Embed Size (px)
Citation preview

43
EFFICACY OF SOMATOSTATIN IN A PATIENTWITH CARCINOID SYNDROME
SIR,-Patients with carcinoid tumours present complica-tions, particularly during anxsthesia and surgery, because ofthe secretion of vasoactive peptides. These peptides may causehypertension, hypotension, bronchospasm, hyperglycaemia,diarrhoea, and electrolyte disturbances. There may also be dif-ficulty in waking the patient up after an operation.’ Somato-statin, a naturally occurring tetradecapeptide, blocks theaction of some peptide hormones,2 and, since some of thesehormones are vasoactive,3 we thought that somatostatin mightcontrol the symptoms of carcinoid syndrome.A man of 63 with alcoholic liver disease presented complain-
ing of profuse diarrhoea and fainting. He subsequently hadseveral hypotensive episodes. He had no obvious cardiac dis-ease. His urinary levels of 5-hydroxyindoleacetic acid(5-H.I.A.A.) and cortisol were high and his serum-calcium waslow. These results pointed to a multiple-hormone-secretingtumour. Angiography confirmed a tumour in the region of theterminal ileum.
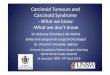
Radial-artery pressure after manipulation of carcinoid tumourand intravenous injection of somatostatin.
The patient was prepared for surgery with somatostatin andmethyldopa. His diarrhoea stopped and his blood-pressurebecame stable, although there was no reduction in the urinary5-H.I.A.A. levels. 1 h before surgery he was given diazepam 5mg and promethazine 25 mg intramuscularly. Ansesthesia wasinduced with thiopentone and intubation was performed underpancuronium. Intermittent positive-pressure ventilation withnitrous oxide and oxygen and increments of fentanyl and pan-curonium were given to maintain anaesthesia. Radial arteryand central venous pressures, expiratory CO2, and electro-cardiogram were recorded.Laparotomy revealed a large tumour in the mesentery and
terminal ileum. The liver was grossly cirrhotic but without evi-dence of metastases. During manipulation of the tumour thepatient experienced three hypotensive episodes, all quickly cor-rected by bolus intravenous injection of 1.5-3.0 µg/l somato-statin per kg body-weight. The arterial recording of the secondepisode is shown in the figure. Both diastolic and systolicblood-pressure rose promptly. No change was observed in theblood-glucose, central venous pressure, or electrocardiogram.
Anaesthesia was readily reversed and the patient was awakeon extubation. Somatostatin was given twice postoperativelyduring the first 24 h to control hypotensive crises.
Somatostatin in this patient proved to be a valuable thera-peutic agent in the management of carcinoid syndrome, par-ticularly in controlling the dangerous complication of hypoten-sion during surgery. We are now investigating the mechanismof action of somatostatin in patients with hormone-producingtumours.
LARS THULINHANS SAMNEGÅRDGUNNAR TYDÉN
Department of Surgery,Karolinska Institutet,Serafimer Hospital,112 83 Stockholm, Sweden
DAVID H. LONGUniversity Department of Anætsthesia,Bristol Royal Infirmary
SUAD EFENDIĆDepartment of Endocrinology,Karolinska Hospital, Stockholm
1. Mason, R. A , Steane, P. A. Anæsthesia, 1976, 31, 228.2. Efendić, S., Lins, P E . Uvnäs-Wallensten, K. Ann. clin. Res. in the press.3. Thulin, L., Samnegard, H. Acta chir scand 1978, 482, 73.
ATROPINE SUPPRESSION TEST FOR PANCREATICPOLYPEPTIDE
SIR,—Dr Taylor and colleagues (April 22, p. 845) showedthat pancreatic polypeptide (PP) concentrations in plasmacould not be used as a marker for gastrinomas. We agree: noneof our twelve patients with the Zollinger-Ellison syndrome(J. G. Stage, F. Stadil, and T. W. Schwartz, unpublished) hadplasma-PP values above 240 pmol/l, the limit suggested to bea marker for pancreatic endocrine tumours.’ Although pan-creatic endocrine tumours are often mixed, PP cells are notencountered more often in such tumours than other endocrinecell types.3 However, PP-cell hyperplasia is frequently found tobe associated with vipomas, insulinomas, glucagonomas, andsomatostatinomas (islet-cell hyperplasia type n of Larsson).2-4Gastrinomas are associated with quite another type of hyper-plasia involving mainly the insulin and glucagon cells (islet-cellhyperplasia type 1).4 In accordance with these morphologicalobservations Floyd et al. found, in insulinoma patients, thatPP levels were unaffected by removal of the tumour. Further-more, the Hammersmith group now reports that PP levels areraised preferentially in patients with vipomas.6 However, pa-tients with non-pancreatic vipomas have normal PP levels inplasma.’ Thus, a raised PP concentration in a patient withwatery diarrhoea suggests that the cause lies in the pancreas.2,7
For the following reasons, the plasma-PP in a fasting pa-tient is a poor discriminator:
(1) The distribution of PP concentrations in healthy subjects is
skew, with a long tail towards high concentrations (Taylor et al.).
1. Polak, J. M., Bloom, S. R., Adrian, T. E., Heitz, P. H., Bryant, M. G.,Pearse, A. G. E. Lancet, 1976, i, 328.
2. Larsson, L.-I., and others Am. J. Path. 1976, 85, 675.3. Larsson, L.-I., and others Lancet, 1977, i, 666.4. Larsson, L.-I. Virchows Archiv A, 1977, 376, 209.5. Floyd, J. C., Fajans, S. S., Pek, S., Chance, R. E. Rec. Progr. Horm. Res.
1977, 33, 519.6. Adrian, T. E., Bloom, S. R., Besterman, H. S., Bryant, M. G. in Gut Hor-
mones (edited by S. R. Bloom); p. 254. Edinburgh, 1978.7. Bloom, S. R. ibid. p. 583.
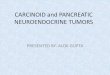
Atropine Suppression Test in Eleven Patients with DuodenalUlcer.
Arrows indicate intravenous injection of 1 mg atropine. Median(), interquartile (hatched areaB and total (line) range areshown.