Embed Size (px)
Citation preview

EMBOLUS PROTECTION WITH THEEDWARDS EMBOL-X SYSTEM
Adverse cerebral outcomes after coronary arterybypass grafting (CABG) surgery are not uncommonand they are serious. They are associated with substan-tial increases in mortality, length of index hospital stay,and greater social and economic burden. Recently,there has been an emphasis on the life-changing effects of CABG, with particular attention to thereduction of strokes and neuropsychological changes.Consequently, stroke prevention is the most formidablechallenge facing heart surgery today.
Strokes and adverse neurological outcomes are amajor financial burden, among other things, to hospi-tals as well as to the individual. Although rare, the costof a perioperative stroke has been estimated to bebetween $60,000 and $200,000.1 Roach has estimat-ed that perioperative neurological injury occurs in asmany as 6.1% of patients undergoing CABG (Table 1).2 Predictors of a frank stroke (Type I injury)or cognitive changes (Type II injury) include, but arenot limited to, hypertension, proximal aortic athero-sclerotic burden, and pulmonary disease.Unfortunately, the stroke rates associated with CABGhave not changed appreciably in the past fifteen yearsdespite major advances in the revascularization itself.
Considering the multitude of variables required toaccomplish heart surgery, it is too simplistic to con-clude that the heart-lung machine, a common scape-goat, is the only source of emboli during cardiopul-monary bypass (CPB). Some studies have failed toshow a discernable difference in neurocognitive func-tion in patients after undergoing off-pump CABG(OPCAB) when compared to a similar cohort of on-pump CABG patients.3,4 While other reasons mayexplain these findings including low cardiac outputduring OPCAB, this highlights the importance ofunderstanding the source of emboli and their directcausal role in neurocognitive changes and strokes.
Embolus Protection with the Edwards EMBOL-X SystemBaron Lloyd Hamman, MD
Director of Cardiovascular Surgery Research, Baylor University Medical Center, Dallas, Texas
John Bryan Sims, MDBaylor University Medical Center, Dallas, Texas
Table 1: Adverse Cerebral Outcomes AfterCoronary Bypass Surgery2
• Design: 2108 CABG patients at 24 U.S. centers evaluated foradverse neurological outcomes
• 6.1% of patients had neurological injury (3.1% Type I, 3.0%Type II)
- Type I patients: 8 deaths, 55 non-fatal strokes, 2 TIAs, 1 stupor
- Type II patients: 55 deterioration of intellectual function, 8 seizures
• Predictors of Type I and Type II injury (odds ratio)
- Type I: proximal aortic atherosclerosis (4.52), prior neurological disease (3.19), age (1.75/decade), history of pulmonary disease (2.09)
- Type II: history of excessive alcohol consumption (2.64), CHF on surgery day (2.46), age (2.20/decade), prior CABG (2.18), postoperative arrhythmia (1.97)
• Average additional length of hospital stay and additionalcosts compared to patients without neurological injury(assuming $890 per day in an ICU and $370 per day on a ward)
- Type I patients: ICU 8 days, Ward 7 days; $10,266 in additional costs
- Type II patients: ICU 4 days, Ward 7 days; $6,150 in additional costs

Transcranial Doppler (TCD) data has provided insight intothis issue. Over 20 years ago, Pugsley et al examined therelationship between TCD signals and actual emboli in thelaboratory setting. Microspheres were injected into theblood stream and confirmed by TCD, suggesting that theTCD signals were indeed from small emboli in the arterialblood. Moreover, the distribution of the microspheres corre-lated with distribution of the experimentally induced strokesconfirming a positive correlation of TCD signals with stroke.In human patients, Pugsley and his associates also observedthat the number of emboli correlated with the severity andthe duration of Type I and II defects measured 8 weeks aftercompletion of the CABG operation.5 High intraoperativecounts of emboli (>1000) resulted in 43% of patientsexhibiting either Type I or II deficits. Conversely, when thenumber of emboli detected was less than 200, the incidenceof either Type I or II defects was less than 9%. This rela-tionship confirmed the correlation of TCD signals with theensuing stroke and neuropsychological impairment.Similarly, TCD became useful as a marker for estimatinginjurious peripheral emboli.
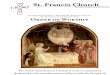
While emboli can be released throughout the entire CABGoperation, they are more prevalent during use of the car-diopulmonary bypass machine. Stump and Newman meas-ured all emboli released during a CABG operation and notedthat nearly 60% were released near the time (<1min) of aor-tic clamping or surgical manipulation.6 Barbut also notedthat nearly 60% were detected upon removal of the aorticcross-clamp or aortic partial occlusion clamp.7 Investigatorshave shown that a correlation exists between the estimatedquantity of emboli released and the length of hospital stay(Figure 1).
When emboli were first studied, it was determined that theuse of a filter in the arterial blood return could greatlydecrease the number of emboli pumped back into thepatient’s arterial circulation, and thus prevent strokes. Thisprinciple became the foundation for the development of theEMBOL-X system (Figure 2).
The system consists of a net attached to a cannula (notunlike the catheters used by cardiologists for vein graft inter-ventions) that deploys just proximal to the aortic perfusioncannula. When emboli are showered, which mainly occurswhen the clamps are released, they are potentially trapped inthe net. Because of the net’s proximal location, it does notinterfere with arterial perfusion from the bypass cannula(Figure 3). In clinical trials, nearly 97% of deployed filterswere shown to have captured emboli.9 Furthermore,deployed filters have been shown to catch not only athero-matous plaque, but also platelet and fibrin aggregates, cal-cific debris, and mechanical debris (i.e. sutures).
0
10
20
30
40
50
60
0-100 101-300 >500
Leng
th o
f Hos
pita
l Sta
y (d
ays)
8.6
No. of Emboli
301-500
13.516.3
55.8
Figure 1: LOS is Directly Related to EmboliDetection8
Figure 2: EMBOL-X System
Figure 3: EMBOL-X System Deployed

Schmitz et al showed that fewer adverse neurologicalevents occur with use of the EMBOL-X system than withoutit on initial study.10 In this prospective, controlled study ofover 500 CABG and/or valve operations, patients were alter-nately assigned to an embolic collection (filter) arm or a tra-ditional (control) arm. The endpoints included stroke, tran-sient ischemic attack, coma, delirium, and memory deficit.Patients in the filter group had a lower incidence of adverseneurological outcomes (the sum of Type I and II injuries)than patients in the control arm (4.3% v. 11.9%; p <0.001).Furthermore, there were significantly less transient ischemicattacks (0% vs 1.4%), delirium (3.0% v. 6.5%), and mem-ory deficits (1.3% v. 6.2%) in the filter group (Figure 4).There was a trend toward fewer strokes (0.7% v. 2.2%) inthe filter group, although the sample size was too small toachieve statistical significance. The authors concluded thatthe extraction of particulate emboli using intra-aortic filtra-tion decreases adverse neurological outcomes.
CASE REPORTAn anxious 70-year-old woman was admitted for elective
aortic valve replacement (AVR) for symptomatic aorticstenosis. The patient had visited with two other cardiac sur-geons prior to coming to us and conveyed to her the risk ofstroke with AVR (about 5%) (Figure 5). Despite her symp-toms, the patient was reluctant to embark on AVR becauseof her fear of having a stroke. After a long discussion aboutthe surgery, our techniques, and results, the patient willfullyconsented to valve replacement surgery.
Her comorbidities included paroxysmal atrial fibrillation,diabetes mellitus, hypertension, and hypercholesterolemia.Physical examination was remarkable for an irregular heartrhythm and a 3/6 systolic ejection murmur best heard at theright upper sternal border. Cardiac catheterization revealed
no flow-limiting lesions in the coronary arteries and a calcu-lated ejection fraction of 75%. The aortic valve was calcifiedwith a peak systolic gradient of 48 mm Hg, mean gradient of33 mm Hg, a valve area of 0.93 cm2, and a cardiac index of3.32 L/min/m2. Echocardiogram demonstrated moderateaortic stenosis and the electrocardiogram showed normalsinus rhythm with left ventricular hypertrophy. Laboratorydata was normal.
In the operating room, cardiopulmonary bypass was established by cannulating the ascending aorta with theEMBOL-X protection system. A clamp was applied to theaorta, and a tri-leaflet aortic valve was removed. The calcif-ic annulus was debrided. A 23mm Carpentier-Edwards PER-IMOUNT Magna valve with Carpentier-Edwards ThermaFixprocess was sutured into position with simple sutures. Therewas no leak by transesophageal echocardiography. TheAtricure device was then used to encircle the paired pul-monary veins on both sides. The EMBOL-X filter wasdeployed before the cross-clamp was released, and then itwas retracted just as the cardiopulmonary bypass was beingweaned. There was a calcific embolus grossly visible in thenet measuring approximately 6 x 5 x 3 mm (Figure 6). Thepatient was in second-degree heart block at the completionof the operation. She returned to the surgical intensive careunit, where she had an uneventful stay with the exception ofintermittent post-operative atrial fibrillation that was man-aged with amiodarone. She was discharged home 4 dayslater in normal sinus rhythm without any evidence of astroke or a neuropsychological deficit.
0
2
4
6
8
10
12
Stroke TIA Memory Deficit
Total
2.2%
0.7%
6.5%
3.0%
6.2%
1.3%
11.9%
4.3%
1.4%
0.0%
Delirium
Control n=278
EMBOL-X n=304
0.4% 0.3%
Coma
Figure 4: Adverse Neurologic Events10
0.00%
2.50%
5.00%
7.50%
10.00%
OPCAB CABG AVR MVR Mutliple Valve
CABG/Valve
Total
Overall (n=16,184) 4.6%
Figure 5: Procedures at Risk for Stroke11

Any quotes used in this material are taken from independent third-partypublications and are not intended to imply that such third partyreviewed or endorsed any of the products of Edwards Lifesciences.
Rx only. See instructions for use for full prescribing information.
Edwards Lifesciences devices placed on the European market meetingthe essential requirements referred to in Article 3 of the Medical DeviceDirective 93/42/EEC bear the CE marking of conformity.
Edwards, the stylized E Logo, Magna, and ThermaFix are trademarks ofEdwards Lifesciences Corporation. Edwards Lifesciences, Carpentier-Edwards, EMBOL-X, PERIMOUNT and PERIMOUNT Magna are trade-marks of Edwards Lifesciences Corporation and are registered in theUnited States Patent and Trademark Office.
Atricure is a trademark of Atricure.
© 2005 Edwards Lifesciences LLCAll rights reserved. AR01030
Edwards Lifesciences LLC · One Edwards Way · Irvine, CA 92614 USA · 949.250.2500 · 800.424.3278 · www.edwards.comEdwards Lifesciences (Canada) Inc. · 1290 Central Pkwy West, Suite 300 · Mississauga, Ontario · Canada L5C 4R3 · Phone 905.566.4220 · 800.268.3993
Edwards Lifesciences S.A. · Ch. du Glapin 6 · 1162 Saint-Prex · Switzerland · Phone 41.21.823.4300Edwards Lifesciences Japan · 2-8 Rokubancho · Chiyoda-ku, Tokyo 102-0085 · Japan · Phone 81.3.5213.5700
References:1. Bergman P, et al. Aortic atheroma is related to number of particulates captured by intra-aortic filtration CABG. European J of
Cardio-thoracic Surg 2002; 22:539-544.2. Roach GW, et al. Adverse cerebral outcomes after coronary bypass surgery. Multicenter Study of Perioperative Ischemia Research
Group and the Ischemia Research and Education Foundation Investigators. N Engl J. Med 1996; 335:1857-1863.2. 3. Taggart DP, et al. Is CPB still the cause of cognitive dysfunction after cardiac operations? J Thorac Cardiovasc Surg
1999;118:414–420.3. 4. Van Dijk D, et al. Cognitive outcomes after off-pump and on-pump coronary artery bypass graft surgery:
a randomized trial. JAMA. 2002; 287:1405–1412.4. 5. Pugsley WB, et al. The impact of microemboli during cardiopulmonary bypass on neuropsychologic functioning. Stroke 1994;
25(7):1393-1399.5. 6. Stump D.A., et al. Emboli detection during cardiopulmonary bypass. In: Tegler C.H., Babikian V.L., Gomez C.T., eds. Neurosonology.
St. Louis, MO: Mosby, 1996:252-255.6. 7. Barbut D, et al. Cerebral emboli detected during bypass surgery are associated with clamp removal. Stroke 1994; 25:2398-2402.7. 8. Barbut D, et al. Impact of Embolization During Coronary Artery Bypass Grafting on Outcome and Length of Stay. Ann Thorac Surg
1997;63:998-1002.9. Data on file at Edwards Lifesciences.10. Schmitz C, et al. Can particulate extraction from the ascending aorta reduce neurologic injury in cardiac surgery. J Thorac Cardiovasc
Surg 2003; 126(6):1829-1838. 11. Bucerius J, et al. Stroke After Cardiac Surgery: A Risk Factor Analysis of 16,184 Consecutive Adult Patients. Ann Thorac Surg
2003;75:472-8.
CONCLUSIONSComplications of open heart surgery are related to the
complexity of the case, physically opening the heart, manip-ulating the valves, the time spent on the pump and comor-bidities. Although the EMBOL-X system is slightly largerthan a standard aortic cannula and requires a secondary stepto deploy the filter, its ability to remove emboli and thereby
Figure 6
a. 6 x 5 x 3 mm calcific embolus caught in deployed “fish net”
b. 6 x 5 x 3 mm calcific embolus seen on a 3 x 3 mm grid
c. emboli caught in other cases
potentially prevent strokes justifies the use of the device.Some cardiac surgeons routinely use the EMBOL-X systemin all valve cases as well as cases with an opened aorta wheresignificant proximal aortic atherosclerotic burden can bedemonstrated by echocardiogram, x-ray, or computerizedtomography scan.

![JD Edwards EnterpriseOne Portal Reference Guide for Oracle ...[1]JD Edwards EnterpriseOne Portal Reference Guide for Oracle WebCenter Release 9.1.x E21052-01 January 2015 Describes](https://img.pdfslide.us/doc/110x75/5eca213082cb7d647f607d26/jd-edwards-enterpriseone-portal-reference-guide-for-oracle-1jd-edwards-enterpriseone.jpg)

![JD Edwards EnterpriseOne Applications Transportation ... · [1]JD Edwards EnterpriseOne Applications Transportation Management Implementation Guide Release 9.1.x E15152-10 October](https://img.pdfslide.us/doc/110x75/5f0824137e708231d4208a9f/jd-edwards-enterpriseone-applications-transportation-1jd-edwards-enterpriseone.jpg)

![JD Edwards EnterpriseOne Applications Data Interface … · [1]JD Edwards EnterpriseOne Applications Data Interface for Electronic Data Interchange Implementation Guide Release 9.1.x](https://img.pdfslide.us/doc/110x75/5b512a517f8b9a56588bbd98/jd-edwards-enterpriseone-applications-data-interface-1jd-edwards-enterpriseone.jpg)
![JD Edwards EnterpriseOne Applications Fulfillment ... · [1]JD Edwards EnterpriseOne Applications Fulfillment Management Implementation Guide Release 9.1.x E17539-08 September 2014](https://img.pdfslide.us/doc/110x75/5ae9f4337f8b9a36698c5e36/jd-edwards-enterpriseone-applications-fulfillment-1jd-edwards-enterpriseone.jpg)

![JD Edwards EnterpriseOne IBM WebSphere Portal … · [1]JD Edwards EnterpriseOne IBM WebSphere Portal Reference Guide Release 9.2.x E53620-09 April 2018 Describes how to use this](https://img.pdfslide.us/doc/110x75/5b14f2507f8b9ab6778cd662/jd-edwards-enterpriseone-ibm-websphere-portal-1jd-edwards-enterpriseone-ibm.jpg)
![JD Edwards EnterpriseOne Applications Tax Processing ... · [1]JD Edwards EnterpriseOne Applications Tax Processing Implementation Guide Release 9.1.x E15153-14 June 2019](https://img.pdfslide.us/doc/110x75/5f2b0c9df9cbb658e11ee6a0/jd-edwards-enterpriseone-applications-tax-processing-1jd-edwards-enterpriseone.jpg)

![JD Edwards EnterpriseOne HTML Web Server WebSphere … · 2020-01-07 · [1]JD Edwards EnterpriseOne HTML Server on WebSphere Reference Guide Release 9.2.x for Microsoft Windows E41914-06](https://img.pdfslide.us/doc/110x75/5ea00661170c702d1476b557/jd-edwards-enterpriseone-html-web-server-websphere-2020-01-07-1jd-edwards-enterpriseone.jpg)










![1[]JD Edwards EnterpriseOneTools Internet ofThings ... · 1[]JD Edwards EnterpriseOneTools Internet ofThings Orchestrator Guide Release 9.1.5.x E64166-04 September 2015 Provides an](https://img.pdfslide.us/doc/110x75/5f0be93f7e708231d432d356/1jd-edwards-enterpriseonetools-internet-ofthings-1jd-edwards-enterpriseonetools.jpg)
![1[]JD Edwards EnterpriseOne Applications OneView Financial ... · 1[]JD Edwards EnterpriseOne Applications OneView Financial Statements Release 9.2.x E60158-06 April 2017 Describes](https://img.pdfslide.us/doc/110x75/5adc83097f8b9a9d4d8be10e/1jd-edwards-enterpriseone-applications-oneview-financial-jd-edwards-enterpriseone.jpg)



![JD Edwards EnterpriseOne Deployment Server …[1]JD Edwards EnterpriseOne Deployment Server Reference Guide for Enterprise Systems Tools Release 9.2.x and Applications Release 9.2.x](https://img.pdfslide.us/doc/110x75/5eae8916933dd824af240c21/jd-edwards-enterpriseone-deployment-server-1jd-edwards-enterpriseone-deployment.jpg)