Embed Size (px)
Citation preview

DR G DI PO ITIO
Clin. Pharmacokinet. 25 (4): 274-282, 1993 0312-5963/93/0004-0274/$04.50/0 © Adis International Limited. All rights reserved.
CPK1355
Enalapril Clinical Pharmacokinetics and PharmacokineticPharmacodynamic Relationships An Overview
Robert J. MacFadyen, Peter A. Meredith and Henry L. Elliott Department of Medicine and Therapeutics, Gardiner Institute, Western Infirmary, Glasgow, Scotland
Contents
274 275 275 275 277 279 280 280 281
Summary
Summary I. Pharmacokinetics - A Conventional Summary
1.1 Enalapril 1.2 Enalaprilat
2. Current Pharmacokinetic Approaches 3. Concentration-Effect Relationships 4. Clinical Consequences
4.1 Variable Concentration-Effect Relationships (Dependent on End-Point) 5. Conclusions
The conventional pharmacokinetic profile of the angiotensin converting enzyme (ACE) inhibitor, enalapril, is a lipid-soluble and relatively inactive prodrug with good oral absorption (60 to 70%), a rapid peak plasma concentration (I hour) and rapid clearance (undetectable by 4 hours) by de-esterification in the liver to a primary active diacid metabolite, enalaprilat.
Peak plasma enalaprilat concentrations occur 2 to 4 hours after oral enalapril administration. Elimination thereafter is biphasic, with an initial phase which reflects renal filtration (elimination half-life 2 to 6 hours) and a subsequent prolonged phase (elimination half-life 36 hours), the latter representing equilibration of drug from tissue distribution sites. The prolonged phase does not contribute to drug accumulation on repeated administration but is thought to be of pharmacological significance in mediating drug effects.
Renal impairment [particularly creatinine clearance <20 mlfmin «1.2 L/h)] results in significant accumulation of enalaprilat and necessitates dosage reduction. Accumulation is probably the cause of reduced elimination in healthy elderly individuals and in patients with concomitant diabetes, hypertension and heart failure.
Conventional pharmacokinetic approaches have recently been extended by more detailed descriptions of the nonlinear binding of enalaprilat to ACE in plasma and tissue sites. As a result of these new approaches, there have been significant improvements in the characterisation of concentration-time profiles for single-dose administration and the translation to steady-state. Such improvements have further importance for the accurate integration of the pharmacokinetic and pharmacodynamic responses to enalapril(at) in a concentration-effect model. This model is able to characterise the concentration-effect relationship in individual recipients of the drug and predict the antihypertensive responses to dosage alterations.

Enalapril Kinetic-Dynamic Relationships 275
Therapeutic use of enalapril has recently expanded to include heart failure. In this condition, responses to enalapril may be mediated by different effector systems in different organs and may occur at different concentration ranges to those observed during treatment of hypertension. However, similar concentration-effect analyses are still relevant. After almost 15 years of clinical use, the therapeutic applicability of enalapril continues to expand and detailed pharmacokinetic description of the agent remains an integral component of this expansion.
Enalapril was the second orally active angiotensin converting enzyme (ACE) inhibitor drug to become widely available for therapeutic use. At the time of its introduction, a long duration of action and the lack of a sulfhydryl (-SH) group were presented as the major features which distinguished it from captopril, the first orally active ACE inhibitor. A further differentiating feature is that en alapril is a prodrug.
Enalapril is administered as a maleate salt and is the monoethyl ester of enalaprilat, an active ACE inhibitor which is poorly absorbed (only about 10%) from the gastrointestinal tract. The disposition characteristics of enalaprilat, therefore, constitute the most important aspects of the pharmacokinetic profile of enalapril. However, the pharmacokinetics of enalapril(at) cannot readily be described by conventional criteria. This article focuses upon the current approaches which have sought to characterise the pharmacokinetics of enalaprilat. These approaches take account the inter-relationships involved in the binding of enalaprilat to ACE.
1. Pharmacokinetics - A Conventional Summary l.l Enalapril
Following oral administration, enalapril is rapidly and well absorbed (60 to 70%) from the gastrointestinal tract. Peak plasma concentrations (Cmax) are attained about I hour after drug administration (Vim 1983). After absorption, enalapril is rapidly de-esterified (hydrolysed) by carboxylesterase to form enalaprilat. As a result, plasma concentrations of parent drug are virtually undetectable about 4 hours after administration (Vim 1983; Vim et al. 1982). In humans this metabolic transformation occurs almost exclusively in the liver.
No other metabolites have been detected in humans. The parent drug has an elimination half-life of about 2 hours. Unchanged enalapril and enalaprilat are excreted both in urine and faeces, with the urinary route predominating (Ulm 1983; Ulm et al. 1982).
The oral bioavailability of enalapril is about 53 to 74% (based upon urinary recovery of enalapril and enalaprilat), whereas the bioavailability for enalaprilat is about 36 to 44% when intravenous enalapril is used as the reference standard (Davies et al. 1984a; Irvin et al. 1984; Till et al. 1984). The bioavailability of enalapril is not affected by food (Swanson et al. 1984), but, predictably, is affected by hepatic function. Clearance is reduced only in advanced uncompensated hepatic impairment (Ohnishi et al. 1989).
There is also a chronopharmacological effect, presumably reflecting differential rates of absorption and hepatic function. Evening administration leads to a significant prolongation of time to Cmax (tmax) for enalapril, with apparently no significant consequences for the disposition of enalaprilat (Weisser et al. 1991).
1.2 Enalaprilat
Following biotransformation of enalapril, the tmax for enalaprilat is about 3 to 4 hours and there is a direct linear relationship between Cmax and enalapril dose (over the usual therapeutic range) [Davies et al. 1984a). In contrast, the area under the plasma concentration-time curve (AVC) for enalaprilat is not linearly related to dose. However, if the contribution of the prolonged terminal phase is subtracted from total AUC, it does appear that AUC is linearly related to dose and that the slope

276
of the correlation between these 2 parameters approximates to I (Davies et al. 1984b).
Enalaprilat is 50% bound to plasma proteins; however, binding is concentration dependent. There are two binding sites: one is low affinity and high capacity, and the other is high affinity, low capacity and is, presumably, plasma ACE (Davies et al. 1984b). Enalaprilat is widely distributed throughout the body and there are important tissue binding sites, particularly in/on vascular endothelial cells. These binding sites are thought to constitute 'tissue' ACE.
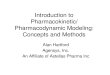
The plasma drug concentration-time profiles for enalapril and enalaprilat following a single dose of enalapril are compared in figure 1. The elimination of enalaprilat is biphasic: the initial phase has a half-life of about 2 to 6 hours while during the second protracted phase drug is detectable for up to 96 hours and has a half-life of ~36 hours. Despite this prolonged terminal elimination phase, steadystate concentrations of enalaprilat are achieved after 3 or 4 oral doses of enalapril. The initial elimination phase for enalaprilat (half-life 2 to 6 hours) reflects clearance of free drug by the kidney, predominantly by glomerular filtration, with a rate of 8 to 10 L/h.
Comparative studies in healthy volunteers and hypertensive patients suggest that the disposition of enalapril and enalaprilat is not altered by hypertension per se (Todd & Goa 1992). However, a number of other studies have investigated the effects of age and disease, particularly renal disease, on the pharmacokinetics of enalapril and enalaprilat.
In some instances this may have a bearing on therapeutic practice in hypertensive patients. For example, single-dose studies have clearly demonstrated that plasma enalaprilat concentrations are increased in the elderly (Hockings et al. 1986) and that this increase, as calculated from the AUC, was closely correlated with a decrease in creatinine clearance. This decrease in systemic clearance is sufficient to result in recommendation of a reduced initial dosage in elderly hypertensive patients.
The influence of various degrees of renal impairment on the disposition of enalaprilat has been
Clin. Pharmacokinet. 25 (4) 1993
investigated in a number of studies using both single- and multiple-dose administration (Fruncillo et al. 1985; Kelly et al. 1984, 1985; Lowenthal et al. 1984). Impaired renal function is associated not only with decreases in the excretion rate and urinary elimination of enalapril and enalaprilat, but also with increased and delayed Cmax of enalaprilat.
It has been suggested that there is a threshold for renal impairment below which the serum concentrations of enalaprilat are seen to markedly increase. This threshold appears to occur at glomerular filtration rates of 20 to 30 mljmin « 1.2 to 1.8 L/h). In such patients there is significant accumulation of enalaprilat in the translation from single-dose to steady-state treatment. As a consequence, reductions in dosage are recommended for patients with glomerular filtration rates below 30 mljmin (1.8 L/h).
In patients with severe renal impairment, with glomerular filtration rates of > 15 mljmin (0.9 L/ h), markedly elevated serum enalaprilat concentrations are seen after repeated doses of enalapril 2.5mg, indicating that further dosage reductions may be warranted (Kelly et al. 1985). In patients receiving regular dialysis treatment, significant amounts of enalaprilat are dialysable and the extent of drug accumulation is reduced (Fruncillo et al. 1985; Saris et al. 1984).
The disposition characteristics of enalaprilat have also been studied in diabetic patients. Again there is evidence that clearance of the active moiety is impaired, presumably as a result of reduced glomerular filtration and possibly of hypoproteinaemia (Baba et al. 1989).
A study in 2 patients with hepatic dysfunction (hepatic congestion and alcoholic cirrhosis) noted a delay in the appearance of enalaprilat in plasma after a single dose of enalapril (Johnston et al. 1984). This may be attributed to a slower rate of deesterification of the parent drug, an effect which has been demonstrated in vitro with liver homogenates from patients with cirrhosis (Larmour et al. 1985). In other patients with decompensated liver cirrhosis, there is evidence of impaired enalapril deesterification compared with healthy con-

Enalapril Kinetic-Dynamic Relationships 277
0.2-L-r-----,------r-----.-----.------.-----,r-----~----._----_.----__. o 10 20 30 40 50
Time (h)
60 70 80 90 100
Fig. 1. Representative plasma concentration-time profiles ofenalapril and enalaprilat following a single oral dose ofenalapril 20mg to patients with essential hypertension (data from Donnelly et al. 1990).
trois (Ohnishi et al. 1989). However, little or no change in enalaprilat disposition was noted in patients with compensated liver cirrhosis (8aba et al. 1990; Hayes et al. 1989).
Following oral doses of enalapril, the clearance of enalaprilat was impaired in patients with congestive heart failure compared with patients with hypertension (Dickstein et al. 1987; Johnston et al. 1984; Schwartz et al. 1985). However, after repeated doses of enalapril, plasma enalaprilat concentrations were similar in patients with congestive heart failure to those observed in patients with hypertension (Johnston et al. 1984). It remains unclear, therefore, whether the apparent decrease in clearance of both enalapril and enalaprilat in congestive heart failure is a function of age and renal dysfunction or of the disease state itself.
The conventional pharmacokinetic approach to enalapril(at) has recently been more extensively reviewed elsewhere (Todd & Goa 1992).
2. Current Pharmacok;net;c Approaches
Till and colleagues (1984) were the first to identify that conventional pharmacokinetic approaches were inappropriate for characterising the disposition of enalaprilat. When the pharmacokinetics of enalaprilat are evaluated by fitting a hierarchy of conventional pharmacokinetic compartmental models governed by first-order processes, it is usually found that a 2-compartment open model can most appropriately be fitted to the data. However, such models do not satisfactorily describe all features of the disposition of enalaprilat on repeated administration, particularly the relative lack of accumulation (Sweet & Vim 1984; Till et al. 1984).
The failure of conventional approaches to describe the accumulation of enalaprilat in translation from single-dose to steady-state administration, led to the suggestion that the calculation of an 'effective' half-life should be based on urinary

278
excretion data (Till et al. 1984). This approach yielded a half-life of approximately II hours, which did indeed predict the relatively modest accumulation of enalaprilat at steady-state. However, this approach failed to identify and account for the physiological processes such as tissue distribution. At that time, these processes were thought to underlie the disposition characteristics of enalaprilat.
Sweet and VIm (1984) concluded that the prolonged terminal elimination phase of enalaprilat represented binding to serum ACE. They further suggested that this binding site corresponded to the high affinity, low capacity plasma protein binding site, particularly since the concentration of enalaprilat was of the same order of magnitude as the concentration of plasma ACE. Despite the fact that additional evidence presented by Abrams et al. (1984) tended to support this view, no attempt was made to adopt a physiologically realistic approach to the disposition characteristics of enalaprilat. However, this approach was subsequently adopted to account for the pharmacokinetic characteristics of another ACE inhibitor drug, cilazaprilat, following oral cilazapril administration (Francis et al. 1987).
The model, based on saturable binding of cilazaprilat to ACE, was developed to account for the pharmacokinetics of that agent and for the relationship of the drug kinetics to the pharmacodynamics of ex vivo ACE inhibition (fig. 2). In this model, ki is the input rate constant and lee is the elimination rate constant. Cilazaprilat and ACE are uniformly distributed throughout a single compartment with a volume (V) but only the free drug (Cr) is available for elimination. Bound drug (Cb) and free drug are inter-related as shown, where Ct is the total drug concentration, p is the concentration of ACE and C50 is the concentration value at 50% receptor occupancy. Measured ex vivo, ACE inhibition (I) and free drug are also interrelated as shown, where Imax is the maximum achievable inhibition and c' 50 is the value of Cf for 50% of the maximum inhibition.
This approach allowed simultaneous description of the drug concentration profile along with ACE inhibition. It also yielded a parameter which
Clin. Pharmacokinet. 25 (4) 1993
PRO-DRUG ACTIVE FORM
Ct=C,+Cb
Cb = p. C, I (C'50 + C,l
I = Imax' C, I (C50 + C,l
Fig. 2. Pharmacokinetic-pharmacodynamic model for an ACE inhibitor drug (derived on the basis of cilazapriljcilazaprilat data). Abbreviations: c'so = free drug concentration at 50% receptor (ACE) occupancy; Cso = total drug concentration at 50% receptor (ACE) occupancy; Cb = bound drug concentration; Cf = free drug concentration; Ct = total drug concentration; I = observed inhibitory response; Imax = maximum inhibitory response; kj = input rate constant; k., = elimination rate constant; p = concentration of converting enzyme; V = volume.
estimated the total amount of ACE which was accessible to the drug. However, the model assumed saturable binding of the drug to circulating ACE alone. An alternative and similar approach has been considered which incorporates saturable binding to both circulating and tissue ACE.
The saturable binding model was first formulated for another ACE inhibitor prodrug, perindopril. This was based on the observed concentration-time profile during the infusion of its active diacid moiety, perindoprilat (Lees et al. 1989). Those authors were able to demonstrate that the most appropriate fit of concentration data to model was obtained with a model which attributed binding both to circulating ACE and to tissue ACE. The validity of this approach has subsequently been confirmed with alternative protracted low dose infusion regimens (MacFadyen et al. 1992). This pharmacokinetic modelling approach used a 1-compartment model with saturable binding, and has been shown to produce satisfactory fits for enalaprilat concentration data following single and

Enalapril Kinetic-Dynamic Relationships
multiple doses (Donnelly et al. 1990; Meredith et al. 1990).
Thus, it is now generally accepted that the plasma concentration-time profile for enalaprilat has 2 principal phases: an initial elimination phase which reflects renal clearance of enalaprilat (free drug) and a protracted phase which reflects the release of enalaprilat mainly from tissue binding sites, before elimination by the kidney.
The protracted terminal half-life, reflecting saturable binding to tissue and plasma ACE, is not a conventional half-life and, consequently, does not influence the rate of drug accumulation. The lack of significant accumulation is therefore a direct reflection of the rapid initial elimination phase. This phase has a half-life of about 4 hours, making it impossible for a true steady-state to be achieved and for drug accumulation to occur with the usual dosage interval of 24 hours. The single- and multiple-dose profiles for enalaprilat are illustrated in figure 3.
The consistency of the saturable binding model has been confirmed by Meredith et al. (1990). These workers demonstrated that a unified approach to
180 Single-dose
:::J 150 C, S c 0
~ 120 C CD U C 0 u 90 iii ~ '" (ij c 60 CD
'" E (/)
'" 1[ 30
0 0 5 10 15 20 25 30
Time (h) 35
279
single-dose and steady-state data by simultaneous fitting of the saturable binding model was superior not only to conventional models but also to independent fitting to several data sets from each individual patient.
3. Concentration-Effect Relationships
It is often claimed that there is no correlation between plasma enalaprilat concentrations and blood pressure reductions. This is a misconception, which reflects not only the complexities of the underlying pharmacokinetic characteristics but also the nonlinear nature of the concentration-effect relationships for all ACE inhibitor drugs. This applies both to ACE inhibition and to blood pressure reduction. Frances and colleagues (1987) clearly identifying the sigmoidal (or Emax) relationship between the extent of ACE inhibition and the corresponding plasma drug concentrations (as applied to cilazapril). On the basis of a I-compartment pharmacokinetic model with saturable binding, it was shown that pharmacokinetic and pharmacodynamic parameters, as reflected by ACE inhibi-
Steady-state
o 5 10 15 20 25 30 35 Time (h)
Fig. 3. Representative plasma concentration-time profiles for enalaprilat following single-dose and steady-state administration of enalapril 20mg once daily to a patient with essential hypertension (data from Donnelly et al. 1990).

280
tion, could be correlated. The values derived from this approach for dissociation constants, ICsQ, etc., were entirely consistent with those calculated from in vitro experiments.
Extending the integrated pharmacokinetic-pharmacodynamic approach to the evaluation of the concentration-effect relationship for blood pressure reduction requires several considerations. First, an appropriate model has to be employed. Secondly, account must be taken of placebo/circadian influences on the blood pressure response. Thirdly, the temporal discrepancy between the time profiles for drug concentration and measured effect must be considered. Fourthly, individual rather than group data should be studied.
With this approach, the predetermined pharmacokinetic model (1 compartment with saturable binding) is augmented by an 'effect compartment'. The concentration effect relationship is characterised by a nonlinear (Langmuir) or sigmoidal maximum inhibition model (Emax), and fitted to the pharmacodynamic data of each individual patient (Donnelly et al. 1990). It is then possible to calculate the maximum blood pressure reduction which any individual patient will achieve for a gi ven plasma concentration of enalaprilat. It is also possible to predict the blood pressure responses in relation to a change in dosage (Reid & Meredith 1990). Furthermore, the increasing perception that ACE inhibitor drugs have 'flat' dose-response curves is merely a rather loose terminology for the Emax nature of the concentration-effect relationship.
4. Clinical Consequences
Alongside the developments in explaining the pharmacokinetics of enalapril(at) and identifying concentration-effect relationships for biochemical and simple haemodynamic (blood pressure) indices, there have been other significant observations in clinical practice. These observations merit further pharmacokinetic or integrated pharmacokinetic-pharmacodynamic analysis.
Many of the recent data shift emphasis away from the initial representation of enalapril as a simple antihypertensive vasodilator. A revised
Clin. Pharmacokinet. 25 (4) 1993
concept suggests that it is a complex agent, which not only affects a variety of vascular beds to varying degrees but also produces hormonal modification of the renin-angiotensin and other systems in a variety of tissue sites. Many of these new clinical perspectives arise from the use of enalapril in the treatment of patients with heart failure.
4.1 Variable Concentration-Effect Relationships (Dependent on End-Point)
The value of ACE inhibitors in the treatment of hypertension has focused on a blood pressure reduction. Until recently, such a reduction has been entirely and directly associated with reductions in circulating and/or local concentrations of angiotensin II (Hodsman et al. 1983). However, it is now clear for enalapril and other ACE inhibitors that ACE itself plays the central role. This is despite the fact that it is a nonspecific enzyme whose in vitro biochemical activity is greater for kinin degradation than for angiotensin II generation (Ehlers & Riordan 1989). Moreover, several reports show, at best, incomplete suppression of the renin-angiotensin system with conventional antihypertensive doses of ACE inhibitors (Aldigier et al. 1993; Juillerat et al. 1990; Kawamura et al. 1992). Nevertheless, this unusual discordancy between response and biochemical indices of effect can be accommodated by concentration-effect studies because the net response (i.e. blood pressure reduction) is the key target regardless of the mode of action.
There is accumulating evidence that differing concentration-effect relationships apply to different end-points. For example, animal studies with very low doses of ramipril (an ACE inhibitor very similar to enalapril in structure, metabolism and pharmacokinetic profile) have shown a remarkable attenuation of the effect of experimental hypertension on left ventricular morphology and structure. These effects occurred without influencing either blood pressure or circulating biochemical parameters and, additionally, continued to inhibit the development of left ventricular hypertrophy after withdrawal of the ACE inhibitor (Linz et al. 1992).
Similarly, although controlled studies are rare,

Enalapril Kinetic-Dynamic Relationships
studies with very low oral doses of captopril in patients with heart failure have intriguingly revealed a differing pharmacodynamic profile. For example, at conventional dosages ACE inhibitors seem to have little effect on the natriuretic response to furosemide (frusemide) [Cleland et al. 1988; Odemuyiwa et al. 1989]. In contrast, very low dose captopril (1 mg) has been shown to substantially increase sodium excretion, relative to the effect of captopril 25mg (Motwani et al. 1992). The mechanism of this response is unclear but again it suggests that there may be differential concentration-dependent effects on renal function which, in this study, were clearly independent of overall changes in blood pressure.
Despite more than 10 years of general clinical use, the indications for ACE inhibitor treatment continue to expand (Pfeffer et al. 1992). Enalapril(at) has been central to this process. Several large studies have now defined efficacy of enalapril in less severe degrees of heart failure (Cohn et al. 1991; SOLVD Investigators 1991) and in asymptomatic left ventricular dysfunction (Yusef et al. 1992). These results have extended the earlier definition of significantly reduced mortality during use of enalapril to treat severe heart failure (CONSENSUS I 1987).
5. Conclusions
Recent research with enalapril and other ACE inhibitor drugs has made it possible to refine our understanding of ACE inhibitor concentration-effect relationships, particularly at low or very low drug dosages. Fundamental to this research is the recognition of the 'unconventional' pharmacokinetic principles which govern the plasma concentration-time profile of enalaprilat. This includes the acceptance that the prolonged terminal phase of the drug represents saturable binding to ACE, rather than an index of potential drug accumulation. Further integrated pharmacokinetic-pharmacodynamic exploration of ACE binding is likely to be of considerable pharmacological importance. Such investigations may also have potential clinical significance in directing more organ-specific or effect-
281
specific therapy in respect of differential dose/concentration-effect relationships. Enalapril, as one of the most widely used ACE inhibitors in clinical practice, merits ongoing exploration in this context.
References
Abrams WB, Davies RO, Gomez HJ. Clinical pharmacology of enalapril. Journal of Hypertension 2 (Suppl. 2): 31-36, 1984
Aldigier IC, Huang H, Dalmay F, Lartigue M, Baussant T, et al. Angiotensin converting enzyme inhibition does not suppress plasma angiotensin II increase during exercise in humans. Journal of Cardiovascular Pharmacology 21: 289-295, 1993
Baba T, Murabayashi S, Tomiyanma T, Takebe K. The pharmacokinetics of enalapril in patients with compensated liver cirrhosis. British Journal of Clinical Pharmacology 29: 766-769, 1990
Baba T, Tomiyama T, Murabayashi S, Tomiyama M, Takebe K. Enalapril pharmacokinetics in diabetic patients. Lancet I: 226-227, 1989
Cohn IN, Johnson G, Zieche S, Cobb F, Francis G, et al. A comparison of enalapril with hydralazine-isosorbide dinitrate in the treatment of chronic congestive heart failure. New England Journal of Medicine 325: 303-310, 1991
CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure: results of the Cooperative North Scandinavian Enalapril Survival Study. New England Journal of Medicine 316: 1429-1435, 1987
Cleland JGF, Gillen G, Dargie HJ. The effects offrusemide and angiotensin converting enzyme inhibitors and their combination on cardiac and renal haemodynamics in heart failure. European Heart Journal 9: 132-141, 1988
Davies RO, Gomez HJ, Irvin JD, Walker JF. An overview of the clinical pharmacology of enalapril. British Journal of Clinical Pharmacology 18 (Suppl. 2): 215S-229S, 1984a
Davies RO, Irvin JD, Kramsch OK, Walker JF, Moncloa F. Enalapril worldwide experience. American Journal of Medicine 77: 23-35, 1984b
Dickstein K, Till AE, Aarsland T, Tjelta K, Abrahamsen AM, et al. The pharmacokinetics of enalapril in hospitalized patients with congestive heart failure. British Journal of Clinical Pharmacology 23: 403-410, 1987
Donnelly R, Meredith PA, Elliott HL, Reid JL. Kinetic-dynamic relations and individual responses to enalapril. Hypertension 15: 301-309, 1990
Ehlers MRW, Riordan JF. Angiotensin converting enzyme: new concepts concerning its biological role. Biochemistry 28: 5311-5317, 1989
Francis RJ, Brown AN, Kler L, Fasanella d'Amore T, Nussberger J, et al. Pharmacokinetics of the converting enzyme inhibitor cilazapril in normal volunteers and the relationship to enzyme inhibition: development of a mathematical model. Journal of Cardiovascular Pharmacology 9: 32-38, 1987
Fruncillo RJ, Rocci Jr ML, Shepley K, Clementi RA, DeRita R, et al. Enalapril accumulates after chronic enalapril dosing in renal failure. Abstract no. A50. Clinical Pharmacology and Therapeutics 37: 197, 1985
Hayes PC, Plevris IN, Bouchier lAD. Pharmacokinetics of enalapril and lisinopril in subjects with normal and impaired hepatic function. Journal of Human Hypertension 3: 153-158, 1989
Hockings N, Ajayi LAA, Reid IL. Age and the pharmacodynamics of the angiotensin converting enzyme inhibitors enala-

282
pril and enalaprilat. British Journal of Clinical Pharmacology 21: 341-348, 1986
Hodsman GP, Isles CG, Murray GD, Vsherwood TP, Webb DJ, et al. Factors related to first dose hypotensive effect of captopril: prediction and treatment. British Medical Journal 286: 832-834, 1983
Irvin JD, Till AE, Vlasses PH. Bioavailability of enalapril maleate. Clinical Pharmacology and Therapeutics 33: 248, 1984
Johnston CI, Jackson BJ, Larmour I, Cubella R, Casley D. Plasma enalapril levels and hormonal effects after short- and long-term administration in essential hypertension. British Journal of Clinical Pharmacology 18 (Suppl. 2): 233S-239S, 1984
Juillerat L, Nussberger J, Menard J, Mooser V, Christen Y, et al. Determinants of angiotensin II generation during converting enzyme inhibition. Hypertension 16: 564-572, 1990
Kawamura M, Imanashi M, Matsushima Y, Ito K, Hiramori K. Circulating angiotensin II levels under repeated administration of lisinopril in normal subjects. Clinical and Experimental Pharmacology and Physiology 19: 547-553, 1992
Kelly J, Doyle G, Donohoe J, Laher M, Vandenburg MJ, et al. The pharmacokinetic profile of enalaprilat in normal subjects and patients with renal impairment. British Journal of Clinical Pharmacology 18: 274P, 1984
Kelly J, Doyle G, Donohoe J, Laher M, Vandenburg MJ, et al. Chronic dose pharmacokinetics of enalapril in renal impairment. British Journal of Clinical Pharmacology 20: 264P-265P, 1985
Larmour I, Jackson B, Cubella R, Johnstone CI. Enalapril (MK42 I ) activation in man: importance of liver status. British Journal of Clinical Pharmacology 19: 701-704, 1985
Lees KR, Kelman A W, Reid JL, Whiting B. Pharmacokinetics of an ACE inhibitor S9780 in man: evidence of tissue binding. Journal of Pharmacokinetics and Biopharmaceutics 17: 529-550, 1989
Linz W, Shaper J, Wiemer G, Albus V, Schwalkens BA. Ramipril prevents left ventricular hypertrophy with myocardial fibrosis without blood pressure reduction: a one year study in rats. British Journal of Pharmacology 107: 970-975, 1992
Lowenthal DT, Saris SD, Haratz A, Packer J, Porter RS, et al. The clinical pharmacology of antihypertensive drugs. Journal of Hypertension 2 (Suppl. 2): 49-56, 1984
MacFadyen RJ, Lees KR, Reid JL. Studies with low dose intravenous diacid ACE inhibitor (perindoprilat) infusions in normotensive male volunteers. British Journal of Clinical Pharmacology 34: 115-121, 1992
Meredith PA, Donnelly R, Elliott HL, Howie CA, Reid JL. Prediction of the antihypertensive response to enalapril. Journal of Hypertension 8: 1085-1090, 1990
Motwani JG, Fenwick MK, Morton JJ, Struthers AD. Frusemide induced natriuresis is augmented by ultra low dose captopril but not by standard doses of captopril in chronic heart failure. Circulation 86: 439-445, 1992
Odemuyiwa 0, Gilmartin J, Kenny D, Hall RJc. Captopril and the diuretic requirements in moderate and severe chronic heart failure. European Heart Journal 10: 586-590, 1989
Ohnishi A, Tsuboi Y, Ishizaki T, Kubota K, Ohno T, et al. Ki-
Clin. Pharmacokinet. 25 (4) 1993
netics and dynamics of enalapril in patients with liver cirrhosis. Clinical Pharmacology and Therapeutics 45: 657-665, 1989
Pfeffer MA, Braunwald E, Moye LE, Basta L, on behalf of the SAVE investigators. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. New England Journal of Medicine 327: 669-677, 1992
Reid JL, Meredith PA. Concentration effect analysis of antihypertensive drug response. Hypertension 16: 12-18, 1990
SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. New England Journal of Medicine 325: 293-302, 1991
Saris S, Lowenthal D, Klein L, Irvin JD, Merrill D, et al. Enalapril maleate in renal failure. Abstract No. A15. Clinical Pharmacology and Therapeutics 35: 272, 1984
Schwartz JB, Taylor A, Abernethy D, O'Meara M, Farmer J, et al. Pharmacokinetics and pharmacodynamics of enalapril in patients with congestive heart failure and patients with hypertension. Journal of Cardiovascular Pharmacology 7: 767-776, 1985
Swanson BN, Vlasses PH, Ferguson RK, Bergquist PA, Till AE, et al. Influence offood on the bioavailability of enalapril. Journal of Pharmaceutical Sciences 73: 1655-1657, 1984
Sweet CS, Vim EH. Enalapril. In Scriabine (Ed.) New drugs annual: cardiovascular drugs, Vol. 2, pp. 1-17, Raven Press, New York, 1984
Till AE, Gomez HJ, Hichens M, Bolognese MS, Lant AF. Pharmacokinetics of repeated single oral doses of enalapril maleate in normal volunteers. Biopharmaceutics and Drug Disposition 5: 273-280, 1984
Todd PA, Goa KL. Enalapril: a reappraisal of its pharmacology and therapeutic use in hypertension. Drugs 43: 346-381, 1992
Vim EH. Enalapril maleate (MK-421), a potent, non-sulphydril angiotensin-converting enzyme inhibitor: absorption, disposition and metabolism in man. Drug Metabolism Review 14: 99-110, 1983
Vim EH, Hichens M, Gomez HJ, Till AE, Hand E, et al. Enalapril maleate and a lysine analogue (MK-521) disposition in man. British Journal of Clinical Pharmacology 14: 357-362, 1982
Weisser K, Schloos J, Lehmann K, Dusing R, Vetter H, et al. Pharmacokinetics and converting enzyme inhibition after morning and evening administration of oral enalapril to healthy subjects. European Journal of Clinical Pharmacology 40: 95-99,1991
YusefS, Pitt B, Davis CE, Hood WB, Cohn IN, for the SOLVD investigators. Effects of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricular ejection fractions. New England Journal of Medicine 327: 685-691, 1992
Correspondence and reprints: Dr R.J. MacFadyen, Department of Medicine and Therapeutics, Gardiner Institute, Western Infirmary, Glasgow Gil 6NT, Scotland.