Embed Size (px)
Citation preview

N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
Emerging Issues and Opportunities in Quitline Operations“Serving Callers with Psychiatric Conditions: Considerations for Quitlines”
Conference Call Objectives and Tips for Ensuring a Successful and Productive Conference Call
Conference Call ObjectivesBy the end of this conference call, participants will:
understand general issues and considerations for quitlines when determining whether or not toserve mentally ill callers, and to what degree they should do so;
understand one expert’s view of the important role quitlines can play in helping mentally illtobacco users quit;
understand one expert’s concerns about treating nicotine dependence via telephone in those withpsychiatric conditions; and
have had an opportunity to ask questions of experts and colleagues.
Tips for Ensuring a Successful and Productive Conference CallEach conference call will include 50-75 NAQC members. For this reason, and in order to ensure that the call isas effective as possible, we ask that you adhere to the following:
Before the conference call: Remember, these calls are reserved for NAQC members only. Please do not forward dial-in
information to colleagues who are not members. First, you must register for each call. You may do so by going to the “General Member
Services” page of the members-only section of the NAQC web site. Click on “Register forConference Calls.” Simply complete the required information on the registration form and clickon “Submit” when you have finished. You will receive verification and important dial-ininformation via email.
Download and review the background materials for the call. These materials will be postedto the members-only section of the web site one week prior to the call. Go tohttp://www.naquitline.org/index.asp?dbsection=workgroupprojects&dbid=3&dbgroup=wgactivities and look under Conference Call Series to find related attachments, PowerPoint presentationsto be delivered, helpful links and the Evaluation and Feedback Form.
During the conference call: Please keep your phone on mute in order to keep background noise to a minimum. IF YOU DO
NOT HAVE A MUTE FUNCTION ON YOUR PHONE, PLEASE PRESS *6 TOMUTE/UNMUTE YOUR PHONE. THANKS!

N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
Do not put the call on “HOLD” to take another call. Instead, hang up and rejoin the call whenyou are able. Entry into the call is silent so do not worry about interrupting the presentations.
State your name and organization before asking a question or making a comment. Please email questions or comments that you would like addressed to
[email protected] or please feel free to state your questions and comments during thecall. The facilitator will be monitoring the NAQC email address during the call and will askquestions that seem most relevant to the entire audience. While every question may not beaddressed during the call, the facilitator will include answers to every question received viaemail in the published call summary.
If you need technical assistance, press *0 to speak to the operator.
After the conference call: Please return to
http://www.naquitline.org/index.asp?dbsection=workgroupprojects&dbid=3&dbgroup=wgactivities and download the Evaluation and Feedback form. Please return the completed form [email protected].

N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
Emerging Issues and Opportunities in Quitline Operations“Serving Callers with Psychiatric Conditions: Considerations for Quitlines”
Conference Call AgendaWednesday, February 1, 20063:30 PM EST – 3:35 PM EST Introductions of speakers
3:35 PM – 3:55 PM Gary Tedeschi, PhDClinical DirectorCA Smokers’ Helpline
3:55 PM – 4:00 PM Transition/Brief Q & A
4:00 PM – 4: 15 PM Elissa KeszlerTechnical and Financial Assistance DirectorSmoking Cessation Leadership Center
4:15 PM – 4:30 PM Linda Ferry, MD MPHAssociate ProfessorLoma Linda University School of Medicine & School of Public HealthChief, Preventive Medicine Section, Jerry L. Pettis VAMC Loma Linda,California
4:30 PM – 4:45 PM Q & A / Discussion_________________________________________________________________________
Friday, February 3, 200612:30 PM EST – 12:35 PM EST Introductions of speakers
12:35 PM – 12:55 PM Gary Tedeschi, PhDClinical DirectorCA Smokers’ Helpline
12:55 PM – 1:00 PM Transition/Brief Q & A
1:00 PM – 1: 15 PM Elissa KeszlerTechnical and Financial Assistance DirectorSmoking Cessation Leadership Center
1:15 PM – 1:30 PM Linda Ferry, MD MPHAssociate ProfessorLoma Linda University School of Medicine & School of Public HealthChief, Preventive Medicine Section, Jerry L. Pettis VAMC Loma Linda,California
1:30 PM – 1:45 PM Q & A / Discussion

N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
Emerging Issues and Opportunities in Quitline Operations
A Look Ahead
April 5th at 3:30 PM EST and April 7th at 12:30 PM ESTWeb-based Cessation Interventions
June 7th at 3:30 PM EST and June 9th at 12:30 PM ESTIntegrating Pieces of a Comprehensive Cessation Program
LOOK FOR HOT TOPIC CALLS TO BE HOSTED IN FEBRUARY, MARCH, AND MAY.
HOT TOPIC calls will follow the same schedule as the calls above (the firstWednesday and Friday of the first full week of the month, 3:30 PM EST onWednesdays and 12:30 PM EST on Fridays). The February HOT TOPIC call willbe hosted on the 8th and 10th.
Notification of these calls will be sent via email.
Likely HOT TOPIC calls include youth cessation, promotion task force efforts, andrecruiting, retaining and supervising quitline specialists.

N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
Emerging Issues and Opportunities in Quitline Operations“Serving Callers with Psychiatric Conditions: Considerations for Quitlines”
Scope of Current Practice
Below are summaries of descriptions of current protocols related to serving mentally ill callers that were sent toNAQC in response to our request for information from our membership on this topic.
American Cancer Society
According to ACS research, 40% of their callers have a depression indicator - they answer yes to thequestion, "have you felt sad and blue every day for the last two weeks?". This question is used as atriage point for some quitlines, as other ACS research indicates that these "yes" callers have bettersuccess rates with longer sessions.
ACS is also currently running a clinical trial, in collaboration with the Beck Institute, that is designed totest a specifically enhanced intervention for quitters who answer yes to the above question. Specificcounselors have been trained in cognitive therapy strategies that focus on reducing depression. Thehypothesis is that "depressed" callers who receive the enhanced protocol will have higher success ratesthan those who do not.
Nevada
Below is a description of how the Nevada Tobacco Users' Helpline™ addresses tobacco/nicotinedependence treatment to those individuals with coexisting medical, psychiatric and/or other addictiondisorders.
The Nevada Tobacco Users’ Helpline is a division of the University of Nevada School of Medicine,Department of Internal Medicine. The Helpline provides nicotine dependence treatment for all forms of tobacco (smoked and smokeless) and for individuals dependent on nicotine replacement therapies.The program includes these distinguishing characteristics:
Counselors are in compliance to the State of Nevada Board of Examiners for Alcohol, Drugand Gambling Counselors and provide substance abuse treatment for the drug nicotine.
Medically driven Research and evidenced-based Follows Center for Disease Control ‘Best Practices’

N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
Follows Agency for Healthcare Research and Quality Guidelines (AHRQ) Only uses FDA approved medications
The Helpline™ minimally hires counselors with a bachelor’s and/or master’s degree in an approvedsocial science field and qualify as an alcohol and drug counselor or counselor interns as specified by theState of Nevada Board of Examiners for Alcohol, Drug and Gambling Counselors.
Comorbid issues of the patient are addressed in treatment per ‘scope of practice’ of a certifiedintern/certified/licensed alcohol and drug counselors in complience to the Nevada Revised StatuesChapter 641C (NRS 641C) and the Nevada Administrative Code (NAC 641C) as specified by the Stateof Nevada Board of Examiners for Alcohol, Drug and Gambling Counselors.
The NRS 641C also requires complience to the Code of Federal Regulations Title 42 Volume 1, Part 2(42 CFR Part 2), regarding confidentiality of alcohol and drug abuse patient records and the HealthInsurance Portability and Accountability Act of 1996 (HIPAA) set forth in 45 CFR Part 160 regardingmedical privacy and national standards to protect the privacy of personal health information.
The Nevada Tobacco Users’ Helpline™ nicotine dependence program is defined as patient-centeredwhereby counselors use an integrated Systems and Solution Focused Theoretical Framework withmotivational interviewing to move patients through stages of change throughout the treatment process.
The counselors address the physiological and psychological effects of the drug nicotine as well as theharmful medical consequences resulting from tobacco use. The goal of the counseling process is tohelp an individual to sustain long term abstinence from tobacco/nicotine use/dependence and restorethe patient to optimal physical, emotional, mental and spiritual well being.
The counselor facilitates change through establishing a therapeutic relationship between counselor andpatient. This is supported by clinical interventions through counseling, education, support,pharmacotherapy as indicated, and relapse prevention regarding continued use and continued problempotential (short term and long term).
The counselor is in contact with other professional providers (i.e. Physician, Psychiatrist, OtherProfessional Counselors, MFT, LADC, LCSW, and LPC) as indicated in compliance to NAC 641C.
The counselor documents all clinical activity and management of drug withdrawal potential. Reportabledata collection is entered into the database by non-counseling staff daily.
The initial intake includes:o Informed consento Helpline™ office practiceso Well-being paradigmo Confidentiality/limits to confidentiality (Mandated reporting)

N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
o The patient in counseling indicates clear and immediate danger to themselveso The patient in counseling indicates clear and immediate danger to an individual in society The patient in counseling indicates direct involvement in child abuse or neglect The patient in counseling indicates direct involvement in elderly abuse or neglecto HIPAA Notice of Privacy Practiceo Release of Information Authorization as indicated for continuance of care treatment needs regarding
disclosure and exchanging of patient information and records.o Demographicso Bio/Psycho/Social Assessment of current information and tobacco use historyo Second Edition Revised American Society of Addictions Medicine (ASAM PPC-2R) Severity
Index Profile, which provides means for assessing: Diagnosis Six assessment dimensions to determine clinical severity for both mental and addiction disorders
(High, medium, low). Acute intoxication and/or withdrawal potential; Biomedical conditions and problems; Emotional, behavioral, cognitive conditions and problem Readiness to change [Treatment acceptance/resistance]; Relapse, continued use or continued problem potential; Recovery/living environment Treatment level of care based on ASAM PPC-2R criteria for five basic levels of careo Appropriate referrals to other medical, mental, social and other addictions.
“Nicotine, cocaine, heroin and alcohol all meet criteria as addictive and dependence producingdrugs… the risk of addiction following any use, the prevalence of frequent use among currentusers, and the occurrence of American Psychiatric Association, DSM-defined dependence amongcurrent users range from 2 to 10 times greater for cigarettes than for these other drugs”.Anthony et al. 1994, Exp. Clinc. Psychopharm; NIDA’s Monitoring The Future Survey, FDA in FedRegister, Aug 11, 1995; Surg Gen 1988.
“Nicotine is both a stimulant and a sedative to the central nervous system”. (National Institute onDrug Abuse/Info fax-Cigarettes and other Nicotine Products 13545).
The Helpline™ recognizes the benefit of quit lines, however, there is a need for proper education andtraining. The other issue we see is the appropriate education on interactions of the drug nicotine withother medications and nicotine’s impact on co morbid conditions. The issue of treating nicotine(reducing a drug, etc) becomes a public health issue. Some people become suicidal when withdrawingfrom nicotine. Nicotine reduction can cause some medications to be overdosed, others to be under

N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
dosed, including heart medications, diabetes medications, and psychiatric medications. In extremecases, reducing nicotine may cause seizure and death in some populations, i.e., schizophrenia (druginteractions). Chemicals in tobacco thicken the blood, and those on blood thinners, aspirin, etc. would beoverdosed. There are many public health and safety issues in the treatment of nicotine dependence. Justfor your information, more than half of our patients are self reporting coexisting issues. (Medical,mental or other addictions).
New Jersey
The protocol for New Jersey’s tobacco quitline does involve the determination of the state of the callerand prior experience with mental health issues. The caller has a brief explanation of how their particularcondition can interfere with their quitting efforts. From our perspective, for a quitlines counselor tobecome involved in treating a caller’s mental illness approaches practicing medicine and projects anenormous set of difficulties, not to mention liabilities.
Instead, these clients are referred to Quitcenters where counselors have had at least 5 days of training inpsychiatric conditions and Quitcenters are located at hospitals with full access to a physician. Thephysician will contact the physician treating the client for mental illness and discuss treatment beingreceived. The Quitcenter counselor can only treat tobacco dependence, but is usually aware of theproblems presented by certain mental illnesses. The client's own physician should be aware of thetreatment being received and be responsible for treating of the mental illness. The Quitcenter physicianand the patient's mental health physician must be aware of and agree on any pharmaceuticals to beutilized.

N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
Emerging Issues and Opportunities in Quitline Operations“Serving Callers with Psychiatric Conditions: Considerations for Quitlines”
Recent Reseach of Interest
Nicotine dependence and psychiatric disorders in the United States: results from the nationalepidemiologic survey on alcohol and related conditions.
Grant BF, Hasin DS, Chou SP, Stinson FS, Dawson DA.
Laboratory of Epidemiology and Biometry, Division of Intramural Clinical and Biological Research,National Institute on Alcohol Abuse and Alcoholism, National Institutes of Health, Bethesda, MD, [email protected]
BACKGROUND: No information is available on the co-occurrence of DSM-IV nicotine dependenceand Axis I and II psychiatric disorders in the US population. OBJECTIVES: To present national data onthe co-occurrence of current DSM-IV nicotine dependence and other psychiatric disorders by sex and toestimate the burden of all US tobacco consumption carried by nicotine-dependent and psychiatrically illindividuals. DESIGN: Face-to-face interviews. SETTING: The United States. PARTICIPANTS:Household and group-quarters adults (N = 43 093). MAIN OUTCOME MEASURES: Prevalence andcomorbidity of current nicotine dependence and Axis I and II disorders and the percentage of cigarettesconsumed in the United States among psychiatrically vulnerable subgroups. RESULTS: Among USadults, 12.8% (95% confidence interval, 12.0-13.6) were nicotine dependent. Associations betweennicotine dependence and specific Axis I and II disorders were all strong and statistically significant(P<.05) in the total population and among men and women. Nicotine-dependent individuals made uponly 12.8% (95% confidence interval, 12.0-13.6) of the population yet consumed 57.5% of all cigarettessmoked in the United States. Nicotine-dependent individuals with a comorbid psychiatric disorder madeup 7.1% (95% confidence interval, 6.6-7.6) of the population yet consumed 34.2% of all cigarettessmoked in the United States. CONCLUSIONS: Nicotine-dependent and psychiatrically ill individualsconsume about 70% of all cigarettes smoked in the United States. The results of this study highlight theimportance of focusing smoking cessation efforts on individuals who are nicotine dependent, individualswho have psychiatric disorders, and individuals who have comorbid nicotine dependence and otherpsychiatric disorders. Further, awareness of industry segmentation strategies can improve smokingcessation efforts of clinicians and other health professionals among all smokers and especially amongthe most vulnerable.

N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
Effects of motivational interviewing on smoking cessation in adolescents with psychiatricdisorders.
Brown RA, Ramsey SE, Strong DR, Myers MG, Kahler CW, Lejuez CW, Niaura R, Pallonen UE,Kazura AN, Goldstein MG, Abrams DB.
Brown Medical School/Butler Hospital, 345 Blackstone Blvd, Providence, RI 02906, [email protected] <[email protected]>
OBJECTIVE: To test the hypothesis that among adolescent smokers hospitalised for psychiatric andsubstance use disorders, motivational interviewing (MI) would lead to more and longer quit attempts,reduced smoking, and more abstinence from smoking over a 12 month follow up. DESIGN:Randomised control trial of MI versus brief advice (BA) for smoking cessation, with pre- and post-intervention assessment of self efficacy and intentions to change, and smoking outcome variablesassessed at one, three, six, nine, and 12 month follow ups. SETTING: A private, university affiliatedpsychiatric hospital in Providence, Rhode Island, USA. PATIENTS OR OTHER PARTICIPANTS:Consecutive sample (n = 191) of 13-17 year olds, admitted for psychiatric hospitalisation, who smokedat least one cigarette per week for the past four weeks, had access to a telephone, and did not meetDSM-IV criteria for current psychotic disorder. INTERVENTIONS: MI versus BA. MI consisted oftwo, 45 minute individual sessions, while BA consisted of 5-10 minutes of advice and information onhow to quit smoking. Eligible participants in both conditions were offered an eight week regimen oftransdermal nicotine patch upon hospital discharge. MAIN OUTCOME MEASURES: Point prevalenceabstinence, quit attempts, changes in smoking rate and longest quit attempt. Proximal outcomes includedintent to change smoking behaviour (upon hospital discharge), and self efficacy for smoking cessation.RESULTS: MI did not lead to better smoking outcomes compared to BA. MI was more effective thanBA for increasing self efficacy regarding ability to quit smoking. A significant interaction of treatmentwith baseline intention to quit smoking was also found. MI was more effective than BA for adolescentswith little or no intention to change their smoking, but was actually less effective for adolescents withpre-existing intention to cut down or quit smoking. However, the effects on these variables wererelatively modest and only moderately related to outcome. Adolescents with comorbid substance usedisorders smoked more during follow up while those with anxiety disorders smoked less and were morelikely to be abstinent. CONCLUSIONS: The positive effect of MI on self efficacy for quitting and theincrease in intention to change in those with initially low levels of intentions suggest the benefits of suchan intervention. However, the effects on these variables were relatively modest and only moderatelyrelated to outcome. The lack of overall effect of MI on smoking cessation outcomes suggests the need tofurther enhance and intensify this type of treatment approach for adolescent smokers with psychiatriccomorbidity.

N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
Nicotine withdrawal and psychiatric symptoms in cigarette smokers with schizophrenia.
Dalack GW, Becks L, Hill E, Pomerleau OF, Meador-Woodruff JH.
Ann Arbor VA Medical Center, University of Michigan, USA.
The prevalence of smoking is markedly elevated in schizophrenia. Low smoking cessation rates andreports that some smokers with schizophrenia experience an acute increase in symptoms during attemptsto quit smoking, suggest a self-medication model. Alternatively, smoking may modulate medication sideeffects. The effects of treated and untreated smoking abstinence on psychotic symptoms and medicationside effects were examined in this study. Nineteen outpatients with schizophrenia or schizoaffectivedisorder participated in a randomized, double-blind, balanced crossover study: 1 day of ad libitumsmoking followed by 3 days of acute smoking abstinence while wearing 22 mg/day active or placebotransdermal nicotine patches, with a return to 3 days of smoking between patch conditions. Dailysymptom and side-effect ratings, nicotine and cotinine blood levels were collected. Twelve subjectscompleted the study. Neither positive symptoms nor mood symptoms changed. An increase in negativesymptoms during the first abstinent day occurred in both placebo and active patch conditions, but wasnot sustained over subsequent abstinent days. Despite physiological signs of withdrawal, completers didnot endorse increased nicotine withdrawal symptoms. Dropouts reported higher withdrawal symptoms,but also had no increase in psychiatric symptoms in either phase of the study. Of note, dyskinesiasdecreased during abstinence and placebo patch treatment, but increased during abstinence and the activepatch conditions. Acute exacerbation of psychiatric symptoms is an unlikely explanation for anydifficulty smokers with schizophrenia have in early abstinence.
Benefits of and barriers to providing smoking treatment in methadone clinics: findings from anational study.
McCool RM, Richter KP, Choi WS.
Department of Preventive Medicine, University of Kansas School of Medicine, Kansas City, KS, USA.
Although smoking increases morbidity and mortality among patients in addictions clinics, few clinicsprovide routine smoking treatment. To understand staff attitudes toward treatment, we surveyed leadersof outpatient methadone treatment clinics nationwide. Our response rate was 59% (408/697). Most clinicleaders thought they should provide smoking treatment (76%) or refer patients for care (91%); however,fewer than half of these had provided treatment in the month prior to the survey. Leaders said smokingtreatment would benefit their clinics, patients and communities, but said barriers-primarily insufficient

N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
staff training-prevented routine care. Addressing these barriers could increase smoking treatment inaddictions clinics and save lives.
Independent effects of tobacco abstinence and bupropion on cognitive function in schizophrenia.
Evins AE, Deckersbach T, Cather C, Freudenreich O, Culhane MA, Henderson DC, Green MF,Schoenfeld DA, Rigotti NA, Goff DC.
Schizophrenia Program , the Tobacco Treatment and Research Center, Massachusetts General Hospital,Boston, MA 02114, USA. [email protected]
OBJECTIVE: The objective of this study was to examine the effects of tobacco abstinence andbupropion treatment on cognitive functioning in adult smokers with schizophrenia in the setting of arandomized, double-blind, placebo-controlled clinical trial of bupropion for smoking cessation.METHOD: Fifty-three adults with schizophrenia (DSM-IV) took part in a trial of bupropion for smokingcessation. Subjects were enrolled in the study from August 1999 to March 2003. Forty-five subjectsremained in the trial at week 4; 41 subjects, 19 taking bupropion and 22 taking placebo, completed thebaseline and week 4 cognitive assessments and were included in the analysis of adjusted effects ofabstinence and bupropion treatment on cognitive function. RESULTS: Controlling for bupropiontreatment and baseline performance, 7 days of tobacco abstinence was associated with slowed motorspeed (finger tapping) but was not associated with worsening of performance on tests of attention (AXContinuous Performance Test [AX-CPT]), verbal learning and memory (California Verbal LearningTest [CVLT]), working memory (digit span), or executive function/inhibition (Stroop) and was notassociated with worsening of any clinical measures. Controlling for abstinence status, bupropion wasassociated with reduction (improvement) in reaction time variability on the AX-CPT and with reductionin perseverative errors on the CVLT. CONCLUSION: We conclude that 1 week of tobacco abstinence isassociated with slowed motor speed but is not associated with detectable worsening in performance on arange of neuropsychological tests or clinical symptoms in the subset of patients who were able to quitsmoking. We also conclude that bupropion treatment may be associated with improvement in variabilityof attention.
Acceptance of nicotine dependence treatment among currently depressed smokers.
Haug NA, Hall SM, Prochaska JJ, Rosen AB, Tsoh JY, Humfleet G, Delucchi K, Rossi JS,Redding CA, Eisendrath S.
Department of Psychiatry, School of Medicine, University of California, San Francisco, [email protected]
N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
This study reports on baseline characteristics associated with acceptance and refusal of availablesmoking treatment among currently depressed smokers in a psychiatric outpatient clinic who wereenrolled in a larger clinical trial. The sample (N=154) was 68% female and 72% White, with a mean ageof 41.4 years and average smoking rate of 17 cigarettes/day. All participants were assigned to a repeatedcontact experimental condition; received a stage-based expert system program to facilitate treatmentacceptance; and were then offered smoking treatment, consisting of behavioral counseling, nicotinepatch, and bupropion. Acceptors (n=53) were defined as those accepting behavioral counseling andpharmacological treatment at some point during the 18-month study, whereas refusers (n=101) receivedonly the expert system. The number of days to treatment acceptance was significantly predicted by stageof change, with those in preparation entering treatment more quickly than contemplators orprecontemplators. In a logistic regression, the variables most strongly associated with acceptingtreatment were current use of psychiatric medication and perceived success for quitting. Severity ofdepressive symptoms, duration of depression history, and history of recurrent depression were notrelated to treatment acceptance. Findings have implications for the psychiatric assessment and treatmentof smokers in clinical settings. Psychiatric medication may play a significant role in smoking cessationtreatment acceptance by currently depressed smokers.
Acceptance of nicotine dependence treatment among currently depressed smokers.
Haug NA, Hall SM, Prochaska JJ, Rosen AB, Tsoh JY, Humfleet G, Delucchi K, Rossi JS,Redding CA, Eisendrath S.
Department of Psychiatry, School of Medicine, University of California, San Francisco, [email protected]
This study reports on baseline characteristics associated with acceptance and refusal of availablesmoking treatment among currently depressed smokers in a psychiatric outpatient clinic who wereenrolled in a larger clinical trial. The sample (N=154) was 68% female and 72% White, with a mean ageof 41.4 years and average smoking rate of 17 cigarettes/day. All participants were assigned to a repeatedcontact experimental condition; received a stage-based expert system program to facilitate treatmentacceptance; and were then offered smoking treatment, consisting of behavioral counseling, nicotinepatch, and bupropion. Acceptors (n=53) were defined as those accepting behavioral counseling andpharmacological treatment at some point during the 18-month study, whereas refusers (n=101) receivedonly the expert system. The number of days to treatment acceptance was significantly predicted by stageof change, with those in preparation entering treatment more quickly than contemplators orprecontemplators. In a logistic regression, the variables most strongly associated with acceptingtreatment were current use of psychiatric medication and perceived success for quitting. Severity of
N O R T H A M E R I C A N Q U I T L I N E C O N S O R T I U M
4142 E. Stanford Drive, Phoenix, AZ 85108
P 602 595 3273 F 602 368 5874 E [email protected]
www.naquitline.org
depressive symptoms, duration of depression history, and history of recurrent depression were notrelated to treatment acceptance. Findings have implications for the psychiatric assessment and treatmentof smokers in clinical settings. Psychiatric medication may play a significant role in smoking cessationtreatment acceptance by currently depressed smokers.
A meta-analysis of worldwide studies demonstrates an association between schizophrenia andtobacco smoking behaviors.
de Leon J, Diaz FJ.
Mental Health Research Center at Eastern State Hospital, 627 West Fourth St., Lexington, KY 40508,USA. [email protected]
A meta-analysis of worldwide studies, found by a 10-year literature follow-up and/or by searchingPubMed, was performed. Forty-two studies across 20 nations consistently demonstrated an associationbetween schizophrenia and current smoking (weighted average odds ratio, OR=5.9; 95% confidenceinterval, CI 4.9--5.7). In 32 male studies across 18 nations, the weighted average OR was 7.2 (CI, 6.1--8.3). In 25 female studies across 15 nations, the weighted average OR was 3.3 (CI, 3.0--3.6). Theassociation between schizophrenia and current smoking remained after using severe mentally ill controls(18 studies across 9 countries, weighted average OR was 1.9, CI 1.7--2.1) and controlling for othervariables (3 studies, adjusted ORs ranged 2-3). Heavy smoking (6 studies across 4 countries, ORsranged 1.9--6.4) and high nicotine dependence were more frequent in smokers with schizophrenia versusthe general population. There was no consistent evidence that heavy smoking or high nicotinedependence was more frequent in smokers with schizophrenia versus severe mentally ill controls.Cessation rates were lower in schizophrenia smokers versus the general population. Schizophreniapatients had a higher prevalence of ever smoking than the general population (9 studies across 6countries, weighted average OR=3.1, CI 2.4--3.8) and than severe mentally ill patients (5 studies across5 countries, OR=2.0, CI 1.6--2.4). Moreover, in two studies adjusting for confounders schizophreniapatients had an increased risk of starting daily smoking than controls. Thus, people who are going todevelop schizophrenia have risk factors that make them more vulnerable to start smoking.

Cessation for People withCessation for People withMental Health Issues: TheMental Health Issues: The
Role ofRole of QuitlinesQuitlines
Elissa KeszlerElissa Keszler
Smoking Cessation Leadership CenterSmoking Cessation Leadership Center
February 1 and 3, 2006February 1 and 3, 2006

Defining Mental IllnessesDefining Mental Illnesses
Mental illness refers to a variety ofMental illness refers to a variety ofdiagnosesdiagnoses
Range of experiences and symptomsRange of experiences and symptomsassociated with eachassociated with each
Mental illness is very common; mostMental illness is very common; mostpeople either have a diagnosis or are inpeople either have a diagnosis or are incontact with someone who doescontact with someone who does
Most are functional citizensMost are functional citizens

Who is Smoking?Who is Smoking?
Studies show 38Studies show 38--44 % of cigarettes in U.S.44 % of cigarettes in U.S.are smoked by people with mental illness orare smoked by people with mental illness orchemical dependency.chemical dependency.
Of those individuals, roughly half smokeOf those individuals, roughly half smokemore than 25 cigarettes per day.more than 25 cigarettes per day.
An estimated 200,000 smokers with mentalAn estimated 200,000 smokers with mentalillness or addiction die each year due toillness or addiction die each year due tosmoking, a figure highly disproportionate tosmoking, a figure highly disproportionate tothe number of those with mental disorders inthe number of those with mental disorders inthe general population.the general population.

International research showsInternational research shows……
Most smokers with mental illness self reportMost smokers with mental illness self reportthe desire to quit (roughly 70%)the desire to quit (roughly 70%)
They feel excluded from mainstreamThey feel excluded from mainstreamcessation programscessation programs
When they do receive treatment many findWhen they do receive treatment many findtheir symptoms are not exacerbated andtheir symptoms are not exacerbated andtheir improvement in overall health helpstheir improvement in overall health helpsthem live more functional livesthem live more functional lives
*ASH Scotland*ASH Scotland
The Changing Profile ofThe Changing Profile ofSmokersSmokers
As we whittle to the hard core of remainingAs we whittle to the hard core of remainingsmokers, more proportionally have mentalsmokers, more proportionally have mentalhealth or chemical dependency issues, orhealth or chemical dependency issues, orbothboth
Our Kaiser Permanente NorthernOur Kaiser Permanente NorthernCalifornia study is revealing at least 40California study is revealing at least 40percent of smokers in that system (12.2percent of smokers in that system (12.2percent prevalence) have copercent prevalence) have co--morbiditiesmorbidities

QuitlinesQuitlines Are Already Serving ThisAre Already Serving ThisPopulationPopulation
AsAs quitlinesquitlines mature and serve moremature and serve moresmokers, they are serving a growingsmokers, they are serving a growingnumber of people in this groupnumber of people in this group
As more become aware ofAs more become aware of quitlinesquitlines, they, theywill attract more of this group, many ofwill attract more of this group, many ofwhom are accustomed to reaching outwhom are accustomed to reaching out
Service quality varies greatlyService quality varies greatly
How CanHow Can QuitlinesQuitlines OptimizeOptimizeCessation?Cessation?
They will have to address this issueThey will have to address this issue
But how can we provide the best serviceBut how can we provide the best servicepossible for people with mental healthpossible for people with mental healthissues without placing an undue burden onissues without placing an undue burden onquitlinesquitlines??

Not a Black and White IssueNot a Black and White Issue
Recognize the spectrum of symptomsRecognize the spectrum of symptoms
A highly functioning mental healthA highly functioning mental healthsubgroup (already treated by primary caresubgroup (already treated by primary carephysicians or through talk therapy) couldphysicians or through talk therapy) couldsuccessfully usesuccessfully use quitlinesquitlines
Phone counselors should already bePhone counselors should already betrained to deal with lifetrained to deal with life--oror--deathdeathemergenciesemergencies

In an Ideal WorldIn an Ideal World……
Psychiatrists, psychologists, socialPsychiatrists, psychologists, socialworkers and counselors would all do theworkers and counselors would all do thewhole Five Awhole Five A’’s with every smokers with every smoker
None of the above would smokeNone of the above would smoke
All would consider it an integral part ofAll would consider it an integral part oftheir jobs to help smokers quittheir jobs to help smokers quit

The Harsh RealityThe Harsh Reality
Most clinicians working in mental healthMost clinicians working in mental healthconsider smoking irrelevant to their workconsider smoking irrelevant to their work
Many smokeMany smoke
Many are conflicted about helpingMany are conflicted about helpingsmokers quitsmokers quit
So smokers are often left without supportSo smokers are often left without supportor resourcesor resources

Where Will These Smokers Go?Where Will These Smokers Go?
To advertisedTo advertised quitlinesquitlines
QuitlinesQuitlines have to be prepared for theirhave to be prepared for theirfuture clientelefuture clientele
QuitlineQuitline counselors can partner withcounselors can partner withproviders and other cessation resources toproviders and other cessation resources togive this population the best treatmentgive this population the best treatmentavailableavailable

When Smokers withPsychiatric Health Issues Call
The California Smokers’ Helpline (CSH)
Presented byGary J. Tedeschi, Ph.D.

Objectives
Discuss commonly seen psychiatrichealth issues in a Quitline setting
Describe how the CSH responds tocallers with psychiatric health issues
CSH approach; Past & present
Assessment
Counseling considerations
Counselor training & supervision

Common Issues
Depressive disorder
Bipolar disorder Manic-depression (older term)
Thought disorder e.g., Schizophrenia
Anxiety disorder
Post traumatic stress disorder (PTSD)
Other chemical abuse/dependency e.g., Drug, alcohol

During a recent study…..
25% CSH smokers reported having beenin counseling or recovery programs.
Almost 15% CSH smokers reportedtaking some kind of psychotropicmedication.

CSH Approach: Past & present
Telephone counseling in San Diego (1990)
Clinical focus
Strict inclusion criteria
CA statewide program established (1992)
Public health focus
Loose inclusion criteria
Bridge clinical & public health approaches(1994-present)
Amended inclusion criteria

Assessment at Intake
Direct vs. indirect Is a direct approach always preferable?
Depression question Past vs. current (or both)?
Psychiatric treatment question Counseling, therapy or recovery?
Medication question Psychotropic medications?
Client report Unprompted disclosure

Assessment at Counseling
Medication question
Prompts further questions and discussionabout psychiatric treatment
Support question
Helps identify current level of professionalsupport and opens discussion on treatment
Client Report
Also prompts questions and discussionabout psychiatric treatment

Counseling Considerations
Psychiatric stability
How are the client’s symptoms?
Is the client in treatment?
How consistent is the client with treatment &how is it working?
Quitting history & symptoms
Past quit attempts are helpful indicators ofwhat to expect.
What changes in symptoms were noticed?

Counseling Considerations (cont.)
Biochemical factors
Nicotine acts much like a psychotropicmedication on brain chemistry.
Medications may need to be adjusted whenclients quit.
Counselor style
How much direction vs. facilitation should acounselor provide?

Counseling Considerations (cont.)
Content, length, & number of calls
Based on level of functioning and professionalsupport
Client contact with prescribing MD
Refer back to the primary physician
Professional support & referral
May need to help clients identify support intheir local area

Counselor Training & Supervision
Oversight by clinical director
Psychiatric health issues
Covered in initial training & ongoing
Risk assessment and emergencyprocedures
Covered in initial training & ongoing
Weekly counselor case review
Individual clients discussed in a groupsetting weekly counselor case review

Counselor Training & Supervision(cont.)
Special action record & review
Documentation of risk assessment, actiontaken, and recommendations.
Continuing ed. & advanced seminar
Regular in-service training
Call monitoring & tape review
Individual supervision (impromptu &scheduled)

Conclusion
Clients with psychiatric health issuescall Quitlines.
Clients with psychiatric health issueshave different levels of functioning.
Quitlines can serve this clientele basedon client level of functioning & localprofessional support: Full protocol
Single session and referral
Referral
NAQC Conference CallNAQC Conference Call
The Foundation for Innovationsin Nicotine Dependence
The Foundation for Innovationsin Nicotine Dependence

Linda Hyder Ferry MD, MPHPreventive Medicine Department
Linda Hyder Ferry MD, MPHPreventive Medicine Department
Loma Linda University
and
Loma Linda VA Healthcare System
Loma Linda University
and
Loma Linda VA Healthcare System
OverviewOverview
Mental health diseases impairthe quitting process
Telehealth management ofco-morbidity of tobaccoaddiction
Prescribing issues & Ethics
Mental health diseases impairthe quitting process
Telehealth management ofco-morbidity of tobaccoaddiction
Prescribing issues & Ethics

Veterans are at high riskVeterans are at high risk
58 yo, Engineer
4 ppd X 40 years
1st cig = 5 minutes
Quit - 3-5 days on NRT
Hx alcoholism andPost Traumatic Stress Disorder
58 yo, Engineer
4 ppd X 40 years
1st cig = 5 minutes
Quit - 3-5 days on NRT
Hx alcoholism andPost Traumatic Stress Disorder
Time to RethinkTime to Rethink
What are essential skills oftelephone counselors?
Who assumes Rx obligation risk of“First No Harm”?
Why not link to providers if highrisk?
What are essential skills oftelephone counselors?
Who assumes Rx obligation risk of“First No Harm”?
Why not link to providers if highrisk?

Why Do You Smoke?Why Do You Smoke?
How to screen for psychhistory?
Many unaware untilscreened—they just self-medicate
How to screen for psychhistory?
Many unaware untilscreened—they just self-medicate

Nicotine WithdrawalNicotine Withdrawal
Depressed mood
Insomnia
Irritability or anger
Impairedconcentration
RestlessnessAnxiety
Depressed mood
Insomnia
Irritability or anger
Impairedconcentration
RestlessnessAnxiety
Increase appetiteor weight gain
Decreased heartrate
Increase appetiteor weight gain
Decreased heartrate

Co-morbidity = high riskCo-morbidity = high risk
Chemical dependency
Psychosis
PTSD
Bipolar depression
Anxiety disorders
Major depression
Chemical dependency
Psychosis
PTSD
Bipolar depression
Anxiety disorders
Major depression

Psychiatric Tobacco PrevalencePsychiatric Tobacco Prevalence
90%85% 85%
70%
40%35%
0%
20%
40%
60%
80%
100%
CD Psychosis PTSD Bipolar Depression Anxiety
Affective DisordersAffective Disorders

Telehealth EthicsTelehealth Ethics
Body language informationmissing
Prescription risks
No verification of medications
History of depression, butfeels “fine” now
Body language informationmissing
Prescription risks
No verification of medications
History of depression, butfeels “fine” now
What is essential?What is essential?
“Why do you smoke?”
Psychiatric illness screen
Assess– Nicotine dependence
– Quitting History
Provide tailored advice
“Why do you smoke?”
Psychiatric illness screen
Assess– Nicotine dependence
– Quitting History
Provide tailored advice

Ultimate GoalUltimate Goal
Every smokershould be able to find help,
when they cannot quit
Every smokershould be able to find help,
when they cannot quit
Calgary Health Region Addiction Centre 1
A Community-Based Smoking Cessation Program for Persons with Mental Illness
Phase II Final Report
AADAC 2002/2004 Tobacco Reduction Grant Program
Submitted 8/31/2005
Prepared by: Shawn Currie, Ph.D., C. Psych.Addiction Centre - Foothills Medical CentreCalgary Health Region1403 – 29th Street NWCalgary, AB T2N 2T9Phone: (403) 944-2009Fax: (403) 944-2056E-mail Address: [email protected]
C E N T R E

Calgary Health Region Addiction Centre 2
Information on the Calgary Health Region and Addiction Centre
Formed in 1994 by the Government of Alberta, the Calgary Health Region (CHR)employs over 18,500 staff, making it the largest employer in the city. The CHR is alsothe largest fully integrated health care network in Canada. The four acute carehospitals offer specialized medical services and programs. The mission of the CHR isto provide an accessible, accountable and integrated, community-based health systemthat promotes shared responsibility for improved health.
Smoking-related diseases cost Calgary's hospitals an estimated $30 million forinpatient expenditures in 1996-1997. The top four causes of death in the CalgaryHealth Region are heart disease, lung cancer, stroke and chronic obstructive pulmonarydisease, all of which can be linked to smoking. Mental disorders account for 5 of the top10 diagnostic categories of leading causes of disabilities worldwide and 39% ofphysician billings in Alberta.
The Addiction Centre is a specialized program within the CHR. It is located atthe Foothills Medical Centre in Calgary, Alberta, Canada. The program operates underthe umbrella of the Regional Mental Health and Psychiatric Services portfolio and isaffiliated with the University of Calgary. The mandate of the Addiction Centre is theassessment and treatment of adults and adolescents with substance related issuescombined with either a major psychiatric (e.g. schizophrenia) or physical disorder (e.g.chronic pain). The Addiction Centre has an active research program and is a trainingfacility for residents, interns, and students from all disciplines.
Background - Smoking and psychiatric illness
The rate of smoking has decreased in Canada in the last 20 years (current rate22%) but remains disproportionately higher in persons with mental illness.1 Individuals withpsychiatric illness are twice as likely to smoke, with the prevalence of smoking in peoplewith schizophrenia an astonishing 80%. Population-based research estimates that 41% ofpersons with any form of current mental illness are regular smokers, and that 40% of thetobacco in the U.S. is consumed by persons with comorbid psychiatric disorders. 2 Despitethe high prevalence of smoking, individuals with chronic mental illness are an under-serviced and often neglected group. Unfortunately, health care providers have a history ofaccommodating smoking for those with a mental illness and very few mental healthprofessionals provide smoking cessation assistance to this population.3
Phase I
Overview
Phase I of our Tobacco Reduction Grant offered an evidence-based smokingcessation treatment to persons with mental illness. The treatment was facilitated byprofessionals and operated primarily out of two Calgary community-based programs forthe mentally ill, Calgary Association of Self-Help (CASH) and Potential Place. Theprimary goals of the project were:
Calgary Health Region Addiction Centre 3
1. Establish a smoking cessation program in the community of Calgary thatis specifically tailored for persons with severe and persistent mental illness
2. Determine the impact of this program on posttreatment, 3, 6 and 12-monthquitting rates.
3. Compare a brief (4 sessions plus booster) and longer version (8 sessions)of the treatment to determine which is more cost-effective and to identifyclient characteristics that may predict success.
Results
The first smoking cessation groups began in October 2002. We alternated runningthe 4-session and 8-session groups at the two sites, CASH and Potential Place. Thesmoking cessation program was very popular in the first 6 months. The quit rates atposttreatment, 3-month, 6-month, and 12-months at the end of Phase I were 10%, 20%,20%, and 30%, respectively. There was no significant difference in quit rates between the4 and 8-session groups. Other results are detailed in the Phase I final report.
Phase II
Overview
In Phase II, peer volunteers (mentally ill individuals who quit smoking) were trainedas co-facilitators. Stakeholders felt that involving peers in running the group would create abase of mentors to attract other smokers into the program and help sustain it in the future.During Phase II eight, complete 6-session smoking cessation groups were completed.Each group has included a peer volunteer as a co-facilitator. The groups were offered on arotating basis among these sites:
- Calgary Association of Self-Help- Potential Place- Alberta Mental Health Board Central Clinic- Foothills Hospital
In addition, a group was completed at the Claresholm Care Centre outpatientmental health clinic involving 15 patients. This was our first smoking cessation grouprun in a rural setting.
Results
The evaluation model for the program is shown in Table I. The smoking cessationgroups in Phases I and II were similar except for the addition of the peer volunteers andswitched to a 6-session format for all groups. Therefore, the results for quit rates andimpact on mental illness from Phases I and II are combined.

Calgary Health Region Addiction Centre 4
Table 1
Template for Evaluating the Smoking Cessation Groups
Domain Measure Interval
Engagement % of clients who attend at least one session ofgroup
Retention % of clients who attend more than half ofsessions
} Posttreatment
Attendance % of clients who attend follow-up } 3, 6, and 12-months
Smoking reduction # cigarettes/day
FTND
Quitting Abstinence, confirmed by CO monitor
Psychiatric symptomsBrief Symptom Inventory
Brief Psychiatric Rating Scale
Medication use
} Posttreatment, 3, 6, and 12months
Client satisfaction Client Satisfaction Questionnaire
Feedback from participants
Facilitator satisfaction Feedback from facilitators on program andquality of supervision
}Posttreatment &
Ongoing
Outcome measures
Smoking variables. At each assessment period, clients were asked about theirsmoking status. In addition, they completed the Fagerström Test for NicotineDependence (FTND).4 Scores on the 8–item FTND range from 0 to 10, with highervalues indicating greater dependence on nicotine. Level of carbon monoxide (CO) inexpired air was assessed using the piCO Smokerlyzer (Bedfont Scientific Ltd, 2002).Values of 10 ppm CO or less confirm abstinence from smoking in the past week.Biochemical verification also served as a powerful motivating tool for smokers trying toquit.
Psychiatric symptoms and functioning. The impact of quitting smoking onpsychiatric symptoms was assessed at each interval by the Brief Psychiatric RatingScale (BPRS). 5 The BPRS is an observor-rated scale with 16 items (anxiety, agitation,psychotic symptoms, etc.) each using an 8-point Likert scale. In addition, clientscompleted the Brief Symptom Inventory.6 The interviewing clinician also assessed theclient’s level of functioning using the Global Assessment of Functioning (GAF) scalefrom the DMS-IV. 7 The GAF ranges from 0 to 100 scale with higher values indicatinggreater functioning in the psychological, social and occupational domains.
Client Satisfaction Questionnaire (CSQ). 8 The 8-item CSQ survey assessesclient satisfaction with mental health treatment.
Calgary Health Region Addiction Centre 5
Peer volunteers
Two individuals, both ex-smokers with a history of serious mental illness, becameregular peer co-facilitators for the smoking cessation groups in Phase II. Because theseindividuals had little group facilitation experience, it was necessary to continue havingan experienced professional (psychiatric nurse) take the lead on organizing and runningthe smoking cessation groups. However, as the peers become more comfortable andexperienced, they gradually assumed a larger role in co-leading the groups. Theseindividuals have since become big advocates for the program and will remain involved iffurther funding is secured.
Participation and quit rates
To date, 128 smokers with mental illness have been recruited into the Phase I andPhase II smoking cessation groups. Another 40 have attended a less-intensiveintervention called the Smoker’s Check-up. 90% of smokers attend at least 1session and 60 percent have attended more than half of the group sessions.Attendance at the follow-up assessments is about 90%. The characteristics ofrecruited smokers are shown in Table 2.
The 6 and 12-month quit rates are 20% and 18%, respectively, which arecomparable to mentally healthy smokers (average quit rate of 15% for groupcounselling programs).9 In addition, the non-quitters show reductions in smoking.We are continuing to collect follow-up data on the 6-session smoking cessationgroups.
There was no significant difference in the quit and participation rates between theprofessional-only led groups in Phase I and the professional plus peer volunteer ledgroups in Phase II. However, satisfaction with the groups was generally higheramong clients in Phase II. Clients appreciate having a program that is tailored forpersons with mental illness and having peers involved in the group to serve as rolemodels.

Calgary Health Region Addiction Centre 6
Table 2
Demographic Characteristics of Cessation Group Participants (N = 128)
Variable Mean SD or %
Age (years) 46.5 9.4
Gender (% male) 42
Years of education 12
Primary diagnosis
Schizophrenia 55
Mood disorders 35
Other 10
GAF (Axis V) 57.0 10.0
Smoking history
Age of smoking initiation (years) 17.2 7.5
Number of quit attempts in lifetime 2.5
Degree of concern about smoking (0=not at all to4=seriously)
3.5
Fagerström Test for Nicotine Dependence (0-10) 6.3 2.1
Impact of quitting on mental illness
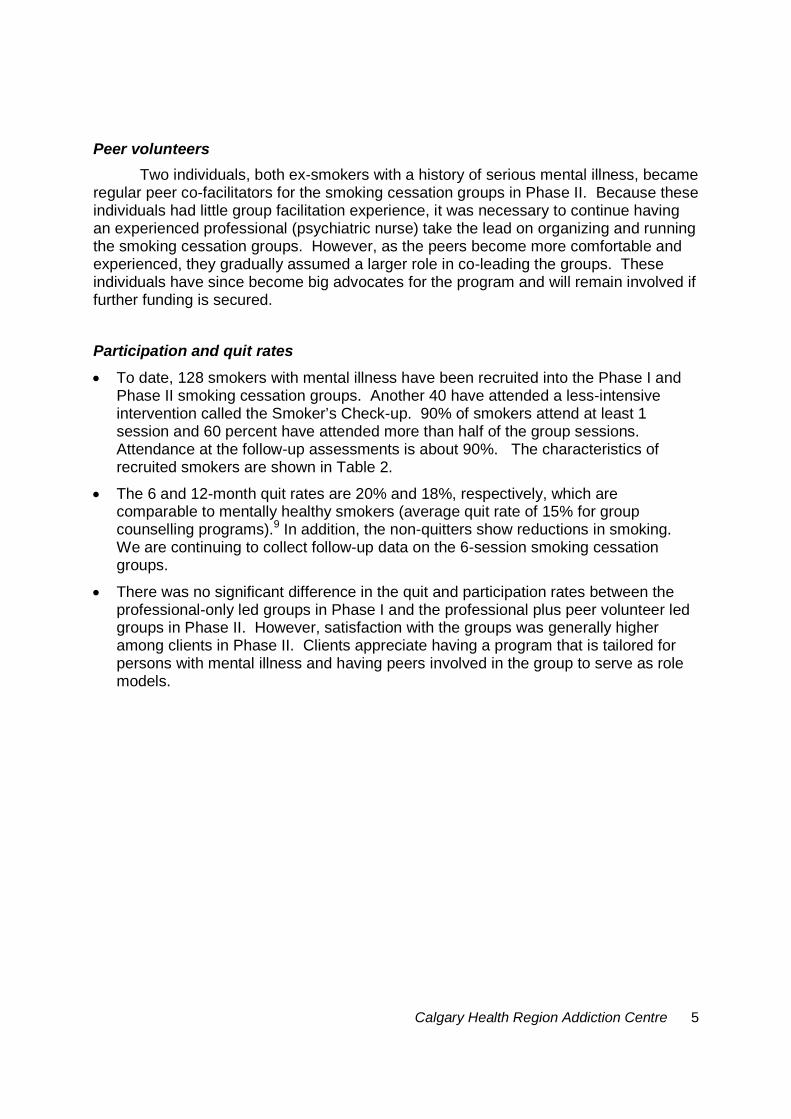
As found in the Phase I results, quitting smoking has no deleterious impact onsymptoms of mental illness. As shown in Figure 1, persons who quit at 12 monthsexhibit the same level of functioning (GAF scale) as persons still smoking. Overallsymptom level, as measured by the Brief Symptom Inventory, also did not differbetween the groups. Hence, there is no evidence that quitting smoking exacerbatesmental illness.
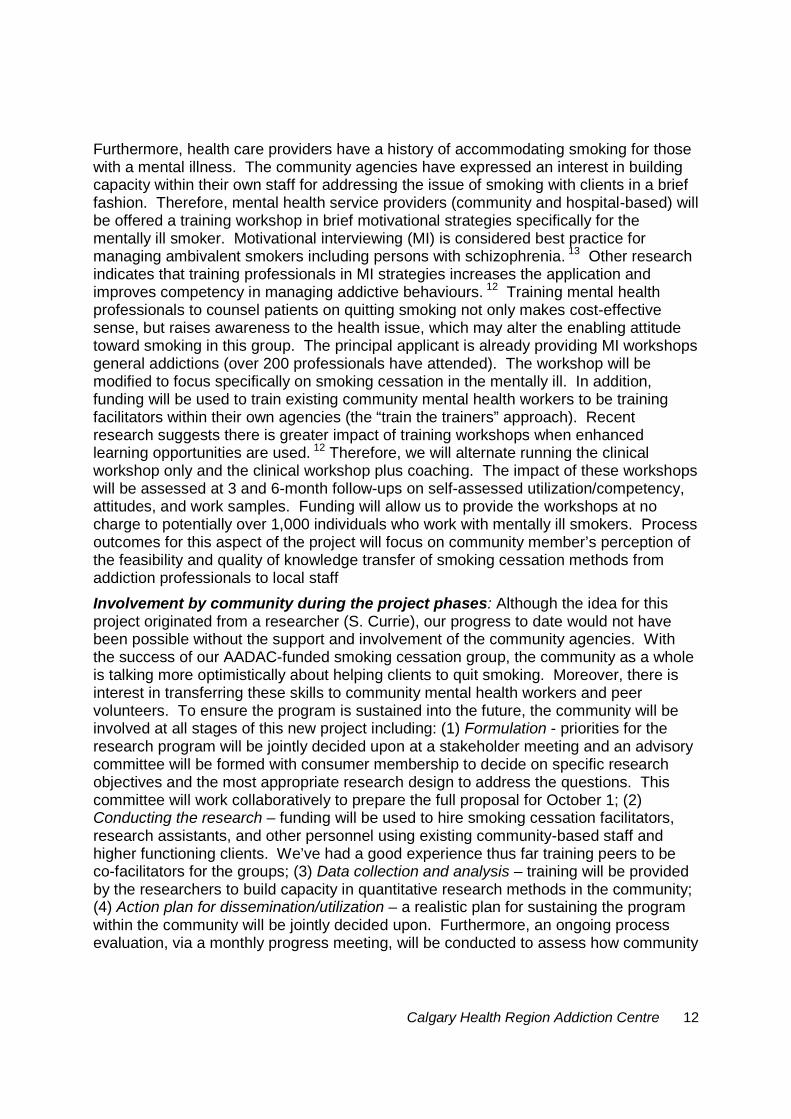
As shown in Figure 2, quitting smoking had no negative effect on thoughtdisturbances or affective distress as measured by the BPRS. In fact, quittersdemonstrated significantly less affective distress than individuals still smoking at 12months.
We examined medication changes in clients who successfully quit smoking and clientswho were unable to quit. It is worth noting that medication changes are common in thispopulation. However, we did not detect any overall difference in medication use amongquitters and smokers at the 12-month follow-up. Furthermore, those who quit displayedno change in medication use from the pre-quitting period.

Calgary Health Region Addiction Centre 7
Figure 1. Change in Brief Symptom Inventory scores and GAF rating across assessmentintervals in persons still quit at 12 months compared to those still smoking. No groupdifferences (p > .05) found at any time point.
Figure 2. Change in Brief Psychiatric Rating Scale (BPRS) scores for thought disturbances andaffective distress across assessment intervals in persons still quit at 12 months compared tothose still smoking. No group difference (p > .05) in thought disturbance scores found at anytime point. Quitters exhibited less affective distress than smokers at the 12-month follow-up (p< .001).
0
0.5
1
1.5
2
2.5
Baseline Post 3M FU 6M FU 12M FU
Brief Symptom Inventory
Quit Smoking
20
30
40
50
60
70
80
Baseline Post 3M FU 6M FU 12M FU
GAF Scale
GA
F(0
-10
0)
2
3
4
5
6
7
8
9
10
Baseline Post 3M FU 6M FU 12M FU
BPRS - Thought Disturbances
Quit Smoking
4
6
8
10
12
Baseline Post 3M FU 6M FU 12M FU
BPRS - Affective distress

Calgary Health Region Addiction Centre 8
Impact on Health Professionals and Community Agencies
The community agencies supporting the program report greater awareness of thehealth issues surrounding smoking in their clients. One community agency closed along-standing smoking room as a result of the program’s continued presence.Another agency noted that non-smoking clients now outnumber the smokers, a trendthey had never observed before.
Physicians are now more aware of the issue and, in turn, have been well supportedby the program. To date, approximately 150 physicians have received a detailedinformation package and a support guide specifically for clients with a mental illness.Feedback has been very positive.
The program has provided training opportunities for nurses, undergraduate students,and mental health professionals.
Promotion and Awareness
A full-length article on the smoking cessation program for the mentally ill appeared inthe physician magazine, Vital Signs.
Dr. Currie was interviewed about the smoking cessation program for the fall issue ofthe mental health magazine, Balance.
This project was featured at the AADAC-sponsored World No Tobacco Daycelebration in Edmonton on May 30, 2005. Our presentation was attended by over150 individuals. We are also scheduled to present the program at the GlobalPerspectives on Chronic Disease Management 2005 conference in September.
Building Capacity
Jordyn Kartlyn, a recent graduate of the University of Calgary nursing program,began working on the smoking cessation project in early 2004 with little experiencein the area. In a short time, she has become an expert on smoking cessationmethods for persons with mental illness and will serve as a mentor/educator forother new nurses in the area. She will be completing her Tobacco TreatmentSpecialist Certification at the Mayo Clinic in the fall of 2005. She also works as anoccupational health nurse at Nortel where she has initiated a smoking cessationprogram for staff.
The AADAC-funded smoking cessation program has provided training opportunitiesfor other nurses, undergraduate students, and mental health professionals.
A small group of peer volunteers (individuals with a mental illness, who have quitsmoking), have been trained as co-facilitators. As well, clinical students have gainedthe skills necessary to complete assessments and be involved in co-facilitating thegroup.

Calgary Health Region Addiction Centre 9
In 2003 we provided a half-day training session on smoking and psychiatricdisorders to the AADAC Smoker’s Help Line counsellors in Edmonton. This sessionwas well received and was attended by approximately 10 counsellors and nurses.The session was also videotaped for the counsellors that could not attend.
Inservices on smoking cessation have been provided to the mental health programstaff of the FMC and Claresholm Care Centre.
The Addiction Centre has been contacted regarding the possibility of expanding theprogram to Alberta Hospital Edmonton and training co-facilitators for this location.
Feedback from consumers who have taken the program
90% of clients rate the smoking cessation program as good or excellent and 95%would recommend the program to other smokers.
The most common suggestions for improving the group were:
o Longer duration
o Longer and more frequent sessions
o More stringent criteria for entry—for example, restrict group to individuals whoare truly committed to wanting to quit smoking
o More support between sessions and after group ended
o Provide NRT at no charge to participants.
Looking to the Future
Two options are being explored to sustain the program indefinitely. Smokingcessation in the mentally ill has been named as a service priority in the CHR mentalhealth plan being submitted to Alberta Health in the fall. It is possible that CHR MentalHealth and Psychiatric Services will allocate permanent resources to sustain theprogram indefinitely.
We are also applying for a community-based research grant from the CanadianTobacco Control Research Initiative. Our letter of intent was successful in June 2005(the accepted letter of intent is provided below). This resulted in a small grant ($5,000)to assist in developing the full proposal (maximum grant is $250,000/year for five years)that is due October 1, 2005. This preliminary funding has been used to hold communitystakeholder meetings to solicit input for planning the full proposal. Between June andSeptember 2005, over 60 community stakeholders (community and hospital-basedmental health professionals and consumers including graduates of the AADAC-fundedSC program) will have been consulted in a series of in-person meetings, telephoneinterviews, and focus groups. Each meeting reviewed the progress to date and soughtinput on the following core issues:
How can the community better be utilized in providing and evaluatinginterventions?

Calgary Health Region Addiction Centre 10
How should outcomes be assessed?
Should interventions target persons with less severe mental illness(depression, anxiety disorders)?
How can services be made sustainable over time?
How can capacity be built in the existing mental health treatment system tomore routinely address smoking in this population?
What can be done to attract more smokers with mental illness into making aquit attempt?
These consultations have been extremely useful. Support for the program is veryhigh. If successful with the full proposal, funding will be used to significantly expand therange of interventions for this population of smokers. Based on stakeholder input fromthese and previous meetings, our next project will involve three core but integratedcomponents: (1) smoking cessation treatment for individuals ready to quit; (2) a consumer-driven social marketing and education campaign on smoking and mental health; (3) trainingof mental health professionals in brief counseling methods for smoking cessation. We feelthat such a coordinated approach, which targets smokers across the continuum of stage ofreadiness to change, will have the best chance of success. Furthermore, research hasshown that a concurrent multipronged tobacco reduction strategy focusing on a targetgroup of smokers is more effective than an individual intervention. Several contextualfactors should also be noted that make this project especially timely. For example, a totalsmoking ban now exists on all CHR property (the only such total smoking ban on hospitalproperty in Canada). Although the inpatient psychiatric units are exempt from the smokingban, the smoking rooms on these units will be closed in 2006. Furthermore, the communityhousing for the mentally ill operated by the CHMA will soon be smoke-free and Calgary isconsidering a by-law to ban smoking in all public locations. These factors combined withother government interventions such as prohibitions on tobacco advertising and high taxesshould only enhance the impact of our program.
Letter of Intent - CTCRI Proposal for Funding
Setting: Smoking-related diseases cost the Calgary Health Region (CHR) an estimated$30 million every year for inpatient expenses alone. Although the general public hasrelatively broad access to smoking cessation services in the CHR, the availableprograms are designed for persons without mental health problems. Furthermore, thereis an associated cost ($15 -$225) which can pose a barrier for individuals on a limited,fixed income. In 2003-2004, the CHR’s mental health programs provided service toover 30,000 clients with mental disorders. Using a conservative 40% rate of smoking inthis group, at least 12,000 clients are available for this research program. This projectis timely given that opportunities to smoke are becoming more restrictive in the region—a total smoking ban exists on CHR property which soon will be extended to communityhousing for the mentally ill.

Calgary Health Region Addiction Centre 11
Who is the community? For the purpose of this project the community includesmentally ill clients, their families, and the agencies and professionals providing serviceand support to these clients.
Objectives: The primary objective is to develop a sustainable, community-drivensmoking cessation program for mentally ill clients in the CHR. In light of the initialsuccess of our tobacco reduction program, we propose to significantly expand theintervention based on greater community involvement. The response from thecommunity thus far has been overwhelmingly positive toward the program. All agreethat a service and knowledge gap exists concerning smoking in the mentally ill, and thateffective methods of helping individuals to quit need to be researched. The communityhas also been involved in establishing and providing the necessary infrastructure to runthe smoking cessation program. However, there has been less involvement from thecommunity in running the actual cessation groups and in the research and evaluationside of the program. For our CTCRI proposal, greater involvement from the communityat all stages of the project is proposed. Furthermore, outcomes from the project willinclude both tobacco reduction endpoints and a process evaluation of the sustainabilityof conducting this type of research in this particular community. This approach isconsistent with the Participatory Action Research model in which ‘”the process is themethod.”10
Comprehensive smoking cessation services for mentally ill clients: The smokingcessation group, offered on site at the local community agencies, will be the mainintervention. Funding will be used to hire group facilitators using existing community-based mental health workers. Based on feedback from consumers and communityagencies, the following modifications to the program will be made: (1) Longer-termsupport is desired. We have observed that many mentally ill smokers quit after ratherthan during the 6-session group. Therefore, we will add a biweekly post-grouptelephone support (up to the 6-month follow-up) component. These brief telephonesessions will employ motivational enhancement strategies to help the smoker quit orprevent relapse; (2) Training more peers as mentors and group co-facilitators forpersons trying to quit. Involving peers in the actual smoking cessation group will createa base of mentors to attract other smokers into the program; (3) The biomedicalcomponent will be enhanced by having prospective smokers assessed and followed bya psychiatrist-expert in smoking cessation (WW or DC) before and after the group; (4)Nicotine patches will be provided at no charge, and; (5) Augmenting the groupcessation program with a targeted social marketing campaign, designed usingcommunity and client input, aimed at attracting more mentally ill smokers into making aquit attempt. Process outcomes will be evaluated on an ongoing basis with a specificfocus on (a) how community members perceive the quality of the partnership betweenaddiction professionals and local staff in delivering such interventions, (b) the valueassigned to, and feasibility of assessing tobacco reduction outcomes in the traditionalway (i.e., conducting 6 and 12-month follow-ups) in a community-based program, and(c) whether the needs of clients and staff in the community are being met in the smokingcessation program.
Training mental health workers in brief counseling methods for cessation: Veryfew mental health professionals counsel their patients to quit.3,11 Lack of confidenceand skill in managing addictions has been identified as a significant barrier.12
Calgary Health Region Addiction Centre 12
Furthermore, health care providers have a history of accommodating smoking for thosewith a mental illness. The community agencies have expressed an interest in buildingcapacity within their own staff for addressing the issue of smoking with clients in a brieffashion. Therefore, mental health service providers (community and hospital-based) willbe offered a training workshop in brief motivational strategies specifically for thementally ill smoker. Motivational interviewing (MI) is considered best practice formanaging ambivalent smokers including persons with schizophrenia. 13 Other researchindicates that training professionals in MI strategies increases the application andimproves competency in managing addictive behaviours. 12 Training mental healthprofessionals to counsel patients on quitting smoking not only makes cost-effectivesense, but raises awareness to the health issue, which may alter the enabling attitudetoward smoking in this group. The principal applicant is already providing MI workshopsgeneral addictions (over 200 professionals have attended). The workshop will bemodified to focus specifically on smoking cessation in the mentally ill. In addition,funding will be used to train existing community mental health workers to be trainingfacilitators within their own agencies (the “train the trainers” approach). Recentresearch suggests there is greater impact of training workshops when enhancedlearning opportunities are used. 12 Therefore, we will alternate running the clinicalworkshop only and the clinical workshop plus coaching. The impact of these workshopswill be assessed at 3 and 6-month follow-ups on self-assessed utilization/competency,attitudes, and work samples. Funding will allow us to provide the workshops at nocharge to potentially over 1,000 individuals who work with mentally ill smokers. Processoutcomes for this aspect of the project will focus on community member’s perception ofthe feasibility and quality of knowledge transfer of smoking cessation methods fromaddiction professionals to local staff
Involvement by community during the project phases: Although the idea for thisproject originated from a researcher (S. Currie), our progress to date would not havebeen possible without the support and involvement of the community agencies. Withthe success of our AADAC-funded smoking cessation group, the community as a wholeis talking more optimistically about helping clients to quit smoking. Moreover, there isinterest in transferring these skills to community mental health workers and peervolunteers. To ensure the program is sustained into the future, the community will beinvolved at all stages of this new project including: (1) Formulation - priorities for theresearch program will be jointly decided upon at a stakeholder meeting and an advisorycommittee will be formed with consumer membership to decide on specific researchobjectives and the most appropriate research design to address the questions. Thiscommittee will work collaboratively to prepare the full proposal for October 1; (2)Conducting the research – funding will be used to hire smoking cessation facilitators,research assistants, and other personnel using existing community-based staff andhigher functioning clients. We’ve had a good experience thus far training peers to beco-facilitators for the groups; (3) Data collection and analysis – training will be providedby the researchers to build capacity in quantitative research methods in the community;(4) Action plan for dissemination/utilization – a realistic plan for sustaining the programwithin the community will be jointly decided upon. Furthermore, an ongoing processevaluation, via a monthly progress meeting, will be conducted to assess how community

Calgary Health Region Addiction Centre 13
representatives feel the project is developing and ensure they continue to feel theirneeds are being met.
To determine the specific roles of a each stakeholder in the project, stakeholdermeetings with representatives from CHR mental health programs (hospital andcommunity-based), family physicians, the Canadian Mental Health Association,graduates from the current smoking cessation program (both quitters and non-quitters),smoking cessation experts and researchers will be held between June and September2005. Additionally, focus groups will be held with clients not involved in the program todate to determine their needs regarding smoking cessation. Feedback from thesemeetings will help determine the final methods to be used for October 1 proposalsubmission.
Exploration of gender issues: Males are more successful at quitting smoking thanfemales but this trend has not been examined in mentally ill smokers. Fear of weightgain is a salient concern for females thinking of quitting, but this has not emerged as anissue in the female smokers we’ve treated to date. Gender differences in quittingsuccess among the mentally ill will be examined in our smoking cessation program. Weare also interested in exploring gender differences in mental health professionals’willingness to address smoking with their clients.
Research team: This project represents a partnership involving the Addiction Centre,Canadian Mental Health Association, the CHR Tobacco Reduction team, PotentialPlace, and Schizophrenia Society of Alberta. The individuals representing theseagencies have committed to being involved in all aspects of the project; there specificroles will be decided at subsequent stakeholder meetings. Although not listed as teammembers, we have the support and cooperation of the Calgary Association of Self-Help,and AADAC.

Calgary Health Region Addiction Centre 14
References
1. Ziedonis, D., Kosten, T., Glazer, W., & Frances, R. (1994). Nicotine dependence andschizophrenia. Hospital and Community Psychiatry, 45, 204-206.
2. Lasser, K., Boyd, W., Woolhandler, S., Himmelstein, D., McCormick, D., & Bor, D.(2000). Smoking and mental illness: a population-based prevalence study. JAMA, 284,2606-2610.
3. Himelhoch, S. & Daumit, G. (2003). To whom do psychiatrists offer smoking-cessation counseling? Psychiatry, 160, 2228-2230.
4. Heatherton, T. F., Kozlowski, L. T., Frecker, R. C., & Fagerstrom, K. (1991). TheFagerstrom test for Nicotine Dependence: a revision of the Fagerstrom ToleranceQuestionnaire. British Journal of Addiction, 86, 1119-1127.
5. Steinberg, M. L., Ziedonis, D. M., Krejci, J. A., & Brandon, T. H. (2004). Motivationalinterviewing with personalized feedback: A brief intervention for motivatiing smokerswith schizophrenia to seek treatment for tobacco dependence. Journal of Consulting &Clinical Psychology, 72, 723-728.
5. Ventura, J., Lukoff, D., Nuechteriein, K., Liberman, R. P., Green, M. F., & Shaner, A.(1993). Manual for the Expanded Brief Psychiatric Rating Scale (BPRS). InternationalJournal of Methods in Psychiatric Research, 22, 1-20.
6. Derogatis, L. R. & Melisaratos, N. (1983). The Brief Symptom Inventory: Anintroductory report. Psychological Medicine, 13, 595-605.
7. American Psychiatric Association (1994). Diagnostic and statistical manual of mentaldisorders (4th ed). Washington, D.C.: Author.
8. Larsen, D. L., Attikinsson, C. C., Hargreaves, W. A., & Nguyen, T. D. (1979).Assessment of client/patient satisfaction: Development of a general scale. Evaluationand Program Planning, 2, 197-207.
9. Abrams, D. B., Niaura, R., Brown, R. A., Emmons, K. M., Goldstein, M. G., & Monti,P. M. (2003). The Tobacco Dependence Treatment Handbook. New York: GuilfordPress.
10. Kidd, S. A. & Kral, M. J. (2005). Practicing participatory Action Research. Journal ofCounseling Psychology, 52, 187-195.
11. McChargue, D. E., Gulliver, S. B., & Hitsman, B. (2002). Would smokers withschizophrenia benefit from a more flexible approach to smoking treatment. Addiction,97, 785-793.
12. Miller, W. R., Yahne, C. E., Moyers, T. B., Martinez, J., & Pirritano, M. (2004). Arandomized controlled trial of methods to help clinicians learn motivational interviewing.Journal of Consulting & Clinical Psychology, 72, 1050-1062.
Mayo Clinic Tobacco Quitline
Depression screeningThe U.S. Preventive Services Task Force reports that a positive response to either of thetwo questions are as effective in screening for depression as other longer screeninginstruments. Both questions are asked of every caller who receives a clinical assessmentfrom MCTQ counselor. We know that depression can negatively impact theeffectiveness of treatment for tobacco dependence. It is, therefore, in the best interest ofthe callers who are treated by MCTQ that each member be screened for depression ateach assessment.
If a caller answers yes to either screen question, he or she will also be screened for intentto inflict self harm.
If a caller responds positively to depression screen and yes to intent to inflict harm, localemergency services will be contacted to make an in person site visit to assess thesituation.
If a caller responds positively to depression screen but negatively to intention to self-harm questions, the counselor will explain how depression can lessen the effectiveness oftobacco dependence treatment. The caller will be encouraged to talk with referringphysician or with a professional about treatment for current depression symptoms.
Alcohol screeningThe U.S. Preventive Services Task Force found good evidence that screening canaccurately identify callers with alcohol consumption patterns that place the person at riskfor increased morbidity and mortality. The four item CAGE is cited as a popular, easy-to-use, effective tool for detecting alcohol abuse or dependence. The questions are askedof every caller who receives a clinical assessment from MCTQ counselor. We know thatalcohol use problems and tobacco use frequently coincide. Alcohol use can cause relapsein those callers who are recovering from nicotine dependence. It is, therefore, in the bestinterest of callers who are treated at MCTQ that each caller be screened for alcohol useproblems.
A positive screen is defined as a response of “yes, this has occurred within the past 12months” to two or more of the CAGE questions. When a member has a positive screen,he or she will be informed that the score indicates a possible problem with alcohol. Therelationship between nicotine and alcohol will be explained. The caller’s motivation tochange and motivation for a referral to an appropriate substance abuse program will beassessed.

Mayo Clinic Tobacco QuitlineGUIDELINES FOR ALCOHOL PROBLEMS SCREENING
PURPOSE
Alcohol use problems and tobacco use frequently coincide. Alcohol use can cause relapse inthose members who are recovering from nicotine dependence. It is, therefore, in the best interestof members who are treated at the MCTQ that each member be screened for alcohol use problemsat each call. This document defines the procedure for screening each member and the procedureto follow if the member screens positive.
Procedure
Screening questions
The U.S. Preventive Services Task Force (USPSTF) found good evidence that screening canaccurately identify members with alcohol consumption patterns that place the person at risk forincreased morbidity and mortality. The four item CAGE is cited by the USPSTF as a popular,easy-to-use, effective tool for detecting alcohol abuse or dependence. This instrument will beused during intake of members at MCTQ.
If there is a positive CAGE screen for alcohol problems
A positive screen is defined as a response of “yes, this has occurred within the past 12 months” totwo or more of the CAGE questions. When a member has a positive screen, he or she will beinformed that the score indicates a possible problem with alcohol. The relationship betweennicotine and alcohol will be explained. The patient’s motivation to change and motivation for areferral to an appropriate substance abuse program will be assessed. If the member is currentlymotivated to make a change, an appropriate referral will be made to the member. If the memberis not currently motivated to address this, the CAGE results will be charted and the member willbe provided a brief motivational intervention and the screen result and intervention will bedocumented in the clinical record.
Additional questions asked
Ask about current drinking patterns. We will not recommend Zyban use if a caller admitsto the following consumption of alcohol:Men: More than 14 drinks per week, 4 drinks on one occasion, 2 drinks per day.Women: More than 7 drinks per week, 3 drinks on one occasion, 1 drink per day.If sober and no drink in past 3 months, then okay to recommend Zyban.

Mayo Clinic Tobacco QuitlineGUIDELINES FOR DEPRESSION SCREENING
PURPOSE
Depressive disorders are much more often found among patients who use tobacco. Depressioncan negatively impact the effectiveness of treatment for tobacco dependence. It is, therefore, inthe best interest of patients who are treated at MCTQ, that each member be screened fordepression at each assessment. This document defines the procedure for screening each memberand the procedure to follow if the patient screens positive.
Procedure
Screening questionsThe U.S. Preventive Services Task Force (USPSTF) reports that a positive response to either oftwo questions are as effective in screening for depression as other longer screening instruments.These questions are listed below. Both will be asked of every patient who receives a clinicalassessment from a MCTQ counselor and this will be documented in the patients’ chart:
1. Over the past two years, have you felt down, depressed, or hopeless?2. Over the past two weeks, have you felt little interest or pleasure in doing things?
If there is a positive screen for depression
If a member answers yes to either screen questions (one or two above), he or she will be screenedfor intent to inflict self-harm. The U.S. Preventive Services Task Force finds insufficientevidence for routine screening to detect suicide risk1, however the following questions will beasked of any member who answers yes to one or two above so that the best referral for additionalhelp can be determined.
1. Have you had any thoughts of harming yourself or others? (Only if yes, go to twootherwise proceed to B below.)
2. Do you have a plan to harm yourself or another? (Only if yes, go to three otherwiseproceed to B below.)
3. Do you think that you will harm yourself or another?
A.) If member responds yes to all three questions concerning intention to self-harm, thefollowing step will be taken while the member remains on the telephone: local emergencyservices will be contacted to make an in person site visit to assess the situation.
B.) If patient responds no to any of the intention to self-harm questions, the MCTQ counselorwill explain how depression can lessen the effectiveness of tobacco dependence treatment. Themember will be encouraged to talk with referring physician or with a professional about treatmentfor current depression symptoms.

Wellness ProgramsMayo Clinic Tobacco Quitline
Depression Screening/Cage Questions
Have you ever received treatment for depression? (Not a trigger for “intent toharm” screening questions)
No – neverYes – within past 12 monthsMore than twelve months ago
In the past two weeks, have you felt sad, blue or depressed most days or everyday?
Yes No No answer
In the past two weeks, have you felt little interest or pleasure in doing things mostdays or everyday?
Yes No No answer
If yes to either of the last two above questions, ask “Have you had any thoughts ofharming yourself or others?”
Yes No No answer
If yes to the above question, “Do you have a plan to harm yourself or another?”
Yes No No answer
If yes to the above question, “Do you think that you will harm yourself or another?”
Yes No No answer
Do you now, or have you ever, drank alcohol, including beer, wine, or distilledspirits?
Yes No No answer
Have you ever felt like you should cut down on your drinking in the past 12months?
Yes No No answer
Have people annoyed you by criticizing your drinking in the past 12 months?

Yes No No answer
Have you ever felt bad or guilty about your drinking in the past 12 months?
Yes No No answer
Have you ever had a drink first thing in the morning to steady your nerves or getover a hang-over (eye opener) in the past 12 months?
Yes No No answer
How much do you drink per week?_______________________________________________
Do you ever drink more than 3 or 4 drinks on one occasion?
Yes No No answer
How often per month do you drink more than 3-4 drinks on one occasion?_______________________________________________
Have you ever received treatment for alcohol or other drugs?
No – neverYes – with past 12 monthsMore than 12 months ago
Current alcohol or drug use concerns?
Yes No No answer
Mental Illness
Anxiety Disorder Past drug addictionDepression SchizophreniaCurrent alcohol abuse OtherCurrent illegal drug useCurrent marijuana useDepressionPast alcoholism

1
Scope of Work: Tobacco Use Prevention and Control Foundation Grant
January 5, 2005
Project Overview
Prevalence
According to the Centers for Disease Control and Prevention, Behavioral Risk FactorSurveillance System Survey Data, 2002, the rate of tobacco use in Ohio is 26.6% versus22.5% nationwide. Even more striking are the disproportionately high rates of tobaccouse and nicotine dependence among individuals with mental illness and/or substanceabuse disorders. For example, approximately 55.5% of individuals with nicotine use anddependence have a comorbid psychiatric disorder, including mental illness and/orsubstance abuse disorder (Grant et al., 2004). Smoking rates have been found to be ashigh as 90% among individuals with schizophrenia (Glassman, 1999). Individuals withschizophrenia are also more likely to be heavy smokers (i.e., smoking more than 25cigarettes per day) (Kelly & McCreadie, 1999). Among individuals in treatment foralcohol and other drug (AOD) problems, the smoking rate ranges from 75% to 100%compared to 23% in the general population (Campbell et al., 1998). When consideringrates by Level of Care, 71-93% of persons in outpatient treatment are smokers (Istvan &Matarazzo, 1984), 85-90% of persons in inpatient care are smokers (Burling & Ziff,1988) and 92% of persons receiving Methadone are smokers (Clemmey et al., 1997).Substance abusers who smoke are often very heavy smokers, smoking 40 or morecigarettes per day (Seidner et al., 1996).
Consequences of smoking
The health risks and consequences of smoking are well-known for people within thegeneral population. These same risks and consequences are experienced by people withsevere mental illness and AOD problems. However, these individuals have higher ratesof chronic health problems and premature death than the general population due tomedical consequences of long-term tobacco use, including cardiovascular disease,coronary heart disease, and respiratory disease (Joukamaa et al., 2001’ Stuyt, Order-Connors, Ziedonis, 2004). For example, the death rate due heart and cerebrovasculardiseases is 1.4 to 5.2 times greater among individuals within Ohio’s inpatient psychiatricfacilities compared to the general population (Svendsen, 2004). Among the recordeddeaths of people with alcohol use disorders, during a 20-year period after receivinginpatient treatment, 51% were tobacco-related, while 34% were alcohol related; theobserved mortality rate was 48% versus an expected 18.5% for the group (Hurt et al.,1996). Among individuals treated for narcotic addictions, the death rate of smokers was4 times that of nonsmokers (Hser et al., 1994). In other words, “most patients in mentalhealth and addition treatment systems smoke tobacco and will die of tobacco-causedillnesses” (Ziedonis & Williams, 2004).

2
Smoking also involves additional health risks and consequences for the population ofindividuals with alcohol use, drug abuse and psychiatric disorders. For example,substances found in tar in cigarettes stimulate enzymes in the liver, which increases themetabolism of many psychiatric medications. As a result, higher doses of thesepsychiatric medications are required to be effective. With higher medication doses, thereis a heightened risk of side effects, such as movement disorders (Williams & Hughes,2004). Moreover, continued smoking generally is associated with a higher relapse riskfor alcohol abuse according to a Canadian study of over 11,000 people over a five-yearperiod (Sobell & Sobell, 1996). Cigarette smokers resumed use of their primary drugs ofchoice more frequently and sooner than did nonsmokers (Sees & Clark, 1993).
Smoking also presents serious health risks and consequences for adolescents within thispopulation, including higher risks of tobacco-related mobidity and mortality. Moreover,cigarette smoking has been implicated as a risk factor for schizophrenia in adolescentmales (Weiser, Riechenberg et al., 2004).
Factors contributing to high rates of nicotine use and dependence among individuals withmental illness, alcohol and drug abuse disorders
Motivation to quit is a strong predictor of attempting to quit and successfully quitting(Krejci & Foulds, 2004). However, the level of motivation to quit smoking amongindividuals with mental illness and substance abuse disorders tends to be lower than inthe general population. About 50% of smokers eventually quit, whereas fewer than 15%of smokers with a psychiatric diagnosis quit (Hughes, 1993). In addition, those whoattempt to quit are less likely to maintain cessation of tobacco use. Among individualswith a history of depression, tobacco cessation is associated with a 20% to 30% chance ofrelapse of depression symptoms (APA, 1996).
In addition, there are positive effects that reinforce smoking for people with mentalillness. Those include the following:
Nicotine may elevate mood, increase alertness and promote relaxation. Amongindividuals with schizophrenia, nicotine has been associated with a reduction innegative symptoms (e.g., lack of energy, flat mood) and an increase of socialinteraction – social quit breaks, alleviates boredom, mood elevation
Boredom can be a trigger for smoking among individuals with schizophrenia(Steinber, Hall, Rustin, 2004)
Smoking breaks have also been used as a means of social interaction. One barriernoted among people with schizophrenia is that by not attending smoking breaks, theyare excluded from opportunities for social interaction. (Steinber, Hall, Rustin, 2004).
Another contributing factor is the lack of systematic assessment and training aboutsmoking cessation among behavioral healthcare providers. Physicians and psychiatristsand other treatment providers do not routinely assess smoking behavior and recommend

3
efforts to quit smoking (Fawcett, 2004). Several reasons have been identified to explainwhy mental health & AOD healthcare providers do not intervene (Hughes, 1997). Theseinclude the following: 1) the belief that they do not have adequate training; 2) the beliefthat people receiving mental health & AOD services cannot or do not want to quitsmoking; 3) the belief that providers will not be reimbursed for treating nicotine use anddependence; 4) the belief that it may be too stressful for people to quit smoking whileaddressing their alcohol and other drug abuse issues simultaneously.
Environmental issues are another important factor contributing to the higher rates ofnicotine use and dependence in this population. For example, policies in manybehavioral healthcare treatment settings do not encourage smokers to quit. Smokingbehavior may also be reinforced and modeled by other patients and providers. However,the stop rate of smoking can be improved if the nicotine use and dependence treatment isprovided in a supportive smoke-free milieu by staff comfortable with interventions (Hurtet al., 1994).
Treatment of nicotine use and dependence
There is limited research available on models for treating nicotine use and dependence inindividuals with mental illness and/or substance use disorders. Recommendations basedon available research and expert consensus suggest that individuals with mental illnessand substance use disorders require more intensive therapy including cognitive behavioraltherapy, relapse prevention and social skills training (APA, 1996; Ziedonis, Williams,2004, Krejci & Foulds, 2004; Stuyt et al., 2004; Williams & Hughes, 2004; Steinberg,Hall, Rustin, 2004).
Many behavioral healthcare professionals already have most of the skills needed to treatpeople with nicotine use and dependence. As little as two hours of training for staff ontobacco cessation approaches has been shown to double quit rates among peoplereceiving behavioral healthcare services (Hughes, 1997).
Standard first-line treatment for nicotine use and dependence in this population includespharmacotherapy (e.g., Buproprion SR and Nicotine Replacement Therapy) andpsychosocial interventions (e.g., assessment, motivational techniques, staged approaches,cognitive behavioral therapy). Experts recommend that the timing of intervention bebased on individual readiness to quit and clinical status. Greater emphasis on the use ofmotivational techniques will help individuals move into successive stages of readiness toquit. People are more motivated to make a change when their treatment is individualizedand their stage of change is taken into consideration (Ohio Women’s Coalition SmokingCessation & Prevention Initiative). The goal of treatment is not neccessarily cessation,but increased motivation to quit, which is a strong predictor of attempting to quit andsuccessfully quitting (Krejci & Foulds, 2004).

4
A longer period between initial evaluation and setting a quit date is also recommended toengage individuals in treatment for nicotine use and dependence and to increase thelikelihood that they will return for additional quit attempts if they relapse. Carefulmonitoring is recommended due to the possibility of relapse and medication toxicity.
Problem Statement
There is a need to expand upon the limited knowledge and treatment alternatives thatcurrently exist regarding tobacco cessation and use prevention approaches for adults andadolescents with AOD disorders and severe mental illness. Such information can be used1) to guide behavioral healthcare providers in implementing treatment for nicotine useand dependence, 2) to better inform the Ohio Departments of Mental Health (ODMH)and Alcohol and Drug Addiction Services (ODADAS), as well as the Tobacco UsePrevention and Control Foundation, about allocation of resources for treatment andprevention of tobacco use, and 3) to promote integration of tobacco use and preventionapproaches in behavioral healthcare agencies throughout the state of Ohio.
The goals of the proposed project are to:
1. Identify and evaluate existing tobacco use prevention and treatmentmodels to increase motivation and quit-rates among individuals withsevere, persistent mental illness and substance abuse
2. Identify and evaluate strategies to successfully integrate assessment andtreatment of nicotine use and dependence into behavioral healthcareagencies in Ohio.
a. Select and implement effective training programs and resources,including consultation, oversight, and guidance to behavioral healthcareagencies.
b. Determine barriers and facilitators to implementation and integrationof tobacco use prevention and treatment into the daily operations ofbehavioral healthcare agencies in Ohio.
3. Address system issues related to implementation, such as reimbursementoptions for treatment of nicotine use and dependence within the mentalhealth & AOD systems.
Proposed Activities
Target population and pilot sites
Target population will include individuals in three diagnostic categories: serious mentaldisorders, AOD disorders, and co-occurring substance abuse and mental health disorders.

5
Because of the critical need to prevent tobacco use early in people’s lives, the project willinclude both adults and adolescents.
Because service providers’ attitudes and knowledge are critical to the successfulimplementation of smoking cessation treatment, the project will also include monitoringof service providers knowledge, attitudes and tobacco use.
Six pilot sites will be selected using a request for proposals (RFP) process. The sites willinclude AOD treatment organizations, mental health organizations, and organizations thattreat co-occurring mental health and substance use disorders.
Organization and Management Plan (see Table of Organization in Appendix A)
ODMH and ODADAS will provide overall fiscal and administrative leadership,direction, oversight of the training and evaluation of the project, and communicationswith the Ohio Tobacco Use Prevention and Control Foundation. A Leadership Team(LT) composed of senior staff of these two state departments will provide these functions.These same individuals have been involved in developing the grant proposal, so there willbe complete continuity of management from the project’s development to operationsphases.
A State Advisory Committee will be convened and will include representatives fromconsumer organizations, national tobacco use prevention & treatment experts,representatives from local ADAS, CMH and/or ADMH boards, members of the ODMH& ODADAS leadership team, representatives from community-based tobacco useprevention & treatment programs (e.g., Quitline, Ohio Chapter of the American LungAssociation), representatives from state agencies who are invested in state-wide healthpromotion programs (e.g, ODH, ODJFS), and representatives of Ohio colleges anduniversities.
The purpose of the advisory committee is to provide overall guidance and advice to theDepartments of Mental Health and Alcohol and Drug Addiction Services. For example,the Advisory Committee could make recommendations about the development of theRFP and review criteria, the selection of treatment models and adaptations for the targetpopulation, and strategies to address barriers to implementation.
Training and consultation to agencies and staff
Ohio-based experts will be selected to serve as the State-wide Coordinator(s) of thepilot project. The Coordinators will be the point of contact for agencies implementingtobacco use prevention and treatment services. A primary function will be to providetraining and consultation. In addition, the State-wide Coordinator(s) will be responsiblefor day-to-day management of the project.

6
Evaluation plan
ODMH & ODADAS will seek and select an Ohio-Based Researcher with expertise inanalyzing outcomes of community-based tobacco use prevention and treatment programs.The evaluator will be expected to design and carry out the evaluation component of theproject.
The focus of the evaluation will include the following:
1. Staff attitudes, staff knowledge, smoking behavior, readiness to quit
2. Extent to which assessment of tobacco use prevention and treatment areintegrated within the pilot sites
3. Identification of agency and system-level barriers and facilitators toimplementation of tobacco use prevention and treatment.
4. Effectiveness of existing tobacco use prevention and treatment programs (or theiradaptations) in increasing consumers’ motivation to quit and reducing tobaccouse.
The evaluation methodology will involve, but not be limited, to the following:
1. Assessment of staff and consumers participating in tobacco use prevention andtreatment;
2. Assessment of changes in tobacco use rates among adults and adolescents in pilotsites;
3. Assessment of adaptations to tobacco use prevention and treatment strategies forthe target populations of consumers.
Time-Frame for the project (See Appendix B)
Year one:
- Convene State Level Advisory Committee
- Disseminate RFP materials, review proposals and select six pilot sites.
- Identify and develop contracts with State-wide coordinator(s).
- Select project evaluator and develop contract.
- Identify models and consider adaptations to existing programs, including theQuitline and the American Lung Association programs.

7
- Begin implementation at pilot sites, which will include the following:establishment of Local Steering Committees (LSC’s); creation of realisticchange plans and timelines; staff training; provision of treatment for interestednicotine-dependent staff in pilot agencies; procedural changes includingroutine, standard assessment of tobacco use, provision of tobacco useprevention and treatment educational materials, and policy modifications.
- Begin to collect evaluation data.
Year two:
- Continue to implement tobacco use prevention and treatment programs.Expand tobacco use prevention and treatment within the agency (i.e., trainadditional staff, offer program to additional consumers).
- Continue to collect evaluation data.
- Conduct analyses.
- Prepare final report.
- Disseminate findings within the AOD and Mental Health systems.
- Disseminate to other stakeholders in cooperation with the TUPCF.
- Begin planning for statewide implementation.
Budget
Explanation
ODMH and ODADAS Administration: Funding is requested to cover personnel costsrelated to the fiscal and administrative leadership that will be devoted to the project by theLeadership Team at ODMH and ODADAS. The leadership team will be composed ofsenior staff of these two state departments and will be involved in all phases of theproject’s development and operations.
The Statewide Coordinator(s) will be responsible for providing expert training andconsultation to organizations adopting tobacco use prevention and treatment services.This will require 1.0 FTE or two .5 FTEs plus additional travel and office expenses.
The project Evaluator will be an Ohio-Based researcher with expertise in analyzingoutcomes of community-based tobacco use prevention and treatment programs. Thisperson will be responsible for designing and carrying out the evaluation component of theproject, including working with all six pilot sites, collecting quantitative and qualitativedata, possibly including surveys and focus groups of consumers and staff.
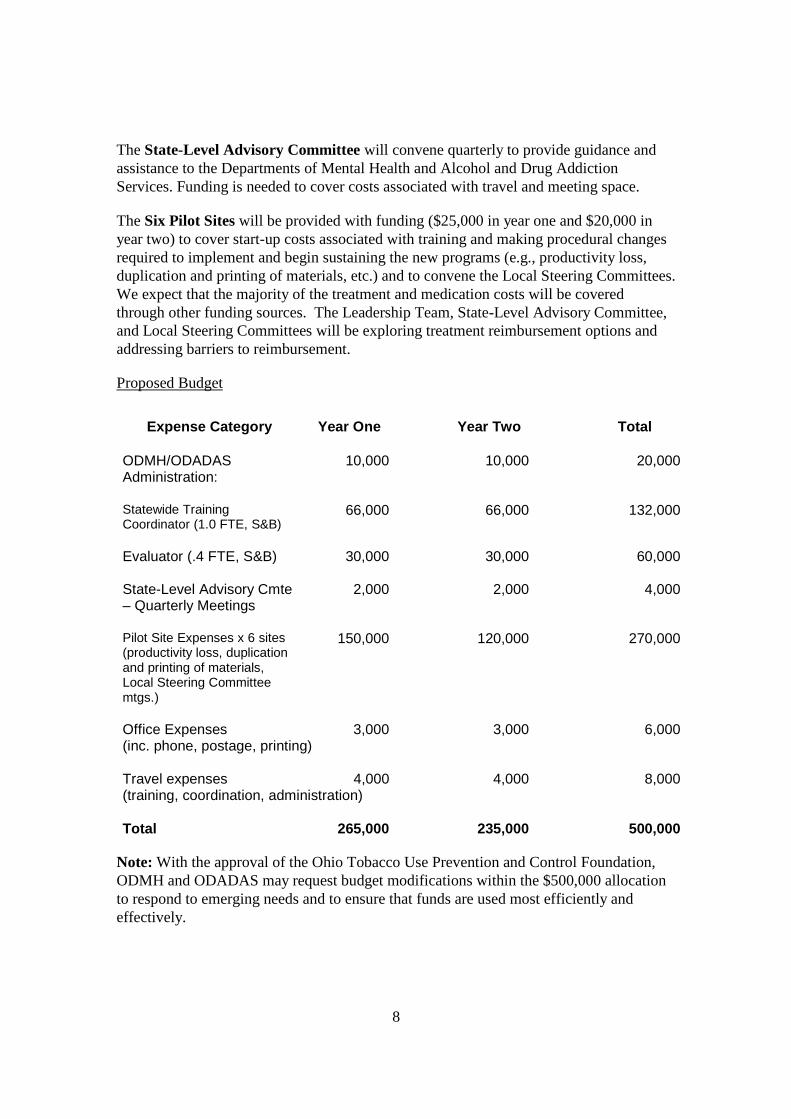
8
The State-Level Advisory Committee will convene quarterly to provide guidance andassistance to the Departments of Mental Health and Alcohol and Drug AddictionServices. Funding is needed to cover costs associated with travel and meeting space.
The Six Pilot Sites will be provided with funding ($25,000 in year one and $20,000 inyear two) to cover start-up costs associated with training and making procedural changesrequired to implement and begin sustaining the new programs (e.g., productivity loss,duplication and printing of materials, etc.) and to convene the Local Steering Committees.We expect that the majority of the treatment and medication costs will be coveredthrough other funding sources. The Leadership Team, State-Level Advisory Committee,and Local Steering Committees will be exploring treatment reimbursement options andaddressing barriers to reimbursement.
Proposed Budget
Expense Category Year One Year Two Total
ODMH/ODADAS 10,000 10,000 20,000Administration:
Statewide TrainingCoordinator (1.0 FTE, S&B)
66,000 66,000 132,000
Evaluator (.4 FTE, S&B) 30,000 30,000 60,000
State-Level Advisory Cmte– Quarterly Meetings
2,000 2,000 4,000
Pilot Site Expenses x 6 sites(productivity loss, duplicationand printing of materials,Local Steering Committeemtgs.)
150,000 120,000 270,000
Office Expenses 3,000 3,000 6,000(inc. phone, postage, printing)
Travel expenses 4,000 4,000 8,000(training, coordination, administration)
Total 265,000 235,000 500,000
Note: With the approval of the Ohio Tobacco Use Prevention and Control Foundation,ODMH and ODADAS may request budget modifications within the $500,000 allocationto respond to emerging needs and to ensure that funds are used most efficiently andeffectively.

9
Appendix AOrganization and Management Plan
The overall management approach for implementing the Tobacco Cessation and UsePrevention Grant has five (5) key components:
(1) ODMH and ODADAS will provide overall fiscal and administrative leadership,direction, oversight of the training and evaluation components of the project, andcommunications with the Ohio Tobacco Use Prevention and Control Foundation. ALeadership Team (LT) composed of senior staff of these two state departments willprovide these functions. These same individuals have been involved in developing thegrant proposal, so there will be complete continuity of management from the project’sdevelopment to operations phases.
(2) A State Level Advisory Committee (SAC) will provide overall guidance and adviceto the Ohio Departments of Mental Health (ODMH) and Alcohol and Drug AddictionServices (ODADAS), who will co-manage the project at the state level. Please refer topage five (5) for the proposed membership of the SAC.
(3) A Statewide Coordinator will relate directly with Mental Health, Alcohol and Drug,and Combined MH/AOD agencies, who serve as the point-of-contact for smokingcessation and prevention services. Training will be provided by Ohio-based individualswho will collaborate with New Jersey-based trainers to ensure that resources are availableroutinely to provide “real-time” training, technical assistance, and reinforcement. Linkagewith the Quitline and the American Lung Association will be emphasized at this level.
(4) Evaluation will be provided by an Ohio-based researcher with expertise in analyzingthe outcomes of community-based programs of this nature.
(5) Local Steering Committees (LSCs) will be responsible for providing consensusbuilding, resource support, linkage to local smoking cessation and prevention affiliates,and other advisory and support functions. Agencies requesting to become Pilot Sites will,as a condition of their approved RFP application, commit to the development of LSCs.
(6) Pilot Sites (PS), consisting of community-based Mental Health, Alcohol and Drug,and combined agencies will be the focus of the training activity with both agencypersonnel and clients receiving cessation and prevention services. It is envisioned that six(6) pilot sites will be selected as a result of a competitive Request for Proposals (RFP)process for Pilot Sites selection managed by the ODMH and ODADAS Leadership Team.
The attached table provides a reference to the Organization and Management Plan.

10
Table of Organization: Ohio Tobacco Cessation and Use Prevention Grant
Ohio Tobacco Use PreventionAnd Control Foundation
Ohio Department of Mental Health, OhioDepartment of Alcohol and Drug Addiction
ServicesLeadership Team (LT)
State-LevelAdvisory Committee
(SAC)
Statewide Coordinator
(Trainer/Consultant)
Local SteeringCommittee (LSC)
Pilot Site(PS)
Local SteeringCommittee (LSC)
Pilot Site(PS)
Local SteeringCommittee (LSC)
Pilot Site(PS)
Local SteeringCommittee (LSC)
Pilot Site(PS)
Local SteeringCommittee (LSC)
Pilot Site(PS)
Local SteeringCommittee (LSC)
Pilot Site(PS)
Note: Solid lines showdirect flow ofcommunications; dottedlines show secondary
communications
ProjectEvaluator

11
Appendix BTime-Frame for Project
Year OneMarch
05April
05May05
June05
July05
August05
Sept.05
Oct.05
Nov.05
Dec.05
Jan.06
Feb.06
Convene State LevelAdvisory Committee
Disseminate RFPmaterials, review proposalsand select six pilot sitesIdentify and developcontracts with State-widecoordinator(s).Select project evaluatorand develop contract.
Identify adaptations to theQuit-line and AmericanLung AssociationprogramsBegin implementation atpilot sites
Begin to collect evaluationdata

12
Year TwoMarch
06April
06May06
June06
July06
August06
Sept.06
Oct.06
Nov.06
Dec.06
Jan.07
Feb.07
Continue implementation
Continue to collectevaluation data
Conduct analyses
Prepare final report.
Disseminate findingswithin the AOD andMental Health systemsDisseminate to otherstakeholders in cooperationwith the TUPCFBegin planning forstatewide implementation.














![PM PM 2015-06-29 [mm] WaStop DN150 std WS146-55-304](https://img.pdfslide.us/doc/110x75/6190275f232b3b12501dcd5e/pm-pm-2015-06-29-mm-wastop-dn150-std-ws146-55-304.jpg)
![PM PM 2010-11-24 [mm] WaStop DN400 WS390-55-304](https://img.pdfslide.us/doc/110x75/6190275e232b3b12501dcd5d/pm-pm-2010-11-24-mm-wastop-dn400-ws390-55-304.jpg)













