Embed Size (px)
Citation preview

Emergency Medical ServicesStroke Training Curriculum
2. Anatomy & PhysiologyAetiology and PathogenesisSymptoms & DiagnosisRisk Factors

Introduction
1. Kollmar R, Schwab S. Ischaemic stroke: acute management, intensive care, and future perspectives. British Journal of Anaesthesia 2009;99(1):95–101.
Stroke is an acute heterogeneous syndrome caused by several disorders leading to anocclusion or rupture of blood vessels supplying brain tissue. After deprivation ofoxygen supply, some neurons die within minutes, resulting in irreversible brain injury.Around the area of necrosis, there is an area in which the blood supply is marginallysufficient to keep these cells alive, but currently dysfunctional. This is called theischaemic penumbra.1
If reperfusion is not performed in a timely manner, or if additional injury is added, atime-related death of the neurons located in the penumbra occurs. Therefore, ‘time isbrain’ summarises the fact that brain function is lost for every second treatment isdelayed.1

Stroke facts1
IF BLOOD FLOW IS NOT RESTORED, BRAIN TISSUE WILL
DIE CAUSING PERMANENT DISABILITY
INSUFFICIENT SUPPLY OF BLOOD TO AN AREA OF THE BRAIN
CAUSES A LACK OF OXYGEN AND NUTRIENTS
STROKE OCCURS WHEN THE BLOOD SUPPLY TO AN AREA OF
THE BRAIN IS BLOCKED OR REDUCED
STROKE IS A MEDICAL EMERGENCY
1. Kollmar R, Schwab S. Ischaemic stroke: acute management, intensive care, and future perspectives. British Journal of Anaesthesia 2009;99(1):95–101.

Anatomy & Physiology The brain receives information through our five senses: touch, smell, taste, sight and hearing. It can storeinformation in our memory and can assemble it in a way that has meaning for us. It controls our thoughts, speech,memory, body movement and also major organ functions. The primary functions of the nervous system are tomonitor, integrate and respond to information inside and outside the body.2
ANATOMICAL AND FUNCTIONAL STRUCTURE OF THE CNS
In general, the human nervous system consists of the central nervous system (CNS) and the peripheral nervoussystem (PNS). The CNS is composed of the brain and spinal cord.2 The PNS is composed of 12 pairs of cranialnerves and 31 pairs of spinal nerves originating from the brain or the spinal cord. It is supported and protected bythe surrounding skin, skull, meninges and cerebrospinal fluid. 2,3
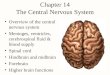
Figure 1. Meninges of the central nervous parts4
2. Mayfield Brain & Spine: Anatomy of the brain [Internet]. © Mayfield Clinic; 1998-2018;1-7 [cited 2019 April 12]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-anatomybrain.pdf 3. Woolsey TA, Hanaway J, Gado MH. TheBrain Atlas: A Visual Guide to the Human Central Nervous System. 4th edition. Hoboken (NJ): John Wiley & Sons; 2017. . 4. File: Meninges-en-svg. In Wikimedia Commons; [cited 2019 April 12]. Available from:https://commons.wikimedia.org/wiki/File:Meninges-en.svg

Anatomy & Physiology
The brain comprises of three main parts (Figure 2)2:
❖ Cerebrum
❖ Cerebellum
❖ Brainstem
Figure 2. Internal anatomy of the brain.2
The surface of the cerebrum is called the cortex and contains nerve cells which are grey giving the cortex its colourand name (grey matter). Beneath the cortex are long connective fibres between neurons and axons (whitematter).2
2. Mayfield Brain & Spine: Anatomy of the brain [Internet]. © Mayfield Clinic; 1998-2018;1-7 [cited 2019 April 12]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-anatomybrain.pdf

Anatomy & Physiology
The cerebrum consists of the right and left hemisphere and is the largest part of the brain. 2
It is sub-divided into the frontal lobe, parietal lobe, temporal lobe and occipital lobe (Figure 3).2
Figure 3. External anatomy of the brain.2
2. Mayfield Brain & Spine: Anatomy of the brain [Internet]. © Mayfield Clinic; 1998-2018;1-7 [cited 2019 April 12]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-anatomybrain.pdf

Anatomy & Physiology2
2FRONTAL LOBE• Personality, behaviour and emotions• Judgment, problem solving and planning • Speech - speaking and writing (Broca’s
area)• Body movement, intelligence,
concentration and self awareness
PARIETAL LOBE
• Interpreting language and words• Sense of touch, pain and temperature• Interpreting signals from vision, hearing,
motor, sensory and memory • Spatial and visual perception
TEMPORAL LOBE
• Understanding language (Wernicke’s area)• Memory• Hearing • Sequencing and organisation
OCCIPITAL LOBE
• Interpreting vision: colour, light, movement
The cerebellum (Figures 2 & 3) is located under the temporal and occipital lobes of the cerebrum. Its function is tocoordinate muscle movements, maintain posture and balance. It also has an important role in motor learning.2
The midbrain, pons and medulla form the brainstem (Figure 2), which acts as a relay centre connecting the cerebrum andthe cerebellum to the spinal cord. Many important functions such as breathing, heart rate, sleeping, swallowing orcoughing are regulated here.2
The brain is protected by the skull on the outside.2
cerebellum
brainstem
2. Mayfield Brain & Spine: Anatomy of the brain [Internet]. © Mayfield Clinic; 1998-2018; 1-7 [cited 2019 April 12]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-anatomybrain.pdf

Anatomy & PhysiologyFUNCTIONAL AREAS OF THE BRAIN.5
Figure 4. Functional areas of the brain.5
5. Functional areas of the brain. [Cited 2019 April 12]. Available from https://www.google.com/search?q=functional+areas+of+the+brain&source=lnms&tbm=isch&sa=X&ved=0ahUKEwirqf14NLhAhUVtHEKHQrHCUgQ_AUIDigB&biw=1366&bih=606#imgrc=XjS2YbQfiiXXbM:

Anatomy & Physiology
Figure 5. Meninges of the central nervous parts4
Then there are three layers of tissue which are called meninges (Figure 5). The meninges cover and protectthe brain and the spinal cord. The inner layer is the pia mater, the middle layer is the arachnoid mater, andthe outermost layer is the dura mater.
The dura mater is a thick and strong membrane which closely aligns to the inside of the skull. It creates smallcompartments, the falx and the tentorium. The falx separates the right and the left hemisphere and thetentorium separates the cerebrum from the cerebellum.
PROTECTION OF THE CNS2
2. Mayfield Brain & Spine: Anatomy of the brain. © Mayfield Clinic; 1998-2018; 1-7 [cited 2019 April 12]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-anatomybrain.pdf 4. File: Meninges-en-svg. In Wikimedia Commons; [cited 2019 April 12]. Available from: https://commons.wikimedia.org/wiki/File:Meninges-en.svg

Anatomy & Physiology
Figure 6. CSF is produced inside the ventricles deep within the brain. CSF fluid circulates inside the brain and spinal cord and then outside the subarachnoid space. Common sites of obstruction: 1) foramen of Monro, 2) aqueduct of Sylvius, and 3) obex.2
CEREBROSPINAL FLUID2
Cerebrospinal fluid (CSF) flows around and within the
brain and spinal cord to cushion it from injuries. It is
produced inside fluid-filled cavities called ventricles.
These contain within them a structure called choroid
plexus that makes the colourless CSF. Two lateral
ventricles, deep in the cerebral hemisphere, are
connected to a third ventricle through the foramen of
Monro. The third ventricle is connected to a fourth
ventricle through the aqueduct of Sylvius. From there,
CSF flows into the subarachnoid space to cushion the
brain.
CEREBROSPINAL FLUID2
2. Mayfield Brain & Spine: Anatomy of the brain [Internet]. © Mayfield Clinic; 1998-2018;1-7 [cited 2019 April 12]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-anatomybrain.pdf

Anatomy & Physiology THE ANATOMY OF THE CEREBRAL CIRCULATORY SYSTEM2
To function, the brain is dependant upon an adequate supply of both oxygen and nutrients, which are provided by a network of blood vessels. Blood is carried to the brain by two paired arteries, the carotid arteries and the vertebral arteries (Figure 7).
• Internal carotid arteries supply most of cerebrum.
• Vertebral arteries supply the cerebellum, brainstem, and the underside of the cerebrum.
• After passing through the skull, the right and left vertebral arteries join together to form the basilar artery.
• The basilar artery and the internal carotid arteries “communicate” with each other at the base of the brain called the circle of Willis (Figure7).
• The communication between the internal carotid and the vertebral-basilar systems is important because if a major vessel is blocked, it is then still possible for the collateral blood flow to come across the circle of Willis and prevent brain damage.
• The venous circulation of the brain is very different than the rest of the body. Usually arteries and veins run together as they supply and drain specific areas of the body.
• The major vein collectors are integrated into the dura to form venous sinuses which collect the blood from the brain and pass it to the internal jugular veins.
• The superior and inferior sagittal sinuses drain the cerebrum, the cavernous sinuses drains the anterior skull base.
• All sinuses eventually drain to the sigmoid sinuses,which exit the skull as the jugular veins.
Figure 7. Top view of the circle of Willis. Theinternal carotid and vertebral-basilar systems arejoined by the anterior communicating (Acom) andposterior communicating (Pcom) arteries.2
THE ANATOMY OF THE CEREBRAL CIRCULATORY SYSTEM2
2. Mayfield Brain & Spine: Anatomy of the brain [Internet]. © Mayfield Clinic; 1998-2018;1-7 [cited 2019 April 12]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-anatomybrain.pdf

Anatomy & Physiology
Cerebral autoregulation is the mechanism by which cerebral blood flow (CBF) remains relatively constant despite
changes in cerebral perfusion pressure (CPP).6
Changes in CPP or mean arterial blood pressure (MAP) that would increase or reduce CBF can be compensated for by
adjusting cerebrovascular resistance. CBF is regulated better than in most other organs; even with mean arterial
pressure variations of between 60 and 150 mm Hg in the normotensive human. CBF is relatively but not absolutely
constant with changes by only a few percentage points. This is different with acute neurological patients where CPP
is highly important.6
AUTOREGULATION
6. Markus HS. Cerebral perfusion and stroke. Journal of Neurology, Neurosurgery & Psychiatry 2004;75(3):353–361.

What is a stroke?
A STROKE IS A MEDICAL EMERGENCY! 7,8
A STROKE OCCURS WHEN THE BLOOD FLOW TO A PART OF THE BRAIN IS INTERRUPTED8,9
LACK OF BLOOD SUPPLY MEANS THAT NOT ENOUGH OXYGEN OR NUTRIENTS REACH THE BRAIN AND THE BRAIN CELLS BECOME
DAMAGED OR PERMANENTLY DESTROYED9
DEPENDING ON WHICH PART OF THE BRAIN IS AFFECTED, DIFFERENT SYMPTOMS CAN OCCUR8,9
IF NOT TREATED IN TIME, A STROKE CAN HAVE EMOTIONAL, PHYSICAL OR EVEN FATAL CONSEQUENCES8,9 Watch video from webpage , below the
slide section
7. Saver JL. Time is brain- Quantified. Stroke 2006; 37: 263-266. 8. Mayfield Brain & Spine: Stroke. © Mayfield Clinic; 1998-2018;1-6 [cited 2019 April 21]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-stroke.pdf 9. What is stroke. National Stroke association® [cited 2019 April 12]. Available from: https://www.stroke.org/understand-stroke/what-is-stroke/

What happens when a stroke occurs? 10
Blood flow stopped
Brain tissue paralysedInstant onset of early symptoms
Brain tissue dies
0 min
Minutes
12 hoursEmbolic stroke
10. Ichai C, Quintard H, Orban JC. Metabolic disorders and critically ill patients. From pathophysiology to treatment. France (Paris): Springer-Verlag; 2012.

What happens when a stroke occurs? 10
Blood flow stopped
Brain tissue paralysed
Brain tissue dies
0 min
Minutes
12 hours
The sooner blood flow is restored -
the more brain death is prevented
10. Ichai C, Quintard H, Orban JC. Metabolic disorders and critically ill patients. From pathophysiology to treatment. France (Paris): Springer-Verlag; 2012.

Clot formation – a quick review11,12
11. Smith SA, Trevers RJ, Morrissey JH. How it all starts: initiation of the clotting cascade. Critical reviews in biochemistry and molecular biology 2015;50(4):326-336. 12. Coagulation. Wikipedia, the free encyclopedia. 2019 [cited 2019 April 21]. Available from: https://en.wikipedia.org/wiki/Coagulation

Aetiology and Pathogenesis of Cerebral Infarct
The World Health Organisation defines a stroke as neurological impairment “caused by the interruption of the bloodsupply to the brain, usually because a blood vessel bursts or is blocked by a clot. This cuts off the supply of oxygen andnutrients, causing damage to the brain tissue. The most common symptom of a stroke is sudden weakness or numbnessof the face, arm or leg, most often on one side of the body. Other symptoms include: confusion, difficulty speaking orunderstanding speech; difficulty seeing with one or both eyes; difficulty walking, dizziness, loss of balance orcoordination; severe headache with no known cause; fainting or unconsciousness”.13
The effects of a stroke depend on which part of the brain is damaged and how severely it is affected. A very severestroke can cause sudden death.13
8. Mayfield Brain & Spine: Stroke. © Mayfield Clinic; 1998-2018;1-6 [cited 2019 April 21]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-stroke.pdf 13. Stroke, Cerebrovascular accident. World Health Organisation [cited 2019, April12]. Available from: https://www.who.int/topics/cerebrovascular_accident/en/
There are two different types of stroke:8
1. Ischaemic stroke
2. Haemorrhagic stroke

Aetiology and Pathogenesis of Cerebral Infarct
In addition, there is also transient ischaemic attacks (TIA), defined as “brief episodes of neurological dysfunctionresulting from focal cerebral ischaemia not associated with permanent cerebral infarction”.14
An ischaemic stroke is caused by a thrombotic or embolic occlusion of a cerebral artery. The rupture of a blood vesselwith bleeding into the brain parenchyma or subarachnoid space is known to lead to a haemorrhagic stroke.8 Both typesof strokes deplete the brain of oxygen and nutrients and cause affected brain cells to die.9
When blood flow to the brain is blocked for only a short time, this is known as a transient ischaemic attack (TIA). It isimportant to know that a TIA has the same causes as a cerebral infarction, and when the causes remain untreated,there is high risk of recurrence. 8,9
8. Mayfield Brain & Spine: Stroke. © Mayfield Clinic; 1998-2018; 1-6 [cited 2019 April 21]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-stroke.pdf 9. What is stroke. National Stroke association® [cited 2019 April 12]. Available from:https://www.stroke.org/understand-stroke/what-is-stroke/ 14. Easton DJ, Saver JL, Albers GW et al. Definition and evaluation of transient Ischemic attack a scientific statement for healthcare professionals from the American HeartAssociation/American Stroke Association stroke council; Council on cardiovascular surgery and anesthesia; council on cardiovascular radiology and intervention; council on cardiovascular nursing; and the interdisciplinary council on peripheralvascular disease. Stroke. 2009;40:2276-2293.

Aetiology and Pathogenesis of Cerebral Infarct
TABLE 1: TOAST CLASSIFICATION (Assessment of the aetiology of stroke, adapted from Amarenco, 2009)
1 Cerebrosclerosis
2 Cardioembolic infarct
3 Small artery occlusion (lacune)
4 Stroke of other determined aetiology
5 Stroke of undetermined aetiology
Stroke can be classified at different levels and, indeed, this is essential for patient admission. A stroke can generally besubdivided by clinical syndromes, aetiology, pathogenesis, time response, severity, localisation and morphology (Table2).15 There are other classifications developed from Adams et al., 1993, during the “Trial of Org 10172 in Acute StrokeTreatment (TOAST)”.16 This classification tool is useful to assess the aetiology of stroke.16 TOAST criteria are based onimaging and angiological findings and observe the aetiology and pathogenesis of stroke (Table 1). This is often used inclinical practice; handling is simple and distinguishes five groups.15,16
The topographic diagnosis of a cerebral ischaemia is based on the clinical examination, and even for acute therapy,magnetic resonance imaging (MRI) is essential.16
15. Amarenco P, Bogousslavsky J, Caplan LR et al. Classification of stroke subtypes. Cerebrovascular disease 2009;27:493-501. 16. Adams HP, Bendixen BH et al. Classification of subtype of acute ischemic stroke definitions for use in a multicenter clinical trial. Stroke 1993;24(1):35-41.

Classification of Stroke TABLE 2: CLASSIFICATION OF STROKE
CLINICAL SYNDROMES FOCAL ISCHAEMIC STROKE
AETIOLOGY17 ArtherosclerosisCardiac embolism
PATHOGENESIS17 Embolic ThromboticSmall vessel disease Inherited diseases (dermatitis)
TIME REPONSE17 Reversible result Irreversible result
SEVERITY17 Minor vs. major stroke
LOCALISATION16 Cortical Subcortical
MORPHOLOGY17 Without lesion → reversible ischaemicdisorder with lesion → cerebral infarct
16. Adams HP, Bendixen BH et al. Classification of subtype of acute ischemic stroke definitions for use in a multicenter clinical trial. Stroke 1993;24(1):35-41. 17. Gund BM, Jagtap PN, Ingale VB et al. Stroke: A brain attack. Journal of Pharmacy2013;3(8):1-23.

How are strokes classified?
A STROKE CAN BE DUE TO A BLOCKAGE IN ONE OF THE ARTERIES (ISCHAEMIC STROKE) OR BLEEDING IN THE BRAIN (HAEMORRHAGIC STROKE)8
THE BLOOD SUPPLY TO AN AREA OF THE BRAIN
IS TEMPORARILY INTERRUPTED BUT IS RESTORED WITHIN 60 MIN AND THE PATIENT
RETURNS TO NORMAL
TRANSIENT ISCHAEMIC ATTACK (TIA)8,14 HAEMORRHAGIC STROKE8,9ISCHAEMIC STROKE8,9
BLEEDING IN THE BRAIN PREVENTS THE NORMAL FLOW OF BLOOD TO THE
TISSUE BEYOND THE DAMAGE AND CAUSES NEUROLOGICAL SYMPTOMS
THE BLOOD SUPPLY TO AN AREA OF THE BRAIN IS COMPLETELY BLOCKED, CAUSING
TISSUE DEATH AND NEUROLOGICAL DAMAGE
ISCHAEMIC STROKE IS THE COMMONEST FORM OF STROKE9
8. Mayfield Brain & Spine: Stroke. © Mayfield Clinic; 1998-2018; 1-6 [cited 2019 April 21]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-stroke.pdf 9. What is stroke. National Stroke association® [cited 2019 April 12].Available from: https://www.stroke.org/understand-stroke/what-is-stroke/14. Easton DJ, Saver JL, Albers GW et al. Definition and evaluation of transient Ischemic attack a scientific statement for healthcare professionals fromthe American Heart Association/American Stroke Association stroke council; Council on cardiovascular surgery and anesthesia; council on cardiovascular radiology and intervention; council on cardiovascular nursing; and theinterdisciplinary council on peripheral vascular disease. Stroke. 2009; 40:2276-2293.

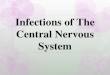
Stroke types and incidence18,45
18. Albers GW, Amarenco P, Easton D et al. Antithrombotic and thrombolytic therapy for ischemic stroke. The seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest 2004; 126: 438S–512S. 45. Mozaffarian D,
Benjamin EJ, Go AS et al. Heart disease and stroke statistics—2016 update. A report from the American Heart Association. Circulation 2015;133:e38-e360 .
Haemorrhagic
13 %
Other
5 %
Cryptogenic
30 %
Cardiac embolism
20 %
Small vesseldisease “lacunes”
25 %
Atheroscleroticcerebrovascular disease
20 %
87

Symptoms, Diagnosis & Differential Diagnosis
As mentioned earlier, in the case of an ischaemic stroke, the blood supply to parts of the brain is decreased, whichleads to dysfunction of the brain tissue in that area. Recognising the pattern of stroke syndromes would be helpful inlocalising the lesion, but can also suggest treatment, identify the underlying cause and provide help withprognostication. The main syndromes are lacunar, embolic and artherosclerotic.19
The lacunar syndrome results in a lack of cortical signs and symptoms distinguishing them from large vessel syndromes.Syndromes are: 19
1. Ataxic Hemiparesis resulting in isolated unilateral weakness and ataxia. The lesion is along the corticospinal andcerebellar pathways.
2. Pure motor stroke/hemiparesis resulting in isolated unilateral weakness of the face, arm, or leg, the lesion is mostlyin posterior limb of the internal capsule or the basic pontis.
3. Pure sensory stroke resulting in isolated unilateral numbness, pain or paraesthesia. The lesion is mostly in thecontralateral thalamus.
4. Mixed sensorimotor stroke resulting in hemiparesis or sensory impairment. The lesion is typically in the thalamusand adjacent posterior internal capsule.
5. Clumsy hand-dysarthria resulting in unilateral mild weakness/clumsiness of the hand and dysarthia with face andtongue weakness. The lesion is mainly in the basis pontis.
ISCHAEMIC SYNDROMES
19. Torbey MT, Selim MH. The stroke book. 2nd edition. Cambridge University press. 2013.

Symptoms, Diagnosis & Differential Diagnosis
Emboli occur in the circulatory system where they enter the cerebral circulation and lodge in and occlude brain bloodvessels. If an embolus is large, occlusion of an intracranial artery may occur. If it is small, it can become struck in asmaller segment of an artery. Signs are: 19
1. Seizure: simple focal or focal-onset2. Cortical signs: aphasia, neglect, dyspraxia, hemianopia and agraphesthesia3. Discrete focal signs: isolated hand weakness, isolated aphasia.
Atherosclerotic Stenosis (extracranial or intracranial) can render cerebral tissue receptive to ischaemia fromhypoperfusion and oligaemia or embolisation. Transient examples are: 19
1. Amaurosis fugax (transient monocular blindness) from the ophthalmic artery or internal carotid stenosis.2. Limb-shaking transient ischaemic attack (TIA): repeated brief episodes of contralateral arm weakness from cervical
or intracranial carotid stenosis/occlusion.
19. Torbey MT, Selim MH. The stroke book. 2nd edition. Cambridge University press. 2013.

Symptoms, Diagnosis & Differential Diagnosis
Haemorrhagic strokes result in tissue injury by causing compression of tissue from a growing hematoma or hematomas. This candistort and injure tissue and the pressure can lead to a loss of blood supply to the affected tissue, resulting in an infarction. It appearsthat the blood released by brain haemorrhage has direct toxic effects on brain tissue and vasculature. Intracerebral haemorrhage (ICH)symptoms are often clinically indistinguishable from ischaemic stroke syndromes. Ischaemic and haemorrhagic strokes produce focaldeficits of acute onset. Nevertheless, the blood within the cranial vault can lead to: Headache, nausea and vomiting, decreased level ofconsciousness. 9,19
The symptoms of an ischaemic stroke syndrome can be exposed as a transient ischaemic attack while ICH symptoms persist and arelikely to worsen. Identifying the location of haemorrhage can help predict the underlying cause. The haemorrhage can be intracerebralor subarachnoidal. 9,19
In individual cases there is a need to separate cerebrovascular emergency syndromes that look like stroke syndromes:20
• Todd’s paresis after epilepsy• seizure with focal motor symptoms• aura in migraine• aphasic disturbances in herpes simplex encephalitis• functional disorders• In contrast to blood clot in the basilar artery: altered consciousness of another origin• In contrast to the vertebrobasilar stroke, peripheral vertigo causes
HAEMORRHAGIC SYNDROMES
CEREBROVASCULAR EMERGENCY SYNDROMES
9. What is stroke. National Stroke association® [cited 2019 April 12]. Available from: https://www.stroke.org/understand-stroke/what-is-stroke/19. Torbey MT, Selim MH. The stroke book. 2nd edition. Cambridge University press. 2013. 20. Fernandes PM, Whiteley WN, Hart SR et al. Strokes: mimics and chameleons. Practical Neurology 2013;13:21-28.

Common stroke mimics20,21,22
20. Fernandes PM, Whiteley WN, Hart SR et al. Strokes: mimics and chameleons. Practical Neurology 2013;13:21-28. 21. Summers D, Leonard A, Wentworth D et al. Comprehensive overview of nursing and interdisciplinary care ofthe acute ischemic stroke patient: A scientific statement from the American Heart Association. Stroke 2009;40:2911-2944. 22. Hatzitolios A, Savopoulos C, Ntaios G et al. Stroke and conditions that mimic it: a protocol secures a safeearly recognition. Hippokratia 2008;12(2):98-102.
ALCOHOL INTOXICATION
CEREBRAL INFECTION
METABOLIC DISORDERS
NEUROPATHY(BELL’S PALSY)
BRAINTUMOURS
SEIZURES AND POST-SEIZURE
STATES, TODD’S PARALYSIS
HYPO-GLYCAEMIA
EPIDURAL HAEMATOMA
DRUG OVERDOSE /
TOXICITY
HYPERTENSIVEENCEPHALOPATHY
MIGRAINE

Time is brain tissue7
7. Saver JL. Time is brain- Quantified. Stroke 2006;37:263-266. 23. Gonzalez RG. Imaging-guided acute ischemic stroke therapy:From “time to brain” to “physiology is brain”. American Journal of Neuroradiology 2006;27:728-735. 24.
Kidwell CS, Alger JR, Saver JL. Evolving paradigms in neuroimaging of the ischemic penumbra. Stroke 2004;35(11):2662-5.
AN UNTREATED PATIENT LOSES APPROXIMATELY
1,9 MILLION NEURONS EVERY MINUTE IN THE ISCHAEMIC AREA7
REPERFUSION OFFERS THE POTENTIAL TO REDUCE THE EXTENT OF
ISCHAEMIC INJURY24
PENUMBRA (SALVAGEABLE BRAIN AREA)23
ISCHAEMIC CORE(BRAIN TISSUE
DESTINED TO DIE)23

Regions of Ischaemia25,26
25. Donnan GA, Baron JC, Ma H et al. Penumbral selection of patients for trials of acute stroke therapy. Lancet Neurology 2009;8:261–69. 26. Moustafa RR, Baron JC. Review: Pathophysiology of ischaemic stroke: insights from imaging, and implications for therapy and drug discovery. British Journal of Pharmacology 2008;153:S44–S54

Time is brain!
In a typical ischaemic stroke:
Every minute the brain loses:7
▪ 1,9 million neurons
▪ 14 billion synapses
▪ 12 km myelinated fibers
Every minute counts!
7. Saver JL. Time is brain- Quantified. Stroke 2006;37:263-266.

Symptoms, Diagnosis & Differential Diagnosis It is important to recognise stroke symptoms and react as fast as possible in order to ensure best medicaltreatment in time. Since effective stroke treatment is very time critical, people have to be aware of thecriteria for identifying a stroke. Below is the face arm speech test (FAST), which can be used to remember the
warning signs, act FAST and call for medical help.27,28
TABLE 3: FAST CRITERIA28
(WARNING SIGNS OF STROKE, NATIONAL STROKE ASSOCIATION)
FFace drooping (asymmetry when asked to smile)
AArm weakness(difficulty when raising arms)
SSpeech difficulties(fuzzy articulation of simple sentences)
TTime(time to call emergency)
27. Jauch EC, Saver JL, MD, HP Adams et al. Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44:870-947. 28. Stroke symptoms: FAST. American Stroke Association; 2019 [cited 2019 April 12]. Available from https://www.strokeassociation.org/en/about-stroke/stroke-symptoms

Symptoms, Diagnosis & Differential Diagnosis
STROKE SYMPTOMS
The most common symptom of stroke is a sudden weakness of the face, arm or legs, most often on one side of the body. But, there are other symptoms, including the sudden onset of:8,27,28
• numbness of the face, arms or legs • confusion, difficulty speaking or understanding speech • difficulty seeing with one or both eyes • difficulty walking, dizziness, loss of balance or coordination• severe headache with no known cause • fainting or unconsciousness
STROKE SYMPTOMS
8. Mayfield Brain & Spine: Stroke. © Mayfield Clinic; 1998-2018; 1-6 [cited 2019 April 21]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-stroke.pdf 27. Jauch EC, Saver JL, MD, HP Adams et al. Guidelines for the early managementof patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44:870-947. 28. Stroke symptoms: FAST. American Stroke Association; 2019[cited 2019 April 12]. Available from https://www.strokeassociation.org/en/about-stroke/stroke-symptoms

How do I know if someone is having a stroke?
IMPORTANTNOTE THE TIME AT WHICH THESE SYMPTOMS STARTED AND
CALL THE EMERGENCY SERVICES IMMEDIATELY
BE SUSPICIOUS OF A STROKE IF ANY OF THE FOLLOWING SYMPTOMS OCCUR8,27,28
SEVERE, SUDDEN-ONSET HEADACHE
UNCONCIOUSNESS
CONFUSSION AND/OR
PROBLEMS UNDERSTANDING
WHAT IS BEING SAID
DROOPING OF THE MOUTH ON
ONE SIDE
DIZZINESS
WEAKNESSOR COMPLETE
LOSS OF MOVEMENTAND/OR SENSATION
IN ONE OR MORELIMBS
VISUAL DISTURBANCE OR LOSS OF SIGHT IN
ONE OR BOTH EYES
DIFFICULTY TALKING,
FORMING WORDS OR SLURRING
WORDS
8. Mayfield Brain & Spine: Stroke. © Mayfield Clinic; 1998-2018; 1-6 [cited 2019 April 21]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-stroke.pdf 27. Jauch EC, Saver JL, MD, HP Adams et al. Guidelines for the early managementof patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44:870-947. 28. Stroke symptoms: FAST. American Stroke Association; 2019[cited 2019 April 12]. Available from https://www.strokeassociation.org/en/about-stroke/stroke-symptoms

What to look out for28,29
IS HS
• Sudden numbness of the face, arm, or leg, especially on one side of the body; X X
• Sudden confusion, trouble speaking or understanding speech; X X
• Sudden trouble seeing in one or both eyes; X X
• Sudden trouble walking, dizziness, loss of balance or coordination X X
• Sudden severe headache with no known cause X X
• In addition, neck pain29 X
• In addition, nausea / vomiting29 X
• In addition, loss of consciousness29 X
28. Stroke symptoms: FAST. American Stroke Association; 2019 [cited 2019 April 12]. Available from https://www.strokeassociation.org/en/about-stroke/stroke-symptoms 29. Ahmed J, Blakeley C, Sakar R et al. Acute neck pain, an atypical presentation of subarachnoid haemorrhage. Emergency Medical Journal 2007;24:e23

Signs and Symptoms – FAST Test27,28
Facial drooping: A section of the face, usually only on one
side, that is drooping and hard to move
Arm weakness: The inability to raise one's arm fully
Speech difficulties: An inability or difficulty to
understand or produce speech
Time: Time is of the essence when having a stroke
– Record time of symptoms onset and treat quickly
27. Jauch EC, Saver JL, MD, HP Adams et al. Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American HeartAssociation/American Stroke Association. Stroke 2013;44:870-947. 28. Stroke symptoms: FAST. American Stroke Association; 2019 [cited 2019 April 12]. Available fromhttps://www.strokeassociation.org/en/about-stroke/stroke-symptoms

Reducing Risk of Stroke
The best way to reduce the risk of getting a stroke is to minimise the risk factors.The risk factors of stroke can be classified into:30,31
• Therapeutically non-influenceable risk factors• Therapeutically influenceable risk factors
The risk factors that can be influenced are treatable with drugs, interventional treatments or through lifestylechanges.32
In 2010, a standardised case-control study entitled “INTERSTROKE” offered much information about the risk factors forstroke in different regions of the world. It revealed that five risk factors could explain more than 80 % of the global riskof strokes: hypertension, smoking, diet, abdominal obesity and physical activity. 33
30. Mackay J, Mensah GA. The atlas of heart disease and stroke. World health organization and center for disease control and prevention. 2004. [cited 2019 April 26]. Available from:http://www.who.int/cardiovascular_diseases/resources/atlas/en 31. Romero JR, Morris J, Pikula A. Stroke prevention: mofifying risk factors. Therapeutic advances in cardiovascular diseases 2008;2(4):287-303 32. Hankey G. The globaland regional burden of stroke. Lancet 2013;1:e239-e240. 33. O‘Donnell MJ, Xavier D, Liu L et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet2010;376:112-123.

Non - Modifiable Risk Factors
Age is the most important independent risk factor for stroke. The risk of stroke doubles every decade after age 55.30,34
The incidence rates are higher in men than in women, but more women die from stroke as they tend to live longer.35
A positive family history of stroke means approximately 1,5 times higher risk of suffering a stroke. In addition, there aresingle mutations to consider, especially at a young age. There is an increased risk of stroke if a first-degree bloodrelative has had a stroke before.30,36,37
Low-income and middle-income countries, as well as populations with a low socioeconomic status in high-incomecountries are disproportionally affected by stroke. This does not only apply to stroke risk but also to short-term andlong-term outcome. These effects are based on increased individual risk factors, such as hypertension, hyperlipidaemia,excessive alcohol intake, smoking obesity, and lack of access to good quality hospital and rehabilitation care.32
The risk of getting a stroke is three times higher for African Americans as it is for Caucasian Americans. In Asia, the riskof getting a stroke or a cerebral haemorrhage is higher than in Western Europe and North America.30,38,39
30. Mackay J, Mensah GA. The atlas of heart disease and stroke. World health organization and center for disease control and prevention. 2004. [cited 2019 April 26]. Available from:http://www.who.int/cardiovascular_diseases/resources/atlas/en 32. Hankey G. The global and regional burden of stroke. Lancet 2013;1:e239-e240. 34. Feigin VL, Forounzafar H, Krishnamuthi R et al. Global and regional burden of strokeduring 1990-2010: findings from the global burden of disease study 2010. Lancet 2014;383:245-255. 35. Turtzo LC, McCullough LD. Sex differences in stroke. Cerebrovascular Disease 2008;26:462–474. 36.Markus H. Genes for stroke. Journalof neurology, neurosurgery and psychiatry. 2004;75(1):1229-1231. 37. Lindgren A. Stroke genetics: A review and update. Journal of stroke 2014;16(3):114-123. 38. Howard G, Labarthe DR, Hu J et al. Regional differences in African Americans’high risk for stroke: The remarkable burden of stroke for Southern African Americans. Annals of epidemiology 2007;17(9):689-696. 39 . Sun Z, Zheng L, Detrano R et al. An epidemiological survey of stroke among rural Chinese adults resultsfrom Liaoning province. Research 2013;8:701-706.

Non - Modifiable Risk Factors
** CADASIL, cerebral autosomal dominant arteriopathy with sub-cortical infarcts and leukoencephalopathy
ADVANCEDAGE30,34 GENDER35
INCREASED RISK OF STROKE IN WOMENRISK OF STROKE MORE THAN DOUBLES IN EACH SUCCESSIVE
DECADE AFTER 55 YEARS
PROBABLY RELATED TO PREGNANCY, GESTATIONAL DIABETES, ORAL CONTRACEPTIVE USE, HORMONE-REPLACEMENT THERAPY & SMOKING
THE RISK OF STROKE DOUBLES EVERY DECADE AFTER 55 YEARS OF AGE
ADVANCEDFAMILY HISTORY36 RACE30,38
INCREASED RISK OF STROKE IN AFRICAN-AMERICANSRISK MAY BE HIGHER WITH A POSITIVE FAMILY HISTORY
PROBABLY DUE TO INCREASED RISK OF HYPERTENSION, DIABETES & OBESITY
SOME CAUSES ARE HEREDITARY, E.G. CADASIL**
30. Mackay J, Mensah GA. The atlas of heart disease and stroke. World health organization and center for disease control and prevention. 2004. [cited: 2019 April 26]. Available from:http://www.who.int/cardiovascular_diseases/resources/atlas/en 34. Feigin VL, Forounzafar H, Krishnamuthi R et al. Global and regional burden of stroke during 1990-2010: findings from the global burden of disease study 2010. Lancet2014;383:245-255. 35. Turtzo LC, McCullough LD. Sex differences in stroke. Cerebrovascular Disease 2008;26:462–474. 36.Markus H. Genes for stroke. Journal of Neurology, Neurosurgery and Psychiatry. 2004;75(1):1229-1231. 37. Lindgren A.Stroke genetics: A review and update. Journal of stroke 2014;16(3):114-123. . 38. Howard G, Labarthe DR, Hu J et al. Regional differences in African Americans’ high risk for stroke: The remarkable burden of stroke for Southern AfricanAmericans. Annals of Epidemiology 2007;17(9):689-696.

Modifiable Risk Factors
Diabetes mellitus is one of the major risk factors for stroke.30
The uncertainty interval around the global estimate of adults with diabetes was estimated to range from 7,2 % to11,4 % (339 – 536 million). This means that while the International Diabetes Federation estimates the prevalenceof diabetes to be 415 million (IDF Diabetes Atlas 7th edition, 2015) the true figure could lie between 339 and536 million.40
The incidence rate is rising. It is estimated that by 2040, one adult in ten will have diabetes (642) million.40
30. Mackay J, Mensah GA. The atlas of heart disease and stroke. World health organization and center for disease control and prevention. 2004. [cited 2019 April 26]. Available from:http://www.who.int/cardiovascular_diseases/resources/atlas/en 40. © International Diabetes Federation. IDF diabetes atlas, 7th edition. Brussels, Belgium. [cited 2019 April 26]. Available from:www.diabetesatlas.org/component/attachments/?task=download&id=180

Modifiable Risk Factors Cholesterol is essential for the formation of cell membranes and the synthesis of steroid hormones andvitamin D. It can be found in the bloodstream and in all cells of the body. In particular, low-densitylipoproteins (LDL) and high-density lipoproteins (HDL) play a role in the transport and metabolism ofcholesterol and triglycerides.41
Smoking significantly increases the risk of heart diseaseand stroke. Smokers are two to four times more likely tohave a stroke than non-smokers. The more you smoke, themore the risk increases.30,43
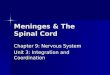
Carotid artery stenosis is the narrowing of the carotid arteries,which are the two main blood vessels in the neck that supplyblood to the brain (Figure 7). Artherosclerotic plaques lead tostenosis of the carotid arteries and can be the reason forsubsequent emboli. Hypertension, smoking, diabetes mellitus,and hyperlipidaemia are major risk factors for thedevelopment of atherosclerotic disease.42
Figure 7: Intracranial stenosis.42
30. Mackay J, Mensah GA. The atlas of heart disease and stroke. World health organization and center for disease control and prevention. 2004. [cited 2019 April 26]. Available from:http://www.who.int/cardiovascular_diseases/resources/atlas/en 41. National Stroke Association. Cholesterol fact sheet. [cited 2019 April 26] Available from:file:///C:/Users/Helen/AppData/Local/Packages/Microsoft.MicrosoftEdge_8wekyb3d8bbwe/TempState/Downloads/Cholesterol_Fact-Sheet.pdf 42. Mayfield Brain & Spine: Intracranial artery stenosis. © Mayfield Clinic; 1998-2018; 1-4 [cited 2019 April 26]. Available from: https://d3djccaurgtij4.cloudfront.net/pe-intracranialstenosis.pdf 43. Shah RS, Cole W. Smoking and stroke: the more you smoke the more you stroke. Expert Review of CardiovascularTherapy 2010;8(7):917–932.

Modifiable Risk Factors The definition and classification of blood pressureaccording to the updated guidelines, show that there is amanifest arterial hypertension when the blood pressureshows > 130/80 mmHg.44
Elevated blood pressure is the most common treatablereason for vascular events. Arterial hypertension is thestrongest risk factor for a stroke; this applies to cerebralhaemorrhage as well as to brain infarcts.33
With increasing blood pressure, the risk of getting astroke rises exponentially. Normalising high bloodpressure is the most effective way to prevent a stroke.30
30. Mackay J, Mensah GA. The atlas of heart disease and stroke. World health organization and center for disease control and prevention. 2004. [cited 2019 April 26]. Available from:http://www.who.int/cardiovascular_diseases/resources/atlas/en 33. O‘Donnell MJ, Xavier D, Liu L et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study.Lancet 2010;376:112-123. 44. Whelton PK, Carey RM, Aronow WS et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressurein adults: Executive summary a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Hypertension 2018;71:1269-1324.

Modifiable Risk Factors Atrial fibrillation is an eminent risk factor for suffering a cerebral infarction even if you exclude the risk factors like age andhypertension, which mostly accompany AF. The relative stroke risk increases about fivefold in the presence of atrial fibrillation. The sizeof this risk is strongly related to the age group of affected individuals.45
The average age of patients with this condition is between 67 (men) and 75 (woman) years and it is expected to rise in the future.46
Validated scores for the prediction of stroke risk such as CHADs2 and CHA2DS2VASc, can be useful tools in the assessment of patients.47
The CHADS2 score can be calculated from the table by adding the relevant points (Table 4).47
TABLE 4: CHADS2 SCORE TO ESTIMATE THE ANNUAL RISK OF STROKE IN PATIENTS WITH AF
CONDITION POINTS
C Congestive heart failure 1 Point
H (Hypertension) Blood pressure consistently above 140/90 mmHg (or treatedhypertension on medication)
1 Point
A (Age) ≥ 75 years 1 Point
D (Diabetes) Diabetes mellitus 1 Point
S (Stroke) Prior Stroke, TIA or Thromboembolism 2 Point
45. Mozaffarian D, Benjamin EJ, Go AS et al. Heart disease and stroke statistics—2016 update. A report from the American Heart Association. Circulation 2015;133:e38-e360 . 46. Roger VL, Go AS, Lloyd-Jones DM et al. Heart Disease andStroke Statistics—2012 Update a report from the American Heart Association. Circulation. 2012;125:e2-e220. 47. Gage BF, Waterman AD, Shannon W et al. Validation of clinical classification schemed for predicting stroke. Results fromthe national registry of atrial fibrillation. The Journal of the American Medical Association 2001;285(22):2864-2870.

Modifiable Risk Factors30,31,33
30. Mackay J, Mensah GA. The atlas of heart disease and stroke. World health organization and center for disease control and prevention. 2004. [cited 2019 April 26]. Available from:http://www.who.int/cardiovascular_diseases/resources/atlas/en 31. Romero JR, Morris J, Pikula A. Stroke prevention: mofifying risk factors. Therapeutic advances in cardiovascular diseases 2008;2(4):287-303 33. O‘Donnell MJ,Xavier D, Liu L et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet 2010;376:112-123.
HIGH BLOOD PRESSURE
(HYPERTENSION)
DIABETESHEART
DISEASELACK OF EXERCISE
ATRIAL FIBRILLATION
ALCOHOLINTAKE
SMOKING OBESITY STRESSHIGH
CHOLESTEROL

Multiple choice Questions – CPD Accreditation
Please see webpage for online questionnaire
Blue button that says:“ACCESS MODULES Q&A”