Embed Size (px)
Citation preview

OBJECTIVES:
To review emerging strategies to improve
upon the coordination of care for cancer
survivors through the adoption and
promotion of cancer treatment summaries
and survivorship care plans. Special
attention is focused on the needs of
childhood cancer survivors.
DATA SOURCES:
Reports from the Institute of Medicine and
the President’s Cancer Panel, and work
being performed by several professional
societies.
CONCLUSION:
Cancer care is poorly coordinated during
and after treatment. The growing number of
cancer survivors demands innovative
strategies to improve the quality and
coordination of post-cancer patient care.
IMPLICATIONS FOR NURSING
PRACTICE:
Nurses play an important role in the
implementation and delivery of treatment
summaries and survivorship care plans.
Incorporation of cancer prevention and
health promotion counseling is a natural
activity for nurses as the health care system
focuses on improving care for cancer
survivors.
KEYWORDS:Quality of care, cancer survivor, care plan
From the Schools of Public Health and
Medicine, University of California, Los
Angeles, CA; the Division of Cancer
Prevention & Control Research, Jonsson
Comprehensive Cancer Center, Los Angeles,
CA; and the Department of Pediatrics, David
Geffen School of Medicine at University of
California, Los Angeles, CA
Work related to this publication was
supported in part by the Breast Cancer
Research Foundation, the Lance Armstrong
Foundation, and an American Cancer
Society Clinical Research Professorship
(P.A.G.).
Address correspondence to Patricia A.
Ganz, MD, UCLA-LIVESTRONG
Survivorship Center of Excellence, Division
of Cancer Prevention and Control Research,
Jonsson Comprehensive Cancer Center, 650
Charles Young Dr. South, Room A2-125 CHS,
Los Angeles, CA 90095-6900; e-mail: pganz@
ucla.edu
� 2008 Elsevier Inc. All rights reserved.
0749-2081/08/2403-$30.00/0
doi:10.1016/j.soncn.2008.05.009
ENSURING QUALITY
CARE FOR CANCER
SURVIVORS:IMPLEMENTING THE
SURVIVORSHIP CARE
PLAN
PATRICIA A. GANZ, JACQUELINE CASILLAS,AND ERIN E. HAHN
OVER THE past decade, the Institute of Medicine (IOM)has been engaged in a concerted effort to examine thequality of health care in the United States, and to iden-
tify critical issues that are central to improving the delivery ofhealth care to the population. The IOM definition of quality is‘‘the degree to which health services for individuals and populationsincrease the likelihood of desired outcomes and are consistent withcurrent professional knowledge.’’1 In its investigations of quality ofcare, various IOM committees have identified overuse, misuse, andunderuse of health care services, as well as poor coordination ofcare, especially for those individuals with chronic illness. In partic-ular, one of the first IOM investigations of quality of care focused onthe disparities in cancer care service delivery in the 1999 report‘‘Ensuring Quality Cancer Care’’2 in which a wide gulf was foundbetween ideal cancer care and that received by most Americans.Subsequently, the IOM Committee on Quality of Health Care inAmerica issued two key reports: ‘‘To Err is Human: Building a SaferHealth System’’3 and ‘‘Crossing the Quality Chasm: a new healthsystem for the 21st Century,’’4 which laid the foundation and cre-ated the vision for the transformation that is necessary to improvethe quality of health care. The former high-profile report brought topublic attention the high human and fiscal cost of medical errorsand the critical issue of patient safety, while the latter identifiedsix key dimensions of quality health care (safety, effectiveness, pa-tient-centered, timely, efficient, equitable) that should be the focusof improvement efforts within the health care system.
208 Seminars in Oncology Nursing, Vol 24, No 3 (August), 2008: pp 208-217

ENSURING QUALITY CARE FOR CANCER SURVIVORS 209
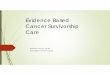
With this background in mind, in 2004 the Na-tional Cancer Policy Board and the IOM estab-lished a committee on cancer survivorship toexamine issues related to improving care and qual-ity of life.5 To this end, the committee decided tofocus its efforts on describing the quality-of-careneeds for patients with cancer who were beyondthe acute phase of treatment and living withcancer–and its aftermath–as a chronic disease.Figure 1 describes the cancer care trajectory andhighlights the enlarging time/phase/place in whichpatients live free of cancer, but often with burdensof long-term and late effects.
Why is cancer survivor care special? Shouldn’tcoordination of care between specialist and gener-alists be expected? Cancer patients often requiretreatment by multiple specialists (surgeons, radia-tion oncologists, medical oncologists) because ofthe use of multi-modal therapies and the frequentuse of organ sparing treatments. Chemotherapyadministration may require both inpatient andoutpatient visits, and radiation therapy may notbe given in the same facility where surgery andchemotherapy are received. As a result, there isseldom a single integrated medical record andthere may be limited formal (written) communica-tion between the specialists. Primary care pro-viders are often not included in the managementof the patient during this time, and it may bemonths to years after the completion of treatmentthat the patient returns for regular check-ups withthe primary care provider. Many patients may
forego the regular care of a primary care provider,thinking that the cancer and its potential recur-rence are the most serious threat that they face.More important, cancer patients at the end ofactive cancer treatment, often feel ‘‘lost in transi-tion,’’ because there is no standard protocol for fol-low-up similar to what they experienced duringtreatment, and often there are no specific guide-lines for follow-up of late effects, with a few excep-tions. In addition, often cancer treatment causesmany physical symptoms, which for the mostpart gradually resolve. Oncology specialists arenot always able to predict the time course of recov-ery, and many patients need a lot of psychologicalsupport during this time–something that is not al-ways forthcoming. Thus, it is both the intensityand complexity of cancer treatment that makes ita special case for coordination of care during thephase of extended survival off cancer treatment.
Thus, there are some unique quality-of-careissues faced by cancer survivors. In the short-term, many survivors need to have an understand-ing of what treatments they received and whatkind of follow-up is necessary. This is for theirown information, so they can understand howthey might recover effectively, but also so theycan tell others (family, friends, employer, otherhealth professionals) what to expect. Often, theyhave put many activities on hold and they arelooking forward to resuming a normal life. Theyneed guidance during this early post-treatmenttime, which is often lacking in the current health
Diagnosis andStaging
PalliativeTreatment
Treatment WithIntent to Cure
Cancer-FreeSurvival
ManagedChronic orIntermittent
Disease
Recurrence/Second Cancer
Cancer Care Trajectory
Death
Treatment Failure
Survivorship
Care
Start Here
IOM, 2005
Figure 1. The cancer treatment trajec-tory with special identification of thepost-treatment survivorship carephase. (Adapted from Hewitt et al.5)

210 P.A. GANZ, J. CASILLAS, AND E.E. HAHN
care delivery system. They are also eager to havea better understanding of whether or not thereare any long-term effects of the treatments thatneed monitoring (eg, cardiac or pulmonary toxic-ity, second cancers, etc) and whether other spe-cialists are required. There is a tendency toworry about every ache and pain, and during thistime, many scans and tests are likely to be doneto look for cancer recurrence, and many addi-tional specialists may be consulted.
There are some special populations that areworthy of mention, as their care coordinationneeds are more substantial. These include theadult survivors of childhood cancer, who often suf-fer from an increased number of chronic condi-tions,6 as well as a substantial risk for secondmalignancies.7,8 Bone marrow transplant patients(both children and adults) also sustain consider-able toxicities from the conditioning regimensand risk for graft versus host disease. There arehigh rates of physical and psychological complica-tions in this patient population.9-11 Finally, olderindividuals make up the majority of cancerpatients and survivors, and in the context of theirfollow-up care, comorbid conditions may add tothe specific toxicities of cancer treatment, espe-cially cardiac, pulmonary, and renal toxicities.
As can be seen, there are many challengesassociated with ensuring quality care for cancersurvivors. One of the proposed first steps in ac-complishing this is the widespread implementa-tion of treatment summaries and survivorshipcare planning. This key recommendation of theIOM report has been embraced by a number ofleading organizations, including the American So-ciety of Clinical Oncology (ASCO). The LanceArmstrong Foundation LIVESTRONG Survivor-ship Centers of Excellence and others are alsoworking hard to incorporate treatment summariesand care plans into their work. The treatmentsummary and care plan is seen as the roadmapand communication vehicle for quality care, andthus we will use this article to describe it insome detail. We also devote time to describingthe already well-developed follow-up scheme forchildhood cancer survivors, as articulated by theChildren’s Oncology Group (COG) and its guide-lines and recommendations for survivorshipcare. Finally, we provide some perspective onthe health policy impact of survivorship care plansas they relate to current legislation, accountabil-ity, and quality improvement activities that areunderway.
WHAT IS THE SURVIVORSHIP CARE PLAN?
T he IOM report recommends the developmentand utilization of a treatment summary and
survivorship care plan, a synoptic document thatdescribes the patient’s cancer treatment experi-ence and provides guidance for the patient’s futurecare for the patient and provider. Per the recom-mendations from the IOM Workshop Summary‘‘Implementing Survivorship Care Planning,’’12
survivorship care plans should always contain cer-tain core elements: a cancer treatment history,the potential long-term and late effects of treat-ment, recommended surveillance for long-termand late effects, and recommended surveillancefor recurrence and new cancers. Additionally,links to resources that provide psychosocial sup-port for survivors should be included in the careplan, as well as information on general healthand wellness for cancer survivors. The plan shouldalso contain a clear timeline for the patient’s fol-low-up care, and ideally will identify the appropri-ate physician to provide it. These core items willallow for improved communication between thetreating oncologist(s) and the primary care pro-vider as well as educating and empowering thepatient.
It is critical for the survivorship care plan tohave a comprehensive cancer treatment historythat includes surgical summaries, chemotherapy,radiation, blood transfusions and/or bone marrowtransplant, and any continuing medical therapiessuch as endocrine therapy. Complications the pa-tient experienced during treatment should also benoted, such as chemotherapy toxicities. This sec-tion should also include provider contact informa-tion for the medical oncologist, surgeon, radiationoncologist, and any other treating clinician. Accu-rate treatment records and a clear understandingof the patient’s cancer treatment experience areessential to create the most effective and informa-tive plan for the patient’s future care.
Based on the patient’s cancer treatment history,the known potential long-term and late effects ofeach treatment should be articulated along withrecommendations for surveillance and evaluationof these effects. Long-term and late effects can in-clude fatigue, pain, sexual dysfunction, cardiacproblems, psychological distress, and many otherconditions.13 It is essential to provide the patientwith guidance on what symptoms require an im-mediate visit with a clinician, such as chest pain,

ENSURING QUALITY CARE FOR CANCER SURVIVORS 211
shortness of breath, or localized limb swelling, andwhat does not. This vital information must be pro-vided to the patient in a clear, easy to read writtenformat so that the patient is not struggling to re-member verbal information given during a visitthat may not be accurately recalled. This sectionwill also assist primary care providers to identifylong-term and late effects that present in theirsurvivor patient population.
It is also critical to address the psychosocialneeds of the survivor by including recommen-dations and/or referrals for depression, anxiety,and relationship issues. Information on organiza-tions that provide support and resources, such asThe Wellness Community or the Lance ArmstrongFoundation, should be included in the care plan.Also important are resources and tools for generalhealth and wellness, such as the nutrition guide-lines for survivors from the American CancerSociety, as maintaining a healthy weight and effec-tively managing co-morbid conditions is essentialfor cancer survivors and may help reduce therisk of early morbidity in this population (seeTable 1 for list of resources). Support for theneed of these physical and emotional servicesamong survivors can be found in a large-scaleInternet-based survey (N ¼ 1,020) conductedby the Lance Armstrong Foundation in 2004,which showed that 54% reported chronic pain,70% reported depression due to cancer, 49% hadunmet non-medical needs, and that 53% foundemotional needs harder than physical needs.14
OBSTACLES AND CHALLENGES TO COMPLETING
THE TREATMENT SUMMARY AND SURVIVORSHIP
CARE PLAN
T he creation of an effective and informativesurvivorship care plan depends on obtaining
primary-source treatment records. Without accu-rate pathology reports, chemotherapy records,operative reports, radiation summaries, and othertreatment records, the survivorship care plancould be greatly compromised. However, depend-ing on where the patient was treated, gettingtimely access to patient records can be a struggle,and all records are not equal in clarity andcontent.
Radiation oncologists often provide a specifictreatment plan and summary note, which areparticularly helpful in identifying the extent of
the patient’s radiation treatment. This typicallyincludes an introductory note at the beginning oftreatment outlining the planned radiation therapycourse and a concluding note summarizing the to-tal radiation received, areas radiated, and detailsof any changes or problems encountered duringthe treatment. Surgeons are required to preparea detailed operative report with the pre- andpost-operative diagnosis clearly stated along withthe details of the procedure. Medical oncologistsseldom provide a treatment plan at the beginningof treatment or a care summary at the end, andthis makes determination of chemotherapy treat-ment actually received a problem. Medical recordsmay contain a brief letter dictated to the primarycare provider outlining the proposed treatmentcourse. Sometimes a chemotherapy treatmentflow sheet can be found to help determine the pre-scribed treatments and the total dose receivedover many weeks or months.
It can be time-consuming to request and collecttreatment records from the surgical, radiation,and medical oncologist offices, and it may requiredogged persistence, but it is absolutely essential tocreating an accurate treatment summary and careplan document. In some cases, the search for ac-curate records may require locating chemother-apy flow sheets from an infusion center ordeciphering hand-written progress notes frommany years ago. Collecting records from large ac-ademic institutions and cancer centers can bemuch simpler than collecting records from indi-vidual physician offices scattered throughout thecommunity, but both can be accomplished. Re-cord retrieval can be carried out by administra-tive, research, or clinical staff; staff can also betrained to abstract records to begin populatingthe treatment summary and care plan before thepatient’s visit.
Real-Time Preparation of the Treatment
Summary and Care Plan
Prospective preparation of the treatment sum-mary and care plan is preferred to retrospectivereconstruction of past treatments. ASCO recentlycreated sample templates for a combined treat-ment plan/treatment summary for breast andcolon cancer patients; there is also an associated1-page survivorship care plan that outlines therecommended follow-up care and surveillance forthese patients (Table 2 provides a website URLfor this document). ASCO has also released

212 P.A. GANZ, J. CASILLAS, AND E.E. HAHN
TABLE 1.Online Resources for Cancer Survivors
Organization and Description Website
American Cancer Society Survivors Network: ACS is a nation-wide
voluntary health organization that provides cancer resources online
and in the community; ACS has developed this site specifically forsurvivors.
http://www.cancer.org; http://www.acscsn.org
CancerCare: CancerCare is a non-profit organization that provides free
professional support services online and by telephone for anyone
affected by cancer.
www.cancercare.org
Lance Armstrong Foundation (LAF): The LAF provides information and
survivorship resources online and in the community.
www.livestrong.org
NCI Office of Cancer Survivorship: OCS provides current information onsurvivorship research, resources, and publications.
http://cancercontrol.cancer.gov/ocs/
The IOM report ‘‘From Cancer Patient to Cancer Survivor: Lost in
Transition’’ can be accessed online at no charge.
www.iom.edu/CMS/28312/4931/30869.aspx.
The Wellness Community (TWC): TWC provides support groups,activities, and other resources online and in their many community
sites.
www.thewellnesscommunity.org
The Children’s Oncology Group (COG): The COG has developed
consensus-based guidelines for screening and management of lateeffects.
http://www.survivorshipguidelines.org/
The National Coalition for Cancer Survivors (NCCS): NCCS is the oldest
survivor-led cancer advocacy organization in the country, advocating
for quality cancer care for all Americans and empowering cancersurvivors.
http://www.canceradvocacynow.org/site/PageServer
People Living With Cancer (PLWC): PLWC provides expert up-to-date
information on cancer and survivorship; it is the patient site of ASCO.
http://www.cancer.net
a generic template that can be used for any cancersite, with plans for other disease-specific sitessuch as lung and prostate cancer. These short tem-plates can be quickly completed before or duringa patient visit by the treating physician or otherstaff, and they cover all of the core elements ofthe survivorship care plan.
A more comprehensive approach to the survi-vorship care plan may include information onthe patient’s co-morbid conditions from primarycare as well as specialist care such as cardiology,endocrinology, or pulmonology. This more holis-tic approach is much more resource-intensiveand may be easier to carry out in specialized sur-vivorship clinical practices or in large healthcare institutions with access to multiple areas ofcare. The comprehensive plan will providea broader picture of the patient’s overall healthalong with the core elements of the survivorshipcare plan; this is especially important for child-hood cancer survivors, who may experiencea greater number and more severe long-term andlate effects.6
Emerging Trends
There is currently a national effort underway toeducate both the health care community and thegeneral public about survivorship issues and toencourage the use of survivorship care plans.
TABLE 2.Links and Online Resources for Preparing Treatment
Summaries and Survivorship Care Plans
ASCO treatment summary and care plan templates forbreast and colon cancer:
www.asco.org/treatmentsummary
OncoLife survivorship care planning tool from the OncoLink
website, maintained by the Abramson Cancer Center ofthe University of Pennsylvania:
http://www.oncolink.com/oncolife/
A Prescription for Living treatment summary and care planfrom the American Journal of Nursing:
http://www.cc.nih.gov/nursing/nursingresearch/Rx_for_
Living.pdf

ENSURING QUALITY CARE FOR CANCER SURVIVORS 213
Organizations such as ASCO, the Lance Arm-strong Foundation, the National Coalition for Can-cer Survivorship, and Blue Cross of California areinvested in educating oncologists, oncologynurses, primary care providers, and patients aboutthe importance of survivorship care and the use ofsurvivorship care plans. These efforts include pro-viding practical information on provider billing,access to publicly available care plan templatesand survivorship guidelines, and survivorshipcare plan tool kits with resources for patientsand providers. There is also momentum to includetreatment plans and care summaries as a report-able quality-of-care measure. As a part of manyof these efforts, programmatic evaluation isplanned to determine patient and provide satisfac-tion with the care plans, and downstream exami-nation of adherence to guideline care for cancersurveillance and health promotion. This is anarea that is ripe for further research to support im-plementation and the most effective models of care.
There are excellent publicly available resourcesand guidelines that can be used to create or sup-plement survivorship care plans in clinical prac-tice. As mentioned above, ASCO has templatesfor breast and colon cancer treatment summaryand care plans, as well as a chemotherapy treat-ment plan and treatment summary and generalbackground materials for care plans. ASCO isalso currently promoting integration of the treat-ment plan and summaries into oncology elec-tronic health records by hosting a vendorchallenge for electronic health record systems.
The National Comprehensive Cancer Networkand the American Cancer Society also have re-sources and materials focused on survivorship is-sues, guidelines, and survivorship care plans;additionally, the COG provides exceptional guide-lines for survivors of childhood cancers. Othere-resources such as the Oncolink survivorshipcare plan tool, Oncolife, and A Prescription forLiving (a care planning tool developed for use innursing), are providing web-based survivorshiptools specifically for patients to use with theirhealth care team (Table 2). All of these resourcesare dedicated to assisting clinicians in providinghigh-quality survivorship care and empoweringand informing cancer survivors.
Implementing the Survivorship Care Plan
Each practice setting needs to decide on a strategythat will permit the implementation of survivor-
ship care plans: prevalent or incident cases?Cover all cancers or begin with one? A focus on in-cident cases may simply mean adding the survi-vorship care plan and discussion into the firstfollow-up visit after active treatment ends; focus-ing on prevalent cases may require doing outreachto patients who are no longer being seen in regularfollow-up care. Concentrating on one commoncancer, such as breast, may ease the transitionto using the care plans in a clinical practice. In ad-dition, decisions must be made on the format ofthe plan and the communication with other treat-ing physicians. Using uniform templates with dropdown menus, check boxes, and pre-populated datafields will reduce the amount of time needed tocomplete the plan. A consistent approach acrossthe practice is the most efficient method for imple-menting survivorship care plans for the survivorpopulation.
The key goal of survivorship care planning isbetter communication. Patients are often empow-ered by receiving a written document summariz-ing their diagnostic information and treatment,along with some discussion of potential late ef-fects. The plan can then be shared with manyfuture physicians. In addition, primary care pro-viders who receive a copy of the treatment sum-mary and survivorship care plan are extremelyappreciative and have reported greater self-effi-cacy in the follow-up care of cancer patients intheir practice. In addition, for busy medical oncol-ogists, having this single note in the chart can sim-plify follow-up care for patients who are seen lessfrequently after treatment ends.
THE CHALLENGE OF PROVIDING QUALITY CARE
FOR ADULT SURVIVORS OF CHILDHOOD CANCER
A lthough there are less than 20,000 childrendiagnosed each year with cancer in the
United States, thus representing only a small per-centage of the US cancer burden, significant bio-medical treatment advances resulting in curehave been made through high enrollment ratesonto pediatric cooperative group clinical trials.Several decades ago, pediatric cancer was consid-ered a uniformly fatal disease; however, througha cooperative nationwide enrollment effort ontoclinical trials, there is now an overall 80% survivalrate across the major 12 diagnostic categories ofchildhood cancer.15 Unlike the diagnostic cate-gories of adult malignancies that place emphasis

214 P.A. GANZ, J. CASILLAS, AND E.E. HAHN
on primary tumor site, childhood cancers repre-sent a diverse group of malignancies that place pri-mary emphasis on tumor morphology over site ofoccurrence. The International Classification ofChildhood Cancers, third edition (ICCC-3) in-clude: (1) leukemias, myeloproliferative and mye-lodysplastic diseases, (2) lymphomas, (3) centralnervous system neoplasms, (4) neuroblastomaand other peripheral nervous cell tumors, (5) ret-inoblastoma, (6) renal tumors, (7) hepatic tumors,(8) malignant bone tumors, (9) soft tissue andother extraosseous sarcomas (eg, rhabdomyosar-coma), (10) germ cell tumors, (11) other malig-nant epithelial neoplasms and malignantmelanomas (eg, thyroid and nasopharyngeal car-cinomas), and (12) other, unspecified malignantneoplasms).16 Thus, the low incidence of pediatricmalignancies coupled with this wide range of diag-nostic categories has dictated the need for enroll-ment onto clinical trials to determine the efficacyof complex combinations of chemotherapy, radia-tion therapy, and surgery. With aggressive treat-ment regimens, high cure rates have beenachieved, now as high as 95% for certain diagno-ses. Thus, there is a rapidly growing populationof childhood cancer survivors.
Currently, we are nearing the 300,000 mark ofchildhood cancer survivors within the US.17 Foryoung adult survivors defined as ages 20 to 39,the prevalence of childhood cancer survivors is1.56 per 1,000 (or an estimated 1 in 640 individ-uals).18 However, the story for childhood cancersurvivors does not end here. This population isat high risk for the development of chronic healthconditions (late effects) due to their previous can-cer treatment because of the long-term toxicity ofthe multimodal cancer therapy. Virtually everydeveloping organ system can be affected as a resultof chemotherapy, radiation, and/or surgery. Com-plications of treatment include problems withheart and lung function, growth, behavior, schoolperformance, and even additional cancers that of-ten occur several years to decades after their pre-vious cancer treatment.19-22 Similar to the needfor cooperative group clinical trials for definingthe best cancer treatment, a cooperative group ef-fort was needed to identify a large national cohortof childhood cancer survivors from which thelong-term health outcomes of this at-risk popula-tion could be defined. The Childhood Cancer Sur-vivor Study (CCSS), which was started in 1993and led by Les Robison, PhD, serves as a resourcedesigned to evaluate the long-term effects of can-
cer and associated therapies in 5-year survivors.The cohort initially included a consortium of 26centers and has over 20,000 subjects <21 yearsof age between 1970-1986 diagnosed with cancer.In 2007, the CCSS is in its 14th year of funding bythe National Cancer Institute, and as a result iscurrently recruiting a second set of survivor par-ticipants who were treated for cancer as childrenbetween 1987 and 1999. It is hypothesized thatthis more recently treated cohort may differ intheir late effects given that they have receivedmore contemporary treatment regimens in whichthere has been modification on treatment inten-sity based the risk for significant late effects.
Several seminal studies have been completed byCCSS investigators. Mertens et al8 have shown sta-tistically significant excess mortality rates be-cause of subsequent malignancies, along withcardiac and pulmonary disease in adult survivorsof childhood cancer when compared with age-matched US population mortality data. Further-more, survivors of childhood cancer have a highrate of illness owing to chronic health conditions,such as cardiovascular disease, congestive heartfailure, and renal failure when compared withthe sibling control group.6 In this CCSS studythe investigators found sobering statistics for therisk for chronic health conditions for this popula-tion. The cumulative incidence of a chronic healthcondition in adult childhood cancer survivorsreached 73.4% 30 years after the cancer diagnosisand 42.4% for severe, disabling, or life-threateningconditions or death caused by a chronic condition.Evaluation of health status of adult childhood can-cer survivors has also shown adverse generalhealth, mental health, activity limitations, andfunctional impairment when compared with sib-lings (with over 40% of survivors reported at leastone adversely affected health status domain).22
Lastly, the adult survivors of childhood cancerwho have the greatest risk for late effects, thosefurthest from their cancer treatment, are leastlikely to report long-term follow-up care.23
Given this growing body of literature clearlydemonstrating the significant risk for late effectsdue to previous cancer therapies, childhood can-cer survivors require risk-based, long-term fol-low-up care. Similar to the cooperative groupeffort to improve survival rates for pediatric malig-nancies, again the COG recognized the need todefine the essential elements of survivorship careat the national level so that the early detectionof late effects could occur for all at-risk survivors.

ENSURING QUALITY CARE FOR CANCER SURVIVORS 215
As a result, risk-based, exposure-related clinicalpractice guidelines have been developed by theCOG24 and are available for review at www.survi-vorshipguidelines.org. These guidelines are a hy-brid of both review of the scientific literature andexpert opinion and are ‘‘intended to increaseawareness of potential late effects and to standard-ize and enhance follow-up care provided to survi-vors of pediatric malignancies across theirlifespan.’’ In addition, there are downloadablehealth education materials for survivors entitled‘‘Health Links’’ to further assist health care pro-viders working with this population.
Even with availability of the COG childhoodcancer survivorship guidelines on the web, coordi-nation of care for adult childhood cancer survivorsremains a challenge given the transition that mustoccur from both the cancer subspecialist to thegeneralist, as well as from pediatric-centeredcare to adult-centered care. As Oeffinger and Robi-son25 discuss in a recent editorial, adult childhoodcancer survivors are now presenting to health careproviders who often are not aware of the associa-tion of previous childhood cancer treatment andthe associated risks of developing (potentiallymodifiable) chronic, common health conditions,such as cardiovascular disease or obesity. Thequestion that directly follows is. then what isthe best practice for coordinating care of adultchildhood cancer survivors? First, childhood can-cer survivors must have an end-of-cancer treat-ment summary prepared by their treatingpediatric oncologist(s) so that the COG survivor-ship guidelines can be used appropriately, giventhat they are exposure based. Second, a survivor-ship care plan is developed based on the COG sur-vivorship screening guidelines. Currently, this ismost often completed in a survivorship subspe-cialty clinic (such as that which is availablethrough the Lance Armstrong Foundation’s Survi-vorship Centers of Excellence network). Third,a primary care provider should be identified to as-sist the survivor with coordination of the recom-mended late-effects screening and referral toneeded subspecialty care.
Coordinating the care for adult childhood can-cer survivors can represent a challenge for pri-mary care providers, given the complexity ofrecommended late effects screening tests coupledwith the risk for significant, life-threateningchronic health problems occurring at earlierthan expected ages. For example, survivors re-quire many screening tests that need to be done
before the standard recommendations for thehealthy US population (eg, mammograms to bedone in the early 20s if there is an exposure tochest radiation because of the higher risk forbreast cancer). In addition, adult childhood can-cer survivors may have common yet non-specificsymptoms, such as pain and fatigue, which are of-ten difficult to determine whether or not they arerelated to their previous cancer history/ treatmentversus other non-cancer related factors. Corre-spondingly, the best treatment plan aimed atresolving the symptoms may be difficult to accom-plish and may instead require a palliative care ap-proach. Often, emphasis must be placed onminimizing symptoms instead of complete elimi-nation of the symptoms. An additional layer ofcomplexity when coordinating care of the adultchildhood cancer survivor is the need for referralto multiple subspecialists (eg, cardiologists, pul-monologists, endocrinologists). Furthermore, sub-specialists must be aware of the accelerated risk ofchronic diseases in childhood cancer survivors(eg, atherosclerosis or the risk for myocardial dis-ease in the fourth decade of life). Ultimately, thekey to maximizing the quality of care for adultchildhood cancer survivors at this point in timeis to have the cancer survivorship subspecialistfacilitate two-way communication between theprimary care provider and the various subspecial-ists involved in the care of the survivor. In addi-tion, the treatment summary/survivorship careplan can serve as the communication vehicleand educational resource for questions regardingthe complexity of care for this at-risk population.
HEALTH POLICY IMPLICATIONS OF THE
SURVIVORSHIP CARE PLAN
T he need for coordination of care for cancersurvivors is emblematic of the challenges
faced by many patients with chronic diseases,where complex care is often delivered by special-ists in the absence of primary care involvement.In addition, the real or perceived shortage of pri-mary care providers in the US leads patients torely heavily on their subspecialty physicians. Un-fortunately, as a result, many important healthcare processes are often ignored or overlooked inspecialty-only care. Indeed, several studies in theMedicare population have shown that optimal can-cer care occurs when adult cancer patients aretreated by both cancer specialists and primary

216 P.A. GANZ, J. CASILLAS, AND E.E. HAHN
care providers.26-28 No doubt similar findingswould occur in other chronic diseases. The impor-tant role of preventive health services for non-cancer conditions, as well as management ofcomorbid conditions, cannot be overlooked inthe cancer survivor. The implementation of treat-ment summaries and survivorship care plans maybe a first step in enhancing better care for cancersurvivors, and may serve as a model testable inother chronic diseases. Two recent efforts callfor the implementation of treatment summariesinto the standard care of cancer patients and sur-vivors: Legislation pending in Congress (‘‘Compre-hensive Cancer Care Improvement Act’’ HR 1078),and the recently developed Oncology PhysicianPerformance Measurement Set developed byASCO and the American Society of TherapeuticRadiation Oncology with the American MedicalAssociation Physician Consortium for Perfor-mance Improvement.
CONCLUSION
M edical and pediatric oncology are relativelyyoung specialties compared with surgery
and radiation oncology. Surgeons have tradition-ally described their cancer treatment (surgery)with a detailed operative note. Similarly, it is cus-tomary for radiation oncologists to provide a treat-ment summary of the amount of radiation givenand the specific ports involved, including a descrip-tion of the local tissue tolerance and acute treat-ment toxicities. Until the last half of the 20thcentury, pharmacologic treatments for cancerwere primarily palliative. With the advent of com-bination chemotherapy and multimodality thera-pies, many pediatric and adult cancers are nowcurable. However, treatment is administeredover a prolonged period of time, largely in the out-patient setting. The tradition of preparing a treat-
ment summary is largely absent from the culture.In childhood cancers, the vast majority of patientsare treated on clinical trials, making recovery ofsuch information somewhat easier, but becauseof dosage reductions or changes in treatment, ex-act drug doses may be difficult to reconstruct.Thus, an end-of-treatment summary is invaluable,and this can be linked to the COG guidelines forsurvivorship care, as described earlier.
Similarly, for adult cancer patients, cure is com-mon for a variety of hematologic and epithelialmalignancies. Documentation of drug type anddosages received will ultimately be important, asmore information is gathered about the late toxic-ities of various treatments. Because cancer inolder adults frequently co-occurs with other co-morbid conditions, communication about knownpotential organ toxicities (eg, heart, lung, kidney)to the patient and their primary care providers arelikely to be critical in the prevention of secondarylate and long-term effects. Furthermore, the devel-opment of a treatment summary and care plan isessential for improving the quality and coordina-tion of care for the growing population of cancersurvivors. The time has come for this to occur,and we predict that 2008 will be the tipping pointfor widespread adoption of the cancer treatmentsummary and survivorship care plan. As theseefforts roll out in the coming years, through bothnatural and planned experiments, there will beample opportunity for formal research and infor-mal evaluative projects. Examination of patientand provider satisfaction are key measures, but re-duction in duplication/unnecessary testing andbetter coordination care will be important out-comes to measure. Nurses are logical participantsin this effort as part of the health care models thatwill deliver this care, as well as researchers whocan examine outcomes in patient populationsthat they serve.
REFERENCES
1. Chassin MR, Galvin RW, and the National Roundtable on
Health Care Quality. The urgent need to improve health care
quality. Institute of Medicine National Roundtable on Health
Care Quality. JAMA 1998;280:1000–1005.
2. Hewitt M, Simone JV. Ensuring quality cancer care. Wash-
ington, DC: National Academy Press; 1999.
3. Kohn LT, Corrigan J, Donaldson M. To err is human: build-
ing a safer health system. Washington, DC: National Academy
Press; 2000.
4. Kohn LT, Corrigan JM, Donaldson MS. Crossing the qual-
ity chasm: a new health system for the 21st century. Washing-
ton, DC: National Academy Press; 2001.
5. Hewitt M, Greenfield S, Stovall E. From cancer patient to
cancer survivor: lost in transition. Washington, DC: The Na-
tional Academies Press; 2006.
6. Oeffinger KC, Mertens AC, Sklar CA, et al. Chronic health
conditions in adult survivors of childhood cancer. N Engl J Med
2006;355:1572-1582.

ENSURING QUALITY CARE FOR CANCER SURVIVORS 217
7. Kenney LB, Yasui Y, Inskip PD, et al. Breast cancer after
childhood cancer: a report from the Childhood Cancer Survivor
Study. Ann Intern Med 2004;141:590-597.
8. Mertens AC, Yasui Y, Neglia JP, et al. Late mortality expe-
rience in five-year survivors of childhood and adolescent can-
cer: the Childhood Cancer Survivor Study. J Clin Oncol 2001;
19:3163-3172.
9. Syrjala KL, Roth-Roemer SL, Abrams JR, et al. Preva-
lence and predictors of sexual dysfunction in long-term survi-
vors of marrow transplantation. J Clin Oncol 1998;16:3148-
3157.
10. Shankar SM, Carter A, Sun CL, et al. Health care uti-
lization by adult long-term survivors of hematopoietic cell
transplant: report from the Bone Marrow Transplant Survi-
vor Study. Cancer Epidemiol Biomarkers Prev 2007;16:834-
839.
11. Fraser CJ, Bhatia S, Ness K, et al. Impact of chronic graft-
versus-host disease on the health status of hematopoietic cell
transplantation survivors: a report from the Bone Marrow
Transplant Survivor Study. Blood 2006;108:2867-2873.
12. Hewitt M, Ganz PA. Implementing cancer survivorship
care planning: workshop summary. Washington, DC: National
Academies Press; 2007.
13. Ganz PA. Monitoring the physical health of cancer survi-
vors: a survivorship-focused medical history. J Clin Oncol 2006;
24:5105-5111.
14. Wolff SN, Nichols C, Ulman D, et al. Survivorship: an un-
met need of the patient with cancer-implications of a survey of
the Lance Armstrong Foundation (LAF) [abstract]. Proc Am
Soc Clin Oncol 2005;23(suppl):6032.
15. Gatta G, Capocaccia R, Coleman MP, et al. Childhood
cancer survival in Europe and the United States. Cancer
2002;95:1767-1772.
16. Steliarova-Foucher E, Stiller C, Lacour B, et al. Interna-
tional classification of childhood cancer. Ed 3. Cancer 2005;
103:1457-1467.
17. Ries LAG, Eisner MP, Kosary CL, et al. SEER cancer
statistics review, 1973-1998. Bethesda, MD: National Cancer In-
stitute; 2001.
18. Weiner SL, Hewitt ME, Simone JV. Childhood cancer sur-
vivorship: improving care and quality of life. Washington, DC:
National Academies Press; 2003.
19. Lipshultz SE, Colan SD, Gelber RD, et al. Late cardiac
effects of doxorubicin therapy for acute lymphoblastic leukemia
in childhood. N Engl J Med 1991;324:808-815.
20. Meister LA, Meadows AT. Late effects of childhood
cancer therapy. Curr Probl Pediatr 1993;23:102-131.
21. Gleeson HK, Shalet SM. Endocrine complications of
neoplastic diseases in children and adolescents. Curr Opin
Pediatr 2001;13:346-351.
22. Hudson MM, Mertens AC, Yasui Y, et al. Health status of
adult long-term survivors of childhood cancer: a report from the
Childhood Cancer Survivor Study. JAMA 2003;290:1583-1592.
23. Oeffinger KC, Mertens AC, Hudson MM, et al. Health care
of young adult survivors of childhood cancer: a report from the
Childhood Cancer Survivor Study. Ann Fam Med 2004;2:61-70.
24. Landier W, Bhatia S, Eshelman DA, et al. Development of
risk-based guidelines for pediatric cancer survivors: the Chil-
dren’s Oncology Group long-term follow-up guidelines from
the Children’s Oncology Group Late Effects Committee and
Nursing Discipline. J Clin Oncol 2004;22:4979-4990.
25. Oeffinger KC, Robison LL. Childhood cancer survivors,
late effects, and a new model for understanding survivorship.
JAMA 2007;297:2762-2764.
26. Earle CC, Neville BA. Under use of necessary care among
cancer survivors. Cancer 2004;101:1712-1719.
27. Earle CC, Burstein HJ, Winer EP, et al. Quality of non-
breast cancer health maintenance among elderly breast cancer
survivors. J Clin Oncol 2003;21:1447-1451.
28. Earle CC. Failing to plan is planning to fail: improving the
quality of care with survivorship care plans. J Clin Oncol 2006;
24:5112-5116.