Embed Size (px)
Citation preview

Endocrine Disorders
Jan Bazner-Chandler
CPNP, MSN, CNS, RN

BMI
In recent years, BMI has received increased attention for pediatric use. In 1994, an expert committee charged with developing guidelines for overweight in adolescent preventive services (ages 11-21 years) recommended that BMI be used routinely to screen for overweight adolescents. In addition, in 1997 an expert committee on the assessment and treatment of childhood obesity concluded that BMI should be used to screen for overweight children, ages 2 years and older, using the BMI curves from the revised growth charts.

BMI Calculation
Can be calculated on-line at various sites including www.cdc.gov
http://nhlbisupport.com/bmi/

Growth Charts
The growth charts consist of a series of percentile curves that illustrate the distribution of selected body measurements in U.S. children. Pediatric growth charts have been used by pediatricians, nurses, and parents to track the growth of infants, children, and adolescents in the United States since 1977. The 1977 growth charts were developed by the National Center for Health Statistics (NCHS) as a clinical tool for health professionals to determine if the growth of a child is adequate. The 1977 charts were also adopted by the World Health Organization for international use.

Endocrine Disorders
Growth hormone deficiencies Hypo and hyper thyroid Diabetes type I and type II Diabetes Insipidus PKU

Growth Charts

Disorders of the Pituitary Gland Disorders of the pituitary gland depend on the
location of the lesion or physiologic abnormality.

Posterior Pituitary
Secretes antidiuretic hormone (ADH or vasopressin) and oxytocin.

Anterior Pituitary
The anterior pituitary is made up of endocrine glandular tissue and secretes growth hormone (GH), adrenocorticotropic hormone (ACTH, TSH, FSH, LH, and prolactin).

Growth Hormone Deficiency
Hypopituitarism 80% are idiopathic Familial patterns 1 in 10,000 children Males are referred more often Short at birth or premie

Causes
Growth hormone produced by the pituitary gland
If the pituitary gland doesn’t produce enough hormones for normal growth, growth slows down or stops.
Underdeveloped, damaged or malfunctioning pituitary gland.

Growth Hormone
GH stimulates the growth of all organs and tissues in the body, particularly the long bones.

Clinical Manifestations
Cherub facial features, frontal bossing, large eyes, and button nose
Males have small testes / micro-penis Look much younger than chronological age Delay of onset of puberty as a teenager

Emotional Difficulties
Emotional difficulties related to small stature are common.
Short child is often treated as if younger. Teased by peers. Child may dress as a younger child. Body image is altered.

Hypopituitarism

Diagnostic Tests
Renal and Liver function test Thyroid function Sedimentation rate / ESR
Done to rule out other causes of delayed growth

Definitive Diagnosis
Deficiency in the Growth Hormone Bone age by x-ray: delayed bone age Slow growth rate: as documented on
standard CDC growth chart

Goals of Therapy
The goal of therapy is to augment growth so that at the time of epiphyseal close, a normal or normally expected adult height is attained.
Child will attain a final adult height consistent with their genetic potential

Growth Hormone Replacement GH products are currently labeled for use in
“children who have growth failure due to an inadequate secretion of normal endogenous growth hormone”

Hormone Replacement Therapy Children should receive GH injections daily
and at a minimum of three times a week Treatment costs $10,000 to 50,000 dollars
annually Therapy can last for 2-4 years or until the
epiphyses close

Management
Children should be managed by a pediatric endocrinologist

Ethical Issues
Social Justice Considerations Children must meet specific criteria to be eligible
for treatment Parents must have access to health insurance
coverage Children who receive GH therapy will obtain the
economic and social benefits of growing taller

Outcomes of Treatment
The child will verbalize positive feelings about his or her body image.
The child will demonstrate an increase in age-appropriate activities with peers.
Child will be able to participate in age related activities of daily living

Long Term Effects
Long term follow up needed: Long term risks unknown Physiologic trauma of daily injection Metabolic effects of the therapy: children on GH
therapy usually lean muscular Therapy associated with increase risk of
malignancies: leukemia, lymphoma, and tumors

Hypersecretion of Growth Hormone In children called gigantism Uncommon disease 15% due to pituitary tumors causing increase
release of GH. Goal of treatment is surgical removal of GH-
secreting adenoma.

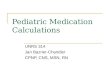
Gigantism
Acromegaly
Anatomy & Physiology: Mosby

Precocious Puberty
Development of sexual characteristics before the usual age of onset of puberty. Girls
Breast development before 7.5 years Pubic hair before 8.5 years Menses before 9.5 years
Boys Secondary sexual characteristics before age 9

Assessment
Chart growth on growth chart. Chronological timing of pubertal events.
Tanner Scale: true precocious puberty is characterized by 2 signs of puberty
Family history

Management / Prognosis
Treatment to halt or reverse sexual development.
Treatment needs to be started prior to closure of epiphysis.
Good outcomes if treatment stared early

Delayed Puberty
Failure to develop sexually at an appropriate age. Girls
No breast development by age 13 or lack on menses within 5 years.
Boys Secondary sexual characteristics not started by 14 years
of age.

Etiology and Incidence
2 to 3% of all adolescents. Bone age moderately delayed. History of small stature during infancy and
early childhood. Familial history

Rule out any Endocrine Abnormalities 12% will have a pathologic reason for
delayed puberty Congenital adrenal hyperplasia Hypothyroidism Growth hormone deficiency

Management
Low dose testosterone for the male.
Oral ethinyl estradiol for the girl.

Hypothyroidism
Most common endocrine disorder of childhood
Hypothyroidism can be congenital, acquired, or secondary

Congenital Hypothyroidism
Results from absence or abnormal development of the thyroid gland or abnormal synthesis of thyroid hormone.
Most common cause is incomplete development of the thyroid gland

Importance of Thyroid Hormones Thyroid hormones promote normal
myelination during brain development in the first two to three years of life and normal skeletal growth
Regulates metabolism



Clinical Manifestations
Dull appearance Feeding difficulties Inactivity Constipation Characteristic faces
Flat nasal bridge Puffy eyelids Thick protruding tongue Low hairline Large posterior fontanel

Diagnosis
Diagnosis Positive health history Physical findings Low levels of T3 and T4 High levels of TSH Neonatal screening is mandatory

Management
Replacement of sodium-l-thyroxine Monitor TSH, T3 and T4 Monitor growth and development Frequent visits with emphasis on importance
of therapy

Acquired Hypothyroidism
15% of Down Syndrome children are hypothyroid
Auto-immune type of thyroiditis is most often the cause
High TSH levels as young as 2 years of age Difficult to diagnose due to overlap of
symptoms

Hyperthyroidism
Excessive secretion of thyroid hormone More common in females 7:1 Genetic and immunologic components HLA-B8 Autoimmune disease of unknown cause

Clinical Manifestations
Cry easily Emotionally labile Nervous Short attention span Can’t sit still / Hyperactive Fatigue but unable to sleep at night Accelerated growth / tall for age

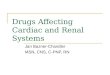
Physical Exam
Enlarged thyroid gland Asymmetric or lobular Patient may present with neck swelling

Exophthalmos

Diagnosis
History and Physical
Levels of T3 and T4 are increased
Levels of TSH are decreased

Treatment
Antithyroid drugs to block T 4 synthesis Prophylthiouracil Methimazole (Tapaxole)

Permanent Treatment
Radioactive Iodine is given to kill off some of the thyroid cells Most common negative outcome is giving too
much iodine that all thyroid producing cells are killed.
Surgical removal of gland or nodule – not always possible since often it is the entire gland resulting in overproduction of the hormone.

Diabetes Mellitus / Type 1
Lack of insulin production in the pancreas. Autoimmunity involved in destruction of beta
cells. 15 new cases per 100,000 children under 20
years of age. Peak incidence between 10 and 14 years.

Diabetes Type I
Result of a genetic-environmental interaction Seasonal variation – midwinter to spring Family history Illness or infection preceding the onset Virus triggers the autoimmune response

Genetic Marker
Genetic Markers: HLA –DR4 and HLA – DR3 20 to 40 % more susceptible

Natural History
Exposure of genetically predisposed individuals to environmental triggers
Leads to inflammation of beta cells of the pancreatic islets (islitis) and subsequent beta-cell injury.

Beta Cell Function
Hyperglycemia 80 to 90% if beta cell function must be lost
before hyperglycemia develops

Pathophysiology
Insulin deficiency causes physiologic and metabolic changes in the body.
Glucose from dietary sources cannot be utilized by the cells.
Renal tubules have difficulty reabsorbing the glucose.

Pathophysiology
If the blood glucose level exceeds the renal threshold for glucose osmotic diuresis ensues.
Renal threshold: when serum glucose levels approach 200mg/dl the renal tubules have difficulty re-absorbing the glucose
Hyperglycemia impairs leukocyte function – yeast infection

Clinical Manifestations
Elevated blood glucose leads to osmotic diuresis. (polyuria and thirst)
Protein and fat breakdown lead to weight loss.
Accumulation of ketones causes a drop in pH. (metabolic acidosis) and spilling of ketones in the urine

Presenting Symptoms
Hyperglycemia / glucose in blood stream Glucosuria / sugar in urine Polyuria / increased urine output Electrolyte imbalance from dehydration Polydipsia / attempt to relieve dehydration Polyphagia / attempt to compensate for lost
calories

Diagnostic Tests
Blood glucose levels greater than 200 mg/dL Urine sample reveals glucosuria and possible
ketonuria. Glucose tolerance test would reveal low
insulin levels in the face of elevated glucose levels.

Goals of Management
Short term goals: Prevent the development of ketosis. Prevent electrolyte abnormalities and volume depletion
secondary to osmotic diuresis. Prevent impairment of leukocyte function Prevent impairment of wound healing
Long term goal: prevention of microcirculatory and neuropathic changes

Interventions
Administration of insulin Blood glucose levels
Initially before every meal Every am when diabetes under control
Dietary management / refer to nutritionist Glycosylated hemoglobin / reflects average
glucose concentration for preceding 2 to 3 months.

Blood Glucose Levels
Target levels Toddler and preschool: 100 to 180 mg/dL School-age: 90 to 180 mg/dL Adolescents (13 to 19 years): 90 to 130 mg/dL

Urine
Test urine for ketones only if blood sugar greater than 250 or during illness

Insulin
Insulin Short acting – often used to cover extra
carbohydrate consumption Combination of regular and intermediate-acting
insulin Morning and evening dosing
Children on mixed insulin dosage schedules tend to experience hypoglycemic episodes at 11:30 and 2:30 as peaking of insulin occurs.


Hypoglycemia
Symptoms: Rapid onset Shaky feeling, hunger Headache Dizziness Vital signs
Shallow respirations tachycardia
Tremors
Lab Values: Glucose = low, below 60 Ketones = negative Urine output
Normal sugar negative negative ketones

Treatment of Hypoglycemia
Day time hypoglycemia: Simple concentrated sugars such as honey by mouth,
hard candy, sugar cubes, or glucose tablets will elevate the blood sugar immediately. Orange juice or sugar containing soda or fruit drink. (Blood Glucose less than 70 mg/dL)
Eat a snack if next meal is more than an hour away Identify reason for hypoglycemia. In children it is often
increase in activity without increase in food intake.

Hypoglycemia Prevention
Using rapid-acting or Lispro insulin Infusion pump (8 to 10 years of age) Night time snack Check blood glucose before bedtime Do not skip snacks Eat an extra snack on days of strenuous
exercise

Night time hypoglycemia
Eat 1 ½ snacks if blood glucose is less than 100 to 120 mg/dL before going to bed
Make sure the blood glucose is 100 – 120 mg/dL before going to bed
Check blood glucose at midnight and 3 am

Hyperglycemia
Symptoms:
Onset = gradual
Lethargic, confused, weak
Thirsty
Abdominal pain often with nausea and vomiting
Signs of dehydration
Vital signs: deep, rapid respirations, fruity acetone breath, and weak pulses

DKA – Diabetic Ketoacidosis
Presenting symptoms may include: Altered level of consciousness Dehydration Electrolyte disturbances Dysrhythmias Shock Complete vascular collapse

Diabetic Ketoacidosis
Mild Moderate Severe

Mild DKA
Hyperglycemia and ketonuria with an ability to take in and retain oral fluids.
Management: increased fluid intake Diet drinks when blood glucose > / = 240 and
supplemental insulin administration Check urine ketone levels

Moderate DKA
Hyperglycemia, ketonuria, and acidosis (ph between 7.25 and 7.4) associated with an impaired ability to retain oral fluids.
Need emergency care: IV fluids (normal saline), supplementary insulin ( regular insulin IV)
Management of underlying medical condition: infections, trauma

Severe DKA
Characterized by severe acidosis (ph < 7.25), dehydration, hyperglycemia, ketosis and a variety of other symptoms including Kussmaul respirations, alteration in mental status, and unconsciousness. Severe dehydration may lead to shock.

Management of severe DKA
3 phases of management Resuscitation Correction of acid-base, glucose and electrolyte
abnormalities Transition to daily routine

Resuscitation
ABC’s: securing an airway, ensuring adequate ventilation, and correcting shock with IV volume expanders such as normal saline.

Phase 2 & 3
Correct acid-base: Intravenous fluids and insulin (regular insulin IV
drip) Administration of bicarbonate if acidosis is severe Slowly bring down plasma glucose levels to avoid
cerebral edema Restart child on regular routine with
emphasis on teaching and review of routine

Life Management
Management by endocrinologist Insulin Blood sugar monitoring Diet Exercise Screen for retinopathy: ophthalmologic exam
annually

Nutritional Management
Goals of nutritional therapy Maintaining near-normal blood glucose by balancing food
intake with insulin and activity. Achieving optimal serum lipid levels. Providing appropriate calories for normal growth and
development. Preventing and treating acute and long-term complications. Improving overall health through optimum nutrition

Exercise
Vital component to management of child with diabetes.
May decrease the amount of insulin required. Enhances insulin absorption. Important for normal growth and
development.

Management During Exercise Eat a snack before exercising. Exercise lasting less than 1 hour usually requires a
small snack / complex carbohydrate or protein. Longer exercising may require more frequent
snacks / complex carbohydrates or a protein. Insulin adjustment may be needed if hypoglycemia
occurs during the activity. Check blood glucose after activity and before
bedtime to prevent night time hypoglycemia

Diabetes Type 2
Between 8 and 45 percent of newly diagnoses cases of childhood diabetes are type 2
Type 2 diabetes is caused by resistance to insulin as well as the inability of the pancreas to keep up with the increase demand of insulin.
Insulin resistance + chronic hyperglycemia

Type 2 diabetes
85% of children are obese Age of onset is middle to late puberty Minority populations have an especially high
rate of type 2 diabetes Native American, Alaska Native, African
American and Mexican American

Who is at risk?
Obesity: BMI greater than 30 (normal range is 15 to 17 in the pediatric population)
Waist to hip ratio: apple shape Acanthosis nigricans: hyper-pigmentation and
thickening of the skin into velvety irregular folds in the neck and flexural areas – reflects hyperinsulinemia
Hypertension + family history of type 2 diabetes Ethnicity

Presenting Symptoms
Chronic hyperglycemia Often diagnosed during routine physical Girls often present with vaginal monilial
infection Severe infections: pharyngitis or
osteomyelitis:

Diagnostic tests
Plasma insulin and C peptide are high reflecting insulin resistance
Autoantibodies to the islet cell are negative in type 2

Management
Comprehensive education on importance of regular exercise and how to self-monitor for blood glucose levels.
Dietary management Glucose-lowering agent: drugs that improve
insulin sensitivity such as Glucophage (Metformin)
A few may need Insulin to initiate control

Diabetes Insipidus
Disorder of the posterior pituitary It results in deficiency in the secretion of ADH ADH concentrates urine Deficiency result in massive renal loss of fluid

Causes
Hypothalamic lesion ¼ occur after craniotomy Idiopathic or familial

Pathophysiology
Antidiuretic hormone works directly on the renal collection ducts and distal tubules to increase membrane permeability for water and urea.
A deficiency in ADH will cause failure of kidneys to reabsorb water.
This leads to massive water loss

Assessment
Polyuria (excessive urination) Polydipsia (excessive thirst) Onset on symptoms abrupt In the older child nocturia and enuresis are
common

CaReminder
The first symptoms of diabetes insipidus seen in children, especially in infants, are irritability and incessant crying that can only be alleviated with feedings of water and not formula or breast milk.

Urine
Very low specific gravity: 1.005 Dilute Colorless NO glucose or ketones

Management
Desmopressin (DDAVP): synthetic analogue of ADH
Administered by nasal insufflation once or twice a day
Aqueous pitressin may be given IV, IM or sub-q

Parent education
Administration of the medication Signs and symptoms of fluid imbalance:
dehydration and over-hydration Sign of hypernatremia Wear medi-alert tag

Nursing Diagnosis
Fluid volume deficit Desmopressin: medication used to treat DI…
over use may result in Fluid volume excess Activity intolerance: due to dehydration,
excessive thirst and frequent urination

Phenylketonuria
PKU First discovered in 1934 PKU is an autosomal recessive genetic defect found on
chromosome 12 Child must receive the defective gene from both parents 1 in 60 people is an asymptomatic carrier Symptoms 1 in 10,000 births In turkey 23 in 10,000

Pathophysiology
Phenylalanine is an essential amino acid found in all protein food.
The accumulation of phenylalanine leads to severe retardation.
With early identification of the defective gene intervention can prevent retardation.

Diagnosis
Heel stick done 24 to 48 hours after birth. Infant must have an adequate intake of breast milk
or formula. (protein) The drop of blood must be large enough to fill the
imprinted space on the filter paper. Squeezing out more blood onto the paper creates a
layered effect that can produce a false-positive test result.

Treatment
Focuses on preventing excessive accumulation of phenylalanine by restricting protein intake.
Maintain levels below 0.9 mmol/L but maintain at0.2 to allow for normal growth and tissue repair.
Aspartame or NutraSweet need to be avoided in diet.

Prognosis
Teaching that reinforces the dietary regimen is critical to the successful management of PKU
Family cohesion and adherence to the restricted diet positively correlates with higher IQ levels.
Children at high risk for learning difficulties. Diet generally discontinued around 10 years with full brain
development Pregnant women with PKU deficiency at high risk for having a
fetus with mental retardation.