Embed Size (px)
Citation preview

9/9/2014
1
Employer Coverage & Benefit Design in a Post-ACA
Environment
Caroline Pearson September 16, 2014
avalerehealth.net
Agenda
2
● Employer-Sponsored Insurance:
o Where Do We Stand?
o Where Are We Going?
● Potential Role for Private Exchanges
● Impact of Public Exchanges
● Looking Ahead: Issues to Watch
How will employer trends in medical coverage impact dental insurance?

9/9/2014
2
Employer-Sponsored Insurance: Where Do We Stand?
The Administration Further Delayed Implementation of the Employer Mandate for Some Businesses in February 2014
4
2014 2015 2016
Mandate goes into effect for employers with 100+ FTEs
Members of Congress, including Senator Warner, continue to call for further delays to the employer mandate. additional reforms to the employer mandate likely over time.
Mandate goes into effect for employers with 50 – 99 FTEs
Sources: Final Rule on Shared Responsibility for Employers Regarding Health Coverage. http://www.gpo.gov/fdsys/pkg/FR-2014-02-12/pdf/2014-03082.pdf, Letter from Sen. Warner to U.S. Secretary of Treasury Jack, July 23, 2014 https://www.politicopro.com/f/?f=28641&inb

9/9/2014
3
Rulemaking Gave Large Employers More Time to Transition to Full Compliance
5
2014 2015 2016E
mp
loye
r M
an
da
te
1-49 full-time employees
Mandate delayed to 2015 plan year
Does not apply Does not apply
50-99 full-time employees
Does not apply
Employers must offer coverage to 95% of full-time employees and dependents to age 26
100 or more full-time employees
Employer must offer coverage to 70% of full-time employees and dependents to age 26
Employer must offer coverage to 95% of full-time employees and dependents to age 26
Source: Final Rule on Shared Responsibility for Employers Regarding Health Coverage. http://www.gpo.gov/fdsys/pkg/FR-2014-02-12/pdf/2014-03082.pdf
6
AC
A: A
s P
asse
d Buy ACA-compliant plan in small group market
Buy coverage through SHOP exchange
Drop coverage
Meanwhile, “Keep Your Plan” Guidance Allowed Small Employers to Also Delay ACA-Related Decision-Making
Source: Final Rule on Shared Responsibility for Employers Regarding Health Coverage. http://www.gpo.gov/fdsys/pkg/FR-2014-02-12/pdf/2014-03082.pdf
AC
A: A
s Im
plem
ente
d
Buy ACA-compliant plan in small group market
Drop coverage
Buy coverage through SHOP exchange (in select states)
Maintain non-ACA-compliant coverage
Small Business Health Insurance Choices 2014

9/9/2014
4
Employer-Sponsored Insurance: Where Are We Going?
What Should Stakeholders Expect from Future Enrollment and Benefit Designs?
8
Enrollment • How many employers offer coverage?• How many employees take up coverage?
Benefit Design
• How do employers use benefit design to control costs?
• What role do narrow networks / Centers of Excellence play in the future of employer-sponsored insurance?
• How do consumers react to new benefit offerings?

9/9/2014
5
Before ACA-Implementation, Large Employer Offer Rates Remained Steady, But Small Employer Offer Rates Declined
9
IN 2000, 68% OF SMALL EMPLOYERS OFFERED COVERAGE, COMPARED TO 57% IN 2013.
99% 98% 99%
68%60% 57%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2000 2006 2013
Per
cen
t o
f F
irm
s
Large Firms
Small Firms
PERCENT OF FIRMS OFFERING HEALTH INSURANCE, 1999-2013
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 1999-2013
Note: Small firm is 3-199 workers. Large firm is 200+.
Estimates of ACA’s Impact on ESI Varied Widely, But Most Predicted Minor Net Changes in Coverage
-30%
-21.5%
-3.8% -3.1% -2.5% -1.6%
2.7% 2.7%McKinsey BoozHoltz-Eakin CBO1
RAND
Lewin
Urban
Benefit consultants and other experts largely agree with the models that predict only small net
changes in coverage
Other policy analysts and politicians, such as
Capretta and Bredesenagree with McKinsey and
Holtz-Eakin
Estimates reflect different ACA phase-in periods from 2010 to 2016
Gruber2
1CBO and Joint Committee on Taxacion (JCT) estimate a decline of 3 – 5 M people with ESI (graphic above uses 4 million for display purposes). CBO and JCT modeled 4 scenarios and results ranged from -20 M to + 3 million people with ESI.
2For percent change calculation, Avalere assumed that Gruber used the current/projected CBO ESI baseline for his estimates
10

9/9/2014
6
California Data Suggests Previously Uninsured Enrolled in Employer-Sponsored Insurance More Often than Exchanges
11
Remaining Eligible Uninsured
39%
Remaining Undocumented
Uninsured18%Somewhere
Else/Unknown8%
Employer-Sponsored Insurance
16%
Other Non-Group7%
Covered California
12%
SOURCE OF COVERAGE AMONG CALIFORNIA’S PREVIOUSLY UNINSURED
Source: Where Are California’s Uninsured Now? Wave 2 of the Kaiser Family Foundation California Longitudinal Panel Survey (April 1 – June 15, 2014)
However, Fourteen Percent of People Purchasing Exchange Plans Nationally Had Coverage Previously Through Their Employer
12
Uninsured57%
Covered by a Different Non-Group
Plan16%
Other/Don't Know/Refused
4%
Covered by Medicaid/Other Public Program
9%
Covered by an Employer/COBRA
14%
Source: Kaiser Family Foundation Survey of Non-Group Health Enrollees (conducted April 3 – May 11, 2014)
PREVIOUS SOURCE OF COVERAGE AMONG EXCHANGE ENROLLEES

9/9/2014
7
Other Estimates Show a Decline in Employer Coverage Could Offset Gains in Individual Coverage in 2014
13
PRIVATE HEALTH INSURANCE ENROLLMENT FROM OCTOBER 1, 2013 TO MARCH 31, 2014
0.5m
-1.7m
2.2m
Net Total
Employer Market
Individual Market The individual market grew by 2.2 million…
…but the employer market declined by 1.7
million…
…leaving a net increase in the total private market
of just over 500,000
Source: Edmund Haislmaier and Drew Gonshorowski, “New Obamacare Enrollment Data: Employer-Based Coverage Declines.” Heritage Foundation. July 28, 2014. http://www.heritage.org/research/reports/2014/07/new-obamacare-enrollment-data-employer-based-coverage-declines
Avalere Projects Employer Coverage Will Continue Growing, But at a Slower Rate Due to ACA
14Source: Avalere Enrollment Model, September 2014,
146
148
150
152
154
156
158
2012 2014 2016 2018 2020 2022 2024
EXPECTED EMPLOYER COVERAGE (IN MILLIONS)
• Individual Mandate (take-up)• Employer Mandate (offer rates)• Population Growth
• Exchanges & Subsidies• Medicaid Expansion• Employer Dumping

9/9/2014
8
Some Employer Coverage Will Shift to Medicaid in 2014 and Subsidized Exchange Coverage in 2015-16
15Source: Avalere Enrollment Model, September 2014,
(7.0)
(6.0)
(5.0)
(4.0)
(3.0)
(2.0)
(1.0)
-
1.0
2.0
3.02014 2015 2016
CHANGES IN EMPLOYER COVERAGE (IN MILLIONS)
Uninsured to ESI
Emp.To PremiumAssistance
Emp. To Medicaid
Emp. to UnsubsidizedExchanges
Emp. To SubsidizedExchanges
94% of employers think it is likely they will be offering coverage 5 years from now
16
Most common
reasons for continuing
coverage for employees
Maintain or increase
loyalty and satisfaction
Attract future talent
Retain current
employees
Source: International Foundation of Employee Benefits Plans, 2014 Employer-Sponsored Healthcare: ACA’s Impact http://www.ifebp.org/pdf/research/ACASurvey_2014.PDF

9/9/2014
9
However, Some Fortune 500 Companies Have Already Begun Dropping ESI for Part-Time Employees, Citing Steep Costs
17
FORTUNE 500 COMPANIES THAT HAVE STARTED DROPPING EMPLOYER-SPONSORED COVERAGE FOR PART-TIME WORKERS IN 2014
Target Home Depot
Trader Joe’s
Sources: Talking Health Care with EVP of Human Resources Jodee Kozlak, Target Press Release. January 2014 http://www.abullseyeview.com/2014/01/talking-health-care-with-evp-of-human-resources-jodee-kozlak/; Trader Joe's To Drop Health Coverage For Part-Time Workers Under Obamacare: Memo, Huffington Post, September 2013 http://www.huffingtonpost.com/2013/09/11/trader-joes-obamacare_n_3902341.html; UPDATE 2-Home Depot to tap health insurance exchanges for part-timers, Reuters, September 2013 http://www.reuters.com/article/2013/09/20/healthcare-exchanges-homedepot-idUSL2N0HF22H20130920
18
Source: PBGH, Health Insurance Exchanges Overview: The Employer Perspective (2013) http://www.ehcca.com/presentations/hixsummitwest/kramer_pc1.pdf; Small Business Majority http://www.smallbusinessmajority.org/small-business-research/downloads/050912_Small_Business_Healthcare_Tax_Credit.pdf
In Particular, Small Employers Continue to Face Unique Challenges Offering Health Insurance Coverage
High Cost of Insurance
• Since 2000, small employer premiums have gone up 239%.
• Small businesses pay on average 18% more than larger businesses for health insurance.
Low-Income Workforce Demographics
• 71% of small businesses with fewer than 25 workers have an average annual wage of less than $50,000.

9/9/2014
10
Low Wage Workers Benefit Financially by Purchasing Through the Exchange
19
THIS FINANCIAL INCENTIVE MIGHT EVENTUALLY IMPACT THE SMALL BUSINESS MARKET
200% FPL 300% FPL 399% FPL 500% FPL
Difference between cost of exchange coverage vs. employer coverage
-$11,300 -$3,000 $700 $6,300
Percent difference between cost of exchange coverage vs. employer coverage
-65% -18% 5% 41%
Source: Congressional Budget Office, March 2012Note: Represents expected costs for a family of four with two adults and two children in 2016. Analysis includes simplifying assumptions. Marginal state income tax calculated as an average across all states.
WellPoint Recently Noted Concern About Small Group Volatility
20
“Small group has now shed 218,000 members year-to-date and stands at 1.63 million members.”
“With respect to our small group business, we continue to be mindful of the potential for employer coverage changes in light of the exchanges.”
“In our commercial business, [our] small group [remains] under enrollment pressure.”
Source: WellPoint Conference Call: Report on Second Quarter 2014 Results, July 30, 2014 http://ir.wellpoint.com/phoenix.zhtml?c=130104&p=irol-newsArticle&ID=1952795&highlight=

9/9/2014
11
Employers of All Sizes Continue to Focus on Ways to Control Costs
21
Increased Cost-Sharing
Narrow Networks / Centers of Excellence
Consumerism
Private exchanges are one tool for employers to implement these approaches.
22
$4,565
$4,316
$4,129
$3,997*
$3,515
$3,354
$3,281*
$2,973*
$2,713
$2,661*
$2,412*
$2,137*
$1,787*
$1,619
$1,543
$11,786
$11,429*
$10,944*
$9,773
$9,860*
$9,325*
$8,824
$8,508*
$8,167*
$7,289*
$6,657*
$5,866*
$5,274*
$4,819*
$4,247
2013
2012
2011
2010
2009
2008
2007
2006
2005
2004
2003
2002
2001
2000
1999
Worker Contribution
Employer Contribution
* Estimate is statistically different from estimate for the previous year shown (p<.05).
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 1999-2013.
AVERAGE ANNUAL WORKER AND EMPLOYER CONTRIBUTIONS TO PREMIUMS AND TOTAL PREMIUMS FOR FAMILY COVERAGE, 1999-2013
Employee Contribution to Employer-Sponsored Insurance Still Increases Even as Employer Costs Rise
Employees contribute 18% on avg. to individual
coverage, 29% for family.

9/9/2014
12
23
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
2015
PROJECTED GROWTH IN EMPLOYER HEALTH COSTS, 2015
NBGH-ProjectedBenefit CostswithoutChangesEmployer-ProjectedBenefit Costswith Changes
2014 National Business Group on Health Annual Survey, NBGH, https://www.businessgrouphealth.org/pressroom/pressRelease.cfm?ID=234
Employers Believe They Can Limit Health Care Cost Growth By Altering Their Benefit Offerings
Healthcare costs for large employers are projected to increase
6.5% in 2015 …
…but employers expect to keep increases to 5%next year after making changes to their plans.
Employers Continue to Focus on Increased Cost Sharing to Control Costs
24
PERCENT OF EMPLOYERS UTILIZING VAROIUS COST CONTAINMENT TOOLS,
2013 vs. 2014
14%
18%
15%
13%
10%
12%
32%
30% 30%
24%
21%
19%
0%
5%
10%
15%
20%
25%
30%
35%
Increased OOP limits Increased cost sharingfor premiums
Increased in-networkdeductibles
Increased cost sharingfor primary care
Increased deductibles fordependents
Increased drug costsharing
2013
2014
Source: International Foundation of Employee Benefits Plans, 2014 Employer-Sponsored Healthcare: ACA’s Impact http://www.ifebp.org/pdf/research/ACASurvey_2014.PDF

9/9/2014
13
The Percentage of Workers with Significant Deductibles Continues to Rise
25
PERCENTAGE OF COVERED WORKERS ENROLLED IN A PLAN WITH A GENERAL ANNUAL DEDUCTIBLE OF $1,000 OR MORE FOR SINGLE COVERAGE, BY FIRM SIZE, 2006-2013
16%
21%
35%
40%
46%
50%49%
58%
10%12%
18%
22%
27%
31%
34%
38%
6%8%
9%
13%
17%
22%
26%
28%
0%
10%
20%
30%
40%
50%
60%
2006 2007 2008 2009 2010 2011 2012 2013
All Small Firms (3-199 Workers)
All Large Firms (200 or MoreWorkers)All Firms
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 2006-2013 http://kff.org/report-section/ehbs-2013-section-1/
26
Narrow Networks
Quality Cost
1 in 4 employers include a narrow network among their choice of
plans.
13% who offer a narrow network
incentivize employees to
use it.
In addition to increasing use of narrow networks in exchanges and Medicare Advantage…
Employers Look Increasingly to Narrow Networks and Centers of Excellence to Control Costs and Improve Quality
…employers are turning to restrictive networks as a way to control cost and drive value-based care.
2014 National Business Group on Health Annual Survey, NBGH, https://www.businessgrouphealth.org/pressroom/pressRelease.cfm?ID=234

9/9/2014
14
Most Workers Are Satisfied With Their Health Insurance, but Increasingly Workers Would Like Higher Wages Rather than Benefits
27
70%
20%
11%
60%
29%
11%
74%
15%
10%
74%
12%14%
0%
10%
20%
30%
40%
50%
60%
70%
80%
You are satisfied with the healthbenefits you receive now
You would rather have morehealth benefits and lower wages
You would rather have fewerhealth benefits and higher wages
ATTITUDES TOWARD CURRENT EMPLOYER-BASED COVERAGE, SELECT YEARS, 2001-2013
2001
2004
2012
2013
Source: Employee Benefit Research Institute and Greenwald & Associates, 2001‒2012 Health Confidence Surveys, and 2013 Health and Voluntary Workplace Benefits Survey.
Choice of Health Plans Remains Important to Employees, and Employers are Providing Decision Support Tools to Help Them Make Informed Choices
28
34%
46%
16%
3%1%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Extremely Important Very Important Somewhat Important Not Too Important Not At All Important
IMPORTANCE TO EMPLOYEE THAT EMPLOYER OFFERS A CHOICE OF HEALTH PLAN, 2013
Source: Employee Benefit Research Institute and Greenwald & Associates, 2013 Health and Voluntary Workplace Benefits Survey. 2014 National Business Group on Health Annual Survey, NBGH, https://www.businessgrouphealth.org/pressroom/pressRelease.cfm?ID=234
3 in 4 employers are adding or
expanding tools to encourage
employees to be better health care
consumers.

9/9/2014
15
In Summary, Most Employers Are Interested in Controlling Healthcare Costs and Promoting Employee Choice
29
HOW DO EMPLOYERS RATE THE FOLLOWING BENEFIT CONSIDERATIONS?
88%
77%
35%
31%
6%
7%
15%
44%
48%
78%
6%
8%
21%
21%
16%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%100%
Interested in controlling costs and budgetary stability
Promoting employee choice, engagement andconsumerism
Consideration of an administrative platform toprovide administrative support
Considering a transition to a defined contributionmodel
Interested in moving away from benefit engagementwith employees
Likely Unlikely Not Applicable
Source: 2014 Willis Health Care Reform Survey Report http://www.willis.com/documents/publications/Services/Employee_Benefits/20140606_Willis_Health_Care_Reform_Survey_Report_2014.pdf
30
As a Result, the Nature of Employer Sponsored Insurance Will Likely Change Considerably Over Time
Sources: Based on “Performance in an Era of Uncertainty”, 17th Annual Towers Watson/National Business Group on Health Employer Survey on Purchasing Value in Health Care , March 2012. AHPI: http://www.americanhealthpolicy.org/Content/documents/resources/What%20CHROs%20Think%20About%20Health%20Care.pdf. Aon Hewitt: http://ir.aon.com/phoenix.zhtml?c=105697&p=irol-newsArticle&ID=1901130&highlight=. EBRI, Views on Employment-Based Health Benefits (January 2014): http://www.ebri.org/pdf/notespdf/EBRI_Notes_12_Dec-13_WBS_DB-DC1.pdf. International Foundation of Employee Benefits Plans, 2014 Employer-Sponsored Healthcare: ACA’s Impact http://www.ifebp.org/pdf/research/ACASurvey_2014.PDF
Continue to Offer
Coverage
Restructure Contributions
Drop Coverage and Gross-up Wages
Drop Coverage with No Wage
Gross-up
• 95% of employers plan to continue offering coverage for the next 3-5years
• 30% of employers are increasing employee cost sharing
• 36% of employers anticipate implementing a defined contribution strategy
• 11% of employers are somewhat likely to drop coverage and direct employees to the public health insurance exchanges with a financial subsidy
• 16% of employers anticipate not continuing to offer coverage over the long term
PRIVATE EXCHANGES

9/9/2014
16
Potential Role for Private Exchanges
32
Employer Interest in Private Exchanges is Highly Variable
Sources: AIS Webinar, “Private Exchanges: What Their Product Design and Results Foreshadow for New ACA Marketplaces,” May 2013; Kaiser Family Foundation/HRET, Employer Health Benefits 2013 Survey, August 2013, http://kaiserfamilyfoundation.files.wordpress.com/2013/08/8465-employer-health-benefits-20131.pdf; Towers Watson: http://www.towerswatson.com/DownloadMedia.aspx?media={3ECBC33E-F9CD-4906-B9E3-29FBD1BA7AED, Accenture: http://www.accenture.com/SiteCollectionDocuments/PDF/Accenture-Growing-Pains-for-Health-Insurance-Exchange-v2.pdf, Aon Hewitt: http://ir.aon.com/phoenix.zhtml?c=105697&p=irol-newsArticle&ID=1901130&highlight=AHPI: http://www.americanhealthpolicy.org/Content/documents/resources/What%20CHROs%20Think%20About%20Health%20Care.pdf
Oliver Wyman:80% of employers
are willing to choose a private exchange model in the future
80%
Kaiser: Just 9% of all employers with 200 employees or more
are considering private exchanges
9% 46%
AHPI: 46% of employers have
already moved or are considering moving post-65
retirees to private exchanges
Aon Hewitt: 33% of employers plan
to move active employees to
private exchanges over
the next 3-5 years
33%
Accenture estimates 3 million people are enrolled in private exchanges in 2014, with private exchange volume approaching enrollment in public exchanges by 2017.
Low Interest High Interest

9/9/2014
17
Private Exchanges Offer Differing Value Propositions to Employers and Employees
33
Defined / decreased healthcare costs
Defined / decreased healthcare costs
Opportunity to decrease costs through more choice
of plans
Opportunity to decrease costs through more choice
of plans
Upfront administrative burden
Upfront administrative burden
Increased exposure to OOP costs / healthcare
cost growth
Increased exposure to OOP costs / healthcare
cost growth
PROS
CONS
EMPLOYERS EMPLOYEES
Ability to deliver more choice to employees / implement alternative
benefit strategies
Ability to deliver more choice to employees / implement alternative
benefit strategies
Potential for portabilityPotential for portability
The ultimate success of private exchanges, likely hinges on the ability to reduce costs for employers over time.
Private Exchange are Particularly Attractive for Retiree Populations
34
Retiree Value Proposition
Decreasing Costs
Offloading Administrative Responsibility
Streamlining Retiree
Management
• Defined contribution to a Health Reimbursement Account (HRA)
• One-time exit in administration of retiree benefits
• Potential for single source for management of retirees and actives
Source: Aon Hewitt. AIS Conference, “Making Private Exchanges Work for Insurers: A Guide to Designing and Executing New Market Strategies.” February 25, 2014

9/9/2014
18
When Purchasing on a Private Exchange, Employees are Choosing Leaner Benefit Options
35
70%
47%
18%
14%
12%
39%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2012 2013 (on-private exchange)
PPO HMO Consumer-Directed High Deductible Plan
Source: Aon Hewitt. AIS Conference, “Making Private Exchanges Work for Insurers: A Guide to Designing and Executing New Market Strategies.” February 25, 2014
42% of employees opted for a leaner plan
25% of employees opted for a richer plan
EMPLOYEE HEALTH PLAN CHOICES, DARDEN AND SEARS
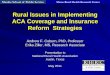
Three-Quarters of Private Exchange Participants are Choosing a Dental Plan
36
PARTICIPATION IN VARIOUS INSURANCE PRODUCTS, LIAZON 2014,
ACCORDING TO PRIVATE EXCHANGE EVALUATION COLLABORATIVE
Participation Product
80% Buy different health insurance, vast majority of which buy down
75% Dental
70% Disability
65% Buy HDHP, with 80% opening HSAs
45% Vision
40% Life
30% Supplemental health
Source: 2014 Private Exchange Employer Survey Findings, Private Exchange Evaluation Collaborative (PEEC) http://machc.org/documents/Session3-PrivateExchanges-FINAL.pdf

9/9/2014
19
Looking Ahead: Key Factors to Growth in Private Exchange Market
37
• Cost savings• Ease of administration
Sustained Employer Value
• User-friendly• Simple-to-use
Accessibility
• Health plans continue participation in exchanges • Wide plan variation persistsAdequate Choice
• Ease of compliance with current regulatory framework (ACA, HIPAA, ERISA, COBRA)Regulatory Feasibility
Source: Aon Hewitt. AIS Conference, “Making Private Exchanges Work for Insurers: A Guide to Designing and Executing New Market Strategies.” February 25, 2014
38
Exchanges – Both Public and Private – Will Influence Employers’ Approach to Insurance
Source: Kaiser Family Foundation Employer Health Benefits, 2013. Available here: http://kaiserfamilyfoundation.files.wordpress.com/2013/08/8466-employer-health-benefits-2013_summary-of-findings1.pdfHDHP = High Deductible Health Plan
Private ExchangeEmployee – not employer – in
direct purchasing role
High-value networks, consumer-
directed plan design
Defined contribution
Lower employer costs
• Private exchanges will make employees / employers more comfortable with exchange model.
• Public exchanges are likely to impact employer demand for innovative benefit design.
Public Exchange
Traditional Employer
Sponsored Insurance

9/9/2014
20
Impact of Public Exchanges on Employer-Sponsored Insurance
The Regulatory Framework Created by the ACA has Likely Accelerated Several Existing Trends in the Employer Market
Essential Health Benefits
Out of Pocket Limits
Guarantee Issue & Rating Rules
Actuarial Value
These parameters constrain plan flexibility…
40
…With Pressure to Keep Premiums Low, Plans Are Focused on Select Levers
• Network Design: Despite requirements that they must offer “adequate networks,” plans are designing high-value, narrow networks
• Formulary Design: Tier placement and utilization management will help plans manage drug use while still meeting EHB drug coverage requirements
• Cost-Sharing Requirements: Cost-sharing is generally higher under exchange plans than the traditional employer market
EHB: Essential Health Benefits

9/9/2014
21
Issuers Designed Narrow Provider Networks to Lower Premium Costs
2,3163,009
3,855
4,9465,705
6,559
8,839
0100020003000400050006000700080009000
10000
There are 28,181 licensed physicians in Los Angeles County.
Figure 10. Case Study: Number of Providers in Los Angeles County Participating In The
Exchange
There are 28,181 licensed physicians in Los Angeles County. Source: Avalere PlanScape, Updated November 18, 2013 and Avalere analysis of information available on http://pnhp.org/blog/2013/09/16/exchange-plans-have-sharply-limited-networks/.Milliman. “2014 Individual Exchange Policies in Four States: An Early Look for Patients with Blood Cancer.” January 9 ,2014
Leading Cancer Centers Excluded From Most Exchange Networks
77% of TX plans surveyed
exclude M.D. Anderson
81% of NY plans
surveyed exclude Memorial Sloan-
Kettering
100% of WA plans exclude Fred Hutchinson
41
Specialty Tiers Are Much More Common in Exchanges Compared to Employer Plans
42
19%9%
59%91%
23%
Exchange (2014) Employer (2013)*
Two or Fewer Tiers Three Tiers Four or More Tiers
DISTRIBUTION OF FORMULARIES BY NUMBER OF TIERS,BY MARKET SEGMENT
PE
RC
EN
T O
F P
LA
NS
*Employer data represented distribution of covered workers whereas exchange and Part D data represent distribution of plans.Source for Exchange Data: Avalere PlanScape, Updated November 2013. Avalere collected plan information from both federally-facilitated and state-based exchanges and captured a sample of over 600 plans for the analysis. Source for Employer Data: Kaiser Family Foundation and Health Research & Educational Trust, Employer Health Benefits 2013 Annual Survey. Source for Part D Data: Avalere Health analysis using DataFrame®, a proprietary database of Medicare Part D plan features, Updated October 2013.

9/9/2014
22
Exchange Plan Deductibles are High, Especially in Bronze and Silver Plans
43
$4,959
$3,132
$1,713
$1,000
$-
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
BronzeN=175
SilverN=207
GoldN=160
PlatinumN=61
ME
DIC
AL
DE
DU
CT
IBLE
AVERAGE MEDICAL DEDUCTIBLES BY METAL LEVEL
*Average deductible for individual coverage ESI = Employer –Sponsored InsuranceSource: Kaiser Family Foundation/ HRET 2013 Employer Health Benefits Survey; Source: Avalere PlanScape, Updated January 28, 2014. Avalere analysis HHS data file of all exchange plans in FFM states.
Employer: $1,135*
Looking Ahead: ACA Issues Impacting Employers
44
• 100 + businesses in 2015• 50 – 99 businesses in 2016
Employer Mandate
• Will public exchanges become more attractive to workers / employers over time?
• Public exchange benefits likely to impact employer offeringsExchanges
• FF-SHOP goes live in 2015• Eligibility expands in 2016 and then again in 2017
SHOP Exchanges
• Balance of power in Congress / White House at stake in next two elections
2014 / 2016 Elections
• 2018 is coming soon!• Employers already making changes to avoid taxCadillac Tax

9/9/2014
23
Key Questions for the Dental Insurance Market
45
● How would ongoing delays (administrative or legislative) to the employer
mandate affect offer rates for medical and dental insurance?
● How will small-group coverage threats impact dental plans?
● Does rising employer healthcare costs put pressure on dental offer rates?
● How do private exchanges impact dental products, take-up and benefit
design?
● Will medical benefit trends of (1) higher employee OOP costs (2) narrower
networks spillover into the dental market?
http://nadpconverge.org/evaluations