Embed Size (px)
Citation preview

Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/10625856
EndovenousLaserTreatmentofSaphenousVeinReflux:Long-TermResults
ARTICLEinJOURNALOFVASCULARANDINTERVENTIONALRADIOLOGY·SEPTEMBER2003
ImpactFactor:2.41·DOI:10.1097/01.RVI.0000082864.05622.E4·Source:PubMed
CITATIONS
301
READS
66
3AUTHORS,INCLUDING:
NeilMKhilnani
CornellUniversity
59PUBLICATIONS1,182CITATIONS
SEEPROFILE
StevenZimmet
ZimmetVeinandDermatology
32PUBLICATIONS807CITATIONS
SEEPROFILE
Availablefrom:StevenZimmet
Retrievedon:07January2016

Endovenous Laser Treatment of SaphenousVein Reflux: Long-Term ResultsRobert J. Min, MD, Neil Khilnani, MD, and Steven E. Zimmet, MD
PURPOSE: To report long-term follow-up results of endovenous laser treatment for great saphenous vein (GSV) refluxcaused by saphenofemoral junction (SFJ) incompetence.
MATERIALS AND METHODS: Four hundred ninety-nine GSVs in 423 subjects with varicose veins were treated overa 3-year period with 810-nm diode laser energy delivered percutaneously into the GSV via a 600-�m fiber. Tumescentanesthesia (100–200 mL of 0.2% lidocaine) was delivered perivenously under ultrasound (US) guidance. Patients wereevaluated clinically and with duplex US at 1 week, 1 month, 3 months, 6 months, 1 year, and yearly thereafter to assesstreatment efficacy and adverse reactions. Compression sclerotherapy was performed in nearly all patients at follow-upfor treatment of associated tributary varicose veins and secondary telangiectasia.
RESULTS: Successful occlusion of the GSV, defined as absence of flow on color Doppler imaging, was noted in 490of 499 GSVs (98.2%) after initial treatment. One hundred thirteen of 121 limbs (93.4%) followed for 2 years haveremained closed, with the treated portions of the GSVs not visible on duplex imaging. Of note, all recurrences haveoccurred before 9 months, with the majority noted before 3 months. Bruising was noted in 24% of patients andtightness along the course of the treated vein was present in 90% of limbs. There have been no skin burns,paresthesias, or cases of deep vein thrombosis.
CONCLUSIONS: Long-term results available in 499 limbs treated with endovenous laser demonstrate a recurrencerate of less than 7% at 2-year follow-up. These results are comparable or superior to those reported for the otheroptions available for treatment of GSV reflux, including surgery, US-guided sclerotherapy, and radiofrequencyablation. Endovenous laser appears to offer these benefits with lower rates of complication and avoidance of generalanesthesia.
J Vasc Interv Radiol 2003; 14:991–996
Abbreviations: GSV � great saphenous vein, RF � radiofrequency, SFJ � saphenofemoral junction
LOWER-extremity venous insuffi-ciency is a common medical conditionafflicting 25% of women and 15% ofmen in the United States (1). Gender,pregnancy, hormones, aging, andgravitational forces from prolongedstanding or sitting are the most com-mon factors that influence the appear-
ance or worsening of primary varicoseveins (2,3). Although many peopleseek medical treatment for varicoseveins because they find them un-sightly, most people with varicoseveins do experience symptoms (4,5).Unfortunately, symptoms of primaryvenous insufficiency are often not rec-
ognized by patients or their physi-cians. Characteristic leg complaints as-sociated with varicose veins includeaching pain, night cramps, fatigue,heaviness, or restlessness. Symptomsarise from pressure on somatic nervesby dilated veins and are typicallyworsened with prolonged standing,during the premenstrual period, or inwarm weather (6). Left untreated,nearly 50% of patients with significantsuperficial venous insufficiency willeventually experience chronic venousinsufficiency characterized by lower-extremity swelling, eczema, pigmenta-tion, hemorrhage, and ulceration (7).
Great saphenous vein (GSV) refluxis the most common underlying causeof significant varicose veins. Tradi-tional treatment of GSV reflux hasbeen surgical removal of the GSV. Al-
From Cornell Vascular (R.J.M., N.K.), Weill MedicalCollege of Cornell University, 416 East 55th Street,New York, New York 10022; and Zimmet Vein andDermatology Clinic (S.E.Z.), Austin, Texas. ReceivedJanuary 24, 2003; revision requested April 11; revi-sion received May 7; accepted May 8. From the 2003SIR Annual Meeting. Address correspondence toR.J.M.; E-mail: [email protected]
R.J.M. is a consultant to Diomed (Andover, MA),assisting in development of medical treatments andphysician training. R.J.M. is coinventor and partowner of a patent on endovenous laser treatment of
veins, for which he receives royalties. R.J.M. andCornell Vascular have paid for all medical equip-ment used in procedures relating to this study.S.E.Z. is a paid consultant to Diomed, Inc. (Andover,MA), assisting in development of medical treat-ments. S.E.Z. is also paid to assist in physican train-ing. S.E.Z. purchased all medical equipment he usedin connection with this study. The other author hasnot identified a potential conflict of interest.
© SIR, 2003
DOI: 10.1097/01.RVI.0000082864.05622.E4
991

though surgical ligation and strippingof the GSV has been the most durabletreatment, it is associated with signif-icant perioperative morbidity. Less-in-vasive surgical treatments includinghigh ligation of the GSV at the saphe-nofemoral junction (SFJ) have been at-tempted with the hope that gravita-tional reflux would be controlledwhile the vein is preserved for possi-ble use as a bypass graft. Unfortu-nately, ligation of the GSV alone usu-ally results in recurrent varicose veins(8). Even when high ligation has beencombined with phlebectomy of vari-cose tributaries or retrograde sclero-therapy, recurrence has been the rule(9,10). Therefore, when it is deter-mined that GSV reflux is the principalunderlying problem, treatment shouldinvolve eliminating this source of re-flux with ablation of any associatedincompetent venous segments.
In 1999, Boné (11) first reported ondelivery of endoluminal laser energy.Since then, a method for treating theentire incompetent GSV segment hasbeen described (12,13). Endovenouslaser treatment, which received ap-proval from the US Food and DrugAdministration in January 2002, al-lows delivery of laser energy directlyinto the blood vessel lumen. Non-thrombotic vein occlusion is accom-plished by heating the vein wall with810-nm-wavelength laser energy de-livered via a 600-�m laser fiber(Diomed, Andover, MA). Sufficientheating of the vein wall is necessary tocause collagen contraction and denu-dation of endothelium. This stimulatesvein wall thickening, eventual luminalcontraction, and fibrosis of the vein.The purpose of this study is to reporton the long-term follow-up results ofendovenous laser treatment for GSVreflux.
MATERIALS AND METHODS
This prospective, nonrandomized,consecutive-enrollment study in-cluded 423 patients who underwentendovenous laser treatment of incom-petent GSV segments with 810-nm di-ode laser energy delivered intralumi-nally for treatment of primary varicoseveins. The study protocol was ap-proved by the Weill Medical Collegeof Cornell University Institutional Re-view Board. All patients gave writteninformed consent before treatment.
Patient Selection
Directed history and physical ex-amination, including duplex ultra-sound (US) evaluation of the superfi-cial venous system, was performed onlimbs of subjects with varicose veins.Study inclusion criteria included vari-cose veins caused by SFJ incompetencewith GSV reflux as demonstrated byduplex US imaging, age of at least 18years, and ability to return for sched-uled follow-up examinations for 12months after endovenous laser treat-ment. Exclusion criteria included non-palpable pedal pulses; inability to am-bulate; deep vein thrombosis; generalpoor health; pregnancy, nursing, orplans to become pregnant during thecourse of participation in the investi-gation; and extremely tortuous GSVsthat would not allow endovenouscatheterization and passage of the la-ser fiber as identified on pretreatmentvenous duplex US mapping. After ini-tial consultation and evaluation, sub-jects meeting the appropriate criteriawere offered surgery versus en-dovenous laser treatment. Nearly allsubjects chose endovenous laser oversurgical ligation and stripping.
Five hundred four incompetentGSVs were treated with endovenouslaser over a 39-month period. Fivelimbs were lost to follow-up. The re-maining 499 limbs in 423 patients com-prise the study population. This groupconsists of 352 women (83%) and 71men (17%) ranging in age from 23 to72 years, with a mean age of 42 years.
Follow-up ranged from 1 month to39 months with a mean follow-up pe-riod of 17 months and an SD of 11months. Aching leg pain was the mostcommon presenting symptom, foundin 87% of limbs. Overall, slightly moreleft legs (n � 263, 53%) were treated,and 76 patients (18%) were treated forbilateral GSV reflux. PretreatmentGSV diameter, measured in the up-right position approximately 2 cm be-low the SFJ, ranged from 4.4 mm to 29mm (mean, 11 mm; SD, 4.2 mm).
None of the patients in this seriesunderwent concomitant ambulatoryphlebectomy. All but seven patientsunderwent compression sclerotherapytreatment of distal varicose tributariesor associated telangiectasias at fol-low-up visits.
Description of Technique
Duplex US was performed in theupright position to map incompetentsources of venous reflux and then tomark the skin overlying the incompe-tent portion of the GSV starting at theSFJ. After venous duplex mapping, apercutaneous entry point was chosen.This point may be where reflux is nolonger seen or where the GSV becomestoo small to access (usually just aboveor below knee level). With use of localanesthesia and sonographic guidance,the GSV was punctured. A 5-F intro-ducer sheath was placed into the GSVover a guide wire and advanced pastthe SFJ into the femoral vein. Intralu-minal position within the GSV wasconfirmed by aspiration of nonpulsa-tile venous blood and visualizationwith US.
The sheath was flushed and a600-�m laser fiber (Diomed) was in-serted in the sheath and advanced upto the first site mark, indicating thatthe distal tip of the laser fiber wasflush with the end of the sheath. Thesheath was then withdrawn to the sec-ond site mark, exposing the distal 3 cmof the bare-tipped laser fiber. Thesheath and fiber were pulled back to-gether and positioned at the SFJ underUS guidance. Position was confirmedby direct visualization of the red aim-ing beam of the laser fiber through theskin.
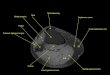
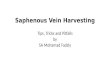
Tumescent local anesthesia consist-ing of 100–200 mL of 0.2% lidocaineneutralized with sodium bicarbonate,was administered along the perive-nous space with use of US guidance.In addition to the anesthetic effects,properly delivered, this fluid servestwo important functions: (1) it com-presses and reduces the diameter ofeven the largest veins to provide veinwall apposition around the fiber tipwith subsequent circumferential heat-ing of the vein wall and (2) it providesa “heat sink” to minimize the possibil-ity of heat-related damage to adjacenttissues. Figure 1a demonstrates thetypical transverse sonographic ap-pearance of the laser fiber and catheterseen centrally within an enlarged GSVlocated in the saphenous space. Properand adequate delivery of tumescentanesthesia should result in fluid sur-rounding a compressed GSV as shownin Figure 1b.
The tip of the laser fiber was repo-
992 • Endovenous Laser Treatment of Saphenous Vein Reflux August 2003 JVIR

sitioned within the GSV 5–10 mm dis-tal to the SFJ. Tip position was checkedby US and direct visualization of thered aiming beam through the skin. La-ser energy (810-nm diode laser;Diomed) was delivered at 14 W in con-tinuous mode. The vein was treatedfrom 5–10 mm below the SFJ to ap-proximately 1 cm above the skin entrysite. Length of GSV treated with en-dovenous laser ranged from 10 cm to55 cm (mean, 35 cm; SD, 10 cm). Thelaser fiber was withdrawn at an aver-age rate of 3 mm per second (18 cm perminute). Of patients treated with 14-Wcontinuous mode (n � 276, or 55% oflimbs), delivery of laser energy rangedfrom 25 seconds (at 358 J) to 187 sec-onds (at 2,615 J), with a mean of 123seconds (SD, 47 sec) or 1,727 J (SD, 650J).
A class II (30–40 mm Hg) full-thighgraduated support stocking or pantyhose was worn for at least 1 week at alltimes except to sleep or to shower.Patients were instructed to ambulateand resume their normal daily activi-ties immediately. Clinical and duplexUS follow-up was obtained at 1 week,1, 3, 6, 9, and 12 months, and thenyearly.
Compression sclerotherapy treat-
ment of distal varicose tributaries wasperformed with use of sodium tetra-decyl sulfate (0.3%–1% concentration).A detailed description of sclerother-apy technique is beyond the scope ofthis article but the approach used wasthe “French school” originally advo-cated by Tournay and more recentlypopularized in the United States byGoldman and other phlebologists (14).This technique relies on starting fromthe highest points of reflux and pro-ceeding downward, and treating veinsfrom the largest to the smallest. Com-pression stockings or panty hose wereworn for at least 1 week after sclero-therapy treatments except to sleep orshower. Sclerotherapy treatmentswere performed at 4-week intervals,starting 1 month after endovenous la-ser ablation of the GSV.
Study Endpoints and Definitions
Duplex US criteria for successfultreatment were the following: at1-week follow-up, an enlarged non-compressible GSV, minimally de-creased in diameter, with echogenic,thickened vein walls, and no flow seenwithin the occluded vein lumen oncolor Doppler interrogation; at 3- and
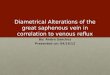
6-month follow-up, an occluded GSVwith substantial (�50%) reduction indiameter; and at 1 year and beyond,complete disappearance of the GSV orminimal residual fibrous cord with noflow detectable. It is important to notethat the expected appearance 1–2weeks after endovenous laser is aslightly smaller GSV demonstratingwall thickening with absence of flowwithin the treated vein segment. Thevein lumen is usually obliterated bythe thickened wall, which has low-level echoes and is incompressible.This wall thickening should be differ-entiated from acute GSV thrombosiswherein the vein is also incompress-ible but the lumen is filled with ane-choic acute thrombus. Several weeksafter successful endovenous lasertreatment, resolution of the acute in-flammation in the vein wall shouldresult in reduction in vein diameter.After several months, most of thetreated vein segments will fibrose andbe difficult to identify. Alternatively,superficial thrombophlebitis with GSVthrombus would result in recanaliza-tion of the vein. A longitudinal view ofan enlarged, incompetent GSV is seenin Figure 2a. Figure 2b demonstratesthe typical color Doppler appearanceof a successfully treated GSV 1 yearafter endovenous laser treatment.
Clinical evaluation was performedon all subjects at 1 week, 1, 3, 6, 9, and12 months, and yearly thereafter bythe same physician (R.M.) who per-formed all the endovenous laser pro-cedures. Patients were queried aboutsymptomatic relief at follow-up visits,particularly improvement or resolu-tion of lower-extremity pain believedto be associated with venous insuffi-ciency. Improvement in the appear-ance of the leg, including reduction invisible varicosities, swelling, pigmen-tation, or other skin changes second-ary to chronic venous insufficiency,were assessed by the patient and withdirect comparison with pretreatmentphotographs obtained from all sub-jects undergoing treatment. Patientswere evaluated for possible adversereactions caused by endovenous lasertreatment at each follow-up visit. Mi-nor complications were defined asthose that had no significant clinicalsequelae, such as bruising. Major com-plications were defined as those neces-sitating an increased level of care, sur-
Figure 1. Duplex US (transverse view) demonstrating appearance of the GSV before andafter proper delivery of tumescent anesthesia. (a) Intraluminal position of laser fiber andcatheter within an enlarged GSV; (b) tumescent anesthesia delivered by echogenic needletip adjacent to laser fiber and catheter with fluid surrounding the compressed GSV.
Min et al • 993Volume 14 Number 8

gery, hospitalization, or permanentadverse sequelae.
RESULTS
Follow-up results ranging from 1month to 39 months (mean, 17months; SD, 11 months) were obtainedin 499 of the 504 limbs treated withendovenous laser during the study pe-riod. Successful endovenous lasertreatment, as defined earlier, was seenin 490 of 499 limbs (98%) at 1-monthfollow-up. Eight of nine GSVs requir-ing repeat endovenous laser were suc-cessfully closed with a second en-dovenous laser treatment. Continuedclosure of the treated GSV segmentswas noted at longitudinal follow-up atthe following rates: 444 of 447 (99.3%)at 3 months, 390 of 396 (98.5%) at 6months, 351 of 359 (97.8%) at 9months, 310 of 318 (97.5%) at 1 year,and 113 of 121 (93.4%) at 2 years. Fortysubjects have been followed for 3years and no new recurrences wereseen at 2 or 3 years that were notpresent at 1-year follow-up. In fact, allrecurrences were noted before 9months, with the majority seen by 3months. This may indicate that thesewere not true recurrences but ratherinadequate initial treatments.
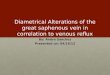
Clinical examination correlatedwell with duplex US findings. All pa-tients showed improvement in the ap-pearance of the limb with disappear-ance or reduction in the size andnumber of visible varicosities. Thetypical appearance of varicose veinscaused by incompetence of the SFJwith GSV reflux is shown in Figure 3a.
One month after endovenous lasertreatment, relief of symptoms and sig-nificant improvement in the appear-ance of the varicose veins was noted(Fig 3b). By 6 months after initialtreatment, pain was greatly im-proved or resolved in all treatedlimbs. Although symptomatic reso-lution and significant improvementin the appearance of the leg is usu-ally noted after endovenous lasertreatment alone, most patients willneed additional complementary pro-cedures (ie, sclerotherapy or phle-bectomy) to fully realize the restor-ative benefits of treatment.
Bruising outside the puncture sitewas noted in 24% of limbs at 1-weekfollow-up. Bruising resolved in allsubjects before 1-month follow-up.Ninety percent of subjects felt a de-layed tightness peaking 4–7 days afterlaser treatment and lasting 3–10 days.This sensation, described as “pulling”along the course of the treated GSV,was not felt in the nine patients inwhom initial treatment failed. Fivepercent of patients developed superfi-cial phlebitis of varicose tributaries af-ter endovenous laser occlusion of theGSV. Most cases required no treat-ment. Symptomatic patients weretreated with graduated compressionstockings and over-the-counter antiin-flammatory agents. All minor compli-cations listed earlier resolved withoutsequelae. There have been no skinburns, paresthesias, cases of deep veinthrombosis, or other minor or majorcomplications. The procedure was
well-tolerated by all subjects withstrictly local anesthesia.
Overall treatment satisfaction wasdetermined by asking subjects if theywould recommend the procedure to afriend with similar leg vein problems,and 422 of 423 subjects (99.8%) indi-cated they would recommend theprocedure.
DISCUSSION
Percutaneous methods for treatingincompetent GSVs are not new. Du-plex-guided sclerotherapy for treat-ment of GSV reflux has been at-tempted, but long-term studies havefailed to prove durability comparableto surgery (15–19). Initial attempts atdamaging vein walls by electrocoagu-lation involved creation of a thrombuswithin the vessel lumen, ultimately re-sulting in recanalization (20–22). Earlymethods of intraluminal delivery ofhigh-frequency alternating-current ra-diofrequency (RF) energy to treat GSVreflux were complicated by skinburns, saphenous nerve and peronealnerve injury, phlebitis, and wound in-fection (23).
A more modern technique of theuse of RF energy to eliminate saphe-nous vein reflux has been developedby VNUS Medical Technologies(Sunnyvale, CA). Early results re-ported from a multicenter trial dem-onstrated a reasonable degree of suc-cess with an overall failure rate of 10%at a mean follow-up of 4.7 months(13% in patients treated with RF aloneand 5% in patients treated with RFplus high ligation of the GSV). Com-plications included transient paresthe-sias (thigh, 9%; leg, 51%), skin burns(3%), deep venous thrombosis (3%),and one pulmonary embolus (24).More recent studies have demon-strated success rates of 73%–90% withfollow-up to 24 months in 21 limbs(25–27).
One of the limitations of our studyis that it does not provide a blinded,randomized comparison of the vari-ous modern percutaneous methodsavailable for treatment of GSV reflux,including RF and wavelengths of laserenergy other than 810 nm. However,review of the literature allows somecomparisons and raises some interest-ing areas for future study.
RF current damages tissue by resis-tive heating of structures in direct con-
Figure 2. Color Doppler examinations (longitudinal views) of the GSV at the SFJdemonstrating successful occlusion after endovenous laser treatment. (a) Pretreatmentevaluation demonstrates an enlarged GSV with reflux after distal calf compression; (b)1-year follow-up examination shows typical “cul-de-sac” appearance of the proximal GSVwith occlusion of the treated segment.
994 • Endovenous Laser Treatment of Saphenous Vein Reflux August 2003 JVIR

tact with the electrodes. Deeper tissueplanes are heated by conduction intonormothermic tissue. Because the po-tential for heating of adjacent perive-nous tissue is high, safe treatmentwith RF depends on proper delivery ofadequate tumescent anesthesia. Effec-tive use of tumescent anesthesia ap-pears to have reduced the incidence ofheat-related complications. In experthands, the incidence of paresthesiasafter RF has occurred in as few as 8.5%of limbs within 1 week of treatmentand decreased to 0.7% at 6 months(27). However, with less-experiencedphysicians, RF still has been compli-cated with heat-related adverse effectssuch as paresthesias (10% at 6 months)and skin burns (3.3%) (25).
Published experience with en-dovenous laser with use of wave-lengths other than 810 nm is limited. Arecent study by Chang and Chua (28)reported the use of 1,064-nm laser en-ergy delivered endovenously for treat-ment of GSV reflux. Although thisstudy reported a success rate of 96.8%
in 244 legs followed up to 28 months,significant complications were noted,including paresthesias (36.5%) andskin burns (4.8%). In addition to en-dovenous laser ablation, all patients intheir study underwent surgical liga-tion and division of the proximal anddistal ends of the treated GSV. In ad-dition, patients treated with the1,064-nm wavelength underwent spi-nal or general anesthesia rather thanstrictly local tumescent anesthesia (28).
In comparison, in our series of morethan 500 limbs treated with 810-nmdiode laser energy delivered en-dovenously, there have been no heat-related complications despite the hightemperatures attained at the laser fibertip. This may be explained by the fol-lowing: (1) improved delivery and useof sufficient amounts of tumescentfluid in the proper tissue plane pro-viding a protective thermal “sink;” (2)selective, homogeneous, and circum-ferential heating of the inner vein wallby absorption of 810-nm laser energyby blood lining the vein wall, as noted
in a recent study by Proebstle et al(29), rather than deeper penetration oflaser energy and less-homogeneousheating from endovenous laser per-formed with wavelengths such as1,064 nm, which are absorbed less byblood and more by water; and (3)faster rates of withdrawal and shal-lower depth of penetration of 810-nmlaser energy, resulting in less damageto surrounding nontarget tissue com-pared with methods that use RF.
It has been suggested that a ran-domized controlled trial comparingoutcomes of endovenous laser abla-tion of the saphenous vein to surgicalligation and stripping should be per-formed; however, such a study wouldbe difficult given patients’ over-whelming desire for minimally inva-sive treatments rather than surgery.Review of the existing surgical litera-ture does provide some insight in as-sessing treatment durability. Multiplestudies have shown that recurrence ofvaricose veins after GSV stripping oc-curs early (30), with 73% of limbs des-tined for recurrent varicosities at 5years already having them at 1 year(31,32). Our results with endovenouslaser have supported this, demonstrat-ing that what is found on duplex im-aging early is predictive of what willbe seen later, with none of the treatedpatients developing recanalization ofsuccessfully occluded GSVs at 2 or 3years that was not seen before 9months.
Performing endovenous ablation ofthe GSV without dissection of the SFJviolates a cardinal rule in saphenousvein surgery that each of the tributar-ies must be individually divided. Sur-prisingly, the combined experienceswith transcatheter endovenous abla-tion procedures have shown lower re-currence rates than with surgical liga-tion and stripping. Perhaps minimizingdissection in the groin and preservingvenous drainage in normal, competenttributaries while removing only theabnormal refluxing segments does notincite neovascularization.
The understanding of venous disor-ders continues to improve with tre-mendous strides being made over thepast decade. Readily available nonin-vasive diagnostic tests allow physi-cians to precisely map out abnormalvenous pathways and identify sourcesof incompetence. Modern percutaneousmethods of sealing incompetent veins
Figure 3. Significant improvement in appearance of varicose tributaries after en-dovenous laser treatment of an incompetent left GSV. (a) Typical appearance of varicoseveins caused by GSV reflux; (b) the same leg 1 month after endovenous laser treatment.
Min et al • 995Volume 14 Number 8

provide patients with alternatives to li-gation and stripping for treatment ofGSV reflux without the familiar morbid-ities associated with surgery (33,34).Given these recent advances, many phy-sicians, when properly trained, will nowbe able to successfully diagnose andtreat the whole spectrum of superficialvenous insufficiency, offering accept-able options to the millions of people inthe United States alone who have vari-cose veins but are unwilling or unable toundergo surgery.
References1. Callam MJ. Epidemiology of varicose
veins. Br J Surg 1994; 81:167–173.2. Rose SS. Anatomic observations on
causes of varicose veins. In: GoldmanMP, Weiss RA, Bergan JJ, eds. Varicoseveins and telangiectasia: diagnosis andtreatment, St Louis: Quality MedicalPublishing, 1999; 12–17.
3. Goldman M. Pathophysiology of var-icose veins. In: Goldman M, ed. Sclero-therapy: treatment of varicose and tel-angiectatic leg veins. St. Louis: Mosby–Year Book, 1995; 85–117.
4. Weiss R, Weiss M. Resolution of painassociated with varicose and telangiec-tatic leg veins after compression sclero-therapy. J Dermatol Surg Oncol 1990;16:333–336.
5. Wilder CS. Prevalence of selectedchronic circulatory conditions. VitalHealth Stat 1974; 10:1–55.
6. Fegan WG, Lambe R, Henry M. Ste-roid hormones and varicose veins.Lancet 1967; 2:1070–1071.
7. Widmer LK, Mall TH, Martin H. Ep-idemiology and social medical impor-tance of diseases of the veins. MunchMed Wochenschr 1974; 116:1421–1426.
8. McMullin GM, Smith PDC, Scurr JH.Objective assessment of high ligationwithout stripping the long saphenousvein. Br J Surg 1991; 78:1139–1142.
9. Stonebridge PA, Chalmers N, Beggs I,Bradbury AW, Ruckley CV. Recur-rent varicose veins: a varicographicanalysis leading to a new practical clas-sification. Br J Surg 1995; 82:60–62.
10. Rutgers PH, Kitslaar PJEHM. Ran-domized trial of stripping versus highligation combined with sclerotherapyin the treatment of incompetent greatersaphenous vein. Am J Surg 1994; 168:311–315.
11. Boné C. Tratamiento endoluminal de
las varices con laser de diodo: estudiopreliminary. Rev Patol Vasc 1999; 5:35–46.
12. Navarro L, Min R, Boné C. En-dovenous laser: a new minimally inva-sive method of treatment for varicoseveins-preliminary observations usingan 810 nm diode laser. Dermatol Surg2001; 27:117–122.
13. Min R, Zimmet S, Isaacs M, ForrestalM. Endovenous laser treatment of theincompetent greater saphenous vein. JVasc Interv Radiol 2001; 12:1167–1171.
14. Cornu-Thenard A, Boivin P. Treat-ment of varicose veins by sclerother-apy: an overview. In: Goldman M,Weiss R, Bergan J, eds. Varicose veinsand telangiectasias: diagnosis andtreatment, second edition. St. Louis:Quality Medical Publishing, 1999; 225–246.
15. Bishop CC, Fronek HS, Fronek A, Dil-ley RB, Bernstein EF. Real-time colorduplex scanning after sclerotherapy ofthe greater saphenous vein. J Vasc Surg1991; 14:505–510.
16. Cornu-Thenard A, de Cottreau H,Weiss RA. Sclerotherapy: continu-ous-wave Doppler-guided injections.Dermatol Surg 1995; 21:867–870.
17. Kanter A. Clinical determinants of ul-trasound-guided sclerotherapy out-come. Part I: the effects of age, gender,and vein size. Dermatol Surg 1998; 24:131–135.
18. Kanter A. Clinical determinants of ul-trasound-guided sclerotherapy out-come. Part II: the search for the idealinjectate volume. Dermatol Surg 1998;24:136–140.
19. Belcaro G, Nicolaides AN, Ricci A, etal. Endovascular sclerotherapy, sur-gery, and surgery plus sclerotherapyfor superficial venous incompetence: arandomized 10-year follow-up trial: fi-nal results. Angiology 2000;51:529–534.
20. Politowski M, Szpak E, Marszalek Z.Varices of the lower extremities treatedby electrocoagulation. Surgery 1964;56:355–360.
21. Watts GT. Endovenous diathermydestruction of internal saphenous. BMJ1972; 4:53.
22. O’Reilly K. Endovenous diathermysclerosis of varicose veins. Aust N ZJ Surg 1977; 47:393–395.
23. Politowski M, Zelazny M. Complica-tions and difficulties in electrocoagula-tion of varices of the lower extremities.Surgery 1966; 59:932–934.
24. Manfrini S, Gasbarro V, Danielsson G,et al. Endovenous management of sa-phenous vein reflux. J Vasc Surg 2000;32:330–342.
25. Rautio TT, Perala JM, Wiik HT, Ju-vonen TS, Haukipuro KA. En-dovenous obliteration with radiofre-quency-resistive heating for greatersaphenous vein insufficiency: a feasi-bility study. J Vasc Interv Radiol 2002;13:569–575.
26. Merchant RF, DePalma RG, KabnickLS. Endovascular obliteration of sa-phenous reflux: a multicenter study. JVasc Surg 2002; 35:1190–1196.
27. Weiss RA, Weiss MA. Controlled ra-diofrequency endovenous occlusionusing a unique radiofrequency catheterunder duplex guidance to eliminate sa-phenous varicose vein reflux: a 2-yearfollow-up. Dermatol Surg 2002; 28:38–42.
28. Chang C, Chua J. Endovenous laserphotocoagulation (EVLP) for varicoseveins. Lasers Surg Med 2002; 31:257–262.
29. Proebstle TM, Sandhofer M, Kargl A, etal. Thermal damage of the inner veinwall during endovenous laser treat-ment: key role of energy absorption byintravascular blood. Dermatol Surg2002; 28:596–600.
30. Sarin S, Scurr JH, Smith PDC. Assess-ment of stripping of the long saphe-nous vein in the treatment of primaryvaricose veins. Br J Surg 1992; 79:889–893.
31. Dwerryhouse S, Davies B, HarradineK, Earnshaw JJ. Stripping the long sa-phenous vein reduces the rate of reop-eration for recurrent varicose veins:five-year results of a randomized trial.J Vasc Surg 1999; 29:589–592.
32. Jones L, Braithwaite BD, Selwyn D,Cooke S, Earshaw JJ. Neovasculariza-tion is the principal cause of varicosevein recurrence: results of a random-ized trial of stripping the long saphe-nous vein. Eur J Vasc Endovasc Surg1996; 12:442–445.
33. Miller GV, Lewis WG, Sainsbury JR,MacDonald RC. Morbidity of vari-cose vein surgery: auditing the benefitof changing clinical practice. Ann RColl Surg Engl 1996; 78:345–349.
34. Mackay DC, Summerton DJ, WalkerAJ. The early morbidity of varicosevein surgery. J R Nav Med Serv 1995;81:42–46.
996 • Endovenous Laser Treatment of Saphenous Vein Reflux August 2003 JVIR