Embed Size (px)
Citation preview
DIABETE ET RESISTANCE AUX ANTI-PLAQUETTAIRES
QUELS OUTILS DE DEPISTAGE?
I. ELALAMY
UNITE HEMOSTASE-THROMBOSE
HOPITAL TENON – UR2 UPMC
PARIS
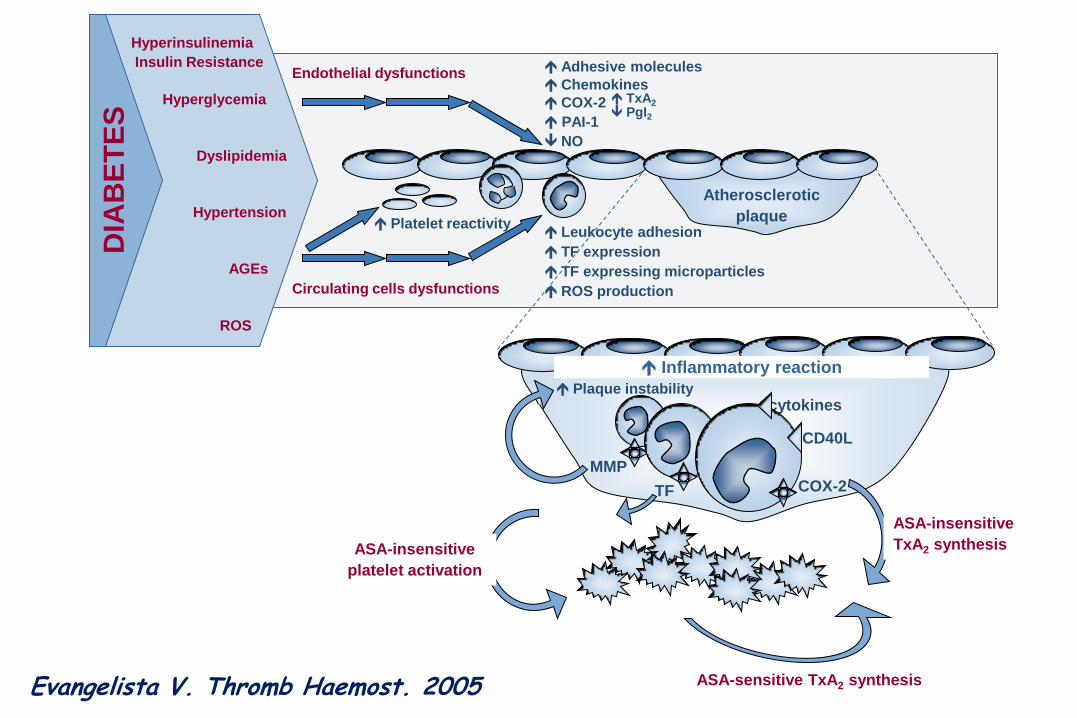
cytokines
CD40L
Inflammatory reaction
MMP
TF
COX-1TxA2
Thrombin
ASA-insensitive
platelet activation
ASA-sensitive TxA2 synthesis
ASA-insensitive
TxA2 synthesis Platelets
AGEs
ROS
Hyperglycemia
Hyperinsulinemia
Insulin Resistance
Dyslipidemia
Hypertension
DIA
BE
TE
S
Platelet reactivity Leukocyte adhesion
TF expression
TF expressing microparticles
ROS production
Endothelial dysfunctions Adhesive molecules
Chemokines
COX-2 TxA2
PgI2
NO
PAI-1
Circulating cells dysfunctions
Atherosclerotic
plaque
Plaque instability
COX-2
Evangelista V. Thromb Haemost. 2005
RÉSISTANCE OU ECHEC DU TRAITEMENT : UNE AFFAIRE D’ÉTAT … PLAQUETTAIRE?
« PLAQUY FAIT DE LA RÉSISTANCE »
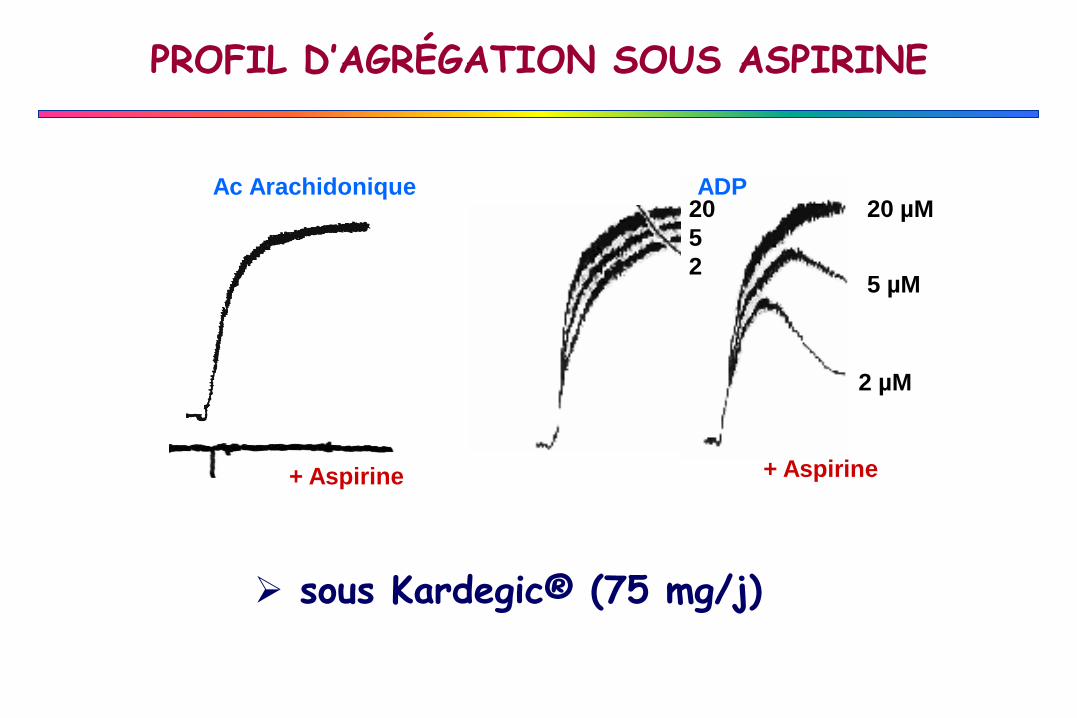
PROFIL D’AGRÉGATION SOUS ASPIRINE
+ Aspirine
Ac Arachidonique ADP
+ Aspirine
20 µM
5 µM
2 µM
20
5
2
sous Kardegic® (75 mg/j)
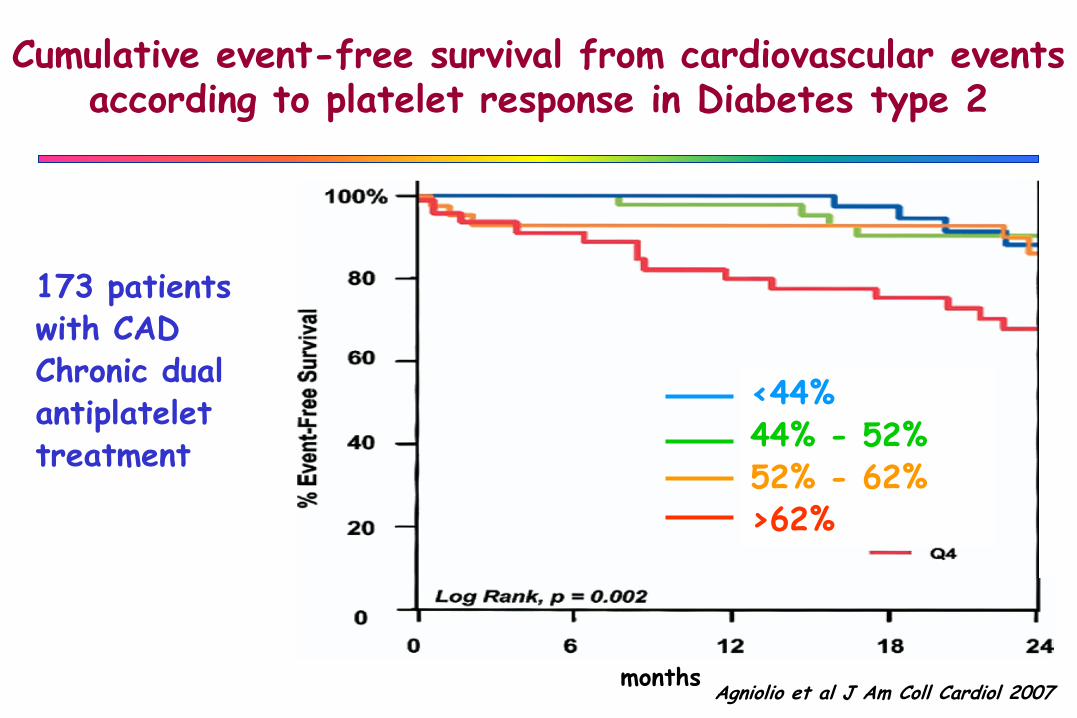
<44%44% - 52%52% - 62%>62%
months
Cumulative event-free survival from cardiovascular events according to platelet response in Diabetes type 2
173 patients with CADChronic dual antiplatelet treatment
Agniolio et al J Am Coll Cardiol 2007
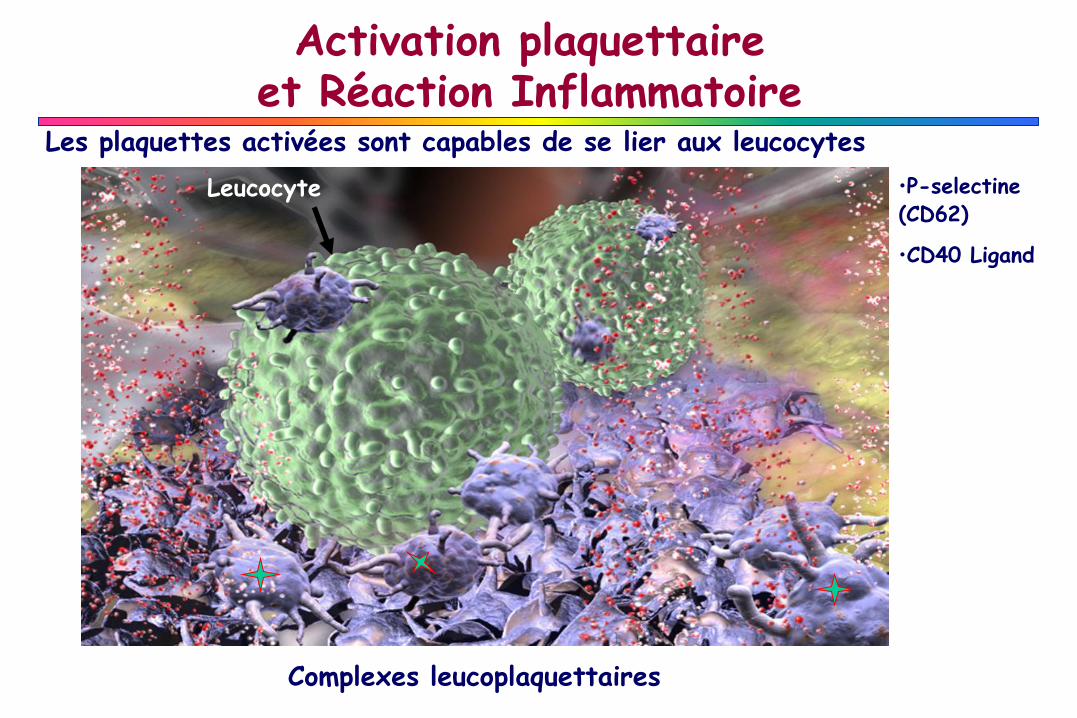
Activation plaquettaireet Réaction Inflammatoire
Les plaquettes activées sont capables de se lier aux leucocytes
Complexes leucoplaquettaires
•P-selectine (CD62)
•CD40 Ligand
Leucocyte
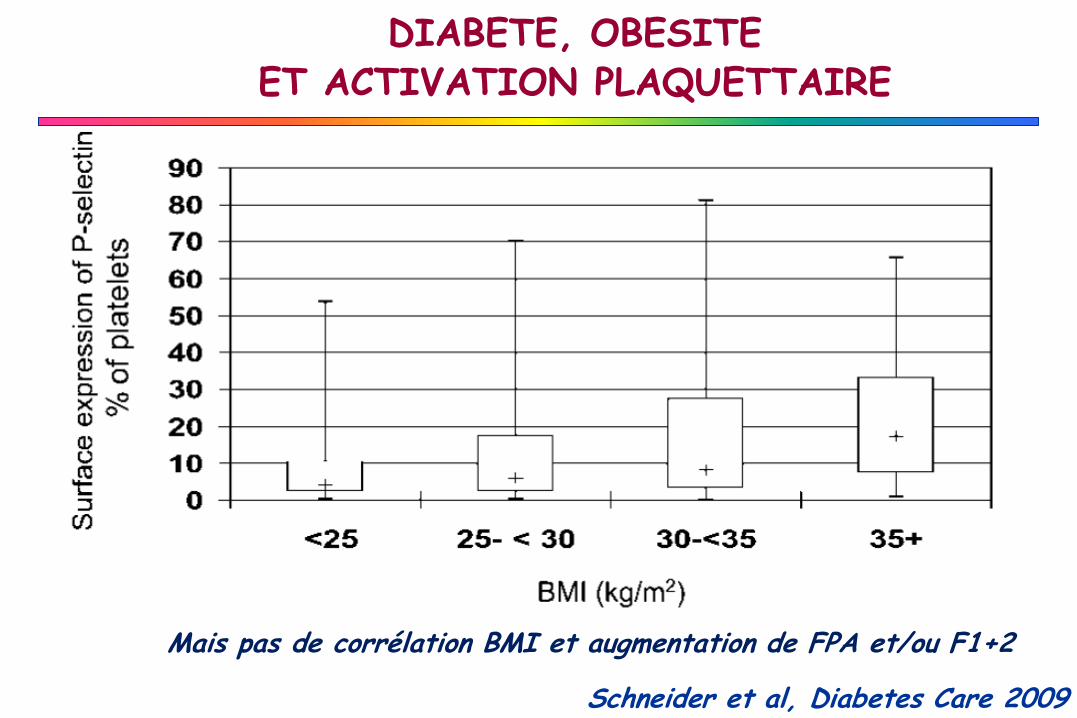
DIABETE, OBESITE ET ACTIVATION PLAQUETTAIRE
Schneider et al, Diabetes Care 2009
Mais pas de corrélation BMI et augmentation de FPA et/ou F1+2
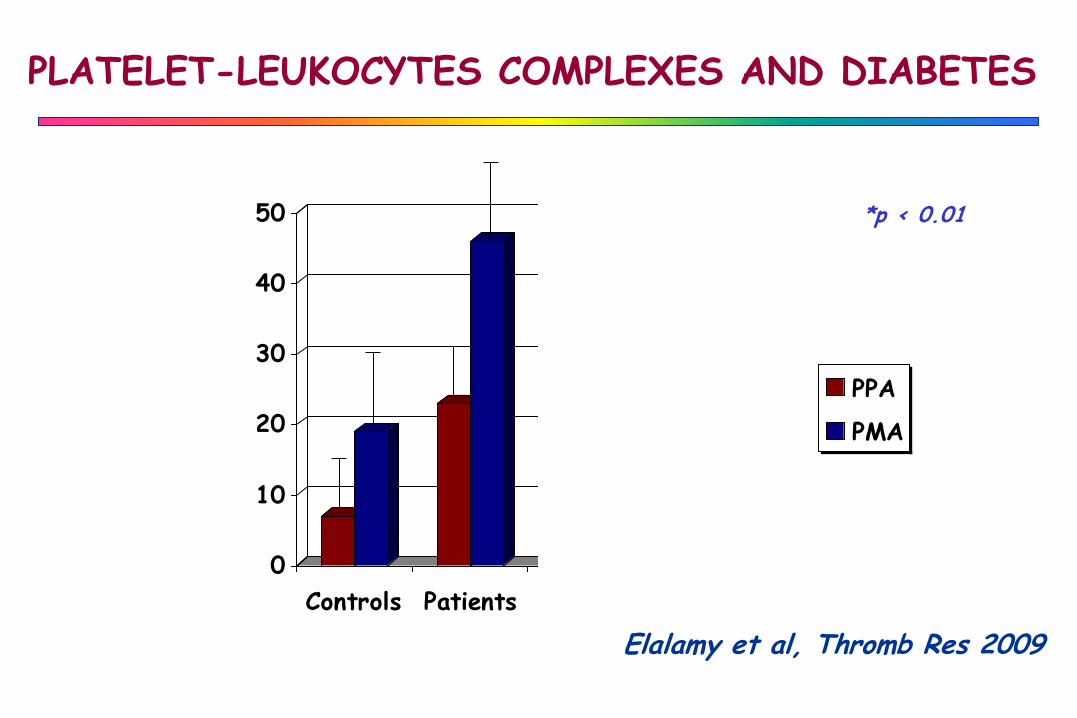
PLATELET-LEUKOCYTES COMPLEXES AND DIABETES
*p < 0.01
*
0
10
20
30
40
50
Controls Patients Type 1 Type 2
PPA
PMA
*
**
*
*
Perc
ent
age
%
Elalamy et al, Thromb Res 2009
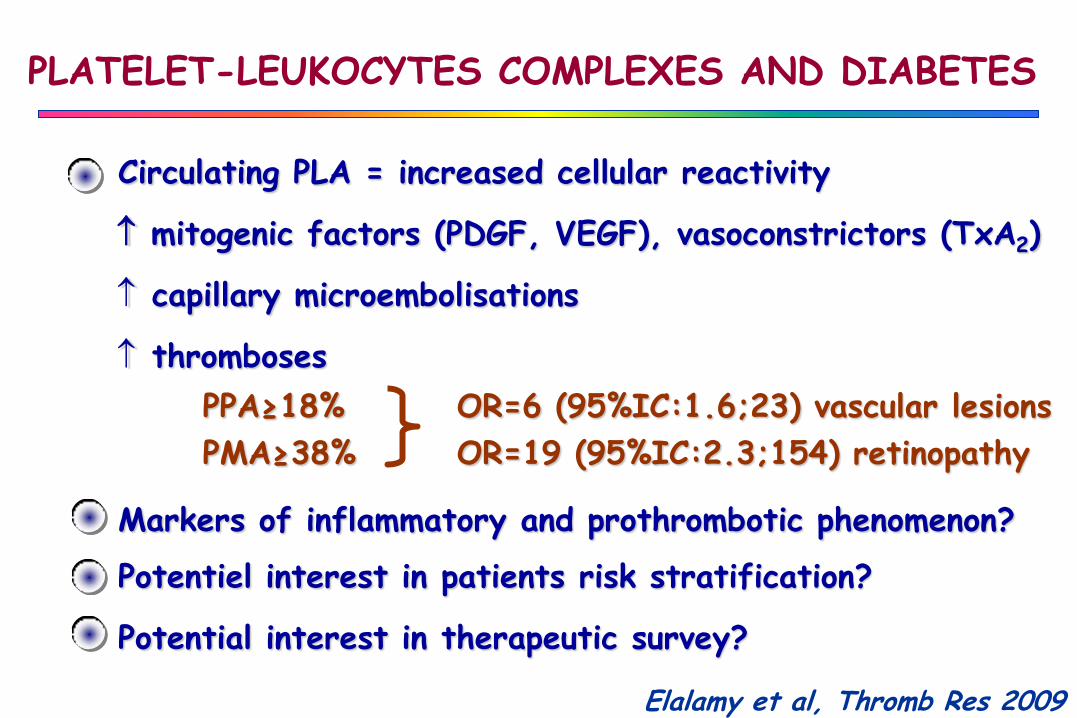
Circulating PLA = increased cellular reactivity
mitogenic factors (PDGF, VEGF), vasoconstrictors (TxA2)
capillary microembolisations
thromboses
PPA≥18% OR=6 (95%IC:1.6;23) vascular lesions
PMA≥38% OR=19 (95%IC:2.3;154) retinopathy
Markers of inflammatory and prothrombotic phenomenon?
Potentiel interest in patients risk stratification?
Potential interest in therapeutic survey?
Elalamy et al, Thromb Res 2009
PLATELET-LEUKOCYTES COMPLEXES AND DIABETES
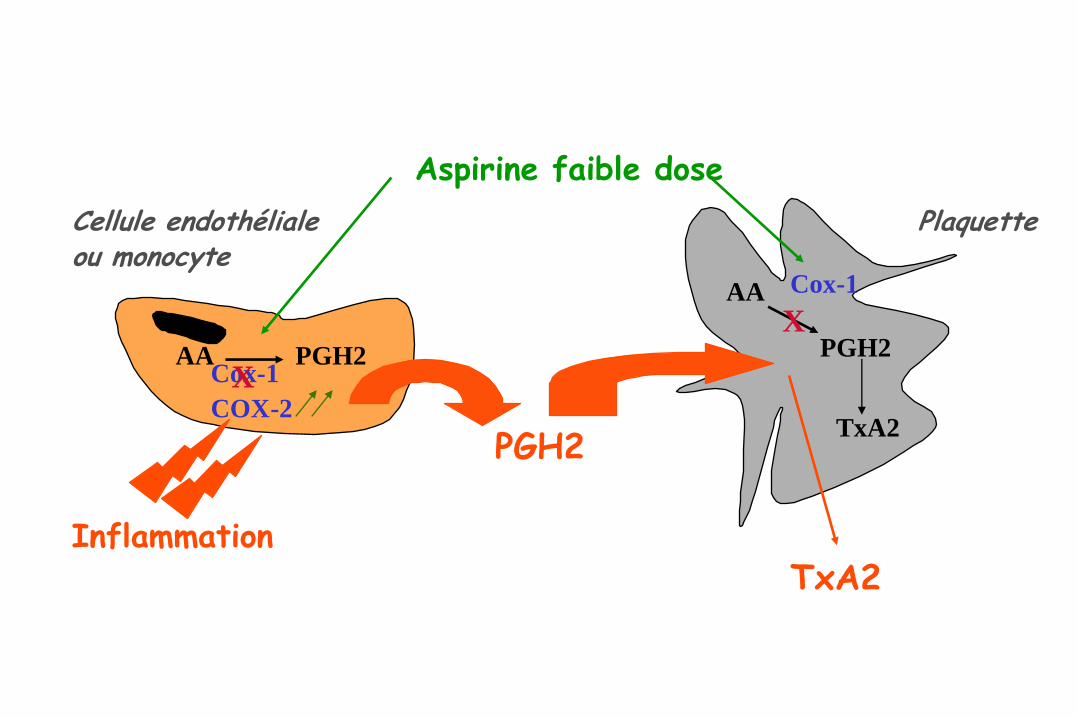
Cellule endothélialeou monocyte
Plaquette
PGH2
Cox-1
Aspirine faible dose
XAA
AA PGH2Cox-1
COX-2
X
Inflammation
PGH2
TxA2
TxA2
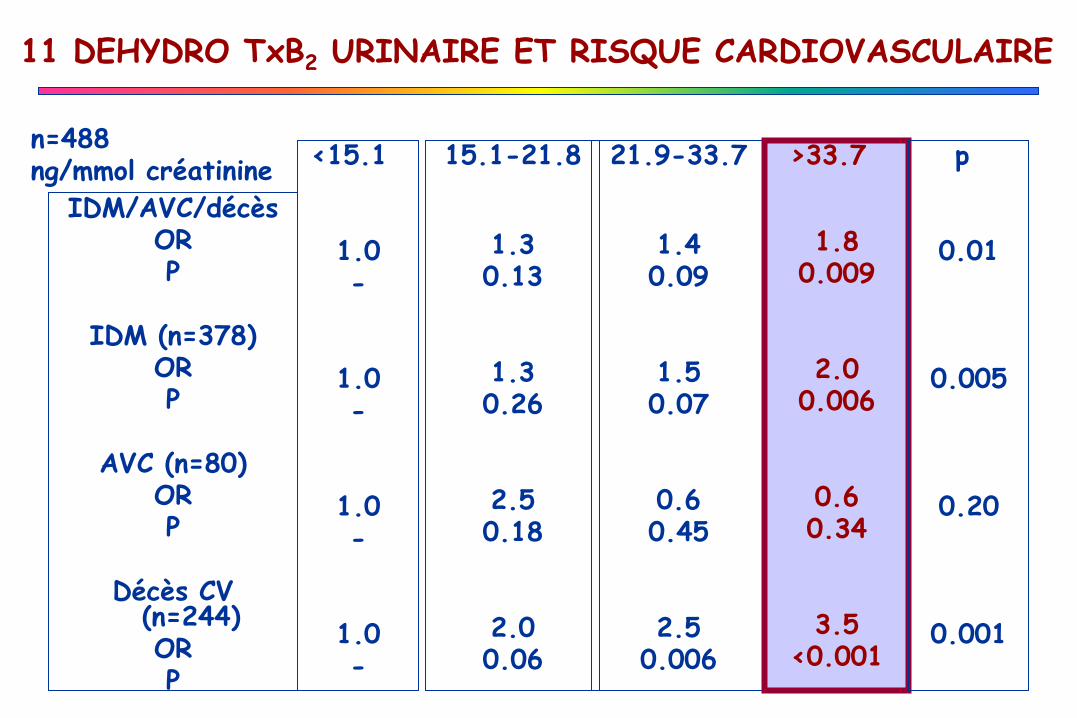
IDM/AVC/décèsORP
IDM (n=378)OR P
AVC (n=80)ORP
Décès CV (n=244)ORP
<15.1
1.0-
1.0-
1.0-
1.0-
15.1-21.8
1.30.13
1.30.26
2.50.18
2.00.06
21.9-33.7
1.40.09
1.50.07
0.60.45
2.50.006
>33.7
1.80.009
2.00.006
0.60.34
3.5<0.001
p
0.01
0.005
0.20
0.001
11 DEHYDRO TxB2 URINAIRE ET RISQUE CARDIOVASCULAIRE
n=488ng/mmol créatinine
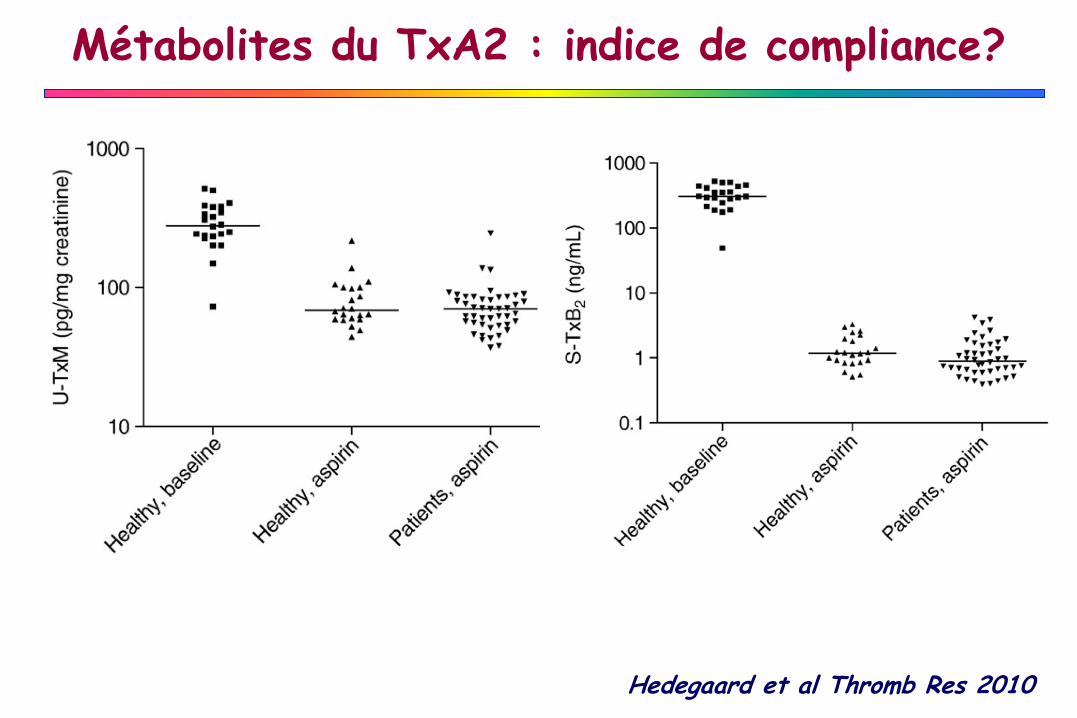
Métabolites du TxA2 : indice de compliance?
Hedegaard et al Thromb Res 2010
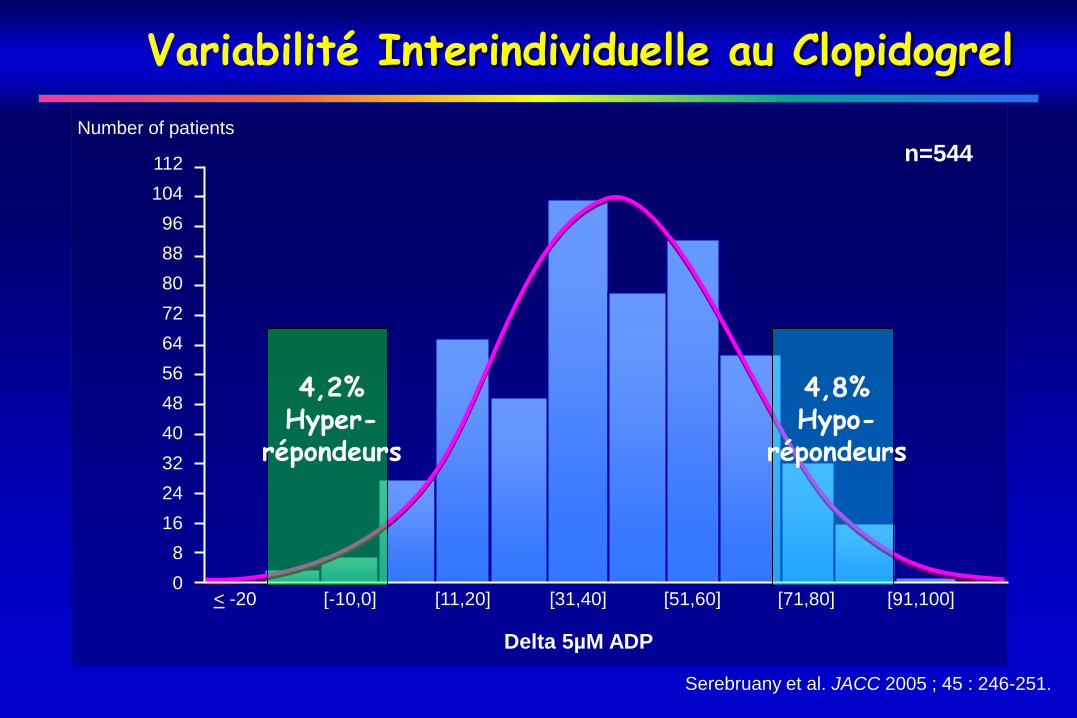
Variabilité Interindividuelle au Clopidogrel
Serebruany et al. JACC 2005 ; 45 : 246-251.
n=544112
104
96
88
80
72
64
56
48
40
32
24
16
8
0
Number of patients
< -20 [-10,0] [11,20] [31,40] [51,60] [71,80] [91,100]
Delta 5µM ADP
4,2%Hyper-
répondeurs
4,8%Hypo-
répondeurs
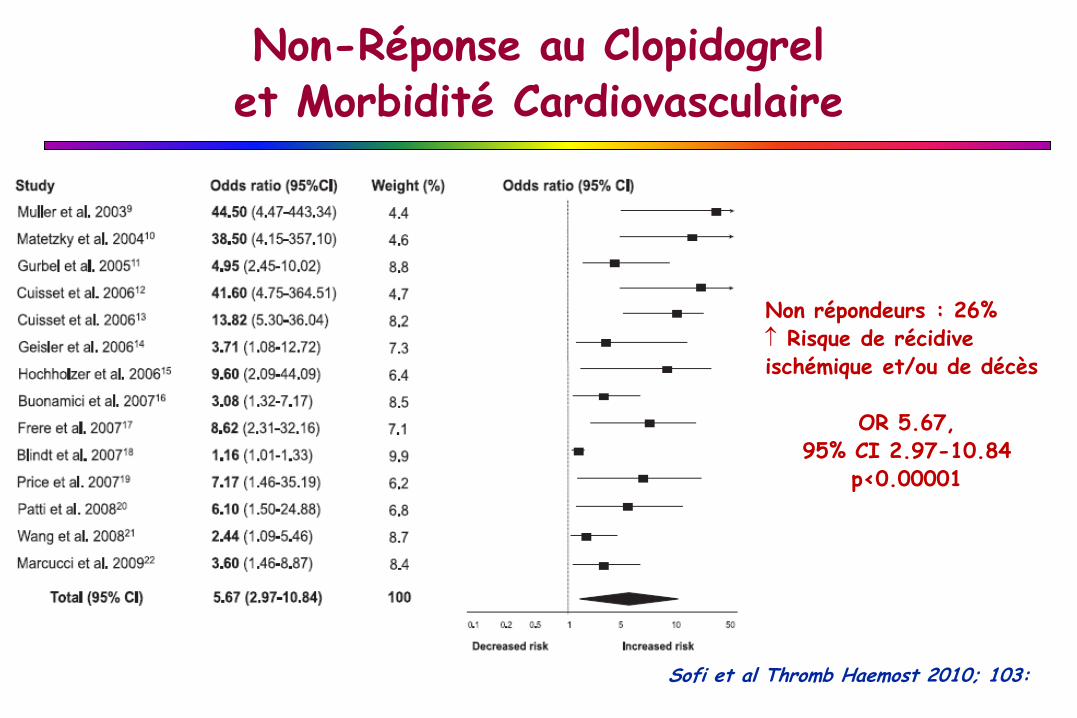
Non répondeurs : 26% Risque de récidive ischémique et/ou de décès
OR 5.67, 95% CI 2.97-10.84
p<0.00001
Sofi et al Thromb Haemost 2010; 103:
Non-Réponse au Clopidogrel et Morbidité Cardiovasculaire
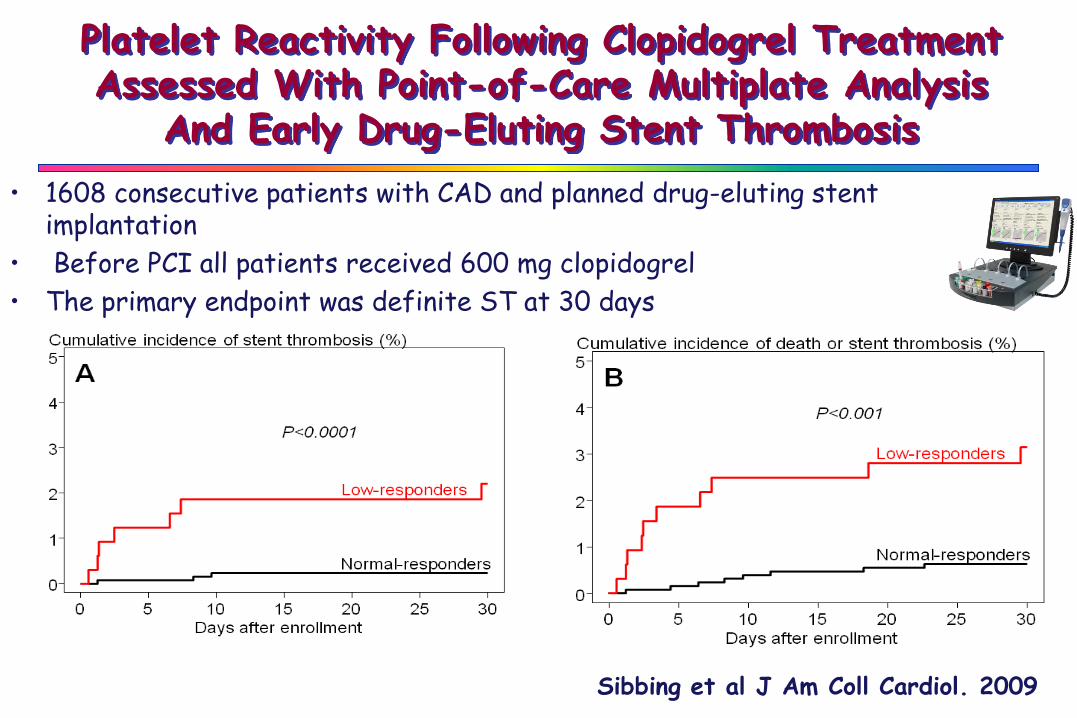
Platelet Reactivity Following Clopidogrel Treatment Assessed With Point-of-Care Multiplate Analysis
And Early Drug-Eluting Stent Thrombosis
Sibbing et al J Am Coll Cardiol. 2009
• 1608 consecutive patients with CAD and planned drug-eluting stent implantation
• Before PCI all patients received 600 mg clopidogrel
• The primary endpoint was definite ST at 30 days

Insérer la cartouche
Rapide Facile Précis
Ajouter échantillon Résultats en quelques minutes
VerifyNowTM
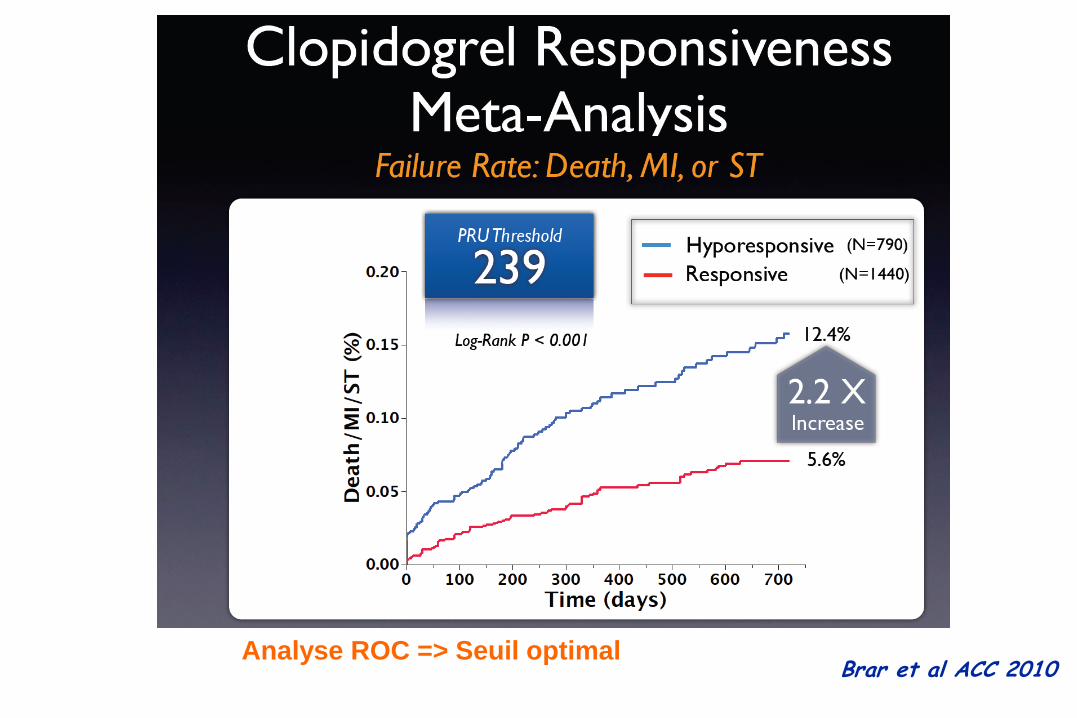
Brar et al ACC 2010Analyse ROC => Seuil optimal
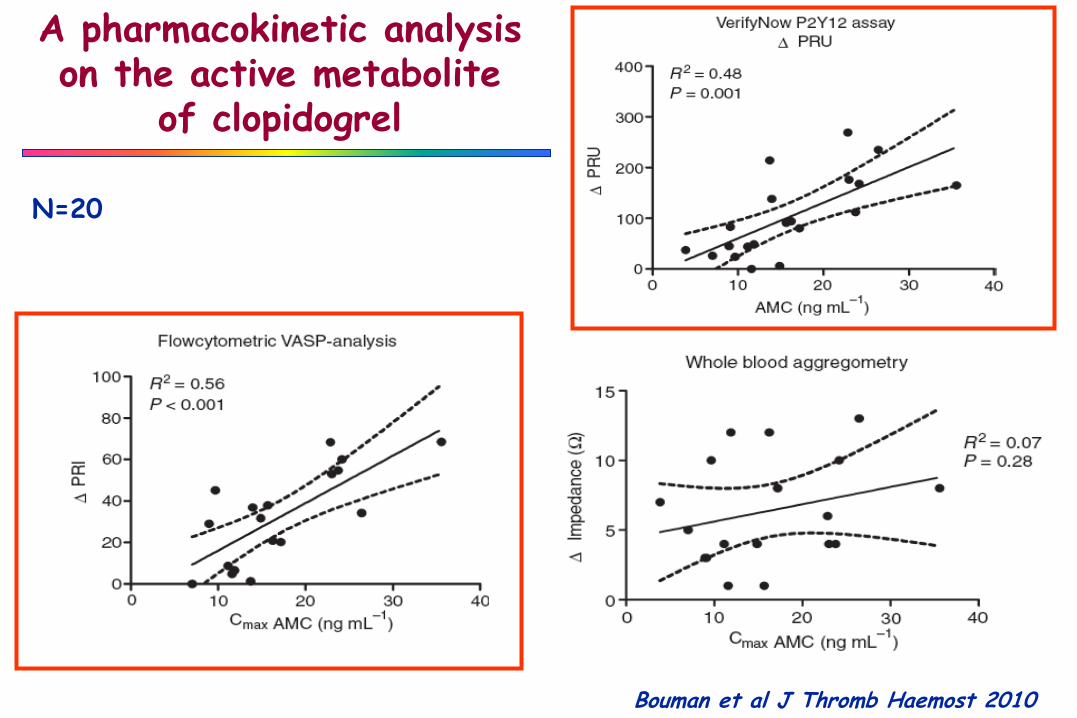
A pharmacokinetic analysis on the active metabolite
of clopidogrel
Bouman et al J Thromb Haemost 2010
N=20
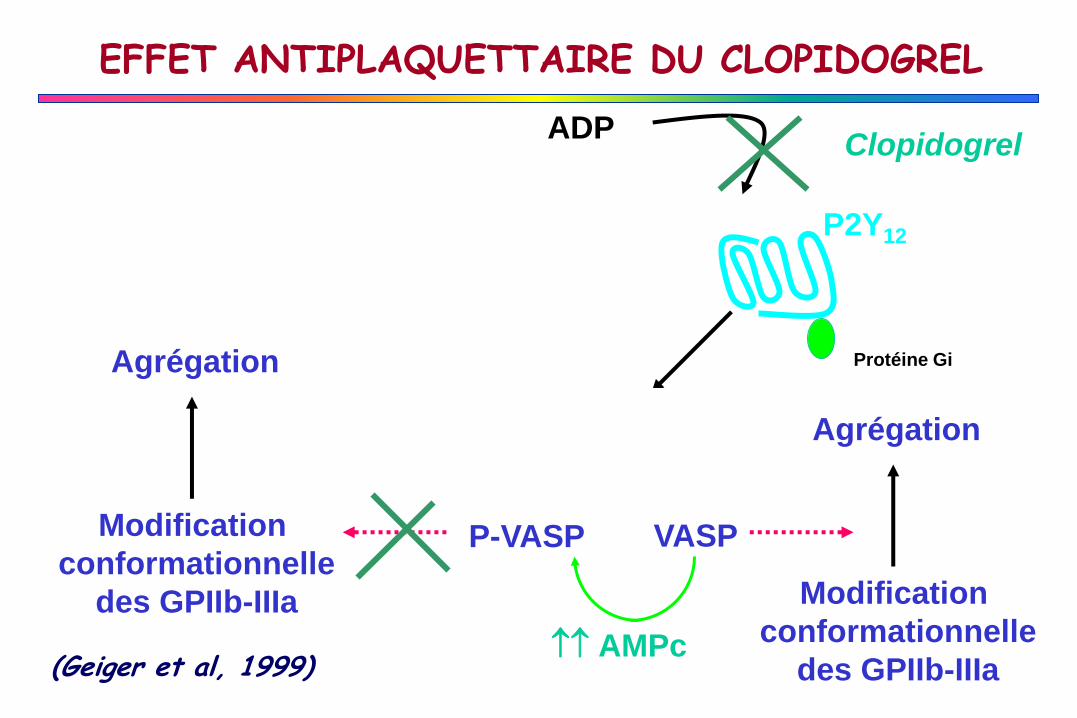
EFFET ANTIPLAQUETTAIRE DU CLOPIDOGREL
(Geiger et al, 1999)
P2Y12
Protéine Gi
ADP
AMPc
P-VASP VASP
Modification
conformationnelle
des GPIIb-IIIa
Agrégation
Clopidogrel
AMPc
Modification
conformationnelle
des GPIIb-IIIa
Agrégation
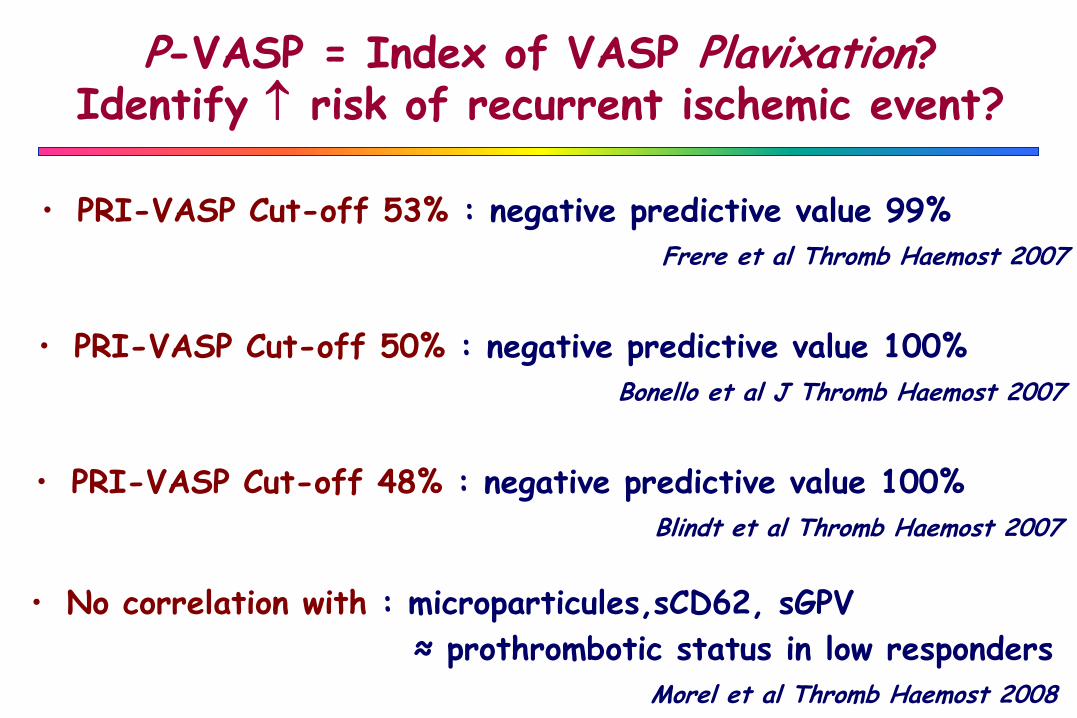
P-VASP = Index of VASP Plavixation?Identify risk of recurrent ischemic event?
• PRI-VASP Cut-off 53% : negative predictive value 99%
Frere et al Thromb Haemost 2007
• PRI-VASP Cut-off 50% : negative predictive value 100%
Bonello et al J Thromb Haemost 2007
• PRI-VASP Cut-off 48% : negative predictive value 100%
Blindt et al Thromb Haemost 2007
• No correlation with : microparticules,sCD62, sGPV
≈ prothrombotic status in low responders
Morel et al Thromb Haemost 2008
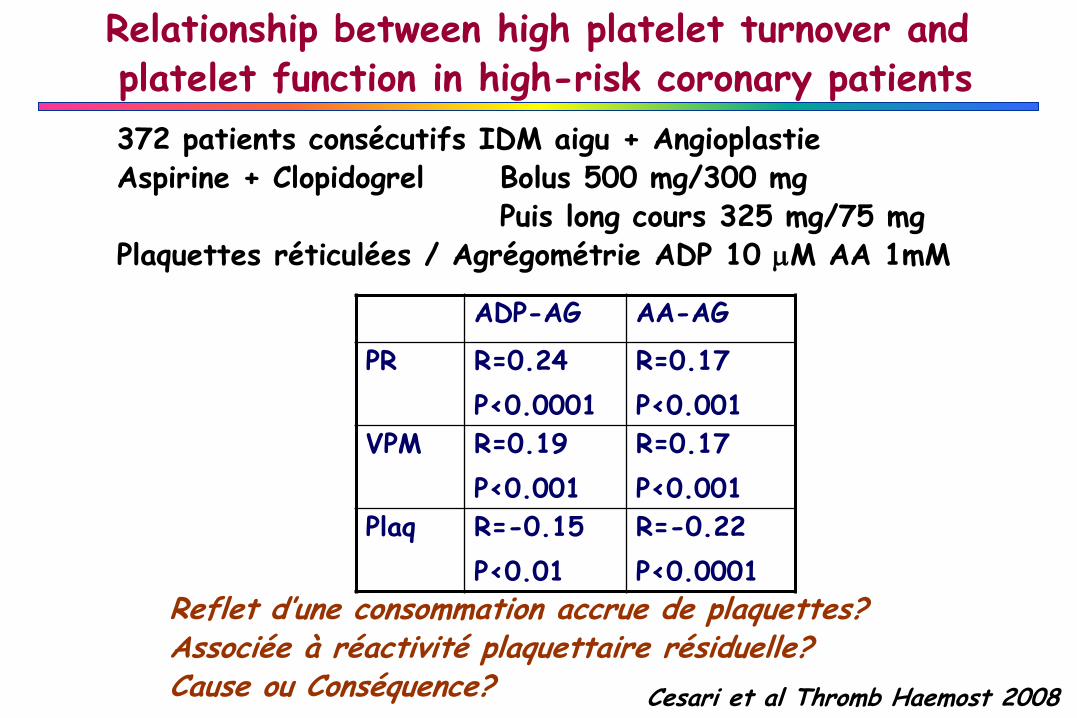
Relationship between high platelet turnover and platelet function in high-risk coronary patients
Cesari et al Thromb Haemost 2008
372 patients consécutifs IDM aigu + AngioplastieAspirine + Clopidogrel Bolus 500 mg/300 mg
Puis long cours 325 mg/75 mgPlaquettes réticulées / Agrégométrie ADP 10 mM AA 1mM
Reflet d’une consommation accrue de plaquettes?Associée à réactivité plaquettaire résiduelle?Cause ou Conséquence?
ADP-AG AA-AG
PR R=0.24
P<0.0001
R=0.17
P<0.001
VPM R=0.19
P<0.001
R=0.17
P<0.001
Plaq R=-0.15
P<0.01
R=-0.22
P<0.0001
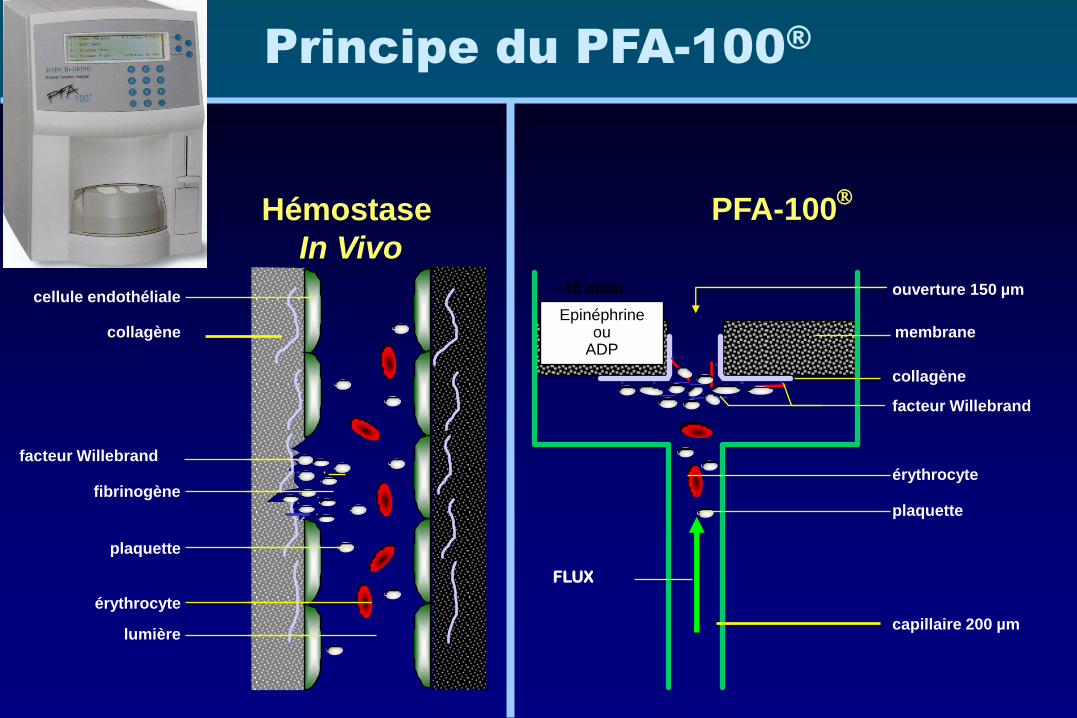
Principe du PFA-100®
Hémostase
In Vivo
PFA-100
capillaire 200 µm
ouverture 150 µm
Epinéphrine ou
ADP
plaquette
facteur Willebrand
érythrocyte
FLUX
lumière
fibrinogène
plaquette
collagène
érythrocyte
cellule endothéliale- 40 mbar
collagène
membrane
facteur Willebrand
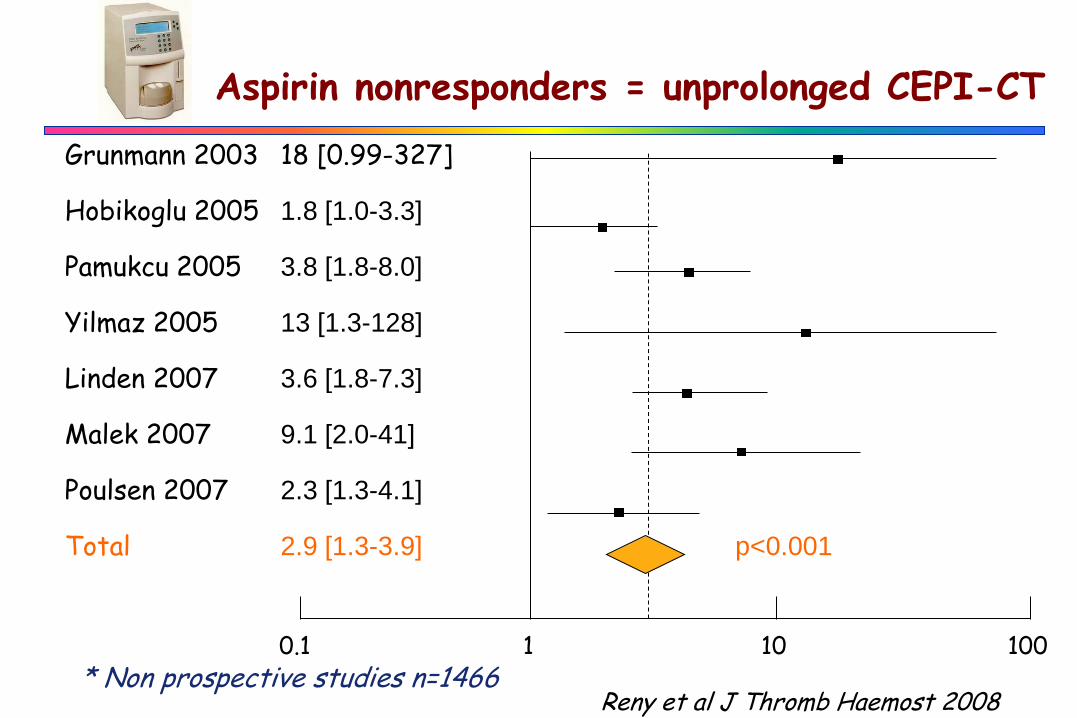
Aspirin nonresponders = unprolonged CEPI-CT
Grunmann 2003 18 [0.99-327]
Hobikoglu 2005 1.8 [1.0-3.3]
Pamukcu 2005 3.8 [1.8-8.0]
Yilmaz 2005 13 [1.3-128]
Linden 2007 3.6 [1.8-7.3]
Malek 2007 9.1 [2.0-41]
Poulsen 2007 2.3 [1.3-4.1]
Total 2.9 [1.3-3.9] p<0.001
0.1 101 100
Reny et al J Thromb Haemost 2008* Non prospective studies n=1466
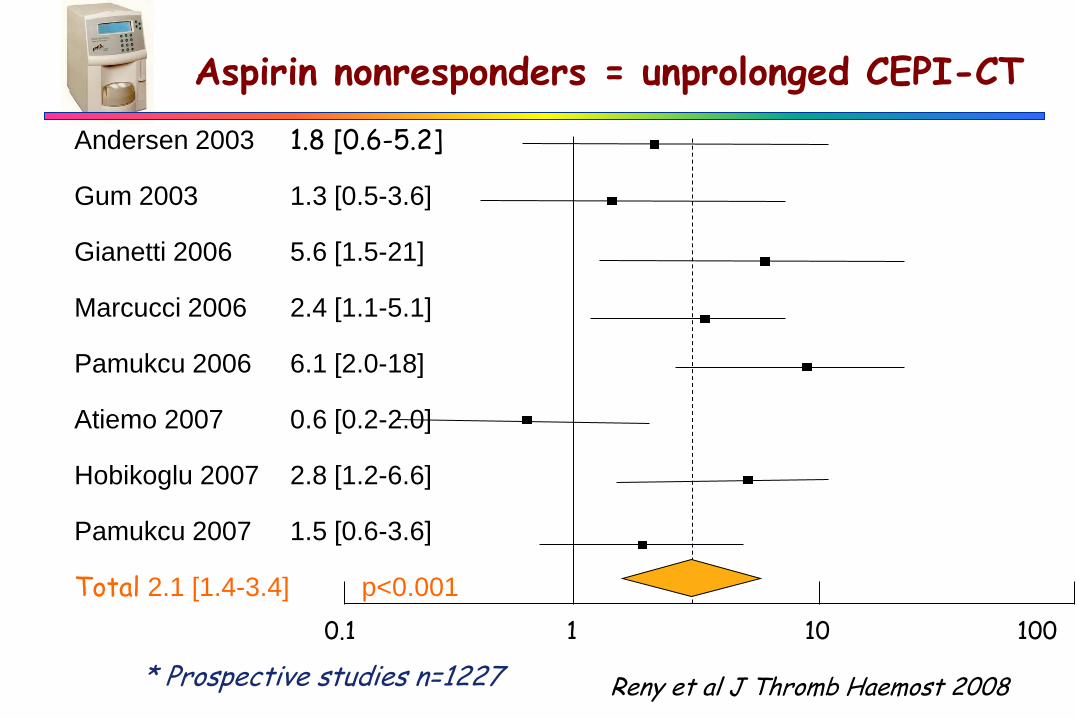
Aspirin nonresponders = unprolonged CEPI-CT
Andersen 2003 1.8 [0.6-5.2]
Gum 2003 1.3 [0.5-3.6]
Gianetti 2006 5.6 [1.5-21]
Marcucci 2006 2.4 [1.1-5.1]
Pamukcu 2006 6.1 [2.0-18]
Atiemo 2007 0.6 [0.2-2.0]
Hobikoglu 2007 2.8 [1.2-6.6]
Pamukcu 2007 1.5 [0.6-3.6]
Total 2.1 [1.4-3.4] p<0.001
0.1 101 100
Reny et al J Thromb Haemost 2008* Prospective studies n=1227
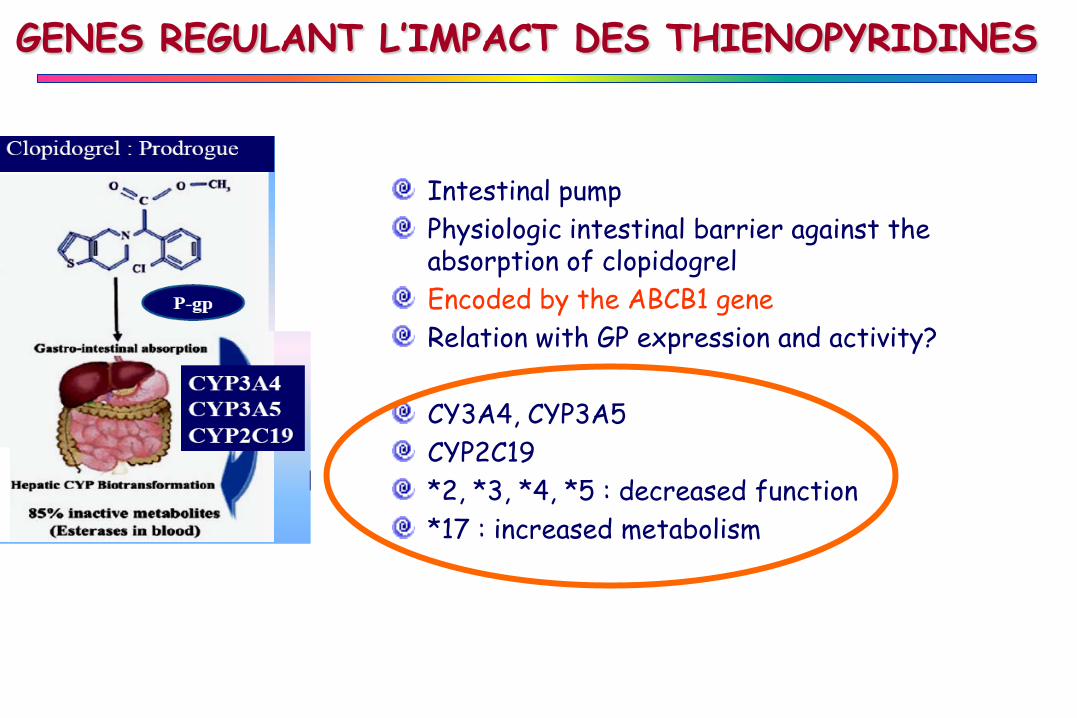
Intestinal pump
Physiologic intestinal barrier against the absorption of clopidogrel
Encoded by the ABCB1 gene
Relation with GP expression and activity?
CY3A4, CYP3A5
CYP2C19
*2, *3, *4, *5 : decreased function
*17 : increased metabolism
GENES REGULANT L’IMPACT DES THIENOPYRIDINES
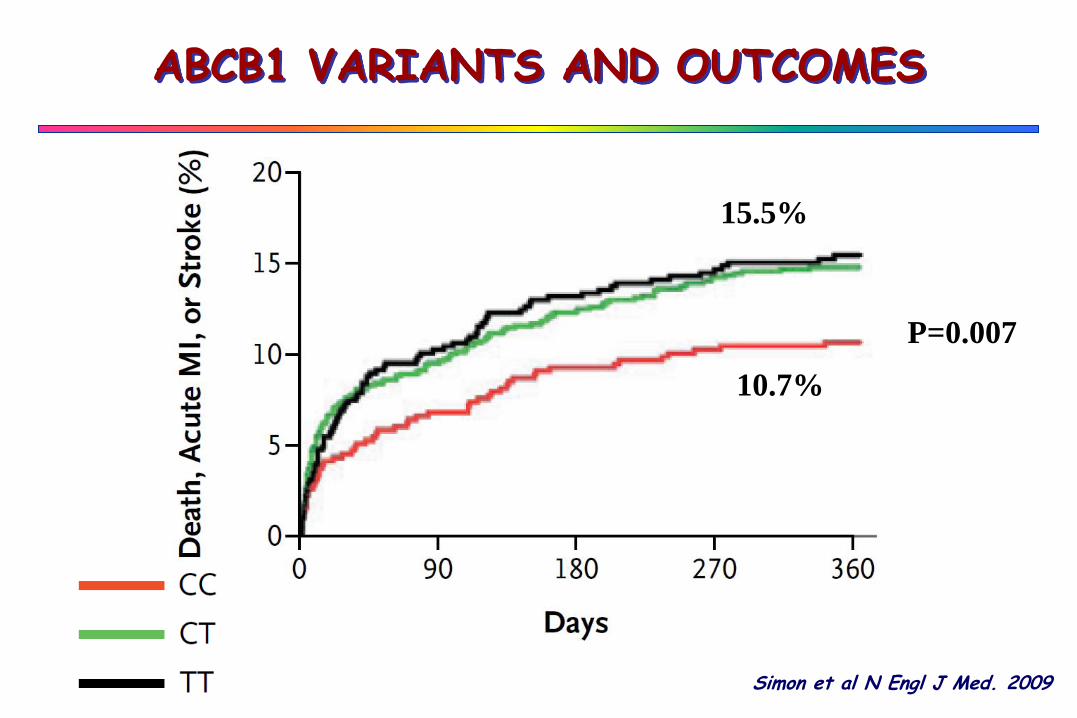
15.5%
10.7%
P=0.007
ABCB1 VARIANTS AND OUTCOMES
Simon et al N Engl J Med. 2009
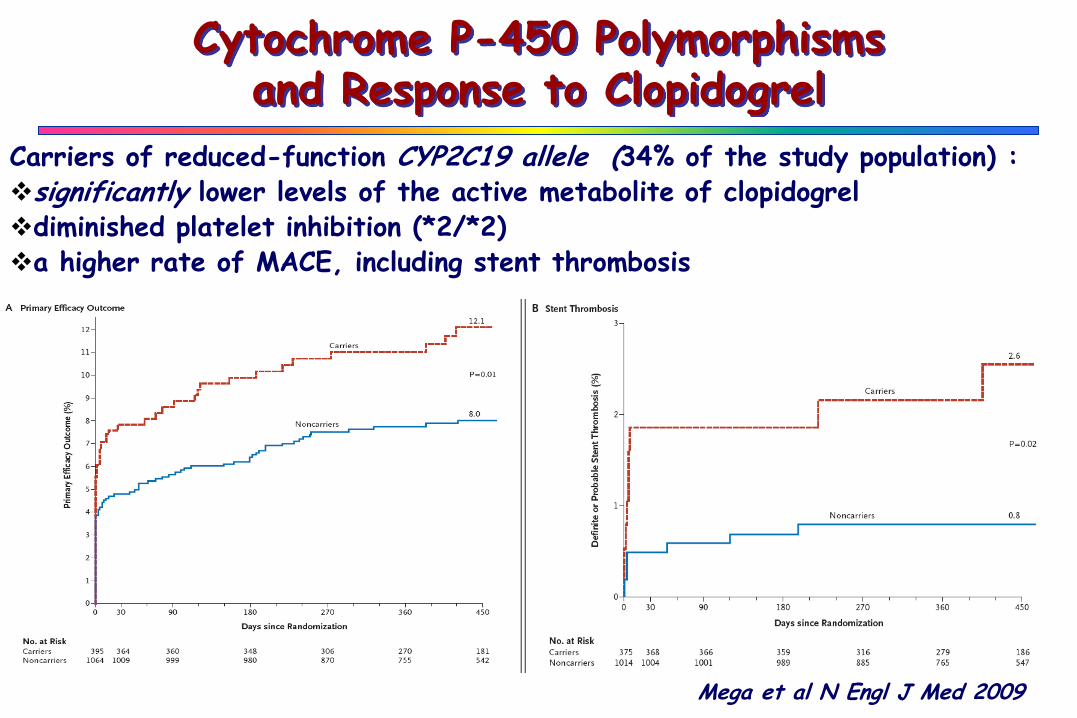
Cytochrome P-450 Polymorphismsand Response to Clopidogrel
Carriers of reduced-function CYP2C19 allele (34% of the study population) :significantly lower levels of the active metabolite of clopidogreldiminished platelet inhibition (*2/*2)a higher rate of MACE, including stent thrombosis
Mega et al N Engl J Med 2009
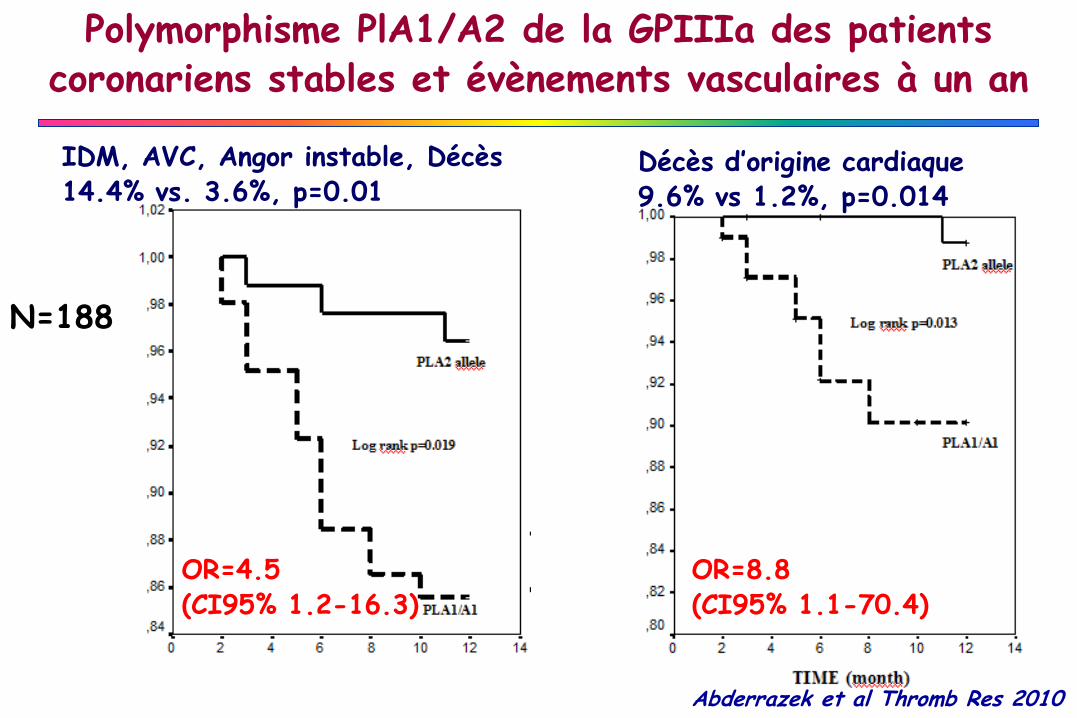
IDM, AVC, Angor instable, Décès 14.4% vs. 3.6%, p=0.01
Décès d’origine cardiaque9.6% vs 1.2%, p=0.014
OR=4.5 (CI95% 1.2-16.3)
OR=8.8 (CI95% 1.1-70.4)
Polymorphisme PlA1/A2 de la GPIIIa des patients coronariens stables et évènements vasculaires à un an
N=188
Abderrazek et al Thromb Res 2010
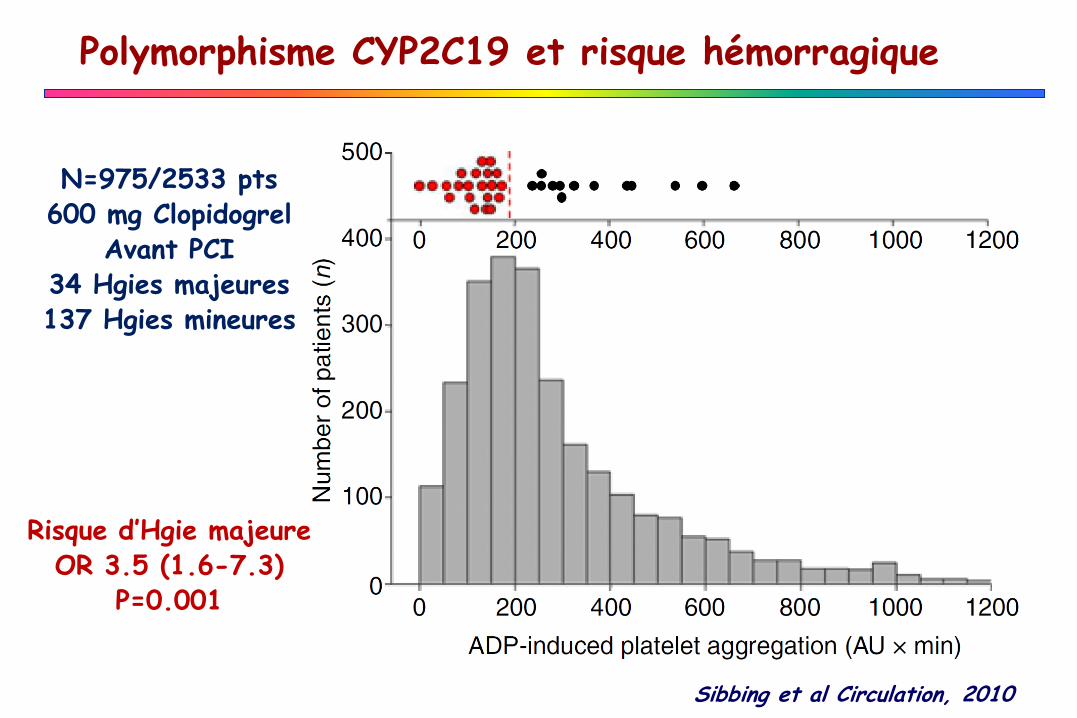
Sibbing et al Circulation, 2010
Polymorphisme CYP2C19 et risque hémorragique
N=975/2533 pts600 mg Clopidogrel
Avant PCI34 Hgies majeures137 Hgies mineures
Risque d’Hgie majeureOR 3.5 (1.6-7.3)
P=0.001
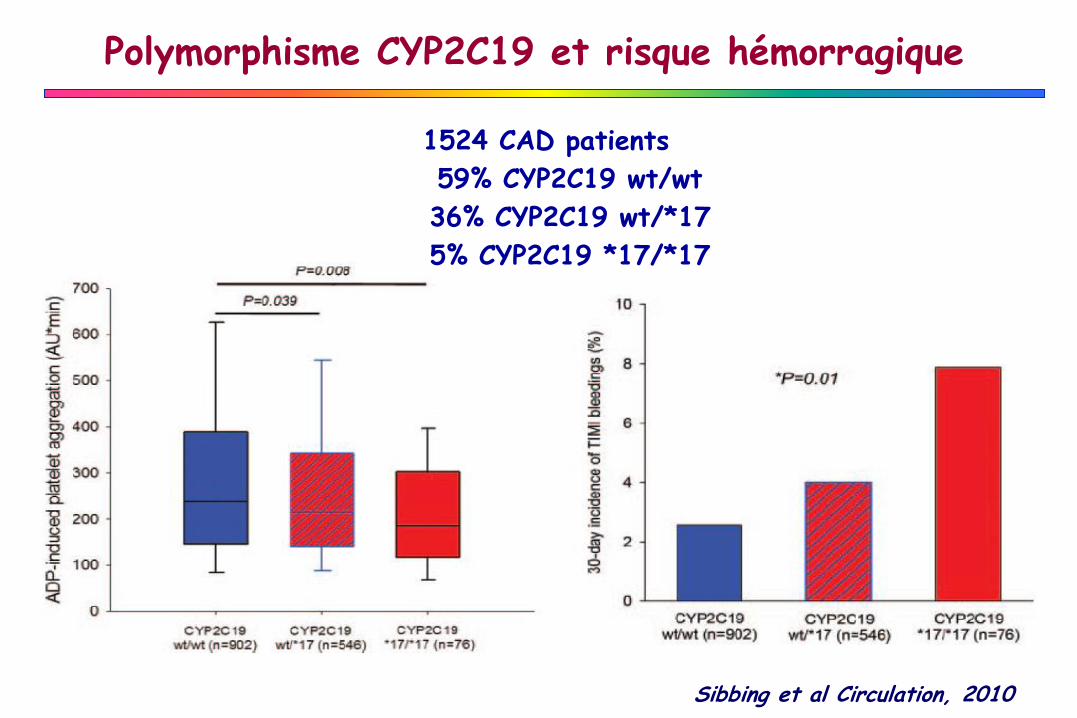
Sibbing et al Circulation, 2010
1524 CAD patients
59% CYP2C19 wt/wt
36% CYP2C19 wt/*17
5% CYP2C19 *17/*17
Polymorphisme CYP2C19 et risque hémorragique
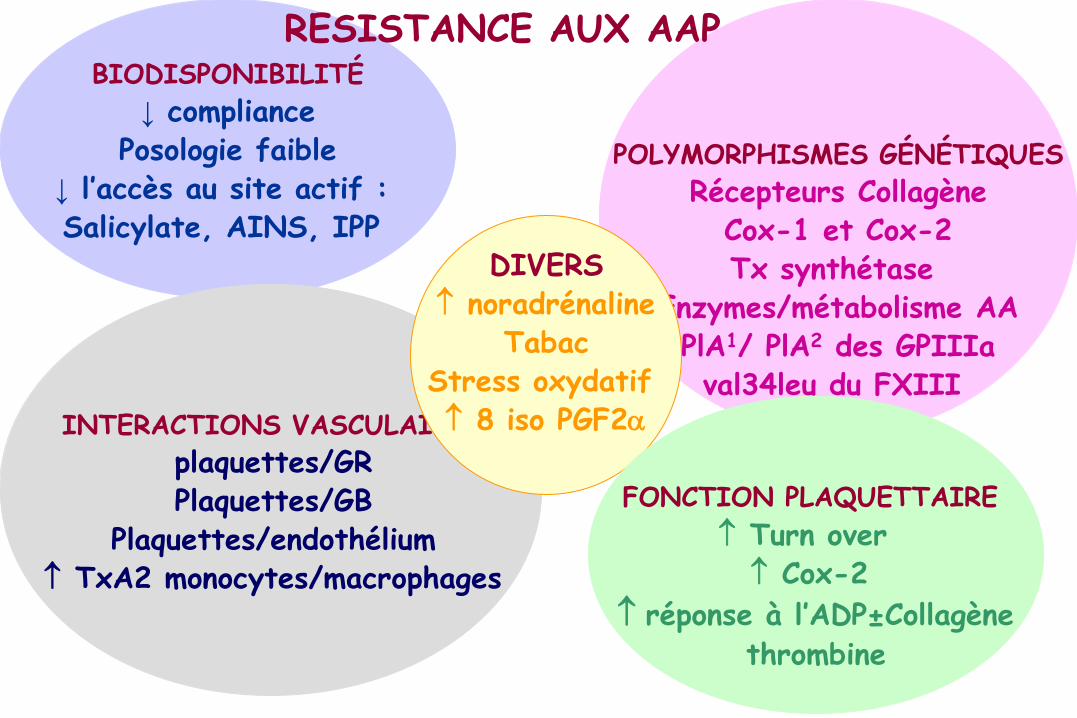
BIODISPONIBILITÉ
↓ compliancePosologie faible
↓ l’accès au site actif : Salicylate, AINS, IPP
POLYMORPHISMES GÉNÉTIQUES
Récepteurs CollagèneCox-1 et Cox-2Tx synthétase
Enzymes/métabolisme AAPlA1/ PlA2 des GPIIIaval34leu du FXIII
INTERACTIONS VASCULAIRES
plaquettes/GRPlaquettes/GB
Plaquettes/endothélium TxA2 monocytes/macrophages
DIVERS noradrénaline
TabacStress oxydatif 8 iso PGF2a
RESISTANCE AUX AAP
FONCTION PLAQUETTAIRE
Turn over Cox-2
réponse à l’ADP±Collagène
thrombine
MONITORING DES ANTIPLAQUETTAIRES ?
Williams et al Thromb Haemost 2010
Manque de recommandations claires Manque de méthodes d’exploration homogènesCutt-off validé?Données concordantes sur cohortes élargies?Risque thrombotique? Risque hémorragique?
Test idéal…?- Facile- Rapide- Reproductible- Standardisé- Pertinence clinique prouvée- Peu onéreux
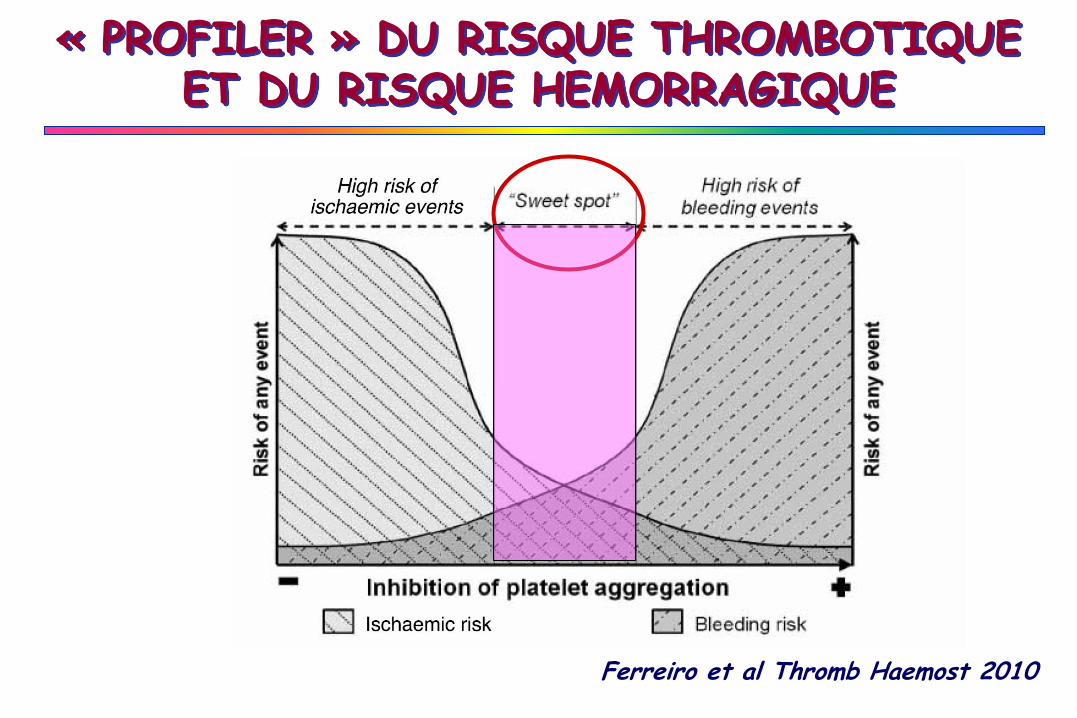
« PROFILER » DU RISQUE THROMBOTIQUE ET DU RISQUE HEMORRAGIQUE
Ferreiro et al Thromb Haemost 2010
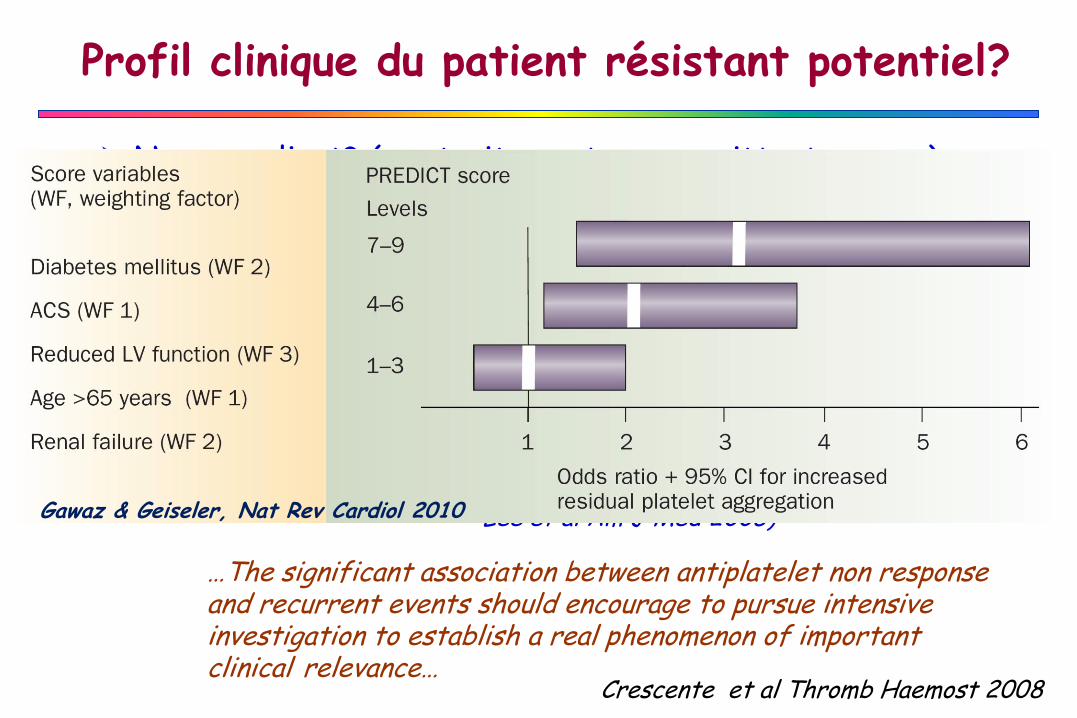
Profil clinique du patient résistant potentiel?
Crescente et al Thromb Haemost 2008
Non compliant? (+++ traitements concomittants oraux)
(Pignatelli et al J Thromb Haemost 2008)
Lésions vasculaires complexes multifocales
Sujet âgé (Ferguson et al Heart Inst J 2008)
Diabétique (Angiolillo et al Am J Cardiol 2006)
Fumeur (Macchi et al Thromb Res 2002)
Troubles de l’Absorption? Pb de biodisponibilité? (Catella-Lawson et al New Engl J Med 2001,
Lee et al Am J Med 2005)
…The significant association between antiplatelet non response and recurrent events should encourage to pursue intensive investigation to establish a real phenomenon of important clinical relevance…
Gawaz & Geiseler, Nat Rev Cardiol 2010
UN ETAT= UN RISQUE?
• Réactivité plaquettaire => thrombogénicité?
• Réponse cellulaire => Echec thérapeutique?
• In vitro / Ex vivo / In vivo => Pertinence clinique?
Plaquettes Certes Responsables MAIS… Pas Seules Coupables?
Facteurs cliniques, pharmacocinétiques et génétiques => Variabilité de réponse
Phénomène plurifactoriel => Phénotype dynamique +++