Embed Size (px)
Citation preview

E L E C T R O - N Y S T A G M O G R A P H Y FOR T H E D I A G N O S I S OF VESTIBULAR D Y S F U N C T I O N IN T H E W E R N I C K E - K O R S A K O W S Y N D R O M E
C. Goor, L. J. Endtz and M. d. P. Mullet" KoboM*
SUMMARY
Electro-nystagmography reveals a characteristic picture of spontaneous nystagmus during fixation and disturbed vestibulo-ocular responses to caloric stimulation in the Wernicke-Korsakow syndrome. Only a small number of cases with pontine processes give similar results.
INTRODUCTION
Diagnosis of the Wernicke-Korsakow syndrome may be difficult due to the absence of one or more of the key symptoms and may be virtually impossible when the clinical picture is dominated by other symptoms. The primary cause can also lead to another syndrome as well. For instance, the syndrome may be obscured in alco- holics by delirium tremens, the patient being admitted to a psychiatric instead of a neurologic ward. The undernourishment which is a co-determinant of the syndrome and in rare cases the sole cause (FRANTZEN, 1966) may lead to other, more distinct symptoms. Thus, a comatose alcoholic with electrolyte dysbalance may be admitted to a general rather than a neurologic ward. Finally, the symptoms of the Wernicke- Korsakow syndrome may lead to another disease. For example, hypotension in in the Wernicke-Korsakow syndrome may give rise to tubular necrosis, the patient being assigned to the nephrology department.
The diagnosis Wernicke-Korsakow syndrome is strongly supported by the finding of the biological lesion (PETERS, 1939) with the aid of pyruvate and transketolase determinations. Transketolase values are reported to return to normal within 12 hours to 3 days after thiamine treatment (BRIN, 1962; DREYFUS, 1962; CAMBIER, MASSON, DAIROU, DELACROIX and BOURNIQUE 1973; TRAVIESA, 1974) whereas pyruvate values after glucose loading take between 7 and 14 days to become normal (JOINER, Me ARDLE and THOMPSON, 1950; GILORY, MEYER, BAUER, VULPE and GREENWOOD, 1966). Hence pyruvate determination, though less specific than transketolase determination, may be of help in establishing the diagnosis in some of the patients who have pre- viously received thiamine (MULLER KOBOLD, ENDTZ and LOMBARTS, 1975). But these
* Departments of Clinical Neurophysiology and Neurology, Municipal Hospital Leyenburg, The Hague, The Netherlands.
Clin. Neurol. Neurosurg. 1975-2

113
diagnostic aids cannot be applied in cases where the thiamine defidiency has already disappeared when the Wernicke-Korsakow syndrome is being considered.
Urged by a 16-fold rise in the frequency of the Wernicke-Korsakow syndrome in The Netherlands (MULLER KOBOLO and ENDTZ, 1975) we sought other diagnostic aids. These methods had to be uninfluenced by the degree of cooperation offered by the patient or by previous prolonged treatment with thiamine. It was thought that electro-nystagmography might satisfy these demands.
Vestibular dysfunction was first mentioned as part of the clinical picture in the original descriptions of both Wernicke's disease (1881) and Korsakow's syndrome (1887, 1890). Wernicke mentions nystagmus in his first case and Korsakow explicitly describes it as a 'symptom of cerebral lesion' in his Cerebropathia psychica toxaemica (KORSAKOW 1890). It has since been accepted as a component of both diseases as well as of the Wernicke-Korsakow syndrome, under which name these diseases were united by VICTOR, ADAMS and COLLINS (1971). We have been unable to find any reports on electro-nystagmography in this condition, but GHEZ (1969) investigated the vesti- bular function clinically in 17 patients by means of an icewater caloric test. Ataxia also forms part of the initial descriptions given by Wernicke and Korsakow, and is still accepted as a mayor symptom of the disease. Its diagnostic value for vestibular dysfunction is seriously diminished by the fact that polyneuropathy alone can also cause ataxia (VICTOR et al., 1971).
The present study was undertaken to evaluate electro-nystagmography as a method for the diagnosis of the Wernicke-Korsakow syndrome.
MATERIAL AND METHODS
The subjects, a series of 39 patients showing unequivocally the Wernicke-Korsakow syndrome, were examined by electro-nystagmography (ENG). In all cases the Wernicke-Korsakow syndrome was caused by chronic alcoholism and malnutrition. Thiamine hydrochloride (100 mg daily) was administered intramuscularly after admission, and ENG was performed 3-8 days later. During the last 24 hours before ENG the patients did not receive any medicament except thiamine. None of the patients had impaired consciousness; some were disorientated or confused to varying degrees. Horizontal nystagmus was detected with surface electrodes placed near the inner and outer canthus of both eyes. Recording was done with standard ENG equipment, using a time-constant of 5 seconds and a filter of 15 Hz (3dB).
A voluntary eye movement over 20 degrees was used for calibration of the amplitude of the beats and the angular velocity of the slow phase of the nystagmus.
Spontaneous nystagmus was recorded with the patient supine during forward fixation and fixation of the gaze over 35 degrees to the left and to the right. The measurements with closed eyes were made with the subject in 4 positions: lying supine, on the right side, on the left side, and prone. Caloric stimulation was applied by irrigating both ears with water at 30 ° and 44°C for 30 seconds. If no response was obtained, water at 0°C was also apllied The features of spontaneous nystagmus

114
measured were the frequency, the amplitude, and the angular velocity of the slow phase. The measurements of caloric nystagmus were done during the cumulation period (TOROK, 1957; VFALTZ and GUUCK, 1962) and the duration was also deter- mined. In addition, directional and vestibular preponderance of the caloric nystagmus (JONGKEES and VHmIPSZOON, 1964) were calculated.
The randomly chosen ENGs of 500 non-alcoholic patients recorded over a 10-year period were analysed for comparison with the results of the patients with the Wernicke- Korsakow syndrome.
RESULTS
In all patients nystagmus could be analysed with the eyes in the primary position. With open eyes none of the cases showed nystagmus. With closed eyes 4 of the
@
I ! : '
i;, i i!: ! ' : I i ' i ' ! .
i : t I I i . ; i ! $eci
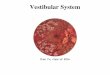
Fig. I. Spontaneous nys- tagmus. Upper trace: fixation of gaze over 35 ° to the left. Lower trace: fixation of gaze over 35 ° to the right.
patients had a nystagmus with a mean frequency of 2.4/sec, an amplitude of 2.7 degrees, and an angular velocity of 8,9°/sec. A pathologic positional nystagmus, i.e. with an angular velocity of more than 5°/sec (VlSSER, 1963), was present in 4 cases. In 30 patients the nystagmus could be examined during fixation over an angle of 35 degrees, the other 9 being too confused for this test. All of these individuals showed a nystagmus with a mean frequency of 3.7/sec, an amplitude of 2.6 °, and an angular velocity of 13.2°/sec.
Caloric stimulation was performed in all 39 patients. Twenty-four of the patients were unresponsive in all caloric tests. In 2 patients responses were only present with water at 0°C. The mean duration of the nystagmus in the other 13 cases was 58 sec. (normal duration: 212 seconds; HAMERSMA, 1957). In none of these cases the lowest recorded value of normal subjects, i.e., 112 seconds (BRASK, 1974), was reached. The mean angular velocity was 10.5°/sec for the patients and for the normal subjects 21°/sec (mNCHCLIFFE, 1967). Significant vestibular preponderance of the angular velocity was present in 3 cases, and directional preponderance in one case.
In the control group hypofunction of the vestibular system comparable with that in Wernicke-Korsakow patients was found in 23 cases. Of these subjects, 6 had a progressive deafness and 6 deafness due to streptomycin administered for tuberculosis.

115
Of the remaining subjects, 4 had a process in the pons, 3 a postcontusional syndrome, and in 4 the origin of the disease was unknown. Of these 11 subjects, 2 had a spon- taneous nystagmus similar to that of the Wernicke-Korsakow patients, one with a pontine tumour the other with a haemorrhage in the pons.
DISCUSSION
Almost all of the clinical descriptions of the Wernicke-Korsakow syndrome mention a spontaneous horizontal nystagmus. The ENG results confirm this symptom. The spontaneous nystagmus appears to be present when the gaze is directed laterally and absent during fixation with the eyes in the primary position. The nystagmus has a small amplitude, a frequency of about 2.4 sec, and is generally symmetrical for the gaze to left and right sides (Fig. 1). In some cases a nystagmus developed in the
V /
i ' [ " ! .
i i i i : I ! s eci.
Fig. 2. Spontaneous nys- tagmus with closed eyes.
primary position when the eyes were closed. This nystagmus was more variable and had a lower frequency (Fig. 2).
Caloric stimulation demonstrated profound abnormalities in the vestibulo-ocular responses with unresponsiveness in 62 ~o and severe hypofunction in the remaining cases. The latter was characterized by a short duration and a low angular velocity of the slow phase of the nystagmus.
Unilateral unresponsiveness, found by GHEZ (1969) in 7 out of 27 cases, did not occur in our series. In his study stimulation was performed with ice-water and the nystagmus was determined by visual observation. The small influence of posture may be related to the symmetry of the vestibular dysfunction.
The question of the frequency of the same ENG abnormalities in other diseases was raised. To answer it, the unselected ENGs of 500 conscious patients without alcoholism were analysed. Of the 23 cases (4.6 ~o) with hypofunction of the vestibular system, 12 (2.3 ~o) had a severe hearing loss and could easily be distinguished from the Wernicke-Korsakow patients, none of whom had a hearing defect. Only the 2 cases (0.4 ~o) with a pontine process had an ENG similar to that of the Wernicke- Korsakow patients. This could be expected, since there are strong indications that in the Wernicke-Korsakow syndrome the thiamine-dependent transketolase is selectively depressed in the pontine region (DREYFUS, 1965) and axonal and synaptic changes occur within the vestibular nuclei (TELLEZ and TERRY, 1968).

116
J
J
p
1 Sec,
Fig. 3. Caloric nystagmus during culmination peri- od. Upper trace: before treatment. Middle trace: after 3 weeks of treatment with thiamine, Lower trace: after l0 weeks of treatment with thiamine. Note increasing angular velocity of the slow phase of the nystagmus.
F r o m these facts it m a y be c o n c l u d e d tha t the E N G f indings in the W e r n i c k e -
K o r s a k o w s y n d r o m e are charac te r i s t i c , and c o n f u s i o n can arise on ly in a ve ry smal l
n u m b e r o f cases wi th p o n t i n e processes . Ser ia l ca lo r i c tes t ing (Fig. 3) m a y be useful
to e v a l u a t e the resul ts o f t h e r a p y wi th t h i amine .
REFERENCES
BRASK, T., FALBE-HANSEN, J. (1974) Electronystagmography on normal persons. Acta oto-laryng. (Stockh.) 77, 412.
BraN, M. (1962). Erythrocyte transketolase in early thiamine deficiency. Ann. N.Y. Acad. Sci. 98, 528. CAMBIER, J., MASSON, M., DAIROU) R., DELACROUX, E. and BOURNIQUE, J. (1973). Evaluation biochimique
de la carence en vitamine B 1. Etude compar6e de la pyruvic6mie et de la transc6tolase. Ann. Mgd. int. 124, 189.
DREYFUS, P. M. 0962) Clinical application of transketolase determinations. N. Engl. J. Med. 267, 596. DREYFUS, P. M. (1965) The regional distribution of transketolase in the normal and the thiamine
deficient nervous system. J. Neuropath. exp. Neurol., 24, l l9. ERANTZEN, E. (1966). Wernicke's encephalopathy in connection with severe malnutrition. Acta neurol.
scand. 42, 426. C, nEZ, ¢. (1969). Vestibular paresis: a clinical feature of Wernicke's disease. J. Neurol. Neurosurg.
Psychiat. 32, 134. G1LROY, J., MEYER, S. S., BAUER, R. B., VULPE, M. and Greenwood, o. (1966) Clinical, biochemical and
neurophysiological studies of chronic interstitial hypertrophic polyneuropathy. Amer. J. Med. 40, 368.
HAMERSMA, H. (1957) The caloric test (thesis). Drukkerij Juten, Bergen up Zoom.

117
HINCHCLIFFE, R. (1967) Normal values for caloric tests using electro-oculography. J. Laryng. 81,221. JOINER, C. L., Me ARDLE, B. and THOMPSON, R. H. S. 0950) Blood pyruvate estimations in the diagnosis
and treatment of polyneuritis. Brain 73, 431. JONGKEES, L. B. W., PHILIPSZOON, A. J. (1964). E lec t ronys tagmography . Acta oto-larying, suppl. 189, I. KORSAKOW, S. S. 0887) Disturbance of psychic function in alcoholic paralysis and its relation to the
disturbance of the psychic sphere in multiple neuritis of non-alcoholic origin (Russian). Vestnik Psichiatrii, 4.
KORSAKOW, S. S. (1890) Ueber eine besondere Form psychischer Sttirung combiniert mit multipler Neurotis. Arch. Psychiat. Nervenkr. 21, 669.
MULLER KOBOLD, M. J. P. and ~NDTZ, L. J. 0975). Her syndroom van Wernicke-Korsakow, een zeld- zaam ziektebeeld? Ned. T. Geneesk. 119, 991.
MULLER KOBOLD, M. J. P., ENDTZ, L. J. and LOMBARTS, A, J. P. E. 0975) Compara t ive value of pyruvate determination after glucose loading and transketolase determination for the diagnosis of the Wernicke-Korsakow syndrome. Clin. Neurol. Neurosurg., 78, 31.
PETERS, R. A. (1936) Biochemical lesion in vitamin B I deficiency; application of modern biochemical analysis in its diagnosis. Lancet i, 1161.
PFALTZ, C., GULICK, R. (1962) Die pathologische calorische Labyrinthreaktion, Arch. klin. exp. Ohr-Nas-Kehlk. Heilk. 179, 525.
TELLEZ, I., TERRY, R. D. (1968) Fine structure of the early changes in the vestibular nuclei of the thiamine deficient rat. Amer. J. Path. 52, 777.
TOROK, N. 0957) The culmination phenomenon and frequency pattern of thermic nystagmus. Acta oto-laryng. (Stockh.) 48, 530.
TRAVIESA, D. C. 0974) Magnesium deficiency: a possible cause of thiamine refractoriness in Wernicke- Korsakow encephalopathy. J. Neurol. Neurosurg. Psychiat. 37, 959.
VICTOR, M., ADAMS, R. D. and COLLINS, C. H. (1971) The Wern icke -Korsakow syndrome, Davis, Philadelphia.
VlSSER, S. L. (1963)Some aspects of evaluating electronystagmographic examination in clinical neuro- logy. Psychiat. Neurol. Neurochir. 66, 24.
WERNICKE, C. (1881) Lehrbuch der Gehirnkrankheiten fur Aerzte und Studierende. Vol. 2, Fischer, Kassel.

![Chapter 3 Wernicke Encephalopathy Definition Wernicke ...is only observed in one-third of patients with Wernicke encephalopathy [1]. Therefore, actually, we accept the definition given](https://img.pdfslide.us/doc/110x75/6014b9b36be08511524bd608/chapter-3-wernicke-encephalopathy-definition-wernicke-is-only-observed-in-one-third.jpg)