Embed Size (px)
Citation preview

EGFR in Early Non-Small Cell Lung Cancer:
Tyrosine Kinase Inhibition in a Neoadjuvant Trial
by
Humberto Lara-Guerra, MD, MSc
A thesis submitted in conformity with the requirements for the degree of
Doctor of Philosophy
Institute of Medical Science, University of Toronto
© Copyright by Humberto Lara-Guerra, 2011

ii
EGFR in Early Non-Small Cell Lung Cancer: Tyrosine Kinase Inhibition in a Neoadjuvant Trial
Humberto Lara-Guerra, MD, MSc
Doctor of Philosophy
Institute of Medical Science, University of Toronto, 2011
Abstract
EGFR TKIs are standard therapy for advanced NSCLC. In order to define their role in early
disease, we implemented a phase II trial of neoadjuvant gefitinib in clinical stage I NSCLC. Tumour
shrinkage was seen in 43 % of patients, with 11% achieving RECIST partial response (PR). Analysis of
molecular markers showed EGFR TKD mutations in 17% of cases, being the only associated with PR.
For the first time we defined the histopathological response of NSCLC to these agents, characterized by
reduction in tumour cellularity and proliferative index as well as presence of non-mucinous BAC
histology. Clinical PR tumours also presented large areas of stromal fibrosis with presence of focal
residual tumour. In a characterization of intracellular signalling response, EGFR dephosphorylation in
the residues Y1068 and Y1173 was not concordant and only the former was significantly reduced. pAkt
Ser473/Akt and Thr308/Akt ratios were significantly reduced but observed among both, clinical
responders and resistant patients. Interestingly, reduction in pEGFR Y1068 was significantly associated
with increase in tumour cellularity (p=0.047), Ki-67 index (p=0.018) and tumour growth (p=0.019) with
a residual perinuclear localization been detected, suggesting a novel mechanism of resistance involving
receptor internalization. Finally, we determined that the EGFR protein remains stable up to one hour of
post resection ischemia but two to three tumour samples are necessary for an adequate tumour
representation. Furthermore, EGFR cytoplasmic compartment presented the best association with clinical
response in our cohort. Taking all together, we were able to generate the first clinical trial exploring the
use of an EGFR TKI in early NSCLC, characterizing for the first time the histopathological and
signalling responses to these agents with an evidence of a potential novel mechanism of resistance.
Finally, we observed that multiple samples collection for an adequate tumour representation, and
assessment of the cytoplasmic compartment, are warrant.

iii
Acknowledgments
Content of this thesis is the result of continuous work, dedication, education and training
performed and obtained at the University of Toronto and its associated hospitals and research institutes.
Firstly, I would like to thank to the technical teams at the Applied Molecular Profiling Laboratory and
the Latner Thoracic Research Laboratory of the University Health Network, in particular to James Ho,
Jing Xu, Trudey Nicklee, Trevor Do, Olga Ludkovski, Ni Liu and Rongyu Jin for their training, input,
smiles and sharing of spaces and materials for the analysis of tumor samples. Similarly important, I
would like to recognize the hard work of our team of clinical research coordinators, in particular of Dr
Alexandra Salvarrey and Jennifer Lister, whose work was essential for the proper ethical enrolment of
patients in our clinical trials.
As in any successful clinical trial program, the development of this work was possible due to the
collaboration of different clinical departments. I am grateful for the efforts from the Division of Chest
Imaging, specifically Dr Narinder Paul and all the Interventional Radiology Fellows, for their
professional help in tumour samples collection. Similarly, I am profoundly thankful to Drs Scott
Boerner, William Geddie, Claudia Cuhna dos Santos, Catherine Chung and David M. Hwang for their
expert assistance in tumour diagnosis. Finally, I deeply appreciate the collaboration from all surgeons
from the Division of Thoracic Surgery including Dr Shav Keshavjee, Michael Johnson, Gail Darling,
Marc de Perrot, Andrew Pierre, and Kazuhiro Yasufuku as well as their administrative assistants, in
particular to Navjyot Chana for their participation in recruiting patients, professional assistance and,
more importantly, friendship.
I was really fortunate during my time in Toronto to share it with friends with whom I am really
thankful for all their support, smiles and advices including Yukiko and Masaaki Sato, Masaki and Ayako
Anraku, Marcelo and Tatiana Cypel, and Joerg and Nhu-An Schowck among others. Similarly, I deeply
appreciate all the professional advices and guidance received from my committee members, Drs Steven
Gallinger and David Hedley. And finally, I am deeply grateful and fortunate with the Neoadjuvant
Targeted Therapy Program at the University Health Network, in particular with Drs Thomas Waddell,
Ming-Sound Tsao and Natasha Leighl for their mentoring, teaching and support, making my doctoral
experience of the highest international standard.

iv
Dedication
To my examples of life, Lucia and Humberto; to my pillar, light and life, Diana.

v
Table of Contents
Abstract ii
Acknowledgments iii
Dedication iv
Table of Contents v
List of Tables xiii
List of Figures xv
List of Abbreviations xvii
Chapter 1 Introduction, Rationale and Hypothesis 1
1.1. Treatment for stage I non-small-cell lung cancer 2
1.1.1. Current standard of care 2
1.1.2. Addition of adjuvant therapies for stage I non-small cell lung cancer 2
1.1.2.1. Adjuvant radiotherapy 2
1.1.2.2. Adjuvant chemotherapy 3
1.1.3. Addition of neoadjuvant therapies for clinical stage I non-small cell lung cancer 11
1.2. Role of epidermal growth factor receptor (EGFR) inhibition as a treatment in
non-small cell lung cancer 15
1.2.1. EGFR pathway 15
1.2.1.1. EGFR activation 15
1.2.1.2. Mitogen-activating protein kinases (MAPKs; Extracellular signal-
regulated kinase, ERK1/2) 19
1.2.1.3. PI3K/Akt pathway 20

vi
1.2.1.4. Phospholipase C γ (PLCγ) 21
1.2.1.5. Signal transducers and activators of transcription (STATs) 21
1.2.1.6. EGFR endocytosis and downregulation 22
1.2.1.7. Special EGFR activation 22
1.2.1.8. EGFR nuclear translocation 24
1.2.2. EGFR expression in NSCLC 25
1.2.2.1. EGFR gene expression 25
1.2.2.2. EGFR Gene mutations 27
1.2.2.2.1. EGFR extracellular domain mutations 27
1.2.2.2.2. EGFR cytoplasmic domain mutations 28
1.2.2.2.2.1. EGFR TKD mutations responsive to EGFR TKIs 28
1.2.2.2.2.2. EGFR TKD mutations resistant to EGFR TKIs 30
1.2.2.3. EGFR protein expression 30
1.2.3. Anti-EGFR strategies 32
1.2.3.1. Anti-EGFR Abs 32
1.2.3.1.1. Cetuximab (IMC-225; ERBITUX ®) 32
1.2.3.1.2. Panitumumab (ABX-EGF; VECTIBIX®) 34
1.2.3.1.3. Matuzumab (EMD72000) 34
1.2.3.2. Reversible TKIs 34
1.2.3.2.1. Gefitinib (ZD1839; IRESSA®) 34
1.2.3.2.2. Erlotinib (OSI-774; TARCEVA®) 35
1.2.4. Current role of anti-EGFR therapy in NSCLC 36
1.2.4.1. First-line therapy in advanced NSCLC 36

vii
1.2.4.1.1. Single agent therapy 36
1.2.4.1.1.1. Gefitinib 36
1.2.4.1.1.2. Erlotinib 40
1.2.4.1.2. In combination 40
1.2.4.1.2.1. Gefitinib 40
1.2.4.1.2.2. Erlotinib 43
1.2.4.1.2.3. Cetuximab 43
1.2.4.2. Second-line therapy or further in advanced NSCLC 44
1.2.4.2.1. Single agent therapy 44
1.2.4.2.1.1. Gefitinib 44
1.2.4.2.1.2. Erlotinib 45
1.2.4.3. Conclusions 45
1.3. Molecular predictors of response/resistance to anti-EGFR inhibition in NSCLC 48
1.3.1. EGFR status strategies 48
1.3.1.1. EGFR protein expression 48
1.3.1.2. EGFR gene copy number 50
1.3.1.3. EGFR TKD mutations 55
1.3.2. Non-EGFR status strategies 59
1.3.2.1. KRAS mutations 59
1.3.2.2. BRAF mutations 61
1.3.2.3. Akt 61
1.3.2.4. Polymorphisms in DNA repair genes 61
1.3.3. Conclusions 62

viii
1.4. Influence of tumour heterogeneity and ischemia on the expression of molecular
predictors of response/resistance to anti-EGFR therapy 62
1.4.1. Tumour heterogeneity of non-EGFR status molecular markers 63
1.4.1.1. KRAS 63
1.4.1.2. BRAF 64
1.4.1.3. Akt 65
1.4.2. Effect of ischemia on tumour expression of non-EGFR molecular markers 65
1.4.2.1. KRAS 65
1.4.2.2. Akt 66
1.4.3. Tumour heterogeneity of EGFR 69
1.4.3.1. EGFR protein 69
1.4.3.2. EGFR gene copy number 71
1.4.3.3. EGFR TKD mutations 73
1.4.4. Effect of ischemia on tumour expression of the EGFR 74
1.5. Use of anti-EGFR therapy in early NSCLC: study rationale 76
1.6. Hypothesis and study aims 77
1.6.1. Hypothesis 77
1.6.2. Study aims 77
Chapter 2 Material and Methods 79
2.1. Clinical trial 80
2.2. Serum samples 80
2.3. Specimen handling and histopathological assessment 80
2.4. IHC assessment 81

ix
2.5. FISH 84
2.6. Mutational analysis 84
2.7. Statistics 84
Chapter 3 Neoadjuvant Gefitinib Trial in Clinical Stage I NSCLC: Feasibility,
Clinical Response, and its Association with Clinical and Molecular
Predictor Markers of Response 86
3.1. Abstract 87
3.2. Introduction 88
3.3. Results 88
3.3.1. Patients enrolment 88
3.3.2. Treatment delivery 91
3.3.3. Safety 91
3.3.4. Surgical treatment and postoperative period 91
3.3.5. Clinical response 93
3.3.6. Analysis of serum samples and tumour specimens 96
3.4. Discussion 99
Chapter 4 Histopathological Features and IHC Markers Associated with Clinical
Response to Neoadjuvant Gefitinib Therapy in Early Stage NSCLC 102
4.1. Abstract 103
4.2. Introduction 104
4.3. Results 104

x
4.3.1. Histopathologic assessment and IHC markers 104
4.3.2. Association of adenocarcinoma growth patterns with molecular markers of
response to EGFR TKIs 105
4.3.3. Histopathological features in adenocarcinomas with EGFR TKD mutations 109
4.3.4. Association of EGFR TKD mutant adenocarcinomas with histopathological
features and IHC markers 111
4.3.5. Correlation of histopathological features and IHC markers with clinical response 111
4.4. Discussion 114
Chapter 5 Neo-adjuvant Gefitinib in Early Stage NSCLC: Association of Changes in
Phosphorylation of EGFR and Its Downstream Signal Transducers with
Clinical and Histopathological Response 116
5.1. Abstract 117
5.2. Introduction 118
5.3. Results 118
5.3.1. Cohort with paired pre/post gefitinib samples collection 118
5.3.2. Changes and associations of phosphorylation-specific IHC evaluation 119
5.3.3. Associations of changes of phosphorylation state with clinical characteristics and
histological features associated with clinical response 125
5.3.4. Associations with molecular predictors of clinical response 128
5.3.5. Associations with histological features of response 128
5.3.6. Associations with clinical response 132
5.4. Discussion 135

xi
Chapter 6 EGFR expression in NSCLC: Intratumoural heterogeneity and effect
of ischemia 139
6.1. Abstract 140
6.2. Introduction 141
6.3. Results 141
6.3.1. Differences in EGFR IHC patterns among tumour quadrants 141
6.3.2. Estimation of EGFR IHC representative patterns 142
6.3.3. Assessment of the representative number of tumour samples 150
6.3.4. Effect of ischemic time in representative EGFR IHC patterns 153
6.3.5. Association of representative EGFR IHC patterns with clinical response 156
6.4. Discussion 159
Chapter 7 Discussion and Future Directions 162
7.1. Discussion 163
7.1.1. EGFR TKI in the treatment of early NSCLC 163
7.1.2. Analysis of the response induced by EGFR TKIs in the treatment of early
NSCLC 164
7.1.3. Significance of the differences in EGFR inhibition in early NSCLC 165
7.1.4. Importance of heterogeneity and ischemic time in the expression of biomarkers
of response to EGFR TKIs 168
7.2. Limitations 168
7.3. Future directions 170
7.3.1. To investigate changes in the phosphorylation profile of EGFR and relevant
intracellular signalling molecules in NSCLC suffered by the effect of tumour
heterogeneity, ischemic time and EGFR TKIs treatment 170

xii
7.3.2. To investigate the expression pattern of EGFR TKD mutations in early
NSCLC 172
7.3.3. To understand novel mechanism of EGFR TKI resistance observed in early
NSCLC 174
7.3.4. To explore the long term clinical value of a neoadjuvant EGFR TKI regimen
in early NSCLC 175
7.3. Conclusions 177

xiii
List of Tables
Table 1-1. Survival in adjuvant regimens involving pathological stage I NSCLC 7
Table 1-2. Disease-free survival in adjuvant regimens involving pathological stage I NSCLC 8
Table 1-3. Survival in adjuvant uracil or uracil-tegafur regimens involving pathological stage I NSCLC 9
Table1-4. Compliance and recurrence rates of adjuvant chemotherapy studies involving pathological stage I NSCLC patients 10
Table 1-5. Survival in neoadjuvant regimens involving clinical stage I NSCLC 13
Table 1-6. Compliance, response-rate and disease-free survival in neoadjuvant regimens involving clinical stage I NSCLC 14
Table 1-7. Compliance and response rate in randomized trials of first-line anti-EGFR as single agents in advanced NSCLC 38
Table 1-8. Progression-free and overall survival in randomized trials of first-line anti-EGFR as single agents in advanced NSCLC 39
Table 1-9. Compliance and response rate in randomized trials of first-line anti-EGFR in combination in advanced NSCLC 41
Table 1-10. Progression-free and overall survival in randomized trials of first-line anti-EGFR in combination in advanced NSCLC 42
Table 1-11. Compliance and response rate in randomized trials of second or further line of anti-EGFR as single agents in locally advanced or metastatic NSCLC 46
Table 1-12. Progression-free and overall survival in randomized trials of second or further line anti-EGFR as single agents in locally advanced or metastatic NSCLC 47
Table 2-1. Abs used in IHC assessments 83
Table 3-1. Baseline patient and tumour characteristics (N=36) 90
Table 3-2. Toxicities observed during gefitinib therapy considered related to study treatment 92
Table 3-3. Association of clinical and molecular characteristics with tumour response 94
Table 3-4. Cases with EGFR TKD mutations and its associated EGFR gene copy number and response 98
Table 4-1. Histopathologic features and changes observed in clinical stage I NSCLC
surgical specimens after preoperative gefitinib treatment 106
Table 4-2. Correlation between predominant histological patterns of adenocarcinoma and molecular markers 108

xiv
Table 4-3. Correlation of histopathological features of tumour and molecular markers with percentage of change in maximum tumour diameter on CT scans before and after gefitinib treatment 113
Table 5-1. Clinical, histological and molecular characteristics of the cohort and its proportion from the entire trial population 120
Table 5-2. Concordance of changes in EGFR phosphorylation levels at tyrosine residues 1068 and 1173 after gefitinib treatment 123
Table 5-3. Change in pEGFR, pErk, and pAkt immunoscores and molecular makers of response 129
Table 5-4. Associations between changes in EGFR phosphorylation and ratios of intracellular signalling molecules with clinical tumour response to gefitinib 133
Table 6-1. Correlations of percentages of positive tumour cells among different compartments and patterns 145
Table 6-2. Correlations of percentages of positive tumour cells with intensities of staining among different compartments and patterns 146
Table 6-3. Correlations of intensities of positive tumour cells with percentages of positive tumour cells among different compartments and patterns 147
Table 6-4. Correlations of intensities of positive tumour cells among different compartments and patterns 148
Table 6-5. Principal component analysis of intensities values at different compartments 149
Table 6-6. Repeated measures general lineal model exploring the effect of ischemic time on different representative EGFR IHC staining patterns 155
Table 6-7. Associations of different EGFR IHC expression patterns with percentage of change in maximum tumour diameter on CT scans before and after gefitinib treatment 158

xv
List of Figures
Figure 1-1. Epidermal Growth Factor Receptor Pathway 18
Figure 3-1. Trial schema, patient enrolment and sample collection 89
Figure 3-2. Waterfall plots illustrating associations of clinical and molecular markers with
changes in tumour diameter. Y-axis indicates percentage of change before and
after neoadjuvant gefitinib treatment; bars represent individual cases. 95
Figure 3-3. Venn diagram illustrating overlapping positive correlative studies 97
Figure 4-1. Distribution of tumour histopathological features among early stage NSCLC patients
treated with neoadjuvant gefitinib 107
Figure 4-2. Histology of four tumors associated with partial response to gefitinib 110
Figure 4-3. Association between histopathological features and immunohistochemical
markers with adenocarcinoma genotypes 112
Figure 5-1. Example of p-EGFR Y1068 perinuclear staining observed and comparison of
pre/post p-EGFR Y1068 immunoscores from different cellular compartments 121
Figure 5-2. Pre/post immunoscores values of pEGFR, Erk, pErk, Akt and pAkt of tumour
samples before and after gefitinib treatment 122
Figure 5-3. Associations between changes in EGFR phosphorylation levels and ratios of
intracellular signalling molecules 124
Figure 5-4. Differences in EGFR, Erk, and Akt phosphorylation scores by clinical characteristics
of response 126
Figure 5-5. Differences in EGFR, Erk, and Akt phosphorylation scores by histological
characteristics. 127
Figure 5-6. Differences in pEGFR, pErk, and pAkt immunoscores according to adenocarcinoma
genotypes 130
Figure 5-7. Differences in histopathological features of tumour response according to changes
in EGFR, Erk, and Akt phosphorylation 131

xvi
Figure 5-8. Waterfall plots illustrating association of changes in pEGFR Y1173, pEGFR Y1068,
pErk T202Y204/Erk ratio, pAkt Ser473/Akt ratio, and pAkt Thr 308/Akt ratio with
clinical response 134
Figure 6-1. Representative tumour samples and staining patterns for EGFR by IHC 143
Figure 6-2. Description of percentages tumour cells and intensities of staining from membrane
and cytoplasmic compartments observed in 4 different quadrants of tumours 144
Figure 6-3. Percentage of change on variance value compared against variance from average
of 4 areas for different EGFR IHC staining patterns 151
Figure 6-4. Variance component analysis indicating differences in variance for different
EGFR IHC staining patterns explained by patients and tumour areas using single
quadrants and average values of duplets, triplets and 4 areas 152
Figure 6-5. Effect of ischaemia on EGFR IHC staining patterns at 15 minutes intervals 154
Figure 6-6. Correlations between ischaemic time and EGFR expression at different cellular
compartments among two sets of samples from a neoadjuvant gefitinib in stage I
NSCLC clinical trial 157
Figure 7-1. Mechanism of response/resistance to gefitinib in early NSCLC 167

xvii
List of Abbreviations
125I Iodine-125
A Alanine, Adenine, Acinar
Ab Antibody
Abl V-abl Abelson murine leukemia viral oncogene homolog
ADAM A disintegrin and metalloprotease
Adenoca Adenocarcinoma
ALP Alkaline phosphatase
ALT Alanine transaminase
AST Aspartate aminotransferase
ATP Adenosine-5’-triphosphate
ATR AT-rich sequences
BAC Bronchioloalveolar carcinoma
Bad Bcl-2-associated death protein
Bax Bcl2-associated X protein
Bcl-2 B-cell lymphoma 2
Bevac Bevacizumab
Bim Bcl-2-interacting mediator of cell death
BUN Blood urea nitrogen
C Cysteine
CA IX Carbonic anhydrase IX
CALGB Cancer and Leukemia Group B
CaMK Ca2+/calmodulin-dependent protein kinase

xviii
CAP Cyclophosphamide, doxorubicin and cisplatin
Carb Carboplatin
Cdk Cyclin-dependent kinase
cDNA Complementary deoxyribonucleic acid
CEP7 Chromosome 7 centromere
Chemo Chemotherapy
CI Confidence interval
CIN85 Cbl interacting protein of 85k
Cis+ Cisplatin-based plus additional chemotherapeutic agent
CISH Chromogenic in situ hybridization
Cisp Cisplatin
C/P Carboplatin/paclitaxel
CR Conserved region
CRC Colorectal carcinoma
CT Computed tomography
C/T Carboplatin/taxanes regimen
D Aspartic acid
Da Dalton
DAG Diacylglycerol
Del Deletion
DNA Deoxyribonucleic acid
DNA-PK Deoxyribonucleic acid-dependent protein kinase
DNA-PKcs Deoxyribonucleic acid-dependent protein kinase catalytic subunit

xix
Doce Docetaxel
E Glutamic acid
EEA1 Early endosome antigen 1
EGF Epidermal growth factor
EGFR Epidermal growth factor receptor
EGFR TK Epidermal growth factor receptor tyrosine kinase
EGFR TKD Epidermal growth factor receptor tyrosine kinase domain
EGFR TKI Epidermal growth factor receptor tyrosine kinase inhibitor
Egr-1 Early growth response factor 1
ELISA Enzyme-linked immunoabsorbent assay
EMT Epithelial mesenchymal transition
EP Cisplatin and etoposide
Eps15 Epidermal growth factor receptor pathway substrate 15
ER Endoplasmic reticulum
ERBB erythroblastic leukemia viral oncogene homolog receptor
Erk Extracellular signal-regulated kinase
FAK Focal adhesion kinase
FDA US Food and Drug Administration
FFPE Formalin-fixed, paraffin-embedded
FISH Fluorescence in situ hybridization
FKHR Forkhead transcription factor
FLA Fragment length analysis
FLEX First-Line trial for patients with EGFR-EXpressing advanced NSCLC

xx
G Glycine, Guanine
Gab-1 Grb2-associated binder-1
GAP GTPase activating protein
GDP Guanosine diphosphate
GEF Guanine exchange factors
Gem Gemcitabine
Grb2 Growth factor receptor-bound protein 2
GTP Guanosine triphosphate
GTPase Guanosine triphosphatase
H Histidine
HB-EGF Heparin-binding epidermal growth facto
H&E Hematoxylin-Eosin
HER Human epidermal growth factor receptor
HIF-1 Hypoxia inducible factor-1
HNE 4-hydroxynonenal
HNSCC Head and neck squamous cell cancer
HR Hazard ratio
Hsp Heat shock protein
IdUrd Iododeoxyuridine
IF Immunofluorescence
Ig Immunoglobulin
IGF-1R Insuline-like growth factor receptor 1
IHC Immunohistochemistry

xxi
IHC+ Immunohistochemistry positive
IHC- Immunohistochemistry negative
iNOS Inducible nitric oxide synthase
IL Interleukin
Ins Insertion
INTACT Iressa NSCLC Trial Assessing Combination Treatment trial
INTEREST Iressa Non-small cell lung cancer Trial Evaluating REsponse and Survival against
Taxotere trial
Inv Invasive
INVITE Iressa in NSCLC Versus Vinorelbine Investigation in the Elderly trial
IP3 Inositol trisphosphate
IPASS Iressa Pan-Asia Study
ISEL Iressa Survival Evaluation in Lung Cancer trial
ISTANA Iressa as Second Line Therapy in Advanced NSCLC-Asia trial
Jak2 Janus kinase 2
JNK c-Jun N-terminal kinase
K Kinase
kb Kilobases
kDa Kilodaltons
KIP1 Kinase inhibitory protein-1
L Leucine
Lamp Lysosomal-associated membrane protein
M Methionine, Mucinous
MAb Monoclonal antibody

xxii
MALDI-MS Matrix-Assisted Laser-Desorption and Ionization Mass Spectrometry
MAP3K Mitogen-activating protein kinases-kinase-kinase
MAPK Mitogen-activating protein kinase
mCA IX Membranous carbonic anhydrase IX
MEF2A Myocyte enhancer factor 2A
MEK Mitogen-activating protein kinase-kinase
MEKK Mitogen-activating protein kinase-kinase-kinase
MKP-1 Mitogen-activating protein kinase phosphatase-1
MLK Mixed lineage kinases
MRI Magnetic resonance imaging
mRNA Messenger ribonucleic acid
MSH2 MutS homolog 2
MVP Mitomycin C, vinblastin and cisplatin
NCIC CTG National Cancer Institute of Canada, Clinical Trials Group
NLS Nuclear localization site
NM Non-mucinous
NSCLC Non-small cell lung cancer
OR Odd ratio
ORR Objective response rate
OS Overall survival
P Proline, Papillary
Pacl Paclitaxel
pAkt Phosphorylated Akt

xxiii
PC Paclitaxel and carboplatin
pCA IX Perinuclear carbonic anhydrase IX
PCNA Proliferating cell nuclear antigen
PCR Polymerase chain reaction
PD Disease progression
PDK1 Phosphoinositide-dependent kinase-1
pEGFR Phosphorylated EGFR
pErk Phosphorylated Erk
PFS Progression-free survival
PH Pleckstrin homology
PI3K Phosphoinositide 3-kinase
PIP2 Phosphatidylinositol 4,5-biphosphate
PIP3 Phosphatidylinositol 3,4,5-triphosphate
PKA Protein kinase A
PKC Protein kinase C
Plat Platinum
Platinum+ Patinum-based plus additional chemotherapeutic agent
PLCγ Phospholipase C-gamma
PP Protein phosphatase
PR Partial response
PS Performance status
PTB Phosphotyrosine binding
PTEN Phosphatase and tensin homolog

xxiv
PUMA p53 upregulated modulator of apoptosis
Pyk2 Proline-rich tyrosine kinase 2
Q Glutamine
qRT-PCR quantitative real-time polymerase chain reaction
R Arginine
RadioTx Radiotherapy
RECIST Response Evaluation Criteria in Solid Tumours
Rpt5 Regulatory particle aTpase 5
RR Response rate
RSK2 Ribosomal S6 protein kinase 2
SAPK Stress activated protein kinase
SATURN Sequential Tarceva in Unresectable NSCLC study
SCLC Small cell lung cancer
Ser Serine
SH2 Src Homology 2
Shc Src homology 2 domain containing transforming protein c
Shp2 Src homology 2-containing tyrosine phosphatase
SOS Son-of-Sevenless
STAT Signal transducers and activators of transcription
Surg Surgical resection
T Threonine, Thymine
TALENT Tarceva Lung Cancer Investigation tiral
TAO Thousand and one kinases

xxv
TC Taxane plus carboplatin
TGF Transforming growth factor
Thr Threonine
TK Tyrosine kinase
TKD Tyrosine kinase domain
TKI Tyrosine kinase inhibitor
TLR Toll-like receptor
TNF Tumour necrosis factor
TRIBUTE Tarceva Responses in Conjunction with Paclitaxel and Carboplatin trial
TTF Time to failure
TTP Time to progression
TRU Terminal respiratory unit
UF Uracil
UFT Tegafur-uracil
uPAR Urokinase plasminogen
USP Ubiquitin-specific protease
UV Ultraviolet
V Valine
VEGF Vascular endothelial growth factor
Vin/Cis Vinorelbine and cisplatin
WHO World Health Organization
WJSG West Japan Study Group
WJTOG West Japan Thoracic Oncology Group

xxvi
XRCC1 X-ray repair cross complementing protein 1
Y Tyrosine

xxvii
Dissemination of Thesis Content
Lara-Guerra, Humberto; Leighl, Natasha; Salvarrey, Alexandra; Sakurada, Akira; Paul, Narinder S;
Boerner, Scott; Pond, Greg R; Shepherd, Frances A; Tsao, Ming S; Waddell, Thomas K. Preoperative
Gefitinib in Clinical Stage I NSCLC. Journal of Thoracic Oncology 2007 August: vol 2 number 8 supp 4
S464.
Lara-Guerra, Humberto; Leighl, Natasha; Salvarrey, Alexandra; Sakurada, Akira; Paul, Narinder;
Boerner, Scott; Pond, Greg; Shepherd, Frances A; Tsao, Ming S; Waddell, Thomas K. Preoperative
Gefitinib in Clinical Stage I NSCLC. Canadian Journal of Surgery 2007 August: 50:32.
Lara-Guerra, H; Waddell, TK; Salvarrey, MA; Joshua, AM; Chung, CT; Paul, N; Boerner, S; Sakurada,
A; Ludkovski, O; Ma, C; Squire, J; Liu, G; Shepherd, FA; Tsao, MS; Leighl, N. Phase II Study of
Preoperative Gefitinib In Clinical Stage I or II Non-Small Cell Lung Cancer. Journal of Clinical
Oncology 2009 Dec20:27(36):6229-36 PMID:19884551.
Lara-Guerra, H
; Chung CT, Schwock J, Pintilie M, Hwang D, Leighl N, Waddell TK, Tsao MS.
Histopathological features and immunohistochemical markers associated with clinical response to
neoadjuvant gefitinib therapy in early stage non-small cell lung cancer. Lung Cancer (submitted).

1
Chapter 1
Introduction, Rationale and Hypothesis

2
1.1. Treatment for stage I non-small-cell lung cancer
1.1.1. Current standard of care
Lung cancer is the leading cause of cancer-related mortality worldwide. In North America, lung
cancer causes more deaths than colorectal, breast and prostate cancer combined annually. There are two
main types of lung cancer: small cell (SCLC) and non-small cell lung cancer (NSCLC). NSCLC
accounts for 85% of all lung cancers diagnosed and includes the histological subtypes squamous cell
carcinoma, adenocarcinoma and large cell carcinoma.
As for any type of cancer, staging of NSCLC is of relevance for prognostic and therapeutic
implications. This is obtained by complete medical history and physical examination, routine laboratory
evaluations and radiologic tests which should include chest- computed tomography (CT) scan with
contrast material, extended to include liver and adrenal glands, bone scans and CT or magnetic resonance
imaging (MRI) of the brain to evaluate distant metastatic disease. Wherever possible, preoperative
biopsies from lymph nodes obtained by bronchoscopy, mediastinoscopy or anterior mediastinotomy must
be obtained and assessed for disease extension (1). If surgical resection is indicated as a therapeutic
option, an extensive macroscopic and microscopic assessment of the specimen must be performed
thoughtfully, including status of resection margins and gross and microscopic invasion, lymphatic node
invasion indicating number and station, grading, histologic classification and, in particular for
adenocarcinomas, cellular subtypes.
The internationally accepted method of describing the extent of any cancer is the TNM
classification. In 2010, an updated NSCLC TNM classification was introduced (2). In this revision, stage
I is defined as tumours up to 5 cm without evidence of pleural invasion, nodal or metastatic disease.
Stage I is subdivided as Ia that includes tumours with a diameter ≤ 3 cm and Ib >3m but ≤ 5 cm. As
implied in its nature, stage I presents the best survival among NSCLC cases. Whenever possible, patients
with stage I NSCLC should be treated by lobectomy with complete mediastinal lymph node dissection
(3) (4). If clinically determined, stage Ia presents a 5-year survival of 50% and up to 73% if
pathologically diagnosed; for stage Ib this is 43% and 58% respectively. Therefore, assessment of
additional therapeutic options for early NSCLC is of importance to improve survival in this population.
1.1.2. Addition of adjuvant therapies for stage I non-small cell lung cancer
1.1.2.1. Adjuvant radiotherapy

3
The rationale behind the use of adjuvant therapy after complete resection of NSCLC is based on
the hypothesis that these types of regimens will overcome any residual disease.
It is well known that adjuvant radiotherapy is detrimental in stage I NSCLC (Table 1-1). In a
meta-analysis of 11 randomized controlled trials from 1965 to 2009 including 2343 patients with
completely resected NSCLC, postoperative radiotherapy presented a 18% relative increase in the risk of
death compared to surgical resection alone (HR=1.18, p=0.02) (5). This was equivalent to an absolute
detriment of 5% at 2 years (95% CI, 2%-9%), reducing overall survival (OS) from 58% to 53%.
Exploratory subgroups analysis indicated that, in fact, this effect was most pronounced among patients
with stage I/II, N0-N1 disease. With the recent design of the ROSEL trial, the role of stereotactic
radiotherapy compared against surgery in IA NSCLC will be evaluated (6) but in the meantime, adjuvant
radiotherapy does not have a role and it is even harmful in surgically resected, early NSCLC.
1.1.2.2. Adjuvant chemotherapy
A recent meta-analysis including trials from 1988 up to 2008 has examined the role of adjuvant
chemotherapy in operable NSCLC (7) (Tables 1-1, 1-2, 1-3). Twenty-six trials involving 8447 patients
were included, 18 reported on cisplatin-based and 8 on uracil-tegafur-based regimens; 67% of cases were
stage I. This effort has confirmed the beneficial role of adjuvant chemotherapy with a 14% reduction in
the risk of death (HR=0.86, 95% CI 0.81-0.92, p<0.001) reflecting an absolute increase in 5-year
survival from 60 to 64%. Either uracil-tegafur-based (HR=0.8, 95% CI 0.71-0.9, p=0.0001) or cisplatin-
based (HR=0.89, 95% CI 0.82-0.97, p=0.006) regimens induced similar results. No significant overall
difference in effect by tumour stage (trend p=0.57) was observed. For platinum-based regimens, the
relative effect did not differ by tumour staging (trend p=0.13), suggesting a 5-year survival improvement
from 70% to 73% for stage IA and from 55% to 60% for stage IB. However, a contradictory HR of 1.19
was estimated for stage IA (95% CI 0.84–1.68), explained by the low number of cases for this group and
wide CIs, resulting in a non significant effect (p=0.33). In uracil-tegafur-based regimens, the relative
effect also did not differ by stage (trend p=0.12) and application of the overall HR gave an absolute
improvements in 5-year survival from 80% to 82% for stage IA, and from 75% to 78% for stage IB.
Although this study confirmed the utility of adjuvant chemotherapy (cisplatin-based outside Japan,
uracil-tegafur-based in Japan) for completely resected stage II and III NSCLC, for stage IA it remained
unclear. For stage IB, adjuvant chemotherapy was also beneficial but it was unsolved if this was
encompassed by larger tumours exclusively.
Included in this meta-analysis were four randomized trials evaluating the specific use adjuvant
cisplatin-based chemotherapy exclusively in early disease (Tables 1-1, 1-2, 1-3, 1-4). A randomized trial

4
conducted by the Lung Cancer Study Group assessed a regimen of four cycles of cyclophosphamide,
doxirubicin and cisplatin in 269 eligible patients (84% pT2N0, 16% pT1N1) (8). With only 53% of
patients receiving the planned number of cycles, disease-free survival (p=0.529) and OS (p=0.915) were
not improved with the use of this regimen. Another randomized trial, including 118 (21 pT1N0, 97
pT2N0) pathological stage I patients, evaluated three or four cycles of combined regimen of mitomycin
C, vinblastin and cisplatin or nothing (9). The regimen was completed only in 57.6% of the study group.
However, a reduction in recurrence rate was observed (40.7% in the control arm vs 15.3% in the
adjuvant arm, p=0.002). The 5 and 10 year disease-free survival rate were also significantly different
(64.8 and 54.8% in the control group and 88.8 and76.8% in the study group; p=0.002, log-rank test) but
the multivariable analysis did not show a significant improvement in OS (p=0.188, Cox’s proportional
hazard model). Not included in the meta-analysis is a recent report of a 3 arms randomized trial by the
Spanish Lung Cancer Group (10). In this trial, 163 patients with stage I NSCLC > 2cm received 3 cycles
of paclitaxel and carboplatin 3 to 5 weeks after complete surgical resection and compared against 154
patients treated by surgery exclusively. HRs for PFS or OS were not significantly different between
groups (HR 1.02; 95% CI, 0.76-1.36). Based on these trials, the use of adjuvant cisplatin-based
chemotherapy in early NSCLC, in particular for stage IA, is not supported.
In trials evaluating adjuvant regimens specifically in pIB NSCLC cases, results have supported
different conclusions (Tables 1-1, 1-2, 1-4). Among 66 patients with completely resected pT2N0 disease,
a regimen of six cycles of cisplatin+etoposide reduced the rate of locoregional and distant recurrences at
5 years compared to surgery alone (18 % and 24 % in the former, 30% and 43 % in the latter) improving
the 5-year disease-free survival from 30% to 59 % (p=0.02) (11). OS also improved from 45% to 63% at
5 years (log-rank test p=0.04). Also, the Cancer and Leukemia Group B (CALGB 9633) trial evaluated 4
cycles of adjuvant paclitaxel and carboplatin versus surgery alone in 342 completely resected stage 1B
NSCLC patients (12). Although OS was significantly different at 2 years (12%), it was not significantly
different at 6.1 years (HR 0.83; 90% CI, 0.64-1.08; p = 0.12). However, patients with larger tumours (>
or = 4 cm in diameter) were favoured by adjuvant chemotherapy (HR 0.69; CI, 0.48-0.99; p = .043).
Consequently, the beneficial effect of adjuvant cisplatin-based chemotherapy in pathological stage I
NSCLC is supported for patients with large tumours.
Recent long term assessments from two trials have shown controversial results (Tables 1-1, 1-2,
1-4). Initially, the IALT trial assessing the use of three or four cycles of doublet cisplatin-based adjuvant
therapy in 1867 completely resected pathological stage I-III NSCLC patients showed a survival benefit
of 4 % at 5 years (13). At a median follow-up of 7.5 years, a disease-free survival for the initial 5 years
showed a HR of 0.85 (95% CI, 0.75 to 0.95; p=0.006) but for after 5 years HR was 1.33 (95% CI, 0.89 to
2.0; p=0.16) (14). In OS, the HR was 0.86 (95% CI, 0.76 to 0.97; p=0.01) in the initial 5 years period,

5
favouring chemotherapy but 1.45 (95% CI, 1.02 to 2.07; p=0.04) for the following years, indicating that
the effect of chemotherapy might be, in fact, deleterious. For stage I, the HR was 1.01 (95% CI, 0.81 to
1.26; p=0.47 for interaction). Another important trial has also reported long term follow-up results. The
BR.10 randomized trial of the National Cancer Institute of Canada, Clinical Trials Group (NCIC CTG)
assessed the use of 4 cycles of adjuvant vinorelbine/cisplatin regimen versus observation in 482 patients
with completely resected stage 1B (T2N0) and stage II NSCLC (excluding T3N0) patients (15). Median
relapse-free survival (not reached vs. 46.7 months; HR for recurrence, 0.60; p<0.001) and OS (94 vs. 73
months; HR for death, 0.69; p=0.04) were significantly prolonged in the chemotherapy group as
compared with observation group. The 5-year survival in the adjuvant chemotherapy arm was 69%
compared to 54% in the surgery alone arm, (HR 0.70, p=0.012). Although the statistical test for stage-by-
treatment interaction was not significant (p=0.13), the survival advantage was most prominent in patients
with stage II disease (7 % benefit at five years for IB, vs. 20 % for stage II disease). At a median follow-
up of 9.3 years, patients in the chemotherapy arm continue to show a survival advantage (HR 0.78; 95%
CI, 0.61 to 0.99; p= 0.04) but this was not observed among stage IB cases (HR 1.03; 95% CI, 0.7 to 1.52;
p=0.87) (16). However, within stage IB, tumour size was predictive of chemotherapy effect. Patients
with tumours of 4 cm or larger in size derived clinically meaningful benefit from chemotherapy (HR,
0.66; 95% CI, 0.39 to 1.14; p=0.13), while those with tumours smaller than 4 cm did not (HR, 1.73; 95%
CI, 0.98 to 3.04; p=0.06). Although these were post-hoc analyses, there is not clear evidence of a
beneficial long-term effect using adjuvant cisplatin-based chemotherapy, with only the BR10 trial
showing a survival advantage. However, in particular to stage I disease, any advantage may be only
experienced by patients with large tumours leaving adjuvant cisplatin-based chemotherapy with a limited
benefit in stage I NSCLC.
Of interest is the use of uracil-tegafur-based therapy, mainly explored in Japan, agent that, in the
metanalysis performed by the NSCLC Meta-analysis Collaborative Group, showed similar overall
beneficial effect to cisplatin-based chemotherapy (Tables 1-2, 1-3, 1-4) (7). Among pathological stage I
patients, uracil-tegafur has improved survival (HR=0.57; 95% CI, 0.32-0.97; p=0.039) with an increase
in eight-year survival rate from 57.6% (95% CI, 46.4–68.8%) for surgery alone to 74.2% (95% CI, 64.4–
84.0%) for surgery plus adjuvant uracil-tegafur (17). Furthermore, analysis among T1 cases showed a
better 8-year survival induced by adjuvant uracil-tegafur (87.7% vs 56.4%, p=0.014) which was not
observed among T2 cases (58.5 for surgery+uracil-tegafur vs 59.4% for surgery, p=0.763). This T status-
based observation was reversed compared with another trial analyzing the use of uracil-tegafur in
pathological stage I adenocarcinomas. Previously, the West Japan Study Group (WJSG) for Lung Cancer
Surgery reported prolonged survival in patients with adjuvant uracil-tegafur treatment compared against
observation alone after complete resection of stage I, II, or III NSCLC (18). The five-year survival rate
was 64 percent in the uracil-tegafur group and 49 percent in the control group (p=0.02). As a better

6
survival was observed among patients with stage I adenocarcinomas, a subsequent randomized trial was
designed around this population. Patients with completely resected pathological stage I adenocarcinomas
were randomized to receive either 2 years of adjuvant oral uracil-tegafur or no treatment (19). The five-
year OS rate was 88 % (95 % CI, 85 to 91%) in the uracil-tegafur group but 85 % (95 % CI, 82 to 89 %)
in the control group. However, the five-year survival rate among patients with T2 disease was 85 % (95
% CI, 79 to 91 %) in the uracil-tegafur group and 74 % (95 % CI, 66 to 81 %) in the control group
(p=0.005 by the log-rank test). The five-year survival rate among patients with T1 disease was 89 % in
the uracil-tegafur group and 90 % in the control group. Nevertheless, a subgroup analysis of patients with
T1 disease showed a trend toward improved survival in patients whose tumours were >2 to <=3 cm in
diameter but not in those whose tumours were <=2 cm in diameter.
Due to a potential different effect by uracil-tegafur based on the tumour size of stage I NSCLC, a
new uracil-tegafur meta-analysis of 6 trials including 1269 cases with T1N0 tumours, of which 90.6 %
were adenocarcinomas, was performed (20). With a median follow-up of 6.5 years, T1a tumours (≤ 2
cm) had a 5-year survival rate of 85% in the surgical group and 87% in the surgical+ adjuvant uracil-
tegafur group. In tumours > 2 cm but ≤ 3cm (T1b), the 5 -year survival rate was significantly different
with 82% in the surgery-alone group, compared with 88% in the uracil-tegafur group (p=0.011). The HR
for death in the uracil-tegafur group was 0.84 (95% CI, 0.58–1.23) for patients with T1a tumours and
0.62 (95% CI, 0.42–0.90) for those with T1b tumours. Therefore, similar size-based effect observed with
cisplatin-based chemotherapy is also observed with uracil-tegafur, with stage I NSCLC cases showing
benefit if they have T2 or T1b tumours. Cases with T1a do not benefit from this adjuvant regimen.
Furthermore, because uracil-tegafur has only been used on Asia, its utility worldwide is still not
determined. Hence, current adjuvant regimens have not shown general applicability on early NSCLC.

7
Table 1-1. Survival in adjuvant regimens involving pathological stage I NSCLC.
5-year Survival Prolonged Survival Study/Year Stage Groups Events/
Patients Rate (%)
HR (95% CI)
p Time-point
(years)
Rate (%)
HR (95% CI)
p
Radiotherapy-based regimens Meta-analysis 2009 I-III Surg +radioTx 2343 53 1.18
(2-9) (2yrs) 0.02 Surg 58
Cisplatin-based regimens
Meta-analysis 2010
I-III Surg +Chemo 1594/4305 64 0.86 (0.81-0.92) <0.001 Surg 1729/4142 60
I-III Surg+platinum 1068/2384 0.89 (0.82-0.97) 0.006 Surg 1160/236
IA Surg+platinum 75/221 73 1.19 (0.84-1.68) 0.33 Surg 57/193 70
IB Surg+platinum 396/1021 60 Surg 465/1054 55 Feld R 1993 IB/II Surg+CAP 64/142 58 0.98 0.915 Surg 63/141 58 Park JH 2005 I Surg+MVP 17/59 81.4 0.188 Surg 23/59 74.6 Mineo TC 2001 IB Surg+EP 14/33 63 0.58
(0.34-0.99) 0.04 Surg 21/33 45 CALGB 9633 2008 IB Surg+PC 81/171 6.1 47.4 0.83
(90% CI 0.64-1.08) 0.12 Surg 74/173 42.7
IALT 2010
I-III Surg+Cis+ 578/932 44.5 0.86 (0.76-0.97) 0.01 7.5 0.91
(0.81-1.02) 0.1 Surg 590/935 40.4
I Surg+Cis+ 160/333 7.5 1.01 (0.81-1.26) 0.47 Surg 160/348
BR10 2005,2010
IB/II Surg+Vin/Cis 128/243 69 0.67 (0.46-0.8) 0.012 9.3 67 0.79
(0.62-1) 0.05 Surg 143/239 54 56
IB Surg+Vin/Cis 46 0.79 9.3 1.03 (0.7-1.52) 0.87 Surg 45

8
Table 1-2. Disease-free survival in adjuvant regimens involving pathological stage I NSCLC.
5 years Disease-Free Survival Prolonged Disease-Free Survival Study/Year Stage Groups Pts Rate
(%) HR
(95% CI) p Years Rate
(%) HR
(95% CI) p
Cisplatin-based regimens Meta-analysis 2010 I-III Surg+Chemo 5379 0.83
(0.77-0.9) <0.0001 Surg Feld R 1993 IB/II Surg+CAP 142 58 1.2 0.529 Surg 141 60 Park JH 2005 I Surg+MVP 59 88.8 0.002 10 76.8 0.002 Surg 59 64.8 54.8 Mineo TC 2001 IB Surg+EP 33 59 0.02 Surg 33 30 CALGB 9633 2008 IB Surg+PC 171 52 0.117 6.1 47 0.8
(90%,0.62-1.02) 0.065 Surg 173 48 54
IALT 2010
I-IIIA Surg+Cis+ 932 39.4 0.85 (0.75-0.95) 0.006 7.5 65 0.88
(0.78-0.98) 0.02 Surg 935 34.3 67.5
I Surg+Cis+ 932 0.92 (0.75-1.14) Surg 935
BR.10 2005,2010 IB/II Surg+Vin/Cis 242 61 0.6
(0.45-0.79) <0.001 Surg 240 49 Felip E 2010 I>2cm Surg+PC 163 1.02
(0.76-1.36) Surg 154 Uracil-based regimens Kato H 2004 I Surg+UFT 498 53 (2yrs) 0.97
(0.74-1.26) 0.81 Surg 501 51 (2yrs)

9
Table 1-3. Survival in adjuvant uracil or uracil-tegafur regimens involving pathological stage I NSCLC.
5-year Survival Prolonged Survival Study/Year Stage Groups Events/
Patients Rate (%)
HR (95% CI)
p Time-point
(years)
Rate (%)
HR (95% CI)
p
Meta-analysis 2010
I-III Surg+tegafur 526/1921 0.8 (0.71-0.9) 0.0001 Surgery 636/1927
IA Surg+tegafur 117/862 82 Surg 165/782 80
IB Surg+tegafur 138/482 78 Surg 134/448 75
Nakawaga K 2006
I Surg+UF 14/85 8 74.2 0.57 (0.32-0.97) 0.039 Surg 26/87 57.6
T1 Surg+UF 44 8 87.7 0.014 Surg 41 56.4 Wada H 1996 I-III Surg+UF 108 64.1 0.55
(0.36-0.86) 0.02 Surg 100 49
Kato H 2004
I Surg+UFT 65/498 88 0.71 (0.52-0.98) 0.04 Surg 89/501 85
T1 Surg+UFT 362 89 0.97 (0.64-1.46) 0.87 Surg 354 90
Metanalysis 2009
T1a Surg+UFT 48/329 87 0.84 (0.58-1.23) 0.37 Surg 60/341 85
T1b Surg+UFT 46/306 88 0.62 (0.42-0.9) 0.01 Surg 67/293 82

10
Table 1-4. Compliance and recurrence rates of adjuvant chemotherapy studies involving pathological stage I NSCLC patients.
Recurrence Study/Year Stage Groups Pts Compliance
(%) Rate (%)
p
Cisplatin-based regimens Feld R 1993 IB/II Surg+CAP 142 53 10 0.52
Surg 141 13 Park JH 2005 I Surg+MVP 59 57.6 15.3 0.002
Surg 59 40.7 Mineo TC 2004 IB Surg+EP 33 75.7 48.5
Surg 33 69.7 CALGB 9633 2008 IB Surg+PC 171 86
Surg 173 IALT 2010 I-IIIA Surg+Cis+ 932 73.8
Surg 935 BR.10 2005 IB-II Surg+Vin/Cis 242 44.6
Surg 240 Uracil-based regimens Wada H 1996 I-III Surg+UF 108 39.9
Surg 100 42.9 Kato H 2004 I Surg+UFT 498 61 (2yrs) 23
Surg 501 26 Kato H 2004 T1 Surg+UFT 362 19
Surg 354 21

11
1.1.3. Addition of neoadjuvant therapies for clinical stage I non-small cell lung cancer
Use of neoadjuvant regimens in early NSCLC are thought to have an advantage over adjuvant
regimens due to better patient compliance, more complete treatment delivery, early control of
micrometastases, reduction in tumour size facilitating its resection, and inhibition of the putative
stimulus to residual cancer by growth factors released during surgery and subsequent wound healing.
However, if either neoadjuvant or adjuvant approaches result in better outcomes in early NSCLC is
unclear.
A meta-analysis of seven trials including 988 resectable patients assessed the effectiveness of
preoperative chemotherapy in NSCLC (Tables 1-5, 1-6) (21). The combined results showed a significant
increase in disease-free survival associated with the use of preoperative chemotherapy (p = 0.04). The
HR of 0.78 (95% CI, 0.52–0.99) represented an overall 22% relative reduction in the risk of progression
of disease or death on preoperative chemotherapy. A significant increase in survival associated with the
use of preoperative chemotherapy was also observed (p = 0.02). The HR of 0.82 (95% CI, 0.69–0.97)
observed represented an overall 18% relative reduction in the risk of death due to preoperative
chemotherapy, being equivalent to an absolute improvement of 6% at 5 years, increasing OS from 14%
to 20%. Specifically, in a sub-analysis by stage the 5-year survival showed an absolute benefit of 4 % (75
to 79) for stage Ia and 6 % for Ib (55 to 61) but due to the nature of the data no meaningful patient level
subgroup analyses could be performed.
In an effort to clarify this question a subsequent meta-analysis was performed including 10
preoperative or perioperative and 22 postoperative randomized trials of resectable NSCLC (22). Eight
out of 10 pre/peri-operative regimens were cisplatin-based. For OS the pooled HR for death was 0.80
(0.74–0.87; p < 0.001) and very similar at 0.81 (0.66–1.00; p = 0.048) in postoperative and preoperative
(excluding perioperative) chemotherapy, respectively; no important differences on the indirect
comparison of OS between the two regimens were observed after adjustment for stage I patients alone
(0.99, 0.83–1.18). Differences in the expected 5-year survivals for stage IA was -0.3 (78.4% vs 78.1%;
95% CI,-4.23 to 4.51) and -0.51 for stage IB (63.2% vs 62.7%; 95% CI, -7.2 to 7.68) indicating that there
was no clear evidence favouring either of the two approaches overall or in early disease.
Not included in this meta-analysis was a randomized trial of three cycles of preoperative
paclitaxel and carboplatin assessed versus surgery alone in 337 patients with clinical stage IB-IIIA
NSCLC (excluding superior sulcus tumours and N2 disease) (23). Planned cycles were completed in
79% of cases; major response was reached in 41%. The trial closed prematurely but the median OS
reached was 41 months in the surgery-only arm and 62 months in the preoperative chemotherapy arm
(HR 0.79; 95% CI, 0.60 to 1.06; p= 0.11) and the median progression-free survival (PFS) was 20 months

12
for surgery alone and 33 months for preoperative chemotherapy (HR 0.80; 95% CI, 0.61 to 1.04; p =
0.10). Although this study found a 21% reduction in the risk of death and a 9% improvement in 5-year
OS rate using preoperative paclitaxel and carboplatin, the improvement was not statistically significant.
Recently, the Spanish Lung Cancer Group has also reported a 3 arms randomized trial comparing
neoadjuvant or adjuvant regimens against surgical resection (10). In this trial, 148 patients with stage I
NSCLC > 2cm received 3 cycles of paclitaxel and carboplatin before surgical resection and compared
against 154 patients treated by surgery exclusively. HRs for PFS or OS were not significantly different
between groups (HR 0.96; 95% CI, 0.83-1.11).
Not a single randomized trial has been performed assessing the role of a specific neoadjuvant
regimen exclusively in clinical stage I NSCLC. Furthermore, despite the minimal benefit demonstrated
for adjuvant vinorelbine/cisplatin or uracil-tegafur regimens in stage IB disease with large tumours,
conventional regimens has not improved survival in stage I disease. Therefore, the assessment of other
therapies, such as the newly developed targeted-therapy class, warrants evaluation of its potential role in
this population.

13
Table 1-5. Survival in neoadjuvant regimens involving clinical stage I NSCLC.
Patients
5-year Survival Study/Year Stage Groups Rate
(%) HR
(95% CI) p HR
(95% CI) p
Meta-analysis 2006
I-III Platinum++Surg 493 20 0.82 (0.69-0.97) 0.022 Surg 495 14
IA Platinum++Surg 79 Surg 75
IB Platinum++Surg 61 Surg 55
Meta-analysis 2009
I-IV
Chemo+Surg 0.81 (0.66-1) 0.048 0.99
(0.81-1.21) 0.91 Surg Surg+Chemo 0.8
(0.74-0.87) <0.001 Surg
I Chemo+Surg 0.99 (0.83-1.18)
Surg+Chemo
IA -0.3 (-4.23-4.51)
IB -0.51 (-7.2-7.68)
SWOGS9900 2010 IB-IIIA PC+Surg 169 50 0.79
(0.6-1.06) 0.11 Surg 168 41

14
Table 1-6. Compliance, response-rate and disease-free survival in neoadjuvant regimens involving clinical stage I NSCLC.
5 years Disease-Free Survival Study/Year Stage Groups Pts Compliance
(%) Response Rate (%)
Rate (%)
HR (95% CI)
p HR (95% CI)
p
Meta-analysis 2006 I-III Platinum++Surg 229 0.78
(0.52-0.99) 0.04 Surg 228
Meta-analysis 2009 I-IV
Chemo+Surg 0.80 (0.66-0.92) 0.021 0.96
(0.77-1.2) 0.7 Surg Surg+Chemo 0.76
(0.68-0.85) <0.001 Surg SWOG9900 2010 IB-IIIA PC+Surg 169 79 41 42 0.8
(0.61-1.04) 0.1 Surg 168 33 Felip E 2010 I>2cm PC+Surg 148 0.96 NS Surg 154 (0.83-1.11)

15
1.2. Role of epidermal growth factor receptor (EGFR) inhibition as a treatment in non-small cell
lung cancer
1.2.1. EGFR pathway
1.2.1.1. EGFR activation
Growth of tumour cells is mediated by a complex network of signalling pathways responsive to
external influences, such as growth factors, as well as internal controls and checks. How tumours cells
respond to external stimuli is controlled by intracellular signalling networks that transmit a signal
through changes in protein phosphorylation, enzyme activation, relocalization and formation of protein-
protein complexes. The end result of these transduction pathways is a wide range of cellular processes,
including cell proliferation, survival, immune response and angiogenesis, among others. Due to their
complexity and tight control, dysregulation in these cellular signalling processes can contribute to
malignant transformation of human cells.
Cell communication is controlled by secreted polypeptides named growth factors or cytokines,
by antigen stimulation, or direct cell contact with extracellular matrix or neighbouring cells. Growth
factors interact with surface receptors on target cells inducing modification in intracellular signalling
pathways. Growth factors induce cellular processes such as growth, proliferation, differentiation,
survival and metabolism via interaction with their transmembrane protein receptor (24). Receptors for
many growth factors are membrane-spanning cell surfaces molecules with the ability to phosphorylate
their tyrosine (Y) residues, activating intracellular signalling cascades (24) (25). Epidermal growth factor
(EGF) is a monomeric polypeptide and one of the first growth factors to be described, with mitogenic
effect mediated by binding its cell surface receptor (EGFR).
EGFR was first detected in 1975 by the specific binding of 125I-labeled EGF to the surface of
fibroblasts (26). EGFR is a transmembrane 170 kDa glycoprotein with a single polypeptide chain of
1186 amino acids and an N-linked oligosaccharide (40 kDa). The approximately 200-kb human EGFR
gene, comprising 28 exons and 27 introns, exists on the short arm of chromosome 7 (7p12). Exons 1 to
16 encode the extracellular domain, while exon 17 codes for the transmembrane domain, and exons 18 to
28 are responsible for the intracellular domains. The tyrosine kinase domain is encoded by exons 18 to
24, while the C-terminal domain is encoded by exons 25 to 28. Screening of complementary
deoxyribonucleic acid (cDNA) libraries using an EGFR probe identified a family of proteins closely
related to EGFR, the HER family, which includes EGFR (also known as ERBB1/HER1), HER2
(ERBB2/HER2/NEU), HER3 (ERBB3/HER3) and HER4 (ERBB4/HER4). Members of the HER family
present four functional domains: glycosylated extracellular ligand-binding, hydrophobic transmembrane,
intracellular tyrosine kinase, and C-terminal regulatory domains (27). ERBB2, ERBB3 and ERBB4 show

16
extracellular homologies, relative to the EGFR, of 44, 36 and 48%, respectively, while those for the
tyrosine kinase domain are 82, 59 and 79%, respectively. The degrees of homology in the C-terminal
regulatory domain are relatively low, being 33, 24 and 28%, respectively (26) (28) (29) (30). The EGFR
extracellular ectodomain is made of 620 amino acids comprising 4 subdomains, L1, CR1, L2, and CR2;
two being rich in leucine and two in cysteine repeats (31). The tyrosine kinase domain consists of an N-
lobe (coded by exons 18-20 of the EGFR gene) and a C-lobe (exons 21-24) (30). C-terminal domain
contains several tyrosine, serine and threonine residues that are phosphorylated upon activation of the
receptor.
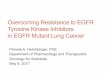
Seven ligands are known to bind to EGFR (Figure 1-1) (31). Among them are included those
binding exclusively to EGFR [EGF, transforming growth factor alpha (TGF-alpha), amphiregulin] or
with the capacity to bind also other ERBB family members (betacellulin, heparin-binding EGF,
heregulin and epiregulin). These ligands are synthesized as transmembrane proteins and soluble ligands
(growth factors) are released into the extracellular environment via proteolytic processing. This shedding
is mediated by ADAM (a disintegrin and metalloprotease) proteins that are membrane-anchored
metalloproteases (32). Upon binding of a ligand to the extracellular domain, EGFR undergoes a 130°
rotation of a rigid body containing domains I and II, about the axis at the domain II/III junction leading
to promotion from a tethered configuration to an extended configuration, exposing the dimerization
domain and leading to the formation of homodimers or heterodimers (27). Once a dimer is formed, the
kinase domain dimerizes asymmetrically in a tail-to-head orientation, then adenosine-5’-triphosphate
(ATP) binds to a cleft between N and C-lobe and sits beneath a N-lobe structure, the phosphate binding
loop (P-loop) containing a highly conserved glycine-rich sequence (GXGXXG motif). Tyrosine kinase
inhibitors (TKIs) such as gefitinib and erlotinib bind to the same cleft. A centrally located activation loop
(A-loop) in the C-lobe provides a platform for downstream protein activation, and is phosphorylated in
the active state. Phosphorylation stabilizes the A-loop in an open and extended state. The most prominent
structure in the N-lobe, the αC-helix, helps regulate the angle of the ATP binding cleft (33). Once ATP
binds the kinase becomes activated, catalyzing the transfer of a γ-phosphate group from ATP to tyrosine
residues within the cytoplasmic C-terminal domain (34). The activation of distinct signalling pathways is
dependent on the respective dimer partner (35).
After dimerization, EGFR autophosphorylates on several tyrosine residues, including Y992,
Y1045, Y1068, Y1086, Y1148 and Y1173 (36) (37). Also, EGFR is phosphorylated by active c-Src,
being Y845, Y891, Y920 and Y1101 its exclusive targets. Janus kinase 2 (Jak2) is also able to
phosphorylate EGFR at Y1068 (38).
Once phosphorylated, these tyrosine residues become binding sites for proteins with
phosphotyrosine-binding motifs, namely SH2 (Src Homology 2) or PTB (phosphotyrosine binding)

17
domains (39). Different classes of proteins bind to EGFR, including adaptors [growth factor receptor-
bound protein 2 (Grb2), Src homology 2 domain containing transforming protein c (Shc)], kinases [c-
Src, phosphoinositide 3-kinase (PI3K)], phosphatases (SHP1/2), lipases [phospholipase C-gamma
(PLCγ)], or members of the ubiquitination machinery (Cbl) (39). These form tight associations with
specific peptide sequences of phosphorylated tyrosine residues. For example, Shc binds via a PTB-
domain to Y1147 and Y1173 as well as via a SH2 domain to Y1173 (40) (41). Y992 and Y1173 were
also identified as binding sites for PLCγ (42). Y1068 and Y1086 are interaction sites for Grb2 (40),
while Cbl binds to Y1045 (43) and SHP1 to Y1173 (44). Result from these associations is the activation
of several relevant intracellular signalling pathways.

18
Figure 1-1. Epidermal Growth Factor Receptor Pathway.

19
1.2.1.2. Mitogen-activating protein kinases (MAPKs; Extracellular signal-regulated kinase,
ERK1/2)
Adaptors bind to signal transducers, resulting in the activation of different cellular signalling
pathways. Grb2 and Shc are key adaptors for the activation of the mitogen-activated protein kinases
(MAPKs) extracellular regulated kinase 1 (Erk1) and Erk 2 (45). Grb2 forms a complex with SOS (son-
of-Sevenless) that binds directly, or indirectly through Shc adaptor protein, to EGFR phosphorylated
tyrosine residues (46) (40). SOS is a guanine nucleotide exchange protein that undergoes three
dimensional changes, leading to activation of the guanine triphosphatase (GTPase) protein Ras. Ras is a
membrane-associated molecule activated by guanine nucleotide exchange factors (GEFs) such as SOS.
Ras cycles between an inactive guanine diphosphate (GDP) bound state and an active GTP. SOS
promotes the exchange of GDP for GTP and a GTPase activating protein (GAPs) is responsible of
enhancing the intrinsic GTPase activity of Ras, causing hydrolysis of GTP and returning Ras to its
inactive state. Inactivation of Ras by Ras-GAP is inhibited by EGFR Y992/SH2 complex (47). Active
Ras binds to distinct effector proteins that, in turn, activate downstream signalling cascades. Among
these effectors is Raf-1. Activated Ras binds to Raf-1, activating its kinase and inducing its
autophosphorylation at Ser338 and Y341 (48) (49). In turn, MAPK-kinases are activated by Raf-1 (50).
All MAPK pathways include a core three-tiered signalling unit, in which MAPKs are activated
by the sequential activation of linked serine/threonine kinases. Activation of MAPKs can leads to cell
proliferation, survival, and, in some cases, transformation. Binding of activator proteins (e.g. Ras) or
interaction with phosphorylated receptors activates MAPK-kinase-kinase (MAP3Ks). MAP3Ks regulate
MEK (MKK, MAPK-kinase) by catalyzing its phosphorylation in serine and threonine residues.
Activated MEK phosphorylates MAPKs on their threonine and tyrosine residues in their kinase
activation loop. Three distinct MAPK pathways have been characterized: ERK1/2, the c-Jun N-terminal
kinase or stress activated protein kinase (JNK/SAPK) and the p38 pathways.
ERK1/2 is activated by the EGFR tyrosine kinase and plays an essential role in cell proliferation.
Activation of Ras by EGFR causes activation of Raf-1, which directly activates MEK1/2 by
phosphorylating it on serine residues (51) (52). Activated MEK1/2 is a dual specificity kinase that
phosphorylates ERK kinases on their threonine/glutamic acid/tyrosine motif, resulting in both catalytic
activation of ERK and its translocation to the nucleus.
Activated Erk1/2 induces transcription of the cyclin D1 gene, through ribosomal S6 protein
kinase 2 (RSK2) activation, regulating assemble and activation of cyclin D1-Cdk4 (cyclin-dependent
kinase 4) complexes (53). Nuclear ERK interacts with specific transcription factors, such as ELK-1 and
c-Myc, leading to their phosphorylation and activation of specific transcriptional targets, inducing cell

20
migration and proliferation (54). Also, ERK 1/2 inhibits the activation of pro-apoptotic proteins Bax
(Bcl2-associated X protein), Bad (Bcl-2-associated death protein), and Bim (Bcl-2-interacting mediator
of cell death) (55) (56).
In contrast, EGFR signalling inhibits the activation of the other two MAPKs, p38 MAPK and
JNK via regulation of Vav2 (57). JNK and p38 pathways mediate responses to cellular stresses. Both
JNK and p38 are triggered by MAP3K. Three MAP3K families act upstream of JNK and p38 pathways:
MEK kinases (MEKKs), the mixed lineage kinases (MLKs), and the thousand and one kinases (TAOs).
JNK activates the nuclear transcription factor c-Jun while p38 phosphorylates myocyte enhancer factor
2A (MEF2A). Inhibition of p38 MAPK induces a conformational change, resulting in activation of Bax
and promotion of apoptosis (58). JNK is activated by EGFR TKIs, resulting in reduced expression of
MAPK phosphatase-1 (MKP-1), a JNK phosphatase, leading apoptosis in the NSCLC cell line PC-9
(59). Furthermore, the inhibition of JNK activation by ectopic expression of MKP-1 or a dominant-
negative form of JNK strongly suppresses EGFR TKI-induced apoptosis. Thus, JNK is critical for the
apoptotic action of EGFR TKIs.
1.2.1.3. PI3K/Akt pathway
Another relevant pathway regulated by EGFR activation is the PI3K/Akt pathway. Activation of
PI3K/Akt has been implicated in cell proliferation and survival, apoptosis resistance, tumour invasion
and migration (60). PI3K is formed by a catalytic subunit, p110, and an adaptor subunit p85. p85 is
responsible for the anchorage with EGFR through interaction of its SH2 domain, through the adaptor
Gab1 (GRB2-associated binding protein-1), with EGFR Y1068 and Y1086 (61). This interaction is
regulated by the phosphatase Shp2 (62). p100 catalyzes the phosphorylation of phosphatidylinositol 4,5-
biphosphate (PIP2) to phosphatidylinositol 3,4,5-triphosphate (PIP3) which in turn activates the protein
serine/threonine kinase Akt (60). PI3K phosphorylates phosphoinositides to produce PIP3. The major
negative regulator of PI3K is phosphatase and tensin homolog (PTEN), a phosphatase that
dephosphorylates PIP3 and PIP2. Loss of PTEN causes deregulated Akt activity and malignant
transformation (63). Signalling proteins containing pleckstrin homology (PH) domains bind to both PIP2
and PIP3 (64). The PH-domain containing protein serine/threonine kinases phosphoinositide-dependent
kinase-1 (PDK1) and Akt are recruited in the vicinity of activated EGFR and binding of PIP3 and PDK1
leads to autophosphorylation of Akt.
Substrates for activated Akt are classified as regulators for apoptosis or cell growth. Activation
of Akt results in anti-apoptotic signals through the phosphorylation of Bad, Bax, procaspase-9, p53
upregulated modulator of apoptosis (PUMA), forkhead transcription factor (FKHR), and up-regulation of

21
survivin, (65) (66) (67) (68) (69) (70). On the other hand, PI3K can also inhibit the cyclin-dependent
kinases p27KIP1 and p21WAF1, and activates the translation and stabilization of cyclin D, phosphorylating
the retinoblastoma protein which in turn promotes the G1-to-S phase transition of the cell cycle and
induces cell proliferation (71) (72) (73). Akt phosphorylates p21, sequestrating it in the cytoplasm and
reducing its ability to bond Cdk2 (74) (75). Akt also phosphorylates p27, impairing its nuclear import
(76). Therefore, PI3K/Akt pathway is crucial not only for survival but also proliferation of tumour cells.
1.2.1.4. Phospholipase C γ (PLCγ)
PLCγ is an enzyme containing two SH2 (C-SH2 and N-SH2) domains that mediates its
recruitment to EGFR. N-SH2 associates with EGFR at Y1173 and C-SH2 at Y992, stimulating its
phospholipase activity (42). PLCγ hydrolyzes the membrane PIP2 generating the second messengers
inositol 1,4,5 triphosphate (IP3) and diacylglycerol (DAG) (77). IP3 mobilizes Ca2+ from intracellular
stores by interacting with its receptor complex, formed by IP3R, the protein kinase A (PKA) and the
protein phosphatases PP1 and PP2A which are ubiquitously expressed on the endoplasmic reticulum
(78). DAG activates the isoenzyme protein kinase C (PKC) (79). Also PKC can inhibit the transfer of
EGFR from early to late endosomes, reducing its degradation.
1.2.1.5. Signal transducers and activators of transcription (STATs)
Signal transducers and activators of transcription (STATs) are a family of cytoplasmic, DNA
binding transcription factors that exist as inactive monomers containing SH2 domains for interacting
with phosphotyrosine residues. Also, STATs contain a single tyrosine phosphorylation site and, in a
dimeric partner molecule, a DNA interaction domain, and a number of protein-protein interaction
domains (80). STATs carry out a dual function: signal transduction and activation of transcription. In
normal cells, STAT activation is transient but in certain tumour cells STATs are constitutively active
(81) (82). In A431 cells, after EGF stimulation, EGFR gets phosphorylated at Y845 and forms a complex
with STAT1, 3, and 5 which in turn get rapidly phosphorylated (83) (84). STAT1 gets phosphorylated at
Y701 and STAT3 at Y705. This EGFR-induced STAT activation is Src-dependent, which is
phosphorylated and rapidly recruited by EGFR/STATs complexes. Proline-rich tyrosine kinase 2 (Pyk2),
a focal adhesion kinase that can be activated by c-Src and EGFR, is also recruited to this complex
facilitating EGFR-mediated STATs phosphorylation and enhancing STAT-induced cell proliferation and
target genes transcription (85). Once phosphorylated, STATs form homo or heterodimers and
subsequently are transported to the nucleus where they regulate gene expression involved in cell-cycle

22
progression, angiogenesis and antiapoptotic signals (86) (87) (88) (81). Following gene regulation
STATs are dephosphorylated by SHP-2 in the nuclei (89).
1.2.1.6. EGFR endocytosis and downregulation
EGFR is removed from membrane by endocytosis, being permanently inactivated through
degradation in lysosomes or recycled back to the plasma membrane. C-terminal sequences 1005-1017
and the 1010LL1011 motif are essential for EGF-induced EGFR endocytosis, a process which is
independent of EGFR tyrosine kinase activation and phosphorylation status (90). Binding of EGFR
pathway substrate 15 (Eps15) is involved in receptor endocytosis (91). EGFR gets ubiquitinated at the
plasma membrane followed by clathrin-dependent EGFR internalization into coated pits, entering the
endocytic pathway and trafficking to lysosomes for degradation (92).
The proto-oncoprotein c-Cbl has a tyrosine kinase binding domain containing E3 ligase that
promotes the ubiquitination of EGFR (93). Grb2 is required for the recruitment of the RING domain of
c-Cbl to the EGFR and subsequent receptor entry into the clathrin-mediated endocytic pathway (94). c-
Cbl is phosphorylated by EGFR, activating its ubiquitin ligase activity, recruiting the ubiquitin-
conjugating enzyme UbcH7 (95). c-Cbl regulates EGFR endocytosis by forming endocytic complexes
formed by CIN85 (Cbl interacting protein of 85k) and endophilins (regulatory components of clathrin-
coated vesicles) with EGFR at the cellular membrane in which CIN85 binds to the distal carboxyl
terminus of Cbl on EGFR phosphorylation (96). This complex forms prior to receptor recruitment into
clathrin-coated pits and remains associated throughout the clathrin-mediated endocytic pathway (97). Cbl
mutants lack ubiquitin ligase activity, resulting in the recycling of the activated EGFR back to the plasma
membrane and prolonging EGFR signalling. EGFR phosphorylation of serines and threonines is
connected to receptor downregulation by regulatory feedback mechanisms (98). Serines are modified by
CaMK, while threonines are targets of Erk1/2 or PKC (37). Protein tyrosine phosphatases can eliminate
docking sites for proteins containing SH2 domains; also they can dephosphorylate regulatory sites in the
kinase activation loop (99).
1.2.1.7. Special EGFR activation
EGFR can also be activated by forming heterodimers with other receptors, including members of
the HER family. A special dimer is the one formed between EGFR and ERBB3, a receptor with an
inactive kinase, as PI3K docking sites are particularly prevalent in ERBB3 (100). EGFR can also be
activated through heterodimerization with insulin-like growth factor receptor 1 (IGF-1R) (101). This

23
IGF-1R/EGFR transactivation is mediated by an autocrine mechanism involving matrix metalloprotease-
dependent release of heparin-binding EGF (HB-EGF). IGF-1R induces phosphorylation of EGFR/Shc
complexes, activating Erk1/2. EGFR can also be activated by extracellular matrix elements. In the
absence of ligand or EGFR overexpression, urokinase plasminogen (uPAR), through its domain1,
induces an association of EGFR with α5ß1 integrin, linked by focal adhesion kinase (FAK), inducing its
activation and subsequent Erk phosphorylation (102).
EGFR can also become phosphorylated by external stimuli. Ionazing radiation can activate
EGFR within minutes, indicated by its phosphorylation on Y845 (103). This early phase is reversible and
return to baseline within 10 minutes. A second activation starts after 30 minutes, induced by a late
release of TGF-α. This biphasic radiation-induced EGFR response stabilizes src kinase and subsequent
caveolin Y14 phosphorylation and also activates Ras, Raf-1, PI3K, PLC-γ and MAPK, inducing x-ray
repair cross complementing protein 1 (XRCC1), DNA-dependent PK catalytic subunit (DNA-PKcs),
proliferating cell nuclear antigen (PCNA) and BCL-XL and resulting in DNA repair and cell
proliferation (104) (105) (106). Also, through a heterodimer with HER2, radiation induces Akt activation
via EGFR phosphorylation (107). After radiation exposure EGFR is translocated to the nucleus where it
is involved in DNA-PK regulation, resulting in DNA repair and survival (108). Ultraviolet-A rays
(UVA), UVB, UVC, H2O2 and SH-alkylating agents also inhibit the dephosphorylation of EGFR by
oxidating SH-groups or by modificating the active centre of tyrosine phosphatases resulting in a
continuous binding of Shc isoforms to tyrosine-phosphorylated EGFR leading to activation of PLCγ,
Ras, Erk1/2 and Elk-1 (109).
Oxygen radicals and cigarette smoke can also induce a prolonged EGFR activation characterized
by an enhanced phosphorylation on Tyr residues 845 and 1173, the former being Src-mediated, and lack
of phosphorylation on Tyr1045, the docking site for the ubiquitin ligase c-Cbl via Grb2. Due to this,
there is a loss in EGFR internalization and degradation, with EGFR remaining at the cell surface and
minimally endocytosed via caveolae-mediated Src-dependent phosphorylation of caveolin-1 (110) (111)
(112). EGFR phosphorylation by oxygen radicals activates PLC-γ but not MAPKs and decreases PKC-α
activity by its translocation to the cytoplasm (113). Cigarette smoking results in activation of Akt and
Erk1/2 pathways (110). Lipid peroxidation after oxidative stress produces 4-hydroxynonenal (HNE)
which in turn activates EGFR followed by phosphorylation of the adaptor Shc and activation of MAPK
(114). However, HNE-induced EGFR activation results in growth inhibition.
In a squamous cell carcinoma cell line hyperthermia induces EGFR activation. Incubation at
42°C induced a ligand-independent, JAK2 mediated, EGFR activation by a transactivation with Toll-like
receptors 2 and 4 (TLR2/4), interaction mediated by a heat shock protein 70 (Hsp70) autocrine loop

24
resulting in the activation of ERK1/2, PLCγ1 and STAT3 (115). Arsenic exposure has also shown to
activate EGFR without involving Y1173, followed by c-Src activation and Erk1/2 phosphorylation (116).
1.2.1.8. EGFR nuclear translocation
Activated EGFR is internalized into clathrin-coated pits formed by the GTPase dynamin and into
the endosomal compartment and then either sorter into lysosomal degradative compartment or recycled
(90) (117). EGFR located within the membrane of late endosomes is transferred to the membranes of
Golgi apparatus by membrane fusion and locates in the endoplasmic reticulum (ER) membrane. EGFR
internalization can be impaired by Abl activation of EGFR at Y1173, allowing it to escape the formation
of complex with Cbl (117). Cell exposure to oxidative stress can lead to internalization of EGFR into
caveolae and is associated with perinuclear accumulation of EGFR with persistent kinase activity (118).
EGFR is translocated into the nuclei after TGF-α (119), ionizing radiation (108) or EGF-induced
(120) (121) activation. The mechanisms proposed for nuclear transport of membrane proteins include the
activity of transmembrane domain-binding chaperones, endosome-mediated nuclear translocation, and
retro-translocation by ER-associated trafficking machinery (122). A putative nuclear localization signal
within the juxtamembrane domain is necessary to enter the nuclei, a process initiated through
internalization/endocytosis machinery (88). For nuclear transport EGFR has to be set free from ER
membrane to become a cytosolic protein followed by interaction between the karyopherin system and the
intrinsic nuclear localization site (NLS) of the EGFR. In the endoplasmic reticulum, where the presence
of mature C-terminal fragments is larger than intact receptors, EGFR associates with Sec61 which in turn
retrotranslocates the receptor into the cytoplasm and is also responsible for its presence in the nuclei
(120). In order to pass through the nuclear pore complex EGFR needs to bind to karyopherin ß, using a
complex formed by karyopherin α and RAN-GTP as adapter (108). Also, movement through the nuclear
pore complex is potentially mediated through importins ß1 and α and exportin CRM1 (108). Necessary
for karyopherin binding is the presence of a NLS in the cargo protein. EGFR has such putative NLS
sequence. In fact, EGFR gets phosphorylated at T654, present in its NLS sequence, after its nuclear
transport (123) (108). This phosphorylation is mediated by activation of the PKCε (124). In addition to
be trafficked into the endoplasmic reticulum, activated EGFR at the Y1173 is trafficked also to the nuclei
in a manner that requires cellular metabolism (120). Nuclear export of EGFR may involve exportin
CRM1 (125).
Nuclear EGFR is composed of both complete receptors and fragments lacking ectodomains
residues (108) (119) (121) (123). Nuclear EGFR functions as transcriptional activator with a functional

25
transactivation domain that recognizes AT-rich sequences (ATRs) of target gene promoters and activates
their expression (123). Nuclear EGFR lacks a putative DNA-binding domain but it activates gene
expression by first associating with DNA-binding transcriptional molecules such as STAT3, STAT5A
and E2F1 enhancing transcription of target genes via intrinsic transactivational activity (88) (125) (126).
Promoters associated with nuclear EGFR are involved in cell proliferation, regulation of G1/S
progression, and tumourigenesis, including cyclin D1 (123) (119), B-Myb (125), c-fos (88), and
inducible nitric oxide synthase (iNOS) (88) and the kinase Aurora-A, involved in cell-cycle progression
(126). Also, nuclear EGFR may play a role in DNA repair through interaction with DNA-PK, an enzyme
involved in repair of double strand breaks, inducing its phosphorylation at residue at residue Thr2609,
which indicates that DNA-PK is active in end-joining DNA repair (127). This has been observed in
response to irradiation or oxidative stress but only with wild-type EGFR, as cells with EGFR TK domain
(TKD) mutations do not translocate into the nuclei in response to radiation enhancing response (128)
(108) (129). Ionizing irradiation has been shown to cause nuclear transport of EGFR through caveolin-
and PKC-dependent mechanisms (108). Furthermore, nuclear EGFR is involved in DNA replication and
repair and finally cell proliferation through phosphorylation at Y211 of PCNA (130). Inhibition of the
phosphorylation led to degradation of the chromatin-bound, but not the unbound, form of PCNA through
a proteasome-dependent manner and consequently suppressed its function in DNA synthesis and DNA
damage repair. EGFR nuclear trafficking can be inhibited by the growth inhibitor vitamin D
(1,25(OH)2D3), which subsequently repressed the cyclin D1 gene and suppressed tumour growth (119).
1.2.2. EGFR expression in NSCLC
EGFR is expressed by many solid malignancies, including gliomas, colorectal, pancreas,
esophageal, gastric, bladder, kidney, prostate, ovary, breast, head and neck, and NSCLC (131) (132)
(28). In NSCLC, presence of EGFR has shown to be dysregulated with adverse prognostic implications
via increased ligand production, receptor overexpression, receptor phosphorylation, increased gene copy
number or presence of gene mutations (133) (134) (131) (132) (27) (35) (135).
1.2.2.1. EGFR gene expression
The EGFR genomic abundance in tumours has been evaluated by Southern and northern
blotting, reverse-transcription and quantitative real-time polymerase chain reaction (qRT-PCR), and
chromogenic (CISH) or fluorescence (FISH) in situ hybridization. EGFR messenger ribonucleic acid
(mRNA) expression is found in normal lung but in comparison with paired tumour samples it shows

26
overexpression in around 50 % of malignant specimens with median EGFR mRNA expression by qRT-
PCR of 1.9 (range, 0.17-28.27) and median EGFR gene dosage by qPCR of 0.36 (range, 0-4.51) relative
to reference genes (136) (137). However, using northern blot analysis in 48 multi-treated, multi-staged
NSCLC patients, Rusch et al observed that mRNA expression of EGFR was comparable at the protein
level by immunohistochemistry (IHC) only when 100% tumour cells showed staining at moderate to
high level (138). Less intense or staining restricted to few cells did not show correlation with mRNA
levels. In fact, 9 cases were excluded due to a small amount of viable tumour cells present in the samples
collected. Overall, EGFR mRNA levels are not different among histological types, tumour advancement,
grade differentiation or survival (136).
Blotting and PCR-based techniques are global extraction-based methods that can be influenced
by the contamination from stroma and infiltration of reactive cells, elements regularly present in human
tumour samples, resulting in the dilution of tumour cell gene copy. Also, with PCR-based assays
normalization using another region of the studied chromosome, such as centromeric sequences, is
difficult as it will detect true amplification but will not detect high polysomy. Due to this, tissue-based
techniques such as CISH and FISH are more widely accepted for assessing EGFR gene levels.
CISH is a tissue-based technique with the advantage of using brightfield microscopy and
therefore being correlated directly with histopathology. Furthermore, as with immunohistochemistry,
CISH-stained slides can be archived and stored permanently. However, CISH has a lower level of
resolution than FISH and is suitable for only a single color assay preventing the simultaneous use of a
control probe. To solve this, gene/chromosome probes are counted in parallel sections and converted into
the number of nuclear signals per cell.
As CISH-scoring systems depend only on an EGFR gene signal, a study comparing the
performance of FISH and CISH for the detection of increased EGFR copy number in 77 female, non-
smokers, Asian patients with NSCLC treated by surgery alone found a significant correlation between
both methods (Spearman's r=0.81; p<0.0001) (139). Discrepancies between the two tests were seen in
only 7% of cases. At a signal of 4.5, CISH had very high sensitivity (89%) and specificity (89%) for the
discrimination of low and high EGFR polysomy (p<0.0001) and at a signal of 7.1, CISH was also
effective at distinguishing between high polysomy and amplification (p=0.0003). Another study
compared CISH and FISH assays for the detection of EGFR gene in NSCLC (140). In 58 specimens, the
concordance between the CISH and FISH was 93% for observer 1 (κ coefficient = 0.64) and 95% for
observer 2 (κ coefficient = 0.76). Therefore CISH is an assay with potential comparable results to FISH,
but the latter is the assay most commonly used for determining EGFR gene status in NSCLC.

27
FISH is an in situ method that allows identification of single cells in the context of the tissue
architecture. FISH enables simultaneous assessing of multiple targets on the same or separate
chromosomes, allowing control probes to be hybridized and used as a reference. The fluorescent labels
enable the visualization of the number of copies and location of the target genes in metaphase as well as
interphase nuclei. FISH assessment of EGFR has been widely used and a clinical classification exists to
categorize patients as responders to EGFR TKIs. The development of an EGFR genomic gain
classification was based on 102 pre-treatment samples of gefitinib-treated patients. Disomy for the EGFR
gene was present in 35.3% of case patients, low trisomy in 16.7%, high trisomy in 2%, low polysomy in
13.7%, high polysomy in 19.6%, and gene amplification in 12.7% (141). Tumours are considered FISH-
positive if they show amplification (the presence of tight gene clusters and a ratio of ≥2
genes/chromosomes per cell or ≥15 gene copies per cell in ≥10% of analysed cells) or high polysomy (≥4
copies of the gene in ≥40% of cells).
In a comparison using FISH, relative gene expression was 2.90 (0.17–28) in 40 specimens with
low EGFR gene copy numbers (disomy to low polysomy) and 7.15 (0.19–28.3) in 23 specimens with
high EGFR gene copy numbers (high polysomy and gene amplification) being particularly high among
nine tumours with gene amplification (average: 8.46, 1.7–21.5) (141). There was a statistically
significant positive correlation between the relative expression and the gene copy number (Pearson r =
.33; P = .007), indicating that specimens with gain in copy numbers had higher levels of gene expression.
However, there are several technical considerations that could compromise the FISH assay, including
lengths of proteinase K digestion, probe hybridization duration and conditions but it can be considered
the assay most often implemented in evaluating the NSCLC response to EGFR TKIs (142).
1.2.2.2. EGFR Gene mutations
1.2.2.2.1 EGFR extracellular domain mutations
Three different types of deletion mutations (categorized according to the extent of deletion, and
termed EGFR vI, EGFR vII and EGFR vIII) have been reported in the extracellular domain of the EGFR
gene (143). The most common of the three is EGFR vIII. EGFR vIII is a deletion of domains I and II in
the extracellular domain of the EGFR gene with the receptor derived from this mutation presenting an
absence of amino acids 30-297 at the N-terminal domain (143). This mutation often accompanies gene
amplification, resulting in its overexpression. EGFR vIII does not form dimers but is constitutively
active, bounding to Shc adapter protein (144). EGFR vIII does not activate MAPK or PLCγ pathways. In
pulmonary tissue, EGFR vIII may play a role in the pathogenesis of NSCLC but its presence in
squamous-cell carcinoma is low (5 %) while it is absent in adenocarcinoma (145) (146).

28
1.2.2.2.2. EGFR cytoplasmic domain mutations
1.2.2.2.2.1. EGFR TKD mutations responsive to EGFR TKIs
Retrospective analysis of clinical data consistently demonstrated that a clinical response to
EGFR TKIs was more common in women than in men, in Asian people than in individuals from Europe
or the USA, in patients with adenocarcinoma than in those with other histological subtypes, and in
individuals who have never smoked than in those with a history of smoking (147). Three independent
reports found that mutations in the tyrosine kinase domain of the EGFR were present at a higher rate in
these populations and were associated with a better response to EGFR TKIs (148) (149) (150). These
mutations are somatic in origin and are found in around 30% and 10% of Asian and North-American
NSCLC patients respectively (151) (152) (153).
Mutations are divided into 4 major types: point mutations in exon 18 (G719A/C), in-frame
deletions in exon 19 eliminating four amino acids (LREA) downstream of the lysine residue at position
745, insertions in exon 20, and point mutations in exon 21 (L858R and L861Q). Particularly, the 2 most
frequent mutations are deletion around codons 746 to 750 of exon 19 and transversion of T to G in codon
858 of exon 21, with an amino acid change from leucine to arginine (L858R). These 2 mutations account
for approximately 90% of intracytoplasmic mutations of EGFR (149) (154) (155) (30).
Mutations in EGFR TKD exons code for the N-lobe and the 5’ portion of the C-lobe (151).
EGFR TKD mutations result in a repositioning of critical residues surrounding the ATP-binding cleft of
the TKD, causing a conformational change which results in constant activation of the EGFR TK due to a
ligand-independent dimerization (156). This in turn results in an increased and sustained phosphorylation
of particular tyrosine residues at the C-terminal (156) (148). In both L858R and exon 19 deletion
mutants, EGF induced an increased phosphorylation of EGFR at Y992 and Y1068 but not at Y1045 and
Y1173 comparing with wild type (157). Also, Y845 was highly phosphorylated only in L858R mutant.
Presence of EGFR TKD mutations also result in a stable interaction with EGFR TKIs, leading to an
increase of <100-fold in sensitivity to inhibition compared with wild-type receptors (148) (157).
Although these mutations are almost exclusively seen in NSCLC they have also been found in
normal lung tissue surrounding malignancies in the majority (158) (159) (160) (161) (162) but not all
(163) studies. EGFR TKD mutations have shown to be oncogenic as well. In transgenic mice expressing
either exon 19 deletion or L858R mutation in type II pneumocytes, controlled expression by doxycyclin
led to adenocarcinoma formation, transformation associated with EGFR, SHC and STAT activation, and
regression following EGFR TKI treatment or doxycycline withdrawal (164) (165) (166). In addition,
EGFR TKD mutations were detected in some cases of atypical adenomatous hyperplasia, known to be

29
precursor lesions for bronchioloalveolar carcinoma (BAC), suggesting that EGFR TKD mutations may
be involved in the early development of pulmonary neoplasias (167).
The prevalence of EGFR TKD mutations is higher among patients with clinical characteristics
associated with response to EGFR TKIs. For example, in an analysis of 617 NSCLC samples from both
Asian and non-Asian origin EGFR TKD mutations were detected in 130 (21%) of the 617 NSCLCs
(168). The frequency of mutations was greater for patients of East Asian ethnicity versus those of other
ethnicities (30% versus 8%, p < .001), females versus males (42% versus 14%, p < .001), never smokers
versus ever smokers (51% versus 10%, p < .001), and for adenocarcinomas versus other histologies (40%
versus 3%, P < .001). On the other hand, in 860 non-Asian, surgically treated multi-staged NSCLC
patients there were no EGFR TKD mutations in 454 squamous-cell carcinoma and 31 large-cell
carcinoma cases investigated but a total of 39 mutations in the 375 patients affected by lung
adenocarcinoma (10%) (162). The frequency of non-smokers in tumours having EGFR TKD mutations
was significantly higher than that observed in the series of tumours without mutations, (p = 0.000006).
Among the 39 tumours with EGFR TKD mutations, 23 (59%) were from non-smokers, and 16 (41%)
were from smokers or former smokers. EGFR TKD mutations were more frequent in women (21 of 71;
30%) than in men (18 of 304; 6%; p= .0000002). Finally, in a large-scale screening program
implemented in Spain for patients with advanced NSCLC in 350 of 2105 patients (16.6%) EGFR TKD
mutations were detected (169). Mutations were more frequent in women (69.7%), patients who had
never smoked (66.6%) and with adenocarcinoma (80.9%). The mutations were deletions in exon 19
(62.2%) and L858R (37.8%). Overall, the prevalence of EGFR TKD mutations varies by ethnicity with
ranges from 20–40% in Asian populations (168) (161) (163) (161) to 5–20% among Caucasians (141)
(162). In fact, even when analysis is confined to a never smoked with adenocarcinoma subgroup (n =
157), the frequency of EGFR TKD mutations is significantly higher for patients from Japan and Taiwan
than for those from the United States and Australia (64% versus 36%), both before and after adjustment
for sex (p = .003 and .004, respectively) (168).
However, these associations with clinical characteristics are not exclusive. Although EGFR TKD
mutations are inversely associated with the total amount of tobacco smoked they have also been detected
in more than 20% of patients with a history of heavy smoking (163). Furthermore, recent studies indicate
that, although associated with adenocarcinoma histology, in fact EGFR TKD mutations may be
encompassed in particular adenocarcinoma cellular sub-types. In a report of 195 adenocarcinomas, 149
were of the terminal respiratory unit (TRU) type (defined as expression of thyroid transcription factor I
and surfactants proteins and lepidic growth in the periphery) with EGFR TKD mutations being detected
in 97/195 adenocarcinomas, specifically 91/149 TRU-type and in only 6/46 tumours of other subtypes)
(167). Also BAC component, lepidic growth, hobnail cells, micropapillary morphology and well to

30
moderately differentiated grade are histologic characteristics reported to predict a higher prevalence of
EGFR TKD mutations in NSCLC adenocarcinoma. (154) (170) (171) (171) (162).
1.2.2.2.2.2. EGFR TKD mutations resistant to EGFR TKIs
EGFR TKD mutations can also be resistant to currently available EGFR TKIs. Substitution at
codon 790, resulting in an amino acid shift from threonine to methionine (T790M) is reported to be an
EGFR TKIs resistance–inducing mutation (148) (172). EGFR T790M is the first mechanism discovered
responsible for the acquired resistance observed in the majority of initial responders to EGFR TKIs (173)
(174). This mutation is observed in approximately 50% of cases developing acquired resistance to EGFR
TKIs. The threonine residue located near the kinase active site appears to be critical for the binding of
ATP. It is also critical for binding of EGFR TKIs resulting in an alteration of the topology of the ATP-
binding pocket (175). Structural modeling suggests that, in fact, the T790M mutation creates steric
hindrance that prevents EGFR TKIs from interacting with the ATP-binding pocket of the receptor and
therefore impeding the inhibition of the phosphorylation of the receptor. It has also been proposed that
T790M increases the affinity of the kinase domain for ATP (176)
T790M mutation was initially thought to occur during the course of treatment with EGFR TKIs,
as it was identified in a patient with NSCLC who relapsed after 24 months of complete remission despite
continued gefitinib therapy (173). However, using sensitive assays, the T790M mutation has also been
detected in NSCLC tumour specimens obtained from patients before treatment with EGFR TKIs (177)
(178). Although significant responses were achieved with EGFR TKIs in these patients, the presence of
T790M before treatment was associated with a significantly shorter PFS compared with patients without
detectable T790M. These observations suggest that a small fraction of NSCLC tumour cells may harbour
the T790M mutation before treatment with EGFR TKIs and that these cells become predominant as a
result of their selective proliferation, resulting in the development of clinical resistance.
Other resistance point mutations, such as aspartic acid-761 to tyrosine (D761Y), have been
reported, some of which may weaken the interaction of EGFR TKI with its target (172).
1.2.2.3. EGFR protein expression
Detection and measurement of EGFR protein itself in tumour specimens can be achieved by
different assays including radioactive-labelled ligand binding, competitive immunoabsorbent, western
blotting and IHC.

31
Using a radioligand binding analysis, Fujino et al showed that concentration of the EGFR from
74 NSCLC specimens is higher than in normal lung tissue without significant difference between
adenocarcinoma and squamous-cell carcinoma (132). Also, Velae et al observed a worse prognosis in 19
NSCLC patients with high membrane EGFR concentration (179). Using an enzyme-linked
immunoabsorbent assay (ELISA) in 190 lung cancer patients, EGFR protein showed a good correlation
with the percentage of positive tumour cells by IHC (r=0.63), improving when a scoring system taking
into consideration percentage, intensity, and relative tumour area was implemented (r=0.76) (180). These
assays confer the advantage of objective quantification but they need protein extracted from fresh or
frozen samples. Such extraction can be affected by the presence of non-tumour content and requires
special resources and facilities.
Although its semiquantitative nature and difficulties with standardization are limiting factors,
assessing EGFR by IHC offers the advantages of evaluating the cellular and sub-cellular compartment
distributions of the receptor, allowing the use of formalin-fixed, paraffin-embedded (FFPE) samples, and
is routinely used in clinical practice.
In normal lung and bronchial tissue, EGFR has shown to be present in 70 % of samples with a
strong band in the basal layer and weak staining in bronchial glands (181) (182). In bronchial epithelium
of high-risk smokers overexpression of EGFR is one of the earliest and most consistent abnormalities; it
is present at the stage of basal cell hyperplasia and persists through squamous metaplasia, dysplasia, and
carcinoma in situ (183).
EGFR staining is stronger in NSCLC than normal lung tissue (181). In multi-staged NSCLC
cohorts, EGFR is expressed and over-expressed in 57 % to 94 % and 67 % to 92 % of squamous cell
carcinoma, in 35 % to 70 % and 45 % to 65 % of adenocarcinoma, and in 23 % to 69 % and 33 % to 65
% of large cell carcinoma respectively (181) (184) (185) (186) (182) (133). Adenosquamous shows an
expression and overexpression of EGFR in 100% and 75% of cases (181). It is not expressed by small
cell lung carcinoma (187).
EGFR is also expressed in stage I NSCLC, with 47% of cases having at least 10% of tumour
cells showing membrane staining. Squamous-cell carcinoma has a higher EGFR prevalence than
adenocarcinoma (59% vs 37%) but its expression is not prognostic of recurrence or survival in the
overall stage I population although EGFR overexpression was shown to be a negative prognostic survival
factor in T1N0 cases (RR=0.12, p=0.04) (188). Nevertheless, in a meta-analysis of 10 studies
investigating the prognostic value of EGFR, Nicholson et al found that the presence of EGFR was a
weak prognostic indicator among NSCLC cases (189).

32
It is necessary to take into consideration that several technical factors can influence the
immunoreactivity and staining of IHC including time and conditions of fixation, storage time, as well as
specificity of the primary antibody implemented (190) (191). Also, the choice of qualitative or semi-
quantitative assessment methods and cut-off point for EGFR IHC scoring systems may affect the
classification of a sample. Finally, the representative value of a single biopsy properly expressing the
whole tumour may raise some concerns. Therefore careful standardization and validation of operational
procedures is necessary to secure consistent results.
1.2.3. Anti-EGFR strategies
Therapies specifically directed against EGFR can be classified as antibodies (Abs) blocking the
extracellular domain and competing with extracellular ligands, or TKIs, either reversible or irreversible,
competing with ATP to bind with the TKD. Although different Abs and compounds specific to EGFR or
developed against different TKs have been in development for several years, EGFR targeting drugs
currently approved for clinical use are the monoclonal Abs (mAbs) cetuximab (IMC-225 or
ERBITUX®) and panitumumab (VECTIBIX®) and reversible TKIs including the quinazoline-based
compounds OSI-774 (erlotinib or TARCEVA®) and ZD 1839 (gefitinib or IRESSA®).
1.2.3.1. Anti-EGFR Abs
Anti-EGFR mAbs are currently being explored as monotherapy and in combination with
radiation, chemotherapy, or other biologically targeted agents for the treatment of NSCLC. Current
evidence indicates a limited role of these in the treatment of NSCLC except for the First-Line trial for
patients with EGFR-EXpressing advanced NSCLC (FLEX) trial which will likely lead to the registration
of cetuximab in combination with chemotherapy as first-line treatment of advanced EGFR-expressing
NSCLC patients (192).
1.2.3.1.1. Cetuximab (IMC-225; ERBITUX ®)
Cetuximab is a chimeric mAb of 152 kDa that acts by binding to the extracellular domain of the
EGFR near its ligand binding site with five times more affinity than natural ligands, blocking
ligand/receptor interaction and subsequent activation of the intracellular signaling pathways PI3K/Akt
and Ras/Raf/MAPKs (193) (194) (195) (196). Interestingly, cetuximab can also induce EGFR
phosphorylation, promoting its internalization and inducing G1 growth arrest by upregulating p27(KIP1)

33
and p15(INK4B) (197) (198). Cetuximab-induced EGFR internalization is slower than that observed
following EGFR stimulation and is independent of EGFR TK activity or entrance to coated-pits (199).
Also, cetuximab induces apoptosis by decreasing Bcl-2 and increasing Bax (200) (201). Furthermore, in
EGFR+ cells, cetuximab reduces vascular endothelial growth factor (VEGF) production (202). Finally,
cetuximab is an IgG1 Ab and therefore may also induce antibody-dependent cell-mediated cytotoxicity,
although the clinical relevance with regard to the antitumour efficacy is likely to be low (135). In
xenograft models, cetuximab has induced response in both wild-type and tumours harbouring EGFRvIII
mutations (203) (204) (205).
Particular observations have been made in regards to cetuximab and EGFR nuclear localization.
Cetuximab induces EGFR nuclear translocation, a process inhibited by radiation (121) (108). Cetuximab-
induced nuclear EGFR localization is Sec61ß translocon retrotranslocation-mediated and is mainly
composed of full length receptors with carboxy-terminal fragments starting to be present after prolonged
cetuximab exposure (121). In the nuclei, cetuximab triggers an early physical interaction between EGFR
and a 350-kDa catalytic subunit of the DNA-PK or its regulatory heterodimer complex Ku70/80. In
response to DNA double strand breaks, one of the main DNA lesions induced by radiation, DNA-PK is
activated by phosphorylation and together with its regulatory subunits KU70 and KU80, stabilizes the
break. Treatment with cetuximab, but not EGFR TKIs, colocalizes DNA-PK with EGFR in the
cytoplasm, reducing the levels of DNA-PK and its activity in the nuclei, increasing residual DNA
damage and reducing survival after radiation (108) (127).
Following safety studies in combination with standard chemotherapy, cetuximab was tested in
phase II trials in previously treated, advanced NSCLC patients. In a trial of EGFR IHC+ patients,
cetuximab combined with docetaxel induced a 20% response rate with 36.4 % of patients having stable
disease (206). Also, in unselected patients cetuximab as a single agent induced a response rate of 4.5%
and stable disease was seen in 30.3 % (207). As a first-line option cetuximab has been amply studied. In
EGFR IHC+ patients, the addition of cetuximab to cisplatin/vinorelbine improved the response rate from
28% to 35% and in unselected patients, its addition to a cisplatin-based regimen improved the response
rate from 18.2% to 27.7% (208) (209). These trials were the foundation for the assessment in phase III
trials of regimens combining cetuximab as first-line options for advanced NSCLC.
Cetuximab has also been assessed in earlier stages combined with other therapies. In a phase II
study in 93 patients with locally advanced stage IIIA/B NSCLC the combination of cetuximab and
chemoradiotherapy gave a response rate of 62% and median survival time of 22.7 months (210). Also, a
phase II study of neoadjuvant cetuximab in combination with cisplatin and gemcitabine in patients with
resectable stage IB–IIIA NSCLC is ongoing but preliminary results on 27 patients include a response
rate of 76% (211).

34
1.2.3.1.2. Panitumumab (ABX-EGF; VECTIBIX®)
Panitumumab is a fully human IgG2 mAb targeting the extracellular domain of the EGFR,
competing with ligands, promoting receptor internalization and inhibiting EGFR signaling (212).
However, panitumumab does not induce receptor degradation upon internalization, suggesting a
recycling process to the surface (213).
In EGFR-overexpressing xenografts models panitumumab has shown antitumour effect alone
and in combination with different agents (212). In clinical practice, only one randomized phase II trial
has evaluated the activity of carboplatin plus paclitaxel with or without the addition of panitumumab in
chemotherapy-naive, EGFR IHC+, advanced NSCLC patients (214). Preliminary results show that
panitumumab failed to improve any outcome.
1.2.3.1.3. Matuzumab (EMD72000)
Matuzumab is a humanized mAb of the IgG1 subclass that binds selectively to EGFR and
inhibits ligand-mediated activation and activation of MAPKs and PI3K/Akt (215). Compared with
cetuximab, matuzumab has a longer half-life of 6–8 days and does not induce autoantibodies (216). In
preclinical xenograft models, substantial antitumour activity has been shown. A phase I study explored
weekly doses of matuzumab (100, 200, 400, or 800 mg) followed by paclitaxel in 18 patients with EGFR
IHC+ advanced NSCLC with a response rate of 22.2% being observed (217).
1.2.3.2. Reversible TKIs
Reversible TKIs have been the most successful agents to date targeting EGFR for the treatment
of NSCLC.
1.2.3.2.1. Gefitinib (ZD1839; IRESSA®)
Gefitinib selectively inhibits the EGFR TK activity by competing with ATP to bind the TK
pocket, blocking activation of EGFR and subsequent intracellular signaling pathways, such as the
ERK1/2 and PI3K/Akt, affecting cell growth and survival (218). Gefitinib also induces apoptotic signals
by promoting cytochrome c release via Bim, Bax, Bad and Puma (219) (220) (221) (222) (223) (224)
(225) (226). Gefitinib depresses cyclin D1 mRNA levels as well as causes the accumulation of p27KIP1
and p21WAF1/CIP1 and up-regulates p15INK4b, resulting in cell growth inhibition by arrest in G0/G1 phase

35
(227) (228) (229). Gefitinib can also inhibit cell invasiveness. In keratinocyte and cutaneous squamous
cancer cells, gefitinib blocks EGF-induced cytoskeleton remodelling and in vitro invasiveness, as well as
cell growth by an inhibitory effect on ERK1/2 and p21-activated kinase 1 (Pak1) activities (230).
In phase I studies, gefitinib showed anti-tumour effects in subjects with various solid tumours
refractory to standard therapies. In phase II studies, gefitinib demonstrated clinically significant anti-
tumour activity, inducing response in 10% and improving symptoms control in 40% of patients with
locally advanced or metastatic NSCLC refractory to platinum-based and docetaxel chemotherapy (231)
(232). Also, in Asian patients harbouring EGFR TKD mutations a response rate of 75% and 1-year
survival of 79% were obtained (233). Several phase II trials have also evaluated the role of gefitinib as
first-line therapy in advanced untreated NSCLC (234) (235) (236) (237). In unselected populations, the
overall response observed was 4% to 9.8% with a median survival of 2.7 to 7.2 months. Particularly in
adenocarcinoma with BAC features, gefitinib use resulted in a response rate from 9% to 17% with a
median survival of 13 months. This was even improved in Asian patients with a response rate of 25% to
54.5% and median survival of 9.4 to 22.4 months. In North-American patients harbouring EGFR TKD
mutations a 55% response rate was also obtained (238). Furthermore, in Asian patients with EGFR TKD
mutations gefitinib induced a response rate of 63.2% to 66% with a median survival of 17.8 months to 20
months (239) (240). Finally in an Asian, never-smokers with adenocarcinoma population a response rate
of 69% and an estimated 1-year survival of 73% was observed (241).
1.2.3.2.2. Erlotinib (OSI-774; TARCEVA®)
Erlotinib or OSI-774 is an orally active quinazolinamine small molecule that acts as a selective,
reversible EGFR TKI. Erlotinib is a specific inhibitor for EGFR (IC50=19 nM), but is less reactive with
other members of the erbB family (IC50 values for erbB2 and erbB4 of 165 nM and 4500 nM,
respectively) (242). Erlotinib-mediated inhibition of EGFR TK occurs through a competitive binding at
the ATP site leading to inhibition of receptor autophosphorylation and related signal transduction
pathways (243). Erlotinib inhibits EGF-dependent proliferation of cells at nanomolar concentrations and
blocks cell cycle progression in G1 phase, resulting in interruption of mitogenic and anti-apoptotic
signals responsible for processes such as proliferation, growth, metastasis, angiogenesis, and
responsiveness to chemotherapy or radiotherapy. A wide range of human tumours have shown sensitivity
to erlotinib both in vitro and in vivo (242).
In phase I studies, erlotinib has showed promising anti-tumour effects or long periods of stable
disease in subjects with various solid malignancies refractory to standard therapies, including NSCLC,
being well tolerated at a daily dose of 150 mg (244). Erlotinib has been tested in phase II trials as a single

36
agent in advanced, previously treated NSCLC Asian patients. In this population erlotinib induced a
response rate of 24.2% to 35.7% with a median survival of 12.9 months to 14.7 months with a better
response seen in female, non smoker and adenocarcinoma patients (245) (246) (247) (248). In selected
EGFR TKD wild type patients, response rate was only of 3.3% and the median survival time was 9.2
months (249). Several phase II trials have also evaluated the role of erlotinib as first-line in advanced
NSCLC (234) (250). As a single agent, in unselected populations an overall response of 7% to 31% with
a median survival of 6 to 13.9 months and 1-year survival of 24% to 54% were obtained. Selecting by
presence of adenocarcinoma with BAC features, female gender or presence of EGFR TKD mutations,
response rates of 21%, 30% and 90% respectively have been obtained.
1.2.4. Current role of anti-EGFR therapy in NSCLC
1.2.4.1. First-line therapy in advanced NSCLC
1.2.4.1.1. Single agent therapy
1.2.4.1.1.1. Gefitinib
A single randomized trial explored the use of gefitinib as a single agent compared to best
supportive care in patients with poor performance status unsuitable for chemotherapy (Table 1-7, 1-8). A
non-significant response rate of 6% vs 1% in favour of gefitinib was observed, failing to demonstrate
improvement in response or survival (251). Another study, the Iressa in NSCLC Versus Vinorelbine
Investigation in the Elderly (INVITE) trial, randomized exclusively elderly patients to vinorelbine or
gefitinib observing similar activity with both agents (response rate 3.1% for gefitinib vs 5.1% for
vinorelbine) with no differences in OS (HR=0.98; 95% CI:0.66-1.47) (252).
More recently, consensus from four randomized trials agree that gefitinib may be superior to
standard chemotherapy as first line agent in selected populations (Table 1-7, 1-8). Two randomized trials
studied gefitinib as first line in patients screened for EGFR TKD mutations.
In a phase III trial from Japan, 172 non-older chemo-naive patients with stage IIIB/IV or
postoperative recurrence harbouring exon 19 deletion or L858R EGFR TKD mutations were randomized
between gefitinib or cisplatin/docetaxel (253). Patients receiving gefitinib experienced a better RR
(62.1% vs 32.2%; HR=3.44, 95% CI 1.6-7.4; p<0.001) and a significant prolonged PFS (9.2 months vs
6.3 months, HR=0.49, 95%CI 0.34-0.71; p<0.0001). Another phase III trial in advanced, previously
untreated, Japanese patients with IIB/IV or recurrent NSCLC harbouring EGFR TKD mutations
randomized between gefitinib and paclitaxel/carboplatin (254). Primary end-point was PFS. Response

37
rate was higher with gefitinib (73.7% vs 30.7%; p<0.001) and this agent induced a longer PFS compared
against standard chemotherapy (10.8 months vs 5.4 months; HR=0.3, 95% CI 0.22-0.41; p<0.001). Two
additional randomized trials compared also gefitinib against standard chemotherapy in populations with
elevated prevalence of EGFR TKD mutations.
A phase III, open-label study enrolled 1217 previously untreated, nonsmokers or former light
smokers, Asian patients with advanced pulmonary adenocarcinoma and randomized them to receive
gefitinib or carboplatin/paclitaxel (255). Gefitinib induced a better RR (43% vs 32.2%; OR=1.59, 95%
CI 1.25-2.01; p<0.001) and the one-year PFS was 24.9% with gefitinib and 6.7% with carboplatin-
paclitaxel with a HR for progression or death of 0.74 (95% CI, 0.65-0.85; p<0.001). Another phase III
trial compared gefitinib versus gemcitabine/cisplatin in 313 chemo-naive, Asian, non-smoker patients
with advanced or metastatic adenocarcinoma (256). Differences in RR were not significant (53.5% for
gefitinib vs 42% for gemcitabine/cisplatin; p=0.08) but gefitinib improved PFS significantly (HR=0.737;
95% CI, 0.58-0.94; p=0.0063). Post-hoc analyses of these two trials have found an even better response
among patients harbouring EGFR TKD mutations. However, none of the four trials comparing gefitinib
against standard chemotherapy as first-line option observed differences in OS. Several factors may
explain this but the two most relevant is that these trials were powered to look for differences in PFS
under the reasoning that OS will be affected by the allowed crossing-over occurring once the initial agent
failed.

38
Table 1-7. Compliance and response rate in randomized trials of first-line anti-EGFR as single agents in advanced NSCLC.
ORR Study/Year Stage Population Groups Patients Compliance
(%) (%) OR
(95%CI) p
Goss G 2010 IIIB/IV Poor PS Gefitinib 100 96.8 6 6.57
(0.74-58.17)
Placebo 101 98.4 1 INVITE 2008 IIIB/IV ≥70 yrs Gefitinib 97 90.4 3.1 (0.6-8.8)
Vinorelbine 99 52.1 5.1 (1.7-11.4)
WJTOG3405 2010
IIIB/IV or recurrent
Asian, EGFR TKD mut+
Gefitinib 86 62.1 3.44 <0.0001
Cisp+doce 86 32.2 (1.6-7.4)
NEJ002 2010
IIIB/IV or recurrent
Japanese, EGFR TKD mut+
Gefitinib 115 73.7 6.32 <0.001
Carb+pacl 115 30.7 (3.5-11.25)
IPASS 2009 IIIB/IV
Asian, Non or former light smokers, Adenoca
Gefitinib 609 24.5 43 1.59 (1.25-2.01) <0.0001
Carb+pacl 608 0 32.2 Lee JS 2009 IIIB/IV Asian, non smokers
Adenoca, PS 0-2 Gefitinib 159 53.5 1.38 0.15 Gem+cisp 150 45.3 (0.89-2.17)
OPTIMAL 2010 IIIB/IV Chinese,
EGFR TKD mut+ Erlotinib 82 83 <0.0001 Gem+carb 72 36
Lilenbaum R 2008 IIIB/IV PS 2 Erlotinib 52 88 4 0.13 Carb+pacl 51 92 12 SATURN 2010 IIIB/IV Maintenance after
first-line plat-doublet Erlotinib 437 84 11.9 0.0006 Placebo 447 97 5.4

39
Table 1-8. Progression-free and overall survival in randomized trials of first-line anti-EGFR as single agents in advanced NSCLC.
Progression-Free Survival Overall Survival Study/Year Stage Population Groups Median
(months) HR
(95% CI) p Median
(months) HR
(95% CI) p
Goss G 2010 IIIB/IV Poor PS Gefitinib 1.4 0.82
(0.6-1.12) 0.217 3.7 0.84 (0.62-1.15) 0.272 Placebo 1.4 2.8
INVITE 2008 IIIB/IV ≥70 yrs Gefitinib 2.7 1.19
(0.85-1.65) 0.31 5.9 0.98 (0.66-1.47)
Vinorelbine 2.9 8
WJTOG3405 2010
IIIB/IV or recurrent
Asian, EGFR TKD mut+
Gefitinib 9.2 0.49 (0.34-0.71) <0.0001
30.9 1.638 (0.75-3.58)
Cisp+doce 6.3 --- 0.211
NEJ002 2010
IIIB/IV or recurrent
Japanese, EGFR TKD mut+
Gefitinib 10.8 0.3 (0.22-0.41) <0.001
30.5 0.79 0.31
Carb+plac 5.4 23.6
IPASS 2009 IIIB/IV Asian, Non/former light
smokers, Adenoca Gefitinib 5.7 0.74
(0.65-0.85) <0.001 18.6 0.91 (0.76-1.1) NS
Carb-pacl 5.8 17.3 Lee JS 2009 IIIB/IV Asian, non smokers Gefitinib 5.9 0.74 0.006 20.3 1.03 0.43 Adenoca, PS 0-2 Gem+cisp 5.8 (0.58-0.94) 23.1 (0.76-1.4) OPTIMAL 2010 IIIB/IV Chinese,
EGFR TKD mut+ Erlotinib 13.1 0.16 <0.0001 Gem+carb 4.6 (0.1-0.26)
Lilenbaum R 2008 IIIB/IV PS 2 Erlotinib 1.9 1.45
(0.98-2.15) 0.063 6.6 1.73 (1.09-2.73) 0.018 Carb-pacl 3.5 9.7
SATURN 2010 IIIB/IV Maintenance after first-
line plat-doublet Erlotinib 2.87 0.71
(0.62-0.82) <0.0001 12 0.81 (0.7-0.95) 0.0088 Placebo 2.59 11

40
1.2.4.1.1.2. Erlotinib
Lilenbaum et al randomized 103 patients with poor performance status between erlotinib or
carboplatin/paclitaxel observing a non-significant higher RR in the latter group (12% vs 4%) with a
median OS of 6.6 months in the erlotinib arm and 9.7 months in the chemotherapy arm (HR=1.73; 95%
CI, 1.09-2.73; p =0.018) concluding that unselected patients with advanced NSCLC and poor
performance status are best treated with combination chemotherapy as first-line therapy (Tables 1-7, 1-8)
(257). In screened patients, the OPTIMAL trial reported the experience in China with first-line erlotinib
compared against gemcitabine/carboplatin in EGFR TKD mutation positive, advanced NSCLC patients.
In this trial erlotinib was superior to chemotherapy in terms of RR (83% vs 36%) and PFS (13.1 months
vs 4.6 months; HR=0.16; 95% CI, 0.1-0.26; p<0.0001) (258). Finally, the Sequential Tarceva in
Unresectable NSCLC (SATURN) trial explored the utility of erlotinib as maintenance therapy in patients
with non-progressive, unresectable or metastatic NSCLC following four cycles of first-line platinum-
doublet chemotherapy (259). Response rate was superior (11.9% vs 5.4%, p=0.0006) and PFS was
significantly prolonged (12.3 vs 11.1 weeks, HR=0.71, 95% CI 0.65-0.82, p<0.0001) with erlotinib
versus placebo. Moreover, OS was also superior with erlotinib (12 vs 11 months, HR=0.81, 95% CI 0.7-
0.95, p=0.0088).
1.2.4.1.2. In combination
1.2.4.1.2.1. Gefitinib
Two large randomized phase III studies (the INTACT studies) evaluated the use of gefitinib in
combination with doublet, platinum-based regimens as first-line treatment in advanced NSCLC (Tables
1-9, 1-10). The INTACT trials compared two different doses of gefitinib or placebo added to either
gemcitabine plus cisplatin (INTACT I) (260) or paclitaxel plus carboplatin (INTACT II) (261). Neither
of the two cisplatin/gemcitabine regimens including gefitinib compared against control improved the
response rate (51.2%, 50.3% vs 47.2%; p=ns) or median survival (9.9, 9.9 vs 10.9 months; p=0.456).
Similar results were observed in the INTACT 2 trial using carboplatin/paclitaxel (response rates 30%,
30.4% with gefitinib vs 28.7% without gefitinib, p=ns; medial survival 8.7, 9.8 months with gefitinib vs
9.9 months without gefitinib, p=0.638). In the West Japan Thoracic Oncology Group (WJTOG0203)
trial, 604 stage IIIB/IV Asian NSCLC patients were randomized to receive platinum-doublet followed by
gefitinib and compared against continued platinum-doublet chemotherapy (262). Addition of gefitinib
did not improve the response rate (34.2% vs 29.3, p=0.2) and the OS did not reach statistical significance
(HR=0.86; 95% CI, 0.72-1.03; p=0.11) However, the chemotherapy plus gefitinib combination induced a
better survival in patients with adenocarcinoma (n = 467; HR=0.79; 95% CI, 0.65-0.98; p= 0.03).

41
Table 1-9. Compliance and response rate in randomized trials of first-line anti-EGFR in combination in advanced NSCLC.
ORR Study/Year Stage Population Groups Patients Compliance
(%) (%) OR
(95%CI) p
INTACT 1 2004 III/IV Unselected
Gefitinib 500+Cis-gem 365 54.2 50.3 NS Gefitinib 250+Cis-gem 365 73.2 51.2
Placebo+Cis-gem 363 82.8 47.2
INTACT 2 2004 III/IV Unselected
Gefitinib 500+Carb-pac 347 45 30 NS Gefitinib 250+Carb-pac 345 73.7 30.4
Placebo+Carb-pac 345 79.5 28.7 WJTOG0203 2010 IIIB/IV Asian Gefitinib+platinum+ 298 34.2 0.2 Platinum+ 297 29.3 TRIBUTE 2005 IIIB/IV Good PS Erlotinib+Carb-pac 526 21.5 0.36 Placebo+Carb-pac 533 19.3 TALENT 2007 IIIB/IV Good PS Erlotinib+Cis-gem 580 78 31.5 0.77
(0.6-1) 0.0453 Placebo+Cis-gem 579 83 29.9 Mok TS IIIB/IV Asian,
Good PS Erlotinib+Gem-plat 76 74 35.5 1.75
(0.86-3.57) 0.12 2009 Placebo+Gem-plat 78 70 24.4 BMS099 IIIB/IV/
recurrent Good PS Cetuximab+TC 325 80 25.7 (21.2-30.7) 0.0066 2010 TC 320 80 17.2 (13.3-21.6) FLEX Wet IIIB/IV EGFR IHC+
(1 cell) Cetuximab+Cis-vin 557 36 0.01 2009 Cis-vin 568 29
Meta-analysis 2009 Unselected Cetuximab+chemotherapy 1003 1.463 <0.001 Chemotherapy 1015 (1.2-1.8)

42
Table 1-10. Progression-free and overall survival in randomized trials of first-line anti-EGFR in combination in advanced NSCLC.
Progression-Free Survival Overall Survival Study/Year Stage Population Groups Median
(months) HR
(95% CI) p Median
(months) HR
(95% CI) p
INTACT 1 2004 III/IV Unselected
Gefitinib 500+Cis-gem 5.5 0.7633
9.9 0.456 Gefitinib 250+Cis-gem 5.8 9.9
Placebo+Cis-gem 6 10.9
INTACT 2 2004 III/IV Unselected
Gefitinib 500+Carb-pac 4.6 0.0562
8.7 0.6385 Gefitinib 250+Carb-pac 5.3 9.8
Placebo+Carb-pac 5 9.9 WJTOG0203 2010 IIIB/IV Asian Gefitinib+platinum+ 4.6 0.68
(0.57-0.8) <0.001 13.7 0.86 (0.72-1.03) 0.11 Platinum+ 4.3 12.9
TRIBUTE 2005 IIIB/IV Good PS Erlotinib+Carb-pac 5.1 0.937 0.36 10.6 0.995
(0.86-1.16) 0.95 Placebo+Carb-pac 4.9 10.5 TALENT 2007 IIIB/IV Good PS Erlotinib+Cis-gem 5.53 0.98
(0.86-1.11) 0.74 10 1.06 (0.9-1.23) 0.4863 Placebo+Cis-gem 5.74 10.3
Mok TS IIIB/IV Asian, Good PS
Erlotinib+Gem-plat 6.86 0.47 (0.33-0.68) 0.0002 17.29 1.09
(0.7-1.69) 0.42 2009 Placebo+Gem-plat 5.46 17.66 ATLAS 2009 IIIB/VI Maintenance
after bevac+plat Erlotinib+bevac 4.76 0.72 0.0012 15.9 0.9 0.2686 Placebo+bevac 3.75 (0.59-0.88) 13.9 (0.74-1.09)
BMS099 IIIB/IV/ recurrent Good PS Cetuximab+TC 4.4 0.902
(0.76-1.07) 0.236 9.69 0.89 (0.75-1.05) 0.169 2010 TC 4.24 8.38
FLEX Wet IIIB/IV
EGFR IHC+ (1 cell)
Cetuximab+Cis-vin 4.8 0.943 (0.825-1.08) 0.39 11.3 0.863
(0.751-0.993) 0.039 2009 Cis-vin 4.8 10.1 Meta-analysis 2009
Unselected Cetuximab+chemo 0.899 0.036 0.878 0.01 Chemotherapy (0.81-0.99) (0.79-0.97)

43
1.2.4.1.2.2. Erlotinib
Two large randomized studies, the Tarceva Responses in Conjunction with Paclitaxel and
Carboplatin (TRIBUTE) and Tarceva Lung Cancer Investigation (TALENT) trials, evaluated the use of
erlotinib as first-line therapy in combination with platinum-based regimens for advanced NSCLC (Tables
1-9, 1-10) (263) (264). These trials added erlotinib to either cisplatin/gemcitabine or
carboplatin/paclitaxel regimens. Addition of erlotinib to cisplatin/gemcitabine did not improve the
response rate (29.9% with erlotinib vs 31.5% without erlotinib; p=0.74) or median survival (44.1 weeks
with erlotinib vs 43 weeks without erlotinib). Also, when added to carboplatin/paclitaxel, erlotinib did
not improve the response rate (21.5% with erlotinib vs 19.3% without erlotinib; p=0.36) or median
survival (10.6 months with erlotinib vs 10.5 months without erlotinib; p=0.95). A phase II Asian trial
in stage IIIB/IV randomized patients between adding sequential erlotinib or placebo to a
gemcitabine/platin-based regimen (265). No differences were observed in response when erlotinib was
added (35.5% with gefitinib vs 24.4% with placebo; ORR=1.75, 95% CI 0.86-3.57; p=0.12) and
although the PFS was longer when erlotinib was added (median PFS 29.4 v 23.4 weeks HR=0.47; log-
rank p=0.0002) there was no significant difference in OS. Finally, the ATLAS trial evaluated the
addition of erlotinib to bevacizumab as maintenance treatment in patients receiving first-line
bevacizumab and platinum-based chemotherapy (266). The primary endpoint was met and trial was
stopped due to a median PFS of 4.76 months for bevacizumab+erlotinib versus only 3.75 months for
bevacizumab+placebo (HR=0.72, CI 0.59 – 0.88; p=0.0012).
1.2.4.1.2.3. Cetuximab
Cetuximab has also been tested in combined regimens as a first therapeutic option (Tables 1-9,
1-10). Four trials and one meta-analysis have studied its value. In a phase III randomized trial including
676 stage IIIB/IV patients, a comparison of a carboplatin plus a taxane (docetaxel or paclitaxel) regimen
with or without cetuximab was assessed (267). Although response rate improved with cetuximab (25.7%
vs 17.2%, p=0.007) the primary end-point did not. Median PFS was 4.40 months in the cetuximab arm vs
4.24 months without cetuximab (HR = 0.902; 95% CI, 0.761-1.069; p=0.236). In another large phase III
randomized trial, the combination of cisplatin plus vinorelbine with and without cetuximab was assessed
(the FLEX trial) (192). One thousand one hundred and twenty five EGFR IHC+ stage IIIB/IV patients
were enrolled. EGFR IHC+ was defined as at least a single cell showing positivity. Response rate was
superior under cetuximab (36% vs 29%, p=0.01) and the addition of cetuximab to chemotherapy did not
affect PFS but it resulted in a statistically significant survival advantage when compared with
chemotherapy alone, with a median survival time of 11.3 months, versus 10.1 months (HR=0.871, 95%

44
CI 0.762-0.996; p=0.044). These two randomized phase III trials were combined with two additional
randomized phase II studies in a meta-analysis assessing the value of adding cetuximab to first-line
chemotherapy (268). This meta-analysis demonstrated a significant benefit for the addition of cetuximab
to platinum-based chemotherapy in terms of ORR (OR=1.46, 95% CI 1.2-1.78; p<0.001), PFS (HR=0.9,
95% CI 0.81-0.99; p=0.04), and OS (HR=0.88, 95% CI 0.79-0.97; p=0.01).
1.2.4.2. Second-line therapy or further in advanced NSCLC
1.2.4.2.1. Single agent therapy
1.2.4.2.1.1. Gefitinib
One phase III trial explored the value of gefitinib in stage III/IV patients who developed tumour
progression while on platinum-based chemotherapy and were not candidates for further conventional
agents (269) (Tables 1-11, 1-12). In this trial, the Iressa Survival Evaluation in Lung Cancer (ISEL) trial,
gefitinib significantly induced a better response rate (8% vs 1%, p<0.0001), PFS (3 months vs 2.6
months, p<0.001) but failed to improve survival in all (5.6 months vs 5.1 months p=0.087) and
adenocarcinoma (6.3 months vs 5.4 months; HR=0.84; 95% CI 0.7-1.02; p=0.072) cases compared
against placebo. Against docetaxel, four trials have explored the value of gefitinib (270) (271) (272)
(273). Two of them involved general population. The SIGN trial, with 141 patients enrolled, did not
observed differences between gefitinib or docetaxel as a second-line options in regards to response rate
(13.2% vs 13.7%) or median survival (7.5 months vs 7.1 months) (270). On the other hand, the Iressa
Non-small cell lung cancer Trial Evaluating REsponse and Survival against Taxotere (INTEREST) trial
with 1466 patients did not find differences in response (9.1 months in gefitinib vs 7.6 months for
docetaxel; OR=1.22, 95 % CI 0.82-1.84; p=0.33) but observed non-inferiority of gefitinib compared with
docetaxel for OS (median survival 7.6 months vs 8 months, HR=1.020, 96% CI 0.905-1.150) (271). Two
additional trials compared gefitinib with docetaxel as a second or further line in Asian population.
The Iressa as Second Line Therapy in Advanced NSCLC-Asia (ISTANA) trial enrolled 161
Asian patients, resulting in a superior response (28.1% vs 7.6% for docetaxel; p=0.0007) and longer PFS
(HR=0.729; 90% CI 0.53-1.0; p=0.044) for gefitinib but did not improve OS (HR:0.87; 95% CI 0.61-
1.24; p=0.44) (272). The V-15-32 trial randomized 489 Asian patients, obtaining a better response in the
gefitinib arm (22.5% vs 12.8%; OR:2.14, 95% CI 1.21-3.78; p=0.009) but did not achieved its primary
objective of noninferiority for OS (HR=1.12; 95.24% CI, 0.89 to 1.40) (273). A subsequent meta-
analysis pooled these 4 randomized trials comparing gefitinib versus docetaxel finding the former to

45
improve response (HR:1.58, 95% CI 1.02-2.45, p=0.04) but not PFS (HR:0.97, 95% CI 0.88-1.07,
p=0.57) or OS (HR:1.02, 95% CI 0.92-1.12, p=0.7) (274).
1.2.4.2.1.2. Erlotinib
Erlotinib is the only tyrosine kinase inhibitor to demonstrate a survival advantage in a
randomized, placebo-controlled trial after failure of chemotherapy in advanced non-small cell lung
cancer, as well as symptom improvement (Tables 1-11, 1-12) (275). The NCIC CTG conducted a phase
III trial (BR.21) comparing erlotinib to placebo as second or third-line therapy in 731 patients with stage
IIIB/IV NSCLC randomly assigned in a 2:1 ratio to erlotinib or placebo. Overall response to erlotinib
was 8.9% (95% CI: 6.6-12.0%, p < 0.001), and median duration of response was 34 wks. Statistically
significant and clinically relevant differences were observed for PFS (2.2 vs. 1.8 months; p < 0.0001) and
OS (6.7 vs. 4.7 months; p < 0.0001) relative to the placebo control group (275).
1.2.4.3. Conclusions
Although different end-points were not reached in these trials, the results observed support
different roles of anti-EGFR therapeutic agents in advanced NSCLC.
In the first-line setting, EGFR TKIs are superior to platinum-based regimens as an initial
treatment for advanced NSCLC in selected populations defined by the following characteristics: Asian
ethnicity, non-smokers, adenocarcinoma histology or, more importantly, tumours harbouring EGFR
TKD mutations (253) (254) (255) (256) (258). In Asian, adenocarcinoma patients, EGFR TKIs either
added to or given after standard chemotherapy may also improve results but additional evidence is
necessary (262) (265). For the general population, cetuximab has improved the survival of patients with
advanced NSCLC given in combination with platinum-based chemotherapy in the first line setting, thus
far, the only role of an anti-EGFR Ab in NSCLC (268). Although minimal, this survival benefit is
noteworthy, because it contrasts with negative studies that used EGFR TKIs (260) (261) (263) (264). As
a maintenance therapy after first-line, erlotinib has also shown a role in non-progressive patients alone
after platinum-based chemotherapy or in combination with bevacizumab after a bevacizumab+cisplatin
regimen (259) (266).
Finally, erlotinib is the only EGFR TKI that has been proven to improve response, PFS and OS
in locally advanced or metastatic NSCLC as a second or further line therapeutic option and currently is
the only approved EGFR TKI for use in this clinical scenario (275).

46
Table 1-11. Compliance and response rate in randomized trials of second or further line of anti-EGFR as single agents in locally advanced or
metastatic NSCLC.
ORR Study/Year Population Groups Patients Compliance
(%) (%) OR
(95%CI) p
ISEL 2005 Unselected Gefitinib+placebo 1129 89 8 7.28
(3.1-16.9) <0.0001 Placebo 563 95 1.3 SIGN IIIB/IV Gefitinib 68 85.3 13.2 2006 Docetaxel 71 84.5 13.7 INTEREST 2008
Gefitinib 733 9.1 1.22 (0.82-1.84) 0.33 Docetaxel 733 7.6
ISTANA 2010 Asian Gefitinib 82 28.1 0.0007 Docetaxel 79 7.6 V-15-32 2008 Asian Gefitinib 245 74 22.5 2.14
(1.21-3.78) 0.009 Docetaxel 244 48 12.8 Meta-analysis 2010 IIIB/IV Gefitinib 1128 13.03 1.58 0.04 Docetaxel 1129 8.59 (1.02-2.45) BR.21 2005 IIIB/IV Erlotinib 488 81 8.9 <0.001 Placebo 243 98 <1

47
Table 1-12. Progression-free and overall survival in randomized trials of second or further line anti-EGFR as single agents in locally advanced or metastatic NSCLC.
Progression-Free Survival Overall survival Study/Year Population Groups Median
(months) HR
(95% CI) p Median
(months) p HR
(95% CI) p
ISEL 2005
Unselected Gefitinib+placebo 3 0.82 (0.73-0.92) 0.0006 5.6 0.03 0.89
(0.79-1.01) 0.074 Placebo 2.6 5.1
Adenoca Gefitinib+placebo 6.3 0.033 0.84 (0.7-1.02) 0.072 Placebo 5.4
SIGN 2006 IIIB/IV Gefitinib 3 0.94
(0.64-1.39) 0.76 7.5 0.97 (0.61-1.52) 0.88 Docetaxel 3.4 7.1
INTEREST 2008
Gefitinib 2.2 1.04 (0.93-1.18) 0.47 7.6 1.02
(96% 0.9-1.15)
Docetaxel 2.7 8 ISTANA Asian Gefitinib 3.3 0.729
(90% 0.5-1) 0.0441 0.87 (0.613-1.236) 0.437 2010 Docetaxel 3.4
V-15-32 2008 Asian Gefitinib 2 0.9
(0.72-1.12) 0.335 11.5 1.12 (95.24% 0.89-1.4) 0.33 Docetaxel 2 14
Meta-analysis 2010 IIIB/IV Gefitinib 0.97 0.57 1.02 0.7 Docetaxel (0.88-1.07) (0.92-1.12) BR.21 2005 IIIB/IV Erlotinib 2.2 0.61
(0.51-0.74) <0.001 6.7 <0.001 0.7 (0.58-0.85) 0.002 Placebo 1.8 4.7

48
1.3. Molecular predictors of response/resistance to anti-EGFR inhibition in NSCLC.
1.3.1. EGFR status strategies
1.3.1.1. EGFR protein expression
In randomized trials evaluating different anti-EGFR strategies for advanced NSCLC treatment,
the high number of patients demonstrating EGFR IHC positivity in addition to the small number of
samples available for assessment has made its evaluation as prognostic or predictive factor difficult.
Overall, randomized trials have implemented the Dako EGFR pharmDxTM IHC kits for assessment of
EGFR expression, defining as positive tumours expressing either complete or incomplete membrane
staining in ≥10% of tumour cells. Based on this predefined cut-off point EGFR IHC+ has been observed
in a range from 56% to 91.7% of tumour samples (252) (265) (276) (277) (278) (279) (280) (281) (259).
Additional definitions for assessment of EGFR expression implemented in randomized trials have
included: percentage of membrane staining as a continuous variable (276) (281), membrane intensity
rank (263) (281), a membrane scoring system consisting of intensity of staining multiplied by percentage
of tumour cells involved (280) (281) and ≥1 tumour cell with staining in any compartment (282).
Among first-line randomized trials only the BMS099 trial assessing the addition of cetuximab to
a carboplatin/taxanes (C/T) regimen reported response rates based on EGFR IHC expression (282). No
significant response rate differences were seen in the comparisons according to EGFR IHC status in
patients treated with cetuximab plus C/T (EGFR IHC+ 31.8% vs EGFR IHC- 18.2 %, p=0.49) or C/T
alone (EGFR IHC+ 21.5% vs EGFR IHC- 33.3%, p=0.61). For second-line therapy trials, three
randomized studies have reported the value of EGFR IHC expression on response rate to EGFR TKIs. In
the ISEL trial non-significantly better response rates were observed with the Dako system under gefitinib
(EGFR IHC+ 8.2% vs EGFR IHC- 1.4%) and placebo (EGFR IHC+ 1.5% vs EGFR IHC- 0%) (280).
Similar results were obtained using the Zymed scoring system (gefitinib: EGFR IHC+ 11% vs EGFR
IHC- 4.4%; placebo: EGFR IHC+ 3.1% vs EGFR IHC- 0%). In a second trial comparing an EGFR TKI,
erlotinib, against placebo EGFR IHC was significantly associated with response in the erlotinib arm
(EGFR IHC+:11.3% vs EGFR IHC-:3.8%, p=0.03) (279). However, in the INTEREST trial, while in the
docetaxel arm EGFR IHC+ patients experienced a tendency towards a better response rate (11% vs
6.1%) the contrary was seen under the gefitinib arm (9% vs 15.8%) (277).
EGFR IHC as prognostic factor for survival has also not proven to be of value. In trials
evaluating first-line therapies two opposite results have been seen. On one hand EGFR IHC+ has shown
a non-significant negative prognostic value in the BMS099 trial. For example, in the chemotherapy
group, survival seemed shorter for the patients who had EGFR IHC+ tumours compared with those who
had EGFR IHC- tumours, but the difference was not statistically significant (HR:1.86, p=0.22) (282). No

49
difference by EGFR IHC status was seen in the cetuximab plus chemotherapy group (HR:1, p=0.99).
However, in the INTACT trial the percentage of membrane staining had a statistically significant
positive prognostic effect as a continuous covariate in both treatment groups (double chemotherapy:
HR:0.52, 95% CI 0.31-0.88, p=0.015; gefitinib + double chemotherapy, HR:0.69, 95% CI 0.47-0.99,
p=0.046) and in both groups combined (HR:0.64, 95% CI 0.48-0.86, p=0.0025) (276). This significance
was lost when EGFR IHC+ was defined as ≥10% of cells staining. Using this cut -off point the HR
comparing the positive to negative groups was 0.812 (95% CI 0.588–1.123) suggesting a similar
tendency such that patients with EGFR expression have a better prognosis. This lack of role as a
prognostic factor has also been seen in second-line therapy trials. For example, analysis from the placebo
arm of the BR.21 trial implementing different scoring systems demonstrated that EGFR IHC expressed
as continuous variables produced hazard ratios of death greater than 1.0 (indicating worse survival for
patients with increasing levels of EGFR) for each of the EGFR measures (HR = 1.008, 1.285, and 1.002
for percentage, intensity or scoring system), but none were statistically significant (281). If results were
dichotomized HR were greater than 1.0 for every cutpoint for each EGFR measure, but again none were
statistically significant (p > 0.20). In the erlotinib arm EGFR expressed as a continuous variable
produced hazard ratios very close to 1.0 for each of the EGFR measures and none were statistically
significant. Using cut-off points hazard ratios were numerically less than 1.0 only for low cutpoints for
each EGFR measure, but none were statistically significant (p > 0.20). Patients with very high EGFR
expression had slightly worse survival than patients with lower EGFR expression, as evidenced by
hazard ratios greater than 1.0. These results suggest that the prognostic significance of EGFR expression
by IHC for patients with advanced NSCLC is modest at best.
As predictor of survival during anti-EGFR therapy, EGFR IHC has failed to show any value in
first-line therapy trials. In the INTACT trial EGFR IHC+ patients survived for a median of 296 days
while EGFR IHC- for 218 days under the gefitinib arm producing a HR of 0.959 (95% CI 0.635–1.449,
p=0.84) (276). Lilembaum et al also reported a non-significant result in a comparison between erlotinib
and carboplatin/paclitaxel with EGFR IHC- patients having a median survival of 5.11 months in the
erlotinib arm and 19.25 months in the chemotherapy arm. For EGFR IHC+ patients, median survival was
10.35 and 15.54, respectively (257). Finally, in the BMS099 trial adding cetuximab to
carboplatin/taxanes did not significantly affect survival in patients with EGFR IHC+ tumours (median:
8.3 vs 9.7 months, HR:1.02, 95% CI 0.71-1.48, p=0.91) or in patients with EGFR IHC- tumours
(median:11.2 vs 17.6 months, HR:1.86, 95% CI 0.57-6.11, p=0.30) (282). Survival did not differ
significantly by EGFR IHC status (HR:1.27, p=0.41).
In the maintenance erlotinib trial after first-line, platinum-based doublet chemotherapy, OS was
significantly prolonged in patients with EGFR IHC+ (HR:0.77, 95% CI 0.64-0.93, p=0.0063) (259).

50
In second-line therapy trials EGFR IHC expression has not been related to prolonged survival
during EGFR TKI therapy. In the INTEREST trial no significant survival differences were observed
(EGFR IHC+: gefitinib 7.9 months vs docetaxel 6.5 months; HR: 1.00, 95% CI 0.77-1.29, p=0.98;
EGFRIHC-: gefitinib 7.5 months vs docetaxel 9.2 months; HR: 1.00, 95% CI 0.65-1.55, p=0.99; EGFR
protein expression status-by-treatment interaction test: p=0.87) (277). On the other hand, in comparisons
against placebo EGFR IHC has shown conflicting results. In the ISEL trial EGFR IHC+ patients
achieved significantly better survival with gefitinib versus placebo than patients with EGFR IHC-
tumours (EGFR IHC+: HR:0.77, 95% CI 0.56-1.08, p=0.126; EGFR IHC-: HR:1.57, 95% CI 0.86-2.87,
p=.14; interaction test p=0.049) (278). However, in the BR.21 trial using different cut-off points, hazard
ratios for death on the erlotinib arm relative to placebo were generally less than 1.0, indicating a survival
benefit for patients with EGFR IHC+ tumours who received erlotinib compared with placebo (281). For
patients with EGFR IHC- tumours the hazard ratios were also less than 1.0 regardless of the cut-off point
used indicating also a survival benefit for patients with EGFR IHC- tumours who received erlotinib
compared with placebo. Tests of interactions using different cut-offs points revealed none to be
significant. Use of any staining to define EGFR positivity produced hazard ratios and interaction p values
that were about the same as those produced when ≥10% staining was used to define EGFR IHC+ (p =
0.2616 and 0.2503, respectively).
Overall these results indicate that EGFR protein expression determined by IHC neither has a role
as prognostic factor nor as a predictor of response to anti-EGFR therapy in advanced NSCLC as it is
currently scored commonly but the results obtained in the analyses exploring different scoring systems
leave unanswered the value of other scoring systems.
1.3.1.2. EGFR gene copy number
The prevalence of EGFR high gene copy number by FISH analysis in randomized trials evaluating anti-
EGFR therapies in NSCLC is in the range of 31% to 70% (251) (252) (257) (282) (277) (278) (273)
(283) (284). Also, prevalence of EGFR gene amplification by PCR analysis has been reported to be 7%
in one randomized trial (285).
Overall, the majority of randomized trials have found either tendencies or significant differences
indicating that EGFR high gene copy number is a predictive factor of better response to anti-EGFR
therapy. As a second-line therapy, patients with high EGFR gene copy number receiving either gefitinib
(ISEL and INTEREST trials) or erlotinib (BR.21) experienced a better response rate (277) (283) (278)
(282) (285). In the INTEREST trial comparing gefitinib versus docetaxel objective response rates were
higher in patients with high copy number receiving gefitinib (13% vs 7.4%, p=0.04) but not in patients

51
with low copy number (7.5% vs 10.1%, p=0.27) (277). In comparisons against placebo, gefitinib (ISEL
trial) and erlotinib (BR.21 trial) presented similar results (high gene copy number: gefitinib 16.4% vs
placebo 3%, low gene copy number: gefitinib 3.2% vs placebo 0%; response to erlotinib in: high 21% vs
low 5% gene copy number patients, p=0.02) (283) (278). Also in the first-line therapy field, addition of
cetuximab to a C/T regimen observed similar, but not significant, results with a larger response rate in
those EGFR high gene copy number patients receiving cetuximab (FISH+ patients: cetuximab 37% vs
C/T 22.2%, p=0 .37; FISH- patients: cetuximab 30.8% vs C/T 16.7%, p=0.33) (282). However, an
unique contradictory result is the one estimated from the INTACT trials where response rates did showed
similar patterns independent of gene copy number (chemotherapy+gefitinib: EGFR amplification 56% vs
no amplification 53%; chemotherapy: EGFR amplification 50% vs no amplification 56%; p=1.0) (285).
PCR-based assay was used in the INTACT trials, detecting only amplified but not high polysomy cases
and being the potential reason for the discrepancy observed. A recent systemic review explored the
value of high EGFR gene copy number as predictor of response to EGFR TKIs in 1539 patients with
advanced NSCLC, finding a sensitivity of 0.61 (95% CI, 0.49-0.71) and a specificity of 0.71 (95% CI
0.66-0.76), confirming its value to predict response of the assay in the general population (286).
The effect of EGFR gene copy number on PFS has not been consistent. The addition of
cetuximab to C/T did not significantly affect PFS in the FISH+ (5.4 months in both arms; HR: 1.54, 95%
CI 0.81-2.93, p=0.18) or in the FISH- (4.3 months vs 3.8 months, HR:0.65, 95% CI 0.35-1.18; p=0.15)
groups (282). In the cetuximab plus C/T group, although FISH+ patients had a median PFS of 5.4
months and FISH- of 4.3 months no significant difference was evident (HR:0.99, p=0.97) but patients
with FISH+ tumours treated with C/T had significantly longer PFS than those with FISH- tumours
(HR:1.41, p=0.007) indicating that presence of EGFR high gene copy number is a potential good
prognostic factor in chemo-naive advanced NSCLC patients. In the first-line therapy setting, four
randomized trials have reported the effect of gefitinib on PFS. In a comparison against placebo, in
gefitinib-treated patients the HR for PFS for FISH+: FISH- was 0.26 (95% CI, 0.11 to 0.61); whereas, in
placebo-treated patients, the HR for PFS for FISH+: FISH- patients was 0.82 (95% CI, 0.41 to 1.62)
(251). Furthermore, EGFR FISH+ induced a significant improvement on PFS under gefitinib (HR:0.29;
95% CI, 0.11 to 0.73) result not reached on EGFR FISH- patients (HR:0.74; 95% CI, 0.38 to 1.45)
indicating that EGFR FISH+ is a predictor factor of prolonged PFS for gefitinib treatment as single agent
in chemo-naive NSCLC patients. However, in a comparison against vinorelbine the results were the
opposite (252). Among EGFR FISH+ patients those treated with vinorelbine achieved better PFS than
patients treated with gefitinib: (HR: 3.13, 95% CI 1.45-6.76). Furthermore, among patients treated with
gefitinib, EGFR FISH+ patients had a non-significant trend toward poorer PFS than EGFR FISH-
patients (HR:1.31, 95% CI, 0.77 -2.22). Conversely, among patients treated with vinorelbine, patients
who were EGFR FISH+ had a non-significant trend toward improved PFS compared to EGFR FISH-

52
patients (HR:0.77, 95% CI 0.43-1.39). In the INTACT trials using PCR to detect EGFR amplification,
PFS was also slightly longer for EGFR amplification-positive (7.3 months vs 4.6 months; HR:0.37 95%
CI 0.20-0.69) patients treated with chemotherapy irrespective of gefitinib therapy indicating a potential
prognostic role (285). Although not significant, EGFR amplification-positive patients experienced a
shorter PFS when gefitinib was added to a chemotherapy regimen (7.3 months vs 6.9 months, HR:0.83,
95% CI 0.32-2.18) while EGFR amplification-negative patients experienced a slight improvement (4.6
months vs 4.8 months; HR:0.77, 95%CI 0.6-1). Finally, in the highly selected population of the IPASS
trial characterized by Asian, non- or former smokers with adenocarcinomas, high EGFR FISH copy
number presented a significant interaction of treatment effect (p=0.0437) (284). While gefitinib was
associated with longer PFS compared to chemotherapy in EGFR FISH+ patients (HR:0.66, 95% CI 0.5-
0.88, p=0.005) and opposite trend was observed among EGFR FISH- patients (HR:1.24, 95% CI 0.87-
1.76, p=0.24). Based on these results no clear prognostic or predictive role of EGFR gene copy number
for PFS in first-line therapy for advanced NSCLC exists. While two randomized trials observed a
positive prognostic role of high EGFR gene copy number or EGFR amplification on anti-EGFR therapy
arms, two additional reports observed the same positive prognostic role but in the control arms.
Furthermore, whilst two trials failed to confirm a predictive role of high EGFR gene copy number in the
response to anti-EGFR agents, one observed a positive predictive role in the response to vinorelbine and
not to gefitinib. Only two trials found a positive predictive role of high EGFR gene copy number in the
response to gefitinib. However, post hoc analyses indicated that the positive effect of gefitinib in EGFR
FISH+ patients observed in the IPASS trial was, in fact, due to an overlapping with EGFR TKD
mutations, losing its value as a predictor of better PFS (284).
Comparison of gefitinib against placebo has also been explored as second-line therapy. In the
ISEL trial patients with high EGFR gene copy number had a time to failure (TTF) of 4.5 months under
gefitinib and 1.9 months under placebo; those with low EGFR gene copy number had a TTF of 2.4
months under gefitinib and 3.9 months under placebo (278). These results suggest a positive predictive
role of better PFS under gefitinib treatment (HR:0.55, 95% CI 0.34-0.89). However, similar results were
not obtained when gefitinib was compared against docetaxel. In the INTEREST trial gefitinib was
similar to docetaxel in terms of median PFS in patients with high (gefitinib 2.5 months vs docetaxel 2.8
months, HR:0.84, 95% CI 0.59-1.19, p=0.33) and low (gefitinib 2.1 months vs docetaxel 2.8 months,
HR:1.30, 95% CI 0.93-1.83, p=0.12) copy number (277). The V-15-32 trial also compared gefitinib
versus docetaxel in Asian patients (273). In this trial EGFR FISH+ patients also appeared to have similar
PFS compared to EGFR FISH– patients on gefitinib (HR:0.75, 95% CI 0.28-1.98) or docetaxel (HR:0.45,
95% CI 0.14-1.41). There were even no differences between gefitinib and docetaxel with wide CI
intervals.

53
Separately, these trials suggest that high EGFR gene copy number does not have a predictive
role in terms of PFS when gefitinib is compared against a second agent. However, these evidence suggest
that high EGFR gene copy number may have a role has a predictive role for PFS under gefitinib
compared against placebo supported by two trials in first and second-lines. In fact, a recent meta-analysis
have found that increased EGFR gene copy number is significantly associated with improved PFS
(HR:0.6, 95% CI 0.46-0.79, p<0.001) under EGFR TKIs without differences based on ethnicity or line
(287).
Four out of five randomized trials involving gefitinib for advanced NSCLC treatment did not
observe a prognostic role for survival for EGFR gene copy number (251) (252) (278) (277). Only the
INTACT trials evaluating the addition of gefitinib to double platinum-based regimens indicated that
EGFR amplification, not high copy number, had a prognostic role (285). A trend towards improved
survival irrespective of gefitinib therapy was seen for chemotherapy-treated patients with amplification
of EGFR (median survival: > 20 months vs 10.2 months HR:0.46, 95% CI 0.25-0.83). Similar result was
observed in the BMS099 trial comparing addition of cetuximab to carboplatin/taxane chemotherapy with
patients with FISH+ tumours having longer survival than those with FISH- tumours when treated with
chemotherapy alone (HR:0.48, p=0.017) but not when adding cetuximab (HR:1.07, p=0.81) (282). Based
on these reports a survival prognostic role of EGFR gene copy number is not clear.
In regards to predicting better OS in comparisons against placebo, in the ISEL trial median
survival among patients with a high EGFR gene copy number was 8.3 and 4.5 months with gefitinib or
placebo, respectively (278). EGFR FISH+ patients achieved significantly better survival with gefitinib
compared with placebo than patients with a low EGFR gene copy number (FISH+ HR 0.61, 95% CI
0.36-1.004, p=0.067; FISH- HR:1.16, 0.811-1.64, p=0.42; comparison of HRs high v low copy number,
p=0.045) meaning that in patients with a high EGFR gene copy number the risk of death during the
follow-up period was 39% lower among patients receiving gefitinib compared with those receiving
placebo. No apparent difference in survival between gefitinib and placebo was observed in patients with a
low EGFR gene copy number (HR, 1.16; 95% CI, 0.81 to 1.64; P = .417). Additional exploratory post-
hoc analyses have shown HRs in favour of gefitinib-treated, high EGFR copy number patients across
subgroups of clinical factors usually considered to be least likely to benefit (e.g., smokers and patients
with nonadenocarcinoma). In the BR.21 trial the survival benefit for erlotinib compared with placebo
was significant (p=0.004) in EGFR FISH+ patients (HR:0.43, 95% CI 0.23-0.78) but not in EGFR FISH-
patients (HR:0.80, 95% CI 0.49-1.29, p=0.35) (283). Furthermore, on multivariate analysis, EGFR
FISH+ status was predictive of greater survival benefit from erlotinib (HR:0.33, 0.15-0.71, p =0.005). On
the other hand, the Iressa Non-small cell lung cancer Trial Evaluating REsponse and Survival against

54
Taxotere (INTEREST) trial did not observe superiority of gefitinib in patients with high EGFR gene
copy number (HR=1.09, 95% CI 0.78-1.51; p=0.62).
Regarding first-line trials, in a comparison against placebo in patients with poor performance
status EGFR FISH+ patients experienced a non-significant improved survival (HR:0.44, 95% CI 0.17-
1.12) under gefitinib, with a HR for survival between FISH+/FISH- patients of 0.47 with gefitinib (95%
CI, 0.21 to 1.05) and 0.95 with placebo (95% CI, 0.47 to 1.96) (251). This beneficial predictive role has
not been seen in other first-line trials in which anti-EGFR agents were compared against others and, in
fact, it has shown to be the opposite. In the INVITE trial gefitinib was compared against vinorelbine
with, in the small subgroup of EGFR FISH+ patients, those treated with vinorelbine achieved better
survival than patients treated with gefitinib (HR: 2.88, 95% CI 1.21-6.83) (252). Furthermore, patients
who were treated with gefitinib and were FISH+ had a non-significant trend toward poorer survival than
patients who were FISH- (HR: 1.61, 95% CI 0.87-3.01) for OS. Conversely, patients in the vinorelbine
group who were FISH+ had a non-significant trend toward improved survival compared patients who
were FISH- (HR: 0.52, 95% CI 0.25-1.10). In the INTACT trials evaluating the addition of gefitinib to
standard chemotherapy regimens a similar trend towards improved survival irrespective of gefitinib
therapy was also seen for chemotherapy-treated patients with amplification of EGFR (median survival >
20 months vs 10.2 months; HR:0.46, 95% CI 0.25-0.83) (285). This harmful result has also been seen
with cetuximab. Addition of cetuximab to standard chemotherapy has shown that patients with EGFR
FISH+ disease appeared to have superior outcomes with chemotherapy alone (282). Patients with EGFR
FISH+ tumours had significantly shorter survival with cetuximab plus carboplatin and taxanes than with
carboplatin and taxanes alone (median survival 8.6 months vs 12.5 months; HR:1.92, 95% CI 1.05-3.54;
p=0.03), whereas survival did not differ by treatment in patients with EGFR FISH- tumours (median
survival 7.4 months in both groups; HR:0.84, 95% CI 0.47-1.52, p=0.57). Patients with EGFR FISH+
tumours had longer survival than those with EGFR FISH- tumours when treated with chemotherapy
alone (HR:0.48, p=0.017) but not when treated with cetuximab plus chemotherapy (HR:1.07, p=0.81).
Based on this evidence high EGFR gene copy number may predict shorter survival for anti-EGFR
therapies compared against other agents when used as first-line options for advanced NSCLC.
Independently of the above mentioned discrepancies, a recent meta-analysis have found
increased EGFR gene copy number to be associated with improved OS among patients treated with
EGFR KIs (HR:0.77, 95% CI 0.66-0.89, p=0.001) (287). Interestingly, subanalyses found increased
EGFR gene copy number to be significantly associated with improved OS in studies including mixed
population (HR:0.70, 95% CI 0.59-0.82, p<0.001) but not in those including Asian patients exclusively
(HR:1.11, 95% CI 0.82-1.5, p=0.5).

55
Overall, it can be concluded that patients with advanced NSCLC showing high EGFR gene copy
number in their tumours will experience a better response rate to anti-EGFR agents with longer PFS, and
OS; establishing it has a good predictive marker. However, as molecular markers coexist in the tumours
overlap assessment of other important molecular markers, such as EGFR TKD mutations is imperative.
1.3.1.3. EGFR TKD mutations
When not implemented as inclusion criteria, presence of EGFR TKD mutations in NSCLC
randomized trials has been reported with a prevalence from 10%, to up to 59.7% in selected Asian
patients (252) (255) (265) (271) (285) (288) (282) (277) (278) (273) (283) (259). The most common
mutations detected in these trials were exon 19 deletions (50%-78.4%), exon 21 L858R (18.75%-42.5%),
exon 20 T790M (2.3%-4.2%), and other mutations (3.8%-17.2%) (255) (285) (277) (288) (283).
With the exception of the BMS099 trial which evaluated the addition of cetuximab to a C/T
regimen, all trials assessing either gefitinib or erlotinib as first or second-line of therapy for advanced
NSCLC have reported that EGFR TKD mutations (exon 19 deletion or exon 21 L858R) are predictive
markers of a better response rate. Among patients with EGFR TKD mutations, the response rate in the
BMS099 trial trended to be higher in those receiving cetuximab plus C/T (50% v 11.1%, p=0.13) but a
similar pattern was also found among the EGFR TKD wild-type group (32.4% v 21.8%, p=0.19) (282).
The association between EGFR TKD mutational status and objective response rate was not significant
(p=0.82). In the rest of the randomized trials, a difference in response rates from 3.2% to 22.4% in favour
of the non-EGFR TKIs arm was observed in patients with wild EGFR TKD, contrary to a difference of
21% to 49% in favour of the EGFR TKI arm in patients with EGFR TKD mutations (255) (271) (264)
(283) (289). With a difference between 20% to 76% in favour of EGFR TKD mutations versus wild type
in EGFR TKI arms, the value of EGFR TKD mutations as predictive marker of response is sustained.
This positive response in tumours harbouring EGFR TKD mutations under EGFR TKI treatment was
confirmed by the randomized trials involving EGFR TKD mutant patients exclusively with differences in
response rates been of 29.9% to 47% in favour of EGFR TKIs against platinum-based doublets (253)
(254) (258). Furthermore, a recent systemic review explored the value of EGFR TKD mutations as
predictor of response to EGFR TKIs in 3101 patients with advanced NSCLC, indicating a sensitivity of
0.78 (95% CI, 0.74-0.82) and a specificity of 0.86 (95% CI 0.82-0.89) (286). Therefore, EGFR TKD
mutations and in particular exon 19 deletions or the exon 21 L858R mutation, are predictive markers of
response to EGFR TKIs.
In regards of PFS, evidence suggests that EGFR TKD mutations may be a marker of good
prognosis irrespective of agent or line of therapy. In first-line therapeutic trials, patients with EGFR TKD

56
mutations presented longer PFS than EGFR TKD wild type patients irrespective of therapeutic arms. In
the BMS099 trial this difference was not significant, with patients under the cetuximab plus C/T arm
experiencing a PFS of 6.1 months if they harbour EGFR TKD mutations and 5.1 months if their EGFR
TKD genotype was wild (282). Patients in the control group also presented a longer PFS if they had
EGFR TKD mutations (6.4 months) compared against those with a wild type genotype (4.6 months).
This was also observed in the INTACT trials where median PFS was slightly longer for mutation-
positive (6.7 months v 4.5 months; HR:0.40, 95% CI 0.23-0.71) patients treated with chemotherapy
irrespective of gefitinib therapy (285). Also, the TRIBUTE trial reported that by combining the erlotinib
plus carboplatin/paclitaxel (C/P) and C/P alone treatment groups, the patients with EGFR TKD-mutant
tumours experienced a prolonged median time to progression of 8 months, compared with 5 months for
those without mutations (p <0.001; 95% CI for HR, 0.5-0.8) (288). Finally, in the SATURN trial
exploring the utility of erlotinib as maintenance after first-line platinum-doublet chemotherapy erlotinib
induced prolonged PFS in patients with EGFR TKD mutations (HR:0.1, 95% CI 0.04-0.25, p<0.0001)
but also in those with wild type EGFR TKD (HR:0.78, 95% CI 0.63-0.96, p=0.0185) (259). With respect
to second-line trials in a comparison of gefitinib against docetaxel EGFR TKD mutation-positive patients
appeared to have better PFS than EGFR TKD mutation-negative patients on both treatment arms
(gefitinib arm: HR:0.33, 95% CI 0.11-0.97; docetaxel arm: HR:0.15, 95% CI 0.04-0.57) (273).
Therefore, EGFR TKD mutations are a prognostic marker of prolonged PFS independently of treatment.
However, the role for EGFR TKD mutations as predictor of prolonged PFS induced by anti-EGFR
therapy is not clear.
A predictive role of EGFR TKD mutations prolonging PFS under anti-EGFR therapy has only
been confirmed in selected populations. In the highly selective first-line randomized trial comparing
gefitinib versus a carboplatin/paclitaxel regimen in Asian, former light or non-smokers patients with
adenocarcinoma histology, patients who were positive for EGFR TKD mutations experienced a
significantly longer PFS if they received gefitinib than those who received carboplatin-paclitaxel
(HR:0.48, 95% CI 0.36-0.64, p<0.001), whereas patients who were negative for the mutation
experienced a longer PFS if they received carboplatin-paclitaxel (HR:2.85, 95% CI 2.05-3.98, p<0.001)
(255). Another first-line randomized trial compared gefitinib against gemcitabine/cisplatin in Asian, non-
smokers patients with adenocarcinoma (256). In this, patients with EGFR TKD mutations under gefitinib
experienced a longer PFS than those with wild EGFR TKD (7.9 months vs 2.1 months; HR=0.385; 95%
CI, 0.21-0.71; p=0.009). In the gemcitabine/cisplatin arm no such difference was observed (5.8 months
vs 5.5 months; HR=1.22; 95% CI 0.65-2.3; p=0.27). This predictive role of EGFR TKD mutations for
PFS was confirmed in trials enrolling patients with EGFR TKD mutations exclusively.

57
In a phase III trial from Japan, 172 chemo-naive patients with stage IIIB/IV or postoperative
recurrence harbouring exon 19 deletion or L858R EGFR TKD mutations were randomized between
gefitinib or cisplatin/docetaxel (253). Patients receiving gefitinib experienced a significant prolonged
PFS (9.2 months vs 6.3 months, HR=0.49, 95%CI 0.34-0.71; p<0.0001). Another phase III trial in
advanced, previously untreated, Japanese patients with IIB/IV or recurrent NSCLC harbouring EGFR
TKD mutations randomized between gefitinib and paclitaxel/carboplatin (254). Primary end-point was
PFS. Gefitinib induced a longer PFS compared against standard chemotherapy (10.8 months vs 5.4
months; HR=0.3, 95% CI 0.22-0.41; p<0.001). The OPTIMAL trial reported the experience in China
with first-line erlotinib compared against gemcitabine/carboplatin in EGFR TKD mutation positive,
advanced NSCLC patients. In this trial erlotinib was superior to chemotherapy in terms of PFS (13.1
months vs 4.6 months; HR=0.16; 95% CI, 0.1-0.26; p<0.0001) (258).
Outside Asia, another randomized trial had observed a predictive role for EGFR TKD under anti-
EGFR therapy. In the INTEREST trial, patients with EGFR TKD mutation experienced a longer PFS
under gefitinib compared with docetaxel (7 months vs 4.1 months, HR:0.16, 95% CI 0.05-0.49, p=0.001)
but not in wild-type EGFR TKD (1.7 months vs 2.6 months, HR:1.24, 95% CI 0.94-1.64, p=0.14) (277).
No other trial has reported a predictive role for EGFR TKD in response to anti-EGFR probably due to
the low frequency of EGFR TKD mutations in non-Asian patients, making it difficult to perform a
significant analysis.
As a prognostic factor for longer OS, in the BR.21 trial EGFR TKD mutations did not predict a
differential treatment effect (interaction p=0.34) (283). Similar result was observed in the INTEREST
trial comparing gefitinib versus docetaxel as a second-line option in which patients with EGFR TKD
mutation-positive tumours experienced a longer survival in both gefitinib and docetaxel groups (median
survival 14.2 and 16.6 months, respectively) compared to the overall population (7.6 and 8.0 months,
respectively) and in the population with EGFR TKD wild-type (6.4 and 6.0 months, respectively), but
there was no a significant difference between treatments (277). In first-line therapy trials, similar non-
significant results have been reported in the BMS099 trial involving cetuximab in which patients with
mutated EGFR TKD tended to have a longer survival compared with those with wild-type EGFR TKD
(HR:0.61, p=0.09) (282). Also, in the SATURN trial exploring the utility of erlotinib as maintenance
after first-line platinum-doublet chemotherapy OS was prolonged with erlotinib versus placebo in
patients whose tumours did not harbour activating EGFR TKD mutations (HR: 0.77, 95% CI 0.61-0.97,
p=0.0243) (259). This raises the possibility that this genetically defined subset of NSCLC may have a
more favourable natural history and that EGFR TKD mutations may serve as a prognostic but not
predictive factor. However, confirmation of this hypothesis has been difficult due to the low frequency
of EGFR TKD mutations. For example, in a combination of both treatment groups of the TRIBUTE trial

58
the median survival of patients with EGFR TKD wild-type tumours was 10 months (p<0.001; 95% CI
0.1-0.5) but Kaplan-Meier estimates of median survival could not be calculated for the EGFR TKD-
mutated subgroup. Also in the INTACT trials EGFR TKD-mutant patients treated with chemotherapy
alone had a better survival compared with EGFR TKD-mutation negative patients (19.4 months vs 9.2
months, HR:0.48, 95% CI 0.29-0.82), but further analysis could not be addressed because of the small
number of EGFR TKD-mutant tumours in the placebo arm of the trial (285). Therefore, all evidence
suggests that presence of EGFR TKD mutation is a potential prognostic marker of prolonged survival but
further trials involving a higher frequency of this type of mutations are necessary in order to confirm this
role.
As a predictive marker of prolonged survival under anti-EGFR therapy, EGFR TKD mutations
have failed to show a role in second-line trials. In the BR.21 trial the survival benefit from erlotinib
compared with placebo was slightly greater with EGFR TKD mutations (HR:0.55, 95% CI 0.25-1.19,
p=0.12) than in EGFR TKD wild-type or indeterminate variants (HR:0.74, 95% CI 0.52-1.05, p=0.09),
but the interaction was not significant (p=0.47) and on multivariate analysis EGFR TKD mutations failed
to show a predictive role of a differential treatment effect (interaction p=0.34) (283). In the INTEREST
trial there was also no significant survival difference in treatment effect between EGFR TKD mutation-
positive and wild-type (mutation-positive: HR:0.83, 95% CI 0.41-1.67, p=0.6; wild-type: HR:1.02, 95%
CI 0.78-1.33, p=0.91) with a non-significant EGFR TKD mutation status-by-treatment interaction test
(p=0.59) (277). In first-line trials, the INTACT, TRIBUTE and BMS099 trials were not able to show a
predictive survival role for EGFR TKD mutations when gefitinib, erlotinib or cetuximab, respectively,
were added to different standard chemotherapeutic regimens (285) (288) (282). At that point consensus
was that, due to the low frequency of EGFR TKD mutations in Non-Asian populations as well as the low
number of tumour sample collected in the clinical trials, the ultimate assessment of EGFR TKD
mutations as predictive marker would be difficult to assess adequately. Due to this, subsequent trials
were designed and performed in Asian countries, involving the assessment of EGFR TKIs in enriched
populations for EGFR TKD mutations.
In first-line trials involving populations with high prevalence of EGFR TKD mutations, EGFR
TKIs have failed to predict survival. In a head-to-head comparison of gefitinib against a
carboplatin/paclitaxel regimen, the HR for survival with gefitinib was 0.78 (95% CI, 0.50 to 1.20) in the
EGFR TKD mutation-positive subgroup and 1.38 (95% CI, 0.92 to 2.09) in the EGFR TKD mutation-
negative subgroup (255). Also, in a trial comparing gefitinib against gemcitabine/cisplatin in Asian, non-
smokers patients with adenocarcinoma, presence of EGFR TKD mutations did not associate with
prolonged survival (HR=1.31; 95% CI 0.7-2.6, p=0.45) (289). Finally, in trials enrolling exclusively
patients with EGFR TKD mutations similar results were observed. In a phase III trial from Japan, 172

59
non-older chemo-naive patients with stage IIIB/IV or postoperative recurrence harbouring exon 19
deletion or L858R EGFR TKD mutations were randomized between gefitinib or cisplatin/docetaxel
(253). Patients enrolled in the gefitinib arm did not experienced a better survival (HR=1.638; 95% CI
0.75-3.58; p=0.211). This was also observed from another phase III trial in advanced, previously
untreated, Japanese patients with IIB/IV or recurrent NSCLC harbouring EGFR TKD mutations,
randomized between gefitinib and paclitaxel/carboplatin with OS not been superior with gefitinib
(gefitinib:30.5 months vs paclitaxel/carboplatin: 23.6 months; HR=0.79, p=0.31) (254).
In conclusion, EGFR TKD mutations predict response and prolonged PFS to EGFR TKIs, but
not to cetuximab, in advanced NSCLC patients. Furthermore, although a lack of survival benefit has
been observed this is due to a confounding effect of salvage chemotherapy. As patients are part of a
population already known to be responsive to EGFR TKIs, once standard chemotherapy failed in the
first-line setting, EGFR TKIs were offered to these patients in subsequent lines, affecting the overall
survival.
1.3.2. Non-EGFR status strategies
1.3.2.1. KRAS mutations
Single amino acid substitutions in either codon 12 or 13 of exon 2 have been the most common
KRAS mutations detected in randomized trials, with a prevalence of 7.9% to 21% in the analyzed
samples (288) (282) (277) (278) (283). Although none has reached significance, observations from these
analyses have been contradictory based on the anti-EGFR approach implemented.
Evidence is unclear in regards of a role for KRAS mutations in determining benefit from
cetuximab treatment. In the BMS099 trial, chemotherapy-naive stage IIIB/IV NSCLC patients were
randomly assigned to C/T with or without cetuximab (282). Addition of cetuximab improved, but not
significantly, response rate, median PFS, and OS in patients with mutated KRAS (RR: 30.8% vs 9.1%;
PFS: 5.6 vs 2.8 months, HR:0.64, 95% CI 0.27-1.50; OS: 16.8 vs 10.8 months, HR:0.97, 95% CI 0.45-
2.07) but not in KRAS wild-type tumours (RR: 32.9% vs 25.6%; PFS: 5.1 vs 5.3 months HR:1.07, 95%
CI 0.77-1.50; OS: 9.7 vs 9.9 months, HR:0.93, 95% CI 0.67-1.30). On the contrary, in the FLEX trial
comparing the addition of cetuximab to a cisplatin/vinorelbine regimen as first line regimen in patients
with stage IIB/IV NSCLC, cetuximab treatment in patients with KRAS wild-type tumours and patients
with KRAS mutant tumours showed no marked differences with regard to OS or PFS (290).
However, presence of KRAS mutations has been associated with decreased response rate, time to
progression, and shorter survival in patients treated with EGFR TKI therapy. In the TRIBUTE trial

60
evaluating the addition of erlotinib to carboplatin/paclitaxel (C/P) as first-line therapy KRAS mutation
affected the response rate to erlotinib (288). KRAS mutant cases presented a non-significant smaller
response rate to erlotinib (23% response rate on C/P vs 8% erlotinib+C/P; p=0.16), effect not observed in
wild KRAS cases (26% response on C/P vs 26% response on erlotinib+C/P). Also, KRAS mutant patients
treated with the erlotinib+C/P combination had shorter median time to progression (TTP) (3.4 months)
and survival (4.4 months). These were shorter than those observed in KRAS wild-type patients receiving
same combination (TTP 5.3 months, survival 12.1 months). Results observed in the control group were
as follow: KRAS mutation: TTP 6 months, survival 13.5 months; KRAS wild: TTP 5.4 months, survival
11.3 months. Among patients with KRAS mutations, the HR of erlotinib+C/P versus C/P alone was 2.1
(95% CI, 1.1- 3.8; p=0.02) for survival and 1.9 (95% CI, 1.1-3.6) for TTP. These results indicate that
patients with KRAS-mutant tumours not only fail to benefit from addition of erlotinib to C/P, but may, in
fact, experience decreased survival and TTP compared with CP alone in the first-line metastatic setting.
In the second-line therapy scenario KRAS mutations have shown a potential detrimental effect
independent of the therapy implemented. In the phase III INTEREST trial, 1,466 pretreated patients with
advanced NSCLC were randomly assigned to receive gefitinib or docetaxel (277). Although this trial did
not find evidence supporting a predictive role for KRAS mutations, patients with KRAS mutations had a
worse course independent of the therapy in regards to response rate (KRAS mutation+: gefitinib 0% vs
docetaxel 3.7%, p=no calculated; KRAS mutation-: gefitinib 9.6% vs docetaxel 11.9%, p=0.63) and PFS
(KRAS mutation+: gefitinib 1.4 months vs docetaxel 1.5 months, HR:1.16 95% CI 0.56-2.41, p=0.68;
KRAS mutation-: gefitinib 2.6 months vs docetaxel 3.3 months, HR:1.23 95% CI 0.9-1.68, p=0.2) but not
in regards of median survival in which patients experienced a better result with gefitinib independent of
KRAS genomic status (KRAS mutation+: gefitinib 7.8 months vs docetaxel 4.2 months, HR:0.81, 95% CI
0.44-1.49, p=0.5; KRAS mutation-: gefitinib 7.5 months vs docetaxel 6.3 months, HR: 1.03, 95% CI
0.77-1.37, p=0.86; KRAS mutation status-by-treatment interaction test p=0.51). The BR.21 phase III trial
is another important trial in the second-line scenario which found erlotinib as superior to placebo in
advanced NSCLC patients who experienced treatment failure under standard chemotherapy (283).
Among 206 KRAS genotype-known patients response rates for erlotinib were 5% for KRAS mutation and
10% for KRAS wild-type patients (p=0.69). The HR for survival (erlotinib vs placebo) was 1.67 (95% CI
0.62-4.5, p=0.31) in patients with KRAS mutations but 0.69 (95% CI, 0.49-0.97, p=0.03) in patients
without mutation with a marginally significant interaction between KRAS genotype and treatment (p
=0.09), suggesting a lack of benefit from erlotinib in patients with KRAS mutations. However, KRAS
genotype failed to show a prognostic (p=0.79) or predictive of a differential treatment (p=0.13) effects on
multivariable analysis.

61
It is difficult to conclude from the non-significant results but consistent trends suggest that
tumours with KRAS mutant genotype may have a poor prognosis in their response independent of
treatment. However, a predictive role is unclear. Trends suggest that patients with KRAS mutations may
benefit from cetuximab treatment and that presence of this genotype may affect negatively patients
treated with erlotinib. However, under multivariable analyses such results failed to show statistical
significance.
1.3.2.2. BRAF mutations
The Raf-1 related kinase BRAF is a recently identified as oncogene (291). Mutations in BRAF
result in kinase activation leading to a permanent activation of Erks. In the ISEL trial, 7% of tumour
samples were evaluated for presence of the BRAF exon 15 mutation V599E (278). None of the samples
was positive indicating that BRAF mutation did not participate in the response observed to gefitinib.
1.3.2.3. Akt
One of the key elements of the EGFR intracellular signaling pathways is Akt. Only one
randomized trial has evaluated its role in the response to EGFR TKI in NSCLC. In the randomized ISEL
trial, comparing gefitinib against placebo, p-Akt IHC+ (defined as 201-400 score) was positive in 40.6%
of assessed cases (278). Differences in response rates between gefitinib and placebo were slightly larger
in p-Akt IHC+ than p-Akt IHC- patients (p-Akt IHC+: 10.1% with gefitinib vs 2.5% with placebo; p-Akt
IHC-: 6.3% with gefitinib vs 0% with placebo). However, there were no differences in time to failure
(HR for gefitinib vs placebo p-Akt IHC+:1.08, 95% CI 0.68-1.71; p-AKt IHC-:0.98, 95% CI 0.67-1.45)
or survival (p-Akt IHC+: 4.2 months with gefitinib vs 5.4 months with placebo; p-Akt IHC-:5.9 months
with gefitinib vs 6.1 months with placebo). Also, no relationship was observed between p-Akt status and
survival outcome (pAkt+ HR: 1.08 0.68-1.71, p=0.736; pAkt- HR:0.98, 0.67-1.45, p=0.937; interaction
test p = .778). This analysis suggests that p-Akt neither has an important role in the clinical response to
gefitinib nor recurrence or survival under this agent.
1.3.2.4. Polymorphisms in DNA repair genes
Recently, single nucleotide polymorphims variations in relevant DNA repair genes were
investigated in samples from a first-line trial comparing gefitinib vs gemcitabine/cisplatin in Asian, non-
smoker patients with advanced adenocarcinomas (289). Patients who harboured XRCC1 399Arg/Arg

62
genotype experience higher RR to gefitinib than those with Arg/Gln or Gln/Gln genotypes (71% vs 35%
vs 43%; p=0.006). When comparing RRs by treatment, patients with a RRM1 2464GG genotype had a
significantly higher RR to gefitinib compared with chemotherapy (88% vs 29%; p=0.041). XRCC1 399
Arg/Arg patients also experienced longer PFS under gefitinib (7.5 months vs 2.1 vs 2.6; p=0.034). When
comparing arms, longer PFS with gefitinib vs chemotherapy was observed in patients with XRCC1 399
Arg/Arg genotype (7.5 months vs 6.6 months; p=0.012). Patients harbouring RRM1 2464GG (11.5
months vs 6 months; p=0.004) and ERCC1 8092CA (7.5 months vs 6.4 months; p=0.024) genotypes also
experienced longer PFS with gefitinib. In fact, when 2 of these 3 specific genotypes, RRM1 2464GG,
ERCC1 8092CA, and XRCC1 399Arg/Arg were present, this was associated with a longer PFS (6.4
months vs 8.1 months; p=0.009) with gefitinib. However, patients with XRCC1 399 Arg/Arg genotype
had more EGFR TKD mutations than other variations (82% vs 29% for Arg/Gln vs 0% for Gln/Gln;
p=0.001).
1.3.3. Conclusions
Only two assays have been widely investigated and have a current role as potential predictive
markers to response to anti-EGFR agents in NSCLC. In a face-to-face run, screening for EGFR TKD
mutations has positioned as the first assay that should be implemented in patients considered to receive
EGFR TKI treatment. Due to the responses obtained from the trials involving enriched populations, it is
considered that the EGFR TKD mutations exon 19 deletions and exon 21 L858R must be determined in
tumour tissue from patients to be considered for EGFR TKI treatment. During which line of treatment
this assay should be implemented is not defined but evidence indicate that at any line it has its value
(169). Also if all or clinically-selected patients must be screening should be determined according to
cost-effectiveness. On the other hand, EGFR copy number determined by FISH was also a promising
assay but analysis of samples from the IPASS trial involving EGFR wild type cases exclusively found
out that the original benefit in EGFR FISH positive cases became nonsignificant in the subset of EGFR
FISH positive, EGFR TKD wild type patients. Nevertheless, roles for EGFR FISH still need to be
determined, in particular in the large population of Caucasian, EGFR TKD wild type patients and as an
inclusion criteria for cetuximab treatment.
1.4. Influence of tumour heterogeneity and ischemia on the expression of molecular predictors of
response/resistance to anti-EGFR therapy

63
As the studies described in this thesis involve correlation between pre-operative (small) sample
biopsies and post-operative samples taken from much larger surgical specimens the issue of
heterogeneity of tumours is quite important. The role of tumour heterogeneity with respect to these
markers will therefore be reviewed.
1.4.1. Tumour heterogeneity of non-EGFR status molecular markers
1.4.1.1. KRAS
KRAS mutations are genomic variations of high relevance in cancer biology. Its role as
prognostic and predictive factor has been explored in different malignancies but evidence indicates that,
in different solid tumours, this particular mutation is heterogeneously expressed within the primary
lesion. Ovarian and pancreatic intraductal-papillary mucinous tumours as well as prostate and pancreatic
ductal adenocarcinomas have been observed with a heterogeneous KRAS mutation expression (292)
(293) (294). In these reports, frequency of KRAS mutations has been in the range of 33% to 100% cases.
Among positive cases, 33% to 100% of them presented an intratumoral heterogeneous expression
without being related to histology or differentiation (294) (292). Due to its clinical relevance,
heterogeneity of KRAS mutations has been studied in colorectal carcinoma (CRC) in more detail.
In colorectal adenomas, around 35% of cases express KRAS mutations with 35% of them
presenting these mutations mainly confined to advanced dysplastic areas (295) (296) (297). In adenomas
with focal carcinoma, 36% harboured KRAS mutations, all presenting a heterogeneous expression (295).
Among CRC studies a report in multistaged cases found 55% of them were positive for KRAS
mutations but 55% of these presented at least one negative crypt (298). A second study compared 2
tumour samples and one colonoscopic biopsy from 67 multistaged CRC patients. Of the former, 34% and
31% of the latter had KRAS mutation (299). Mutations were identical between both surgical specimens
and a concordance of 97% between the biopsy and surgical specimens was observed (kappa=0.93,
McNemar’s p=0.5). In a third report involving 100 multistaged CRC patients a sample from the tumour
center and another from the invasive front were compared (300). Forty one percent of cases presented
KRAS mutation (68% in codon 12, 32% in codon 13). In 20% of positive cases heterogeneity was
observed, with 6 cases presenting KRAS mutation at the center and two at the border exclusively.
Interestingly, this mosaicism was not observed in stage IV cases. Finally, a comparison of early (T1N0
or T2N0) against advanced (T3N1 or T4N1) CRCs has been done with 60% of the former and 53% of
the latter expressing KRAS mutations (301). All early KRAS mutation+ cases were heterogeneous, with
mutations being present in 11% to up to 93% of samples per tumour. Among the advanced KRAS

64
mutation-positive cases only 37% were heterogeneous with mutations being present in 17% to 85% of
total samples per tumour. Based on these reports, KRAS mutations present a heterogeneous expression in
CRC and other malignancies, particularly in earlier stages, with advanced disease presenting a more
homogenous expression. However, presence of a heterogeneous expression of KRAS mutations in
NSCLC has not been studied in detail.
In NSCLC heterogeneity of KRAS mutations has been studied in less detail but potentially is less
common. In an analysis of 41 adenocarcinoma, by selecting several tumour cell foci (100-200 cells) per
slide, point mutations of the c-K-ras gene were detected in 19.5% of cases with none of normal cell areas
or premalignant lesions showing this mutation (302). Eighty-sevent percent of positive tumours were
stage I and all presented a homogenous distribution with wild-type allele being detected in only 5% of
foci analyzed. In a second report 13 cases (11 adenocarcinoma, 1 large-cell carcinoma, 1 atypical
carcinoid) using similar approach (selective UV radiation DNA fractionation) KRAS mutation on codon
12 was homogeneously distributed, being present in all 71 (mean 5.5/case) areas (100-200 cells)
screened and absent in normal and preneoplastic areas (303). Although this evidence is not completely
definitive it indicates that KRAS mutations are, when present, homogenously distributed in NSCLC
adenocarcinoma type and potentially from an early stage.
1.4.1.2. BRAF
Assessment of heterogeneity of the presence of BRAF mutation in solid cancers is poor. Only
two studies have given us an introductory assessment of this, none of them in NSCLC. In 50 patients
with multifocal papillary thyroid carcinoma presenting one dominant tumour and additional smaller foci,
52% of the cases presented a BRAF V600E mutation (304). Of these, only 37.5% presented similar
mutations in both dominant and surrounding tumour and 6% showed the same BRAF mutation from the
dominant tumour in only few foci. Fifty three percent presented BRAF mutation only on the main tumour
but in none of the foci whilst 3% showed the contrary, with BRAF V600E mutation being present only at
foci. These results may suggest that presence of BRAF mutation is heterogeneous but the unclear nature
of the foci, as to where it is part of the primary, intrathyroid metastases, or second primary tumours
obscure the interpretation. A second study performed in samples from 100 CRC patients in which two
samples were obtained and compared, one from the center and a second from the invasion front, 7% of
cases presented BRAF mutation with 14% of them showing heterogeneity (300). Due to these, BRAF
mutations may have a heterogeneous presence in malignancies but a similar pattern in NSCLC remains
to be investigated.

65
1.4.1.3. Akt
There is only one study providing direct evidence exploring the heterogeneity status of Akt in
tumour samples. In a melanoma study, a heterogeneous cytoplasmic and/or nuclear p-Akt staining was
observed in 54% of benign nevi, 71.3% of primary tumours, and 71% of metastases (305). No p-Akt
immunoreactivity was seen in normal skin adjacent to the tumours. However, indirect evidence suggests
that p-Akt may be expressed heterogeneously in NSCLC. In 130 lung adenocarcinoma Asian cases,
EGFR TKD mutations were detected in 32% (306). Of these, 71% expressed phosphorylated Akt at
Ser473 residues, being significantly associated (p=0.0014). In another study of 93 NSCLC patients,
mainly in stage I, EGFR TKD mutations were found in 39.8% of them and p-Akt Ser473 in 62.4% (307).
Both were significantly associated (EGFR TKD: p-Akt+ 78.4% vs p-Akt- 21.6%, p=0.01). However,
another study of 53 pI-IIIA NSCLC cases, activated Akt (Ser473) did not associate with EGFR TKD
mutations (EGFR TKD mutation: p-Akt strong 43% vs p-Akt weak 36%, p=0.76) (308). Based on these
studies, whether the presence of Akt and p-Akt in NSCLC or other malignancies is heterogeneous has
not been defined. A potential association with EGFR TKD mutations, a molecular marker previously
defined to be heterogeneously present in NSCLC, may suggest that Akt has similar heterogeneity but
until it is directly investigated its expression pattern remains unclear.
1.4.2. Effect of ischemia on tumour expression of non-EGFR molecular markers
The studies described in this thesis involve evaluation of surgical specimens retrieved during the
course of resection. Thus there is a variable but unavoidable period of ischemia inherent in the
processing of the specimens. A review of the effect of ischemia on the markers to be studied seems
germane.
1.4.2.1. KRAS
The detection and even presence of KRAS mutations in solid tumours may be affected by
ischemia. An in vitro and xenograft-based in vivo study showed human colorectal cancer cells are
enriched for the KRAS G13D mutation under ischemic conditions (309). This enrichment was only
induced by the hypoglycemic component rather than the hypoxic part of the ischemic injury after 48
hours incubation. A concomitant reduction in expression of the mismatch repair protein MSH2 was
necessary for such induction. Interestingly, expression of MSH2 in tumour xenografts was heterogeneous
between different areas of the same tumour presenting an inverse relationship with regions of ischemia.
In a subsequent study, it was demonstrated that in response to antiangiogenic therapy, treated tumours

66
displayed highly accelerated growth compared to control tumours in the 2-week period after cessation of
therapy (310). Antiangiogenic therapy induced tumour ischemia but this also induced KRAS G13D
mutations in cells with deficient mismatch repair mechanisms with KRAS G13D mutations being
observed heterogeneously, primarily in hypoxic xenograft areas. Therefore, KRAS mutations can be
induced in vitro and in vivo xenografts of colonic cancer cells by ischemia but only after prolonged time
and, in particular, in the absence of mismatch repair protein MSH2. Similar effects in NSCLC have not
been reported.
1.4.2.2. Akt
Based on tumour cell hypoxic culture studies, overall evidence indicate that Akt levels are not
increased under hypoxic conditions. Only one report, using a head and neck squamous cell line, indicated
that Akt levels were higher under hypoxic compared against normoxic conditions after 6 hours
incubation (311). There were no differences at 15 or 30 minutes, or at 1 or 2 hours incubation. Incubation
of Hey-A8 cells (ovarian papillary cystadenocarcinoma) under 1% O2 did not cause any change in Akt
levels from 30 up to 150 minutes (312). Also, 3 breast cancer cell lines HTB30, HTB130 and HTB132
and 293T (human embryonic kidney epithelial), HTB125 (human mammary gland fibroblast), WI38
(human lung fibroblast) and HaCat (human keratinocyte) lines exhibited no measurable loss or gain in
Akt level from 2 to 24 hours under severely hypoxic (<0.5% 02) culture conditions (313).
On the other hand, an early report of reduction in Akt expression under hypoxic culture used the
human tongue squamous cell carcinoma cell line SCC-9 in which Akt showed a small reduction in
expression at 4 hours of 1% O2 culture (314). The cervical carcinoma cell line HeLa incubated in <0.5%
O2 also showed a reduction in Akt1 at 12 and 24 hours and in Akt2 at 6 up to 24 hours; neither was
affected at 2 hours incubation (313). However, a second report indicated that the cervix carcinoma HeLa
cell line did not change Akt levels after 6 hours of 1% O2 culture (315). Several additional reports using
different malignant cell lines, including pancreatic, cervical, and hepatoma lines, did not find a change
in Akt levels during the initial 6 hours of incubation under hypoxia (316) (317) (315) (318). Also, normal
cell culture did not demonstrate changes in Akt due to hypoxia at 6 hours incubation (313).
However, further hypoxic incubation time has produced confounding results. Different studies
based on malignant cell lines have reported that at 12 (316) (318), 24 (316) (313) (318) or even 48 (319)
hours of incubation under hypoxic conditions Akt levels are not modified. Conversely, a report based on
the prostate cell line LNCaP being incubated at 5% O2 observed Akt down-regulation by 8 hours of
hypoxia but returned to control levels with increasing hypoxia time (320). Additional studies based on

67
malignant cell lines reported Akt level reductions at 12 (313) (318) (321) or 24 (322) (313) (318) (321)
hours of hypoxic culture.
Particularly in NSCLC lines, A549 (adenocarcinoma) and NCI-H157 (squamous-cell carcinoma)
cell lines under 1% O2 incubation reduced total Akt after 24 hours in the former and 3 hours in the latter
(323).
Total Akt protein levels were significantly decreased in late hypoxia on several studies. Different
mechanisms may achieve this. Interestingly, a gene expression study of non-neoplastic PWR-1E prostate
epithelial cell exposed to 1% O2 for 24 hours did not identify any alterations in Akt mRNA (fold change
of 0.93 ± 0.12 with no significant difference between normoxic and hypoxic groups) (324). As Akt is
also regulated by post-translational modifications, loss of Akt expression during late hypoxia may be
explained by a decreased translation, intracellular compartmentalization, or increased
turnover/degradation.
In regards to Akt activation, different studies using malignant cell cultures indicate that Akt
phosphorylation status is modified during the initial hour of hypoxic incubation. In the HN6 HNSCC cell
line, at 15 minutes hypoxia, p-Akt is reduced from basal condition, then starts to rise above basal levels
at 0.5, 1, and 2 hours and is maintained for 6 hours (311). In the human tongue squamous cell carcinoma
SCC-9 results were the opposite. Exposure to 1% O2 resulted in a transient increase in p-Akt Ser473
levels with a maximum increase at 15 minutes and subsequent decrease until it reached basal levels at 2
hours (314). Finally, incubation of Hey-A8 cells (ovarian papillary cystadenocarcinoma) under 1% O2
induced p-Akt activation after 30 minutes, effect sustained up to 2 hours and starting to decline at 150
minutes (312). Based on these reports, Akt phosphorylation status is modified during the initial hour of
hypoxic insult in malignant cells, with a rise being the most frequent result observed, but the effects
thereafter are unclear.
The above mentioned results are not consistent in subsequent studies of Akt phosphorylation
status after two hours of hypoxia with one reporting no change, two reporting a rise with subsequent
decline at 2.5 hours in one. Only the apoptosis-sensitive HeLa cervical carcinoma cell line reported a
rapid increase in p-Akt Ser473 and Thr308 after hypoxia with <0.5% O2, being elevated at 2 and 6 hours
of hypoxic incubation, similar to the HN6 report, but long-term exposure resulted in decreased levels
with a complete loss of p-Akt at 12 and 24 hours (318). However, 3 breast cancer cell lines HTB30,
HTB130 and HTB132 exhibited no measurable loss of p-Akt from 2 to 24 h of severe hypoxia (313).
Similar observation was obtained from the apoptosis-resistant Hep3B liver adenocarcinoma cell line,
which did not show p-Akt levels modification in either Ser or Thr residues in the same time frame of 2 to
24 hours. Also, hypoxia at 1% O2 induces phosphorylation of Akt not at 2 but after 4 hours in HepG2

68
hepatoma cell line (325). Therefore, modification of Akt phosphorylation after 2 hours of hypoxia is
unclear with three studies indicating a rise while six reported no change.
The report on the ovarian cystadenocarcinoma line Hey-A8 indicates an initial rise in
phosphorylated Akt at 2 hours of hypoxia with subsequent reduction at 2.5 hours (312). On the other
hand, a report with the HepG2 cell line indicates a normal level at 2 hours but a rise at 4 (325). These
opposite results are not clarified by other studies. Two reports have indicated an increase in Akt
phosphorylation at 3 and 4 hours in gliobastoma and fibrosarcoma cell lines, respectively (326) (327).
On the other hand, in a human pancreatic carcinoma BxPC3 model in vivo, after 3 hours of 7% O2
continuous ventilation, a non-significant modest decrease of p-Akt Ser473 in hypoxic regions in relation
to non-hypoxic EF5 regions (p=0.09) was reported (328). Also, incubation of the HepG2 human
hepatoma cell line in 1% O2 resulted in a reduction in 55% and 90% of a p-Akt Ser473/total Akt ratio
after 5 and 16 hours incubation respectively (317). At 6 hours of hypoxic culture, results continue to be
controversial with the HeLa cervical carcinoma (318) (315), the HN6 HNSCC (311) and the L3.6pl
(316) pancreas cancer cell line experiencing an increase in Akt phosphorylation levels while in Hep3B
(313), HepG2 (315) hepatoma cell lines this was not modified. Therefore, Akt phosphorylation is not
homogeneously modified by 2 to 6 hours of hypoxia with studies indicating either a reduction or increase
in its status.
Particularly in NSCLC, after 6 hours of 1% O2 culture, Choi et al reported no changes in p-Akt
Ser473 phosphorylation status compared against a normoxic culture in the A549 cell line (329). A
second study in NSCLC cell lines reviewed p-Akt levels after 12 or 24 hours hypoxia. NSCLC lines
A549 (adenocarcinoma) and NCI-H157 (squamous-cell carcinoma) under 1% O2 hypoxia culture
demonstrated minimal Akt activation after 12 hours but a reduction was seen by 24 hours in the former
while in the latter it was increased at 12 hours of hypoxia and continued elevated at 24 hours (323).
Comparisons between 12 and 24 hours of hypoxic cultures have been reported in other cell lines. All
studies have reported no changes when 12 and 24 hours are compared, but while two have reported
normal values (313) (321), other two have seen low phosphorylation levels (318).
Although these discrepancies may be explained by the cell type used, inconsistency has also
been observed using the same cell type. In five studies reporting the effect hypoxic culture on Akt
phosphorylation using on the HepG2 human hepatoma cell line no change in p-Akt level was observed at
2 hours of ischemia (325). Levels were reported to be increased after 4 hours but from 5 to 24 hours
reports found either normal (315) (321) or decreased (317) values. Furthermore, a fifth report found
levels to be increased after 3 days of hypoxic culture (330).

69
Despite these results, a consistency can be observed among studies exploring p-Akt levels at
different hypoxic time points. Independently of cell type or culture time, all but one report found
continuity of normal or negative p-Akt levels in subsequent time-points if the initial finding was in this
range (313) (313) (321). More importantly, if the first p-Akt level measured is above normal values, it
will eventually reduce to normal or even below normal values subsequently (314) (312) (318) (316)
(323).
Based on this evidence, Akt levels are not modified due to hypoxia in the initial 6 hours with a
potential reduction under prolonged hypoxic time. Also, Akt phosphorylation will not be modified if the
cell is resistant to ischemic changes. However, if Akt activation is elevated due to hypoxia it will
eventually return to pre-hypoxic levels or reduce even below them. Due to a potential role as a
prognostic and predictive marker of response, these effects on Akt status are of high relevance as delayed
tissue processing time might potentially modify actual Akt and p-Akt levels, affecting their detection and
measurement.
1.4.3. Tumour heterogeneity of EGFR
1.4.3.1. EGFR protein
Several reports have observed that EGFR in solid malignancies is heterogeneously expressed
among the totality of tumour cells, making the representative value of a single biopsy questionable. A
particular malignancy in which this issue has been explored is gastric adenocarcinoma. By implementing
the quantitative advantage of a radioligand binding assay, EGFR membrane content was observed to be
widely variable (1-1239 fmol/mg of protein) (331). Also, under the semiquantitative nature of IHC, in 89
patients EGFR frequently showed variability with some cases showing only few tumour cells with high
intensity while the rest showing low or complete absence (332). Furthermore, in a comparison of
multiple endoscopic biopsies against surgical specimens for EGFR IHC positivity 100% concordance
was only observed if surgical specimens were EGFR IHC- (333). However, among positive surgical
specimens only 37.5% of biopsies presented a similar score. Even more, all positive surgical cases
showed intratumoral heterogeneity with different percentages of positive membrane staining among
negative cells. This heterogeneity has not been exclusively seen in gastric adenocarcinoma.
In a study involving breast infiltrating ductal carcinoma samples with presence of carcinoma in
situ Chhieng et al investigated the intraslide heterogeneity (334). By comparing independent intraslide
quadrants against the complete slide, infiltrating ductal carcinomas showed a mean difference of regional
versus overall score for EGFR membranous staining of 20% and for cytoplasmic staining of 13%.

70
Infiltrating ductal carcinoma has higher cytoplasmic, but not membrane, expression than in situ
carcinoma. Although each quadrant presented a good correlation with the overall slide score in both
types of malignancies, one intraslide quadrant of infiltrating carcinoma has a significantly lower value
than overall slide in regards to both, membrane and cytoplasmic compartments. In carcinomas in situ no
differences were observed with individual quadrant scores been similar than the overall slide in both,
membrane and cytoplasmic compartments. However, Nassar et al has just explored the heterogeneity of
different biomarkers using tissue microarray in breast cancer (335). One milimeter core in triplicate from
3 different areas of 44 blocks from breast cancer cases and 5 tissue samples from normal breast tissue
were stained. EGFR IHC+ was defined as ≥1% tumour cell, even if only part of the cell membrane was
stained. When a visual scoring was used, EGFR staining presented a perfect correlation among the 9
cores in regards of percentage of tumour cells and a high correlation was observed in regards of intensity.
However, when an automated image analysis was implemented, this correlation was lost. Therefore,
EGFR is heterogeneous also in breast cancer in particular when a non-robust analysis is implemented.
This heterogeneity has also has been described in NSCLC.
In an early report, negative or weakly stained areas were observed adjacent to strongly positive
areas in squamous-cell carcinomas (187). Recent reports have observed this heterogeneity as well. In 181
NSCLC cases, 61(34%) were positive for EGFR by IHC (336). Among positively stained samples,
heterogeneity was observed even within a single tumour nodule in all tumours examined. This
heterogeneity may be explained, in part, to a potential relationship with other histological or molecular
characteristics. In NSCLC adenocarcinoma cases with EGFR amplification EGFR IHC was most
consistent with a stronger signal in areas with EGFR amplification (337). Furthermore, regions with
BAC or acinar histology presented low polysomy and absent or low EGFR protein expression.
Importantly, this heterogeneity of EGFR IHC in NSCLC may affect its value as a prognostic or
predictive factor.
In 36 NSCLC patients (18 squamous, 18 adenocarcinoma) several resection specimens were
compared against one preoperative biopsy per patient (338). Positive tumour cells were scored by
quartiles. Five (14%) of the tumours were entirely positive (4 squamous, 1 adenocarcinoma) and five
(14%) completely negative (1 squamous-cell and 4 adenocarcinoma cases), with the remaining 26 cases
showing variable staining within individual blocks and between different blocks. All squamous cases
were positive on biopsy but one case had all surgical blocks negative; 4 cases had at least one surgical
block negative. Eight out of 18 adenocarcinoma biopsies were positive. Of them, 5 cases have at least
one surgical block negative with one case having all surgical blocks negative. Among the 10
adenocarcinoma biopsy-negative cases 7 had at least one block positive with five having all blocks
positive. Overall, a predictive value for a positive result obtained with the small biopsy was high (0.92,

71
95% CI 0.82–1.03) but the predictive value of a negative result was not acceptable (0.3 95% CI 0.02–
0.58). By recognizing the presence of a heterogeneous EGFR IHC expression in NSCLC, initial efforts
have been made to take it into account for patient categorization.
At the Molecular Assays in NSCLC Meeting at New York in 2006, Dr Wistuba presented data
regarding molecular heterogeneity observed in NSCLC samples (339). In 9 EGRF TKD mutation
positive patients, 65 tumour sites were selected within the tumours. Forty-two sites were scored as EGFR
IHC+ (H score >200), whereas 23 sites scored as EGFR IHC-. Due to the concern that tumour samples
might not accurately represent the entire tumour, a recommendation that at least 3 representative areas
per tumour in a given patient should be assayed was given. Nevertheless, no actual statistical justification
was provided.
This evidence implies that EGFR protein expression is heterogeneous in different solid tumours,
including NSCLC. Although EGFR expression has shown a more homogenous presence in certain
histological subtypes and/or cells with EGFR amplification, these characteristics are also heterogeneous
within a single tumour, probably contributing to heterogeneous expression at the protein level.
1.4.3.2. EGFR gene copy number
The presence and expression of the EGFR gene has also been observed to be heterogeneous.
In a study of primary gastric carcinomas comparing multiple endoscopic biopsies against
surgical specimens for EGFR amplification if the case was EGFR FISH-negative 100% concordance
between both types of tissue sources was found (333). However, all biopsies were negative either by
EGFR copy number or EGFR/CEP7 ratio among EGFR FISH-positive cases raising the question if this
was due to a heterogeneous expression. In NSCLC, several reports have observed a heterogeneous EGFR
gene presence.
Exploring this issue in adenocarcinoma cases with EGFR amplification, it has been seen that
cells are distributed heterogeneously, with EGFR gene amplification detected as 1 or 2 large clusters of
orange signals affecting its quantification due to the tight clustering of signals (336). In the remaining
samples, FISH analysis revealed more than 10 homogeneous, multiple, scattered signals over the nuclei.
In fact, by implementing CISH analysis in EGFR amplification cases a heterogeneous copy number
distribution was observed (337). Interestingly, CISH analysis showed BAC and acinar areas expressing
low polysomy whilst solid and papillary areas had amplification indicating a potential EGFR
amplification relationship to histology. This relationship with histology has also been reported in another
study. Among 48 adenocarcinoma cases with EGFR TKD mutations three different areas were analyzed

72
for gene amplification using Taq Man followed by FISH (340). Eleven cases presented amplification (2-
fold increase from normal tissue) with signals being loosely clustered. In nine of these 11 cases EGFR
amplification level was heterogeneous among areas but it was always present in all cases. EGFR
amplification was associated with high histological grade and/or invasive growth. Peripheral areas with
lepidic growth did not harbour EGFR amplification. Nevertheless, although heterogeneous expression of
EGFR gene is potentially related to histology, its prevalence has been observed to be heterogeneous in
up to 82 % of positive adenocarcinoma cases (340).
Among a more selected population, specifically adenocarcinoma cases with EGFR TKD
mutations, EGFR gene copy number still is heterogeneous. In an analysis of 9 adenocarcinoma cases
harbouring EGFR TKD mutations only 2 presented identical copy number pattern among several
samples analyzed per tumour, one with high gene polysomy and a second with amplification (341). Two
cases presented exclusively EGFR high gene polysomy but in only 83% and 43% of samples analyzed,
the rest being negative for increased copy number. One more case expressed EGFR amplification in 4
out of 5 samples. Furthermore, one case presented 80% of samples with EGFR high polysomy and 20%
with EGFR amplification. Moreover, the remaining three cases presented a mix of non-increased EGFR
gene copy number, EGFR high polysomy and EGFR amplification. Therefore, in adenocarcinoma
harbouring EGFR TKD mutations, EGFR gene copy is heterogeneously expressed not only with respect
to a positive/negative classification but even within EGFR high gene copy number cases showing
different patterns of expression.
In fact, the Colorado group responsible for developing EGFR gene copy number FISH
classification also recognizes this heterogeneity. According to Dr Varella-Garcia, EGFR gene
amplification may be homogenously distributed over the tumour areas in a tissue section or may be
confined to certain cells (142). In the latter situation, it may be present in specific foci of tumour cells or
diffusely interspaced among non-amplified tumour nuclei. These findings have supported the definition
of EGFR amplification in lung tumours in their studies based on a minimum percentage of cells (≥10%)
instead of using the gene to chromosome ratio >2 classically accepted and approved by the US Food and
Drug Administration (FDA) for the HER2 gene in breast cancer. In fact, in the heterogeneous specimens,
the ratio EGFR to CEP 7 can be significantly impacted by the selection of cells to be scored, thus
sustaining the proposed scoring in multiple tumour areas as an attempt to obtain a more representative
result.
This multi-area approach was discussed at the Molecular Assays in NSCLC Meeting at New
York in 2006, at which Dr Wistuba presented data regarding molecular heterogeneity observed in
NSCLC samples (339). In 9 EGRF TKD mutation positive patients, EGFR gene copy number
determined by FISH was described to be heterogeneous. Of 9 tumours with EGFR TKD mutations,

73
seven presented heterogeneity including FISH+ and – areas (42 sites assessed in total). Due to the
concern that tumour samples might not accurately represent the entire tumour, a recommendation that at
least 3 representative areas per tumour section multiple sections in a given patient should be assayed was
given.
In conclusion, several studies have observed that the EGFR gene is heterogeneously expressed in
NSCLC independent of the assay implemented and specimen selection by other characteristics, including
histology or presence of EGFR TKD mutations, questioning the validity of a single biopsy as
representative of the totality of the lesion.
1.4.3.3. EGFR TKD mutations
The other important molecular marker associated with clinical response to EGFR TKIs in
NSCLC, EGFR TKD mutations, also has a heterogeneous expression in tumour samples.
In an analysis of four cases harbouring EGFR TKD mutations detected originally on frozen
samples, heterogeneity of the EGFR gene mutation was explored in 10 paraffin blocks (342). EGFR
TKD mutations were identical between frozen and paraffin samples in 8 of 10 samples by direct
sequencing and in 9 of 10 by fragment length analysis; an exon-19 deletion could not be identified in one
paraffin block analyzed by both techniques, despite multiple repeated assays. Also, in an analysis of 9
adenocarcinoma cases known to harbouring EGFR TKD mutations, five cases presented the same
mutation in different areas analyzed with at least 1,000 cells. However, 2 out of 7 areas were wild-type in
one case and the remaining 3 showed different mutations in different areas (341). This suggests that
some tumours may demonstrate intratumoral heterogeneity for the occurrence of EGFR TKD mutation
expression pattern. This heterogeneous expression has also been explored using recently developed anti-
EGFR TKD mutation-specific antibodies.
Using an exon 19 deletion-specific antibody it was observed that this particular mutation is
heterogeneously distributed in EGFR gene-amplified specimens, mostly concentrating in areas with solid
growth pattern (337). Also, among 226 NSCLC cases with at least 3 microarray cores, the distribution of
a positive reaction among cores showed that 45% of cases harbouring EGFR TKD mutations presented a
heterogeneous immunohistochemical reaction (343).
In fact, heterogeneity of EGFR TKD mutations may in fact affect response to EGFR TKIs. In 21
NSCLC surgical specimens from patients treated with gefitinib due to recurrence after surgical resection,
50-60 areas from each tissue were purified by laser-capture microdissection and analyzed in 100x100x35
μm areas containing 30-60 cells (344). Fifteen cases contained only EGFR TKD mutated areas while 6

74
showed a mixture of mutated and wild-type. Of the initial 15, 8 had equal proportion of mutated and wild
type genes while 7 had more of the mutated (amplification or polyploidy). Six cases had EGFR mutated
and wild-type cells. When cases were classified between presence of only EGFR TKD-mutated cells (15
cases) and those with EGFR TKD-mutated and non-mutated cells (six cases) PFS (18 vs 7.5 months,
p=0.009) and OS (27 vs 16.5 months, p=0.003) after gefitinib treatment were significantly shorter in
those patients with EGFR TKD mutation heterogeneity.
At the Molecular Assays in NSCLC Meeting at New York in 2006, Dr Wistuba presented data
regarding molecular heterogeneity observed in NSCLC samples (339). In 9 EGFR TKD mutation
positive patients 59 tumour sites were assessed. Three patients showed multiple different mutations at
different sites within the primary tumours. One patient had some sites with exon 19 mutations but other
sites with wild-type EGFR in both the primary and metastatic sites. Due to the concern that tumour
samples might not accurately represent the entire tumour, a recommendation that at least 3 representative
areas per tumour section multiple sections in a given patient should be assayed was given.
By different assays EGFR TKD mutations have been found to be heterogeneous in NSCLC.
Direct sequencing, restriction fragment length analysis, and specific antibody staining have all found
EGFR TKD mutations to be heterogeneous within tumours with potential clinical relevance.
1.4.4. Effect of ischemia on tumour expression of the EGFR
There is contradictory evidence in regards to the potential for modification of EGFR protein
level induced by ischemia. In human pulmonary endothelial cells, culture under 1% O2 for 24 hours
resulted in an increase in both mRNA and protein EGFR levels compared against 20% O2 (345). These
effects on protein and mRNA levels were also observed in human osteosarcoma cell lines incubated for 8
hours (346). Also, exposure of the lung adenocarcinoma cell line A459 to 0.1% O2 induces EGFR
expression (347). This hypoxia-induced EGFR overexpression has been seen to be mediated via
translational and transcriptional mechanisms and, at least partially, by upregulation of Egr-1 due to
enhanced activity on the EGFR promoter (346) (348).
However, these observations may not be of relevance. For example, although exposure of the
A431 squamous carcinoma cell lines to 0.2% O2 levels for 12 hours causes 2-fold increase in EGFR
mRNA and protein synthesis rate, in fact, there was not a difference in the number of membrane receptor
per cell between aerobic and hypoxic cells (349). Moreover, in 5 different HNSCC cell lines cultivated at
1% O2 for 0.25, 0.5, 1, 2, 6, or 24 hours none experience changes in the amount of total EGFR (311).
Also, in two cell lines HN4 and HN6, gene expression was not modified after 6 hours of hypoxia. Even

75
more, in the L3.6pl pancreatic cancer cell line incubated at 1% O2 for 12 hours total EGFR was reduced
at 6 hours hypoxia and continued similarly up to 1 day in culture (316). Therefore, cell culture-based
evidence does not indicate a consistent influence of hypoxia on EGFR expression, and these effects are
probably specific to the cell type cultivated.
Clinical evidence of a potential relationship between hypoxia and EGFR levels outside of
NSCLC is not clear as well. By measuring tumour hypoxia using 60Cu-ATSM tumour uptake 6 hypoxic
and 9 nonhypoxic cervical cancer patients were detected. EGFR IHC+ was more frequently observed in
hypoxic tumours (83% vs 33%, p=0.057) (350). However, in 20 CRC patients, hypoxia was determined
by injecting the hypoxia markers pimonidazole followed by IdUrd (chronic and acute hypoxia markers
respectively) preoperatively followed by immunostaining of tumour samples. Tumour specimens were
also stained for carbonic anhydrase IX (CA IX) another hypoxia marker (351). Median percentages of
tumours cells expressing pimonidazole-IdUrd 16.7% (2.2-37.8%), CA IX 10% (0-77.9%), and EGFR
10.3% (0-95%) were determined. Both pimonidazole-IdUrd and CA IX increased with distance from
blood vessels and both were highly positive around areas of debris. However, good co-localization
between pimonidazole-IdUrd and CA IX was only found in 30% of tumours with no correlation between
them (R=0.07, p=0.76), between pimonidazole and EGFR (R=0.36, p=0.21) or CA IX and EGFR
(R=0.2, p=0.38).
In NSCLC only one clinical study has explored the association between hypoxia and EGFR.
Hypoxia inducible factor-1 (HIF-1) is a transcription factor that is stabilized by hypoxia and consists of 2
subunits. Subunit alpha is rapidly degraded under normoxic conditions. Also, HIF-1α transcription gets
upregulated under hypoxia. In a series of 178 stage I-IIIA NSCLC patients who had undergone resection
with curative intent, nuclear HIF-1α expression was observed in 55.8% of cases (352). Using the median
as a cut-off point, HIF-1α was associated with EGFR IHC+ defined as ±20% of membranous and
cytoplasmic staining of any intensity (HIF-1α-: EGFR- 53 vs EGFR+ 39, HIF-1α+: EGFR- 30 vs
EGFR+ 49; p=0.01). Also, HIF-1α regulates CA IX. Both perinuclear (pCA IX) and membranous (mCA
IX) CA IX were associated with EGFR IHC+ (353). Univariate survival analysis did not find EGFR was
a prognostic factor (EGFR IHC+: HR 1.08, 95% CI 0.77-1.51, p=0.64) but absence of pCA IX was
(HR:1.50, 95% CI 1.03-2.19, p=0.044) as was the co-expression of EGFR and pCA IX (HR=1.86, 95%
CI 1.24-2.8, p=0.003). In multivariable analyses co-expression of pCA IX and EGFR was of borderline
significance for survival (HR: 3.55, 95% CI 1-5.85, p=0.05). However, HIF-1α can also be regulated by
stress and non-hypoxic mechanisms, making its utility as hypoxia marker not definitive (354).
Based on these studies, the evidence for modification of total EGFR induced by hypoxic
conditions is not clear. Cell culture studies are contradictory and potentially cell type-dependent. Also,
clinical reports are inconclusive due to the lack of a definitive marker. Nevertheless, if hypoxia is able of

76
influence EGFR expression, this would be achieved most certainly through translational and
transcriptional mechanisms.
1.5. Use of anti-EGFR therapy in early NSCLC: study rationale
Meta-analyses have confirmed the beneficial effect of adjuvant or neoadjuvant cisplatin or
uracil-tegafur-based chemotherapy in operable NSCLC (21) (7) (22). However, the small 5-year survival
improvement observed in stage IA (2% to 4%) and IB (3% to 6%) has left unclear if adjuvant cisplatin or
uracil-tegafur-based therapy after completed resection of stage I disease, especially in tumours smaller
than 4 cm, is of any value. Furthermore, a long-term follow-up in the BR.10 trial has observed that the
initial survival benefit observed for stage IB is eventually lost in lesions smaller than 4 cm (16). Similar
size-based long-term results were obtained in Asian patients with T1N0 tumours treated with uracil-
tegafur (20). Therefore, cisplatin-based or uracil-tegafur-based regimens have not been shown to
improve survival of stage I NSCLC. Thus, surgical resection alone remains the standard of care. With the
current 5-year survival obtained by surgical resection in this population, there remains a population of
50% to 25% who are not cured by surgery alone and for whom novel approaches are needed.
In advanced NSCLC anti-EGFR therapeutic agents have been demonstrated to be of benefit. As
first-line agents, EGFR TKIs are superior to platinum/taxane-based regimens in highly selected patients
(253) (255). Also, gefitinib added to a platinum-doublet regimen and cetuximab in combination with
cisplatin-based chemotherapy prolong survival in selected patients (262) (192). Finally, in unselected
patients, EGFR TKIs may have a role as maintenance therapy in non-progressive patients after a
platinum-doublet regimen (259). As second-line options, erlotinib is the only EGFR TKI that has been
proven to prolong PFS and OS (275). Based on their activity in advanced disease, anti-EGFR agents may
have a role as therapeutic options in early NSCLC due to their activity and minimal toxicity profile, with
a potential subset of patients who may benefit by these agents.
A neoadjuvant therapeutic approach offers a unique advantage for the assessment of agents in
early NSCLC. It has been proven that neoadjuvant trials confer similar benefit to adjuvant regimens in
resectable NSCLC. In addition, they are safe and feasible, without increasing the rate of surgical
complications (22). Also, neoadjuvant approaches present different potential advantages such as better
patient compliance and treatment delivery than adjuvant regimens, theoretical early control of
micrometastasis, and reduction in tumour size facilitating complete resections. A neoadjuvant trial also
confers the advantage of allowing a clinical assessment of an agent, with radiological comparison of
tumour status before and after therapeutic period. Furthermore, while adjuvant trials are able to generate
biological samples before drug exposure, neoadjuvant regimens have the unique advantage of collecting

77
tumour specimens after exposure to the agent under assessment. While with the former studies try to
detect predictors of response, the latter approach gives the opportunity of characterizing samples in
which response has been observed for a better understanding of tumour response in vivo.
Anti-EGFR agents, given their activity in advanced disease, may benefit and potentially improve
cure in the subset of patients with early NSCLC. With a preoperative trial of gefitinib, it is possible to
identify patients undergoing clinical and pathologic response. It may be that this subset of patients,
commonly with EGFR TKD mutations or amplification, may benefit from adjuvant therapy. Based on
this rationale, we investigated the use of an EGFR TKI, gefitinib, in a neoadjuvant phase II trial
implemented in clinical stage I NSCLC patients. This study provided the opportunity to explore the
impact and feasibility of EGFR inhibition on early stage NSCLC in humans. The neoadjuvant design
facilitated the identification of predictive markers for response to gefitinib in early stage NSCLC by
analyzing samples obtained after gefitinib treatment. Also, by a comparative approach, the intracellular
signaling pathways that are being inhibited by EGFR TKI therapy in vivo were examined. Furthermore,
through a detailed review of surgical experiments histopathological changes suffered by NSCLC
specimens under EGFR TK inhibition were characterized and their association with clinical response
examined. Finally, due to a potential influence observed in clinical samples and cell cultures, the effect
of ischemic time and heterogeneity on the EGFR expression was examined. This approach may help
further define the subset of patients who would benefit from adjuvant EGFR TKIs and the potential role
of these agents in early NSCLC.
1.6. Hypothesis and study aims
1.6.1. Hypotheses
A neoadjuvant regimen with an EGFR TKI will confer clinical response in early NSCLC.
Clinical response to be defined by histopathological changes in primary tumours, suppression of
intracellular signaling and associated with the same molecular predictors observed in advanced
NSCLC. EGFR will be affected by ischemia and expressed heterogeneously in tumour specimens.
1.6.2. Specific study aims
Our hypotheses were to be tested by following specific study aims:
1. To assess clinical response to a neoadjuvant gefitinib regimen in clinical stage I NSCLC.

78
2. To investigate the association of clinical response induced by a neoadjuvant gefitinib regimen with
clinical and molecular predictive markers in early NSCLC.
3. To characterize histopathologic response in early NSCLC after a neoadjuvant gefitinib regimen.
4. To assess the relationship of cellular subtypes with clinical and molecular predictors of response.
5. To evaluate the association of epithelial-mesenchymal transition markers with clinical and
histopathological response.
6. To assess the inhibition of epidermal growth factor receptor as well as related intracellular signaling
pathways and their association with clinical and histopathological response after a neoadjuvant gefitinib
regimen in early NSCLC.
7. To explore the heterogeneity and effect of ischemic time in the expression of epidemal growth factor
receptor in NSCLC.

79
Chapter 2
Materials and Methods

80
2.1. Clinical trial
This was an open label, single arm phase II study in patients with clinical stage I NSCLC. This
study was approved by the institutional Research Ethics Board. Patients were eligible for the trial if they
were 18 years of age or older with biopsy-proven NSCLC, had clinical stage I with T≥10 mm on high
resolution computed tomography or CT scan and were fit for surgical resection. Patients were excluded if
they had received previous therapy for lung cancer, had another cancer diagnosis in the last 5 years
except adequately treated non-melanoma skin cancer or in-situ cervical cancer, incomplete healing from
previous surgery, were taking medications that induced or inhibited cytochrome P450 3A4 or decreased
gastric acid production, had uncontrolled intercurrent illness, were pregnant or breastfeeding, or had
active human immunodeficiency virus infection.
Consenting patients underwent an additional core-needle biopsy at the time of their diagnostic
fine needle aspirate. Patients were staged with CT scans of the chest and upper abdomen, MRI of the
brain and bone scan, complete medical history and physical examination, complete blood count and
biochemistry panel.
Patients received gefitinib 250 mg orally once daily for up to 28 days. Treatment was
discontinued within 48 hours prior to surgical resection. Patients were evaluated with weekly physical
examination and bi-weekly blood tests. Toxicity was evaluated continuously (National Cancer Institute
Common Terminology Criteria for Adverse Events, version 3.0). Treatment was withheld, reduced or
discontinued if patients developed unacceptable toxicity, refused to continue, or at the investigators’
discretion. CT scan of the chest was repeated immediately prior to surgical resection. Tumour response
was evaluated by Response Evaluation Criteria in Solid Tumours (RECIST) except confirmatory scan
(355).
2.2. Serum samples
Serum samples were obtained and stored at –80° C. Detection of serum TGF-alpha was
performed by ELISA (Human TGF-alpha antibody ELISA kit, Biosource, Sunnyvale, CA).
2.3. Specimen handling and histopathological assessment
Pre-treatment core-needle biopsies and post-treatment surgical biopsies were snap-frozen and
stored at -80° C. Intraoperative tumour ischemic time was recorded. FFPE blocks were also processed

81
from surgical specimens. Hematoxylin-Eosin (H&E) stained sections from all samples were evaluated
for tumour cellularity.
For each case the routine surgical pathology H&E slides and their corresponding blocks were
retrieved and evaluated blinded to clinical data on response. Tumours were staged according to the 7th
edition of the TNM classification (356). Tumour features assessed included histological type according
to 2004 WHO classification of NSCLC and the recently published International Association for the
Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification of lung
adenocarcinoma (357) (358) (359), tumour differentiation/grade, tumour cellularity, presence of local
invasion (lymphatic, vascular, pleural), intra- and peri-tumoral inflammatory response and lymphocytic
aggregates, elastin staining pattern and degree of fibrosis by Mason’s trichrome staining. For
adenocarcinomas, the proportion of various histological patterns (BAC, acinar, papillary, and solid) was
also estimated (359) and the pattern observed in ≥50% of the tumour area was designated as the
predominant pattern. Since the effect of prolonged (4 weeks) gefitinib therapy on adenocarcinoma with
predominantly lepidic type is unknown, the subcategories of adenocarcinoma in situ or minimally
invasive adenocarcinoma were not included.
For the ischemia-heterogeneity study tumour samples were obtained from 10 patients with
adenocarcinomas and 10 with squamous-cell carcinomas who did not receive neoadjuvant therapy and
underwent surgical tumour resection. Intraoperative tumour ischemic time was recorded. After resection,
surgical specimens were immediately processed. Tumours were dissected through their major diameter,
dividing them in roughly similar halves. Using the same half, four tumour samples were harvested from
the center of imaginary quadrants. These four samples were immediately fixed in buffered formalin and
the time recorded. Three additional samples from one of the quadrants were obtained and fixed in
buffered formalin at 15, 30 and 45 minutes following initial fixation time. All samples were maintained
in buffered formalin for 24 hours, transferred to 70% ethanol and processed in a standard fashion.
2.4. IHC assessment
FFPE blocks with the greatest tumour cellularity from the clinical trial and all derived from the
ischemia/heterogeneity study were selected for IHC studies. All available frozen pre- and post-
treatment samples also underwent IHC assessment. IHC was performed using the avidin-biotin
method. Briefly, for FFPE blocks four micron sections were dried overnight at 60°C, deparaffinised with
xylene, transferred through changes of ethanol and rehydrated using standard histological protocol.
Endogenous hydrogen peroxide activity was blocked by 10 min incubation in 3% hydrogen peroxide

82
buffer. Microwave antigen retrieval was performed in MicroMed T/T (Hacker Instruments, Fairfield, NJ)
oven for 10 min at 120°C unless otherwise specified. For frozen samples consecutive 5 micron sections
were obtained at -20° C and immediately fixed in 5°C 2% paraformaldehyde for 20 min. Endogenous
hydrogen peroxide activity was blocked by 10 min incubation in 0.3% hydrogen peroxide buffer. All
sections were incubated overnight with primary Abs listed in Table 2-1. After washing, slides were
incubated for one hour with biotinylated secondary antibody, followed by streptavidin-horseradish
peroxidase using the Multi-Species Ultra Streptavidin Kit (Signet Laboratories, Dedham, MA). The
immunoreactivity was revealed by 5 min incubation with the NovaRed substrate kit (Vector
Laboratories, Burlingame, CA), and then counterstained with Mayer’s hematoxylin. Negative control
slides omitting the primary antibodies were included in all staining procedures. Assessment of stained
slides was performed under a bright field microscope (Axioskop, Zeiss, Germany) under 5, 10, and 40x.
Slides were reviewed without knowledge of the clinical data. After initial training with a senior
pathologist presence of heterogeneity, cellular compartment, intensity of the signal and percentage of
tumour cells showing staining were recorded from whole slide. For the clinical trial, EGFR IHC+
expression was defined as more than 10% of tumour cells showing any membranous staining of any
intensity. For proliferative index (Ki-67), Met, E-cadherin, vimentin and Snail percentages of tumour
cells independent of intensity were used. In the pre/post-gefitinib comparison a score was calculated
taking including an intensity scale as follow: 0=negative, 1=weak, 2=moderate, 3=strong. Immunoscore
from each cellular compartment (membrane, cytoplasmic and nuclei) was calculated by multiplying
intensity by percentage of tumour cells involved with final score adding individual values from each
compartment giving a range from 0 to 900. A ratio was calculated by dividing staining of phosphorylated
isoforms by their respective total immunoscores.

83
Table 2-1. Abs used in IHC assessments.
Antigen clone Host Species
Type Company Dilution Incubation time
Antigen retrieval
FFPE EGFR 31G7 mouse monoclonal Zymed 1:300 overnight pepsin Ki-67 MIB-1 mouse monoclonal Dako 1:200 1 hour microwave Met DL-21 mouse monoclonal Upsate 1:200 overnight microwave E-cadherin 36B5 mouse monoclonal Vector Lab 1:100 overnight microwave Vimentin VIM 3B4 mouse monoclonal Dako 1:300 1 hour pepsin Snail goat polyclonal R&D 1:1000 overnight microwave Frozen pEGFR Y1173 9H2 mouse monoclonal CalBiochem 1:100 Overnight pEGFR Y1068 1H12 mouse monoclonal Cell Signaling 1:400 overnight Akt 5G3 mouse monoclonal Cell Signaling 1:100 overnight pAkt Thr308 rabbit polyclonal Cell Signaling 1:100 overnight pAkt Ser473 736E11 rabbit monoclonal Cell Signaling 1:200 overnight Erk 1/2 rabbit polyclonal Cell Signaling 1:100 overnight pErk 1/2 Thr202/Y204 20G11 rabbit monoclonal Cell Signaling 1:100 overnight

84
2.5. FlSH
FISH for EGFR gene copy number assessment was performed on FFPE sections with the use of
probes specific for the EGFR locus and the CEP7 chromosome 7 centromere (Abbott Molecular, Des
Plaines, IL, USA). Signals were analyzed in at least 100 non-overlapping tumour cell nuclei. EGFR gene
copy number was determined and tumours were classified with samples with high polysomy or
amplification grouped as high EGFR gene copy number (279) (141).
2.6. Mutational analysis
For mutation analyses tumours were microdissected from 5 μm frozen sections stained with
toluidine blue (Fisher Scientific Co, Edmonton, AB, Canada). DNA was isolated according to the
phenol-chloroform protocol. Two assays, in duplicate, were used to determine the presence of mutations
on exons 19 and 21 of the EGFR gene. The initial screen was performed by fragment length analysis
(FLA) method (360). For the exon 19 deletion assay, the amplicons were subjected to capillary
electrophoresis on an ABI 3130x1 genetic analyzer (Applied Biosystems, Foster City, CA). For the exon
21 L858R mutation, the PCR product was subjected to Sau96I digestion followed by sequence analysis
using the ABI 3130 sequence analyzer. All samples were confirmed by running a second independent
nested PCR and sequenced directly with an ABI3100 sequence analyzer (Applied Biosystems, Foster
City, CA). For EGFR T790M and KRAS analyses, exon 20 of the former and exon 2 of the latter were
amplified and sequenced directly in duplicate.
2.7. Statistics
For the clinical trial, the primary endpoint was the objective response rate by RECIST. Based on
a 20% response rate with a 95% confidence interval equal to the response rate plus or minus 12%, a
sample size of 42 patients was estimated. This sample size provides 80% power to detect a 45%
difference of clinical benefit amongst the secondary endpoints. Patient characteristics, toxicity and
tumour response were summarized using descriptive statistics.
Associations between variables and molecular markers were analyzed using either Spearman
correlation coefficient between two continuous variables, Wilcoxon signed rank test between paired
immunoscores, Wilcoxon 2-sample test between a continuous variable and a binary variable, Kruskal-
Wallis test between a continuous variable and a categorical variable with 3 or more levels, and Fisher’s

85
exact test between two categorical variables with 2 levels each. Associations with radiologic
measurements of tumour change were tested using linear regression.
For the ischemic/heterogeneity study Principal Component Analysis was used to determine the
minimum variables retaining most of the database variance. To estimate the contribution of cellular type,
patient, tumour quadrants and randomness to the total variance, Variance Component Analyses for each
selected variable was estimated. A repeated measures general lineal model was used to analyze the
influence of ischemic time.
All statistical tests were two-sided and any p-value of less than 0.05 was considered statistically
significant. All statistical analyses were performed using PASW Statistics version 18.0 (SPSS Inc,
Chicago, IL, USA).

86
Chapter 3
Neoadjuvant gefitinib trial in clinical
stage I NSCLC: feasibility, clinical
response and its association with clinical
and molecular predictor markers of
response
Portions of this chapter were presented at the International Association for the Study of Lung
Cancer 12nd World Conference on Lung Cancer poster discussion session (September 2007, Seoul
Korea) and the Canadian Association of Thoracic Surgery Annual Meeting oral session (September
2007, Toronto, Canada). Abstracts were published in the Journal of Thoracic Oncology, 2007;2(8):S464
and the Canadian Journal of Surgery, 2007;50:32, respectively.
The content of this chapter was published in the Journal of Clinical Oncology 2009;27(36):6229-
36.

87
3.1. Abstract
EGFR TKIs have proven efficacy in NSCLC. However, their role in early stage NSCLC has not
been established. We hypothesize that the use of preoperative gefitinib in clinical stage I NSCLC will
induce tolerable toxicity and a tumour response that will relate to clinical and molecular predictors of
response. We designed an open label, single arm trial in which patients received 250 mg/day of gefitinib
for up to 28 days followed by mediastinoscopy and surgical resection. Tumour response was evaluated
by RECIST. Thirty-six patients completed preoperative treatment (median duration 28 days, range 27-
30). Three patients experienced grade 3 toxicities [rash, diarrhea, and elevated alanine transaminase
(ALT)]. Partial response (PR) was seen in 4 (11%) cases and disease progression (PD) in 3 (9%). Blood
samples and tumour biopsies were collected and analyzed for TGF-alpha level, EGFR protein
expression, EGFR gene copy number, and EGFR TKD (exon 19 to 21) and KRAS mutations. Tumours
demonstrated EGFR positive protein expression in 83%, high gene copy number in 59%, EGFR
mutations in 17%, and KRAS mutations in 17%. Tumour shrinkage was more frequent among female
patients and non-smokers. The strongest predictor of response was EGFR TKD mutation. We conclude
that preoperative window therapy with gefitinib is a safe and feasible regimen in early NSCLC and
clinical response is associated with presence of EGFR TKD mutations.

88
3.2. Introduction
Lung cancer leads causes of cancer-related deaths in North America with NSCLC accounting for
80-85% of cases. Stage I NSCLC is amenable to potentially curative surgery with a 5-year survival rate
of 60 to 70% (4). In more advanced stages, poor survival rates have led to extensive investigation of
adjuvant and neoadjuvant therapies.
Adjuvant cisplatin-based therapy has become the standard of care for patients with completely
resected stage II and III NSCLC, but data are less compelling in stage I (361). Neoadjuvant therapy has
also failed to improve survival for this subpopulation (362) (21) (363) (364) (365) (366). Therefore,
assessment of new agents in early NSCLC is of considerable interest.
EGFR has been the target of drug development for several years. EGFR TKIs include
quinazoline-based compounds, such as gefitinib (IRESSA®, AstraZeneca, Wilmington, DE) and
erlotinib (TARCEVA®, OSI Pharmaceuticals, Inc., Melville, NY). In advanced NSCLC clinical trials,
gefitinib has demonstrated anti-tumour activity but in early stages its utility has not yet been defined
(367) (368) (251) (252) (232) (269) (154) (273) (369) (370) (271). Adenocarcinomas, never smoking
status, female sex and Asian ethnicity have been related to clinical response. EGFR TKD mutations,
increased EGFR gene copy number and EGFR protein expression have been reported as molecular
predictors of response, and KRAS mutations as a potential negative predictor (234). Given the activity of
EGFR TKIs in advanced disease, there is potentially a subset of early NSCLC patients who may benefit
from neoadjuvant and/or adjuvant EGFR TKIs. In this study, we administered oral gefitinib to clinical
stage I NSCLC patients during a four-week preoperative window, exploring the impact of gefitinib on
clinical response and investigation of potential laboratory predictive markers.
3.3. Results
3.3.1. Patients enrolment
Between February 2005 and August 2007, 81 patients were invited to participate, 73 accepted
but only 36 were eligible and completed treatment (Figure 3-1). Demographic and clinical characteristics
are described in Table 3-1. Accrual was stopped after 36 patients were enrolled, as it was deemed highly
unlikely that further enrolment would reach the target response rate (probability 0.19%), or contribute
significant additional data.

89
Figure 3-1. Trial schema, patient enrollment and sample collection.

90
Table 3-1. Baseline patient and tumour characteristics
Characteristic Frequency
Median age at surgery (range) 65 years (38 – 81)
Sex
Male
Female
18 (50%)
18 (50%)
Ethnic group
Asian
Other
3 (8%)
33 (92%)
Smoking status
Current smoker
Ex-smoker
Never smoker
12 (33%)
18 (50%)
6 (17%)
Histology
Adenocarcinoma
Squamous-cell carcinoma
Large cell undifferentiated carcinoma
28 (78%)
7 (19%)
1 (3%)
Clinical T stage
T1
T2
24 (67%)
12 (33%)

91
3.3.2. Treatment delivery
Thirty-two (89%) patients took preoperative gefitinib for 28 days; two patients for 27 days, one
for 29, and one for 30 due to timing of surgery. Median time from last dose to surgery was 3 days. One
patient was delayed for 20 days due to fever unrelated to gefitinib treatment.
3.3.3. Safety
Toxicities during gefitinib therapy are summarized in Table 3-2. Three patients developed grade
3 toxicities (rash, diarrhea, and ALT elevation) but did not require either dose reduction or
discontinuation.
3.3.4. Surgical treatment and postoperative period
All patients underwent surgical resection; 2 (5%) patients underwent bilobectomy and the rest
lobectomy.
Median post-operative hospital stay was 5 days (range 3-87). One patient, with undiagnosed
hypertrophic obstructive cardiomyopathy, developed grade 4 pulmonary edema, requiring prolonged
ventilation (66 days). Other grade 3 or 4 postoperative toxicities included one pulmonary embolism, one
delayed pneumothorax, and one pneumonia with respiratory failure requiring ventilation. There were not
perioperative or 90 days postoperative deaths.

92
Table 3-2. Toxicities observed during gefitinib therapy considered related to study treatment.
Toxicity Number of patients (%)
Total (%) Grade I Grade II Grade III Grade IV
Dermatological
Dry skin 18 (50) 6 (17) - - 24 (67)
Pruritus 13 (36) 2 (6) - - 15 (42)
Acne/rash 11 (31) 5 (14) 1 (3) - 17 (47)
Constitutional
Fatigue 21 (58) 6 (17) - - 27 (75)
Anorexia 5 (14) 1 (3) - - 6 (17)
Gastrointestinal
Diarrhea 9 (25) 4 (11) 1 (3) - 14 (39)
Nausea 6 (17) 1 (3) - - 7 (19)
Constipation 1 (3) - - - 1 (3)
Vomiting 1 (3) 1 (3) - - 2 (6)
Ophthalmologic
Dry eyes 6 (17) 1 (3) - - 7 (19)
Blurry vision 3 (8) - - - 3 (8)
Laboratory
↑ BUN 1 (3) 1 (3) - - 2 (6)
↑ ALT - 1 (3) 1 (3) - 2 (6)
↑ AST - 1 (3) - - 1 (3)
↑ ALP - 1 (3) - - 1 (3)

93
3.3.5. Clinical response
Thirty-five patients were evaluable for response. One patient had an endobronchial lesion and
could not be assessed. Four (11%) patients had PR and three (8%) PD. Fifteen (43%) patients had some
tumour reduction, 15 had an increase and 5 were unchanged. Among patients with growing tumours, one
clinically upstaged due to a change from 3.0 to 3.1 cm. In final pathologic stage two tumours were pT3
because of local invasion and one was pT4 because of a satellite intralobar nodule. Clinical and
pathologic stages were concordant in 83% of cases.
Associations of various clinical and pathological characteristics with tumour response are shown
in Table 3-3 and Figure 3-2. Of the 4 patients who experienced a PR three were female, one Asian, two
lifetime non-smokers and two former smokers; all had adenocarcinoma. Of the 6 lifetime non-smokers in
the study, only 4 had EGFR TKD mutations.

94
Table 3-3. Association of clinical and molecular characteristics with tumour response.
N % Tumour
reduction n=15
% p PR
n=4 % p
Sex Female 18 51 11 61
0.04* 3 17
0.6 Male 17 49 4 23 1 6
Ethnicity Asian 3 9 2 67
0.56 1 33
0.31 Other 32 91 13 41 3 9
Smoker
Active 12 34 4 33
0.009*
0 0
Ex - 17 49 5 29 2 12 0.1
Never 6 17 6 100 2 33
Acne or
Rash
Yes 17 49 5 33 0.18
1 6 0.6
No 18 51 10 67 3 11
Histology Adenoca 27 77 13 48
0.42 4 15
0.56 Other 8 23 2 25 0 0
Change in TGF-alpha
Decrease 9 47 4 44 0.63
2 22 0.58
None 10 53 3 30 1 10
EGFR IHC Positive 29 83 14 48
0.21 4 14
1 Negative 6 17 1 17 0 0
EGFR gene copy
High 20 59 10 50 0.49
4 20 0.13
Low 14 41 5 36 0 0
KRAS mutation
Yes 6 17 2 33 0.68
0 0 1
No 29 83 13 45 4 14
EGFR mutation
Yes 6 17 6 100 0.003*
3 50 0.01*
No 29 83 9 31 1 3
* Statistically significant.
Two-sided p-values are from Fisher’s Exact Test (FET) and Chi-square. PR: partial response

95
Figure 3-2. Waterfall plots illustrating associations of A) sex, B) ethnicity, C) smoking, D) acne or rash, E) histology, F) TGF-alpha, G) EGFR IHC, H) EGFR gene copy number, I) KRAS mutation, and J) EGFR TKD mutation with changes in tumour diameter. Y-axis indicates percentage of change before and after neoadjuvant gefitinib treatment; bars represent individual cases.

96
3.3.6. Analysis of serum samples and tumour specimens
Associations of molecular characteristics with response are summarized in Table 3-3 and Figure
3-2. Overall, of the 4 patients with PR, 2 had decreasing TGF-alpha levels on treatment, all were EGFR
IHC+, had high EGFR gene copy number, were KRAS wild type, and 3 had EGFR TKD mutations.
Figure 3-3 illustrates overlapping molecular features.
Serum TGF-alpha (pg/ml) was measured in 21 patients with paired samples pre- and post-
gefitinib in 19. Mean concentrations (+/- standard deviation) at baseline, post-gefitinib and at 30 days
post-surgery were 7.79 (12.5), 6.02 (6.9), and 5.04 (7.2). Changes in pre/post-gefitinib levels were not
associated with PR or tumour reduction.
EGFR IHC scoring was performed in all tumours; 83% were scored as EGFR IHC+.
EGFR FISH testing was successful in 35 surgical samples; one case had insufficient tumour cells
(<100 cells). High copy number was seen in 60%, amplification in 17% and high polysomy in 43%.
Among the six cases with amplification, 2 presented with small tumour growth, 1 did not change, 2 were
PR and one was the case not able to be measure.
EGFR TKD mutation analysis was performed on pre- and post-treatment samples of the initial
12 patients. No differences were observed and therefore only post-treatment specimens were analyzed
subsequently. EGFR TKD mutations on exon 19 or 21 were detected in 4 and 2 patients respectively
(Table 3-4). Two were ex-smokers, 4 were non-smokers. No mutation was detected in exon 20. All six
patients with EGFR TKD mutation experienced at least some reduction in tumour size. The only
significant predictor of PR was the presence of an EGFR TKD mutation. Four patients with EGFR TKD
mutations also had high EGFR gene copy number. Of the remaining 17 patients with high EGFR gene
copy number but no mutation, one experienced PR and 37% had some tumour reduction.
Six patients had KRAS mutations, two smokers with transition type (GGT→GAT) and 4
transversions in 3 active smokers and 1 ex-smoker (GGT→TGT); all of them were EGFR TKD mutation
negative; none reached PR.

97
Figure 3-3. Venn diagram illustrating overlapping positive correlative studies.

98
Table 3-4. Cases with EGFR TKD mutations and its associated EGFR gene copy number and response.
Exon Mutation Nucleotide Change FISH Response (RECIST)
19 delE746_A750 Δ2236_2250 High polysomy --
19 delE746_S752insV Δ2237_2255 + Tins High polysomy PR
19 delL747_P753 Δ2240_2257 Low polysomy --
19 delL747_S752 Δ2239_2256 Amplification PR
21 L833V; H835L 2743 T>G; 2750 A>T Low polysomy --
21 L858R 2573 T>G High polysomy PR
Note: all six cases were EGFR IHC+

99
3.4. Discussion
Using a preoperative window trial we were able to assess tumour response in 97% of cases with
gefitinib demonstrating to be an active agent with minimal toxicity without additional surgical risk in
patients with clinical stage I NSCLC. After 28 days of treatment, tumour shrinkage was seen in almost
half of patients, with an overall PR of 11%. In an exploratory study of potential predictors of response
EGFR TKD mutations was the only associated with PR.
Exploring other therapeutic options for early NSCLC is of high importance. Cisplatin-based
chemotherapy has improved survival for resected stage II and III NSCLC, but not in stage I (361). In
addition, toxicity and decreased compliance persist with up to 67 % patients in adjuvant and 32 % in
neoadjuvant clinical trials failing compliance and, in daily practice, only half of patients accepting
adjuvant therapy (361) (362) (363) (365) (12) (371) (372) (373) (13) (374) (375) (23). Therefore, it is
important to find more acceptable and less toxic treatments with equivalent or improved efficacy for the
early NSCLC population.
Clinical predictors of response to EGFR TKIs have been reported in advanced NSCLC, usually
after prior chemotherapy (232) (269) (154) (369) (231) (264) (275). Female gender and non-smokers
have been associated with tumour response. While we did not see an association of these characteristics
with PR, we did see an association with decrease in tumour size.
Among patients with advanced NSCLC, increased levels of serum TGF-alpha have been
associated with resistance to gefitinib and shortened survival (376). Although we did not have samples
from our entire cohort, reduction in TGF-alpha was not significantly associated with response.
The value of EGFR IHC in patient selection for EGFR TKIs remains controversial. Positive
EGFR IHC has been associated with higher response rate and improved survival in some (369) (279)
(141) (278) but not all trials (263) (277) (377) (378) (379). These conflicting results may be due to
several variables, including the lack of standards for antibody, staining protocol, scoring methodology
and its semi-quantitative nature (191) (339). Eighty-three percent of our samples were EGFR IHC+ and,
although there was a 31 % difference between EGFR IHC+ and IHC- patients, there was no association
with tumour reduction. Indeed, one patient identified as EGFR IHC- approached PR. Thus, assessment of
the membrane compartment in a simple tumour sample by IHC is a weak marker at best to predict
response to gefitinib in early NSCLC.
In advanced NSCLC, high EGFR gene copy number appears predictive for response (278) (369)
(370) (279) (141) (379) (380) (283). Results from the current study (RR 20% high copy number, 0% low
copy number) are consistent with findings from advanced disease. However, eight of 15 (53%) patients

100
experiencing tumour growth had high EGFR gene copy number, suggesting that EGFR gene copy
number may not be adequate to select patients for adjuvant therapy. A possible explanation is the
elevated EGFR high gene copy number rate observed. In the BR.21 and ISEL trials, patients with a high
copy number represented only 38% and 31% of the sample, but recent data has reported higher
prevalence (41% and 48%) (278) (283) (381) (382). Our cohort had a higher rate of high EGFR copy
number of 59%. It is unclear why we observed this high frequency of EGFR FISH+ cases but one
possible explanation is that our cohort consisted of early stage NSCLC patients, for whom the
distribution of EGFR gene copy number has not been reported.
Accumulating data suggest that advanced NSCLC patients whose tumours have KRAS mutations
may not benefit from EGFR TKI (288) (277). In fact, KRAS mutations may be a marker of resistance for
both EGFR TKI treatment and chemotherapy (277). Our KRAS mutation rate of 17% is similar to what
has been reported previously in advanced NSCLC and was not associated with tumour response, being in
accordance with an analysis derived from the NCIC-CTG JBR.10 study, in which the presence of RAS
mutations was neither prognostic nor predictive of response to adjuvant cisplatin/vinorelbine (383).
However, it is important to recall preclinical data showing that cell lines with KRAS mutations may still
exhibit sensitivity to EGFR TKI (384).
EGFR TKD mutations have been widely described as a predictor of benefit to EGFR TKI. Our
response rate of 11% is consistent with previous reports in advanced disease (283) (288) (370) (380)
(381) (382) (383) (255) (148) (149) (150). We detected EGFR TKD mutations in 6 (17%) tumours, 4
exon 19 deletions and 2 mutations in exon 21, similar to previous reports from Caucasian populations
(278) (279) (288) (141) (168). Although all six patients with EGFR TKD mutations showed reduction in
tumour size, only half reached PR. Also, 60 % of patients with tumour reduction, including one patient
who achieved PR, had wild type EGFR reminding us that even patients without EGFR TKD mutations
can derive benefit from EGFR TKI therapy (279) (283). Although EGFR TKD mutations have been
associated with a survival benefit in cohort analyses, it is important to recall that despite predicting
tumour response and PFS, EGFR TKD mutations have not yet been shown to predict better OS with
EGFR TKI treatment in controlled trials (279) (285) (288) (255).
Eleven percent of our samples were positive for all three EGFR biomarkers, and 58% of samples
had at least 2 biomarkers of response positive. Overlapping of EGFR biomarkers has been described
previously, with 30-70 % of cases being positive for a second marker once a first has been detected (369)
(381). This makes assessment of the individual contribution of each marker difficult with additive effects
may be important. However, we were unable to identify additional predictive biomarkers in patients with
wild type EGFR TKD for benefit from gefitinib. Nevertheless, at present, neither clinical characteristics
nor molecular biomarkers are adequate to select patients for EGFR TKI therapy (385). While certain

101
groups are more likely to experience response, it has not been demonstrated that they derive greater
survival benefit. In this scenario, a window of preoperative therapy may enhance selection of patients
with responsive disease, serving as a strategy for planning adjuvant EGFR TKI therapy, particularly in
early NSCLC if ongoing trials suggest a benefit for this population.
In conclusion, the low adverse events rate, high compliance, and response rate observed indicate
that neoadjuvant gefitinib is a feasible regimen for early NSCLC, with EGFR TKD mutations being
associated with response with a preoperative window trial suggesting to be a promising design in
exploring the impact of EGFR TKI and other novel molecularly-targeted therapies in NSCLC.

102
Chapter 4
Histopathological features and IHC
markers associated with clinical response
to neoadjuvant gefitinib therapy in early
stage NSCLC
The content of this chapter has been submitted to the Lung Cancer for consideration for publication.

103
4.1. Abstract
Gefitinib was able to induce clinical response as neoadjuvant regimen in early NSCLC. In order
to define pathological features associated with response to EGFR TKIs in NSCLC, the 36 surgical
specimens from early NSCLC patients treated preoperatively with gefitinib were evaluated for tumour
histopathological features and IHC markers of proliferation (Ki-67) and epithelial mesenchymal
transition (EMT). Six adenocarcinomas harboured an EGFR TKD mutation; five were the sensitizing
type. Five adenocarcinomas with EGFR TKD mutation demonstrated non-mucinous lepidic growth
pattern as the dominant histological feature. Post-gefitinib treated EGFR TKD mutant adenocarcinomas
demonstrated lower tumour cellularity and proliferative index compared to EGFR TKD wild type
adenocarcinomas and non-adenocarcinoma cases, features correlating with clinical response. Responding
tumours also showed large areas of fibrosis, within which focal residual viable tumour cells were noted.
However, there was no significant correlation between the degree of fibrosis and radiological changes in
tumour size. Expression of EMT markers was not associated with significant change in tumour size. To
our knowledge this is the first report of the histopathological changes in NSCLC tumours after EGFR
TKI therapy and their association with clinical response. These results suggest that radiologically
assessed response to EGFR TKIs in NSCLC is related to loss of tumour cellularity and reduced tumour
cell proliferation but residual viable tumour cells may persist even after prolonged treatment. This
provides a unique evidence of the pathological and biomarker changes induced by EGFR TKIs in
NSCLC.

104
4.2. Introduction
It is now established that EGFR TKIs can improve the survival of previously treated and
untreated advanced NSCLC patients (275) (255). Higher response rates to EGFR TKI therapy have been
observed in NSCLC patients who are East Asian, never-smokers, female or present with adenocarcinoma
histology (275) (234). Among adenocarcinoma patients, better response rate was also reported in
tumours with prominent BAC growth pattern (154) (379). However, molecular studies have
demonstrated that the presence of mutations in the TKD of the EGFR is a better predictor of response
than adenocarcinoma histology (234) (283) (385). In contrast, EMT is a potential marker of resistance to
EGFR TKI therapy (386) (387). Met is a tyrosine kinase receptor involved in EMT whose activation or
gene amplification has been associated with resistance to EGFR TKIs in advanced NSCLC (388) (389).
Due to the lack of surgical therapy offered to patients with advanced disease, detailed correlation
of the pathological changes associated with EGFR TKI therapy has been limited. In the previous chapter
we explored the feasibility of neoadjuvant gefitinib therapy in early stage NSCLC and demonstrated that
EGFR TKD mutations are the strongest predictor of clinical response. This trial has provided us with the
unique opportunity to examine the histology of NSCLC tumours post-EGFR TKI therapy, allowing for a
correlation of the histological findings with clinical response and selected molecular features. Due to
this, the objectives of the present study are to report the histopathological findings in early stage NSCLC
specimens after EGFR TKI therapy, the expression of Met and EMT markers, and the correlation
between these histological and molecular factors with radiologic changes of the tumour.
4.3. Results
4.3.1. Histopathologic assessment and IHC markers
The median number of tumour slides available and reviewed per case was 4 (range 2-10).
Pathologic stages of the tumours were: 19 cases (53 %) stage IA (14 pT1a, 5 pT1b; N0), 9 (25 %) stage
IB (pT2aN0), 1 (3 %) stage IIA (pT2bN0), 6 (16 %) stage IIB (3 pT2bN1, 3 pT3N0), 1 (3 %) stage IIIB
(pT3N1). Pleural (n=10), vascular (n=7) or lymphatic (n=1) invasion was observed in 36 % of cases.
Twenty-seven of the 36 cases were adenocarcinomas; these included nine (33%) non-mucinous with
lepidic predominant pattern and two (7%) mucinous with predominant lepidic pattern. Among the
remaining 16 adenocarcinomas, the predominant histological patterns were acinar in 11 and papillary in
5 (Table 4-1).
Tumours showed varying degrees of inflammatory cell infiltrates with 11 (31%) demonstrating
moderate to marked infiltration. Seven tumours showed prominent lymphocytic aggregates (Table 4-1)

105
and one tumour showed a marked eosinophilic infiltrate. The distribution of tumour cellularity and
percentages of tumour fibrosis and necrosis are shown in Figure 4-1. Intratumoural fibrosis was observed
in 53% of the cases, with the mean area of fibrosis being 16% (range 0-100%). Thirteen (36%) cases
demonstrated tumour necrosis, but all involved less than 25% of the total tumour area. The mean tumour
cellularity was 52% (range 5-95%).
For all IHC markers the medians of percent tumour cells stained (range) were: Ki-67
proliferative index 26.7% (1-76%), Met 1.1% (0-60%), E-cadherin 70.8% (10-95%), vimentin 0% (0-
15%), and Snail 0.3% (0-70%) (Figure 4-1).
4.3.2. Association of adenocarcinoma growth patterns with molecular markers of response to
EGFR TKIs
The six cases with EGFR TKD mutations were adenocarcinomas. EGFR TKD mutations were
present in a significantly higher proportion of tumours with non-mucinous lepidic predominant histology
(56%) (Table 4-2). Seven out of 9 (78%) non-mucinous adenocarcinomas with lepidic predominant
pattern demonstrated EGFR high polysomy while EGFR amplification was found mainly in
adenocarcinomas with papillary/acinar predominant patterns, and not in those with a lepidic predominant
pattern. In contrast, KRAS mutations were found in all patterns of adenocarcinoma. The two cases of
mucinous adenocarcinoma with lepidic pattern did not harbour aberrations in any of the molecular
markers tested (Table 4-2).

106
Table 4-1. Histopathologic features and changes observed in clinical stage I NSCLC surgical
specimens after preoperative gefitinib treatment.
Tumours and features Frequency Squamous cell carcinoma 7 Large cell carcinoma 1 Adenosquamous carcinoma 1 Adenocarcinomas 27 Well differentiated 12 Moderately differentiated 12 Poorly differentiated 3 Non-mucinous predominantly lepidic 9 Mucinous predominantly lepidic 2 Predominant papillary pattern 5 Predominant acinar pattern 11 All cases 36 Intra-/peri-tumoral inflammatory cell infiltrate Minimal - mild 25 Moderate - severe 11 Lymphocytic aggregates 7 Fibrosis 19 Necrosis 13

107
Figure 4-1. Distribution of tumour histopathological features among early stage NSCLC patients
treated with neoadjuvant gefitinib.

108
Table 4-2. Correlation between predominant histological patterns of adenocarcinoma and
molecular markers.
N PR EGFR FISH+
EGFR amplification
KRAS mutation
EGFR TKD mutation
Total number
27 4 (15%) 18 (69%) 4 (15%) 6 (22%) 6 (22%)
Mucinous lepidic
2 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%)
Non-mucinous lepidic
9 2 (22%) 7 (78%) 0 (0%) 1 (11%) 5 (56%)*
Acinar
11 1 (9%) 8 (73%) 2 (18%) 3 (27%) 1 (9%)
Papillary 5 1 (20%) 3 (60%) 2 (40%) 2 (40%) 0 (0%) *p=0.031

109
4.3.3. Histopathological features in adenocarcinomas with EGFR TKD mutations
Four of the six adenocarcinomas with EGFR TKD mutation harboured an exon 19 deletion. Two
of these fulfilled the criteria of radiological PR according to the RECIST criteria (355). The other two
cases demonstrated 10% and 27% reduction in tumour diameter, which did not reach the RECIST criteria
level for PR. All four tumours demonstrated extensive central fibrosis with marked loss of cellularity
(Figure 4-2, A-C and D-F). Residual viable tumour cells were present focally within the fibrous stroma
and particularly in areas with marked lymphocytic infiltrates (Figure 4-2, F and H). Residual tumour
cells demonstrated low proliferative activity (Ki-67 staining) in the fibrous areas (Figure 4-2, D) and
high activity in lymphocyte rich areas (Figure 4-2, J). One adenocarcinoma with radiological PR and
harbouring an exon 21 L858R demonstrated lepidic predominant histology (Figure 4-2, J) with tumour
cells showing a low cuboidal appearance (Figure 4-2, K). This tumour also showed a focal area of
collapse with alveolar haemorrhage. A tumour with exon 21 L833V/H835L mutation did not respond to
gefitinib treatment; this tumour also showed a non-mucinous lepidic predominant histology but with
marked lymphocytic infiltration of the alveolar interstitium.

110
Figure 4-2. Histology of four tumors associated with partial response to gefitinib.
A-C: An Exon 19 L747_P752 deletion tumor shows fibrosis with extensive loss of tumor cells (A) and
focal residual viable tumor cells (B) with low proliferative activity (C).
D-F: An Exon 19 E746_S750insV tumor shows focal intense lymphocytic infiltrates (D), prominent
fibrosis (E) and focal residual viable tumor cells (F).
G-I: An EGFR wild type but amplified tumor shows large areas of tumor cell loss and fibrosis (G) and
areas with marked lymphocytic infiltration (G, H) and foci of residual highly proliferative tumor cells (I)
within in.
J-K: An exon 21 L858R mutant tumor shows a predominant lepidic growth pattern (J) with low cuboidal
tumor cells growing along the pre-existing alveolar framework (K).
L: An exon 21 L833V/H835L tumor not responsive to gefitinib shows a predominantly lepidic pattern
and prominent stromal lymphocytic infiltrate.

111
4.3.4. Association of EGFR TKD mutant adenocarcinomas with histopathological features and
IHC markers
The histopathological features observed in the adenocarcinoma cases with EGFR TKD mutations
were compared with the rest of the cohort. A moderate to severe inflammatory response was observed in
one EGFR TKD mutant adenocarcinoma (17%) but 4 (19%) and 6 (67%) of non-mutant
adenocarcinomas and non-adenocarcinoma tumours, respectively, also presented this type of response.
Although EGFR TKD mutant adenocarcinomas showed extensive fibrotic changes (mean: 32.8%
of tumour area), this was not significantly different from EGFR wild type adenocarcinomas (19.88%) or
non-adenocarcinoma tumours (7.48 %) (Figure 4-3). In contrast, EGFR TKD mutant adenocarcinomas
cases demonstrated significantly lower cellularity (mean: 24.17 % of tumour area) and Ki-67
proliferative index (mean: 4.61%) compared to EGFR wild type adenocarcinomas (cellularity: 58.57%,
p=0.01; Ki-67: 31.43%, p=0.002) and non-adenocarcinoma tumours (cellularity: 55%, p=0.026; Ki-67:
49.81%, p=0.001).
Met membrane staining levels were low in all groups, with no significant differences detected
between adenocarcinomas with EGFR TKD mutation (2.53 %o of tumour cells), EGFR wild type (7.88
%) or non-adenocarcinomas (1.83 %) tumours (Figure 4-3). In contrast, E-cadherin levels were
significantly higher in EGFR TKD mutant adenocarcinomas (70.44 % of tumour cells) compared to non-
adenocarcinoma tumours (44.4%, p=0.026), but were similar when compared to EGFR wild type
adenocarcinomas (64 %) (Figure 4-3). Vimentin and Snail levels were low in all groups with the only
significant difference was observed in Snail staining between EGFR TKD mutant ADC (0.6%) and non-
ADC tumors (2.7%) probably due to a single outlier in the last group (70% of tumor cells positive for
Snail).
4.3.5. Correlation of histopathological features and IHC markers with clinical response
Among the histopathological features, gefitinib response assessed by radiologic tumour diameter
reduction was significantly associated with non-mucinous lepidic predominant pattern, higher tumour
grade and lower tumour cellularity (Table 4-3). Among IHC markers, only low proliferative index (Ki-
67) was significantly associated with radiologic response to pre-operative gefitinib therapy. Radiologic
response did not correlate significantly with either acinar or papillary growth patterns in
adenocarcinomas, extent of tumour fibrosis, inflammatory response or tumour necrosis.

112
Figure 4-3. Association between histopathological features and immunohistochemical markers
with adenocarcinoma genotypes.

113
Table 4-3. Correlation of histopathological features of tumour and molecular markers with
percentage of change in maximum tumour diameter on CT scans before and after gefitinib
treatment
Characteristic R2 ß (SE) p BAC (NM pure and predominant)
0.200 -4.588(1.6) 0.007 Acinar component 0.013 1.076(1.65) 0.52 Papillary component 0.044 3.035(2.46) 0.227 Differentiation grade 0.166 9.684(3.77) 0.015 Inflammatory response 0.005 1.657(3.98) 0.68 Lymphocytic aggregate 0.05 -9.964(7.53) 0.195 Fibrosis % 0.07 -0.197(0.125) 0.125 Necrosis % 0.109 0.904(0.45) 0.053 Cellularity % 0.217 0.31(0.102) 0.005 Ki-67 index 0.152 0.289(0.119) 0.02 Met membranous staining 0.024 0.242(0.27) 0.375 E-cadherin membranous staining 0.057 -0.17(0.12) 0.167 Vimentin cytoplasmic staining 0 0.005(1.11) 0.997 Snail nuclear staining 0.047 0.328(0.258) 0.213 R2= coefficient of determination (proportion of the variation explained by the model); ß (SE)=
standardized coefficient (Relative importance of the contribution of the predictor to the model. Negative
value means larger the predictor, larger tumour reduction; positive value means larger the predictor,
larger tumour growth).

114
4.4. Discussion
It is well established that EGFR TKI therapy can induce dramatic tumour shrinkage in a NSCLC
subpopulation mainly defined by the presence of EGFR TKD mutations, but the histological correlates of
this response have not been previously described. This is because EGFR TKIs have been used primarily
to treat advanced NSCLC patients in whom histopathological evaluation of treated tumours is not
feasible since surgical resection is not part of their standard of care. Taking advantage of our neoadjuvant
trial we are able to assess the histopathological correlates of response in early NSCLC after EGFR TKI
therapy. Our results demonstrate that significant radiologic tumour response is observed mainly in non-
mucinous adenocarcinomas with lepidic-predominant growth pattern, which is also most often found in
tumours with EGFR TKD mutations. Radiological tumour reduction was associated with a decrease in
tumour cellularity and proliferation (Ki-67 index), but not with other factors evaluated, including acinar
or papillary histology, inflammatory infiltration, fibrosis, and markers of EMT phenotype
(Met/hepatocyte growth factor receptor, E-cadherin, vimentin and Snail).
Previous reports have documented the histological features found in adenocarcinomas that are
more commonly associated with EGFR TKD mutations in untreated tumours. These include low grade
(well/moderate) and tumours with prominent lepidic (previously called BAC pattern) and/or papillary or
micropapillary growth patterns (359) (390) (391) (171). These histological patterns have also been
associated with higher response rate to EGFR TKI therapy (154) (278) (392). However, other reports
have not found significant associations of these or other specific histological patterns with EGFR TKD
mutations (393) (168) (394). In our small series, 5 of 6 (83%) EGFR TKD mutant adenocarcinomas were
non-mucinous with a predominant lepidic pattern, while the sixth tumour had a predominant acinar
pattern. With one-quarter of our cohort being adenocarcinomas with lepidic predominant pattern, the
prevalence of EGFR TKD mutations in this adenocarcinoma subtype accounts for their association with
clinical response.
One of the most important aspects of this report is the description of histopathological changes in
tumours showing significant clinical response to gefitinib therapy. These tumours were characterized by
extensive fibrosis and loss of tumour cells. However, there was no significant association between the
extent of fibrotic changes and clinical response. This discrepancy is likely due to the difficulty in
distinguishing between treatment and non-treatment related fibrosis, as focal fibrosis occurs commonly
during cancer development (395). Among responding tumours, residual viable tumour cells were noted
most commonly in areas with marked lymphocytic infiltrate. However, this tumour response was not
exclusive of adenocarcinomas harbouring EGFR TKD mutations as it was also noticed in other
histologies. Nevertheless, this observation warrants further study, as it may raise the possibility that
tumour cell viability might be supported in a tumour microenvironment with high cytokine levels

115
secreted by the inflammatory cells (396) (397) (398). Response to gefitinib was, however, significantly
associated with low tumour cellularity and a low proliferative index. Not surprisingly, significantly lower
tumour cellularity and proliferative index were also found in adenocarcinomas harbouring EGFR TKD
mutations. These findings are in keeping with previous reports indicating that EGFR TKI therapy
reduces cellular proliferation in advanced NSCLC (399) (400).
Because EMT is a potential marker of resistance to EGFR TKI therapy, we assessed the
expression of various markers of EMT in our cohort. Met gene amplification has been identified as
potential predictor of resistance to EGFR TKI in different advanced NSCLC cohorts (389) (401), but in
our cohort of early NSCLC, we found uniformly low expression of Met with no association of Met
protein expression with radiologic response to therapy. E-cadherin expression was significantly higher in
EGFR TKD mutant adenocarcinomas compared with non-adenocarcinomas cases but not when
compared with EGFR TKD wild-type adenocarcinomas. Taken together with the lack of differences in
expression of other EMT markers, this suggests variability of expression between histologic NSCLC
subtypes, rather than variation based on genotypic differences between adenocarcinoma tumours.
Despite limited by a lack of corresponding pre-treatment data, this study is to the best of our
knowledge the first to report the specific histopathological findings in NSCLC, particularly in EGFR
TKD mutant adenocarcinomas, demonstrating clinical response to treatment with an EGFR TKI. This
assessment was enabled by the unique design of our neoadjuvant study, suggesting that similar designs
may offer important opportunities for future studies aiming to correlate clinical response,
histopathological changes, biomarker expression, and novel functional imaging modalities. This will lead
to a better understanding of the tumour response to targeted therapies.

116
Chapter 5
Neoadjuvant gefitinib in early stage
NSCLC: association of changes in
phosphorylation of EGFR and its
downstream signal transducers with
clinical and histopathological response

117
5.1. Abstract
By using paired biopsy/tumour samples collected before and after 4 weeks of gefitinib during
our phase II clinical trial we investigated whether molecular response to gefitinib was associated with
clinical and histological response as well as predictive molecular markers. pEGFR Y1068 and Y1173 as
well as Akt, pAkt Ser473, pAkt Thr308, Erk 1/2 and pErk 1/2 Thr202/Y204 were evaluated by IHC
using specific antibodies in paired pre/post frozen tumour specimens from 23 cases. Less than half the
cases showed a reduction in pEGFR at the Y1173 residue while at Y1068, 70% showed a significant
reduction (p=0.011); changes in these two pEGFR were not concordant. Although a decrease in pErk
was significant (86% of cases, p=0.001) total Erk was also decreased (78% of cases, p=0.002). Reduction
in pErk T202/Y204/Erk ratio was not associated with response. Gefitinib decreased both pAkt Ser473
(65% cases, p=0.068) and Thr308 (73% cases, p<0.001). EGFR TKD mutant cases demonstrated
reduction in pAkt Thr308/Akt and pAkt Ser473/Akt ratios but changes in pAkt/Akt ratios were not
associated with response. Surprisingly, reduction in pEGFR Y1068 was significantly associated with
greater tumour cellularity (p=0.047), increased Ki-67 index (p=0.018) and clinical response (p=0.019).
There was no association with changes in pErk/Erk ratio with response to gefitinib. Changes in the
phosphorylation state at Y1173 did not correlate with tumour reduction. Although gefitinib reduced the
pAkt/Akt ratios, pEGFR Y1068 levels were inversely related to tumour response, suggesting the
mechanisms of action in humans are more complex than predicted by in vitro models.

118
5.2. Introduction
EGFR is a transmembrane tyrosine kinase receptor that is frequently expressed in various solid
malignancies including NSCLC (28) (132). Activation of the EGFR leads to autophosphorylation of
specific tyrosine residues in its intracellular domain. Two of these residues, Y1068 and Y1773, are
reported as relevant for its biological activity (40) (402). Different intracellular signalling pathways are
initiated after EGFR phosphorylation, Erk and PI3K/Akt being the two most important. EGFR induces
Erk 1/2 kinase activation via Ras and is responsible for cell proliferation. This pathway depends on
Y1173 phosphorylation. Akt is activated via either phospholipase C γ or PI3K and is involved in tumour
survival (403). Phosphorylation of Y1068 is critical for this latter pathway.
EGFR TKIs are established therapeutic options for advanced NSCLC patients (255) (275). In the
first line setting, the effectiveness of EGFR TKIs is limited to patients with EGFRT TK domain mutant
tumours (255) (169) (258). However, no biomarker has been established as predictive for differential
beneficial effect for EGFR TKIs against placebo or chemotherapy (275) (279) (283) (277). In the latter
settings, EGFR TKIs still elicited response and survival benefit in patients who are not likely to have
EGFR TK mutant tumours, such as squamous cell carcinoma or smokers (275). Therefore, a rationale
remains to investigate the mechanism of action and pharmacodynamics of EGFR TKIs activity in patient
tumours. The lack of surgical therapy offered to advanced NSCLC patients limits the in vivo assessment
of the inhibition of the EGFR pathway by EGFR TKIs. So far only attempts at predicting response based
on pre-treatment specimens have been attempted. Our phase II neoadjuvant trial has given us the
opportunity to assess the molecular response to EGFR TKIs in patients’ tumours directly by comparing
samples collected systematically prior to and after gefitinib treatment. Therefore, our objectives were to
assess the impact of gefitinib on the phosphorylation levels of the EGFR itself and its relevant
downstream signal transducers Erk and Akt, and to correlate these changes with clinical and molecular
predictors of response as well as the actual histological and clinical responses observed.
5.3. Results.
5.3.1. Cohort with paired pre/post gefitinib samples collection
Twenty-six patients (72% of the original trial population) underwent tumour core-needle biopsy
after an initial fine-needle cytologic diagnosis; the remaining patients did not undergo biopsy as they
were enrolled with an established tumours diagnosis or the radiologists who performed the biopsy felt
that a core procedure was too risky for the patient. Three cases did not show tumour cells in the core
specimen. Overall there were 23 evaluable cases with tumour cells in their core-needle biopsies, 64% of

119
the original trial population. All cases had post-gefitinib samples collected from surgically resected
tumours which were snap-frozen immediately. The median number of core needle and surgical
specimens analyzed were 2 for both but the range was wider for the latter (1 to 2 vs 1 to 8).
Clinical, histological, and molecular characteristics of the cohort with evaluable pre/post
gefitinib frozen samples are described in Table 5-1. No patients with mucinous tumours and only half of
the well differentiated adenocarcinomas were available and included in this analysis.
5.3.2. Changes and associations in phosphorylation-specific IHC evaluation
While three cases were negative for pEGFR Y1173 in their pre-gefitinib samples, 3 others were
negative at pEGFR Y1068. Changes in different cellular compartments after gefitinib were not uniform
with cytoplasmic perinuclear pEGFR Y1068 remaining stable (Figure 5-1). Overall, basal pEGFR
immunoscores were not significantly different, although pEGFR Y1068 showed higher levels than
pEGFR Y1173 (83.07 vs 56.18, p=0.361). After 4 weeks gefitinib therapy, less than half the cases
showed a reduction in pEGFR Y1173 immunoscore (Figure 5-2). At pEGFR Y1068, 70% showed
reduction (p=0.011). Changes in the phosphorylation status between these pEGFR tyrosine residues were
not significantly correlated as only 52% of cases were concordant (Table 5-2). The Erk, pErk T202/Y204
and pAkt Thr308 immunoscores presented a reduction in their respective levels in 78, 86 and 73 percent
of cases (p<0.05) (Figure 5-2). Although 56 % and 65 % of cases experienced reductions in Akt and
pAkt Ser473 levels, these changes were not significant. Since changes in both total Erk and Akt were
observed, ratios of phosphorylated to total protein immunoscores were calculated to account for these
changes. All but one case experiencing reduction in pEGFR Y1173 level also demonstrated a fall in pAkt
Thr308/Akt ratio (p=0.025); no other association between reduction in pEGFR and changes in other
intracellular signalling molecules were observed (Figure 5-3).

120
Table 5-1. Clinical, histological and molecular characteristics of the cohort and its proportion from
the entire trial population.
Characteristic N % of total trial population Clinical Female 11 61 Asian 2 67 Non-smokers 4 67 Histological Adenocarcinomas 18 67 Mucinous predominantly lepidic 0 0 Non-mucinous predominantly lepidic 7 78 Predominant acinar pattern 8 73 Predominant papillary pattern 3 60 Differentiation Poor 2 67 Moderate 10 83 Well 6 50 Molecular EGFR IHC+ 20 67 EGFR FISH+ 16 76 High polysomy 12 80 Amplification 4 67 EGFR TKD mutation 4 67 KRAS mutation 4 67

121
Figure 5-1. Example of p-EGFR Y1068 perinuclear staining observed and comparison of pre/post
p-EGFR Y1068 immunoscores from different cellular compartments.

122
Figure 5-2. Pre/post immunoscore values of pEGFR, Erk, pErk, Akt, and pAkt of tumour samples
before and after gefitinib treatment.

123
Table 5-2. Concordance of changes in EGFR phosphorylation levels at tyrosine residues 1068 and
1173 after gefitinib treatment.
pEGFR Y1068
increased no change decreased p
pEG
FR Y
1173
increased 4 (17%) 0 (0%) 6 (26%)
0.507 no change 0 (0%) 0 (0%) 2 (9%)
decreased 3 (13%) 0 (0%) 8 (35%)

124
Figure 5-3. Associations between changes in EGFR phosphorylation levels and ratios of
intracellular signalling molecules.

125
5.3.3. Associations of changes of phosphorylation state with clinical characteristics and histological
features associated with clinical response
Differences in immunoscores between different clinical groups associated with response to
EGFR TKIs were explored (Figure 5-4). Male patients experienced a larger decrease in pEGFR Y1068
score than their female counterparts (-54.42 vs -2.14; p=0.009). Also, Asian patients presented
significant reduction in their pAkt Thr308/Akt ratio level compared to patients of other ethnicity (-
292.55 vs -26.19; p=0.047). No other differences were observed in other immunoscores based on gender
or ethnicity; no significant differences were observed in changes in pEGFR, pAkt or pErk immunoscores
based on smoking history.
There were no significant differences between adenocarcinoma and other histologic types
(Figure 5-5). Poorly differentiated adenocarcinomas expressed a more significant reduction in their
pEGFR Y1173 immunoscore compared to moderately or well differentiated cases (-112.37 vs 0.87;
p=0.026). Overall, no histological subtype was significantly different than others in regards to
immunoscores.

126
Figure 5-4. Differences in EGFR, Erk, and Akt phosphorylation scores by clinical characteristics
of response.

127
Figure 5-5. Differences in EGFR, Erk, and Akt phosphorylation scores by histological
characteristics.

128
5.3.4. Associations with molecular predictors of clinical response
Associations of changes in immunoscores with the established molecular predictors of response
to EGFR TKIs were explored (Table 5-3). No correlation between EGFR FISH status and change in
pEGFR Y1173 was observed. Nine out of 10 cases (90%) demonstrating an increase in pEGFR at Y1173
were EGFR FISH+ (high EGFR gene copy number) but 6 out of 11 cases (55%) with reduction in
pEGFR Y1173 were also EGFR FISH+. Most of EGFR FISH+ cases expressed a reduction in pErk/Erk
(50% of FISH+ cases), pAkt Ser473/Akt (62%), and pAkt Thr308/Akt (75%) but none of these
differences were significant. Interestingly, more cases with EGFR TKD mutations expressed an increase
in pEGFR Y1068 (75% vs 21% of EGFR TKD wild type cases) after gefitinib treatment but this was not
statistically significant. All cases with EGFR TKD mutation demonstrated reduction in pAkt Thr308/Akt
and pAkt Ser 473/Akt but only the last association was significant.
Further analysis of changes in phospho-specific immunoscores by tumour genotype showed that
EGFR TKD mutant adenocarcinomas experienced a significant reduction in pAkt Thr308 (Figure 5-6).
Adenocarcinomas harbouring EGFR TKD mutations presented a mean reduction in pAktThr308/Akt
ratio of -205.99 (±275.59), immunoscore that was significantly different compared against
adenocarcinomas with EGFR TKD wild type (-22.21, ±101.04; p= 0.035) and also non-adenocarcinoma
cases (-0.03, ±0.48; p=0.016). However, significant reductions in pEGFR immunoscores were not
observed in adenocarcinomas with EGFR TKD mutations (Figure 5-6). Changes in pErk/Erk and pAkt
Ser473/Akt were also no significant.
5.3.5. Associations with histological features of response
Association of changes in immunoscores with percentage of change in tumour fibrosis,
cellularity and proliferative status post gefitinib are shown in Figure 5-7. Overall, there was no
significant relationship between tumour fibrosis and phosphorylation status. Tumours experiencing
reduction in pEGFR Y1068 showed a significantly greater tumour cellularity compared with those with
increase in pEGFR Y1068 (60.63% vs 37.86%; p=0.047). Changes in pEGFR Y1173, pErk/Erk and
pAkt/Akt ratios were not associated with any differences in cellularity. Cases with reduced pEGFR
Y1068 staining also had a significantly higher proliferative index (41.84% vs 17.43%; p=0.018). No
other phosphorylation staining was associated with proliferation index.

129
Table 5-3. Change in pEGFR, pErk, and pAkt immunoscores and molecular makers of response.
N EGFR IHC+ (n=20)
EGFR FISH+ (n=16)
EGFR Amplification+
(n=4)
KRAS mutation+
(n=4)
EGFR TKD mutation+
(n=4)
ΔpEGFR Y1068 decreased 16 13 (81%) 11 (69%) 2 (12%) 3 (19%) 1 (6%) no change 0 0 0 0 0 0 increased 7 7 (100%) 5 (71%) 2 (29%) 1 (14%) 3 (43%)
ΔpEGFR Y1173 decreased 11 9 (82%) 6 (55%) 2 (18%) 1 (9%) 2 (18%) no change 2 2(100%) 1 (50%) 0 2 (100%)* 0 increased 10 9 (90%) 9 (90%) 2 (20%) 1 (10%) 2 (20%)
ΔpErk T202Y204/Erk decreased 10 9 (90%) 8 (80%) 3 (30%) 2 (20%) 1 (10%) no change 0 0 0 0 0 0 increased 12 10 (83%) 7 (58%) 1 (8%) 2 (17%) 2 (17%)
ΔpAkt Ser473/Akt decreased 11 11 (100%) 10 (91%) 3 (27%) 0 4 (36%)* no change 0 0 0 0 0 0 increased 12 9 (75%) 6 (50%) 1 (8%) 4 (33%) 0
ΔpAkt Thr308/Akt decreased 17 14 (82%) 12 (71%) 3 (18%) 2 (12%) 4 (23%) no change 0 0 0 0 0 0 increased 6 6 (100%) 4 (67%) 1 (17%) 2 (33%) 0
* p<0.05

130
Figure 5-6. Differences in pEGFR, pErk, and pAkt immunoscores according to adenocarcinoma
genotypes

131
Figure 5-7. Differences in histopathological features of tumour response according to changes in EGFR, Erk, and Akt phosphorylation

132
5.3.6. Associations with clinical response
Of the 23 patients included, 10 (43%) experienced tumour reduction under gefitinib treatment,
including 3 (13%) reaching PR status by RECIST criteria. Associations with clinical response are shown
in Table 5-4 and Figure 5-7. Sixty percent of cases experiencing tumour reduction expressed an increase
in pEGFR Y1068 while nine out of ten growing tumours presented a decrease in pEGFR Y1068 after
gefitinib treatment (p=0.019). There was no relationship between changes in pEGFR Y1173 staining and
clinical response. All PR cases presented reduction in both pAkt/AKt rations (Table 5-4) and also
tumours with reduced pAkt Ser473/Akt ratio clustered to clinical response (Figure 5-7) but neither of
these associations were significant.

133
Table 5-4. Associations between changes in EGFR phosphorylation levels and ratios of
intracellular signalling molecules with clinical tumour response to gefitinib
N (%) Tumour Reduction (n=10)
PR (n=3)
N (%) p N (%) p ΔpEGFR Y1068 0.019 0.209 decreased 16 (70) 4 (25%) 1 (6%) increased 7 (30) 6 (86%) 2 (29%) ΔpEGFR Y1173 0.805 0.727 decreased 11 (48) 4 (36%) 2 (18%) no change 2 (9) 1 (50%) 0 increased 10 (43) 5 (50%) 1 (10%) ΔpErk T202Y204/Erk 1 1 decreased 10 (45.5) 4 (40%) 1 (10%) increased 12 (55.5) 5 (42%) 1 (8%) ΔpAkt Ser473/Akt 0.1 0.093 decreased 11 (48) 7 (64%) 3 (27%) increased 12 (52) 3 (25%) 0 (0%) ΔpAkt Thr308/Akt 0.66 0.539 decreased 17 (74) 8 (47%) 3 (18%) increased 6 (26) 2 (33%) 0 (0%)

134
Figure 5-8. Waterfall plots illustrating association of changes in (A) pEGFR Y1173, (B) pEGFR
Y1068, (C) pErk T202Y204/Erk ratio, (D) pAkt Ser473/Akt ratio, and (E) pAkt Thr 308/Akt ratio
with tumour size changes using CT imaging. The y axis indicates percentage of change in
maximum tumour diameter before and after neoadjuvant gefitinib treatment, bars represent
individual patients; r=reducing tumour, PR=partial response by RECIST criteria.

135
5.4. Discussion
The molecular assessment of response to EGFR TKIs in NSCLC has been limited to prediction
based on archival diagnostic biopsy or surgical specimens. By utilizing the uniqueness of the pre/post
gefitinib sample collection from our window of opportunity neoadjuvant trial in early NSCLC we have
been able to generate the first assessment of the molecular responses in patient tumours following EGFR
TKI therapy. Our findings indicate that gefitinib does not affect phosphorylation of EGFR tyrosine
residues equally, with significant changes at Y1068, but not Y1173, observed. pErk Thr202/Tyr204,
pAkt Thr308 and pAkt Ser473 all decreased after 4 weeks of gefitinib treatment. More importantly,
while tumour reduction tended to correspond to reduction in Akt phosphorylation (at Ser473), decrease
in pEGFR Y1068 was surprisingly associated with tumour growth, increase cellularity and cell
proliferation.
Despite the small sample size inherent in phase II trial design, three important points are
suggested by this analysis. First, although Erk phosphorylation at Thr202/Tyr204 is significantly reduced
by gefitinib, this is not associated with tumour response. This may be explained by the differences
observed in total Erk, as less than half of cases experienced a reduction in the pErk/Erk ratio. Other
studies have reported that changes in Erk phosphorylation are not associated with response to EGFR
TKIs. For example, cells with EGFR TKD mutations lack constitutive Erk Thr202/Tyr204
phosphorylation and EGF-induced phosphorylation level is lower than in wild-type cells (157) (404).
Also, gefitinib is able to reverse only EGF-induced but not constitutive Erk phosphorylation.
Proliferation of EGFR TKD mutant cells seems not to be driven by Erk signaling (218) (405). These
observations were confirmed in our trial, with adenocarcinomas harbouring EGFR TKD mutations
presenting no significant differences in pErk Thr202Y204/Erk ratio in a comparison against other cases.
This has been supported in other clinical settings where there was either no or a negative association with
pErk levels and EGFR TKD mutation status (306) (406) (407). Therefore, at least for EGFR TKD mutant
tumours, inhibition of phosphorylation of Erk Thr202/Tyr204 is not important for the clinical response
seen with gefitinib in vivo.
Secondly, gefitinib treatment resulted in reduction in phosphorylation of Akt at both tyrosine
residues, Ser473 and Thr308, with all EGFR TKD mutant cases and those reaching PR by RECIST
criteria experiencing these changes. Akt dephosphorylation observed in EGFR TKD mutants might be
explained by their particular differences in activation of intracellular pathways. EGFR TKD mutations
demonstrate both higher constitutive and EGF-induced phosphorylation of Akt at Ser473 compared to
wild type cells (157) (407) (408) (409). This has also been observed in clinical samples of surgically
treated patients, where the presence of EGFR TKD mutations was significantly associated with high
pAkt levels (306) (406). Therefore, EGFR TKD mutations may signal preferentially through the Akt

136
pathway which may explain the response induced by gefitinib in their presence. In fact, EGFR TKIs
reverse the phosphorylation of both constitutive and activated Akt in cells harbouring EGFR TKD
mutations (408) (410) (411). The contrary has been observed in resistant cells, with neither constitutive
nor EGF-induced Akt phosphorylation affected by gefitinib (404) (410) (411) (412). However, Akt
phosphorylation was also reduced in tumours growing during gefitinib treatment. This is in consistent
with the ISEL trial in which, although response rates between gefitinib and placebo were slightly higher
in pAkt IHC-positive compared to pAkt IHC-negative patients (pAkt IHC-positive: 10.1% with gefitinib
vs 2.5% with placebo; pAkt IHC-negative: 6.3% with gefitinib vs 0% with placebo), no significant
correlation between pAkt status and time to progression or survival were observed (278). Therefore,
although Akt phosphorylation is reduced during treatment with gefitinib, this is not sufficient to explain
the differences in response observed between cases.
Finally, gefitinib treatment did not affect all EGFR phosphorylation sites equally, with changes
between Y1068 and Y1173 being concordant in only half of cases. Also only decreases in Y1068
phosphorylation was seen in significantly more than half of cases. These results are somewhat surprising
considering those obtained from EGF or TGF-alpha stimulated A431 cells with treatment by EGFR
TKIs, where only the phosphorylation status at Y1173 showed sensitivity to TKIs and the Y1068 site
continued to be phosphorylated even at high inhibitor concentrations (413). However, our cohort
includes patients with EGFR TKD mutations. As A431 cells are EGFR TKD wild-type this may partially
explain the difference with our results. Using computer-based simulation, Liu et al determined that
L585R mutation should show an increase and decrease, respectively, of the phosphorylation in Y1068
and Y1173 compared to the wild-type receptor (414). This was confirmed in cell lines, with EGFR TKD
mutants showing higher Y1068 levels (157) (415). Furthermore, in other reports, both the constitutive
and EGF-induced phosphorylation of EGFR at Y1068 was reduced by gefitinib in both EGFR TKD
mutant and wild type cells (408) (410). Therefore, these basal differences between EGFR TKD mutant
and wild type cases may explain the higher basal immunoscores and why gefitinib may induce a more
significant reduction in Y1068 than Y1173. Nevertheless, reduction in pEGFR Y1068 score was not
associated with EGFR TKD mutations, indicating that this not may the explanation of the ultimate
difference between clinically responding and resisting cases. In fact, a rather contrary observation in
pEGFR Y1068 score was observed.
Most surprising was the association of reduced phosphorylation at the EGFR Y1068 site with
tumour growth, higher cellularity, and cell proliferation. Although this finding may contradict the
expected mechanism of action of gefitinib, particular biological processes affecting Y1068 may elucidate
this observation. The Y1068 functions as docking site for Grb2, allowing recruitment of Cbl and
inducing EGFR ubiquitylation at the plasma membrane, essential steps for clathrin-dependent EGFR

137
internalization into coated pits (416). In fact, Grb2-SOS-mediated signalling has been observed as
inactive in gefitinib resistant cells (417). Hence, reduced phosphorylation at Y1068 could potentially
interfere with receptor internalization and degradation and paradoxically increase EGFR-mediated
signalling. However, other reports have suggested that gefitinib does not affect receptor internalization,
indicating that another mechanism may explain the association between change in Y1068 and tumour
response (418). In this regards, a particular EGFR activation mechanism may explain it.
EGFR is localized in the cell membrane in lipid rafts, with basal tyrosine kinase activity
minimal, until activated by the binding of ligands (419). However, ligand-independent EGFR activation
due to UV radiation, oxygen radicals, TNF-alpha, IL-1 and cholesterol depletion do not follow usual
endocytic pathway (420) (421). Instead, EGFR gets internalized independently of ligand-binding and
ubiquitination (422). Lipid raft disruption induces a weak EGFR phosphorylation on Y1068, followed by
delayed internalization, clathrin-dependent endocytosis, and localization in perinuclear vesicles. Under
these conditions EGFR gets concentrated in endosomes in a cytoplasmic punctuate pattern, resulting in
either receptor recycling to the cell surface or arresting in intracellular vesicles. This is in accordance
with the staining pattern observed here, with only perinuclear but not pEGFR Y1068 cytoplasmic
staining remaining stable after gefitinib treatment. Also, evidence suggests that this internalized EGFR is
not dormant as it may continue to be active. At endosomes, several EGFR downstream signalling
partners such as Grb2, Shc and mSOS are also localized shortly after EGFR internalization (422). This
delayed internalization, and partial EGFR Y1068 phosphorylation, is controlled by p38 MAPK activity
with phosphorylation of Akt Ser473 undergoing transient decreases but cell survival and proliferation
remaining unchanged (420). In fact, this particular EGFR activation has already been described in cancer
cells under stress conditions (421) (422). Therefore, delayed EGFR internalization induced by ligand-
independent mechanisms may be the explanation of the reduction in pEGFR Y1068 but maintained
perinuclear localization and association with resistance to therapy. Further characterization of this
particular observation is necessary in order to elucidate the association between EGFR Y1068
dephosphorylation and tumour resistance to gefitinib.
A question may be raised due to the validity of the immunostainings reported here as a reflection
of the status, in particular phosphorylation, of the transmembrane receptor and intracellular molecules. It
is well known that Abs used in IHC need to be validated across various applications in order to ensure
specificity, sensibility, and lack of cross-reactivity. Nevertheless, information regarding validation of
antibodies employed here can be found on their providers’ websites. Also, different investigators have
reported the use of these Abs, confirming their specificity, sensibility, modification in response to EGFR
TKI, and validity on different platforms (423) (424) (425) (426) (427) (428). Furthermore, our group has
employed these clones in different reports with anteriority, following standard procedures, and confirmed

138
their value in several platforms using clinical specimens, tumour xenografts and cell cultures (328) (429)
(430). Finally, a negative control section was always processed in parallel during immunostainings.
Therefore, we are confident that our results employing immunostainings are reflect of the real status of
tumour sample analyzed.
These results should be interpreted as hypothesis-generating as the lack of samples derived from
a control arm makes it difficult to interpret them. However, we have been able to assess systematically
the molecular response to EGFR TKIs in vivo. Our results confirm that NSCLC response induced by
gefitinib is associated with reduction in Akt but not Erk phosphorylation. Tumour progression during
gefitinib treatment was observed with reduction in pEGFR Y1068, supporting further assessment of the
mechanism of EGFR activity in human trials.

139
Chapter 6
EGFR expression in NSCLC:
Intratumoral heterogeneity and effect of
ischemia

140
6.1. Abstract
EGFR protein expression assessed by IHC has been widely used in selecting patients for EGFR
TKI therapy. However, although potentially it is the most common biomarker explored in randomized
trials of anti-EGFR strategies in NSCLC, EGFR IHC has failed to predict response consistently. Among
others, two factors that may potentially affect the EGFR protein assessment by IHC are an intratumoral
heterogeneous presence as well as ischemic time derived from tissue processing. Therefore the
hypotheses of this study were to assess if EGFR is heterogeneously expressed in NSCLC, and if its
expression evaluated by IHC gets altered by ischemic time derived from tissue processing. Tumour
samples were collected from 40 NSCLC resected specimens. Representative samples from each quadrant
were formalin fixed at the same time and three additional samples from one quadrant were collected and
fixed at 15 minutes intervals. Samples were processed and sections stained for EGFR. Percentage of cells
stained, intensities and patterns from each cellular compartment were assessed. Also, time to fixation
was recorded for samples derived from the neo-adjuvant gefitinib clinical trial. We found that EGFR is
heterogeneously expressed on NSCLC. After correlation and principal component analyses three
tumoral membranous, two cytoplasmic and two stromal patterns measures represented up to 82% of the
variance observed. An average of two and three sections encompassed between 68 to 75% and 86 to 89%
respectively of the variance between patients among patterns analyzed. Membrane staining showed
intratumoral variance even when sections from different quadrants were averaged (6.4% to 0.5 %). The
cytoplasmic compartment did not show important intratumoral heterogeneity. Membrane and
cytoplasmic compartment were stable during ischemia. Analysis of samples from the clinical trial
showed no indication of change under ischemia and a better correlation with clinical response from
cytoplasmic staining. We concluded that two to three samples are necessary to properly assess EGFR
IHC expression in NSCLC. The small intratumoral heterogeneity, stability under ischemia and
correlation with clinical response support further assessment of the role of cytoplasmic EGFR staining in
EGFR TKIs treatment.

141
6.2. Introduction
Targeted agents against EGFR are a major therapeutic option against NSCLC. EGFR TKIs are
currently recommended as a second and third –line agents in patients with advanced disease (275).
Protein expression assessment by IHC is a practical assay routinely used in clinical practice. By IHC,
EGFR can be roughly quantified and its cellular localization identified. However, in randomized trials of
NSCLC patients undergoing EGFR TKIs therapy, EGFR IHC has failed to predict survival in all (257)
(276) (277) (281) but one trial (278). Furthermore, in two recent meta-analyses, EGFR IHC has not
shown to have predictive value due to wide variability in its positive predictive value (431) (432). In
these studies, EGFR IHC was assessed using a single slide per patient without a standardized processing
methodology from those with available tissue, raising the concern that EGFR tumour status was not
adequately represented.
At the Molecular Assays in NSCLC Working Group it was recommended that at least 3 areas per
tumour section should be assessed due to EGFR heterogeneity (339). However, this number was based
on consensus but a formal assessment of the EGFR tumour heterogeneity was not performed. Also,
results derived from cell culture experiments indicate that hypoxic conditions raise EGFR expression
suggesting that EGFR status could potentially be modified by ischemic time derived from tissue
processing (346) (348) (349) (350) (347).
Based on these questions, and following a strict tissue processing protocol, the objectives of the
following study were to determine if EGFR IHC staining is heterogeneously expressed in surgically
resected NSCLC, the number of biopsies necessary to properly represent the intra-tumour variability of
tumour quadrants, to explore which intracellular compartment present the lowest heterogeneity and to
determine the influence of ischemic time in EGFR IHC expression.
6.3. Results
6.3.1. Differences in EGFR IHC patterns among tumour quadrants
Examples of staining patterns observed are described in Figure 6-1. Percentages and intensities
of stained tumour cells in the four tumour quadrants are represented in Figure 6-2. In an initial
assessment, the quantitative scoring between areas was highly variable. For example, 9 out of 10
adenocarcinomas and 8 out of 10 squamous-cell carcinomas had at least one quadrant with more than a
10% difference in membrane staining compared to the others. All 4 adenocarcinomas with at least one
negative quadrant for membrane staining presented some positive cells in the others; the same
discordance was seen in the 3 squamous cell carcinomas with at least one negative area. In regards to

142
cytoplasmic staining, 4 adenocarcinomas and 6 squamous-cell carcinomas showed a difference larger
than 10 % in one of their quadrants compared against the others. The 2 adenocarcinomas with a negative
area for cytoplasmic staining presented some staining in the others; none of the squamous-cell
carcinomas had negative cytoplasmic staining. With respect to staining intensities, 4 adenocarcinomas
and 2 squamous-cell carcinomas showed a difference of more than one level in at least one of their
quadrants.
6.3.2. Estimation of EGFR IHC representative patterns
In the scoring of EGFR IHC staining, it is possible to assess both the intensity of the staining as
well as the percentage of cells involved. Also several intracellular locations (staining patterns) for EGFR
IHC staining can be easily recognized. To address which of the parameters are independent of the others
and to understand the heterogeneity of different aspects of staining, detailed histological scoring of these
variables were recorded for all specimens. Several variables (percentages and intensities) were correlated
but only the percentage of complete and incomplete membrane staining, as well as diffuse, granular, and
perinuclear cytoplasmic staining patterns were significantly correlated with their intensity counterparts
(Tables 6-1 to 6-4). Because intensity grades appeared to be more reproducible than percentages, the
former were chosen for further analysis. Also, diffuse and granular cytoplasmic intensities were highly
inversely correlated and the former was therefore eliminated arbitrarily. Seven intensity variables
remained in the database and subsequent principal component analysis was implemented to further
recognize those properly explaining the total variance.
The principal component factor loadings and the importance of each intensity variable from
different compartments are reported in Table 6-5. Four eigenvalues accounted for almost 82% of total
variance. The larger and more separated coefficients in these 4 eigenvalues corresponded to intensity of
complete membrane, overall membrane, granular cytoplasmic and stroma stainings. These were grouped
with the three percentage variables remaining after the correlation analysis for further analysis.

143
Figure 6-1. Representative tumour samples expressing intraslide homogeneity (A) and
heterogeneity (B) for EGFR by IHC. Descriptive EGFR staining patterns observed including a
negative (C), a moderate incomplete membrane pattern with weak cytoplasmic staining (D), strong
complete membrane with strong diffuse cytoplasmic stainings (E and F), strong granular
perinuclear staining (G).

144
Figure 6-2. Description of percentages tumour cells and intensities of staining from membrane and cytoplasmic compartments observed in 4
different quadrants of tumours; patient 1-10 adenocarcinomas, patients 11-20 squamous-cell carcinomas.

145
Table 6-1. Correlations of percentages of positive tumour cells among different compartments and
patterns; underlined values represent significant correlation at p<0.05; * represents a strong
correlation with one variable been excluded for subsequent analysis.
Percentages
Membrane Cytoplasm Stroma
complete incomplete overall diffuse granular overall perinuclear
Membrane
complete -.366 .052 .59 .065 .148 -.164 .067
incomplete -.366 .052 .535 .107 .196 .096 -.124
overall .59 .535 .092 .152 -.065 .304 -.047
Cytoplasm
diffuse .052 .052 -.009 -.69 .029 .51 .023
granular .065 .107 .09 -.69 .106 .27 -.134
overall .148 .196 .115 .51 .27 .165 -.129
perinuclear -.164 .096 -.065 .029 .106 .165 -.116
Stroma .067 -.124 -.047 .023 -.134 -.129 -.116

146
Table 6-2. Correlations of percentages of positive tumour cells with intensities of staining among
different compartments and patterns; underlined values represent significant correlation at
p<0.05; * represents a strong correlation with one variable been excluded for subsequent analysis.
Percentages
Membrane Cytoplasm Stroma
complete incomplete overall diffuse granular overall perinuclear
Membrane
complete .977* -.583 -.086 .505 .008 -.107 .056 -.293
incomplete -.592 .054 .765* -.133 .298 .216 .152 -.04
overall .162 .335 .517 -.163 .264 .139 -.14 -.024
Cytoplasm
diffuse .018 .043 .036 .719* -.006 -.788* .072 .105
granular .036 .029 .103 -751* .171 .984* .045 -.06
overall .11 .114 .1 .237 .043 .148 .026 .088
perinuclear .139 -.288 -.19 -.01 .084 .102 -.055 .982*
Stroma -.025 -.089 -.153 .086 -.161 -.108 -.113 .27

147
Table 6-3. Correlations of intensities of positive tumour cells with percentages of positive tumour
cells among different compartments and patterns; underlined values represent significant
correlation at p<0.05; * represents a strong correlation and one variable was excluded for
subsequent analysis.
Intensities
Membrane Cytoplasm Stroma
complete incomplete overall diffuse granular overall perinuclear
Membrane
complete .977* -.592 .018 .335 .036 .11 -.025 -.288
incomplete -.583 .162 .765* .043 .029 .114 .139 -.089
overall .054 .505 .036 .517 .103 -.19 .237 -.153
Cytoplasm
diffuse -.086 .298 .264 .719* .1 -.751* -.01 .086
granular .008 -.133 -.163 -.788* .043 .984* .084 -.161
overall -.107 .216 .139 -.006 .171 .148 .102 -.108
perinuclear .152 -.293 -.14 .072 .045 .026 -.113 .982*
Stroma .056 -.04 -.024 .105 -.06 .088 -.055 .27

148
Table 6-4. Correlations of intensities of positive tumour cells among different compartments and
patterns; underlined values represent significant correlation at p<0.05; * represents a strong
correlation and one variable was excluded for subsequent analysis.
Intensities
Membrane Cytoplasm Stroma
complete incomplete overall diffuse granular overall perinuclear
Membrane
complete -.601 .041 .383 .01 .1 -.062 -.301
incomplete -.601 .214 .462 -.115 .166 .157 -.017
overall .383 .462 -.146 .332 -.139 .322 -.111
Cytoplasm
diffuse .041 .214 .332 -.784* .072 .45 .135
granular .01 -.115 -.146 -.784* .132 .044 -.14
overall .1 .166 .322 .132 .45 .037 .061
perinuclear .157 -.301 -.139 .072 .044 .037 -.147
Stroma -.062 -.017 -.111 .135 -.140 .061 -.147

149
Table 6-5. Principal component analysis of intensities values at different compartments;
underlying components were chosen for subsequent analyses. Percentages values did not add to the
model and were also included in subsequent analysis.
Initial Eigenvalues Component Total % of Variance Cumulative %
1 1.78 25.55 25.55
2 1.65 23.61 49.16
3 1.23 17.58 66.73
4 1.06 15.19 81.92 Pattern Matrix
Components 1 2 3 4 Membrane complete .189 .04 -.944 -.064 Membrane incomplete .673 .68 -.11 -.012 Membrane overall -.213 .937 -.074 -.084 Cytoplasm granular -.151 -.044 -.101 .878 Cytoplasm overall .578 .012 .623 .102 Perinuclear -.038 .496 .09 -.558 Stroma -.063 .125 -.012 .902

150
6.3.3. Assessment of the representative number of tumour samples
To represent the difference in dispersion around mean values for each variable, percentage of
change in variance from using the average of four samples was calculated for the use of one, two, or
three samples (Figure 6-3). Stroma characteristics showed the largest differences when using a single
sample with a range of 100 to 933 percent for intensity and 51 to 495 percent for percentage of stroma
staining. These differences continued to be present when two (233 % for intensity, 142.7% for
percentage) and three (73% for intensity, 42% for percentage) samples were averaged. Among other
variables, only the intensity of complete membrane staining (128% for two samples, 54.9% for 3)
showed large disparities. Due to these differences and the fact that the role of stroma in clinical response
to therapy has not been defined, stroma staining variables were excluded from further analysis.
Because clinically it is of value to measure the differences between patients, differences in the
variance explained by histology, inter-patient, intra-patient, and random variability were estimated
(Figure 6-4). Overall, it was necessary to use at least 2 areas of tumour for the variance of the inter-
patient component to reach between 68 to 76% of the total variance. Further addition of a third sample
increased the inter-patient component up to 89%. In regards to other components, histology did not play
a role in any of the variables but differences between areas did. Among variables addressing the
membrane compartment (complete membrane intensity, overall membrane intensity, overall membrane
percentage), differences between areas contributed part of the total variance when one (from 2.6 to 6.4
%), two (from1.2 to 2.9 %), and three (from 0.5 to 1.2 %) areas were used. In contrast, for the
cytoplasmic variables (intensity of granular pattern and overall cytoplasmic percentage) differences
between areas did not play a role, leaving total variance to be explained by differences among patients
and random effects.

151
Figure 6-3. Percentage of change on variance value compared to total variance from average of 4
areas for different EGFR IHC staining patterns. A) complete membrane intensity, B) overall
membrane intensity, C) overall membrane percentage, D) granular cytoplasm intensity, E) overall
cytoplasm percentage, F) stroma intensity, G) stroma percentage.

152
Figure 6-4. Variance component analysis indicating differences in variance for different EGFR
IHC staining patterns explained by patients and tumour areas using single quadrants and average
values of doublets, triplets and 4 areas. A) complete membrane intensity, B) overall membrane
intensity, C) overall membrane percentage, D) granular cytoplasm intensity, E) overall cytoplasm
percentage.

153
6.3.4. Effect of ischemic time in representative EGFR IHC patterns
In order to determine if the different EGFR IHC patterns maintain stability during ischemia,
changes in subsequent ischemic time points were analyzed (Figure 6-5 and Table 6-6). In regards to 3
measures of membrane staining (intensity of complete membrane, intensity of overall membrane and
percentage of overall membrane) 15%, 30%, and 40% of cases respectively presented values outside of
the initial 95% confidence interval based on the four time zero specimens. Furthermore, an overall
significant effect of ischemic time on the intensity of overall membrane staining was observed (Wilks’
Lambda=0.512, F=5.08, p=0.012, partial eta squared=0.488) with all subsequent time-points been
significantly different compared against baseline value. Also, although an effect was observed at 15
minutes (F=5.352, p=0.033, partial eta squared=0.221) compared against baseline, ischemia did not
affect the percentage of tumour cells presenting membrane staining in subsequent timepoints or overall
(Wilks’ Lambda=0.687, F=2.433, p=0.103, partial eta squared=0.313). Intensity of complete membrane
staining was not affected by ischemia (Wilks’ Lambda=0.847, F=0.961, F=0.435, partial eta
squared=0.153).
In 90% and 50% of cases, values observed in subsequent timepoints for cytoplasmic granular
intensity and percentages of overall cytoplasmic staining respectively were encompassed inside the 95 %
confidence interval of the initial values of the 4 areas. An effect was observed at 30 minutes (F=5.164,
p=0.036, partial eta squared=0.223) but the overall influence of ischemia on percentage of cytoplasmic
staining was not significant (Wilks’ Lambda=0.728, F=1.99, p=0.156, partial eta squared=0.272).
Granular cytoplasmic intensity of staining was also not affected by ischemia (Wilks’ Lambda=0.843,
F=0.996, p=0.420, partial eta squared=0.157). Ischemia did not show different effects between cell types.

154
Figure 6-5. Effect of ischemia on EGFR IHC staining patterns at 15 minutes intervals; T1
represents mean values from 4 tumour quadrants (bars 95% CI).

155
Table 6-6. Repeated measures general lineal model exploring the effect of ischemic time on
different representative EGFR IHC staining patterns.
Characteristic Wilk’s
Lambda F p
Partial eta
Squared
Intensity of complete membrane ischemia 0.847 0.961 0.435 0.153 0 vs 15 min 0.014 0.906 0.001 0 vs 30 min 2.399 0.139 0.118 0 vs 45 min 1.897 0.185 0.095 ischemia*histology 0.874 0.770 0.528 0.126 Intensity of overall membrane ischemia 0.512 5.080 0.012 0.488 0 vs 15 min 9.339 0.007 0.342 0 vs 30 min 9.226 0.007 0.339 0 vs 45 min 8.108 0.011 0.311 ischemia*histology 0.804 1.302 0.308 0.196 Percentage of overall membrane ischemia 0.687 2.433 0.103 0.313 0 vs 15 min 5.352 0.033 0.229 0 vs 30 min 1.555 0.228 0.080 0 vs 45 min 3.651 0.072 0.169 ischemia*histology 0.640 2.998 0.062 0.360 Intensity of granular cytoplasm ischemia 0.843 0.996 0.420 0.157 0 vs 15 min 0.068 0.797 0.004 0 vs 30 min 0.983 0.335 0.052 0 vs 45 min 2.039 0.170 0.102 ischemia*histology 0.990 0.055 0.982 0.010 Percentage of overall cytoplasm ischemia 0.728 1.994 0.156 0.272 0 vs 15 min 0.017 0.899 0.001 0 vs 30 min 5.164 0.036 0.223 0 vs 45 min 4.160 0.056 0.188 ischemia*histology 0.812 1.231 0.331 0.188

156
6.3.5. Association of representative EGFR IHC patterns with clinical response
Finally, in order to explore if ischemic time affected EGFR protein expression in our clinical
trial setting, two sets of paraffin blocks for each patient from the neoadjuvant gefitinib trial were stained
and percentage and intensity of staining patterns were correlated with time from ischemia until tissue
fixation (Figure 6-6). None of the different EGFR protein expression patterns correlated with ischemic
time indicating that EGFR protein expression is not altered by additional ischemia resulted from standard
tissue processing time. Subsequently, the potential clinical value of different EGFR staining patterns
using multiple tumour sites were explored (Table 6-7). Overall, none of the membrane staining patterns
associated with response adequately. However, while percentage of cytoplasmic staining did not predict
response, the intensity of staining from this compartment was inversely correlated with change on
tumour diameter.

157
Figure 6-6. Correlations between ischaemic time and EGFR expression at different cellular
compartments among two sets of samples from a neoadjuvant gefitinib in stage I NSCLC clinical
trial.

158
Table 6-7. Associations of different EGFR IHC expression patterns with percentage of change in
maximum tumour diameter on CT scans before and after gefitinib treatment.
Characteristic R2 ß (SE) p Percentage of complete membrane 0.004 0.085(0.226) 0.71 Intensity of complete membrane 0.022 2.867(3.298) 0.391 Percentage of incomplete membrane 0.018 -0.101(0.13) 0.446 Intensity of incomplete membrane 0.035 -4.807(4.42) 0.285 Percentage of overall membrane 0.006 -0.048(0.107) 0.657 Intensity of overall membrane 0.018 -3.487(4.493) 0.443 Percentage of cytoplasmic 0.012 -0.074(0.118) 0.534 Intensity of cytoplasmic 0.117 -9.418(4.509) 0.045

159
6.4. Discussion
Based on a detailed examination of staining patterns from different cellular compartments and
following a strict tissue processing and IHC protocol, we observed that EGFR is expressed
heterogeneously in NSCLC. We used quantitative analysis of the scoring of these staining patterns to
determine which ones were most reliable. Overall, the average of two samples encompassed between 68
to 75% of the variance observed between patients, improving to between 86 to 89 % when 3 samples
were used. Although membrane staining showed relatively small intratumoral heterogeneity, this was
still present even when averaging 3 separate tumour areas. Furthermore, overall membrane intensity was
affected significantly by ischemic time. In comparison, variance of two cytoplasmic staining patterns,
overall percentage and intensity of granular staining, were well represented with two samples and
showed overall stability during ischemic time. Furthermore, intensity of cytoplasmic staining was the
only averaged variable associated with the clinical response observed during our EGFR TKI neoadjuvant
regimen in early NSCLC.
Assessment of a potentially heterogeneous expression of a biomarker used for patient selection is
of significant clinical importance. Tumour heterogeneity has been observed among different IHC
markers used as predictors and/or prognostic instruments in different malignancies. For example, in
breast cancer, nuclear estrogen receptor, progesterone receptor, ki-67 and nuclear p53 have all been
reported to show intratumoral regional variation (433) (434) (435) (436) (437) (438) (334) (439) (440).
Her-2neu (C-erbB-2), a tyrosine kinase receptor against which targeted therapy has been developed, has
also been observed to be heterogeneous in different solid malignancies, including gastric
adenocarcinomas, ductal carcinoma in situ and invasive ductal carcinoma, affecting the final scoring of
tumour samples (333) (334). Therefore, intratumoral heterogeneity is an important factor to be
considered when a biomarker is used for prognostic evaluation or patient selection.
EGFR detected by IHC has shown a heterogeneous expression in colon adenocarcinomas (441),
head and neck carcinomas (442) (443), gastric adenocarcinomas (333) (332) and breast cancer (444).
Results obtained from this study indicate that EGFR is also heterogeneously expressed in NSCLC.
Heterogeneous presence of EGFR in NSCLC has been previously observed. Based on samples from 36
NSCLC cases, Ferrigan reported that EGFR is heterogeneous with only 28% of cases being completely
positive or negative (338). Among the remaining cases, 35% had at least one block completely negative
but the rest had some degree of expression. Also, in 131 NSCLC specimens Suzuki et al observed
intratumoral heterogeneity among positive tumours (336). Finally, at the Molecular Assays in NSCLC
Working Group, Dr. Wistuba reported that, in a total of 65 tumour sites obtained from 9 NSCLC cases,
42 scored as positive (H score>200), whereas 23 sites scored as negative (H score<200) (339). Our
observations are in concordance with these reports but the novelty of our results indicate that by

160
averaging two or three tumour samples from different quadrants, 68 to 89 % of the variance between
patients is encompassed, indicating that multiple tumour sites are necessary for an adequate
representation of the EGFR presence in NSCLC.
It is not clear why intensity of overall membrane staining was the only variable affected by
ischemia but a potential explanation may be the involvement of a particular receptor internalization
mechanism. EGFR is internalized in as early as 15 min under oxidative stress, such conditions as may
occur during pulmonary ischemia (118). However why only the overall membrane intensity was affected
remains obscure. The observation that cytoplasmic EGFR is stable during ischemia is consistent with
time-specific assays performed in cell lines. In osteosarcoma (346), breast (348), prostate (348),
squamous (349), and adenocarcinoma (347) cell lines, culture in hypoxic conditions increases EGFR
levels. However, this EGFR over-expression was transcriptionally (346) (349) or translationally (348)
regulated, being observed only after 8 hours of hypoxic culture. It is known that NSCLC are tumours
undergoing hypoxia (445) but as several hours of hypoxic conditions may be necessary to influence
EGFR expression, additional hypoxic time during tissue processing might not influence the immediate
postsurgical expression of EGFR in NSCLC.
In addition to the lack of variance among quadrants and being stable during ischemia,
cytoplasmic EGFR expression correlated with shrinkage of the tumour during preoperative gefitinib
therapy. However, a role for EGFR cytoplasmic staining is not well established. In a report derived from
185 cases of renal cell carcinoma overall and membrane EGFR intensities were not associated with poor
prognosis but cytoplasmic EGFR was associated with worse grade, stage, and a trend towards poor
prognosis (risk ratio 3.3, p=0.07) (446). On the other hand, in another report derived from biopsies of 63
patients, cytoplasmic EGFR was higher in normal tissues rather than in renal carcinoma (447). In
NSCLC, cytoplasmic staining with EGFR IHC has not been routinely reported. Only in one report of 172
NSCLC specimens, Richardson et al indicated that cytoplasmic EGFR expression was more predominant
than membrane staining (50% specimens for cytoplasmic vs 23% for membrane staining) but it did not
show prognostic value (448). Therefore, the clinical value of cytoplasmic EGFR staining is not clear but
its greater intratumoral homogeneity compared to the membrane compartment as well as its stability
during ischemia support further assessment of its value.
In addition to intratumoral heterogeneity, the nature of IHC creates several variables affecting its
reproducibility and quantitative value. Other potential factors needing to be controlled include duration
and type of fixation, storage, primary antibody, staining protocol, scoring system implemented and
tumour area biopsied (190) (442) (280) (449) (450) (191) (451) (339). Also, it is not clear if the
minimum, mean or maximum value derived from multiple samples should be used as a prognostic and/or
predictive marker of response (435).

161
Nevertheless, based on our results two to three tumour samples should be collected in order to
properly assess EGFR expression in NSCLC. This is in accordance with additional evidence that EGFR
has also presented heterogeneity at the gene copy and mutational level. In reports from adenocarcinoma
cases, EGFR amplification was also observed to be heterogeneous, associated with different cellular
subtypes (337) (340). Previously we reported that EGFR TKD mutations are also heterogeneous in
NSCLC (342). These observations have also been obtained by others with potential association with
response to EGFR TKIs (337) (344). This evidence, in addition to the recommendations made by the
Molecular Assays in NSCLC Working Group, supports our conclusions that a proper NSCLC EGFR
characterization should include 2 or even 3 separate samples with a report from all cellular
compartments, including cytoplasmic staining, for an adequate EGFR IHC assessment in NSCLC.

162
Chapter 7
Discussion and Future Directions

163
7.1. Discussion
7.1.1. EGFR TKI in the treatment of early NSCLC
Lung cancer is the leading cause of cancer-related deaths worldwide. NSCLC is the main lung
cancer subtype accounting for 85% of all cases and includes the histological subtypes squamous cell
carcinoma, adenocarcinoma and large cell carcinoma. In its early stage NSCLC is treated by surgical
resection with patients experiencing a survival of 58% to up to 73%. Therefore, room for improvement
remains and, therefore, the value of additional neoadjuvant or adjuvant regimens in surgically treated
early NSCLC patients has been assessed.
While adjuvant radiotherapy has shown to be detrimental two main chemotherapeutic options,
cisplatin or uracil-tegafur-based regimens, has improved survival of patients with stage I NSCLC but
only in those with large tumours (5) (7) (12) (17) (19) (20). However, long-term follow-up studies have
found that the beneficial effect of cisplatin regimens is lost or even deleterious after 5 years (13) (16).
Furthermore, because uracil-tegafur has only been used on Asia, its utility worldwide is still not
determined. Finally, the value of neoadjuvant cisplatin-based regimens is not clear for stage I (21) (22).
Moreover, not a single randomized trial has assessed a neoadjuvant regimen exclusively in clinical stage
I NSCLC.
In the present work we hypothesized that EGFR TKIs can be an important therapeutic tool for
the treatment of early NSCLC. Due to the beneficial effect obtained in advanced NSCLC patients, EGFR
TKIs are recently developed agents with potential benefits for patients with early disease. As
maintenance therapy following platinum-based chemotherapy in unresectable or metastatic NSCLC,
EGFR TKIs have been able to prolong survival (12 vs 11 months, HR:0.81, 95% CI 0.7-0.95, p=0.0088)
(259). Also, in Asian patients with advanced NSCLC, platinum-doublet regimen followed by gefitinib
induced a prolonged survival in those patients with adenocarcinoma (HR=0.79; 95% CI, 0.65-0.98; p=
0.03) (262). Finally, the BR.21 trial demonstrated that EGFR TKIs improve survival as second or third-
line therapy in patients with advanced NSCLC (OS: 6.7 vs. 4.7 months; p < 0.0001) (275). Therefore,
exploring the value of these agents in early NSCLC is warranted.
We implemented a neoadjuvant trial based on the assumption that this design provides the
advantages of a better patient compliance and drug delivery in addition of allowing in vivo assessment of
tumour response and tumour sample collection before and after EGFR TKI exposure. This phase II trial
established an original precedent as this is the first of its kind evaluating this type of agent in early
NSCLC. Results demonstrated that EGFR TKIs are well tolerated as a one month preoperative course,
having minimum adverse events or the necessity to suspend treatment. More importantly, this clinical
trial design allowed us to assess the in vivo clinical response by comparing tumour changes in CT scans

164
before and after a course of gefitinib. It is important to mention that, although it was not an objective of
this study, the results of the trial supported future implementation of this neoadjuvant design in exploring
the utility of other agents. Furthermore, this preoperative window did not alter the standard surgical
waiting time as patients were expecting to have their surgical resection between 4 to 6 weeks after first
visit to the surgical clinic. Therefore, a 4 weeks window treatment is a reasonable time for the assessment
of the response to agents under investigation. Also, the large number of tumour sample collection before
and after the preoperative window and the actual correlation with clinical response derived from the
paired CT scans allows an unique assessment of the response induced with actual changes suffered by
tumours been evaluated.
The present thesis establishes the first report of the use of an EGFR TKI for the treatment of
early NSCLC, establishing a feasible neoadjuvant regimen and inducing tumour regression in a patient
subpopulation. Furthermore, using this innovative clinical trial design, we found that tumours
experiencing clinical shrinkage demonstrated large amounts of fibrosis, lower cellularity as well as a low
proliferation. Moreover, we have been able to characterize for the first time the signalling pathways
modified by EGFR inhibition in vivo, observing that EGFR TKI-induced response in NSCLC may be
mediated through Akt pathway. More importantly, a novel finding was observed in patients experiencing
resistance to an EGFR TKI, with an altered receptor internalization mechanism being potentially
involved.
7.1.2. Analysis of the response induced by EGFR TKIs in the treatment of early NSCLC
As expected, not all patients experienced reduction in their tumour, with 43% experiencing some
degree of shrinkage and only 11% reaching PR status determined by RECIST criteria. Although the lack
of randomization makes analysis of OS not feasible, the objective of this trial was to evaluate if EGFR
TKIs are well tolerated and able to induce clinical response in early NSCLC. Although 43% of patients
experienced tumour growth and one patient experienced an increase in T status, this, in fact, was due to a
one millimetre tumour growth. Also, only 14% of the cohort was characterized as neither growing nor
shrinking tumours.
Using the advantage of our trial design, we were able to collect tumours samples exposed to
EGFR TKIs. Previous randomized trials have analyzed, when available, tumour samples before EGFR
TKI exposure in an effort to identify predictors of clinical response. As part of this work, we have been
able to generate the first report of the histopathological changes suffered by NSCLC treated with EGFR
TKIs and to correlate it with the degree of tumour shrinkage observed on CT scans. Our results suggest
that radiological tumour reduction induced by EGFR TKIs is correlated with lower cellularity. Also,

165
shrinking tumours demonstrated extensive tumour fibrosis. However, nests of surviving cells were
observed, surrounded by lymphocytic infiltrate and presenting low proliferation. These findings may
have various clinical implications.
The extensive fibrotic changes in addition to the lower cellularity imply a relevant clinical effect
of EGFR TKIs in NSCLC as it suggests that tumour cells are eliminated in vivo by gefitinib. The lack of
correlation between the extend of fibrosis and radiological tumour shrinkage should not be
misinterpreted as it has been observed before under other neoadjuvant regimens (452). In fact, extensive
fibrosis in advanced NSCLC induced by non-EGFR TKIs has also been observed in tumours
experiencing important tomographic reduction. We also observed this, with tumours reaching PR
presenting extensive tumour fibrosis and lower cellularity. Reduction in tumour cellularity is another
outcome obtained by non-EGFR TKIs neoadjuvant regiments, mainly analyzed in breast cancer studies
(453) (454). In these studies, earlier stage breast cancer was more likely to achieve complete
pathological response with residual disease not increasing risk for relapse. If this can be extrapolated to
early NSCLC, an adequate agent(s) should be able to achieve complete eradication of tumour cells using
a neoadjuvant regimen. Nevertheless, to observed extensive fibrosis and reduction in cellularity may
indicate and important result of the action of EGFR TKIs.
Despite this extensive pathological response, islets of tumour cells remained. These presented a
low proliferation status and were surrounded by lymphocytes. These observations suggest important
EGFR TKIs mechanisms of action. Reduction in Ki-67 index has been observed in consecutive biopsies
from skin and different solid malignancies including advanced NSCLC from patients treated with EGFR
TKIs (399) (455) (400). Here we confirmed that lower proliferation is another result of EGFR TKIs
treatment and, furthermore, it was related with degree of clinical response. While low ki-67 been related
to a better prognosis in early NSCLC, this effect may translate through to a prolonged OS (456) (457)
(458). On the other hand, the role of the lymphocytic infiltrate surrounding surviving tumour cells is not
clear. Studies using in vitro models have reported an increased leukocyte infiltration under anti-EGFR
Abs (396) (397) (398). This infiltration results in a cytokine-mediated, Ab-dependent cytoxicity. The
lack of the Ab component makes our observation unexpected with possibly having a contrary effect by
preserving tumour cell viability. Nevertheless, with these results, we expeculate that not only clinical
tumour shrinkage but loss in cellularity, fibrotic changes, and reduced tumour proliferation are the result
of treatment with EGFR TKIs.
7.1.3. Significance of the differences in EGFR inhibition in early NSCLC

166
Both, clinical and histopathological responses are expected to be the result of the inhibition of
the EGFR tyrosine kinase. By interacting with the EGFR at its ATP binding cleft, EGFR TKIs do not
allow the transfer of γ-phosphate group from the ATP to tyrosine residues within the cytoplasmic C-
terminal domain (34). With approximately 10 known tyrosine residues existing in the EGFR C-terminal
domain their phosphorylation should, in theory, be blocked homogenously by the action of an EGFR
TKI (36) (37). Here, we study changes in phosphorylation of two of the main tyrosine residues, Y1068
and Y1173, by analyzing samples obtained before and after gefitinib treatment (Figure 7.1). Overall,
Y1173 pre-gefitinib immunoscores were lower than those using anti-pEGFR Y1068. Also, not all
patients experienced reduction at these tyrosine residues. Finally, and unexpectedly, changes in Y1068
and Y1173 were not concordant. These observations are of high clinical importance. First,
heterogeneous EGFR tyrosine residues phosphorylation may be the reflection of different cellular
processes being taking place in early NSCLC but also they may either been originated of real differences
between patients or been a reflection of different cellular subtypes having different EGFR activation.
As expected from studies derived from cell lines, gefitinib caused inhibition of the Akt, but not
Erk, pathway. Interestingly, reductions in p-Akt/Akt ratios were observed not only among patients
experiencing clinical shrinkage but also those which demonstrated growth or resistance. However, a
novel finding was that, among patients not responding to gefitinib, reduction in overall pEGFR Y1068
immunoscore was observed but a specific pattern remained. In post-gefitinib samples derived from
patients demonstrating tumour growth a perinuclear granular pattern was observed, opening a new
explanation of a potential mechanism of differentiation between patients responding to or progressing on
EGFR TKI treatment. These observations confirm that EGFR TKIs are able to induce Akt
dephosphorylation in the majority of cases but the distinction between responders and resistant patients is
due, in fact, to a residual phosphorylated receptor, being trapped in a perinuclear compartment. This is in
accordance to observations made on cell line studies in which similar activated EGFR
compartmentalization has been observed in cellular under stress conditions (421) (422). In fact, these
cells experienced reduction in pAkt levels and are able to recover after stressor is removed (420).
Therefore, this observation of pEGFR Y1068 compartmentalization may be an indication of a novel in
vivo clinical mechanism of resistance.

167
Figure 7-1. Mechanism of response/resistance to gefitinib in early NSCLC.

168
7.1.4 The importance of heterogeneous expression and effects of ischemic time on biomarkers of
response to EGFR TKIs
In the current work we found that EGFR is expressed heterogeneously in early NSCLC,
necessitating the analysis of two to three tumours samples in order to properly represent the total tumour
expression of any cellular compartment. We also observed that the intensity of the staining of the
membrane compartment is affected by ischemia. Moreover, we observed that cytoplasmic staining
correlates with radiological shrinkage in our clinical trial. These observations support the notion that
multiple tumour samples are necessary to adequately represent EGFR in early NSCLC, and give support
of further assessment of the value of cytoplasmic compartment in the response to EGFR TKIs.
EGFR TKD mutation was the molecular marker best associated with clinical response, present in
three out of four PR patients. We also examined several histological characteristics and searched for an
association with response. The prevalence of non-mucinous BAC/ lepidic cell growth was related with
tumour reduction. EGFR TKD mutations were present in tumours with this predominant histologic
subtype. However, there were also 4 out of six invasive adenocarcinomas with predominant lepidic
growth without evidence of EGFR TKD mutations. Furthermore, one of the invasive adenocarcinoma
with predominant acinar component harboured a mutation. Previous reports by our group and others
indicate that EGFR TKD mutations are, in fact, heterogeneously expressed in NSCLC (342) (344). In our
EGFR TKD mutation analysis, only one representative tumour sample per patient was processed. If
EGFR TKD mutations are also heterogeneously expressed in our trial, this is may be in accordance with
the tumour response observed with tumour areas showing extensive fibrosis or collapse but others
presenting surviving cells. In fact, the main cellular subtype was the one taken into consideration but it is
possible that tumours presented smaller areas of non-mucinous BAC/ lepidic cells in which EGFR TKD
mutations may be present. Based on this, it is possible that EGFR TKD mutations were heterogeneously
present in our clinical trial. This open the possibility that patients experiencing tumour reduction and
classified as EGFR TKD wild type may, in fact, harbouring EGFR TKD mutations in non-analyzed
tumour areas. Whether EGFR TKD mutations are only expressed in non-mucinous BAC or lepidic cells
remains to be elucidated but this possibility may provide a new evidence of intratumoral molecular and
cellular heterogeneity with important clinical implications as different cellular subtypes will respond
differently to EGFR TKIs and, potentially, other agents. Future investigation is necessary to reveal if
EGFR TKD mutations are heterogeneous in early NSCLC, are present in specific cellular subtypes, and
any possible clinical relevance of this heterogeneity.
7.2. Limitations

169
Although relevant results were obtained from these experiments, we recognize that
improvements could be done.
Samples obtained and analyzed are derived from a phase II trial with a relatively small number
of patients recruited. Trial was designed for testing the feasibility of neoadjuvant gefitinib in early
NSCLC and not for detecting small differences in biomarkers. Nevertheless, important, strong
differences should be able to be detected even with this number of samples and correlated them with
clinical response and therefore this is not a limitation for the biomarkers explored. However, a manner of
improving this could be the inclusion of control samples derived from pathological stage I NSCLC
patients. This approach would allow us to add an extra “negative control” as these samples will reflect
the natural status of EGFR TKIs untreated tumours, in particular phosphorylation profile.
Another concern is the ischemia suffered by tumours samples from the time of surgical ischemia
is established until fixation/frozen happens. Although this may be an additional, unaccounted bias on the
expression of biomarkers explored here, it is also a reflection of standard clinical practice. As mentioned
in the Introduction section genotype variations and protein expression are not modified, if any, by
ischemic time until several hours or even days of modified conditions and, therefore, it is not expected
that these may be affected by ischemic time. Even so, an approach for future improvement is to collect
core-needle biopsies from tumours directly during surgery, immediately before surgical ischemic time is
initiated, which will immediately been frozen to reduce its exposure to ischemic conditions. Such
biopsies would be processed in parallel with pre-neoadjuvant and regularly collected post-neoadjuvant
samples. Although evidence does not support and relevant influence of surgical ischemia on biomarkers
investigated here, this extra set of samples would improve future investigations as it would serve as an
additional internal control.
IHC is a universally implemented assay used to detect protein expression on tissues. However, it
has its flaws as it does not provide a quantitative value, but semi-quantitative at best. Other assays that
have been implemented for a direct quantification of EGFR are radioactive labelled ligand binding assay
(179), enzyme-linked immunoabsorbent assays (180) and Western blotting but their special training and
facilities required, the required fresh tissue, but more importantly the potential false negative resulted
from the presence of no-tumoral elements in samples collected, such as stroma and infiltrative
lymphocytes, do not support their implementation in the current studies. Another potential approach
could have been to use immunofluoresence (IF) instead of IHC. IF gives a quantitative signal while
allowing co-stainings. This would have helped us to estimate the differences in signals between pre- and
post-gefitinib samples to be more reliable while also allowed to determine the intracellular compartment
from which such signals emerge. However, as we were expected small signals after treatment with
gefitinib (e.g. low phosphorylation), IHC allowed us to screen large tumor samples using low power

170
fields. Also, IHC has greatest sensitivity than IF. Therefore, IHC was the best assay to be implemented at
this step but it for future experiments it could be complemented with IF if localization and co-stainings
of a signal is important.
Finally, and for future reproducibility, our tissue processing was stricter than standard clinical
tissue processing. Tumour samples were obtained immediately after surgical resection and fixed always
in the same fixative and concentration. Furthermore, after paraffin blocks were generated, slides were not
cut until they were required and were processed following a strict protocol. If such strict protocol is not
followed it is possible that results are not reproducible in the future. For example, for EGFR, it is know
the fixative and concentration used as well as storage time of unstained sections affect EGFR IHC (190).
However, our strict protocol was necessary in order to control different potential bias from tissue
processing and to obtain the best expression of the actual tumour status and this must be taken into
consideration for future experiments.
Therefore, methodology implemented in these experiments was adequate for the comparisons
needed but different approaches can be incorporated in future directions that would improve results to be
searched.
7.3. Future directions
To answer the questions generated in the present work, the following hypothesis should be tested via
specific study aims as follows.
7.3.1. To investigate changes in the phosphorylation profile of EGFR and relevant intracellular
signalling molecules in NSCLC induced by the effect of tumour heterogeneity, ischemic time and
EGFR TKIs treatment.
Hypothesis: Phosphorylation of EGFR, Akt and Erk are not influenced by intratumoral
heterogeneity or ischemic time but they are heterogeneously dephosphorylated in
response to EGFR TKIs.
Aims: To evaluate the expression of phosphorylated EGFR, Akt and Erk in NSCLC.
To assess modification of EGFR, Akt and Erk phosphorylation profiles affected by
ischemia.

171
We have found that gefitinib induces significant dephosphorylation of Erk. However, differences
in total Erk were also observed, which may bias the changes observed in its phosphorylated isoform.
Furthermore, in regards to Akt phosphorylation, although 74% of cases experienced a reduction in
pAktThr308/Akt ratio, only 48% showed similar tendency for pAkt Ser473. Moreover, no changes in
pEGFR Y1173 but only in Y1068 were significant and these were not concordant among patients. These
results are the first in vivo evidence of the mechanism of action of gefitinib but overall these studies raise
the possibility of individual dephosphorylation profiles of EGFR and its relevant intracellular signalling
molecules in response to gefitinib. For predictive implications, only in the ISEL trial one of these
phosphorylated isoforms has been evaluated, in which p-Akt failed to predict prolonged survival (278).
However, as demonstrated in this thesis in regards to EGFR, if any molecular marker would be
implemented as predictor of response a proper characterization of a potential heterogeneous tumoral
expression and a modification by ischemia is warranted.
As described previously, p-Akt has shown a heterogeneous expression in melanoma (305).
Furthermore, as pAkt has been associated with EGFR TKD mutations, it is possible that the former is
influenced by the heterogeneous expression of the latter (306) (307) (342) (341) (337) (343) (344) (339).
Also, different studies suggest that pAkt is modified by ischemia in susceptible cell lines (314) (312)
(318) (316) (323). Furthermore, non-cancer cell models have suggested that Erk is activated transiently
under ischemic conditions (459) (460). However, no study has explored if the activation status of EGFR
and its related intracellular signalling molecular partners Akt and Erk are heterogeneously expressed in
NSCLC or modified by ischemia in vivo or during specimen processing.
With the development of new genomic and proteomic technologies, recent efforts have focused
on finding “fingerprints” of molecular patterns that can be related to patients’ outcomes and response to
therapy. Matrix-Assisted Laser-Desorption and Ionization (MALDI-MS) is a Mass Spectrometry-based
technique that allows direct profiling of protein complexes and amino acid sequences with a mass
accuracy of 1 Da in 10 000 with the advantage of allowing direct analysis from tissue sections and
requiring a simple sample preparation with a small number of cells. Using MALDI-based techniques,
protein expression profiles related to tumour characteristics and stage have been identified in NSCLC,
predicting the presence of metastasis and better survival (461) (462). Another relevant technique in the
“omics” era is the protein microarray which allows testing of hundred of specific antibodies in a single
sample, giving information on the expression level or protein modifications (e.g. phosphorylation),
which may shed light on specific pathways or patterns of expression. Because of the specificity of
antibody binding and the use of signal amplification by sensitive labeling methods, the detectable range
of protein concentration can be as low as less than 10 cell equivalents. For example, using global
phosphoproteomic approaches, activated protein kinases and their phosphorylated substrates could be

172
identified in a preclinical study (463). This methodology is a promising approach to study targeted
therapies specific to protein kinases.
It is possible that using these techniques, samples collected for the ischemia/heterogeneity
analysis of EGFR will be utilized to explore the phosphorylation profile of EGFR, Akt and Erk and a
potential modification due to ischemia and/or heterogeneous tumour expression. Furthermore, using the
set of paired tumour samples obtained from our neoadjuvant gefitinib trial in early NSCLC an important
comparison could be obtained of the significant proteins phosphorylation patterns after gefitinib therapy.
This study could bring valuable information not only by determining if phosphorylation status of
different residues are modified by ischemia and are heterogeneous but also by exploring changes
observed in patient who responded to therapy. This may ultimately provide valuable information in the
response induced by EGFR TKIs in NSCLC.
7.3.2. To investigate the expression pattern of EGFR TKD mutations in early NSCLC.
Hypothesis: EGFR TKD mutations are heterogeneously present in early NSCLC after gefitinib
treatment, been confined to non-mucinous/lepidic cells and the degree of heterogeneity
is correlated with response.
Aims: To evaluate the expression of EGFR TKD mutations in early NSCLC specimens after
gefitinib treatment.
To determine the cellular subtype in which EGFR TKD mutations are present in early
NSCLC.
To determine dephosphorylation profiles of EGFR, Akt and Erk in cells with and
without EGFR TKD mutations in response to EGFR TKI treatment.
To correlate the degree of heterogeneity of EGFR TKD mutations with clinical and
histopathological responses.
We have found that EGFR TKD mutations present the best association with gefitinib-induced
clinical response in early NSCLC. However, only 40% of shrinking tumours harbor this genotype, with
even one PR case not presenting an EGFR TKD mutation. A histological characteristic, non-mucinous
BAC/lepidic growth cells, was also associated with clinical response. Among tumours presenting mainly
such histology, all non-mucinous BAC harboured EGFR TKD mutations. However, in only 33% of
invasive adenocarcinoma with predominant BAC pattern such genotype was found. Furthermore, in a

173
predominantly acinar adenocarcinoma EGFR TKD mutation was also detected suggesting that EGFR
TKD mutations are not exclusive to tumours with such predominant histology.
Previously we reported that the two most common EGFR TKD mutations, exon 19del and
L858R are heterogeneously expressed in surgically treated NSCLC, implementing a microdissection and
fragment-length analysis and direct sequencing detection techniques (342). Similar observations were
obtained by Tang et al in adenocarcinoma cases (341). However, no histological subtypes were reported
in these studies.
Recently, specific-antibodies against mutant receptors have been developed. By using these,
EGFR exon19 deletion has been observed to be heterogeneously distributed, concentrating in areas of
solid growth pattern (337) (343). Furthermore, it is suggested that heterogeneity of EGFR TKD
mutations my affect clinical response to EGFR TKIs (344). However, no study has explored all factors,
heterogeneity of EGFR TKD mutations, histological correlation and influence on response to EGFR
TKIs.
To answer this question a detailed analysis of the heterogeneity of EGFR TKD mutations in our
clinical trial should be performed. Consecutive sections could be obtained from all available blocks
collected after gefitinib treatment. A detailed database of the cellularity present in each intraslide area
could be generated from a H&E-processed slide. Subsequent slides could undergo a careful laser-capture
microdissection, taking care to separate material obtained from each identified area. EGFR TKD
mutations will be detected using a highly sensitive fragment length analysis and the gold-standard
technique direct sequencing. Subsequent slides could undergo IHC detection of EGFR TKD mutations.
Correlation between cellularity type and presence of EGFR TKD mutations can be determined
accordingly. These experiments would allow us to determine if EGFR TKD mutations are heterogeneous
in early NSCLC and, more importantly, if these are present in a particular cellularity.
In order to determine if heterogeneity of EGFR TKD mutations influences the response induced
by EGFR TKIs ratio of mutant/wild type areas will be calculated per block and overall case and
association with clinical response, tumour fibrosis and reductions in cellularity and proliferation will be
determined. Furthermore, in order to determine if gefitinib induces different signalling responses in vivo
based on presence of EGFR TKD mutations dual immunofluoresence staining could be performed
pairing EGFR TKD and specific relevant phosphoisoform antibodies as determined by previous
experiments. Analysis derived from these assays would further characterize the clinical, histological and
signalling responses observed in early NSCLC and among different adenocarcinoma subtypes. Such
results will be fundamental for further patient selection for EGFR TKI therapy and/or combination with
other type of agents.

174
7.3.3. To understand novel mechanism of EGFR TKI resistance observed in early NSCLC.
Hypothesis: EGFR is internalized via a clathrin-dependent pathway due to an activation of p38
MAPK and is associated with resistance to gefitinib.
Aims: To characterize the receptor internalization machinery involved in the EGFR
internalization under gefitinib treatment
To elucidate if clathrin-dependent EGFR internalization is associated with resistance to
gefitinib
To investigate the role of p38 MAPK in resistance to gefitinib.
Our observations suggest a novel mechanism of resistance to gefitinib in NSCLC.
Dephosphorylation of EGFR on Y1068 was associated with tumour growth, higher cellularity and cell
proliferation. Furthermore, a particular perinuclear punctuate pattern remained.
Normally, EGFR is found concentrated in the membrane mainly in caveolae fractions (419). To
stop EGFR signalling, the receptor needs to move out of caveolae. Internalization of EGFR consists of
three steps: exist from caveolae, migration in the bulk plasma membrane and capture by coated pits,
ending in lysosomal degradation (421). This EGFR internalization is triggered after binding of ubiquitin
by ubiquitin E3 ligase to Y1045 or Grb2 to Y1068 or Y1086 and dynamin (420) (422). At endosomes,
ubiquitin acts as a targeting signal for degradation through interaction with the multivesicular body-
sorting machinery. However, a particular EGFR internalization mechanism has been observed under
stress conditions.
UVB, H2O2 or cholesterol depletion can result in EGFR internalization without ligand-binding
or ubiquitination (420) (421) (422). This effect is believed to be due to EGFR phosphorylation on serine
1002 or threonine 1008 as well as non-tyrosine residues located within 1012–1022 sites. Under these
conditions, EGFR is internalized in a slower pace than with EGF but it does not undergo lysosomal
degradation. Stress-induced EGFR internalization initially follows a clathrin-dependent pathway but,
instead, EGFR is concentrated in cytoplasmic Rab5-containing endosomes, escaping from late
endosomes/lysosomes and potentially undergoing a slow degradation via proteosomes (422). Also, TNF-
alpha has been reported to induce a rapid and transient EGFR internalization with rapid recycling to cell
surface, temporarily accumulating in a cytoplasmic punctuate pattern (421). During internalization by
this particular mechanism, p38 MAPK undergoes long lasting phosphorylation (420) (421) (422).
Activation of p38 MAPK has been reported to be responsible of ligand-independent EGFR
internalization with p38 MAPK promoting endocytosis via a dual mechanism involving EGFR and
EEA1/GDI phosphorylation, two Rab5 effectors (421).

175
In order to explore the localization of internalized total EGFR and pEGFR Y1068 under gefitinib
treatment co-immunostainings of this receptor and its phosphorylated isoform could be performed with
different markers including caveolin-1 for caveolae, AP2 for endocytic vesicles, transferrrin for recycling
endosomes, EEA1 (Early Endosome Antigen 1) and Rab5 for early endosomes, Rab7 for late
endosomes, lamp (lysosomal-associated membrane protein) 1 and 2 for lysosomes, Rpt5 (Regulatory
particle aTpase 5) for proteasome-enriched structures, 53FC3 for and galactosyltransferase for Golgi
apparatus, and MitoTracker dye for mitochondria. By coimmunostaining of these markers with EGFR
and pEGFR Y1068 the precise localization of the internalized receptor observed in our tumour samples
after gefitinib treatment will be determined. Furthermore, the E3-ubiquitin ligase c-Cbl, an ubiquitin-
specific protease 8 (USP8) for deubiquitination, and the ubiquitin marker P4D1 could be examined by
IHC staining to investigate the ubiquitination status of EGFR. These experiments will allow us to
characterize the internalization of EGFR following gefitinib treatment. These results could be correlated
with clinical response to allow determination of a potential role in resistance to gefitinib.
Activation of p38 MAPK has been found to be responsible of this non-ligand, non-
ubiquitination-mediated EGFR internalization (420) (421) (422). The presence of p38 MAPK and its
phosphorylated isoform Thr180/Tyr182 in NSCLC specimens treated with gefitinib could be examined
to determine a role in the resistance to EGFR TKI. With the recent development of a p38 MAPK
inhibitor, the association of p38 MAPK activation with resistance to gefitinib may support the
exploration of the value of a dual therapeutic regimen including an anti-EGFR and an anti-p38 MAPK
agent.
7.3.4. To explore the long term clinical value of a neoadjuvant EGFR TKI regimen in early
NSCLC
Hypothesis: A neoadjuvant EGFR TKI regimen improves PFS in early NSCLC. Longer PFS will be
observed in patients whose tumours harbour EGFR TKD mutations or have predominant
BAC/lepidic growth.
Aims: To investigate if a neoadjuvant gefitinib regimen will improve PFS in patients with early
NSCLC.
To assess the role of clinical and pathological responses induced by neoadjuvant
gefitinib in prolonging the PFS of early NSCLC patients.

176
To determine a predictive role of EGFR TKD mutations and non-mucinous BAC/lepidic
growth for PFS in early NSCLC patients treated with a neoadjuvant gefitinib regimen
before surgical resection.
To evaluate the role of Ki-67 index in regards to PFS in patients with early NSCLC
treated with a neoadjuvant gefitinib regimen.
By implementing our innovative trial design we have been able to demonstrate that a
neoadjuvant gefitinib regimen induces clinical and pathological responses in a subpopulation of early
NSCLC. However, the value of these responses in prolonging PFS remains unexplored. Also, tumours
harbouring EGFR TKD mutations and those with predominant non-mucinous BAC/lepidic cells
experienced better clinical responses and, on the other hand, dephosphorylation/intracellular
compartmentalization of EGFR Y1068 was associated with tumour growth under gefitinib treatment.
However, if these associations would also influence progression free survival remains to be studied. A 5-
year follow-up of our population enrolled in this trial could allow us to explore the value of these
responses and molecular and histopathological characteristics in PFS. If an association is observed, this
will help us to better select patients with early NSCLC to receive EGFR TKI before surgical resection.
In order to determine if heterogeneity of EGFR TKD mutations and type of cellularity may
influence patient selection all core needle biopsies as well as samples collected from surgical specimens
would be analyzed for presence of EGFR exon 19del or exon 21 L858R mutations in addition of
determine the main histology. By comparing the degree of variation between samples we would be able
to determine if multiple samples are necessary to better predict clinical response and prolonged PFS.
Also, by comparing results from before and after EGFR TKI treatment we would be able to determine
not only the positive and negative predictive values of EGFR TKD mutations and histology assessment
but also the feasibility of detecting them in fine and/or core needle biopsies for clinical practical
implications. Finally, the presence of EGFR TKD mutations would be also assessed by IHC using the
recently developed EGFR TKD antibodies in order to explore if they are encompassed to a particular
histological subtype and the value of this assay for patient selection.
We also observed that clinical shrinkage was associated with proliferation index. In order to
determine if Ki-67 index is reduced by gefitinib or presents a prognostic role, Ki-67 index will be
determine in tumour specimens collected both before and after EGFR TKI treatment. By performing this
analysis we will able to determine if Ki-67 is modified by EGFR TKI therapy, if preoperative biopsy
represent Ki-67 index adequately and if it has any value for patient selection for EGFR TKI therapy.
Lastly, to ultimately determine the value of neoadjuvant EGFR TKI therapy in early NSCLC, a
randomized phase III trial would be necessary. Such study could be designed similar to our phase II trial,

177
with diagnostic fine-needle aspiration and core-needle sample collection been obtained before
neoadjuvant course with gefitinib, in addition of pre and post-EGFR TKI CT scans and collection of
samples from surgical specimens. As patients with EGFR TKD mutations and those with non-mucinous
BAC/lepidic cellularity experienced better association with clinical and pathological responses in our
phase II trial, fine-needle aspirations and core-needle biopsies will be assessed in order to detect EGFR
exon 19del or L858R mutations or the specific cellularity present. While patients with either of these
characteristics would receive a neoadjuvant gefitinib course, those without any would be randomized
between a neoadjuvant EGFR TKI course or direct surgical resection. Such trial would allow us to
determine the clinical value of a neoadjuvant EGFR course in early NSCLC and to better characterize
patients responding to these agents
7.3. Conclusions
By performing these series of studies not only we will able to support our original hypothesis
that EGFR TKIs have clinical value as neoadjuvant regimen in early NSCLC but also to further
characterize responding patients for treatment selection. By obtaining these novel results, we will be able
to support further use of these agents in early NSCLC.

178
REFERENCES
1. Pfister DG, Johnson DH, Azzoli CG, et al. American Societe of Clinical Oncology treatment of
unresectable non-small-cell lung cancer guideline: update 2003. J Clin Oncol. 2004;22(2):330-353.
2. Detterbeck FC, Boffa DJ, Tanoue LT. The new lung cancer staging system. Chest. 2009;136(1):260-
271.
3. Lung Cancer Study Group: Ginsberg RJ, Rubinstein LV, et al. Randomized trial of lobectomy vresus
limited resection for T1N0 non-small cell lung cancer. Ann Thorac Surg. 1995;60(3):615-622.
4. Manser R, Wright G, Hart D, et al. Surgery for early stage non-small cell lung cancer. Cochrane
Database Syst Rev. 2005;1:CD004699.
5. Group, PORT Meta-analysis Trialists. Postoperative radiotherapy for non-small cell lung cancer
(Review). The Cochrane Library 2010;1:1-37.
6. Hurkmans CW, Cuijpers JP, Lagerwaard FJ, et al. Recommendations for implementing stereotactic
radiotherapy in peripheral stage IA non-small cell lung cancer: report from the Quality Assurance
Working Party of the randomised phase III ROSEL study. Radiat Oncol. 2009;4:1.
7. NSCLC Meta-analyses Collaborative Group: Arriagada R, Auperin A, Burdett S, et al. Adjuvant
chemotherapy, with or without postoperative radiotherapy, in operable non-small-cell lung cancer: two
meta-analyses of individual patient data. Lancet 2010;375(9722):1267-1277.
8. Feld R, Rubinstein L, Thomas PA, and the Lung Cancer Study Group. Adjuvant chemotherapy with
cyclophosphamide, doxorubicin and cisplatin in patients with completely resected stage I non-small cell
lung cancer. J Natl Cancer Inst. 1993;85:299-306.
9. Park JH, Lee CT, Lee HW, et al. Postoperative adjuvant chemotherapy for stage I non-small cell lung
cancer. Eur J Cardiothorac Surg. 2005;27:1086-1091.
10. Felip E, Rosell R, Maestre JA, et al. Preoperative chemotherapy plus surgery versus surgery plus
adjuvant chemotherapy versus surgery alone in early-stage non-small-cell lung cancer. J Clin Oncol.
2010;28(19):3138-3145.
11. Mineo TC, Ambrogi V, Corsaro V, Roselli M. Postoperative adjuvant therapy for stage IB non-small
cell lung cancer. Eur J Cardiothorac Surg. 2001;20:378-384.
12. Strauss GM, Herndon JE 2nd, Maddaus MA, et al. Adjuvant paclitaxel plus carboplatin compared
with observation in stage IB non-small-cell lung cancer: CALGB 9633 with the Cancer and Leukemia

179
Group B, Radiation Therapy Oncology Group, and North Central Cancer Treatment Group Study
Groups. J Clin Oncol. 2008;26(31):5043-5051.
13. Arriagada R, Bergman B, Dunant A, et al. Cisplatin-based adjuvant chemotherapy in patients with
completely resected non-small-cell lung cancer. New Engl J Med. 2004;350(4):351-360.
14. Arriagada R, Dunant A, Pignon JP, et al. Long-term results of the International Adjuvant Lung
Cancer Trial Evaluating Adjuvant Cisplatin-Based Chemotherapy in Resected Lung Cancer. J Clin
Oncol. 2010;28(1):35-42.
15. Winton T, Livingston R, Johnson D, et al. Vinorelbine plus cisplatin vs. observation in resected non-
small-cell lung cancer. N Engl J Med. 2005; 352(25):2589-2597.
16. Butts CA, Ding K, Seymour L, et al. Randomized phase III trial of vinorelbine plus cisplatin
compared with observation in completely resected stage IB and II non-small-cell lung cancer: updated
survival analysis of JBR-10. J Clin Oncol. 2010;28(1):29-34.
17. Nakagawa K, Tada H, Akashi A, et al. Randomised study of adjuvant chemotherapy for completely
resected p stage I-IIIA non-small cell lung cancer. BJ Cancer. 2006;95:817-821.
18. Wada H, Hitomi S, Teramatsu T. Adjuvant chemotherapy after complete resection in non-small-cell
lung cancer. J Clin Oncol. 1996;14:1048-1054.
19. Kato H, Ichinose Y, Ohta M, et al. A Randomized Trial of Adjuvant Chemotherapy with Uracil–
Tegafur for Adenocarcinoma of the Lung. N Engl J Med. 2004;350(17):1713-1721.
20. Hamada C, Tsuboi M, Ohta M, et al. Effect of postoperative adjuvant chemotherapy with tegafur-
uracil on survival in patients with stage IA non-small cell lung cancer: an exploratory analysis from a
meta-analysis of six randomized controlled trials. J Thorac Oncol. 2009;4(12):1511-1516.
21. Burdett S, Stewart L, Rydzewska L. A Systematic Review and Meta-analysis of the Literature:
Chemotherapy and Surgery versus Surgery Alone in Non-small Cell Lung Cancer. J Thorac Oncol.
2006;1(7):611-621.
22. Lim E, Harris G, Patel A, et al. Preoperative versus postoperative chemotherapy in patients with
resectable non-small cell lung cancer: systematic review and indirect comparison meta-analysis of
randomized trials. J Thorac Oncol. 2009;4(11):1380-1388.
23. Pisters KM, Vallières E, Crowley JJ, et al. Surgery with or without preoperative paclitaxel and
carboplatin in early-stage non-small-cell lung cancer: Southwest Oncology Group Trial S9900, an
intergroup, randomized, phase III trial. J Clin Oncol. 2010;28(11):1843-1849.

180
24. van der Geer P, Hunter T, Lindberg RA. Receptor protein tyrosine kinases and their signal
transduction pathways. Annu Rev Cell Biol. 1994;10:251-337.
25. Blume-Jensen P, Hunter T. Oncogenic kinase signalling. Nature. 2001;411:355-365.
26. Gschwind A, Fischer OM, Ullrich A.The discovery of receptor tyrosine kinases: targets for cancer
therapy. Nat Rev. 2004;4:361-370.
27. Burgess AW, Cho H-S, Elgenblot C, et al. An open- and -shut case? Recent insights into the
activation of EGF/ErbB receptors. Mol Cell. 2003;12:541-552.
28. Salomon D, Brandt R, et al. Epidermal growth factor-related peptides and their receptors in human
malignancies. Crit Rev Oncol Hematol. 1995;19(3):183-232.
29. Olayioye MA, Neve RM, et al. NEW EMBO MEMBERS' REVIEW: The ErbB signaling network:
receptor heterodimerization in development and cancer. EMBO J. 2000;19(13):3159-3167.
30. Mitsudomi T, Yatabe Y. Epidermal growth factor receptor in relation to tumor development: EGFR
gene and cancer. FEBS J. 2010;277(2):301-308.
31. Hynes NE, Lane HA. ERBB receptors and cancer: the complexity of targeted inhibitors. Nat Rev.
2005;5:341-354.
32. Schneider MR, Wolf E. The epidermal growth factor receptor ligands at a glance. J Cell Physiol.
2009;218:460-466.
33. Gazdar AF, Shigematsu H, Herz J, Miinna JD. Mutations and addiction to EGFR: the Achilles heal
of lung cancers? Trends Mol Med. 2004;10:481-486.
34. Zhang X, Gureasko J, Shen K, et al. An allosteric mechanism for activation of the kinase domain of
epidermal growth factor receptor. Cell. 2006;125:1137-1149.
35. Citri A, Yarden Y. EGF-ERBB signalling: towards the systems level. Nat Rev Mol Cell Biol.
2006;7:505-516.
36. Morandell S, Stasyk T, Skvortsov S, et al. Quantitative proteomics and phosphoproteomics reveal
novel insights into complexity and dynamics of the EGFR signaling network. Proteomics. 2008;8:4383-
4401.
37. Oda K, Matsuoka Y, Funahashi A, Kitano H. A comprehensive pathway map of epidermal growth
factor receptor signaling. Mol Syst Biol. 2005:1-17.

181
38. Yamauchi T, Ueki K, Tobe K, et al. Tyrosine phosphorylation of the EGF receptor by the kinase
Jak2 is induced by growth hormone. Nature. 1997;360:91-96.
39. Schlessinger J, Lemmon MA. SH2 and PTB domains in tyrosine kinase signaling.. Sci STKE.
2003:RE12.
40. Batzer AG, Rotin D, Urena JM, et al. Hierarchy of binding sites forGrb2 and Shc on the epidermal
growth factor receptor. Mol Cell Biol. 1994;14:5192–5201.
41. Okabayashi Y, Kido Y, Okatuni T, et al. Tyrosines 1148 and 1173 of activated human epidermal
growth factor receptors are binding sites of Shc in intact cells. J Biol Chem. 1994;269:18674-18678.
42. Chattopadhyay A, Vecchi M, Ji Q, et al. The role of individual SH2 domains in mediating
association of phospholipase C-gamma1 with the activated EGF receptor. J Biol Chem.
1999;274:26091–26097.
43. Levkowitz G, Waterman H, Ettenberg SA, et al. Ubiquitin ligase activity and tyrosine
phosphorylation underlie suppression of growth factor signaling by c-Cbl/Sli-1. Mol Cell. 1999;4:1029-
1040.
44. Keilhack H, Tenev T, Nyakatura E, et al. Phosphotyrosine 1173 mediates binding of the protein-
tyrosine phosphatase SHP-1 to the epidermal growth factor receptor and attenuation of receptor
signaling. J Biol Chem 1998;273:24839-24846.
45. Kolch, W. Meaningful relationships: The regulation of the Ras/Raf/MEK/ERK pathway by protein
interactions. Biochem J. 2000;351:289-305.
46. Lowenstein EJ, Daly RJ, Batzer AG, et al. The SH2 and SH3 domain-containing protein GRB2 links
receptor tyrosine kinases to ras signaling. Cell. 1992;70:431-442.
47. Agazie YM, Hayman MJ. Molecular mechanism for a role of SHP2 in epidermal growth factor
receptor signaling. Mol Cel Biol. 2003;23(21):7875-7886.
48. Moodie SA, Willumsen BM, Weber MJ, Wolfman A. Complexes of Ras. GTP with Raf-1 and
mitogen-activated protein kinase kinase. Science. 1993;260(5114):1658-1661.
49. Carey KD, Watson RT, Pessin JE, Stork PJ. The requirement of specific membrane domains for Raf-
1 phosphorylation and activation. J Biol Chem. 2003;278(5):3185-3196.
50. Kyriakis JM, App H, Zhang XF, et al. Raf-1 activates MAP kinase-kinase. Nature.
1992;358(6385):417-421.

182
1992;358(6385):417-421.
51. Hallberg B, Rayter SI, Downward J. Interaction of Ras and Raf in intact mammalian cells upon
extracellular stimulation. J Biol Chem. 1994;269:3913–3916.
52. Liebmann C. Regulation of MAP kinase activity by peptide receptor signalling pathway:paradigms
of multiplicity. Cell Signal. 2001;13:777–785.
53. Cheng M, Sexl V, Sherr CJ, Roussel MF. Assembly of cyclin D-dependent kinase and titration pf
p27Kip1 regulated by mitogen-activated protein kinase kinase (MEK1). Proc Natl Acad Sci USA.
1998;95:1091-1096.
54. Hill CS, Treisman R. Transcriptional regulation by extracellular signals: mechanisms and specificity.
Cell. 1995;80:199-211.
55. Ley R, Balmanno K, Hadfield K, et al. Activation of the ERK1/2 signaling pathway promotes
phosphorylation and proteasome-dependent degradation of the BH3-only protein, Bim. J Biol Chem.
2003;278:18811–18816.
56. Marani M, Tenev T, Hancock D, et al. Identification of novel isoforms of the BH3 domain protein
Bim which directly activate Bax to trigger apoptosis. Mol Cell Biol. 2002;22:3577–3589.
57. Tamas P, Solti Z, Bauer P, et al. Mechanism of epidermal growth factor regulation of Vav2, a
guanine nucleotide exchange factor for Rac. J Biol Chem. 2003;278(7):5163-5171.
58. Van Laethem A, Van Kelst S, Lippens S, et al. Activation of p38 MAPK is required for Bax
translocation to mitochondria, cytochrome c release and apoptosis induced by UVB irradiation in human
keratinocytes. FASEB. 2004;18:1946-1948.
59. Takeuchi K, Shin-ya T, Nishio K, Ito F. Mitogen-activated protein kinase phosphatase-1 modulated
JNK activation is critical for apoptosis induced by inhibitor of epidermal growth factor receptor-tyrosine
kinase. FEBS J. 2009;276:1255-1265.
60. Vivanco I, Sawyers CL. The phosphatidylinositol 3-kinase AKT pathway in human cancer. Nat Rev
Cancer. 2002;2:489–501.
61. Mattoon DR, Lamothe B, Lax I, Schlessinger J. The docking protein Gab1 is the primary mediator of
EGF-stimulated activation of the PI-3K/Akt cell survival pathway. BMC Biol. 2004;2:24.
62. Zhang SQ, Tsiaras WG, Araki T, et al. Receptor-specific regulation of phosphatidylinositol 3'-kinase
activation by the protein tyrosine phosphatase Shp2. Mol Cell Biol. 2002;22(12):4062-4072.

183
63. Jiang G, Zhang BB. PI 3-kinase and its up- and down-stream modulators as potential targets for the
treatment of type II diabetes. Front Biosci. 2002;7:d903-d907.
64. Cantley, LC. The phosphoinositide 3-kinase pathway. Science. 2002;296:1655-1657.
65. Gardai SJ, Hildeman DA, Frankel SK, et al. Phosphorylation of Bax Ser184 by Akt regulates its
activity and apoptosis in neutrophils. J Biol Chem. 2004;279:21085–21095.
66. Tsuruta F, Masuyama N, Gotoh Y. The phosphatidylinositol 3-kinase (PI3K)-Akt pathway
suppresses Bax translocation to mitochondria. J Biol Chem. 2002;277:14040–14047.
67. del Peso L, Gonzalez-Garcia M, Page C, et al. Interleukin-3-induced phosphorylation of BAD
through the protein kinase Akt. Science. 1997;278:687-689.
68. Marte BM, Downward J. PKB/Akt: connecting phosphoinositide 3-kinase to cell survival and
beyond. Trends Biochem Sci 1997;22(9):355-358.
69. Cardone MH, Roy N, Stennicke HR, et al. Regulation of cell death protease caspase-9 by
phosphorylation. Science. 1998;22:1318-1321.
70. Peng XH, Karna P, Cao Z, et al. Cross-talk between epidermal growth factor receptor and hypoxia-
inducible factor-1alpha signal pathways increases resistance to apoptosis by up-regulatin survivin gene
expression. J Biol Chem. 2006;281(36):25903-25914.
71. Busse D, Doughty RS, Ramsey TT, et al. Reversible G(1) arrest induced by inhibition of the
epidermal growth factor receptor tyrosine kinase requires up-regulation of p27(KIP1) independent of
MAPK activity. J Biol Chem. 2000;275:6987–6995.
72. Muise-Helmericks RC, Grimes HL, Bellacosa A, et al. Cyclin D expression is controlled post-
transcriptionally via a phosphatidylinositol 3-kinase/Akt-dependent pathway. J Biol Chem.
1998;273:29864-29872.
73. Diehl JA, Cheng M, Roussel MF, Sherr CJ. Glycogen synthase kinase-3beta regulates cyclin D1
proteolysis and subcellular localization. Genes Dev. 1998;12:3499-3511.
74. Rossing L, Jadidi AS, Urbich C, et al. Akt-dependent phosphorylation of p21(Cip1) regulates PCNA
binding and proliferation of endothelial cells. Mol Cell Biol 2001;21:5644-5657.
75. Zhou BP, Liao Y, Xia W, et al. Cytoplasmic localization of p21Cip1/WAF1 by Akt-induced
phosphorylation in HER-2/neu-overexpressing cells. Nat Cell Biol 2001;3:245-252.

184
76. Liang J, Zubovitz J, Petrocelli T, et al. PKB/Akt phosphorylates p27, impairs nuclear import of p27
and opposes p27-mediated G1 arrest. Nature Med. 2002;8:1153-1160.
77. Carpenter G, Ji Q. Phospholipase C-gamma as a signal-transducing element. Exp Cell Res.
1999;253(1):15-24.
78. DeSouza N, Reiken S, Ondrias K, et al. Protein kinase A and two phosphatases are components of
the inositol 1,4,5-triphosphate receptor macromolecular signaling complex. J Biol Chem.
2002;277(42):39397-39400.
79. Patterson RL, van Rossum DB, Nikolaidis N, et al. Phospholipase C-gamma: Diverse roles in
receptor-mediated calcium signaling. Trends Biochem Sci. 2005;30:688-697.
80. Darnell, JE. STATs and gene regulation. Science. 1997;277(5332):1630-1635.
81. Haura EB, Turkson J, Jove R. Mechanisms of disease: insights into the emerging role of signal
transducers and activators of transcription in cancer. Nat Clin Pract Oncol. 2005;2:15–324.
82. Niu G, Wright KL, Huang M, et al. Constitutive Stat3 activity up-regulates VEGF expression and
tumor angiogenesis. Oncogene. 2002;21:2000-2008.
83. Olayioye MA, Beuvink I, Horsch K, et al. ErbB receptor-induced activation of stat transcription
factors is mediated by Src tyrosine kinases. J Biol Chem. 1999;274(24):17209-17218.
84. Sato K, Nagao T, Iwasaki T, et al. Src-dependent phosphorylation of the EGF receptor Tyr-845
mediates Stat-p21waf1 pathway in A431 cells. Genes Cells 2003;8(12):995-1003.
85. Sh CS, Kehrl JH. Pyk2 amplifies epidermal growth factor and c-Src-induced Stat3 activation. J Biol
Chem. 2004;279(17):17224-17231.
86. Zhong Z, Wen Z, Darnell JE Jr. Stat3: a STAT family member activated by tyrosine phosphorylation
in response to epidermal growth factor and interleukin-6. Science. 1994;264:95–98.
87. Yu H, Jove R. The STATs of cancer – new molecular targets come of age. Nat Rev Cancer.
2004;4:97-105.
88. Lo HW, Hsu SC, Ali-Seyed M, et al. Nuclear interaction of EGFR and STAT3 in the activation of
the iNOS/NO pathway. Cancer Cell. 2005;7(6):575-589.

185
89. Wu TR, Hong YK, Wang XD, et al. SHP-2 is a dual-specificity phosphatase involved in Stat1
dephosphorylation at both tyrosine and serine residues in nuclei. J Biol Chem. 2002;277(49):47572-
47580.
90. Wang Q, Zhu F, Wang Z. Identification of EGF receptor C-terminal sequences 1005-1017 and di-
leucine motif 1010LL1011 as essential in EGF receptor endocytosis. Exp Cell Res. 2007;313:3349–
3363.
91. Salcini AE, Chen H, Iannolo G, et al. Epidermal growth factor pathway substrate 15, Eps15. Int J
Biochem Cell Biol 1999;31:805-809.
92. Rotin D, Staub O, Haguenauer-Tsapis R. Ubiquitination and endocytosis of plasma membrane
proteins: role of NEdd4/Rsp5p family of ubiquitin-protein ligases. J Membr Biol. 2000;176:1-17.
93. Lill NL, Douillard P, Awwad RA, et al. The evolutionarily conserved N-terminal region of Cbl is
sufficient to enhance down-regulation of the epidermal growth factor receptor. J Biol Chem.
2000;275(1):367-377.
94. Huang F, Sorkin A. Growth factor receptor binding protein 2-mediated recruitment of the RING
domain of Cbl to the epidermal growth factor receptor is essential and sufficient to support receptor
endocytosis. Mol Biol Cell. 2005;16:1268-1281.
95. Yokouchi M, Kondo T, Houghton A, et al. Ligand-induced ubiquitination of the epidermal growth
factor receptor involves the interaction of the c-Cbl RING finger and UbcH7. JBC. 1999;274:31707-
31712.
96. Soubeyran P, Kowanetz K, Szymkiewiccz I, et al. Cbl-CIN85-endophilin complex mediates ligand
induced downregulation of EGF receptors. Nature. 2002;416:183-187.
97. de Melker AA, van der Horst G, Calafat J, et al. c-Cbl ubiquitinates the EGF receptor at the plasma
membrane and remains receptor associated throughout the endocytic route. J Cell Sci. 2001;114:2167-
2178.
98. . Schlessinger, J. Cell signaling by receptor tyrosine kinases. Cell. 2000;103:211-225.
99. Chernoff, J. Protein tyrosine phosphatases as negative regulators of mitogenic signaling. J Cell
Physiol. 1999;180:173-181.
100. Lurje G, Lenz HJ. EGFR signaling and drug discovery. Oncology. 2009;77(6):400-410.

186
101. Roudabush FL, Pierce KL, Maudsley S, et al. Transactivation of the EGF receptor mediates IGF-1-
stimulated shc phosphorylation and ERK1/2 activation in COS-7 cells. J Biol Chem.
2000;275(29):22583-22589.
102. Liu D, Aguirre Ghiso JA, Estrada Y, Ossowski L. EGFR is a transducer of the urokinase receptor
initiated signal that is required for in vivo growth of a human carcinoma. Cancer Cell. 2002;1(5):445-
457.
103. Schmidt-Uldrich RK, Contessa JN, Lammering G, et al. ERBB receptor tyrosine kinases and
cellular radiation responses. Oncogene. 2003;22:5855-5865.
104. Toulany M, Kehlbach R, Florczak U, et al. Targeting of Akt1 enhances radiation toxicity of human
tumor cells by inhibiting DNA-PKcs-dependent DNA double-strand break repair. Mol Cancer Ther.
2008;7:1772-1781.
105. Yacoub A, McKinstry R, Hinman D, et al. Epidermal growth factor and ionizing radiation up-
regulate the DNA repair gene XRCC1 adn ERCC1 in DU145 and LNCaP prostate carcinoma through
MAPK signaling. Radiat Res. 2003;159:439-452.
106. Contessa JN, Reardon DB, Todd D, et al. The inducible expression of dominant-negative epidermal
growth factor receptor-CD533 results in radiosensitization of human mammary carcinoma cells. Clin
Cancer Res. 1999;5(2):405-411.
107. Toulany M, Minjgee M, Kehlbach R, et al. ErbB2 expression through heterodimerization with
erbB1 is necessary for ionizing radiation- but not EGF-induced activation of Akt survival pathway.
Radiother Oncol. 2010;97(2):338-345.
108. Dittmann K, Mayer C, Fehrenbacher B, et al. Radiation-induced epidermal growth factor receptor
nuclear import is linked to activation of DNA-dependent protein kinase. J Biol Chem.
2005;280(35):31182-31189.
109. Knebel A, Rahmsdorf HJ, Ullrich A, Herrlich P. Dephosphorylation of receptor tyrosine kinases as
target of regulation by radiation, oxidants or alkylating agents. EMBO J, 1996;15(19):5314-5325.
110. Khan EM, Lanir R, Danielson AR, Goldkorn T. Epidermal growth factor receptor exposed to
cigarette smoke is aberrantly activated and undergoes perinuclear trafficking . FASEB J. 2008;22:910-
917.
111. Gamour S, Shimizu M. Hydrogen peroxide preferentially enhances the tyrosine phosphorylation of
epidermal growth factor receptor. FEBS Lett. 1995;357(2):161-164.

187
112. Ravid T, Sweeney C, Gee Peter, et al. Epidermal growth factor receptor activation under oxidative
stress fails to promote c-Cbl mediated down-regulation. JBC. 2002;277:31214-31219.
113. Goldkorn T, Balaban N, Matsukuma K, et al. EGF-receptor phosphorylation and signaling are
targeted by H2O2 redox stress. Am J Respir Cell Mol Biol. 19(5):786-798.
114. Liu W, Akhand AA, Kato M, et al. 4-hydroxynonenal triggers an epidermal growth factor receptor-
linked signal pathway for growth inhibition. J Cell Sci 1999;112:2409-2417.
115. Evdonin AL, Guzhova IV, Margulis BA, Medvedeva ND. Extracellular heat shock protein 70
mediates heat-stress induced epidermal growth factor receptor transactivation in A431 carcinoma cells.
FEBS Lett 2006;580(28-29):6674-6678.
116. Simeonova PP, Wang S, Hulderman T, Luster MI. c-Src-dependent activation of the epidermal
growth factor receptor and mitogen-activated protein kinase pathway by arsenic. JBC. 2002;277:2945-
2950.
117. Tanos B, Pendergast AM. Abl tyrosine kinase regulates endocytosis of the epidermal growth factor
receptor. J Biol Chem 2006;281:32714-32723.
118. Khan EM, Heidinger JM, Levy M, et al. Epidermal growth factor receptor exposed to oxidative
stress undergoes Src- and caveolin-1-dependent perinuclear trafficking. J Biol Chem. 2006;281:14486–
14493.
119. Cordero JB, Cozzolino M, Lu Y, et al. 1,25-Dihydroxyvitamin D downregulates cell membrane
growth- and nuclear growth-promoting signals by the epidermal growth factor receptor. JBC.
2002;277:38965-38971.
120. Liao HJ, Carpenter G. Role of the Sec61 translocon in EGF receptor trafficking to the nucleus and
gene expression Mol Biol Cell. 2007;18(3):1064-1072.
121. Liao HJ, Carpenter G. Cetuximab/C225-induced intracellular trafficking of epidermal growth factor
receptor. Cancer Res. 2009;69(15):6179-6183.
122. Wells A, Marti U. Signalling shortcuts: cell-surface receptors in the nucleus? Nat Rev Mol Cell
Biol. 2002;3:697-702.
123. . Lin SY, Makino K, Xia W, et al. Nuclear localization of EGF receptor and its potential new role as
a transcription factor. Nat Cell Biol. 2001;3(9):802-808.

188
124. Wanner G, Mayer C, Kehlbach R, et al. Activation of protein kinase Cepsilon stimulates DNA-
repair via epidermal growth factor receptor nuclear accumulation. Radiother Oncol. 2008;86:383-390.
125. Hanada N, Lo HW, Day CP, et al. Co-regulation of B-Myb expression by E2F1 adn EGF receptor.
Mol Carcinog 2006;45(1):10-17.
126. Hung LY, Tseng JT, Lee YC, et al. Nuclear epidermal growth factor receptor (EGFR) interacts with
signal transducer and activator of transcription 5 (STAT5) in activating Aurora-A gene expression.
Nucleic Acids Res. 2008;36(13):4337-4351.
127. Bandyopadhyay D, Mandal M, Adam L, et al. Physical interaction between epidermal growth factor
receptor and DNA-dependent protein kinase in mammalian cells. J Biol Chem. 1998;273(3):1568-1573.
128. Das AK, Chen BP, Story MD, et al. Somatic mutations in the tyrosine kinase domain of the
epidermal growth factor receptor (EGFR) abrogate EGFR-mediated radioprotection in non-small cell
lung carcinoma. Cancer Res. 2007;67:5267-5274.
129. Das AK, Sato M, Story MD, et al. Non-small-cell lung cancers with kinase domain mutations in the
epidermal growth factor receptor are sensitive to ionizing radiation. Cancer Res. 2006;66:9601-9608.
130. Wang SC, Nakajima Y, Yu YL, et al. Tyrosine phosphorylation controls PCNA function through
protein stability. Nat Cell Biol. 2006;8(12):1359-1368.
131. Pavelic K, Banjac Z, Pavelic J, Spaventi S. Evidence for a role of EGF receptor in the progression
of human lung carcinoma.. Anticancer Res 1993;13(4):1133-1137.
132. Fujino S, Enokibori T, Tezuka N, et al. A comparison of epidermal growth factor receptor levels
and other prognostic parameters in non-small cell lung cancer. Eur J Cancer. 1996;32A(12):2070-2074.
133. Hirsch FR, Varella-Garcia M, Bunn PA Jr, et al. Epidermal growth factor receptor in non-small-cell
lung carcinomas: correlation between gene copy number and protein expression and impact on
prognosis. J Clin Oncol. 2003;21(20):3798-3807.
134. Kanematsu T, Yano S, Uehara H, et al. Phosphorylation, but not overexpression, of epidermal
growth factor receptor is associated with poor prognosis of non-small cell lung cancer patients. Oncol
Res. 2003;13(5):289-298.
135. Mendelsohn J, Baselga J. Status of epidermal growth factor receptor antagonists in the biology and
treatment of cancer. J Clin Oncol. 2003;21(14):2787-2799.

189
136. Brabender J, Danenberg KD, Metzger R, et al. Epidermal growth factor receptor and HER2-neu
mRNA expression in non-small cell lung cancer is correlated with survival. Clin Cancer Res.
2001;7(7):1850-1855.
137. Dziadziuszko R, Witta SE, Cappuzzo F, et al. Epidermal growth factor receptor messenger RNA
expression, gene dosage, and gefitinib sensitivity in non-small cell lung cancer. Clin Cancer Res.
2006;12:3078-3084.
138. Rusch V, Baselga J, Cordon-Cardo C, et al. Differential expression of the epidermal growth factor
receptor and its ligands in primary non-small cell lung cancers and adjacent benign lung. Cancer Res.
1993;53(10 Suppl):2379-2385.
139. Sholl LM, John Iafrate A, Chou YP, et al. Validation of chromogenic in situ hybridization for
detection of EGFR copy number amplification in non-small cell lung carcinoma. Mod Pathol.
2007;20:1028-1035.
140. Gallegos Ruiz MI, Floor K, Vos W, et al. Epidermal growth factor receptor (EGFR) gene copy
number detection in non-small-cell lung cancer; a comparison of fluorescence in situ hybridization and
chromogenic in situ hybridization. Histopathology. 2007;51(5):631-637.
141. Cappuzzo F, Hirsch FR, Rossi E, et al. Epidermal growth factor receptor gene and protein and
gefitinib sensitivity in non-small-cell lung cancer. JNCI. 2005;97(9):643-655.
142. Varella-Garcia, M. Stratification of non-small cell lung cancer patients for therapy with epidermal
growth factor receptor inhibitors: the EGFR fluorescence in situ hybridization assay. Diagn Pathol.
2006:1-19.
143. Voldborg BR, Damstrup L, Spang-Thomsen M, Poulsen HS. Epidermal growth factor receptor
(EGFR) and EGFR mutations, function and possible role in clinical trials. Ann Oncol. 1997;8:1197-
1206.
144. Chu CT, Everiss KD, Wikstrand CJ, et al. Receptor dimerization is not a factor in the signalling
activity of a transforming variant epidermal growth factor receptor (EGFRvIII). Biochem J. 1997;324(Pt
3):855-861.
145. Wikstrand CJ, McLendon RE, Friedman AH, Bigner DD. Cell surface localization and density of
the tumor-associated variant of the epidermal growth factor receptor, EGFRvIII . Cancer Res.
1997;57(18):4130-4140.

190
146. Ji H, Zhao X, Yuza Y, et al. Epidermal gorwth factor receptor variant III mutations in lung
tumorigenensis and sensitivity to tyrosine kinase inhibitors. Proc Natl Acad Sci USA. 2006;103:7817-
7822.
147. Ando M, Okamoto I, Yamamoto N, et al. Predictive factors for interstitial lung disease, antitumor
response, and survival in non-small-cell lung cancer patients treated with gefitinib. J Clin Oncol.
2006;24:2549-2556.
148. Lynch TJ, Bell DW, Sordella R, et al. Activating mutations in the epidermal growth factor receptor
underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350:2129-
2139.
149. Paez JG, Janne OA, Lee JC, et al. EGFR mutations in lung cancer: correlation with clinical
response to gefitinib therapy. Science. 2004;304:1497-1500.
150. Pao W, Miller V, Zakowski M, et al. EGF receptor gene mutations are common in lung cancers
from "never smokers" and are associated with sensitivity of tumors to gefitinib or erlotinib. Proc Natl
Acad Sci USA. 2004;101:13306-13311.
151. Shigematsu H, Gazdar AF. Somatic mutations of epidermal growth factor receptor signaling
pathway in lung cancers. Int J Cancer. 2006;118(2):257-262.
152. Mitsudomi T, Kosaka T, Yatabe Y. Biological and clinical implications of EGFR mutations in lung
cancer. Int J Cancer. 2006;11:190-198.
153. Sequist LV, Bell DW, Lynch TJ, Haber DA. Molecular predictors of response to epidermal growth
factor receptor antagonists in non–small-cell lung cancer. J Clin Oncol. 2007;25(5):587-595.
154. Miller VA, Kris MG, Shah N, et al. Bronchioloalveolar pathologic subtype and smoking history
predict sensitivity to gefitinib in advanced non-small-cell lung cancer. J Clin Oncol. 2004;22:1103-1109.
155. Mitsudomi T, Yatabe Y. Mutations of the epidermal growth factor receptor gene and related genes
as determinants of epidermal growth factor receptor tyrosine kinase inhibitors sensitivity in lung cancer.
Cancer Sci. 2007;98(12):1817-1824.
156. Okabe T, Okamoto I, Tamura K, et al. Differential constitutive activation of the epidermal growth
factor receptor in non-small cell lung cancer cells bearing EGFR gene mutation and amplification.
Cancer Res. 2007;67:2046-2053.
157. Sordella R, Bell DW, Haber DA, Settleman J. Gefitinib-sensitizing EGFR mutations in lung cancer
activate anti-apoptotic pathways. Science. 2004;305:1163-1167.

191
158. Matsuo K, Ito H, Yatabe Y, et al. Risk factors differ for non-small-cell lung cancers with and
without EGFR mutation: assessment of smoking and sex by a case-control study in Japanese. Cancer Sci.
2006;98:96-101.
159. Barber TD, Vogelstein B, Kinzler KW, Velculescu VE. Somatic mutations of EGFR in colorectal
cancers and glioblastomas. N Eng J Med. 2004;351:2883.
160. Lee JW, Soung YH, Kim SY, et al. Absence of EGFR mutation in the kinase domain in common
human cancers besides non-small-cell lung cancer. Int J Cancer. 2005;113, 2005:510-511.
161. Tokumo M, Toyooka S, Kiura K, et al. The relationship between epidermal growth factor receptor
mutations and clinicopathologic features in non-small cell lung cancers. Clin Cancer Res.
2005;11(3):1167-1173.
162. Marchetti A, Martella C, Felicioni L, et al. EGFR mutations in non-small-cell lung cancer: analysis
of a large series of cases and development of a rapid and sensitive method for diagnostic screening with
potential implications on pharmacologic treatment. J Clin Oncol. 2005;23(4):857-865.
163. Kosaka T, Yatabe Y, Endoh H, et al. Mutations of the epidermal growth factor receptor gene in
lung cancer: biological and clinical implications. Cancer Res. 2004;64:8919–8923.
164. Ji H, Li D, Chen L, et al. The impact of human EGFR kinase domain mutations on lung
tumorigenesis and in vivo sensitivity to EGFR-targeted therapies. Cancer Cell. 2006;9:485-495.
165. Politi K, Zakowski MF, Fan PD, et al. Lung adenocarcinomas induced in mice by mutant EGF
receptors found in human lung cancers respond to a tyrosine kinase inhibitor or to down-regulation of the
receptors. Genes Dev. 2006;20:1496-1510.
166. Tang X, Shigematsu H, Bekele BN, et al. EGFR tyrosine kinase domain mutations are detected in
histologically normal respiratory epithelium in lung cancer patients. Cancer Res. 2005;65:7568-7572.
167. Yatabe Y, Kosaka T, Takahashi T, Mitsudomi T. EGFR mutation is specific for terminal respiratory
unit type adenocarcinoma. Am J Surg Pathol. 2005;29:633-639.
168. Shigematsu H, Lin L, Takahashi T, et al. Clinical and biological features associated with epidermal
growth factor receptor gene mutations in lung cancers. J Natil Cancer Inst. 2005;97(5):339-346.
169. Rosell R, Moran T, Queralt C, et al. Screening for epidermal growth factor receptor mutations in
lung cancer. N Engl J Med. 2009;361(10):958-967.

192
170. Hsieh RK, Lim KH, Kuo HT, et al. Female sex and bronchioloalveolar pathologic subtype predict
EGFR mutations in non-small cell lung cancer. Chest. 2005;128:317-321.
171. Ninomiya H, Hiramatsu M, Inamura K, et al. Correlation between morphology and EGFR
mutations in lung adenocarcinomas: significance of the micropapillary pattern and the hobnail cell type.
Lung Cancer. 2009;63:235-240.
172. . Balak MN, Gong Y, Riely GJ, et al. Novel D761Y and common secondary T790M mutations in
epidermal growth factor receptor-mutant lung adenocarcinomas with acquired resistance to kinase
inhibitors. Clin Cancer Res. 2006;12:6494-6501.
173. Kobayashi S, Boggon TJ, Dayaram T, et al. EGFR mutation and resistance of non-small-cell lung
cancer to gefitinib. N Engl J Med 2005. 352:786-792.
174. Kosaka T, Yatabe Y, Endoh H, et al. Analysis of epidermal growth factor receptor gene mutation in
patients with non-small cell lung cancer and acquired resistance to gefitinib. Clin Cancer Res.
2006;12(19):5764-5769.
175. Kumar A, Petri ET, Halmos B, Boggon TJ. Structure and clinical relevance of the epidermal growth
factor receptor in human cancer. J Clin Oncol. 2008;26:1742-1751.
176. Yun C-H, Mengwasser KE, Toms AV, et al. The T790 mutation in EGFR kinase causes drug
resistance by increasing the affinity for ATP. Proc Natl Acad Sci USA. 2008;105:2070-2075.
177. Inukai M, Toyooka S, Ito S, et al. Presence of epidermal growth factor receptor gene T790M
mutation as a minor clone in non-small cell lung cancer. Cancer Res 2006;66:7854-7858.
178. Maheswaran S, Sequist LV, Nagrath S, Ulkus L. Detection of mutations in EGFR in circulating
lung cancer cells. N Engl J Med. 2008;359:1-12.
179. Veale D, Kerr N, Gibson GJ, et al. The relationship of quantitative epidermal growth factor receptor
expression in non-small cell lung cancer to long term survival. Br J Cancer 1993;68(1):162-165.
180. Pfeiffer P, Nexo E, Bentzen SM, et al. Enzyme-linked immunosorbent assay of epidermal growth
factor receptor in lung cancer: comparisons with immunohistochemistry, clinicopathological features and
prognosis. Br J Cancer. 1998;78(1):96-99.
181. Veale D, Ashcroft T, Marsh C, et al. Epidermal growth factor receptors in non-small cell lung
cancer. Br J Cancer. 1987;55(5):513-516.

193
182. . Hsieh ETK, Shepherd FA,Tsao MS. Co-expression of epidermal growth factor receptor and
transforming growth factor-α is independent of ras mutations in lung adenocarcinoma. Lung Cancer.
2000;29(2):151-157.
183. Rusch V, Klimstra D, Linkov I, Dmitrovsky E. Aberrant expression of p53 or the epidermal growth
factor receptor is frequent in early bronchial neoplasia, and coexpression precedes squamous cell
carcinoma development. Cancer Res. 1995;55:1365-1372.
184. Franklin WA, Veve R, Hirsch FR, et al. Epidermal growth factor receptor family in lung cancer and
premalignancy. Semin Oncol 2002;29(1Suppl4):3-14.
185. Rush V, Klimstra D, Venkatraman E, et al. Overexpression of the epidermal growth factor receptor
and its ligand transforming growth factor alpha is frequent in resectable non-small cell lung cancer but
does not predict tumor progression. Clin Cancer Res 1997;3(4):515-522.
186. Fontanini G, De Laurentiis M, Vignati S, et al. Evaluation of epidermal growth factor-related
growth factors and receptors and of neoangiogenesis in completely resected stage I-IIIA non-small-cell
lung cancer: amphiregulin and microvessel count are independent prognostic indicators of survival. Clin
Cancer Res. 1998;4(1):241-249.
187. Cerny T, Barnes DM, Hasleton P, et al. Expression of epidermal growth factor receptor (EGF-R) in
human lung tumours. Br J Cancer. 1986;54(2):265-269.
188. Pastorino U, Andreola S, Tagliabue E, et al. Immunocytochemical markers in stage I lung cancer:
relevance to prognosis. J Clin Oncol. 1997;15:2858-2865.
189. . Nicholson RI, Gee JM, Harper ME. EGFR and cancer prognosis. Eur J Cancer. 2001;37(suppl
4):S9-S15.
190. Atkins D, Reiffen KA, Tegtmeier CL, et al. Immunohistochemical detection of EGFR in paraffin-
embedded tumor tissues : variation in staining intensity due to choice of fixative and storage time of
tissue sections . J Histochem and Cytochem 2004;52(7):893-901.
191. Dei Tos AP, Ellis I. Assessing epidermal growth factor receptor expression in tumours: what is the
value of current test methods? Eur J Cancer 2005;41:1383-1392.
192. Pirker R, Pereira JR, Szczesna A et al. Cetuximab plus chemotherapy in patients with advanced
non-small-cell lung cancer (FLEX): An open-label randomised phase III trial. Lancet. 2009;373:1525-
1531.

194
193. Bleeker WK, Lammerts van Bueren JJ, van Ojik HH, et al. Dual mode of action of a human anti-
epidermal growth factor receptor monoclonal antibody for cancer therapy. J Immunol. 2004;173:4699–
4707.
194. Fan Z, Masui H, Altas I, et al. Blockade of epidermal growth factor receptor function by bivalent
and monovalent fragments of 225 anti-epidermal growth factor receptor monoclonal antibodies. Cancer
Res. 1993;53:4322-4328.
195. Fan Z, Lu Y, Wu X, Mendelsohn J. Antibody-induced epidermal growth factor receptor
dimerization mediates inhibition of autocrine proliferation of A431 squamous carcinoma cells. J Biol
Chem. 1994;269:27595-27602.
196. Prewett M, Rockwell P, Rockwell RF, et al. The biologic effects of C225, a chimeric monoclonal
antibody to the EGFR, on human prostate carcinoma. J Immunother Emphasis Tumor Immunol.
1996;19:419-427.
197. Wu X, Rubin M, Fan Z, et al. Involvement of p27KIP1 in G1 arrest mediated by an anti-epidermal
growth factor receptor monoclonal antibody. Oncogene. 1996;12:1397-1403.
198. Kiyota A, Shintani S, Mihara M, et al. Anti-epidermal growth factor receptor monoclonal antibody
225 upregulates p27(KIP1) and p15(INK4B) and induces G1 arrest in oral squamous carcinoma cell
lines. Oncology. 2002;63:92-98.
199. Jaramillo ML, Leon Z, Grothe S, et al. Effect of the anti-receptor ligand-blocking 225 monoclonal
antibody on EGF receptor endocytosis and sorting. Exp Cell Res. 2006;312(15):2778-2790.
200. Liu B, Fan Z. The monoclonal antibody 225 activates caspase-8 and induces apoptosis through a
tumor necrosis factor receptor family-independent pathway. Oncogene. 2001;20:3726–3734.
201. Huang SM, Bock JM, Harari PM. Epidermal growth factor receptor blockade with C225 modulates
proliferation apoptosis, and radiosensitivity in squamous cell carcinomas of the head and neck.. Cancer
Res. 1999;59:1935-1940.
202. Petit AM, Rak J, Hung M-C, et al. Neutralizing antibodies against epidermal growth factor and
ErbB-2/neu receptor tyrosine kinases down-regulate vascular endothelial growth factor production by
tumor cells in vitro and in vivo. Am J Pathol. 1997;151:1523-1530.
203. Doody JF, Wang Y, Patel SN, et al. Inhibitory activity of cetuximab on epidermal growth factor
receptor mutations in non small cell lung cancers. Mol Cancer Ther. 2007;6:2642–2651.

195
204. Steiner P, Joynes C, Bassi R, et al. Tumor growth inhibition with cetuximab and chemotherapy in
non-small cell lung cancer xenografts expressing wild-type and mutated epidermal growth factor
receptor. Clin Cancer Res. 2007;13:1540–1551.
205. Perez-Torres M, Guix M, Gonzalez A, Arteaga CL. Epidermal growth factor receptor (EGFR)
antibody down-regulates mutant receptors and inhibits tumors expressing EGFR mutations. J Biol Chem.
2006;281:40183–40192.
206. Kim ES, Mauer AM, William WN Jr, et al. A phase 2 study of cetuximab in combination with
docetaxel in chemotherapy-refractory/resistant patients with advanced nonsmall cell lung cancer. Cancer.
2009;115:1713-1722.
207. Hanna N, Lilenbaum R, Ansari R et al. Phase II trial of cetuximab in patients with previously
treated non-small-cell lung cancer. J Clin Oncol. 2006;24:5253-5258.
208. Rosell R, Robinet G, Szczesna A, et al. Randomized phase II study of cetuximab plus
cisplatin/vinorelbine compared with cisplatin/vinorelbine alone as first-line therapy in EGFR-expressing
advanced non-small-cell lung cancer. Ann Oncol. 2008;19(2):362-369.
209. Butts CA, Bodkin D, Middleman EL, et al. Randomized phase II study of gemcitabine plus cisplatin
or carboplatin [corrected], with or without cetuximab, as first-line therapy for patients with advanced or
metastatic non small-cell lung cancer. J Clin Oncol. 2007;25(36):5777-5784.
210. Blumenschein GR, Paulus R, Curran WJ et al. A phase II study of cetuximab (C225) in
combination with chemoradiation (CRT) in patients (pts) with stage IIIA/B non-small cell lung cancer
(NSCLC): A report of the 2 year and median survival (MS) for the RTOG 0324 trial [abstract 7516]. J
Clin Oncol. 2008;26(15 suppl):401s.
211. Coate LE, Cuffe S, McDowell D et al. Open non-randomised phase II pilot study of neoadjuvant
cetuximab in combination with cisplatin and gemcitabine in patients with resectable non small cell lung
cancer [abstract D7–06]. J Thorac Oncol. 2007;2(suppl 4):S412.
212. Yang XD, Jia XC, Corvalan JR, et al. Eradication of established tumors by a fully human
monoclonal antibody to the epidermal growth factor receptor without concomitant chemotherapy. Cancer
Res. 1999;59:1236-1243.
213. Yang XD, Jia XC, Corvalan JR et al. Development of ABX-EGF, a fully human anti-EGF receptor
monoclonal antibody, for cancer therapy. Crit Rev Oncol Hematol. 2001;38:17-23.

196
214. Crawford J, Swanson P, Prager D et al. Panitumumab, a fully human antibody, combined with
paclitaxel and carboplatin versus paclitaxel and carboplatin alone for first line advanced non-small cell
lung cancer (NSCLC): A primary analysis [abstract 1123]. Eur J Cancer. 2005;3(suppl):324.
215. Kim, T. Technology evaluation: matuzumab, Merck KGaA. Curr Opin Mol Ther. 2004;6:96-103.
216. Vanhoefer U, Tewes M, Rojo F et al. Phase I study of the humanized antiepidermal growth factor
receptor monoclonal antibody EMD72000 in patients with advanced solid tumors that express the
epidermal growth factor receptor. J Clin Oncol. 2004;22:175-184.
217. Kollmannsberger C, Schittenhelm M, Honecker F et al. A phase I study of the humanized
monoclonal anti-epidermal growth factor receptor (EGFR) antibody EMD 72000 (matuzumab) in
combination with paclitaxel in patients with EGFR-positive advanced non-small-cell lung cancer
(NSCLC). Ann Oncol. 2006;17:1007-1013.
218. Janmaat ML, Kruyt FA, Rodriguez JA, Giaccone G. Response to epidermal growth factor receptor
inhibitors in non-small cell lung cancer cells: limited antiproliferative effects and absence of apoptosis
associated with persistent activity of extracellular signal-regulated kinase or Akt kinase pathways. Clin
Cancer Res. 2003;9(6):2316-2326.
219. Gilmore AP, Valentijn AJ, Wang P, et al. Activation of BAD by therapeutic inhibition of epidermal
growth factor receptor and transactivation by insulin-like growth factor receptor. J Biol Chem.
2002;277:27643–27650.
220. Sun Q, Ming L, Thomas SM, et al. PUMA mediates EGFR tyrosine kinase inhibitor-induced
apoptosis in head and neck cancer cells. Oncogene. 2009;28:2348–2357.
221. Gong Y, SomwarR, Politi K, et al. Induction of BIM is essential for apoptosis triggered by EGFR
kinase inhibitors in mutant EGFR-dependent lung adenocarcinomas. PLoS Med. 2007;4:1655–1668.
222. Cragg MS, Kuroda J, Puthalakath H, et al. Gefitinib-induced killing of NSCLC cell lines expressing
mutant EGFR requires BIM and can be enhanced by BH3 mimetics. PLoS Med. 2007;4:1681–1689.
223. Costa DB, Halmos B, Kumar A, et al. BIM mediates EGFR tyrosine kinase inhibitor-induced
apoptosis in lung cancers with oncogenic EGFR mutations. PLoS Med. 2007;4:1669–1679.
224. Wood DE, Newcomb EW. Cleavage of Bax enhances its cell death function. Exp Cell Res.
2000;256:376-382.

197
225. Gao G, Dou QP. N-terminal cleavage of bax by calpain generates a potent proapoptotic 18-kDa
fragment that promotes bcl-2-independent cytochrome C release and apoptotic cell death. J Cell
Biochem. 2000;80:53-72.
226. Toyota H, Yanase N, Yoshimoto T, et al. Calpain-induced Bax-cleavage product is a more potent
inducer of apoptotic cell death than wild-type Bax. Cancer Lett. 2003;189:221-230.
227. Ariyama H, Qin B, Baba E, et al. Gefitinib, a selective EGFR tyrosine kinase inhibitor, induces
apoptosis through activation of Bax in human gallbladder adenocarcinoma cells. J Cell Biochem.
2006;97:724–734.
228. Di Gennaro E, Barbarino M, Bruzzese F, et al. Critical role of both p27KIP1 and p21CIP1/WAF1 in
the antiproliferative effect of ZD1839 ('Iressa'), an epidermal growth factor receptor tyrosine kinase
inhibitor, in head and neck squamous carcinoma cells. J Cell Physiol. 2003;195:139-150.
229. Koyama M, Matsuzaki Y, Yogosawa S, et al. ZD1839 induces p15INK4b and causes G1 arrest by
inhibiting the mitogen-activated protein kinase/extracellular signal-regulated kinase pathway. Mol
Cancer Ther. 2007;6(5):1579-1587.
230. Barnes CJ, Bagheri-Yarmand R, Mandal M, et al. Suppression of epidermal growth factor receptor,
mitogen-activated protein kinase, and Pak1 pathways and invasiveness of human cutaneous squamous
cancer cells by the tyrosine kinase inhibitor ZD1839 (Iressa). Mol Cancer Ther. 2003;2:345-351.
231. Fukuoka M, Yano S, Giaccone G, et al. Multi-institutional randomized phase II trial of gefitinib for
previously treated patients with advanced non-small-cell lung cancer. J Clin Oncol. 2003;21:2237-2246.
232. Kris MG, Natale RB, Herbst RS, et al. Efficacy of gefitinib, an inhibitor of the epidermal growth
factor receptor tyrosine kinase, in symptomatic patients with non-small-cell lung cancer: a randomized
trial. JAMA. 2003;290:2149-2158.
233. Tamura K, Okamoto I, Kashii T, et al. Multicentre prospective phase II trial of gefitinib for
advanced non-small cell lung cancer with epidermal growth factor receptor mutations: results of the
West Japan Thoracic Oncology Group trial (WJTOG0403). Br J Cancer. 2008;98(5):907-914.
234. Ellis PM, Morzycki W, Melosky B, et al. The role of the epidermal growth factor receptor tyrosine
kinase inhibitors as therapy for advanced, metastatic, and recurrent non-small-cell lung cancer: a
Canadian national consensus statement. Curr Oncol. 2009;16(1):25-46.

198
235. Cadranel J, Quoix E, Baudrin L, et al. IFCT-0401 Trial: a phase II study of gefitinib administered as
first-line treatment in advanced adenocarcinoma with bronchioloalveolar carcinoma subtype. J Thorac
Oncol 2009;4(9):1126-1135.
236. Ebi N, Semba H, Tokunaga SJ, et al. A phase II trial of gefitinib monotherapy in chemotherapy-
naïve patients of 75 years or older with advanced non-small cell lung cancer. J Thorac Oncol.
2008;3(10):1166-1171.
237. Yang CH, Yu CJ, Shih JY, et al. Specific EGFR mutations predict treatment outcome of stage
IIIB/IV patients with chemotherapy-naive non-small-cell lung cancer receiving first-line gefitinib
monotherapy. J Clin Oncol. 2008;26(16):2745-2753.
238. Sequist LV, Martins RG, Spigel D, et al. First-line gefitinib in patients with advanced non-small-
cell lung cancer harboring somatic EGFR mutations. J Clin Oncol. 2008;26(15):2442-2449.
239. Inoue A, Kobayashi K, Usui K, et al. First-line gefitinib for patients with advanced non-small-cell
lung cancer harboring epidermal growth factor receptor mutations without indication for chemotherapy. J
Clin Oncol. 2009;27(9):1394-1400.
240. Sugio K, Uramoto H, Onitsuka T, et al. Prospective phase II study of gefitinib in non-small cell
lung cancer with epidermal growth factor receptor gene mutations. Lung Cancer. 2009;64(3):314-318.
241. Lee DH, Han JY, Lee HG, et al. Gefitinib as a first-line therapy of advanced or metastatic
adenocarcinoma of the lung in never-smokers. Clin Cancer Res. 2005;11:3032-3037.
242. de Bono JS, Rowinsky EK. The ErbB receptor family: a therapeutic target for cancer. Trends Mol
Med. 2002;8(4 Suppl):S19-26.
243. Sausville E, Verweij J. Highlights from the EORTC-NCI-AACR 2002 meeting: molecular targets
and cancer therapeutics. Clin Adv Hematol Oncol. 2003;1(1):22-23.
244. Hidalgo M, Siu LL, Nemunaitis J, et al.Phase I and Pharmacologic Study of OSI-774, an Epidermal
Growth Factor Receptor Tyrosine Kinase Inhibitor, in Patients With Advanced Solid Malignancies. J
Clin Oncol. 2001;19(13):3267-3279.
245. Takahashi T, Yamamoto N, Nukiwa T, et al. Phase II study of erlotinib in Japanese patients with
advanced non-small cell lung cancer. Anticancer Res. 2010;30(2):557-563.
246. Uhm JE, Park BB, Ahn MJ, et al. Erlotinib monotherapy for stage IIIB/IV non-small cell lung
cancer: a multicenter trial by the Korean Cancer Study Group. J Thorac Oncol. 2009;4(9):1136-1143.

199
247. Zhou S, Ren S, Yan L, et al. Clinical efficacy of erlotinib in patients previously treated for
advanced non-small cell lung cancer. Respirology. 2009;14(5):709-715.
248. Kubota K, Nishiwaki Y, Tamura T, et al. Efficacy and safety of erlotinib monotherapy for Japanese
patients with advanced non-small cell lung cancer: a phase II study. J Thorac Oncol. 2008;3(12):1439-
1445.
249. Yoshioka H, Hotta K, Kiura K, et al. A phase II trial of erlotinib monotherapy in pretreated patients
with advanced non-small cell lung cancer who do not possess active EGFR mutations: Okayama Lung
Cancer Study Group trial 0705. J Thorac Oncol. 2010;5(1):99-104.
250. Akerley W, Boucher KM, Bentz JS, et al. A phase II study of erlotinib as initial treatment for
patients with stage IIIB-IV non-small cell lung cancer. J Thorac Oncol. 2009;4(2):214-219.
251. Goss G, Ferry D, Wierzbicki R, et al. Randomized phase II study of gefitinib compared with
placebo in chemotherapy-naive patients with advanced non-small-cell lung cancer and poor performance
status. J Clin Oncol. 2009;27(13):2253-2260.
252. Crinò L, Cappuzzo F, Zatloukal P, et al. Gefitinib versus vinorelbine in chemotherapy-naive elderly
patients with advanced non-small-cell lung cancer (INVITE): a randomized, phase II study. J Clin Oncol.
2008;26(26):4253-4260.
253. Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with
non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405):
an open label, randomised phase 3 trial. Lancet Oncol 2010;11(2):121-128.
254. Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non-small-cell lung
cancer with mutated EGFR. N Eng J Med. 2010;362(25):2380-2388.
255. Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary
adenocarcinoma. N Engl J Med. 2009;361(10):947-957.
256. Lee JS, Park K, Kim SW, et al. A randomized phase III study of gefitinib (IRESSATM) versus
standard chemotherapy (gemcitabine plus cisplatin) as a first-line treatment for never-smokers with
advanced or metastatic adenocarcinoma of the lung. J Thorac Oncol. 2009;4:S283-S284.
257. Lilenbaum R, Axelrod R, Thomas S, et al. Randomized Phase II Trial of Erlotinib or Standard
Chemotherapy in Patients With Advanced Non–Small-Cell Lung Cancer and a Performance Status of 2.
J Clin Oncol. 2008;26(6):863-869.

200
258. Zhou C, Wung YI, Chen G, et al. Efficacy results from the randomised phase III OPTIMAL
(CTONG 0802) study comparing first-line erlotinib versus carboplatin plus gemcitabine in Chinese
advanced non-small-cell lung cancer patients with EGFR activating mutations. Presented at European
Society of Medical Oncology Meeting. 2010;Abstract LBA13.
259. Cappuzzo F, Ciuleanu T, Stelmakh L, et al. Erlotinib as maintenance treatment in advanced non-
small-cell lung cancer: a multicentre, randomised, placebo-controlled phase 3 study. Lancet Oncol.
2010;11(6):521-529.
260. Giaccone G, Herbst RS, Manegold C, et al. Gefitinib in combination with gemcitabine and cisplatin
in advanced non-small-cell lung cancer: a phase III trial-INTACT 1 J Clin Oncol. 2004;22:777-784.
261. Herbst RS, Giaccone G, Schiller JH, et al. Gefitinib in combination with paclitaxel and carboplatin
in advanced non-small-cell lung cancer: a phase III trial – INTACT 2. J Clin Oncol. 2004;22:785–794.
262. Takeda K, Hida T, Sato T, et al. Randomized phase III trial of platinum-doublet chemotherapy
followed by gefitinib compared with continued platinum-doublet chemotherapy in Japanese patients with
advanced non-small-cell lung cancer: results of a west Japan thoracic oncology group trial. J Clin Oncol.
2010;28(5):753-60.
263. Gatzemeier U, Pluzanska A, Szczesna A, et al. Phase III study of erlotinib in combination with
cisplatin and gemcitabine in advanced non-small-cell lung cancer: the Tarceva Lung Cancer
Investigation Trial. J Clin Oncol. 2007;25(12):1545-1552.
264. Herbst RS, Prager D, Hermann R, et al. TRIBUTE: a phase III trial of erlotinib hydrochloride (OSI-
774) combined with carboplatin and paclitaxel chemotherapy in advanced non-small-cell lung cancer. J
Clin Oncol. 2005;23(25):5892-5899.
265. Mok TS, Wu YL, Yu CJ, et al. Randomized, placebo-controlled, phase II study of sequential
erlotinib and chemotherapy as first-line treatment for advanced non-small-cell lung cancer. J Clin Oncol.
2009;27(30):5080-5087.
266. Miller VA, O'Connor P, Soh C, Kabbinavar F. A rondimized, double-blind, placebo-controlled,
phase IIIb trial (ATLAS) comparing bevacizumab (B) therapy with or without erlotinib (E) after
completion of chemotherapy with B for first-line treatment of locally advanced, recurrent, or metastatic
non-sma. J Clin Oncol. 2009;27:18s[abstr LBA8002].
267. Lynch TJ, Patel T, Dreisbach L, et al. Cetuximab and first-line taxane/carboplatin chemotherapy in
advanced non-small-cell lung cancer: results of the randomized multicenter phase III trial BMS099. J
Clin Oncol. 2010;28(6):911-917.

201
268. Thatcher N, Lynch TJ, Butts C, et al. Cetuximab plus platinum-based chemotherapy as 1st-line
treatment in patients with non-small cell lung cancer (NSCLC): a meta-analysis of randomized phase
II/III trials. J Thorac Oncol. 2009;4(9):S5-968[abstr A3.7].
269. Thatcher N, Chang A, Parikh P, et al. Gefitinib plus best supportive care in previously treated
patients with refractory advanced non-small-cell lung cancer: results from a randomised, placebo-
controlled, multicentre study (Iressa Survival Evaluation in Lung Cancer). Lancet. 2005;366:1527-1537.
270. Cufer T, Vrdoljak E, Gaafar R, et al. Phase II, open label, randomized study (SIGN) of single agent
(Iressa) or docetaxel as second-line therapy in patients with advanced (stgae IIIB or IV) non-small-cell
lung cancer. Anticancer Drugs. 2006;17:401-409.
271. Kim ES, Hirsh V, Mok T, et al. Gefitinib versus docetaxel in previously treated non-small-cell lung
cancer (INTEREST): a randomised phase III trial. Lancet. 2008;372(9652):1809-1818.
272. Lee DH, Park K, Kim JH, et al. Randomized Phase III trial of gefitinib versus docetaxel in non-
small cell lung cancer patients who have previously received platinum-based chemotherapy. Clin Cancer
Res. 2010;16(4):1307-1314.
273. Maruyama R, Nishiwaki Y, Tamura T, et al. Phase III study, V-15-32, of gefitinib versus docetaxel
in previously treated Japanese patients with non-small-cell lung cancer. J Clin Oncol. 2008;26(26):4244-
4252.
274. Jiang J, Huang L, Liang X, et al. Gefitinib versus docetaxel in previously treated advanced non-
small-cell lung cancer: A meta-analysis of randomized controlled trials. Acta Oncol. 2010.
275. Shepherd FA, Rodrigues Pereira J, Ciuleanu T, et al. Erlotinib in Previously Treated Non-Small-
Cell Lung Cancer. N Engl J Med, 2005;353(2):123-132.
276. Giaccone G, Iacona RB, Fandi A, et al. Epidermal growth factor receptor expression analysis in
chemotherapy-naive patients with advanced non-small-cell lung cancer treated with gefitinib or placebo
in combination with platinum-based chemotherapy. J Cancer Res Clin Oncol. 2009;135(3):467-476.
277. Douillard JY, Shepherd FA, Hirsh V, et al. Molecular predictors of outcome with gefitinib and
docetaxel in previously treated non-small-cell lung cancer: data from the randomized phase III
INTEREST trial. J Clin Oncol. 2010;28(5):744-752.
278. Hirsch FR, Varella-Garcia M, Bunn PA Jr, et al. Molecular predictors of outcome with gefitinib in a
phase III placebo-controlled study in advanced non-small-cell lung cancer. J Clin Oncol.
2006;24(31):5034-5042.

202
279. Tsao MS, Sakurada A, Cutz JC, et al. Erlotinib in lung cancer - molecular and clinical predictors of
outcome. N Engl J Med. 2005;353(2):133-144.
280. Hirsch FR, Dziadziuszko R, Thatcher N, et al. Epidermal growth factor receptor
immunohistochemistry: comparison of antibodies and cutoff points to predict benefit from gefitinib in a
phase 3 placebo-controlled study in advanced nonsmall-cell lung cancer. Cancer. 2008;112(5):1114-
1121.
281. Clark GM, Zborowski DM, Culbertson JL, et al. Clinical utility of epidermal growth factor receptor
expression for selecting patients with advanced non-small cell lung cancer for treatment with erlotinib. J
Thorac Oncol. 2006;1(8):837-846.
282. Khambata-Ford S, Harbison CT, Hart LL, et al. Analysis of potential predictive markers of
cetuximab benefit in BMS099, a phase III study of cetuximab and first-line taxane/carboplatin in
advanced non-small cell lung cancer. J Clin Oncol. 2010;28(6):918-927.
283. Zhu CQ, da Cunha Santos G, Ding K, et al. Role of KRAS and EGFR as biomarkers of response to
erlotinib in National Cancer Institute of Canada Clinical Trials Group Study BR.21. J Clin Oncol.
2008;26(26):4268-4275.
284. Fukuoka M, Wu Y, Thongprasert S, et al. Biomarker analyses from a phase III, randomized, open-
label, first-line study of gefitinib (G) versus carboplatin/paclitaxel (C/P) in clinically selected patients
(pts) with advanced non-small cell lung cancer (NSCLC) in Asia (IPASS). J Clin Oncol.
2009;27(15s):abstr 8006.
285. Bell DW, Lynch TJ, Haserlat SM, et al. Epidermal growth factor receptor mutations and gene
amplification in non-small-cell lung cancer: molecular analysis of the IDEAL/INTACT gefitinib trials. J
Clin Oncol. 2005;23(31):8081-8092.
286. Dahabreh IJ, Linardou H, Siannis F, et al. Somatic EGFR mutation and gene copy gain as predictice
biomarkers for response to tyrosine kinase inhibitors in non-small cell lung cancer. Clin Cancer Res.
2010;16(1):291-303.
287. Dahabreh IJ, Linardou H, Kosmidis P, et al. EGFR gene copy number as a predictive biomarker for
patients receiving tyrosine kinase inhibitor treatment: a systematic review and meta-analysis in non-
small-cell lung cancer. Ann Oncol. 2011;22(3):545-552.
288. Eberhard DA, Johnson BE, Amler LC, et al. Mutations in the epidermal growth factor receptor and
in KRAS are predictive and prognostic indicators in patients with non-small-cell lung cancer treated with
chemotherapy alone and in combination with erlotinib. J Clin Oncol. 2005;23(25):5900-5909.

203
289. Han JY, Yoon KA, Park JH, et al. DNA repair gene polymorphisms and benefit from gefitinib in
never-smokers with lung adenocarcinoma., Cancer. 2011.
290. O’Byrne KJ, Bondarenko I, Barrios C, et al. Molecular and clinical predictors of outcome for
cetuximab in non-small cell lung cancer (NSCLC): data from the FLEX study. J Clin Oncol.
2009;27(15s):abstr 8007.
291. Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene in human cancer. Nature.
2002;417:949-954.
292. Takeshima Y, Amatya VJ, Daimaru Y, et al. Heterogeneous genetic alterations in ovarian mucinous
tumors: application and usefulness of laser capture microdissection. Hum Pathol. 2001;32(11):1203-
1208.
293. Kitago M, Ueda M, Aiura K, et al. Comparison of K-ras point mutation distributions in intraductal
papillary-mucinous tumors and ductal adenocarcinoma of the pancreas. Int J Cancer. 2004;110(2):177-
182.
294. Konishi N, Hiasa Y, Matsuda H, et al. Intratumor cellular heterogeneity and alterations in ras
oncogene and p53 tumor suppressor gene in human prostate carcinoma. Am J Pathol. 1995;147(4):1112-
1122.
295. Ohnishi T, Tomita N, Monden T, et al. A detailed analysis of the role of K-ras gene mutation in the
progression of colorectal adenoma. Br J Cancer. 1997;75(3):341-347.
296. Giaretti W, Rapallo A, Sciutto A, et al. Intratumor heterogeneity of k-ras and p53 mutations among
human colorectal adenomas containing early cancer. Anal Cell Pathol. 2000;21(2):49-57.
297. Saraga E, Bautista D, Dorta G, et al. Genetic heterogeneity in sporadic colorectal adenomas. J
Pathol. 1997;181(3):281-286.
298. Ishii M, Sugai T, Habano W, Nakamura S. Analysis of Ki-ras gene mutations within the same tumor
using a single tumor crypt in colorectal carcinomas. J Gastroenterol. 2004;39(6):544-549.
299. Zauber NP, Sabbath-Solitare M, Marotta S, et al. Adequacy of colonoscopic biopsy specimens for
molecular analysis: a comparative study with colectomy tissue. Diag Mol Pathol. 2006;15(3):162-168.
300. Baldus SE, Schaefer KL, Engers R, et al. Prevalence and heterogeneity of KRAS, BRAF, and
PIK3CA mutations in primary colorectal adenocarcinomas and their corresponding metastases. Clin
Cancer Res. 2010;16(3):790-799.

204
301. Losi L, Baisse B, Bouzourene H, Benhattar J. Evolution of intratumoral genetic heterogeneity
during colorectal cancer progression. Carcinogenesis. 2005;26(5):916-922.
302. Li ZH, Zheng J, Weiss LM, Shibata D. c-k-ras and p53 mutations occur very early in
adenocarcinoma of the lung. Am J Pathol. 1994;144(2):303-309.
303. Sagawa M, Saito Y, Fujimura S, Linnoila RI. K-ras point mutation occurs in the early stage of
carcinogenesis in lung cancer. Br J Cancer. 1998;77(5):720-723.
304. Giannini R, Ugolini C, Lupi C, et al. The heterogeneous distribution of BRAF mutation supports
the independent clonal origin of distinct tumor foci in multifocal papillary thyroid carcinoma. J Clin
Endocrinol Metab. 2007;92(9):3511-3516.
305. Slipicevic A, Holm R, Nguyen MT, et al. Expression of activated Akt and PTEN in malignant
melanomas: relationship with clinical outcome. Am J Clin Pathol. 2005;124(4):528-536.
306. Ikeda S, Takabe K, Inagaki M, et al. Correlation between EGFR gene mutation pattern and Akt
phosphorylation in pulmonary adenocarcinomas. Pathol Int. 2007;57:268-275.
307. Hosokawaa S, Toyookab S, Fujiwaraa Y, et al. Comprehensive analysis of EGFR signaling
pathways in Japanese patients with non-small cell lung cancer. Lung Cancer. 2009;66:107-113.
308. Sonobe M, Nakagawa M, Takenaka K, et al. Influence of Epidermal Growth Factor Receptor
(EGFR) gene mutations on the expression of EGFR, phosphoryl-Akt, and phosphoryl-MAPK, and on the
prognosis of patients with non-small cell lung cancer. J Surg Oncol. 2007;95:63-69.
309. Shahrzad S, Quayle L, Stone C, et al. Ischemia-induced K-ras mutations in human colorectal cancer
cells: role of microenvironmental regulation of MSH2 expression. Cancer Res. 2005;65(18):8134-8141.
310. Shahrzad S, Shirasawa S, Sasazuki T, et al. Low-dose metronomic cyclophosphamide treatment
mediates ischemia-dependent K-ras mutation in colorectal carcinoma xenografts. Oncogene.
2008;27(26):3729-3738.
311. Wang X, Schneider A. HIF-2alpha-mediated activation of the epidermal growth factor receptor
potentiates head and neck cancer cell migration in response to hypoxia. Carcinogenesis.
2010;31(7):1202-1210.
312. Xu L, Pathak PS, Fukumura D. Hypoxia-induced activation of p38 mitogen-activated protein kinase
and phosphatidylinositol 3'-kinase signaling pathways contributes to expression of interleukin 8 in
human ovarian carcinoma cells. Clin Cancer Res. 2004;10(2):701-707.

205
313. Box AH, Kim SM, Demetrick DJ. AKT loss in human epithelial cells treated with severe hypoxia.
Biochim Biophys. 2010;1803(8):951-959.
314. Zhang Q, Tang X, Lu QY, et al. Resveratrol inhibits hypoxia-induced accumulation of hypoxia-
inducible factor-1alpha and VEGF expression in human tongue squamous cell carcinoma and hepatoma
cells. Mol Cancer Ther. 2005;4(10):1465-1474.
315. Alvarez-Tejado M, Alfranca A, Aragonés J, et al. Lack of evidence for the involvement of the
phosphoinositide 3-kinase/Akt pathway in the activation of hypoxia-inducible factors by low oxygen
tension. J Biol Chem. 2002;277(16):13508-13517.
316. Yokoi K, Fidler IJ. Hypoxia increases resistance of human pancreatic cancer cells to apoptosis
induced by gemcitabine. Clin Cancer Res. 2004;10(7):2299-2306.
317. Mottet D, Dumont V, Deccache Y, et al. Regulation of hypoxia-inducible factor-1alpha protein
level during hypoxic conditions by the phosphatidylinositol 3-kinase/Akt/glycogen synthase kinase 3beta
pathway in HepG2 cells. J Biol Chem. 2003;278(33):31277-31285.
318. Box AH, Yuen C, Ponjevic D, et al. Signaling and apoptosis differences between severe hypoxia
and desferoxamine treatment of human epithelial cells. Biochem Cell Biol. 2008;86(5):425-436.
319. Furuta E, Pai SK, Zhan R, et al. Fatty acid synthase gene is up-regulated by hypoxia via activation
of Akt and sterol regulatory element binding protein-1. Cancer Res. 2008;68(4):1003-1011.
320. Ghafar MA, Anastasiadis AG, Chen MW, et al. Acute hypoxia increases the aggressive
characteristics and survival properties of prostate cancer cells. Prostate. 2003;54(1):58-67.
321. Suzuki A, Kusakai G, Shimojo Y, et al. Involvement of transforming growth factor-beta 1 signaling
in hypoxia-induced tolerance to glucose starvation. J Biol Chem. 2005;280(36):31557-31563.
322. Sasabe E, Tatemoto Y, Li D, et al. Mechanism of HIF-1alpha-dependent suppression of hypoxia-
induced apoptosis in squamous cell carcinoma cells. Cancer Sci. 2005;96(7):394-402.
323. Lee SM, Lee CT, Kim YW, et al. Hypoxia confers protection against apoptosis via PI3K/Akt and
ERK pathways in lung cancer cells. Cancer Lett. 2006;242(2):231-238.
324. Walsh S, Gill C, O'Neill A, et al. Hypoxia increases normal prostate epithelial cell resistance to
receptor-mediated apoptosis via AKT activation. Int J Cancer. 2009;124(8):1871-1878.
325. Xue J, Bi X, Wu G, et al. Fludarabine reduces survivability of HepG2 cells through VEGF under
hypoxia. Arch Biochem Biophys. 2007;468(1):100-106.

206
326. Arsham AM, Plas DR, Thompson CB, Simon MC. Phosphatidylinositol 3-kinase/Akt signaling is
neither required for hypoxic stabilization of HIF-1 alpha nor sufficient for HIF-1-dependent target gene
transcription. J Biol Chem. 2002;277(17):15162-15170.
327. Chen EY, Mazure NM, Cooper JA, Giaccia AJ. Hypoxia activates a platelet-derived growth factor
receptor/phosphatidylinositol 3-kinase/Akt pathway that results in glycogen synthase kinase-3
inactivation. Cancer Res. 2001;61(6):2429-2433.
328. Pham NA, Magalhaes JM, Do T, et al. Activation of Src and Src-associated signaling pathways in
relation to hypoxia in human cancer xenograft models. Int J Cancer. 2009;124(2):280-286.
329. Choi YJ, Rho JK, Lee SJ, et al. HIF-1alpha modulation by topoisomerase inhibitors in non-small
cell lung cancer cell lines. J Cancer Res Clin Oncol 2009;135(8):1047-1053.
330. Yan W, Fu Y, Tian D, et al. PI3 kinase/Akt signaling mediates epithelial-mesenchymal transition in
hypoxic hepatocellular carcinoma cells. Biochem Biophys Res Commun. 2009;382(3):631-636.
331. Garcia I, Vizoso F, Martin A, et al. Clinical Significance of the Epidermal Growth Factor Receptor
and HER2 Receptor in Resectable Gastric Cancer. Ann Surg Oncol. 2003;10(3):234-241.
332. Gamboa-Dominguez A, Dominguez-Fonseca C, Quintanilla-Martinez L, et al. Epidermal growth
factor receptor expression correlates with poor survival in gastric adenocarcinoma from Mexican
patients: a multivariate analysis using a standardized immunohistochemical detection system. Mod
Pathol. 2004;17:579-587.
333. Kimura M, Tsuda H, Morita D, et al. Usefulness and limitation of multiple endoscopic biopsy
sampling for epidermal growth factor receptor and c-erbB-2 testing in patients with gastric carcinoma.
Jpn J Clin Oncol. 2005;35(6):324-331.
334. Chhieng DC, Frost AR, Niwas S, et al. Intratumor heterogeneity of biomarker expression in breast
carcinomas. Biotech Histochem. 2004;79(1):25-36.
335. Nassar A, Radhakrishnan A, Cabrero IA, et al. Intratumoral heterogeneity of immunohistochemical
marker expression in breast carcinoma: a tissue microarray-based study. Appl Immunohistochem Mol
Morphol. 2010;18(5):433-441.
336. Suzuki S, Dobashi Y, Sakurai H, et al. Protein overexpression and gene amplification of epidermal
growth factor receptor in nonsmall cell lung carcinomas. An immunohistochemical and fluorescence in
situ hybridization study. Cancer. 2005;103(6):1265-1273.

207
337. Sholl LM, Yeap BY, Iafrate AJ, et al. Lung adenocarcinoma with EGFR amplification has distinct
clinicopathologic and molecular features in never-smokers. Cancer Res. 2009;69(21):8341-8348.
338. Ferrigan L, Wallace WAH. Predicting non-small cell lung cancer expression of epidermal growth
factor receptor and matrix metalloproteinase 9 from immunohistochemical staining of diagnostic biopsy
samples. Eur J Cancer. 2004;40(10):1589-1592.
339. Eberhard DA, Giaconne G, Johnson BE. Biomarkers of response to epidermal growth factor
receptor inhibitors in non-small cell lung cancer working group: standardization for use in clinical trial
setting. J Clin Oncol. 2008;26(6):983-94.
340. Yatabe Y, Takahashi T, Mitsudomi T. Epidermal growth factor receptor gene amplification is
acquired in association with tumor progression of EGFR-mutated lung cancer. Cancer Res.
2008;68:2106-2111.
341. Tang X, Varella-Garcia M, Xavier AC, et al. Epidermal Growth Factor Receptor abnormalities in
the pathogenesis and progression of lung adenocarcinomas. Cancer Prev Res. 2008;1(3):192-200.
342. Sakurada A, Lara-Guerra H, Liu N, et al. Tissue heterogeneity of EGFR mutation in lung
adenocarcinoma. J Thorac Oncol. 2008;3(5):527-529.
343. Kitamura A, Hosoda W, Sasaki E, et al. Immunohistochemical detection of EGFR mutation using
mutation-specific antibodies in lung cancer. Clin Cancer Res. 2010;16(13):3349-3355.
344. Taniguchi K, Okami J, Kodama K, et al. Intratumor heterogeneity of epidermal growth factor
receptor mutations in lung cancer and its correlation to the response to gefitinib. Cancer Sci.
2008;99(5):929-935.
345. Toby IT, Chicoine LG, Cui H, et al. Hypoxia-induced proliferation of human pulmonary
microvascular endothelial cells depends on epidermal growth factor receptor tyrosine kinase activation.
Am J Physiol Lung Cell Mol Physiol. 2010;298(4):L600-606.
346. Nishi H, Nishi KH, Johnson AC. Early Growth Response-1 gene mediates up-regulation of
epidermal growth factor receptor expression during hypoxia. Cancer Res. 2002;62(3):827-834.
347. Swinson DE, O'Byrne KJ. Interactions between hypoxia and epidermal growth factor receptor in
non–small-cell lung cancer. Clin Lung Cancer. 2006;7(4):250-256.
348. Franovic A, Gunaratnam L, Smith K, et al. Translational up-regulation of the EGFR by tumor
hypoxia provides a nonmutational explanation for its overexpression in human cancer. Proc Natl Acad
Sci U S A. 2007;104:13092–13097.

208
349. Laderoute KR, Grant TD, Murphy BJ, Sutherland RM. Enhanced epidermal growth factor receptor
synthesis in human squamous carcinoma cells exposed to low levels of oxygen. Int J Cancer.
1992;52(3):428-432.
350. Grigsby PW, Malyapa RS, Higashikubo R, et al. Comparison of molecular markers of hypoxia and
imaging with 60Cu-ATSM in cancer of the uterine cervix. Mol Imaging Biol. 2007;9:278-283.
351. Goethals L, Debucquoy A, Perneel C, et al. Hypoxia in human colorectal adenocarcinoma:
comparison between extrinsic and potential intrinsic hypoxia markers. Int J Radiat Oncol Biol Phys.
2006;65(1):246-254.
352. Swinson DE, Jones JL, Cox G, et al. Hypoxia-inducible factor-1 alpha in non small cell lung
cancer: relation to growth factor, protease and apoptosis pathways. Int J Cancer. 2004;111(1):43-50.
353. Swinson DE, Cox G, O'Byrne KJ. Coexpression of epidermal growth factor receptor with related
factors is associated with a poor prognosis in non-small-cell lung cancer. Br J Cancer. 2004;91(7):1301-
1307.
354. Görlach, A. Regulation of HIF-1alpha at the transcriptional level. Curr Pharm Des.
2009;15(33):3844-3852.
355. Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment
in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute
of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92:205-216.
356. Union Internacional Contra el Cancer. TNM classification of malignant tumours. [ed.] Wittekind C,
Sobin L Gospodarowicz M. 7th. s.l. : Wiley-Blackwell, 2009.
357. World Health Organization/International Agency for Research on Cancer. World Health
Organization Classification of Tumours: Pathology and Genetics of Tumours of the Lung, Pleura,
Thymus and Heart. [ed.] Brambilla E, Muller-Hermelink HK, Harris CC. Travis WD. s.l. : IARC Press,
2004.
358. Travis WD, Brambilla E, Noguchi M, et al. International Association for the Study of Lung
Cancer/American Thoracic Society/Europeran Respiratory Society International Multidisciplinary
Classification of Lung Adenocarcinoma. J Thorac Oncol 2011;6:244-285.
359. Motoi N, Szoke J, Riely GJ, et al. Lung adenocarcinoma: modification of the 2004 WHO mixed
subtype to include the major histologic subtype suggests correlations between papillary and

209
micropapillary adenocarcinoma subtypes, EGFR mutations and gene expression analysis. Am J Surg
Pathol. 2008;32(6):810-827.
360. Pan QPW, Ladanyi M. Rapid polymerase chain reaction-based detection of epidermal growth factor
receptor gene mutations in lung adenocarcinomas. J Mol Diagm. 2005;7(3):396-403.
361. Pignon JP, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin evaluation: a pooled analysis
by the LACE Collaborative Group. J Clin Oncol. 2008;26(21):3552-3559.
362. Ramnath N, Sommers E, Robinson L, et al. Phase II study of neoadjuvant chemotherapy with
gemcitabine and vinorelbine in resectable non-small cell lung cancer. Chest. 2005;128(5):3467-3474.
363. Depierre A, Milleron B, Moro-Sibilot D, et al. Preoperative Chemotherapy Followed by Surgery
Compared With Primary Surgery in Resectable Stage I (Except T1N0), II, and IIIa Non–Small-Cell Lung
Cancer. J Clin Oncol. 2002;20(1):247-253.
364. Detterbeck FC, Socinski MA, Gralla RJ, et al. Neoadjuvant chemotherapy with gemcitabine-
containing regimens in patients with early-stage non-small cell lung cancer. J Thorac Oncol.
2008;3(1):37-45.
365. Bepler G, Sommers KE, Cantor A, et al. Clinical efficacy and predictive molecular markers of
neoadjuvant gemcitabine and pemetrexed in resectable non-small cell lung cancer. J Thorac Oncol.
2008;3(10):1112-1118.
366. Scagliotti GV, Pastorino U, Vansteenkiste JF, et al. A phase III randomized study of surgery alone
or surgery plus preoperative gemcitabine-cisplatin in early-stage non-small cell lung cancer (NSCLC):
Follow-up data of Ch.E.S.T. Presented at the ASCO Annual Meeting 2008. J Clin Oncol.
2008;26(20suppl):abstr 7508.
367. Inoue A, Suzuki T, Fukuhara T, et al. Prospective phase II study of gefitinib for chemotherapy-
naive patients with advanced non-small-cell lung cancer with epidermal growth factor receptor gene
mutations. J Clin Oncol. 2006;24(21):3340-3346.
368. Asahina H, Yamazaki K, Kinoshita I, et al. A phase II trial of gefitinib as first-line therapy for
advanced non-small cell lung cancer with epidermal growth factor receptor mutations. Br J Cancer.
2006;95(8):998-1004.
369. Hirsch FR, Varella-Garcia M, Cappuzzo F, et al. Combination of EGFR gene copy number and
protein expression predicts outcome for advanced non-small-cell lung cancer patients treated with
gefitinib. Ann Oncol 2007;18(4):752-760.

210
370. Takano T, Ohe Y, Sakamoto H, et al. Epidermal growth factor receptor gene mutations and
increased copy numbers predict gefitinib sensitivity in patients with recurrent non-small-cell lung cancer.
J Clin Oncol. 2005;23(28):6829-6837.
371. Douillard JY, Rosell R, De Lena M, et al. Adjuvant vinorelbine plus cisplatin versus observation in
patients with completely resected stage IB-IIIA non-small-cell lung cancer (Adjuvant Navelbine
International Trialist Association [ANITA]): a randomised controlled trial. Lancet Oncol. 2006;7(9):719-
721.
372. Aljubran A, Leighl N, Pintilie M, Burkes R. Improved compliance with adjuvant vinorelbine and
cisplatin in non-small cell lung cancer. Hematol Oncol Stem Cell Ther. 2009;2(1):265-71.
373. Scagliotti GV, Fossati R, Torri V, et al. Randomized Study of Adjuvant Chemotherapy for
Completely Resected Stage I, II, or IIIA Non-Small-Cell Lung Cancer. J Natl Cancer Inst
2003;95(19):1453-1461.
374. Kassam F, Shepherd FA, Johnston M, et al. Referral patterns for adjuvant chemotherapy in patients
with completely resected non-small cell lung cancer. J Thorac Oncol. 2007;2(1):39-43.
375. Gilligan D, Nicolson M, Smith I, et al. Preoperative chemotherapy in patients with resectable non-
small cell lung cancer: results of the MRC LU22/NVALT 2/EORTC 08012 multicentre randomised trial
and update of systematic review. Lancet. 2007;369(9577):1929-1937.
376. Ishikawa N, Daigo Y, Takano A, et al. Increases of amphiregulin and transforming growth factor-
alpha in serum as predictors of poor response to gefitinib among patients with advanced non-small cell
lung cancers. Cancer Res. 2005;65(20):9176-9184.
377. Parra HS, Cavina R, Latteri F, et al. Analysis of epidermal growth factor receptor expression as a
predictive factor for response to gefitinib ('Iressa', ZD1839) in non-small-cell lung cancer. Br J Cancer.
2004;91(2):208-212.
378. Pérez-Soler R, Chachoua A, Hammond LA, et al. Determinants of tumor response and survival with
erlotinib in patients with non--small-cell lung cancer. J Clin Oncol. 2004;22(16):3238-3247.
379. Miller VA, Riely GJ, Zakowski MF, et al. Molecular characteristics of bronchioloalveolar
carcinoma and adenocarcinoma, bronchioloalveolar carcinoma subtype, predict response to erlotinib. J
Clin Oncol. 2008;26(9):1472-1478.
380. Hirsch FR, Varella-Garcia M, McCoy J, et al. Increased epidermal growth factor receptor gene copy
number detected by fluorescence in situ hybridization associates with increased sensitivity to gefitinib in

211
patients with bronchioloalveolar carcinoma subtypes: a Southwest Oncology Group Study. J CLin Oncol.
2005;23(28):6838-6845.
381. Soh J, Toyooka S, Ichihara S, et al. Impact of HER2 and EGFR gene status on gefitinib-treated
patients with nonsmall-cell lung cancer. Int J Cancer. 2007;121(5):1162-1167.
382. Sone T, Kasahara K, Kimura H, et al. Comparative analysis of epidermal growth factor receptor
mutations and gene amplification as predictors of gefitinib efficacy in Japanese patients with nonsmall
cell lung cancer. Cancer. 2007;109(9):1836-1844.
383. Tsao MS, Aviel-Ronen S, Ding K, et al. Prognostic and predictive importance of p53 and RAS for
adjuvant chemotherapy in non small-cell lung cancer. J Clin Oncol. 2007;25(33):5240-5247.
384. Suzuki T, Nakagawa T, Endo H, et al. The sensitivity of lung cancer cell lines to the EGFR-
selective tyrosine kinase inhibitor ZD1839 ('Iressa') is not related to the expression of EGFR or HER-2
or to K-ras gene status. Lung Cancer. 2003;42(1):35-41.
385. Shepherd FA, Tsao MS. Unraveling the mystery of prognostic and predictive factors in epidermal
growth factor receptor therapy. J Clin Oncol. 2006;24(7):1219-1220.
386. Yauch RL, Januario T, Eberhard DA, et al. Epithelial versus mesenchymal phenotype determines in
vitro sensitivity and predicts clinical activity of erlotinib in lung cancer patients. Clin Cancer Res.
2005;11:8686-8698.
387. Miyanaga A, Gemma A, Ando M, et al. E-cadherin expression and epidermal growth factor
receptor mutation status predict outcome in non-small cell lung cancer patients treated with gefitinib.
Oncol Rep. 2008;19:377-383.
388. Zucali PA, Ruiz MG, Giovannetti E, et al. Role of cMET expression in non-small-cell lung cancer
patients treated with EGFR tyrosine kinase inhibitors. Ann Oncol. 2008;19:1605-1612.
389. Cappuzzo F, Jänne PA, Skokan M, et al. MET increased gene copy number and primary resistance
to gefitinib therapy in non-small-cell lung cancer patients. Ann Oncol. 2009;20:298-304.
390. Haneda H, Sasaki H, Shimizu S, et al. Epidermal growth factor receptor gene mutation defines
distinct subsets among small adenocarcinomas of the lung. Lung Cancer. 2006;52(1):47-52.
391. Matsumoto S, Iwakawa R, Kohno T, et al. Frequent EGFR mutations in noninvasive
bronchioloalveolar carcinoma. Int J Cancer. 2006;118(10):2498-2504.

212
392. Kim YH, Ishii G, Goto K, et al. Dominant papillary subtype is a significant predictor of the
response to gefitinib in adenocarcinoma of the lung. Clin Cancer Res. 2004;10(21):7311-7317.
393. Chantranuwat C, Sriuranpong V, Huapai N, et al. Histopathologic characteristics of pulmonary
adenocarcinomas with and without EGFR mutation. J Med Assoc Thai 2005;88 Suppl 4:S322-S329.
394. Dacic S, Kelly L, Shuai Y, Nikiforova MN. miRNA expression profiling of lung adenocarcinomas:
correlation with mutational status. Mod Pathol. 2010;23:159-168.
395. Goldstein NS, Mani A, Chmielewski G, et al. Prognostic factors in T1 NO MO adenocarcinomas
and bronchioloalveolar carcinomas of the lung. Am J Clin Pathol. 1999;112:391-402.
396. Hoffmann TK, Schirlau K, Sonkoly E, et al. A novel mechanism for anti-EGFR antibody action
involves chemokine-mediated leukocyte infiltration. Int J Cancer. 2009;124:2589-2596.
397. López-Albaitero A, Lee SC, Morgan S, et al. Role of polymorphic Fc gamma receptor IIIa and
EGFR expression level in cetuximab mediated, NK cell dependent in vitro cytotoxicity of head and neck
squamous cell carcinoma cells. Cancer Immunol Immunother. 2009;58:1853-1864.
398. Roda JM, Joshi T, Butchar JP, et al. The activation of natural killer cell effector functions by
cetuximab-coated, epidermal growth factor receptor positive tumor cells is enhanced by cytokines. Clin
Cancer Res. 2007;13:6419-6428.
399. Baselga J, Rischin D, Ranson M, et al. Phase I safety, pharmacokinetic, and pharmacodynamic trial
of ZD1839, a selective oral epidermal growth factor receptor tyrosine kinase inhibitor, in patients with
five selected solid tumor types. J Clin Oncol. 2002;20:4292-4302.
400. Felip E, Rojo F, Reck M, et al. A phase II pharmacodynamic study of erlotinib in patients with
advanced non-small cell lung cancer previously treated with platinum-based chemotherapy. Clin Cancer
Res. 2008;14:3867-3874.
401. Bean J, Brennan C, Shih JY, et al. MET amplification occurs with or without T790M mutations in
EGFR mutant lung tumors with acquired resistance to gefitinib or erlotinib. Proc Natl Acad Sci USA.
2007;104:20932-20937.
402. Ward CW, Gough KH, Rashke M , et al. Systematic mapping of potential binding sites for Shc and
Grb2 SH2 domains on insulin receptor substrate-1 and the receptors for insulin, epidermal growth factor,
platelet-derived growth factor, and fibroblast growth factor. J Biol Chem. 1996;271(10):5603-5609.
403. Jorrinssen, RN. Epidermal growth factor receptor: Mechanism of activation and signaling. Exp Cell
Res. 2003;284:31-53.

213
404. Noro R, Gemma A, Kosaihira S, et al. Gefitinib (IRESSA) sensitive lung cancer cell lines show
phosphorylation of Akt without ligand stimulation. BMC Cancer. 2006;6:277.
405. Ono M, Hirata A, Kometani T, et al. Sensitivity to gefitinib (Iressa, ZD1839) in non-small cell lung
cancer cell lines correlates with dependence on the epidermal growth factor (EGF) receptor/extracellular
signal-regulated kinase 1/2 and EGF receptor/Akt pathway for proliferation. Mol Cancer Ther.
2004;3(4):465-472.
406. Emery IF, Battelli C, Auclair PL, et al. Response to gefitinib and erlotinib in non-small cell lung
cancer: a restrospective study.BMC Cancer. 2009;9:333.
407. VanMeter AJ, Rodriguez AS, Bowman ED, et al. Laser capture microdissection and protein
microarray analysis of human non-small cell lung cancer: differential epidermal growth factor receptor
(EGPR) phosphorylation events associated with mutated EGFR compared with wild type. Mol Cell
Proteomics. 2008;7(10):1902-1924.
408. Tracy S, Mukohara T, Hansen M, et al. Gefitinib induces apoptosis in the EGFRL858R non-small-
cell lung cancer cell line H3255. Cancer Res. 2004;64(20):7241-7244.
409. Lazzara MJ, Lane K, Chan R, et al. Impaired SHP2-mediated extracellular signal-regulated kinase
activation contributes to gefitinib sensitivity of lung cancer cells with epidermal growth factor receptor-
activating mutations. Cancer Res. 2010;70(9):3843-3850.
410. Mukohara T, Engelman JA, Hanna NH et al. Differential effects of gefitinib and cetuximab on non-
small-cell lung cancers bearing epidermal growth factor receptor mutations. J Natl Cancer Inst
2005;97:1185-1194.
411. Engelman JA, Zejnullahu K, Mitsudomi T, et al. MET amplification leads to gefitinib resistance in
lung cancer by activating ERBB3 signaling. Science. 2007;316:1039-1043.
412. Guix M, Faber AC, Wang SE, et al. Acquired resistance to EGFR tyrosine kinase inhibitors in
cancer cells is mediated by loss of IGF-binding proteins. J Clin Inv 2008;118(7):2609-2619.
413. Guo L, Kozlosky CJ, Ericsson LH, et al. Studies of ligand-induced site-specific phosphorylation of
epidermal growth factor receptor. J Am Soc Mass Spectrom. 2003;14(9):1022-1031.
414. Liu Y, Purvis J, Shih A, et al. A multiscale computational approach to dissect early events in the
Erb family receptor mediated activation, differential signaling, and relevance to oncogenic
transformations. Ann Biomed Eng. 2007;35(6):1012-1025.

214
415. Chen YR, Fu YN, Lin CH, et al. Distinctive activation patterns in constitutively active and
gefitinib-sensitive EGFR mutants. Oncogene 2006;25(8):1205-1215.
416. Jiang X, Huang F, Marusyk A, Sorkin A. Grb2 regulates internalization of EGF receptors through
clathrin-coated pits. Mol Biol Cell. 2003;14(3):858-870.
417. Koizumi F, Shimoyama T, Taguchi F, et al. Establishment of a human non-small cell lung cancer
cell line resistant to gefitinib. Int J Cancer. 2005;116(1):36-44.
418. Yang Z, Bagheri-Yarmand R, Wang RA, et al. The epidermal growth factor receptor tyrosine kinase
inhibitor ZD1839 (Iressa) suppresses c-Src and Pak1 pathways and invasiveness of human cancer cells.
Clin Cancer Res. 2004;10(2):658-667.
419. Mineo C, Gill GN, Anderson RG. Regulated migration of epidermal growth factor receptor from
caveolae. J Biol Chem 1999;274:30636-30643.
420. Lambert S, Ameels H, Gniadecki R, et al. Internalization of EGF receptor following lipid rafts
disruption in keratinocytes is delayed and dependent on p38 MAPK activation. J Cell Physiol.
2008;217(3):834-845.
421. Zwang Y, Yarden Y. p38 MAP kinase mediates stress-induced internalization of EGFR:
Implications for cancer chemotherapy.. EMBO J. 2006;25:4195-4206.
422. Vergarajauregui S, San Miguel A, Puertollano R. Activation of p38 mitogen-activated protein
kinase promotes epidermal growth factor receptor internalization. Traffic. 2006;7:686-698.
423. Malik SN, Siu LL, Rowinsky EK, et al. Pharmacodynamic evaluation of the epidermal growth
factor receptor inhibitor OSI-774 in human epidermis of cancer patients. Clin Cancer Res.
2003;9(7):2478-2486.
424. Saxinger C, Conrads TP, Goldstein DJ, Veenstra TD. Fully automated synthesis of
(phospho)peptide arrays in microtiter plate wells provides efficient access to protein tyrosine kinase
characterization. BMC Immunol. 2005;6:1.
425. Buerger C, Nagel-Wolfrum K, Kunz C, et al. Sequence-specific peptide aptamers, interacting with
the intracellular domain of the epidermal growth factor receptor, interfere with Stat3 activation and
inhibit the growth of tumor cells. J Biol Chem. 2003;278(39):37610-37621.
426. Zimmer S, Kahl P, Buhl TM, et al. Epidermal growth factor receptor mutations in non-small cell
lung cancer influence downstream Akt, MAPK and Stat3 signaling. J Cancer Res Clin Oncol.
2009;135(5):723-730.

215
427. Zwaenepoel K, Goris J, Erneux C, et al. Protein phosphatase 2A PR130/B"alpha 1 subunit binds to
the SH2 domain-containing inositol polyphosphate 5-phosphatase 2 and prevents epidermal growth
factor (EGF)-induced EGF recpetor degradation sustaining EGF-mediated signaling., FASEB J. 2010;
24(2):538-47.
428. Murata H, Ihara Y, Nakamura H, et al. Glutaredoxin exerts and antiapoptotic effect by regulating
the redox state of Akt. J Biol Chem. 2003;278:50226-50233.
429. Pham NA, Schwock J, Iakovlev V, et al. Immunohistochemical analysis of changes in signaling
pathway activation downstream of growth factor receptors in pancreatic duct cell carcinogenesis. BMC
Cancer. 2008;8:43.
430. Yau CY, Wheeler JJ, Sutton KL, Hedley DW. Inhibition of integrin-linked kinase by a selective
small molecule inhibitor, QLT0254, inhibits the PI3K/PKB/mTOR, Stat3, and FKHR pathways and
tumor growth, and enhances gemcitabine-induced apoptosis in human orthotopic primary pancreatic
cancer xenograf. Cancer Res. 2005;65(4):1497-1504.
431. Garassino MC, Borgonovo K, Rossi A, et al. Biological and clinical features in predicting efficacy
of epidermal growth factor receptor tyrosine kinase inhibitors: a systematic review and meta-analysis.
Anticancer Res. 2009;29(7):2691-2701.
432. Gupta R, Dastane AM, McKenna R Jr, Marchevsky AM. The predictive value of epidermal growth
factor receptor tests in patients with pulmonary adenocarcinoma: review of current "best evidence" with
meta-analysis. Hum Pathol. 2009;40(3):356-365.
433. Layfield LJ, Saria E, Mooney EE, et al. Tissue heterogeneity of immunohistochemically detected
estrogen receptor. Implications for image analysis quantification. Am J Clin Pathol. 1998;110(6):758-
764.
434. Chung GG, Zerkowski MP, Ghosh S, et al. Quantitative analysis of estrogen receptor heterogeneity
in breast cancer. Lab Invest 2007;87(7):662-669.
435. Moeder CB, Giltnane JM, Harigopal M, et al. Quantitative justification of the change from 10% to
30% for human epidermal growth factor receptor 2 scoring in the American Society of Clinical
Oncology/College of American Pathologists guidelines: tumor heterogeneity in breast cancer and its
implications for tissue microarray based assessment of outcome. J Clin Oncol. 2007;25(34):5418-5425.
436. Meyer JS, Wittliff JL. Regional heterogeneity in breast carcinoma: thymidine labelling index,
steroid hormone receptors, DNA ploidy. Int J Cancer. 1991;47(2):213-220.

216
437. Romain S, Chinot O, Guirou O, et al. Biological heterogeneity of ER-positive breast cancers in the
post-menopausal population. Int J Cancer. 1994;59(1):17-19.
438. Paradiso A, Mangia A, Barletta A, et al. Heterogeneity of intratumour proliferative activity in
primary breast cancer: biological and clinical aspects. Eu J Cancer. 1995;31A(6):911-916.
439. Siitonen SM, Isola JJ, Rantala IS, Helin HJ. Intratumor variation in cell proliferation in breast
carcinoma as determined by antiproliferating cell nuclear antigen monoclonal antibody and automated
image analysis. Am J Clin Pathol. 1993;99(3):226-231.
440. Dodd LG, Kerns BJ, Dodge RK, Layfield LJ. Intratumoral heterogeneity in primary breast
carcinoma: study of concurrent parameters. J Surg Oncol. 1997;64(4):280-287.
441. Goldstein NS, Armin M. Epidermal growth factor receptor immunohistochemical reactivity in
patients with American Joint Committee on Cancer Stage IV colon adenocarcinoma: implications for a
standardized scoring system. Cancer. 2001;92(5):1331-1346.
442. Ang KK, Berkey BA, Tu X, et al. Impact of epidermal growth factor receptor expression on
survival and pattern of relapse in patients with advanced head and neck carcinoma. Cancer Res.
2002;62(24):7350-7356.
443. Kearsley JH, Leonard JH, Walsh MD, Wright GR. A comparison of epidermal growth factor
receptor (EGFR) and c-erbB-2 oncogene expression in head and neck squamous cell carcinomas.
Pathology. 1991;23(3):189-194.
444. Tonkin KS, McKay JW, Stitt LW, et al. Tumour epidermal growth factor receptor, erbB-2 and
cathepsin D in node-negative invasive breast cancer: their impact on the selection of patients for systemic
adjuvant therapy. Cancer Prev Control. 1999;3(2):131-136.
445. Le QT, Chen E, Salim A, et al. An evaluation of tumor oxygenation and gene expression in patients
with early stage non-small cell lung cancers. Clin Cancer Res. 2006;12(5):1507-1514.
446. Langner C, Ratschek M, Rehak P, et al. Are heterogenous results of EGFR immunoreactivity in
renal cell carcinoma related to non-standardised criteria for staining evaluation? J Clin Pathol.
2004;57(7):773-775.
447. Pu YS, Huang CY, Kuo YZ, et al. Characterization of membranous and cytoplasmic EGFR
expression in human normal renal cortex and renal cell carcinoma. J Biomed Sci. 2009;16:82.

217
448. Richardson CM, Richardson D, Swinson DE, et al. Cyclooxygenase-2 protein levels are
independent of epidermal growth factor receptor expression or activation in operable non-small cell lung
cancer. Lung Cancer. 2005;48(1):47-57.
449. Lee HJ, Xu X, Choe G, et al. Protein overexpression and gene amplification of epidermal growth
factor receptor in nonsmall cell lung carcinomas: Comparison of four commercially available antibodies
by immunohistochemistry and fluorescence in situ hybridization study. Lung Cancer. 2010;68(3):375-
382.
450. Mathieu A, Weynand B, Verbeken E, et al. Comparison of four antibodies for
immunohistochemical evaluation of epidermal growth factor receptor expression in non-small cell lung
cancer. Lung Cancer. 2010;69(1):46-50.
451. Buckley AF, Kakar S. Comparison of the Dako EGFR pharmDx kit and Zymed EGFR antibody for
assessment of EGFR status in colorectal adenocarcinoma. Appl Immunohistochem Mol Morphol.
2007;15(3):305-309.
452. Liu-Jarin X, Stoopler MB, Raftopoulos H, et al. Histologic assessment of non-small cell lung
carcinoma after neoadjuvant therapy. Mod Pathol. 2003;16:1102-1108.
453. Kuerer HM, Sahin AA, Hunt KK, et al. Incidence and impact of documented eradication of breast
cancer axillary lymph node metastases before surgery in patients treated with neoadjuvant chemotherapy.
Ann Surg. 1999;230:72-78.
454. Symmans WF, Peintinger F, Hatzis C, et al. Measurement of residual breast cancer burden to
predict survival after neoadjuvant chemotherapy. J Clin Oncol. 2007;25:4414-4422.
455. Petty WJ, Dragnev KH, Memoli VA, et al. Epidermal growth factor receptor tyrosine kinase
inhibition represses cyclin D1 in aerodigestive tract cancers. Clin Cancer Res. 2004;10:7547-7554.
456. Mehdi SA, Tatum AH, Newman NB, et al. Prognostic markers in resected stage I and II non small-
cell lung cancer: an analysis of 260 patients with 5 year follow-up. Clin Lung Cancer. 1999;1:59-67.
457. Inoue M, Takakuwa T, Minami M, et al. Clinicopathologic factors influencing postoperative
prognosis in patients with small-sized adenocarcinoma of the lung. J Thorac Cardiovasc Surg.
2008;135:830-6.
458. Woo T, Okudela K, Yazawa T, et al. Prognostic value of KRAS mutations and Ki-67 expression in
stage I lung adenocarcinomas. Lung Cancer. 2009;65:355-362.

218
459. Sabha N, Aitken K, Lorenzo AJ, et al. Matrix metalloproteinase-7 and epidermal growth factor
receptor mediate hypoxia-induced extracellular signal-regulated kinase 1/2 mitogen-activated protein
kinase activation and subsequent proliferation in bladder smooth muscle cells. In Vitro Cell Dev Biol.
2006;42:124-133.
460. Park KM, Chen A, Bonventre JV, et al. Prevention of kidney ischemia/reperfusion-induced
functional injury and JNK, p38, and MAPK kinase activation by remote ischemic pretreatment. J Biol
Chem. 2001;276:11870-11876.
461. Yanagisawa K, Shyr Y, Xu BJ, et al. Proteomic patterns of tumour subsets in non-small-cell lung
cancer. Lancet. 2003;362(9382):433-439.
462. Kikuchi T, Massion PP, Shyr Y et al. Proteomic analysis of lung cancer tumors. J Clin Oncol.
2006;24.
463. Rush J, Moritz A, Lee KA, et al. Immunoaffinity profiling of tyrosine phosphorylation in cancer
cells. Nat Biotechnol. 2005;23(1):94-101.