Embed Size (px)
Citation preview

PharmacologyPharmacology ofofTyrosine Kinase Tyrosine Kinase InhibitorsInhibitors
Alain Astier, Pharm D, Ph DProfessor in Clinical Pharmacy and Biotechnics
Vice-President ESOPDepartment of Pharmacy and Toxicology, CNRS-UMR 7054
Henri Mondor University Hospital, Creteil, France

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
BackgroundBackground
MolecularMolecular targetedtargeted therapies (therapies (MTTsMTTs) are major ) are major advances in modern cancer careadvances in modern cancer care““NibsNibs”” are prototype of are prototype of MTTsMTTsTheir mechanisms of action are very different Their mechanisms of action are very different from classical from classical cytotoxiccytotoxic drugsdrugsMTTsMTTs come with broad range of unique side come with broad range of unique side effects different from classical effects different from classical cytotoxiccytotoxic agentsagentsMTTsMTTs are usually administered by oral route and are usually administered by oral route and for long time, mimicking classical treatments of for long time, mimicking classical treatments of chronic diseases chronic diseases

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
BackgroundBackground
Classical cancer treatment act by inhibition of cell Classical cancer treatment act by inhibition of cell proliferation at DNA level (DNA synthesis, DNA proliferation at DNA level (DNA synthesis, DNA duplication= duplication= cytotoxiccytotoxic drugs)drugs)
No specificity = strong toxicity upon normal proliferating No specificity = strong toxicity upon normal proliferating cells (gut, BMcells (gut, BM……))
MTT act by interactions with MTT act by interactions with Extra or intracellular signaling pathways (Extra or intracellular signaling pathways (TKIsTKIs))MicroMicro--environment: environment: vascularizationvascularization of tumor of tumor ((antiangiogenicantiangiogenic bevacizumabbevacizumab), ), metastasingmetastasing potentialpotential……More specific for some kind of cancer cells= no toxicity (or More specific for some kind of cancer cells= no toxicity (or modest) on normal proliferating cellsmodest) on normal proliferating cells

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Normal Cell Communication
Proteins
mRNA
Genes
Some communications pathways
Cell autodestructs
Cell divides
Receptors
From NCI Understanding Cancer and Related TopicsUnderstanding Molecular Diagnostics

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Cancer: A Communication Failure
Retinoblastoma, bone, bladder, lung, breast
Genes
Sarcomas
LeukemiaSome neuronal tumors
Colon Many cancers
Leukemia, brain,
breast, stomach,
lung
ProteinsmRNA
From NCI Understanding Cancer and Related TopicsUnderstanding Molecular Diagnostics
Target

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Receptors with tyrosine Receptors with tyrosine kinasekinase activityactivity
HER2 HER3 HER4EGFR
TGF-α, ΑR,ΒΤC
EGF
NR NR, BTC, EPR, HB-
EGF
HER (erbB) family
VEGFR-2 VEGFR-3VEGFR-1
VEGF-A VEGF-B
VEGF-C VEGF-D
Flt-3
VEGFR family
PDGFR KIT
FL PDGF SCF
PDGFR family
PP
PP
VEGFRs, PDGFR, KIT, Flt-3
Mutant Flt-3
P
P
P
P
EGFR/HER2
PP
PP
Receptor Dimerization and Activation
VEGF-A VEGF-CVEGF-D
IGF-1R
P
P
P
P
IGF-1 IGF-2
FGFR1 FGFR2 FGFR3 FGFR4
FGFR family

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008 FromFrom Kuhn, NZW Kuhn, NZW congresscongress, , HamburgHamburg, 2008, 2008

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
A target : BCRA target : BCR--ABL proteinABL proteinFusion protein produced by Fusion protein produced by bcr/ablbcr/abl oncogeneoncogene issued from issued from chromosomicchromosomic translocation 9 translocation 9 -->22 in chronic myeloid leukemia>22 in chronic myeloid leukemia
Derivative chromosome 22 referred to as Philadelphia (Ph1) chromosome.
BCRBCR--ABL have strong tyrosine ABL have strong tyrosine kinasekinase activity and induce cell activity and induce cell proliferation (= proliferation (= oncogeneoncogene))
Target of some Target of some TKIsTKIs ((imatinibimatinib, , erlotiniberlotinib, , dasatinibdasatinib))
In BCR-ABLexpressing cells, imatinib produces three related effects: inhibition of BCR-ABL, autophosphorylation and substrate phosphorylation, inhibition of proliferation, and induction of apoptosis

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
CML or GIST tyrosine CML or GIST tyrosine kinasekinaseinhibitorsinhibitors
Drugs inhibit tyrosineDrugs inhibit tyrosine--kinasekinase activities at activities at intracellular levelsintracellular levels
Drug mustDrug mustpenetrate inside cellspenetrate inside cellsbe maintained continuously at an efficient be maintained continuously at an efficient
levellevel
What are the factors influencing What are the factors influencing TKIsTKIsactivity ?activity ?

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
BehaviorBehavior of of drugdrug insideinside the bodythe bodyPharmacokineticsPharmacokinetics PharmacodynamicsPharmacodynamics
[ ]
Absorption
Elimination
Métabolism
Distributioneffects
Transporters (ABC, OCT)
Concentration and residence time

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
MechanismMechanism of action for of action for imatininbimatininb
Competitive blockade at the site of fixation for ATP
Blockade is depending of the concentration and length of exposure of TKIs at the active site of BCR-ABL

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Resistances to Resistances to imatinibimatinib

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Elimination of drugs (Elimination of drugs (TKIsTKIs))Sum of metabolism and excretionSum of metabolism and excretion
Elimination of drugs can strongly depend on Elimination of drugs can strongly depend on individual patient characteristics:individual patient characteristics:
Heredity: enzymatic activities depending on Heredity: enzymatic activities depending on heredity (metabolism enzymes, transporters)heredity (metabolism enzymes, transporters)Acquired pathologies :renal or hepatic Acquired pathologies :renal or hepatic dysfunctionsdysfunctionsInteractions with food, drugs, alcohol, Interactions with food, drugs, alcohol, tobaccotobacco……
Variability in drug responses and/or drugVariability in drug responses and/or drug--related toxicitiesrelated toxicities

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Consequences for treatmentsConsequences for treatments
It is not possible to modify hereditaryIt is not possible to modify hereditary--acquired acquired pharmacokinetic and pharmacokinetic and pharmacodynamicpharmacodynamic capacities but capacities but possible to identify patients possible to identify patients a prioria priori
It is possible and recommended to manage acquired It is possible and recommended to manage acquired elimination impairmentselimination impairments
It is It is mandatorymandatory to control behavioralto control behavioral--linked linked pharmacokinetics alterations i.e.pharmacokinetics alterations i.e.
Food interactionsFood interactionsDrug interactionsDrug interactionsComplianceComplianceHabits (smoking, drinkingHabits (smoking, drinking……))

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Plasma concentrationPlasma concentration--effect effect relationshipsrelationships
FromFrom Kuhn, NZW Kuhn, NZW congresscongress, , HamburgHamburg, 2008, 2008

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
ConsequencesConsequencesIt is essential to obtain It is essential to obtain and maintain adequate and maintain adequate plasmatic levelsplasmatic levelsAvoid any cause lowering Avoid any cause lowering plasmatic levelsplasmatic levels
inefficacyinefficacyAvoid any cause Avoid any cause increasing plasmatic increasing plasmatic levels levels
toxicitytoxicityAvoid any cause inducing Avoid any cause inducing plasmatic levels variabilityplasmatic levels variability
Inefficacy
Toxicity
Ratio of toxic level to efficacy level
is the therapeutic index
inefficacy, toxicity, induction of inefficacy, toxicity, induction of resistanceresistance

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Adherence to medication Adherence to medication Major problem with oral drugsMajor problem with oral drugsin chronic diseases:in chronic diseases:
AntiAnti--hypertensivehypertensiveLipids lowering Lipids lowering AntidiabeticAntidiabeticAntiretroviral ! Antiretroviral ! Anticancer !Anticancer !
Difference betweenDifference betweenExecution: irregularity of takingExecution: irregularity of takingPersistence: length of time during which the medication is takenPersistence: length of time during which the medication is taken

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Incidence of nonIncidence of non--adherenceadherenceAntihypertensive drugsAntihypertensive drugs
3232--38 % 6 months (38 % 6 months (VrijensVrijens et al, BMJ, 2008et al, BMJ, 2008))4949--52 % 12 months (52 % 12 months (Bloom et al, BMJ, 2001Bloom et al, BMJ, 2001))
TamoxifenTamoxifen35 % at 3.5 years 35 % at 3.5 years
((Barron et al, Cancer, 2007Barron et al, Cancer, 2007))
GefitinibGefitinib (TKI)(TKI)1414--36 %36 %
((Lesley, Lung Cancer 2005Lesley, Lung Cancer 2005))
ImatinibImatinib28 % at 5 years28 % at 5 years
(IRIS trial)(IRIS trial)

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
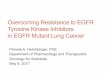
ImatinibImatinib adherenceadherence
*Time on therapy without significant gaps in refills.
685
Patie
nts
Months0–1
35003000250020001500
0
1000500
1–2 2–3 3–4 4–5 5–6 6–7 7–8 8–9 9–1010–1111–1212–1313+
2921Patients taking recommended dose of
imatinib
In this US study of patients with either CML and GIST persistency* was near 100% at month 4 Persistency declined from 94% at month 5, to 23% at month 14
Tsang J-P, Rudychev I, Pescatore SL. J Clin Onc. 2006; 24:330s. Abstract 6119

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
NonNon--adherenceadherence
Adherence could strongly depend on the Adherence could strongly depend on the sideside--effects acting on the overall quality of effects acting on the overall quality of lifelife
Reducing Reducing evitable sideevitable side--effectseffects could could increase adherenceincrease adherence
Major role of Major role of patient education

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
MetabolismMetabolism
Phase I Phase II

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Drug interactions Drug interactions Example of Example of NilotinibNilotinib
Competitive inhibitor of CYP3A, 2C8, 2C9, 2D6, Competitive inhibitor of CYP3A, 2C8, 2C9, 2D6, UGT1A1UGT1A1
Increasing concentration of Increasing concentration of midazolammidazolam 30 %30 %
Drug affecting Drug affecting nilotinibnilotinib metabolism metabolism KetoconazoleKetoconazole (400 mg 6 days) : inhibitor(400 mg 6 days) : inhibitor
AUC 300 %AUC 300 %
RifampicinRifampicin (600 mg 12 days) : activator(600 mg 12 days) : activatorAUC 80 %AUC 80 %
OverOver--exposure : serious effects, lifeexposure : serious effects, life--threatening threatening

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008 FromFrom Kuhn, NZW Kuhn, NZW congresscongress, , HamburgHamburg, 2008, 2008
Proton pump inhibitors (famotidine, omeprazole) decrease absorption of Dasatinib by 60 % (10 hr before) and anti-acids by 55 % (2 hr window)

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Effects of food interactionEffects of food interactionAs compared to fasting:
ImatinibNo difference
Nilotinib 2 hrs PC (No food X 1 hr Post)Cmax ↑30% 2 hr post light meal;55% 30 min post light meal112% 30 min post high fatNot to be taken within 2hr after eatingWait 1 hr before any food
DasatinibNo difference

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008 Wilkinson GR, N Engl J Med 2005;352:2211-21.
PrePre--systemic interaction: grapefruitsystemic interaction: grapefruit
Same behavior with several other TKIs

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Drug interactionsDrug interactionsPrescribed medications Prescribed medications
potentially important but not really a problempotentially important but not really a problem
SelfSelf--medication: medication: important problem, underestimatedimportant problem, underestimated
Alternative (herbal) medicines, OTC products Alternative (herbal) medicines, OTC products (e.g. vitamins, (e.g. vitamins, NSAIDsNSAIDs), nutritional supplements ), nutritional supplements and foodstuffsand foodstuffs (grapefruit(grapefruit……))
major problem, very underestimatedmajor problem, very underestimated

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
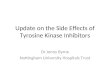
Effect of (bad) habitsEffect of (bad) habits
FromFrom Kuhn, NZW Kuhn, NZW congresscongress, , HamburgHamburg, 2008, 2008

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
ConclusionConclusion
TKIsTKIs are efficient new treatments for CML, GIST are efficient new treatments for CML, GIST and many other malignanciesand many other malignancies
Best efficacy will be only obtained if several Best efficacy will be only obtained if several major problem are managed:major problem are managed:
DrugDrug--related siderelated side--effectseffectsToxicity or inefficacy induced byToxicity or inefficacy induced by
Drugs interactionsDrugs interactionsFoods interactionsFoods interactions
Insufficient adherenceInsufficient adherence

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
Conclusion: Patient educationConclusion: Patient educationEssential forEssential for
Drug efficacyDrug efficacyControl of sideControl of side--effectseffects
Major role ofMajor role ofDoctorsDoctorsPharmacistsPharmacistsNursesNursesPatient advocatesPatient advocatesIndustry ?Industry ?
Respective roles could differ from country to countryRespective roles could differ from country to country
Multidisciplinary approach neededMultidisciplinary approach needed

A. A. AStierAStier ,,BavBavèènene, 28 juin 2008, 28 juin 2008
ThankThank youyou !!