Embed Size (px)
Citation preview

EFFECTS OF ORTHODONTIC APPLIANCES ON
DIAGNOSTIC QUALITY OF MR IMAGES OF THE
HEAD
By
Dzmitry Zhylich
A thesis submitted in conformity with the requirements
for the degree of Master of Science (Orthodontics)
Graduate Department of Dentistry
University of Toronto
© Copyright by Dzmitry Zhylich, 2015

ii
EFFECTS OF ORTHODONTIC APPLIANCES ON DIAGNOSTIC QUALITY OF MR IMAGES OF THE
HEAD
Dzmitry Zhylich
MSc Degree, 2015
Discipline of Orthodontics, Faculty of Dentistry, University of Toronto
Toronto, Ontario, Canada
Abstract
Introduction: The influence of four common fixed orthodontic appliances on artifact formation and
diagnostic quality of head MR images produced by a 3 Tesla MR scanner was studied. Methods:
Stainless steel brackets, ceramic brackets, combination of ceramic brackets and steel molar tubes, and
multistranded steel mandibular lingual retainers were embedded into custom made Essix® trays for each
of 10 adult subjects. Head MR scans of nine regions were acquired for each subject wearing these trays.
Sagittal T1-weighted, axial T2-weighted, axial gradient-recalled, axial diffusion-weighted, non-contrast
axial MR angiography and axial fluid-attenuated inversion recovery MR sequences were included. Two
neuroradiologists evaluated image distortions and diagnostic qualities of the 13860 acquired images.
Results: Images were affected by appliance, head region and MR sequence. Conclusions: Head MR
images are differentially affected by the presence of orthodontic appliances. The appliance, region imaged
and MR sequence need consideration before imaging patients wearing different fixed orthodontic
appliances.

iii
Acknowledgments:
I would like to express my sincere gratitude to my primary supervisor Dr. Sunjay Suri for the
idea of the project and his great support and guidance through and through. I would also like to
thank my knowledgeable committee members: Dr. Bryan Tompson, Dr. Wendy Lou and Dr.
Andrea Doria for their advice and input during this study. I very much appreciate the work of the
radiologists Dr. Pradeep Krishnan and Prakash Muthusami who spent long hours reading
thousands of images as well as Dr. Manohar Shroff’s support and expertise.
My sincere thanks goes to very accommodating and professional MR technicians Ms. Tammy
Rayner-Kunopaski and Ms. Ruth Weiss.
I am very grateful to my patient colleagues who participated in the study.
Finally, I would like to thank my family, especially my wife Irina, son Antony and my mother
Safiya whose love and support gave me inspiration and strength to complete the project.

iv
Table of contents:
Chapter Page
1. Introduction 1
1.1 Orthodontic appliances and MRI 1
1.2 Current state of the literature on orthodontic appliances in MRI 3
1.3 Purpose and statement of the problem 4
1.4 Aims and objectives 4
1.5 Hypothesis 5
2. Materials and methods 6
2.1 Study sample 6
2.2 Consent 7
2.3 Appliances tested 7
2.4 Procedures 8
2.5 Pilot test 9
2.6 Main study 12
2.7 Statistical analysis 17
3. Results 18
3.1 Pilot test: assessment of MR image distortion produced by the Essix® tray 18
material
3.2 Main study: comparison of the distortion scores between different subjects 18
3.3 Comparison of the distortion scores between different anatomic regions 25
3.4 Comparison of the distortion scores between different MR sequences 31

v
3.5 Comparison of the distortion scores of different orthodontic appliances 37
3.6 Calculation of inter and intrarater agreements 71
4. Discussion 73
4.1 Scientific novelty of the study 74
4.2. Explanation of findings 76
4.3 Recommendations for clinical practice. 80
4.4 Strengths and limitations of the study 82
4.5 Recommendations for future studies 84
5. Conclusions 86
6. Bibliography 87
7. Appendices 91
7.1 University of Toronto Research Ethics Board approval 91
7.2 The Hospital for Sick Children Research Ethics Board approval 93
7.3 Invitation letter to subjects for participation 94
7.4 Research consent form 98
7.5 MRI screening form 108
7.6 Case Report Form 109
7.7 Randomized order of the appliances for 10 subjects 110
7.8 Representative sagittal and axial images for scores 1 to 5 111

vi
List of figures:
Figure Description Page
1. Appliances tested 13
2. Complete sets of maxillary and mandibular appliances 14
3. Flowchart of image acquisition 16
4. Mean distortion scores by the appliance type for each subject 20
5. Diagnostic scores for stainless steel brackets and tubes for each subject 21
6. Diagnostic scores for ceramic brackets for each subject 22
7. Diagnostic scores for ceramic brackets and stainless steel buccal tubes for each 23
subject
8. Diagnostic scores for ceramic brackets for each subject 24
9. Mean diagnostic scores for different appliances for each anatomic region 26
10. Diagnostic scores for stainless steel brackets and tubes for each anatomic region 27
11. Diagnostic scores for ceramic brackets for each anatomic region 28
12. Diagnostic scores for ceramic brackets and stainless steel buccal tubes for each 29
anatomic region
13. Diagnostic scores for lingual retainer for each anatomic region 30
14. Diagnostic scores of different appliances for each sequence 32
15. Diagnostic scores for stainless steel brackets and tubes for each MR sequence 33
16. Diagnostic scores for ceramic brackets for each MR sequence 34
17. Diagnostic scores for ceramic brackets and stainless steel tubes for each MR 35
sequence
18. Diagnostic scores for lingual retainer for each MR sequence 36

vii
19. Mean diagnostic scores for different anatomic regions according to the MR 39
sequence for the appliance type: stainless-steel brackets and buccal tubes
20. Diagnostic scores for stainless steel brackets and tubes for sagittal T1 sequence 40
according to anatomic regions
21. Diagnostic scores for stainless steel brackets and tubes for axial T2 sequence 41
according to anatomic regions
22. Diagnostic scores for stainless steel brackets and tubes for axial gradient-recalled 42
sequence according to anatomic regions
23. Diagnostic scores for stainless steel brackets and tubes for axial diffusion-weighted 43
sequence according to anatomic regions
24. Diagnostic scores for stainless steel brackets and tubes for axial MRA sequence 44
according to anatomic regions
25. Diagnostic scores for stainless steel brackets and tubes for axial FLAIR sequence 45
according to anatomic regions
26. Mean diagnostic scores for different anatomic regions according to the MR sequence 47
for the appliance type: ceramic brackets
27. Diagnostic scores for ceramic brackets for sagittal T1 sequence according to 48
anatomic regions
28. Diagnostic scores for ceramic brackets for axial T2 sequence according to anatomic 49
regions
29. Diagnostic scores for ceramic brackets for axial gradient-recalled sequence 50
according to anatomic regions
30. Diagnostic scores for ceramic brackets for axial diffusion-weighted sequence 51

viii
according to anatomic regions
31. Diagnostic scores for ceramic brackets for axial MRA sequence according to 52
anatomic regions
32. Diagnostic scores for ceramic brackets for axial FLAIR sequence according to 53
anatomic regions
33. Mean diagnostic scores for different anatomic regions according to the MR 55
sequence for the appliance type: ceramic brackets and stainless steel buccal tubes
34. Diagnostic scores for ceramic brackets + steel buccal tubes for sagittal T1 56
sequence according to anatomic regions
35. Diagnostic scores for ceramic brackets + steel buccal tubes for axial T2 sequence 57
according to anatomic regions
36. Diagnostic scores for ceramic brackets + steel buccal tubes for axial 58
gradient-recalled sequence according to anatomic regions
37. Diagnostic scores for ceramic brackets + steel buccal tubes for axial 59
diffusion-weighted sequence according to anatomic regions
38. Diagnostic scores for ceramic brackets + steel buccal tubes for axial MRA 60
sequence according to anatomic regions
39. Diagnostic scores for ceramic brackets + steel buccal tubes for axial FLAIR 61
sequence according to anatomic regions
40. Mean diagnostic scores for different anatomic regions according to the MR 63
sequence for the appliance type: lingual retainer
41. Diagnostic scores for lingual retainer for sagittal T1 sequence according to anatomic 64
regions

ix
42. Diagnostic scores for lingual retainer for axial T2 sequence according to anatomic 65
regions
43. Diagnostic scores for lingual retainer for axial gradient-recalled sequence according 66
to anatomic regions
44. Diagnostic scores for lingual retainer for axial diffusion-weighted sequence according
66
to anatomic regions
45. Diagnostic scores for lingual retainer for axial MRA sequence according to anatomic 68
regions
46. Diagnostic scores for lingual retainer for axial FLAIR sequence according to 69
anatomic regions
47. Approximate relative distances from the orthodontic appliances to the anatomic 77
regions of the head assessed in the study

x
List of tables:
Table Description Page
Table 1: Parameters of the MR sequences used 10
Table 2: Modified ROC (receiver operating characteristic) score system used for 11
MR image diagnostic quality determination
Table 3: Mean distortion scores with standard deviations (in brackets) by the 19
appliance type for each subject, overall mean distortion scores for each
appliance and pairwise comparisons with scores of ceramic brackets
Table 4: Mean distortion scores with standard deviations for different appliances 25
according to the anatomic regions
Table 5: Mean distortion scores with standard deviations for different appliances 31
according to the imaging sequence
Table 6: Mean diagnostic scores with standard deviations for different anatomic 38
regions according to the MR sequence for the appliance type: stainless steel
brackets and buccal tubes
Table 7: Mean diagnostic scores with standard deviations for different anatomic 46
regions according to the MR sequence for the appliance type: ceramic brackets
Table 8: Mean diagnostic scores with standard deviations for different anatomic 54

xi
regions according to the MR sequence for appliance type: ceramic brackets
and stainless steel buccal tubes
Table 9: Mean diagnostic scores with standard deviations for different anatomic 62
regions according to the MR sequence for appliance type: lingual retainer
Table 10: Intrarater agreements for reviewers 1 and 2 72
Table 11: Clinical recommendations for cranial MR imaging with 4 commonly 81
used orthodontic appliances and 6 common MR sequences

xii
List of abbreviations:
MRI: Magnetic Resonance Imaging
MR Magnetic Resonance
TMJ: Temporomandibular Joint
ECG: Electrocardiography
GRE: Gradient recalled
DWI: Diffusion-weighted
FLAIR: Fluid Attenuation Inversion Recovery
MRA: Magnetic Resonance Angiography
T: Tesla
RMO: Rocky Mountain Orthodontics
AO: American Orthodontics
SEMAC: Slice Encoding for Metal Artifact Correction
MAVRIC: Multiacquisition Variable Resonance Image Combination
SAR: Specific Absorption Rates
M: Metal
C: Ceramic

xiii
TMA: Titanium Molybdenum Alloy
C+M: Ceramic + Metal
LR: Lingual Retainer
N Number
ROC Receiver Operating Characteristic

1
CHAPTER 1.
Introduction
Magnetic resonance imaging (MRI) is a diagnostic modality widely used in medicine and
dentistry for soft tissue imaging. MRI is indispensable when investigating soft tissue tumors,
including those of the head and neck1, TMJ pathology
2, cardiovascular pathology
3, seizures
4 and
cerebral palsy.5 In addition, new applications for MR 3D hard tissue images are emerging.
6 MRI
offers several advantages. It offers the best resolution of soft tissues and does not involve
ionizing radiation.7 The number of MR scans that are conducted is steadily increasing each year.
For example, in the US, the estimated annual number MRI procedures is 26 million every year.8
An MR image is obtained by manipulating protons within the body by a very strong
magnetic field9. Metallic objects within the body including common orthodontic appliances can
produce artifacts on MR images, which are defined as distortions of signal intensity or voids that
do not have any anatomic basis in the plane being imaged.10
These artifacts are caused by a)
differences in magnetic susceptibility between the metallic object and the adjacent tissues
regions11
and b) by magnetic fields caused from eddy currents induced in the object by the
excitation radio frequency field or switched gradient fields.12,13
Artifacts caused by a metallic
object depend on the material of the object (its magnetic susceptibility and electric conductivity),
the object size, shape, orientation in magnetic field, and on the parameters of the MR scan.13

2
1.1 Orthodontic appliances and MRI
Costa et al. (2009)14
in a retrospective analysis of MR images in a university medical
center, revealed artifacts in 6% of all head scans and it was found that orthodontic appliances
produced 78% of all the artifacts. Fixed orthodontic treatment is relatively common and
increasingly prescribed for children and adults.15
It involves having orthodontic attachments
(braces) that are fixed in the patients’ mouth for the duration of treatment, which generally lasts
24-30 months.16
Orthodontic treatment is routinely followed by long-term retention to maintain
the treatment result. This usually includes a metallic wire that is fixed to the lingual surfaces of
the lower anterior teeth, and remains in situ for several years, even decades after the active
treatment with fixed appliances has been completed.17
Patients with fixed multibracket orthodontic appliances (braces) occasionally require MR
examinations of the head and neck region. While it is known that fixed multibracket orthodontic
appliances cause image artifacts on MR images, the extent and severity of image loss is not clear
from the literature. Consequently, to circumvent the problem of image artifacts caused by
orthodontic appliances, orthodontists are often requested to remove fixed orthodontic appliances
or fixed retainers before the planned MR scan, or orthodontic hardware is removed in emergency
rooms of the hospitals before an urgent MR examination.18,19
This increases the financial and
biological burdens since removal and later reinstallation of fixed orthodontic appliances is costly
and labor intensive.20
Debonding is also accompanied by risks of potential enamel loss21
,
tearouts21
and cracks.22
Because of the increase in orthodontic treatment utilization, the long-
term use of fixed lingual bonded metallic wire retainers and the ever rising utilization of MRI
each year, the problem of MR image loss from fixed orthodontic appliances is likely to become
even more significant in years to come.

3
1.2 Current state of the literature on orthodontic appliances in MRI
There have been a number of studies published on the subject of MRI artifacts produced
by dental materials. Lissac et al. (1991)23
found that precious alloys, dental ceramics, amalgams
and composite materials did not cause MR image distortion whereas titanium caused slight
image artifacts, and base alloys caused considerable artifacts. Abbaszadeh et al. (2000)24
found
that gold alloy and amalgam produced small artifacts while gold alloy produced large artifacts.
Although there are a number of studies that investigated artifacts on MR images of the head
caused by orthodontic appliances, the matter still remains controversial and unclear.14
Sadowsky
et al. (1988)9, Hinshaw et al. (1988)
25 found that artifacts caused by stainless steel bracket and
wires do cause some distortion of the MR image of the brain, but it still remains diagnostic. On
the other hand, a number of other studies confirmed that orthodontic appliances can render TMJ
and brain MR images undiagnostic.26,27
Some authors reported that titanium causes only minor
artifacts28-30
while other researchers stated the opposite.14,25
In addition, the effects of different
types of commonly used fixed orthodontic appliances on the MR image quality have not been
studied systematically. Elison et al. 26
undertook a structured investigation to study MR image
distortions caused by steel, ceramic, composite, and titanium brackets on images acquired using
an MR scanner with a 1.5 T magnet. Ceramic brackets without metal slot, composite and
titanium brackets were found not to have caused significant distortion on the MR images taken
with 1.5 Tesla strength scanner.19,26
In current practice of diagnostic imaging, 3 Tesla MR machines are becoming
increasingly popular because they offer better image resolution.26
Since the width of the artifact

4
depends on the strength of the magnetic field among other factors, an MRI compatible device
with a 1.5 T scanner might not be compatible with a 3T scanner.13,31,32
Elison et al 26
determined
that of the two types of steel commonly used in fixed orthodontic appliances, 18-8 stainless steel
did not cause deformation of the MRI image in vitro as opposed to type 17-4 stainless steel that
did. Although plastic and composite brackets might be compatible with MRI scanners, they have
several problems related to material performance such as bracket deformation under stress,
especially with torque expression, decreased wear resistance.33,34
These drawbacks have
prevented plastic and composite brackets from routine use in most clinical orthodontic practices.
1.3. Purpose and statement of the problem
Commonly used fixed orthodontic appliances cause image distortions of MR images of
the head and are therefore often required to be removed before the scanning is undertaken. The
effects of routine orthodontic appliances made of different types of materials on MRI artifact
formation, when used in a 3T MR scanner have not been studied in detail in a systematic manner
to elucidate the extent and severity of the artifact on the diagnostic quality of the MR images.
Consequently, there is a lack of consensus regarding the best practice protocols to be employed
for patients who need MR imaging during the period of their fixed orthodontic appliance
treatment or retention with fixed retainers.

5
1.4 Aims and Objectives
To investigate in-vivo, the influence of selected commonly used orthodontic appliances:
stainless steel brackets and molar buccal tubes, ceramic brackets, combination of ceramic
brackets and stainless steel molar buccal tubes, multistranded stainless steel lingual retainer on
the extent of artifact formation and the diagnostic quality of the MR images of the head obtained
by a 3 Tesla MR scanner using common MR image modalities.
1.5 Hypothesis
Commonly used stainless steel brackets, buccal tubes and lingual retainers cause
significant MR image distortion on 3T MR scanners to render the image nondiagnostic for MR
investigations of all the regions of the head.

6
CHAPTER 2
Materials and Methods
This clinical study assessed the influence of commonly used orthodontic appliances on
the extent of artifact formation and the diagnostic quality of the MR images of the head in a
sample of 10 adult volunteers. The study protocol, case report forms, patient consent forms and
the invitation letters were approved by the University of Toronto Research Ethics Board
(#30332, appendix 1) and the SickKids Research Ethics Board (#1000045973, appendix 2) prior
to commencing the study.
2.1 Study sample
10 healthy adult participants who were recruited from among staff and students and
patients at the Faculty of Dentistry, University of Toronto, and among staff at The Hospital for
Sick Children Toronto, through posting an invitation to participate (appendix 3) at prominent
sites in the Faculty of Dentistry, University of Toronto and in The Hospital for Sick Children:
Inclusion criteria:
Adults of both sexes who were informed about the purpose, benefits and risks of the
study and consented to participate.
Exclusion criteria:
1. Pregnant women.35

7
2. Individuals having metal objects in the body (e.g. aneurysm clips, pacemakers, fixed
orthodontic appliances, crowns and bridges, implants, amalgam restorations, traditional and
cosmetic tattoos etc).
3. Individuals who needed sedation before MRI.
4. Individuals wearing drug patches36
5. Individuals having any monitoring equipment (such as ECG leads or respiratory monitoring
leads) attached to their bodies.
2.2 Consent
An invitation letter (Appendix 3) describing the study and explaining its benefits and
risks and the compensation for participation were given to the volunteers. The informed consent
form (Appendix 4) was thoroughly reviewed with the participants. Informed consent was
obtained from each volunteer before the commencement of the study. There were 6 males and 4
females in the sample ages. Their median age was 29 years.
2.3 Appliances tested
a) Stainless steel brackets made of 17-4 and 18-8 stainless steel components brazed together with
silver alloy for all teeth erupted anterior to the first permanent molars, and bondable tubes for the
molars made of the same materials in both, maxillary and mandibular arches. (Mini Master®,
American Orthodontics, Sheboygan, WI)

8
b) Ceramic brackets for all teeth erupted anterior to the first permanent molars in both, maxillary
and mandibular arches, without any metal attachments for any teeth. (monocrystalline aluminum
oxide, Radiance®, American Orthodontics, Sheboygan, WI).
c) Ceramic brackets for all teeth erupted anterior to the first permanent molars in both, maxillary
and mandibular arches and with 18-8 stainless steel single piece bondable molar tubes for the
molars in both, maxillary and mandibular arches. (Radiance®, American Orthodontics,
Sheboygan, WI and FLI®, Rocky Mountain Orthodontics, Denver, CO).
d) Mandibular 18-8 stainless steel multistranded wire 3-3 retainer (Tri-Flex®, Rocky Mountain
Orthodontics, Denver, CO).
2.4 Procedures
The appliances listed above were placed in close contact with the subjects’ teeth, by
incorporating them into a clear 0.035’ Essix ACE® (GAC International, Bohemia, NY) retainer
in a manner similar to that used in indirect bracket bonding. This allowed the Essix® retainer to
be snapped on to the teeth for undertaking the tests in the MR scanner, obviating the need to
actually bond and debond these appliances for each subject. The Essix® material used in this
study has previously been used in MRI research26,27
and was reported not to have caused any
measurable MR image deformation in 1.5 and 0.5 Tesla MR scanners. To determine whether the
Essix® retainer causes any significant MR image deformation under the conditions of the current
study in a 3T MR scanner, a pilot test was done on one volunteer.

9
2.5 Pilot test
Maxillary and mandibular polyvinylsiloxane (Reflection®, Patterson Dental, Saint Paul,
MN) impressions (putty wash technique) were taken for one subject, and 4 sets of dental stone
models were poured from the impressions. Maxillary and mandibular Essix retainers were
fabricated on the models using Biostar® (Great Lakes Orthodontics, Tonawanda, NY) machine.
Similarly, the 4 appliances tested in the current study (listed in 2.3) were placed on the models
using indirect bonding with Transbond® (3M Unitek, Monrovia, CA). The appliances were
incorporated into the maxillary and mandibular Essix retainers that were made over them using
Biostar® machine. The retainers were checked for fit and comfort and adjusted as necessary.
Following this step, MR scans were acquired at the Hospital for Sick Children, Toronto. MR
scans were acquired for the volunteer in a 3T Siemens MAGNETOM® MRI machine (Siemens,
Erlangen, Germany) using a 12-channel head coil, with and without the Essix retainers, as well
as with 4 selected orthodontic appliances in random order, using the following sequences:
sagittal T1-weighted, axial T2–weighted, axial gradient-recalled, axial diffusion-weighted, non-
contrast axial magnetic resonance angiography (MRA), axial fluid attenuated inversion recovery
(FLAIR). The parameters of the above sequences are listed in Table 1.

10
Table 1. Parameters of the MR sequences used.
Sequence TR/TE
(msec)
Slice
thickness
(mm)
Gap
(mm)
Band
width
(Hz/Px)
Flip
angle
(degr.)
Matrix Scan
time
(min:sec)
Sagittal
T1-
weighted
1950.0/4.4 1.0 - 140 12 256x256 4:14
Axial
T2–
weighted
4500.0/83.0 3.5 - 219 120 256x256 1:54
Axial
gradient-
recalled
620.0/20.0 3.5 - 200 20 256x256 4:16
Axial
diffusion-
weighted
5000.0/93.0 4.0 - 1184 - 192x192 1:37
Axial
MRA
20.0/3.6 0.5 10 165 18 384x384 5:18
Axial
FLAIR
9000.0/88.0 3.5 - 271 120 256x256 3:56
TR-repetition time, TE-echo time, msec - milliseconds, Hz/Px-hertz/pixels, degr.-degrees, min :
sec-minutes : seconds, MRA-magnetic resonance angiography, FLAIR-fluid attenuation
inversion recovery.
The participant was screened before the scans (MRI screening form, Appendix 5), ear plugs were
provided to reduce the noise levels, and an emergency signaler was given to the participant.
After the scout scans, alignment of the images was adjusted by the MRI technician according to
the accepted neuroanatomical landmarks. Since the orthodontic appliances were securely
embedded into the Essix appliance which was firmly retained on the subject’s teeth, there were
no special precautions taken regarding possible dislodgement of the appliances. No special
precautions were taken regarding possible heating of the appliances as previous studies found
appliance temperature changes clinically insignificant, within 1 degree.37
Resultant images were
analyzed by a panel of 2 neuroradiologists who were routinely assigned to read MR scans of the

11
brain and TMJ. The diagnostic value of the scans with and without Essix retainers was
determined using a modified ROC (receiver operating characteristic) score system described by
Elison et al26
(Table 2).
Table 2. Modified ROC (receiver operating characteristic) score system used for MR image
diagnostic quality determination.
Score Image appearance Diagnostic/Nondiagnostic
1 No distortion/Artifact Diagnostic
2 Minimal distortion/Artifact Diagnostic
3 Moderate distortion/Artifact Moderately diagnostic
4 Severe distortion Nondiagnostic
5 Complete obliteration Nondiagnostic
In this particular method of distortion classification, the score of 3 represents a cut-off for
clinical usability. This means that images with the score of 3 have moderate distortion/artifact,
but still can be used for diagnosis. To develop verbal definitions of each distortions score,
images acquired were discussed between the reviewers and another neuroradiologist, the head of
Diagnostic Imaging at The Hospital for Sick Children, Toronto to establish consensus in regard
to the definitions of the scores described in Table 2.
Nine regions of the head were assessed:
a) Base of the tongue
b) Hard palate
c) Body of the mandible

12
d) Nasopharynx
e) Globes of the eyes
f) Pituitary gland
g) Frontal lobe
h) Temporal lobe
i) Brain stem
For the axial diffusion-weighted and axial gradient-recalled sequences, only brain regions of
frontal lobe, temporal lobe and brain stem were assessed as these sequences are routinely used
for assessment of the brain regions and inclusion of the other anatomic regions would have
resulted in artificially increased distortion scores for these sequences. No score was assigned to
the anatomic region if it was not included in the scan.
Whether a statistically significant difference existed in the diagnostic score of the scans with and
without Essix retainers was determined by using non-parametric Wilcoxon signed rank test.
2.6 Main study
Following the pilot test, maxillary and mandibular polyvinylsiloxane impressions were
taken for all the participants. 3 sets of dental stone models were poured from the impressions and
trimmed. Separating agent was applied on all the models. For each subject, the 4 appliances
listed in section 2.3 were placed on the models using indirect bonding with Transbond® (3M
Unitek, Monrovia, CA). One set of models was used to fabricate Essix trays with ceramic
brackets and separate Essix trays for the metal molar buccal tubes. This allowed using the same
trays with ceramic brackets as a separate appliance and in combination with metal buccal tubes.

13
The appliances were incorporated into the maxillary and mandibular Essix® retainers using
Biostar® machine. The retainers were checked for fit and comfort and adjusted if necessary. Fig.
1 demonstrates the appliances tested.
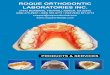
Fig.1. Appliances tested: a) Stainless steel brackets and buccal tubes; b) Ceramic brackets; c)
Ceramic brackets and stainless steel molar buccal tubes; d) Stainless steel mandibular lingual
retainer
a) b)
c) d)

14
Note: Only maxillary arch appliances are shown here for steel brackets and bucal tubes, ceramic
brackets, and the combination of ceramic brackets and steel molar buccal tubes. In the tests,
similar appliances were made for the maxillary and mandibular arches as shown in Fig.2.
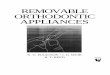
Fig.2. Complete sets of maxillary and mandibular appliances: a) Stainless steel brackets and
buccal tubes; b) Ceramic brackets; c) Ceramic brackets and stainless steel molar buccal tubes;
a) b)
c)

15
MR scans were taken for the participants with a 3T MRI scanner using a head coil with
the appliances listed in 2.3 embedded into Essix trays, in random order using the following
sequences: sagittal T1-weighted, axial T2 –weighted, axial gradient-recalled (GRE), axial
diffusion-weighted (DWI), non-contrast axial magnetic resonance angiography (MRA), and axial
fluid attenuated inversion recovery (FLAIR).The parameters of the above sequences were the
same as in the pilot test. The total time each participant spent in the MR department of the
Hospital was around 2 hours. Resultant images were analyzed by the same 2 neuroradiologists
described in the pilot study, who were routinely assigned to read MR scans of the brain and TMJ.
The images of the subjects were reviewed randomly and not in sequence form 2 to 10.The nine
regions of the head described in the pilot study were assessed using the diagnostic score system
described earlier. For the diffusion-weighted and gradient-recalled sequences, only brain regions
of frontal lobe, temporal lobe and brain stem were assessed as these sequences are routinely used
for assessment of the brain regions and inclusion of the other anatomic regions would have
resulted in artificially increased distortion scores for these sequences. No score was assigned to
the anatomic region if it was not included in the scan. The data from the pilot test were included
in the final analysis of data from a total of 10 subjects (Case report form, Appendix 6). Figure 3
represents a flowchart of image acquisition.

16
Fig. 3 Flowchart of image acquisition (for 1 subject).
For intrarater reliability assessment, each radiologist was asked to re-evaluate 3 randomly
selected subjects.26
Reviewer 1 re-assessed subjects 9, 3, and 4. Reviewer 2 re-evaluated subjects
6, 2 and 9. The assignment of cases for re-evaluation was based on the computer-generated
random number allocation.

17
2.7 Statistical analysis
Statistical analysis was performed using SPSS 21 (SPSS , Chicago, Ill):The following tests were
used:
1. Kappa statistics for agreement within and between the raters. The diagnostic scores were
grouped: 1-3 were reassigned as 1 (diagnostic scan), 4-5 were assigned 2 (nondiagnostic
scan).26
2. Wilcoxon signed rank test for the differences between materials, anatomic sites, imaging
sequences with regard to the image distortion scale rating. This non-parametric test was
used because of the non-normal distribution of the distortion scores as was determined by
Shapiro-Wilk test.
A p value of less than 0.05 was chosen to indicate statistical significance.

18
CHAPTER 3
Results
3.1 Pilot test: assessment of MR image distortion produced by the Essix® tray
material
In the pilot test, mean diagnostic score for Essix® appliance was 1.89±1.382 (all
appliances, sequences and reviewers were included, 76 images were analyzed). Mean diagnostic
score for no appliance was 1.89±1.362 (all appliances, sequences and reviewers were included,
76 images were analyzed). There were no statistically significant differences between the
distortion scores for Essix® and no appliance (p=1.00, Wilcoxon Signed Rank test). Mean
diagnostic score for ceramic brackets was 1.82±1.382 (all appliances, sequences and reviewers
were included, 78 images were analyzed). There were no statistically significant differences
between the distortion scores for ceramic brackets and no appliance (p=1.00, Wilcoxon Signed
Rank test). Therefore, scans with no appliances were not performed for the subsequent subjects
to decrease the burden on the participants and redundant use of highly specialized equipment and
resources, and scores for ceramic brackets could arguably serve as a gold standard for
comparisons between different appliances.
Main study.
Examples of representative sagittal and axial images for scores 1 to 5 are given in Appendix 8
(frontal lobe of the brain was scored).
3.2 Comparison of the distortion scores between different subjects
Mean distortion scores of different appliances for each subject, overall mean distortion scores for
each appliance and pairwise comparisons with ceramic brackets are given in Table 3.

19
Table 3. Mean distortion scores with standard deviations (in parentheses) by the appliance type for each
subject, overall mean distortion scores for each appliance and pairwise comparisons with scores of
ceramic brackets (included all sequences, anatomic regions and reviewers).
Subject Stainless steel Ceramic Ceramic+Stainless steel Lingual Retainer
1
N for each appliance=66
Mean (SD)
2.61 (1.68)
Mean (SD)
1.39 (0.78)
Mean (SD)
2.09 (1.37)
Mean (SD)
1.67 (0.9)
2
N for each appliance=66
2.89 (1.59) 1.59 (0.88) 2.18 (1.4) 1.85 (1.07)
3
N for each appliance=66
2.68 (1.6) 1.7 (0.79) 2.32 (1.43) 1.74 (0.98)
4
N for each appliance=66
2.97 (1.53) 1.89 (0.93) 2.52 (1.43) 1.86 (0.99)
5
N for each appliance=66
2.65 (1.53) 1.67 (0.85) 2.29 (1.29) 1.82 (0.89)
6
N for each appliance=66
2.73 (1.62) 1.58 (0.88) 2.38 (1.38) 1.91 (0.94)
7
N for each appliance=66
2.8 (1.34) 1.59 (0.78) 2.34 (1.2) 2.08 (0.9)
8
N for each appliance=66
2.88 (1.53) 1.6 (0.82) 2.42 (1.5) 1.92 (0.92)
9
N for each appliance=66
2.94 (1.64) 2.12 (0.9) 2.35 (1.34) 2.03 (1.13)
10
N for each appliance=66
3.17 (1.38) 2.3 (1.19) 2.71 (1.23) 1.94 (1.16)
Mean scores 2.83 (1.55) 1.74 (0.93) 2.36 (1.36) 1.88 (0.99)
Ceramic vs. other material (Z)*
-18.116 - -14.638 -6.763
P value*
<0.0001 - <0.0001 <0.0001
*Wilcoxon Signed Rank test. SD-standard deviation, N-number of images

20
There were statistically significant differences between the distortion scores for stainless
steel brackets and molar tubes, combination of ceramic brackets and stainless steel molar tubes,
and lingual retainer when compared to the distortion scores for ceramic brackets.
Fig 4 demonstrates a composite view of the mean distortion scores for different
appliances according to the subject. It can be noted that mean distortion scores for subject 10
were higher than for the rest of the subjects
Fig 4. Mean distortion scores by the appliance type for each subject.

21
Figures 5-8 (box plots) demonstrate diagnostic scores variability and the differences between the
diagnostic scores for each of the 10 subjects for a specific appliance. For all the following box
plots in the Results section, the bottom and top of each box represent the first and third quartiles
respectively. Middle band represents the median. Whiskers represent data within 1.5 times the
interquartile range. Dots represent data exceeding 1.5 times the interquartile range (outliers).
Stars represent data exceeding 3 times the interquartile range (extreme values).
Fig.5

22
For stainless steel brackets and tubes, almost all mean diagnostic scores were close to
nondiagnostic range between 2.5 and 3.0. Only for subject 10, the mean distortion score was
above 3.0 (3.17). Scores for all subjects showed high variability with the minimum of 1 and
maximum of 5.
Fig.6
For ceramic brackets, most of the mean scores were in the diagnostic range between 1.5 and 2.
Mean scores for subjects 9 and 10 were 2.12 and 2.3 respectively. Notably, scores for subjects 4,
9 and 10 were higher than for the rest of the subjects with greater variability and maximum

23
scores above 3.0. Scores for almost all the subjects included several outliers above 3.0. Scores
for subject 1 showed little variability and were uniformly 1 with the exception of 2 outliers.
Fig.7
Mean diagnostic scores for the combination of ceramic brackets and stainless steel buccal tubes
were almost uniformly between 2 and 2.5 with the mean score for subject 10 notably higher,
2.71. The scores variability was high for all subjects, with minimum of 1 and maximum of 5.

24
Fig.8
For the stainless steel mandibular lingual retainer, mean diagnostic scores for most subjects
showed fairly uniform distribution with median of 2 and interquartile range of 1 to 3.Subjects 1-3
had median scores of 1. All subjects with the exception of subjects 2 and 5 had upper quartile
scores bordering the non-diagnostic range.

25
3.3 Comparison of the distortion scores between different anatomic regions
Table 4. Mean distortion scores with standard deviations (in parentheses) for different appliances
according to the anatomic regions (all subjects, MR sequences, reviewers were included).
Anatomic region Stainless steel Ceramic Ceramic + Stainless
steel
Lingual Retainer
Base of the tongue
N for each
appliance=19
Mean (SD)
4.84 (0.38)
Mean (SD)
2.20 (0.89)
Mean (SD)
4.26 (0.45)
Mean (SD)
3.00 (0.69)
Body of the mandible
N for each
appliance=20
4.90 (0.31) 2.24 (0.89) 4.74 (0.45) 2.90 (0.72)
Hard palate
N for each
appliance=20
5.00 2.50 (0.83) 4.21 (0.54) 3.85 (0.81)
Nasopharynx
N for each
appliance=80
2.04 (1.05) 1.41 (0.63) 1.84 (0.93) 1.56 (0.63)
Globes of the eyes
N for each
appliance=80
3.35 (1.31) 1.85 (0.84) 2.36 (1.15) 1.99 (0.84)
Pituitary gland
N for each
appliance=80
1.96 (0.85) 1.39 (0.65) 1.66 (0.69) 1.47 (0.65)
Frontal lobe
N for each
appliance=120
2.91 (1.50) 1.78 (0.95) 2.25 (1.27) 1.87 (0.93)
Temporal lobe
N for each
appliance=120
2.83 (1.51) 1.93 (1.14) 2.46 (1.41) 1.93 (1.08)
Brain stem
N for each
appliance=120
2.49 (1.71) 1.61 (0.91) 2.21 (1.46) 1.60 (0.85)
SD-standard deviation, N-number of images

26
Fig. 9 Mean diagnostic scores for different appliances for each anatomic region.
It can be noted that there is a general trend for the regions farther from the teeth and orthodontic
appliances to have lower diagnostic scores although it is also apparent that images for certain
tissues are more significantly affected then others despite their relatively greater distance from
the appliances compared to other regions.
Figures 10-13 (box plots) demonstrate the distortion scores for each appliance according to
anatomic region.

27
Fig.10
For stainless steel brackets and tubes, scores for intraoral regions of base of the tongue, hard
palate and body of the mandible were uniformly 5 (complete image obliteration) with the
exception of several outliers. Mean distortion scores for nasopharynx, pituitary gland and brain
stem were in the diagnostic range. Frontal lobe and temporal lobe received mean scores close to
the non-diagnostic range. Globes of the eyes had the mean score above 3. Variability of the
scores for nasopharynx, temporal lobe, frontal lobe, and brain stem was high with the lower
quartile being below 3 and upper quartile above 3.

28
Fig.11
Mean diagnostic scores for ceramic brackets for all anatomic regions were in the diagnostic
range. Scores for intraoral regions of base of the tongue, body of the mandible, hard palate, as
well as for frontal and temporal lobes showed high variability with the upper quartile bordering
the non-diagnostic range.

29
Fig. 12
For the combination of ceramic brackets and 18-8 stainless steel buccal tubes, intraoral regions
of the base of the tongue, body of the mandible, and hard palate received high scores between 4
and 5, in the non-diagnostic range. The other regions received mean scores below 3 (the cut off
for diagnostic image). Scores for nasopharynx, globes of the eyes, frontal and temporal lobes had
high variability with the median scores of 2 and the maximum scores being in the non-diagnostic
range. Frontal, temporal lobes and brain stem had an interquartile range from 1 to 4.

30
Fig. 13
For lingual retainer, mean scores for intraoral regions of base of the tongue and body of the
mandible were close to 3. Hard palate received scores in the non-diagnostic range. For the rest of
the regions, the mean scores were below 3 with the scores for globes of the eyes, frontal lobe,
and temporal lobe showing high variability with the upper quartile bordering the non-diagnostic
range.

31
3.4 Comparison of the distortion scores between different MR sequences
For axial gradient-recall and axial diffusion-weighted sequences, only the brain regions
of frontal lobe, temporal lobe and brain stem were assessed because these sequences are
routinely used for assessment of the brain regions and inclusion of the other anatomic regions
would have resulted in artificially increased distortion scores for these sequences.
Table 5 and Fig.14 illustrate mean diagnostic scores for different appliances according to the
imaging sequence.
Table 5. Mean distortion scores with standard deviations (in parentheses) for different appliances
according to the imaging sequence (all subjects, anatomic regions, and reviewers were included).
MR sequence Metal Ceramic Ceramic + Metal Lingual Retainer
Sagittal T1
N for each appliance=179
3.66 (1.23) 1.82 (0.85) 3.10 (1.22) 2.30 (1.03)
Axial T2
N for each appliance=120
2.08 (1.00) 1.40 (0.64) 1.63 (0.77) 1.44 (0.65)
Axial GRE
N for each appliance=60
4.68 (0.47) 3.10 (0.68) 4.05 (0.50) 3.03 (0.49)
Axial DWI
N for each appliance=60
4.83 (0.38) 2.93 (0.52) 4.08 (0.66) 3.02 (0.50)
Axial MRA
N for each appliance=120
1.33 (0.55) 1.18 (0.51) 1.25 (0.49) 1.15 (0.42)
Axial FLAIR
N for each appliance=120
1.93 (1.00) 1.26 (0.59) 1.40 (0.63) 1.28 (0.57)
N-number of images, SD-standard deviation, GRE-gradient recalled, DWI-diffusion-weighted,
MRA-magnetic resonance angiography, FLAIR-fluid attenuation inversion recovery

32
Fig.14.Mean diagnostic scores of different appliances for each sequence.
Figures 15-18 (box plots) demonstrate diagnostic scores and their variability for different
appliances according to the MR sequence.

33
Fig.15
For stainless steel brackets and tubes, mean diagnostic scores for sagittal T1, axial diffusion-
weighted, axial gradient-recalled sequences were above 3 (non-diagnostic). Scores for T1
sequence showed significant variability with interquartile range of 3 to 5. Mean scores for the

34
axial T2, axial FLAIR and axial MRA sequences were in the diagnostic range with the upper
quartile for T2 and FLAIR sequences bordering the non-diagnostic range.
Fig.16

35
For ceramic brackets, scores for the axial diffusion-weighted and axial gradient-recalled
sequences were uniformly 3 with the exception of several outliers. For the rest of the sequences,
the scores were in the diagnostic range.
Fig.17

36
For the combination appliance, the scores for axial diffusion-weighted (DWI) and axial gradient-
recalled (GRE) sequences were in the non-diagnostic range. For sagittal T1 sequence, the
diagnostic scores were symmetrically distributed with the median of 3 and interquartile range
from 2 to 4. The scores for axial T2, axial MRA and axial FLAIR sequences were below 3
(diagnostic).
Fig. 18

37
For lingual retainer, scores for axial DWI and axial GRE sequences were uniformly 3 with the
exception of several outliers. For sagittal T1 sequence, the scores showed variability with
interquartile range from 2 to 3 and median of 2. For the rest of the sequences, the scores were in
the diagnostic range with scores for MRA and FLAIR sequences uniformly 1, with the exception
of several outliers.
3.5 Comparison of the distortion scores of different orthodontic appliances
Table 6 and Fig.19 demonstrate mean diagnostic scores for different anatomic regions according
to the imaging sequence for stainless steel brackets and tubes.

38
Table 6. Mean diagnostic scores with standard deviations (in parentheses) for different anatomic regions
according to the MR sequence for the appliance type: stainless steel brackets and buccal tubes (included
all subjects and reviewers).
Anatomic region Sag.T1 Axial T2 Axial
GRE
Axial
DWI
Axial
MRA
Axial
FLAIR
Base of the tongue
N=19
4.84
(0.38)
- - - - -
Body of the mandible
N=20
4.90
(0.31)
- - - - -
Hard palate
N=20
5.00 - - - - -
Nasopharynx
N for each
sequence=20
3.30
(0.57)
1.75
(0.79)
- - 1.35 (0.59) 1.75 (0.97)
Globes of the eyes
N for each
sequence=20
4.65
(0.49)
3.80
(0.52)
- - 1.45 (0.69) 3.50 (0.61)
Pituitary gland
N for each
sequence=20
2.70
(0.93)
1.95
(0.51)
- - 1.45 (0.69) 1.75 (0.72)
Frontal lobe
N for each
sequence=20
3.00
(0.32)
2.10
(0.45)
4.75
(0.44)
4.75
(0.44)
1.15 (0.37) 1.7 (0.73)
Temporal lobe
N for each
sequence=20
2.70
(0.57)
1.80
(0.62)
4.60
(0.50)
4.90
(0.31)
1.35 (0.49) 1.65 (0.59)
Brain stem
N for each
sequence=20
1.95
(0.67)
1.05
(0.22)
4.70
(0.47)
4.85
(0.37)
1.20 (0.41) 1.20 (0.41)
N-number of images, SD-standard deviation, GRE-gradient recalled, DWI-diffusion-weighted,
MRA-magnetic resonance angiography, FLAIR-fluid attenuation inversion recovery

39
Fig.19 Mean diagnostic scores for different anatomic regions according to the MR sequence for
the appliance type: stainless steel brackets and buccal tubes.
Distribution and variability of the scores for stainless steel brackets and tubes for each sequence
according to the anatomic region are shown in the box plots below (figures 20-25).

40
Fig. 20
For stainless steel brackets and tubes in T1 sequence, diagnostic scores for intraoral regions were
almost uniformly 5 with the exception of several outliers. Mean diagnostic scores for the rest of
the regions were in or close to non-diagnostic range with one notable exception: brain stem
(1.96). Scores for pituitary gland showed greatest variability of 1 to 4 with a median of 3 and
interquartile range from 2 to 3.

41
Fig. 21
For T2 sequence, only globes of the eyes had a mean score above 3, the rest of the regions
received scores in the diagnostic range. Scores for nasopharynx and temporal lobe showed
significant variability with a range from 1 to 3.

42
Fig. 22

43
Fig. 23
For axial gradient-recalled and axial diffusion-weighted sequences, the scores for stainless steel
brackets and tubes were uniformly above 3, between 4 and 5.

44
Fig. 24
For MRA sequence, stainless steel brackets and tubes received low scores with a median of 1 for
all regions. Scores for nasopharynx, globes of the eyes, and pituitary gland showed significant
variability, and the ranged from 1 to 3.

45
Fig.25
For axial FLAIR sequence, stainless steel brackets and tubes received scores in the diagnostic
range with the exception of globes of the eyes (mean score 3.5). Scores for nasopharynx showed
significant variability, with a range from 1 to 4, median of 1 and interquartile range from 1 to
2.5.
Table 7 and Fig. 26 demonstrate mean diagnostic scores for ceramic brackets for different
sequences and regions.

46
Table 7. Mean diagnostic scores with standard deviations (in parentheses) for different anatomic
regions according to the MR sequence for the appliance type: ceramic brackets (included all
subjects and reviewers).
Anatomic region Sag.T1 Axial T2 Axial GRE Axial DWI Axial MRA Axial FLAIR
Base of the tongue
N=20
2.20 (0.89) - - - - -
Body of the mandible
N=20
2.30 (0.86) 1 - - - -
Hard palate
N=20
2.50 (0.83) - - - - -
Nasopharynx
N for each sequence=20
1.80 (0.83) 1.35 (0.59) - - 1.15 (0.37) 1.35 (0.49)
Globes of the eyes
N for each sequence=20
1.95 (0.83) 2.35 (0.59) - - 1.25 (0.55) 1.85 (0.99)
Pituitary gland
N for each sequence=20
1.65 (0.67) 1.4 (0.60) - - 1.20 (0.7) 1.30 (0.57)
Frontal lobe
N for each sequence=20
1.40 (0.68) 1.20 (0.41) 3.05 (0.39) 2.90 (0.31) 1.10 (0.31) 1.05 (0.22)
Temporal lobe
N for each sequence=20
1.50 (0.61) 1.15 (0.37) 3.45 (0.69) 3.20 (0.52) 1.30 (0.73) 1.00
Brain stem
N for each sequence=20
1.10 (0.31) 1.00 2.80 (0.79) 2.70 (0.57) 1.05 (0.22) 1.00
N-number of images, SD-standard deviation, GRE-gradient recalled, DWI-diffusion-weighted,
MRA-magnetic resonance angiography, FLAIR-fluid attenuation inversion recovery.

47
Fig 26 Mean diagnostic scores for different anatomic regions according to the MR sequence for
the appliance type: ceramic brackets.
For the axial T2-weighted sequence, hard palate was not included in the scan.
Distribution and variability of the scores for ceramic brackets for each sequence according to the
anatomic region can be seen in box plots in figures 27-32.

48
Fig. 27
For sagittal T1 sequence, ceramic brackets received mean diagnostic scores below 3 for all
regions. However, the scores for intraoral regions of base of the tongue, body of the mandible,
and hard palate had a large variability from 1 to 4 with the upper quartile bordering 3.

49
Fig.28
For axial T2 sequence, diagnostic scores for most of the regions were in the diagnostic range,
and were clustered around 1. The highest scores were received by globes of the eyes with median
of 2 and intrequartile range of 2 to 3. Scores for nasopharynx and pituitary gland showed
significant variability and ranged from 1 to 3.

50
Fig. 29
For axial gradient-recalled sequence, ceramic brackets received scores of 3 for frontal lobe with
the exception of 3 outliers. Temporal lobe scans received a median score of 3.0 with a range of 2
to 5 and interquartile range of 3 to 4. Brain stem scans had scores with a median of 3 and
interquartile range of 2 to 3.

51
Fig. 30
For axial diffusion-weighted sequence, ceramic brackets received diagnostic scores of 3 for
frontal lobe. Temporal lobe received a median score of 3 with a range from 3 to 4. Scores for
brain stem had significant variability with a median of 3, range from 2 to 4, and interquartile
range from 2 to 3.

52
Fig.31
Scores for axial MRA sequence for ceramic brackets were uniformly 1 for all regions with the
exception of several outliers.

53
Fig.32
For axial FLAIR sequence, ceramic brackets received scores in the diagnostic range for all
regions. Median scores were 1, scores for globes of eyes showed significant variability with the
range of 1 to 3.
Mean diagnostic scores with standard deviations (in brackets) for combination of ceramic
brackets and steel molar buccal tubes for all the regions and sequences are given in Table 8 and
illustrated in Fig.33.

54
Table 8. Mean diagnostic scores with standard deviations for different anatomic regions
according to the MR sequence for the appliance type: ceramic brackets and stainless steel molar
buccal tubes (included all subjects and reviewers).
Anatomic region Sag.T1 Axial T2 Axial GRE Axial DWI Axial MRA Axial FLAIR
Base of the tongue
N =20
4.26 (0.45) - - - - -
Body of the mandible
N =20
4.74 (0.45) - - - - -
Hard palate
N =20
4.21 (0.54) - - - - -
Nasopharynx
N for each sequence =20
3.10 (0.45) 1.50 (0.69) 1.30 (0.57) 1.45 (0.61)
Globes of the eyes
N for each sequence =20
3.60 (0.75) 2.65 (0.81) 1.25 (0.44) 1.95 (0.94)
Pituitary gland
N for each sequence=20
2.20 (0.7) 1.70 (0.57) 1.35 (0.67) 1.40 (0.50)
Frontal lobe
N for each sequence =20
2.00 (0.65) 1.45 (0.61) 4.10 (0.31) 3.60 (0.5) 1.10 (0.31) 1.25 (0.44)
Temporal lobe
N for each sequence =20
2.25 (0.72) 1.40 (0.5) 4.15 (0.49) 4.30 (0.66) 1.40 (0.5) 1.25 (0.44)
Brain stem
N for each sequence=20
1.70 (0.66) 1.10 (031) 3.90 (0.64) 4.35 (0.49) 1.10 (0.31) 1.10 (0.31)
N-number of images, SD-standard deviation, GRE-gradient recalled, DWI-diffusion-weighted,
MRA-magnetic resonance angiography, FLAIR-fluid attenuation inversion recovery

55
Fig 33. Mean diagnostic scores for different anatomic regions according to the MR sequence for
the appliance type: ceramic brackets and stainless steel buccal tubes (combination appliance).
Distribution and variability of the scores for ceramic brackets and stainless steel buccal tubes for
each sequence according to the anatomic region is illustrated in box plots in figures 34-39.

56
Fig.34
For sagittal T1 sequence, the combination of ceramic brackets and stainless steel molar buccal
tubes received scores in the diagnostic range for brain regions. For temporal lobe, 25% of the
scores were in the non-diagnostic range The rest of the regions had scores in the non-diagnostic
range

57
Fig. 35
For axial T2 sequence, the combination appliance received scores below 3 for brain regions and
nasopharynx. The mean score for the globes of the eyes was 2.65. The scores for the globes
showed significant variability with the range for 2 to 4 and interquartile range from 2 to 3.

58
Fig.36

59
Fig. 37
For axial gradient-recalled and axial diffusion-weighted sequences, the combination of ceramic
brackets and stainless steel buccal tubes received scores above, 3 in the non-diagnostic range.

60
Fig 38
The combination appliance received diagnostic scores for axial MRA sequence for all the
regions with medians of 1 and scores generally ranging from 1 to 2 with a few outliers.

61
Fig 39
For FLAIR sequence, ceramic brackets+stainless steel buccal molar tubes received scores in the
diagnostic range for all regions. Scores for nasopharynx and globes of the eyes showed the
greatest variability with a range from 1 to 3 and medians of 1 and 2, respectively.

62
Table 9 and Fig.40 show mean diagnostic scores for lingual retainer for all anatomic regions and
sequences.
Table 9. Mean diagnostic scores with standard deviations for different anatomic regions
according to the MR sequence for the appliance type: lingual retainer (included all subjects and
reviewers).
Anatomic region Sag.T1 Axial T2 Axial GRE Axial DWI Axial MRA Axial FLAIR
Base of the tongue
N=20
3.00 (0.69) - - - - -
Body of the mandible
N=20
2.90 (0.72) - - - - -
Hard palate
N=20
3.85 (0.81) - - - - -
Nasopharynx
N for each sequence=20
2.35 (0.81) 1.40 (0.5) - - 1.15 (0.37) 1.35 (0.49)
Globes of the eyes
N for each sequence=20
2.35 (0.67) 2.47 (0.61) - - 1.30 (0.57) 1.85 (0.93)
Pituitary gland
N for each sequence=20
1.85 (0.67) 1.45 (0.51) - - 1.10 (0.45) 1.35 (0.49)
Frontal lobe
N for each sequence=20
1.60 (0.60) 1.30 (0.47) 3.05 (0.22) 3.05 (0.22) 1.10 (0.31) 1.10 (0.31)
Temporal lobe
N for each sequence=20
1.75 (0.75) 1.05 (0.22) 3.35 (0.49) 3.25 (0.44) 1.15 (0.49) 1.05 (0.22)
Brain stem
N for each sequence=20
1.10 (0.31) 1.00 2.70 (0.47) 2.70 (0.57) 1.10 (0.31) 1.00
N-number of images, SD-standard deviation, GRE-gradient recalled, DWI-diffusion-weighted,
MRA-magnetic resonance angiography, FLAIR-fluid attenuation inversion recovery

63
Fig 40. Mean diagnostic scores for different anatomic regions according to the MR sequence for
the appliance type: lingual retainer.
Distribution and variability of the scores for lingual retainer for each sequence according to the
anatomic region are illustrated in figures 41-46.

64
Fig.41
For sagittal T1 sequence, mean scores for intraoral regions were above 3 (non-diagnostic). The
rest of the anatomic regions received mean scores in the diagnostic range. The scores for
nasopharynx and globes of the eyes showed significant variability with medians of 2, range from
1 to 4 and interquartile range from 2 to 3.

65
Fig.42
For mandibular stainless steel lingual retainer, the mean scores for T2 sequence were in the
diagnostic range for all anatomic regions. For globes of the eyes, the median score was 2, range
was from 2 to 4, and interquartile range was from 2 to 3.

66
Fig.43

67
Fig.44
For axial gradient-recalled and axial diffusion-weighted sequences, lingual retainer received
scores of 3 for frontal lobe with little variability. Scores for temporal lobe had median of 3, range
from 3 to 4. Brain stem received the scores with median of 3, and the interquartile range from 2
to 3.

68
Fig.45
For the lingual retainer, the scores for MRA sequence were in the diagnostic range in all
anatomic regions with median scores of 1. Only scores for globes of the eyes showed significant
variability. The interquartile range was between 1 and 2.

69
Fig.46
All anatomic regions for FLAIR sequence received scores below 3. The scores for globes of the
eyes showed greatest variability with median of 1.5 and range from 1 to 3.

70
In the pilot test, there were no statistically significant differences between the distortion
scores of ceramic brackets and no appliance. Therefore, scores of ceramic brackets could
arguably serve as a gold standard to compare other appliances to. Distortion scores for ceramic
brackets for axial T1, axial T2, axial MRA and axial FLAIR sequences were in the diagnostic
range. For these sequences, a diagnostic score cut off of 3 was used to determine the diagnostic
usability of the MR images for steel brackets and tubes, the combination appliance, and lingual
retainer. For GRE and DWI sequences, diagnostic scores for ceramic brackets were close to, or
slightly above 3. For GRE and DWI sequences, the diagnostic scores for stainless steel brackets
and tubes and the combination appliance were much higher than those of ceramic brackets
(between 4 and 5). Only for lingual retainer, the diagnostic scores for GRE and DWI sequences
were close to, or slightly above 3, similar to the scores of ceramic brackets. Mean diagnostic
scores for lingual retainer for axial GRE and axial DWI sequences were 3.03±0.49 and
3.00±0.49, respectively (60 images were analyzed, all regions and reviewers were included).
Mean diagnostic scores for ceramic brackets for axial GRE and axial DWI sequences were
3.10±0.68 and 2.93±0.52, respectively (60 images were analyzed, all regions and reviewers were
included). To determine whether there were statistically significant differences between the
diagnostic scores for ceramic brackets and lingual retainer for GRE and DWI sequences,
Wilcoxon signed ranks tests were performed. There were no statistically significant differences
in the diagnostic scores between lingual retainer and ceramic brackets for axial gradient-recalled
sequence (p=0.822) and for axial diffusion-weighted sequence (p=0.204).
For axial diffusion-weighted and axial gradient recalled sequences, the distortion scores
were in close or slightly above 3 even with no appliances. The scores for non-contrast axial
magnetic resonance angiography (MRA), axial fluid attenuated inversion recovery (FLAIR), and

71
axial T2-weighted sequences were found to be below 3 (diagnostic) in all the appliances and
regions with the exception of globes of the eyes for metal brackets and tubes in T2 and FLAIR
sequences. Stainless steel brackets and buccal tubes rendered images nondiagnostic in 3 Tesla
cranial MRI for sagittal T1-weighted, axial gradient-recalled, and axial diffusion-weighted
sequences. Ceramic brackets showed minimal MR image distortion in all anatomic regions. The
combination of ceramic brackets and metal buccal tubes caused image distortions with the scores
above 3.0 for axial gradient-recalled and axial diffusion-weighted sequences. For sagittal T1
scan, the combined appliance received nondiagnostic scores in oral, pharyngeal regions of the
head and globes of the eyes. Brain regions had diagnostic scores. Multistranded stainless steel
mandibular lingual retainer received scores above 3.0 for axial gradient-recalled and axial
diffusion-weighted sequence. However, there were no statistically significant differences
between the scores of lingual retainer and the control appliance (ceramic brackets). For sagittal
T1-weighted sequence, the scores were in the nondiagnostic range for oral and pharyngeal
regions of the cranial MRI. Brain regions remained diagnostic.
3.6 Calculation of intra and interrater agreements
Interrater agreement was calculated using unweighted Kappa statistics. The scores were
categorized into two groups. Group 1 included scores of 1-3 (diagnostic scans), group 2 included
scores above 3 (non-diagnostic).26
Because the diagnostic score definitions were developed
based on the raters’ collective discussion of the images of subject 1, kappa was calculated for the
images of subjects 2-10 excluding subject 1 to avoid artificially increased value for the interrater

72
agreement. A total of 1181 scores per each reviewer were used to calculate the interrater
agreement.
Interrater kappa was 0.761, 95% CI=0.712-0.81 (p<0.0001) (substantial agreement,
Landis and Koch interpretation).
Inrarater agreement was calculated for each reviewer after they independently re-scored 3
randomly selected subjects26
(Table 10). Reviewer 1 re-scored images for subjects 3, 4, and 9;
reviewer 2 re-scored images for subjects 6, 2, and 9. Inrarater agreement calculation for reviewer
1 was based on 398 repeated scores; intrarater agreement calculation for reviewer 2 was based on
394 repeated scores.
Table 10. Intrarater agreements for reviewers 1 and 2.
Kappa SE p Lower
CI
Upper CI
Reviewer 1 0.559 0.051 <0.0001 0.459 0.659
Reviewer 2 0.667 0.048 <0.0001 0.573 0.761
SE-standard error, CI-confidence interval.
Intrarater agreement was moderate for reviewer 1 and substantial for reviewer 2.

73
CHAPTER 4
Discussion
MRI is a diagnostic modality increasingly used for a vast variety of medical conditions.
Among them, there are tumors, epilepsy, cardiovascular abnormalities, headaches, TMJ
pathology, multiple sclerosis etc. Management of these conditions often requires multiple
periodic MR examinations. With the ever increasing utilization of MRI and orthodontic
treatment, especially by adults, and ubiquitous use of fixed retainers after orthodontic treatment,
it seems very likely that every orthodontic provider will sooner or later face the problem of fixed
orthodontic appliances potentially interfering with MR examination in their orthodontic patients.
Therefore, it is important to have clear best practice protocols for patients who need MR imaging
during the period of their fixed orthodontic appliances treatment or retention with fixed retainers.
Currently, there is a lack of consensus regarding best practices for imaging patients with fixed
orthodontic appliances in MR scanners. The issue of artifacts produced by dental materials on
MR images of the head have been addressed in a number of studies. Sadowsky et al. (1988)9
investigated in-vitro and in-vivo the influence of stainless steel orthodontic appliances on cranial
MR images produced by a 0.5 Tesla MR scanner and came to the conclusion that only archwires
should be removed before cranial MRI; brackets and bands can be left in place. On the other
hand, Lissac et al. (1992)38
found that dental appliances made of non-precious metals caused
significant disturbances in the cranial MR images produced by a 0.5 Tesla scanner and need to
be removed before the scan. These findings were confirmed by the studies of Masumi et al.
(1993)39
using 0.1 Tesla MR scanner, and Elison et al. (2008)26
using 1.5 Tesla MR scanner.
Artifact intensity is directly proportional to the strength of magnetic field.13,40
Additional
difficulty in summarizing the available data comes from the fact that unambiguous classification

74
of dental material MR compatibility based on material properties only without specification of
MRI parameters and the device geometry is impossible.13
4.1 Scientific novelty of the study.
To our knowledge, this study is the first systematic investigation to analyze the effects of
orthodontic appliances on cranial MR scans made with a 3 Tesla magnet. 3 Tesla MR scanners
are becoming a standard of care in the field of clinical MRI because they offer better image
resolution.13
Since the intensity of the artifact is directly proportional to the strength of the
magnetic field , an MRI compatible device with a 0.5 or 1.5 Tesla scanner might potentially
render image non-diagnostic in a 3Tesla scanner.13,31,32
In addition, the study looked into artifact formation caused by molar tubes made of
austenitic non-magnetic 18-8 stainless steel in addition to orthodontic brackets and tubes made of
magnetic 17-4 stainless steel brazed to 18-8 stainless steel bases. Elisson et al 26
found that of the
two types of steel commonly used in fabrication of fixed orthodontic appliances, 18-8 stainless
steel did not cause deformation of the MR image in vitro on a phantom grid as opposed to the
17-4 type stainless steel that did. They predicted that orthodontic appliances made entirely of 18-
8 steel would not compromise the quality of cranial MR scans. However, in the current study,
buccal tubes which were made of only austenitic 18-8 stainless steel as a single piece via metal
injection molding did cause significant distortion of cranial MR scans. It can possibly be
explained by several factors. Firstly, it is possible that buccal tubes made of austenitic 18-8 steel
could undergo stress-induced martensitic transformation caused by cold working or slow
cooling.41
This can increase magnetic susceptibility of the attachment and thus, artifact

75
formation. Secondly, apart from the material magnetic susceptibility, artifact size is also
dependent on the material electric conductivity.13
Therefore, even non-magnetic metallic objects
can create sizable artifacts in MR images.
Next, MR artifacts caused by one of the most common types of fixed lingual retainers
were studied systematically in vivo for the first time to the best of our knowledge. Fixed lingual
wires, especially in the mandibular arch, are now a universally-accepted means of long-term
retention after orthodontic treatment, and can remain attached to the teeth for many years, after
treatment completion. With the ever-increasing utilization of orthodontic treatment and MRI,
fixed lingual retainers are likely to be the most frequent problem encountered in MR imaging of
patients with orthodontic appliances. Shalish et al. (2015)40
investigated artifacts produced by
two common types of lingual retainer wires in the MR images of a dry skull immersed in a
gadolinium contrast agent. The images were acquired by 1.5 Tesla and 3 Tesla MR scanners. The
investigators found that stainless steel lingual retainers did not have to be removed before the
MR scans unless the region of interest was near the retainer. However, dry skull does not allow
for a representation of soft tissues of the face and brain tissues for which MRI is most commonly
used. Results of the current study support those of Shalish et al. (2015). It was found that
mandibular stainless steel lingual retainer did not cause significant distortion of the cranial MR
images with the exception of the intraoral regions in the close proximity to the retainer.
Finally, a systematic investigation of the two frequently used MR sequences (FLAIR and
MRA) with fixed orthodontic appliances was undertaken for the first time, to the best of our
knowledge. Fluid-attenuation inversion recovery (FLAIR) is a special sequence with long T1 to
remove the effects of fluid from the resultant images. This sequence is particularly useful in the
detection of subtle changes at the periphery of the hemispheres and in the periventricular region

76
close to CSF. The usefulness of FLAIR sequences has been established in diseases of the central
nervous system such as infarction, multiple sclerosis, subarachnoid haemorrhage, head injuries
etc.42
Non-contrast axial magnetic resonance angiography also known as time of flight
angiography (TOF) is an MRI technique to visualize flow within vessels, without the need to
administer contrast.43
It is useful in diagnosis of vascular stenosis, occlusions, most often in
atherosclerosis, as well as aneurysms and other vascular abnormalities. The current study
suggests that none of the appliances we tested produced significant artifacts on brain MR images
using axial FLAIR and axial MRA sequences. Therefore, none of the appliances, including
stainless steel brackets and molar tubes, may need to be removed before the brain MR scans
using these sequences.
4.2. Explanation of findings
There was individual variability in the distortion scores depending on the study subject.
Subjects 7, 9, and 10 showed mean distortion scores higher the other participants for all the
appliances used. It can be explained by possible motion artifacts caused by the subjects’ physical
movement during image acquisition. Another possible explanation may be individual’s unique
tissue susceptibility which may be dependent on the tissue anatomy (different lipid-water
interfaces, air-bone interfaces), vascularity, chemical composition.44
The results of this study are
similar to the findings of Elison et al. (2008)26
where the researchers found individual variations
in the distortion scores of images of different subjects.
Mean distortion scores for different anatomic regions demonstrated a general trend of
reduction in the image distortion with the increasing distance from the orthodontic appliance.

77
These findings are in accordance to the results of previously done studies. 9,26
However, some
anatomic regions demonstrated mean distortion scores higher than the regions more distant from
the appliances. For example, globes of the eyes demonstrated significantly higher distortion
scores than nasopharynx for all appliances. A possible explanation to this phenomenon can be
organ movement as well as unique tissue interfaces in a particular anatomic area. Approximate
relative distances from the appliances to the anatomic regions assessed in this study can be seen
in Fig.47.
Fig.47 Approximate relative distances from the orthodontic appliances to the anatomic regions of
the head assessed in the study.

78
In 3 Tesla cranial MRI, axial gradient-recalled and axial diffusion-weighted sequences
received scores close to, or in the nondiagnostic range even with no appliances. These results
coincide with the data from the previously done study by Elison et al.26
where in 1.5 Tesla MRI,
mean distortion scores for axial gradient-recalled and axial diffusion-weighted sequences were
close to, or in the non-diagnostic range. The distortion scores for axial diffusion-weighted
sequence in this study were higher for all the appliances compared to the scores in the study by
Elison et al. This difference in the results can possibly be explained by the strength of the
magnetic field, which is one of the main factors determining the artifact size, and which was
twice as strong in our study compared to Elison et al.26
High distortion scores for axial gradient-
recalled and axial diffusion-weighted sequences can be explained by the nature of these
sequences (use of strong gradient pulses, eddy currents, rapid switching of strong gradient pulses
and thus, high sensitivity to artifacts due to metallic objects, bone/air interface, and movement).45
Gradient-recalled and diffusion-weighted sequences are routinely used to evaluate brain regions.
Therefore, we included only brain regions of frontal lobe, temporal lobe and brain stem into the
assessment for these two sequences to avoid artificially increased scores due to inclusion of other
regions.
The intrarater agreement was based on the reviewer 1 independently re-scoring images of
3 randomly selected subjects (398 repeated scores, about 132 scores per each subject), and
reviewer 2 independently re-scoring images of 3 randomly selected subjects (394 repeated
scores, about 131 scores per each subject). The intrarater agreement was moderate for reviewer 1
(kappa=0.059, 95% CI=0.459-0.659) and substantial for reviewer 2 (0.667, 95% CI=0.573-
0.761). The interrater agreement was based on the image scores of subjects 2-10 (a total of 1181
scores per reviewer) because the diagnostic score definitions were developed based on the raters’

79
collective discussion of the images of subject 1. The interrater agreement was substantial (0.761,
95% CI=0.712-0.81).
The scores for non-contrast axial magnetic resonance angiography (MRA), axial fluid
attenuated inversion recovery (FLAIR), and axial T2-weighted sequences were found to be
below 3 (diagnostic) in all the appliances and regions with the exception of globes of the eyes for
metal brackets and tubes in T2 and FLAIR sequences. High scores for the globes of the eyes
could be explained by eye movement.46
If brain is the area of interest, none of the four
appliances need removal before imaging with axial T2-weighted, axial MRA and axial FLAIR
sequences according to the data from our sample. MRA and FLAIR sequences were
systematically studied for the first time. The results for axial T2-weighted sequence are in
accordance with the findings of Elison et al.26
, where the researchers found mean distortion
scores for axial T2 sequence to be the lowest from all the used sequences, and in the diagnostic
range even for stainless steel brackets and buccal tubes (although the distortion scores for this
appliance were close to the non-diagnostic range). However, Elison et al. concluded that stainless
steel brackets needed to be removed before the axial T2 cranial MR scans even if the region of
interest was brain. The difference in the recommendations regarding axial T2 sequence
compared to the current study can be explained by the fact that the researchers in the study by
Elison et al. calculated mean distortion score for axial T2 sequence with stainless steel brackets
and tubes for all anatomic regions which does not allow for assessment of each anatomic region
separately. In our sample, intraoral regions of base of the tongue, body of the mandible and hard
palate were not included in axial T2 sequence, globes of the eyes received scores in the
nondiagnostic range, nasopharynx and brain regions received scores around 2, in the diagnostic
range, for stainless steel brackets and molar tubes.

80
4.3 Recommendations for clinical practice.
Stainless steel brackets and buccal tubes rendered images nondiagnostic in 3 Tesla cranial
MRI for sagittal T1-weighted, axial gradient-recalled, and axial diffusion-weighted sequences.
Therefore, it is suggested in the current study that stainless steel brackets and tubes should be
removed before imaging with these sequences. Ceramic brackets did not cause significant image
distortions in 3 Tesla cranial MRI. Even though the scores for ceramic brackets for axial
gradient-recalled and axial diffusion-weighted sequences were close to, or in the nondiagnostic
range, they were not statistically significantly different from the distortion scores for the cranial
images with no appliances. Therefore, ceramic brackets may not need to be removed before the
imaging with all the used sequences. The combination of ceramic brackets and metal buccal
tubes had scores in the nondiagnostic range for axial gradient-recalled and axial diffusion-
weighted sequences, thus buccal tubes should be removed before these scans. For cranial sagittal
T1 scan, the combined appliance received scores in the nondiagnostic range for oral, pharyngeal
regions of the head and globes of the eyes. Brain regions remained diagnostic. Therefore, metal
buccal tubes may not need to be removed before 3 Tesla T1 sagittal brain scans. Multistranded
stainless steel lingual retainer received scores above 3 (nondiagnostic) for axial gradient-recalled
and axial diffusion-weighted sequences. However, they were not statistically significantly
different from the scores of the control appliance (ceramic brackets). In sagittal T1-weighted
sequence, the scores of the oral and pharyngeal regions of the cranial MRI were above 3.0, but
the brain regions remained diagnostic. Therefore, for brain imaging, an orthodontic lingual
retainer made from 18-8 stainless steel multistranded wire may not need to be removed for
imaging with any of the used sequences. Clinical recommendations from this study are
summarized in Table 11.

81
Table 11. Clinical recommendations for cranial MR imaging with 4 commonly used
orthodontic appliances and 6 common MR sequences.
Bas
e o
f th
e
ton
gu
e
Bo
dy
of
the
man
dib
le
Har
d p
alat
e
Nas
op
har
ynx
Glo
bes
of
the
eyes
Pit
uit
ary
gla
nd
Fro
nta
l lo
be
Tem
po
ral
lob
e
Bra
in s
tem
Sagittal
T1
M M M M M M M M M
C C C C C C C C C
C+M C+M C+M C+M C+M C+M C+M C+M C+M
LR LR LR LR LR LR LR LR LR
Axial
T2
M M M M M M
C C C C C C C
C+M C+M C+M C+M C+M C+M
LR LR LR LR LR LR
Axial
GRE
M M M
C C C
C+M C+M C+M
LR LR LR
Axial
DWI
M M M
C C C
C+M C+M C+M
LR LR LR
Axial
MRA
M M M M M M
C C C C C C
C+M C+M C+M C+M C+M C+M
LR LR LR LR LR LR
Axial
FLAIR
M M M M M M
C C C C C C
C+M C+M C+M C+M C+M C+M
LR LR LR LR LR LR
M represents stainless steel brackets and molar tubes, C represents ceramic brackets,
C+M represents combination of ceramic brackets and stainless steel molar buccal tubes, LR
represents stainless steel lingual retainer. Red color of the cell indicates that the appliance should
be removed before the imaging. Green color of the cell indicates that removal of the appliance is
not necessary before the imaging. Yellow color of the cell indicates that 25% or fewer images
received a score of 4 (nondiagnostic) although the majority of scores were in the diagnostic
range; thus removal of the appliances could be considered based on the individual assessment of
the case by the prescribing physician/radiologist. Empty cell indicates that the anatomic region is
either not included in the MR scan, or not assessed. GRE-gradient recalled, DWI –diffusion-
weighted, MRA-magnetic resonance angiography, FLAIR-fluid attenuation inversion recovery.

82
It seems prudent for an orthodontist to pay close attention to the patient’s medical history
pertaining to the current or potential need for MRI. Questions regarding previous MRI
examinations, conditions such as seizures, TMJ disorders, tumors, cerebral palsy, cardiovascular
abnormalities, , multiple sclerosis, autism etc. may positively influence the practitioner’s
appliance choice to potentially reduce patient’s and practice burden.
MR imaging of patients with metal appliances causes some potential safety concerns.
One potential risk is rapid movement of the metal objects in the magnetic field. In this study,
orthodontic appliances were securely embedded into the rigid Essix retainers which were firmly
attached to the teeth. Previously conducted studies using same methods of appliance fixation did
not find any perceivable movement of orthodontic appliances during image acquisition.26,27
Therefore, in this study, no special precautions were taken in regard to the potential appliance
movement. MR imaging of patients with metal appliances poses another potential risk of
appliance overheating during image acquisition. However, changes in the temperature of
orthodontic appliances were found to be clinically insignificant, within 1 degree.37
None of the
participants in this study had any discomfort during the procedure.
4.4 Strengths and limitations of the study
Development of a scientific basis for the clinical protocol of MR imaging of patients with
fixed orthodontic appliances in 3 Tesla MR scanners should be considered the strength of this
study. Also, comparison of artifact formation by molar buccal tubes made of different types of
steel is of high clinical relevance. Despite advances in material science and presence of
alternatives to stainless steel brackets such as ceramic, titanium and composite brackets which

83
were found not to cause significant artifacts in 1.5Tesla MRI 26
, stainless steel brackets remain
most frequently used ones. Although plastic and composite brackets might be compatible with
MRI scanners, they have several problems related to material performance such as bracket
deformation under stress, especially with torque expression, decreased wear resistance.33,34
These
drawbacks have prevented plastic and composite brackets from routine use in most clinical
orthodontic practices. In addition, inclusion of a multistranded stainless steel lingual retainer into
the study added to its strength because of potentially frequent presence of this appliance in MRI
subjects.
The study has, however, a few limitations. Firstly, with 4 different appliances and 6 MR
sequences for each appliance, the study sample size is small. This study found individual
variability in the distortion scores depending on the study subject. The influence of the study
subject on the distortion scores could not be investigated fully because of the small sample size.
In addition, limited sample size creates interdependence of the data, thus multiple statistical tests
performed on the same small number of subjects pose a risk of a Type I error. Intrarrater
agreement calculation was based on each reviewer independently repeating close to 400 scores.
However these scores were from scans of only 3 randomly selected subjects, thus creating data
interdependence. In this study, all the statistical differences found were highly significant
(p<0.0001). This increases confidence in the data obtained. Increasing the sample size would
have increased the statistical power of the study and decreased the risks associated with data
interdependence. However, significant increase of the sample size was cost-prohibitive in this
study due to the high cost of MR scans and appliances. The sample size of 10 seems to be the
largest in the in-vivo studies26,27
published on the topic of MRI and dental appliances presumably
because of high MRI and material costs.

84
Secondly, there is a great variety of brackets including self-ligating brackets on the
market made of different combinations of materials and with the aid of various technological
processes e.g. metal injection molding, casting, milling, brazing etc. All of the above variables
influence magnetic susceptibility of the final product and thus, its MRI compatibility.13,41
It
would certainly be unrealistic to test every bracket on the market, and the only possible way
would be to generalize MR compatibility of different bracket systems by grouping them
according to the material combination and the technological processes involved. Keeping these
limitations in perspective, we chose to investigate the most commonly used fixed orthodontic
appliances and MR sequences. Taking in account high cost of MRI and orthodontic appliances,
we elected not to include archwires into the study because they can be relatively easily and
quickly removed from the patients’ mouths before the MR scans Therefore, archwires do not
pose as significant a clinical problem in MRI as do bonded orthodontic appliances.
4.5 Recommendations for future studies
It would be beneficial to study more appliance types such as titanium or cobalt-chromium
(no-nickel) brackets and buccal tubes, different types of archwires and lingual retainer wires (e.g.
gold retention chains, titanium molybdenum alloy (TMA), wires, metal bands to determine their
MR compatibility at 3Tesla. It also seems very useful to study surgical fixation screws and plates
in head MRI as these appliances remain permanently embedded into the tissues after
maxillofacial surgery and are rarely removed. Apparently, this potential investigation would
have to be retrospective considering invasive nature of surgery.

85
In addition, the influence of commonly used orthodontic appliances on
temporomandibular joint images in 3 Tesla MRI needs to be systematically investigated. Not
only is MRI a gold standard for TMJ imaging in patients with TMJ pathology, but fixed
orthodontic appliances are also frequently used in such patients as treatment of a significant
proportion of these patients includes orthodontics and orthognathic surgery.27
Finally, new MRI modalities are emerging which are specifically designed to suppress
metal artifacts.47,48
Two new sequences were used in recent descriptive pilot studies to suppress
metal artifacts in imaging patients with metal implants of the hip joints and spine in 1.5 and 3
Tesla MRI. Slice encoding for metal artifact correction (SEMAC) and multiacquisition variable
resonance image combination (MAVRIC) showed promising results compared to traditional MR
sequences. The slice-encoding for metal artifact correction (SEMAC) technique is based on two-
dimensional multi-slice spin-echo imaging, and uses additional slice-encodings to deal
with the through-plane distortion. SEMAC corrects artifacts via encoding of each excited slice
against metal-induced field inhomogeneities.48
The multiacquisition variable resonance image
combination (MAVRIC) technique is based on the three-dimensional acquisition, and acquires
multiple images with different center of excitation frequency to deal with a broad field
perturbation.49
Prospective studies using head MR imaging in patients with orthodontic
appliances acquired with SEMAC and MAVRIC sequences compared to traditional MR imaging
would be of great clinical value.

86
CHAPTER 5
Conclusions
The hypothesis: “commonly used stainless steel brackets, buccal tubes and lingual
retainers cause significant MR image distortion on 3T MR scanners to render the image
nondiagnostic for MR investigations of all the regions of the head” was rejected because this in-
vivo investigation revealed that head MR images in different regions were differentially affected by
the presence of orthodontic appliances.
1. Ceramic brackets caused minimal MR image distortions in 3 Tesla head MRI.
2. Multistranded stainless steel lingual retainer did not cause significant image distortions in MR
images of the brain with any of the used sequences.
3. None of the 4 appliances we tested caused significant image distortions in 3 Tesla brain MRI
using non-contrast axial magnetic resonance angiography (MRA), axial fluid attenuated
inversion recovery (FlAIR), and axial T2-weighted sequences.
4. Stainless steel brackets and buccal tubes rendered images nondiagnostic in 3 Tesla head MRI
for sagittal T1-weighted, axial gradient-recalled, and axial diffusion-weighted sequences.
5. The combination of ceramic brackets and metal buccal tubes rendered images nondiagnostic
for axial gradient-recalled and axial diffusion-weighted sequences. For sagittal T1 head scan,
buccal tubes rendered images of oral, pharyngeal regions of the head and globes of the eyes non-
diagnostic. T1 sagittal brain scans remained diagnostic with this appliance.

87
BIBLIOGRAPHY
1. Wu LM, Xu JR, Liu MJ, Zhang XF, Hua J, Zheng J et al. Value of magnetic resonance
imaging for nodal staging in patients with head and neck squamous cell carcinoma: a meta-
analysis Acad Radiol. United States: 2012 AUR. Published by Elsevier Inc; 2012. p. 331-340.
2. Liedberg J, Panmekiate S, Petersson A, Rohlin M. Evidence-based evaluation of three imaging
methods for the temporomandibular disc. Dentomaxillofac Radiol 1996;25:234-241.
3. Kim DE, Bae HJ, Lee SH, Kim H, Yoon BW, Roh JK. Gradient echo magnetic resonance
imaging in the prediction of hemorrhagic vs ischemic stroke: a need for the consideration of the
extent of leukoariosis Arch Neurol. United States; 2002. p. 425-429.
4. Hauser WA. The prevalence and incidence of convulsive disorders in children. Epilepsia
1994;35 Suppl 2:S1-6.
5. Scheck SM, Boyd RN, Rose SE. New insights into the pathology of white matter tracts in
cerebral palsy from diffusion magnetic resonance imaging: a systematic review. Dev Med Child
Neurol 2012;54:684-696.
6. Tymofiyeva O, Vaegler S, Rottner K, Boldt J, Hopfgartner A, Proff P et al. Influence of dental
materials on dental MRI. Dentomaxillofac Radiol 2013;42:20120271.
7. SC W, MJ P. Oral Radiology: principles and interpretation. St. Louis: Mosby; 2000.
8. Baker LC, Atlas SW, Afendulis CC. Expanded use of imaging technology and the challenge
of measuring value Health Aff (Millwood). United States; 2008. p. 1467-1478.
9. Sadowsky PL, Bernreuter W, Lakshminarayanan AV, Kenney P. Orthodontic appliances and
magnetic resonance imaging of the brain and temporomandibular joint. Angle Orthod 1988;58:9-
20.
10. Edelman R, Hesselink J. Clinical magnetic resonance imaging. Philadelphia: WB Sanders;
1990.
11. Brown MA, Semelka RC. MRI Basic Principles and Aplications. New York: Wiley-Liss;
1995.
12. Bennett LH, Wang PS, Donahue MJ. Artifacts in magnetic resonance imaging from metals.
Gaithersburg, MD 20899, USA: National Institute of Standanrds and Technology.
13. Starcukova J, Starcuk Z, Jr., Hubalkova H, Linetskiy I. Magnetic susceptibility and electrical
conductivity of metallic dental materials and their impact on MR imaging artifacts Dent Mater.
England; 2008. p. 715-723.

88
14. Costa AL, Appenzeller S, Yasuda CL, Pereira FR, Zanardi VA, Cendes F. Artifacts in brain
magnetic resonance imaging due to metallic dental objects Med Oral Patol Oral Cir Bucal.
Spain; 2009. p. E278-282.
15. Bentson C. The business of private practice of orthodontics in the United States [Internet].
[cited 2014 Jan 8]. Available from: www.dentaltribune.com.
16. Mavreas D, Athanasiou AE. Factors affecting the duration of orthodontic treatment: a
systematic review. Eur J Orthod 2008;30:386-395.
17. TM G, RL V, KW V. Orthodontics:Current Principles and Techniques. Elsivier; 2005.
18. Patel A, Bhavra GS, O'Neill JR. MRI scanning and orthodontics J Orthod. England; 2006. p.
246-249.
19. Harris TM, Faridrad MR, Dickson JA. The benefits of aesthetic orthodontic brackets in
patients requiring multiple MRI scanning J Orthod. England; 2006. p. 90-94.
20. Cassiafesta V. Difference in bonding/debonding chair time between a resin-modified, self-
cured glass-ionomer cement and a composite resin: a radomized controlled trial. Prog. Orthod.
2001:9-13.
21. Diedrich P. Enamel alterations from bracket bonding and debonding: a study with the
scanning electron microscope. Am J Orthod 1981;79:500-522.
22. Zachrisson BU, Skogan O, Hoymyhr S. Enamel cracks in debonded, debanded, and
orthodontically untreated teeth. Am J Orthod 1980;77:307-319.
23. Lissac M, Metrop D, Brugirard J, Coudert JL, Pimmel P, Briguet A et al. Dental materials
and magnetic resonance imaging. Invest Radiol 1991;26:40-45.
24. Abbaszadeh K, Heffez LB, Mafee MF. Effect of interference of metallic objects on
interpretation of T1-weighted magnetic resonance images in the maxillofacial region Oral Surg
Oral Med Oral Pathol Oral Radiol Endod. United States; 2000. p. 759-765.
25. Hinshaw DB, Jr., Holshouser BA, Engstrom HI, Tjan AH, Christiansen EL, Catelli WF.
Dental material artifacts on MR images. Radiology 1988;166:777-779.
26. Elison JM, Leggitt VL, Thomson M, Oyoyo U, Wycliffe ND. Influence of common
orthodontic appliances on the diagnostic quality of cranial magnetic resonance images Am J
Orthod Dentofacial Orthop. United States; 2008. p. 563-572.
27. Okano Y, Yamashiro M, Kaneda T, Kasai K. Magnetic resonance imaging diagnosis of the
temporomandibular joint in patients with orthodontic appliances Oral Surg Oral Med Oral Pathol
Oral Radiol Endod. United States; 2003. p. 255-263.

89
28. Fache JS, Price C, Hawbolt EB, Li DK. MR imaging artifacts produced by dental materials.
AJNR Am J Neuroradiol 1987;8:837-840.
29. Eggers G, Rieker M, Kress B, Fiebach J, Dickhaus H, Hassfeld S. Artefacts in magnetic
resonance imaging caused by dental material. MAGMA 2005;18:103-111.
30. Holton A, Walsh E, Anayiotos A, Pohost G, Venugopalan R. Comparative MRI
compatibility of 316 L stainless steel alloy and nickel-titanium alloy stents. J Cardiovasc Magn
Reson 2002;4:423-430.
31. Kemper J, Priest AN, Schulze D, Kahl-Nieke B, Adam G, Klocke A. Orthodontic springs and
auxiliary appliances: assessment of magnetic field interactions associated with 1.5 T and 3 T
magnetic resonance systems. Eur Radiol 2007;17:533-540.
32. Schenck JF. The role of magnetic susceptibility in magnetic resonance imaging: MRI
magnetic compatibility of the first and second kinds. Med Phys 1996;23:815-850.
33. Russell JS. Aesthetic orthodontic brackets. J Orthod 2005;32:146-163.
34. Faltermeier A, Rosentritt M, Reicheneder C, Mussig D. Experimental composite brackets:
influence of filler level on the mechanical properties. Am J Orthod Dentofacial Orthop
2006;130:699.e699-614.
35. Shellock FG, Kanal E. Magnetic resonance: Bioeffects, safety and patient management. New
York: Raven Press; 1994.
36. Kuehn BM. FDA warning: remove drug patches before MRI to prevent burns to skin Jama.
United States; 2009. p. 1328.
37. Regier M, Kemper J, Kaul MG, Feddersen M, Adam G, Kahl-Nieke B et al. Radiofrequency-
induced heating near fixed orthodontic appliances in high field MRI systems at 3.0 Tesla. J
Orofac Orthop 2009;70:485-494.
38. Lissac M, Coudert JL, Briguet A, Amiel M. Disturbances caused by dental materials in
magnetic resonance imaging. Int Dent J 1992;42:229-233.
39. Masumi S, Arita M, Morikawa M, Toyoda S. Effect of dental metals on magnetic resonance
imaging (MRI). J Oral Rehabil 1993;20:97-106.
40. Shalish M, Dykstein N, Friedlander-Barenboim S, Ben-David E, Gomori JM, Chaushu S.
Influence of common fixed retainers on the diagnostic quality of cranial magnetic resonance
images. Am J Orthod Dentofacial Orthop 2015;147:604-609.
41. Magnetism in Stainless Steel Fasteners.[Internet] [cited: 2014 Jan 14]. Available from:
https://www.fastenal.com/en/75/magnetism-in-stainless-steel-fasteners

90
42. Di Muzio B, Taghi Niknejad M. Fluid attenuaton inversion recovery [Internet]. [updated:
June 2015; cited: 2015 July]. Available from: http://radiopaedia.org/articles/fluid-attenuation-
inversion-recovery.
43. Bashir U. Time of flight angiography [Internet]. [updated: June 2015; cited: 2015
July].Available from: http://radiopaedia.org/articles/time-of-flight-angiography-1.
44. Krupa K, Bekiesińska-Figatowska M. Artifacts in magnetic resonance imaging. Pol J Radiol
2015;80:93-106.
45. Le Bihan Dea. Artifacts and Pitfalls in Diffusion MRI. Journal of Magnetic Resonance
Imaging 2006:478-488.
46. Fanea L, Fagan AJ. Review: magnetic resonance imaging techniques in ophthalmology. Mol
Vis 2012;18:2538-2560.
47. Gutierrez LB, Do BH, Gold GE, Hargreaves BA, Koch KM, Worters PW et al. MR imaging
near metallic implants using MAVRIC SL: initial clinical experience at 3T. Acad Radiol
2015;22:370-379.
48. Liebl H, Heilmeier U, Lee S, Nardo L, Patsch J, Schuppert C et al. In vitro assessment of
knee MRI in the presence of metal implants comparing MAVRIC-SL and conventional fast spin
echo sequences at 1.5 and 3 T field strength. J Magn Reson Imaging 2015;41:1291-1299.
49. Zho SY, Kim MO, Lee KW, Kim DH. Artifact reduction from metallic dental materials in
T1-weighted spin-echo imaging at 3.0 tesla. J Magn Reson Imaging 2013;37:471-478.

91
APPENDICES
Appendix 1. University of Toronto Research Ethics Board approval

92

93
Appendix 2: The Hospital for Sick Children Toronto Research Ethics Board approval

94
Appendix 3: Invitation letter to subjects for participation
Version: Sep 3 2014
FACULTY OF DENTISTRY, UNIVERSITY OF TORONTO
124 Edward Street, Toronto, Ontario M5G 1G6
HOSPITAL FOR SICK CHILDREN, TORONTO
555 University Avenue, Toronto Ontario M5G 1X8
CANADA
Title of the Project:
Effects of orthodontic appliances on diagnostic quality of MR images of the head.
Dear
You are invited to participate in a clinical research study being conducted at the Faculty
of Dentistry, University of Toronto and the Hospital for Sick Children, Toronto. The aim of the
study is to investigate the influence of commonly used orthodontic braces and appliance parts on
magnetic resonance images (MRI) frequently used in hospitals to diagnose different medical

95
conditions. MRI has been used in medicine for more than 30 years and has not been shown to
have deleterious effects on humans.
The study will involve your MR imaging with removable braces. First, you will have two
appointments in the Orthodontic Clinic, Faculty of Dentistry, University of Toronto which will
last about 30 and 15 minutes respectively. In the first appointment, orthodontic impressions of
your upper and lower teeth will be taken. In the second visit, the Essix retainer trays with the
appliances embedded in them will be tried on your teeth to check for their fit. After that, you will
be taken to the MRI section of the department of Diagnostic Imaging at the Hospital for Sick
Children where your MR scans will be made. It will take about 2 hours. Your total time spent
will be around 2hours and 45 minutes.
Your participating in this study will provide information that will be useful for MR
imaging of the patients with braces. You will always retain the right to withdraw your consent to
participate in the study at any time.
If you agree to participate in this study, you will help to improve understanding of MR
imaging of the patients with braces. You will also be compensated $ 75 for the participation at
the end of the MRI acquisition.
Thank you in advance for your participation in the study.

96
The study is being conducted by Dr Dzmitry Zhylich as a part of his Masters project at the
Faculty of Dentistry, University of Toronto under primary supervision of Dr Sunjay Suri,
Associate Professor of Discipline of Orthodontics.
Co-investigators:
Dr. Andrea Doria, Chief of Research, Radiologist, Department of Diagnostic Imaging The
Hospital for Sick Children, Associate Professor, Co-Director of Research, Department of
Medical Imaging, University of Toronto
Dr. Bryan Tompson,Head, Division of Orthodontics, Department of Dentistry The Hospital
for Sick Children, Discipline Head, Orthodontics Faculty of Dentistry, University of Toronto
Dr. Wendy Lou
Head, Division of Biostatistics, Dalla Lana School of Public Health
University of Toronto
Ms. Tammy Rayner-Kunopaski
MRI Technologist, Department of Diagnostic Imaging,
The Hospital for Sick Children
Feel free to contact Dr Zhylich for any questions or concerns by telephone at 416-979-
4750 ext 3039 or via e-mail: [email protected] or his supervisor, Dr Suri by

97
telephone at 416 979 4924 ext 4397 at the Discipline of Orthodontics, Faculty of Dentistry,
University of Toronto, 124 Edward Street, Toronto M5G 1G6.

98
Appendix 4. Research Consent Form
Version: Sep 10 2014
Appendix 2 : Consent Form.
Research Consent Form
Title of Research Project:
Effects of orthodontic appliances on diagnostic quality of MR images of the head
Investigators:

99
1. Principal Investigator:
Dr Sunjay Suri,
Staff Orthodontist, Department of Dentistry
The Hospital for Sick Children
Associate Professor
Discipline of Orthodontics, Faculty of Dentistry, University of Toronto
Telephone 416-979-4924 ext 4397
e-mail: [email protected]
2. Co-investigator 1.
Dr. Dzmitry Zhylich
Graduate MSc. Student
Discipline of Orthodontics, Faculty of Dentistry, University of Toronto.
Telephone 416-979-4750 ext 3039
e-mail: [email protected]
3. Co-investigator 2.
Dr. Andrea Doria
Chief of Research, Radiologist, Department of Diagnostic Imaging
The Hospital for Sick Children
Associate Professor, Co-Director of Research, Department of Medical Imaging,
University of Toronto
Telephone 416-813-6079

100
e-mail: [email protected]
4. Co-investigator 3.
Dr. Bryan Tompson
Head, Division of Orthodontics, Department of Dentistry
The Hospital for Sick Children
Discipline Head, Orthodontics
Faculty of Dentistry, University of Toronto
Telephone 416-979-4924 ext.4396
e-mail: [email protected]
5. Co-investigator 4.
Dr. Wendy Lou
Head, Division of Biostatistics, Dalla Lana School of Public Health
University of Toronto
Telephone 416-946-7804
e-mail: [email protected]
6. Co-investigator 5
Ms. Tammy Rayner-Kunopaski
MRI Technologist, Department of Diagnostic Imaging,
The Hospital for Sick Children
Telephone: 416-813-6060

101
e-mail: [email protected]
Purpose of the Research:
The aim of the study is to investigate the influence of commonly used orthodontic braces and
appliance parts on magnetic resonance images (MRI) frequently used in hospitals to diagnose
different medical conditions. We wish to make your MR images with different removable
braces. Your participating in this study will provide information that will be useful for MR
imaging of the patients with braces.
Description of the Research:
The study will involve your MR imaging with removable braces. First, you will have two
appointments in the Orthodontic Clinic, Faculty of Dentistry, University of Toronto which will last
about 30 and 15 minutes respectively. In the first appointment, orthodontic impressions of your
upper and lower teeth will be taken. In the second visit, the Essix retainer trays with the appliances
embedded in them will be tried on your teeth to check for their fit. After that, you will be taken to
the MRI section of the department of Diagnostic Imaging at the Hospital for Sick Children where
your MR scans will be made. It will take about 2 hours. Your total time spent will be around 2hours
and 45 minutes
Potential Harms:
We know of no harm that taking part in this study could cause you.

102
Potential Discomforts or Inconvenience:
Potential Discomforts or Inconveniences include the length of MRI acquisition, participation in 3
visits, potential discomfort of dental impressions (although these are very routine and are not known
to cause any significant level of discomfort or inconvenience). Increase in skin temperature during 3
Tesla MRI scanning of the head has been described in the literature to be insignificant (within 0.5
degrees), with no discomfort reported. The use of imaging at 3 Tesla MRI scanners is common
practice in Canada, scanners are commercially available and have Health Canada approval. The 3T
MRI machines have Specific Absorption Rates set which do not allow the sequences to go beyond
FDA approved limits and the SAR values for all such sequences are much below allowed limits.
Also the sequences described in the proposal are those which are used routinely in clinical practice.
However, if you feel any discomfort or a significant rise in temperature during MR scanning, please
notify the MRI technician immediately, and further tests on the material that led to the rise in
temperature will be terminated.
Potential Benefits:
To individual subjects:
A better understanding of the MR imaging of the patients with braces will result from the study. This
will reduce the financial and biological burden and risks associated with removal and reinstallation
of braces for orthodontic patients needing MRI. Considering orthodontic treatment is very common

103
today, the results of this study will potentially benefit you if you need to have MRI concurrently with
braces in your future life.
There may be a possibility of incidental findings on your MRI of which you will be fully informed.
The results of the research will be available to the public in the University of Toronto Faculty of
Dentistry Library. A short summary of the study findings will additionally be provided to you.
To society:
A better understanding of the MR imaging of the patients with fixed braces will result from the
study. This will reduce the financial and biological burden and risks associated with removal and
reinstallation of the fixed braces for the orthodontic patients needing MRI which is a major
limitation under existing conditions.
Confidentiality:
We will respect your privacy. No information about who you are will be given to anyone or be
published without your permission, unless required by law. For example, the law could make us give
information about you if a child has been abused, if you have an illness that could spread to others, if
you or someone else talks about suicide (killing themselves), or if the court orders us to give them
the study papers.

104
The data produced from this study will be stored in a secure, locked location. Only members of the
research team (and maybe those individuals described above) will have access to the data. This could
include external research team members. Following completion of the research study the data will be
kept as long as required then destroyed as required by Sick Kids policy. Published study results will
not reveal your identity.
Reimbursement:
If you agree to participate in this study, you will help to provide information that will be useful for
MR imaging of the patients with braces. We will also provide you with some compensation, $ 75 in
recognition of your time and effort after the completion of the MR imaging.
Participation:
It is your choice to take part in this study. You can stop at any time. The care you get at Sick Kids or
at the Faculty of Dentistry, University of Toronto will not be affected in any way by whether you
take part in this study.
New information that we get while we are doing this study may affect your decision to take part in
this study. If this happens, we will tell you about this new information. And we will ask you again if
you still want to be in the study.

105
If you become ill or are harmed because of study participation, we will treat you for free. Your
signing this consent form does not interfere with your legal rights in any way. The staff of the study,
any people who gave money for the study, or the hospital are still responsible, legally and
professionally, for what they do.
Sponsorship:
The sponsors/funders of this research are:
1) Principal investigator Dr. Sunjay Suri, Department of Orthodontics, Faculty of Dentistry,
University of Toronto.
2) Department of Orthodontics, Faculty of Dentistry, University of Toronto
3) Companies donating braces for the study
Conflict of Interest:
I, and the other research team members have no conflict of interest to declare.
Consent :
By signing this form, I agree that:
1) You have explained this study to me. You have answered all my questions.

106
2) You have explained the possible harms and benefits (if any) of this study.
3) I know what I could do instead of taking part in this study. I understand that I have the right not
to take part in the study and the right to stop at any time. My decision about taking part in the study
will not affect my health care at Sick Kids.
4) I am free now, and in the future, to ask questions about the study.
5) I have been told that my medical records will be kept private except as described to me.
6) I understand that no information about who I am will be given to anyone or be published without
first asking my permission.
7) I agree, or consent, to take part in this study.
_________________________________
Printed Name of Subject & Age Subject’s signature & date
_________ _________________________________
Printed Name of person who explained consent Signature of Person who explained consent & date

107
_______________________________________ __________________________________
Printed Witness’ name (if the subject/legal guardian Witness’ signature & date
does not read English)
If you have any questions about this study, please Dr.Dzmitry Zhylich at 416-979-4750 ext.3039
If you have questions about your rights as a subject in a study or injuries during a study, please call
the Research Ethics Manager at 416-813-5718.

108
Appendix 5. MRI screening form.

109
Appendix 6. Case Report Form for the study: “Effects of orthodontic appliances on
diagnostic quality of MR images of the head. Version: Sep 3 2014

110
Appendix 7. Randomized order of the appliances for 10 subjects.
N Appliance sequence MRI Date
1 1-metal (M)
2-ceramic (C)
3-ceramic+metal(C+M)
4-lingual retainer (LR)
5-Essix (E)
6-No appliance (N)
14.10.2014
2 1-M
2-C
3-C+M
4-LR
14.10.2014
3 1-M
2-C
3-C+M
4-LR
14.10.2014
4 1-C
2-LR
3-M
4-C+M
1.12.2014
5 1-LR
2-M
3-C
4-C+M
2.12.2014
6 1-C
2-C+M
3-M
4-LR
3.12.2014
7 1-C
2-LR
3-M
4-C+M
4.12.2014
8 1-C+M
2-M
3-LR
4-C
11.12.2014
9 1-C
2-M
3-C+M
4-LR
19.12.2014
10 1-C
2-LR
3-M
4-C+M
23.12.2014

Appendix 8. Representative sagittal and axial images for scores 1 to 5 (frontal lobe of the brain was scored). Sa
gitt
al im
ages
(T1
)
Sco
re
1 2 3 4 5
Axi
al im
ages
Axial T2 Axial DWI Axial DWI Axial DWI Axial DWI
DWI-diffusion-weighted sequence.