Embed Size (px)
Citation preview
Effects of interferon-beta on plasma lipid and lipoproteincomposition and post-heparin lipase activitiesin patients with chronic hepatitis C
R. J. ANDRADE, M. D. GARCIÂA-ESCANÄ O, P. VALDIVIELSO, R. ALCAÂ NTARA,
M. A. SAÂ NCHEZ-CHAPARRO & P. GONZAÂ LEZ-SANTOS
Liver Unit, Department of Medicine, School of Medicine, University of MaÂlaga, MaÂlaga, Spain
Accepted for publication 16 March 2000
INTRODUCTION
Interferons are naturally occurring cytokines involved
in host defenses against a variety of infectious agents
and in¯ammation.1 Interferons are clinically useful in
some malignant, viral, immmunological, angiogenic,
in¯ammatory and ®brotic diseases.2 Currently, inter-
ferons are also the ®rst line therapy for chronic hepatitis
C virus infection.3 Most studies of the effects of
interferons in patients with chronic hepatitis C have
used recombinant-derived (alpha 2a or 2b) or naturally
produced (lymphoblastoid) interferon-a,3, 4 and some
authors have found changes in lipid and lipoprotein
composition during interferon-a therapy. The most
notable changes have been an increase in total and
very low density lipoprotein (VLDL) triglycerides and a
decrease in high density lipoprotein (HDL) choles-
terol.5, 6 In addition, severe hypertriglyceridaemia and
chylomicronaemia have been reported in a few patients
treated with interferon-a.6±10 In such patients, pre-
treatment triglyceride levels were usually elevated.6, 7
Interferon-b, a naturally produced cytokine derived
from epithelial cells and ®broblasts is also marketed for
the treatment of chronic hepatitis C in several European
countries and Japan.3 Recently, interferon-b has also
shown ef®cacy in the therapy of multiple sclerosis.11
SUMMARY
Background: Interferon therapy has been shown to
induce lipid abnormalities.
Aim: We assessed the effects of interferon-b on the
lipoprotein pro®le and post-heparin lipase activities in
26 normolipaemic patients with chronic hepatitis C.
Methods: Interferon-b was administered subcutaneously
at doses of 6 ´ 106 U (units) three times a week, over
6 months, and lipoproteins and post-heparin lipases
were measured at baseline and at the end of therapy.
Results: Plasma triglycerides increased by 21% due to
preferential enrichment in those contained in the very
low density lipoprotein (VLDL) and low density lipo-
protein (LDL) fractions. The concentration of choles-
terol decreased slightly in the high density lipoprotein
(HDL) subfractions. Lipoprotein lipase, but not hepatic
lipase activity decreased by a 36%, and this change
showed a signi®cant negative correlation with changes
in plasma triglycerides. Five patients (19.5%) responded
to interferon-b therapy. The lipoprotein pro®le was no
different between responders and non-responders to
therapy.
Conclusions: Interferon-b treatment in normolipaemic
patients with chronic hepatitis C induced moderate
disturbances in plasma lipoproteins, associated with
inhibition of lipoprotein lipase activity.
Correspondence to: Dr R. J. Andrade, Unidad de HepatologõÂa, Departamento
de Medicina, Facultad de Medicina, Campus Universitario de Teatinos s/n,
29071, MaÂlaga, Spain.E-mail: [email protected]
Aliment Pharmacol Ther 2000; 14: 929±935.
Ó 2000 Blackwell Science Ltd 929

Although lipid disturbances have been noted in associ-
ation with interferon-b therapy, neither the lipoprotein
pro®le nor the mechanism whereby interferon-b causes
such changes have been fully investigated.12, 13
In the present study we prospectively evaluated the
effects of interferon-b therapy on lipoprotein pattern and
post-heparin lipase activities in normolipaemic patients
with chronic hepatitis C, and examined the relationship
of these effects with the response to treatment.
MATERIALS AND METHODS
The study was designed and conducted at the Liver
Unit, University Hospital of MaÂlaga (Spain) and was
supported by Department of Medicine. It was not a part
of a sponsored study.
Patients
A total of 26 consecutive patients with chronic hepatitis
C were prospectively included in the study between
April and June 1996. To be included, a patient had to
have hepatitis C virus antibodies detectable by ELISA
(Ortho Diagnostics, NeckargemuÈ n, Germany),1 RNA
positivity by the polymerase chain reaction (Amplicor,
Hoffmann-La Roche, Basel, Switzerland), and biopsy-
proven chronic hepatitis within 6 months prior to the
study. Exclusion criteria were: positive serology for
hepatitis B virus infection or human immunode®ciency
virus; cirrhosis; marked obesity (body mass index > 30);
diabetes; hyperlipemia (cholesterol > 240 mg/dL; tri-
glycerides > 150 mg/dL), or any other disease known
to alter the lipid pro®le; history of alcohol use; or
therapy with drugs known to in¯uence plasma lipid or
lipoproteins. Patients were instructed not to alter their
dietary habits during the course of the study.
Patients received interferon-b (Frone, Serono, Madrid,
Spain) subcutaneously at a dose of 6 ´ 106 U, three
times a week over a 6-month period. The objective of this
study, speci®cally designed to evaluate lipid changes
during interferon-b therapy, was thoroughly explained
to all participants, who signed an informed consent.
Assessment of ef®cacy
Parameters monitored in all patients at baseline and
at the end of therapy were: body mass index, serum
glucose, aspartate aminotransferase, alanine amino-
transferase, bilirubin, albumin and prothrombin activity.
The response to treatment was de®ned according to the
criteria of the National Institutes of Health Consensus
Development Conference on Hepatitis C as normal
serum alanine aminotransferase concentrations and
undetectable serum hepatitis C virus RNA levels at the
end of therapy.14
Liver biopsy specimens obtained before treatment and
at the end of the follow-up period were interpreted by a
single pathologist in a blinded fashion. The degree of
hepatic in¯ammation and ®brosis was scored with the
Knodell histological activity index.15 In¯ammation and
®brosis scores were evaluated separately.
Lipoprotein analysis
Lipid and lipoproteins were evaluated at baseline and at
the end of therapy. Fasting blood specimens were
collected by venipuncture into tubes containing sodium
EDTA, and were centrifuged at 1500 g for 30 min at
4 °C. Total cholesterol, triglycerides and phospholipids
in plasma, and lipoprotein fractions were assayed
enzimatically in a Cobas MIRA autoanalyser (Hoff-
mann-La Roche). Very low density lipoprotein (VLDL),
low density lipoprotein (LDL), and high ensity lipopro-
tein subfractions (HDL2 and HDL3) were isolated by
sequential ¯otation in a preparative ultracentrifuge
(Beckman L8±55 M, Palo Alto, California, USA) accord-
ing to the method of Havel et al.,2 using a 50.3 Ti
Beckman rotor.16 With the addition of a KBr + NaCl
mixture, each lipoprotein was fractionated at the follow-
ing densities: VLDL, d < 1.006 g/mL; LDL, d � 1.006±
1.063 g/mL; HDL2, d � 1.063±1.125 g/mL; and HDL3,
d � 1.125±1.210 g/mL.
Activities of lipoprotein lipase and hepatic lipase
in postheparin plasma
Lipolytic enzymes are anchored to the vessel wall, but
can be removed by infusing molecules with high af®nity
to lipases3 , such as heparin. Lipolytic activities should
therefore be assayed in post-heparin plasma. Plasma
samples were obtained 10 min after the intravenous
injection of heparin at a dose of 50 UI/kg body weight,
and stored at )70 °C until assay. The activities of
lipoprotein lipase and hepatic lipase were measured by a
radioisotopic method using H3-Triolein as a substrate,
emulsi®ed by sonication with Triton X-100 (Branson
250, Danbury, Connecticut, USA). Post-heparin lipase
activity was measured as the difference in salt sensitiv-
930 R. J. ANDRADE et al.
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 929±935
ity: the enzymatic activity of lipoprotein lipase is
inhibited by high salt concentrations, whereas hepatic
lipase is active in 1 M NaCl.17 In addition, apolipopro-
tein (Apo) C-II is required as a co-factor for maximal
lipoprotein lipase activity, whereas hepatic lipase has no
co-factor requirements.
To measure post-heparin lipase activities, each assay
was performed in triplicate tubes, including a no-plasma
blank, with plasma, and with plasma plus 1 M NaCl. All
tubes (refrigerated on ice) contained 200 lL of substrate
and 10 lL of post-heparin plasma. For the tubes with
salt (hepatic lipase activity), 50 lL 5 M NaCl was added.
For tubes without a high salt concentration, 50 lL of
human plasma with Apo-CII (0.1 M NaCl; total activity
of post-heparin plasma) was added. The tubes were
incubated at 37 °C for 1 h and the reaction was then
stopped by adding 3 mL of methanol/chloroform/hep-
tane (1.4:1.25:1.0; v/v/vol) with 1 mL carbonate/
borate buffer, pH 10.5. Fatty acids were extracted by
the method of Belfrage and Vaughan.18 After vortexing,
the samples were centrifuged at 1500 g4 for 15 min at
4 °C. One millilitre of the top fraction (aqueous phase)
was then removed and radioactivity was determined.
Lipoprotein lipase activity was determined by subtract-
ing hepatic lipase activity (samples plus 1 M NaCl) from
total Phepatic lipase activity. Paired samples (i.e. before
and after treatment) were assayed in the same batch.
Whitin-batch coef®cient of variation for total post-
heparin lipase activity and hepatic lipase activity were
2.3% and 9.4%, respectively. All enzyme activities are
expressed as micromoles of free fatty acids per hour per
millilitre of plasma.
Statistical analysis
All values are expressed as the mean � s.d. Statistical
analysis was performed with statistical software (SPSS/
PC+, SPSS Inc, Chicago, IL) on a personal computer.
Student's paired t-test was used for comparisons
between values before and after treatment with inter-
feron-b, when the means of variables were distributed
normally. For lipoproteins and post-heparin lipase
activities, pairwise comparisons were tried. However,
the Wilcoxon signed ranks test was used because the
values did not show a normal distribution. For other
comparisons we used the non-parametric Mann±Whit-
ney test. Data were analysed by calculating Pearson's
correlation coef®cient.
RESULTS
The characteristics of the patients at the start of
interferon-b therapy are shown in Table 1. No patient
had any serious or potentially life-threatening complica-
tions, and all patients completed the trial, receiving the
same total dose of interferon-b (432 ´ 106 U). No
signi®cant changes were observed, after interferon-btreatment, in body mass index, leucocyte and platelet
count or liver function as measured by bilirubin, albumin
and prothrombin time. A slight increase in haemoglobin
levels and a decrease in serum glucose (both within the
normal range) at the end of therapy was noted (median
values: basal 15 � 1.1 g/dL; 6 months 15.5 � 1.2 g/dL,
P < 0.01; basal 106.3 � 19.1 mg/dL; 6 months
102.6 � 19.5 mg/dL, P < 0.05, respectively).
Table 2 shows the effect of interferon-b therapy on the
concentration of cholesterol, triglycerides and phospho-
lipids in plasma and on the lipoprotein fractions. After
6 months of treatment, mean plasma triglyceride level
had increased by 21%, whereas no changes were noted
in the plasma concentration of total cholesterol and
phospholipids. All lipoprotein fractions were enriched in
triglycerides, but the increases were statistically signif-
icant only in the VLDL and LDL fractions. In contrast
there was a slight (but not statistically signi®cant)
decrease in HDL cholesterol due to that contained in
both subfractions HDL2 and HDL3.
Table 1. General characteristics and demographic variables
before treatment with interferon-b in patients with chronic
hepatitis C*
Age (years) 39 � 12
Male sex (%) 15 (58%)
Body mass index (kg/m2) 27.1 � 3.5
Serum glucose (mg/dL) 106 � 19
Leucocyte ´109/L 6.9 � 1.8
Platelet ´109/L 190 � 43
Haemoglobin (g/dL) 15 � 1.1
Bilirubin (mg/dL) 0.75 � 0.2
AST (U/L) 61 � 28
ALT (U/L) 97 � 48
c-GT (U/L) 51 � 32
Alkaline phosphatase (U/L) 182 � 62
Albumin (g/dL) 4.6 � 0.3
Prothrombin activity (%) 115 � 15
Knodell HAI 9 � 4
* Values are means � s.d. or number of cases (%).
AST, aspartate aminotransferase; ALT, alanine aminotransferase;
HAI, histological activity index.
INTERFERON-BETA AND POST-HEPARIN LIPASES IN CHRONIC HEPATITIS C 931
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 929±935
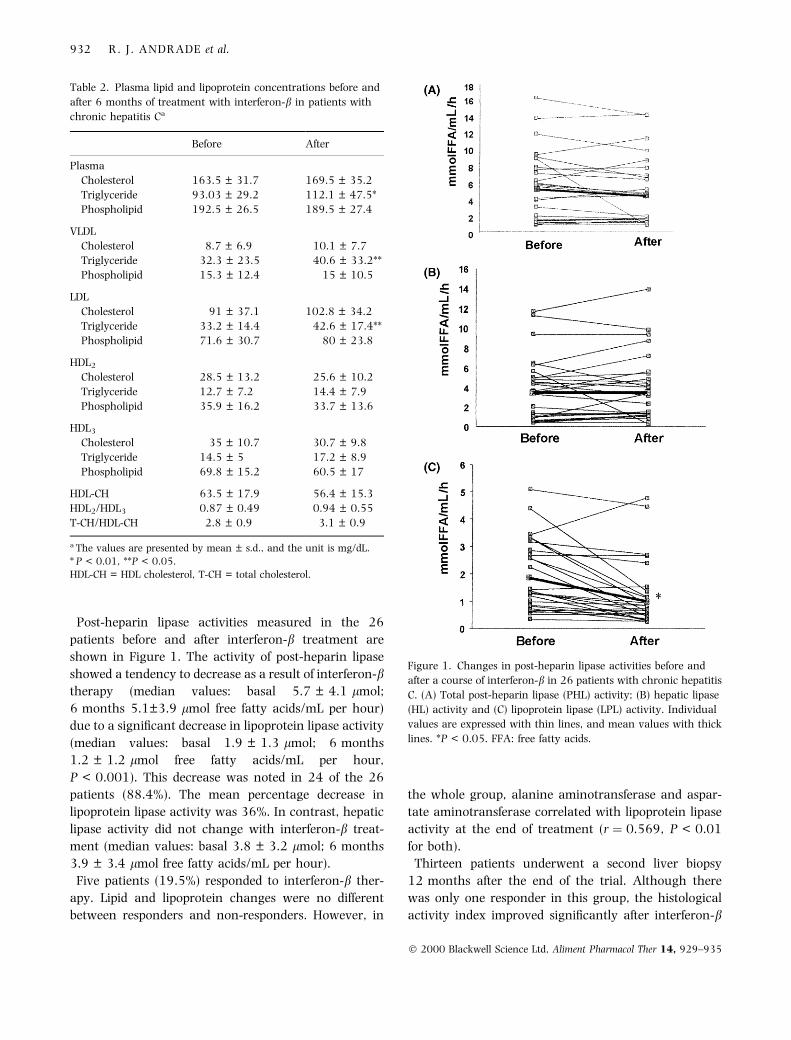
Post-heparin lipase activities measured in the 26
patients before and after interferon-b treatment are
shown in Figure 1. The activity of post-heparin lipase
showed a tendency to decrease as a result of interferon-btherapy (median values: basal 5.7 � 4.1 lmol;
6 months 5.1�3.9 lmol free fatty acids/mL per hour)
due to a signi®cant decrease in lipoprotein lipase activity
(median values: basal 1.9 � 1.3 lmol; 6 months
1.2 � 1.2 lmol free fatty acids/mL per hour,
P < 0.001). This decrease was noted in 24 of the 26
patients (88.4%). The mean percentage decrease in
lipoprotein lipase activity was 36%. In contrast, hepatic
lipase activity did not change with interferon-b treat-
ment (median values: basal 3.8 � 3.2 lmol; 6 months
3.9 � 3.4 lmol free fatty acids/mL per hour).
Five patients (19.5%) responded to interferon-b ther-
apy. Lipid and lipoprotein changes were no different
between responders and non-responders. However, in
the whole group, alanine aminotransferase and aspar-
tate aminotransferase correlated with lipoprotein lipase
activity at the end of treatment (r � 0.569, P < 0.01
for both).
Thirteen patients underwent a second liver biopsy
12 months after the end of the trial. Although there
was only one responder in this group, the histological
activity index improved signi®cantly after interferon-b
Table 2. Plasma lipid and lipoprotein concentrations before and
after 6 months of treatment with interferon-b in patients with
chronic hepatitis Cã
Before After
Plasma
Cholesterol 163.5 � 31.7 169.5 � 35.2
Triglyceride 93.03 � 29.2 112.1 � 47.5*
Phospholipid 192.5 � 26.5 189.5 � 27.4
VLDL
Cholesterol 8.7 � 6.9 10.1 � 7.7
Triglyceride 32.3 � 23.5 40.6 � 33.2**
Phospholipid 15.3 � 12.4 15 � 10.5
LDL
Cholesterol 91 � 37.1 102.8 � 34.2
Triglyceride 33.2 � 14.4 42.6 � 17.4**
Phospholipid 71.6 � 30.7 80 � 23.8
HDL2
Cholesterol 28.5 � 13.2 25.6 � 10.2
Triglyceride 12.7 � 7.2 14.4 � 7.9
Phospholipid 35.9 � 16.2 33.7 � 13.6
HDL3
Cholesterol 35 � 10.7 30.7 � 9.8
Triglyceride 14.5 � 5 17.2 � 8.9
Phospholipid 69.8 � 15.2 60.5 � 17
HDL-CH 63.5 � 17.9 56.4 � 15.3
HDL2/HDL3 0.87 � 0.49 0.94 � 0.55
T-CH/HDL-CH 2.8 � 0.9 3.1 � 0.9
ã14 The values are presented by mean � s.d., and the unit is mg/dL.
* P < 0.01, **P < 0.05.HDL-CH = HDL cholesterol, T-CH = total cholesterol.
Figure 1. Changes in post-heparin lipase activities before and
after a course of interferon-b in 26 patients with chronic hepatitis
C. (A) Total post-heparin lipase (PHL) activity; (B) hepatic lipase
(HL) activity and (C) lipoprotein lipase (LPL) activity. Individual
values are expressed with thin lines, and mean values with thick
lines. *P < 0.05. FFA: free fatty acids.
932 R. J. ANDRADE et al.
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 929±935
treatment (median values: ®rst biopsy 9.8 � 3.75 ; second
biopsy 7.2 � 3.36 , P < 0.05). Histological improvement
was exclusively due to a decrease in the in¯ammatory
scores from 7.6 � 2.77,8 to 5.0 � 2.67,8 (P < 0.01); there
was no changes in the ®brosis score (median values:
®rst biopsy 2.0 � 1.19;10 ; second biopsy 2.1 � 1.19;10 ).
Table 3 shows simple correlation coef®cients for the
changes in lipoprotein lipase, hepatic lipase and post-
heparin lipase activities and those of serum lipids and
lipoproteins during 6 months of treatment with inter-
feron-b. The change (D) in post-heparin lipase and
lipoprotein lipase activities before and after 6 months of
treatment with interferon-b showed a signi®cant neg-
ative correlation with D plasma triglycerides. In addi-
tion, the change in HL11 activity after treatment with
interferon-b showed a signi®cant positive correlation
with D histological activity index in all 13 patients
evaluated (r � 753, P < 0.01).
DISCUSSION
Among their multiple systemic effects, interferons have
been found to in¯uence lipid and lipoprotein metabo-
lism.19, 20 Taking into account that lipoprotein lipase
and hepatic lipase are two key enzymes in the
metabolism and interconversion of lipoproteinsÐas
demonstrated by the major derangements of lipopro-
teins in individuals with genetic defectsÐlipase
activities should be measured in studies of the effects
of diet, drugs or other factors on lipoprotein metabo-
lism.21
In this prospective study a 6-month course of inter-
feron-b in normolipemic patients with chronic hepatitis
C was associated with disturbances in plasma lipopro-
tein metabolism as de®ned by a signi®cant increase in
total, VLDL and LDL triglycerides as well as a tendency
for HDL cholesterol levels to decrease. These changes
paralleled a marked inhibition in lipoprotein lipase (but
not in hepatic lipase) activity. Because no other
confounding factors such as diabetes, liver function
deterioration, changes in body mass index or concur-
rent therapy with other drugs were present during the
trial, the lipid alterations were probably related to
interferon-b. We did not include hyperlipaemic patients
because of the potential risk of severe hypertrygliceri-
daemia and to avoid interferences with lipases assay.
We used 6 ´ 106 U of interferon-b three times a week.
However, the optimal dose regimen of interferon-b for
chronic hepatitis C has not yet been established.3, 22
Doses of 9±12 ´ 106 U three times a week have been
reported to be as effective as 6 ´ 106 U of interferon-a in
terms of response to treatment.23
The effects of interferon-b on lipid metabolism are little
known. When administered for 10 days, to patients
with stable renal cancer, daily interferon-b serine (a
recombinant DNA-derived interferon-b) injections dur-
ing 9 days produced rapid and dose-dependent increases
in plasma triglyceride concentrations of 74% at 4.5 MU,
and 136% at 9.0 MU.24 Furthermore, in this study the
reductions in LDL cholesterol of 28% and 50% occurred
later than the reductions in triglycerides. In a small
study involving patients with chronic hepatitis C, 6 MU
of interferon-b daily caused a time-dependent increase
in triglycerides during 14 days of therapy.12 Therefore,
the more modest increase in triglyceride concentrations
and the absence of reduction in LDL cholesterol
observed in our study could be due to the different dose
regimen and time-point.
Similar changes have recently been reported in
association with interferon-a therapy.5, 6 Shinohara
et al. also tested the activity of post-heparin lipases
before and after a short-term course (2 weeks) of high
daily doses (9 MU) of interferon-a 2a, and found a
Table 3. Simple correlation coef®cients between changes in lipo-
protein lipase, hepatic lipase and post-heparin lipase activities and
serum lipids and lipoproteins during 6 months of interferon-btreatment in patients with chronic hepatitis C
DLPL
Activity
D HL
activity
D PHL
activity
D Total cholesterol 0.024 0.383 0.353
D Triglycerides )0.397* )0.321 )0.468*
D HDL-cholesterol )0.016 0.312 0.264
VLDL
D Cholesterol )0.295 0.012 )0.123
D Triglycerides )0.306 )0.103 0.037
LDL
D Cholesterol 0.075 0.050 0.084
D Triglycerides )0.220 )0.252 0.192
HDL2
D Cholesterol 0.050 0.319 0.306
D Triglycerides )0.051 )0.304 )0.309
HDL3
D Cholesterol )0.073 0.203 0.137
D Triglycerides 0.028 )0.001 0.083
* P < 0.05.
D, change in value after treatment with interferon-b.
INTERFERON-BETA AND POST-HEPARIN LIPASES IN CHRONIC HEPATITIS C 933
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 929±935

decrease in both lipoprotein lipase and hepatic lipase
activities.5
The mechanism(s) for such interferon-b-induced dis-
turbances in lipoprotein metabolism are unclear. A
variety of cytokines, including TNF12 -a, interleukin-1,
interferon-a and interferon-c, inhibit lipoprotein lipase
activity in post-heparin plasma, adipose tissue, or both,
and these cytokines and interferon-b inhibit adipose
tissue lipogenesis.25±28 The reduced lipoprotein lipase
activity found in our study might be associated with a
lesser availability rather than an inhibition of the
released enzyme into plasma. Indeed, some studies
indicate that cytokines down-regulate mRNA of lipo-
protein lipase.29 Measurement of lipoprotein lipase mass
in addition to lipoprotein lipase activity may con®rm
this view. The inhibition of lipoprotein lipase activity is
consistent with the major changes in lipoproteins
observed in our study, since lipoprotein lipase is thought
to be necessary for the clearance of VLDL, which
transfers surface constituents to HDL particles, enhanc-
ing HDL cholesterol.30 In fact, the negative correlation
between D lipoprotein lipase activity and D plasma
tryglycerides supports an interferon-b-induced impair-
ment in the lipolytic pathway. In addition, the enrich-
ment in LDL triglycerides could be ascribed to impaired
cholesterol ester transfer protein or lecithin cholesterol
acyltransferase activities.31 Reduced lecithin cholesterol
acyltransferase activity is seen in cholestatic syndromes
and/or in hepatic failure.32 Because no patient in our
study had evidence of worsening liver function or
cholestasis, this mechanism is unlikely. Cholesterol ester
transfer protein de®ciency in humans may also result in
triglyceride-rich LDL.33 A decrease in cholesterol ester
transfer protein activity and mass was recently demon-
strated in patients with chronic hepatitis C during
treatment with interferon-a.5 Nevertheless, interferon-
b, by inhibiting the activity of lipoprotein lipase, could
also have an effect on cholesterol ester transfer protein
activity, since adequate activity of lipoprotein lipase
enhances the ability of cholesterol ester transfer protein
to bind triglyceride-rich substrates such as VLDL.34 On
the other hand, an interferon-b-induced increase in
lipogenesis and VLDL secretion in the liver is unlikely in
our patients, because interferon-b does not stimulate
hepatic fatty acid synthesis as do other cytokines,
including interferon-a, TNF-a and interleukin-1.35
We found no differences in lipoprotein pro®le between
patients strati®ed into responders and non-responders to
interferon-b, according to accepted criteria of response to
treatment, and this has also been observed with inter-
feron-a.6 However, liver enzyme behaviour correlated
with that of lipoprotein lipase, suggesting that the effects
of interferon-b on liver in¯ammation paralleled, to some
degree, the effects on lipoprotein metabolism. In addition,
although in our study hepatic lipase activity was not
modi®ed after interferon-b therapyÐin contrast to the
effect of interferon-aÐthe signi®cant positive correlation
between D HL activity and the improvement in histolog-
ical lesions in the subset of patients who had a second
biopsy also suggests this possibility.5, 10 In fact, whereas
the short-term effects of high daily doses of interferon-awere found to be associated with an inhibition of hepatic
lipase activity, the stable hepatic lipase activity after long-
term therapy with interferon-b observed in our study
might re¯ect less in¯ammatory activity in hepatocytes.5
No patient in our study had marked increases of serum
triglycerides. This is probably due to the fact that we
included only patients with normal triglycerides at
baseline, since severe hypertriglyceridemia after inter-
feron-a therapy has been reported in relationship to
high pre-treatment triglyceride levels and recommen-
dations for monitoring triglyceride levels have been
given for this subset of patients.6±10 We believe that the
same policy is reasonable for hypertriglyceridemic
patients who are to receive treatment with interferon-b.
ACKNOWLEDGEMENTS
We thank to Javier Rubio for reviewing the liver biopsy
specimens and Karen Shashok for improving the use of
English in the manuscript.
REFERENCES
1 Baron S, Tyring SK, Fleischmann WR, et al. The interferons.
Mechanism of action and clinical applications. J Am Med
Assoc 1991; 266: 1375±83.
2 Gutterman JU. Cytokine therapeutics: lessons from interferon
alpha. Proc Natl Acad Sci USA 1994; 91: 1198±205.
3 Hoofnagle JH, Di Bisceglie AM. The treatment of chronic viral
hepatitis. N Engl J Med 1997; 336: 347±56.
4 Lindsay KL. Therapy of hepatitis C. Overview. Hepatol 1997;
26 (Suppl. 1): 71S±77S.
5 Shinohara E, Yamashita S, Kihara S, et al. Interferon alpha
induces disorder of lipid metabolism by lowering postheparin
lipases and cholesteryl ester transfer protein activities in pa-
tients with chronic hepatitis C. Hepatol 1997; 25: 1502±6.
6 Fernandez-Miranda C, Castellano G, Guijarro C, et al. Lipo-
protein changes in patients with chronic hepatitis C treated
with interferon-a. Am J Gastroenterol 1998; 93: 1901±4.
934 R. J. ANDRADE et al.
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 929±935

7 PenÄ arrubia MJ, Steegmann JL, Lavilla E, et al. Hypertrigly-
ceridemia may be severe in CML patients treated with inter-
feron-a. Am J Hematol 1995; 49: 240±1.
8 SunderkoÈtter C, Luger T, Kolde G. Severe hypertriglycerida-
emia and interferon-a. Lancet 1993; 342: 1111±2.
9 Graessle D, Bonacini M, Chen S. Alpha-interferon and re-
versible hypertriglyceridemia. Ann Intern Med 1993; 118:
316±7.
10 Yamagishi S, Abe T, Sawada T. Human recombinant inter-
feron a-2a (rIFN a-2a) therapy suppresses hepatic triglyceride
lipase, leading to severe hypertriglyceridemia in a diabetic
patient. Am J Gastroenterol 1994; 89: 2280.
11 Goodkin DE. Interferon b therapy for multiple sclerosis. Lancet
1998; 352: 1486±7.
12 So K, Kioka K, Moriyoshi Y, et al. Changes in serum lipids in
patients with chronic hepatitis C during interferon beta ther-
apy. Gastroenterology 1995; 108: A1174(Abstract).
13 Kioka K, So K, Moriyoshi Y, et al. Comparison between the
effects of interferon a and interferon b on lipid metabolism.
Gastroenterology 1995; 108: A1098(Abstract).
14 National Institutes of Health. Consensus Development Con-
ference Panel statement: management of hepatitis C. Hepatol
1997; 26: 2S±10S.
15 Knodell RG, Ishak KG, Black WC, et al. Formulation and ap-
plication of a numerical scoring system for assessing histo-
logical activity in asymptomatic chronic active hepatitis.
Hepatol 1981; 1: 431±5.
16 Havel RJ, Eder HA, Bragdon JH. The distribution and
chemical composition of ultracentrifugally separated
lipoprotein in human serum. J Clin Invest 1955; 374:
1345±53.
17 Jackson R, Mc Lean L. Human postheparin plasma lipoprotein
lipase and hepatic triglyceride lipase. Meth Enzymol 1991;
197: 339±45.
18 Belfrage P, Vaughan M. Simple liquid±liquid partition system
for isolation of labelled oleic acid from mixtures with glyce-
rides. J Lipid Res 1969; 10: 341±4.
19 Dixon RM, Bordes EC, Keim NL, et al. Decreases in serum
high-density lipoprotein cholesterol and total cholesterol re-
sulting from naturally produced recombinant DNA-derived
leukocyte-interferons. Metabolism 1984; 33: 400±4.
20 Massaro E, Borden E, Hawkins J, Wiebe D, Shrago E. Effects of
recombinant interferon-a2 treatment upon lipid concentra-
tions and lipoprotein composition. J Interferon Res 1986; 6:
655±65.
21 Bengtsson-Olivecrona G, Olivecrona T. Assay of lipoprotein
lipase and hepatic lipase. In: Converse CA, Skinner ER, eds.
Lipoprotein Analysis. A Practical Approach Oxford: Oxford
University Press, 1992: 169±85.
22 Fesce E, Airoldi A, Mondazzi L, et al. Intramuscular beta
interferon for chronic hepatitis C. is it worth trying? Ital J
Gastroenterol Hepatol 1998; 30: 185±8.
23 Habertsetzer F, Marcellin P, Boyer N, et al. Recombinant in-
terferon beta for the treatment of chronic hepatitis C. Hepatol
1995; 22: 2.
24 Rosenzweig B, Wiebe D, Borden E, Storer B, Shrago E. Plasma
lipoportein changes in humans induced by b-interferon.
Atherosclerosis 1987; 67: 261±7.
25 Feingold KR, Grunfeld C. Role of cytokines in inducing hy-
perlipidemia. Diabetes 1992; 41(Suppl.): 97±101.
26 Ehnholm C, Aho K, Huttunen JK, et al. Effect of interferon on
plasma lipoproteins and on the activity of postheparin plasma
lipases. Arteriosclerosis 1982; 2: 68±73.
27 Patton JS, Shepard HM, Wilking H, et al. Interferons and
tumor necrosis factor have similar catabolic effects on 3T3-L1
cells. Proc Natl Acad Sci USA 1986; 83: 8313±7.
28 Dinarello CA, Mier JW. Lymphokines. New Engl J Med 1987;
317: 940±5.
29 Porat O. The effect of tumor necrosis factor alpha on the
activity of lipoprotein lipase in adipose tissue. Lymphokine Res
1989; 8: 459±69.
30 Patsch JR, Gotto AM Jr, Olivecrona T, Eisenberg S. Formation
of high density lipoprotein2-like particles during lipolysis of
very low density lipoprotein in vitro. Proc Natl Acad Sci 1978;
75: 4519±23.
31 Schectman G, Kaul S, Mueller RA, Borden EC, Kisseban AH.
The effect of interferon on the metabolism of LDLs. Arterioscler
Thrombos 1992; 12: 1053±62.
32 Cooper AD. Hepatic lipoprotein and cholesterol metabolism.
In: Zakim D, Boyer TD, eds. Hepatology. A Textbook of Liver
Disease, 2nd edn. Philadelphia: W.B. Saunders, 1990:
96±123.
33 Bisgaier CL, Sieberker MU, Brown ML, et al. Familial cholesteryl
ester transfer protein de®ciency is associated with triglyceride-
rich low density lipoproteins containing cholesteryl esters of
probable intracellular origin. J Lipid Res13 1991; 32: 21±33.
34 Tall AR, Sammett D, Vita G, Deckelbaum RJ, Olivecrona T.
Lipoprotein lipase enhances the cholesteryl ester transfer
protein mediated transfer of cholesteryl esters from high
density lipoproteins to very low density lipoproteins. J Biol
Chem 1984; 259: 9587±94.
35 Feingold KR, Soued M, Serio MK, Moser AH, Dinarello CA,
Grunfeld C. Multiple cytokines stimulate hepatic lipid syn-
thesis in vivo. Endocrinol 1989; 125: 267±4.
INTERFERON-BETA AND POST-HEPARIN LIPASES IN CHRONIC HEPATITIS C 935
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 929±935





























