Embed Size (px)
Citation preview
4560
Age Specific Care For The
Population We Serve
Clinical Guide

Age Specific Care__________________________________________________________________
For the Population We Serve
CLINICAL GUIDE
Every person who enters a healthcare care facility is an individual, and should be treated as such. And yet, as differentas our backgrounds may be, there is often something we have in common: the way we experience growth and development. By understanding the various age-related stages, you will more fully anticipate and meet the physical and psychosocial needs of the population your facility serves. Age Specific Care promotes safety, reduces errors, andenhances the value of the healthcare you provide to your patients and their families.
This Comprehensive Tool is designed to give an overview and guide to each stage of growth and development. It provides hands-on tips, practical examples and helpful insights, as well as clinical information on Vital Signs, PhysicalGrowth Characteristics, Special Considerations, Safety Concerns, Psychosocial Needs, and Patient and Family Education.Please note that because everyone is an individual, your patients may or may not exhibit the characteristics of that stage.Your role is to give full attention to the patient and family in order to meet their needs.
ACKNOWLEDGEMENTS
We would like to express our sincere appreciation to the following individuals
CLINICAL ADVISORS
Janet Cross, M. Ed., CCLSDirector, Child Life Services
Monroe Carell Jr. Children’s Hospital at Vanderbilt
Wanda Faircloth, RN, MSN, CEN, FNP-CEmergency Services
Southeastern Regional Medical CenterAdjunct Faculty
University of North Carolina-Pembroke
Terrell Smith MSN, RNDirector, Patient/ Family Centered Care
Vanderbilt University Hospital and Clinics
© 2008 Envision, Inc.All copyright laws apply.
2

Table of Contents
Neonates/Infants up to 1 Y/O. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 - 5
Toddlers 1-3 Y/O . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 - 7
Pre-School 3-5 Y/O . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 - 9
School Age 5-12 Y/O . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 - 11
Adolescents 13-18 Y/O . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 - 13
Early Adulthood 18-29 Y/O . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Young Adulthood 30-44 Y/O . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Middle Adulthood 45-65 Y/O . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 - 17
Elderly or Geriatric 65+ Y/O. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 - 20
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Post Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22 - 23
Post Test Answers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
3

Vital Signs
Physical GrowthCharacteristics
SpecialConsiderations
Safety Concerns
Temperature 97.90-100° F Respiratory rate initially 40-60 breaths/minute; dropping to 30-40 after first few minutes of life and at 1 yearHeart rate (beats/minute) approximate mean 140 newborns to 3 months; 130 three months to 1 yrSBP 60-76 at birth, increasing to 68-104 at 1 yrDBP 30-45 at birth, 22-60 at 1 yr
• First 4 months centers around the head: smiling, following objects with eyes, maintaining head control and oral activities such as sucking.
• Posterior fontanelle closes by 6 to 8 months; 2 pairs of lateral fontanelles close by second or third month.• Birth weight drops 5-10% in first week of life due to excretion of extracellular fluid. Exceeds birth weight
by second week, doubles weight within 4 to 6 months, triples by one year. Infants head equal to 25% of total body weight.
• Infants have rapid growth in the first year, especially in the brain. They learn through playing, exploring and using their senses.
• Strong coordinated suck and gag reflexes. Extremities move equally when the infant is stimulated.• Between 5 and 7 months, teething begins.• Increased development of the distal limb portions demonstrated by creeping, standing and walking with assistance.• Passive immunity is based on maternal antibodies.• Airways in infants are narrower, shorter, and more easily obstructed. Infants are primarily nose breathers
until 4 weeks of age. Noisy breathing can indicate restricted airflow and the need to reposition the air way.
• Respiratory rate should never be greater than 60 in any child. Rapid respiratory rates can lead to rapid heat and fluid loss. Slow heart rate with signs of poor perfusion may indicate the need for external cardiac compressions.
• Tub baths should only be given after umbilical cord falls off. Infants have sensitive skin that dries easily, so moisturize after the bath while damp to protect the skin. In between baths, keep face and bottom very clean.
• Health-immunization schedules should be followed, as should routine medical screenings.• Observation alone is an essential component of the exam. Be aware of overall mood of infant, general level
of activity, the parent/child interaction, whether the infant is rolling, crawling, etc. and responding to visual and auditory cues.
• A cultural assessment may reveal special arrangements during and after the birth of the child that may include traditions, beliefs or rituals.
Utilize equipment that is specific to size and age.To help prevent the possibility of sudden infant death syndrome (SIDS), remember to lay the infant on their back or side, never on their front.Crib side rails should be kept up at all times.Never leave an infant alone on changing tables, beds, sofas or chairs.Never leave an infant unattended near water.When giving an infant a bath, use water that is warm, never hot or cold. If a toy or detachable piece could fit inside a toilet paper tube, it is unsafe for this age child. Car seat is required.
Safe medication administration:• The rate for potential adverse drug events is 3 times higher in children than adults, and substantially higher
in neonates in intensive care.• Always perform double checks for all high risk medications by making sure you have the right patient, drug, time,
dose and route. Medications should be labeled with drug name and strength.
Age Specific Care For the Population We Serve
4
Neonates/Infants up to 1 Y/O

5
Safety Concerns(Cont’d)
PsychosocialNeeds
Patient/FamilyEducation
• Use ready-to-use (unit dose) form prepared by pharmacy. • To ease administration, draw the medication into a syringe, slide the syringe along the inner cheek
to the back of the mouth, and gently dispense into back of the throat.
Communication:• The child is learning to communicate through facial expressions, crying, cooing, and babbling.
Eventually vocalizes syllable sounds like Ma-ma, Da-da, and imitates adult sounds.• Likes to be held, touched, cuddled, smiled at and talked to.• Cries strongly when hungry or uncomfortable.• Learns to show emotion such as frustration, fear, anger, jealousy, affection.• Approach infant indirectly, never too quickly.• Call the infant by name.
Infant Stress: • Can be brought on by over-stimulation.• Stranger and separation anxiety emerge at 6 to 8 months. • Physical indicators of stress include: the closing of eyes, fretting, turning away, increased formation of stool,
increased motor activity, change in color or hyper-alertness.• Try to assign the same staff to each patient daily.• Encourage parents to stay with the child as much as possible.• To reduce stress when assessing, caring or conducting procedures and to promote development:
– Incorporate the concepts of play into the environment– Attend to physical needs promptly and provide consistency in routines and responses– Social interaction like talking, singing or reading will help to reduce stress– Keep the infant on the parent’s lap if possible
Parental Stress:• Parents often suffer from stress while their child is ill. This stress may be exhibited as anger, hostility,
rudeness, demanding behavior, lack of cooperation, or feeling suspicious toward healthcare staff. • Try to stay calm and show your understanding. • You can relieve stress through flexibility - by modifying care or making changes when possible - and showing
the parent you consider them a partner in the infant’s care.
Bolster the skills of the parents in routine tasks such as feeding, bathing, and changing diapers so that parental confidence in these areas is then transferred to the baby.Promote physical closeness and swaddling with a light blanket. This will help the infant feel safe and promote healthy parental bonding.
Provide education to parents on the following:• Car seats required.• Never leave an infant alone in or near water, on changing tables, sofas or chairs.• Provide a safe environment for exploring and playing. For example, crawl-proof and baby-proof by covering
electrical plates and removing small objects that could be eaten, cords or ropes that could strangle, etc.• Infants younger than 6 months old should not be exposed to direct sunlight, and should use sunscreen
after this age when in the sun. • Encourage proper nutrition, oral health, skin care, and follow immunization and screening schedules.
Age Specific Care For the Population We Serve
Vital Signs
Physical GrowthCharacteristics
SpecialConsiderations
Safety Concerns
Temperature 98.6 to 99.6° FRespiratory rate 24 to 40Heart rate 80 to 130 beats/minuteSBP 68 to 106 DBP 20-65
• Closing of the anterior fontanelle by 15-18 months.• A protruding abdomen of subcutaneous fat.• Muscle mass increases, bone density increases.• An increase in heart size with corresponding decrease in heart rate.• Eruption of all primary teeth by 36 months.• Diaphragmatic breathing.• A vulnerability to fluid volume deficits.• Physical growth slows.• Basic motor skills, effortless walking, developing fine motor skills.• Passive immunity is lost, more susceptible to minor respiratory and gastrointestinal infections.• As exposure to common pathogens occurs, immunity develops.
A respiratory rate should never be consistently greater than 60 breaths/minute in any child.
Medication Administration:• Offer choices if possible. For example, let toddlers choose the timing, such as before or after a bath; or location,
such as on a chair or in their bed. • Some pharmacies offer flavors formulated per physician orders or per parent request. This is a great way
to give the child a choice in their care, and have them take their medicine more easily.
Procedures/Exams:• Provide distraction by making exams and assessments into a game and allowing for choices when
and if appropriate. • Consider performing painful or invasive procedures in the treatment room so the child’s room remains
a safe place.• Areas of focus when assessing the toddler include visual and hearing acuity, speech pattern and clarity,
verbal and motor skills, and emerging independence and associated behaviors.
Utilize equipment that is specific to size and age.The rate for potential adverse drug events is 3 times higher in children than adults. Always perform double checks forall high risk medications by making sure you have the right patient, drug, time, dose and route.Toys must be safe and age-appropriate. Toddlers are incredibly mobile and curious and should be watched very closely. Toddlers explore their world by puttingeverything in their mouths, even if it doesn’t taste good, and are know to open doors and drawers, take things apartand open bottles.A child can drown in a very small amount of water. Never leave any small child unattended when giving a bath, orleave buckets of water or cleaning solutions unattended.When sedating a toddler, remember the airways are much smaller and there is a greater risk of compromise.Adequate airway management skills are essential.
Age Specific Care For the Population We Serve
6
Toddlers 1-3 Y/O

7
Safety Concerns(Cont’d)
PsychosocialNeeds
Patient/FamilyEducation
If the child is combative or throwing a temper tantrum:• Be aware you could be kicked, scratched or hit.• Use bumper pads on side rails/cribs to protect child from harm.• May need to protect property around the child that may break or could harm the child during a tantrum.
Psychosocial Aspects:• Emotionally, toddlers are dependent and trusting, but will often assert their independence by throwing
temper tantrums. They do not readily ask for help.• Believe the world revolves around him or her and has a strong sense of “mine.”• Develops magical thinking and can have a hard time separating fantasy from reality. Do not lie or
make up stories about a procedure or treatment.• Love to play by themselves and with others, running, looking at books, scribbling, repetitive songs and toys.
Communication:• Toddlers have a comprehension level much greater than their verbal capacity which progresses from babbling
to baby talk and simple sentences. Basics of language mastered by 36 months, with continued refinement throughout childhood.
• Learns to verbalize needs.• Understands the meaning of “No”, and will respond to this command. • Short attention span.• Recognizes the names of various people.• Responds better to visual rather than spoken cues. For example, when preparing for procedures, allow
toddlers to manipulate play instruments, hold a piece of equipment or push buttons if possible.• Offering all children, from Toddlers to Adolescents, verbal praise will help you gain cooperation and give
the child a sense of mastery. The most effective praise is to tell the child specifically what they did well. For example, “You did a really good job being still.”
Toddler Stress:• Very often significantly stressed by the dark, pain, and separation from loved ones. • Allow parents to participate in procedures; or if they are unable to participate, have parents tell their child
they are leaving and when they will return.• Try to avoid invasive techniques; and if movement must be restricted, alleviate stress through play. • Encourage the use of comforting objects such as a stuffed animal or a blanket from home, according to facility policy.
Parental Stress:• Parents often suffer from stress while their child is ill. This stress may be exhibited as anger, hostility, rudeness,
demanding behavior, or lack of cooperation, or feeling suspicious toward healthcare staff. • Try to stay calm and show your understanding. • Relieve stress through flexibility - by modifying care or making changes when possible - and showing the parent
you consider them a partner in the toddler’s care.
Proper nutrition should be promoted, as well as the need for routine medical screenings and vaccinations.
Provide education to parents on the following:• Care seats required• Never leave an infant alone in or near water, on changing tables, sofas or chairs • Provide a safe environment for exploring and playing• Make sure toddler does not run out into street, elevators, escalators, parking lots, etc.
Age Specific Care For the Population We Serve
Vital Signs
Physical GrowthCharacteristics
SpecialConsiderations
Safety Concerns
PsychosocialNeeds
Temperature of 96.8-99.6° FHeart rate 60-140Respiratory rate 24-34 SBP 73-110 DBP 30-70
• Develops and improves motor skills.• Physical growth is slower than a toddler’s.• Brain 90% of adult weight.• Begins to lose baby teeth.• Baby fat becomes muscle tissue.• Becomes toilet trained. • Begins dressing him or herself.
A respiratory rate should never be consistently greater than 60 breaths/minute in any child.
Medication Administration:If medications are to be given orally, check to see if the pharmacy offers flavors formulated per physician orders orpatient preference. This is a great way to give the child a choice in their care, and have them take their medicinemore easily.
• Since a child can drown in a very small amount of water, never leave any small child unattended when giving a bath or leave buckets of water or cleaning solutions unattended.
• Toys must be safe and age-appropriate.• Utilize equipment that is specific to size and age.• The rate for potential adverse drug events is 3 times higher in children than adults. Always perform double
checks for all high risk medications by making sure you have the right patient, drug, time, dose and route.• Encourage bicycle/tricycle safety, seat belt safety, car seats.• Be aware that pretend behavior and fantasies can be dangerous and the child may need to be protected from them.
Communication:• Preschoolers have vivid imaginations and like to hear stories.• Understands long and complex sentences.• Knows physical needs.• May take statements quite literally.• Keep explanations short and simple.• Lean down and forward when speaking and interacting with the child.
Psychosocial:• Becomes more independent. Negative behavior and temper tantrums may continue.• Becomes more sensitive to the feelings of others.• Provide praise and rewards.• Set clear rules.• Honor requests from child on how to place foods on plate. For example, food not touching, etc.
Age Specific Care For the Population We Serve
8
Pre-School 3-5 Y/O

9
PsychosocialNeeds (Cont’d)
Patient/FamilyEducation
Stress:• Greatly fears separation from parents, as well as the dark and pain. • Preschoolers may believe that they or their misbehavior caused the illness or injury. • Reassure the preschooler often that procedures are not a form of punishment – that they have done nothing
wrong, and offer explanations about the procedure or treatments. Validate feelings and emotions often.• Always be honest with preschoolers. If a procedure or treatment will hurt or be uncomfortable, tell them so
by using statements such as “other kids tell me this feels like a bee sting…I wonder what it will feel like to you.”• Keep parents involved in the care process and allow them to stay with the child as much as possible.• Avoid invasive techniques whenever possible. • If movement must be restricted, alleviate stress through play. • Encourage the use of comforting objects such as a stuffed animal or a blanket from home,
according to facility policy.
Parents/Family:• To help manage pain during care, or stress during procedures, encourage and coach parents to distract
the preschooler by telling stories, counting, or reciting the alphabet.• Promote healthy habits such as hygiene, nutrition, etc.• Encourage keeping up with immunizations, scheduled checkups.• Ask parent to teach and reinforce safety rules.• Television may be a cause of aggression in this age group and careful screening may be effective.
Preschooler:• May take statements quite literally, so be careful how to describe a procedure.• Keep explanations short and simple and use the softest language possible, such as make a “small opening”
rather than a “cut.” • Try giving explanations in terms of sensations and time frames they understand (i.e. “as long as it takes to
watch your favorite cartoon.”)• Encourage the child to ask questions and play with others.• Use toys and games to teach. Allow the preschooler to touch and play with instruments if possible.• Teach the difference between safe and unsafe behavior and the consequences of dangerous behavior.
Age Specific Care For the Population We Serve

Vital Signs
Physical GrowthCharacteristics
SpecialConsiderations
Safety Concerns
PsychosocialNeeds
Temperature 98.6° FHeart rate 5 to 10 yrs 60-140; 10+ yrs 60-100.Respiratory rate 18-30SBP 80-120 DBP 54-90
• Pubescent changes begin, accompanied by a growth spurt.• Hand-eye coordination is well established.• Loss of primary teeth and eruption of permanent teeth is completed by age 12.• Fluctuations in appetite occur due to uneven growth patterns.• Growing pains due to the stretching of muscles.
A respiratory rate should never be consistently greater than 60 breaths/minute in any child.
• Encourage yearly health exams and update immunizations. • Safety for sports, such as helmets, wrist and knee pads, and bicycle safety. • Proper car seats and seat belts in a vehicle. • Be aware that pretend behavior and fantasies can be dangerous and child may need to be protected from them.
Psychosocial Aspects:• Is an eager learner who is developing a much larger sense of self while at the same time learning
how to fit in with peers. • The need for independence from parents begins. May be disobedient or defiant.• Attention span lengthens and learns by doing.• Can be helped to make logical decisions.• School and after school activities are a major focus. • Around 10 or 12 begins to copy teenage dress. Appearances become important. May model behavior
of early adults.• May exhibit anxiety, nervousness, or become worried.• Need for privacy begins.• Self esteem tends to be higher in younger years than later years, and may be affected by peer popularity
or rejection, neglect, and emotional support. Negative self esteem can be damaging to further development.• Build self esteem by helping the school age child feel useful and recognize their achievements.
Help them feel competent by asking for their assistance.
Communication:• School age children understand cause and effect, and deal with several concepts in sequence.• Interact with the child as you would with an adult. Don’t ignore the child when talking to the parent.• When explaining a procedure, give concrete information using correct medical terminology. Be specific
about body areas or parts affected. • Use toys or games to teach the younger school age child and reduce fears.• If there will be pain or discomfort, discuss this with them prior to the procedure.
Age Specific Care For the Population We Serve
10
School Age 5-12 Y/O

11
PsychosocialNeeds (Cont’d)
Patient/FamilyEducation
Stress:• School age children’s biggest fears are separation from loved ones, school, failure, disability, death, pain,
and invasive procedures especially if they involve the genitals. • They communicate stress with regression, anxiety, withdrawal, depression, or increased dependency. • Reduce stress by incorporating deep breathing or comforting objects into care, and not leaving the child
unattended during stressful events. Games and other concepts of play may also be helpful.• Humor can alleviate stress and help develop the patient/caregiver relationship.
Parents:• Support parents and help them talk with their school age child about sexual health, drugs,
and peer pressure issues.
Child:• Help the child make healthy lifestyle choices. • Teach the child the difference between safe and unsafe behavior. Remind the child of dangerous situations
as they get older, and discuss the consequences of dangerous behavior.• Encourage the child to talk about their feelings, ask questions, and play with other children.
When conducting a procedure or treatment:• Show the equipment you will use and explain why the procedure is needed, how it will make them better,
and what they can expect to experience after the procedure. • Give the child a feeling of control by explaining how he may assist you in his/her treatment and allow them
to make some decisions regarding care. For example, which arm they would prefer to have the IV in. • Talk with them to discover what their misconceptions may be and correct them. • When the procedure is through, be sure to reward them and praise a job well done.
Age Specific Care For the Population We Serve

Vital Signs
Physical GrowthCharacteristics
SpecialConsiderations
Safety Concerns
PsychosocialNeeds
Temperature 98.6° FHeart rate 60-100Respiratory rate 12-16 (Adult range by 15 y/o) SBP 90-131 DBP 60-85
• Velocity of growth in an adolescent increases significantly, although in spurts. Girls usually finish growing by 16, boys by 18 years of age.
• There is maturation of the reproductive system and development of primary and secondary sexual characteristics. • Onset of menarche in girls and nocturnal emissions in boys will occur.• Depression and suicide are more common than in any other age group, and self destructive behaviors begin.
It is important to build teamwork and respect with this age group. If the adolescent establishes a good relationshipwith a favorite caregiver, then assignments should reflect that preference.
A respiratory rate should never be consistently greater than 60 breaths/minute in any child.
• Discourage risk taking in this age group, and instead promote safe practices such as self defense, safe driving and resisting gangs or other violent activities.
• Promote regular checkups, avoiding the use of drugs and alcohol, safe sexual practices.
Psychosocial Aspects:• Becomes emotionally independent from parents and uses peers as support.• Begins to prepare for adulthood and develops more mature relationships with others.• Develops sexual role identity.• Feelings of control are important. Often challenges authority.• Extremely idealistic.• Has difficulty understanding consequences of behavior.• Able to consider various alternatives to situation not yet experienced. Often has trouble making decisions.• Reasons through trial and error.• Experiments with adult behavior.• Mood changes are common and may be unpredictable. • When reaches 15 to 18 y/o, becomes increasingly independent and decisions influenced more by peers,
significant adults.• If perceives a situation to be unfair, may seek ways to change it.• Often self-conscious and concerned about body image. Remember to respect their privacy and fear of
embarrassment. Be sensitive to how treatments or procedures may affect their appearance or relationshipswith others.
• Adolescents usually do not show their fear but this does not mean they are not scared. Adolescents most often fear loss of control, especially loss of consciousness, such as that which occurs with anesthesia.
Communication:• Do not refer to the person as child, boy, girl, etc.• Adolescents want to be treated as adults; so when explaining procedures, never talk down to them.
Use proper medical terms and always explain thoroughly - even if the explanation is complex or abstract.• Adolescents should be given choices and allowed to express how much pain they feel they can handle. • Use logical explanations and reasoning.
Age Specific Care For the Population We Serve
12
Adolescents 13-18 Y/O

13
Patient/FamilyEducation
Because the adolescent may not ask questions for fear of appearing unintelligent, instruct away from parents andpeers, if possible, and encourage questions.
Do not ask personal questions, for example, about sex or drugs, in front of parents as you probably will not get the truth.
Encourage open communication and joint decision making between teen and parents.
Encourage positive lifestyle choices. Immunizations such as the new HPV vaccine should be discussed.
Emphasize seat belts; no smoking under age 18; no drinking under age 21; be wary of peer pressure that may result in unsafe behavior.
Clearly communicate consequences of dangerous behavior. Use reasoning, self preservation and explanations thatwill help enforce limits, rather than just parental power.
Age Specific Care For the Population We Serve

Vital Signs
Physical GrowthCharacteristics/SpecialConsiderations
PsychosocialNeeds
Patient/FamilyEducation
Temperature 98.6° FHeart rate average 70Respiration 16-20 Blood pressure 120/80
• Reaches physical and sexual maturity.• The body is usually in peak physical condition and body systems are at optimal performance.• Nutritional needs are for maintenance, not growth. • Main causes of death are motor vehicle accidents, other traumatic accidents, suicides and homicides.• During the period of hospitalization, a thorough health assessment for the Early Adult should include
screening for STD’s, hypertension and cholesterol levels. Obese patients may be considered candidates for diabetes screening.
Psychosocial Aspects:• Becomes an independent adult. Develops own lifestyle, personal identity and residence.• Seeks close ties with others, intimate relationships, may start a family.• Establishes a career that provides security, satisfaction, feelings of contribution.• Recognizes responsibilities and commitments to family, career, friends and community.
Communication:• Be honest, supportive, respectful. • Be non-judgmental of lifestyle choices and personal values.• Anticipate and meet needs.• Listen to concerns and respond appropriately.
Stress:• Newfound independence from parents as well as competition in the workplace often lead to stress resulting
in anxiety, depression, experimentation with various lifestyles and sometimes substance abuse. • The early adult patient will worry about the impact of hospitalization on their work and family life.
Openly discuss these situations with them and watch for body language as a cue to their true feelings.
Encourage healthy care decisions such as good nutrition, the importance of regular exercise, update of immunizations,no drinking until 21 y/o.
Provide information on health risks, such as heart disease, cancer.
Provide information on hazards associated with work or home.
Communicate the consequences of being an adult from legal point of view.
Age Specific Care For the Population We Serve
14
Early Adulthood 18-29 Y/O
15
Vital Signs
Physical GrowthCharacteristics/SpecialConsiderations
PsychosocialNeeds
Patient/FamilyEducation
Temperature 98.6° FHeart rate average 70 beatsRespiration 16-20Blood Pressure 120/80, 115/75 in a diabeticOptimal LDL Cholesterol <100Desirable Total Cholesterol <200HDL Cholesterol <40 Low, > 60 High
• The Young Adult should be screened for breast, cervical and testicular cancer, hypertension (BP > 140/90 mmHg), anemia, cholesterol levels, diabetes, as well as dental health.
• A diabetic patient’s blood pressure and lipid control are held to tighter measures than non-diabetics.• Women may begin peri-menopause.
Psychosocial Aspects:• May start and care for a family.• Uses life experiences to solve problems, learn.• Balances dreams with reality.• Continues to develop personal identity and set of values.
Stress:• Stress centers around employment, marriage, adjusting to parenting, and assuming financial responsibilities. • Will worry about the impact of hospitalization on work and family life. Openly discuss these situations
with them and watch for body language as a cue to their true feelings.
Communication:• Be respectful.• Recognize responsibilities, priorities and commitments to family, career, friends and community. • Listen to concerns and respond.• Anticipate and meet needs.
Because the Young Adult is approaching middle age, it is important to develop awareness of a healthier body.
Instruct on the reduction of sodium and sugar in their diet and the importance of maintaining a normal body weight.
Encourage regular checkups and preventative health exams, provide information on health risks.
Reinforce the dangers of substance abuse and the benefits of exercise.
Special suggestions can be made for smoking cessation and weight loss.
Reinforce seat belt use and no drinking and driving.
Age Specific Care For the Population We Serve
Young Adulthood 30-44 Y/O
Vital Signs
Physical GrowthCharacteristics/SpecialConsiderations
PsychosocialNeeds
Temperature 98.6° FHeart rate 70 beatsRespiration is 16-20Blood Pressure 120/80, 115/75 in diabeticsOptimal LDL Cholesterol <100Desirable Total Cholesterol <200HDL Cholesterol <40 Low, > 60 High
The major health concerns/Common causes of death: • Lung, breast and other cancers• Menopause• May develop chronic health conditions such as:
– Chronic respiratory disease– Hypertension (BP > 140/90)– Diabetes– Cardiovascular problems such as stroke and heart attack
May begin to experience the following physical characteristics:• Bone mass begins to decrease due to calcium loss, especially in women after menopause,
causing loss of skeletal height.• Endurance declines resulting in decreased muscle strength and mass.• Muscles and joints respond more slowly; and there is decreased balance and coordination.• Loss of skin elasticity and drying of skin causing wrinkles.• Increased cholesterol and decreased cardiac output.• Decreased renal functioning, metabolic rate and tolerance to heat and cold.• Increased susceptibility to infection.• Slowing of the reflexes.• Visual changes, especially farsightedness.• Noticeable loss of hearing and taste.• By age 55 most men will develop some stage of hyperplasia and have problems urinating.
Psychosocial:• Most of the factors contributing to illness and death are external and include job stress, marital and
parenting problems and caring for older parents. • Wants to be productive, not “stuck” in one job or situation; balances work and other roles.• Works on achieving social and civic responsibility.• Begins planning for retirement.• Begins accepting and adjusting to physical changes.
Communication:• Be respectful.• Keep a positive, hopeful attitude that focuses on the strengths of the patient rather than the limitations.• Encourage discussions about future plans.• Address any worries about the future.
Age Specific Care For the Population We Serve
16
Middle Adulthood 45-65 Y/O
17
Patient/FamilyEducation
Discuss occupational hazards, sexual dysfunction, adjustment to menopause, use of over-the-counter medications,and alcohol and tobacco use.
Assess for exercise and nutritional needs.
To help with psychosocial pressures of multiple priorities, warn against trying to do too much with not enoughresources.
Become familiar with the signs and symptoms of stroke, and help your patients recognize them as well:• Have the patient raise both arms, smile, and repeat a simple phrase. • If one arm is lower, the smile is one sided, and the speech is slurred, the family should call 911 because
the probability of stroke is high.
Age Specific Care For the Population We Serve

Vital Signs
Physical GrowthCharacteristics
SpecialConsiderations
There is no “normal” range for vital signs, as they all depend on the physical and health status of the individual.
The Geriatric person is often dealing with limitations, such as:• Decreased mobility.• Decreased ability to respond to stimuli.• Decreased sense of balance.• Paresthesia or abnormal sensations such as pricking and burning.• Development of cataracts.• The need for stronger stimulation for all senses.
Physical changes in the geriatric person include:• Loss of fat layers on limbs and face.• Decreased perspiration.• Change in skin pigmentation.• Bones become prominent and joints become stiff, as do areas such as the rib cage causing decreased vital capacity.• Shrinking in intervertebral disc.• Increased susceptibility to infection, and decreased ability to fight infection.• Increased susceptibility to high blood pressure.• Progression of atherosclerosis which can lead to heart attack and stroke.• Loss of teeth likely.• The kidneys are less efficient causing genitourinary problems.• Decrease in GI absorption rate, cardiac output and airway capacity.• By age 55 most men will develop some stage of hyperplasia and have problems urinating.
The elderly require regular assessments of physical, cognitive, functional, and social status. The older or frail thepatient, the more frequent should be the assessments.
The elderly are more likely to die from slowly progressive diseases or the impact of multiple chronic diseases, andexperience symptoms over an extended period of time. This may occur more as a roller coaster ride rather than adownhill course.
If you have concerns that a patient is unable to meet their healthcare needs, a social services consult should bearranged.
Atypical presentation of symptoms:• Atypical presentation of symptoms is common in the elderly.• Mental status may be altered by illness or medication.• Vague symptoms are more common than acute.• Loss of appetite, falls, and inability to perform usual activities may all be clues to underlying illnesses.• Signs of infection present differently. Fever is rare, but there may be tachycardia, tachypnea,
and often a change in mental status.
Pain is a common symptom for patients with certain diseases and chronic conditions. Pain should be assessed regularly, and responded to immediately.
Relieve other physical symptoms such as constipation, and attend to oral hygiene needs.
The skin of a geriatric is extremely delicate. Handle the body with the palms of your hands rather than with fingers.
Age Specific Care For the Population We Serve
18
Elderly or Geriatric 65+ Y/O
19
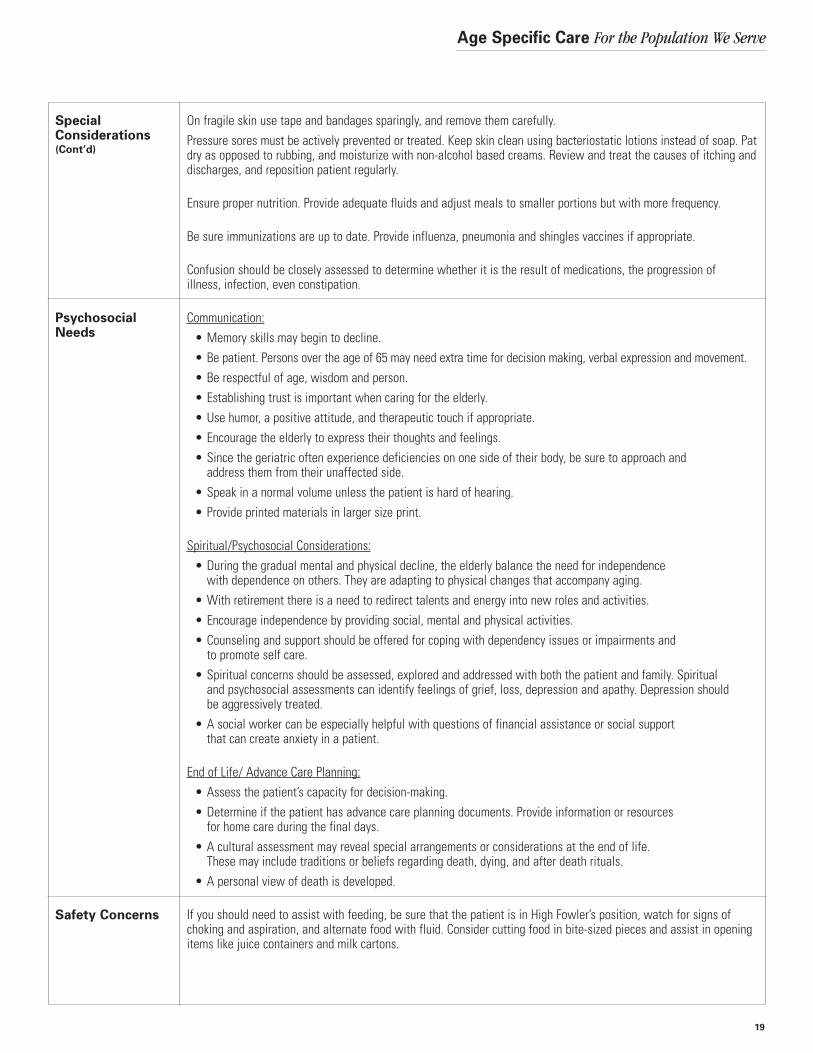
On fragile skin use tape and bandages sparingly, and remove them carefully.Pressure sores must be actively prevented or treated. Keep skin clean using bacteriostatic lotions instead of soap. Patdry as opposed to rubbing, and moisturize with non-alcohol based creams. Review and treat the causes of itching anddischarges, and reposition patient regularly.
Ensure proper nutrition. Provide adequate fluids and adjust meals to smaller portions but with more frequency.
Be sure immunizations are up to date. Provide influenza, pneumonia and shingles vaccines if appropriate.
Confusion should be closely assessed to determine whether it is the result of medications, the progression of illness, infection, even constipation.
Communication:• Memory skills may begin to decline.• Be patient. Persons over the age of 65 may need extra time for decision making, verbal expression and movement.• Be respectful of age, wisdom and person.• Establishing trust is important when caring for the elderly. • Use humor, a positive attitude, and therapeutic touch if appropriate.• Encourage the elderly to express their thoughts and feelings. • Since the geriatric often experience deficiencies on one side of their body, be sure to approach and
address them from their unaffected side.• Speak in a normal volume unless the patient is hard of hearing.• Provide printed materials in larger size print.
Spiritual/Psychosocial Considerations:• During the gradual mental and physical decline, the elderly balance the need for independence
with dependence on others. They are adapting to physical changes that accompany aging.• With retirement there is a need to redirect talents and energy into new roles and activities.• Encourage independence by providing social, mental and physical activities.• Counseling and support should be offered for coping with dependency issues or impairments and
to promote self care. • Spiritual concerns should be assessed, explored and addressed with both the patient and family. Spiritual
and psychosocial assessments can identify feelings of grief, loss, depression and apathy. Depression should be aggressively treated.
• A social worker can be especially helpful with questions of financial assistance or social support that can create anxiety in a patient.
End of Life/ Advance Care Planning:• Assess the patient’s capacity for decision-making.• Determine if the patient has advance care planning documents. Provide information or resources
for home care during the final days. • A cultural assessment may reveal special arrangements or considerations at the end of life.
These may include traditions or beliefs regarding death, dying, and after death rituals.• A personal view of death is developed.
If you should need to assist with feeding, be sure that the patient is in High Fowler’s position, watch for signs ofchoking and aspiration, and alternate food with fluid. Consider cutting food in bite-sized pieces and assist in openingitems like juice containers and milk cartons.
Age Specific Care For the Population We Serve
SpecialConsiderations(Cont’d)
PsychosocialNeeds
Safety Concerns
Age Specific Care For the Population We Serve
20
Medication safety:• Medication safety and polypharmacy are very problematic as the elderly usually take multiple medications
prescribed by various sources, and may be given medications to treat the side effects of another drug. • In addition, medications may react differently in the elderly due to physical changes in the body. • Have the elderly bring their medications to the hospital for evaluation. • When giving new medication, it is generally better to start with a lower dose and revaluate before
increasing the level.
Fall Prevention:• Take extra precautions to prevent falls and other injuries in the healthcare setting by providing
a bedside commode at night or performing elimination rounds.• Utilize walkers, canes and wheelchairs as appropriate.• Keep electrical cords from medical equipment and furniture out of the patient’s path.• Having a family member at the bedside or frequent staff rounding are also good ways to prevent falls.• Promote fall prevention in the home, and a safe living environment.
As the patient progresses from Young Old to Oldest Old, the speed of learning and memory skills may decline and this should be considered during the presenting of information.
A family member or advocate should be encouraged to attend and ask questions during the education session.
Elderly or Geriatric 65+ Y/O (Continued)
Safety Concerns(Cont’d)
Patient/FamilyEducation

1. ASHP Member Update. ASHP Recommends Hospitals Take Key Steps to Improve Safety. September 22, 2006. American Society of Health-System Pharmacists. http://www.ashp.org/s_ashp/docs/files/GAD_ASHPMedErrorsReccomHosp.pdf
2. ATP III Guidelines At-A-Glance Quick Desk Reference. National Institutes of Health, National Heart, Lung, and Blood Institute. NIH Publication No. 01-3305, May 2001.
3. Erikson, E H. Childhood and Society. Second edition, New York: W. W. Norton, 1963.
4. Illinois Emergency Medical Services for Children. Initial Pediatric Assessment Teaching Tool. April 4, 1999. www.luhs.org/depts/emsc/Teaching.pdf
5. The Johns Hopkins Health System, the Johns Hopkins Hospital. Age-Specific Criteria for Clinical Staff– Self-Learning Packet. Revised 1998.
6. JNC 7 Express: The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. National Institutes of Health, National Heart, Lung, and Blood Institute. NIH Publication No. 03-5233, December 2003.
7. Krysiak T. Pediatric Physical Assessment. www.western.cc.ok.us/nursing/NURS%201129/powerpoints/tina%20pwrpoints/Pediatric_physical_Assessment.ppt
8. Pediatric Advanced Life Support. Editors: Ralston M, Hazinski MF, Zaritsky AL, Schexnayder SM, Kleinman, ME. American Academy of Pediatrics and American Heart Association. AHA, 2006.
9. Paramedic: National Standard Curriculum. United States Department of Transportation, National Highway Traffic Safety Administration. www.health.state.ny.us/nysdoh/ems/original/prepar/1-10.pdf
References
21

1. The following can be said about the Neonate/Infant Stage:A The most rapid growth and development occurs in the first year of life.B During the Neonate/Infant stage, the child is learning to communicate through facial expressions and babbling.C At 4 months stranger anxiety emerges.D All of the above.E A and B only.
2. The following can be said about potential adverse drug events in Neonates/Infants:A The rate is 3 times higher in children than adults, and substantially higher in neonates in intensive care.B The rate is the same in children and adults.C The rate is 5 times higher in children than adults and 10 times higher in neonates.D The rate is lower in children than in adults.
3. The following can be said about Toddlers:A Respond better to visual rather than spoken cues.B Have a comprehension level much greater than their verbal capacity.C Their physical growth is slower than an infant’s.D All of the above.
4. Some safety concerns to keep in mind with an Infant/Toddler/Preschooler:A Toddlers explore the world by putting things in their mouths.B Only leave a small child alone near water if the water is very shallow.C Always provide toys that are bigger than their heads.D All of the above
5. To help reduce stress in the School Age child:A Incorporate deep breathing or comforting objects into care.B Encourage parents to participate with their children during or after procedures.C Allow for play and normal activity.D All except C.E All of the above.
6. The following can be said about Adolescents:A Depression and suicide are less common than in any other age group.B Adolescents want to be treated as adults.C The Adolescent may not ask questions for fear of appearing unintelligent.D Adolescents normally do not show fear.E All except A.F All of the above.
Post Test
22
Age Specific Care For the Population We Serve
23
7. The main causes of death for the Early and Young Adult are:A Motor vehicle accidents and other traumatic accidents. B Cancer.C Suicides and homicides.D STD’s.E All of the above.F A and C only.
8. For the Middle Adult, most of the factors contributing to illness and death are:A Cardiovascular, such as strokes and heart attacks, and cancers such as lung and breast.B External and include job stress, marital and parenting problems and caring for older parents.C Substance abuse.D A and B only.E All of the above.
9. The following can be said about the Geriatric or Elderly person:A They are more susceptible to infection and less able to fight infection.B Are less likely to die from slowly progressive diseases.C Are often dealing with various limitations, such as less mobility and sense of balance.D Often present symptoms differently than other age groups.E All except B.F All except D.
10. When caring for an Elderly or Geriatric person, provide a safe environment by:A Utilizing walkers, canes and wheelchairs.B Providing a bedside commode or performing elimination rounds.C Keeping electrical cords and furniture out of the patient’s path.D Having family members at the bedside or frequent staff rounding.E All of the above.
Post Test

1. E. A and B only. C is incorrect as stranger anxiety emerges at 6 to 8 months.
2. A. The rate is 3 times higher in children than adults and substantially higher in neonates in intensive care.
3. D. All of the above.
4. A. Toddlers explore the world by putting things in their mouths. B is incorrect as an infant or small child should never be left alone in or near any amount of water. C is incorrect as toys should be safe and age appropriate, but not necessarily bigger than their heads. For infants, toys should not be smaller than can fit inside a toilet paper tube.
5. E. All of the above.
6. E. All except A. Depression and suicide are more common in Adolescents than in any other age group.
7. F. A and C only. Cancer and STD’s may occur, but are not the most common cause of death in these age groups.
8. D. A and B only. Substance abuse may occur, but is not a common cause of death or illness in this age group.
9. E. All except B. The elderly are more likely to die from slowly progressive diseases or the impact of multiple chronic diseases and experience symptoms over an extended period of time.
10. E. All of the above.
Post Test Answers
24
Age Specific Care For the Population We Serve