Embed Size (px)
Citation preview

European Journal of Cancer (2015) 51, 1822– 1830
A v a i l a b l e a t w w w . s c i e nc e d i r e c t . c o m
ScienceDirect
jour na l homepage : www.e jcancer . com
Elimination of primary tumours and control of metastasiswith rationally designed bacteriochlorin photodynamictherapy regimens
http://dx.doi.org/10.1016/j.ejca.2015.06.002
0959-8049/� 2015 Elsevier Ltd. All rights reserved.
⇑ Corresponding authors at: Faculty of Chemistry, JagiellonianUniversity, 30-060 Krakow, Poland. Tel.: +48 126632293(J.M. Dabrowski). Chemistry Department, University of Coimbra,3004-535 Coimbra, Portugal. Tel.: +315 239854484 (L.G. Arnaut).
E-mail addresses: [email protected] (J.M. Dabrowski),[email protected] (L.G. Arnaut).
Luis B. Rocha a, Lıgia C. Gomes-da-Silva b, Janusz M. Dabrowski c,⇑, Luis G. Arnaut a,b,⇑
a Luzitin SA, R. Bayer, S. Martinho do Bispo, 3045-016 Coimbra, Portugalb Chemistry Department, University of Coimbra, 3004-535 Coimbra, Portugalc Faculty of Chemistry, Jagiellonian University, 30-060 Krakow, Poland
Received 13 December 2014; received in revised form 9 February 2015; accepted 15 June 2015Available online 29 June 2015
KEYWORDS
Anti-cancer activityAnti-tumour immunityBacteriochlorinsCancerMetastasisPhototoxicityPhotosensitiserPhotodynamic therapyPhotodynamic-immunotherapy
Abstract Photodynamic therapy (PDT) with current photosensitisers focuses on local effectsand these are limited by light penetration in tissues. We employ a stable near-infrared (NIR)absorbing bacteriochlorin with ca. 8 h plasma half-life to increase the depth of the treatmentand elicit strong systemic (immune) responses. Primary tumour growth delays and cures ofBALB/c and nude mice bearing CT26 mouse colon carcinoma are related to the parametersthat control PDT efficacy. The systemic anti-tumour protection elicited by the optimisedPDT regimen is assessed by tumour rechallenges and by resistance to the establishment ofmetastasis after intravenous injection of CT26 cells. The optimised treatment regime offered86% cure rate in BALB/c mice but no cures in BALB/c nude mice. Cured mice rechallengedover 3 months later with CT26 cells rejected the tumour cells in 67% of the cases. PDT of asubcutaneous CT26 tumour 5 days after the additional intravenous injection of CT26 cellsvery significantly reduced lung metastasis. The PDT regimen optimised for the bacteriochlorinleads to remarkable long-term survival rates, effective immune memory and control of lungmetastasis.� 2015 Elsevier Ltd. All rights reserved.
1. Introduction
Photodynamic therapy (PDT) is a promising cancertreatment owing to its selectivity and absence of adversedrug reactions [1]. PDT is based on the photosensitiseradministration, its accumulation in tumours and thenillumination with light. Photosensitisers absorbing light

Table 1Factors that limit the range of the parameters controlled in photody-namic therapy (PDT).
Parameter Lower limit range Higher limit range
Drug-to-light interval(DLI)
Selectivity Drug clearance
Irradiance Sub-lethal damage Oxygen depletionLight dose Depth of treatment Photosensitiser
bleachingDrug dose Photosensitiser
bleachingInner filter
Margins Re-supply ofnutrients
PDT-inducedlethality
L.B. Rocha et al. / European Journal of Cancer 51 (2015) 1822–1830 1823
in the NIR, where tissues have higher optical penetra-tion depths (d = 2.3 mm at 750 nm) [2], increase thetreatment depth. Excited photosensitiser moleculestransfer energy or electrons to oxygen leading to singletoxygen or hydroxyl radicals [3,4], respectively, that trig-ger various biological mechanisms (vascular shutdown,[5,6] apoptosis/necrosis of tumour cells [7,8] andimmunogenic cell death [5,9]) eventually leading totumour remission.
Photosensitisers characterised by long plasmahalf-lives, such as temoporfin, t1/2 = 45.4 h, are pre-scribed with drug-to-light intervals (DLIs) of 4–6 days[10,11]. Long exposure to temoporfin is associated withhigh tumour selectivity but prolonged skin photosensi-tivity. The period of photosensitivity is reduced usingverteporfin (t1/2 = 5–6 h) [12]. Verteporfin first used inage-related macular degeneration (ARMD) is currentlyin clinical trials on pancreatic cancer [13]. Verteporfinis irradiated at DLI = 15 min in ARMD or 60–90 minin pancreatic cancer treatments. Table 1 presents thisand other factors that contribute to the treatment out-come. Finding the best combination of drug dose, lightdose, DLI, radiant exposure R, irradiance E and tumourmargin is crucial for primary tumour destruction.Additionally the PDT protocol may determine antitu-mour immune responses [14]. Thus, the success ofPDT depends on the development of photosensitisersand treatment regimens.
We recently described a photostable bacteriochlorin(redaporfin) with intense infrared absorption, high yieldof ROS generation, high phototoxicity [15], low skinphotosensitivity and favourable pharmacokinetics[16,17]. This work uncovers relationships betweenPDT regimens, cure rates, antitumour immunememory and resistance to metastasis using redaporfin.Our results supported to regulatory approval toconduct a phase I/II clinical study of redaporfin(ClinicalTrials.gov identifier: NCT02070432).
2. Materials and methods
2.1. Chemicals and Cells
Bacteriochlorin (F2BMet or redaporfin) was recentlydescribed [15]. CT26 colon carcinoma cells lead to sub-cutaneous tumours in BALB/c mice that are consideredminimally to moderately immunogenic tumours [18].Female 8–10 week old mice (17–22 g) were organisedin groups as shown in Table 2. Details on drugformulation, cell cultures and mice are presented inSupplementary Materials.
2.2. Antitumour immune memory
Mice cured with the optimised PDT protocol weresubcutaneously rechallenged with 350,000 CT26 cells
in the contralateral thigh more than 90 days after thetreatment. An age-matched group of BALB/c mice withCT26 tumours was subjected to surgery. The mice thatafter the surgery remained tumour free >90 days andan age-matched control group of naive BALB/c micewere inoculated with 350,000 CT26 cells.
2.3. Lung metastasis
BALB/c mice were subcutaneously inoculated with350,000 CT26 cells and 7 days later 500.000 CT26 cellswere injected in the tail vein. On day 12, one group withsubcutaneous tumours was submitted to the optimisedPDT regimen, and 11 days later all the mice were sacri-ficed, the lungs were harvested, fixed with Bouin’s solu-tion, weighted and the metastases were counted by tworesearchers.
2.4. Immunohistochemistry
Four micrometer paraffin slices from tumours weredeparanized and hydrated. Antigen retrieval was donein 0.1 M citrate buffer upon microwave treatment.Samples were blocked with 10% goat serum and incu-bated, overnight at 4 �C, with a CD3 antibody (Dako).After washing, sections were incubated withanti-rabbit EnVision + System-HRP Labelled Polymer(Dako), revealed with 3,30-diaminobenzidine (DAB),counterstained with Harris’ Haematoxylin and exam-ined by light microscopy.
3. Results
3.1. Intermediate DLI have low phototherapeutic indexes
Table 2 reveals that the protocol parameters testedfor vascular-PDT (DLI = 0.25 h) covered observationsranging from the absence of cures to 100%PDT-induced lethality. High light doses (>70 J) associ-ated with large drug doses (P0.75 mg/kg) delivered tolarge areas (>1 cm2) led to lethality within the two daysafter treatment. For comparable doses (1.5 mg/kg, 78 or95 J), PDT-induced lethality and efficacy decreased as

Table 2Pilot studies of photodynamic therapy (PDT) regimes with redaporfin, exploring drug-to-light intervals, drug and light doses, tumour margins and laser fluence (or radiant exposure), using N mice ineach group.
Group Drug-to-light interval(DLI)(h)
Drug dose(mg/kg)
Laser power(mW)
Light dose (J) Diameter (cm) Radiantexposure (J/cm2)
N Survivals Cured Efficacy (%)
C NA 0.0 0 0 NA 6 6 0 0C + L NA 0.0 130 179 Manual 7 7 0 01 0.25 0.37 130 31 1.4 20 10 10 1 102 0.25 0.37 130 44 1.2 39 6 6 0 03 0.25 0.37 130 78 Manual 6 6 3 504 0.25 0.37 65 78 Manual 4 4 1 255 0.25 0.52 130 44 1.2 39 6 6 0 06 0.25 0.52 185 63 1.2 56 7 7 2 297 0.25 0.52 130 78 1.2 69 7 7 2 298 0.25 0.75 130 47 Manual 6 6 5 839 0.25 0.75 130 59 Manual 6 6 5 8310 0.25 0.75 130 44 1.2 39 7 7 2 2911 0.25 0.75 130 60 1.2 53 7 7 4 5712 0.25 0.75 130 �73 1.1 74 19 19 10 5313a 0.25 0.75 173 67 1.3 50 8 8 7 88
13b 0.25 0.75 173 67 1.3 50 6 6 5 83
14 0.25 0.75 185 75 1.4 49 4 2 215 0.25 0.75 185 81 1.4 53 6 4 416 0.25 0.75 173 85 1.4 50 7 6 417 0.25 1.5 130 47 Manual 6 5 218 0.25 1.5 130 59 Manual 8 6 619 0.25 1.5 130 78 Manual 6 1 020 0.25 1.5 130 117 Manual 6 0 021 12 0.75 65 59 Manual 5 5 0 022 12 1.5 130 59 Manual 6 1 023 12 1.5 130 94 Manual 6 1 024 24 1.5 130 94 Manual 9 4 025 48 1.5 130 94 Manual 6 5 026 72 1.5 130 94 Manual 6 6 1 1727 72 2.2 130 94 Manual 6 6 0 028 72 1.5 130 119 1.2 105 9 7 029 72 1.5 130 140 Manual 6 5 1
1824L
.B.
Ro
cha
eta
l./Eu
rop
ean
Jo
urn
al
of
Ca
ncer
51
(2
01
5)
18
22
–1
83
0

L.B. Rocha et al. / European Journal of Cancer 51 (2015) 1822–1830 1825
the DLI increased, which is related with the photosensi-tiser clearance. Although the concentration of reda-porfin in the tumour equals that in the plasma atDLI = 12 h [16], this did not improve PDT efficacy.The therapeutic index of the regimes using DLI = 12,24 and 48 h is narrow, with no cures and lethality. Itis again possible to obtain cures without lethality for adrug dose of 1.5 mg/kg when DLI is increased to 72 h,although this bears a high safety risk.
3.2. Factors that improve PDT outcome
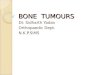
Increasing the irradiance from 65 to 130 mW/cm2 ingroups 3 and 4 (0.37 mg/kg, 78 J) increased efficacyfrom 25% to 50%. The difference between these groupsis not statistically significant but the lower efficacy atlower irradiances suggests that oxygen depletion in thetissues is not a limiting factor in vascular-PDT. The irra-diance was not increased above 164 mW/cm2 (group 6)to avoid photothermal effects. PDT efficacy did notrespond to the increased light dose in groups 1 and 2(0.37 mg/kg, 31 or 44 J) or in groups 6 and 7(0.52 mg/kg, 63 and 78 J) suggesting that photobleach-ing becomes a limiting factor for 0.37 mg/kg with lightdoses >35 J and for 0.52 mg/kg with light doses >60 J.The groups 10 and 11, with DLI = 0.25 h and0.75 mg/kg, show a positive response to the light doseincrease (Fig. 1A).
The compensation of a lower photosensitiser dose bya higher light dose indicates that the photosensitiserdose is sufficiently high to be insensitive to photobleach-ing at the light dose used [19]. The median tumour delayafter treatment in groups 27 (2.2 mg/kg, 94 J) and 29(1.5 mg/kg, 140 J) at DLI = 72 h and the unchangedPDT efficacy in groups 6 (0.52 mg/kg, 63 J) and 10(0.75 mg/kg, 44 J) at DLI = 0.25 h insures that photo-bleaching is not a limiting factor at these dose ranges.Thus, the full potential of vascular-PDT is attained fora drug dose of 0.75 mg/kg and a radiant exposure of50 J/cm2.
Fig. 1. Kaplan–Meier plots for survival times of mice with untreated tuPhotobleaching is an efficacy-limiting factor for PS dosages lower than 0.75tumour margin in long-term PDT efficacy.
The evaluation of inner filter effects, where the photo-sensitiser concentration is sufficiently high to compro-mise the light penetration depth and PDT efficacy, isobscured by the onset of lethality at high drug dosesin groups 17–20.
Fig. 1B shows that for a 0.75 mg/kg dose and a51 ± 2 J/cm2 radiant exposure, the PDT-efficacyincreases with the tumour margin. The onsetPDT-induced lethality for an illuminated fieldP1.5 cm2 limits the success of this protocol. Group 13corresponds to the optimised protocol for BALB/c micewhere 86% of the mice were cured after PDT. This pro-tocol was repeated (groups 13a and 13b) with consistentresults.
PDT at DLI = 72 h leads to a small eschar within 72 hof the treatment, and DLI = 0.25 h leads to tissuedestruction, with eschar formation in 48 h. The localresponse to vascular-PDT is very strong, but the animalsmaintained their normal behaviour, and the necroticeschar disappeared and a good cosmetic effect wasobserved. Significantly larger oedemas were observedwith DLIs 0.25 and 12 h than with 72 and 48 h. On theother hand, larger erythemas were observed withDLI = 72 h than 0.25 h. The larger oedemas doubledthe diameter of the mice leg in the vicinity of the tumour.
3.3. Vascular-PDT generates anti-tumour immunity
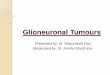
Mice cured with PDT, mice with surgically removedtumours and a control group of naıve animals wereinoculated again three or more months later withCT26 cells into the contralateral thigh. Fig. 2 shows that67% of the mice cured with the optimised PDT protocolrejected the rechallenge with CT26 cells and remainedtumour free for at least 70 days. When the rechallengeresults of all PDT-cured mice are pooled together (43mice), the rate of tumour rejection dropped to 40%.This indicates that the optimised protocol is especiallyeffective in stimulating the immune system, presumablybecause it leads to a very strong local reaction.
mours or after photodynamic therapy (PDT) at DLI = 0.25 h. (A)mg/kg when combined with light doses higher than 60 J. (B) Effect of

Fig. 2. Kaplan–Meier plots. (A). Survival times of BALB/c mice after rechallenge with CT26 cells of mice cured with vascular-photodynamictherapy (V-PDT) (0.75 mg/kg, drug-to-light interval (DLI) = 0.25 h, 50 J/cm2, 130 mW/cm2, / 13 mm) or cured by surgical removal of the CT26tumour, compared with a group of naive animals with the same age, never exposed to such tumour cells; log-rank test for PDT cured vs. naıve:p = 0.0005. PDT cured vs. surgery cured: p = 0.0031. (B). Survival times of BALB/c nude mice with untreated tumours (control) or after vascular-PDT (0.75 mg/kg, DLI = 0.25 h, 50 J/cm2, 130 mW/cm2, / 13 mm); log-rank test for naıve PDT treated vs. naıve control: p = 0.0006. (C).Photographs of typical local reactions at 24 and 96 h after PDT.
1826 L.B. Rocha et al. / European Journal of Cancer 51 (2015) 1822–1830
To test the hypothesis that T cells mediated the adap-tive immune response, we performed the optimisedredaporfin-PDT protocol in BALB/c nude mice. Fig. 2shows that the cure rate dropped from 86% to zero whenchanging to nude mice. Moreover, the oedema andeschar after the treatment of the normal mice are muchlarger than in the nude mice. The difference between nor-mal and nude mice unveils the role played by the stimu-lation of the adaptive immune system, and of thepresence of functional T cells, in long-term PDT efficacy.
3.4. Systemic anti-tumour protection against metastasis
The systemic anti-tumour protection after PDT wasfurther assessed combining subcutaneous and intra-venous injection of CT26 cells. The subcutaneoustumour was induced as in the other experiments andafter 7 days, 500,000 CT26 cells were injected in the tailvein. The subcutaneous tumour develops, while the cellsinjected produce lung metastasis. The observation ofdeaths in the control group 23 days after inoculation,due to the lung metastasis, dictated the end of the exper-iment at that point, and the animals treated with theoptimised PDT regimen were sacrificed 12 days afterinoculation. The treatment regimen and its outcomeare presented in Fig. 3. Necropsies revealed multipletumour foci in the lungs of control mice but two ofthe seven treated animals were free of lung metastasisat the time of the sacrifice. Two-tail unpaired t-test gavean extremely statistically significant difference betweentreated and control groups.
3.5. Recruitment of lymphocytes
CD3+ is a general T-lymphocyte marker and its infil-tration in tumours is associated with a positive effect on
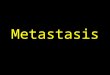
survival [20]. Fig. 4 shows that CD3+ cells wereobserved in untreated tumours, which evidenced thechronic inflammatory status typical of cancer. Six hoursafter tumour irradiation, these cells were almost com-pletely absent of the tumour mass, presumably due tothe treatment. This effect might be beneficial as theseT cells are commonly immunosupressor T regulatorycells. In contrast, 24 h post-treatment, CD3+ cells sig-nificantly increased, reaching levels superior to the onesobserved in untreated tumours. This T cell infiltrationmay be mediated by the signals emitted by the tumourcells killed by PDT, which recruit lymphocytes fromthe blood stream into the tumour with especially inci-dence to the tumour periphery. Such infiltrations havebeen observed in studies with vascular PDT [21].
4. Discussion
Various authors reported systemic PDT-inducedanti-tumour immune responses [22–25], including casesof vascular-PDT of BALB/c mice bearing CT26tumours when verteporfin [26] orPd-bacteriopheophorbide WST11 [21] were used.However, PDT with verteporfin failed to cure in micebearing wild-type CT26 tumours. Only mice withCT26.CL25 tumours expressing the tumour antigenb-galactosidase could be cured and acquired immunememory [26]. Cures in BALB/c mice bearing CT26tumours with verteporfin-PDT required the preliminaryadministration of cyclophosphamide, an anti-cancerdrug that selectively depletes Treg cells in mice, and thiscombination produces a greater local oedema than PDTalone [27]. Vascular-PDT with WST11 resulted in cureof 70% BALB/c and 19% BALB/c nude mice withimplanted CT26 tumours [21]. The cured mice chal-lenged two weeks later with injection of CT26 cells

Fig. 3. Impact of vascular-photodynamic therapy (PDT) (0.75 mg/kg, drug-to-light interval (DLI)= 0.25 h, 50 J/cm2, 130 mW/cm2, / 13 mm) ondistant metastasis evaluated in terms of the number of lung metastasis and weight of the lungs. The photographs show the lungs stained withBouin’s solution in control and PDT-treated groups.
L.B. Rocha et al. / European Journal of Cancer 51 (2015) 1822–1830 1827
resisted the development of lung metastases, which wereobserved in control mice.
The optimised redaporfin-PDT regimen (0.75 mg/kg,0.25 h, 50 J/cm2, 130 mW/cm2, / 13 mm), that emergedfrom our studies cured 12 out of 14 mice in two indepen-dent experiments. The overall cure rate of 86% is partic-ularly remarkable because CT26 were the most resistantcells in vitro [15]. The antitumour immune memory ofmice cured with the optimised PDT regimen was com-pared with that of an age-matched group cured by sur-gery. All the mice in the surgery groups developedtumours when rechallenged with CT26 cells in the con-tralateral thigh, whereas 67% of the mice treated withthe optimised redaporfin-PDT regime remainedtumour-free more than 70 days later. This unprece-dented immune memory with a minimally to moderatelyimmunogenic tumour model reveals that the optimised
treatment regimen was effective in the stimulation theimmune system.
The systemic response was further explored in apseudo-metastatic model. Fig. 3 shows that PDT ofestablished tumours controlled lung metastasis resultingfrom CT26 cells’ injection five days before the treatment.The photographs of the lungs illustrate thatvascular-PDT with redaporfin is an effectivephotodynamic-immunotherapy. The drop in cure ratesfrom normal to nude BALB/c mice, from 86% to 0%,together with the T cell infiltration in the tumour massillustrated in Fig. 4 strongly suggested that our opti-mised protocol activates T cell adaptive immunity. Theprotocol optimised for redaporfin elicits an immuneresponse against CT26 tumours that is only paralleledby other photosensitisers when strongly immunogenicmodels are used [23].

Fig. 4. T cells (CD3+) infiltration into CT26 sc tumours. Images of two sections (distance of �600 lm) of a representative tumour from eachgroup: control, 6 and 24 h post treatment. T cells (CD3+) can be visualised in brown (10� magnification) while the nuclei of tumour cells are inblue. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
1828 L.B. Rocha et al. / European Journal of Cancer 51 (2015) 1822–1830
Vascular-PDT with redaporfin led to a large oedemaand eschar formation, mounted a high local inflamma-tion and was very efficient in controlling the primarytumour and protecting from tumour rechallenges. Thisagrees with expected relation between high inflamma-tion and durable immune responses but challenges theview that high-inflammation PDT regimens are less effi-cient in primary tumour control than low-inflammationPDT regimes [14,28]. For the tumours with thicknessesof 3–4 mm used in this study, the 3–4 mm margin shouldbe associated with an irradiance at a depth z = 7 mmcapable of producing ROS above the therapeuticthreshold.
The threshold concentration for tissue necrosis bysinglet oxygen was estimated as [1O2] = 0.9 mM fromthe necrosis of rat liver with Photofrin [29]. The estimateof the [1O2] threshold for skin necrosis is substantiallyhigher, 93 mM, because of the lack of sensitivity of nor-mal epidermal cells to PDT [30]. According to theAAPM, a typical threshold dose for necrosis is 17 mMand the amount of ROS produced per unit volume oftissue is given by [31]:
½ROS� ¼ UROSð1000k=hcN AÞRe½F2BMet�local
¼ 460R½F2BMet�local ð1Þ
where R = tirrE is the radiant exposure in J/cm2 and thenumeric value results from the use of the parameters ofredaporfin (F2BMet). The Supplementary Material pre-sents calculations on [F2BMet] and [ROS]. AtDLI = 0.25 h we have [F2BMet]plasma = 13 lM for a0.75 mg/kg drug dose and [ROS] = 0.3 M at the tumoursurface when R0 = 50 J/cm2. At a depth of z = 7 mm,where R = R0exp(�z/d), for the optimised regimen withillumination at 750 nm we obtain [ROS] = 14 mM,which should produce tissue necrosis. Thus, the
success of the optimised regimen is related with thethree-dimensional tumour margin of 3–4 mm.
Gomer reported a tumour margin of 1–2 mm forPDT and a resection margin of 4 mm in surgical excisionof the same tumours [32], whereas Hamblin used tumourmargins of 2–3 mm [33–34]. Increasing the illuminatedsurface may improve the PDT outcome. This dependson d from Eq. (1) and on the photosensitiser photode-composition. The drug-light dose compensationobserved in the range of the values of the optimised pro-tocol shows that the F2BMet photodecompostion doesnot limit the depth of the treatment under theseconditions.
Hypoxia in tissues during PDT may also diminish theamount of ROS produced. Indeed, high irradiances curbthe median survival time of mice bearing tumours whenthe photosensitiser is predominately localised in thetumour cells (DLI > 6 h) [35–37], although exceptionswere observed [38,39]. A study using 10 mg/kg of motex-afin lutetium irradiated at DLI = 3 h concluded that theoutcome of the treatment was not related with the oxy-genation [40]. The abundance of oxygen in the vascula-ture, the long-lived triplet state of redaporfin and itsparticipation in Type I reactions, circumvent oxygendepletion effects in vascular-PDT even at the highestirradiance tested (E = 164 mW/cm2). The higher irradi-ances in vascular-PDT even improved the outcome ofthe therapy, because they produce an acute vascularresponse at a greater tumour depth and enable stronghypoxia after PDT, which is correlated with PDT effi-cacy [6].
The protocols with DLI between 12 and 48 h have anarrow phototherapeutic index that is related with phar-macokinetics because �80% of redaporfin is clearedfrom the plasma within 12 h post-iv administration[16]. PDT with DLI = 72 h (1.5 mg/kg, 100 J/cm2) isthe most selective, but considering that the final goal

L.B. Rocha et al. / European Journal of Cancer 51 (2015) 1822–1830 1829
must be eliciting a favourable long-term tumourresponse, vascular-PDT (0.75 mg/kg, DLI = 0.25 h,50 J/cm2, tumour margin of 4 mm) is preferable becauseit provides the highest cure rates and long-lasting sys-temic anti-tumour immunity.
5. Conclusion
The PDT regimen optimised with redaporfin combi-nes local oxidative stress in the target tissue capable ofeliminating the primary tumour, with a systemicimmune response that controls metastasis. The successof the treatment is related with the three-dimensionalmargin >3 mm and with the strong immune responsetriggered by the high local inflammation after PDT, evi-denced by the recruitment of lymphocytes. The clinicalimplications of this study are currently being exploredin a Phase I/II clinical trial with F2BMet (redaporfin)using an adaptation of the optimised regimen.
Grant support
This work was funded by National ScienceCentre – Poland (DEC-2013/11/D/ST5/02995)and FCT – Portugal (PEst-OE/QUI/UI0313/2014,PTDC/QUI-QUI/120182/2010), QREN/5356. LCGdSthanks FCT for a scholarship (SFRH/BPD/93562/2013).
Conflict of interest statement
Luzitin SA sponsors PhD studies of LBR. LGA isinventor of patents licenced to Luzitin SA.
Acknowledgements
We appreciate the technical assistance of AnaCatarina Lobo and the surgery training provided byDiogo Cabrita MD.
Appendix A. Supplementary data
Supplementary data associated with this article canbe found, in the online version, at http://dx.doi.org/10.1016/j.ejca.2015.06.002.
References
[1] Agostinis P, Berg K, Cengel KA, Foster TH, Girotti AW,Golinick SO, et al. Photodynamic therapy of cancer: an update.CA Cancer J Clin 2011;61:250–81.
[2] Bashkatov AN, Genina EA, Kochubey VI, Tuchin VV. Opticalproperties of human skin, subcutaneous and mucous tissues in thewavelength range from 400 to 2000 nm. J Phys D Appl Phys2005;38:2543–55.
[3] Silva EFF, Schaberle FA, Monteiro CJP, Dabrowski JM, ArnautLG. The challenging combination of intense fluorescence andhigh singlet oxygen quantum yield in photostable chlorins – acontribution to theranostics. Photochem Photobiol Sci2013;12:1187–92.
[4] Arnaut LG. Design of porphyrin-based photosensitizers. AdvInorg Chem 2011;63:187–233.
[5] Preise D, Scherz A, Salomon Y. Antitumor immunity promotedby vascular occluding therapy: Lessons from vascular-targetedphotodynamic therapy (VTP). Photochem Photobiol Sci2011;10:681–8.
[6] Krzykawska-Serda M, Dabrowski JM, Arnaut LG, Szczygieł M,Urbanska K, Stochel G, et al. The role of strong hypoxia intumors after treatment in the outcome of bacteriochlorin-basedphotodynamic therapy (PDT). Free Radic Biol Med2014;73:239–51.
[7] Castano AP, Demidowa TN, Hamblin MR. Mechanisms inphotodynamic therapy: Part one – photosensitisers, photochem-istry and cellular localization. Photodiagn Photodyn Ther2004;1:279–93.
[8] Zhao H, Xing D, Chen Q. New insights of mitochondria reactivespecies generation and cell apoptosis induced by low dosephotodynamic therapy. Eur J Cancer 2011;47:2750–61.
[9] Castano AP, Mroz P, Hamblin MR. Photodynamic therapy andanti-tumour immunity. Nat Rev Cancer 2006;6:535–45.
[10] Peng Q, Moan J, Ma LW, Nesland LM. Uptake, localization, andphotodynamic effect of meso-tetra(hydroxyphenyl)porphine andits corresponding chlorin in normal and tumor tissues of micebearing mammary carcinoma. Cancer Res 1995;110:1698–704.
[11] Andrejevic-Blant S, Hadjur C, Ballini J-P, Wagnieres G,Fontolliet C, van den Berg H, et al. Photodynamic therapy ofearly squamous cell carcinoma with tetra(m-hydroxyphenyl)chlo-rin: optimal drug-light interval. Br J Cancer 1997;76:1021–8.
[12] Houle J-M, Strong A. Clinical pharmacokinetics of verteporfin. JClin Pharmacol 2002;42:547–57.
[13] Huggett MT, Jermyn M, Gillams A, Illing R, Mosse S, Novelli M,et al. Phase I/II study of verteporfin photodynamic therapy inlocally advanced pancreatic cancer. Br J Cancer 2014;110:1698–704.
[14] Kousis PC, Henderson BW, Maier PG, Gollnick S.Photodynamic therapy enhancement of antitumor immunity isregulated by neutrophils. Cancer Res 2007;67:10501–10.
[15] Arnaut LG, Pereira MM, Dabrowski JM, Silva EFF, SchaberleFA, Abreu AR, et al. Photodynamic therapy efficacy enhanced bydynamics: the role of charge transfer and photostability in theselection of photosensitizers. Chem Eur J 2014;20:5346–57.
[16] Saavedra R, Rocha LB, Dabrowski JM, Arnaut LG. Modulationof biodistribution, pharmacokinetics and photosensitivity withthe delivery vehicle of a bacteriochlorin photosensitizer forphotodynamic therapy. ChemMedChem 2014;9:390–8.
[17] Krzykawska M, Dabrowski JM, Szczygiel M, Stochel G, ArnautLG, Pereira MM, et al. Non-invasive prognostic tools forphototherapeutic response in murine tumors. Eur J Cancer2012;48:S193.
[18] Agrawal N, Bettegowada C, Cheong I, Geschwind J-F, DrakeCG, Hipkiss EL, et al. Bacteriolytic therapy can generate a potentimmune response against experimental tumors. Proc Natl AcadSci U S A 2004;101:15172–7.
[19] Fingar VH, Henderson B. Drug and light dose dependence ofphotodynamic therapy: a study of tumor and normal tissueresponse. Photochem Photobiol 1987;46:837–41.
[20] Gooden MJM, de Bock GH, Leffers N, Daemen T, Nijman HW.The prognostic influence of tumour-infiltrating lymphocytes incancer: a systematic review with meta-analysis. Br J Cancer2011;105:93–103.
[21] Preise D, Oren R, Glinert I, Kalchenko V, Jung S, Scherz A, et al.Systemic antitumor protection by vascular-targeted photody-namic therapy involves cellular and humural immunity. CancerImmunol Immunother 2009;58:71–84.
[22] Wachowska M, Gabrysiak M, Muchowicz A, Bednarek W,Barankiewicz J, Rygiel T, et al. 5-Aza-20-deoxycytidine potenti-ates antitumour immune response induced by photodynamictherapy. Eur J Cancer 2014;50:1370–81.

1830 L.B. Rocha et al. / European Journal of Cancer 51 (2015) 1822–1830
[23] Kabingu E, Vaughan LA, Owczarczak B, Ramsey KD, GollnickSO. CD8+ T cell-mediated control of distant tumoursfollowing local photodynamic therapy in independent of CD4+T cells and dependent on natural killer cells. Br J Cancer2007;96:1839–48.
[24] Korbelik M, Cecic I, Merchant S, Sun J. Acute phase responseinduction by cancer treatment with photodynamic therapy. Int JCancer 2008;122:1411–7.
[25] Schreiber S, Gross S, Brandis A, Harmelin A, Rosenbach-BelkinV, Scherz A, et al. Local photodynamic therapy (PDT) of rat C6glioma xenografts with Pd-Bacteriopheophorbide leads todecreased metastases and increase of animal cure compared withsurgery. Int J Cancer 2002;99:279–85.
[26] Mroz P, Szokalska A, Wu MX, Hamblin MR. Photodynamictherapy of tumors can lead to development of systemicantigen-specific immune response. PLoS One 2010;5, e15194–05.
[27] Reginato E, Mroz P, Chung H, Kawakubo M, Wolf P, HamblinMR. Photodynamic therapy plus regulatory T-cell depletionproduces immunity against a mouse tumour that expresses a self-antigen. Br J Cancer 2013;109:2167–74.
[28] Henderson BW, Gollnick SO, Snyder JW, Busch TM, Kousis PC,Cheney RT, et al. Choice of oxygen-conserving treatmentregimen determines the inflammatory response andoutcome of photodynamic therapy of tumors. Cancer Res2004;64:2120–6.
[29] Farrel TJ, Wilson BC, Patterson MS, Chow R. Dependence ofphotodynamic threshold dose on treatment parameters in normalrat liver in vivo. Proc SPIE 1991;1426:146–55.
[30] Niedre MJ, Secord AJ, Patterson MS, Wilson BC. In vitro tests ofthe validity of singlet oxygen luminescence measurements as adose metric in photodynamic therapy. Cancer Res 2003;63:7986–94.
[31] AAPM, Photodynamic Therapy Dosimetry. AmericanAssociation of Physicists in Medicine, 2005.
[32] Gomer CJ, Ferrario A, Murphree AL. The effect of localizedporphyrin photodynamic therapy on the induction of tumormetastasis. Br J Cancer 1987;56:27–32.
[33] Castano AP, Mroz P, Wu MX, Hamblin MR. Photodynamictherapy plus low-dose cyclophosphamide generates antitumorimmunity in a mouse model. Proc Natl Acad Sci U S A2008;105:5495–500.
[34] Mroz P, Vatansever F, Muchowicz A, Hamblin MR.Photodynamic therapy of murine mastocytoma induces specificimmune responses against the cancer/testis antigen P1A. CancerRes 2013;73:6462–70.
[35] Coutier S, Bezdetnaya L, Foster TH, Parache R-M, Guillemin F.Effect of irradiation fluence rate on the efficacy of photodynamictherapy and tumor oxygenation in meta-tetra (hydroxyphenyl)chlorin (mTHPC)-sensitized HT29 xenografs in nude mice.Radiat Res 2002;158:339–45.
[36] Gibson SL, VanDerMeid KR, Murant RS, Raubertas RF, HilfR. Effects of various photoradiation regimens on the antitumorefficacy of photodynamic therapy for R3230AC mammarycarcinomas. Cancer Res 1990;50:7236–41.
[37] Henderson BW, Busch TM, Snyder JW. Fluence rate as amodulator of PDT mechanisms. Lasers Surg Med2006;38:489–93.
[38] Busch TM, Xing X, Yu G, Yodh A, Wileyto EP, Wang H-W,et al. Fluence-rate dependent intramolecular heterogeneity inphysiologic and cytotoxic responses to Photofrin photodynamictherapy. Photochem Photobiol Sci 2009;8:1683–93.
[39] Wang H-W, Rickter E, Yuan M, Wileyto EP, Glatstein E, YodhA, et al. Effect of photosensitizer dose on fluence rate responses tophotodynamic therapy. Photochem Photobiol 2007;83:1–9.
[40] Busch TM, Wang H-W, Wileyto EP, Yu G, Bunte RM.Increasing damage to tumor blood vessels during motexafinlutetium-PDT through use of low fluence rate. Radiat Res2010;174:331–40.