Embed Size (px)
Citation preview

Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
9
Available at http:// www.cancercellresearch.org ISSN 2158-0820
Effects of cell phone radio-frequency radiation on the sleep outcomes: A systematic review and Meta-Analysis of randomized controlled trials Han Zhou1, Rui Xu1, Kunxing Ding1, Cuiping Liu2, Feng Zhong1, * 1School of Public Health, Qingdao University, Qingdao, 266021, China
2School of Nursing, Qingdao University, Qingdao, 266021, China
Abstract: Sleep disorders have become an important public health issue affecting people's physical health. In recent years, the impact of mobile phone radio-frequency (RF) radiation on the outcome of sleep caused the attention of scholars. We systematically searched EMBASE, Web of Science, Cochrane Library and PubMed until November 2018. All articles on the relationship between radiofrequency radiation and sleep results from polysomnography were included. These articles were randomized controlled trials (RCT) in English only. The aim was to investigate the effects of radio frequency (RF) radiation from mobile phones on sleep outcomes. 17 RCTs, including 398 participants, met the criteria for a meta-analysis. The results showed that exposure to mobile phone radio frequency radiation had no effect on sleep staging indicators and sleep quality indicators. However, results of subgroup analysis according to the exposure frequency, publication years, and exposure time demonstrated that exposure to non-217Hz RF radiation could increase arousal-index per hour (standardized mean difference = 1.22, 95% confidence interval [0.68, 1.76]; p < 0.001). The articles published before 2000 showed that total sleep time (mean difference = 4.80, 95% confidence interval=[3.70, 5.90]; p < 0.001) had increased, while articles published after 2001 showed that total sleep time (mean difference = -2.56, 95% confidence interval= [-4.25, -0.87]; p = 0.003) had decreased. RF exposure before sleep could increase the time of stage 1 (mean difference = 0.91, 95% confidence interval= [0.32, 1.50]; p = 0.003). Therefore, short-term exposure to cell phone RF radiation had no impacts on people's overall sleep outcomes.
Keywords: Cell phone; RF radiation; Sleep; Meta-analysis
Received 26 December 2019, Revised 23 January 2020, Accepted 30 January 2020
*Corresponding Author: Feng Zhong, [email protected]
1. Introduction
According to the World Health Organization
(WHO), 27% of people worldwide has sleep
disorders, which has become a major public health
problem in the world. Many people suffered from
sleep disorders such as insufficient sleep and daytime
sleepiness, etc. [1, 2] Fernando AT et al. found that
37.2% subjects were suffering from sleep-phase
disorders in New Zealand[3]. Falavigna A et al.
found that 60 percent of people were reported
sleeping problems in Southern Brazil[4]. Decreased
sleep quality in adults could lead to short- and long-
term detrimental health outcomes, including an
increase in daily stress, impaired memory, emotional
abnormalities, reduced athletic ability, reduced
immunity, stunted growth, accelerated aging, and
substance abuse, etc.[5-10] Therefore, good sleep
quality be beneficial to prevent a range of disorders
and keep health.
Sleep problems can be caused by several factors
including disease status, dietary factors, mental
health, and lifestyle. The number of people using
mobile phones is growing year by year [11]. More
and more scholars believed that radio-frequency (RF)
radiation from cell phones can be an important factor
affecting the quality of sleep. The potential health
effects of mobile phone (MP) electromagnetic field
(EMF) exposure has been identified by WHO as a
high priority research area, and the health effects of
prolonged exposure to RF radiation needed to be
studied further[12]. Whether the use of cell phones
could result in prolonged sleep latency and
subsequent side effects remains unclear[13]. Several
studies has found that RF radiation of a cell phone
can cause sleep disorders by changing rapid-eye
movement (REM) sleep[14, 15]. Some believed that
exposure to RF radiation in cell phones could shorten
slow wave sleep (SWS) time[16, 17] or extend the
REM sleep latency[18], while others argued that RF
radiation has no effects on sleep outcomes[19-23].
To sum up, the effects of cell phone RF radiation
on sleep outcomes remains controversial and there be
no evidence of the overall effects' evaluation.
Therefore, we performed meta-analysis and
systematic review to explore the impacts of mobile
phone RF radiation on sleep outcomes.
2. Method
2.1. Types of participants
All subjects were non-smokers and reported to be
healthy and had no sleep problems. Elimination of
personal or family psychopathology, chronic illness,
sleep disorders, and current history of the use of
psychotropic or other medications. During the study

Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
10
period, alcohol was banned and the subject was
informed in detail of the study's intentions and
obtained written consent.
2.2. Types of studies and interventions
Randomized controlled double-blind crossover
design experiment. The control group was sham
group, and the experimental group was radio
frequency radiation (cell phone or analog cell phone
signal) exposure group.
2.3. Search strategy
This search strategy was developed in order to
identify studies which explored the association
between exposure to cell phone RF and sleep
outcomes. This review was conducted using
PRISMA-P guidelines[24]. We conducted MeSH and
keywords search using terms such as RF, sleep, and
cell phone, etc. Search queries were performed on
the electronic databases PubMed, EMBASE, Web of
Science and the Cochrane Library. The entire search
process was completed on November 17th, 2018.
PubMed was searched using the following
terminology: ((‘cell phone’ OR ‘mobile phone’ OR
‘cellular phone’ OR ‘smart phone’ OR ‘electronic
media’ OR ‘cell phone’ [MeSH Terms] OR ‘mobile
equipment’ OR ‘mobile communication’ OR
‘handset’ OR ‘mobile telephone’) AND (‘RF’ OR
‘radio frequency’ OR ‘radiation’ OR ‘RF energy’)
AND (‘sleep’ OR ‘sleep’ [MeSH Terms]) AND
(‘randomized controlled trial’ [Publication Type] OR
‘random’ OR ‘controlled’ OR ‘trial’)). The other
databases were searched using similar terminologies.
Specific search strategies were detailed in
supplement Figure 1.
Figure 1. PRISMA Flowchart of the Searched, Identified, and Included Studies.
2.4. Inclusion and exclusion criteria Included studies met the following criteria: (a)
original double-blinded randomized controlled trials;
Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
11
(b) RF radiation signals generated strictly from cell
phones; (c) outcomes including sleep staging and
sleep quality experimented by polysomnography
analyzer; (d) complete data records and (e) the study
was published in English as a full-text article in
journal. Excluded studies if (a) Animal experiments,
(b) Non-English papers, (c) Reviews, letters or
comments and (d) Incomplete data. The development
of the standard was independently evaluated by two
researchers (Han Zhou and Feng Zhong).
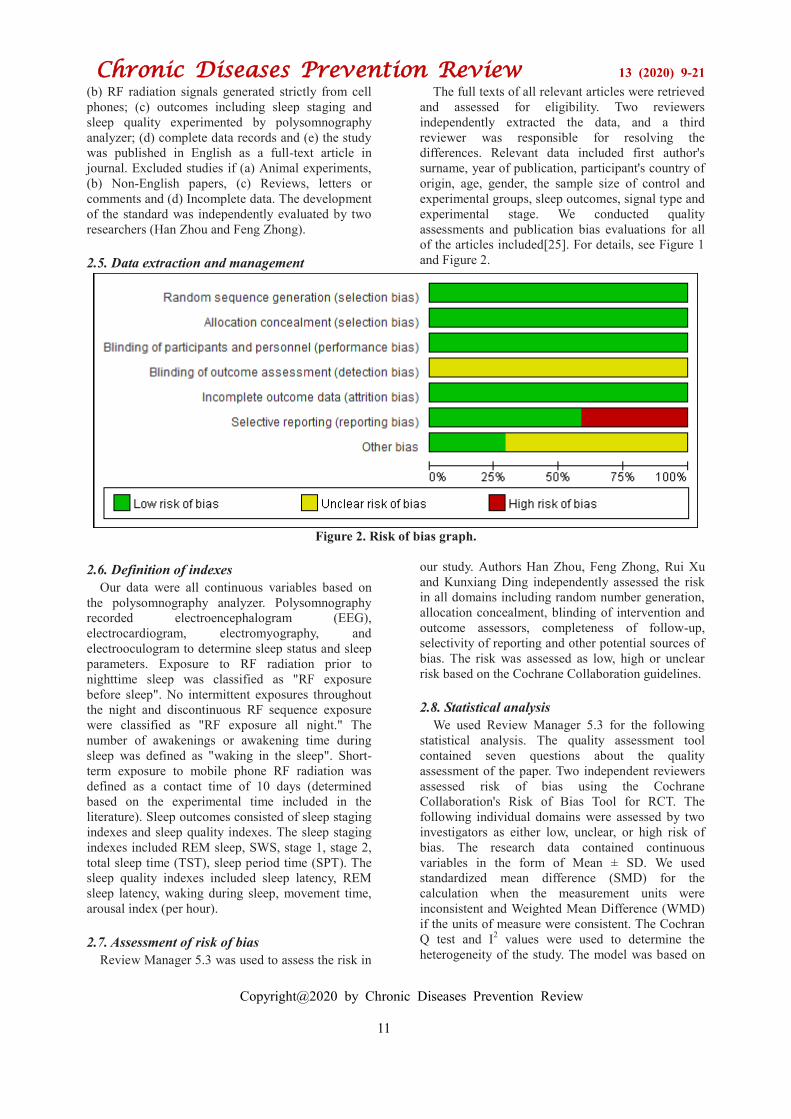
2.5. Data extraction and management
The full texts of all relevant articles were retrieved
and assessed for eligibility. Two reviewers
independently extracted the data, and a third
reviewer was responsible for resolving the
differences. Relevant data included first author's
surname, year of publication, participant's country of
origin, age, gender, the sample size of control and
experimental groups, sleep outcomes, signal type and
experimental stage. We conducted quality
assessments and publication bias evaluations for all
of the articles included[25]. For details, see Figure 1
and Figure 2.
Figure 2. Risk of bias graph.
2.6. Definition of indexes
Our data were all continuous variables based on
the polysomnography analyzer. Polysomnography
recorded electroencephalogram (EEG),
electrocardiogram, electromyography, and
electrooculogram to determine sleep status and sleep
parameters. Exposure to RF radiation prior to
nighttime sleep was classified as "RF exposure
before sleep". No intermittent exposures throughout
the night and discontinuous RF sequence exposure
were classified as "RF exposure all night." The
number of awakenings or awakening time during
sleep was defined as "waking in the sleep". Short-
term exposure to mobile phone RF radiation was
defined as a contact time of 10 days (determined
based on the experimental time included in the
literature). Sleep outcomes consisted of sleep staging
indexes and sleep quality indexes. The sleep staging
indexes included REM sleep, SWS, stage 1, stage 2,
total sleep time (TST), sleep period time (SPT). The
sleep quality indexes included sleep latency, REM
sleep latency, waking during sleep, movement time,
arousal index (per hour).
2.7. Assessment of risk of bias
Review Manager 5.3 was used to assess the risk in
our study. Authors Han Zhou, Feng Zhong, Rui Xu
and Kunxiang Ding independently assessed the risk
in all domains including random number generation,
allocation concealment, blinding of intervention and
outcome assessors, completeness of follow-up,
selectivity of reporting and other potential sources of
bias. The risk was assessed as low, high or unclear
risk based on the Cochrane Collaboration guidelines.
2.8. Statistical analysis
We used Review Manager 5.3 for the following
statistical analysis. The quality assessment tool
contained seven questions about the quality
assessment of the paper. Two independent reviewers
assessed risk of bias using the Cochrane
Collaboration's Risk of Bias Tool for RCT. The
following individual domains were assessed by two
investigators as either low, unclear, or high risk of
bias. The research data contained continuous
variables in the form of Mean ± SD. We used
standardized mean difference (SMD) for the
calculation when the measurement units were
inconsistent and Weighted Mean Difference (WMD)
if the units of measure were consistent. The Cochran
Q test and I2 values were used to determine the
heterogeneity of the study. The model was based on
Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
12
the size of I2. Considering the existence of
heterogeneity, when I2 > 50%, a random effects
model was used, and a fixed effects model was used
when I2 ≤ 50%. We performed a subgroup analysis
of the study of I2 > 25%[26]. After comparisons with
significant heterogeneity, we made a sensitivity
analysis in which one study was removed to identify
the possible source of heterogeneity; the study that
resulted in the greatest decrease in heterogeneity was
excluded. Subgroup analyses were also performed to
check for possible sources of heterogeneity
attributable to the study characteristics. Review
manager 5.3 was used for sensitivity, heterogeneity
analyses, quality assessment and publication bias.
3. Results
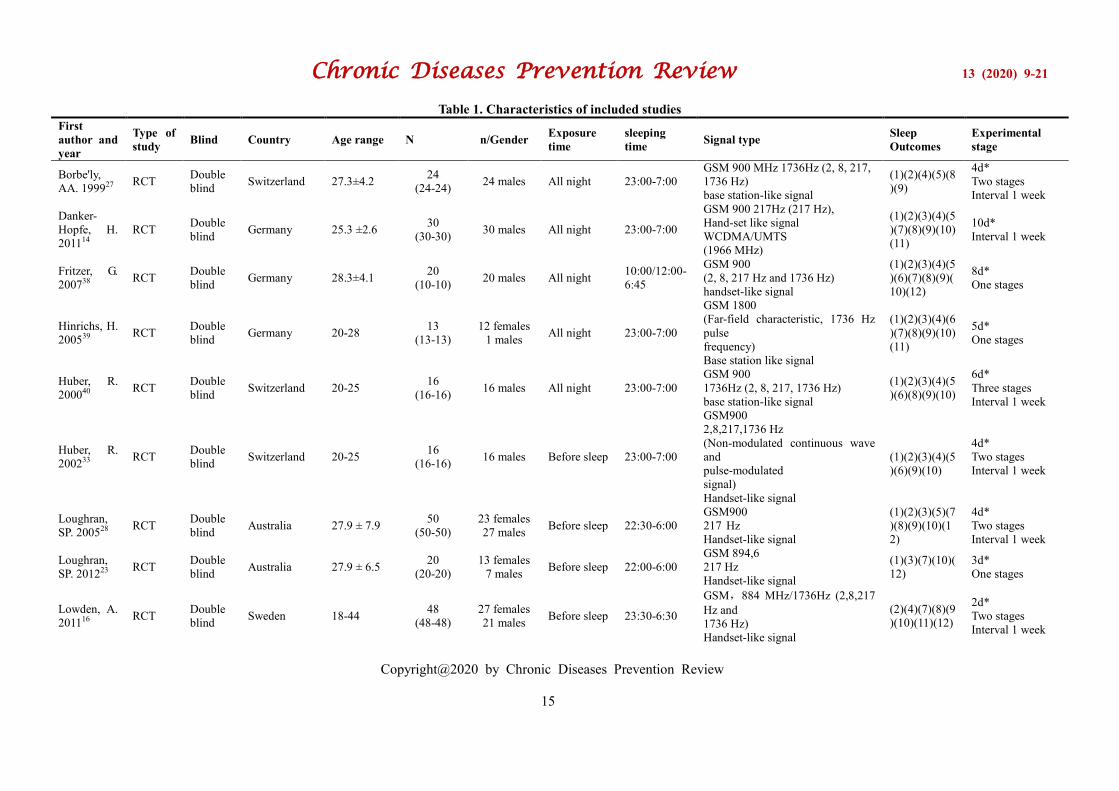
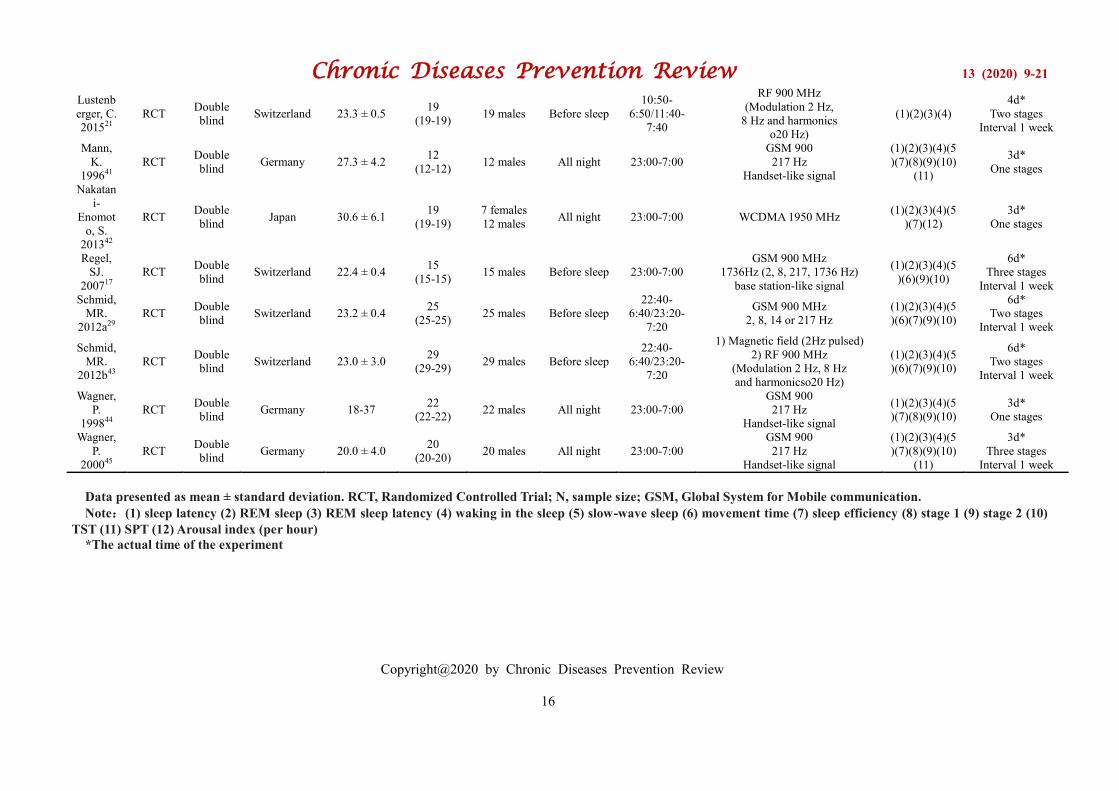
3.1. Characteristics of Studies
A PRISMA flow diagram of the search results was
seen in Figure 1. 17 experiments were included in
this meta-analysis. Overall, studies in the meta-
analysis included Germans (n = 6); Swiss (n = 7);
Swedes (n = 1); Japanese (n = 1); and Australians (n
= 2). The subjects in nine trials were exposed to RF
radiation before going to sleep, and the others were
exposed all night. A comparison of the included
study characteristics was detailed in Table 1. All
records of sleep outcomes were based on
polysomnography.
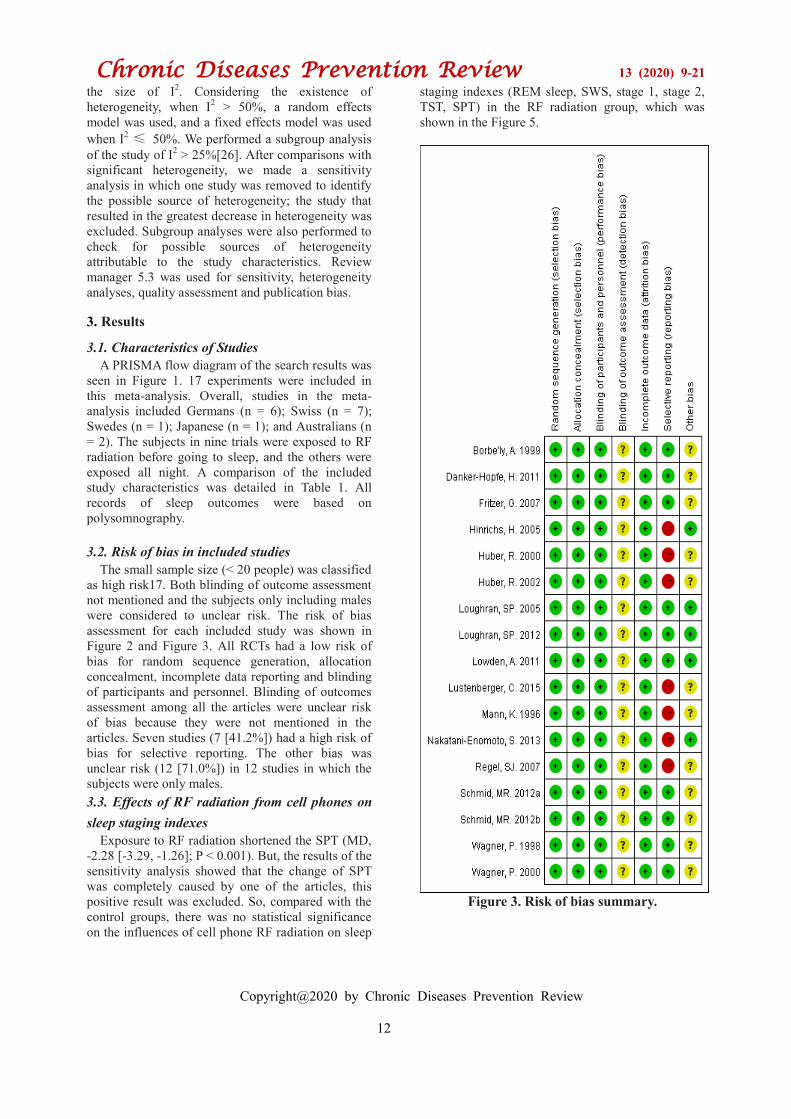
3.2. Risk of bias in included studies
The small sample size (< 20 people) was classified
as high risk17. Both blinding of outcome assessment
not mentioned and the subjects only including males
were considered to unclear risk. The risk of bias
assessment for each included study was shown in
Figure 2 and Figure 3. All RCTs had a low risk of
bias for random sequence generation, allocation
concealment, incomplete data reporting and blinding
of participants and personnel. Blinding of outcomes
assessment among all the articles were unclear risk
of bias because they were not mentioned in the
articles. Seven studies (7 [41.2%]) had a high risk of
bias for selective reporting. The other bias was
unclear risk (12 [71.0%]) in 12 studies in which the
subjects were only males.
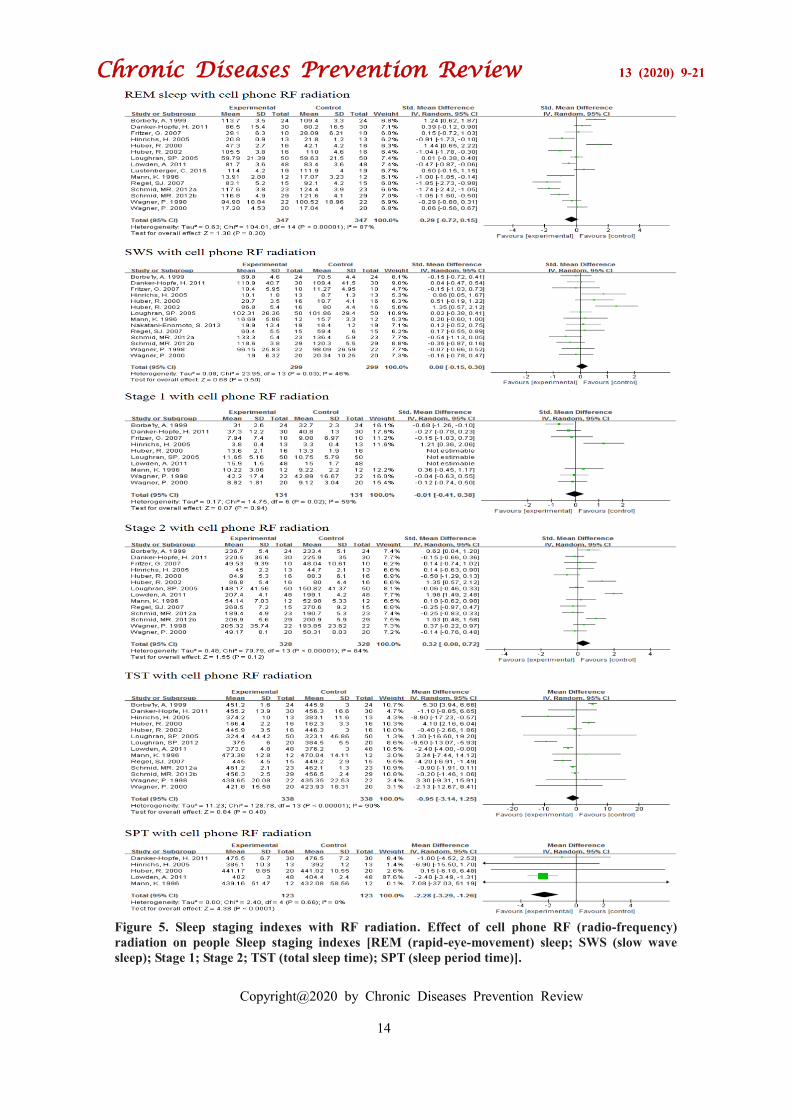
3.3. Effects of RF radiation from cell phones on
sleep staging indexes
Exposure to RF radiation shortened the SPT (MD,
-2.28 [-3.29, -1.26]; P < 0.001). But, the results of the
sensitivity analysis showed that the change of SPT
was completely caused by one of the articles, this
positive result was excluded. So, compared with the
control groups, there was no statistical significance
on the influences of cell phone RF radiation on sleep
staging indexes (REM sleep, SWS, stage 1, stage 2,
TST, SPT) in the RF radiation group, which was
shown in the Figure 5.
Figure 3. Risk of bias summary.
Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
13
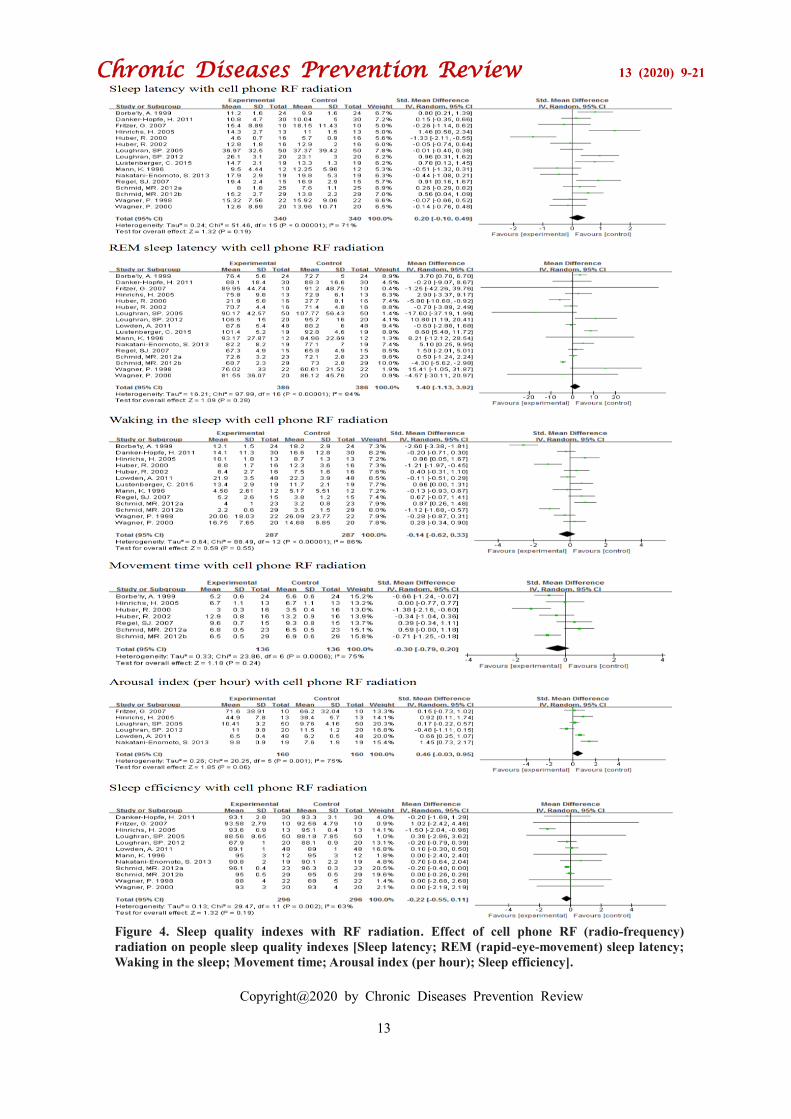
Figure 4. Sleep quality indexes with RF radiation. Effect of cell phone RF (radio-frequency)
radiation on people sleep quality indexes [Sleep latency; REM (rapid-eye-movement) sleep latency;
Waking in the sleep; Movement time; Arousal index (per hour); Sleep efficiency].
Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
14
Figure 5. Sleep staging indexes with RF radiation. Effect of cell phone RF (radio-frequency)
radiation on people Sleep staging indexes [REM (rapid-eye-movement) sleep; SWS (slow wave
sleep); Stage 1; Stage 2; TST (total sleep time); SPT (sleep period time)].
Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
15
Table 1. Characteristics of included studies
First
author and
year
Type of
study Blind Country Age range N n/Gender
Exposure
time
sleeping
time Signal type
Sleep
Outcomes
Experimental
stage
Borbe'ly,
AA. 199927 RCT
Double
blind Switzerland 27.3±4.2
24
(24-24) 24 males All night 23:00-7:00
GSM 900 MHz 1736Hz (2, 8, 217,
1736 Hz)
base station-like signal
(1)(2)(4)(5)(8
)(9)
4d*
Two stages
Interval 1 week
Danker-
Hopfe, H.
201114
RCT Double
blind Germany 25.3 ±2.6
30
(30-30) 30 males All night 23:00-7:00
GSM 900 217Hz (217 Hz),
Hand-set like signal
WCDMA/UMTS
(1966 MHz)
(1)(2)(3)(4)(5
)(7)(8)(9)(10)
(11)
10d*
Interval 1 week
Fritzer, G.
200738 RCT
Double
blind Germany 28.3±4.1
20
(10-10) 20 males All night
10:00/12:00-
6:45
GSM 900
(2, 8, 217 Hz and 1736 Hz)
handset-like signal
(1)(2)(3)(4)(5
)(6)(7)(8)(9)(
10)(12)
8d*
One stages
Hinrichs, H.
200539 RCT
Double
blind Germany 20-28
13
(13-13)
12 females
1 males All night 23:00-7:00
GSM 1800
(Far-field characteristic, 1736 Hz
pulse
frequency)
Base station like signal
(1)(2)(3)(4)(6
)(7)(8)(9)(10)
(11)
5d*
One stages
Huber, R.
200040 RCT
Double
blind Switzerland 20-25
16
(16-16) 16 males All night 23:00-7:00
GSM 900
1736Hz (2, 8, 217, 1736 Hz)
base station-like signal
(1)(2)(3)(4)(5
)(6)(8)(9)(10)
6d*
Three stages
Interval 1 week
Huber, R.
200233 RCT
Double
blind Switzerland 20-25
16
(16-16) 16 males Before sleep 23:00-7:00
GSM900
2,8,217,1736 Hz
(Non-modulated continuous wave
and
pulse-modulated
signal)
Handset-like signal
(1)(2)(3)(4)(5
)(6)(9)(10)
4d*
Two stages
Interval 1 week
Loughran,
SP. 200528 RCT
Double
blind Australia 27.9 ± 7.9
50
(50-50)
23 females
27 males Before sleep 22:30-6:00
GSM900
217 Hz
Handset-like signal
(1)(2)(3)(5)(7
)(8)(9)(10)(1
2)
4d*
Two stages
Interval 1 week
Loughran,
SP. 201223 RCT
Double
blind Australia 27.9 ± 6.5
20
(20-20)
13 females
7 males Before sleep 22:00-6:00
GSM 894,6
217 Hz
Handset-like signal
(1)(3)(7)(10)(
12)
3d*
One stages
Lowden, A.
201116 RCT
Double
blind Sweden 18-44
48
(48-48)
27 females
21 males Before sleep 23:30-6:30
GSM,884 MHz/1736Hz (2,8,217
Hz and
1736 Hz)
Handset-like signal
(2)(4)(7)(8)(9
)(10)(11)(12)
2d*
Two stages
Interval 1 week
Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
16
Data presented as mean ± standard deviation. RCT, Randomized Controlled Trial; N, sample size; GSM, Global System for Mobile communication.
Note:(1) sleep latency (2) REM sleep (3) REM sleep latency (4) waking in the sleep (5) slow-wave sleep (6) movement time (7) sleep efficiency (8) stage 1 (9) stage 2 (10)
TST (11) SPT (12) Arousal index (per hour)
*The actual time of the experiment
Lustenb
erger, C.
201521
RCT Double
blind Switzerland 23.3 ± 0.5
19
(19-19) 19 males Before sleep
10:50-
6:50/11:40-
7:40
RF 900 MHz
(Modulation 2 Hz,
8 Hz and harmonics
o20 Hz)
(1)(2)(3)(4)
4d*
Two stages
Interval 1 week
Mann,
K.
199641
RCT Double
blind Germany 27.3 ± 4.2
12
(12-12) 12 males All night 23:00-7:00
GSM 900
217 Hz
Handset-like signal
(1)(2)(3)(4)(5
)(7)(8)(9)(10)
(11)
3d*
One stages
Nakatan
i-
Enomot
o, S.
201342
RCT Double
blind Japan 30.6 ± 6.1
19
(19-19)
7 females
12 males All night 23:00-7:00 WCDMA 1950 MHz
(1)(2)(3)(4)(5
)(7)(12)
3d*
One stages
Regel,
SJ.
200717
RCT Double
blind Switzerland 22.4 ± 0.4
15
(15-15) 15 males Before sleep 23:00-7:00
GSM 900 MHz
1736Hz (2, 8, 217, 1736 Hz)
base station-like signal
(1)(2)(3)(4)(5
)(6)(9)(10)
6d*
Three stages
Interval 1 week
Schmid,
MR.
2012a29
RCT Double
blind Switzerland 23.2 ± 0.4
25
(25-25) 25 males Before sleep
22:40-
6:40/23:20-
7:20
GSM 900 MHz
2, 8, 14 or 217 Hz
(1)(2)(3)(4)(5
)(6)(7)(9)(10)
6d*
Two stages
Interval 1 week
Schmid,
MR.
2012b43
RCT Double
blind Switzerland 23.0 ± 3.0
29
(29-29) 29 males Before sleep
22:40-
6:40/23:20-
7:20
1) Magnetic field (2Hz pulsed)
2) RF 900 MHz
(Modulation 2 Hz, 8 Hz
and harmonicso20 Hz)
(1)(2)(3)(4)(5
)(6)(7)(9)(10)
6d*
Two stages
Interval 1 week
Wagner,
P.
199844
RCT Double
blind Germany 18-37
22
(22-22) 22 males All night 23:00-7:00
GSM 900
217 Hz
Handset-like signal
(1)(2)(3)(4)(5
)(7)(8)(9)(10)
3d*
One stages
Wagner,
P.
200045
RCT Double
blind Germany 20.0 ± 4.0
20
(20-20) 20 males All night 23:00-7:00
GSM 900
217 Hz
Handset-like signal
(1)(2)(3)(4)(5
)(7)(8)(9)(10)
(11)
3d*
Three stages
Interval 1 week
Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
17
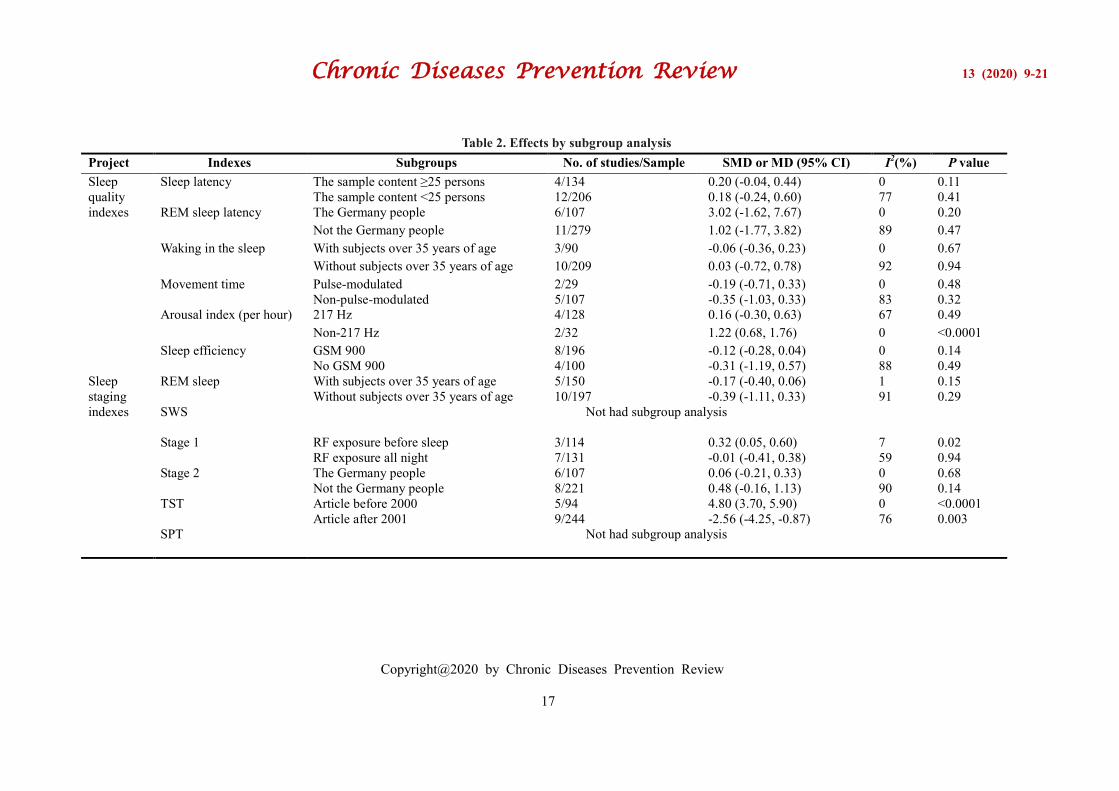
Table 2. Effects by subgroup analysis
Project Indexes Subgroups No. of studies/Sample SMD or MD (95% CI) I2(%) P value
Sleep
quality
indexes
Sleep latency The sample content ≥25 persons 4/134 0.20 (-0.04, 0.44) 0 0.11
The sample content <25 persons 12/206 0.18 (-0.24, 0.60) 77 0.41
REM sleep latency The Germany people 6/107 3.02 (-1.62, 7.67) 0 0.20
Not the Germany people 11/279 1.02 (-1.77, 3.82) 89 0.47
Waking in the sleep With subjects over 35 years of age 3/90 -0.06 (-0.36, 0.23) 0 0.67
Without subjects over 35 years of age 10/209 0.03 (-0.72, 0.78) 92 0.94
Movement time Pulse-modulated 2/29 -0.19 (-0.71, 0.33) 0 0.48
Non-pulse-modulated 5/107 -0.35 (-1.03, 0.33) 83 0.32
Arousal index (per hour) 217 Hz 4/128 0.16 (-0.30, 0.63) 67 0.49
Non-217 Hz 2/32 1.22 (0.68, 1.76) 0 <0.0001
Sleep efficiency GSM 900 8/196 -0.12 (-0.28, 0.04) 0 0.14
No GSM 900 4/100 -0.31 (-1.19, 0.57) 88 0.49
Sleep
staging
indexes
REM sleep With subjects over 35 years of age 5/150 -0.17 (-0.40, 0.06) 1 0.15
Without subjects over 35 years of age 10/197 -0.39 (-1.11, 0.33) 91 0.29
SWS
Not had subgroup analysis
Stage 1 RF exposure before sleep 3/114 0.32 (0.05, 0.60) 7 0.02
RF exposure all night 7/131 -0.01 (-0.41, 0.38) 59 0.94
Stage 2 The Germany people 6/107 0.06 (-0.21, 0.33) 0 0.68
Not the Germany people 8/221 0.48 (-0.16, 1.13) 90 0.14
TST Article before 2000 5/94 4.80 (3.70, 5.90) 0 <0.0001
Article after 2001 9/244 -2.56 (-4.25, -0.87) 76 0.003
SPT
Not had subgroup analysis

Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
18
Subgroup analysis results showed that the
effectiveness of exposure RF radiation for sleep
outcomes was significant for both the articles
published before 2000 and the articles published
after 2001. Stage 1 time (RF radiation before sleep)
was extended in the RF radiation group (MD, 0.91
[0.32, 1.50]; P = 0.003). No statistically significant
differences were found in RF radiation in all night
subgroups. Additionally, no statistically significant
differences in REM sleep (with subjects over 35
years of age or without subjects over 35 years of age)
and stage 2 (RF radiation exposure is before sleep or
all night) were found. Details are shown in Table 2.
3.4. Effects of RF radiation on sleep quality
indexes
The exposure to the cell phone RF radiation
revealed no significant effects on sleep quality
indexes including sleep latency, REM sleep latency,
waking during sleep, movement time, arousal index
(per hour), and sleep efficiency. The details could be
seen in Figure 4. Subgroup analysis indicated that the
non-217Hz RF could increase arousal index (per
hour) (SMD, 1.22 [0.68, 1.76]; P < 0.001). The
217Hz RF had no significant impact on arousal index
(per hour). In the other subgroups, no significant
difference was found between experiments groups
and control groups.
4. Discussion
Our research provided evidence that short-term
exposure to cell phone RF radiation had no impacts
on people's sleep outcomes (including sleep staging
indexes and sleep quality indexes). In previous
studies, many results had shown that cell phone RF
exposure had effects on sleep outcomes, but whether
the effects were harmful to the body remained
unclear. For example, some researchers had found
that prolonged RF radiation could change SWS time
and stage 2[16, 17], or minimized frequency of
waking during sleep[27]. In addition, exposure to RF
radiation could reduce the REM sleep latency[28, 29].
Others believed that exposure to RF radiation could
prolong REM sleep latency[18]. However, there
were also many other studies which showed that RF
radiation had no effects on sleep outcomes[19-23].
An one-year cohort study by Evelyn Mohler showed
that RF-EMF exposure in the environment (including
cell phones) had no effects on sleep quality[30].
Therefore, it was important to analyze these studies,
and our findings provide a comprehensive analysis of
the results of all RCT trials.
In general, global system for mobile
communications (GSM) cell phone generates 217Hz
electromagnetic field. In other cases, GSM cell
phone also generates magnetic field of other
frequencies such as low-frequency radios or high-
frequency radios. Pall's research showed that low
frequency RF could cause a wide range of changes in
the nervous system, resulting in a variety of mental
symptoms or nerve dysfunction including sleep
disorders[31, 32]. Our analysis had shown that the
non-217Hz RF could increase the arousal index (per
hour). Pall's research was supported by the non-
217Hz subgroup containing low-frequency radios
such as 2, 4, and 8Hz in our results. In addition,
Huber[33, 34] found that pulsed RF EMF could alter
the awake and sleep state of EEG. As mentioned
above, the equipments and frequencies used in
different experiments were different. The operating
frequencies of cell phones such as 217Hz RF
radiation could affect the level of electromagnetic
absorption of the human brain[35]. However, the
overall results mask this effect because of all
radiation at frequencies incorporated in our study.
Therefore, we believe that non-217Hz frequency
radio frequencies may reduce sleep quality.
Our data suggest that the cell phone RF radiation
could increase TST in the articles published before
2000 (MD: 4.80). And cell phone RF radiation could
decrease TST in the articles published after 2001
(MD: -2.56). The reason may be the difference in
results caused by changes in mobile communication
networks. Around 2000, cell phone communication
had changed from a 2G network to a 3G network,
and its frequency and mode of occurrence had also
changed. Today, 4G and 5G networks were gradually
evolving, however relevant research data was lack.
Moreover, it was a common phenomenon for people
to use cell phones before going to bed, which will
inevitably lose sleep time[36]. Therefore, we could
only think that this result may be related to the
change of mobile communication technology and
cell phone user's habit. Some research had shown
that insufficient sleep was associated with decreased
alertness and impairment of cognitive ability[37]. In
addition, sufficient sleep could improve sustained
attention and reduce sleep pressure. So, the
shortening of the TST time caused by the RF
radiation from cell phones should also attract
people's attention.
Finally, stage 1 represents the stage before the
sleep begins, which means that using the phone
before going to bed could cause a delay in sleep. We
believed that RF radiation may affect stage1 by
stimulating the brain nervous system. Indeed, in the
current study, the exposure time and the process of
"exposure to cell phone RF radiation" in different
experiments were quite different. One possible
explanation was that the effects was not constant and
ever changing throughout the night, so the level of
significance may not always be reached, especially
considering individual differences in response. So,
the result of "RF exposure all night" was not

Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
19
statistically significant, but "RF exposure before
sleep" shows its effects because time and process
were relatively constant. In addition, the combined
effects of contact time and the contact method
(process) of cell phone RF radiation to people sleep
require further research.
The effects of radiofrequency radiation from cell
phones on sleep outcomes were influenced by many
other factors. For example, we suspect that the
prolonged use of a cell phone may lead to changes in
sleep habits. During a short period of time, subjects
may not be able to effectively adjust their sleep
habits when exposed to cellular RF radiation, which
resulted in differences in outcomes. However, there
was currently no relevant placebo-controlled study,
so further research was needed. Equipment and RF
frequencies used in the experiment were not exactly
the same. Some researchers used GSM 900 or GSM
1800, some used 217Hz RF or not. Some studies
used pulse-modulated RF, others used hand base
signals. Researches showed that when the distance
between the brain and the RF radiation point was
40cm[17], the REM sleep was extended, and when
the distance was 3 meters[22], the influence
disappears. In the studies that we included, the
distance between the radiation points and the brain
was not identical. So, this distance may also be a
potential factor affecting sleep outcomes.
The results of this study were meaningful. Above
all, all experiments included were double-blind,
randomized controlled studies. Although meta-
analysis found significant heterogeneity between
studies, further sensitivity analyses and publication
bias tests favored the coherence effects among
different populations. Next, the experiments
conducted in different countries and regions followed
the same design method. Thirdly, polysomnography
analyzer was used to objectively record sleep
outcome indicators. Therefore, we had reason to
believe that at least the overall role of the radio band
(short-time) included in this study does not had much
impacts on human sleep. These results were
important in guiding the current assessment of
evidences and the formulation of public health
strategies.
We analyzed the overall results of previous studies
through systematic quality assessments for the first
time and concluded from the subgroup that different
RF exposure times and frequencies may had impacts
on total sleep time, number of awakenings during
sleep, and time to fall asleep. However, our analysis
still had some limitations. First, the results of the
data assessment were a synthesis of the results
contained only in our study. Second, the research
project did not involve the use of the screen blue
light of cell phones on the quality of sleep, because
they were not within the evaluation range. Third,
although our studies were all RCT studies, the
confusion and bias could not be completely avoided.
Finally, all studies were from developed countries,
we do not know the specific situations in developing
countries. Even so, the study could serve as a guide
for the use of cell phones to encourage young people
to appropriately reduce the use of cell phones, and
ensure adequate sleep. At present, experimental data
on the effects of long-term radiofrequency radiation
on sleep are lacking. No one has done research on
the susceptibility of sleep disturbance caused by RF
radiation, which may be the future research
directions.
5. Conclusions
In this meta-analysis, there was no statistically
significant association between RF exposure and
sleep outcomes. Therefore, at least in our study, we
believe that short-term exposure to mobile phone RF
radiation had no effects on sleep outcomes. However,
considering the impact of mobile phone usage time
and non-RF radiation factors on sleep, we
recommend to rationalize the use of mobile phones
and develop good sleep hygiene habits.
Author Contributions The abstracts of citations obtained from the
primary broad search were read independently by
reviewers Han Zhou, Feng Zhong, Rui Xu, Cuiping
Liu and Kunxiang Ding to identify potentially
eligible studies. Full-text articles of these studies
were obtained and assessed for eligibility by
reviewers Han Zhou, Feng Zhong, and Rui Xu
independently, using the predefined eligibility
criteria. Differences in opinion were resolved by
panel discussion to reach a consistent result. To avoid
duplication of data, care was taken to ensure that
multiple publications of the same study were
excluded.
Funding No Funding
Conflicts of Interest None declared
References [1] Zhou J, Zhang J, Lam SP, et al. Excessive
Daytime Sleepiness Predicts
Neurodegeneration in Idiopathic REM Sleep
Behavior Disorder[J]. SLEEP. 2017, 40(1),
268-268.
[2] Carter B, Rees P, Hale L, et al. Association
Between Portable Screen-Based Media
Device Access or Use and Sleep Outcomes: A
Systematic Review and Meta-analysis. Jama
Pediatrics. 2016; 170(12):1202-1208.
[3] Fernando AT SC, Blank CJ, et al. Sleep
Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
20
disorders among high school students in New
Zealand[J]. J Prim Health Care. 2013,
5(4):276-282.
[4] Falavigna A, Bezerra MLDS , Teles AR , et al.
Sleep disorders among undergraduate students
in Southern Brazil[J]. Sleep & breathing =
Schlaf & Atmung, 2011, 15(3):519-524.
[5] Winzeler K, Voellmin A, Schafer V, et al. Daily
stress, presleep arousal, and sleep in healthy
young women: a daily life computerized sleep
diary and actigraphy study[J]. Sleep Med.
2014, 15(3):359-366.
[6] Coughlin JW, Smith MT. Sleep, obesity, and
weight loss in adults: is there a rationale for
providing sleep interventions in the treatment
of obesity?[J]. International review of
psychiatry (Abingdon, England). 2014,
26(2):177-188.
[7] Campbell P, Tang N, McBeth J, et al. The role
of sleep problems in the development of
depression in those with persistent pain: a
prospective cohort study[J]. Sleep. 2013,
36(11):1693-1698.
[8] Ford DE, Kamerow DB. Epidemiologic study
of sleep disturbances and psychiatric disorders.
An opportunity for prevention?[J]. JAMA.
1989, 262(11):1479-1484.
[9] Johnson EO, Roth T, Breslau N. The association
of insomnia with anxiety disorders and
depression: exploration of the direction of
risk[J]. J Psychiatr Res. 2006, 40(8):700-708.
[10] Morphy H, Dunn KM, Lewis M, et al.
Epidemiology of insomnia: a longitudinal
study in a UK population[J]. Sleep. 2007,
30(3):274-280.
[11] Poon J, Gjorgiievski M, Mogal I, et al.
Quality and Accuracy of Information
Available on Websites for Distracted Driving:
Qualitative Analysis[J]. Interact J Med Res.
2019, 8(4):e16154.
[12] Van Deventer E, van Rongen E, Saunders R.
WHO research agenda for radiofrequency
fields[J]. Bioelectromagnetics. 2011,
32(5):417-421.
[13] Hysing M, Pallesen S, Stormark KM, et al.
Sleep and use of electronic devices in
adolescence: results from a large population-
based study[J]. BMJ Open. 2015,
5(1):e006748.
[14] Danker-Hopfe H, Dorn H, Bolz T, et al.
Effects of mobile phone exposure (GSM 900
and WCDMA/UMTS) on polysomnography
based sleep quality: An intra- and inter-
individual perspective[J]. Environ Res. 2016,
145:50-60.
[15] Soderqvist F, Carlberg M, Zetterberg H, et al.
Use of wireless phones and serum beta-trace
protein in randomly recruited persons aged
18-65 years: a cross-sectional study[J].
Electromagnetic biology and medicine. 2012,
31(4):416-424.
[16] Lowden A, Akerstedt T, Ingre M, et al. Sleep
after mobile phone exposure in subjects with
mobile phone-related symptoms[J].
Bioelectromagnetics. 2011, 32(1):4-14.
[17] Regel SJ, Tinguely G, Schuderer J, et al.
Pulsed radio-frequency electromagnetic fields:
dose-dependent effects on sleep, the sleep
EEG and cognitive performance[J]. J Sleep
Res. 2007, 16(3):253-258.
[18] Hung CS, Anderson C, Horne JA, et al.
Mobile phone 'talk-mode' signal delays EEG-
determined sleep onset[J]. Neurosci Lett.
2007, 421(1):82-86.
[19] Lustenberger C, Murbach M, Durr R, et al.
Stimulation of the brain with radiofrequency
electromagnetic field pulses affects sleep-
dependent performance improvement[J].
Brain Stimul. 2013, 6(5):805-811.
[20] Danker-Hopfe H, Dorn H, Bahr A, et al.
Effects of electromagnetic fields emitted by
mobile phones (GSM 900 and
WCDMA/UMTS) on the macrostructure of
sleep[J]. J Sleep Res. 2011, 20(1):73-81.
[21] Lustenberger C, Murbach M, Tushaus L, et al.
Inter-individual and intra-individual variation
of the effects of pulsed RF EMF exposure on
the human sleep EEG[J]. Bioelectromagnetics.
2015, 36(3):169-177.
[22] Nakatani-Enomoto S, Furubayashi T ,
Ushiyama A , et al. Effects of electromagnetic
fields emitted from W-CDMA-like mobile
phones on sleep in humans[J].
Bioelectromagnetics, 2013, 34(8):589-598.
[23] Loughran SP, McKenzie RJ, Jackson ML, et
al. Individual differences in the effects of
mobile phone exposure on human sleep:
rethinking the problem[J].
Bioelectromagnetics. 2012, 33(1):86-93.
[24] Shamseer L, Moher D, Clarke M, et al.
Preferred reporting items for systematic
review and meta-analysis protocols
(PRISMA-P) 2015: elaboration and
explanation[J]. BMJ. 2015, 349(1):7647-7647.
[25] Gordon H Guyatt, Andrew D Oxman, Gunn E
Vist, et al. GRADE: An emerging consensus
on rating quality of evidence and strength of
recommendations[J]. Bmj British Medical
Journal, 2008, 336(7650):924-926.
[26] Jonathan J. Shuster. Review: Cochrane
handbook for systematic reviews for
interventions, Version 5.1.0, published 3/2011.
Julian P.T. Higgins and Sally Green,
Editors[J]. Research Synthesis Methods, 2011,
2(2):126-130.
[27] Borbely AA, Huber R, Graf T, et al. Pulsed
Chronic Diseases Prevention Review 13 (2020) 9-21
Copyright@2020 by Chronic Diseases Prevention Review
21
high-frequency electromagnetic field affects
human sleep and sleep
electroencephalogram[J]. Neurosci Lett. 1999,
275(3):207-210.
[28] Loughran SP, Wood AW, Barton JM, et al.
The effect of electromagnetic fields emitted
by mobile phones on human sleep[J].
Neuroreport. 2005, 16(17):1973-1976.
[29] Schmid MR, Loughran S P , Regel S J , et al.
Sleep EEG alterations: effects of different
pulse-modulated radio frequency
electromagnetic fields[J]. Journal of Sleep
Research, 2012b, 21(1):50-58.
[30] Mohler E, Frei P, Frohlich J, et al. Exposure
to radiofrequency electromagnetic fields and
sleep quality: a prospective cohort study[J].
PloS one. 2012, 7(5):e37455.
[31] Pall ML. Scientific evidence contradicts
findings and assumptions of Canadian Safety
Panel 6: microwaves act through voltage-
gated calcium channel activation to induce
biological impacts at non-thermal levels,
supporting a paradigm shift for
microwave/lower frequency electromagnetic
field action[J]. Reviews on Environmental
Health, 2015, 30(2):99-116.
[32] Pall ML. Microwave frequency
electromagnetic fields (EMFs) produce
widespread neuropsychiatric effects including
depression[J]. J Chem Neuroanat. 2016, 75(Pt
B):43-51.
[33] Huber RTV, Borbely AA, et al.
Electromagnetic fields, such as those from
mobile phones, alter regional cerebral blood
flow and sleep and waking EEG[J]. J Sleep
Res. 2002, 11(4):289-295.
[34] Huber R, Treyer V, Schuderer J, et al.
Exposure to pulse-modulated radio frequency
electromagnetic fields affects regional
cerebral blood flow[J]. Eur J Neurosci. 2005,
21(4):1000-1006.
[35] Lee AK, Hong SE, Kwon JH, et al. Mobile
phone types and SAR characteristics of the
human brain[J]. Phys Med Biol. 2017,
62(7):2741-2761.
[36] Exelmans L, Bulck JVD. Bedtime Mobile
Phone Use and Sleep in Adults[J]. Social
Science & Medicine, 2016, 148:93-101.
[37] Arnal PJ, Fabien S, Damien L, et al. Benefits
of Sleep Extension on Sustained Attention and
Sleep Pressure Before and During Total Sleep
Deprivation and Recovery[J]. Sleep(12):12.
[38] Fritzer G, Göder R, Friege L, et al. Effects of
short‐and long‐term pulsed radiofrequency
electromagnetic fields on night sleep and
cognitive functions in healthy subjects.
Bioelectromagnetics: Journal of the
Bioelectromagnetics Society. The Society for
Physical Regulation in Biology and Medicine,
The European Bioelectromagnetics
Association. 2007, 28(4): 316-325.
[39] Hinrichs H, Heinze HJ, Rotte M. Human
sleep under the influence of a GSM 1800
electromagnetic far field. Somnologie-
Schlafforschung and Schlafmedizin. 2005,
9(4): 185-191.
[40] Huber R, Graf T, Cote KA, et al. Exposure to
pulsed high-frequency electromagnetic field
during waking affects human sleep EEG.
Neuroreport. 2000, 11(15): 3321-3325.
[41] Mann K, Röschke J. Effects of pulsed high-
frequency electromagnetic fields on human
sleep. Neuropsychobiology. 1996, 33(1): 41-
47.
[42] Nakatani ‐ Enomoto S, Furubayashi T,
Ushiyama A, et al. Effects of electromagnetic
fields emitted from W‐CDMA‐like mobile
phones on sleep in humans.
Bioelectromagnetics. 2013, 34(8): 589-598.
[43] Schmid MR, Loughran SP, Regel SJ, et al.
Sleep EEG alterations: effects of different
pulse ‐ modulated radio frequency
electromagnetic fields. Journal of Sleep
Research. 2012b, 21(1): 50-58.
[44] Wagner P, Röschke J, Mann K, et al. Human
sleep under the influence of pulsed
radiofrequency electromagnetic fields: a
polysomnographic study using standardized
conditions. Bioelectromagnetics: Journal of
the Bioelectromagnetics Society, the Society
for Physical Regulation in Biology and
Medicine, The European Bioelectromagnetics
Association. 1998, 19(3): 199-202.
[45] Wagner P, Röschke J, Mann K, et al. Human
sleep EEG under the influence of pulsed radio
frequency electromagnetic fields.
Neuropsychobiology. 2000, 42(4): 207-212.