Embed Size (px)
Citation preview

P
p38MAPK
P38 mitogen-activated protein kinases are a class of
mitogen-activated protein kinases that are similar to the
SAPK/JNK pathway; responsive to stress stimuli, such
as cytokines, lipopolysaccharides (LPS), ultraviolet light,
heat and osmotic shock; and are involved in cell differen-
tiation and apoptosis. Four isoforms of p38MAPK, p38-a(MAPK14), -b(MAPK11), -g (MAPK12 or ERK6), and -d(MAPK13 or SAPK4) have been identified. Similar to the
SAPK/JNK pathway, p38 MAP kinase is activated by
a variety of cellular stresses including osmotic shock,
inflammatory cytokines, lipopolysaccharides (LPS), ultra-
violet light, and growth factors.
p53
Protein (also known as protein 53 or tumor protein 53)
which was named according to its apparent molecular
mass of 53 kDa in gel electrophoresis. It is the product
of the TP53 tumor suppressor gene which is located on
the short arm of chromosome 17p13.1. p53 is involved
in the regulation of cell cycle and apoptosis. P53 deficit
plays a critical in the development of certain tumors.
Cross-References▶Apoptosis
Pancreatic Insufficiency
Eighty-five to ninety percent of patients with cystic fibro-
sis have exocrine pancreatic insufficiency characterized by
poor growth, malnutrition, failure to thrive, abnormal
stools (“steatorrhea”), and deficiencies of fat-soluble vita-
mins. As a consequence, these patients require pancreatic
enzyme replacement therapy and fat-soluble vitamin
supplementation.
Frank C. Mooren (ed.), Encyclopedia of Exercise Medicine in Health and Disea# Springer-Verlag Berlin Heidelberg 2012
Paralympic
The word Paralympic stands for parallel Olympics. The
Paralympic Games are the elite platform for competitive
sport for athletes with disabilities. These games are hosted
by the International Paralympic Committee once every
4 years at the same venues as the summer and winter
Olympic Games.
Paralympic Athletes
▶Disabled Athletes
Paraplegia
(Para: Beside; Plegia: Paralysis). This term refers to
impairment or loss of motor and/or sensory function
related to the thoracic, lumbar, or sacral spinal cord seg-
ments. With paraplegia, arm functioning is spared, but,
depending on the level of the spinal cord lesion, the trunk,
legs, and pelvic organs may be involved. The term is used
also for cauda equina and conus medullaris lesions.
Paraxanthine
Paraxanthine (1,7-dimethylxanthine) is the primary
metabolite of caffeine. Unlike other metabolic by-
products of caffeine, there are no plant sources of
paraxanthine. Paraxanthine is a phosphodiesterase inhib-
itor, adenosine receptor antagonist, and a central nervous
system stimulant.
Parenteral Nutrition
Intravenous feeding which bypasses gastric emptying.
Nutritional formulas are administered which contain
se, DOI 10.1007/978-3-540-29807-6,

690 P Parkinson’s Disease
nutrients such as essential salts, glucose, amino acids
and lipids and some vitamins. This type of nutrient mix-
ture is called total parenteral nutrition (TPN) or total
nutrient admixture (TNA), when no food is given by
other routes.
Parkinson’s Disease
A brain disorder characterized by the progressive degen-
eration of dopamine-producing neurons resulting in
difficulties in the control of movement and cognition.
Cross-References▶Neurodegenerative Disease
Participation
▶Promotion of and Adherence to Physical Activity
Passive Heating
Forced hyperthermia induced by reducing the capacity
for heat loss and increasing the rate of exogenous heat
gain. Achieved during resting conditions, usually by
placing an individual in air or water higher than body
temperature or with the use of a liquid-conditioned
garment.
Passive Tension
Tension in a muscle in the absence of activation. This is
taken as the tension produced by structures other than
crossbridges.
Pathogen
An infectious agent that causes disease in an animal or
plant. They are microbes and microorganisms, such as
a virus, bacteria, prion, or fungus.
Pathological Cardiac Hypertrophy
The growth of the heart in response to pathological stress
stimuli such as myocardial or valve injury, hypertension, or
neurohormonal activation; also called pathological cardiac
remodeling. The condition is associated with reduced con-
tractile pump function of the myocardium and, further-
more, is often but not always also associated with
development of heart disease or failure. In contrast to phys-
iological cardiac hypertrophy, pathological cardiac hyper-
trophy may present with different phenotypes and growth
patterns (eccentric, concentric,mild, severe, and inclusionof
fibrosis and cell death/apoptosis) that depend on the specific
stimuli inducing andmaintaining the hypertrophy. As such,
diverse cellular phenotypes may also be observed in associ-
ation with different myocardial hypertrophy phenotypes.
Cross-References▶Cardiac Hypertrophy, Pathological
PCO2
The partial pressure of CO2 gas within a physiological
solution. The PCO2 is itself dependent on the dissolved
CO2 in solution, the rate of metabolic CO2 production,
the rate of ventilatory CO2 elimination and on whether
CO2 is being added to or removed from tissue stores.
PCr
PCr stands for Phosphocreatine. High-power energy com-
pound stored in cells such as skeletal muscle fibers that can
produce ATP at very high rates for short periods of time.
Peak Aerobic Power
This is the maximum (peak) amount of oxygen that the
athlete can utilize during an incremental exercise test
performed to voluntary exhaustion. Exercise testing is
conducted on a wheelchair, arm crank, cycle, rowing, or
double poling ergometer suited to the athlete’s functional
capacity. The oxygen consumption is expressed in abso-
lute values in Liters/min (L.min�1) or relative to body
weight (ml�1 kg�1 min�1). This is a measure of the ath-
lete’s peak aerobic fitness which is dependent upon the
overall ability to transport, deliver, and utilize oxygen.

Performance P 691
Peak Anaerobic Power
This is the peak power (Watts) that can be generated by
the athlete during upper or lower body exercise in a 30 s
interval. It is expressed in absolute values as Watts or
relative to body weight as Watts/kg. The decline in power
output [(peak minus minimum)/peak] during the test
determines the fatigue index which can be used tomonitor
the athletes progress during a training season.
Peak O2 Uptake
▶Aerobic Power, Tests of
Peak Oxygen Consumption( _VO2peak)
The highest oxygen uptake elicited during an exercise test to
exhaustion, in the absence of an oxygen uptake plateau. It is
expressed either as an absolute rate in liters of oxygen per
minute (l/min) or as a relative rate in milliliters of oxygen
per kilogram of bodyweight per minute (ml/kg/min).
Cross-References▶Maximal Oxygen Uptake ( _VO2 max)
P
Peak Walking Time
The walking time at which ambulation cannot continue
due to maximal leg pain, thereby forcing the discontinu-
ation of a treadmill test.
Pedometer/Accelerometer
A pedometer/acceleromter is a relatively inexpensive form
of personal motion sensor. It was originally based on
a watch, with the impulse arising from each pace trigger-
ing a single turn of the escape mechanism. Modern forms
of the device still have a lever arm that is moved by each
pace, but the lever actuates a piezo-electric crystal. Filters
are set so that incidental movements are eliminated, and
each step records as a single count. From the force of the
impulse, the intensity of energy expenditure can be
gauged. A storage device records information for
up to 60 days. Data can later be analyzed in terms of the
intensity of energy expenditure during each 4 s interval
(11 potential levels) and the cumulative step count over
selected portions of a day or week.
Pennation Angle
The angle between the longitudinal axes of the whole
muscle and its fibers. Large pennation angles allow more
fibers to be packed into a muscle producing more force at
the cost of a reduced velocity of shortening.
Peptide F
▶Opioid Peptides, Endogenous
Perception and Action
Processes by which information is picked up and used to
coordinate ongoing behaviors in a specific performance
environment. In ecological dynamics the emphasis is on
the cyclical relationship between perception and action,
where one needs to act in order to perceive information as
well as perceive information to support further actions. In
this approach, knowledge of a performance environment is
predicated on perception and action. The key idea of the
cyclical mutuality of action and perception has significant
implications for the design of experimental research and
practice settings in sport. In order to achieve the goals of
better understanding or better performance, respectively, it
is imperative that participants/athletes be allowed to move
and seek information for action in experiments/training.
Performance
JULIEN S. BAKER, FERGAL GRACE, LON KILGORE
Health & Exercise Science, School of Science,
University of the West of Scotland, Hamilton,
Scotland, UK
SynonymsPerformance factors

692 P Performance
DefinitionPerformance in sport is the expression of the human
body’s capacity to achieve a specific movement task within
a sporting or games environment. There is a tremendous
breadth of action variables that determine some or all
aspects of ▶ performance outcomes. Good performance
outcomes involve the efficient synchronization of all ana-
tomical, physiological, neurological, and psychological
systems. Performance outcomes can be determined by
simple objective measurement, however, in many
instances it is measured by points scored, proximity of
the performance to a predetermined standard, or by sub-
jective evaluation. Regardless of performance measure
type, to be useful, ▶ performance measures must relate
to successful performance.
Performance, in the general context of exercise, refers
to the execution of an exercise, training protocol, or phys-
ical activity, i.e., performance of exercise, performance of
training, or performance of physical activity. The two uses
of the term are fundamentally different.
DescriptionPerformance across all sports is multifaceted and involves
the interaction of many biological and environmental
factors. Assessment of performance is variably complex,
depending on the sport and on the level of complexity in
analysis required (see Fig. 1). Examples of simple analyses
are how much weight was lifted, how fast was the distance
covered, and were the points scored greater than those
scored by the opponent. More complex analyses are usu-
ally performed on higher-level athletes where physiologi-
cal, biomechanical, and psychological assessments are
Endurance
PhysicalFitness
EnvironmentPsychological
Status
Skill
CompetencyExperience Strategy
Performance
Strength Mobility
Performance. Fig. 1 Schematic outlining of the contribution
of peripheral markers of performance
used frequently to identify weaknesses in athletes in
respect to performance enhancement [1]. Other complex
assessmentmethods can be related to teamperformance and
dynamics. At higher levels of sport, it is fairly common to
have exercise and sport scientistsmeasure individual or team
performance and provide coaches and managers with per-
formance profiles of an individual, a team, or elements of a
team. These results can sometimes be used in a comparative
way, with opponents, other athletes or peer groups of ath-
letes or teams, but often they are used in isolation as
a measure of the performance of a team or individual
alone. Exercise scientists generally have concentrated their
analyses of performance on sports in which the movement
technique is critical. Such sports involve predominantly
closed skills and are classified as acrobatic (including gym-
nastics, trampolining, diving, and freestyle skiing), athletic
(including jumping and throwing), and cyclic (including
running, swimming, skating, and wheelchair racing). Very
few investigations into performance have been done on
athletic events that do not lend themselves well to the labo-
ratory environment such as rock climbing and dance.
ApplicationThe technique used to accomplish the performance goal,
or primary performance parameter (such as the distance
jumped in the long jump), is initially partitioned into
secondary performance parameters, such as the take-off,
height, and landing distances. For each performance goal
there is generally an accepted technical standard that
serves as a reference. The use of the hierarchical technique
model then allows performance parameters expressed by
the athlete to be compared to the movements of the
standard and that a teaching/corrective protocol can be
developed to treat critical differences and thus contribute
to successful execution of the performance goal. Any
parameter or movement variable can be considered as
a performance indicator, providing that its manipulation
meaningfully contributes to future performance. These
performance indicators are usually externally visible kine-
matic phenomena. Body segment velocities, joint angles,
changes in center of mass, anthropometric variation,
among many other individual and observable variables
contribute to performance specific to the individual.
Observable interactions or results of interactions with
the environment or objects also directly affect sport per-
formance. The means by which a pitcher or bowler moves
the body to produce high velocity and varied trajectory
projectile movement are examples. Although the end
results of these two performance goals are similar,
launching a high-velocity projectile, the performance of
the two skills is quite different as they are executed under

Performance Factors P 693
P
different conditions and rules. Analysis of such perfor-
mance is often done via high-speed video analysis, digiti-
zation, measurement of net joint reaction forces, and
▶ electromyography (EMG). Relating all of these indicators
to the improvement of efficiency of movement is the short-
term goal, augmenting performance is the culminating goal.
Exercise scientists have historically paid far less atten-
tion to team sports than to individual sports, perhaps
because of the perception that physiological and biome-
chanical interventions are less important in those sports
compared to psychological preparation and tactics. Per-
haps it is because team sports do not lend themselves easily
to in-the-laboratory study. There are some exceptions to
this. They include analyses of fast bowling in cricket,
soccer skills, and limited studies of other games such as
rugby and racquet sports. Even then, however, the focus is
predominantly on isolated individual closed skills within
the game. There are also physiological profiles of sports
teams by position available but little prospective work on
how best to train them for optimal performance. The lack
of analyses of team sports performance is regrettable,
given that the most important requirement for success
for any athlete is skill, which is the element of performance
that scientists try to evaluate, understand, and measure.
The result is insufficient attention to the interaction of
skill and successful performance.
Athletic preparation for performance includes [A]
physical training to meet the physiological, mechanical,
and environmental demands of sport and [B] skill practice
where neuromuscular coordination, synchrony, and
within game strategies are developed. Many coaches
attend to these two aspects of performance and expect to
achieve great performances in their competitions. What
many fail to realize is that there are many complicated
interactions that can change the way they perform, and
not all of them can be solved by technical improvement,
physiological development, or through psychological
preparation. Innate athletic ability (the genotype of the
individual) is important determining sports performance
outcomes [2]. Another physiological factor that affects
performance is nutrition. Nutritional interventions do
not independently drive physiological adaptations, train-
ing improves fitness and performance. Rest, the time
allotted between training sessions, and recovery, the pro-
cess of regaining cellular, systemic, and organismal
homeostasis must also be attended to for best results in
performance. This concept was first elucidated by Hans
Selye in 1936 [3]. In the ensuing decades, the concept has
steadily been adopted for application in fitness enhance-
ment and sports training applications. Psychological fac-
tors such as confidence, self-efficacy, arousal, and
motivation may also intrude upon performance in both
positive and negative manners [4].
The coach–athlete interrelationship is complex and
can be crucial in performance outcomes. Coaching style
can be an advantage or impediment to performance
depending on the learning style, maturational, and emo-
tional status of the athlete. In team sports this interaction
is compounded as there is an added set of interactions
between the coach and team within peers on the team.
The last, and arguably the most critical element of
sport performance is the competitor or team against
which the performance occurs. A cycling time trial pro-
vides a vastly different experience than a rugby scrum.
Cycling’s indirect means of competition requires
a different approach to preparation than rugby’s head-on
competition. The caliber of the opposing competition can
also affect performance. Competing against a lower level
athlete may not provide the more talented or prepared
athlete a means by which to perform at the fullest ability.
Conversely competing against a perceived superior com-
petition may elevate an athlete to a new best performance.
Sports performance issues are vast and complex. The
means by which we maximize potential to perform is
a difficult problem and remains an area of uncertainty
[5]. As a result true or maximal performances are rare
and may only happen on very few occasions in an athlete’s
competitive career.
Cross-References▶Overtraining Syndrome
▶Overtraining-Biochemical Markers
References1. Phillips E, Davids K, Renshaw I, Portus M (2010) Expert perfor-
mance in sport and the dynamics of talent development. Sports Med
40(4):271–283
2. Jones A, Montgomery HE, Woods DR (2002) Human performance:
a role for the ACE genotype? Exercise Sport Sci Rev 30(4):184–190
3. Selye H (1936) A syndrome produced by diverse nocuous agents.
Nature 138:32
4. Arent SM, Landers DM (2003) Arousal, anxiety, and performance:
a reexamination of the Inverted-U hypothesis. Res Q Exerc Sport
74(4):436–444
5. Midgley AW,McNaughton LR, Jones AM (2007) Training to enhance
the physiological determinants of long-distance running perfor-
mance: can valid recommendations be given to runners and coaches
based on current scientific knowledge? Sports Med 37(10):857–880
Performance Factors
▶Performance

694 P Performance Measure
Performance Measure
A direct performance measure assesses the performance
outcome (event time, mass moved, points scored, win or
lose). An indirect performance measure assesses nondirect
variables that contribute to achievement of a performance
outcome.
Performance Outcome
The end movement result of an intended sport perfor-
mance, usually linked to success or failure of the individ-
ual effort, winning or losing, and competency or
incompetency.
Performance Standard
A recognized referent marker of performance capacity rel-
ative to a given sport. A standard can be a set of anatomical
andmechanical descriptors of technique or it can be a set of
values in a specific sport indicative of level of achievement.
Ideally these are developed scientifically, however, many
experiential (nonscientific) standards are commonly used.
Perimenopause
▶Menopause
Perimysium Externum
Older equivalent (used particularly in Europe) for epimy-
sium, that is, the connective tissue tubes that surround and
delimits muscles. It is continuous with both the perimysial
stroma of the muscle and extramuscular structures.
Perimysium Internum
Older equivalent (used particularly in Europe) for peri-
mysium, that is, the connective tissue tube that surrounds
a group of muscle fibers or a group of fascicles within
a muscle. It is continuous with the endomysial stroma.
Periodic Limb MovementsDuring Sleep
A sleep disorder characterized by repetitive and stereo-
typed limb movements, often the legs, while asleep; com-
monly abbreviated PLMS.
Periodization
DAVID J. SMITH1, STEPHEN R. NORRIS
2
1Human Performance Laboratory, University of Calgary,
Calgary, AB, Canada2Canadian Sport Centre - Calgary, University of Calgary
and Mount Royal University, Calgary, AB, Canada
SynonymsMethod of planning athletic training
DefinitionThe concept of▶Periodization at its most fundamental or
base level simply encompasses the practice of effective
time management in the pursuit of an aspired-
to-performance level at some future date or targeted com-
petition. Bompa [1] describes periodization as a planning
process which is a methodical, scientific procedure to help
athletes achieve high levels of training and performance. It
is the most important tool a coach has in conducting
a well-organized training program where a coach is only
as efficient as his or her organization and planning.
Periodization is the purposeful sequencing of different
▶ training units (long duration, medium duration,
and short-term training cycles and sessions) so that
athletes could attain the desired state and planned
results [2].
DescriptionThe advancement of this fundamental concept is the array
of suggested and/or systematic assemblies of training direc-
tions and methodologies put forward by a myriad of
authors, theorists, and practitioners over literally
thousands of years. Furthermore, periodization has
evolved in the lexicon of training methodology to become
“a synonym for the planning of training” [3] and may be
generally thought of as the process and execution of
a purposeful organization of training and competition.
This observation reinforces the notion that the concept is
not some fixed entity with one set of guiding principles,
but rather a more varied construct, typically based around

Periodization P 695
P
some central doctrine that shapes or influences both the
content and sequencing of training.
The training of humans for athletic endeavors
(whether for peaceful or military pursuits) has long been
characterized by a “periodized” or “segmentalized”
approach. For example, Siff [4] remarks that “in the for-
malized sports setting, the Greeks of more than 2,000 years
ago prepared for the Olympic Games by allocating a
preparatory training period of at least 10 months a year.”
From this commentary one can deduce that the remaining
2 months of the year were utilized for competition
(and possibly recovery), therefore, at least a twophasic
(if not three) approach. Indeed, this is revealed in more
detail by Bompa’s [1] extensive research and commentary
concerning the work of Philostratus around the
planning and training processes of Greek Olympians
(circa A.D. 200).
The Twentieth Century saw prolific advancement in
periodization constructs, particularly driven by protago-
nists in the Soviet Union, Scandanavia, and other eastern
European states. Texts produced during the early part of
the 1900s revealed the now classic three-phase format
(general, preparatory, and specific) of training, as well as
the realization of the need for alternating periods of
work and rest/training and recovery. By the 1950s and
1960s several authors had begun to produce “scientific
rationales” for organized training citing underlying bio-
chemical processes, maturation influences, fatigue and
fitness indices, as well as analyses of training “loads”
[1, 2, 7]. Often cited as the “father of periodization,”
Matveyev has had a profound effect upon the literature
and thinking surrounding periodization in the “modern
era” (arguably defined as 1960 onward). Central to
Matveyev’s thinking was the suggestion that the periodi-
zation of training was governed by a predetermined set of
laws that describe the content, degree of training stress
(load), and actual sequencing of training on some chro-
nological and likely cyclical basis.
The division of the training and competition calendar
into segments of varying duration based around specific
themes (i.e., general, preparatory, competitive, transition,
or recovery phases) [1, 2, 4] has yielded a unique language
(set of terms or jargon) concerning periodization. Terms
such as▶microcycle (typically a period of training lasting
a week or several days), ▶mesocycle (several weeks), and
▶macrocycle (several months or an entire competitive
season) have become the backbone of understanding,
along with phrases such as yearly or annual training plan
or single, double, or multiple periodized plans, when
describing training and competition designs. These
terms are related often to the traditional cyclic nature of
training whereby common themes are repeated at
predetermined periods within the ▶ yearly training plan
(YTP) and even over multiple years of training as
described by Harre (1973) [5] and Matveyev (1981) [6]
in the commentary by Issurin [2]. Bompa [1] has built
specific themes of periodization such as strength,
▶ endurance, speed and power, skill acquisition and sta-
bilization, nutrition and psychology, all of which must be
interwoven into a program that has a holistic approach.
This last point emphasizes that a comprehensive
periodized plan has many different elements that must
be considered in the design and effective implementation
such that a critical supporting element of a modern
periodized plan is an appropriately administered testing
and monitoring regime.
The modern approach to the planning of training and
competition involves a systematic evaluation of previous
training and▶ performance, a thorough assessment of the
athlete’s current status and projected target level, and
the establishment of a framework of training cycles
designed to bring about optimal performance within the
specified period of time. This process is then characterized
by a methodical and scientifically based procedure
that can be viewed as a critical tool for a coach striving
to establish a well-organized training program. A well-
designed program seeks to remove or reduce possible
uncertainties in the entire process and ensure that
the plan is organized into focused and manageable
periods, often associated with defined benchmarks or
criterion measures to constantly assess both the
predicted competition performance level and the degree
of relative training and non-training load imposed upon
the athlete.
The aspect of ▶ individualization is also a fundamen-
tal component for consideration for a periodized plan
to be ultimately successful. Essentially, the plan must
effectively pay attention to the various training and
training-related stimuli acting upon the individual, even
in a team sport setting. However, Norris and Smith [7]
remark that, “A wealth of information, both documented
and anecdotal, reveals, at least superficially, a massive
range in the structure or type of training programs that
have been successful in terms of elite competitive perfor-
mance. This probably reflects the ‛elasticity’ of response to
various stimuli and human diversity (as largely dictated by
the underlying genetic matrix and supported by the envi-
ronment in which an athlete or team is immersed).”
Finally, periodization, as manifest in most recent situa-
tions, tends to reflect the underlying training philosophy
of the coach in question rather than some adherence to
a fixed methodology.

696 P Periodization
ApplicationIn the traditional model, pre-1980s, elements include the
hierarchical system of training units (macro-, meso- and
microcycles), the differentiation between general and spe-
cialized preparation together with changes in volume and
intensity of training [2]. The model was centered around
Olympic Games and World Championships performance
with one or two peaks per year with training based around
general, preparatory, competitive, transition, or recovery
phases. However, when the exponential commercializa-
tion of sport occurred and scientific knowledge of training
adaptation increased, the sport environment created pres-
sure to rethink the traditional model of periodization.
Identified limitations of the traditional approach included
simultaneous development of multiple technical
skills; the capability to achieve multi-peak performances
together with excessively long basic and sport-specific
preparation [2]. The forces of change included an
increase in the number of international competitions
requiring more multi-peaking throughout a season rather
than the one or two peaks per year; an increase in financial
remuneration for sport organizations, promoters, and
athletes alike due to the increased competitive schedule;
and an increase in international coaching cooperation
together with enhanced training methods and quality.
With the addition of more frequent competition, interna-
tional level competitors could use the additional compe-
titions to enhance their preparation for end macro cycle
key competitions since competition can be regarded as the
Week Date 02 09 16 23 30 06 13 20
Competition Schedule
Major
Comp
Minor
Comp
MacrocycleTraining StageMicrocycle # 34 35 36 37 38 39 40 41
Competition Block Specific Block
Recovery (days) /General Block 3
Months May June
Periodization. Fig. 1 An example of a summer sport internation
together with mesocycle blocks. The numbers denoted in a block
highest form of training. However, correct competition
sequencing is necessary in the planning process to avoid
under-performance.
The alternative model that has emerged is termed
Training Block Periodization or ▶Block Periodization
Concept (BPC) consists of three types of specialized train-
ing blocks. In general, the training blocks are 2–6 weeks in
length and correspond to a mesocycle of training, where
the blocks provide for consecutive development of specific
capacities including skills and physiological components
in successive mesocycles [8]. The key principles of BPC are
that the mesocycles are structured to produce one of three
different effects: accumulation of basic motor and techni-
cal skills; transformation of skills into event-specific pre-
paredness, and readiness for competition with a planned
result. The transformation block may consist of volume
extensive or intensity intensive training depending on the
sport. Furthermore, it has been suggested that the BPC
allows focused training on selected rather than multiple
abilities in a block, and that athletes are able to maintain
fundamental and sport-specific training effects within
a narrow range allowing for maximization of multi-peak
performance (Fig. 1).
The training effect retention is a cornerstone of the
concept where training effects remain for a period of time
after the training of that capacity or skill stops. The process
of building a YTP involves determining the mandatory
competitions followed by dividing the training stages into
macro-, meso-, and microcycles. The next detailed
27 04 11 18 25 01 08 15 22 29 05 12 19
Major
Comp
Minor
Comp
World
Champ
42 43 44 45 46 47 48 49 50 51 52 1 2
4
3
4 7 7
Competition Cycle
July Aug Sept
al calendar with macrocycles, training stages, and microcycles
refer to number of days. (Adapted from Issurin, 2008) [8]

Peripheral Arterial Disease P 697
development of the planning process requires determina-
tion of the durations of training cycles, additional compe-
titions, and incorporation of training camps.
Furthermore, recovery regeneration periods together
with fundamental training must not be overlooked but
rather be regarded as essential to the training process.
Overall, the block periodization concept utilizes
sequenced mesocycles where training is focused on
a small number of athlete skills and capacities. Issurin
[8] comments that where traditional periodization simul-
taneously develops many athletic skills and physiological
systems, the block method focuses on consecutive devel-
opment in successive mesocycles and nutrition and
recovery programs can be targeted at the predominant
type of training.
In summary, the periodization of training should be
viewed as a critical tool incorporating both theoretical
elements and practical scientific knowledge in the applied
setting such that the processes of preparation, competition
execution, and recovery are optimized.
P
References1. Bompa TO (1999) Periodization: theory and methodology of
training, 4th edn. Human Kinetics, Champaign
2. Issurin VB (2010) New horizons for themethodology and physiology
of training periodization. Sports Med 40(3):189–206
3. Verkhoshansky Y (1999) The end of “periodization” in the training of
high performance sport. Modern Athlete Coach 37(2):14–18
4. Siff MC (2003) Supertraining. Supertraining Institute, Denver
5. Harre D (ed) (1973) Trainingslehre. Sportverlag, Berlin
6. Matveyev LP (1981) Fundamental of sport training. Progress
Publishers, Moscow
7. Norris SR, Smith DJ (2002) Planning, periodization, and sequencing
of training and competition: the rationale for a competently planned,
optimally executed training and competition program, supported by
a multidisciplinary team. In: Kellmann M (ed) Enhancing recovery:
preventing underperformance in athletes. Human Kinetics,
Champaign, pp 121–141
8. Issurin VB (2008) Block periodization: breakthrough in sport
training. Ultimate Athlete Concepts, Michigan
Periodized Resistance Training
A set of methods used to provide variation in the pro-
gression of a resistance training program involving set
methods for altering the intensity (resistance used) and
volume (total work done) over time. Additionally,
changes in the acute program variables can also be
made to provide variation in the training stimulus over
time.
Peripheral Arterial Disease
ANDREW W. GARDNER
CMRI Hobbs-Recknagel Professor, General Clinical
Research Center, University of Oklahoma Health Sciences
Center, Oklahoma City, OK, USA
SynonymsPeripheral vascular disease
Definition▶Peripheral artery disease (PAD) is a slowly progressive
disease characterized by stenoses and occlusions of the
abdominal aorta, iliac, femoral, popliteal, and tibial arter-
ies of the lower extremities. Reduction in blood flow distal
to arterial lesions results in low ankle pressure and low
ankle/brachial systolic pressure index (ABI), the hallmark
clinical measure for detecting PAD [1]. Presence of PAD is
defined by ABI values of �0.90, with ABI values >0.90
considered in the normal range. Clinical PAD has been
recognized since as early as 1831, and the disease spectrum
varies from asymptomatic PAD to gangrene and limb
ischemia requiring amputation. Two schemes, both
based on symptoms and clinical measures, are commonly
used to classify severity of PAD (Tables 1 and 2).
Patients with PAD become symptomatic during
ambulation when peripheral circulation is inadequate to
meet metabolic requirement of the active leg musculature.
Insufficient circulation results in leg pain, termed▶ inter-
mittent claudication, thereby limiting daily ambulation.
Consequently, patients with PAD have severe limitation in
exercise performance, and decreases in physical activity
and quality of life. While the primary pathophysiology is
limitation in blood flow, macrovasculature abnormalities
do not entirely explain the functional limitations imposed
by PAD. Even though severity of PAD is based on ABI
measurements, ABI by itself does not reliably predict
exercise performance. Other various explanations such as
oxidative stress with resultant oxidative injury, alterna-
tions in skeletal muscle metabolism, and changes in
microcirculation have been proposed as the pathophysio-
logical bases for claudication. A primary therapeutic goal
for PAD patients with claudication is to regain lost
physical function through exercise rehabilitation mainly
focused on ambulation. Numerous studies have
documented the efficacy of exercise rehabilitation to
improve ▶ claudication onset time (COT), ▶ peak walk-
ing time (PWT), and other functional outcome measures
using the standard model of supervised exercise.

Peripheral Arterial Disease. Table 1 Fontaine classification
of peripheral artery disease
Stage Symptoms
I Asymptomatic
II Claudication
IIa Pain-free, claudication walking >200 m
IIb Pain-free, claudication walking <200 m
III Rest/nocturnal pain
IV Necrosis/gangrene
Peripheral Arterial Disease. Table 2 Rutherford classifica-
tion of peripheral artery disease
Grade Category Clinical description
I 0 Asymptomatic; not hemodynamically
correct
1 Mild claudication
2 Moderate claudication
3 Severe claudication
II 4 Ischemic rest pain
5 Minor tissue loss; nonhealing ulcer, focal
gangrene with diffuse pedal ischemia
III 6 Major tissue loss extending above
transmetatarsal level; foot no longer
salvageable
698 P Peripheral Arterial Disease
CharacteristicsCharacteristics of PAD Patients. PAD shares risk factors
with coronary artery disease (CAD). In addition to age
andmale sex, risk factors for PAD include smoking, hyper-
cholesterolemia, diabetes,▶ hypertension, chronic kidney
disease, hyperhomocysteinemia, elevated fibrinogen con-
centration, family history of premature atherosclerosis
(suggesting that genetic factors may influence the devel-
opment of PAD), and being non-white. Although PAD can
be seen in the absence of clinical CAD, asymptomatic CAD
is frequently present in patients with PAD. Additionally,
patients with PAD have increased risk for cerebral artery
disease, cardiovascular events, and cardiovascular mortal-
ity. The relative risk of all-cause mortality associated with
PAD is 1.4–3.8, and increases with worsening symptom-
atology. Due to increased cardiovascular risk associated
with PAD, every subject presenting with PAD should be
considered to have CAD until proven otherwise. Evalua-
tion and treatment for PAD should include evaluation and
control of CAD risk factors. Exercise rehabilitation is one
approach to attempt to reduce the risk for both morbidity
and mortality in patients with PAD.
Characteristics of Exercise Programs. Exercise therapy
was first suggested in 1898, with the first randomized
controlled trial published in 1966 demonstrating an
improvement in treadmill walking ability. In contrast to
either drug treatment or surgical procedures, the clinical
management of claudication in patients with PAD can be
significantly improved with little cost, morbidity, and
mortality through physical conditioning. Significant
improvements in claudication pain have occurred follow-
ing supervised exercise rehabilitation. For example, the
average increase in COT is 179% following rehabilitation,
and the average increase in PWT is 122% [2]. A recent
report from our laboratory found that a home-based
exercise program, quantified with a step activity monitor,
has high adherence and is efficacious in improving clau-
dication measures [3]. Furthermore, home-based exercise
appears more efficacious in increasing daily ambulatory
activity in the community setting than standard super-
vised exercise. The clinical implication is that home-based
exercise programming, with patient monitoring and peri-
odic feedback, may serve as a new model for improving
claudication measures in more patients with less effort
and fewer resources.
Optimal improvements in claudication symptoms are
elicited by having patients walk intermittently beyond the
onset of pain for as long as they can safely tolerate, and
perform this exercise program for aminimum of 6months
[2]. Although the duration and frequency of the exercise
sessions are not independent predictors of the change in
claudication pain times, a reasonable goal for patients
should be to eventually walk for at least 30 min per session
for at least three sessions per week. A recent review of only
five controlled trials recommends that the optimal exercise
program for treating claudication consists of exercising
under supervised conditions for at least 2 months and at
high intensity. However, provided that a similar volume of
exercise is completed, we found that changes in COT and
PWT are not different following training at a relative low
intensity (40% of maximal intensity) compared to a rela-
tively high intensity (80%) [4]. A recent report has also
confirmed the efficacy of low-intensity pain-free exercise
[5]. Thus, beginning the training program at relatively low
intensity and short duration, and gradually increasing the
intensity and duration throughout the program is a pru-
dent approach to safely rehabilitate patients with claudi-
cation. Table 3 summarizes proposed recommendations
for an exercise program for patients with PAD.
Numerous mechanisms have been proposed to explain
the improvement in walking distances to the onset and to

Peripheral Arterial Disease. Table 3 Proposed recommen-
dations for an exercise program for patients with peripheral
artery disease
Exercise
component Comment
Frequency Three exercise sessions per week
Intensity Initially, 40% of peak exercise capacity, with
gradual progression to 80% by the end of
the program
Duration Initially, 15 min of exercise per session, with
gradual progression to 40–50 min by the
end of the program
Mode Walking is preferred, but nonweight-
bearing tasks (e.g., bicycle and arm
ergometry) may be used to supplement
ambulatory training, or be the primary
mode of training if patients have difficulty
ambulating
Pain threshold Exercise to moderate-to-severe
claudication pain (score of 3 using a 4-point
pain scale) is efficacious. However,
evidence is emerging that low intensity
exercise eliciting less severe pain, and
pain-free exercise are efficacious as well
Program
length
2–6 months
Peripheral Arterial Disease P 699
P
maximal claudication pain following exercise rehabilita-tion. The mechanisms primarily center on hemodynamic
and enzymatic adaptations within the exercising muscu-
lature of the symptomatic leg(s). These mechanisms
include an increase in blood flow to the exercising leg
musculature, a more favorable redistribution of blood
flow, greater utilization of oxygen because of a higher
concentration of oxidative enzymes in the mitochondria
of exercising muscles, improvement in hemorheologic
properties of the blood, a decrease in the reliance upon
anaerobic metabolism, and an improvement in the effi-
ciency of walking. It is likely that a combination of changes
in these factors contribute to the improved walking
distances. Improvements in psychosocial attitude due to
accomplishments that are achieved during exercise reha-
bilitation may further enhance this effect.
MeasurementsNoninvasive Vascular Tests. The most common measure to
assess the presence and severity of PAD is the ABI. PAD is
typically defined by an ABI value. The sensitivity of using
the ABI cut point of �0.90 is greater than 90%. Generally,
a patient whose ABI is <0.8 will be symptomatic with
claudication during exercise, and a patient whose ABI
is <0.30 will generally complain of pain at rest. Very
high ABIs >1.3 are considered invalid because they do
not reflect the true ankle blood pressure. Rather, it is
caused by arteries that have become calcified or non-
compressible, termed calcific medial sclerosis, which is
often observed in patients with diabetes.
Segmental systolic blood pressure measures in the
brachial, upper thigh, lower thigh, and ankle locations
have been used to access the extent of PAD. Additional
noninvasive tests for PAD include Doppler ultrasonogra-
phy (i.e., measurement of blood flow velocity), plethys-
mography (pressure-wave tracing), and measurement of
post-occlusive reactive hyperemia (PORH). PORH is
performed by occluding arterial flow by inflating a blood
pressure cuff above systolic pressure at the level of the
upper thigh or knee for 3 min, followed by measurement
of the systolic blood pressure at the ankle or calf blood
flow within seconds after releasing the occlusion. When
compared to patients without vascular disease, patients
with PADwill demonstrate a lower post-occlusive ABI and
a delayed return to pre-occlusion pressures. The sensitivity
of the post-occlusive ABI is >95%. For individuals who
present with classic claudication and who have ABI values
in the borderline-to-normal range (0.91–1.30), or who
have ABI values above normal (greater than 1.30), alter-
native diagnostic strategies should be used to confirm the
diagnosis of lower extremity PAD. These alternative
methods include the toe-brachial index, ABI after tread-
mill exercise, segmental systolic blood pressures, duplex
ultrasound, Computed tomographic angiogram, and
magnetic resonance angiogram.
Treadmill Testing. The primary effect of PAD has on
acute exercise is the development of claudication pain in
the leg musculature as a result of insufficient blood flow.
As a result, claudication and peripheral hemodynamic
measurements obtained from a treadmill test are the
primary criteria to assess the effectiveness of an exercise
program. The specific claudication variables that are mea-
sured to assess the functional severity of PAD include the
COT and PWT. ABI measurements obtained before and
after the treadmill test, in addition to COT and PWT,
provide a more objective assessment of disease severity.
The primary objective of a treadmill test for patients
with PAD is to obtain reliable measures of (1) COT and
PWT, (2) the ABI response to exercise, and (3) the pres-
ence of coexisting coronary heart disease. The test should
be a progressive test with gradual increments in grade. By
having a test with small increases in exercise intensity,
COT and PWT measures of patients can be stratified

700 P Peripheral Vascular Disease
according to disease severity. A highly reliable treadmill
test for patients with PAD uses a constant walking speed of
2 mph and gradual increases in grade of 2% every 2 min
beginning at 0% grade. By using this treadmill protocol,
typical COTand PWT values are approximately 3 min and
6 min, respectively. Measurement of the ABI immediately
after a treadmill exercise stress test can help diagnose PAD
in difficult cases, as well as determine the extent of impair-
ment of the peripheral circulation. Exercise increases sys-
temic blood pressure (i.e., the brachial pressure), while
pressure distal to an arterial lesion in the lower extremity
falls with exercise as a consequence of dilation of second-
ary arterioles. As a result, ABI typically drops from a
resting value of 0.7 to approximately 0.3 immediately
following the treadmill test. The sensitivity of ABI mea-
sured after treadmill walking is >95%. Gas-exchange
measures during the treadmill test show that PAD patients
with claudication have peak oxygen consumption values
in the range of 12–15 mL kg�1 min�1 which is approxi-
mately 50% of age-matched controls. Favorable changes
following a program of exercise rehabilitation should
include increases in COT and PWT, an increase in
peak oxygen consumption, and possibly a blunted drop
in ABI and a faster rate of recovery in ABI to the resting
baseline value.
Cross-References▶Arteriosclerosis
References1. At H, Zj H, NrH, Cw B,MaC, Jl H et al (2006) Acc/Aha 2005 practice
guidelines for the management of patients with peripheral arterial
disease (lower extremity, renal, mesenteric, and abdominal aortic):
a collaborative report from the American Association For Vascular
Surgery/Society For Vascular Surgery, Society For Cardiovascular
Angiography And Interventions, Society For Vascular Medicine and
Biology, Society of Interventional Radiology, and The Acc/Aha Task
Force On Practice Guidelines (Writing Committee to develop guide-
lines for the management of patients with peripheral arterial disease):
endorsed by the American Association of Cardiovascular and Pul-
monary Rehabilitation; National Heart, Lung, and Blood Institute;
Society for Vascular Nursing; Transatlantic Inter-Society Consensus;
and Vascular Disease Foundation. Circulation 113:E463–E654
2. Aw G, Et P (1995) Exercise rehabilitation programs for the treatment
of claudication pain. A meta-analysis. JAMA 274:975–980
3. Aw G, De P, Ps M, Kj S, Sm B (2011) Efficacy of quantified home-
based exercise and supervised exercise in patients with intermittent
claudication: a randomized controlled trial. Circulation 123:491–498
4. Aw G, Ps M, Wr F, Li K (2005) The effect of exercise intensity on the
response to exercise rehabilitation in patients with intermittent
claudication. J Vasc Surg 42:702–709
5. Barak S, Stopka Cb, Archer Martinez C, Carmeli E (2009) Benefits of
low-intensity pain-free treadmill exercise on functional capacity
of individuals presenting with intermittent claudication due to
peripheral arterial disease. Angiology 60:477–486
Peripheral Vascular Disease
▶Peripheral Arterial Disease
Peroxisome Proliferator–Activated Receptors
ROBERT RINGSEIS, KLAUS EDER
Justus-Liebig-University Giessen Interdisciplinary
Research Center (IFZ), Institute of Animal Nutrition
and Nutrition Physiology, Giessen, Germany
SynonymsNR1C1 for PPARa; NR1C2 for PPARb/d; NR1C3 for
PPARg
DefinitionPeroxisome proliferator–activated receptors (▶PPARs)
are ligand-activated transcription factors that belong to
the nuclear hormone receptor superfamily, in which
PPARs constitute group C in subfamily 1 [1]. There are
three different PPAR isotypes: PPARa (NR1C1), PPARb/d(NR1C2), and PPARg (NR1C3). PPARa was first
described as a receptor being activated by peroxisome
proliferators, which explains its name [2]. The PPARb/disotype was initially called PPARb when it was first iso-
lated from a Xenopus oocyte library. Because the mam-
malian PPARb protein sequence was not highly
homologous to the Xenopus PPARb protein sequences,
it was named PPARd when identified in the mouse. Sub-
sequent characterization of the PPARs in the chick and
comparison with murine and Xenopus PPARs revealed
that themammalian PPARd is the ortholog of the amphib-
ian PPARb, hence it was denoted PPARb/d. All three PPARisotypes share a high degree of structural homology, espe-
cially in the DNA-binding domain and ligand- and
cofactor-binding domain, but the different PPARs are
encoded by distinct genes with different chromosomal
locations. PPARg is the only PPAR isotype that is
expressed in two different full-length translated isoforms,
PPARg1 and PPARg2. However, several splice variants are
known for all PPAR isotypes, with the physiological roles
of these splice variants remaining to be demonstrated.
Basic MechanismsTranscriptional regulation by PPARs requires heterodi-
merization with the retinoid X receptor (▶RXR; NR2B)

Peroxisome Proliferator–Activated Receptors P 701
P
which is a member of the same receptor superfamily.
Formation of the PPAR/RXR heterodimer occurs in
response to binding of a ligand to the ligand-binding
domain (LBD) of the receptor leading to a conformational
change in the ligand-dependent activation function
which is a prerequisite for the binding of transcriptional
coactivators and the release of transcriptional corepres-
sors. The PPAR/RXR heterodimer is permissive because it
can stimulate gene transcription in response to only one
ligand binding, either 9-cis retinoic acid or a PPAR ligand,
but ligand binding to both receptors results in an
increased stimulation of gene transcription. The activated
PPAR/RXR heterodimer then binds to specific DNA
sequences, called peroxisome proliferator response ele-
ments (▶PPREs). The PPRE sequence is a DR-1
(direct repeat-1) type motif because it consists of two
direct repeats of the consensus hexanucleotide sequence
AGGTCA separated by one spacer nucleotide (consensus
PPRE: AGGTCAAAGGTCA). Functional PPREs are
typically found in the promoter region of target genes,
but recent studies showed that functional PPREs are also
present in intronic regions [3] and in the 50-untranslatedregion [4]. Upon binding of the PPAR/RXR heterodimer
to the PPREs in the regulatory region of PPAR target
genes, the transcription of these genes in stimulated.
Proteins encoded by PPAR target genes are involved in
many metabolic and regulatory pathways including lipid
and lipoprotein metabolism, glucose metabolism, insulin
signaling, thermogenesis, inflammatory pathways, cell
proliferation, and cellular differentiation.
PPARs can be activated by both endogenous and syn-
thetic ligands. Endogenous ligands of PPARs are fatty
acids, in particular long-chain, and their derivatives
such as prostaglandins and leukotrienes (leukotriene B4,
15Δ-deoxy-12,14-prostaglandin J2). The vitamin A
metabolite retinoic acid has also been shown to be
a ligand for ▶PPARb/d. The selectivity of PPARs for
different endogenous ligands is determined by various
factors including the structure of the LBD and the nuclear
ligand availability. The three-dimensional structure of the
LBD, which forms a very large Y-shaped, hydrophobic
cavity enabling the binding of a broad range of lipophilic
ligands, determines the shape complementarity between
the cavity, which is smallest for PPARb/d, and the ligand.
This explains why a small difference in the amino acid
sequence of the LBD has a significant effect on the ligand
selectivity. Since the PPARs are bound to the DNA, the
ligands are required to be transported to the nucleus. It has
been shown that fatty acid-binding proteins (FABPs) can
shuttle the ligands to the PPARs with different selectivity.
FABP5 shuttles ligands particularly to PPARb/d, whereas
FABP3 and FABP4 preferentially transfer ligands to
PPARa and PPARg, respectively.Synthetic ligands with high specificity for each of the
three PPAR isotypes include: WY-14,643 and the fibrate
class of lipid lowering drugs (clofibrate, fenofibrate,
bezafibrate, and gemfibrozil) for PPARa; the insulin-
sensitizing thiazolidinediones (rosiglitazone, pioglitazone,
troglitazone) for PPARg; and GW0742, GW501516,
L-165041 and the novel PPARb/d-targeting compound
MBX-8025 (formerly RWJ-800025) for PPARb/d. PPARb/d-specific compounds are not in clinical use yet, but the few
clinical trials conducted so far revealed beneficial effects on
plasma triacylglycerols, HDL and LDL concentrations, and
fasting glucose and insulin levels without inducing any
significant adverse reactions, like liver andmuscle responses.
Transcriptional activity of PPARs is also dependent on
cofactors (also called coregulators), which modify and
alter chromatin structure. The cofactors can act as either
coactivators or corepressors. There are also coactivator-
associated proteins which directly interact with
coactivators but not with the PPARs itself. The coactivator
proteins enhance transcriptional activity of PPARs
through their histone acetyl transferase or methyl trans-
ferase activities that remodel the chromatin structure.
Other coactivators stimulate gene transcription by creat-
ing multiprotein complexes that form bridges between the
PPARs and the basal transcriptional machinery. In con-
trast, corepressors possess or recruit histone deacetylases
or other enzyme activities which leads to a tight chromatin
structure thereby inhibiting gene transcription. So far
more than 200 cofactors of nuclear receptors including
the PPARs have been described. One of the best described
PPAR coactivators is the PPARg coactivator 1a(▶PGC1a), which binds to and activates all PPAR
isoforms. Interestingly, overexpression of PGC1a in skeletalmuscle was shown to cause similar effects onmusclemetab-
olism and function as overexpression of PPARb/d. A typical
PPAR corepressor is RIP140 playing also important roles in
regulating metabolic processes in skeletal muscle.
Exercise InterventionThe distribution pattern and expression levels of the
PPARs show great differences between tissues (Fig. 1). In
tissues with high rates of fatty acid oxidation like liver,
kidney, heart, and skeletal muscle PPARa is highly
expressed, whereas PPARg1 is poorly expressed in these
tissues. Both, PPARa and PPARg1 are found in cells of the
immune system and the vessel wall and in epithelial cells.
The adipocyte-specific PPARg2 isoform is exclusively
and highly expressed in adipose tissue. PPARb/d is ubiqui-
tously expressed and the predominant PPAR isotype in

PPARa PPARd PPARg
Liver Muscle Adipose tissue
Functions:
• Fatty acid catabolism
• Lipoprotein metabolism
• Gluconeogenesis
• Ketogenesis
Functions:
• Fatty acid uptake
• Fatty acid oxidation
• Fiber type distribution
• Mitochondria biogenesis
• Heat production
Functions:
• Adipocyte differentiation
• Lipid storage
Peroxisome Proliferator–Activated Receptors. Fig. 1 Main functions of the different PPAR isotypes
702 P Peroxisome Proliferator–Activated Receptors
skeletalmuscle. Exercise is well documented to influence the
expression of PPAR isotypes in skeletal muscle which is the
major organ of lipid and glucose catabolism in mammals.
Influence on Skeletal Muscle PPARb/dSeveral studies reported that both, short-term exercise and
endurance exercise increase skeletal muscle expression of
the most abundant PPAR isoform in skeletal muscle,
PPARb/d, of humans and rodents (reviewed by [5]). Mus-
cles with a high content of oxidative type I (slow-twitch)
fibers like soleus muscle exhibit a higher expression levels
of PPARb/d than muscles with more glycolytic type II
(fast-twitch) fibers like plantaris muscle. From these find-
ings but also from studies with transgenic mice with
targeted skeletal muscle overexpression of PPARb/d or
its target gene and coactivator PGC1a or reduced expres-
sion of the RIP140 corepressor, it could be shown that
PPARb/d activity plays a key role in regulating muscle
fiber types. Indeed, mice with a targeted mutation in
skeletal muscle PPARb/d have a lower type I fiber content.In addition, PPARb/d enhances expression of genes
involved in lipid oxidation in skeletal muscle including
fatty acid transporters and enzymes involved in fatty acid
b-oxidation. Moreover, PPARb/d increases mitochondria
numbers and biogenesis in skeletal muscle via
PGC1a-mediated pathways. Regarding these beneficial
effects of PPARb/d on fiber type distribution, mitochon-
dria content, and oxidative capacity of skeletal muscle it is
not surprising that mice with muscle-specific PPARb/doverexpression exhibit an increased endurance capacity,
enabling these so-called marathon mice to run twice as far
as their wild-type littermates.
Influence on Skeletal Muscle PPARaIn contrast to PPARb/d, marginal or no changes occur in
PPARa expression in skeletal muscle in response to acute
or long-term exercise training. Noteworthy, a significant
reduction in exercise capacity can be observed in PPARaknockout mice, without significant alterations in meta-
bolic capacity (i.e., fatty acid oxidation capacity)
of skeletal muscle, with the latter being explained
by a compensatory increase in PPARb/d expression
which has similar, partially overlapping functions as
PPARa.
Influence on Skeletal Muscle PPARgExpression of PPARg1, which is only poorly expressed in
skeletal muscle, has been found to be increased in soleus
and plantaris muscle of rats and in human quadriceps
muscle biopsies in response to exercise training. However,
in another study reductions in PPARg1 expression in
human quadriceps muscle biopsies following exercise
training were also reported indicating that the effect of
exercise intervention on skeletal muscle PPARg1 expres-
sion is inconsistent. However, due to the very low expres-
sion level of PPARg1 in skeletal muscle the physiological
role of alterations in skeletal muscle PPARg1 expression is
probably less important.
References1. Nuclear Receptors Nomenclature Committee (1999) A unified
nomenclature system for the nuclear receptor superfamily. Cell
97:161–163
2. Issemann I, Green S (1990) Activation of a member of the steroid
hormone receptor superfamily by peroxisome proliferators. Nature
347:645–650

Physical Activity P 703
3. Wen G, Ringseis R, Eder K (2010) Mouse OCTN2 is directly regu-
lated by peroxisome proliferator-activated receptor a (PPARa) viaa PPRE located in the first intron. Biochem Pharmacol 79:768–776
4. Gutgesell A,Wen G, Konig B, Koch A, Spielmann J, Stangl GI, Eder K,
Ringseis R (2009) Mouse carnitine-acylcarnitine translocase (CACT)
is transcriptionally regulated by PPARa and PPARd in liver cells.
Biochim Biophys Acta 1790:1206–1216
5. Ehrenborg E, Krook A (2009) Regulation of skeletal muscle physiol-
ogy and metabolism by peroxisome proliferator-activated receptor d.Pharmacol Rev 61:373–393
Perspiration
▶ Sweat
PGC1a
The PPARg coactivator 1a (PGC1a) is a transcriptional
co-activator of the PPARs which enhances transcriptional
activity of the PPAR/RXR heterodimer.
P
pH Regulation
pH regulation is the sum of processes involved in H+ (pH)
homeostasis. The basic function in pH regulation is to
remove H+ from the cell to counteract the tendency
toward H+ accumulation.
Phagocyte
▶Macrophage
Phagocytosis
Phagocytosis is the engulfment of extracellular material
among which bacteria, opsonised microbes and necrotic
and apoptotic cells. This material is eventually degraded in
the lysosomes. Macrophages are professional phagocytes.
Phenotype
A measured variable that is not genotype. Examples
include height, eye color, muscle size.
Phosphagen System
▶Anaerobic Metabolism
Phosphocreatine
▶PCr
Phospholipids
Are a class of complex organic molecule comprised of
a glycerol base with a phosphate moiety (polar head)
and two distinct fatty acids (nonpolar legs). Phospholipids
serve as a natural interface between aqueous environments
because of their ability to form membranes due to their
amphipathic structure and attraction between the nonpo-
lar legs maintaining a fluid alignment.
Phosphorylation
The process of adding a phosphate group (PO4) to a
protein. The addition of the phosphate is a common
means of activating or deactivating proteins. Kinases are
enzymes that catalyze the phosphorylation of proteins,
while phosphatases catalyze the dephosphorylation reaction.
Physical Activity
ROY J. SHEPHARD
University of Toronto, Toronto, ON, Canada
University of Toronto, Brackendale, BC, Canada
SynonymsBody movement; Muscular activity
DefinitionPhysical activity is a broad generic concept, encompassing
all forms of muscular activity that induce a significant
increase in the oxygen consumption of the skeletal muscles
[1]. It embraces a wide range of the components of normal
daily life, including sport (physical activity undertaken

704 P Physical Activity
individually or as a team that involves either a personal or
an external competitive challenge,), exercise (deliberate
bouts of physical activity undertaken with a view
to maintaining or improving personal health), training
(a regular program of physical activity undertaken with
a view to enhancing competitive performance or restoring
function following injury or illness), physically demand-
ing employment, active commuting (walking or cycling),
domestic work (activities around the home and garden,
including do-it-yourself projects and the care of
dependent relatives), dance (movement undertaken with
artistic and/or social goals), and active forms of recreation
(such as walking or hiking for pleasure).
CharacteristicsThe characteristics of physical activity are important in
understanding relationships to the prevention of disease.
Activity is usually described in terms of its type, intensity,
frequency, duration, and total volume.
Types of physical activity. The types of physical activity
recommended for the maintenance of health include
rhythmic movements, muscular work, and range of
motion activities. Rhythmic activity, if of moderate inten-
sity, is aerobic in type, and stimulates the individual’s
cardiorespiratory system.More vigorous rhythmic activity
that can be sustained for only a fraction of a minute relies
upon anaerobic energy supply; it may be useful to an
athlete, but is not usually recommended to enhance the
health of the average individual. Muscular activity may
involve the lifting and/or the lowering of weights (concen-
tric and eccentric contractions) or contraction of the mus-
cles without external movement (isometric exercise).
Range of motion exercises are designed to take the major
joints of the body through their normal range of
movement.
Intensity of physical activity. The intensity of ▶ aerobic
activity may be expressed absolutely, in terms of a rate of
energy expenditure (Watts), in similar units relative to the
individual’s body mass (Watts/kg) or relative to the indi-
vidual’s resting energy expenditure (METs, an alternative
approach, also intended to compensate for interindividual
differences of body mass), or as a percentage of the
individual’s maximal aerobic effort (percent of _VO2max).
The last mentioned index has the advantage of adjusting
intensity to account for the age-related decline in
a person’s maximal oxygen intake.
For muscular contractions, the intensity of effort may
be expressed in absolute units of muscle force (N), as force
relative to body mass (N/kg) or muscle mass (N/L), or as
a percentage of a maximal single effort (the percentage of
a 1-repetition maximum effort).
Frequency of physical activity. The frequency of physical
activity is usually summarized as the number of bouts
performed per week (e.g., five sessions of aerobic exercise
and two bouts of muscle-strengthening activity).
Duration of physical activity. The duration of aerobic
activity is usually stated as the number of minutes of
sustained rhythmic activity that a person undertakes per
session (e.g., 30 or 60 min of cycle ergometry). However,
there is some evidence that the physiological equivalent of
the usually recommended daily 30minute of brisk walking
can be accumulated, for instance, through three 10-min
bouts of walking. The detection of short-lasting bursts of
activity may be particularly important when assessing the
activity patterns of young children, since they usually have
little inclination to engage in themore prolonged activities
of their parents.
Muscular activity is commonly stated as the number of
repetitions of a given activity that are undertaken – for
instance, three bouts of a “set” of ten repetitions of
a particular task, with each contraction performed at
60% of the one repetition maximum.
Total volume of physical activity. The total volume or
amount of physical activity reflects the product of frequency,
duration and intensity, accumulated over a specified period
such as a typical week. It has importance for certain aspects
of health, particularly the control of obesity. The total
volume of activity is commonly expressed as gross MJ of
energy expenditure per week, but such units can be mislead-
ing, since a prolonged period of activity at a low intensity
includes a larger component of the individual’s resting
energy expenditure than a short period at a higher intensity;
the total volume of activity is better expressed as the net
increase of energy expenditure per week.
Clinical RelevanceAccurate techniques for the assessment of physical activity
and appropriate patterns of sampling allow health agen-
cies to recommend minimum levels of physical activity to
maintain health and prevent disease.
Methods of assessment. A person’s habitual physical
activity can be assessed by direct observation, interview,
questionnaires, or the use of various types of personal
monitor. It can also be inferred from measurement of an
individual’s level of physical fitness [2].
When seeking correlations with various aspects
of health, physical activity is commonly assessed by
questionnaires. Often, instruments that ask relatively few
questions provide more valid information than complex
and time-consuming forms. Correlations between scores
and health outcomes often provide useful epidemiological
information, but attempts to translate questionnaire

Physical Activity and Mortality Risk P 705
P
responses into absolute energy expenditures can be mis-
leading, since activity levels are sometimes exaggerated
two or threefold [3].
Of potential personal monitors, the most practical is
the latest type of uniaxial ▶ pedometer/accelerometer.
Such devices are sufficiently inexpensive that large num-
bers can be purchased for use in epidemiological surveys.
A memory device within the instrument allows the
observer to record the number of steps taken and their
intensity for periods as long as 60 days. Walking, the main
activity of much of the population, is measured relatively
accurately when the device is suspended from a waist belt,
but other activities such as cycling are poorly estimated.
Patterns of sampling. The minimum sampling time
needed to assess an individual’s habitual activity is longer
than is commonly believed [4]. Information is often
collected simply on 1 or 2 weekdays and weekend days,
but unfortunately many active pursuits are followed only
at specific times during the year. Participation in even the
commonest of daily activities such as walking is strongly
modified by meteorological factors such as environmental
temperature and rainfall [5]. In order to ensure that 90%
of the variance in step count is appropriately attributable to
between subject variance, 105 consecutive days of observa-
tion are needed in elderly men and 37 days in elderly
women. If data collection is stratified by day of the week
and by season, the necessary collection period drops to 16
and 12 days, respectively, and if observation days are dis-
tributed randomly across the year, the observation period
can be shortened further to 11 and 9 days, respectively.
Health recommendations. Various national and inter-
national bodies have attempted to specify the minimum
amount of physical activity needed to maintain specific
aspects of an individual’s health [6]. Conclusions
have been based mainly on epidemiological studies using
questionnaires, and as noted above, the absolute volumes
of physical activity estimated in this way are liable to
substantial error. Nevertheless, the evidence obtained to
date from pedometer/accelerometers generally supports
questionnaire-based recommendations [2].
The minimum amount of activity depends on health
objectives. Relatively small volumes of physical activity
appear to enhance mental health and the quality of
life, but larger weekly volumes are needed to maintain
cardiovascular, metabolic and bone health. A common
recommendation for the average adult is at least 30 min
of moderate intensity exercise performed on most days of
the week, supplemented by resistance exercise for the main
muscle groups and range of motion exercises for the
principal joints performed on at least 2 days per week [6].
However, some groups have warned that this minimum
may be insufficient to control obesity; this may demand
60 or even 90 min of exercise per day [7].
Cross-References▶AIDS, Exercise
References1. Bouchard C, Shephard RJ, Stephens T (1994) Physical activity, fitness
and health. Human Kinetics, Champaign
2. Shephard RJ, Aoyaji Y (2011) Motion sensors and the physical
activity needs of the elderly. Phys Ther Rev (in press)
3. Shephard RJ (2003) Limits to the measurement of habitual physical
activity by questionnaires. Br J Sports Med 37:197–206
4. Aoyagi Y, Shephard RJ (2009) Steps per day: the road to senior
health? Sports Med 39:423–438
5. Shephard RJ, Aoyagi Y (2009) Seasonal variations in physical activity
and implications for health. Eur J Appl Physiol 107:251–271
6. Warburton DER, Katzmarzyk PT, Rhodes RE, Shephard RJ
(2007) Evidence-informed physical activity guidelines for Canadian
adults. Appl Physiol Nutr Metab 32(Suppl 2E):S16–S68
7. World Health Organization. Obesity (1998) Preventing and managing
the global epidemic. Report of a WHO Consultation Geneva, Switzer-
land World Health Organisation
Physical Activity and MortalityRisk
PETER KOKKINOS
Cardiology Department, Veterans Affairs Medical Center,
Washington, DC, USA
George Washington University School of Medicine and
Health Sciences, Washington, DC, USA
SynonymsMET level; Mortality
DefinitionMortality risk is the risk of mortality over a given period
of time. This is expressed as an absolute risk. When
two or more groups are compared, the difference in mor-
tality risk rates between two groups is referred to as the
relative mortality risk. Physical activity describes
a physiologic state that requires a degree of muscular effort
and results in energy expenditure beyond resting
conditions.
CharacteristicsIt is well established that increased physical activity that
leads to a higher capacity to perform work results in
certain physiologic adaptations that encompass the

706 P Physical Activity and Mortality Risk
musculoskeletal, cardiovascular, and metabolic systems.
These adaptations have been associated with preventive
and therapeutic attributes. For example, strong evidence
supports that increased physical activity or exercise of
adequate volume prevents or attenuates the development
and progression of chronic diseases [1]. Adequate exercise
also modulates blood glucose and insulin levels in indi-
viduals with type 2 diabetes, blood lipids and lipoproteins,
lowers blood pressure in hypertensive individuals, and
improves cardiac function and structure [1].
Clinical RelevanceThe aforementioned exercise-related physiologic
adaptations have significant clinical implications in the
prevention and management of chronic diseases. In addi-
tion, a plethora of evidence now exists to support
unequivocally that a physically active lifestyle or struc-
tured exercises of adequate intensity, duration, and
volume is associated with a reduced risk for cardiovascular
and all-cause mortality in healthy and diseased
populations. The physical activity–mortality risk relation-
ship is graded and persists regardless of age, gender, race,
age, risk factors, or other co-morbidities [1, 2]. The reduc-
tion in mortality risk for each 1-MET increase in
▶ exercise capacity ranges between 10–25%, regardless of
gender, race, age, the presence of traditional risk factors, or
cardiovascular disease [1, 2].
Although the physical activity–mortality risk relation-
ship is well established, less clear is the exercise volume
(exercise threshold and plateau) and the independent
contribution of the activity components (intensity, dura-
tion, frequency), for the induction of these benefits. In this
regard, most data support that an age-related exercise
capacity threshold exists for a mortality risk reduction of
approximately 20–40% at the exercise capacity of 4–6
METs. Mortality risk continues to decline with increased
fitness to approximately 70%, reaching an exercise capac-
ity asymptote of approximately 10 METs [1–3]. The
recommended intensity for physical activity is in the
range of 3–6 METs and an overall energy expenditure of
at least 1,000 kcals/week, the equivalent of brisk walking
for roughly 30 min per day [1, 2]. It also appears that
exercise intensity and duration are inversely related to
mortality risk independent of overall exercise volume.
However, some evidence suggests that exercise intensity
has a more significant effect on the incidence of coronary
heart disease (CHD) than duration. Limited evidence also
suggests that the reduction in CHD risk achieved by par-
ticipation in resistance training is similar to that provided
by brisk walking, but was approximately half of that pro-
vided by running [1, 2].
▶ Physical Fitness and Mortality Risk in Special
Populations: The exercise-related reduction in mortality
risk has also been reported in older populations and
those with various co-morbidities. For example, the asso-
ciation between exercise capacity and mortality risk for
individuals >70 years of age was inverse and graded,
similar to younger individuals (Fig. 1). The mortality
risk for those with an exercise capacity >5 METs
(moderate to high-fit) was 45–60% lower when compared
to those with an exercise capacity of �4 METs among
elderly men [3]. The association and the degree of change
in mortality risk are similar to that observed in younger
populations [1–3].
Similarly, mortality rate was approximately 40%
and 60% lower, respectively, for individuals with type 2
diabetes mellitus who achieved 5.1–7.9 METs
(moderately-fit) and >8 METs (high-Fit), when com-
pared to those in the lowest-fit category (�5 METs).
Some evidence suggests that exercise capacity may have
a greater impact on Caucasian than African-American
men with type 2 DM. Each 1-MET increase in exercise
capacity yielded 14% and 19% lower risks for African
Americans and Caucasians, respectively. Similarly, the
risks were 34% and 46% lower for moderate and high-fit
versus low fit African Americans, respectively. For Cauca-
sians, the comparable reductions were 43% and 67%,
respectively [4].
In hypertensive individuals with an exercise capacity
of 5.1–7.0 METs the mortality rate was 34% lower com-
pared to those who achieved and exercise capacity of
�5METs (lowest-fit category) (Table 1). The risk declined
progressively with increased exercise capacity and reached
70% for those with an exercise capacity of >10 METs.
More importantly, when the presence of co-morbidities
is considered, the combination of low fitness and addi-
tional co-morbidities increased the risk by approximately
50% in individuals without co-morbidities. However, this
risk is eliminated for the next fitness category, with an
exercise capacity of 5.1–7 METs. The mortality risk reduc-
tion beyond the 7 MET level between hypertensive indi-
viduals with and without additional risk factors is similar.
These findings suggest that relatively moderate fitness
levels as indicated by an exercise capacity of 5.1–7 METs
eliminate any additional risk that is evident in the lowest
fitness category. Furthermore, the mortality risk in those
with an exercise capacity of more than 7 METs is approx-
imately 50–60% lower regardless of the presence or
absence of additional risk factors [5].
Reverse Causality: The lower mortality rates observed
in those with moderate and high exercise capacity may be
exaggerated by the relatively higher mortality rates among

0.92
0.68
0.53
0.45
0.37
Source: Modified from Kokkinos P., et al. Circulation 2010; 122: 790-97
0.55
0.92
71–92 yrsN=2,754
65–70 yrsn=2,560
0.54
4MET
4.1-5 MET
5.1-6 MET
6.1-8 MET
8.1-9 MET
>9 MET
0.5
0.4
1
0.8
0.6
0.4
0.2
Rel
ativ
e R
isk
Physical Activity and Mortality Risk. Fig. 1 Mortality risk for different age-groups according to exercise capacity (Source:
Modified from [3])
Physical Activity and Mortality Risk. Table 1 Adjusted mor-
tality risk according to fitness categories in Hypertensive indi-
viduals with and without additional risk factors (Source:
Modified from [5])
�5
MET
5.1–7
MET
7.1–10
MET
>10
MET
No additional risk
factors
1 0.66b 0.48a 0.33a
Additional risk
factors
1.47a 0.97a 0.56a 0.37a
aDifferent from the �5 MET category with no additional risk factors
(p < 0.007)bDifferent from the 5.1–7 MET category with additional risk factors
(p = 0.016)
Physical Activity and Mortality Risk P 707
P
clusters of individuals with subclinical chronic diseases
and low fitness resulting from the disease (reverse causal-
ity). Although such a possibility cannot be eliminated by
epidemiologic evidence, scientific scrutiny of the data can
provide evidence in support or against such probability. In
this regard, we examined the mortality risk of individuals
by systematically removing from the analyses individuals
with certain parameters suggestive of subclinical chronic
diseases and re-analyzed the data. We observed no sub-
stantial deviations from the mortality trends of the entire
group. We also examined the change in fitness status and
mortality risk in a subgroup of individuals with multiple
assessments of fitness over a follow-up period of 12 years.
Again, we found the lowest mortality rates in individuals
who were fit at both assessments and the highest mortality
in those who were unfit during both tests. Interestingly,
the mortality rate decreased for unfit individuals who
improved their fitness status by the second evaluation
and increased for individuals who were initially fit, but
became unfit at the second evaluation. These findings
strengthen the argument that the lower mortality rate in
fit individuals is the result of increased fitness, not spuri-
ous or artificially inflated by the higher mortality among
low fit individuals consequent to subclinical diseases [3].
Summary: Evidence from large epidemiologic studies
now supports unequivocally an inverse and graded asso-
ciation between physical activity and cardiovascular and
all-cause mortality in healthy and diseased populations.
Significantly lower mortality risk (approximately 20%) is
observed in individuals with a relatively modest exercise
capacity (4–6 METs), with a progressively decline to

708 P Physical Activity and Socioeconomic Status
approximately 70% at an exercise capacity asymptote of
approximately 10 METs. The adjusted reduction in mor-
tality risk for each 1-MET increase in exercise capacity
ranges between 10% and 25%.
References1. Kokkinos P (2010) Physical Activity and Cardiovascular Disease
Prevention. Jones and Bartlett Publishers, Sudbury, MA
2. Kokkinos P, Myers J (2010) Exercise and physical activity: clinical
outcomes and applications. Circulation 112:1637–1648
3. Kokkinos P, Myers J, Faselis C, Panagiotakos D, Doumas M, Pittaras A,
Manolis A, Kokkinos JP, Karasik P, Greenberg M, Papademetriou V,
Singh S, Fletcher R (2010) Exercise capacity andmortality in oldermen:
a 20-year follow-up study. Circulation 122:790–797
4. Kokkinos P, Myers J, Nylen E, Panagiotakos D, Manolis A, Pittaras A,
Blackman M, Jocob-Issac R, Faselis C, Abella J, Singh S (2009)
Exercise capacity and all-cause mortality in african american and
caucasian men with type 2 diabetes. Diabetes Care 32:623–628
5. Kokkinos P, Manolis A, Pittaras A, Doumas M, Giannelou A,
Panagiotakos DB, Faselis C, Narayan P, Singh S, Myers J (2009)
Exercise capacity and mortality in hypertensive men with and with-
out additional risk factors. Hypertension 53:494–499
Physical Activity andSocioeconomic Status
REBECCA E. LEE, ANGELA HO
Texas Obesity Research Center, Health & Human
Performance, University of Houston, Houston, TX, USA
SynonymsPosition in the social hierarchy; Social class
Definition▶Physical activity is defined as any bodily movement
produced by skeletal muscles that result in energy expen-
diture [1, 2]. It is recommended that children aged 6–17
perform 60 min each day of aerobic activity, 3 days per
week of muscle strengthening, and 3 days per week of bone
strengthening. Adults of 18 years and older should per-
form 150 min of moderate-intensity aerobic activity per
week with at least 2 days of muscle strengthening or
85 min of vigorous activity per week with at least 2 days
of muscle strengthening [1].
▶ Socioeconomic status (SES) is a method of group-
ing based on one’s economic position. Race or ethnicity,
gender, educational attainment, occupation, or disability
status can also affect SES [3]. Those of higher SES
typically have access to more resources and opportunities
enabling them to lead more comfortable lives.
CharacteristicsThere are several different kinds of physical activity that
may be performed. Aerobic activity, also called endurance
activity, is activity in which the body’s large muscles move
in a rhythmic manner for a sustained period of time that
causes improvements in cardiorespiratory fitness. Moder-
ate-intensity physical activity is working at 50–70% of
one’s maximum heart rate. Some activities include walk-
ing briskly, ballroom dancing, or doubles tennis. Muscle-
strengthening activity is physical activity that includes
exercise aimed at increasing skeletal muscle strength,
power, endurance, and mass. Vigorous-intensity physical
activity is working at 70–85% of one’s maximum heart
rate. Some vigorous activities include running, swimming
laps, or jumping rope [1].
Some subgroups of the population, such as ethnic
minorities, women, and those with disabilities, have higher
chances of being categorized as lower SES. Discrimination
toward these subgroups can result in inferior quality edu-
cation, skewed unemployment rates, wage inequalities, and
reduced opportunities that push these subgroups toward
this classification. Inferior education may lack adequate
training in a variety of physical activity skills reducing the
range of potential physical activity opportunities. As well,
lower income reduces the ability to afford equipment,
shoes, garments, supplies, or memberships necessary to
do some types of physical activity. As well, people from
lower SES tend to work longer hours or multiple jobs in
order to meet daily needs, reducing time available for
doing physical activity. People of lower SESmay experience
greater daily stress from a variety of sources including
discrimination that can increase distress and hinder phys-
ical activity [4].
Persons of lower SES also tend to reside in low SES
neighborhoods where housing is less costly, but these
neighborhoods often have problems related to safety, less
access to goods and services, and other physical character-
istics that may reduce quality of life and impede daily
physical activity. Even if high quality resources are avail-
able, negative perceptions associated with one’s neighbor-
hood and way of life act as a hindrance to physical activity
[3]. One study classified leisure-time physical activity rates
based on employment status before and after a 5–7 year
follow-up period. There was an increase in physical
activity among the upper classes (professionals, semi-
professionals) and a decrease among the lower classes
(routine non-manual employees, manual workers), illus-
trating the typical relationship between SES and physical
activity [5].
The▶ EcologicModel of Physical Activity (EMPA) [4]
classifies environmental factors related to SES and physical
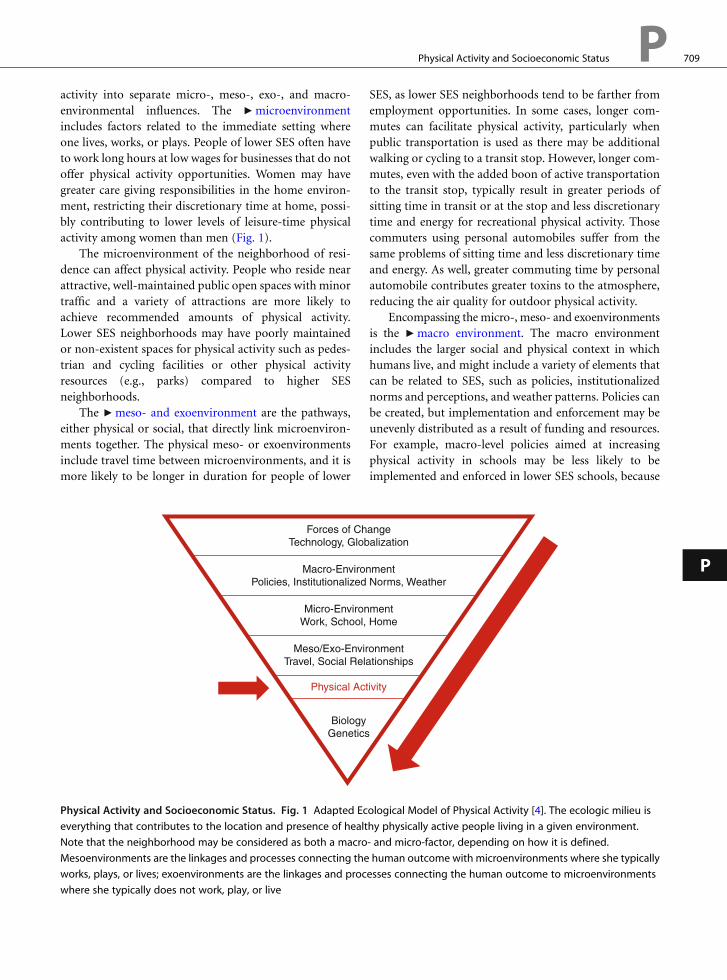
Physical Activity and Socioeconomic Status P 709
activity into separate micro-, meso-, exo-, and macro-
environmental influences. The ▶microenvironment
includes factors related to the immediate setting where
one lives, works, or plays. People of lower SES often have
to work long hours at low wages for businesses that do not
offer physical activity opportunities. Women may have
greater care giving responsibilities in the home environ-
ment, restricting their discretionary time at home, possi-
bly contributing to lower levels of leisure-time physical
activity among women than men (Fig. 1).
The microenvironment of the neighborhood of resi-
dence can affect physical activity. People who reside near
attractive, well-maintained public open spaces with minor
traffic and a variety of attractions are more likely to
achieve recommended amounts of physical activity.
Lower SES neighborhoods may have poorly maintained
or non-existent spaces for physical activity such as pedes-
trian and cycling facilities or other physical activity
resources (e.g., parks) compared to higher SES
neighborhoods.
The ▶meso- and exoenvironment are the pathways,
either physical or social, that directly link microenviron-
ments together. The physical meso- or exoenvironments
include travel time between microenvironments, and it is
more likely to be longer in duration for people of lower
Forces of ChTechnology, Glob
Macro-EnvironPolicies, Institutionalized
Micro-EnvironWork, School,
Meso/Exo-EnvirTravel, Social Rela
Physical Act
BiologyGenetics
Physical Activity and Socioeconomic Status. Fig. 1 Adapted Ec
everything that contributes to the location and presence of healt
Note that the neighborhood may be considered as both a macro
Mesoenvironments are the linkages and processes connecting the
works, plays, or lives; exoenvironments are the linkages and proc
where she typically does not work, play, or live
SES, as lower SES neighborhoods tend to be farther from
employment opportunities. In some cases, longer com-
mutes can facilitate physical activity, particularly when
public transportation is used as there may be additional
walking or cycling to a transit stop. However, longer com-
mutes, even with the added boon of active transportation
to the transit stop, typically result in greater periods of
sitting time in transit or at the stop and less discretionary
time and energy for recreational physical activity. Those
commuters using personal automobiles suffer from the
same problems of sitting time and less discretionary time
and energy. As well, greater commuting time by personal
automobile contributes greater toxins to the atmosphere,
reducing the air quality for outdoor physical activity.
Encompassing the micro-, meso- and exoenvironments
is the ▶macro environment. The macro environment
includes the larger social and physical context in which
humans live, and might include a variety of elements that
can be related to SES, such as policies, institutionalized
norms and perceptions, and weather patterns. Policies can
be created, but implementation and enforcement may be
unevenly distributed as a result of funding and resources.
For example, macro-level policies aimed at increasing
physical activity in schools may be less likely to be
implemented and enforced in lower SES schools, because
angealization
ment Norms, Weather
ment Home
onmenttionships
ivity
ological Model of Physical Activity [4]. The ecologic milieu is
hy physically active people living in a given environment.
- and micro-factor, depending on how it is defined.
human outcome with microenvironments where she typically
esses connecting the human outcome to microenvironments
P

710 P Physical Activity Dose
these schools may have fewer resources to meet the poli-
cies or not have the ability to hire trained physical activity
teachers [4].
Clinical RelevanceRegularly done physical activity helps to control weight,
strengthens muscles and bones, improves mental health
and mood, increases life span, improves ability to perform
daily activities and prevents falls, and reduces risk of
cardiovacular disease, type 2 diabetes mellitus, metabolic
syndrome and some cancers [1]. Despite these well publi-
cized and recognized health benefits, most people do not
achieve sufficient physical activity to meet even the most
minimal recommendations, resulting in direct and indi-
rect medical costs. According to the National Medical
Expenditure Survey, the direct medical costs associated
with physical inactivity among nondisabled persons aged
15 and up were estimated to be $330 per year [6].
Ethnic minorities, women in particular, have the low-
est rates of physical activity and the highest rates of obesity
and obesity-related health issues. Recommendations to
increase physical activity to improve health are simply
not sufficient. Statistics clearly demonstrate that factors
such as race or ethnicity, gender or ability contribute to the
level of SES that one will attain. SES contributes both
directly and indirectly to the ability to achieve physical
activity recommendations, by reducing resources and
opportunities. There are few programs available for
lower SES groups that seek to balance this inequality.
Opportunities to be healthy should be an equal right
shared by all. Physical activity has the capability of
improving health, but SES can act as a major inhibitor to
leading a physically active lifestyle and obtaining those
health benefits regardless of knowledge, education, or
skills [4].
References1. Centers for Disease Control and Prevention (CDC) (2010) Physical
activity for everyone. http://www.cdc.gov/physicalactivity/everyone/
health/index.html
2. Pate RR et al (1995) Physical activity and public health. A recom-
mendation from the centers for disease control and prevention and
the American college of sports medicine. J Am Med Assoc
273(5):402–407
3. Giles-Corti B, Donovan RJ (2002) Socioeconomic status differences
in recreational physical activity levels and real and perceived access to
a supportive physical environment. Prev Med 35(6):601–611
4. Spence JC, Lee RE (2003) Toward a comprehensive model of physical
activity. Psychol Sport Exerc 4(1):7–24
5. Seiluri T et al (2011) Changes in occupational class differences in
leisure-time physical activity: a follow-up study. Int J Behav Nutr
Phys Act 8:14
6. Macera CA, Hootman JM, Sniezek JE (2003) Major public health
benefits of physical activity. Arthritis Rheum 49(1):122–128
Physical Activity Dose
The intensity and/or volume of PA. Thus, an individual
who jogs at 6 mph for 1 h would obtain a larger dose of PA
than someone whowalks 6miles in 2 h. And someone who
walks for 1 h/day for 6 days/week would obtain twice the
PA dose of someone who walks for 1 h/day, 3 times/week.
Physical Activity EnergyExpenditure
The energy expenditure related to physical activity.
Physical Exercise Training
▶Coronary Heart Disease
Physical Fitness
Is defined by The Centers for Disease Control and Preven-
tion (CDC) and the American College of Sports Medicine
as “a set of physical attributes that people have or achieve
that relates to the ability to perform physical activity.” The
degree of physical fitness can be improved by an appro-
priate increase in daily physical activity related to one’s
occupation, leisure time activity, or by engaging in
a structured exercise program. Although fitness is
influenced by age, in general a peak MET level of <6
METs for middle-aged or older individuals is considered
low-fitness and ≥10 MET high-fitness.
Physical Training
▶Hypertension, Training
▶ Endurance Training
Physical-Cognitive Activity
The physical exercise plus the processing of information that
is novel and much higher than normally processed by con-
trol animals that is induced by environmental enrichment.

Plyometric Training P 711
Physico-chemical
The term is a combination of physical and chemical, and
recognizes the physical as well as chemical interactions
that occurs amongst molecules in an aqueous solution.
With respect to acid-base balance, it is a combination of
physical interactions and chemical interactions that deter-
mines the [H+] of a physiological solution.
Physiologic Adaptation
The functional or morphological changes that occur in
physiological function or structures in response to
a repeated stimulus.
P
Physiological CardiacHypertrophy
Balanced growth of the heart in response to physiological
stress stimuli such as pregnancy and strenuous physical
activity or exercise training, in which case the condition is
also referred to as the athlete’s heart. The condition is
associated with sustained or improved contractile pump
function of the myocardium. The myocardium grows
mainly due to longitudinal and transverse enlargement
of existing ventricular muscle cells (cardiomyocytes) due
to increased protein synthesis and sarcomere increase of
the cell; however, myocardial growth due to contributing
hyperplasia caused by generation of new mature ventric-
ular cardiomyocytes or proliferation of existing cells can-
not be excluded, especially due to recent reports of the
existence of a pool of resident cardiac progenitor cells
within the myocardium as well as at least limited mitotic
capacity.
Cross-References▶Athlete’s Heart
▶Cardiac Hypertrophy, Physiological
PIgR (Polymeric-Ig Receptor)
A receptor molecule that specifically binds dimeric secre-
tory IgA and transports it across the mucosal epithelial
cells.
Plasma Membrane
The lipid bilayer with membrane proteins that surrounds/
envelops a cell separating it from the extracellular
environment.
Plyometric Exercise
▶ Eccentric Muscle Damage
Plyometric Training
GORAN MARKOVIC
School of Kinesiology, University of Zagreb,
Zagreb, Croatia
SynonymsReactive training; Stretch-shortening cycle training
Definition▶Plyometric training refers to performance of ▶ stretch-
shortening cycle (SSC) movements that involve a high
intensity concentric or shortening muscle action immedi-
ately after a rapid and powerful eccentric or lengthening
muscle action. The SSC is a natural type of muscle func-
tion in which muscle is stretched immediately before
being contracted. The SSC enhances the ability of the
neural and musculotendinous systems to produce maxi-
mal force in the shortest amount of time, prompting the
use of plyometric exercise as a bridge between strength and
speed [1, 2]. For the lower body, plyometric training
includes performance of various types of body weight
jumping-type exercise, like drop jumps, countermovement
jumps, alternate-leg bounding, hopping, and other SSC
jumping exercises. For the trunk and upper body, plyomet-
ric training includes performance of various types of
throwing exercises, mainly using medicine balls.
CharacteristicsIn general, the SSC or plyometric exercises have been
classified as either slow (ground contact time >0.25 s) or
fast (ground contact time <0.25 s) [3]. This is best illus-
trated in vertical jumping. Figure 1 shows three different
types of vertical jumps: concentric-only jump (A; squat
jump), slow SSC jump (B; countermovement jump), and
fast SSC jump (C; bounce drop jump). Note that slow SSC

Plyometric Training. Fig. 1 Example of explosive concentric muscle action (a; squat jump), slow stretch-shortening cyclemuscle
action (b; countermovement jump), and fast stretch-shortening cycle muscle action (c; depth jump)
712 P Plyometric Training
movements are characterized by greater angular joint dis-
placements and lower rates of force development, while
the opposite is true for fast SSC movements.
The SSC movements consist of at least three (and in
many cases, four) phases:
1. Loading or eccentric phase (e.g., lowering of the body’s
center of mass during countermovement jump)
2. Transition or coupling phase (the transition between
the loading and unloading phase)
3. Unloading or concentric phase (e.g., raising the body’s
center of mass during countermovement jump)
In the loading phase of a SSC or plyometric exercise
the muscle-tendon units of the prime movers and syner-
gists are stretched as a result of kinetic energy or loading
applied to the joint(s) [1]. Thus, the loading phase begins
when the active muscle-tendon units begin to lengthen
and perform negative work. Stretch of active muscle-
tendon units during the loading phase elicits several
mechanisms associated with the SSC: (1) greater time
available for force development; (2) storage and
reutilization of elastic energy; (3) potentiation of the con-
tractile machinery; (4) interaction between the series elas-
tic component and the contractile machinery; and (5) the
contribution of reflexes [4]. Note that the contribution of
a particular mechanism to force and work augmentation
during SSC movement is task specific.
The transition or coupling phase is essentially a period
of (quasi) isometric action, when the muscle-tendon units
of the prime movers and synergists do not change their
length (although this could be both muscle- and task-
specific). In other words, this is a brief period of transition
from eccentric to concentricmuscle action. If the transition
phase is not continuous, the activity will no longer be
considered as plyometric because the benefits of SSC (par-
ticularly those related to storage and reutilization of elastic
energy and reflex potentiation) will be lost [1].
Finally, the unloading phase of a plyometric exercise
occurs immediately after the transition phase and involves
shortening of the muscle-tendon units of the prime
movers and synergists. For SSC jumps, the unloading
phase begins at the start of upward movement and ends
when ground contact ceases [1].
Notably, in many SSC or plyometric exercises an-
additional (fourth) phase can be recognized – the pre-
activation phase. This phase includes a well timed
pre-activation of relevant muscle(s), which plays a very
important role in stiffness regulation during the loading or
eccentric phase. For example, it has been suggested that the
co-contraction between the plantarflexor and dorsiflexor
muscles and the knee extensor and knee flexor muscles
increases joint stiffness throughout the whole leg in prepa-
ration for ground impact, thereby allowing greater amount
of elastic energy to be stored within the tendinous tissue.

Plyometric Training P 713
P
Overall, we may conclude that SSC action represents
a unique movement quality that has relevance not only in
sport, but also in everyday life [3]. Its major advantages
over other three types of muscle actions are: (1) enhance-
ment of force and power output of skeletal muscles,
and (2) reduction of the metabolic cost of movement
[2]. Consequently, many coaches and physical condition-
ing specialists look to incorporate training drills that can
enhance the person’s use of the SSC. This is best achieved
by using plyometric drills.
Aside from enhancing the person’s use of the SSC,
plyometric training, either alone or in combination with
other typical trainingmodalities, elicits numerous positive
changes in the neural andmusculoskeletal systems, muscle
function, and athletic performance of healthy individuals.
Specifically, recent literature review has shown that long-
term plyometric jump training (i.e., 3–5 sessions per week
for 5–12 months) represents an effective training method
for enhancing bone mass in prepubertal/early pubertal
children, young women, and premenopausal women [2].
Short-term plyometric training also improves the strength
and power in healthy individuals. These adaptive changes
in neuromuscular function are likely the result of
(1) increased neural drive to the agonist muscles,
(2) changes in the muscle activation strategies (i.e.,
improved intermuscular coordination), (3) changes in
the mechanical characteristics of the muscle-tendon com-
plex of plantar flexors, (4) changes in muscle size and/or
architecture, and (5) changes in single-fiber mechanics
[2]. Literature review also showed that plyometric train-
ing, either alone or in combination with other training
modalities, has the potential (1) to enhance a wide range
of athletic performance (i.e., jumping, sprinting, agility,
and endurance performance) in children and young adults
of both sexes, and (2) to reduce the risk of lower-extremity
injuries in female athletes [2].
Collectively, we may recommend the use of plyometric
training as a safe and effective training modality for
improving muscle function and functional performance
of healthy individuals. For performance enhancement and
injury prevention in competitive sports, we recommend
an implementation of plyometric training into a well
designed, sport-specific physical conditioning program.
Note, however, that maximizing plyometric program
effectiveness and preventing injuries depends on the
logical progression of exercise intensity. Thus, developing
a progressive plyometric training system requires a basic
knowledge of the factors that determine plyometric inten-
sity. These include: the speed and amplitude of movement,
the height of the jump, the number of points of contact
(e.g., single- or double-leg jump), and individuals weight.
Measurement/DiagnosticsAs already mentioned, SSC of muscle function represents
a unique humanmotor quality. This is particularly evident
for fast SSC action. Specifically, experimental data indicate
that slow and fast SSC movement performance represent
distinctive motor qualities, at least when it comes to
jumping movements [3]. Thus, there is a need to assess
the efficacy of both slow and fast SSC. The efficacy of the
slow SSC in lower extremities is usually assessed through
pre-stretch augmentation during vertical jumping and
expressed in either centimeters (countermovement jump
height – squat jump height), or in percentages
([countermovement jump height – squat jump height]/
squat jump height 100). Usually, this pre-stretch augmen-
tation amounts 2–4 cm, or, in percentages, 5–10%.
The efficacy of the fast SSC, also known as “▶ reactive
strength,” is usually assessed by dividing the depth jump
height with ground contact time, or by dividing the depth
jump flight time with ground contact time [2]. In the first
case, the “reactive strength index” is expressed in cm/s,
while in the second case a dimensionless “reactive strength
index” is obtained. “Reactive strength index” is usually
tested over the following drop heights: 30, 45, 60, and
75 cm. This allows coaches and specialists to determine
the fast SSC ability of athletes/clients, as well as to define
the optimal dropping height for performing various fast
SSC drills. When the “reactive strength index” is
maintained or improves in depth jump dropping height,
and ground contact time is less than 0.25 s, it is assumed
that an individual’s reactive strength capabilities are suffi-
cient at that height of depth jump [5]. The dropping
height at which the “reactive strength index” decreases,
or ground contact time goes above 0.25 s, indicates
a height, which may represent a heightened injury risk
for that individual or provide a suboptimal training
stimulus [5].
Figure 2 illustrates the results of testing the reactive
strength (depth jump flight time/ground contact time) of
an experienced male athlete and an untrained individual
of similar age. Note that in the case of the well-trained
athlete there is an increase in reactive strength index with
an increase of drop jump height up to 60 cm. In contrast,
reactive strength capability of the untrained individual is
compromised already at relatively low stretch loads (i.e., at
dropping height of 30 cm). This graphical example indi-
cates clear differences in the efficacy of fast SSC between
well-trained and untrained individuals.
Once the efficacy of both slow and fast SSC has been
established (together with other relevant motor qualities),
coaches and specialists can decide whether the implemen-
tation of plyometrics into an overall training program is

Plyometric Training. Fig. 2 Graphical presentation of the results of testing the efficacy of fast SSC in one trained and one
untrained individual. Both individuals performed maximum effort depth jumps from five different dropping heights. Flight times
and ground contact times were recorded for each depth jump bymeans of a contact mat. Reactive strength index (y-axis) = depth
jump flight time/depth jump ground contact time
714 P Poincare Plot
warranted and, if so, which type of plyometric exercises
should be prescribed.
References1. Chmielewski TL,MyerGD,KauffmanD, Tillman SM(2006) Plyomet-
ric exercise in the rehabilitation of athletes: physiological responses
and clinical application. J Orthop Sports Phys Ther 36(5):308–319
2. Markovic G, Mikulic P (2010) Neuro-musculoskeletal and perfor-
mance adaptations to lower-extremity plyometric training: a review.
Sports Med 40(10):859–895
3. Schmidtbleicher D (1992) Training for power events. In: Komi PV
(ed) Strength and power in sport. Blackwell, Oxford, UK, pp 169–179
4. van Ingen Schenau GJ, Bobbert ME, de Haan A (1997) Does elastic
energy enhance work and efficiency in the stretch-shortening cycle.
J Appl Biomech 13:389–415
5. Flanagan EP, Comyns TM (2008) The use o contact time and
reactive strength index to optimize fast stretch-shortening cycle
training. Strength Cond J 30(5):32–38
Poincare Plot
A non-linear graphical technique used to quantify self-
similarity in periodic processes such as the beat-to-beat
variability in a continuous series of normal R-R intervals
(i.e., beats that originate from the atrial pacemaker cells).
In this example, the R-R interval (n) is plotted on the
X-axis against the preceding R-R interval (n + 1) on the
Y-axis. The resulting graph displays the variability by
the scatter of data points, the greater the variability the
larger the scatter in the plotted data points.
Polymorphism
A point or region in the DNA sequence at which variation
between members of a species is likely to occur.
Polysomnography
The gold standard of sleep assessment, inwhich continuous
and simultaneous recording of brain (electroencephalo-
graphic), eye (electroencephalographic), muscle
(submentalis electromyographic), and heart (electrocardio-
graphic) activity are collected during the overnight period;
additional measurement of respiratory effort, airflow, oxy-
gen saturation, and limb movement are performed during
diagnostic studies; commonly abbreviated PSG.

Postactivation Potentiation P 715
POMC-Proopiomelanocortin
The POMC system is activated under the conditions
of physical exercise, which results in the release of its
derivative ACTH and other POMC fragments containing
b-endorphin immunoreactive material (IRM) from the
pituitary gland into the blood.
Position in the Social Hierarchy
▶Physical Activity and Socioeconomic Status
Position Stand
“Position Stands are official statements of the American
College of Sports Medicine (ACSM) on topics related to
sports medicine and exercise science. Position Stands are
based on solid research and scientific data and serve as
a valued resource for professional organizations and govern-
mental agencies.” (Quoted directly from: http://www.acsm.
org/Content/NavigationMenu/News/Pronouncements_
Statements/PositionStands/Position_Stands1.htm).
P
Postactivation PotentiationBRIAN R. MACINTOSH
University of Calgary, Calgary, AL, Canada
SynonymsActivity-dependent potentiation; Complex training;
Posttetanic potentiation; Staircase.
DefinitionPostactivation potentiation (PAP) is an enhanced contrac-
tile response, for a given stimulation, that can be attrib-
uted to prior voluntary muscle activation. In its simplest
form, PAP is an enhanced twitch contraction following
a maximal or a submaximal voluntary activation (see
Fig. 1). The twitch would have to be obtained with a stim-
ulus strong enough to activate all motor units to allow full
quantification of the enhancement of contractile response.
Only motor units that were activated during the voluntary
contraction will undergo potentiation, and fast-twitch
units are enhanced to a greater extent than slow-twitch
motor units. Potentiation is more evident when measured
at short sarcomere lengths, regardless of the length at
which the voluntary contraction occurred. PAP can also
be detected with very brief tetanic contractions and longer
duration tetanic contractions when activation to test it is
applied at low frequencies. Maximal voluntary force is not
enhanced, and neither is sustained high frequency stimu-
lated response. It is important to recognize that prior
voluntary activation can also elicit muscle fatigue, so
there is an optimal level (combination of intensity and
duration) of voluntary muscle activation that will create
the greatest enhancement of subsequent contractile
response. There has been considerable interest lately in
whether or not PAP can be obtained during warm-up,
and whether or not it can contribute to improved physical
performance, particularly performance requiring very
brief maximal effort contractions.
Postactivation potentiation, or PAP as it is commonly
referred to is a term that is sneaking into the sport training
and competition jargon. There is a strong belief among
athletes and coaches that PAP can contribute to enhanced
performance and improved training. However, there is
confusion over what constitutes PAP. In many cases, the
reported improvement might be a consequence of some
other mechanism, independent of PAP. In order to be
certain that PAP is contributing to an improved perfor-
mance, other potential factors need to be excluded, and
the presence of PAP needs to be confirmed. At the current
time, we have little or no evidence that PAP actually can
enhance performance. It will become clear why this is the
case, once we critically evaluate the research that purports
to involve PAP. The first step in this direction is to under-
stand the mechanism of PAP.
Basic MechanismsIt is generally accepted that PAPoccurs as a consequence of
phosphorylation of the regulatory light chains of myosin
[4]. On each activation of a skeletal muscle, [Ca2+]
increases in the muscle cells of each activated motor
unit. In addition to activating contraction, by binding to
troponin, this Ca2+ binds to calmodulin and the Ca2+-
calmodulin complex activates myosin light chain kinase
(MLCK), an enzyme that phosphorylates the regulatory
light chains of myosin. Phosphorylation of the regulatory
light chains increases the mobility of the myosin heads,
and increases the probability of the myosin head binding
to actin, during muscle activation. The phosphorylation
of myosin persists past the time of muscle relaxation, so
the next contraction, if it occurs soon enough, will have
a higher probability of myosin binding to actin.

0
20
40
60
80
100
−5.0 0.0 5.0 10.0 15.0 20.0 25.0 30.0
Mom
ent (
% o
f Max
imum
)
Time (seconds)
0
2
4
6
8
10
12
14
16
18
20
50 150 250 350 450 550 650
Mom
ent (
% o
f Max
imum
Vol
unta
ry)
Time (seconds)
b
a
Postactivation Potentiation. Fig. 1 Amaximal effort voluntary contraction is shownwith a twitch contraction immediately prior
to and following the voluntary contraction. The amplitude of the twitch contraction is augmented by the intervening voluntary
contraction. Themagnitude of enhancement is dependent on the effort and the duration of the voluntary contraction. During the
ensuing recovery period, the enhancement dissipates. By 5–6 min after the voluntary contraction, the twitch will return to the
baseline value
716 P Postactivation Potentiation
This higher probability of myosin binding to actin permits
a faster rate of force development and more force at
a given submaximal [Ca2+] (improved Ca2+ sensitivity).
Dephosphorylation of the regulatory light chains and
hence dissipation of the enhanced contractile response
associated with PAP is achieved by another enzyme, light
chain phosphatase. The decrease in twitch amplitude illus-
trated in Fig. 1 can be attributed to a decline in RLC
phosphorylation because the activity of the phosphatase
is greater than that of myosin light chain kinase once the
conditioning contraction is discontinued. In the absence
of activation, phosphorylation is typically returned to the
resting level by about 4–6 min after the voluntary contrac-
tion that induced the phosphorylation.
Some excellent research has been done to quantify the
type of voluntary activation needed to achieve PAP, and
the magnitude and time-course of enhancement typically
seen. We know that fast-twitch motor units are more
sensitive to prior activation than are slow-twitch motor
units. However, PAP has been observed after submaximal

0
0.2
0.4
0.6
0.8
1
1.2
0 100 200 300 400 500 600
Act
ive
For
ce (
rela
tive
to m
axim
um)
Time (ms)
Control
Potentiated
Postactivation Potentiation. Fig. 2 Two brief contractions
are shown, along with the maximal force that would be
achieved if these contractions were continued longer. The
brief gray contraction is not potentiated, and the black one is
potentiated. The rate of rise is greater for the potentiated
contraction, so it reaches a higher peak force at about the
same time as the peak of the weaker (unpotentiated)
contraction. Both contractions would have the same maximal
force if they were continued long enough to reach maximum
Postactivation Potentiation P 717
P
contractions at just 50% of maximal effort. This is prob-
ably because 50% of maximal effort actually involves the
majority of motor units, but they are submaximally acti-
vated. Further increase in voluntary force is obtained
primarily by “rate coding,” which is increasing the fre-
quency of firing of individual motor units. The greatest
magnitude of enhancement attributable to PAP occurs
after maximal isometric contraction lasting 10 s. Longer
activation will result in a higher level of▶ regulatory light
chain phosphorylation, but less apparent potentiation, due
to a greater impact of fatigue. Fatigue and PAP are
the opposing consequences of prior activation [6],
and the net result can be increased or decreased active
force, depending on the balance of these two opposing
influences.
It has been suggested that PAP could be achieved
during warm-up, and could contribute to enhanced phys-
ical performance in subsequent maximal effort trials [7].
Similarly, complex training involves maximal effort
weight-lifting contractions, which are thought to enhance
subsequent plyometric contractions. The theoretical basis
for this enhanced performance relates to the fact that PAP
is associated with an increased maximal rate of force
development, and that in a very brief maximal contractile
effort, the ability to achieve a higher rate of force devel-
opment would translate to improved performance. This
concept is illustrated in Fig. 2. It has been demonstrated
that this theory is feasible [1], peak rate of force develop-
ment is increased for brief maximal effort voluntary con-
tractions, but the translation to an actual competitive
situation is somewhat clouded. In particular, there have
been very few studies that have considered whether or not
PAP can be achieved with dynamic contractions, like those
typically performed in a warm-up. However, there are
several animal studies that demonstrate that when light
chains are phosphorylated, brief dynamic contractions are
enhanced. These observations are encouraging.
Exercise InterventionThe relevance of PAP to physical exercise is twofold: PAP
should counteract low-frequency fatigue and there is the
potential that PAP can enhance maximal effort dynamic
contractions. Low-frequency fatigue is a long-term nega-
tive consequence of previous exercise, and results in
diminished contractile response when motor unit activa-
tion is at low frequencies. Considering that PAP enhances
low-frequency contractions, there is a direct counterbal-
ance to these properties: fatigue and PAP. However, it is
very difficult to separate fatigue and PAP, because they
often exist at the same time [6]. In fact, the conditioning
contraction that elicits PAP will also elicit fatigue. These
two properties coexist, with different mechanisms that
have opposing effects.
The functional implication of PAP that has received
more attention is the notion that PAP can enhance brief
maximal effort dynamic contractions. This contribution
was proposed by Sale, in 2002. There has been a flurry of
research concerned with warm-up that has putatively
demonstrated that prior activation results in improved
performance, and these studies claim that the mechanism
of this enhancement is PAP. However, few of these research
studies have confirmed the presence of PAP when the
improved performance was accomplished. Most studies
have not included stimulated contractions to show
increased force for a given stimulation. Most of the
improved performances could be attributed to other fac-
tors associated with warm-up: improved motor coordina-
tion, highermuscle temperature, etc. In fact, inmost cases,
the criterion performance was assessed at a time when
light chain phosphorylation would have diminished to
a level consistent with that expected prior to the warm-
up. PAP could not have been the cause of the improved
performance.
Until recently [5], direct attempts to demonstrate that
PAP can enhance performance have failed. Gossen and
Sale [3] used a voluntary 10 s maximal isometric

718 P Postexercise Hypotension
contraction to elicit PAP, and assessed performance 1 min
later, a time when PAP was known to be present. Perfor-
mance of maximal effort dynamic knee extension was not
enhanced. It was concluded that fatigue dominated over
potentiation during the maximal effort contraction at that
time.
Although Chiu has stated that there is evidence that
PAP should persist for 5–20 min [2], the references given
in support of this statement are not convincing. Two of the
three references given do not measure PAP or light chain
phosphorylation, and the other one only measures these
up to 2 min after the brief maximal effort voluntary
contraction that elicited PAP. Furthermore, in that article,
PAP amounted to just 12% increase in twitch force, when
measured 20 s after the maximal dynamic voluntary con-
traction that was intended to elicit PAP.
Further critical review of the article by Chiu [2] dem-
onstrates why we still do not know if PAP can enhance
physical performance. The general design used by Chiu
and colleagues is actually quite strong. They allowed the
subjects two practice sessions to become familiar with the
testing protocol. This is an important feature of any warm-
up research. They compared their “potentiating” warm-up
with a control warm-up that they assumed would not
potentiate. Although not specified, they may have actually
randomized the order of testing: control versus experimen-
tal, another important feature of good warm-up research.
However, despite the strengths of their design, there are
three reasons why their results are not very helpful in
addressing the question: does PAP contribute to enhanced
performance? (1) They did not measure PAP. (2) They
measured performance at 5 and 18.5 min after the warm-
up, times when regulatory light chain phosphorylation
should have returned to the baseline. (3) Their control
condition included exercises that might have elicited PAP.
Further problems are evident in their analysis, where the
result is a comparison between athletes and recreational
subjects, not between control and experimental conditions.
Although Chiu et al. [2] speak of PAP, they present no
evidence that performance enhancements can be attributed
to PAP. The study by Chiu et al is very valuable, in that it is
an appropriate design, and it does show that the warm-up
with high-intensity effort is better for athletes than for the
recreational subjects. However, it does not address the issue
of whether or not PAP, achieved during warm-up, can
contribute to enhanced performance.
The theory is still viable. It seems quite logical that
PAP can result in an enhanced performance of high-
intensity exercise. However, to prove this, the test must
demonstrate that PAP is actually present at the time that
the performance is enhanced. Other contributing factors
must be ruled out. We will have to wait for better research
to demonstrate this potentially valuable aspect of warm-
up for competitive performance.
Cross-References▶Muscle Contraction
References1. Beaudry S, Duchateau J (2007) Postactivation potentiation in human
muscle: effect on the rate of torque development in tetanic and
voluntary isometric contractions. J Appl Physiol 102:1394–1401
2. Chiu LZ, Fry AC, Weiss LW, Schilling BK, Brown L, Smith SL (2003)
Postactivation potentiation response in athletic and recreationally
trained individuals. J Strength Conditioning Res 17:671–677
3. Gossen ER, Sale DR (2000) The effect of postactivation potentiation on
dynamic knee extension performance. Eur J Appl Physiol 83:524–530
4. Grange RW, Vandenboom R, Houston ME (1993) Physiological sig-
nificance of myosin phosphorylation in skeletal muscle. Can J Appl
Physiol 18:229–242
5. Mitchell CJ, Sale DR (2011) Enhancement of jump performance after
a 5-RM squat is associated with postactivation potentiation. Eur J
Appl Physiol 111:1957–1963
6. MacIntosh BR, Rassier DE (2002)What is fatigue? Can J Appl Physiol
27:42–55
7. Sale DR (2002) Postactivation potentiation: role in human perfor-
mance. Exercise Sport Sci Rev 30:138–143
Postexercise Hypotension
A change in blood pressure below resting levels following
an exercise bout that persists for 22 h after the exercise
session.
Post-Poliomyelitis Syndrome
▶Postpolio Syndrome
Postpolio Syndrome
FRANS NOLLET
Department of Rehabilitation, Academic Medical Centre,
University of Amsterdam, Amsterdam, AZ,
The Netherlands
SynonymsPost-poliomyelitis syndrome

Postpolio Syndrome P 719
P
Definition▶Postpolio syndrome (PPS) is the late decline in muscle
function that occurs after many years of stability following
the recovery from acute paralytic poliomyelitis. The
criteria [1] are as follows:
1. A confirmed history of acute paralytic poliomyelitis
characterized by an acute illness with fever and
a usually asymmetrically distributed, flaccid paresis
of a varying number of muscle groups. Evidence of
motor neuron loss on neurological examination with
signs of residual weakness, atrophy, loss of tendon
reflexes, and intact sensation. Signs of denervation or
reinnervation on electromyography.
2. A period of partial to fairly complete neurological
recovery after the acute phase followed by neurological
and functional stability for at least 15 years.
3. New or increased muscle weakness or abnormal mus-
cle fatigability (decreased endurance), with or without
generalized ▶ fatigue, muscle atrophy, or muscle and
joint pain.
4. The onset of the new symptoms is usually gradual and
symptoms should persist for at least 1 year.
5. No other medical diagnosis to explain the symptoms.
The prevalence of PPS among polio survivors is esti-
mated at 40–60%. Risk factors for PPS aremore severe initial
polio paresis, better recovery from the ▶ acute polio, more
severe residual impairments, the contraction of acute
polio at older age, the number of years elapsed since
acute polio, increasing age, and female gender. Symptoms
of PPS may be aggravated by comorbidities, especially
degenerative disorders of the locomotory system.
Pathogenic MechanismsAcute paralytic polio occurs in 0.1–2% of polio virus
infections when the polio virus invades the central nervous
system and destructs themotor neurons in the spinal cord,
causing acute flaccid paresis. After the paralytic phase,
muscle function recovers partial to fairly complete due
to extensive reinnervation of denervated muscle fibers
through collateral sprouting of axons frommotor neurons
that survived the acute phase and regained their function.
Motor units may increase five to eight times in size.
Strength furthermore improves because of muscle fiber
hypertrophy and fiber areas may increase up to twice the
normal size. It is assumed that muscle fiber hypertrophy
develops in response to the relatively high loads on paretic
muscles in performing daily life activities. Studies have
shown a predominance of type I muscle fibers in leg
muscles, which may express an adaptation to increased
load. After the recovery phase, the severity and extent of
residual paresis, with large intra- and interindividual var-
iation, remains stable for decades.
The cause of PPS is unknown. The leading hypothesis
is that excessive metabolic stress on the remaining motor
neurons over many years eventually causes premature
degeneration of the nerve terminals that were newly
formed through reinnervation. Based on findings of raised
concentrations of cytokines in the cerebrospinal fluid, it
has been suggested that an inflammatory process might
underlie PPS [2].
The role of aging seems limited since most PPS
patients develop new symptoms in their 40s, an age
range in which normally a physiological loss of motor
neurons is not yet supposed to occur. In a longitudinal
study, age did not influence the decline in functioning in
a time period of 5 years [3].
The central issue in PPS is the gradual loss of muscle
function, i.e., new muscle weakness. The decline in muscle
strength progresses slowly, estimated at 1–3%per year [3, 4].
This implies that over longer periods of time, i.e., one or
two decades, muscle strength may markedly diminish.
Studies have shown that in polio survivors, motor
neurons are more widespread affected by polio than clin-
ically apparent. Traditionally, acute poliowas distinguished
in two forms, paralytic and non-paralytic, depending on
the presence of acute paresis. However, in reality paralytic
and non-paralytic polio are not two distinctly different
forms of polio virus infection. Already in the 1960s it was
demonstrated that paresis in patients who had recovered
from polio showed a continuum from severe to normal.
Fixed isometric strength measurements demonstrated that
strength, especially in the larger lower extremity muscles,
was often markedly reduced which was not detected with
manual muscle testing on clinical examination. This is due
to the upper limit in measurement range of manual muscle
testing to detect paresis. Modern imaging techniques have
confirmed that loss of muscle mass may be present while
manualmuscle strength is objectively normal. These obser-
vations are relevant in understanding that even patients
without clinically detectedweaknessmay retain residuals of
their polio and can sometimes develop PPS later in life.
Manual strength testing may easily lead to an
overestimation of muscle strength and hence, the individ-
ual’s physical capacities, for instance to walk.
A major complaint in PPS is fatigue. Fatigue may be
associated with exertion but often there is also the percep-
tion of general fatigue. Several causes of fatigue have been
considered such as impaired calcium kinetics leading to
disturbances in excitation contraction coupling of the
actin and myosin filaments, decreased capillary density
and reduced oxidative and glycolytic enzyme potentials,

720 P Postpolio Syndrome
impaired voluntary muscle activation, that can be due to
impaired reflex mechanism, increased neuromuscular
transmission defects in degenerating nerve terminals,
and degeneration of neurons of the reticular formation
and basal ganglia.
For PPS no cure exists. No pharmacological therapies
have been sufficiently proven to arrest the decline in mus-
cle function. The evidence for the effectiveness of intrave-
nous immunoglobulins is at present insufficient and needs
further study.
Exercise InterventionsLow maximal work capacity and maximal oxygen uptake
of polio survivors has been demonstrated in several stud-
ies. Although some studies concluded from these findings
that cardiorespiratory condition was poor, this can be
questioned. It has been demonstrated that the exercise
capacity of individuals with PPS was comparable with
the exercise capacity of age- and gender-comparable sed-
entary healthy individuals, when taking into account the
individual’s muscle capacity.
That exercise is beneficial for the preservation of phys-
ical functioning and well-being with aging is not debated.
Exercise aims at maintaining muscle function and cardio-
respiratory condition to preserve functional capacity,
a prerequisite to execute activities in daily life. Physically
active PPS patients were found to have less symptoms and
a higher functional level than inactive patients. Therefore,
in individuals with progressive and often marked
weakness and muscle degeneration due to PPS, exercise
may be especially relevant to maintain muscle function.
The dilemma, however, has been what intensities
should be individually applied. Overexerting muscles
might accelerate disease progression. On the other hand,
lack of exercise may lead to disuse of muscles and aggra-
vate disability.
A limited number of studies have been done to the
effects of aerobic exercise, muscle strengthening training,
and the combination of both in PPS. Based on the insuf-
ficient quality of the studies, a systematic review of efficacy
and safety of physical training in neuromuscular diseases
including PPS [5] and a recent Cochrane review on ther-
apies for PPS [6] concluded that at present the evidence is
insufficient to conclude that exercise is beneficial. Also the
effects of exercise on activities and health-related quality
of life have hardly been investigated. No studies have
reported adverse effects of exercise in PPS. Further
research is needed to establish whether physical training
is effective and beneficial in PPS. One of the challenges is
how to tailor the exercise intensity to the individual with
reduced muscle capacity.
Therapeutical ConsequencesThe ▶ rehabilitation treatment of PPS aims to maintain
physical and societal functioning and to preserve the qual-
ity of life. Treatment is multidisciplinary and symptomatic
and secondary conditions, such as ▶ osteoarthritis,
comorbidities, and aging, should be taken into account.
Therapy consists of three main components: exercise,
lifestyle modifications, and environmental adaptations.
The treatment recommendations considering exercise
are at present that supervised muscular training, both
isokinetic and isometric, is safe and may prevent further
decline of muscle strength in slightly or moderately weak
muscle groups and can reduce symptoms of muscular
fatigue, muscle weakness, and pain [7]. In severely affected
muscles strength training is likely not effective. Precautions to
avoid muscular overuse should be taken with intermittent
breaks, periods of rest between series of exercises, and
submaximal loads should be applied. Regarding aerobic exer-
cise submaximal and “non-fatiguing” intensities are advised.
In general patients should easily recover and muscle pain or
prolonged fatigue following exercise should be avoided.
It is important to realize that polio survivors are often
overachievers, as they were learned during the recovery
phase in their youth that they should deny their symptoms
and strive for normality. Later in life, it may be difficult to
adapt their behavior to the declining functional capacities
due to PPS, and many polio survivors have the tendency
to overload themselves. Therefore, avoidance of overuse
should receive specific emphasis in exercise guidance.
References1. March of Dimes Foundation (2001) Post-polio syndrome: identify-
ing best practices in diagnosis & care. March of Dimes, White Plains
2. Gonzalez H, Olsson T, Borg K (2010) Management of postpolio
syndrome. Lancet Neurol 9(6):634–642
3. Stolwijk-Swuste JM, Tersteeg I, Beelen A, Lankhorst GJ, Nollet F,
CARPA Study Group (2010) The impact of age and comorbidity on
the progression of disability in late-onset sequelae of poliomyelitis.
Arch Phys Med Rehabil 91(4):523–528
4. Stolwijk-Swuste JM, Beelen A, Lankhorst GJ, Nollet F, CARPA Study
Group (2005) The course of functional status and muscle strength in
patients with late-onset sequelae of poliomyelitis: a systematic
review. Arch Phys Med Rehabil 86(8):1693–1701
5. Cup EH, Pieterse AJ, Ten Broek-Pastoor JM, Munneke M, van
Engelen BG, Hendricks HT, van der Wilt GJ, Oostendorp RA
(2007) Exercise therapy and other types of physical therapy for
patients with neuromuscular diseases: a systematic review. Arch
Phys Med Rehabil 88(11):1452–1464
6. Koopman FS, Uegaki K, Gilhus NE, Beelen A, de Visser M, Nollet F
(2011) Treatment for postpolio syndrome. Cochrane Database Syst
Rev 16(2):CD007818
7. Farbu E, Gilhus NE, Barnes MP, Borg K, de Visser M, Driessen A,
Howard R, Nollet F, Opara J, Stalberg E (2006) EFNS guideline on
diagnosis and management of post-polio syndrome. Report of an
EFNS task force. Eur J Neurol 13(8):795–801

Preadolescence P 721
P
Posttetanic Potentiation
The term “posttetanic potentiation” (PTP) has two mean-
ings, but it appears that they are not related. The two
meanings can be divided into neural andmuscular. Neural
PTP occurs when repeated activation at a synapse results
in facilitation of nerve-nerve transmission. This mecha-
nism is not relevant in muscular activation, at least
between the motoneuron and the muscle fiber, because
there is typically a one-to-one transmission of action
potentials at the neuromuscular junction. Each action
potential on the motoneuron is sufficient to elicit one
action potential on each muscle fiber innervated by that
motoneuron. Muscular PTP refers to enhanced
submaximal contractile response due to a prior tetanic
contraction.When a twitch or subfusion frequency tetanic
contraction follows a tetanic contraction the active force
of that contraction will be enhanced relative to the con-
traction elicited with identical stimulation without prior
activation. This enhancement is referred to as posttetanic
potentiation. The mechanism of enhancement of such
submaximal contractions is the same as that for staircase
and for postactivation potentiation; the regulatory light
chains of myosin get phosphorylated, and this increases
the likelihood of myosin-actin interaction and increases
Ca2+ sensitivity.
Cross-References▶Postactivation Potentiation
Postural Balance
Postural balance is the ability to maintain the projection of
the body’s centre of mass within manageable limits of the
base of support, as in standing or sitting, or in transit to
a new base of support, as in walking.
Postural Control
▶Balance
Postural Stability
▶Balance
Power
Power is the rate of performing work and is the product of
force and velocity.
Power Output
The amount of work performed per unit of time. The SI
unit of power is watt (W), that is, the joule per second
(J s�1).
PPARs
Peroxisome proliferator-activated receptors (PPARs) are
ligand-activated transcription factors that belong to the
nuclear hormone receptor superfamily.
Cross-References▶Peroxisome Proliferator-Activated Receptors
PPARb/d
The peroxisome proliferator-activated receptor b/d(PPARb/d) represents one of three PPAR isotypes and is
the predominant PPAR isotype in skeletal muscle.
PPREs
Peroxisome proliferator response elements (PPREs) are
specific DNA sequences in the regulatory region of target
genes to which the active PPAR/RXR heterodimer binds in
order to stimulate gene transcription.
Preadolescence
A stage of human development following early childhood
and prior to adolescence (approximately up to age 11 in
girls and 13 in boys) in which children have not yet
developed secondary sex characteristics.

722 P Preconditioning
Preconditioning
The prior exposure of functioning cells or organs to
a sublethal stress which, through the activation of various
intracellular adaptive mechanisms, renders those cells or
organs resistant to a subsequent stress, even if it is different
than the initial stressor.
Precursor Cells
▶ Stem Cells
Predictive Value
Predictive value is another term that describes the diag-
nostic accuracy of a test. Predictive value of an abnormal
test (positive predictive value) is the percentage of people
with an abnormal test result who have disease. Predictive
value of a normal test (negative predictive value) is the
percentage of people with a normal test result who do not
have disease.
Pregnancy
RUBEN BARAKAT
Universidad Politecnica de Madrid, Madrid, Spain
SynonymsNon-adverse maternal and fetal outcome
DefinitionPregnancy is the unique vital process in which all body
control systems are modified in women to generate the
fetal life and thereby ensure its growth and development.
During a gestational period of about 38 weeks, pregnant
women must make constant adjustments to maintain
balance and biological homeostasis, to allow them to
deliver without maternal and fetal complications [5].
Any disarrangement or imbalance in the pregnant
body would be an adverse outcome.
Difficult deliveries are due to a sedentary lifestyle....
(Aristoteles, C. III b.C.) [2]
Why exercise during pregnancy?
What science supports encouraging the practice of an
adequate program of physical exercise during pregnancy?
Historically, pregnant women were denied an active
gestation. Most current research, however, shows that
a pregnant woman with no obstetric complications can
exercise during pregnancy without adverse maternal-fetal
outcome.
Today, more women want to exercise during
pregnancy. Physical activity is an important part of
life for many people, pregnant women being no
exception [3].
Our concept of health has evolved from an “absence of
disease” to a larger, holistic concept that includes not only
the most important vital functions (cardiocirculatory
response, metabolic parameters, hormonal functions,
etc.) but also psychological and social well-being.
A sedentary lifestyle creates complications in all
humans, and according to recent scientific evidence, preg-
nancy is not a time of immunity from this problem.
Therefore, for pregnant women, exercise is an important
part of achieving and maintaining health in all areas and
systems.
Pregnancy should not reduce quality of life, Options
for physical activity should be found so that pregnant
women do not abruptly discontinue the practice
of physical sport. Variants that guarantee a minimum
amount of exercise during pregnancy should be provided.
Description
Changes caused by pregnancy
Relevant changes that occur in pregnantwomen related to physical activity
Circulatory System
Two basic facts should be taken into account:
● Increased requirements due to the regular develop-
ment of the fetus.
● The upwardmovement of certain structures as a result
of the increased size of the uterus.
Cardiac output (product of stroke volume and heart
rate) increases by 30–40% from the beginning of the first
trimester to the end of pregnancy as a result of
increased heart rate (from 70 beats/min non-pregnant to
85 beats/min in late pregnancy) and a slight increase in
stroke volume [2].
Peripheral vascular resistance decreases, which causes
a slight change in blood pressure. Diastolic blood pressure
decreases in the first and second trimesters and returns to

Aorta
Inferior CavaVein
Pregnancy. Fig. 1 Inferior cava vein compression by gravid uterus
Pregnancy P 723
P
pre-pregnancy values in third trimester. Systolic blood
pressure is modified slightly, with a tendency to decrease
in the first and second trimesters [2].
Possibly the most significant change (and most
consequential) during pregnancy is the compression of
the inferior cava vein by the gravid uterus. When a
woman adopts the supine position there is decreased
venous return to heart (Fig. 1). This affects cardiac output
and some parameters related to the circulatory blood flow
in the heart return phase.
Hematologic Changes
Blood volume increases by 45% (1,800 ml), both from an
increase in blood volume or plasma (about 1,500 ml) and
from citemia (about 350 ml). This “hemodilution” main-
tains adequate utero-placental flow [2].
Respiratory Changes
Changes in the respiratory system cause anatomical and
functional alterations; these modifications are due to hor-
monal influences and the incremental volume changes of
the pregnant body and include changes in lung dimension,
capacity, and respiratory mechanisms.
The combination of reduced functional residual
capacity and increased oxygen consumption generates
decreased oxygen reserves. Moreover, higher oxygen con-
sumption in respiration (due to increased diaphragmatic
work) occurs.
Also, increased ventilation/minute exists, resulting in
respiratory alkalosis, in this case by the action of estrogen
and progesterone. However, the acid-base is maintained
by a compensatory metabolic acidosis, in which the blood
pH values remain around 7.44.
The main purpose of these maternal breathing mech-
anisms is to reduce the arterial PCO2 and generate a mild
alkalosis, which ensures maternal placental gas exchange
and acts to prevent fetal acidosis [2].
Metabolic Changes
Normal metabolic processes are altered during pregnancy
to accommodate the needs of the developing fetus. Protein
content in body tissue increases. Carbohydrates accumu-
late in the liver, muscles, and placenta; some fat deposits
appear under the skin, especially in the chest and buttocks.
There is also an increased concentration of both choles-
terol and fat in the blood [5].
A pregnant woman’s body accumulates salts of various
minerals essential for normal fetal development, including
calcium, phosphorus, potassium, and iron.
Furthermore, hormonal changes stimulate the reten-
tion of water in the tissues.
Maternal weight gain is one of the most obvious
changes during pregnancy. Adequate maternal gain is
between 10 and 13 kg during pregnancy, with individual
variations. Maternal weight increase depends on several
factors (Table 1).

Pregnancy. Table 1 Maternal weigh gain during pregnancy
Maternal weight gain (g)
10 week 20 week 30 week 40 week
Fetus 5 300 1,500 3,400
Placenta 20 170 430 650
Amniotic fluid 30 350 750 800
Uterus 140 320 600 970
Breast 45 180 360 405
Blood 100 600 1,300 1,250
Interstitial fluid 0 30 80 1,680
Fat deposit 310 2,050 3,480 3,345
Total increase 650 4,000 8,500 12,500
724 P Pregnancy
Locomotor Changes
Pregnant women often suffer paresthesia and pain in the
upper extremities as a result of a marked sinking of
the cervical lordosis and shoulder girdle, frequently in
the third trimester. An important change in the pregnant
body is the “hyperlordosis of pregnancy,” which has tra-
ditionally been considered an alteration caused by growth
of the uterus, but nowadays the scientific evidence shows
that the mother outweighs the deviation of its center of
gravity, not by a hyperlordosis, if not moving back all the
skull-caudal axis (Fig. 2).
Occasionally, rectus abdominis muscles are separated
from themidline, creating a diastasis of variable extension.
Sometimes it is so severe that the uterus is only covered by
a thin layer of peritoneum, fascia, and skin. The mobility
of the sacroiliac joints is increased due to hormonal
action, particularly relaxin. In this sense, the joints can
cause relaxation diffuse pains [2].
ApplicationRecent scientific evidence has shown that a program of
aerobic and moderate exercise performed during preg-
nancy does not cause adverse maternal and fetal outcomes
in healthy pregnant women, including social and emo-
tional factors [3, 4].
● Contraindications [1]:
ABSOLUTE
– Hemodynamically significant heart disease
– Restrictive lung disease
– Incompetent cervix/cerclage
– Multiple gestation at risk for premature labor
– Persistent second or third trimester bleeding
– Placenta previa after 26 weeks gestation
– Premature labor during the current pregnancy
– Ruptured membranes
– Pregnancy-induced hypertension
ATIVE
REL– Severe anemia
– Unevaluated maternal cardiac arrhythmia
– Chronic bronchitis
– Poorly controlled type I diabetes
– Extreme morbid obesity
– Extreme underweight (body mass index <12)
– History of extremely sedentary lifestyle
– Intrauterine growth restriction in current
pregnancy
– Poorly controlled hypertension/preeclampsia
– Orthopedic limitations
– Poorly controlled seizure disorder
– Poorly controlled thyroid disease
– Heavy smoker
rning signs to terminate exercise while pregnant [1]:
● Wa– Vaginal bleeding
– Dyspnea before exertion
– Dizziness
– Headache
– Chest pain
– Muscle weakness
– Calf pain or swelling (need to rule out
thrombophlebitis)
– Preterm labor
– Decreased fetal movement
– Amniotic fluid leakage
Medical Permission: For the reasons cited above, it is
●important for pregnant women to have medical per-mission before starting a fitness program. The overall
health, obstetric, and medical risks should be reviewed

Pregnancy. Fig. 2 Deviation of center of gravity in pregnancy
Pregnancy P 725
P
before a pregnant woman is prescribed an exercise
program. In the absence of contraindications,
a pregnant woman should be encouraged to engage
in regular, moderate-intensity physical activity to con-
tinue to derive the same associated health benefits
during pregnancy as before pregnancy. However,
there are contraindications to exercise because of
preexisting or developing medical conditions, and
pregnancy is no different. In addition, certain obstetric
complications may develop in pregnant women
regardless of the previous level of fitness, which
could preclude them from continuing to exercise
safely during pregnancy [1].
● Type of exercise: Many activities may be performed
during pregnancy; it is only important that pregnant
women do not perform the physical activity with
excessive intensity or long duration. Activities that
increase the risk of falls, such as skiing, or those that
may result in excessive joint stress, such as jogging and
tennis, should be avoided.
The recommended options are [1]:
– Supervised program of physical activity for preg-
nant women: undoubtedly the best choice because
it is guided and supervised by a qualified practi-
tioner of sports science and therefore provides the
quality, quantity, and intensity of activity adequate
for a pregnant woman to feel comfortable and safe
when exercising.
– Walking.
– Bicycling: Caution: Do not perform the activity on
unstable surfaces that increase the risk of imbal-
ance and falls, especially in the third trimester.
– Stationary cycling
– Swimming or aquatic activities.
– Yoga, Pilates, different aerobic dances or similar.
Intensity: Intensity is the most difficult component of
●an exercise regimen to prescribe for pregnant women.Two mechanisms have been used by researchers to
properly control the intensity of exercise in pregnant
women: heart rate and perceived exertion scale.
60–70% of maximal heart rate (or 50–60% ofmaximal
oxygen uptake) appears to be appropriate for most
pregnant women. Given the variability in maternal
heart rate responses to exercise, target heart rates can-
not be the only mechanism used to monitor exercise
intensity in pregnancy.
Ratings of perceived exertion have been found to
be useful during pregnancy as an alternative to heart
rate monitoring of exercise intensity. For moderate
exercise, ratings of perceived exertion should be
12–14 (somewhat hard) on the 6–20 scale [1].
Duration: Two concerns should be addressed before
●prescribing prolonged exercise regimens for pregnantwomen. The first is thermoregulation and the second
is energy balance. A session of moderate exercise,
performed in appropriate conditions (see below),
may have a duration of 35–45 min [1].
● Frequency: In the absence of either medical or obstet-
ric complications, pregnant women may exercise three
to five times per week.
● Considerations:
– Exercise preferably should be performed in a
thermoneutral environment or in controlled envi-
ronmental conditions (air conditioning).
– Attention to proper hydration and subjective feel-
ings of heat stress are essential.
– Valsalva mechanism should be avoided.
– Tasks in the supine position should be avoided for
more than 3–4 min of exercise.
– Impact exercises should be avoided.
References1. Artal R, O’Toole M (2003) Guidelines of the American College of
Obstetricians and Gynecologists for exercise during pregnancy and
the postpartum period. Br J Sports Med 37:6–12
2. Artal R, Wiswell R, Drinkwater B (eds) (1991) Exercise in pregnancy,
2nd edn. Williams and Wilkins, Baltimore
3. Barakat R, Lucia A, Ruiz J (2009 Sep) Resistance exercise training
during pregnancy and newborn’s birth size: a randomised controlled
trial. Int J Obes (Lond) 33(9):1048–1057

726 P Pre-hypertension
4. Barakat R, Pelaez M, Montejo R, Luaces M, Zakynthinaki M (2011)
Exercise during pregnancy improves maternal health perception: a
randomized controlled trial. Am JObstetGynecol 204(5):402.e1–402.e7
5. Wolfe L, Ohtake P, Mottola M, McGrath M (1989) Physiological
interactions between pregnancy and aerobic exercise. In: Pandolf
KB (ed) Exerc and spotrs sci reviews. Baltimore, Willians and
Wilkins, pp 295–351
Pre-hypertension
Systolic blood pressure ≥120 to <140 and/or diastolic
blood pressure ≥80 to <90 mmHg.
Premenopausal
The time in a woman’s life when menstrual cycles are
normal (e.g., 10–12 menses per year).
Preventing Accidental Falls
▶ Fall Prevention
Preventing Loss of PosturalBalance
▶ Fall Prevention
Preventing Slips and Trips
▶ Fall Prevention
Primary Active Transport
Uphill transport dependent on the energy from ATP.
Primary Amenorrhea
Primary amenorrhea is the failure to achieve menarche by
age 15 in the presence of normal development of second-
ary sex characteristics.
Primary Hypertension
▶Hypertension, Training
Primary Stroke Prevention
Anticipatory strategies employed to avoid the develop-
ment of stroke. Examples include smoking cessation,
blood pressure control, proper diet and exercise.
Procaspases
The inactive zymogen of caspases.
Production of Erythrocytes
▶ Erythropoiesis
Prodynorphin
▶Opioid Peptides, Endogenous
Proenkephalin
▶Opioid Peptides, Endogenous
Progenitor Cells
▶ Stem Cells
Progesterone
Sex steroid (ovarian hormone) involved in the female
menstrual cycle. Data indicate progesterone may impact
blood flow both via direct and indirect mechanisms.

Promotion of and Adherence to Physical Activity P 727
Prognosis
Prognosis is a medical term to describe the likely outcome
of an illness.
Programmed Cell Death
▶Apoptosis
Progressive Overload
A fundamental principle in resistance training that states
in order to see adaptations in body structures, physiolog-
ical function, or performance, an increasing demandmust
be placed on the neuromuscular system, e.g., increasing
the resistance over time.
P
Pro-inflammatory Activation
Pro-inflammatory activation (or classical activation) is
a macrophage inflammatory state characterized by the
secretion of pro-inflammatory chemokines (CCL2,
CCL8), and cytokines (IL-12, TNFalpha), ROS, a high
microbicidal activity. It can be triggered in vitro by
IFNgamma and/or LPS treatment. Proinflammatory mac-
rophages are associated with acute inflammation.
Pro-inflammatory Cytokines
Cytokines produced predominantly by activated immune
cells and are involved in the amplification of inflammatory
reactions. These include IL-1, IL-6, TNF-a, and TGF-b.
Promotion of and Adherence toPhysical Activity
MARLENE N. SILVA, PEDRO J. TEIXEIRA
Department of Sports and Health, Faculty of Human
Kinetics, Technical University of Lisbon, Lisbon, Portugal
SynonymsCompliance; Develop; Encourage; Engagement; Involve-
ment; Participation; Prompt; Raise; Retention
DefinitionPromotion refers to the encouragement of something
(e.g., physical activity) to happen or develop. However,
getting started and continuing an activity, such as an
exercise program, can be two different processes, requiring
different strategies. Generally, adoption refers to the
beginning stage of an exercise regimen, while adherence
refers to maintaining it for a prolonged period of time,
following the initial adoption phase, that is, the level of
participation achieved in a behavioral regimen once the
individual has agreed to undertake it. Central to adherence
is the assumption that the individual voluntarily
and independently chooses to engage in the activity.
Adherence is generally regarded as a largely psychological
issue and knowledge about it becomes paramount in
health promotion efforts [1]. Unfortunately, inconsis-
tencies in the literature on definitions and measurement
of adherence make valid comparisons among studies
difficult. Also, long-term follow-up of behavioral inter-
vention methods and their effect on exercise adherence is
generally lacking [2, 3]. Current studies suggest that
there are different processes associated with short-term
versus long-term behavior change. Consequently, some
behavioral strategies may be more important for
the ▶maintenance phase compared with initiation of
▶ physical activity. In this regard, it is critical that future
studies provide information on the greatest influences to
the initiation and long-term adherence to physical
activity [4].
Increasing the prevalence of people who are physically
active (i.e., foster promotion and adherence) demands
several contributions including understanding/investigating
the determinants (correlates, ▶mediators) of active and
inactive lifestyles, both in the short- and the long-term,
developing assessment tools for the behavior and outcomes
from both acute and chronic involvement in activity, testing
appropriate theoretical frameworks and related adherence
strategies for interventions, and conducting robust evalua-
tions of interventions and training other professionals in
behavior change strategies [5]. Furthermore, research on
exercise adherence has typically focused on planned bouts
of high-intensity exercise scheduled for specific times and
days. A focus on other types of physical activity (e.g.,
occupational, transportation, routine activities) that
strongly influence total daily energy expenditure demands
a reconceptualization of both definitions and measures of
adherence. It has become clear that in order to continue to
advance the field of exercise behavior, researchers
must develop broader definitions of physical activity
participation that extend beyond the traditional definitions
of program adherence.

728 P Promotion of and Adherence to Physical Activity
CharacteristicsGiven the complexity of the processes involved, exercise
adherence is not the domain of a single field. Theoretical
and practical contributions on its promotion come from
several fields such as exercise science, sports medicine,
preventive medicine, health psychology, behavioral
medicine, epidemiology, nutrition, health promotion,
rehabilitative medicine, communication, marketing
sciences, and public policy. Regardless, the high prevalence
of physical inactivity raises the central question of how to
optimally facilitate the adoption of a physically active
lifestyle over the long term. The continued development
and expansion of conceptual approaches that can broaden
our understanding of factors that potentially influence
physical activity participation is critical. In order for inter-
ventions to be effective a sound understanding of physical
activity determinants or correlates, preferably rooted in
sound theoretical frameworks, is needed [6].
Research in the physical activity promotion arena has
focused on the application of theoretical perspectives
aimed primarily at personal levels of understanding and
analysis. The investigation of such theories has provided
important insights related to potentially useful correlates
of physical activity behavior and have been cogently
reviewed elsewhere [6]. In brief, the main theories used
have been the health belief model, theory of planned
behavior, social cognitive theory, the transtheoretical
model and, more recently, self-determination theory.
Background on these theories is available elsewhere [7, 8].
Taking research beyond the personal level, there has
been a greater recognition of the “bigger picture” of the
influences in physical activity, whereby factors associated
with, or directly influencing physical activity, are placed
within a wider framework that go beyond the psychological
level to Social (societal values and preferences, public pol-
icies, economic/market factors) and Built Environments
(land use patterns, the transportation system, and design
features). Factors associated with physical activity can fall in
several arenas: (1) demographic and biological; (2) psycho-
logical, cognitive, and emotional; (3) behavioral attributes
and skills; (4) social and cultural; (5) physical environmen-
tal; or (6) physical activity characteristics. The fact that
there are multiple correlates within each category of vari-
ables strongly suggests a very complex causal web. The
documentation of intrapersonal, interpersonal, social/cul-
tural, and physical environmental correlates seems to
demand a multilevel ecologic approach to understanding
physical activity [6]. However, identifying social and envi-
ronmental determinants of physical activity is complex and
it is far from complete. For example it is difficult to sort out
which characteristics of the built environment have the
strongest association. Nor does the literature illuminate
the strength of the associations or the populations affected.
More important, the evidence falls short of establishing
causal connections. Weaknesses of the current literature
include the lack of a sound theoretical framework, inade-
quate research designs, and incomplete data. Nevertheless,
it provides preliminary evidence that some characteristics
of the built environment may affect physical activity levels,
or at least certain types of physical activity (e.g., destina-
tion-oriented travel or recreational physical activity).
These characteristics include certain land use measures
(e.g., density, diversity of uses), accessibility, certain design
features, and certain aspects of the transportation
infrastructure (sidewalks in particular) [11].
Table 1, adapted from a previous review [6], shows the
pattern of findings pertaining to the influences on overall
physical activity in adults, depicting variables evaluated in
multiple studies (combined by levels of evidence), and,
when applicable, the theory or theories involved. Even if
an initial scan of the field (documented in the table)
suggests that variables involved are too numerous to pro-
vide definitive guidelines for behavior change, a closer
inspection shows that approaches that articulate the
important role of support, perceptions of competence
and beliefs concerning autonomy and control have degrees
of overlap and provide important guides for behavior
change. In addition, stage-based, hybrid models, and
Motivational Interviewing-based protocols, provide prag-
matic frameworks to apply theoretical principles [5].
Regarding the most common strategies used to pro-
mote physical activity behavior, they can typically be
grouped into: (1) behavior modification approaches
(e.g., prompts, contracts); (2) reinforcement approaches
(e.g., charting attendance and participation, rewarding
attendance and participation, feedback and testing);
(3) cognitive–behavioral approaches (e.g., goals, self-talk,
thought focus strategies, association, dissociation);
and (4) social support approaches (e.g., social support
from partner, group, or class). A recent comprehensive
meta-analysis found that behavioral interventions appeared
to be more effective than cognitive interventions and that
interventions to increase physical activity should emphasize
components such as self-monitoring, stimuli to increase
physical activity, rewards, behavioral goal setting, and
modeling of actual physical activity behavior [9]. However,
when long-term sustained adherence is considered,
additional strategies need to be taken into account,
namely, the use of “intrinsic” approaches, which focus
on the experience or the process of engaging in (meaning-
ful) physical activity and require addressing motivation in
a more detailed way. Because of their clinical relevance
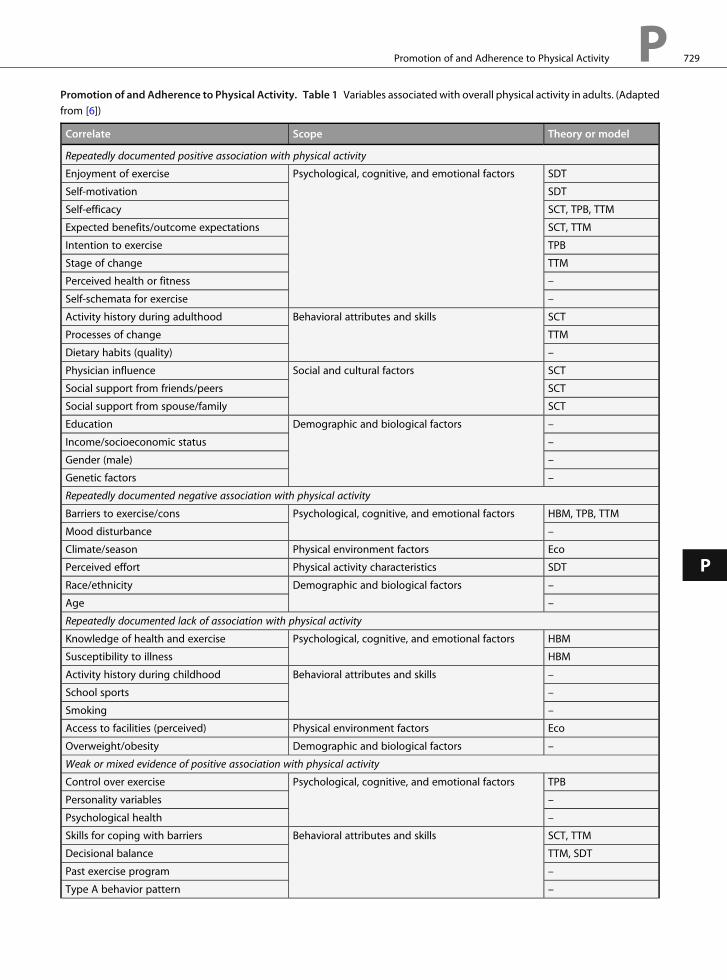
Promotion of and Adherence to Physical Activity. Table 1 Variables associated with overall physical activity in adults. (Adapted
from [6])
Correlate Scope Theory or model
Repeatedly documented positive association with physical activity
Enjoyment of exercise Psychological, cognitive, and emotional factors SDT
Self-motivation SDT
Self-efficacy SCT, TPB, TTM
Expected benefits/outcome expectations SCT, TTM
Intention to exercise TPB
Stage of change TTM
Perceived health or fitness –
Self-schemata for exercise –
Activity history during adulthood Behavioral attributes and skills SCT
Processes of change TTM
Dietary habits (quality) –
Physician influence Social and cultural factors SCT
Social support from friends/peers SCT
Social support from spouse/family SCT
Education Demographic and biological factors –
Income/socioeconomic status –
Gender (male) –
Genetic factors –
Repeatedly documented negative association with physical activity
Barriers to exercise/cons Psychological, cognitive, and emotional factors HBM, TPB, TTM
Mood disturbance –
Climate/season Physical environment factors Eco
Perceived effort Physical activity characteristics SDT
Race/ethnicity Demographic and biological factors –
Age –
Repeatedly documented lack of association with physical activity
Knowledge of health and exercise Psychological, cognitive, and emotional factors HBM
Susceptibility to illness HBM
Activity history during childhood Behavioral attributes and skills –
School sports –
Smoking –
Access to facilities (perceived) Physical environment factors Eco
Overweight/obesity Demographic and biological factors –
Weak or mixed evidence of positive association with physical activity
Control over exercise Psychological, cognitive, and emotional factors TPB
Personality variables –
Psychological health –
Skills for coping with barriers Behavioral attributes and skills SCT, TTM
Decisional balance TTM, SDT
Past exercise program –
Type A behavior pattern –
Promotion of and Adherence to Physical Activity P 729
P

Promotion of and Adherence to Physical Activity. Table 1 (continued)
Correlate Scope Theory or model
Access to facilities (actual) Physical environment factors Eco
Childlessness Demographic and biological factors –
Injury history –
Weak or mixed evidence of negative association with physical activity
Lack of time Psychological, cognitive, and emotional factors –
Poor body image –
Social isolation Social and cultural factors –
Intensity Physical activity characteristics –
High risk for heart disease Demographic and biological factors –
Marital Status –
Weak or mixed evidence of no association with physical activity
Attitudes Psychological, cognitive, and emotional factors HBN, TPB
Health locus of control TPB
Value of exercise outcomes TPB
Alcohol Behavioral attributes and skills –
Sports media use –
Exercise models Social and cultural factors SCT
Past family influences SCT
Cost of programs Physical environment factors SCT, Eco
Home equipment Eco
HBM health belief model, TPB theory of planned behavior, TTM transtheoretical model, SCT social cognitive theory, SDT self-determination theory,
Eco ecological models
730 P Promotion of and Adherence to Physical Activity
these approaches are better explained below. Indeed, while
some interventions proved to be effective and successfully
increased physical activity in the short term, subjects often
fall back into their original routines once the intervention
period is completed. Maintenance and long-term adher-
ence to physical activity are essential to achieve sustainable
health effects. However, knowledge of effective interven-
tion strategies for long-term maintenance of physical
activity is at an early stage and is not often reported/
achieved [3, 4].
Clinical RelevanceUnderstanding the mechanisms behind sustained physical
activity is an important topic for conceptual and practical
reasons, namely to develop more effective exercise promo-
tion interventions and practices. Research on theory-
based treatment-induced mediators of physical activity
participation (i.e., intervention mechanisms contributing
to physical activity change) is critical to identify potential
causal mechanisms through which interventions operate,
which can streamline and improve the program by focus-
ing on effective components; active therapeutic
components could be intensified and refined whereas
inactive or redundant elements could be discarded.
Thus, progress in identifying the most effective treatments
and understanding why treatments work or do not work
depends on efforts to identify mediators of treatment
outcome, a research endeavor that led to the recommen-
dation that randomized controlled trials routinely include
and report such analyses [6].
Motivation and Long-Term Promotion ofPhysical ActivityAs pointed out, experimental research and increased the-
oretical and methodological clarity could accelerate the
identification of effective behavior change techniques and
the development of evidence-based practices. In the gen-
eral population, research has now shown that mainte-
nance of exercise is especially related to the process and
the quality of the exercise participation experience, which
emphasizes intrinsic or well-integrated motives, stressing
the need to shift from outcome-focused treatments to
process-oriented approaches. Results from a recent large
randomized controlled trial [10] highlighted that exercise

Promotion of and Adherence to Physical Activity P 731
P
autonomous motivation, a particular type of motivation,
predicts long-term adherence to physical activity
and weight loss maintenance in women. Contrary to the
popular perception that all motivation is good motiva-
tion, this study showed that intrinsic reasons and well-
internalized sources of (psychological) energy to be active,
pertaining to autonomous motivation (as in feeling
a sense of “ownership” and personal endorsement about
one’s exercise routine), are potentially very useful for
lasting behavior change, while more external/extrinsic
types of motivation are not. The results of this trial
highlighted the importance of interventions targeting the
internalization of exercise behavioral regulation and mak-
ing exercise and physical activity positive and meaningful
experiences rather than simply focusing on immediate
behavior change. In opposition, exerting pressure,
establishing deadlines, having external contingencies
such as using financial or similar incentives, and offering
little choice about how to lose weight are all strategies with
reduced likelihood of success. They can produce results
but essentially they are a short-term solution for a long-
term problem. Presently, researchers are finding that the
qualitative aspects of motivation need to be more empha-
sized in interventions, as disappointing long-term results
of interventions may be due to the fact that existing
programs largely ignore the potentially crucial element
of motivation for sustained behavioral change. Under-
standing better how to motivate physical activity and
lifestyle changes is a critical issue.
These are significant issues also from a mental health
perspective. Indeed, in the view of self-determination the-
ory, physical activity can be an inherently rewarding activ-
ity that contributes to both happiness and subjective
vitality. Intrinsic aspirations for exercise can contribute
to the satisfaction of basic needs and an overall sense of
wellness [8]. Thus, health professionals should be encour-
aged to help participants make the transition from
“should” to “want to” motivation. Partially, this means
going beyond teaching/training particular behavior
change skills (e.g., goal setting, self-monitoring) to
encompass strategies like participants’ verbalization of
their own behavioral goals and exploration of how these
goals can be accomplished in the context of their lifestyle,
identifying factors that encourage more identified and
intrinsic reasons for change (while downplaying external
reasons to exercise), and promoting competence and
confidence (e.g., through modeling). Also, and most
importantly, the support of autonomy and self-initiation
are recommended by assuring choice (e.g., promoting
active experimentation, supporting subjects’ initiatives,
minimizing external sources of control/pressure),
exploring individual values, meanings, and goals and
how they can be linked to the targeted behavioral changes,
and interpreting and deconstructing social pressures/
expectations. In sum, it is important to help participants
focus on their own valued goals (e.g., health and fitness,
improved well-being) as well as behavioral targets (i.e.,
adopting certain exercises or attending a certain number
of sessions per week), and also encourage the creation of
enjoyable exercise environments. Fortunately, a wide vari-
ety of sports and physical activities are available, and these
provide multiple opportunities for optimal challenges
and different experiences that can help all people
develop the sense of ownership and mastery that under-
pins autonomous regulation. Recommending lifestyle
and informal physical activity over formal and
programmed exercise may be another key to adherence.
Adherence may be increased because of the relative ease of
incorporating lifestyle exercise into daily life, enhancing
confidence in the ability to perform physical activity (self-
efficacy).
References1. Dishman RK (ed) (1994) Advances in exercise adherence. Champaign,
Human Kinetics
2. Belanger-Gravel A, Godin G, Vezina-Im LA, Amireault S, Poirer P
(2011) The effect of theory-based interventions on physical activity
participation among overweight/obese individuals: a systematic
review. Obes Rev 12:430–439
3. Fjeldsoe B, Neuhaus M, Winkler E, Eakin E (2011) Systematic review
of maintenance of behavior change following physical activity and
dietary interventions. Health Psychol 30:99–109
4. Marcus B (2000) Physical activity behavior change: issues in adoption
and maintenance. Health Psychol 19:32–41
5. Bidle SJH, Mutrie N (2008) Psychology of physical activity: determi-
nants, well-being and interventions. Routledge, New York
6. Bauman AE, Sallis JF, Dzewaltowski DA, Owen N (2002) Toward
a better understanding of the influences on physical activity: the role
of determinants, correlates, causal variables, mediators, moderators,
and confounders. Am J Prev Med 23(2):5–14
7. Glanz K, Lewis FM, Rimer BK (eds) (2002) Health behavior and
health education: theory, research, and practice. Jossey-Bass, San
Francisco
8. Ryan R, Deci E (2007) Active human nature: self-determinant theory
and the promotion and maintenance of sport, exercise and health.
In: Hagger M, Chatzisarantis N (eds) Intrinsic motivation and
self-determination in exercise and sport. Human Kinetics,
Champaign
9. Conn V, Hafdahl A, Mehr D (2011) Interventions to increase physical
activity among healthy adults: meta-analysis of outcomes. Am
J Public Health 101:751–758
10. Silva MN, Markland D, Carraca EV, Vieira PN, Coutinho SR,
Minderico CS, Matos MG, Sardinha LB, Teixeira PJ (2011) Exercise
autonomous motivation predicts 3-year weight loss in women. Med
Sci Sports Exerc 43(4):728–737. doi:10.1249/MSS.0b013e3181f3818f
11. Handy S, Boarnet M, Ewing R, Killingsworth R (2002) How the built
environment affects physical activity views from urban planning.
Am J Prev Med 23(2S):64–73

732 P Prompt
Prompt
▶Promotion of and Adherence to Physical Activity
Proopiomelanocortin
▶Opioid Peptides, Endogenous
Prooxidant–Antioxidant Balance
▶Oxidative Stress
Prostaglandins
Hormone-like molecules, derived from fatty acids, which
are released in a paracrine fashion, and are involved in the
stimulation of bone formation.
Proteases
Enzymes that break down (i.e., hydrolyze) the peptide
bonds of proteins.
Proteasomes
Proteasomes are large self-compartmented multicatalytic
proteases. Proteasomes are formed of a 20 S proteasome
that binds to one or two regulatory particles. The
20 S catalytic core comprises four rings of seven a- andb-subunits organized as a7-, b7-, b7-, a7. The inner ringsof b-subunits contain the protease active sites and the
outer rings of a-subunits bind to various regulatory par-
ticles such as the 19 S or the 11 S regulatory particles. The
most common proteasomes are 26 S proteasomes that
comprise a central 20 S proteasome and two 19 S regula-
tory particles responsible for the recognition of a
polyubiquitin degradation signal. Each 19 S regulatory
particle contains six ATPases that provide energy for sev-
eral functions including the unfolding of the substrate, the
gating of the catalytic chamber, and the breakdown of
the target protein into peptides.
Protein
A protein is a molecule comprised of multiple polypeptide
chains (linear sequences of amino acids) that performs
a precise biological function. Proteins serve a variety of
roles in the human body such as catalyzing metabolic
reactions (i.e., enzymes), providing structural support
(i.e., cytoskeleton), actively transporting molecules in
and out of cells, and providing intracellular communica-
tion (i.e., cell signaling). The specific sequence of amino
acids in each polypeptide chain creates the structure of the
protein and this specific structure is imperative for proper
functioning of the protein.
Cross-References▶Nutrition
Protein Balance
Protein balance is the net contribution of protein synthesis
and protein breakdown. Positive protein balance occurs
when the rate of protein synthesis exceeds protein break-
down.Conversely, negative protein balance occurswhen the
rate of protein breakdown exceeds protein synthesis. Pro-
tein balance can bemeasuredwithin an organismor a single
protein pool. It is the primary determinant of muscle mass.
Protein Breakdown
Protein breakdown is the release of amino acids from
existing proteins. Protein breakdown functions to remove
damaged proteins, change the protein content of a cell, or
to liberate amino acids to the amino acid pool.
Protein Building Blocks
▶Amino Acids
Protein Chaperone
A protein that forms a non-covalent complex with other
proteins, typically to perform intracellular housekeeping
actions, such as the folding of nascent or unfolded

Proteome P 733
proteins, prevention/assistance of protein degradation,
intracellular transport, and signaling. Chaperone function
may sometimes utilize ATP although this is not the case in
all chaperone actions. Although chaperones are not nor-
mally involved in protein function, they may add to their
stability or ensure they are ideally located within the cell.
Many chaperones are heat shock or stress proteins, but this
is not always the case; some chaperones are not inducible
with stress. Groups of proteins that have chaperone func-
tion are often called chaperonins (such as GroEL in E.
coli). Co-chaperones (such as Hsp40–DNAJ) help modu-
late chaperone function.
Protein Degradation
The regulated breakdown of proteins into their composite
amino acids.
P
Protein Kinase
A protein kinase is an enzyme that catalyzes the transfer of
a phosphate group from ATP to a target protein in
a process called phosphorylation. A serine/threonine
kinase transfers phosphate to serine or threonine amino
acid residues in proteins. A tyrosine kinase transfers phos-
phate to tyrosine amino acid residues. A phosphorylation
reaction is reversed by dephosphorylation, or removal of a
phosphate group, in a reaction catalyzed by a phosphatase.
Protein Kinase A (PKA)
Cyclic AMP-Dependent Kinase A.
Cross-References▶ Excitation–Contraction Coupling
Protein Kinase C
Protein kinase C (PKC) belongs to a family of enzymes
which modulate the function of target proteins via the
phosphorylation of hydroxyl groups of serine and threo-
nine amino acid residues. The PKC family consists of at
least 12 different subtypes, which have been grouped into
three groups according to their biochemical
characteristics. The major intracellular activator of PKC
is diacylglycerol (DAG) which is generated via different
enzymatic reactions with different time constants. Initially
DAG is recruited transiently from hydrolysis of phosphati-
dylinositol-4,5-bisphosphate followed by a more
sustained increase due to hydrolysis of phosphatidylcho-
line. Upon activation, PKC is redistributed from cytosol to
the membrane in a calcium-dependent manner. The acti-
vation-induced membrane association is responsible for
some of the specific functions of PKC like downregulation
of receptors, modulation of ion channel activity, and
rearrangement of cytoskeletal structures during exo- and
endocytosis. Moreover, PKC is a part of cellular signaling
pathways involved in cell growth and differentiation.
Protein Synthesis
Protein synthesis is the process of linking amino acids into
a linear chain that is folded to a final functional form.
Specific proteins are synthesized in response to cellular
signals to meet the particular requirements of a changing
environment.
Protein Turnover
Protein turnover is the combination of protein synthesis
and breakdown. Protein turnover maintains cellular pro-
tein pools through the synthesis of new proteins and the
breakdown of existing proteins. Protein turnover differs
from protein balance in that one is a process and one is
a result.
Cross-References▶Metabolism, Protein
Proteolytic System
▶Ubiquitin-Proteasome System
Proteome
The entire set of proteins expressed by a genome, cell,
tissue, or organism.

734 P Proteosome
Proteosome
Very large protein complex degrading ubiquitin tagged
proteins.
Cross-References▶Proteasomes
Prothrombin/Thrombin
Thrombin (or coagulation factor IIa) is as a serine prote-
ase produced by proteolytic cleavage of the proenzyme,
prothrombin. Prothrombin is a glycoprotein of 72 kDa
consisting of a single polypeptide chain. Thrombin is
a multifunctional highly specific enzyme mainly involved
in hemostasis. The activation of thrombin is the final step
in the coagulation cascade. Thrombin cleaves soluble
fibrinogen to form insoluble fibrin. Thrombin also acti-
vates coagulation factors such as factor V, factor VIII, and
factor XIII. It also mediates activation of platelets and
possesses vasoactive properties.
Apart from being a blood coagulation factor with
a central role in hemostasis, thrombin has pleiotropic
activities. Several reports suggest a broader physiologic
role with functions in wound healing, inflammation, and
atherosclerosis. Thrombin modulates a variety of cell
functions, includingmitogenic activities, through the acti-
vation of various intracellular-signaling pathways,
through a variety of cellular receptors.
Psychiatric/PsychologicalDisorders
PETER HASSMEN
Department of Psychology, Umea University, Umea,
Sweden
SynonymsChronic mental illness; Mental disease; Mental disorders;
Mentally ill; Mood disorders
DefinitionSerious mental disorders include major depression,
▶ bipolar disorder, anxiety related disorders, and schizo-
phrenia. The lifetime prevalence of anxiety and depressive
disorders exceeds 30% in some countries; higher
prevalence rates are reported for anxiety than depressive
disorders [1]. Both anxiety and depressive disorders have
been associated with obesity [2]. Most people afflicted
with serious mental disorders display an unhealthy life-
style, which may include a high-fat diet and smoking.
They also tend to be even less physically active than the
general population. This partly explains why the mentally
ill to a higher degree than the general population suffer
from diseases linked to a sedentary lifestyle and obesity,
such as coronary heart disease, diabetes mellitus, hyper-
tension, and certain cancers. A sedentary lifestyle has by
itself been associated with the onset of mental disorders, in
both cross-sectional and prospective longitudinal studies.
The World Health Organization (WHO) estimates
that close to 80% of all cardiovascular diseases afflicting
people can be prevented by physical activity, a well-
balanced diet, and smoking cessation. Corresponding sta-
tistics are not available for mental disorders, although
WHO estimate that they in the year 2020 will account
for 15% of the total burden of disease. In addition –
and more importantly – WHO states that the principal
cause of Years Lived with Disability is mental illness.
Pathogenetic MechanismsIn studies comparing concordance rates between twins, it
has been shown that heritability for mental disorders
varies; it is higher for bipolar disorder and schizophrenia
than for anxiety disorders and major depression [3]. The
latter have to a higher degree been associated with external
traumatic events and chronic mental stress. A number of
viable hypotheses have been suggested to explain the onset
of depression, including the ▶monoamine-deficiency
hypothesis (increased uptake of noradrenaline and
▶ serotonin by presynaptic neurons causes depression).
The ▶ hypothalamic-pituitary-cortisol hypothesis more
directly links depression to chronic mental stress. Release
of corticotropin-releasing hormone ultimately releases cor-
tisol into the bloodstream; elevated cortisol levels have been
observed in patients with depression [4]. By increasing the
level of monoamines in the synapse by antidepressant
treatment, some of the long-term effects of stress can be
reversed, potentially by affecting the hypothalamic-pitui-
tary-adrenal axis.Whether this can explain that antidepres-
sants in some studies also seem to be effective for a number
of stress related disorders, such as panic disorder, post-
traumatic stress disorder, and ▶ obsessive-compulsive
disorder, has not been conclusively determined [3].
▶Psychotropic drugs may be necessary in the acute
treatment phase, but somemore than others are associated
with subsequent weight gain. Known associations between
stress – either acute or chronic – mental disorders, and

Psychiatric/Psychological Disorders P 735
P
weight gain also suggest that regularly performed exercise
may offer a solution by its stress- and weight-reducing
effects. Chronic exercise produces both ▶ anxiolytic and
antidepressant effects; possibly by promoting mechanisms
such as upregulation of brain-derived neurotrophic factor,
increased central noradrenaline neurotransmission, and
synthesis and metabolism associated with the neurotrans-
mitter serotonin [5]. The central nervous system is nega-
tively affected by oxidative stress, and has been identified
in the pathogenesis of mood disorders [6]. The antioxi-
dant effects of exercise on the brain may explain why
mood improvements occur.
Exercise InterventionAmong acute effects, the anxiolytic effect associated
with exercise has been highlighted in the literature.
Improvements of cognitive functions and reduction of
depressive symptoms have also been described. Apart
from biological explanations, a number of psychological
explanations are offered, such as improvements stemming
from enhanced self-esteem and improved ▶ self-efficacy.
Regularly performed exercise, in combination with
a healthy diet and cessation of smoking, reduces the risk
for premature death related to cardiovascular disease,
hypertension, and diabetes type 2. It also reduces the risk
for recurrent depressive episodes, alleviates stress and
enhances overall wellness.
The fact that people suffering from serious mental
illness are less physically active than the general population
can be related to psychosocial factors such as low self-
esteem and self-efficacy, the lack of social support, fatigue,
and lack of motivation. Also fear of falling is a barrier to
exercise as balance issues and postural instability has been
associated with for example schizophrenia. When serious
mental illness is combined with ▶ obesity, cardiovascular
risk factors, and a sedentary behavior, it is necessary to
initiate an exercise program with caution and in close col-
laboration with health professionals. On the upside, many
psychiatric patients express an interest in exercise [7].
Walking is by far the most used and recommended
form of exercise. For sedentary people, possibly suffering
from physical health issues in combination with mental
illness, a low-impact, low-intensity exercise can indeed be
recommended. As previously mentioned, lack of social
support is frequently mentioned as a barrier to exercise –
and more so in people suffering from mental disorders.
Consequently, by exercising with others, both social sup-
port and the positive effects of social interaction can be
obtained. More recently, leisure as a context for active
living has been investigated. While physical activity
and regularly performed exercise still constitutes a core
component, the concept of active living also incorporates
other aspects enabling people to be actively involved in
their community to recover from or prevent mental illness
to develop [8]. From a mental health perspective, exercise
is but one of many activities with the potential to alleviate
mental health problems.
The question, however, is not whether exercise should
be incorporated or not, the question is rather what other
measures are to be involved when trying to help people
with mental disorders. The biochemical and physiological
benefits of exercise alone speaks for its use to prevent
obesity, cardiovascular disease, etc. However, mental ill-
ness often stems from a complex interplay between genetic
predispositions and environmental factors; regularly
performed exercise may be sufficient for some individuals
whereas others may need additional activities to have
a significant impact on their illness – exercise can then
be considered an adjunct treatment.
The real challenge for health professionals is to con-
vince the mentally ill to become physically active as there
are so many barriers to exercise. Lack of access to facilities,
expensive fitness gear and membership fees, and lack of
knowledge are frequently mentioned in the research liter-
ature. In addition, being “forced” to exercise with others
explains why some people – predominantly those suffering
from body image concerns in addition to anxiety and/or
depression – avoid exercising with others. Thus, somemay
benefit from the social support offered when exercising
together; others may instead avoid all group-exercise pro-
grams. Personal trainers or a buddy system are alternatives
that may offer the advantage of social support and moti-
vation, yet avoid ▶ self-presentational doubts that nega-
tively influence exercise adherence.
In conclusion, physical exercise has a lot to offer
people suffering from seriousmental illness. If commence-
ment, progression, and the physical and social environ-
ment are tailor made to the particular needs of each
individual, few if any adverse side effects will be encoun-
tered and many positive health-related outcomes, both
physiological and psychological, may result.
Cross-References▶Depression
References1. Kessler RC, Angermeyer M, James C et al (2007) Lifetime prevalence
and age-of-onset-distributions of mental disorders in the World
Health Organization’s world mental health survey initiative. World
Psychiatry 6:168–176
2. de Wit LM, Fokkema M, van Straten A, Lamers F, Cuijpers P, Penninx
BWJH (2010) Depressive and anxiety disorders and the associationwith
obesity, physical and social activities. Depress Anxiety 27:1057–1065
736 P Psychotropic Drugs
3. Belmaker RH, Agam G (2008) Major depressive disorder. N Engl J
Med 358:55–68
4. Burke HM, Davis MC, Otte C, Mohr DC (2005) Depression and
cortisol responses to psychological stress: a meta-analysis.
Psychoneuroendocrinology 30:846–856
5. Duman CH, Schlesinger L, Russell DS, Duman RS (2008) Voluntary
exercise produces antidepressant and anxiolytic behavioral effects in
mice. Brain Res 1199:148–158
6. Raison CL, Capuron L, Miller AH (2006) Cytokines sing the blues:
Inflammation and the pathogenesis of depression. Trends Immunol
27:24–31
7. Ussher M, Stanbury L, Cheeseman V, Faulkner G (2007) Physical
activity preferences and perceived barriers to activity among persons
with severe mental illness in the United Kingdom. Psychiatr Serv
58:405–408
8. Iwasaki Y, Coyle CP, Shank JW (2010) Leisure as a context for active
living, recovery, health and life quality for persons with mental illness
in a global context. Health Promot Int 25:483–494
Psychotropic Drugs
A generic term for all drugs affecting the mind, such as
lithium and selective serotonin reuptake inhibitors –
SSRIs – (for depression). Also illicit drugs, such as cocaine
and LSD (Lysergic acid diethylamide), are p-sychotropic.
Pulmonary System Adaptations
▶Pulmonary System, Training Adaptation
Pulmonary System DuringExercise
▶Pulmonary System, Performance Limitation
Pulmonary System Limitations toExercise Performance
▶Pulmonary System, Performance Limitation
Pulmonary SystemMaladaptations
▶Pulmonary System, Training Adaptation
Pulmonary System, PerformanceLimitation
HANS CHRISTIAN HAVERKAMP
Department of Environmental and Health Sciences, JSC
Hodgepodge, Johnson State College, Johnson, VT, USA
SynonymsExercise capacity; Exercise ventilation; Exercise-Induced
Airway Dysfunction; Limitations to exercise capacity;
Pulmonary system during exercise; Pulmonary system
limitations to exercise performance
DefinitionThe physiologic variable that has the greatest impact upon
aerobic exercise performance is maximal oxygen con-
sumption, also known as maximal aerobic capacity or
power (▶VO2max) [1]. Moreover, inasmuch as exercise
performance is a difficult “variable” to assess and assign
a value, it is common practice to use VO2max as a surro-
gate for exercise performance. Maximal aerobic capacity is
the maximum volume of O2 that can be utilized by the
body during exercise; it is the maximal volume of oxygen
that can be processed per minute by the electron transport
chain in the mitochondria. Maximal aerobic capacity is
reported in either absolute terms (liters O2�min�1) or
relative to body mass (ml O2�kg�1�min�1).
Maximal aerobic capacity is assessed during a graded
exercise test to exhaustion. These tests, usually completed on
a treadmill or cycle ergometer, require patients to exercise at
increasingly higher work rates until they are no longer able
to continue; the highest oxygen consumption (VO2)
achieved during the exercise is their VO2max. Pulmonary
minute ventilation is assessed with a pneumotachometer
and the exhaled gas is analyzed for concentrations of
oxygen and carbon dioxide (CO2); these data are then
used to calculate VO2 and metabolic carbon dioxide pro-
duction (VCO2). True VO2max is achieved when an
increased work rate is not accompanied by an increase in
VO2. In patients with lung disease, however, breathing
discomfort or muscular weakness often causes cessation
of exercise prior to achieving ▶VO2max. In these cases,
the value is reported as the symptom-limited VO2max.
CharacteristicsWhole-body oxygen consumption is the total volume of
O2 that is processed per minute by the electron transport
chain in the mitochondria. Oxygen consumption is thus
the final physiologic outcome of a pathway of travel for O2

Pulmonary System, Performance Limitation P 737
from the environment to the mitochondria – a pathway
that requires multiple physiologic processes (Fig. 1). Max-
imal oxygen consumption arises because one or more of
these processes achieves its maximal working capacity.
A brief discussion of these processes follows, with chief
emphasis placed on the components related to the pulmo-
nary system. Following this discussion, the role of the
pulmonary system in determining exercise performance
will be discussed.
As seen in Fig. 1, ventilation of the alveoli with
inspired gas is the first step along the O2 transport path-
way. Alveolar ventilation (VA) is determined by minute
ventilation (VE) – the product of breathing frequency (fb)
and tidal volume (VT) – and dead space ventilation (VD),
2
1
VE
VA
3
Airways
Lungs
Blood -gasbarrier
Circulation
Muscle
4
5
Mitochondria
O2
O2
O2
O2
O2O2
CO2
CO2
CO2
CO2
CO x O2content
Pulmonary System, Performance Limitation. Fig. 1
Schematic representation of the pathway of travel for O2 from
the environment to the skeletal muscle mitochondria. Oxygen
consumption is the final physiologic outcome of inspired O2
completing this pathway. This pathway of travel includes the
following steps: Step 1, ventilation of alveoli with inspired gas
from the atmosphere; Step 2, diffusion of O2 across the
alveolar-capillary membrane; Step 3, conductive transport of
O2 to working skeletal muscle by the circulatory system;
Step 4, diffusive transfer of O2 from capillaries to the skeletal
muscle; Step 5, processing of O2 by mitochondria in
skeletal muscle. VEminute ventilation, VA alveolar ventilation,
CO cardiac output, CO2 carbon dioxide
P
which is the portion of VT that does not participate in gas
exchange at the alveolar level. In healthy people, the
majority of VD is equal to the volume of the conducting
airways. In patients with pulmonary disease, however,
pathology in lung structure and alterations in lung
mechanical behavior can lead to increases in VD. This
decreased efficiency for ventilation necessitates propor-
tionately greater increases in VE to maintain arterial
blood gas homeostasis in individuals with an already
compromised capability for increasing ventilation.
During exercise, VA must increase in proportion to the
increased VO2 and VCO2 or arterial blood levels for O2
and CO2 will decrease and increase, respectively. The lungs
thus provide the first line of defense for blood gas homeo-
stasis by maintaining adequate values for alveolar PO2 and
PCO2 (PAO2 and PACO2).
The passive diffusion of oxygen across the alveolar and
pulmonary capillary membranes is the second step along
the O2 transport pathway. The adequacy of diffusion is
assessed by the equilibration for O2 between the alveoli
and the pulmonary capillary blood; an identical PO2 in the
alveoli and pulmonary capillaries represents perfect gas
exchange. Even in health, however, there is a difference in
PO2 between the alveoli and pulmonary capillaries
(�5 mmHg at rest), known as the alveolar-to-arterial
PO2 difference (AaDO2). At rest, the AaDO2 is due to an
imperfect matching of alveolar ventilation and perfusion
within the lungs. The AaDO2 increases progressively
during exercise to values of �20 mmHg at VO2max in
the healthy adult, reflecting a work-rate-dependent
decrease in the efficiency for pulmonary gas exchange.
After O2 has diffused across the alveolar-capillary
membrane and bound with hemoglobin, it must be
transported to the exercising muscle. The conductive
transport of oxygen by the circulatory system is the third
step along the O2 transport system. The amount of O2
transported by the cardiovascular system is determined by
cardiac output, which is the product of heart rate and
stroke volume, and by the O2 content of the arterial
blood, as determined by the hematocrit and the slope of
the oxyhemoglobin-dissociation curve.
The fourth step along the O2 transport pathway is the
diffusive transfer of O2 from the capillaries to the muscle
cells. Capillary cross-sectional area and diffusion distance
between the capillaries and muscle cell membranes
are important determinants of this process. Due to the
extremely low PO2 located within muscle mitochondria
(�2 mmHg), the diffusion of O2 to the muscle cells is not
normally thought to limit exercise capacity.
In the final step along the pathway for O2 transport
and utilization, O2 is processed within the mitochondria

738 P Pulmonary System, Performance Limitation
at the end of the electron transport chain. The maximal
volume of O2 that can be processed by the mitochondria is
a function of mitochondrial volume and the amount
of aerobic enzymes located within the active skeletal
muscle.
Pulmonary System as a Determinant ofVO2maxAs discussed above,▶VO2max is determined by the func-
tioning of several physiologic processes – arranged in
series – involved with the intake, transport, and utilization
of O2 by the body. Theoretically, any one of these processes
could reach its maximal working capacity before the
others have reached theirs, and it would thus become the
principle factor determining VO2max.
In the healthy person, the major physiologic factor
limiting VO2max is the capacity of the cardiovascular
0.0
a b
0.5 1.0 1.5 2.0 2.5 3.0 3.5
PO
2 (m
mH
g)
70
80
90
100
110
120
PaC
O2
(mm
Hg)
30
32
34
36
38
40
42
Arterial PO2
Alveolar PO2
Arterial PCO2
Oxygen Consumption (L/min)
Ven
tilat
ion
(L/m
in)
0
40
80
120
160
200
0.16
0.20
0.24
0.28
0.32
0.36Minute VentilationAlveolar VentilationVD/VT
Normally Trained
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5
VD/V
T
Pulmonary System, Performance Limitation. Fig. 2 Characteris
exercise of increasing intensity to maximum (a) and for a subset o
hypoxemia (b). Note the significantly higher maximal oxygen con
trained, arterial blood levels for O2 are maintained while arterial C
during exercise. In the highly trained, arterial PO2 is decreased co
(minimal decrease in arterial PCO2) during the exercise. PO2 partia
VD/VT ratio of dead space ventilation to tidal volume
system to transport oxygen to the working muscle [1].
Thus, cardiac output reaches its maximum before the
metabolic machinery of skeletal muscle reaches its maxi-
mal O2 processing capacity and well before the maximal
capacity for ventilation and pulmonary gas exchange has
been reached.
Figure 2a depicts the exercise responses in a healthy,
normally trained person for several physiologic variables
that are determined by the functioning of the pulmonary
system. The maintenance of PaO2 and the decreased
PaCO2 during exercise at VO2max provides the ultimate
evidence that the pulmonary system has not reached its
maximal capacity for ventilation and gas exchange. There-
fore, the pulmonary system does not impose an important
limitation to VO2max in the healthy adult.
In general, the pulmonary system might become the
limiting factor for VO2max in two populations: (1) in
Highly Trained
PO
2 (m
mH
g)
70
80
90
100
110
120
PaC
O2
(mm
Hg)
30
32
34
36
38
40
42
Arterial PO2
Alveolar PO2
Arterial PCO2
Oxygen Consumption (L/min)
0 1 2 3 4 5
0 1 2 3 4 5
Ven
tilat
ion
(L/m
in)
0
40
80
120
160
200
0.16
0.20
0.24
0.28
0.32
0.36Minute VentilationAlveolar VentilationVD/VT
VD/V
T
tic exercise responses in normally trained humans during
f highly trained athletes that develop exercise-induced arterial
sumption in the highly trained athletes. In the normally
O2 is decreased due to a compensatory hyperventilation
mmensurate with a minimized hyperventilatory response
l pressure of oxygen, PaCO2 partial pressure of carbon dioxide,

VE 169 I/min
152 I/min
117 I/min
73 I/min50 I/min
1234567
Flo
w R
ate
(L/s
)
12
8
4
0
4
8
12
A
32 yr
Volume (L)
Pulmonary System, Performance Limitation. Fig. 3
Spontaneous exercise flow-volume loops (eFVL) during
exercise of increasing intensity plotted within the maximal
volitional flow-volume loop (MFVL) from a highly trained male
endurance athlete. At �117 L/min, the expiratory limb of the
eFVL begins to overlap with that of the MFVL. This is known as
expiratory flow limitation, and indicates that the subject has
reached (or nearly reached) his maximal ability to generate
expiratory airflow as dictated by the mechanical properties
of his airways. As exercise intensity increases further,
end-expiratory lung volume begins to increase toward resting
levels, heralding dynamic hyperinflation and increased elastic
work of breathing
Pulmonary System, Performance Limitation P 739
P
the extremely fit aerobic athlete, or (2) in those with
pulmonary disease (discussed under Clinical Relevance).
Pulmonary System and Exercise Performance in the
Highly Trained Athlete. In a significant number of highly
trained male and female athletes, PaO2 decreases during
high-intensity exercise (Fig. 2b). This indicates that the
substantial reductions in both venous blood O2 content
and pulmonary capillary transit time during exercise have
overwhelmed the individual’s capacity for ventilation and
pulmonary gas exchange to fully oxygenate pulmonary
capillary blood. In the majority of these cases, arterial
hypoxemia occurs concomitantly with a minimized
hyperventilatory response (i.e., minimal decrease in
PaCO2), which is a crucial compensatory mechanism for
maintaining arterial blood oxygenation during exercise.
The insufficient exercise ventilation is due to the fact that
highly trained athletes can approach or even reach their
maximal limits for generating expiratory flow during
exercise. The maximal limits for expiratory flow are deter-
mined by the mechanical properties of the airways,
lungs, and chest wall, and are described by the maximal
volitional flow-volume envelope (MFVL) (Fig. 3). In
highly trained athletes that reach very high ventilation
rates during exercise, the exercise tidal flow-volume
loops can approach or intersect the boundaries formed
by the MFVL. This is known as expiratory flow-limitation
(EFL), and essentially represents a mechanical
limit to expiration during exercise [2]. Furthermore, due
to the smaller airways and lung volumes in females com-
pared to males, EFL is more prevalent in the female athlete
[3]. Thus, in females, EFL occurs at much lower ventila-
tion rates and exercise workloads than in male
counterparts.
The AaDO2may also widen excessively during exercise
in the highly trained athlete (see Fig. 2b). This indicates a
lack of equilibration for O2 between alveoli and the pul-
monary capillaries. At very high metabolic rates,
a worsened matching of alveolar ventilation with pulmo-
nary capillary perfusion and a greatly shortened pulmo-
nary capillary red blood cell transit time both contribute
to the widened AaDO2. Insufficient pulmonary capillary
transit time becomes a factor when cardiac output con-
tinues to increase after pulmonary capillary blood volume
has reached its maximal value. In fact, maximal cardiac
output can reach 40 L/min in the trained male athlete,
which results in a pulmonary capillary transit time of only
�0.40 s. Thus, in some highly trained male and female
endurance athletes, excessive gas exchange inefficiency in
the face of an insufficient compensatory hyperventilation
can become an important limitation to VO2max. Indeed,
preventing a decreased SaO2 by inhalation of a hyperoxic
gas during exercise increases VO2max and time-to-
exhaustion during constant load exercise [4]. Moreover,
preventing arterial hypoxemia also reduces peripheral
muscle fatigue following exhaustive exercise [4].
In health, then, the lungs may become the limiting
factor to VO2max and exercise performance in the highly
trained aerobic athlete who has developed a great capacity
for transporting oxygen throughout the cardiovascular
system and processing oxygen within the working skeletal
muscles. This is because the lungs and pulmonary system,
unlike the cardiovascular and muscular systems, do not
adapt to exercise training; the pulmonary system can thus
become the weak link in the O2 transport pathway.
Clinical RelevanceThere are several clinical conditions in which the pulmo-
nary system is likely to be the primary organ system
responsible for limiting exercise capacity. In each of these

740 P Pulmonary System, Performance Limitation
cases, derangements in the mechanical properties of
the airways and lung parenchyma compromise the
ability to increase ventilation during exercise. Further-
more, altered lung mechanical function may lead to
inefficient gas exchange, which increases the requirement
for VE in those with an already compromised capacity
for doing so.
Chronic Obstructive Pulmonary Disease. The primary
pathologic change in lung structure in COPD is destruc-
tion of the lung parenchyma and alveoli. Destruction of
these tissues causes reduced lung elastic recoil and
narrowing of the conducting and peripheral airways
during expiration. During exercise, these changes in lung
mechanical function lead to EFL and dynamic compres-
sion of the airways, air trapping, and lung hyperinflation.
Even at rest, however, COPD patients breathe at inflated
lung volumes and with greatly diminished inspiratory and
expiratory reserve volumes. Given this limited
capacity for increasing ventilation, patients with COPD
have a correspondingly limited capacity for meeting the
increased metabolic rate of exercise. The ratios of tidal
volume to both inspiratory capacity (which defines the
maximum possible tidal volume) and vital capacity far
exceed those reached in normal subjects, and the
elastic work of breathing is greatly increased during exer-
cise. Consequently, exercise in the COPD patient is
accompanied by severe exertional breathlessness (i.e., dys-
pnea) and a limited capacity to increase VE (and VA) in
response to the increased demand caused by exercise. The
extent of these physiologic changes in pulmonary function
depend on the severity of disease, and FEV1.0 values
less than 2.0 L are common in patients with moderate-
to-severe disease [5]. Thus, the capacity for increasing
ventilation is limited in patients with COPD,
which greatly compromises their ability to meet the chal-
lenges of exercise. Furthermore, VD is increased in COPD,
which equates to an increased requirement for total
ventilation in those with a greatly compromised ability
to do so.
Bronchial Asthma. Bronchial asthma is a pathologi-
cally, symptomatically, and phenotypically diverse condi-
tion. The primary pathology of the disease, however, is
inflammation of the tracheobronchial tree. In asthmatics,
the sequelae of airway inflammation causes the airways
to become hypersensitive to a variety of inhaled agents
(e.g., antigens such as animal dander, pollens, and molds,
and chemical agents) and a variety of other stimuli includ-
ing exercise and cold, dry air. Furthermore, variable and
potentially chronic changes in the structure of the airways
also occurs in asthma; the changes in airway structure lead
to a thickened airway wall with increased potential for
causing airway narrowing and breathing difficulties.
Thus, a variable airflow limitation and variable decreases
in pulmonary function are seen in asthmatic patients.
In the asthmatic, narrowed airways decrease the size of
the maximal flow-volume envelope, which limits the
capacity to increase ventilation during exercise (Fig. 4).
Thus, asthmatics are more likely to encroach on their
maximal flow-volume envelope at much lower metabolic
rates than healthy counterparts [6]. When this occurs, EFL
and dynamic hyperinflation will develop. In asthma, then,
the narrowed airways may limit ventilatory capacity to
such an extent that VA is insufficient to maintain PaO2
during moderate-to-severe exercise. Moreover, the airway
narrowing in asthma causes a heterogeneous distribution
for alveolar ventilation, which decreases the efficiency of
pulmonary gas exchange and leads to a widened AaDO2.
As in COPD, this essentially increases the VE necessary to
maintain oxygenation of arterial blood in a population
that is already under mechanical constraint to increase
ventilation.
The Aged Athlete. Healthy aging causes two major
changes in lung structure that result in both a reduced
capacity for ventilation and a decreased efficiency for gas
exchange within the lung [7]. Although these changes in
lung structure begin in early adulthood, they do not begin
to significantly influence exercise ability until the fifth
decade. The first change in lung structure with aging is
a gradual deterioration of the parenchymal tissues of the
lung, which causes reduced elastic recoil. Reduced elastic
recoil leads to excessive airway narrowing during forced
expiration, a “scooped” expiratory limb of the MFVL,
airway closure at higher lung volumes compared to the
young, and a decrease in the size of the MFVL. Conse-
quently, EFL is reached at lower exercise workloads and
ventilation rates than in healthy young adults. Further-
more, the EFL leads to dynamic hyperinflation and
a concomitant increase in the elastic work of breathing.
Thus, as in the COPD patient, the elderly athlete has
a compromised ability to increase ventilation during
exercise.
A second change in lung structure that occurs with
normal aging is a decrease in the number of alveoli and in
the total alveolar-capillary diffusion surface area. This
decrease in surface area for diffusion, in combination
with a more heterogeneous distribution of alveolar venti-
lation and increased deadspace:tidal volume in the aged
lung, causes a decreased efficiency for gas exchange. Thus,
the AaDO2 is increased at rest and during exercise in the
healthy elderly person. Again, in a situation similar to that
in the COPD patient, the increased AaDO2 in combina-
tion with a limited capacity for increasing ventilation can

PaO
2 (T
orr)
72
76
80
84
88
PaC
O2
(Tor
r)
36
38
40
42
44
46
48
PaO2
PaCO2
pH
7.24
7.28
7.32
7.36
7.40
Lact
ate
(mm
ol)
0
2
4
6
8
10
pHLactate
SaO
2 (%
)
88
90
92
94
96
98
Volume (L)
Flo
w (
L/se
c)
−8
−6
−4
−2
0
2
4
6
8
55 L/min
74 L/min
81 L/min
81 L/min
94 L/min
Rest Warmup
Constant Load Exercise90% VO2 max
−8 −7 −6 −5 −4 −3 −2 −1
1 3 5 7 9
Pulmonary System, Performance Limitation. Fig. 4 Exercise data in a 37 year male with bronchial asthma. Note the “scooped”
expiratory limb of themaximal flow-volume loop and the significant expiratory flow-limitation and dynamic hyperinflation during
the exercise. Arterial PO2 decreased to 72 mmHg and arterial PCO2 increased to 46 mmHg during the exercise, indicating an
insufficient ventilatory response to the exercise. The arterial hypoxemia and acidosis combined to cause a significant decrease in
oxyhemoglobin saturation. PaO2 arterial oxygen pressure, PaCO2 arterial carbon dioxide pressure, SaO2 arterial oxyhemoglobin
saturation
Pulmonary System, Training Adaptation P 741
P
result in arterial hypoxemia during exercise in the agedathlete. Thus, in the elderly but healthy athlete, normal,
age-related decrements in lung function cause decreased
efficiency for gas exchange and a limited capacity for
increasing ventilation during exercise.
References1. Di Prampero PE (2003) Factors limiting maximal performance in
humans. Eur J Appl Physiol 90:420–429
2. Johnson BD, Saupe KW, Dempsey JA (1992) Mechanical constraints
on exercise hyperpnea in endurance athletes. J Appl Physiol
73:874–886
3. Sheel WA, Guenette JA (2008) Mechanics of breathing during
exercise in men and women: sex versus body size differences? Exerc
Sports Sci Rev 36:128–134
4. Romer LM, Haverkamp HC, Lovering AT, Pegelow DF, Dempsey JA
(2006) Effect of exercise-induced arterial hypoxemia on quadriceps
muscle fatigue in healthy humans. Am J Physiol Regul Integr Comp
Physiol 290:R365–375
5. O’Donnell DE, LamM,Webb KA (1998)Measurement of symptoms,
lung hyperinflation, and endurance during exercise in chronic
obstructive pulmonary disease. Am J Resp Crit Care Med
158:1557–1565
6. Haverkamp HC, Dempsey JA, Miller JD, Romer LM, Pegelow DF,
Rodman JR, Eldridge MW (2005) Gas exchange during exercise in
habitually active asthmatic subjects. J Appl Physiol 99:1938–1950
7. Dempsey JA,Miller JD, Romer LM (2006) The respiratory system. In:
Tipton CM, SawkaMN, Tate CA, Terjung RL (eds) ACSM’s advanced
exercise physiology, 1st edn. Lippincott Williams and Wilkins,
Baltimore, pp 246–299
Pulmonary System, TrainingAdaptation
HANS CHRISTIAN HAVERKAMP
Department of Environmental and Health Sciences, JSC
Hodgepodge, Johnson State College, Johnson, VT, USA
SynonymsAirway inflammation; Bronchial hyperresponsiveness;
Exercise training; Exercise-induced airway dysfunction;
Pulmonary system adaptations; Pulmonary system
maladaptations

742 P Pulmonary System, Training Adaptation
Definition▶ Exercise training refers to habitual engagement in
dynamic, whole-body exercise consisting of repeated
skeletal muscle contractions and significantly increased
metabolic rate. Examples include jogging/running, hiking,
road or mountain cycling, rowing, and cross-country
skiing. A variety of other physical activities are also
relevant, however, such as ▶ soccer, ice hockey, figure
skating, field hockey, and speed skating, among others.
Thus, any activity that requires significantly increased
metabolic and ventilation rates for extended periods of
time during training or competition may be regarded as
germane to this discussion. A key point for this chapter is
that any chronic adaptations or ▶maladaptations to the
airways and lungs with exercise training occur due to
repeated increases in pulmonary ventilation with training.
Mechanisms and Exercise Response
Pulmonary System Adaptations to ExerciseTraining in the Healthy AdultThe cardiovascular and neuromuscular systems undergo
well-known ▶ adaptations to chronic exercise training
that result in a greatly improved capacity for transporting
and utilizing oxygen. These adaptations lead to increased
maximal aerobic power and increased exercise capacity.
Conversely, the pulmonary system does not appear to
undergo significant beneficial adaptations to chronic
exercise training.
Many important indices of pulmonary system struc-
ture and function remain unchanged after endurance exer-
cise training. Lung diffusion surface area and diffusion
capacity, and pulmonary capillary blood volume do not
adapt to endurance training. Static lung volumes and the
size of the maximum flow-volume envelope are also unaf-
fected by exercise training [1]. Thus, exercise training does
not appear to stimulate lung growth or cause other positive
adaptations in the capacity of the airways and lungs to take in
and exchange oxygen across the alveolar-capillary membrane.
Why do the lung parenchyma and airways remain
unchanged with exercise training? The lungs do adapt to
several types of chronic stress, such as chronic ▶ hypoxia,
lung pneumonectomy, and caloric imbalance [2]. Thus,
the lack of response to exercise training is not due to an
inability of the lungs to remodel in response to chronic
stress. Furthermore, well-trained athletes can develop
arterial hypoxemia and expiratory flow-limitation during
whole-body exercise, and strenuous exercise can cause
diaphragmatic fatigue in both trained and untrained
subjects. Therefore, the demands placed on the pulmonary
system by exercise can be of a magnitude that surpasses the
structural and functional capacities of the system. It might
be the case that the intermittent nature of the exercise
stress is not of sufficient magnitude to elicit compensatory
adaptations by the airways and lung parenchyma. An
alternative possibility – and one with supportive data –
is that chronic exercise is damaging to airway structure
and function (discussed below); any deleterious effects
of exercise might thus derail the possible beneficial effects
of exercise on lung structure.
A likely exception to the general nonresponsiveness of
pulmonary system structure to exercise training is in the
competitive swimmer. Lung volumes tend to be larger
in swimmers compared to the general population, and
longitudinal data suggests that lung volumes and diffusion
capacity increase during the course of a competitive train-
ing program [3]. The increased lung volumes with swim
training may be related to the repeated inspirations to
total lung capacity required in swimming. Exaggerated
inflation of the lungs might lead to an improved ability
to contract the inspiratory muscles or alter inhibitory
neural feedback from lung afferents at high lung volumes.
Pulmonary System Maladaptations toExercise Training in the Healthy AdultIn contrast to the adaptive effects of exercise training
on cardiovascular and muscular system structure and
function, a variety of evidence suggests that exercise train-
ing may be detrimental to airway and lung parenchymal
structure and function.
The prevalence of asthma and bronchial hyperrespon-
siveness (BHR) to exercise are higher in trained athletes
compared to the general population [4]. Both summer
and winter athletes exhibit an increased prevalence of
BHR, but cold weather athletes appear to be especially
susceptible. Additionally, inflammatory cells are increased
in and around the airways of endurance athletes [5].
Furthermore, altered airway structure similar to that
seen in asthma (i.e., airway remodeling) has been shown
in elite cross-country skiers [6]; this includes an increased
subepithelial collagen deposition and increased thickness
of the subepithelial layer.
As shown in Fig. 1, the mechanisms linking exercise
training with airway and lung pathophysiology are likely
related to the sequellae of ventilation of large volumes of air
during exercise, which causes dehydration and altered
osmolarity of the airway surface. The airway fluid imbal-
ances are thought to lead to a cascade of cellular events that
stimulate release of an array of inflammatory mediators
from resident (i.e., epithelium and airway smooth muscle)
and nonresident (i.e., mast cells and eosinophils) airway
cells [7]. Acutely, these mediators would trigger increased

↑ Allergens
Outdoors Indoors
Pool,chlorine derivatives
BV
↑↑ Pollutants↑ Cold/dry air Ice Rink,
particulate matterASM
Inflammatorycells
Plasmaexudation
Contractionand hypertrophy EOS
Edema
EC GC Inflammatorymediators
Mucinrelease
MC
InflammatoryMediators
Airway Wall
↑ ↑ osmolarity
Chemotacticagents
VE•
↑ VE•
EC Epithelialshedding
Epithelialdamage
Airwayremodeling
↑ collagen
InflammatoryResponse
Repeated damageand repair
Pulmonary System, Training Adaptation. Fig. 1 Increased ventilation (and airflow) during exercise causes a relative
dehydration and increased osmolarity of the airway surface. Inflammatory mediators are released from resident (i.e., epithelial)
and nonresident (e.g., eosinophils and mast cells) airway cells (when present) as a consequence of cellular events that take place
to restore water balance. These mediators (e.g., histamine, leukotrienes, prostaglandins) stimulate mucin release, contraction
of airway smooth muscle, plasma exudation, and recruitment of inflammatory cells. Increased airflow during exercise might also
damage the airway epithelium, leading to a further inflammatory response and subsequent restorative processes. In the trained
athlete who regularly achieves high ventilation rates, these insults to the airways are recurrent and are thought to cause
remodeling of airway structure (i.e., increased subepithelial collagen and increased smooth muscle mass) and sensitization of
airway smoothmuscle. ASM airway smoothmuscle, BV blood vessel, EC epithelial cell, EOS eosinophil, GC goblet cell,MCmast cell,
V�E minute ventilation
Pulmonary System, Training Adaptation P 743
P
capillary permeability and plasma exudation, mucus
hypersecretion, contraction of airway smooth muscle,
and recruitment of inflammatory cells into the airways.
Injury to the airway epithelium is also a likely consequence
of high-intensity exercise [8]; this would further contrib-
ute to the airway inflammatory response. In those who
exercise regularly, the net result of these repetitive inflam-
matory and injurious stimuli might be sensitization of
airway smooth muscle, remodeling of the airways, and
BHR to exercise and other stimuli.
Finally, in athletes who regularly achieve high ventila-
tion rates, exposure of the airways to harsh environmental
conditions and noxious inhalants may further contribute
to altered airway structure and function. During exercise,
inhalation of cold and dry air, environmental pollutants
and irritants (e.g., ozone, vehicle exhaust, particulate
matter in ice rinks, chlorine derivatives in pools),
and allergens might exacerbate the inflammatory-based
sequellae described above. For the atopic athlete,
exercise increases exposure to airborne allergens manifold.
Thus, in contrast to the cardiovascular and muscular
systems, the pulmonary system is continually exposed to
a variety of external conditions and inhaled agents that
may cause damage to the airway tree.

744 P Pulmonary Ventilation
Pulmonary System Responses to ExerciseTraining in the Asthmatic PatientIn contrast to the primarily maladaptive effects of exercise
training on the pulmonary system in healthy humans,
some evidence suggests that moderate exercise training
may improve airway function in asthmatic patients. In
human asthmatics, moderate exercise training decreases
asthma symptoms, improves aerobic fitness and exercise
capacity, and improves dyspnea during exercise [9].
Recent evidence also suggests that regular exercise might
improve both nonspecific BHR and EIB, at least in children
[10]. The majority of studies, however, have failed to
show a beneficial effect of exercise on BHR. Moreover,
there are no reports of improved (i.e., decreased) airway
inflammation in response to an exercise program. Given
the pro-inflammatory nature of exercise on the airways in
non-asthmatic humans, it is likely that the improvements
in clinical symptoms are related to improved aerobic
fitness and decreased exercise ventilation after training
rather than to improvements in airway pathophysiology.
In any case, collectively, studies have convincingly shown
that exercise training in mild-to-moderate asthmatic
patients is beneficial for asthma symptoms and quality
of life, and that asthmatics respond to exercise training
similarly to non-asthmatics.
Interestingly, in mice with ovalbumin-induced
asthma, exercise training clearly decreases pulmonary
inflammation and reduces airway remodeling [11].
These findings are difficult to reconcile with the findings
in human asthmatics, which have failed to show improved
airway inflammation with training. There are many
possibilities for these discrepant findings, including
differences in the inflammatory stimuli, differences in
the systemic immune response to exercise, or differences
in the exercise stimulus.
ConclusionsExercise training appears to be largely deleterious to
pulmonary system structure and function. This stands in
stark contrast to the beneficial effects of exercise on
cardiovascular and muscular system function. Given that
the pulmonary systemmaladaptations are likely due to the
sequellae of increased airflow during exercise, the extent of
these maladaptations are apt to be related to the regularity
and intensity of training; thus, highly-trained athletes are
more likely to experience these maladaptations. In asth-
matic patients, exercise training improves aerobic capac-
ity, quality of life, and asthma symptoms. To date, there is
minimal evidence that training in asthmatics has a positive
effect on airway inflammation or BHR. Moreover, the
exercise stimulus (i.e., workload and frequency) in studies
investigating training responses in asthmatic subjects has,
understandably, been significantly lower than the training
stimulus in trained athletes. Elucidation of the relation-
ships between training and airway function in asthmatics
is an important area for future investigation.
AcknowledgementI would like to express immeasurable thanks to Dr. Jerome
Dempsey for his constant and ongoing support of my
career, for the many opportunities this support has
afforded me, and for expecting nothing but the best
from my (our) work.
References1. Dempsey JA, Miller JD, Romer LM (2006) The respiratory system.
In: ACSM’s advanced exercise physiology, 1st edn. Lippincott, Wil-
liams and Wilkins, Baltimore, pp 246–299
2. Green D, Naylor L, George K et al (2008) Physiological bases of human
performance during work and exercise. In: Taylor N, Groeller H (eds)
Cardiovascular and pulmonary adaptations to endurance training.
Churchill Livingstone, Edinburgh/New York, pp 49–70
3. Mickleborough TD, Stager JM, Chatham K, Lindley MR, Ionescu AA
(2008) Pulmonary adaptations to swim and inspiratory muscle
training. Eur J Appl Physiol 103:635–646
4. Fitch KD, Sue-Chu M, Anderson SD et al (2008) Asthma and the
elite athlete: summary of the international Olympic committee’s
consensus conference, Lausanne, Switzerland January 22–24, 2008.
J Allergy Clin Immunol 122:254–260
5. Bonsignore MR, Morici G, Vignola AM et al (2003) Increased airway
inflammatory cells in endurance athletes: what do they mean? Clin
Exp Allergy 33:14–21
6. Karjalainen EM, Laitinen A, Sue-Chu M et al (2000) Evidence
of airway inflammation and remodeling in ski athletes with and
without bronchial hyperresponsiveness to methacholine. Am
J Respir Crit Care Med 161:2086–2091
7. Anderson SD, Kippelen P (2008) Airway injury as a mechanism for
exercise-induced bronchconstriction in elite athletes. J Allergy Clin
Immunol 122:225–235
8. Hallstrand TS, Moody MW, Wurfel MM et al (2005) Inflammatory
basis of exercise-induced bronchoconstriction. Am J Respir Crit Care
Med 172:679–686
9. Lucas SR, Platts-Mills TAE (2005) Physical activity and exercise in
asthma: relevance to etiology and treatment. J Allergy Clin Immunol
115:928–934
10. Bonsignore MR, La Grutta S, Cibella F et al (2008) Effects of exercise
training and montelukast in children with mild asthma. Med Sci
Sports Exerc 40:405–412
11. Pastva A, Estell K, Schoeb TR et al (2004) Aerobic exercise attenuates
airway inflammation in a mouse model of atopic asthma. J Immunol
172:4520–4526
Pulmonary Ventilation
Is the rate at which gas enters or leaves the lungs. It is
defined as tidal volume � respiratory rate [L/min].

Pyrogen P 745
Pulsed Field Gel Electrophoresis
Gel electrophoresis technique with an alternating voltage
gradient which allows to separate very large DNAmolecules.
Pure Fiber
A muscle fiber type containing a single myosin heavy
chain isoform.
Purinergic Receptors
Receptors located in the endothelium and smooth muscle
cells of vasculature and other cell structures that are acti-
vated by nucleotides and nucleosides.
Pyrogen
Any substance, which is capable of causing fever, is
a pyrogen. Febrile illness is induced by pyrogens of infec-
tious agents. Fever is a very important symptom of infec-
tious disease, and a hallmark of the acute phase reaction.
Fever is linked with catabolism, which seems obligatory in
febrile illness, as a lot of energy is needed for fueling the
emergency defense response, which must be run in the
interest of host defense.
P






























