Embed Size (px)
Citation preview

EHC Workshop on Economics and HTA’s for EU Member Organisations
September 20th, 2014Keith Tolley
Director
Tolley Health Economics Ltd

2

These are economically challenging times for health care payers!
3

Pressures on the payers…Drug expenditures continue to rise
New drugs are rarely cost savingNew drugs for previously untreated conditionsAgeing, obesity, etcGrowing patient awareness
Budgets for health care becoming even more constrainedAlways been constrained - Economic austerity of last few years
meaning becoming even more constrained
4

In economically challenged times new innovative therapies need to represent good value for money!
Need to provide the patient, health service and societal benefits at a cost that payers are willing to pay
The more an unmet need is met the more payers may be willing to pay!
This willingness to pay can be expected to vary across healthcare payers in Europe (depending on budgets and health care priorities)
5

Innovation is about addressing an unmet need!
Source: Morgan et al. 2008, Open Medicine 2 (1):E4-7
“Neither newness nor effectiveness separately or together constitute innovation”
6

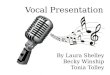
COST
Health Benefit
RISK
Clinical Benefit
GETTING MARKETING AUTHORISATION
GETTING MARKET ACCESS

Not all drugs that get marketing authorisation get market access.
CONTROLLED by:
………..restrictions on the price for public reimbursement
……….limiting the level of reimbursement
……….controlling market access through Health Technology Assessment (HTA) – UK situation
Market access controls

Health Technology AssessmentHealth Technology Assessment (HTA) is “a form of policy
research that systematically examines the short-and long-term consequences, in terms of health and resource use, of the application of a health technology” (Henshall et al., 1997)
HTA has been used as a tool across many countries to help national and regional authorities and payers assess the added value new pharmaceuticals bring: To determine reimbursement and/or price at market access To inform clinical guidance/prescribing
HTA in Europe is co-ordinated through organisations such as EUnetHTA
9

10
Decision makers:National reimbursement and HTA bodiese.g. NICE in UK,TLV in Sweden,IQWiG in Germany, AHTAPol in Poland Local Payers:
Local payers are health authorities and hospitals

What are health care decision makers and payers willing to pay for?
11
Not just newness, or new mechanism of
action alone, or new formulation!
But……
The health care benefits a drug brings: •Clinical benefits•Survival improvements•Quality of life (QoL) improvements
Healthcare resource savings:•Reductions in hospital inpatient use•Significant improvements in the quality of care
Wider Societal benefits: •Quality of life benefits for family members and caregivers•Improved economic and social returns

What does a payer want to know?What offers best value – payers want value based assessments?
What can we afford?
Perspective and what is included within “value” is important and varies by country/type of payer: In Sweden a societal perspective is adopted In UK a healthcare and social service perspective is adopted, but moving more ‘societal’Regional payers (Spain, Italy) concerned with budget impact, cost offsetsLocal payers focussed on affordability in every country
Other factors could be important: orphan, unmet need, clinician and patient demand
12

Assessments of cost-effectiveness
The QALY is growing in use around Europe as the ‘standard’ measure of the health benefits (and hence value) of new pharmaceutical interventions
Long established in UK and several other European countries
More recently seen to be adopted in European countries relatively new to the use of HTA e.g. Estonia, Croatia
13

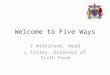
UK Benchmark for decisions:incremental cost per QALY gained (Historical) UK Benchmark for decisions:incremental cost per QALY gained (Historical)
Source: Rawlins and Culyer, BMJ 2005;329:224-227
A = <£20,000 per QALY gained:-Considered an efficient use ofresources
B = >£30,000 per QALY gained-Would need specialcircumstances to accept
Increasing cost/QALY (log scale)
Pro
bab
ility
of
reje
ctio
n
on
gro
un
ds
of
cost
in
eff
ect
iven
ess

Questions of value in haemophilia
Possible questions an HTA organisation could ask:
Which approach to the treatment of haemophilia A with inhibitors offers the best value?
Is the reimbursement of prophylactic use of factor VIII better value than treating bleeds on-demand in haemophilia A or B?
Do new recombinant factor VIII products offer good value for money for use in prophylaxis compared to existing recombinant products such that they should be reimbursed? What additional benefits do they bring e.g. less frequent administration?
15

Published studiesMost attention given to cost-effectiveness of prophylaxis versus
on-demand factor VIII treatment (more recent attention on cost-effectiveness of inhibitors treatment)
Early health economic studies (90’s) did not have QALY as the outcome measure
Recent systematic review found 7 cost per QALY studies (CUA’s):Two were assessments of treatments for inhibitorsFive were assessments prophylaxis v on-demand
16

Cost-utility analysesStudy Study design and countries Utility measure used
Ekert et al, 2001 CUA of recombinant factor VIIa (Novo7) v usual care for haemophilia with inhibitors
Before and after NovoSeven. Single hospital - Australia
Generic EQ 5D
Knight et al, 2003Alternative on-demand regimens for haemophilia A with inhibitors
Decision model - UK Generic EQ 5D
Miners et al. 2002 & Miners 2009Prophylaxis vs on-demand in severe haemophlia
Markov model – UK Generic EQ 5D
Lippert et al, 2005 Prophylaxis vs on-demand in severe haemophlia
Cross sectional study patients aged 14+ years – Ger, Swe, UK, Neth
Generic SF 6D
Risebrough et al 2008Tailored prophylaxis, vs primary prophylaxis vs on-demand in young children 0-6 years
Markov model - Canada Direct Standard gamble in general public
Colombo et al 2011Prophylaxis vs on-demand in severe haemophlia
Markov model - Italy Generic EQ 5D
Farrugia et al 2013Prophylaxis vs on-demand in severe haemophlia
Markov model – US, UK, Swe Generic EQ 5D/SF 6D

Key resultsStudy Treatment/patients
consideredIncremental costs
QALYs gained in a cohort
Cost/QALY Result
Miners 2009
Lifetime treatment with prophylaxis vs on-demand for severe haemophilia in UK (70 yrs follow-up)
£214,000 5.63 £38,000 per QALY gained for primary prophylaxis
Colombo, 2011
Lifetime treatment with prophylaxis vs on-demand for severe haemophilia in Italy (70yrs follow-up)
€787,000 16.03 €40,000 per QALY gained for primary prophylaxis
Ferrugia 2013
Lifetime treatment with prophylaxis vs on-demand for severe haemophilia in 4 countries
-£280,000 (UK)
SEK 5.3 million (Swe)
9.69
10.99
-
SEK 485,000 per QALY gained
18

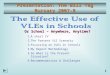
Importance of uncertainty! Cost-effectiveness prophylaxis vs on-demand is sensitive to:
Perspective adopted Dosage and cost of factor VIII assumed Probability of inhibitor with prophylaxis vs on-demand Time horizon and discounting Quality of life estimated for prophylaxis vs. on-demand:
19Source: Noone et al, 2013

HTA and payer questions of value of a new treatmentWhat are the patient reported benefits – how many
QALYs can be gained for the population?
How high is the incremental cost per QALY gained – what is the opportunity cost of funding the new treatment?
How robust, how uncertain are we of the costs and benefit – how much risk do we want to take?
20

Summary – HTA and payer perspective
HTA is a supportive tool for decision making, based on demonstration of value.
It takes a population rather than individual perspective, but what’s important in that perspective can vary.
Can expect closer HTA scrutiny of haemophilia in the future: focussed on what value do new haemophilia treatments bring, are they worth paying a premium price? What value for longer half life, less frequent administration?Will payers be willing to pay more for this?
21