Embed Size (px)
Citation preview

ElderTrauma:2012 Update
Robert D. Barraco, MD, MPH, FACS, FCCP
Chief, Geriatric Trauma
Lehigh Valley Health NetworkAllentown, PA

Objectives
■ Describe the epidemiology and physiology of geriatric trauma and its impact on our system.
■ Discuss recent literature in the area of geriatric trauma.

Committee Update
NO ONEIN THIS ROOM
IS GETTING YOUNGER


Background■ Injury rates are
rising ■ 38% of inpatients
were aged 65 years and over, 43% days of care
■ Those aged 75 years and over 24% of all inpatients
Source: NHDS

Epidemiology
■ Trauma is the 5th leading cause of death in the elderly
– In order of most to least common:• Falls• MVC• Pedestrian struck• Stab wounds• Gunshot wounds• others

Mechanism of Injury
■ Falls– Most common method of injury in the
elderly– Most responsible for cause of death– By 2020, 47.8 billion dollars spent on the
treatment of geriatric falls

Mechanism of Injury
■ Motor Vehicle Crash– MVC are #1 cause of trauma related
cause of death ages 65-74– In accidents involving elderly patients
• 80% were found to be at fault• 18% syncopal episode was the inciting agent

Mecahnism of Injury
■ Pedestrian struck by MV– Involves the elderly more than any other
age group.– Cause
• Confusion• Vision or hearing deficiency• Poor gait

Bodily Changes:Sunset or Sunrise?
■ Changes in all body systems■ Less reserve■ Relatively unable to compensate■ Physical exam findings unreliable

Nervous System
■ Sensory decline■ Motor decline■ Memory impairment■ Impaired
temperature/ blood pressure control
■ Sleep changes

Cardiovascular System
■ Stretch of cardiac muscle
■ Atherosclerosis: Hardening of the arteries
■ Can’t compensate with heart rate
■ Fat in-growth of SA and AV nodes

Respiratory System
■ Stiffening of chest wall and lung
■ Oxygen ■ amount of air with
maximal breath■ Work of respiratory
muscles

Urologic System
■ Kidney failure■ Drug clearance
and processing■ Response to
dehydration

GI System
■ Swallowing problems
■ Reflux■ Diverticuli

Immune System
■ Cancer■ Autoimmune
disease like Rheumatoid Arthritis
■ Infections/ complications

Endocrine System
■ Reduced ability to respond to stress
■ Loss of glucose tolerance leads to diabetes

Bones, Joints and Muscles
■ Muscle strength, endurance and size
■ Osteoporosis■ Fractures■ Joint disease■ Osteoarthritis




2001 2002 2003 2004 2005 2006 2007 2008 2009 20100
2000
4000
6000
8000
10000
12000
14000
0.0
2.0
4.0
6.0
8.0
10.0
12.0
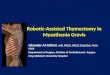
% Mortality By Year for All State Registry Patients Age 65 and Older
Total pts Percent
To
tal
Pat
ien
ts
% M
ort
alit
y

Factors affecting outcome and mortality in Eldertrauma

2001■ Triage Issues■ Parameters (End Points) for
Resuscitation
2010■ Correction of anti-coagulation■ Age as indicator for trauma alert■ Supraphysiologic Resucitation

What is “Elderly”?
Level II
In general, where specific guidance is not otherwise given for the purposes of determining independent risk for adverse outcomes following trauma, patients >65 years of age can be considered as “elderly”.

Prehospital Triage and Activation
Level II■ Injured patients with advanced age (>65) and
pre-existing medical conditions (PEC’s) should lower the threshold for field triage directly to a designated/verified trauma center.

Prehospital Triage and Activation
Level III■ A lower threshold for trauma activation should
be utilized for injured patients>70 years age who are evaluated at trauma centers.
■ Elderly patients with at least one body system with an AIS>3 should be treated in designated trauma centers, preferably in ICU’s staffed by surgeon-intensivists.

Literature Support: Trauma Center Triage/Care

Effectiveness of Prehospital Trauma Triage…
■ Retrospective study■ Three NJ counties with Level 1 trauma
centers■ 18% undertriage in elderly men, 15% in
elderly women■ Age cutoff 65 years
J Emerg Nursing 2003; 29:109-15

Old Age as a Criterion for Trauma Activation
■ Retrospective review 7.5 years■ Level 1 urban trauma center■ 25% of age 70 and over met one standard
criteria– Mortality 50%, ICU 40%, OR 35%
■ 75% not meet criteria– Mortality 16%, ICU 24%, OR 19%
■ Age 70 a stand alone criteria for activation
J Trauma 2001 Oct; 51(4): 754-6

Should Age be a Factor…
■ NTDB review■ At all levels of injury, patients older than
60 have 3 fold increased morbidity and 5 fold increased mortality with minor ISS (0-15), 2- and 4-fold with major ISS.
■ Minor ISS were often Level II activations
■ Suggests Level 1 activation age 60 and over
J Trauma Issue/Volume 69(1), July 2010, pp 88-92

The impact of advanced age on trauma triage decisions and outcomes:
a statewide analysis
■ 13,820 (27%) elderly patients. ■ Significantly less likely trauma team
activation despite similar severity■ More often required urgent craniotomy
and orthopedic procedures ■ Undertriaged elderly patients had 4
times the mortality rate
Am J Surg. 197(5):571-4; discussion 574-5, 2009 May.

Undertriage of elderly trauma patients to state-designated trauma centers
■ Even when trauma is recognized and acknowledged by EMS, providers are consistently less likely to consider transporting elderly patients to a trauma center.
Arch Surg. 143(8):776-81; discussion 782, 2008 Aug.

Elderly Injury: A Profile of Trauma Experience in the Sunshine (Retirement)
State
■ In the moderate and minor injury categories, TC survival was significantly better for both groups.
■ The proportion of NTC fatalities as potentially preventable is significantly higher than trauma centers.

Elderly Injury: A Profile of Trauma Experience in the Sunshine (Retirement)
State■ When the effects of all reported
diagnoses are considered, potentially preventable mortality for patients with noninjury comorbidity is significantly lower in TC.
■ Moreover, by using “discharge to home” as an indicator of completeness of recovery, TCs seem to be significantly more effective than NTC
The Journal of Trauma: Issue: Volume 48(4), April 2000, pp 581-586

Trauma in the very elderly: a community-based study of outcomes at trauma and
nontrauma centers
■ Head injury, injury severity, and lack of TC verification are associated with hospital mortality in very elderly trauma patients.
J Trauma. 52(1):79-84, 2002 Jan.

AnticoagulationLevel III■ All elderly patients who receive daily therapeutic
anticoagulation should have appropriate assessment of their coagulation profile as soon as possible after admission.
■ All elderly patients with suspected head injury receiving daily anticoagulation should be evaluated with head CT as soon as possible after admission.
■ Patients receiving warfarin with a post-traumatic intra-cranial hemorrhage should receive initiation of therapy to correct their INR toward a normal range within 2 hours of admission.

PTSF Geriatric Trauma Committee
Vision: Pennsylvania’s Trauma System will pioneer and excel in the care of the injured elderly.
Goals:■ Evaluate/Examine Best Practices in Geriatric Trauma Care in
the Commonwealth■ Limit variation and improve outcomes through standardization
of care■ Discuss and resolve issues of importance to the care of the
Geriatric Trauma Patient■ Evidence-Based Reviews as available or create our own to
guide care■ Research to provide tools to change practice and provide the
best care to our community■ Trauma Systems approach to issues

Definition
■ Geriatric trauma will be defined in the Commonwealth of Pennsylvania as injured patients age 65 and over.

PTSF Geriatric Trauma Committee
On the agenda: ■ Best practices/usable protocols■ Interfacility standard work:
– Common protocols for clinical situations• Anticoagulant reversal• Syncope
■ Triage■ Prevention Initiatives

Coumadin and CHI protocol:Non-trauma vs. Level 3/4
Mechanism for Head Injury and taking Coumadin:
GCS < 14?
Stat PT/INR/PTTType and Cross
Obtain stat head CT with stat read
Transfer to Level 1 or 2 trauma center
Begin correction as able
YesNo
Injury on CT?
Admit, observeConsider CT in AM
No
Yes
Mechanism for Head Injury and taking Coumadin:
Able to obtain stat head CT and read it?
Stat PT/INR/PTTType and Cross
Stat head CT with stat readSee Level 3-4 algorithm
Transfer to Level 1 or 2 trauma center
Yes No

Geriatric Triage Research
■ No denominator■ Need to see if numbers would
overwhelm resources■ Rich database of PCRs with PEHSC■ Will look at data points for answers at
state level■ Will use locoregional EMS if needed

Geriatric Issues in Trauma Care

Frailty

AAST 2011
■ PREDICTORS OF CRITICAL CARE RELATED
COMPLICATIONS IN COLECTOMY PATIENTS USING THE
NATIONAL SURGICAL QUALITY IMPROVEMENT
PROGRAM: EXPLORING FRAILTY AND AGGRESSIVE
LAPAROSCOPIC APPROACHES.
■ ARE THE FRAIL DESTINED TO FAIL?: FRAILTY INDEX AS
A PREDICTOR OF SURGICAL MORBIDITY AND
MORTALITY IN THE ELDERLY

Surgery in the Elderly
■ 21% of those over age 60 will undergo surgery and anesthesia as compared with only 12 percent of those aged 45 to 60 years by 2030
■ 20% of all open heart surgery >70

Surgery in the Elderly
■ Overall risk steadily declining
■ Heart disease mortality 3-5%
■ Heart attack 1-4%■ CHF 4-10%■ Lungs most
common: 15-45%

Frailty
■ Unintentional weight loss (10 pounds or more in a year)
■ General feeling of exhaustion ■ Weakness (as measured by grip strength) ■ Slow walking speed ■ Low levels of physical activity.

Trauma in the Elderly: Frailty
■ Frailty Scales: Measure thinking, functionality and general health status.
■ Higher scores were associated in increased complications and decreased chance of being discharged to home.

VES-13
■ The VES-13 relies on patient self-report.■ VES-13 is function-based. ■ In the national sample of elders, a score of 3+
identified 32% of individuals as vulnerable. ■ This vulnerable group had four times the risk
of death or functional decline when compared to elders scoring 3 or less.


Frailty Outcomes
■ Increasing frailty was associated with postoperative complications, increased length of hospitalization and inability to be discharged home independent of age.
■ EFS scores of 3 or less were associated with a lower risk of having a complication and a higher chance of being discharged home.
■ EFS scores exceeding 7 were associated with increased complications and a lower chance of being discharged home.


Cardiac evaluation
■ Diagnostic testing in at risk patients■ EKG, Stress, Cath■ Assign risk, NOT CLEAR■ Recommendations
– Statins, Beta blockers– Perioperative monitoring

Putting it all together…

Preoperative Risk Assessment■ What is missing?
– Medications– Frailty evaluation– Optimization beyond Cardiac
■ Utilizing VES-13 as part of preop screen to undergo Comprehensive Geriatric Assessment, more accurate prognostication and optimization
■ Journal of the American College of Surgeons Recommendations

Models of Care: CGA
■ Geriatrics-focused interdisciplinary management of older adults can be grouped into 2 models of care:
– Geriatric evaluation and management (GEM), in which the interdisciplinary team actively follows up on the patient and directs medical care
– Comprehensive geriatric assessment (CGA), in which the consultative interdisciplinary team makes specific recommendations to the patient’s primary care provider rather than directly implementing care

Using nurse practitioners to implement best practice care for the elderly during
hospitalization: the NICHE journey at the University of Virginia Medical Center
■ Nurses Improving Care for Hospitalized Elders
■ These include the Geriatric Resource Nurse model, the Acute Care of the Elderly model, and, most recently, the Geriatric Consultation Service model.
Critical Care Nursing Clinics of North America. 19(3):321-37, vii, 2007 Sep.

NICHE Models at UVA■ Nurse practitioners (NPs) with geriatric
expertise have provided the leadership in implementing these initiatives to achieve the goal of improving geriatric care delivery within the health system.
■ Each NP functions in a broad role that is tailored to meet the needs of the patients and staff and includes the role components of clinician, educator, team leader, and care coordinator.

Models of Care: ACE
■ Geriatrician-led interdisciplinary team approach
– Improve functional status, reduce acute care hospital days and readmission, and lower mortality rate in hospitalized acutely ill frail older patients
■ Acute Care of the Elderly (ACE) unit– More homelike environment– Patient-centered care that includes plans for
preventing disability and iatrogenic illness, and comprehensive discharge planning and management

Models of Care: ACE
■ ACE Units bring evidence-based practices to hospital care
– Better patient outcomes – Better staff retention
■ Geriatric Resource Nurses are a relatively low-cost option for putting aging knowledge across units and clinics.

Models of Care: ACE
■ Geriatrics expertise, when coupled with high-margin procedures can lead to better patient outcomes and shorter stays in hospital.
– Better margins– Better downstream revenues– Competitive edge in recruiting patients

Treatment
■ Exercise and geriatric interdisciplinary assessment and treatment models improve outcomes

Delirium

Delirium: History
■ First century AD - mental disorders during fever or head trauma
■ Current - transient, reversible syndrome that is acute and fluctuating, and which occurs in the setting of a medical condition

Delirium: Epidemiology
■ Incidence - 14–56% of all hospitalized elderly patients.
■ Postoperative delirium - in 15–53% of surgical patients over the age of 65
■ 70–87% of elderly in the ICU■ At least 20% of the hospitalized patients
over 65 each year in the US experience complications due to delirium

Delirium: FactorsPotentially modifiable risk
factors■ Sensory impairment (hearing
or vision) ■ Immobilization (catheters or
restraints) ■ Medications ■ Acute neurological diseases ■ Intercurrent illness ■ Metabolic derangement ■ Surgery ■ Environment ■ Pain ■ Emotional distress ■ Sustained sleep deprivation
Nonmodifiable risk factors
■ Dementia or cognitive impairment
■ Advancing age (>65 years) ■ History of delirium, stroke,
neurological disease, falls or gait disorder
■ Multiple comorbidities ■ Male sex ■ Chronic renal or hepatic
disease

Diagnosing Delirium

CAM and CAM-ICU
■ Form■ Algorithm■ Video■ Website: icudelirium.org

Delirium: Imaging
■ CT scan: marked cortical atrophy in the prefrontal cortex, temporoparietal cortex, and fusiform and lingual gyri in the nondominant hemisphere, and atrophy of deep structures,
■ Reflect a state of increased vulnerability of the brain to any insult

Delirium: Prevention
■ 30–40% of cases of delirium are preventable ■ Beers Criteria drugs should be avoided■ The Hospital Elder Life Program (HELP)
uses tested delirium prevention strategies to improve overall quality of hospital care.

Inappropriate Medications in the Elderly
■ 30 percent of hospital admissions in elderly patients may be linked to drug-related problems or toxicity
■ Overall human and economic consequences of medication-related problems vastly exceed the findings of the Institute of Medicine (IOM) on deaths from medical errors
■ In 2000, it is estimated that medication-related problems caused 106 000 deaths annually at a cost of $85 billion.
■ Fifth leading cause of death in the United States

Beers Criteria
■ The Beers List: Potentially Inappropriate Medications for the Elderly
■ CBC News In Depth: Drugs seniors should avoid - The Beers criteria

Delirium: Prevention
■ In a controlled trial that evaluated HELP, delirium developed in 9.9% of the intervention group, compared with 15.0% of the usual-care group
■ The HELP interventions can also effectively reduce the total number of episodes and days of delirium
■ Proactive geriatric consultation reduces risk of delirium after acute hip fracture by 40%

Delirium: Treatment
■ Reorientation and behavioral intervention. ■ Caregivers should use clear instructions and
make frequent eye contact with patients. ■ Sensory impairments, such as vision and
hearing loss, should be minimized ■ Physical restraints should be avoided
because they lead to greater risk of injury and prolongation of delirium

Delirium: Treatment
■ An environment with minimal noise at night■ Nonpharmacological sleep protocol
– First, a glass of warm milk or herbal tea– Second, relaxation tapes or relaxing music– Third, back massage
■ Reduced the use of sleeping medications from 54% to 31%

Fong TG et al. (2009) Delirium in elderly adults: diagnosis, prevention and treatment Nat Rev Neurol doi:10.1038/nrneurol.2009.24

Summary
■ Delirium is a serious cause and complication of hospitalization in elderly patients and should be considered to be a medical emergency until proven otherwise.
■ Potential to markedly affect the overall outcome and prognosis of severely ill patients, as well as substantially increasing health-care utilization and costs.

“ The alleviation of suffering is the warrant of medicine and its test of
adequacy…it is a test that contemporary medicine fails despite the brilliance of its science and its
awesome technical power”Eric J. Cassell, J Clin Ethics. 1991; 2(2): 81-82

What is Palliative Care?
■ Good patient care■ Caring for terminally-ill patients and
their families■ Aggressive symptom management
– Primary goal
■ Communication■ Spirituality

Curative vs. Palliative Models
■ Primary goal is cure
■ Object is disease■ Symptoms treated as
clues■ Measurable data■ Devalue subjective■ Therapy indicated if cures
or slows■ Patient’s body different
from mind■ Death is failure
■ Primary goal relief of suffering
■ Object is patient/family■ Symptoms treated as
entities in themselves■ Subjective is valued;
patient’s experience■ Therapy if relieve
suffering■ Patient a complex of
physical, emotional, social and spiritual
■ Live fully and comfortably till death a success

What Palliative Care is Not…
■ End-of-Life Care■ Withdrawal of
Care■ Do not Treat■ Giving up

“ A medicine that embodies an acceptance of death would represent a great change in the common conception, and might set
the stage for viewing the care of dying people not as an afterthought when all
else has failed but as one part of the ends of medicine.”
Daniel Callahan, from The Troubled Dream of Life

Five Basic Palliative Care Interventions
■ Control Pain and other Distressing Physical Symptoms
■ Alleviate Psychosocial Problems■ Communicate Effectively■ Empathic Presence■ Foster Hope

“We are a culture that denies death…therefore we are all
walking towards death backwards! It is better to turn around.”
Michael Meade

Geriatric Trauma Data:LVH CC

Beers’ Criteria Medications
■ Preliminary data■ Compared one year prior to
implementation to 4 and 6 years after■ 7.6% reduction in patients discharged
on Beers’ meds■ 20.8% increase in patients taken off
Beers’ meds

Geriatric Trauma Data LVH CC
10.410.6 11.3
ISS11
13.7

Geriatric Mortality Comparison2006-2009
Alive Dead
LVHNISS 13.7
3811 212 (5.6%)
State (adjusted)ISS 12.5
32047 1931 (8.5%)


Fong TG et al. (2009) Delirium in elderly adults: diagnosis, prevention and treatmentNat Rev Neurol doi:10.1038/nrneurol.2009.24

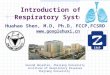
Frailty domain Item 0 Point 1 Point 2 Points
Cognition
Please imagine that this pre-drawn circle is a clock. I would like you to place the numbers in the correct positions then place the hands to indicate a time of ‘ten after eleven’
No errors Minor spacing errors Other errors
General health status
In the past year, how many times have you been admitted to a hospital?
0 1–2 ≥2
In general, how would you describe your health?
Excellent/Very good/Good
Fair Poor
Functional independence
With how many of the following activities do you require help? (meal preparation, shopping, transportation, telephone, housekeeping, laundry, managing money, taking medications)
0–1 2–4 5–8
Social supportWhen you need help, can you count on
someone who is willing and able to meet your needs?
Always Sometimes Never
Medication use
Do you use five or more different prescription medications on a regular basis?
No Yes
At times, do you forget to take your prescription medications?
No Yes
NutritionHave you recently lost weight such that your
clothing has become looser?No Yes
Mood Do you often feel sad or depressed? No Yes
ContinenceDo you have a problem with losing control of
urine when you don't want to?No Yes
Self-reported performance
Two weeks ago were you able to:
(1) Do heavy work around the house like washing windows, walls or floors without help?
Yes No
(2) Walk up and down stairs to the second floor without help?
Yes No
(3) Walk 1 km without help? Yes No
Not Frail 0–5Apparently Vulnerable 6–7Mild Frailty 8–9 Moderate Frailty 10–11Severe Frailty 12–18
REFS

Importance of a Comprehensive Geriatric Assessment in Prediction of Complications
Following Thoracic Surgery in Elderly Patients
■ Dependence for the performance of ADLs and impaired cognitive conditions are important predictors of postoperative complications, especially when the operation time is long. CGA is necessary in addition to the conventional cardiopulmonary functional assessment in elderly patients.

Geriatric Trauma Data Query
January 1, 2011- July 30, 2011

Queried EMS patient care reports for patients age 65 and older with the following reported causes of injury:◦ Fall◦ Pedestrian Struck◦ Motor Vehicle Accident
27,009 Records Returned
Geriatric Trauma Data



3
4
5
6
7
8
9
10
11
12
13
14
15
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90
0.72
0.09
0.09
0.26
0.14
0.27
0.40
0.40
0.82
1.20
2.17
12.31
81.16
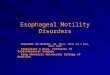
22144 (82%) Records Reported GCS Score
Percentage of Total Reported
GC
S S
core



Requirement Level 1 Level 2 Level 3
Interdisciplinary care E E D
Geriatrician as liaisonInternist/family
medicine/rehab medicine interested in geriatrics as liaison
D D D
Geriatric Resource Nurse(1 FTE if >1000/yr)
D D D
Geriatric PI E E D
Palliative Care program D D D
Geriatric Education E (may be internal) E (may be internal) E
Geriatric prevention E E D
Geriatric Trauma Chief E E D
Geriatric Standards

Fong TG et al. (2009) Delirium in elderly adults: diagnosis, prevention and treatmentNat Rev Neurol doi:10.1038/nrneurol.2009.24
Relationships between various etiological factors in delirium

Symptom ManagementPatient Centered GoalsConcordance between patient, caregiver, Healthcare team
Frailty
screen
Exercise
TX
CGA
and TX
PACE
outpt
ACE
inpt
Hospice and
Palliative
Care
Comfort
and Dignity