Embed Size (px)
Citation preview
Electrocardiography
part 2
.
QRS complex
Normal values
Duration: < 2.5 mm.
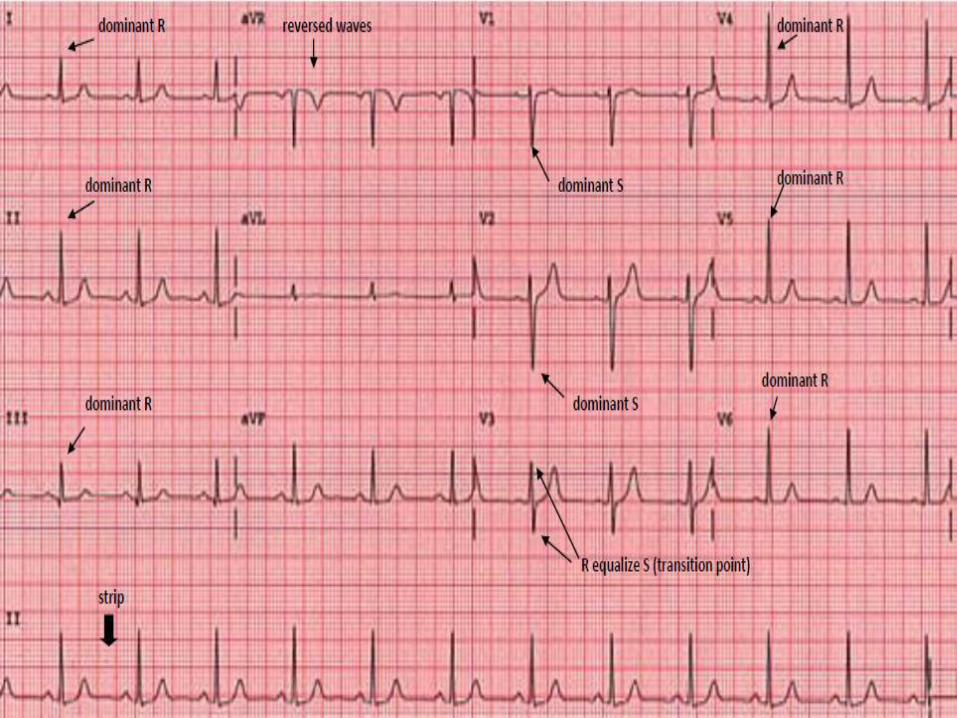
Morphology: progressionfrom Short R and deep S (rS) in V1 to tall R and short S in V6 with small Q in V5-6 (qRs).
Abnormalities: 1. Wide QRS complex
Bundle branch block.
Ventricular rhythm
Tall R in V1
RVH.
RBBB.
Posterior MI.
WPW syndrome.
3. Abnormal Q wave
[ > 25% of R wave]
MI.
Hypertrophiccardiomyopathy.
Normal variant
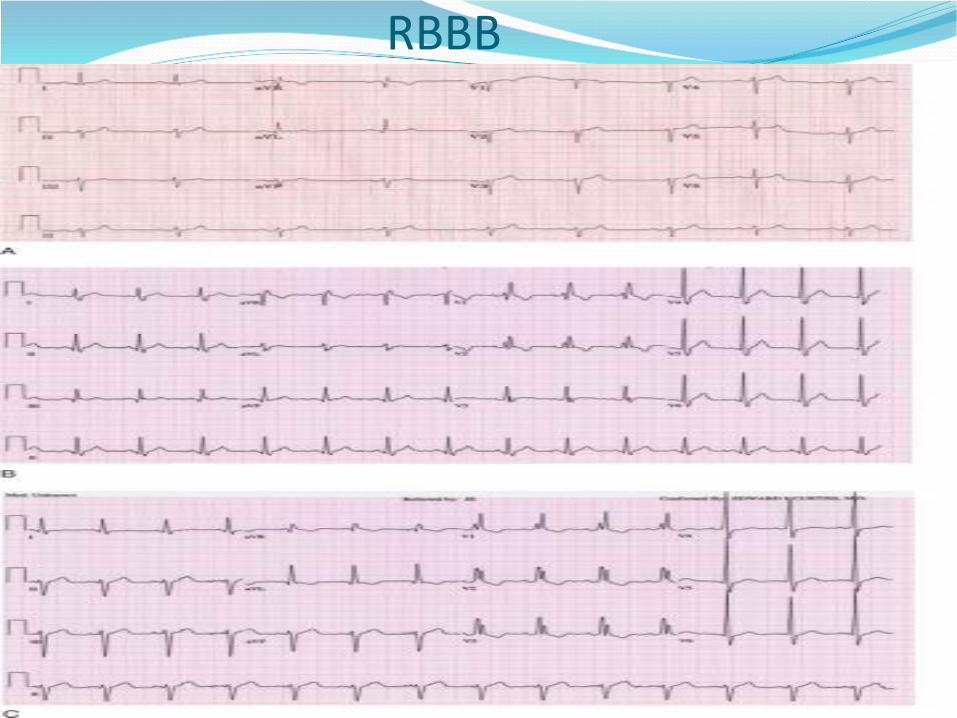
RBBB
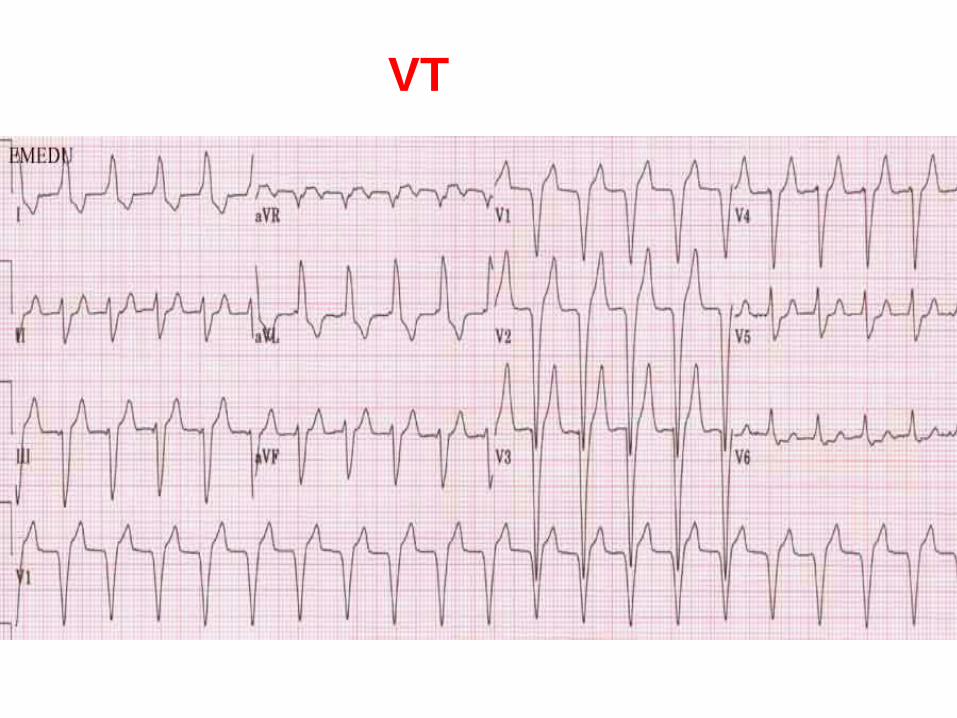
VT
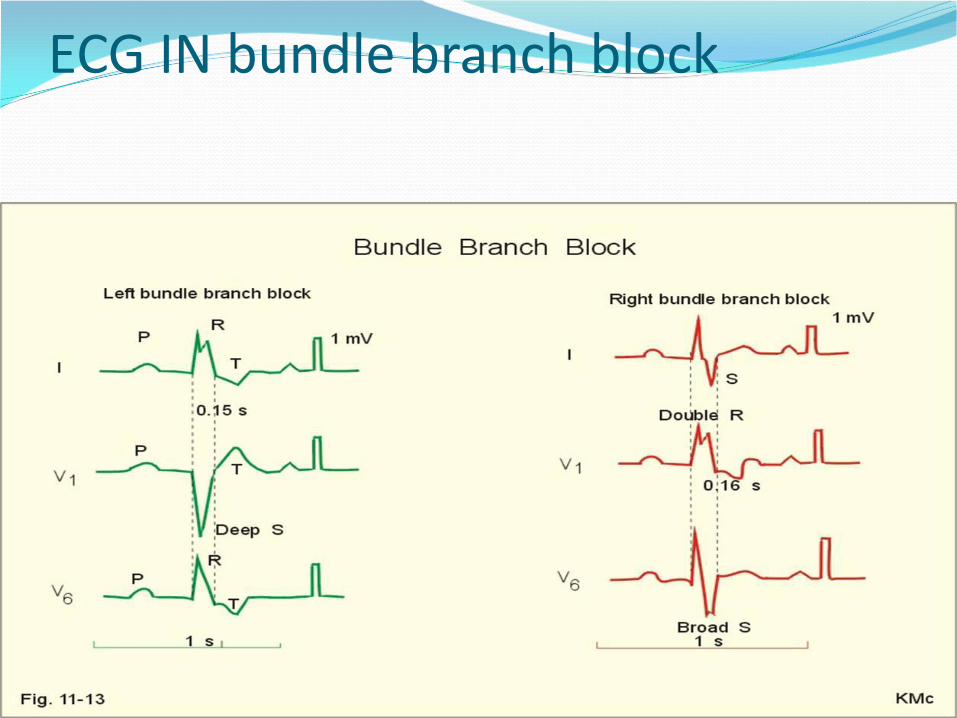
ECG IN bundle branch block
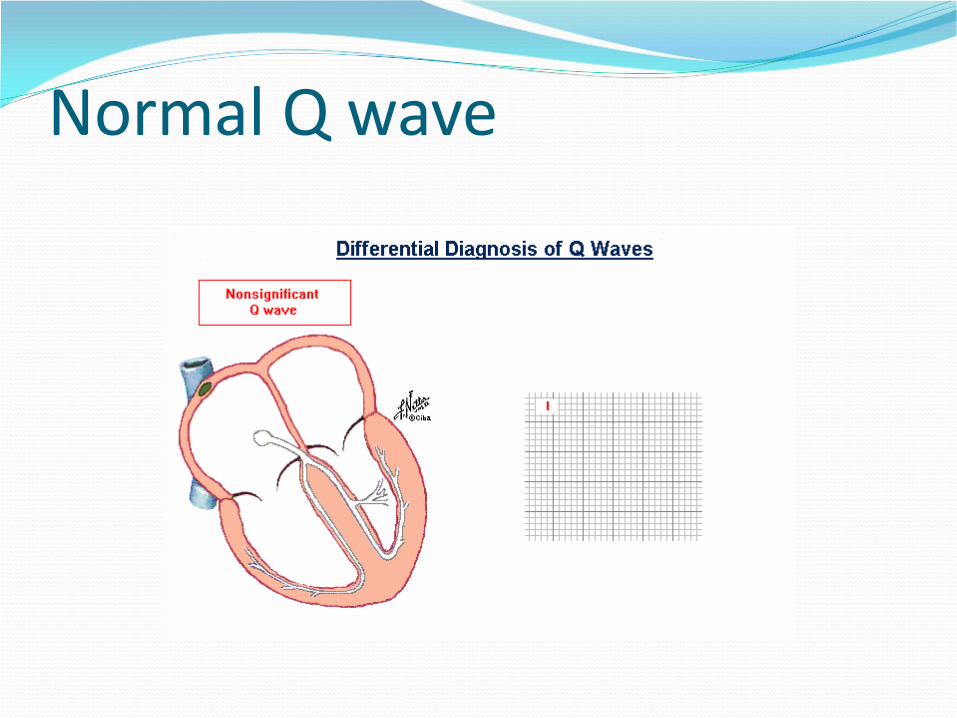
Normal Q wave
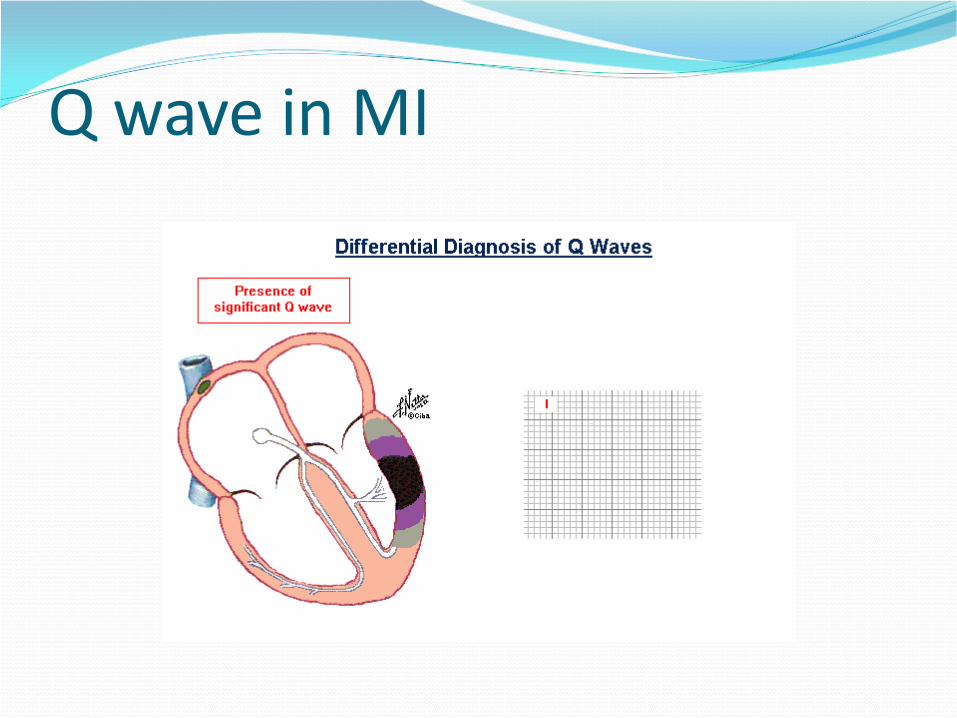
Q wave in MI
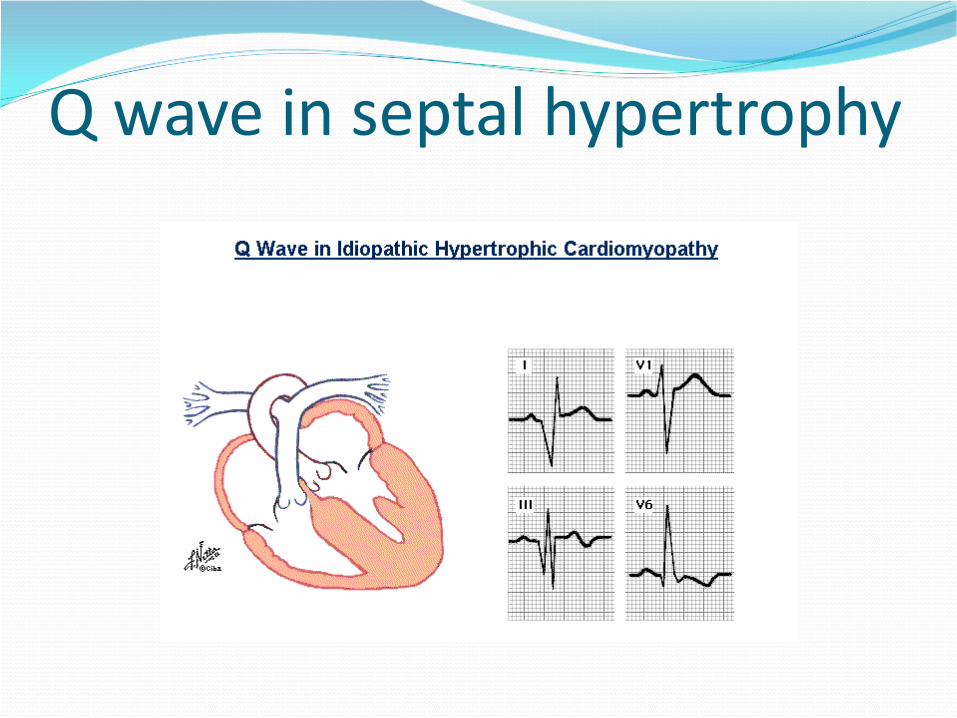
Q wave in septal hypertrophy
ST- segment
Normally it's isoelectric.
[i.e. at same level of PR segment]
Abnormalities:
1. ST elevation: Acute MI.
Prinzmetal angina.
Acute pericarditis.
Early repolarization.
2. ST depression:
Ischemia.
Ventricular strain.
BBB.
Hypokalemia.
Digoxin effect
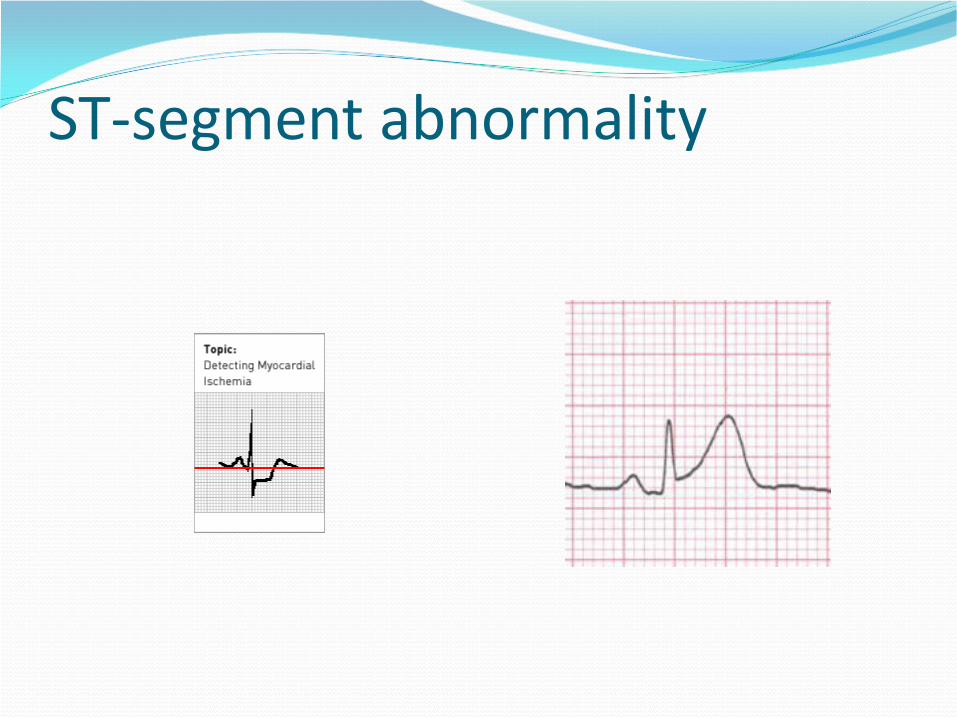
ST-segment abnormality
T-waveNormal values. 1. Polarity: Always up in I,II,V4-5 Always down in aVR. Variable in III, aVL,
aVF, V1-3.
2. amplitude: < 10mm inthe chest leads.
Abnormalities: 1. Peaked T-wave: Hyper-acute MI. Hyperkalemia. Normal variant. 2. T- inversion: Ischemia. Myocardial infarction. Myocarditis Ventricular strain BBB. Hypokalemia. Digoxin effect
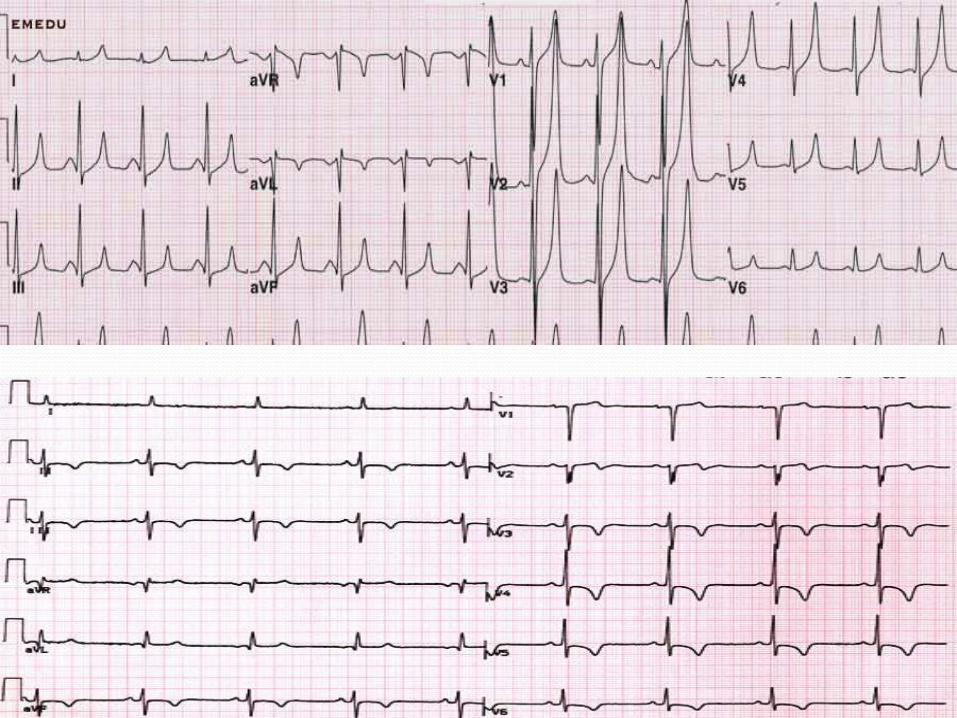
QT-Interval
Definition: Time interval between beginning of
QRS complex to the end of T wave.
Normally: At normal HR: QT ≤ 11mm (0.44 sec)
Abnormalities:
1. Prolonged QT interval: hypocalcemia and congenital long QT syndrome.
2. Short QT interval: hypercalcemia
ECG in IHD
ECG IN STEMIHyper acute T wave
ST segment elevation
• development of Q waves
• ST segment returns to the baseline
• T waves become inverted
This changes should follow either surface or specificartery
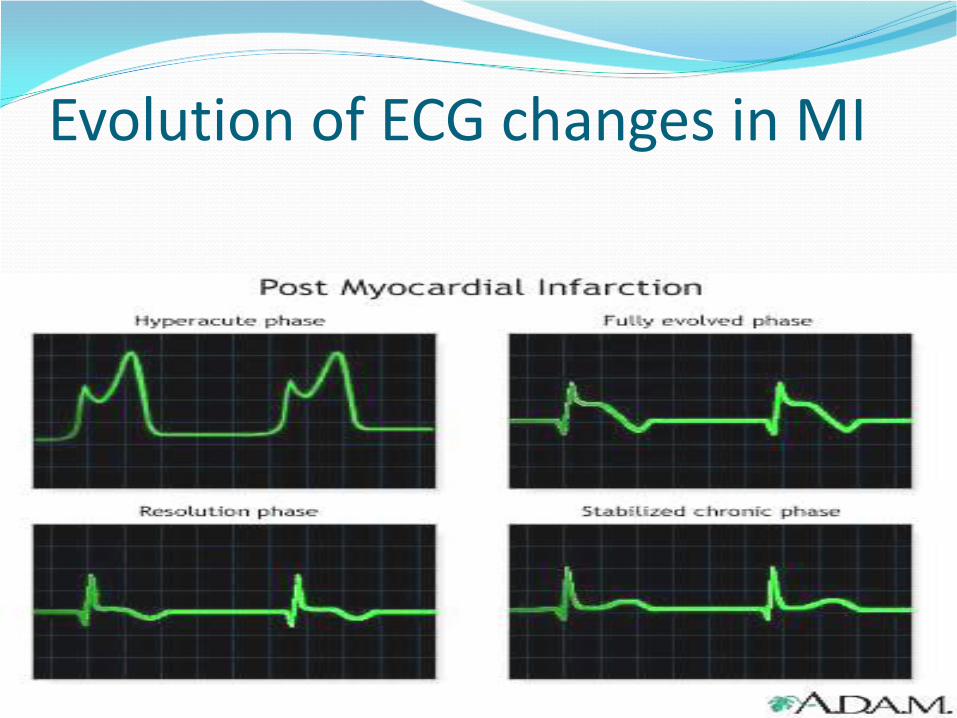
Evolution of ECG changes in MI
ECG in other IHD (NSTEMI ,
unstable angina , angina pectoris)
• ST segment depression
• T waves become inverted
• may be normal
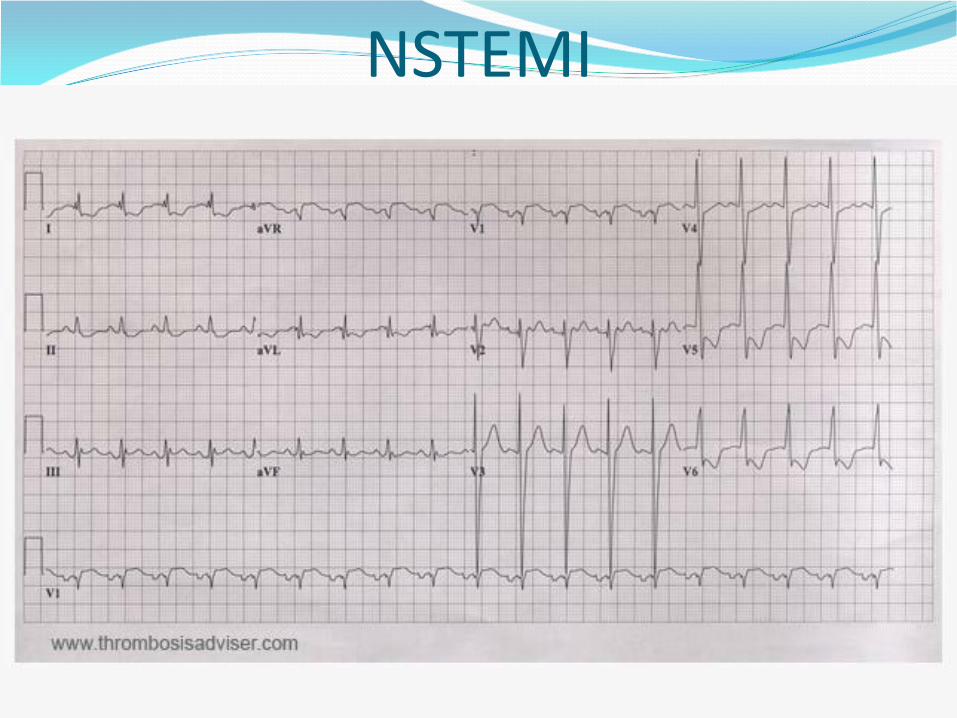
NSTEMI
ECG IN ARRYTHMIAS
Tachyrythmias
Narrow complex QRS
Rate >100 with narrow QRS
Broad complex QRS
Rate >100 with broad QRS
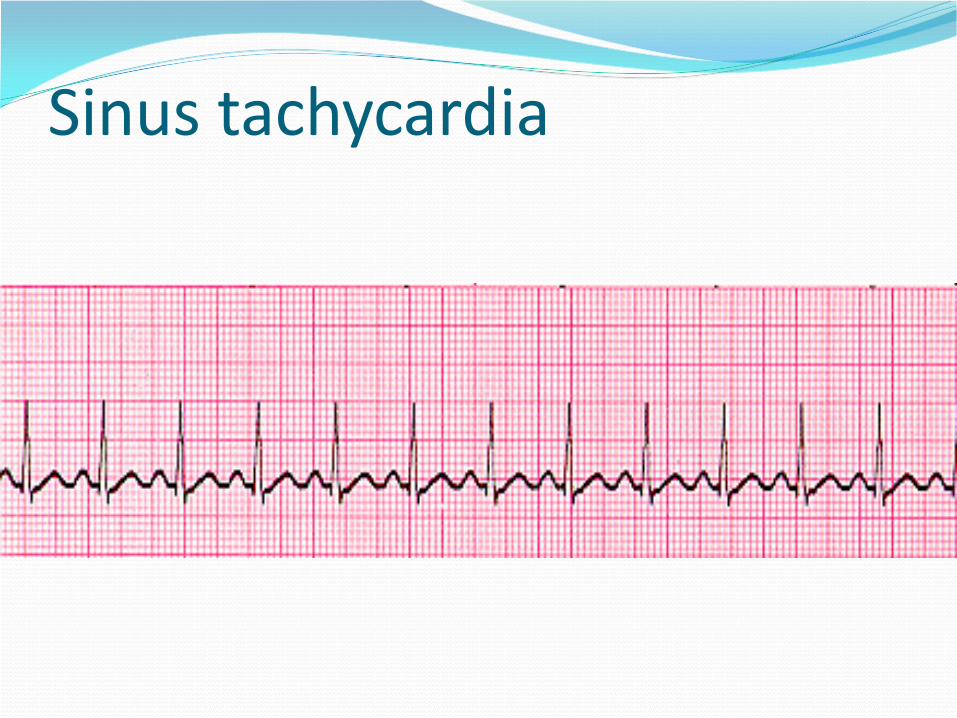
Sinus tachycardia
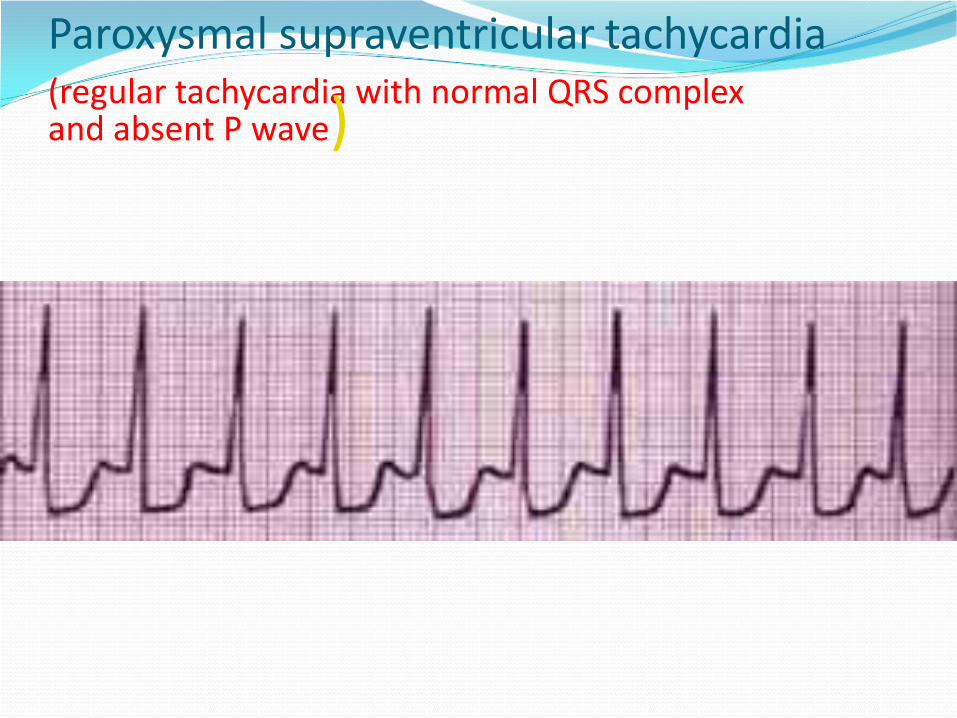
Paroxysmal supraventricular tachycardia(regular tachycardia with normal QRS complex and absent P wave)
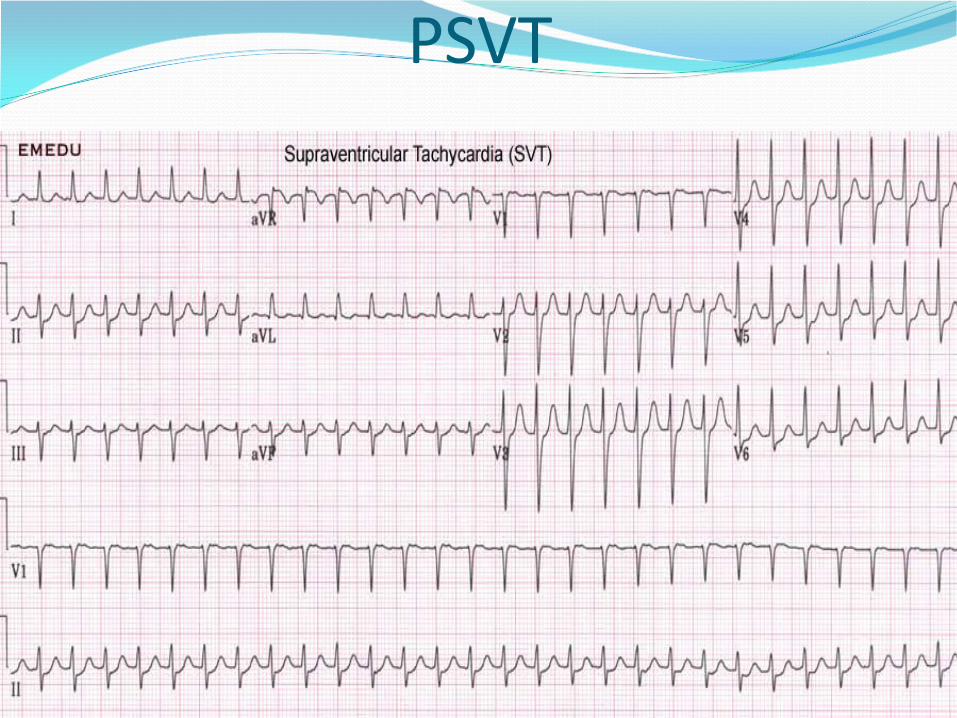
PSVT
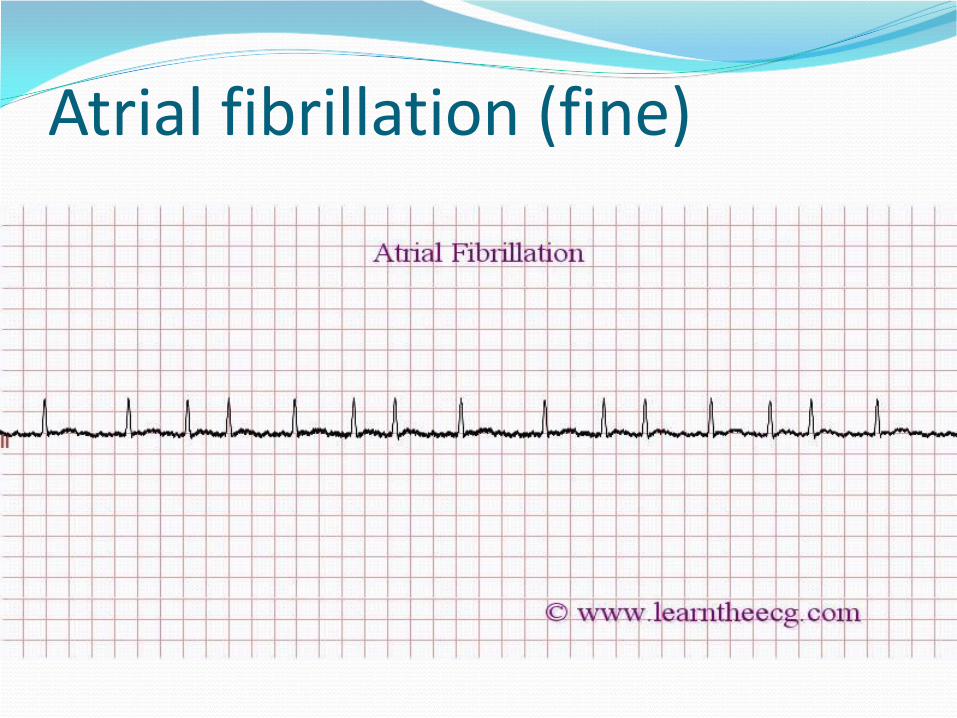
Atrial fibrillation (fine)
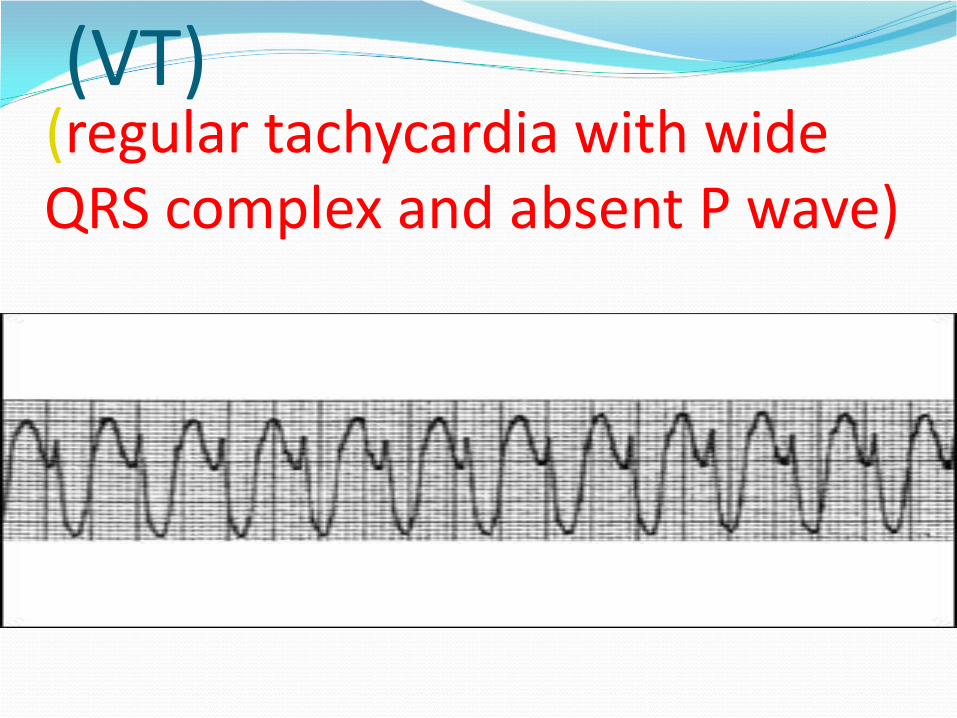
(VT)(regular tachycardia with wide QRS complex and absent P wave)
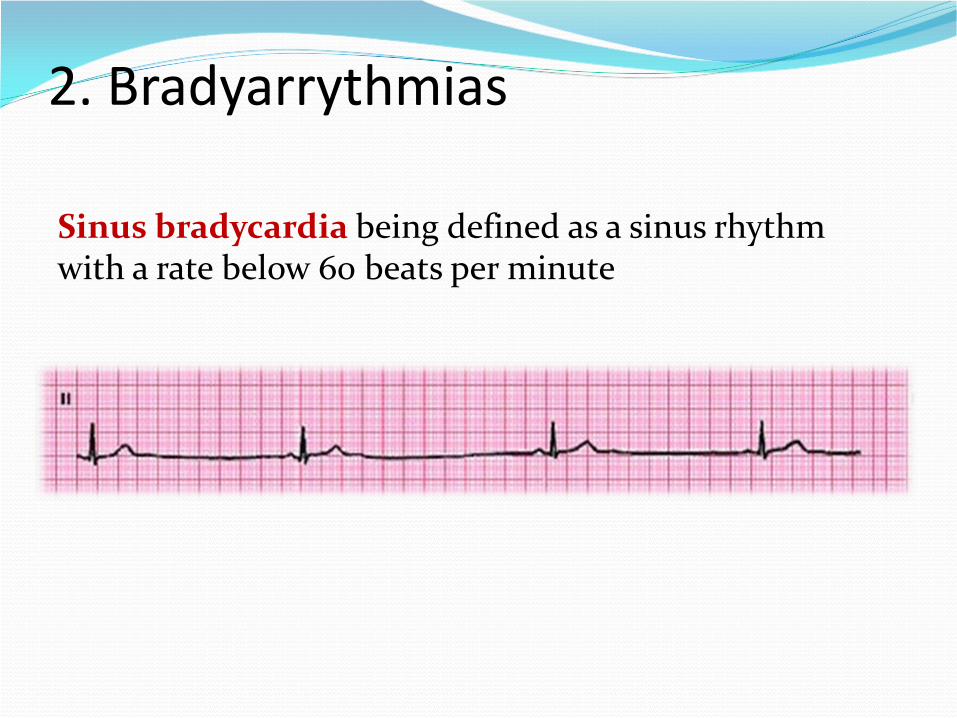
2. Bradyarrythmias
Sinus bradycardia being defined as a sinus rhythmwith a rate below 60 beats per minute
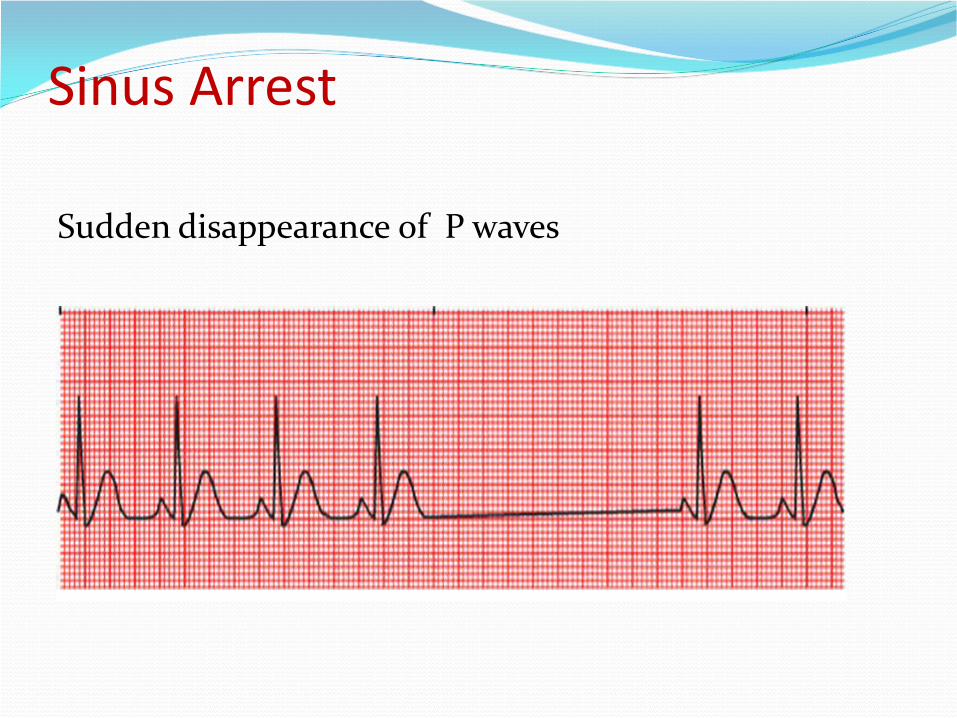
Sinus Arrest
Sudden disappearance of P waves
ATRIOVENTRICULAR (AV) BLOCK
delay or interruption in the transmission of an impulse
from the atria to the ventricles
The conduction disturbance can be transient or
permanent
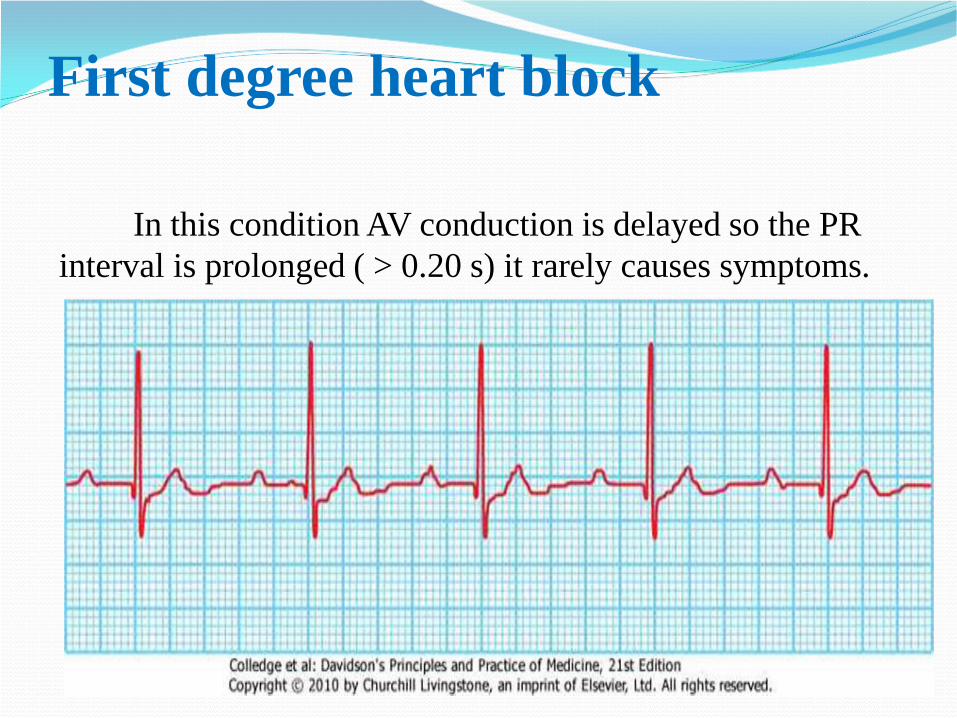
First degree heart block
In this condition AV conduction is delayed so the PR
interval is prolonged ( > 0.20 s) it rarely causes symptoms.
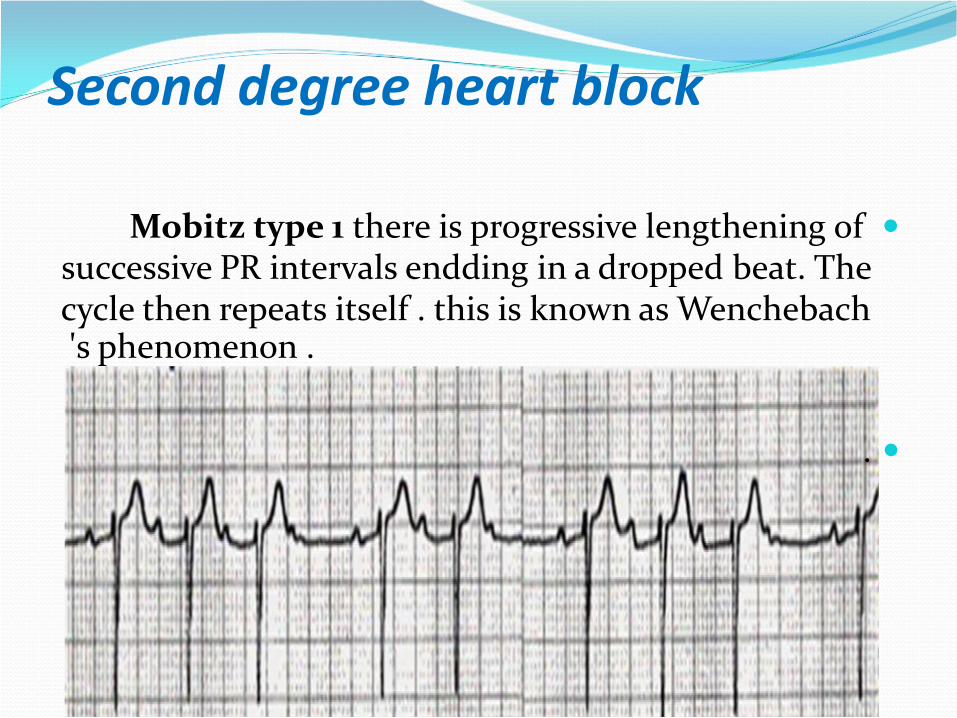
Second degree heart block
Mobitz type 1 there is progressive lengthening of
successive PR intervals endding in a dropped beat. Thecycle then repeats itself . this is known as Wenchebach's phenomenon .
.
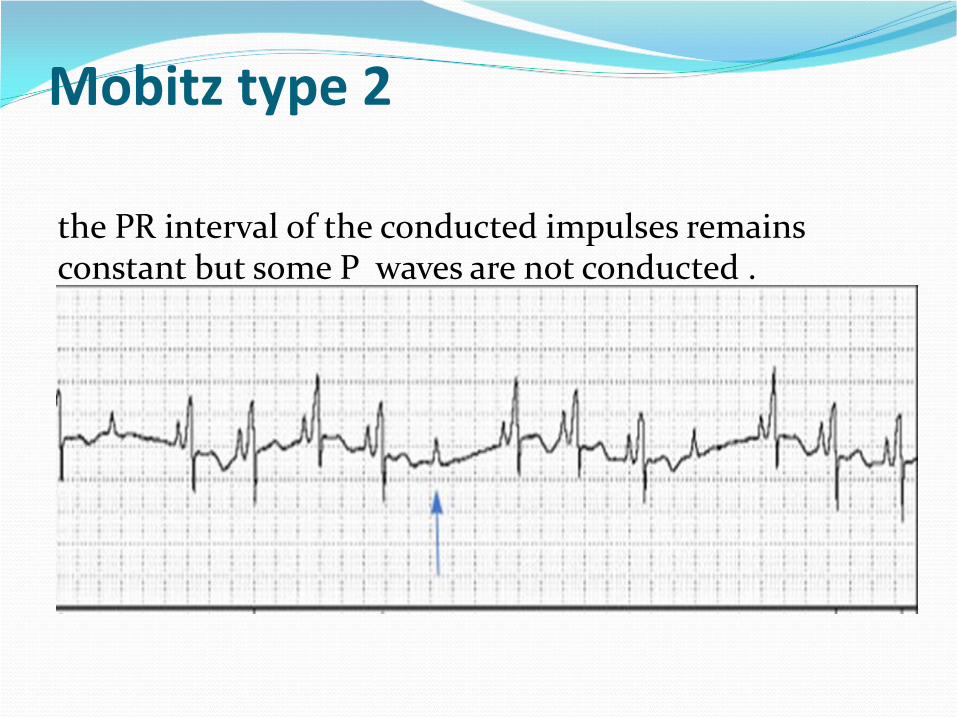
Mobitz type 2
the PR interval of the conducted impulses remainsconstant but some P waves are not conducted .
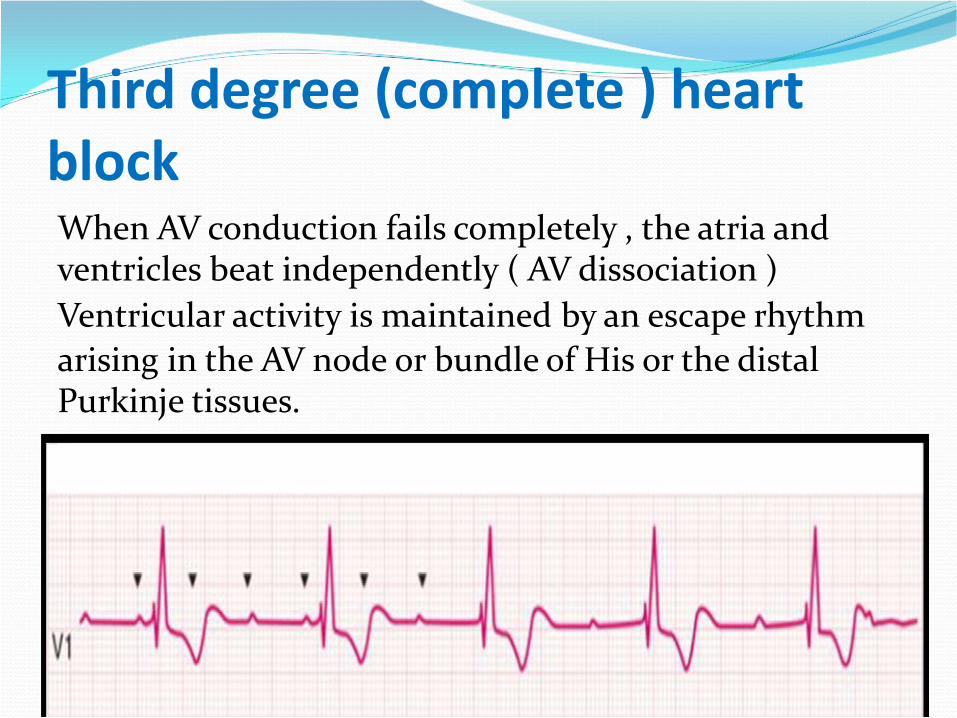
Third degree (complete ) heart block When AV conduction fails completely , the atria and ventricles beat independently ( AV dissociation )
Ventricular activity is maintained by an escape rhythm
arising in the AV node or bundle of His or the distal Purkinje tissues.
ECG in ventricular hypertrophy
LVH ➢
R(v6 or v5)+S(v1+v2) > 3.5 mv(7 LS)
Or R(v6 or v5)> 2.5 mv(5 LS)
RVH ➢
R(v1)≥ 0.5 mv
R/S (v1)≥ 1
S(v5)≥ 0.5 mv




![Electrocardiography - samagra.itschool.gov.in · 2 2 MEDICALUSES theinitialletterPtofollowtheexamplesetbyDescartes ingeometry.[11] Whenamoreprecisewaveformwasob-tainedusingthestringgalvanometer,whichmatchedthe](https://img.pdfslide.us/doc/110x75/5c6b302209d3f262278b6c40/electrocardiography-2-2-medicaluses-theinitialletterptofollowtheexamplesetbydescartes.jpg)