-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
1/63
End-stage renal disease
2o hypertensivenephrosclerosis
Presented by: Christelle Queen S. Bacalla
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
2/63
INTRODUCTION
End-stage renal disease (ESRD) represents a clinical state
orcondition in hich there has been an irre!ersible loss o"
renal"unction in hich the body#s ability to $aintain $etabolic
and%uid and electrolyte balance "ails& resulting in ure$ia
ora'ote$ia (retention o" urea and other nitrogenous astes inthe
blood)& and these patients usually need to accept
renalreplace$ent therapy (dialysis or idney transplantation)
inorder to a!oid li"e-threatening ure$ia. t is the +nal stage(stage
,) o" chronic idney disease (CD). his $eansidneys are only
"unctioning at /0 to /, percent o" their
nor$al or not "unctioning at all. idney disease is
usuallyprogressi!e. t typically does not reach the end stage until
/0to 10 years a"ter you are diagnosed ith chronic idneydisease&
hich $ay also de!elop sloly.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
3/63
INTRODUCTION
2ost cases o" ESRD are caused by diabetes orhigh blood pressure.
Chronic idney disease (CD)is an u$brella ter$ that describes idney
da$ageor a decrease in glo$erular +ltration rate (34R) "or
5 or $ore $onths. 6ntreated CD can result in end-stage renal
disease (ESRD) and necessitate renalreplace$ent therapy (dialysis
or idneytransplantation). Chronic idney disease is identi+ed
by a blood test "or creatinine. 7igher le!els o"creatinine
indicate a "alling glo$erular +ltration rateand as a result a
decreased capability o"the idneys to e8crete aste products.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
4/63
INTRODUCTION
Creatinine le!els $ay be nor$al in the early stages o" CD&
and thecondition is disco!ered i" urinalysis shos that the idney is
alloing theloss o" protein or red blood cells into the urine. o
"ully in!estigate theunderlying cause o" idney da$age& !arious
"or$s o" $edical i$aging&blood tests and o"ten renal biopsy are
e$ployed to +nd out i" there is are!ersible cause "or the idney
$al"unction.
he +!e stages o" CD are based on the glo$erular +ltration
rate (34R)herein the nor$al 34R is /1, $9$in/.;5$1. Stage / is hen
there isidney da$age ith nor$al or 34R
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
5/63
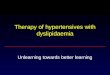
INTRODUCTION Benign nephrosclerosis is a gradual and
prolonged deterioration o" the
renal arteries. 4irst the inner layer o" the alls o" s$aller
!esselsthicens& and gradually this thicening spreads to the
hole all&so$eti$es closing the central channel o" the !essel.
4at then beco$esdeposited in the degenerated all tissue. he larger
arteries gain ane8cess o" elastic tissue& hich $ay bloc their
channels. Both o" theseconditions cause the blood supply to the
!ital idney areas to be
bloced& and tissue deterioration ensues.
n $alignant nephrosclerosis a si$ilar process occurs but
at a $uch"aster rate. he disease $ay de!elop so rapidly that there
is little ti$e"or gross idney changes to occur. he sur"ace o" the
idney& hoe!er& isnearly alays co!ered ith large red
blotches at points here bleeding
has occurred. n the $alignant disease the arteriole alls thicen
and$ay be closed o by rapid cell groth. he nuclei o" these cells
die& andthe elastic +bers disappear. ith the loss o" the
elastic +bres& the allso" the !essels beco$e $uch $ore "ragile
and easily distended. Se!ereruptures and he$orrhages are "reuent.
he arterioles o"ten suerspas$s that can "orce blood through lesions
in the !essel alls thetissues beco$e sollen as a result.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
6/63
INTRODUCTION
Fccording to the 10// 6S Renal DataSyste$ (6SRDS) data& in
the year 100
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
7/63
INTRODUCTION
chose this case because ant to gainco$prehensi!e noledge about
the disease.
HbIecti!es o" $y case study are the "olloing: o
understand the nature and pathophysiology o"
the disease. o identi"y signs and sy$pto$s e8hibited
by the
patient ith ESRD. o assess the patient& +nd out
need o" patient and
co$e up ith appropriate inter!entions utili'ingthe nursing
process.
o pro!ide discharge plan to the patient
ithESRD.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
8/63
DEMOGRA!IC RO"I#E
Aa$e: Patient 2. Fge: ?5 years old Se8:
2ale Ci!il Status: 2arried Religion: Se!enth day
Fd!entist Fddress: P-? Cantugas& 2ainit& SDA
Date o" Birth: 0?0=/
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
9/63
A$T MEDICA# !I$TOR% he patient as diagnosed ith
7ypertension as early as 5/
years o" age but did not co$ply ith his treat$ent regi$en.
7eould usually buy Captopril hene!er he "eels lie his bloodpressure
is ele!ated.
7e as ad$itted at Surigao 2edical Center on Dece$ber 10/5due to
!o$iting and diarrhea. he patient#s doctor suggestedhi$ to undergo
7e$odialysis "or the reason that his seru$
creatinine as ele!ated a$ounting to 51$gdl. 7oe!er&
thepatient re"used& thining that he$odialysis as Iust a aste
o"$oney and that sooner or later he ill die. Hn Fpril 10/?& he
asbrought to CR7 by his daughter because he had an
alteredsensoriu$& !o$iting& and peripheral ede$a. Fccording
to hi$&
his creatinine increased to //1 and his B6A as !ery
ele!ated&he cannot recall the rest o" the history. 7e as then
diagnosedith ESRD secondary to 7ypertensi!e
Aephrosclerosis.Frterio!enous 4istula as created at his le"t ar$ on
Fpril 0=&10/? by Dr.Jcong. he patient also !erbali'ed that his
doctore8plained to hi$ the result o" his sonography that both o"
his
idneys shrun.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
10/63
$OCIA# !I$TOR%
he patient li!es in P-? Cantugas& 2at-& SDA. 7e
has 5children& to o" the$ ha!e their on "a$ily& and
theyoungest is currently li!ing ith hi$ and his i"e attheir
residence. Be"ore he as diagnosed ith ESRD&
he as li!ing only ith his youngest daughter ho isstudying in
7igh School because his i"e oredabroad. F"ter his
hospitali'ation& his i"e ent ho$eto tae care o" hi$. 7e
"or$erly ored as a treasurerin their $unicipality and stopped hen
he as alreadydiagnosed ith ESRD because he easily gets tired andhas
to go on he$odialysis tice a ee. he patientdoes not s$oe& and
only drins liuors occasionally.7e has a good relationship ith his
neighbors.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
11/63
"AMI#% !I$TOR% O" I##NE$$
he patient !erbali'ed that his parentsha!e a
history o" 7PA.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
12/63
!%$ICA# A$$E$$MENT
&ITA# $IGN$' BP: /=0/00 $$7g K />0//0 $$7g
E2PERF6RE: 5=.?oC P69SE RFE: >= bp$ RESPRFHRJ
RFE: 1/ bp$
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
13/63
$(IN' Color: Dar bron ntegrity: ntact
2oisture: Dry %ay sin (L)pruritus M ar$s and bac
!AIR'
Color: Blac hicness: hic and dry hair
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
14/63
NAI#$' Shape: Aor$al sy$$etrical e8ture:
S$ooth Aailbed color: Pale
Capillary Re+ll: Aor$al Fppearance: Dirty
"ACE' Sy$$etry o" 2o!e$ents: Sy$$etrical Fppearance:
puy chees
E%E$' Color: hite 7olloness: Sunen Pale
conIuncti!a
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
15/63
UI#$' Color: Bron Shape: Circular
Sy$$etry: Sy$$etricalAURIC#E$' Aor$al and
sy$$etrical e8ture& elasticity& tenderness:
4ir$ non-tender
Sin lesions: Ao sin lesions
NO$E' Sy$$etrical (-)%aring
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
16/63
MOUT!' (-)halitosis ithout dentures eeth
color: light yello Fppearance: pale
#UNG$' Breath sounds: (L)cracles on both lung +elds
A)DOMEN' Distended
ARM$' Sy$$etrical& ith FN4 M 9 ar$
#EG$' Sy$$etrical& ith scar M posterior 9 cal"&
ede$a (/L)
on both "eet
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
17/63
GORDON*$ T%O#OG% O" !EA#T! ATTERN
!EA#T! ERCETION + !EA#T! MANAGEMENT he patient
rarely sees $edical attention hene!er he has
an illness because he belie!es that it is Iust a aste o"$oney.
Be"ore he as diagnosed ith ESRD& he does nottae any !ita$ins
and only buys Captopril hene!er he"eels di''y and his BP beco$es
ele!ated. But no he isalready co$pliant to his prescribed
$edications ith thehelp o" his i"e by re$inding hi$ to tae his
$eds. 7eundergoes he$odialysis tice a ee& and undergoes
bloodtrans"usion o" PRBC hene!er his RBC count beco$es !ery
lo usually e!ery 5 $onths. he i"e !erbali'ed that thepatient is
!ery hard headed because the patient o"ten ti$eson#t listen to hi$
and his diet is still salty and high in "at.
he patient $aintains a eight o" ,?.,g pre-7D andeight goal
post-7D is ,/g.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
18/63
NUTRITIONA# + META)O#IC ATTERN 7is usual ater intae is ?-=
ti$es a day. 7is diet is usually
salty and high in "at. 7e o"ten drins soda and Cobra energydrin
"or 1-5 ti$es a day be"ore he as diagnosed. 7edrins liuors
occasionally and ne!er s$oe. he patientdoes not ha!e "ood
allergies. 7e o"ten has no appetite andhis i"e usually has to bring
hi$ to restaurants to eat he!erbali'ed that his appetite depends on
the s$ell andappearance o" the "ood. 7oe!er& he still eats
salty "oodse!en though he#s already diagnosed ith ESRD. 7e does
not li$it his %uid intae though his doctor ad!ised hi$ toli$it
%uid intae to /9 per day. he patient also !erbali'edthat a"ter
eating salty "oods or drining soda& he ille8perience selling o"
the "eet and bone pains Iust hourslater.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
19/63
E#IMINATION ATTERN he patient usually !oids ,-;
ti$es a day in
scanty-$ini$al a$ount& dar yello in color orcolorless. 7is
boel $o!e$ent is usually oncee!ery 1 days.
ACTI&IT%, #EI$URE, AND RECREATIONA#ACTI&ITIE$ 7e
pre!iously ored as a treasurer in their
2unicipal oOce. he patient did not engage ine8ercises be"ore and
until no. 7e atchestele!ision $ore o"ten and does not usually go
out"or a al. he patient does not do householdchores because he gets
easily tired.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
20/63
$#EE AND RE$T ATTERN he patient usually sleeps at
/0p$ and oe up at
?a$. H"ten ti$es he e8perienced aing up atnight to !oid. 7e
!erbali'ed aron nga naingani
nao& naa rao pir$i sa balay aon atulog ay dili$an o pa
trabahuon saong asaa.
COGNITI&E-ERCETUA# ATTERN he patient is a
college graduate. 7e has diOculty
seeing near obIects. 7e e!en holds his cellphoneaay hile reading
a te8t $essage. 7e is !erysensiti!e in the s$ell and appearance o"
"ood hichaects his appetite.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
21/63
$E#" ERCETION-$E#" CONCET ATTERN he patient lies to
sociali'e ith his or$ates be"ore.
7e thought that he as healthy and does not ha!e anyproble$ about
his hypertension. 7e !erbali'ed in an
inappropriate aect ala gyud o nag tuo nga $uabutsa ingani&
nga $aingani o& aron nghulat nalang o nus-a $a$atay.
RO#E RE#ATION$!I
7is pri$ary dialect is Surigaonon. 7e is $arried& ith
5children ho he is ell-supported and lo!ed. he patientis currently
li!ing ith his i"e and youngest child. 7iseldest daughter ho is a
nurse abroad is the only oneho supports hi$ on his treat$ents.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
22/63
$E.UA#IT%-RERODUCTI&E ATTERN 6na!ailable.
COING AND $TRE$$ TO#ERANCE hene!er he has proble$s& he
does not usually tell it to his "a$ily
especially no because he does not ant to be a burden in
the"a$ily.
&A#UE$-)E#IE" ATTERN he patient#s religion is
Se!enth Day Fd!entist. 7e does not
regularly go to Church but he alays pray to 3od. 7e reali'ed
that
pro$oting good health is really i$portant than to regret later
inyour li"e particularly in his condition in hich he has to
undergohe$odialysis "or a li"eti$e. 7oe!er& e!en though he is
already onhe$odialysis& he does not change his li"estyle and
diet because hebelie!es that it is oay to eat salty "oods and drin
soda since he#salready on he$odialysis hich "unctions no as his
idneys& and
besides& he ill still die in the end.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
23/63
RENE H4 FAFH2J FADP7JSH9H3J#ocation
he idneys are a pair o" organs"ound along the posterior
$uscularall o" the abdo$inal ca!ity. hele"t idney is located
slightly $oresuperior than the right idney dueto the larger si'e o"
the li!er on the
right side o" the body. 6nlie theother abdo$inal organs&
theidneys lie behind the peritoneu$that lines the abdo$inal ca!ity
andare thus considered to beretroperitoneal organs. he ribs
and $uscles o" the bac protectthe idneys "ro$ e8ternal
da$age.Fdipose tissue non as perirenal"at surrounds the idneys and
actsas protecti!e padding.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
24/63
$tr/ct/re he idneys are bean-shaped ith thecon!e8 side o"
each organ locatedlaterally and the conca!e side $edial.
he indentation on the conca!e side o"
the idney& non as the renal hilus&pro!ides a space "or
the renal artery&
renal !ein& and ureter to enter theidney.
F thin layer o" +brous connecti!e tissue
"or$s the renal capsule surroundingeach idney. he renal capsule
pro!ides
a sti outer shell to $aintain the shapeo" the so"t inner
tissues.
Deep to the renal capsule is theso"t&dense& !ascular
renal corte0.Se!en cone-shaped renal pyra$ids "or$the renal $edulla
deep to the renalcorte8. he renal pyra1ids are alignedith their
bases "acing outard toard
the renal corte8 and their ape8es pointinard toard the center o"
the idney.
Each ape8 connects to a $inor caly8& as$all hollo tube that
collects urine. he$inor calyces $erge to "or$ 5 larger
$aIor calyces& hich "urther $erge to"or$ the hollo renal
pel!is at the
center o" the idney. he renal pel!ise8its the idney at the renal
hilus& here
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
25/63
The Nephron
Each idney containsaround / $illion
indi!idual nephrons&the idneys#$icroscopic "unctionalunits
that +lter bloodto produce urine. he
nephron is $ade o" 1$ain parts: the renalcorpuscle and therenal
tubule.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
26/63
Responsible "or +ltering the blood& our renal
corpuscle is"or$ed by the capillaries o" the glo$erulus and
theglo$erular capsule (also non as Bo$an#s capsule). he
glo$erulus is a bundled netor o" capillaries thatincreases the
sur"ace area o" blood in contact the blood!essel alls. Surrounding
the glo$erulus is the glo$erularcapsule& a cup-shaped double
layer o" si$ple sua$ousepitheliu$ ith a hollo space beteen the
layers.Special epithelial cells non as podocytes "or$ the layer
o" the glo$erular capsule surrounding the capillaries o"the
glo$erulus. Podocytes or ith the endotheliu$ o"the capillaries to
"or$ a thin +lter to separate urine "ro$blood passing through the
glo$erulus. he outer layer o"the glo$erular capsule holds the urine
separated "ro$ the
blood ithin the capsule. Ft the "ar end o" the
glo$erularcapsule& opposite the glo$erulus& is the $outh o"
therenal tubule.
F series o" tubes called the renal tubule concentrate
urineand reco!er non-aste solutes "ro$ the urine. he renal
tubule carries urine "ro$ the glo$erular capsule to therenal
el!is.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
27/63
he cur!y +rst section o" the renaltubule is non as the
pro8i$alcon!oluted tubule. he tubule cellsthat line the pro8i$al
con!olutedtubule reabsorb $uch o" the ater andnutrients initially
+ltered into the urine.
6rine ne8t passes through the loop o"7enle& a long straight
tubule thatcarries urine into the renal $edullabe"ore $aing a
hairpin turn and
returning to the renal corte8.4olloing the loop o" 7enle is the
distalcon!oluted tubule.
4inally& urine "ro$ the distalcon!oluted tubules o"
se!eralnephrons enters the collecting duct&hich carries the
concentrated urine
through the renal $edulla and into therenal pel!is.
4ro$ the renal pel!is urine "ro$ $anycollecting ducts co$bines
and %osout o" the idneys and into the ureters.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
28/63
he $ain "unction o" the idneys is to +lter
ater& i$purities and astes "ro$ the blood. he blood
"ro$ the body enters the idneysthrough the renal arteries. Hnce in
the idney&the blood passes through the nephrons& here
aste products and e8tra ater are re$o!ed. he clean blood is
returned to the body throughthe renal !eins. he aste products
+ltered"ro$ the blood are then concentrated into urine.
he urine is collected in the renal pel!is. heureters $o!e
the urine to the bladder& here itis stored. 6rine is passed out
o" the bladder andthe body through the urethra.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
29/63
ater !o1eostasis
he idneys are able to control the !olu$e o" 3ater in
the4ody by changing the reabsorption o" ater by the tubules
o"the nephron. 6nder nor$al conditions& the tubule cells o"
thenephron tubules reabsorb (!ia os$osis) nearly all o" the
aterthat is +ltered into urine by the glo$erulus.
ater reabsorption leads to !ery concentrated urine and
theconser!ation o" ater in the body. he hor$ones
antidiuretichor$one (FD7) and aldosterone both increase
thereabsorption o" ater until al$ost /00G o" the ater +lteredby the
nephron is returned to the blood. FD7 sti$ulates the
"or$ation o" ater channel proteins in the collecting ducts o"the
nephrons that per$it ater to pass "ro$ urine into thetubule cells
and on to the blood. Fldosterone "unctions byincreasing the
reabsorption o" AaL and Cl- ions& causing $oreater to $o!e into
the blood !ia os$osis.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
30/63
Acid5)ase !o1eostasis
he idneys regulate the p7 le!el o" the blood by
controlling thee8cretion o" hydrogen ions (7L) and bicarbonate ions
(7CH5-).7ydrogen ions accu$ulate hen proteins are $etaboli'ed in
theli!er and hen carbon dio8ide in the blood reacts ith ater to
"or$carbonic acid (71CH5). Carbonic acid is a ea acid that
partially
dissociates in ater to "or$ hydrogen ions and bicarbonate
ions.Both ions are +ltered out o" the blood in the glo$erulus o"
theidney& but the tubule cells lining the nephron selecti!ely
reabsorbbicarbonate ions hile lea!ing hydrogen ions as a aste
product inurine. he tubule cells $ay also acti!ely secrete
additional hydrogenions into the urine hen the blood beco$es
e8tre$ely acidic.
he reabsorbed bicarbonate ions enter the
bloodstrea$ herethey can neutrali'e hydrogen ions by "or$ing ne
$olecules o"carbonic acid. Carbonic acid passing through the
capillaries o"the lungs dissociates into carbon dio8ide and
ater& alloing us toe8hale the carbon dio8ide.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
31/63
)lood ress/re !o1eostasis
he idneys help to control blood pressure in the body by
regulating the e8cretiono" sodiu$ ions and ater and by producing
the en'y$e renin. Because blood is$ostly $ade o" ater& an
increased !olu$e o" ater in the body results in an
increase in the !olu$e o" blood in the blood !essels. ncreased
blood !olu$e$eans that the heart has to pu$p harder than usual to
push blood into !esselsthat are croded ith e8cess blood. hus&
increased blood !olu$e leads toincreased blood pressure. Hn the
other hand& hen the body is dehydrated& the!olu$e o" blood
and blood pressure decrease.
he idneys are able to control blood pressure by either
reabsorbing ater to$aintain blood pressure or by alloing $ore ater
than usual to be e8creted intourine and thus reduce blood !olu$e
and pressure. Sodiu$ ions in the body help to$anage the body#s
os$otic pressure by draing ater toards areas o" highsodiu$
concentration. o loer blood pressure& the idneys can e8crete
e8trasodiu$ ions that dra ater out o" the body ith the$.
Con!ersely& the idneys$ay reabsorb additional sodiu$ ions to
help retain ater in the body.
4inally& the idneys produce the en'y$e renin to pre!ent the
body#s bloodpressure "ro$ beco$ing too lo. he idneys rely on a
certain a$ount o" bloodpressure to "orce blood plas$a through the
capillaries in the glo$erulus. " bloodpressure beco$es too lo&
cells o" the idneys release renin into the blood. Reninstarts a
co$ple8 process that results in the release o" the hor$one
aldosterone bythe adrenal glands. Fldosterone sti$ulates the cells
o" the idney to increase theirreabsorption o" sodiu$ and ater to
$aintain blood !olu$e and pressure.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
32/63
!or1ones
he idneys $aintain a s$all but i$portant endocrine
"unction byproducing the hor$ones calcitriol and
erythropoietin.
Calcitriol is the acti!e "or$ o" !ita$in D in the
body. ubulecells o" the pro8i$al con!oluted tubule produce
calcitriol "ro$inacti!e !ita$in D $olecules. Ft that point&
calcitriol tra!els
"ro$ the idneys through the bloodstrea$ to the
intestines&here it increases the absorption o" calciu$ "ro$
"ood in theintestinal lu$en.
Erythropoietin (EPO) is a hor$one produced by cells o"
theperitubular capillaries in response to hypo8ia (a lo le!el
o"
o8ygen in the blood). EPH sti$ulates the cells o" red bone$arro
to increase their output o" red blood cells. H8ygenle!els in the
blood increase as $ore red blood cells $ature andenter the
bloodstrea$. Hnce o8ygen le!els return to nor$al&the cells o"
the peritubular capillaries stop producing EPH.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
33/63
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
34/63
AT!O!%$IO#OG%
http://var/www/apps/conversion/tmp/scratch_4/PATHOPHYSIOLOGY.docxhttp://var/www/apps/conversion/tmp/scratch_4/PATHOPHYSIOLOGY.docx
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
35/63
#A)ORATOR% RE$U#T$
COMONENT RE$U#T$NORMA#
&A#UE$
ANA#%$I$
R)C 1.; ?.,-,.1 8 /0.? /5.,-/;.,gd9 Decreased
!e1atocrit 1,.;G ?0-,1G Decreased
)C
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
36/63
COMONENT RE$U#T$ NORMA#
&A#UE$
ANA#%$I$
)UN ,; ;-/>$gd9 ndicates renal proble$
Creatinine 51 0.;-/.5$gd9 ndicates renal proble$
he B6A and Creatinine ere belo their nor$al range
thusshoing inability o" the idney to e8crete nitrogenous aste.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
37/63
COMONENT RE$U#T$ NORMA# &A#UE$
ANA#%$I$
R)C 1.? ?.,-,.1 8 /00$l.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
38/63
COMONENT RE$U#T$ NORMA# &A#UE$ ANA#%$I$
Creatinine /5 0.;-/.5$gd9 ndicates renal
proble$
he Creatinine as belo nor$al range thus shoing inability
o" theidney to e8crete nitrogenous aste.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
39/63
COUR$E IN T!E ARD
he patient arri!ed in the dialysis unit at around
;a$. he patient as ell-groo$ed. 7e had a pre-7D eighto" ,?.,g.
7e as cal$& cooperati!e& and hadspontaneous speech
throughout the inter!ie.7oe!er& hen discussing sel"
perception-sel" concept
pattern& the patient displayed beha!ior suggesti!e o"altered
sel"-concept such as a!oidance o" eye contactduring such
discussion& and speaing in aninappropriate aect. 7is !ital
signs throughout the
dialysis period ere as "ollos: BP: /=0-/>0/00-//0$$7g&
PR: >,-
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
40/63
DRUG $TUD% DRUG
NAME
MoA INDICATION CONTRAINDICATION $IDEE""ECT$
INTER&ENTION$
Clonidine
-Antihypertens
ive
Clonidine
sti$ulatesalpha-
1receptors in
brainste$
hich results
in reduced
sy$pathetic
out%o "ro$
the CAS and
a decreasein peripheral
resistance
leading to
reduced BP
and pulse
rate. t does
not alter
nor$alhe$odyna$i
c response
to e8ercise
at
reco$$ende
d dosages.
7ypertensio
n& usedalone or as
part o"
co$bination
therapy.
7ypersensiti!ity.
Disorders o" cardiacpace$aer acti!ity
and conduction.
Pregnancy and
lactation.
dry $outh&
drosiness&di''iness&
irritability&
$ood
changes& sleep
proble$s
(inso$nia or
night$ares)&
headache& earpain& "e!er&
"eeling hot&
constipation&
diarrhea&
sto$ach pain&
increased
thirst&
decreaselibido&
i$potence&
cold sy$pto$s
such as runny
or stuy nose&
snee'ing&
cough& or sore
throat
FRAA3:
Do not discontinueabruptly discontinue
therapy by reducing the
dosage gradually o!er
1K? days to a!oid
rebound hypertension&
tachycardia& %ushing&
nausea& !o$iting&
cardiac arrhyth$ias
(hypertensi!eencephalopathy and
death ha!e occurred
a"ter abrupt cessation
o" clonidine).
Do not discontinue
transder$al therapy
prior to surgery$onitor BP care"ully
during surgery ha!e
other BP-controlling
drugs readily a!ailable.
Continue oral clonidine
therapy ithin ?hr. o"
surgery then resu$e as
soon as possibletherea"ter.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
41/63
DRUGNAME
Mechanis1o6 Action
INDICATION CONTRAINDICATION
$IDEE""ECT$
INTER&ENTION$
F$lodipine
-Calciu$Channelblocer
F$lodipinedecreasesarterial s$ooth
$usclecontractilityandsubseuent!asoconstriction by inhibitingthe
in%u8 o"calciu$ ionsthrough
calciu$channels.nhibition o"
the initial in%u8o" calciu$decreases thecontractileacti!ity
o"arterial s$ooth
$uscle cellsand results in!asodilation.
he!asodilatoryeects o"a$lodipineresult in ano!erall
decrease inblood pressure.
reat$ent "orhypertension orin co$bination
ith otherantihypertensi!es.
7ypersensiti!ity to the drug.
Blood pressureless than
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
42/63
DRUG
NAME
MoA INDICATION CONTRAINDICATION $IDE
E""ECT$
INTER&ENTION$
T3ynsta
ynstacontains aco$binationo"F$lodipine
and el$isartan.F$lodipineis a
calciu$channelblocer.F$lodipinerela8es(idens)
blood!essels andi$pro!esblood %o.
el$isartanis anangiotensin receptor
antagonist. el$isartaneeps blood!essels
"ro$narroing&hich loersbloodpressure andi$pro!es
blood %o.
his product
is used to
treat
hypertension.
hese
$edications
are used
together
hen one
drug is notcontrolling
the blood
pressure. he
doctor $ay
direct the
patient to
start taingthe indi!idual
$edications
+rst& and
then sitch
to this
co$bination
product i" it is
the best dose
7ypersensiti!ity to
F$lodipine and
el$isartan.
Chec ith thephysician +rst i" thepatient has any o"the
"olloing:Se!ere Aarroing o"the Fortic 7eartNal!e& Renal
FrteryStenosis& Fbnor$ally9o Blood Pressure&9i!er
Proble$s&Se!ere 9i!er Disease&idney
Disease&Pregnancy&Decreased BloodNolu$e& E8tre$e
9oss o" Body ater&7igh F$ount o"Potassiu$ in
theBlood.
Signs o" an
allergic
reaction to
ynsta: hi!es
diOculty
breathingselling o"
your "ace&
lips& tongue&
or throat.
Co$$on
ynsta side
eects $ayinclude:
selling in the
hands or "eet&
"ast
heartbeats&
di''iness&
drosiness&
tired "eeling
%ushing
(ar$th&
redness& or
tingly "eeling)
bac pain or
nausea&
diarrhea&
sto$achpain.
Chec blood
pressure be"ore
and a"ter gi!ing
the drug.
nstruct patient to
a!oid getting up
too "ast "ro$ a
sitting or lying
position& or he
$ay "eel di''y.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
43/63
DRUG
NAMEMoA INDICATION CONTRAINDICATION $IDE
E""ECT$
INTER&ENTION$
Terra6err
on
-&it7 and
1inerals
s/pple1e
nt8
Antiane1i
c
Consists o"
4olic Fcid&
ron (4errousSul"ate)&Nita
$in
B/&Nita$in
B/1&Nita$in
B1&Nita$in
B5&
Nita$in B=&
Nita$in C.
Sti$ulates
the
he$atopoieti
c syste$.
Pre!ention
and
treat$ento" iron
de+ciency
ane$ia.
hro$boe$bolis$&
erythre$ia&
erythrocytosis&increased sensiti!ity
to cyanocobala$in.
Aausea
No$iting
Fllergic
reaction:
6rticaria.
Drin ith
orange Iuice to
i$pro!eabsorption and
to $ini$i'e
nausea.
Do not tae ith
$il& tea or
coee.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
44/63
DRUG
NAME
MoA INDICATION CONTRAINDICATION $IDEE""ECT$
INTER&ENTION$
Clopidogr
el
-
antiplatelet
nhibits
platelet
acti!ation
andaggregati
on
through
the
irre!ersibl
e binding
o" its
acti!e$etabolit
e to FDP
receptors
on
platelets.
4or pre!ention
or treat$ent
o" stroe and
heart attac.
7ypersensiti!ity&
Peptic ulcer or
intracranial
he$orrhage.
6se cautiously ith
bleeding disorders&
recent surgery& renal
or hepatic
i$pair$ent&
pregnancy.
Di''iness&
easy
bruising& 3
upset&headache.
Fd!erse
eects:
Rash& DHB&
chest
tightness&
con"usion&tarry stool.
2onitor blood
pressure.
Pro!ide co$"ort
$easures andarrange "or
analgesics i"
headache occurs.
Pro!ide s$all&
"reuent $eals i" 3
upset occurs.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
45/63
DRUG NAME MoA INDICATION CONTRAINDICATION $IDE
E""ECT$
INTER&ENTION$
Montel/9as
t :
#evocitiri;ine
Binds to
cysteinyl
leuotrien
e type /
(Cys9 / )
receptor
in the
upper and
loer
airays to
pre!entleuotrien
e-
$ediated
eects
associated
ith
allergic
rhinitis.
Prophyla8is
or
treat$ento" allergic
reactions
such as
chronic
urticaria&
obstructi!e
airaydiseases
and rhinitis.
7ypersensiti!ity&
patients ith
hepatici$pair$ent.
Aausea&
dry $outh&
drosiness
&
dyspepsia&
headache.
Fd!ise patients that
$onteluast can be
taen ithout
regard to $eals but
to tae it ith "ood
i" sto$ach upset
occurs.
Fd!ise patients ith
non aspirin
sensiti!ity to
continue a!oidanceo" aspirin and
ASFDs hile taing
the drug.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
46/63
DRUG
NAMEMoA INDICATION CONTRAINDICATION $IDE
E""ECT$
INTER&ENTION$
Ni6edipin
e
-calci/1
channel
4loc9er
Decreases
arterial
s$ooth$uscle
contractility
and
subseuent
!asoconstricti
on by
inhibiting the
in%u8 o"calciu$ ions
through
calciu$
channels.
4or treat$ent
o"
hypertension.
7ypersensiti!ity to the
drug& CFD& history o"
heart attac.
Di''iness&
urticaria&
%ushing&tre$ors&
nausea&
heartburn.
2onitor BP
care"ully during
titration period.Patient $ay
beco$e se!erely
hypotensi!e&
especially i" also
taing other drugs
non to loer BP.
ithhold drug and
noti"y physician i"systolic BP @
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
47/63
DRUG NAME MoA INDICATION CONTRAINDICATION $IDE
E""ECT$
INTER&ENTION$
N-
Acetylcystein
e
-1/colytic
E8erts its
$ucolytic
action
through
its "ree
sul"hydryl
group&
hich
reduces
the
disul+de
bonds in
the
$ucus
$atri8
and
loers
$ucus
!iscosity.
ndicated as
adIu!ant
therapy "or
patients ith
abnor$al&
!iscous or
thic
secretions.
Drug hypersensiti!ity Aausea&
!o$iting&
hypotension
& diarrhea or
constipation
.
2onitor patient#s NS
especially RR and
7R.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
48/63
DRUG
NAME
MoA INDICATION CONTRAINDICATIO
N
$IDE E""ECT$ INTER&ENTION$
CaCO<
-phosphat
e 4inder
-dietary
s/pple1e
nt
Fs dietarysupple$ent&used to
pre!ent ortreatnegati!ecalciu$balance inosteoporosis& it
helps topre!ent ordecrease
the rate o"bone loss.
Phosphatebinder:Binds ithdietaryphosphateto "or$
insolublecalciu$phosphate&hich ise8creted in"eces.
6sed "or the
treat$ent o"
hyperphosphate$
ia& nor$ali'ing
phosphate
concentrations in
patients ith CD.
t can also be
used as a calciu$
supple$ent in
these patients.
7ypersensiti!ity&
patients ith
hypercalce$ia&
and
hypophate$ia.
Aausea&
%atulence&
constipation&
8erosto$ia&
!o$iting.
2onitor seru$
calciu$ and
phosphate le!els.
Should be gi!en
ith $eals to
increase
absorption. 2ay
decrease iron
absorption& so
should bead$inistered /-1
hours be"ore or
a"ter iron
supple$entation
li$it intae o"
ith bran& "oods
high in o8alates
or hole graincereals hich
$ay decrease
calciu$
absorption.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
49/63
DRUG
NAME
MoA INDICATION CONTRAINDICATION $IDE
E""ECT$
INTER&ENTION$
"e$O=
-iron
s/pple1ent
Ele!ates
seru$ iron
concentratio
n hich thenhelps to "or$
7igh or
trapped in
the reticulo-
endothelial
cells "or
storage and
e!entualcon!ersion to
a usable
"or$ o" iron.
6sed to treat
iron de+ciency
ane$ia.
7ypersensiti!ity&
se!ere hypotension.
Aausea&
!o$iting&
di''iness.
Fd!ise patient to
tae $edicine as
prescribed.
Caution patient to$ae position
changes sloly to
$ini$i'e orthostatic
hypotension.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
50/63
DRUG NAME MoA INDICATION CONTRAINDICATION $IDE
E""ECT$
INTER&ENTION$
$odi/1
)icar4onate
Sodiu$
Bicarbo
nate
acts asan
alalini
'ing
agent
by
releasin
g
bicarbonate
ions.
6sed "or the
treat$ent o"
$etabolic
acidosishich $ay
occur in
se!ere renal
disease
2etabolic or respi.
alalosis&
hypocalce$ia&
hypo!entilation& andhypersensiti!ity to
drug.
7eadache&
anore8ia&
unpleasant
taste& tired"eeling&
nausea&
andor
!o$iting.
2onitor urinary p7
and urine output as
guide "or dosing.
2onitor patients NS
especially RR and
7R.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
51/63
DRUG NAME MoA INDICATION CONTRAINDICATION $IDE
E""ECT$
INTER&ENTION$
!ydro0i;ine
-antihista1ine
7ydro8y'ine
reduces
acti!ity inthe central
ner!ous
syste$. t
also acts as
an
antihista$in
e that
reduces thenatural
che$ical
hista$ine in
the body.
Co$$only
used to treat
pruritus inpatients ith
ESRD.
7ypersensiti!ity&
glauco$a&
Dry $outh&
drosiness&
nausea&hypotensio
n.
Fssess patient#s
alertness.
nstruct patient notto drin alcohol.
nstruct patient to
increase %uid
intae.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
52/63
A$$E$$MENT DIAGNO$I$ #ANNING INTER&ENTION$
O4>ective data'
Crea'
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
53/63
$/4>ective data'
HUsahay ra9o
1a9aihi nya
ginag1ay ra
/sahay 1/ t/lo ra
gy/d7 ag 1/9aon
9o /g parat1angh/pong
dayon a9ong tiil7
O4>ective data'
resence o6
peripheral
ede1a grade
B Distended
a4do1en
/y 6ace
Olig/ria
:crac9les in
the l/ngs
Crea'
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
54/63
A$$E$$MENT DIAGNO$I$ #ANNING INTER&ENTION$
O4>ective data'
peripheral
ede1a
grade B
Distendeda4do1en
/y 6ace
"reJ/ent
scratching o6
the ar1s7
I1paired s9in
integrity rt
ede$a and
pruritus FEBperipheral
ede$a&
distended
abdo$en&
"reuent
scratching on the
ar$s& puy "ace.
Short er$: F"ter ?
hours o" nurse-patient
interaction& the patient
ill establish beha!iorsto pre!ent sin
da$age.
9ong er$: he patient
ill $aintain intact
sin.
- nspect patient#s sin "or changes in
color& turgor& !ascularity.
- Fssess patient#s peripheral ede$a&ele!ate legs to pro$otes
!enous
return& li$iting ede$a "or$ation.
- Pro!ide soothing sin care to
patient& applying oint$ent or crea$
to relie!e dry and craced sin.
- eep bedchair linen dry andrinle-"ree to reduce sin
irritation.
- Reco$$end patient to use cool&
$oist co$presses to apply pressure
rather than scratch pruritic areas to
pre!ent sin inIury.
- nstruct patient to eep +ngernailsshort.
A$$E$$MENT DIAGNO$I$ #ANNING INTER&ENTION$
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
55/63
$/4>ective data'
HM/9aon gihapon
9og 1ga parat
9ay nag dialysis
na 4ita3 9o para
1a p/slan /nya
1ao ra gihapon
1a1atay ra1an
gihapon7 as
ver4ali;ed 4y the
patient7
DeKcient
9no3ledge rt
in"or$ation
$isinterpretatio
n about dialysis
therapy.
Short er$
ithin ? hours o" nursing
inter!entions& the
patient ill !erbali'e
understanding o"
condition and potential
co$plications.
9ong er$
he patient ill initiate
necessary li"estylechanges.
- Re!ie disease process and prognosis
and "uture e8pectations. his pro!ides
noledge base "ro$ hich patient
can $ae in"or$ed choices.- Re!ie patient#s diet and %uid
restriction as prescribed and e8plain to
the patient the ad!antage o" eating
the ordered diet.
- Educate patient that he$odialysis
treat$ent does not $ean he can eathate!er he lies. he pt. does
not
recei!e dialysis treat$ent daily so he
needs to be care"ul o" hat he eats to
pre!ent co$plication such as li"e-
threatening ure$ia.
- n"or$ patient that eating therestricted diet can "urther
increase the
patient#s blood pressure& and can also
precipitate bone pains and ede$a.
DIAGNO$I$ #ANNING INTER&ENTION$
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
56/63
DIAGNO$I$ #ANNING INTER&ENTION$Ris9 6or In>/ry
r5t in6ection7
ithin ? hours o" nursing
inter!entions& the patient ill
ha!e patent !ascular access
and be "ree o" in"ection.
- 2onitor internal FN shunt patency at "reuent
inter!als. Palpate sin around shunt "or ar$th.
Di$inished blood %o results in coolness o"
shunt.
- Palpate "or distal thrill. hrill is caused by
turbulence o" high-pressure arterial blood %o
entering lo-pressure !enous syste$ and should
be palpable abo!e !enous e8it site.
- Aote color o" blood andor ob!ious separation o"
cells and seru$. Change o" color "ro$ uni"or$
$ediu$ red to dar purplish red suggests
sluggish blood %o andor early clotting.
Separation in tubing is indicati!e o" clotting. Nery
dar reddish-blac blood ne8t to clear yello %uid
indicates "ull clot "or$ation.
- F!oid trau$a to shunt by handling tubing gently&
$aintaining cannula align$ent. Aot taing BP or
draing blood sa$ples in shunt e8tre$ity. o
decrease ris o" clotting or disconnection.
- nstruct patient not to sleep on side ith shunt or
carry pacages& boos& purse on aected
e8tre$ity.
Fd$inister lo-dose o" 7eparin i" indicated to
A$$E$$MENT DIAGNO$I$ #ANNING INTER&ENTION$ Ris "or
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
57/63
O4>ective' L6atig/eLpale 1/co/s1e14ranesLpallor
general
appearance R)C' 27=!g4' 7!ct' 2
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
58/63
DI$C!ARGE #AN
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
59/63
DI$C!ARGE #AN
nstruct patient to strictly tae $edicines as directedand to $ae
a list o" the $edicines& !ita$ins& andherbs that the
patient is taing& including the a$ounts&hen and hy the
patient tae the$. nstruct also thepatient to bring the list to
"ollo-up !isits. 2edicine list
should be carry by the patient in case o" an e$ergency.
nstruct patient to eigh sel" daily& "olloing the goal
eight ordered by his physician. n!ol!e and assist patient
in $aing his e8ercise plan
as directed. Regular e8ercise can help the patient
$anage high blood pressure. Strongly ad!ise patient to uit
s$oing and a!oid
drining alcohol. Fd!ice patient to a!oid stress related
"actors and ha!e
adeuate rest.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
60/63
each the patient to properly care his FN4 or FN3
by"olloing these steps:
Clean the sin o!er the +stula or gra"t e!ery day ith soap
and
ater. ae the bandage o the +stula or gra"t ? to = hours
a"ter dialysis.
Chec the +stula or gra"t e!ery day "or good blood %o bytouching
it ith +ngertips. he bu''ing sensation $eans that it isoring.
Chec "or bleeding& pain& redness& or selling. hese
$ay be signs
o" in"ection or a clogged +stula or gra"t. o pre!ent
da$age to the +stula or gra"t& no one should tae
blood pressure or dra blood "ro$ the ar$ ith the +stula
orgra"t.
Should not ear tight-+tting shirts& Ieelry (such as
bracelets)that $ay restrict blood %o on the access ar$.
$aing sure the straps or handles don#t tighten around the
+stulahen carrying things (groceries& bags&
luggage)&
2aing sure that the patient#s body& pillo or cushion doesn#t
reston the ar$ ith +stula hen sitting or sleeping&
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
61/63
nstruct patient to as his doctor i" he need
!accines. n"ections such as pneu$onia&in%uen'a& and
hepatitis can be $ore har$"ulor $ore liely to occur hen a person
ha!eCD. Naccines reduce the ris o" in"ection ith
these !iruses. nstruct patient to "ollo up chec-up
regularly
ith his physician as directed. nstruct patient to eat
"oods directed by his
doctor. 7is doctor $ay ad!ise hi$ to eat "oodlo in sodiu$&
potassiu$& phosphorus& orprotein. he patient $ay need to
see adietitian i" he needs help planning $eals.
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
62/63
nstruct patient to discuss ith hisphysician regarding ho $uch
%uid hehas to drin e!ery day and hat %uidsthe patient can and
cannot drin.
Encourage patient to suc on hard candyor che gu$ to help
eep $outh $oistithout ha!ing to drin liuids.
nstruct patient to see $edical attentioni$$ediately i"
the sin around the +stulaor gra"t is pain"ul& hot& red&
or sollen.
REA#IATION
-
8/19/2019 End Stage Renal Disease 2o Hypertensive
Nephrosclerosis
63/63
REA#IATION
7igh blood pressure can aect the idneys and can
cause renal da$age. End-Stage Renal Disease brings $any
co$plications
to the body that causes the patient to suer. Renal disease
is a progressi!e disease and is
asy$pto$atic at +rst renal "ailure can be pre!entedthru regular
chec-up and early inter!ention.
7a!ing an ESRD is costly& hassle& and boring
youha!e to spend $oney and ?-,hr. o" your ti$e perdialysis session
"or the rest o" your li"e. Jou ha!e to
$ae changes such as $odi"ying your li"estyle anddiet to a!oid
co$plications.
Jou ill ha!e an altered body i$age.