Embed Size (px)
Citation preview

(CANCER RESEARCH 52, 1222-1227, March 1, 1992]
CA 72-4 Measurement of Tumor-associated Glycoprotein 72 (TAG-72) as a SerumMarker in the Management of Gastric Carcinoma1
Fiorella Guadagni, Mario Roseli!, Teresa Amato, Maurizio Cosimeli!, Pasquale Ferri, Vincenzo Casale,Massimo Carlini, Eugenio Santoro, Renato Cavaliere, John W. Greiner, and Jeffrey Schlom2
/ Department of Surgery [M. Co., P. P., R. C.], Department of Digestive Endoscopy /K C.], and II Department of Surgery [M. Ca., E. S.J, Regina Elena Cancer Institute[F. G., T. A.¡,and Department of Surgery, II University of Rome, School of Medicine [M. R.], Rome, Italy, and Laboratory of Tumor Immunology and Biology, NationalCancer Institute, NIH, Bethesda, Maryland 20892 [J. W. G., J. S.J
ABSTRACT
The presence of three distinct serum markers of carcinoma, tumor-associated glycoprotein 72 (TAG-72; as measured by the CA 72-4 assay),CA 19-9, and carcinoembryonic antigen (CEA), was evaluated in 194patients diagnosed with either malignant (n = 94) or benign (n = 100)
gastric disease. Of the 94 patients diagnosed with gastric carcinoma, thepercentage of patients whose serum samples were positive for TAG-72,
CA 19-9, or CEA was 42.6, 31.9, and 20.2%, respectively. Furthermore,fewer false positive samples were observed for TAG-72 than either CA19-9 or CEA. The analysis of serum TAG-72, CA 19-9, and CEA levels
in patients diagnosed with early (stage I and II) versus advanced (stageIII and IV) disease revealed a significantly higher level of TAG-72 and
CA 19-9 in the serum of patients with advanced stage gastric carcinoma.The serum samples were also analyzed to determine whether any advantage might be gained by simultaneously measuring two or more of thetumor markers. The data clearly indicate that the measurement of TAG-72 with CA 19-9 significantly increased the percentage of gastric carci
noma patients with positive serum levels of either antigen. This advantagewas achieved with no significant increase in the number of false positives.Twenty-one patients were followed postsurgically for up to 3 years todetermine whether the appearance or reappearance of TAG-72, CA 19-9, or CEA accurately predicted disease recurrence. Positive serum TAG-
72 levels correlated with disease recurrence in 7 of 10 patients, comparedwith 5 and 2 patients for CA 19-9 and CEA, respectively. The findingssuggest that serum TAG-72 as measured by the CA 72-4 assay may be
a useful marker for late stage gastric carcinoma and its measurementalone or in combination with CA 19-9 may have utility in the clinical
management of gastric carcinoma.
INTRODUCTION
Although the incidence and death rate from gastric cancer inthe United States have declined in past decades, it remains acommon cause of cancer-related death (1, 2). The highestincidence rates of gastric carcinoma are found in certain Mediterranean countries, in Eastern Europe, and in the Pacific Rim,with Japan having the highest incidence worldwide (3-5). InItaly, the incidence of gastric carcinoma is 25.1/100,000 formales and 16.1/100,000 for females, representing the secondleading cause of cancer-related death in males and the thirdmost common cause of cancer-related deaths (14,500/year, inthe past 5 years) (3).
The early stage of gastric carcinoma is often complicated andextremely difficult to diagnose due to presentation with vague,nonspecific symptoms which are sometimes associated withnonmalignant diseases (6, 7). The development of additionalmethods for this diagnosis includes the desire for efficient,noninvasive diagnostic procedures such as the identification of
Received 10/14/91; accepted 12/17/91.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
' This work has been partially supported by a grant from A.I.R.C., 1991.2To whom requests for reprints should be addressed, at Laboratory of Tumor
Immunology and Biology, Building 10, Room 8B07, National Cancer Institute,NIH, Bethesda, MD 20892.
serum markers specifically associated with a high percentage ofpatients diagnosed with gastric carcinoma. Among the serummarkers currently available for the diagnosis of gastric carcinoma are CEA3 and CA 19-9 (8-13). CEA, a M, 180,000glycoprotein, and CA 19-9, a sialylated Lewis3 antigen, are
distinct tumor markers expressed by human gastric carcinomas(9, 14). An analysis of the data shows that of all patientsdiagnosed with gastric carcinoma, 20.6% had positive serumCEA levels. Of those patients with advanced stage (stage IV)gastric carcinoma, measurable serum CEA was found in 37%(13). CA 19-9 has also been evaluated as a possible serummarker for gastric cancer. Elevated serum levels of this tumorantigen were found in 26% (15) to 72% (11) of the patientswith gastric carcinoma, while 7% of the patients diagnosed withbenign gastric disease had positive serum CA 19-9 levels (11).The studies revealed some potential utility as well as limitationsfor monitoring CEA and/or CA 19-9 serum levels in patientsdiagnosed with gastric carcinoma. The data also suggest theneed to evaluate other serum tumor markers for their potentialrole in the management of gastric cancer.
For several years, the potential utility of a novel serumantigen, TAG-72, has been investigated (16, 17). TAG-72 wasoriginally identified and characterized by MAb B72.3 (18-22)and the B72.3 epitope has, subsequently, been identified as asialosyl-2—»6a-TV-acetylgalactosaminyl epitope (23). A seriesof "second generation" MAbs were produced by immunizationwith purified TAG-72 (24). One such MAb is CC49 which hasa higher affinity for TAG-72 than B72.3 and also recognizesan epitope on TAG-72 which is distinctive from that recognizedby B72.3. CC49 was used in combination with B72.3 to developa double-determinant immunoradiometric assay, designatedCA 72-4 (25, 26), which detects TAG-72 in sera or body fluidsof carcinoma patients. Using the CA 72-4 assay, several groupshave studied the presence of TAG-72 in the serum of patientsdiagnosed with gastrointestinal malignancies (27-30). Thestudies revealed that a significant percentage of patients diagnosed with gastrointestinal carcinoma whose serum CEA levelswere negative had elevated TAG-72 (>6 units/ml), indicating acomplementarity between the two tumor antigens. Moreover,the measurement of serum TAG-72 in patients during postsur-gical follow-up was predictive of the appearance of recurrentdisease (30).
The present study evaluates the preoperative serum levels ofTAG-72, CEA, and CA 19-9, alone or in combination, inpatients diagnosed with primary gastric carcinoma or benigngastric disease. The findings suggest the potential utility ofusing the CA 72-4 assay to detect serum TAG-72, either aloneor in combination with CA 19-9, for the diagnosis of gastriccarcinoma. In addition, a longitudinal follow-up of gastriccarcinoma patients also revealed the potential utility of the CA72-4 assay alone, or in combination with CA 19-9, as part of
3The abbreviations used are: CEA, carcinoembryonic antigen; TAG-72, tumor-
associated glycoprotein 72; MAb, monoclonal antibody.
1222
Research. on December 2, 2020. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

ÇA72-4 MEASUREMENT OF TAG-72 AS SERUM MARKER
the clinical management of postsurgical gastric carcinomapatients.
MATERIALS AND METHODS
Patient Information. One hundred ninety-four patients, 94 with histologically diagnosed primary gastric adenocarcinoma [SO males, 44females; mean age, 58 ±1.3 (SE) years, ranging from 30 to 89 yearsold], and 100 patients with histologically confirmed benign [gastritis,ulcer, adenomas, polyps] gastric disease [54 males, 46 females; meanage, 53 ±1.9 years] were evaluated. All patients with malignant diseaseunderwent surgery for their primary tumor at the Department ofSurgery, while patients diagnosed with benign gastric disease underwentendoscopie examination at the Department of Digestive Endoscopy ofthe Regina Elena National Cancer Institute, Rome, Italy. Malignantgastric disease was pathologically staged according to the tumor-nodes-metastasis classification (Union International Contre le Cancer tumor-nodes-metastasis classification of malignant tumors, 1983): Stage I (n= 14); Stage II (n = 16); Stage III (n = 36); and Stage IV (n = 28).Serum samples were drawn within 1 week prior to surgery; 3, 7, and14 days postoperatively; and every 3 months during clinical follow-up.Serum samples from patients with benign disease were drawn at thetime of endoscopy. All samples were aliquoted, coded, and stored at-20°Cuntil assays were performed.
CA 72-4, CEA, and CA 19-9 Radioimmunoassays. Serum TAG-72antigen levels were determined by a double-determinant immunoradi-ometric assay kit, CA 72-4, supplied by Centocor (Malvern, PA), asdescribed previously (25). Samples and TAG-72 standards were assayedin duplicate. Briefly, 100 n\ of specimen in the presence of 100 n\ ofphosphate buffer were incubated at 37°Cfor 4 h with beads coated with
MAb CC49. The beads were washed 3 times with distilled water andincubated with '"I-B72.3 for 18 to 20 h at 4'C. After 3 washes with
distilled water, bound radioactivity was measured in a gamma counter.TAG-72 levels, expressed as units/ml, were determined by convertingcpm to concentration values using a concurrently obtained standardcurve. The cutoff limit for this assay was set at 6 units/ml as suggested(25). CEA serum levels were determined using a CEA RIA MAb kit(Abbott Laboratories, Inc., Chicago, IL). Several different cutoff limits,ranging from 2.5 to 10.0 ng/ml, have been used for the analysis of CEAserum levels (31-33). In the present study, we used a cutoff limit of 5.0ng/ml for better specificity. CA 19-9 serum levels were determined aspreviously described using the suggested cutoff limit of 37 units/ml(12). Measurement of serum TAG-72, CEA, and CA 19-9 was donewithout any prior knowledge of the clinical diagnosis. A significantincrease of the serum marker levels was considered, either when negative serum levels became positive or when there was an increase of>50% over the mean of previous positive levels.
Statistical Analysis. A Student t test (STATVIEW softwear package)was used to evaluate statistical differences among the serum tumormarkers.
RESULTS
Sera from 94 patients with primary gastric carcinoma and100 patients with benign gastric disease were evaluated for thepresence of TAG-72 using the CA 72-4 assay, for 19-9 usingthe CA 19-9 assay, and for CEA using the CEA-radioimmuno-
Table 2 Correlation of presurgical TAG-72, Ca 19-9 and CEA serum levels andclinical stage in gastric cancer patients
Serum antigenlevelsStageI
IIIIIIVTotalNo.
ofpatients14
16362894TAG-72
>6units/ml1(7.1)°
2(12.5)19(52.8)18(64.3)40 (42.6)CA
19-9>37units/ml4
(28.6)2(12.5)
11 (30.6)13(46.4)30(31.9)CEA
>5ng/ml1
(7.1)2(12.5)7 (19.5)9 (32.2)
19 (20.2)" Numbers in parentheses, percentage of patients within each stage of malig
nant gastric cancer in which their serum samples contain positive titers of theindicated tumor antigen.
assay-monoclonal antibody assay. As shown in Table 1, 42.6%of the sera from patients diagnosed with primary gastric carcinoma had elevated TAG-72 levels (>6.0 units/ml). In contrast,only 1 of 100 of the sera from patients with benign gastricdisease had positive TAG-72 levels. CA 19-9 serum levels wereelevated (>37.0 units/ml) in 31.9 and 7% in patients withmalignant and benign disease, respectively. Serum CEA waselevated (>5.0 ng/ml) in 20.2% of sera from patients withgastric carcinoma and 9% of sera from patients with benigndisease.
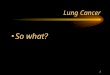
The relationships between serum TAG-72, CA 19-9, andCEA levels and the clinical staging of the patients with gastriccarcinoma were also evaluated (Table 2). In particular, positiveserum TAG-72 levels were found in patients diagnosed withadvanced stage gastric carcinoma. Of the 40 patients which hadpositive serum TAG-72 levels, 37 were diagnosed with eitherstage III or stage IV gastric carcinoma. Likewise, elevatedserum CA 19-9 and CEA were also found predominantly insera samples from patients with advanced stage gastric carcinoma (Table 2). Fig. 1 summarizes the statistical analysis ofthe mean CA 72-4, CEA, and CA 19-9 presurgery serum levelsfor gastric carcinoma patients classified as early (stages I andII) and advanced (stages HI and IV) disease. The mean serumTAG-72 levels from patients with stage I and II gastric carcinoma was 3.3 ±0.6, while the mean value from patients withstage III and IV disease was 24.1 ±7.8 (Fig. 14) (P < 0.002).A statistically significant difference between serum CA 19-9levels in patients diagnosed with early and advanced gastriccarcinoma was also observed. As shown, the mean serum CA19-9 level from patients with stage III or IV gastric carcinomawas 92.3 ±25.2 compared with 23.2 ±4.0 from patientsdiagnosed with stage I or II disease (P < 0.05) (Fig. \B). Nostatistical difference was observed for differences in serum CEAlevels between those patients diagnosed with early and advanceddisease. Thus, these results indicate that measurement of TAG-72 may be useful in differentiating early versus advanced gastriccarcinoma.
Studies were then conducted to determine if there was anyadvantage in the use of combinations of the CA 72-4, CA 19-9, and CEA assays. Fig. 2 illustrates the presence of TAG-72and/or CA 19-9 in the sera of the 94 patients diagnosed with
Table 1 Summary of TAG-72, CA 19-9, and CEA levels in sera of patients diagnosed with malignant or benign gastric diseases
Serum tumor antigen levels
TAG-72(units/ml)DiagnosisCarcinoma
BenignNo.
ofpatients94
100Range1-478.01-6.1Mean17.7±4.2"
1.9 ±0.2No.
of patients>6units/ml40
(42.6)'
KDRange1.5-10401.5-122.9CAI
9-9(units/ml)Mean68.9
±16.715.1 ±3.2No.
of patients>37units/ml30(31.9)
7(7)Range1-184.21-23.7CEA
(ng/ml)Mean10.4
±1.93.4 ±0.3No.
of patients>5ng/ml19
(20.2)9(9)
" Mean ±SE.'' Numbers in parentheses, percentage of patients' serum samples with detectable levels of the respective tumor antigen.
1223
Research. on December 2, 2020. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

ÇA72-4 MEASUREMENT OF TAG-72 AS SERUM MARKER
40
- 3010)
20
S 10
< 6
p <0.002 I 3.3t0.6 | 24.1±7.8
I + II III + IV
B120
3 100
80LU
60-3
KLUV)
o> 37
20-
p<0.05 92.3±25.2
III + IV
40
EÌ 30-
Mpj111tu 20-
CELU
OT
111o
10-
5 -
p <O.OB
l + II III t IV
Fig. 1. Comparison of the presence of TAG-72 (A), CA 19-9 (B) and CEA (C)in the serum of patients diagnosed with early (stage I and II) (C) or advanced(stage III and IV) (•)gastric carcinoma. , cutoff serum values for each ofthe tumor markers. The mean ±SE for each group is listed in each column.
gastric carcinoma. As shown in Table 1, serum samples from30 of the 94 patients has positive CA 19-9 levels. Of those 30,17 serum samples also had positive TAG-72 levels. Of theremaining 64 samples which were negative for CA 19-9, 23(35.9%) had positive titers of TAG-72. Therefore, combiningthe measurement of TAG-72 with CA 19-9, 53 of the 94
(56.4%) serum samples were positive for either tumor marker.Similar analyses were done with TAG-72 versus CEA (Fig. 3)and CEA versus CA 19-9 (Fig. 4). As shown in Fig. 3, of 94patients serum samples 8 (8.5%) were CEA positive, and 11(11.7%) were positive for both CEA and TAG-72. Of the
1000
Iin
sCE111(O
¡
100-
n =23O
0o°
'•osO
o 0 000„¿�0»
a S0°o0o°o°o0°o0°00
° ° 0° »00°°o
°o ° ° on=41 o °n
=17o00
°o
o0000°
'
00o°
00•••"n
= 13
10 100 1000
CA19-9 SERUM LEVELS (U/ml)
Fig. 2. Serum TAG-72 and CA 19-9 levels in patients diagnosed with gastriccarcinoma. , serum cutoff values for TAG-72 (6 units/ml) and CA 19-9 (37units/ml), n, number of patients in each quadrant (i.e., 23 patients were TAG 72positive and CA 19-9 negative).
lUUU:100:10-6
'n=
290ooo0
0°000
«i O»0° 0°o0°
°0°O
O o O nO00 0 0 Oo®300°00
0Q^?oo
oo °oo°n= 46n=
11oo0
0o00
° o°o00ooo
on=8o
10 100 1000
CEA SERUM LEVELS (ng ml)
Fig. 3. Serum TAG-72 and CEA levels in patients diagnosed with gastriccarcinoma. See Fig. 2 for explanation of symbols.
ED
CO_lLU
III
E111CO
<ü
1UUU-100-37io-n= 2000
°°o0
00
000
00°°°0 00°8V°°°
°od6ooo30
°oI° %oo°0
o 00o
o oooo3OOo°
oon
=550
°n=lOO0
00°o
°°o00
00n=9
10 100 1000
CEA SERUM LEVELS (nq ml)Fig. 4. Serum CA 19-9 and CEA levels in patients diagnosed with gastric
carcinoma, n, number of patients grouped according to the presence/absence ofthe respective serum marker as analyzed with the indicated cutoff values ( ).
1224
Research. on December 2, 2020. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

ÇA72-4 MEASUREMENT OF TAG-72 AS SERUM MARKER
Table 3 Summary of CA 72-4, TAG-72, and CEA serum levels in patients withbenign or malignant disease
MalignantTAG-72
CEACA 19-9TAG-72 and/or CEATAG-72and/or CA 19-9TAG-72 and/or CEAAll 3 markersNo.
ofpatients"40
193048533957%of
patients"42.6
20.231.951.156.441.560.6BenignNo.
ofpatients'1
7989
1213%of
patients*1
7989
1213
" Number and percentageof carcinoma patients with elevatedtumor antigenserum levels(total patients evaluated,94).
bNumber and percentageof benignpatientswith elevatedtumor antigenserumlevels(total patients evaluated, 100).
remaining 75 patients whose serum samples were CEA negative, 38.7% were TAG-72 positive. When combining the measurement of serum CEA with TAG-72, serum samples from 48of the 94 (51.1%) patients were positive. The relationshipbetween serum CEA and CA 19-9 in the serum samples fromthese patients was also investigated (Fig. 4). Serum from 9 ofthe 94 patients was positive for CEA, and serum samples from10 patients contained positive levels of both CEA and CA 19-9. Of the 75 patients whose serum CEA levels were negative,26.7% had positive CA 19-9 serum levels. Combining themeasurement of both tumor markers revealed that 41.5% ofserum samples were positive for either CEA or CA 19-9.
Table 3 summarizes the percentage of patients diagnosedwith gastric carcinoma (n = 94) or with benign gastric disease(n = 100) whose serum samples contained either TAG-72, CA19-9, and/or CEA. Serum TAG-72 (42.6%) alone was foundin a higher percentage of patients with gastric carcinoma thaneither CEA (20.2%) or CA 19-9 (31.9%) alone. Furthermore,combining serum TAG-72 measurement with either CA 19-9or CEA increased the percentage of serum positive to 56.4 and51.1%, respectively. It should be noted that a concomitantincrease in the percentage of false-positive serum levels was notobserved when TAG-72 measurement was combined with eitherCA 19-9 or CEA. Sixty % of gastric cancer sera were positivewhen using all three markers.
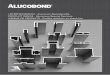
Serum TAG-72, CA 19-9, and CEA levels were followedlongitudinally in 21 patients for up to 3 years postsurgery forprimary gastric carcinoma or until the clinical diagnosis ofrecurrence of malignant disease (Table 4). Eleven of the 21patients with no clinical evidence of disease had no detectableserum levels of any of the 3 tumor antigens. One patient (PF)without clinical evidence of disease had a positive serum CEAat 207 days postsurgery. Ten clinical recurrences were diagnosed in 9 patients (patient RA, 2 recurrences). Serum TAG-72 levels were elevated in 7 of the 10 clinical recurrences,whereas serum CA 19-9 and CEA levels were positive in 5 and2 cases, respectively. In all cases, detectable serum levels ofTAG-72 either occurred prior to or concomitant with theclinical diagnosis of recurrent disease. As an example, Fig. 5illustrates the changes in serum TAG-72 (panel A), CA 19-9(panel B), and CEA (panel C) in patient DSA who was diagnosed with stage II gastric carcinoma and was followed forapproximately 2 years after surgical resection of the primarytumor. Prior to surgery, serum samples from patient DSA werepositive for CEA and negative for TAG-72 and CA 19-9. Duringthe postsurgical follow-up, positive TAG-72 serum was detected, whereas serum CA 19-9 and CEA remained negative.Elevation of serum TAG-72 was detected at 297 days prior toclinical recurrence.
DISCUSSION
The present study indicates that the measurement of serumTAG-72 levels may be an important component in the diagnosisand clinical follow-up of patients with malignant gastric disease.When compared with other serum tumor markers that arecurrently used for the diagnosis and monitoring of patients forgastric carcinoma, i.e., CA 19-9 and CEA, a higher percentageof patients with gastric cancer had positive TAG-72 serumlevels. In addition, the specificity of serum TAG-72 for differentiating carcinoma versus benign gastric disease was betterthan for either CA 19-9 or CEA. The 94 patients diagnosedwith gastric carcinoma were also staged according to tumor-nodes-metastasis classification and the presence of serum TAG-
Table 4 Summaryof longitudinalevaluationof TAG-72serumlevelsin gastricpatients
PatientFGBLDSAMDPAPFPURASFFEGFIFLMLPMPVUADADAPCMFAPAPresurgeryStageTAG-72 CEA CA19-9I-IIII
-+II+IIII
- -+IIIIIIIII
- +-IIIIII
+ ++III+ +-III
+IIIIIIIII
+ -+IV++IV++IV-+IVFollow-up
(days)860427665f372505241384550C989160C43460C769155504757145130180f200C80°First
detectableelevationof tumorantigens"TAG-72ND*ND211NDNDNDND207368ND63ND16NDNDNDNDND6354NDNDCEANDNDNDNDND207NDNDNDND102ND16NDNDNDNDNDNDNDNDNDCA
19-9NDNDNDNDNDNDNDND368ND63ND16NDNDNDNDND637NDNDTimeof clinical
evidence(days)NEDNED508NEDNEDNEDNED248440NED133NED45NEDNEDNED365NED639717340
" Days postsurgery.* ND, not detectable; NED, no evidence of disease.cPatients in which detectableserum TAG-72, CEA, and/or CA 19-9precededthe time of diagnosisof clinicalrecurrentdisease.
1225
Research. on December 2, 2020. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

ÇA72-4 MEASUREMENT OF TAG-72 AS SERUM MARKER
10 100DAYS POST SURGERY
100
I »
(A
iLU-1 10
10 100DAYS POST SURGERY
10 100
DAYS POST SURGERY
Fig. 5. Longitudinal postsurgery evaluation of serum TAG-72 (A), CA 19-9(A), and CEA (C) in patients diagnosed with stage II gastric adenocarcinoma.Arrow, time of surgery; , serum cutoff values for each of the tumor antigens.
72, CA 19-9, and CEA in the different stages were evaluated.Serum levels for both TAG-72 and CA 19-9 were highly correlated with the advanced stages of gastric carcinoma. Theseobservations suggest that the presence in the serum of TAG-72and CA 19-9 closely reflects the clinical staging of the diseaseand that additional studies are needed which may elucidate theroles that those tumor markers play in the biology of humangastric carcinoma.
It is generally agreed that the sensitivity as well as thespecificity of a single serum tumor marker for the diagnosis ofprimary and recurrent carcinoma is limited. No one serumtumor marker will unfailingly predict the presence of malignantdisease or differentiate between benign versus malignant disease. The present data clearly indicate that serum TAG-72, CA19-9, and CEA appear in 42.6, 31.9, and 20.2%, respectively,of the serum of patients diagnosed with gastric carcinoma(Table 1). Therefore, a majority of patients (i.e., >50%) withmalignant gastric disease do not contain measurable serumlevels of any of these three tumor markers if analyzed sepa
rately. Recent findings have suggested a complementarityamong various serum tumor markers which may be exploitedin the diagnosis of gastrointestinal carcinoma (30). Ideally, onewould envision that the complementarity might increase thesensitivity with respect to clinical diagnosis with little changein the specificity (i.e., little increase in false positives). Forexample, the present data indicate that combining the measurement of serum TAG-72 with CA 19-9 increased the percentageof patients diagnosed with gastric carcinoma who also hadmeasurable serum titers of either tumor antigen. At the sametime, there was no change in the number of false positive serumsamples (i.e., patients with benign gastric disease), suggestingthat the simultaneous measurement of TAG-72 and CA 19-9may selectively identify a higher percentage of patients withgastric cancer. Additional studies with higher numbers of samples are needed to further investigate whether the analysis ofmultiple serum tumor markers may be advantageous in thediagnosis of gastric carcinoma.
One of the important applications of any serum marker isthe ability to use the measurement of the serum tumor antigenin predicting the clinical course of the malignant disease, particularly, the diagnosis of disease recurrence. In the presentstudy, 21 patients diagnosed with primary gastric cancer werefollowed postsurgery for up to 3 years or to time of diseaserecurrence. As seen in Table 4, none of the 12 patients with noclinical evidence of disease had positive TAG-72 levels. Six of9 patients [1 patient (RA) had 2 recurrences], however, withclinically confirmed disease recurrence had elevated serumTAG-72 levels. In 5 of the 6 patients with recurrent disease,positive serum TAG-72 levels were detected prior to the clinicaldiagnosis (Table 4) and, in some patients, positive serum TAG-
72 levels preceded clinical evidence of disease by 100 to 300days. Monitoring both serum CA 19-9 as well as CEA did notcorrelate as well as TAG-72 with the onset of recurrent disease.While additional studies with larger population groups anddifferent population bases are needed, these findings indicatethat the measurement of serum TAG-72 levels may be usefulin the clinical diagnosis of primary and recurrent gastric cancer.
REFERENCES
1. Silverberg, E. Cancer statistics. CA Cancer J. Clin., 36:9-25, 1986.2. Devesa, S. S., and Silverman, D. T. Cancer incidence and mortality trends
in the United States 1935-1974. J. Nati. Cancer Inst., 60: 545-561, 1978.3. Decarli, A., and LaVecchia, C. Cancer mortality in Italy, 1985-1987. Tumori,
77:1-6, 1991.4. Dunham, L. J., and Bailar, J. ( '., III. World maps of cancer mortality rates
and frequency ratios. J. Nati. Cancer Inst., 41: 155-203, 1968.5. WHO. World Health Statistics Annals, 1988.6. Goldsmith, H. S., and Ghosh, B. C. Carcinoma of the stomach. Am. J. Surg.,
720:317-319, 1970.7. Adashek, K., Sanger, J., and Longmire, W. P., Jr. Cancer of the stomach.
Review of consecutive ten-year intervals. Ann. Surg., 189: 6-10, 1979.8. Goldenberg, D. M., Neville, A. M., Carter, A. C., Go, V. L., Holyoke, E.,
Kjisselbacher, K., Schein, P., and Schwartz, M. Carcinoembryonic antigen:its role as a marker in the management of cancer: a National Institutes ofHealth Consensus Development Conference. Ann. Intern. Med., 94: 407-409, 1981.
9. Sikorska, H., Shuster, J., and Gold, P. Clinical applications of carcinoem-bryonic antigen. Cancer Detect. Prev., 12: 321-355, 1988.
10. Herlyn, M., Sears, H. F., Steplewski, /... and Koprowski, H. Monoclonalantibody detection of a circulating tumor-associated antigen. I. Presence ofantigen in sera of patients with colorectal, gastric, and pancreatic carcinoma.J. Clin. Immunol., 2: 135-140, 1982.
11. Ritts, R. E., Jr., Del Villano, B. C., Go, V. L., Herberman, R. B., Klug, T.L., and Zurawski, V. R., Jr. Initial clinical evaluation of an immunoradiome-tric assay for CA 19-9 using the NCI serum bank. Int. J. Cancer, 33: 339-345, 1984.
12. Del Villano, B. C., Brennan, S., Brock, P., Bucher, C., Liu, V., McClure, M.,Rake, B., Space, S., Westrick, B., Schoemaker, H., and Zurawski, V. R., Jr.Radioimmunometric assay for a monoclonal, antibody-defined tumor
1226
Research. on December 2, 2020. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

ÇA72-4 MEASUREMENT OF TAG-72 AS SERUM MARKER
marker, CA 19-9. Clin. Chem., 29: 549-552, 1983.13. Koga, T., Kano, T., Souda, K., Oka, N., and Inokuchi, K. The clinical
usefulness of preoperative CEA determination in gastric cancer. Jpn. J. Surg.,17: 342-347, 1987.
14. Sipponen, P., and Lindgren J. Sialylated Lewis' determinant CA 19-9 in
benign and malignant gastric tissue. Acta Pathol. Microbiol. Immunol.Scand. Sect. A, 94: 305-311, 1986.
15. Staab, H. J., Hournung, A., Anderer, F. A., and Kieninger, G. Clinicalsignificance of the circulating tumor-associated antigen CA 19-9 in cancersof the digestive tract. Dtsch. Med. Wochenschr., 109: 1141-1147, 1984.
16. Paterson, A. J., Schlom, J., Sears, H. F., Bennett, J., and Colcher, D. Aradioimmunoassay for the detection of a tumor-associated glycoprotein(TAG-72) using monoclonal antibody B72.3. Int. J. Cancer, 37: 659-666,1986.
17. Klug, T. L., Sattler, M. A., Colcher, D., and Schlom, J. Monoclonal antibodyimmunoradiometric assay for an antigenic determinant (CA 72) on a novelpancarcinoma antigen (TAG-72). Int. J. Cancer, 38: 661-669, 1986.
18. Colcher, D., Horan Hand, P., Nuti, M., and Schlom, J. A spectrum ofmonoclonal antibodies reactive with human mammary tumor cells. Proc.Nati. Acad. Sci. USA, 78: 3199-3203, 1981.
19. Johnson, V. G., Schlom, J., Paterson, A. J., Bennett, J., Magnani, J. L., andColcher, D. Analysis of a human tumor-associated glycoprotein (TAG-72)identified by monoclonal antibody B72.3. Cancer Res., 46: 850-857, 1986.
20. Thor, A., Viglione, M. J., Muraro, R., Ohuchi, N., Schlom, J., and Gorstein,F. Monoclonal antibody B72.3 reactivity with human endometrium: a studyof normal and malignant tissues. Int. J. Gynecol. Pathol., 6: 235-247,1987.
21. Thor, A., Ohuchi, N., Szpak, C. A., Johnston, W. W., and Schlom, J.Distribution of oncofetal antigen tumor-associated glycoprotein-72 definedby monoclonal antibody B72.3. Cancer Res., 46: 3118-3124, 1986.
22. Wolf, R. C., D'Emilia, J. C., Salem, R. R., De Coste, D., Sears, H. F.,Gottlieb, L. S., and Steele, G. D., Jr. Detection of the tumor-associatedglycoprotein antigen (TAG-72) in premalignant lesions of the colon. J. Nati.Cancer Inst., 81:1913-1917, 1989.
23. Kjeldsen, T., Clausen, H., Hirohashi, S., Ogawa, T., lijima, H., and Hako-mori, S. Preparation and characterization of monoclonal antibodies directedto the tumor-associated O-linked sialosyl-2—»6a-JV-acetylgalactosaminyl(Sialosyl-Tn) epitope. Cancer Res., 48: 2214-2220, 1988.
24. Muraro, R., Kuroki, S. M., Wunderlich, D., Poole, D. J., Colcher, D., Thor,
A., Greiner, J. W., Simpson, J. F., Molinolo, A., Noguchi, P., and Schlom,J. Generation and characterization of B72.3 second generation monoclonalantibodies reactive with the tumor associated glycoprotein 72 antigen. CancerRes., 48: 4588-4596, 1988.
25. Gero, E. J., Colcher, D., Ferroni, P., Melsheimer, R., Giani, S., Schlom, J.,and Kaplan, P. The CA 72-4 radioimmunoassay for the detection of theTAG-72 carcinoma associated antigen in serum of patients. J. Clin. Lab.Anal., J: 360-369, 1989.
26. Ferroni, P., Szpak, C., Greiner, J. W., Guadagni, F., Simpson, J. F., Johnston, W. W., and Colcher, D. CA 72-4 radioimmunoassay in the diagnosisof malignant effusions. Comparison of various tumor markers. Int. J. Cancer,«.-445-451, 1990.
27. Ohuchi, N., Takahashi, K., Matoba, N., Sato, T., Taira Y., Sakai, N.,Masuda, M., and Mori, S. Comparison of serum assay for TAG-72, CA 19-9, and CEA in gastrointestinal carcinoma patients. Jpn. J. Clin. Oncol., 19:242-248, 1989.
28. Ohuchi, N., Gero, E., Mori, S., Akimoto, M., Matoba, N., Nishihira, T.,Ilirayama. K., Colcher, D., and Schlom, J. Clinical evaluation of CA 72-4immunoradiometric assay for serum TAG-72 antigen in patients with carcinoma. J. Tumor Marker Oncol., 5: 1-10, 1990.
29. Byrne, D. J., Browning, M. C. K., and ¿uscieri, A. CA-72-4: a new tumormarker for gastric cancer. Br. J. Surg., 77: 1010-1013, 1990.
30. Guadagni, F., Roselli, M., Amato, T., Cosimelli, M., Mannella, E., Ferri, P.,Abbolito, M. R., Cavalière,R., Colcher, D., Greiner, J. W., and Schlom, J.Tumor-associated glycoprotein-72 (TAG-72) serum levels complement car-cinoembryonic antigen (CEA) levels in monitoring patients with gastrointestinal carcinoma: a longitudinal study. Cancer (Phila.), 68: 2443-2450, 1991.
31. Goldenberg, D., Neville, A. M., Cortes, A. C., Go, V. L. V., Holyoke, E. D.,Issellbacher, K. J., Schein, P. S., and Schwartz, M. Carcinoembryonic antigen: its role as a marker in the management of cancer: a National Institutesof Health Consensus Development Conference. Ann. Intern. Med., 94:407-409, 1981.
32. Mach, J-P., Jaeger, P., and Berholet. M-M. Detection of recurrence of large-bowel carcinoma by radioimmunoassay of circulating carcinoembryonic antigen (CEA). Lancet, 7: 535-540, 1974.
33. Moertel, C. G., O'Fallon, J. R., Go, V. L., O'Connell, M. J., Thynne, G. S.
The preoperative carcinoembryonic antigen test in the diagnosis, staging andprognosis of colorectal cancer. Cancer (Phila.), 58: 603-610, 1986.
1227
Research. on December 2, 2020. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

1992;52:1222-1227. Cancer Res Fiorella Guadagni, Mario Roselli, Teresa Amato, et al. Carcinoma(TAG-72) as a Serum Marker in the Management of Gastric CA 72-4 Measurement of Tumor-associated Glycoprotein 72
Updated version
http://cancerres.aacrjournals.org/content/52/5/1222
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/52/5/1222To request permission to re-use all or part of this article, use this link
Research. on December 2, 2020. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from