Embed Size (px)
DESCRIPTION
embryo
Citation preview

REVIEW
Can We Better Understand the Known Variationsin Coronary Arterial Anatomy?Ing-Sh Chiu, MD, PhD, and Robert H. Anderson, BSc, MDDepartment of Surgery, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei,Taiwan; Division of Pediatric Cardiology, Department of Pediatrics, Medical University of South Carolina, Charleston, SouthCarolina; and Institute of Genetic Medicine, Newcastle University, Newcastle upon Tyne, United Kingdom
Coronary arterial anatomy is remarkably diverse. Iden-tification of surgical risk factors, however, requiresdescription in a uniform fashion. Such descriptionmandates that account be given of both aortic sinusalorigin and variability in aortopulmonary relationships.Currently, however, it is rare to find all this informa-tion provided either in clinical reports or publishedreviews. In this review, therefore, we summarize why
both these features are important, emphasizing themarriage of convenience between the aortic root posi-tion within the cardiac base and the arrangement of theepicardial coronary arteries. The inductive approachaccounts for all potential variations.
(Ann Thorac Surg 2012;94:1751– 60)© 2012 by The Society of Thoracic Surgeons
Variations from the normal distribution of the coro-nary arteries are known to be of major clinical
significance. For example, the so-called intramuralcourse of a proximal coronary artery in the otherwisenormal heart is known to be a harbinger of suddencardiac death [1, 2]. Surgeons have long been aware ofthe problems produced by inadvertent intraoperativedamage to the coronary arteries, especially duringreentry. At present, the surgeon ideally should enterthe operating room with a full appreciation of thearrangement to be encountered, including featuressuch as intramural origin [2– 4] or passage of a signif-icant coronary artery across an obstructed ventricularoutflow tract [5]. There is as yet however no consensusas to how the potential variations in coronary arterialanatomy can best be categorized [6]. Classifications aremanifold yet none has achieved uniform acceptance,nor do they provide all the information required toproduce meaningful analysis of potential risk. Thesituation with greatest anatomic variability is transpo-sition. However, some well-accepted classifications forthis lesion, such as that proposed by Yacoub andRadley-Smith [7], do not permit inclusion of all theknown variables. Others [8] are so complicated as todefeat all but the most dedicated users [9 –11]. Thesystem proposed by Quaegebeur and colleagues [12,13], which is well accepted by surgeons, is foundwanting when information is needed concerning epi-cardial course [4, 9]. Attempts to provide new, andperhaps more complicated, classifications [11, 14] havenot been greeted with enthusiasm. An alternativeapproach therefore is to emphasize the factors thatunderscore the potential variations. That is our goal inthis review, in which we argue that such understand-
ing requires knowledge not only of the sinusal origin[13, 15] but also of the marriage of convenience be-tween the aortic valvar sinuses and the epicardialcourse of the coronary arteries [16, 17].
What Determines the Anatomy of the CoronaryArteries?
The major coronary arteries occupy the atrioventricularand interventricular grooves [18]. Although there are 4such grooves—right and left atrioventricular and anteriorand inferior interventricular—we describe only 3 majorcoronary arteries. This is because the inferior interven-tricular artery, usually described incorrectly as the pos-terior descending artery [19], takes its origin from 1 or theother, or sometimes both, of the 2 arteries located withinthe atrioventricular grooves. These arteries, the rightcoronary artery (RCA) and the circumflex coronary artery(CXA), extend around the orifices of the tricuspid andmitral valves, respectively. The third major coronaryartery is located in the anterior interventricular groove(anterior interventricular artery [AIVA]), also known asthe left anterior descending (LAD) artery. The arteriestake their proximal origin from the aortic valvar sinusesthat are adjacent to the pulmonary trunk [18, 20, 21],with the right-sided adjacent aortic sinus giving rise tothe RCA and the left-sided adjacent sinus to the CXA andAIVA, usually through a short common stem. This nor-mal pattern can be described as dual sinus origin. Itsessential feature is that irrespective of the relationship ofthe arterial roots to each other, coronary arteries enterthe aortic root from each side. An alternative descriptiontherefore is bilateral root entry (Fig 1A). One well-recognized variation is seen when the CXA extendsthrough the transverse pericardial sinus, taking its originfrom the right-sided adjacent aortic sinus (Fig 1B). An-other important variation is found when either the RCA
Address correspondence to Dr Chiu, Department of Surgery, NationalTaiwan University Hospital, No. 7 Chung-Shan S. Road, Taipei, Taiwan100; e-mail: [email protected].
© 2012 by The Society of Thoracic Surgeons 0003-4975/$36.00Published by Elsevier Inc http://dx.doi.org/10.1016/j.athoracsur.2012.05.133
REV
IEW

or the main stem of the left coronary artery runs betweenthe subpulmonary infundibulum and the aortic root,taking origin from the opposite adjacent aortic sinus [1,22]. This produces an interarterial variation, which canexist with or without an additional intramural variant(Fig 2) [23]. Other variations include those in which asingle coronary artery takes its origin from either side ofthe aortic root, or all major coronary arteries arise fromthe same sinus in the absence of interarterial coursing.These patterns, with their variations [22, 24, 25], cancollectively be described as unilateral root entry, thusdistinguishing the arrangements from the more usualsituations in which the coronary arteries take origin fromeach side of the aortic root, in other words bilateral rootentry. As we will show, these differences are crucial inunderstanding the overall variations in coronary arterialanatomy.
Embryologic Development of the CoronaryArteries
In the past, concepts based on embryology have beensaid to serve as a hindrance rather than a help inanalyzing normal and abnormal anatomic arrange-ments [26]. Nonetheless, advances in the understand-ing of the mechanisms of development require reeval-uation of this opinion. Thus all of the normal patternsfor coronary artery disposition, along with their varia-tions, can now readily be understood on the basis ofrecent findings concerning their embryologic develop-ment [20, 27–30]. The major epicardial coronary arter-ies attain their aortic connections relatively late indevelopment, subsequent to the process of aortopul-monary rotation [28, 30]. It used to be thought that the
proximal parts of the coronary arteries budded outfrom the aortic sinuses. It is now accepted that thecoronary arteries develop within the epicardial atrio-ventricular and interventricular grooves and that theirproximal parts grow into the aortic valvar sinuses [27].
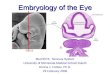
Fig 1. Anatomy of normal coronary arteries is well shown by computed tomography. (A) The aortic root as viewed from above. Right and leftcoronary arteries arise from the aortic valvar sinuses adjacent to the subpulmonary infundibulum, which has been transected to provide thisimage. (B) Variant in an otherwise normal heart in which the circumflex coronary artery arises from the right coronary artery and then ex-tends through the transverse sinus. The anterior interventricular artery takes origin from sinus #2 (not seen). ([A] Courtesy of Dr Tony Hlava-cek, Medical University of South Carolina.)
Fig 2. Computed tomographic image shows intramural origin ofthe right coronary artery (RCA). The aortic root is viewed frombehind. The RCA crosses the commissure (white arrow) betweenthe leaflets of the aortic valve supported within sinuses adjacentto the subpulmonary infundibulum and takes its origin from theleft-hand sinus #2. The left coronary artery is also seen taking itsorigin from sinus #2. (Courtesy of Dr Tony Hlavacek, MedicalUniversity of South Carolina.)
1752 REVIEW CHIU AND ANDERSON Ann Thorac SurgUNDERSTANDING CORONARY ARTERIAL ANATOMY 2012;94:1751–60
REV
IEW

The existence of arteries coursing anterior or posteriorto the arterial roots also supports the notion that acrown-like configuration of arterial primordia is to befound around the developing aortic and pulmonaryroots [29]. Since the major coronary arteries hardlyever take origin from the nonadjacent aortic sinus, andwhen arising anomalously from the pulmonary trunkalso frequently arise from adjacent sinuses [31], factorsrelated to the separation of the arterial roots by fusionof the major outflow cushions almost certainly guidetheir proximal in-growth toward the valvar sinuses[20]. This notion is further supported by the markedvariability in sinusal origin of the coronary arteries inthe setting of a common arterial trunk [32, 33], whichexists because of failure of septation of the developingoutflow tract [34]. An exaggeration of this guidingpattern would also be sufficient to direct one or theother of the right and left coronary arteries beyond itsintended site of origin, producing the intramural vari-ant with single-sinus origin but bilateral root entry [35,36]. We can expect therefore that these intramuralpatterns will be seen as variants of the patterns alreadywell recognized for dual sinus entry [11, 36]. It is alsointuitive to suggest that part of the guiding mechanismdepends on the proximity of the 2 adjacent aorticsinuses to the atrioventricular and anterior interven-tricular groove. Since the coronary arteries must per-force pierce the sinusal wall only subsequent to theestablishment of aortic position, it is the final locationof the aortic root relative to the cardiac base that isresponsible for producing the marriage of conveniencebetween the major coronary arteries and their sinusesof origin [11, 16, 17, 37, 38].
Evidence From Previous Descriptions
Review of publications describing the patterns of thecoronary arteries in transposition, congenitally cor-rected transposition, and tetralogy of Fallot shows thatthe coronary arteries are not always arranged in theiranticipated fashion and that this fact also holds for theotherwise normal heart [1, 2, 9]. In tetralogy of Fallot,eg, the rightward location of the aorta reduces thedistance between sinus #1 and the AIVA, thus explain-ing why an AIVA is often found crossing the narrowedsubpulmonic infundibulum (Fig 3c) [39]. Furthermore,the anomalous course in this setting is more frequentwhen the aortic root is rotated and located even moreanteriorly [40]. Nonetheless, the greatest variation incoronary artery arrangement [8, 14] is found whentransposed arterial trunks exist in the setting of con-cordant atrioventricular connections [41], in otherwords “regular” transposition (Fig 3). In this setting,the right-sided aortic valvar sinus, known as sinus #2,is the one that is closest to the right atrioventriculargroove. An artery exiting from this sinus will enter theright-sided atrioventricular groove directly. The left-sided aortic valvar sinus, sinus #1, is directly adjacentto the anterior interventricular groove. An artery exit-ing from this sinus is able not only to enter the anterior
groove but also to give a branch that passes directlyinto the left atrioventricular groove. It is not surprisingtherefore that the most frequent arterial relationship intransposition (when the aorta is positioned rightwardand anterior) is associated with the origin of the AIVAand CXA from sinus #1 and the RCA arising from sinus#2 (Fig 3a). There are nonetheless multiple alternatepatterns. Most existing classifications were devised inattempts to cater for description of these variations. Nosingle classification has achieved universal acceptance.The classification of Yacoub and Radley-Smith [7, 42],eg, accounts for relatively few of the known variations.It also mixes the features used for classification, with 4of the described patterns accounting for varying si-nusal origin of the main coronary arteries, but 2 ofthem (types B and C) showing the same sinusal anat-omy. This classification was subsequently expanded toinclude details of the course of the proximal coronaryarteries relative to the arterial pedicle, a feature ofobvious surgical significance [43– 45]. In this regard,the feature of the second most common pattern is forthe CXA to run a retropulmonary course, passing
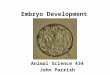
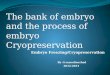
Fig 3. The 5 basic options for dual sinus origin of coronary arter-ies recognized thus far in the setting of regular transposition, il-lustrating the arterial relationships most frequently seen with thedifferent patterns [11]. (a) Usual pattern. (b) As aortic root ro-tates more obliquely toward the right, the circumflex coronaryartery (CXA) tends to move posteriorly and can originate, alongwith the right coronary artery (RCA), from sinus #2, the anteriorventricular artery (AIVA) retaining its origin from sinus #1. (c)When the aortic root moves further rightward and lateral, it ismore frequent for the RCA and the AIVA to arise from sinus #1,the CXA originating from sinus #2 but taking a retropulmonarycourse. (d) When arterial trunks are “normally related” in trans-position, however, the origin of the coronary arteries is as usuallyseen in the normal heart. (e) Should the aortic root be rotated toa left lateral location, the AIVA, along with the RCA, often takesits origin from sinus #2, with the RCA running in an anteropul-monary position, the CXA taking origin from sinus #1. (A !AIVA; L ! CXA; R ! RCA.)
1753Ann Thorac Surg REVIEW CHIU AND ANDERSON2012;94:1751–60 UNDERSTANDING CORONARY ARTERIAL ANATOMY
REV
IEW

through the transverse pericardial sinus to reach theleft atrioventricular groove (Fig 3b). This retropulmo-nary passage of the CXA can also be found when boththe RCA and AIVA arise from sinus #1 (Fig 3c).Furthermore, the latter patterns with retropulmonaryCXA are known to be more frequent when the arterialtrunks are rotated from the oblique orientation towarda more side-by-side arrangement [10, 42– 44]. One ofthe oldest classifications, that proposed by Elliott andcolleagues [46], had previously emphasized this effectof rotation of the aortic root. The clockwise rotation ofthe aortic root from the anticipated right anteriorlocation takes the left-handed aortic sinus into a pos-terior position and closer to both the transverse peri-cardial sinus and the left atrioventricular groove (Fig3b, 3c). This influence of the location of the aortic rootrelative to the cardiac base also offers an explanationfor why, when the aorta arises from the right ventriclebut in a posterior position (Fig 3d) (the arrangementknown as posterior transposition), the coronary arter-ies arise in the fashion expected for the normal heart[11, 47]. It also explains why, when the aorta is anteriorbut leftward located in so-called regular transposition,the RCA has to cross in front of the pulmonary trunk totake origin, along with the AIVA, from sinus #2 (Fig 3e)[11, 48].
Taken together, these associations point to the sig-nificant influence of aortic position in determiningsinusal origin of the coronary arteries [12, 37, 48 –50].There are nonetheless other subtle variations to befound in arterial anatomy, such as duplication orabsence of the major epicardial branches. An attemptto incorporate all this information into one system [8]produced huge complexity (Fig 4). Another system,devised by Gittenberger-de Groot and colleagues [12],with its roots in the doctoral thesis of Quaegebeur [13],removed the necessity for describing the location ofthe aortic root. These studies showed that irrespectiveof arterial relationships, the 2 aortic sinuses adjacent tothe pulmonary root could always be designated asbeing to the right or left of the observer standing in thenonadjacent sinus and codified as #1 and #2. Althoughthe system is now well accepted by the surgical com-munity [4, 13–15, 37, 51, 52], it fails to provide for eachindividual patient the crucial information concerningthe location of the aortic root. It is only when we takenote of the location of the aortic root in addition tosinusal origin that we can explain one of the conun-drums that remains concerning the arrangement of thecoronary arteries in the setting of transposed arterialtrunks.
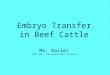
Fig 4. Numeric-alphabetic classification devised by Shaher and Puddu [8], combining information concerning sinusal origin and the epicardialcourse of the coronary arteries. All variants drawn in a fixed aortic position rightward and anteriorly have been modified to show the moretypical locations of the aortic root for the various patterns identified [11]. Type 9, the arrangement seen in the normal heart, is a mirror imageof type 1. Types 3, 5, and 7 illustrate variants of single coronary artery, whereas types 2, 4, 6, and 8 elucidate various types of unusual cir-cumflex coronary artery.
1754 REVIEW CHIU AND ANDERSON Ann Thorac SurgUNDERSTANDING CORONARY ARTERIAL ANATOMY 2012;94:1751–60
REV
IEW

The “Missing Option” in Patients WithTransposition
When one of us (RHA) was working with the archive ofcongenitally malformed hearts housed at Children’sHospital of Pittsburgh, a selection was made at randomof 100 hearts with concordant atrioventricular anddiscordant ventriculoarterial connections. At the time,RHA was convinced that the system proposed byQuaegebeur [13] was the optimal means of describingcoronary arterial anatomy, so as discussed earlier, heneglected to note the specific relationship of the trans-posed aortic root relative to the ventricular base whendescribing the sinusal origins. It remains impressive,nonetheless, that 7 of the 8 possibilities predicted onthe basis of 3 coronary arteries arising from only 2aortic sinuses [15, 41] were present within the smallgroup of hearts selected from the archive (Fig 5, first 2rows). The question was not posed, however, as to whyone of the patterns had not been encountered. Oursubsequent review of the salient published literatureproviding details on more than 6,000 patients [3, 4, 7–9,
11, 12, 35, 42– 44, 46, 48 –50, 53, 54] now shows that thisoption was not only missing in the 100 hearts selectedat random from Pittsburgh but also that it has neverbeen described in the setting of “regular” transposi-tion. The missing option exists when the RCA and theCXA are supposed to arise from sinus #1 and the AIVAis supposed to arise from sinus #2 (Fig 5, third rowmiddle). We are now able, based on marriage ofconvenience, to explain the lack of this option. Asalready discussed, usually the aorta is anterior andright-sided in patients with typical transposition. Inthis situation, sinus #2 is located rightward and poste-rior relative to the heart itself. If the AIVA was takingorigin from this sinus, as would be necessary to pro-duce the missing option, this artery would need tocross the epicardial territory of either the RCA or theCXA to reach the anterior interventricular groove (Fig5, gray figure in third row left). This is unlikely tohappen. The only situation that would favor the missingoption on the basis of marriage of convenience is whenthe aortic root is positioned posterior and leftward rela-
Fig 5. Eight theoretical possibilities for sinusal origin of the coronary artery patterns on the basis of 3 major coronary arteries taking originfrom the 2 adjacent aortic valvar sinuses. The numbers show the frequency of the various patterns discovered within a cohort of 100 heartsselected from the archive of congenitally malformed hearts held at Children’s Hospital of Pittsburgh. The 8 potential patterns in three rowsinclude the 2 variations with origin of a solitary coronary artery, which is shown in the middle and right panels, middle row. These 2 patternsthen have multiple variations in terms of epicardial branching, which are grouped together here on the basis of identical sinusal origin. Theremaining 6 possibilities are those with bilateral root entry. (Left-hand panel, bottom row) The missing option is impossible when the aorta isanterior and rightward. (Right hand panel, bottom row) The missing option is possible if the aorta is positioned posteriorly and leftward. Thisaortic position, however, has never been encountered in patients with “regular” transposition. (A ! anterior ventricular artery; L ! circumflexcoronary artery; PT ! pulmonary trunk; R ! right coronary artery.)
1755Ann Thorac Surg REVIEW CHIU AND ANDERSON2012;94:1751–60 UNDERSTANDING CORONARY ARTERIAL ANATOMY
REV
IEW

tive to the pulmonary trunk so that both the RCA and theCXA could arise from sinus #1, which would be locatedposteriorly, whereas the AIVA would arise from theanteriorly located sinus #2. This aortic position has yet tobe described in regular transposition but does exist whencongenitally corrected transposition coexists with a pos-terior aorta (Fig 6A) [16] or when the arterial trunks ariseconcordantly in parallel fashion from the ventricularmass [17] but with the aorta posteriorly located relative tothe pulmonary trunk (Fig 6B). It cannot be coincidental,therefore, that this missing option has been encounteredin both these situations, as well as in a relatively commonvariation in the otherwise normal heart (Figs 1B, 6C).Furthermore, this variation is advantaged when the aortais more posteriorly located than is usually the case [55], inthis way bringing sinus #1 closer to the left atrioventric-ular groove (Fig 6C). These findings further reinforce thenotion of marriage of convenience.
How Should We Describe the Variations inCoronary Artery Pattern?
The sophistication in diagnostic techniques is now suffi-ciently great for nearly all the crucial information relatingto coronary artery patterns to be provided preoperatively[22, 56]. This information should now include analysis ofthe precise relationship of the aorta to the pulmonarytrunk, as well as the location of the facing commissureand sinuses [8, 57]; the sinusal origin of the 3 majorcoronary arteries; information relating to ectopic loca-tion, including eccentric origin and high or low takeoff [1,21, 35, 36, 57]; intramural course of their orifices; theirepicardial course relative to the arterial pedicles; andsalient information concerning the individual branchingof the arteries themselves, such as dual origin ofanterior interventricular arteries. Ideally, descriptionsshould also include details of the origin of the artery to
Fig 6. (A) Missing option for coronary artery arrangement in the setting of “regular transposition” has been observed in patients with congenitally correctedtransposition with a left posterior aortic root. There was retropulmonary coursing of the right-sided circumflex coronary artery (CXA) to sinus #1, the left-sided right coronary artery (RCA) taking a retroaortic course, also to take origin from sinus #1, whereas the anterior ventricular artery (AIVA) took directorigin from sinus #2. (B) This option was also discovered in the setting of arterial trunks arising concordantly and in parallel fashion from the ventricularmass, but with the aorta posteriorly located relative to the pulmonary trunk. In this instance, the retroaortic CXA arose from the RCA, which itself took ori-gin from sinus #1, whereas the AIVA took origin from sinus #2. (C) This pattern is a more frequent finding in the otherwise normal heart, as shown in Fig-ure 1B. In this setting, an almost directly posterior aortic position produces greater adjacency between the left atrioventricular groove and sinus #1.
1756 REVIEW CHIU AND ANDERSON Ann Thorac SurgUNDERSTANDING CORONARY ARTERIAL ANATOMY 2012;94:1751–60
REV
IEW

the sinus node [50, 58], which may need to be redi-rected if it originates directly from an aortic valvarsinus (Fig 4), albeit current resolution of computedtomography still makes the identification of this detaildifficult. The diagnostician will hopefully, nonetheless,seek to provide as much information as possible foreach patient being discussed for corrective surgery.When we compare the accounts given by differentgroups, all this information may prove to be of clinicalsignificance. It is the information regarding the loca-tion of the aortic root, however, that currently is mostoften ignored [4, 14, 15, 51, 52].
Patterns With Origins From Two Aortic Sinuses andWith Bilateral Entry to the Aortic RootSinusal origin and aortic position are closely related interms of the development of the given patterns to thearrangements seen in those patients in whom 2 aorticsinuses give rise to 3 major coronary arteries, thesesinuses almost without exception being adjacent to thepulmonary trunk. It was recognition of this associationthat underscored the system proposed by our groupworking in Taiwan, which uses the concept of “2 " 3” toproduce a unifying system for the various patterns seenin transposition [11, 54, 59] and other congenitally mal-formed hearts [16, 17, 40]. We now recognize the need toconstruct 2 circles to provide full understanding of the
potential patterns (Fig 7). The first circle accounts for themarriage of convenience between the rotated aortic rootand the proximal orifices of the coronary arteries locatedin 3 anatomic grooves in the setting of right-hand ven-tricular topology, whereas the second circle accounts forleft-hand topology [16, 59]. Both circles are proposedbecause in the presence of left-handed topology, themorphologically right and left atrioventricular groovesare on the opposite side of the heart relative to the facingaortic coronary sinuses (Fig 6A). In the setting of left-hand topology, the CXA, occupying the right-sided atrio-ventricular groove, is closest to sinus #2, as in the usualvariant of congenitally corrected transposition, andtherefore usually arises from this sinus, along with theAIVA (Fig 7B, illustrated at the 3 o’clock position). Ap-preciation of the orientation of the aortic root within our2 suggested circles can therefore provide a rational ex-planation for all the known anomalous patterns of themajor coronary arteries in the setting of dual sinus originwith bilateral root entry.
Patterns in Which the Coronary Arteries Arise From aSingle Aortic Sinus but With Bilateral Entry to theAortic RootAppreciation of the orientation of the aortic root rela-tive to the cardiac base inside the circle in Figure 8Aalso provides a rational explanation for the anomalous
Fig 7. The 6 potential options for bilateral root entry illustrated relative to most likely locations of the aortic root. (A) Options for right-hand (RH) ventricu-lar topology. (B) Left-hand (LH) topology. The patterns reported most frequently for transposition (TGA), tetralogy of Fallot (TF), congenitally correctedtransposition (CCT), and concordant ventriculoarterial connection with parallel arterial trunks (Conc VA conn with PAT) and otherwise normal heart eachoccupy a different portion of the horizontal circle representing the location of the aortic root within the cardiac base. The gap between panels (d) and (e) inFigure 3 is now filled by the missing option in Figure 6. In patients with left-hand ventricular topology, the left-sided atrioventricular groove contains themorphologic right coronary artery (RCA), whereas the right-sided groove contains the morphologic circumflex coronary artery (CXA). (A ! anterior inter-ventricular artery; L ! circumflex coronary artery; R ! right coronary artery.)
1757Ann Thorac Surg REVIEW CHIU AND ANDERSON2012;94:1751–60 UNDERSTANDING CORONARY ARTERIAL ANATOMY
REV
IEW

coronary artery patterns observed when both arteriestake their origin from the same sinus but with thearteries entering from opposite sides of the aortic root,one or the other then taking an interarterial course (Fig8A, outside the circle). The pattern illustrated betweenthe 10 and 11 o’clock positions outside the circle inFigure 8A is the interarterial and intramural variantshown in Figure 2, known now to be a harbinger ofsudden cardiac death.
Patterns With Unilateral Entry to the Aortic RootOur review of the salient literature indicates that aorticposition varies not only for the different patterns seenwhen coronary arteries enter through both sides of theaortic root but also when all the coronary arteries enterthe aortic root from the same side (Fig 8B), these beingthe variants for single coronary artery. For example, thesingle artery above the right circle at the 11 o’clockposition in Figure 8B is reported in tetralogy of Fallot [60].However, this type has not yet, to the best of ourknowledge, been reported in “regular” transposition.Our analysis to date therefore suggests that the potentialpatterns for single sinus origin with unilateral entry tothe aortic root are also influenced by the location of theaortic root itself.
Surgical Implications
It could be argued that the full clinical significance of themultiple variations we have reviewed has yet to be
established. It might also be thought that intraventricularanatomy also influences coronary artery arrangements.We are unaware of any convincing evidence supportingthis latter notion. Indeed, evidence supporting such asuggestion could not be assembled unless a unifiedconcept is constructed to provide the basis for under-standing all the variations. Our hope is that our reviewmight provide the impetus for agreement on such aconcept. Nonetheless, in the current surgical climate,information concerning the origins and course of thecoronary arteries, and their orientation to the aortic root,is of most significance to those performing the arterialswitch procedure, in which optimal redirection of all thecoronary arteries in situ remains the cornerstone ofsurgical success [61, 62]. All known patterns are amena-ble to transfer [3, 53], although the late recurrence ofcoronary artery obstruction, which has been reported tobe as high as 3% to 7.8 % [63, 64], may well be related tovariations in coronary arterial anatomy [50, 53]. We havealready proposed diagnostic techniques for the recogni-tion of potentially dangerous coronary artery patternsand surgical techniques for their correction [36, 57, 62]. Inparticular, when redirecting the origin of coronary arter-ies adjacent to the facing commissure, or an arterypassing intramurally across this commissure, we con-sider it advantageous to create a single arterial button bymeans of a superiorly based trapdoor. In addition to theshort axis rotation, which reflects the juxtacommissuralorigin of the coronary artery [36], it is also frequentlynecessary to be aware of additional rotation in the long
Fig 8. Variants for single coronary artery can also be understood on the basis of marriage of convenience. (A) Variants with bilateral root en-try, with the 6 established options for dual sinus origin inside the circle, and the small black images positioned outside the circle representingthe options passing interarterially into the opposite sinus to produce the variants of bilateral root entry with single sinus origin. (B) Potentialvariations for unilateral root entry are shown in blue outside the circle, these being the variants with single coronary arteries. The specifictypes discovered in each disease entity labeled in the center have occupied different portions of the circle, suggesting that these abnormal pat-terns are also influenced by the location of the aortic root. (AVG ! atrioventricular groove; CCT ! congenitally corrected transposition;IVG ! interventricular groove; TF ! tetralogy of Fallot; TGA ! transposition.)
1758 REVIEW CHIU AND ANDERSON Ann Thorac SurgUNDERSTANDING CORONARY ARTERIAL ANATOMY 2012;94:1751–60
REV
IEW

axis should the abnormal coronary artery also show hightakeoff [50, 57], this being a frequent additional finding inthe setting of intramural origin.
Conclusions
We suggest that in the future when charting details ofsurgical correction of coronary artery anomalies or de-scribing the operative procedure for the arterial switch,information should be provided not only of sinusal originbut also of the location of the aortic root relative to thecardiac base. Emphasis should also be given to whetherthe coronary arteries enter the aortic root from both sidesor whether there is unilateral entry. Only when all thisinformation is widely available will we be able to judgewhether it is truly possible to provide a universallyacceptable classification for coronary arterial anatomy.Irrespective of whether we achieve a suitable classifica-tion, the provision of information concerning aortic po-sition as well as sinusal origin will make it easier to assessthe remaining surgical risk factors for procedures such asthe arterial switch.
We are indebted to all our colleagues in Taiwan who contributedto earlier studies establishing the importance of the aortic rootposition in determining the options for coronary artery patternsin congenitally malformed hearts, and to Drs Tony Hlavacek andMarios Loukas, and Mrs Diane Spicer, who worked extensivelywith us to establish the arrangement of the normal coronaryarteries. We also thank Dr Hlavacek for permitting us to repro-duce Figures 1 and 2. We are grateful to Miss Chang-Ying Lin forthe preparation of Figures 3 through 8. This study was supportedby a grant from the National Science Council in Taiwan(NSC97–2314–B–002–043–MY3).
References1. Angelini P. Coronary artery anomalies. An entity in search of
an identity. Circulation 2007;115:1296–305.2. Angelini P, Velasco JA, Ott D, Khoshnevis GR. Anomalous
coronary artery arising from the opposite sinus: descriptivefeatures and pathophysiologic mechanisms, as documentedby intravascular ultrasonography. J Invasive Cardiol 2003;15:507–14.
3. Pasquali SK, Hasselblad V, Li JS, Kong DF, Sanders SP.Coronary artery pattern and outcome of arterial switchoperation for transposition of the great arteries: a meta-analysis. Circulation 2002;106:2575–80.
4. Asou T, Karl TR, Pawade A, Mee RB. Arterial switch:translocation of the intramural coronary artery. Ann ThoracSurg 1994;57:461–5.
5. Dabizzi RP, Caprioli G, Aiazzi L, et al. Distribution andanomalies of coronary arteries in tetralogy of Fallot. Circu-lation 1980;61:95–102.
6. Planche C, Sousa-Uva M. Invited commentary on “Coronaryartery anatomy in complete transposition of the great arter-ies.” Ann Thorac Surg 1994;57:894.
7. Yacoub MH, Radley-Smith R. Anatomy of the coronaryarteries in transposition of the great arteries and methodsfor their transfer in anatomical correction. Thorax 1978;33:418 –24.
8. Shaher RM, Puddu GC. Coronary arterial anatomy in com-plete transposition of the great vessels. Am J Cardiol 1966;17:355–61.
9. Yamaguchi M, Hosokawa Y, Imai Y, et al. Early and midtermresults of the arterial switch operation for transposition of
the great arteries in Japan. J Thorac Cardiovasc Surg1990;100:261–9.
10. Kurosawa H, Imai Y, Kawada M. Coronary arterial anatomyin regard to the arterial switch procedure. Cardiol Young1991;1:54–62.
11. Chiu IS, Chu SH, Wang JK, et al. Evolution of coronaryartery pattern according to short-axis aortopulmonary rota-tion: a new categorization for complete transposition of thegreat arteries. J Am Coll Cardiol 1995;26:250–8.
12. Gittenberger-de Groot AC, Sauer U, Oppenheimer-DekkerA, Quaegebeur J. Coronary arterial anatomy in transpositionof the great arteries: a morphologic study. Pediatr Cardiol1983;4 (Suppl I):15–24.
13. Quaegebeur JM. The arterial switch operation: rationale,results, perspectives. Thesis, Leiden University, The Neth-erlands;1986:43–71.
14. Amato JJ, Zelen J, Bushong J. Coronary arterial patterns incomplete transposition–classification in relation to the arte-rial switch procedure. Cardiol Young 1994;4:329–39.
15. Massoudy P, Baltalarli A, de Leval MR, et al. Anatomicvariability in coronary arterial distribution with regard to thearterial switch procedure. Circulation 2002;106:1980–4.
16. Chiu IS, Wu SJ, Chen SJ, et al. Sequential diagnosis ofcoronary arterial anatomy in congenitally corrected transpo-sition of the great arteries. Ann Thorac Surg 2003;75:422–9.
17. Huang SC, Chiu IS, Lee ML, et al. Coronary artery anatomyin anatomically corrected malposition of the great arteriesand their surgical implications. Eur J Cardiothorac Surg2011;39:705–10.
18. Loukas M, Groat C, Khangura R, Owens DG, Anderson RH.The normal and abnormal anatomy of the coronary arteries.Clin Anat 2009; 22:114–28.
19. Cook AC, Anderson RH. Editorial. Attitudinally correctnomenclature. Heart 2002;87:503–6.
20. Hutchins GM, Kessler-Hanna A, Moore GW. Developmentof the coronary arteries in the embryonic human heart.Circulation 1988;77:1250–7.
21. Angelini P, de la Cruz MV. The relationship between thecoronary arteries and congenital heart disease. In: AngeliniP, ed. Coronary Artery Anomalies: A Comprehensive Ap-proach. Philadelphia, PA: Lippincott Williams & Wilkins;1999:173–89.
22. Hlavacek A, Loukas M, Spicer D, Anderson RH. Anomalousorigin and course of the coronary arteries. Cardiol Young2010;20(Suppl 3):20–5.
23. Brothers JA, Gaynor JW, Jacobs JP, et al. The registry ofanomalous aortic origin of the coronary artery of the Con-genital Heart Surgeons’ Society. Cardiol Young 2010;20(Suppl 3):50–8.
24. Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L.Isolated single coronary artery: diagnosis, angiographicclassification, and clinical significance. Radiology 1979;130:39 – 47.
25. Desmet W, Vanhaecke J, Vrolix M, et al. Isolated singlecoronary artery: a review of 50,000 consecutive coronaryangiographies. Eur Heart J 1992;13:1637–40.
26. Becker AE, Anderson RH. Cardiac embryology: a help orhindrance in understanding congenital heart disease? In: NoraJJ, Takao A, eds. Congenital Heart Disease: Causes and Pro-cesses. Mount Kisco, NY: Futura Publishing Co;1984:339–58.
27. Bogers AJ, Gittenberger-de Groot AC, Poelmann RE, PeaultBM, Huysmans HA. Development of the origin of the coro-nary arteries, a matter of ingrowth or outgrowth? AnatEmbryol 1989;180:437–41.
28. Angelini P. Normal and anomalous coronary arteries: defi-nitions and classification. Am Heart J 1989;117:418–34.
29. Corone P, Corone A, Dor X, Binet JP. Coronary arteries andtheir variations. An embryological explanation. [Article inFrench] C R Acad Sci III. 1984;299:451–8.
30. Theveniau-Ruissy M, Dandonneau M, Mesbah K, et al. Thede122q11.2 candidate gene Tbx1 controls regional outflowtract identity and coronary artery patterning. Circ Res 2008;103:142–8.
1759Ann Thorac Surg REVIEW CHIU AND ANDERSON2012;94:1751–60 UNDERSTANDING CORONARY ARTERIAL ANATOMY
REV
IEW

31. Smith A, Arnold R, Anderson RH, et al. Anomalous origin ofthe left coronary artery from the pulmonary trunk. Anatomicfindings in relation to pathophysiology and surgical repair.J Thorac Cardiovasc Surg 1989;98:16–24.
32. Crupi G, Macartney FJ, Anderson RH. Persistent truncusarteriosus. A study of 66 autopsy cases with specialreference to definition and morphogenesis. Am J Cardiol1977;40:569 –78.
33. Suzuki A, Ho SY, Anderson RH, Deanfield JE. Coronaryarterial and sinusal anatomy in hearts with a commonarterial trunk. Ann Thorac Surg 1989;48:792–7.
34. Van Mierop LHS, Patterson DF, Schnarr WR. Pathogene-sis of persistent truncus arteriosus in light of observationsmade in a dog embryo with the anomaly. Am J Cardiol1978;41:755– 62.
35. Li J, Tulloh RM, Cook A, Schneider M, Ho SY, Anderson RH.Coronary arterial origins in transposition of the great arter-ies: factors that affect outcome. A morphological and clinicalstudy. Heart 2000;83:320–5.
36. Chiu IS, Wu MH, Chang CI, et al. Clinical implications ofshort-axis aortopulmonary rotation on juxtacommissural or-igin of the coronary artery in transposition of the greatarteries and surgical strategy. J Card Surg 1997;12:23–31.
37. Wernovsky G, Sanders SP. Coronary artery anatomy andtransposition of the great arteries. Coron Artery Dis 1993;4:148–57.
38. Landolt CC, Anderson JE, Zorn-Chelton S, Guyton RA,Hatcher CR, Jr, Williams WH. Importance of coronary arteryanomalies in operations for congenital heart disease. AnnThorac Surg 1986;41:351–5.
39. Longenecker CG, Reemtsma K, Creech O, Jr. Anomalouscoronary artery distribution associated with tetralogy ofFallot: a hazard in open cardiac repair. J Thorac CardiovascSurg 1961;42:258–62.
40. Chiu IS, Wu CS, Wang JK, et al. Influence of aortopulmonaryrotation on the anomalous coronary artery pattern in tetral-ogy of Fallot. Am J Cardiol 2000;85:780–4.
41. Anderson RH, Weinberg PM. The clinical anatomy of trans-position. Cardiol Young 2005;15(Suppl 1):76–87.
42. Yacoub MH. Anatomic correction of transposition of thegreat arteries: surgical technique. Pediatr Cardiol 1983;4(Suppl 1):61–6.
43. Serraf A, Lacour-Gayet F, Bruniaux J, et al. Anatomic cor-rection of transposition of the great arteries in neonates.J Am Coll Cardiol 1993;22:193–200.
44. Planche C, Lacour-Gayet F, Serraf A, et al. Anatomic repairof transposition of the great arteries. Bull Acad Natl Med1998;182:1739–55.
45. Lacour-Gayet F, Anderson RH. A uniform surgical tech-nique for transfer of both simple and complex patterns of thecoronary arteries during the arterial switch procedure. Car-diol Young 2005;15(Suppl 1):93–101.
46. Elliott LP, Amplatz K, Edwards JE. Coronary arterial patternsin transposition complexes. Anatomic and angiocardio-graphic studies. Am J Cardiol 1966;17:362–78.
47. Van Praagh R, Perez-Trevino C, Lopez-Cuellar M, et al.Transposition of the great arteries with posterior aorta,anterior pulmonary artery, subpulmonary conus and fibrouscontinuity between aortic and atrioventricular valves. Am JCardiol 1971;28:621–31.
48. Kirklin JW, Barratt-Boyes BG. Complete transposition of thegreat arteries. In: Kirklin JW, Barratt-Boyes BG, eds. CardiacSurgery. New York: Wiley;1986:1136.
49. Sim EK, van Son JA, Edwards WD, Julsrud PR, Puga FJ.Coronary artery anatomy in complete transposition of thegreat arteries. Ann Thorac Surg 1994;57:890–4.
50. Angelini P, de la Cruz MV, Valencia AM, et al. Coronaryarteries in transposition of the great arteries. Am J Cardiol1994;74:1037–41.
51. Day RW, Laks H, Drinkwater DC. The influence of coronaryanatomy on the arterial switch operation in neonates. J Tho-rac Cardiovasc Surg 1992;104:706–12.
52. Jaggers JJ, Cameron DE, Herlong R, Ungerleider RM. Con-genital heart surgery nomenclature and database project:transposition of the great arteries. Ann Thorac Surg 2000;69:S205–35.
53. Losay J, Touchot A, Serraf A, et al. Late outcome after arterialswitch operation for transposition of the great arteries.Circulation 2001;104(Suppl I):I-121–I-126.
54. Lee CH, Chiu IS, Chang CC, Wu SJ, Chen CA, Chiu HH.Coronary artery anatomy in complete transposition withsitus solitus and dextrocardia. Pediatr Cardiol 2010;31:615–9.
55. McAlpine WA. The origin of the coronary arteries. In:McAlpine WA, eds. Heart and coronary arteries: an anatom-ical atlas for clinical diagnosis, radiological investigation,and surgical treatment. Berlin: Springer-Verlag;1975:138.
56. Chen SJ, Ling MT, Lee WJ, et al. Coronary artery anatomy inchildren with congenital heart disease by computed tomog-raphy. Int J Cardiol 2007;120:363–70.
57. Chiu IS, Wang JK, Wu MH, et al. Angiographic evidence oflong-axis rotation in addition to short-axis aortopulmonaryrotation: its implication in transposition of the great arteries.Cathet Cardiovasc Diagn 1996;39:21–30.
58. Busquet J, Fontan F, Anderson RH, Ho SY, Davies MJ. Thesurgical significance of the atrial branches of the coronaryarteries. Int J Cardiol 1984;6:223–34.
59. Chiu IS, Wang JK, Wu MH. Coronary artery anatomy incomplete transposition of the great arteries with situs inver-sus. Am J Cardiol 2002;89:94–5.
60. Meng CCL, Eckner FAO, Lev M. Coronary artery distribu-tion in tetralogy of Fallot. Arch Surg 1965;90:363–6.
61. De Leval MR, Francois K, Bull C, Brawn W, Spiegelhalter D.Analysis of a cluster of surgical failures. Application to aseries of neonatal arterial switch operations. J Thorac Car-diovasc Surg 1994;107:914–24.
62. Chiu IS, Chen MR, Huang SC, et al. Restoration of trans-posed great arteries to nature. World J Pediatr CongenitHeart Surg 2011;2:287–95.
63. Tanel RE, Wernovsky G, Landzberg MJ, Perry SB, BurkeRP. Coronary artery abnormalities detected at cardiaccatheterization following the arterial switch operation fortransposition of the great arteries. Am J Cardiol 1995;76:153–7.
64. Bonnet D, Bonhoeffer P, Piechaud JF, et al. Long-term fate ofthe coronary arteries after the arterial switch operation innewborns with transposition of the great arteries. Heart1996;76:274–9.
1760 REVIEW CHIU AND ANDERSON Ann Thorac SurgUNDERSTANDING CORONARY ARTERIAL ANATOMY 2012;94:1751–60
REV
IEW