Embed Size (px)
Citation preview
ENDODONTIC EMERGENCIES
FLOWCHART Definition Introduction Presentation of endodontic emergency
1) Pre- Treatment Pulpal pain
Reversible pulpitis Hypersensitive Dentine Definition
Theories Irreversible pulpitis
Acute pulpitis with apical periodontitis Acute periapical abscess Management Injection Techniques Different types of Flaps Cracked tooth syndrome Traumatic injury
2) Patients Under Treatment Recent restorative treatment Periodontal treatment Exposure of the pulp Fracture of the root or crown Flare-ups Treatment and Prevention of flare – ups Medications Hypochlorite accident
3) Post- Endodontic Treatment High restoration Over filling Under filling Root fracture
CONCLUSION
Endodontic emergency (def)
Occurrence of severe pain and / or swelling following an endodontic treatment appointment, requiring an unscheduled visit and active treatment (Watson and Foud –1992).
Endodontic emergencies include situations of pain or swelling that require the immediate attention of a dentist.1
The aim of emergency endodontic treatment is to relive pain and control inflammation or infection that may be present.
It has been reported by Hasslar and Mitchell. Later corroborated by Mitchell and Tarplee that 90% of patients seeking emerging dental treatment have symptoms of pulpal or periapical disease.
Presentation of endodontic emergency 2
Patients who present endodontic emergencies can be divided into three main groups:
1) Pre- Treatment Pulpal pain
Reversible pulpitis Irreversible pulpitis
Acute pulpitis with apical periodontitis Acute periapical abscess Cracked tooth syndrome Traumatic injury
2) Patients Under Treatment
Recent restorative treatment Periodontal treatment Exposure of the pulp Fracture of the root or crown Flare-ups
3) Post- Endodontic Treatment
High restoration Over filling Under filling Root fracture
Before Treatment 1) Pulpal pain Irritation of the pulp causes inflammation and the level of response
will depend on the severity of the irritant. If it is mild, the inflammatory process may resolve in a similar fashion to that of other connective tissues, a layer of reparative dentine may be formed. However, if the irritation is more severe, with extensive cellular destruction, further inflammatory changes could eventually lead to pulpal neorosis.
a) Reversible pulpitis The essential feature of a reversible pulpitis is that pain ceases as soon
as the stimulus is removed. The teeth are non tender to percussion. Initially, the following treatment may be all that is necessary.
Check the occlusion and remove non-working facets. Place a sedative dressing in a cavity after removal of deep caries. Apply a fluoride varnish to sensitive dentine.
Hypersensitive Dentine
Definition: The term dentine hypersensitivity has been used to describe a specific condition that is defined as pain arising from exposed dentine.3
Dentinal hypersensitivity is a painful response to a non-noxious stimulus applied to exposed dentine in the oral environment .4
Exposed cervical dentine from gingival recession, periodontal surgery, abrasion or erosion can result in root hypersensitivity. Any chemical (osmotic gradient), thermal (contraction / expansion) or mechanical (Biting or digital scratching) irritant can disturb the fluid contact in the dentinal tubules and excite nociceptors in the pulp.
Theories
Several theories have been cited to explain the mechanism involved in dentinal hypersensitivity.5
The transducer theory, The modulation theory, The “gate” control and Vibration theory, and The hydrodynamic theory
The latter, “hydrodynamic theory”,developed in the 1960’s and based upon two decades of research, is widely accepted as the cause of tooth sensitivity.6
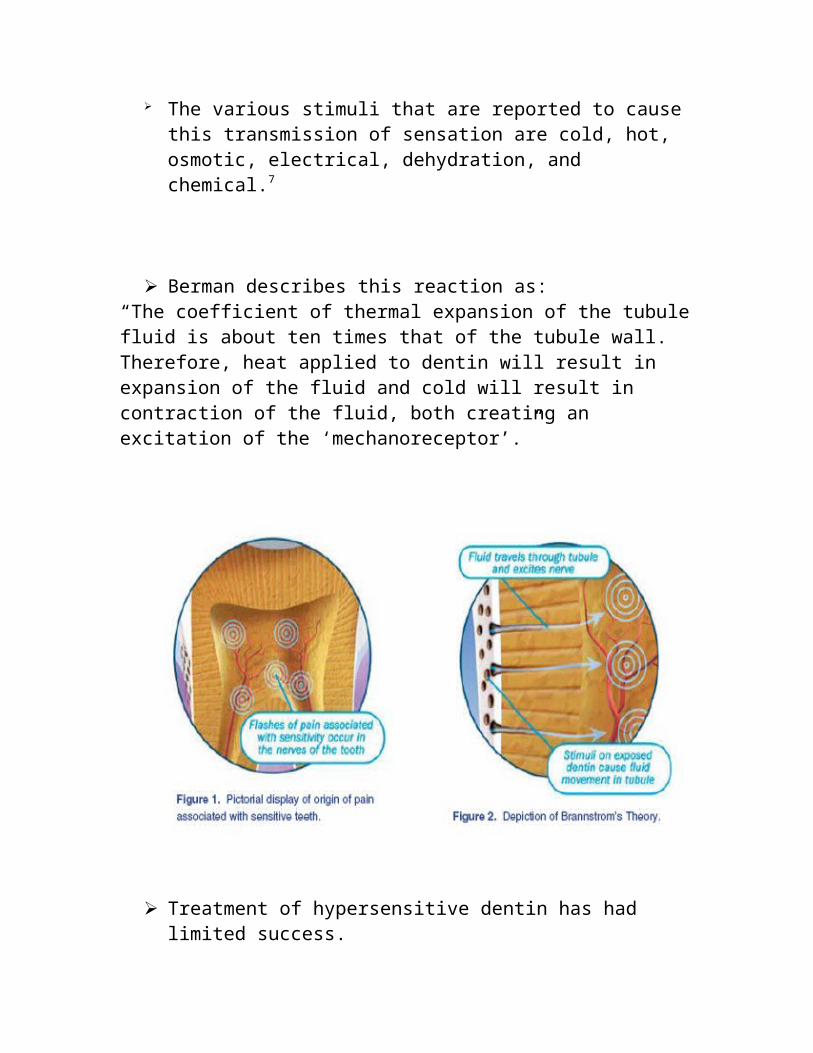
Assumptions of the hydrodynamic theory conclude that when the fluids within the dentinal tubules are subjected to temperature changes or physical osmotic changes, the movement stimulates a nerve receptor sensitive to pressure, which leads to the transmission of the stimuli.
The various stimuli that are reported to cause this transmission of sensation are cold, hot, osmotic, electrical, dehydration, and chemical.7
Berman describes this reaction as:“The coefficient of thermal expansion of the tubule fluid is about ten times that of the tubule wall. Therefore, heat applied to dentin will result in expansion of the fluid and cold will result in contraction of the fluid, both creating an excitation of the ‘mechanoreceptor’.”
Treatment of hypersensitive dentin has had limited success. Treatment modalities include, chemical on physical blockage of the
patent dentinal tubules to prevent fluid movement from within, chemical desensitization attempts to sedate the cellular processes within the tubules with cortiscosteriods or to occlude the tubules with a protein precipitate, a remineralised barrier or a crystallized oxalate deposit.
Physical techniques attempt to block dentinal tubules with composite resins, varnishes, sealants, soft tissue grafts, and glass ionomer cements. The lontophoresis technique electrically drives fluoride deep into dentinal tubules to occlude them.
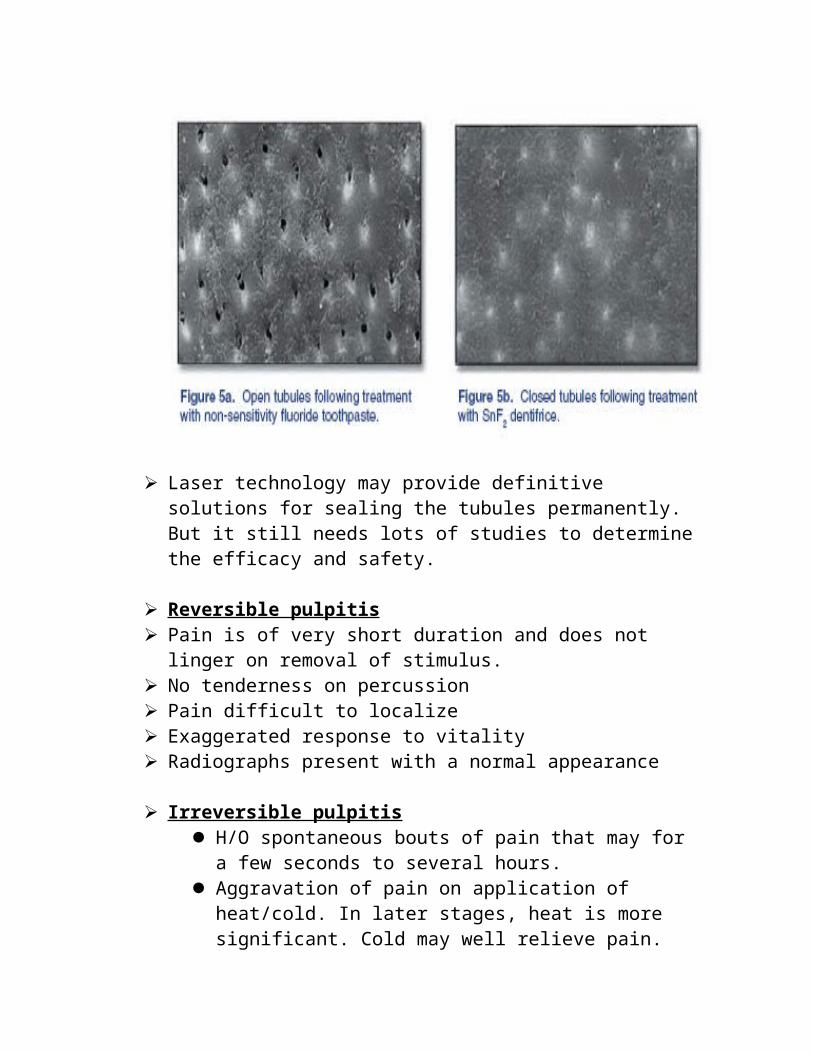
Laser technology may provide definitive solutions for sealing the tubules permanently. But it still needs lots of studies to determine the efficacy and safety.
Reversible pulpitis Pain is of very short duration and does not linger on removal of
stimulus. No tenderness on percussion Pain difficult to localize Exaggerated response to vitality Radiographs present with a normal appearance
Irreversible pulpitis H/O spontaneous bouts of pain that may for a few seconds to
several hours. Aggravation of pain on application of heat/cold. In later stages,
heat is more significant. Cold may well relieve pain. Pain may radiate initially, but once the PDL is involved, the
patient will be able to localize the tooth. Widened PDL space may be seen on the radiographs in the later
stages.
Patients with irreversible pulpitis wait longer to seek emergency endodontic treatment. Most (81-83%) patients with mod. to severe pain will use analgesics to control their discomfort (narcotic 20-23%, non-narcotic 75-80%, antibiotic 6-10%). IP patients who take analgesics will get pain relief 62-65% of the time.8
Treatment: Pulpectomy is done for tooth single rooted and multirooted both. No formocresol or other drugs used.
Occlusion checked after placing the temporary cement. Supraocclusion may cause pericementitis. This would complicate the next phase of endodontic therapy since healing of the periapical tissue is the objective of endodontic treatment. Also, a high occlusion may result in loss of portion of ZnOE, leaving the tooth open for salivary contamination.
Acute Pulpitis with Apical Periodontitis Most difficult emergency condition to treat. This is particularly true in
mandibular molars, where an insufficiency in depth of anesthesia is not an uncommon problem.
Diagnosis is usually simple. Pt. is a aware of the tooth’s tenderness to
percussion. In the classic situation, heat causes, intense pain and cold relieves it.
Radiograph may show a small periapical radiolucency, exhibit a thickening of PDL space or appear normal.
Management Heavy dosage of local anaesthetic may be needed. Complete pulpectomy. Painful teeth with acute apical periodontitis that had been dressed with
Ledermix paste gave rise to less pain than that experienced by patients who had a dressing of calcium hydroxide or no dressing at all. Ledermix is an effective intracanal medicament for the control of postoperative pain associated with acute apical periodontitis, with a rapid onset of pain reduction.9
Acute Periapical Abscess Is an inflammatory process in the periradicular tissues of teeth, often
accompanied by exudate formation within the lesion. This condition is related to bacterial invasion of the periradicular region from an infected and necrotic pulp canal. It may develop spontaneously or may follow initial endodontic treatment if bacteria are forced into the periradicular tissue.
Diagnosis
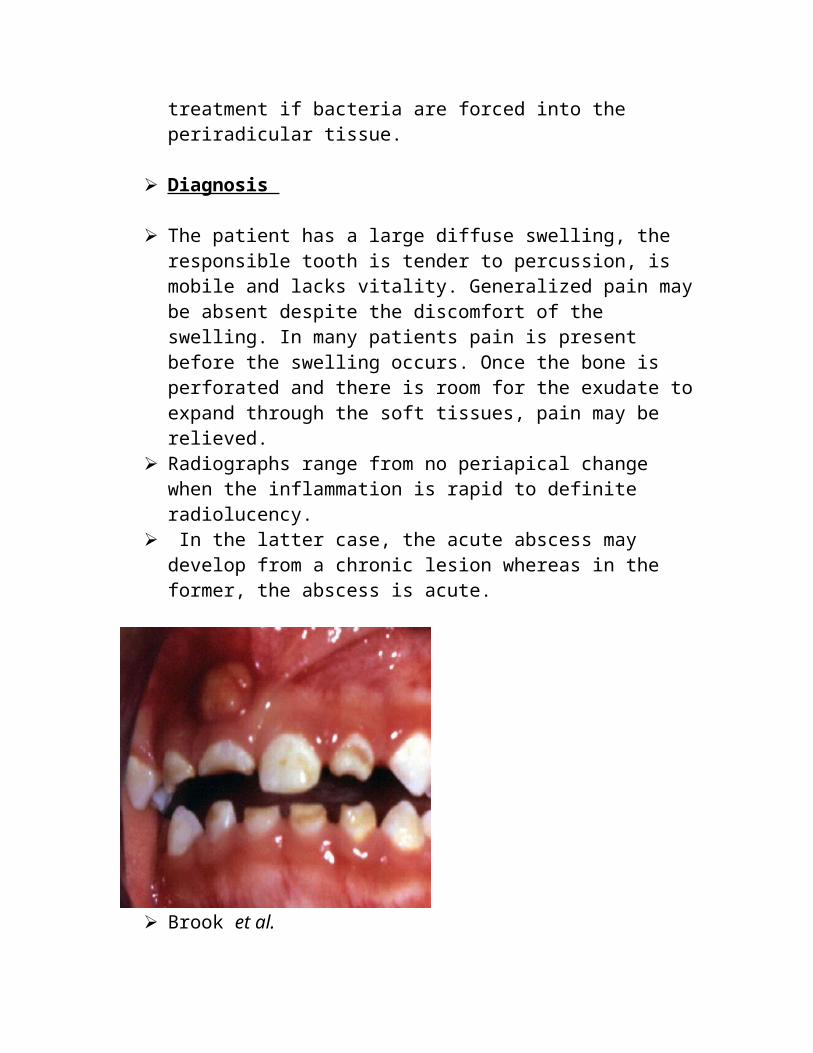
The patient has a large diffuse swelling, the responsible tooth is tender to percussion, is mobile and lacks vitality. Generalized pain may be absent despite the discomfort of the swelling. In many patients pain is present before the swelling occurs. Once the bone is perforated and there is room for the exudate to expand through the soft tissues, pain may be relieved.
Radiographs range from no periapical change when the inflammation is rapid to definite radiolucency.
In the latter case, the acute abscess may develop from a chronic lesion whereas in the former, the abscess is acute.
Brook et al. Sampled the exudate from endodontic abscesses in 39 patients, and
demonstrated anaerobic bacteria in the majority of cases (94 per cent). Polymicrobial anaerobic and aerobic flora have been recovered from endodontic
abscesses. The predominant anaerobes are Bacteroides spp, Porphyromonas gingivalis and P.endodontalis, Fusobacterium spp (especially F.nucleatum), Prevotella spp (P. intermedia and P. oralis).10
Management The abscess should be drained via the root canal space. Access
prepared. Patients may be sensitive to vibration, which results in increased pain. A stick impression compound may be softened and placed against the labial surfaces of the abscessed and adjacent teeth. It acts as a splint to lessen the vibrations.
Local infiltration anasthetic should not be administered as it may cause pain, chance for dissemination of microorganisms and the ineffectiveness of such anaesthesia. Block anaesthesia usually is effective.
Injection Techniques Maxillary Anesthesia Supraperiosteal Injection Posterior Superior Alveolar Nerve Block Middle Superior Alveolar Nerve Block Infraorbital Nerve Block
Palatal Anesthetic Techniques Greater Palatine Nerve Block Nasopalatine Nerve Block
Maxillary Nerve Block
Mandibular Anesthesia Inferior Alveolar Nerve Block Mental Nerve Block Incisive Nerve Block
Periodontal Ligament Injection Intraseptal Injection Intraosseous Injection
Intrapulpal injection
Other Methods of Anesthesia
Electronic Dental Anesthesia: Transcutaneous electrical nerve stimulation (TENS) has been used for management of chronic and acute pain.
Theory on the mechanism of action of electrical stimulation of the nerve for pain control involves the release of endorphins and enkephalins after prolonged (over 10 minutes) exposure to electrical stimulation.
It has been postulated that quicker healing may be aided by the muscle contraction and vasodilation provided during electric stimulation.
Lidocaine Patch (DentiPatch)
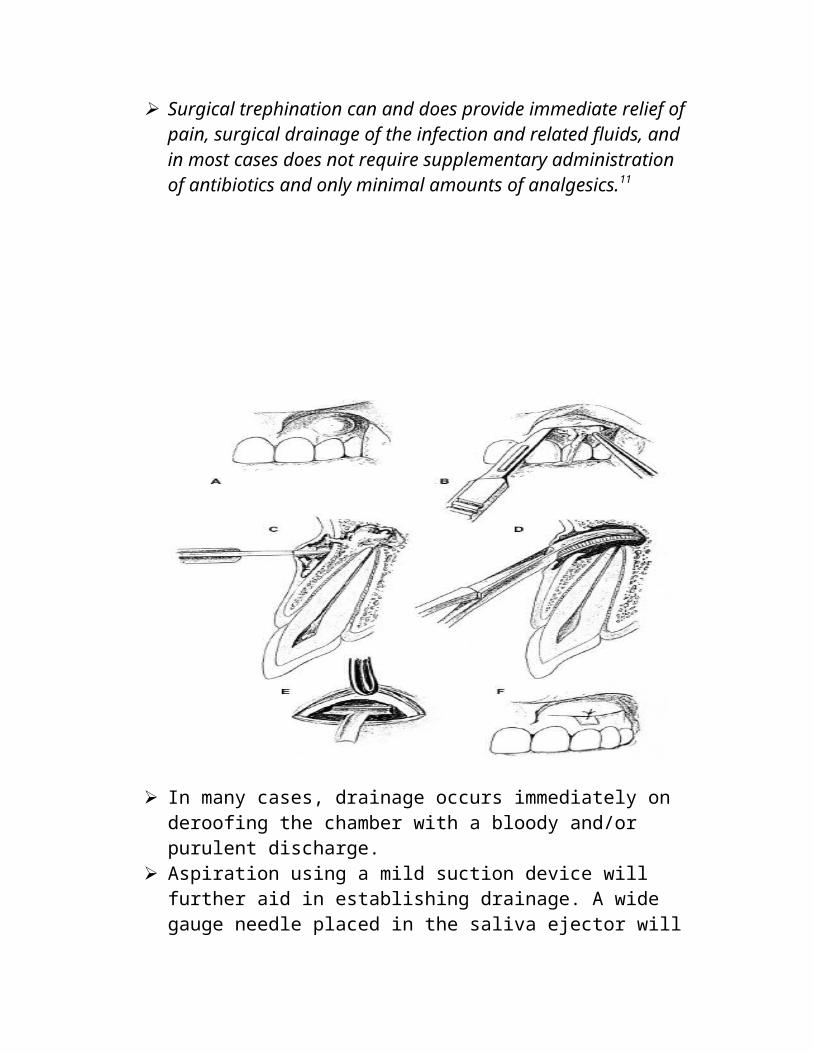
Surgical trephination can and does provide immediate relief of pain, surgical drainage of the infection and related fluids, and in most cases does not require supplementary administration of antibiotics and only minimal amounts of analgesics.11
In many cases, drainage occurs immediately on deroofing the chamber with a bloody and/or purulent discharge.
Aspiration using a mild suction device will further aid in establishing drainage. A wide gauge needle placed in the saliva ejector will give sufficient negative pressure to establish and maintain exudation.
The apical constriction prevents the inflammatory products form draining through the tooth. To relieve this problem, the apical constriction is purposely violated and enlarged to a minimum of #20 / 25 instrument to allow for exudates drainage through the tooth. If drainage still doesn’t occur, use a to #30 file. But even then if there is no drainage do not attempt further.
Which sufficient drainage has occurred and patient is a febrile – antibiotics prescribed.
For many years, the patient was dismissed with the access cavity open after establishment of drainage. Recently there has been an alteration in this regimen. The access cavity is closed but only after the patient has sat with the tooth draining for as long as an hour or even more.
The drainage follows a very predictable pattern, starting with pus of a yellowish, whitish or greenish color mixed with bloo. Gradually, the pus decreases and primarily blood drains. Finally, the blood flow decreases, and only a clear serum exudation emerges. At this point, a
film with files in place is taken and the working length calculated. The canal is enlarged and may be closed with sterile cotton and ZnOE.
Advantages of this approach are that no new type of micro-organisms are introduced into root canal system.
As suggested by Frank et al, a sulfonamide (sulfanilamide or sulfathiozole) powder is taken onto a paper point dipped in sterile distilled water and placed into the canal. A sterile pledget of cotton is then placed into the chamber and access sealed with ZOE.
In case of patients allergic to sulfonamide, this method is contraindicated.
Use of antimicrobials (e.g.,250 mg amoxycillin plus 125 mg clavulanic acid tds,or metronidazole 200 mg tds) is indicated when pyrexia and other systemic signs are present.12
If amoxycillin is selected, the therapy should account for the fact that
many anaerobes of importance in periapical abscesses produce beta-lactamase.13
Finally, it should be emphasized that antimicrobial therapy without surgical drainage is not an effective therapy over the long term.
In the management of localized acute apical abscess in the permanent dentition, the abscess should be drained through a pulpectomy or incision and drainage. This analysis indicated that antibiotics are of no additional benefit. In the event of systemic complications (e.g., fever, lymphadenopathy or cellulitis), or for an immunocompromised patient, antibiotics may be prescribed in addition to drainage of the tooth.14
Culturing the exudates Culture is invaluable when information on antibiotic needed is
required.
The culture is not taken of the initial portion of the exudate as majority of the microorganisms are dead and incapable of reproduction.
However, when the exudate starts to change from yellowish to reddish hue, the sample is taken with a sterile paper point.
Microbes often Detected in Infected Root Canals 15 Obligate Anaerobes Facultative Anaerobes Gram-negative bacilli Gram-negative bacilli Porphyromonas Capnocytophaga Prevotella Eikenella Fusobacterium Campylobacter Bacteroides
Irrigants used in treating acute abscesses At the emergency appointment – warm sterile water or saline Naocl
has the tendency to clump the exudates which might cause plugging of the apical constriction and halt drainage.
When patients returns after emergency opening – alternating use of Naocl and H2O2. These two solutions will cause foaming when used together and will aid in the bubbling out of debris. To prevent building up Nascent Oxygen, NaOCl must be the final irrigant used, until all foaming has stopped.
Drainage through tissue and bone The presence of a post and core crown, sectioned silver points,
calcified canals, prevent obtaining intra canal drainage. Therefore, drainage is established either by Trephination or Artificial Fistulation (Artifistulation).
When intracanal drainage is possible, trephination or cutting a hole in the bone is undesirable as the effect is short lived since, nidus of infection remains undisturbed in the canal.
Artifistulation / trephinaton is performed only when the swelling is sufficiently localized to permit adequate drainage following incision.
For artifistulation a stab incision is made just below the most dependent point of the swelling with a #11 scalpel. Apical bone is probed with an endodontic explorer to locate a perforation which may be enlarged with a spoon excavator (or) endodontic file to ensure venting of the apical area.
This is done by using a strip of rubber dam material. (20mmx20mm) which is cut to resemble the letter H or rolled into a tube and disinfected by dipping into a chemical solution. One half of the dam drain is placed underneath the flap the wings allowed to extend underneath the tissue. A suture is placed to attach the unretracted edge of the flap.
An antibiotic is prescribed and the patient rescheduled after 4-7day.
Only if artifistulation fails to provide drainage, trephination is done. The flap should increased in size for visualization. By using a fissure bur in the airotor with water spray, the periapical bone is removed until the tip of the root is uncovered and drainage established.
The H or tube drain is placed and an antibiotic prescribed..
Cracked tooth syndrome Crazing of the enamel surface is a common finding but on occasions it
may indicate a cracked tooth. If the crack runs deep into dentin chewing may be painful. Initially, this may not be of sufficient intensity but once it involves the pulp, symptoms of pulpitis will ensue the various types of presentations are.
Pain especially on chewing Sensitivity to hot /cold Pain difficult to localize Pain referred to areas supplied by V nerve Acute pulpal pain Alveolar abscess.
A tooth that is susceptible to cracking is one that is extensively restored but lacks cuspal protection (“cuspal crack”) or an intact tooth that has an opposing plunger cusp occluding centrically against a marginal ridge (“vertical crack”).
Pain generated by disocclusion, drives oral fluids within the crack in the pulpal direction. This phenomenon is unique to a crack, and it is inspired by the the diagnostic test of selective closure on the suspected tooth to elicit pain on release.
Other diagnostic aids are transillumination. Radiographs reveal a fracture only if it runs in a bucolingual plane.
Management Urgent care – immediate reduction of the tooth’s occlusal contact by
selective grinding.
Definitive treatment – pulp vitality preserved for a vertically cracked tooth by means of a full coverage crown. Otherwise, the defect will migrate pulpally and cause symptoms requiring endodontic intervention. The extent of the fracture line determines if the tooth can be saved or not.
If it is a vertical fracture involves the RC system and extends below the level of alveolar crest. Extraction is indicated. However, if the fracture line is horizontal or diagonal and superficial to the alveolar crest then the prognosis is better.
Traumatic injury Endodontic treatment may be required as a result of traumatic injury:
Emergency treatment can be complicated by local edema, bleeding or other consequences of the accident.
Crown fracture without pulp exposure
Chipped enamel is smoothened with a sandpaper disk and rubber which to prevent irritation to the lips and tongue. Exposure of dentin requires definitive treatment. A thin mix of ZOE is placed over the exposed dentin. Then a celluloid crown is festooned, filled with a thick mix of ZOE accelerated with zine acetate crystals and cemented into place. This provisional restoration is replaced with a more permanent restoration later.
Radio radiographically assesed and vitality tests are done regularly.
Crown fracture with vital pulp exposure If apical closure has taken place, treatment is similar to that of acute
pulpitis which is the condition present. Pulp extirpation is done via the fractured opening instead of the lingual access cavity whenever permissible.
If apical closure has not taken place, a formocresol pulptomy is done to keep the apical pulp tissue unimpeded in its function of completing apexogenesis. Pulpotomy is preferred over pulp capping as the temporary crown/dressing covering the pulp explosure is difficult to retain which results in further contamination of the pulp which microorganism leading to pulpal necrosis eventually.
The pulpotomy dressing is placed deep enough into the canal so that it will be unaffected if the crown becomes loosened.
Radiographic evaluation done every 3-6 months to determine degree of apical development. Then routine endodontic treatment may be instituted.
Crown fracture with necrotic pulp exposure
This condition may occur as a result of an earlier accident, caries or deep restoration or by severing of pulpal blood vessels in the most recent traumatic accident. Emergency treatment is that of an acute periapical absces /pulpal necrosis. If apical closure is complete routine endodontic treatment if apical closure is incomplete apexification.
Horizontal root: fracture
Does not always require endodontic treatment. Periodic radiographic evaluation and vitality tests done. If mobility is present, however, some types of stabilization is needed. It may be in the form of orthodontic wires, acrylic wire combination etc.
Avulsed teeth The replacement of tooth that has been removed from the alveolar
socket, either intentionally or by accident is called replantation.
Treatment Protocol
Part I: Emergency treatment at the site of injury
Best results obtained if tooth is replanted as soon as possible, even at the site of accident. (Within 30 minutes) even if badly contaminated, it should be replaced without sterilization or scrubbing with soap or detergent. The tooth may be rinsed under running water. Firm pressure by means of a small towel between incisal edges keeps the tooth in the socket. If it is not possible to reinsert the tooth, it is carried in a suitable transport medium.
Part II Emergency treatment at the Dental office If tooth has not been replanted, it is kept in a glass of saline. History
and examination and radiographs made as quickly as possible. The tooth is held in a wet gauze sponge and grasped only at the crown. Wipe away gross debris gently from the root surface with a wet sponge. Irrigate socket with saline. Measure the tooth length and record it.
Splinting is done after placing the tooth back in the socket. If tooth
was already been replanted and seems acceptable, splinting is done directly.
Splint with wire – composite, soft diet advised.
Part III: Completion of endodontic treatment One week after replantation prepare access cavity and perform canal
debridement, ZOE placed. If tooth had an incomplete root apex, no treatment is done. Only routine evaluation is done as it allows for repair of severed pulpal vessels. If pulp necrosis develops canal debridement and apexification procedures undertaken. To prevent ankylosis, remove splint at this appointment.
Two weeks after replantation (1 week after canalpreparation) place Ca (OH)2 paste in the canal to inhibit external resorption. If the paste is placed too soon, before PDL is regenerated, it may cause increased resorption. Recall monthly.
Re- open the tooth after 3-6 months prepare the canals and fill with Gutta Percha and sealer. Recall after one month initially, then at 3 months. External resorption occurs usually in the first year or not at all.
Use of transport medium Hank’s balanced salt solution (HBSS) Very favourable transport medium Developed for endodontics by Krasner HBSS contains – Nacl, glucose, kcl, NaHCo3, sodium phosphate,
Cacl2, Mgcl2, MgSo4. Krasner has developed an avulsed tooth storage system called
“emergency tooth preserving system” (ETPS) containing HBSS a net for holding the tooth and a container for bringing the submerged tooth to the dentist.
Saliva The tooth is placed in the patient’s mouth under the tongue. But
chance of swallowing if the patient is to young. Because of its non physiologic osmolality and presence of microorganisms it is not may desirable to use saliva as a transport medium.
Milk Physiologic osmolality and markedly fewer bacteria than saliva.
Storage in milk for >6 hours is not satisfactory.
Water Last resort if no other medium is available Post operative instructions and systemic treatment:
Soft diet Systemic antibiotics contribute significantly to replantation
success (within 1 week of replantation) Anti tetanus booster (in consultation with the physician)
Mild analgesics
Replantations after an extended extraoral time: Replantation should be attempted. But chances of resorption increase.
Andreason and Andreason and Hjorting Harsen have divided periodontal healing into 3 types.
Healing with normal periodontal ligament: Complete repair of PDL. No inflammatory changes small areas of
resorption at the site of damage to the PDL (surface resorption). Healing with ankylosis or replacement resorption.
Root resorption followed by its replacement with bone. Etiology is absence of a vital PDL on the root surface, progenitor
cells with osteogenic potential from adjacent bone marrow migrate into the damaged area.
Radiographically no PDL space can be seen.
Inflammatory Resorption Root resorption with surrounding granulation tissue in PDL space.
These defects occurs on root surface adjacent to areas of damage of PDL.
Etiology is communication between surface resorption and pulp via the dentinal tubules.
Mechanism of action is toxic products/bacteria migrating into the PDL from the pulp via the dentinal tubules.
Patients under treatment Recent restorative treatment : Following a restorative procedure, pain
may be provoked by a thermal stimulus that would normally not cause a response (hyperalgesia) this may be a result of
High filling Micro leakage Micro-exposure of the pulp Thermal mechanical injury cavity preparation or an inadequate lining
under metallic restorations Chemical irritation from the restoration or restorative material Galvanism due to dissimilar metal restorations. Inadequate/excessive interproximal contacts which promote food
impaction or excessive stresses along the root.
Periodontal treatment : chance of exposure of lateral canals that communicate with PDL when periodontal treatment is carried out.
Exposure of the pulp : If carious exposure is suspected the decision to extirpate the pulp or simply carry out pulp capping depends on whether the pulp has been irreversibly damaged or not.
Crown / root fractures : Most crown root fractures can be prevented by adequately protecting the tooth during the course of endodontic treatment. If tooth structure is damaged, pain might result as a consequence of salivary and bacterial contamination of the root canal.
If the fracture is vertical, and below the crest of the alveolar bone the prognosis is poor.
In multi rooted teeth, radisection of the involved root may be done.
Flare ups. American Association of Endodontics definition : An acute
exacerbation of periaradicular pathosis after initiation or continuation of root canal treatment.(1998).
Inter-appointment flare-up is characterized by the development of pain, swelling or both, following endodontic intervention.16
Before Obturation Etiology :
(1) Contents of the Root Canal (a) pulp tissue (b) bacteria (c) bacterial products (d)endodontic therapy material
(2) Dentist Controlled Factors (a) overinstrumentation (b) inadequate debridement
(c) missed canal (d) hyperocclusion (e) debris extrusion (f) procedural complications perforation separated instrument zip strip
hypochlorite accident air emphysema wrong tooth
(3) Host Factors (a) allergies (b) age (c) sex (d) emotional state (e) tooth After Obturation Etiology :
Debris Extrusion Overinstrumentation Overfilling Underfilling Missed Canal
Contributing factors : Inadequate debridement Residual pulp in inadequately instrumented or undetected canals teeth
with necrotic pulps with or without periradicular lesions are more predisposed than vital teeth to develop mid treatment flare ups.
Debris extrusion : Pulpal fragments, necrotic tissue,dentin filings canal irrigants and
microorganism and their toxins may extrude beyond the apical foramen during instrumentation. More likely to cause flare up if tooth pulp is necrotic and infected.
Debris extrusion occurs with all techniques of root canal instrumentation. The crown down technique and balanced force technique shows significantly less debris extrusion.
The presence of an apical dentinal plug may prevent debris extrusion, over instrumentation and over obturation. But since it may harbor infectious material, the longterm prognosis is compromised.
Over instrumentation
Over instrumentation beyond the apical foramen results in intra-operative or post operative pain. In vital teeth, the apical periodontium is crushed producing pain and inflammation.
Problematic exudation due to overinstrumentation can be controlled by placing a Ca(OH)2 preparation. Also corticosteroid antibiotic combination. Endodontic therapy may be continued, analgesics relieve pain. Occlusal reduction is necessary.
Overfilling : Is an indication/sign of over instrumentation and the resultant pain
may be due to that, rather than due to the extruded GP/sealer furthermore, it may not be possible to achieve a good apical seal in over instrumented canals if the foramen has been transported. In such cases residual bacteria are not sealed off and percolation of apical tissue fluids into the root canal space may provide the nourishment for these bacteria to grow.
Large overfills are a factor in post obturation pain. Gross nerve damage due to chemical toxicity of the extruded material
or mechanical nerve damage caused by compression.17
J. F. Siqueira Jr. The causative factors of flare-ups encompass mechanical, chemical
and/or microbial injury to the pulp or periradicular tissues. Of these factors, microorganisms are arguably the major causative agents of flare-ups.
Microbiology and immunologyLocal adaptation syndrome
Introduction of a new irritant into inflamed tissue exacerbates chronic inflammation.
Changes in periapical tissue pressure Increase in exudate - increased pressure - pain due to pressure on
nerve endings Increase in pressure - aspiration of irritant/microbes into periapical
space - exacerbation of inflammation Chemical mediators such as PG, leukotrienes, Hageman factor and
complement cascade Changes in cyclic neucleotides such as a cAMP and biodegradative
pathways Immunologic response-production of antibiodies.
Psychologic factors- fear and anxiety may exacerbate the patients perception of pain.
Periapical lesions The pulps of teeth with large periapical radiolucencies have more
bacterial strains and are more infected. These may cause an a acute problem if inoculated periapically. There
were fewer problems when an apical lesion or sinus tract is found because of the potential space for pressure release.
Intact PDL cannot vent the increased pressure that develops after an inflammatory response.
Retreatment: Higher incidence of flare ups. Due to host response to extruded filling material, toxic solvents (xylene) or due to presence of periapical pathoses with symptoms.
Host factors: Patients with dental phobias: Phychophysiologic tolerance to pain premedication makes their endodontic experience less traumatic.
Other factors include paitents age, gender,tooth position and presence of allergies.
Ten endodontic flare-ups (8.1%) were recorded in the multiple visit group compared to 19 (18.3%) flare-ups for the single visit group, P = 0.02. For both single and multiple visit procedures, there were statistically significant correlations between pre-operative and post-obturation pain (P = 0.002 and P = 0.0004 respectively). Teeth with vital pulps reported the lowest frequency of post-obturation pain (48.8%), while those with nonvital pulps were found to have the highest frequency of post-obturation pain (50.3%), P = 0.9.18
Treatment and Prevention of flare – ups Cleaning And Shaping -especially concepts of crown down technique
and confirming apical patency are important in management of teeth most likely to exhibit mid treatment flare ups.
Incision and drainage for swellings Periapical surgery1. In cases such as gross overfills, 2. Failing retreatment and 3. Correction of procedural errors.
Leaving teeth open : tooth is left open for purulence to escape, it is left open for upto 20min or longer and then closed with a temporary dressing.
Leaving the tooth open results in recontamination and increased incidence of mid treatment flare up.
Occlusal reduction : High temporary filling, over instrumentation pain, is reduced by selective occlusal reduction.
Intracanal Medicaments : the decision to use intracanal medicaments should be guided by antibacterial efficacy, toxicity and specificity of the drug.
Medicament of choice - chlorhexidine Ca(OH)2
Iodine potassium iodide
Medications19
Analgesics 1) Mild Pain (1) Aspirin 325 mg (2) Ibuprofen 200 mg Tylenol 325 mg 2) Moderate Pain a) Ibuprofen 400, 600,800 mg X 12 1 tab every 4 - 6 hrs. b) Aspirin Intolerance Tylenol 500 mg X 20 2 tabs every 4 - 6 hrs. 3) Severe Pain a) Tylenol 325mg X 10 1 tab every 4 hrs. b) Combination Tylenol 325mg Ibuprofen
Comparative Efficacy of Oral Analgesics 20 Ibuprofen 800 mg Ibuprofen 600 mg
Acetaminophen 650 mg + Oxycodone 10 mg Acetaminophen 1,000 mg + Codeine 60 mg Ibuprofen 400 mg Morphine 10 mg IM injection Acetaminophen 1,000 mg Ibuprofen 200 mg Acetaminophen 600/650 mg Tramadol 100 mg Codeine 60 mg Placebo
Antibiotics 1) Penicillin 500 mg X 28 1 tab every 6 hrs. Generally, Antibiotic of 1st Choice Loading Dose for Penicillin (1) 2.0 g stat 2) Penicillin Allergy a) Cleocin 150 mg X 28 1 tab every 6 hrs. Cleocin Generally, Antibiotic of 2nd Choice
Use of antimicrobials (e.g.,250 mg amoxycillin plus 125 mg clavulanic acid tds,or metronidazole 200 mg tds) is indicated when pyrexia and other systemic signs are present.
If amoxycillin is selected, the therapy should account for the fact that many anaerobes of importance in periapical abscesses produce beta-lactamase.
The21 majority of patients with symptomatic necrotic teeth had significant postoperative pain and require analgesic medication to manage this pain. The administration of penicillin postoperatively did not significantly (p > 0.05) reduce pain, percussion pain, swelling, or the number of analgesic medications taken for symptomatic necrotic teeth with periapical radiolucencies.
Hypochlorite accident A hypochlorite accident refers to any event in which sodium
hypochlorite extruded beyond the apex of a tooth and the patient
immediately manifests a combination of some of the following symptoms:
Severe pain swelling Profuse bleeding both interstitially and thorugh the tooth.
Causes : Forceful injection of NaOCl due to wedging of the irrigating needle into the root canal.
Irrigating a tooth with a large apical foramen, apical resorption or an immature apex.
Features : Oedema and ecchymosis, accompanied by tissue necrosis,
paraesthesia and secondary infection. Although most patients recover within 1-2 weeks. Longterm paraesthesia and scarring have been reported.
Management: Immediate aspiration Cold pack over the affected area. Regional block anesthesia administered. Pain management difficult
because symptoms from distant anatomic structures will continue to cause discomfort.
Monitor tooth for the next half hour. Bloody exudation extended from canal denotes the bodies reaction to the irritant. Remove the fluid with high volume suction to encourage further drainage. If drainage is persistent consider leaving the tooth open.
Antibiotic coverage to prevent secondary infection Analgesics prescribed. Because of possible bleeding complication
with aspirin and NSAIDs an acetaminophen-narcotic combination may be more appropriate.
Corticosteroids – inflammatory process Home care instructions:Cold compress to minimize pain and swelling.
Subsequently warm compresses to encourage healing. Prevention : Bend the irrigating needle at centre to confine the tip of the needle to
higher/coronal levels of root canal. Never bind the needle in the canal Oscillate the needle in and out to ensure that the tip is free to express
the irrigant with out resistance express the irrigant slowly and gently
check the heads of the needle for a tight fit to prevent in advertent separation and accidental exposure of the irrigant to the patients eyes.
Post endodontic treatment : Pain after completion of RCT may be due to:
High restoration Over filling Under filling Root fracture
A high restoration is managed by occlusal rehabilitation to avoid apical periodontitis or worse, a fractured tooth.
Over filling cause pain more as a result of over instrumentation and trauma to apical periodontium/presence of infected material in root canal space.
The options are : Prescription of analgesics and in case of infection – antibiotics removal of the root filling and reprepration of the canal. Apisectomy, in case retrieval of the extruded filling is not possible to
be considered only in case of gross extrusion or persistence of infection due to improper apical seal.
1. Underfilling cause pain due to inadequate debridement management is re-treatment.
2. Root fracture occurs due to excessive forces during lateral condensation. the most common type is the vertical root fracture. Prognosis is poor extraction of sectioning of the root in case of a multirooted tooth, is all that can be recommended.
Conclusion The majority of patients seeking dental treatment report to the dentist
with complaints of pain. Pain of endodontic origin is distressing and agonizing and providing prompt relief from such pain may require an emergency appointment. Although this may inconvenient the dentist, the procedures, are relatively simple and relieving the patients agony may be a truly rewarding experience.
REFERENCES1. Madison S.Curr Opin Dent. 1991 Dec;1(6):744-9.2. P.Carrotte.BDJ 2004 Sept:63. Cohen4. Al-Sabbagh M, Andreana S, Ciancio SG.J Int Acad Periodontol. 2004
Jan;6(1):8-12.5. Berman LH. Dentinal sensation and hypersensitivity. A review of
mechanisms and treatment alternatives.J Periodontol 1985;56;216-22.6. Brannstrom M, Astrom A. The hydrodynamics of the dentine; its
possible relationship to dentinalpain.Int Dent J 1972;22:219-27.7. Pader M. Oral Hygiene Products and Practice. Dekker, New York,
1988, Chap. 10.8. Dr.Borer.Oral Surg 96;2003:207-214.9. Brook I, Frazier E, Gher M. Aerobic and anaerobic microbiology of
periapical abscesses. Int Endod J. 2003 Dec;36(12):868-7510.Oral Microbiol Immunol 1991;6:123-5.11.Trephination for Acute Pain Management. Henry, Brian M. Fraser,
John G.Journal of Endodontics. 29(2):144-146, February 2003.12.Lewis MA, Carmichael F, MacFarlane TW, Milligan SG. A
randomised trial of co-amoxiclav (Augmentin) versus penicillin V in the treatment of acute dentoalveolar abscess. Br Dent J 1993;175:169-74.
13.Finegold SM, Strong CA, McTeague M, Marina M. The importance of black-pigmented gram-negative anaerobes in human infections. FEMS Immunol Med Microbiol 1993;6:77-82.
14.Matthews DC, Sutherland S, Basrani B.J Can Dent Assoc. 2003 Nov;69(10):660.
15.J. Craig Baumgartner.JUNE.2004.VOL.32.NO.6.CDA.JOURNAL16.J. F. Siqueira Jr.JOE.200317.International Endodontic Journal.Volume 36 Issue 7 Page 453 -
July 200318.Endodontic flare-ups: comparison of incidence between single and
multiple visit procedures in patients. Adeleke O Oginni* and Christopher I Udoye*.BioMed Central
19.(NAVAL POSTGRADUATE DENTAL SCHOOL BETHESDA, MARYLAND, S. B. MCCLANAHAN)
20.(Kenneth Hargreaves,JUNE.2004.VOL.32.NO.6.CDA.JOURNALThe Oxford League Table of Analgesic Efficacy
21.Journal of Endodontics. 27(2):117-123, February 2001.Henry, Mark DDS, MS; Reader, Al DDS, MS; Beck, Mike DDS, MA
![Untitled-1 []Clinical Diagnostic Methods . Endodontic Emergencies Diseases of Dental Pulp Diseases of Periradicular Tissues Pulpotomy and Apexification Rationale of Endodontic Treatment](https://img.pdfslide.us/doc/110x75/5e77e90e3c586d38116f8a30/untitled-1-clinical-diagnostic-methods-endodontic-emergencies-diseases-of.jpg)