Embed Size (px)
Citation preview

Copyright © 2007 John Wiley & Sons, Ltd. Biomed. Chromatogr. 22: 301–305 (2008)DOI: 10.1002/bmc
Elevation of anions in exercise-induced acidosis 301ORIGINAL RESEARCHORIGINAL RESEARCH
Copyright © 2007 John Wiley & Sons, Ltd.
BIOMEDICAL CHROMATOGRAPHYBiomed. Chromatogr. 22: 301–305 (2008)Published online 15 October 2007 in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/bmc.930
Elevation of anions in exercise-induced acidosis: a studyby ion-exchange chromatography/mass spectrometry
William McKinnon,1 C. Pentecost,2 Gwyn A. Lord,3* Lui G. Forni,4 Jean-Marie Peron5 and Philip J. Hilton1
1Renal Laboratory, St Thomas’s Hospital, London SE1 7EH, UK2Dorothea Lead, Guy’s, King’s & St Thomas’s School of Medicine, London SE1 7EH, UK3MRC Bioanalytical Science Group, Birkbeck, University of London, London WC1E 7HX, UK4Department of Critical Care, Worthing Hospital, Worthing, West Sussex BN11 2DH and Brighton & Sussex Medical School, University of Sussex,
Brighton, East Sussex BN1 9PX, UK5Department of Chemistry, Kingston University, Surrey KT1 2EE, UK
Received 10 May 2007; revised 7 August 2007; accepted 8 August 2007
ABSTRACT: Acidosis is a major factor that determines the upper limit of exercise endurance. We have previously shown thatanions usually associated with intermediary metabolism are elevated in critically ill patients with metabolic acidosis and contributesignificantly to acidosis generation. This study was to determine whether volunteers with normal metabolism would exhibit similarelevations in anions associated with intermediate metabolism when exposed to a short-term physiological stress leading to a brieflactic acidosis. Physiological stress was induced on five healthy male subjects by means of a ramped exercise protocol. Blood wasobtained immediately prior to and post-exercise, plasma ultrafiltrate was prepared and analysed immediately both by enzymeassay and liquid chromatography coupled to electrospray–mass spectrometry (LC/ESI-MS). Metabolic acidosis concomitant witha significant increase in blood lactate occurred in each subject, but in addition, anions normally associated with intermediatemetabolism were significantly elevated after exercise. The contribution of these anions to generating an acidosis, and thus poten-tially limiting the extent of exercise, has never been acknowledged. Copyright © 2007 John Wiley & Sons, Ltd.
KEYWORDS: exercise; acidosis; Krebs cycle; ion-exchange; LC/ESI-MS
INTRODUCTION
It is widely acknowledged that an increase in mech-anical load past the anaerobic threshold results in anincreased lactic acid generation as oxygen demand bythe muscle exceeds supply and the muscle cells switchto anaerobic respiration to maintain function. As theconcentration of lactic acid increases it results in aglobal lactic acidosis. This is associated with a fall inblood pH and results in compensatory hyperventilation(Wasserman et al., 1973; Beaver et al., 1986; Meyeret al., 2004). The generation of this acidosis has longbeen associated with skeletal muscle fatigue (Lawleret al., 1997) and thus limits the extent of the exercisethat can be endured by the athlete.
In a similar manner, patients who have undergonephysiological insult that results in a compromisedcirculation commonly show lactic acidosis as a result oftissue under-perfusion (Mizock and Falk, 1992; Cohen
and Woods, 1993). However, in these critically illpatients the anion gap calculated from the contributionof the lactate concentration alone is often significantlyless than that measured, suggesting that other endo-genous anions may also play some part in the generationof the acidosis (Mecher et al., 1991; Rackow et al., 1990;Kaplan et al., 2004; Dondorp et al., 2004). Indeed, manystudies on critically ill patients have demonstrated thepresence of such ‘unmeasured anions’ but until recentlylittle was known as to their identity (Forni et al., 2005).We have previously demonstrated that, in critically illpatients with metabolic acidosis, there is a significantincrease in the anions normally associated with inter-mediary metabolism. In total, these anions contributesignificantly to the observed anion gap (Forni et al.,2005). Given this novel finding we decided to see if theelevation of such anions also occurred in subjects withnormal metabolism undergoing lactic acidosis inducedby physiological stress.
EXPERIMENTAL
This study was approved by the ethics committee of Guy’s &St Thomas’s NHS Trust (reference no. EC03/104). Prior to
*Correspondence to: G. A. Lord, MRC Bioanalytical Science Group,Birkbeck, University of London, London, WC1E 7HX, UK.E-mail: [email protected]
Abbreviations used: ECG, electro-cardiogram; RER, respiratoryexchange ratio.
Contract/grant sponsor: The Special Trustees of St Thomas’ Hospital.

Copyright © 2007 John Wiley & Sons, Ltd. Biomed. Chromatogr. 22: 301–305 (2008)DOI: 10.1002/bmc
302 W. McKinnon et al.ORIGINAL RESEARCH
blood samples being obtained, written informed consent wasobtained from the subject.
Subjects and general design. Five healthy subjects (meanage 45 ± 11.9 years) were asked to complete a Par-Q form toidentify contraindications to exercising. Once cleared, 15 mLof venous blood was obtained from the antecubital vein ofa supine subject at rest. The blood sample was drawn into anunheparinized syringe before 14 mL was transferred rapidlyinto SST II (Kodak) Vaccutainers (BD Vaccutainer SystemsLtd, Plymouth, UK). The sample was immediately chilledand transported rapidly to the laboratory. The plasma wasisolated by centrifugation of the Vaccutainers at 1500g at 4°Cfor 10 min. The plasma was transferred to an Amicon 30 kDafilter (Millipore, Herts, UK) where centrifugation at 2500gfor 15 min produced ultrafiltrate. The generated ultrafiltratewas analysed immediately by both liquid chromatographycoupled to mass spectrometery (LC/ESI-MS) and by enzymaticdetermination with reference to internal standards (Forniet al., 2005; McKinnon et al., 2006). The remaining 1 mL ofblood was introduced to a blood gas analyser (Instrumenta-tion Laboratories) in order to determine the pH, pCO2,serum bicarbonate, base deficit and lactate concentration. Anidentical protocol was performed to obtain the blood sampleimmediately post-exercise.
Exercise testing. Resting heart rate was recorded prior toexercise. Participants were then subjected to physiologicalstress by means of an electronically braked bicycle ergonometer(Lode, Excaliber Sport, Groningen, Nederlands). Exercisecommenced for 5 min at 65% max heart rate as a warm up.Wattage was then increased in 60 W increments every 2 minuntil the patient was exercising at 95% of their predictedmaximum heart rate as calculated using the Karvonianmethod. The heart rate was then maintained at 95% of thesubjects’ maximal value by making minor adjustments to theresistance on the bicycle flywheel. Participants were asked torate their perceived exertion using Borg’s 6–20 scale and allpatients rated their exertion to be between 17 and 20 duringthe latter part of the physiological load. Subjects typicallyendured this maximal load for a period ranging between2 and 5 min. Respiratory exchange ratio (RER) was observedat 1.25 at the end for each patient. The participants’ electro-cardiograms (ECG) were monitored throughout.
Enzyme assay. Enzyme assay with reference to internalstandards gave a reliable and quantitative estimation of theconcentrations of anions present in the plasma ultrafiltratepre- and post-exercise. The enzymatic determination of plasmaultrafiltrate concentrations of citrate, malate, D- and L-lactateanions were estimated using commercially available kits (Roche,Glasgow, UK). The levels of the isocitrate and α-ketoglutaratewere measured using enzyme assays developed in-house usingisocitrate dehydrogenase and α-ketoglutarate dehydrogenaserespectively and their associated co-factors in a 150 mM MOPSbuffer at pH 7.4 (Sigma Chemicals, Poole, UK). Briefly thelevels of isocitrate and α-ketoglutaric acids were determinedas follows.
Isocitrate: to 1 mL of MOPS buffer was added 1.36 mM
MgCl2, 0.226 mM β-NADP and 0.08 U isocitrate dehydro-genase (final concentration). The reaction was commenced by
the addition of 200 μL of plasma ultrafiltrate. α-Ketoglutarate:to 1 mL of MOPS buffer was added 0.23 mM MgCl2, 0.012 mM
CaCl2, 0.35 mM thiamine, 0.14 mM co-enzyme A, 2.3 mM NAD,3 mM cys-HCl and 0.7 U α-ketoglutarate dehydrogenase. Thereaction was commenced by the addition of 200 μL of plasmaultrafiltrate. All the enzymatic assays relied upon the inter-conversion of NAD+ and NADH or NADP+ and NADPHand utilized the change in absorbance due to the reducedco-enzyme at 340 nm. Owing to its short half-life in aqueoussolution, oxaloacetate proved impossible to measure (Tsai,1967).
LC/ESI-MS. Although enzyme assay gave a quantitativevalue for the levels of anions in plasma ultrafiltrate pre- andpost-exercise, the assays were slow and laborious. Applicationof LC-MS gave a rapid qualitative fingerprint that allowedeasy identification of the anions that increased post-exercise.This method is described in detail elsewhere (McKinnonet al., 2006), but briefly 200 μL of plasma ultrafiltrate wasdiluted with 1.8 mL of running buffer (water–HCl at pH 3.2).This material was passed through a 0.22 μm filter and 200 μLof this diluted filtrate was fractionated using an Agilent 1100liquid chromatography system coupled directly to an Agilent1100 mass spectrometer with electrospray ionization operatingin negative ion mode (Agilent Technologies Ltd, Wokingham,Berks, UK). Anion fractionation was attained by use of anAminex HPX-87H ion exclusion column (300 × 7.8 mm,Bio-Rad, Hemel Hempstead, Herts, UK) maintained at aconstant temperature of 31°C. The mobile phase consisted ofa linear ramp from 100% water–HCl pH 3.2 to 50:50 water–HCl pH 2.6 and water–HCl pH 3.2 over 25 min at a flow rateof 0.8 mL/min. Prior to entering the MS the flow was split sothat 92% was voided to waste. The HCl in the mobile phasewas partially neutralized before entering the nebulizer by theinfusion of 10 mM ammonium acetate in 50:50 methanol–water mix at 0.09 mL/h.
Statistics. The data are presented as means ± the standarddeviation. Since all the data were normally distributed apaired t-test was used to determine significance. Data setswere deemed to differ significantly if the resultant p-valuereturned by the t-test was equal to or less than 0.05. If nosignificant difference was present between the data sets this isindicated by ns.
RESULTS
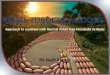
All tests were medically uneventful and no ECGabnormalities were detected in any of the subjectsduring the test. Post-exercise, venous blood gas analysisdemonstrated that blood pH had fallen to 7.15 ± 0.05,whilst the blood bicarbonate concentration had fallento 17.72 ± 2.26. The pCO2 had increased to 6.84 ± 1.44,and the base deficit was 11.40 ± 1.48. The changes ofanions in the plasma ultrafiltrate post-exercise, meas-ured enzymatically, are shown in Table 1. A typicalmass spectrum for selected ions pre- and post-exerciseis shown in Fig. 1.

Copyright © 2007 John Wiley & Sons, Ltd. Biomed. Chromatogr. 22: 301–305 (2008)DOI: 10.1002/bmc
Elevation of anions in exercise-induced acidosis 303ORIGINAL RESEARCH
Table 1. Concentrations of measured anions in plasma pre and post-exercise (mM/L)
Anion Pre-exercise Post-exercise p-Value
Ketoglutarate 0.0153 (±0.008) 0.040 (±0.008) 0.019Citrate 0.183 (±0.038) 0.300 (±0.034) <0.001Malate 0.028 (±0.017) 0.061 (±0.036) 0.024Isocitrate 0.0195 (±0.01) 0.033 (±0.004) 0.02Pyruvic 0.03 (±0.028) 0.17 (±0.07) 0.027Lactate 1.65 (±0.75) 16.0 (±2.43) <0.001
Statistical analysis presented as ± standard deviation.
DISCUSSION
Generation of exercise-induced metabolic acidosisand its association with skeletal muscle fatigue is awell-recognized phenomenon, although the source ofobserved acidosis continues to provoke much debate(Bouhuys et al., 1966; Robergs et al., 2004). Lactic acidis the best known acid produced under conditions ofhypoxia induced by physiological stress and its role inexercise has been well described. Recently, however,the full role of lactate in the generation of acidosis hasbecome controversial, with some authors suggestingthat lactate production may retard, rather than acceler-ate, acidosis and hence be of some physiological benefitin exercise (Tafaletti, 1991).
In the critically ill patient the generation of lacticacidosis is well understood (Cohen and Woods, 1993),
arising from a combination of lactate over-production(as a by-product of tissue hypoxia) coupled to a decreasedrate of lactate removal by the liver, both caused by afailing circulation. In critically ill patients with a lacticacidosis, lactate levels per se are often insufficient toaccount for the extent of the acidosis generated, noris the excess acidosis a result of exogenous agents orfluids administered during resuscitation. The nature ofthe ‘missing’ anions which are responsible for generat-ing the remaining acidosis have been the cause of muchdebate and controversy. Previous work in this labora-tory has shown that anions normally associated withintermediary metabolism are elevated in critically illpatients with lactic acidosis and the results obtainedfrom this preliminary study suggest that these anionsare also significantly elevated after a short period ofexercise. These findings are supported by results from
Figure 1. Before/after exercise changes in some plasma ultrafiltrate anions associated with the Krebs cycle.Three-dimensional offset selected ion chromatograms (M − H)− for (1) pyruvic acid at m/z 87, (2)hydroxybutyric acid at m/z 103, (3) malic acid at m/z 133, (4) α-ketoglutaric acid at m/z 145 and (5) citricacid at m/z 191.

Copyright © 2007 John Wiley & Sons, Ltd. Biomed. Chromatogr. 22: 301–305 (2008)DOI: 10.1002/bmc
304 W. McKinnon et al.ORIGINAL RESEARCH
other authors who have reported that the level ofanions normally associated with intermediate metabo-lism are elevated in exercising muscle (Essen andKaijser, 1978; Gibala et al., 1997). The work presentedin this paper extends this observation to the circulation.Hence, the effect of over-production of these anionsmay result in a global physiological effect and may notjust be localized as previously postulated.
On first glance, it may appear that the contributionto the generation of exercise acidosis made by theseanions usually associated with intermediate metabolismis small. However, once the nature of these anionsis taken into account the contribution they make toacidosis is greater than their molar concentrationssuggest. One must remember that all the anions exam-ined in this study are effectively fully ionized at thepH attained during exercise. Furthermore, it must beremembered that, unlike lactic acid, malic, succinic andα-ketoglutaric acids are dibasic anions and contributetwo protons on ionization whilst citric and isocitric acidare tribasic and will contribute three protons on ioniza-tion. The role of these anions in contributing to thegeneration of acidosis in exercising individuals has notpreviously been reported, thus their potential effect oninfluencing skeletal muscle fatigue has previously neverbeen considered.
We can only speculate as to the ultimate source ofthese anions usually associated with intermediary metabo-lism. They are best known for their role in the Krebscycle, which is essential if oxidative phosphorylation isto occur. However that system is linked at various pointsto other aspects of metabolism such as gluconeogenesis,lipogenesis and amination/deamination of amino acids.For these purposes, the anions must leave the mito-chondria for the cytosol, thereby making them poten-tially more liable to escape into the extracellular fluid.Reactions which increase the levels of components ofthe Krebs cycle are referred to as anaplerotic reactionswhile those that reduce the levels are referred to ascataplerotic. The most important anaplerotic reactionis the deamination of amino-acids to their respectiveketo-acids, for example:
Glutamate → α-ketoglutarate.
It would not be unreasonable to believe that whatis being seen in these exercising individuals and incritically ill patients is an increase in the generationof keto-acids by deamination.
The resting levels of anions normally associatedwith intermediary metabolism are normally tightlyregulated (Lehninger et al., 1993). However, duringexercise the concentrations of these anions have beenshown to be elevated in skeletal muscle (Essen andKaijser, 1978; Gibala et al., 1997). This implies thatduring early exercise anaplerotic reactions exceed thecataplerotic processes, resulting in a net accumulation
of Krebs cycle intermediates. Indeed, studies havedemonstrated that the levels of succinate, malate andfumarate rise significantly within the first minute ofexercise (Gibala et al., 1997). Following exercise, thelevels of anions normally associated with intermediarymetabolism decline.
In the study reported in this paper we used enzymeassays to determine quantitatively acid concentrationspre- and post-exercise. Although enzyme assay givesabsolute values for each anion studied, the assay doeshave the disadvantage of being slow and laborious.However, application of the LC/ESI-MS techniquedescribed in this paper gives an approximate, but rapidprofile of the changes in circulating anion concentra-tions that occur upon exercise. Coupled together, theLC/ESI-MS and enzyme assay provide a powerful tech-nique to investigate global changes in anions normallyassociated with intermediary metabolism under con-ditions of physiological stress. The LC/ESI-MS tech-nique described has the added advantage in that it isflexible and can easily be modified to examine thechanges that occur in other circulating compoundsunder conditions of physiological stress.
Although the concentrations of the anions attainedin the subjects used in this study do not approachthose previously observed in the critically ill, it must beremembered that the subjects in this study enduredexercise at 95% of their cardiac maxima for, at most,5 min. The period of physiological stress experiencedby the critically ill is much greater than that experi-enced by the subjects in our study. Furthermore, theeffect in the critically ill is compounded by a failingcirculation and a concomitant reduction in tissueperfusion, both of which were absent in our subjects.
In conclusion, we have demonstrated the presenceof significantly increased concentrations of anions nor-mally associated with intermediate metabolism in theplasma ultrafiltrate of normal subjects under conditionsof physiological stress induced by exercise. Owing tothe nature of these anions, the contribution they maketo the generation of acidosis is greater than that whichappears on consideration of their molar concentra-tion alone. The role of these anions in generatingexercise-induced acidosis, and thus the role they playin influencing skeletal muscle fatigue, has never beforebeen considered. It would be interesting to extend thework presented in this paper to study the response thatoccurs in athletes undertaking endurance sports to seeif the changes in their anions normally associated withintermediate metabolism attain values similar to thoseobserved in the critically ill.
Acknowledgements
Work in the laboratory at St Thomas’s is sponsored byThe Special Trustees of St Thomas’s Hospital.

Copyright © 2007 John Wiley & Sons, Ltd. Biomed. Chromatogr. 22: 301–305 (2008)DOI: 10.1002/bmc
Elevation of anions in exercise-induced acidosis 305ORIGINAL RESEARCH
REFERENCES
Beaver W, Wasserman K and Whipp B. A new method fordetecting anaerobic threshold by gas exchange. Journal of AppliedPhysiology 1986; 60: 2020–2027.
Bouhuys A, Pool J, Binkhorst RA and Van Leeuwen P. Metabolicacidosis of exercise in healthy males. Journal of Applied Physiology1966; 21: 1040–1046.
Cohen RD and Woods HF. Lactic acidosis revisited. Diabetes 1993;32: 181–191.
Dondorp AM, Chau TTH, Phu NH, Mai NTH, Loc PP, Van ChuongL, Sinh DX, Taylor A, Hien TT, White NJ and Day NPJ. Uniden-tified ions of strong prognostic significance in sever malaria. CriticalCare Medicine 2004; 32: 1683–1688.
Essen B and Kaijser L. Regulation of glycolysis in intermittentexercise in man. Journal of Physiology 1978; 281: 499–511.
Forni LG, McKinnon W, Lord GA, Treacher DF, Peron JMR andHilton PJ. Circulating anions usually associated with the Krebscycle in patients with metabolic acidosis. Critical Care 2005; 9:R591–R595.
Gibala MJ, MacLean DA, Graham TE and Saltin B. Anapleroticprocesses in skeletal muscle during brief dynamic exercise. Journalof Physiology 1997; 502: 703–713.
Kaplan LJ and Kellum JA. Initial pH, base deficit, lactate, anion gap,strong ion difference and strong ion gap predict outcome frommajor vascular injury. Critical Care Medicine 2004, 32: 1120–1124.
Lawler JM, Cline CC, Hu Z and Coast JR. Effect of oxidative stressand acidosis on diaphragm contractile function. American Journalof Physiology 1997; 273: R630–R636.
Lehninger AL, Nelson DL and Cox MM. Principles of Biochemistry,2nd edn. Worth: New York, 1993.
McKinnon W, Lord GA, Forni LG, Peron JMR and Hilton PJ. Arapid LC-MS method for determination of plasma anion profilesof acidotic patients. Journal of Chromatography B 2006; 833(2):179–185.
Mecher C, Rackow EC, Astiz ME and Weil MH. Unaccounted foranion in metabolic acidosis during severe sepsis in humans. CriticalCare Medicine 1991, 19: 705–711.
Meyer T, Faude O, Scharhag J, Urhausen A and Kindermann W. Islactic acidosis a cause of exercise induced hyperventilation at therespiratory compensation point? British Journal of Sports Medicine2004; 38: 622–625.
Mizock BA and Falk JL. Lactic Acidosis in critical illness. CriticalCare Medicine 1992; 20: 80–93.
Rackow EC, Mecher C, Astiz ME, Goldstein C, McKee D and WeilMH. Unmeasured anion during severe sepsis with metabolic-acidosis. Circulatory Shock 1990, 30: 107–115.
Robergs RA, Ghiasvand F and Parker D. Biochemistry ofexercise-induced metabolic acidosis. American Journal of Physi-ological-Regulatory Integrative and Comparative Physiology 2004;287: R502–R516.
Tafaletti JG. Blood lactate: biochemistry, laboratory methods andclinical interpretation. Critical Reviews in Clinical LaboratorySciences 1991; 28: 253–268.
Tsai CS. Spontaneous decarboylation of oxalacetic acid. CanadianJournal of Chemistry 1967; 45: 873–880.
Wasserman K, Whipp BJ, Koyal SN and Beaver WL. Anaerobicthreshold and respiratory gas exchange during exercise. Journal ofApplied Physiology 1973; 35: 236–243.