Embed Size (px)
Citation preview

CASE REPORT
Epstein–Barr virus expression in plasma cell neoplasmsand its association with plasmablastic morphologic features
Whitney Pasch & William Wu & Dylan Bach &
Nagesh Rao & Xiaohui Zhao & Sherif A. Rezk
Received: 4 October 2012 /Accepted: 18 March 2013# Springer-Verlag Berlin Heidelberg 2013
Abstract Plasma cell neoplasms include plasma cell mye-loma, plasmacytoma, primary amyloidosis, and light andheavy chain deposition diseases. Epstein–Barr virus (EBV)expression has rarely been reported to be associated withplasma cell neoplasms except for patients with a previoushistory of transplantation or severe immunodeficiency. Incontrast, EBV expression has been reported in the majorityof plasmablastic lymphoma, a subtype of diffuse large B celllymphoma. We report three cases with a plasma cell neo-plasm (two plasma cell myelomas and one case ofplasmacytoma), where EBV infection was diffusely detectedby in situ hybridization. All three patients were under theage of 40 years, and one of the three patients was an HIV-positive individual while the other two patients did not haveany identifiable source for immunosuppression. All threecases showed multifocal plasmablastic features, which isconcordant with the most recent reports about the possibleassociation of EBV expression with plasmablastic morpho-logic features and increased proliferative activity.
Keywords Epstein–Barr virus . Plasma cell neoplasms .
Plasmablastic features
Introduction
Plasma cell neoplasms encompass a spectrum of plasma celldisorders that include plasma cell myeloma, plasmacytoma,primary amyloidosis, and light and heavy chain depositiondiseases [1, 2]. They are characterized by a monoclonal prolif-eration of immunoglobulin-producing plasma cells that repre-sent post-germinal center, terminally differentiated Blymphocytes [1, 2]. Two types of plasmacytomas are recog-nized in the 2008 World Health Organization (WHO) classifi-cation: solitary plasmacytoma of bone (osseous plasmacytoma)and extraosseous plasmacytoma (extramedullaryplasmacytoma) [1, 2]. Solitary plasmacytoma of bone usuallypresents as a lytic lesion involving the axial skeleton andfrequently progresses to plasma cell myeloma in up to two-thirds of the patients, while the extramedullary type has apredilection for the upper aerodigestive tract and has a moreindolent clinical behavior with only 15 % progressing to anovert plasma cell myeloma [1, 2].
True plasma cell neoplasms have been rarely reported to beassociated with Epstein–Barr virus (EBV) expression.Plasmablastic lymphoma, a subtype of diffuse large B celllymphoma with near-identical immunophenotype to plasmacell neoplasms, has been reported to show EBVexpression inabout two-thirds of the cases and near 100 % expression in theoral mucosa subtype [3, 4]. Post-transplant patients and se-verely immunocompromised patients, especially patients withestablished HIV infection, have been reported to have slightlyincreased incidence for EBV-positive plasma cell neoplasmsalthough the cytomorphologic features of the neoplastic cellsin such cases have been mainly described as plasmablastic oranaplastic [2, 5]. Plasmablastic cytomorphologic features aredefined as plasma cells having larger concentrically placednucleus with little or no cytoplasmic hof and exhibiting openor coarse chromatin, prominent nucleoli (usually central), and
W. Pasch :W. Wu :D. Bach :X. Zhao : S. A. RezkDepartment of Pathology & Laboratory Medicine, University ofCalifornia, Irvine (UCI), Irvine, CA, USA
N. RaoDepartment of Pathology & Laboratory Medicine, University ofCalifornia, Los Angeles (UCLA), Los Angeles, CA, USA
S. A. Rezk (*)Department of Pathology, University of California Irvine MedicalCenter (UCI), 101 The City Drive, Bldg 54, Rm 4702,Orange, CA 92867, USAe-mail: [email protected]
J HematopatholDOI 10.1007/s12308-013-0180-1

less abundant cytoplasm [6]. The anaplastic cytomorphologicfeatures are defined as plasma cells with a hyperchromaticnuclei and more pleomorphic appearance with irregular nu-clear and cytoplasmic contours [7]. Plasma cell myelomapatients with plasmablastic or anaplastic morphology tend tohave a more aggressive clinical course and are generallyconsidered to carry a more guarded prognosis [2]. We reportthree cases with a plasma cell neoplasm (two plasma cellmyelomas and one case of plasmacytoma), where EBV ex-pression was diffusely detected by in situ hybridization. Allthree patients were under the age of 40 years, and oneof the three patients was an HIV-positive individualwhile the other two patients did not have any identifi-able source for immunosuppression.
Clinical history, methods, and results
Case 1
A 39-year-old Hispanic male presented to the emergencyroom in early 2012 with a 2-month history of abdominalpain radiating to his back and with leg numbness for 2 daysprior to presenting to the hospital. His past medical historywas unremarkable except for hypothyroidism. A computedtomography (CT) and magnetic resonance imaging bonescans revealed lytic bony lesions at the cervical, thoracic,and lumbar spine as well as at the skull and left rib. A biopsyof the thoracic lesion revealed sheets of kappa-restrictedplasma cells that showed strong expression of EBV by insitu hybridization (EBV-encoded RNA (EBER)) with asmall subset expressing EBV-latent membrane protein 1(LMP-1) by immunohistochemistry. The neoplastic plasmacells showed lack of expression for the B cell markers CD20and PAX-5 as well as for cyclin D1, CD56, and humanherpesvirus 8 (HHV-8). Focal plasmablastic features werenoted on morphologic examination and an overall low Ki-67proliferative activity was noted (10 %) although theplasmablastic areas showed slightly increased proliferativeactivity. The intensity of staining and percentage of EBER-positive cells were similar in both areas. Subsequent biop-sies from the cervical spine and a right parietal mass showedan identical process with a similar immunophenotype. Abone marrow biopsy was performed and showed a slightlyhypocellular marrow with active trilineage hematopoiesisand no evidence of involvement by a plasma cell neoplasm.EBER stain showed negative results when performed on thebone marrow clot biopsy sections. EBV serology testingwas not performed. Cytogenetic studies performed on thebone marrow aspirate showed a normal male karyotype.Fluorescence in situ hybridization (FISH) with the dual-color MYC “split” probe was unsuccessful due to the de-calcification method used to fix the cells but hinders DNA
probe hybridization and the visualization of the fluorescentsignals. HIV testing by serology showed negative results.Serum protein electrophoresis showed a prominent beta-restricted band quantitated at 1.29 g/dl and was identifiedas an IgA kappa paraprotein by immunofixation. Urineelectrophoresis and immunofixation showed free kappalight chains. Laboratory tests showed mild leukopenia, hy-percalcemia, elevated serum free light chains, and elevatedIgA levels. The patient also had mild anemia and mildthrombocytopenia. The patient’s mental status rapidly de-clined and a lumbar puncture was performed, which re-vealed involvement of the cerebrospinal fluid by theneoplastic plasma cells having the same morphological pic-ture as the previous biopsy. The patient is currently receiv-ing radiation therapy and has shown relative overallimprovement despite the persistence of the monoclonalparaproteins in his serum.
Case 2
A 39-year-old Hispanic female who was diagnosed withHIV in 2000 presented to our institution in early 2008 withabdominal pain and distension for 5 days prior. Her CD4+ Tcell count at presentation was 47 cells/μL. Multiple diffusebony lesions were visualized on skeletal survey in additionto several ovarian and liver masses. An ultrasound-guidedfine needle aspiration biopsy of the liver mass showedsheets of kappa-restricted plasma cells that express CD138and CD56 by immunohistochemistry. The neoplastic plasmacells were negative for EBV-LMP-1, HHV-8, and cyclin D1stains. By in situ hybridization, the neoplastic plasma cellswere EBV (EBER) positive. EBV serology testing was notperformed. Serum protein electrophoresis showed a bandwith restricted mobility in the fast gamma region that wasquantitated at 3.25 g/dl. Immunofixation revealed an IgAkappa and IgG kappa biclonal gammopathy. Her urine pro-tein electrophoresis showed free kappa light chains. A bonemarrow biopsy from bilateral iliac crests showed 70–80 %marrow involvement by the neoplastic myeloma cells thatexhibited anaplastic and plasmablastic features and demon-strated CD138 and kappa light chain expression by immu-nohistochemistry and flow cytometry. A subset of theneoplastic plasma cells within the bone marrow was positivefor EBER stain. Cytogenetic studies performed on the bonemarrow aspirate showed a normal female karyotype. FISHwith dual-color MYC split probe did not yield unambiguousfluorescent signals. The patient succumbed to the disease2 months later after complications from myeloma.
Case 3
A 38-year-old Caucasian male presented to our institute inlate 2000 with altered mental status and epistaxis. A CT scan
J Hematopathol

of the head and neck revealed a lesion in the right nasalcavity extending into the right frontal lobe. A subsequentskeletal survey revealed multiple lytic bony lesions through-out the body. Laboratory testing showed elevated serumBUN and creatinine in addition to normocytic anemia. Test-ing for HIV-1 and HIV-2 by polymerase chain reaction(PCR) showed negative results. Serum protein electropho-resis showed a band in the fast gamma region that wasquantitated at 1.25 g/dl. Immunofixation showed an IgGkappa monoclonal paraprotein. A free kappa light chainband was demonstrated in the urine by immunofixation aswell. A biopsy of the rapidly growing nasal lesion revealedsheets of kappa-restricted plasma cells that exhibitedplasmablastic morphology in many areas although areas ofplasma cells with normal morphology were also seen. EBVstudies by in situ hybridization (EBER) showed positivity inthe vast majority of the neoplastic plasma cells includingthose with normal and plasmablastic morphologic features.The intensity of staining and percentage of EBER-positivecells were relatively similar in both areas (Fig. 1). Theneoplastic cells were negative for EBV-LMP-1, HHV-8,cyclin D1, and CD56 by immunohistochemistry. A bonemarrow biopsy of the iliac crest showed a normocellularmarrow with active trilineage hematopoiesis and no evi-dence of involvement by clonal plasma cells. EBER stainshowed negative results when performed on the bone mar-row clot biopsy sections. Attempts to obtain MYC gene
status by dual-color FISH were unsuccessful. The patientunderwent treatment with vincristine, doxorubicin, anddexamethasone with pamidronate and radiation therapy butdid not show initial response to treatment and was ultimatelylost to follow-up and his living status is unknown.
Discussion
In contrast to plasmablastic lymphomas, true plasma cellneoplasms have been rarely associated with EBV infectionalthough post-transplant patients and severely immunocom-promised patients may have slightly increased incidence ofhaving an EBV-positive plasma cell neoplasm [2, 5]. Thedistinction of plasmablastic lymphoma from plasma cellmyeloma or plasmacytoma with plasmablastic features canbe difficult at times and usually depends on clinical corre-lation with the presence of serum monoclonal paraproteins,bone marrow involvement, and radiographically evidentlytic lesions, which are all factors that would favor plasmacell myeloma with plasmablastic features [7, 8]. Althoughthe expression of EBV and a positive HIV status have beenhistorically associated with a diagnosis of plasmablasticlymphoma, other more reliable factors have been postulatedto support a diagnosis of plasmablastic lymphoma overmyeloma such as markedly increased mitotic activity, pres-ence of numerous apoptotic bodies, and paucity of maturing
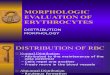
Fig. 1 The composite picture represents two different fields from case3. The upper half shows sheets of neoplastic plasma cells that show noatypical features. a Low-power magnification (×10) of the plasma cellsand b high-power magnification (×40). c EBER expression (EBV by insitu hybridization) (×40) and d Ki-67 expression shows minimal pro-liferative activity (×40). The lower half of the composite picture shows
sheets of plasma cells with atypical and plasmablastic features and ahigher proliferative activity. e Low-power magnification (×10) of theatypical plasma cells and f high-power magnification (×40). gEBER expression (×10) and h Ki-67 expression shows increasedproliferative activity than the areas without the plasmablasticfeatures (×40)
J Hematopathol

Tab
le1
Review
ofEBV-positive
plasmacellneop
lasm
casesin
correlationwith
plasmablastic
morph
olog
y
Cases
Age
Sex
Diagn
osis
Immun
estatus
Mcompo
nent
Plasm
ablastic
features
CNSlesion
sDisease
course
Com
ments
Chang
etal.[5],
firstcase
40M
Extraosseou
splasmacytom
aCom
petent
Absent
Yes
ND
F/U
for6years
show
sremission
All4caseswereEBERpo
sitiv
eand
LMP-1
negativ
eexcept
foron
ecase
that
was
focally
positiv
eforLMP-1
Chang
etal.[5],
second
case
27M
Plasm
acellmyeloma
Com
petent
IgG
No
ND
Diedof
diseasein
6years
Chang
etal.[5],
thirdcase
60M
Plasm
acellmyeloma
Com
petent
IgG
Yes
ND
Diedof
diseasein
8years
Chang
etal.[5],
fourth
case
51M
Plasm
acellmyeloma
Com
petent
IgG
Yes
ND
Diedof
diseasein
1year
Qinget
al.[12]
69M
Plasm
ablastic
lymph
oma
transformingfrom
plasmacytom
a
Com
petent
Absent
Yes,mainlyplasmablastic
with
adjacent
mature
mon
oclonalplasmacells
No
Patient
alivebu
twith
disease
prog
ression
EBERpo
sitiv
ein
plasmablastic
cells,
while
theclon
almatureplasmacells
arenegativ
e
Sasakiet
al.[10]
62M
Plasm
acellmyeloma
Com
petent
IgA
Yes,in
themaxillarysinu
stumor
while
bone
marrow
show
edno
n-plasmablastic
morph
olog
y
No
Patient
respon
sive
tofirstcycleof
intensive
chem
otherapy
EBERpo
sitiv
ein
maxillarylesion
with
plasmablastic
features,while
negativ
ein
themarrow
with
nonp
lasm
ablastic
morph
olog
y
Wuet
al.[11]
40M
Extraosseou
splasmacytom
aSup
pressedHIV
+Absent
Yes,focal
Yes
Patient
sent
toho
spicein
less
than
ayear
EBERpo
sitiv
e,LMP-1
stainnegativ
e
Current
repo
rt,
firstcase
39M
Plasm
acellmyeloma
Com
petent
(mild
leuk
openia)
IgA
Yes,admixed
with
nonp
lasm
ablastic
areas
Yes
Patient
aliveafter
1year
butwith
deteriorationof
clinical
status
EBERpo
sitiv
e,LMP-1
stainpo
sitiv
e
Current
repo
rt,
second
case
39F
Plasm
acellmyeloma
Sup
pressedHIV
+BiclonalIgA
andIgG
Yes,admixed
with
nonp
lasm
ablastic
areas
No
Diedof
diseasein
2mon
ths
EBERpo
sitiv
e,LMP-1
stainnegativ
e
Current
repo
rt,
thirdcase
38M
Multip
leplasmacytom
as(osseous
and
extraosseous)
Com
petent
IgA
Yes,admixed
with
nonp
lasm
ablastic
areas
Yes
NoF/U
available
EBERpo
sitiv
e,LMP-1
stainnegativ
e
ND
notdescribed
J Hematopathol

plasma cells [7]. Vega et al. have postulated in their studythat EBV expression constitutes the differentiating factorbetween plasma cell neoplasms and plasmablastic lympho-ma, where the latter show EBVexpression in the majority ofcases [3]; however, others have reported the detection ofEBV in extramedullary plasmacytoma of the head and neckin immunocompetent individuals in up to 15 % of all cases[9]. Moreover, other investigators have reported the identi-fication of EBV expression in immunocompetent patientswith plasma cell myelomas and plasmacytomas, where theplasma cells in these cases exhibited plasmablastic morphol-ogy, and they concluded that the presence of EBV in plasmacell neoplasms is significantly associated with plasmablasticmorphologic features suggesting that these tumors may havebeen driven by EBV to gain the plasmablastic morphologicfeatures and a higher proliferation rate [5, 10–12]. Also, theidentification of EBV expression in a subtype of patientswith plasmablastic lymphoma that occurred as a result ofplasma cell myeloma progression/transformation has beenreported [13]. A more recent study has identified EBVexpression by PCR in 33 % of bone marrows with plasmacell myeloma compared to only 10 % of normal bonemarrow specimens [14], although the results may not betruly representative due to small sample size and the ethnic-ity of patients.
In healthy individuals who are seropositive for EBV,terminal differentiation of EBV-infected memory B cellsinto plasma cells has been reported to be associated withviral replication and initiation of the EBV productive (lytic)cycle [15, 16]. In contrast, individuals with plasmacytoidtumors frequently associated with EBV such as primaryeffusion lymphoma or plasmablastic lymphoma have beenshown to establish a nonproductive (latent) cycle and ex-hibit a restrictive EBV latency pattern (latency I/II) [16, 17].In addition, a strong reduction in plasma cell-associatedmarkers such as CD38 and CD138 and a regression to aless mature B cell phenotype were observed in the EBV-infected plasmacytoid tumor cells as well as in few plasmacell myeloma cell lines examined in vitro [16]. As such,plasma cell myeloma or plasmacytoma cases that expressEBV, whether as a result of an associated immunodeficiencyor for unknown reasons, may follow the same path asplasmablastic lymphoma and exhibit a non-productive(latent) cycle, increase proliferation, and exhibit plasmablasticcytologic features starting in focal areas and probably eventu-ally progressing to plasmablastic lymphoma.
Despite the fact that plasma cell neoplasms occur rarelyin young individuals with the vast majority of cases occur-ring over the age of 50 and a median age at diagnosis of70 years for plasma cell myeloma and 55 years forplasmacytoma (osseous and extraosseous) [2, 18], all threeof our patients were under the age of 40 years at diagnosisand all three had presented with a very aggressive clinical
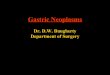
course including involvement of the central nervous system(CNS) in two cases. All three patients presented with mor-phologic evidence of a plasmablastic morphology whetherwithin the majority of cells or within a subset of the neo-plastic plasma cells. One patient was HIV positive, while theother two showed no definitive evidence of an associatedimmunosuppressive state. All three of our cases showed noreduction in CD138 expression and two out of the threecases were negative for EBV-LMP-1 expression by immu-nohistochemistry but positive for EBER by in situ hybridi-zation, which is suggestive of a restricted EBV latencypattern, probably latency I. Based on our case series andother cases reported in the literature (Table 1), there may beindeed a notable correlation between EBV expression andthe presence of plasmablastic morphologic features aswell as with increased proliferative activity and a po-tential aggressive clinical course compared to the rela-tively more indolent and prolonged clinical courseusually seen in EBV-negative plasma cell neoplasmcases, especially plasmacytomas. The EBV role maybe through alternate pathway other than the LMP-1protein-related neoplastic transformation. Further studieswith a larger series of cases are needed to validate thesefindings.
Conflict of interest The authors declare that they have no conflict ofinterest.
References
1. Lorsbach RB, His ED, Dogan A, Fend A (2011) Plasma cellmyeloma and related neoplasms. Am J Clin Pathol 136(2):168–182
2. McKenna RW, Kuehl WM, Grogan TM, Harris NL, Coupland RW(2008) Plasma cell neoplasms. In: Swerdlow SH, Harris NL, JaffeES, Pileri SA, Stein H, Thiele J, Vardiman JW (eds) WHO classi-fication of tumors of hematopoietic and lymphoid tissues. IARC,Lyon, pp 200–214
3. Vega F, Chang CC, Medeiros LJ, Udden MM, Cho-Vega JH, LauCC, Finch CJ, Vilchez RA, McGregor D, Jorgensen JL (2005)Plasmablastic lymphomas and plasmablastic plasma cell myelo-mas have nearly identical immunophenotypic profiles. Mod Pathol18(6):806–815
4. Stein H, Campo E (2008) Plasmablastic lymphoma. In: SwerdlowSH, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, VardimanJW (eds) WHO classification of tumors of hematopoietic andlymphoid tissues. IARC, Lyon, pp 256–258
5. Chang ST, Liao YL, Lu CL, Chuang SS, Li CY (2007)Plasmablastic cytomorphologic features in plasma cell neoplasmsin immunocompetent patients are significantly associated withEBV. Am J Clin Pathol 128(2):339–344
6. Greipp PR, Raymond NM, Kyle RA, O'Fallon WM (1985)Multiple myeloma: significance of plasmablastic subtype in mor-phological classification. Blood 65(2):305–310
J Hematopathol

7. Dong HY, Scadden DT, de Leval L, Tang Z, Isaacson PG, HarrisNL (2005) Plasmablastic lymphoma in HIV-positive patients: anaggressive Epstein-Barr virus-associated extramedullaryplasmacytic neoplasm. Am J Surg Pathol 29(12):1633–1641
8. Taddesse-Heath L, Meloni-Ehrig A, Scheerle J, Kelly JC, Jaffe ES(2010) Plasmablastic lymphoma with MYC translocation: evi-dence for a common pathway in the generation of plasmablasticfeatures. Mod Pathol 23(7):991–999
9. Aguilera NS, Kapadia SB, Nalesnik MA, Swerdlow SH (1995)Extramedullary plasmacytoma of the head and neck: use of paraffinsections to assess clonality with in situ hybridization, growth fraction,and the presence of Epstein-Barr virus. Mod Pathol 8(5):503–508
10. Sasaki S, HashimotoK, Nakatsuka S, HasegawaM,Nakano T, NagataS, Kanakura Y, Hayashi N (2011) Plasmablastic extramedullaryplasmacytoma associated with Epstein-Barr virus arising in an immu-nocompetent patient with multiple myeloma. Intern Med50(21):2615–2620
11. Wu W, Pasch W, Zhao X, Rezk SA (2012) Extraosseousplasmacytoma with an aggressive course occurring solely in theCNS. Neuropathology. doi:10.1007/s00277-013-1722-4
12. Qing X, Sun N, Chang E, French S, Ji P, Yue C (2011) Plasmablasticlymphoma may occur as a high-grade transformation fromplasmacytoma. Exp Mol Pathol 90(1):85–90
13. Colomo L, Loong F, Rives S, Pittaluga S, Martinez A, Lopez-Guillermo A, Ojanguren J, Romagosa V, Jaffe ES, Campo E(2004) Diffuse large B-cell lymphomas with plasmablastic differ-entiation represent a heterogeneous group of disease entities. Am JSurg Pathol 28(6):736–747
14. Sadeghian MH, Ayatollahi H, Keramati MR, Memar B, JamedarSA, Avval MM, Sheikhi M, Shaghayegh G (2011) The associationof Epstein-Barr virus infection with multiple myeloma. Indian JPathol Microbiol 54(4):720–724
15. Anastasiadou E, Vaeth S, Cuomo L, Boccellato F, Vincenti S,Cirone M, Presutti C, Junker S, Winberg G, Frati L, WadePA, Faggioni A, Trivedi P (2009) Epstein-Barr virus infectionleads to partial phenotypic reversion of terminally differenti-ated malignant B cells. Cancer Lett 284(2):165–174
16. Laichalk LL, Thorley-Lawson DA (2005) Terminal differentiationinto plasma cells initiates the replicative cycle of Epstein-Barrvirus in vivo. J Virol 79(2):1296–1307
17. Rezk SA, Weiss LM (2007) Epstein-Barr virus-associatedlymphoproliferative disorders. Hum Pathol 38(9):1293–1304
18. International Myeloma Working Group (2003) Criteria for theclassification of monoclonal gammopathies, multiple myelomaand related disorders: a report of the International MyelomaWorking Group. Br J Haematol 121(5):749–757
J Hematopathol