Embed Size (px)
Citation preview

CORRESPONDING AUTHOR
ALBANY MEDICAL COLLEGE
ALBANY MEDICAL CENTER
OBJECTIVE
INTRODUCTION
CASE REPORT
DISCUSSION IMAGES
Optimal management of frontal sinus fractures continues to be a controversial issue. Advances in endoscopic technology as well as development of less morbid techniques has led to a shift away from open surgical management of frontal sinus. We present an uncommon case of nasocutaneous fistula after a delayed diagnosis of frontal sinus posterior table fracture resulting in outflow tract obstruction. Through a transnasal endoscopic Draf III approach, we successfully restored outflow tract function and the repair of the nasocutaneous fistula utilizing a free mucosal graft.
To review a case of nasocutaneous fistula formation after frontal sinus fracture.
CONCLUSIONS
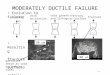
This is a 21 year-old male with a history of a recurrent left periorbital abscess. Four months prior, he was assaulted and sustained a nasal laceration that became infected and was treated with debridement and intravenous antibiotics by another service. After discharge, the wound continued to swell and drain. On exam, a hyperemic and edematous region of the left nasal dorsum skin was spontaneously draining purulent secretions from an area of necrosis. CT revealed a significantly displaced and dehiscent left frontal sinus posterior table fracture with obstruction of the outflow tract, mucosal thickening, and bony erosion of the frontal process of the maxilla with contiguous soft tissue fullness anterior to the frontal sinus and dorsum (Figure 1).
Frontal sinus fractures account for 5-15% of all facial fractures.1 Involvement and/or displacement of the anterior and posterior tables, obstruction of the frontal outflow tract, and intracranial injury should be determined. Successful management requires creation of a safe sinus while preserving function and cosmesis. Early complications encompass infectious processes (e.g. meningitis, cerebral abscess, osteomyelitis) and CSF leak. Late complications include mucoceles, mucopyoceles, cerebral abscesses, encephaloceles, and cosmetic defects. Nasocutaneous fistula has never been described in the literature as a sequela of frontal sinus fractures.
Figure 1. Preoperative CT: A) Left frontal sinus fracture B) Outflow tract obstruction with bony fragment and mucosal thickening; dehiscence between sinus and dorsum C) Fragment in left frontal sinus D) Posterior table fracture with dehiscence E) Fragment obstructing outflow tract. Another view of dehiscence between sinus and dorsum F) Fracture and dehiscence of anterior table/floor.
Figure 2. Intraoperative findings A) Bony fragment from posterior table impeding outflow tract B) Bony fragments after endoscopic removal C) Final view after Draf III frontal sinusotomy with reestablishment of outflow tract.
SURGICAL TECHNIQUE The patient underwent endoscopic endonasal exploration of the anterior skull base and Draf III frontal sinusotomy. The outflow tract was obstructed by displaced bony fragments originating from the posterior table (Figure 2). Posterior to these fragments, purulent drainage in the frontal sinus communicated with a cutaneous fistula tract to the left nasal sidewall. Pulsation was visualized in the dehiscent region of the posterior table and frontal lobe dura was mucosalized with no evidence of CSF leak. A free mucosal graft was harvested from the nasal floor and positioned at the frontal recess beak, covering the anterior table, frontal sinus, and internal portion of the soft tissue wound. A steroid-eluting stent was then placed in the outflow tract. Postoperatively, the patient was aggressively managed with saline irrigations and antibiotics. On evaluation in clinic, the external portion of the fistula had healed. Endoscopic exam revealed an appropriately positioned free mucosal graft and absence of purulent discharge.
The goals of treatment of frontal sinus injuries have remained relatively steadfast but debate around treatment algorithms continues.5 Traditionally, obliteration or cranialization was proposed for recess or outflow tract injuries. However, recent authors advocate a more conservative approach. A similar debate revolves around management of mild-moderately displaced posterior table fractures.1
Unrecognized frontal recess injury can occur in ⅓ or more of frontal sinus trauma, commonly resulting in long-term sequelae.2 Identification of outflow tract fractures is difficult. Thin-section CT can help, as in our case, but no pathognomonic signs are agreed upon. Previous authors proposed aggressive management of fractures involving the floor or anterior ethmoid as these injuries increase the risk of outflow obstruction.3 However, other series did not find preoperative CT to be an accurate predictor of outflow tract function in the absence of NOE fracture. 2 Though nasocutaneous fistula is recognized as a complication of chronic sinusitis or radiation, it is an uncommon development after frontal sinus fracture. To our knowledge, it has not been reported in the literature after frontal sinus injury. We performed an endoscopic approach to repair the outflow tract and fistula. This offers benefits over open approaches. Transnasal drainage avoids risk of injury to supratrochlear and supraorbital nerves (avoiding forehead hypoesthesia, neuralgia, and frontal headache) and postoperative assessment is readily accomplished with endoscopic examination or CT. These modalities are less helpful after obliteration as the sinus no longer communicates with the nasal passages and imaging studies become difficult to interpret.2,4
References 1. Guy WM, Brissett AE. Contemporary management of traumatic fractures of the frontal sinus. Otolaryngol Clin North Am 2013;46:733-48. 2. Smith TL, Han JK, Loehrl TA et al. Endoscopic management of the frontal recess in frontal sinus fractures: a shift in the paradigm? Laryngoscope 2002;112:784-90. 3. Heller EM, Jacobs JB, Holliday RA. Evaluation of the frontonasal duct in frontal sinus fractures. Head Neck 1989;11:46-50. 4. Seiden AM, Stankiewicz JA. Frontal sinus surgery: the state of the art. Am J Otolaryngol 1998;19:183-93. 5. Fox, PM, Garza R, Dusch M et al. Management of frontal sinus fractures: treatment modality changes at a level I trauma center. J Craniofac Surg 2014;25:2038-42.
Nasocutaneous fistula: a rare complication of frontal sinus posterior table fracture
Tiffany Chen MD1, Kristina Piastro MD1, Tyler Kenning MD2, Carlos D. Pinheiro-Neto MD PhD1 1 Division of Otolaryngology Head and Neck Surgery, Department of Surgery, Albany Medical Center, Albany, New York.
2 Department of Neurosurgery, Albany Medical Center, Albany, New York.
Carlos D. Pinheiro-Neto, MD PhD
Division of Otolaryngology – Head & Neck Surgery Albany Medical Center 47 New Scotland Avenue MC-41 Albany, NY 12208 Phone: (518) 262-5575 Fax: (518) 262-5184 Email: [email protected]
Surgical VIDEO
www.amc.edu/cranialbase