 Treatment Mare Pony 2018 14
MB412 Euthanasia Mare Trotter 2018 7
MB412 Treatment Mare Trotter 2018 7
MB412 Treatment Mare Trotter 2018 7
MB412 Treatment Mare Trotter 2017 0
MB412 Euthanasia Mare Trotter 2017 0
MB412 Treatment Stallion Riding horse 2018 10
MB412 Treatment Stallion Sport horse 2018 10
MB412 Euthanasia Mare Sport horse 2017 8
MB422 Euthanasia Mare Pony 2018 9
MB422 Treatment Mare Pony 2017 14
MB422 Euthanasia Mare Pony 2017 14
MB422 Treatment Mare Pony 2017 14

46
MB422 Treatment Mare Pony 2018 14
MB422 Treatment Mare Sport horse 2018 16
MB422 Treatment Mare Sport horse 2018 16
MB422 Treatment Mare Pony 2017 13