Embed Size (px)
Citation preview

Experimental and Clinical Psychopharmacology1993, Vol. 1, Nos. 1-4, 215-241
Copyright 1993 by the American Psychological Association, Inc.1064-1297/93/$3.00
Effects of Adolescent Drug Use on Adult Mental Health:A Prospective Study of a Community Sample
Michael D. Newcomb, Lawrence M. Scheier, and P. M. Bentler
Mental health problems are often observed among drug abusers, althoughdirectional effects between drug use and psychopathology remain unclear.Latent-variable models were constructed with prospective data from acommunity sample of 487 participants who were assessed 4 times over 12 years,beginning when they were young adolescents. Drug use in adolescence andyoung adulthood included frequency of using alcohol, cigarettes, cannabis,cocaine, and hard drugs and reflected Polydrug Use constructs at both times.A strong stability effect was found for Polydrug Use, and the disturbance termcaptured the change in polydrug use over this time. Teenage Polydrug Use hadfew effects on adult mental health, whereas increased Polydrug Use exacer-bated later Psychoticism, Suicide Ideation, and other indicators of mentaldistress. Specific drug use in adolescence and changes in these into youngadulthood predicted later psychopathology.
Despite the common assumption that drug usecauses emotional distress and psychopathology,there is little scientific evidence for this beliefbeyond anecdotal and correlational findings. Forexample, it has been noted that drugs are oftenused to improve mood and relieve emotionaldistress (Labouvie, 1986; Newcomb, Chou, Bentler,& Huba, 1988) and that psychiatric impairment isfrequently observed in drug-abusing populations(e.g., Bukstein, Brent, & Kaminer, 1989; Ford,Hillard, Giesler, Lassen, & Thomas, 1989). Suchassociations lead many to conclude (perhaps pre-maturely) that drug use impairs mental health(e.g., Ross, Glaser, & Germanson, 1988; Rounsa-ville, Weissman, Chrits-Christoph, Wilber, & Kle-
Michael D. Newcomb, School of Education, Divisionof Counseling and Educational Psychology, Universityof Southern California; Lawrence M. Scheier, Depart-ment of Psychology, Temple University (now at Institutefor Prevention Research, Cornell University MedicalCollege); P. M. Bentler, Department of Psychology,University of California, Los Angeles.
This research was supported by Grant DA 01070 fromthe National Institute on Drug Abuse.
Correspondence concerning this article should beaddressed to Michael D. Newcomb, School of Educa-tion, Division of Counseling and Educational Psychol-ogy, University of Southern California, Los Angeles,California 90089-0031.
ber, 1982). However, a clear resolution of whetherdrug abuse truly contributed to or simply co-occurswith psychopathology and emotional distress hasevaded researchers (e.g., Kandel, Davies, Karus, &Yamaguchi, 1986). Research on the associationsbetween drug use and mental health has emergedprimarily from three sources: (a) studies of treat-ment and clinical samples, (b) cross-sectional ex-aminations of more general samples, and (c) analy-ses of prospective data.
Treatment and Clinical Studies
Most evidence regarding the relationship be-tween psychopathology and drug use comes fromclinical samples (e.g., Hesselbrock, Meyer, &Keener, 1985; Ross et al., 1988). In general, thesestudies reveal that drug abuse is strongly associ-ated with psychopathology before, during, andsomewhat less after treatment (e.g., Dorus &Senay, 1980; Kosten, Rounsaville, & Kleber, 1988).However, several confounds typically precludedrawing causal inferences regarding drug abuseand psychopathology from these treatment data.These include the presence of many diverse psychi-atric symptoms, inconsistent diagnostic practices,different patient population characteristics, andpremorbid symptoms that may be misconstrued assequelae. The most limiting problem, however, is
215

216 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
that all patients have some type of severe problemor dysphoria. Thus, they are distressed individualswilling to seek help, whose pathology is manifestand a problem; the development of drug abuse andpsychopathology has already occurred and thedevelopmental process cannot be observed accu-rately. Results from such samples cannot be gener-alized to nonclinical, community samples.
Cross-Sectional Studies
Findings from cross-sectional studies reveal mod-erate to strong associations between drug use andpsychopathology. For example, Gold, Washton,and Dackis (1985) screened a subset of cocaineabusers who called a national hotline and reportedhigh levels of self-reported depression (83%),irritability (87%), paranoid feelings (65%), andsuicide attempts (5%), with users reporting anaverage of 4 years of drug use. Based on theirgeneral population sample, Newcomb, Bentler,and Fahy (1987) reported several significant asso-ciations between cocaine use and psychopathol-ogy. For example, compared with male nonusers,male cocaine users reported higher levels of anx-ious mood, impaired cognitive functions, and im-paired motivation. They also reported greaterhostility, negative affect, a lack of purpose in life,and proneness toward psychotic thinking. Like-wise, female cocaine users, when compared withtheir nonusing counterparts, reported greater lev-els of depressed and anxious mood, impairedcognitive functions, greater hostility, and greaterproneness toward psychotic thinking, along with ahost of other distressful symptoms. Kandel (1984)reported that heavier marijuana users were morelikely to be hospitalized for mental health prob-lems, were less happy about life, and were morelikely to consult a mental health professional ascompared with lower level users. However, allthese analyses were cross-sectional, so that thecausal directions remain obscure.
Prospective Studies
A few longitudinal studies have examined themental health consequences of drug use in generalcommunity populations, and varied findings haveemerged (e.g., Kandel et al., 1986; Newcomb &Bentler, 1988a, 1988b). Some have reported causalrelationships between drug use and deteriorated
emotional health (e.g., Dackis & Gold, 1983;Newcomb & Bentler, 1988a, 1988b). Others havesuggested that, though much accepted as commonknowledge, evidence for causal relationships be-tween early drug use and later deficits in emotionaldevelopment is "hard to verify scientifically" (New-comb & Bentler, 1988b, p. 64). For example,adequate controls for preexisting conditions andimportant confounds may not have been made. Inaddition, several studies have reported apparentlypositive effects from moderate alcohol use, includ-ing greater positive affect, stress reduction, andlimited improvements in cognitive performance(Baum-Baicker, 1985; Kandel et al., 1986; New-comb & Bentler, 1988a, 1988b; Newcomb, Bentler,& Collins, 1986).
Explanatory Models
Several theoretical models have been advancedto explain the association between drug use-abuseand psychopathology. These explanations rangefrom biochemical to psychosocial processes. Sev-eral of these perspectives are summarized here.
Biochemical Mechanisms
Recent attention has been directed at the biologi-cal mechanisms of drugs on mood changes and thepossible pharmacological treatments for drug andalcohol addiction (e.g., Gawin & Kleber, 1984,1985; Gold et al., 1985; Kleber & Gawin, 1984).Several researchers have suggested that chronicdrug use or abuse creates long-term changes inbrain chemistry and synaptic transmission (e.g.,Dackis & Gold, 1985; Wise, 1984).
Expectancies
A different literature documents the critical roleof psychosocial expectations and learning on drugreactions and effects (e.g., Adesso, 1985; New-comb et al., 1988; Sher & Levenson, 1982). Ethicaland scientific restrictions limit these experimentsto short-term outcomes and prevent controlledstudy of the long-term consequences of chronicdrug use. With the exception of alcohol, much ofthis research has been limited to animal experi-ments, which cannot be generalized with accuracyto humans (for a review, see Adesso, 1980). Never-theless, prospective studies have begun to address

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 217
these causal mechanisms in community samples(e.g., Newcomb et al., 1988; Stacy, Newcomb, &Bentler, 1991a). This leaves unresolved whetherpsychopharmacological, psychobehavioral, or life-style changes from chronic drug use create long-term mental health consequences.
Self-Medication and Biphasic Mechanisms
Alcohol and drug use can have paradoxical orbiphasic psychological effects. Initially, alcoholand other drugs are used for their positive acutebenefits to improve mood, reduce stress, andrelieve emotional discomfort (Dackis & Gold,1983; Newcomb et al., 1988; Sadava, Thistle, &Forsythe, 1978). These acute positive effects areoften followed by emotional and cognitive distressand are exacerbated with continued, recurring,and chronic alcohol and drug consumption (e.g.,Beckman, 1980; Bibbs & Chambless, 1986; Keykin,Levy, & Wells, 1987; Malow, West, Williams, &Sutker, 1989). Both learning and opponent processtheories have been used to explain drug addictionmechanisms (e.g., Shipley, 1987).
Some hypothesize that drug use may be a formof self-medication: to relieve dysphoria and copewith stress (Khantzian & Treece, 1985; Kleber &Gawin, 1984; Wills, 1985). Barrett (1985) sug-gested that drug abusers increase their drug use toachieve an affective homeostasis, relying on previ-ously learned psychological reactions and expectan-cies from ingestion. With increasing physiologicaland psychological tolerance, drug abusers requiregreater amounts of the drug to prevent emotionaldistress, which potentiates an abusive and addic-tive cycle (Barrett, 1985; Marlatt, Baer, Donovan,& Kivlahan, 1988; Washton & Gold, 1984). More-over, a drug-abusing lifestyle may create economic,medical, relationship, and work problems that canlead to secondary emotional problems (Newcomb,1988; Newcomb & Bentler, 1988a). Refuge fromthese accumulating psychological strains may besought in continued or increased drug use, whichthen reinforces the addictive cycle.
Developmental Disruption
Adolescence is an essential developmental pe-riod during which rapid emotional, social, biologi-cal, and cognitive growth occur (e.g., Newcomb,1987). It is a time to consolidate psychological,
emotional, cognitive, and problem-solving growthand maturity to assume adult roles and responsibili-ties (Havighurst, 1972). Disruption of this processthrough precocious development, persistent druguse, or other interference may impair the learningof adequate psychological adaptational skills neces-sary for adult roles and responsibilities and createor exacerbate psychopathology (Newcomb, 1987;Newcomb & Bentler, 1988a).
Some Problems in Longitudinal Research
Although prospective studies offer hope fordisentangling causal sequences, there are severallimitations with earlier research. Often, only a fewmeasures of mental health were used. Kandel et al.(1986) only used scales of depression and psychoso-maticism, whereas Newcomb and Bentler (1988a)examined a wider, but still restricted, array ofmental health constructs. A more diverse set ofmental health measures is necessary to captureprecise and specific effects of drug use on psycho-logical functioning.
The maturational course and development ofpsychological states unfold throughout life. Tostudy these patterns requires long-term prospec-tive data (e.g., Gollob & Reichardt, 1987; New-comb et al., 1987). Most studies designed to assessinfluences of drug use on mental health havespanned relatively brief time periods, which pro-hibit investigation of major developmental transi-tions (e.g., Kandel et al., 1986; Newcomb & Bentler,1988a). In their earlier longitudinal investigation,Newcomb and Bentler (1988a) found some limitedsupport for negative effects from early drug use. Itis quite possible that effects may be more pro-nounced over longer periods of time (e.g., Hartkaet al., 1989). Certain developmental processes (i.e.,including psychological disorders) may take manyyears to unfold, making it likely that more severedisturbances might only be identified over lengthyperiods of time (e.g., Weissman et al., 1984).
In some cases (e.g., Kandel et al., 1986), compos-ite drug use measures were used. This practiceobscures potential differential mental health ef-fects related to specific drugs and prevents exami-nation of across-time drug-specific effects (New-comb, in press; Newcomb & Bentler, 1988a, 1988b).
Finally, most research depicts drug use at dis-crete points in time that reflect static "snapshots"of drug involvement and do not capture dynamic,

218 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
evolving patterns of use. Such static measures ofdrug use are certainly incomplete, because they donot reflect changes (increases or decreases) orstability of drug use behaviors as they evolve overtime. A more comprehensive approach involvescomparing early and later drug use measures tocapture dynamic drug use transition. One impor-tant reason for making this distinction in drug usepatterns is to understand whether drug use duringadolescence alone affects later mental health orwhether any subsequent changes (i.e., escalation,discontinuation) in drug use behaviors influencesubsequent mental health. In other words, areteenagers doomed to suffer throughout life be-cause of their adolescent drug use, or do subse-quent changes in their drug use patterns alter theeffects of earlier drug use?
Importance of This Research
Although research has documented the comor-bidity of psychopathology and drug abuse in treat-ment samples, no casual priority between thesedisorders has been established, and little clarifica-tion has emerged from general community samples(Newcomb et al., 1987). It is unclear whether highrates of comorbidity in treatment populations alsoexist in community samples. Most important is theneed to determine in a rigorous, empirical mannerif and how teenage drug use and dynamic changesinto adulthood are associated with or exacerbate •mental health problems in later life.
This study was designed to answer the followingresearch questions: (a) Does teenage drug use ordo changes in subsequent drug use affect psycho-logical functioning in adulthood? (b) Do staticmeasures of adolescent polydrug and use of spe-cific drugs better predict changes in psychologicalfunctioning than dynamic measures of the samedrugs that capture changes in drug use patternsover an 8-year period reflected in residual vari-ances? and (c) What specific types of mentalhealth are most vulnerable to which type andpattern of adolescent drug use?
To answer these questions, we used latent-variable structural equation models (SEMs) toanalyze four waves of data spanning a 12-yearperiod. Numerous measures of drug use weregathered in early and late adolescence and youngadulthood, and constructs of psychological func-tioning, emotional distress, traditional attitudes
(social conformity), and interpersonal contact (so-cial support) from late adolescence were used topredict a wide range of mental health constructs inadulthood. The study spanned a 12-year period inits entirety, with early adolescent drug use mea-sures obtained at baseline (1976) and follow-upmeasures obtained at Year 13 (1988), althoughcausal inferences can only be made over the last 8years (because Year 1 and Year 5 drug use datawere combined).
This research cannot determine definitivelywhether types and extents of teenage drug use(and subsequent dynamic changes in these pat-terns of drug involvement) caused or created in-crements or decrements for various types of men-tal health functioning over time. Such precise andunequivocal conclusions can only be made withtrue experimental designs, including random assign-ment (e.g., Newcomb, 1990). Such strict controlcannot ethically be imposed on long-term issues ofdrug use and psychopathology. Therefore, we chosethe most powerful, nonexperimental method avail-able to study these evolving relationships so thatwe can make the strongest conclusions regardingpotential causal inferences and effects. This ap-proach involves testing appropriate prospectivedata in complex SEMs and meeting as many causalcriteria as possible (Newcomb, 1990, in press). Wewere able to conform with most criteria underwhich a causal inference may be made (Newcomb,1987, 1990). The one critical criterion that thisresearch and all other nonexperimental designscannot meet is the need to control for all possibleconfounds and spurious influences. We controlledfor the most likely "omitted third variable" prob-lem by including numerous measures of socialsupport and social conformity (e.g., Newcomb &Rentier, 1988a), but these clearly do not capturethe universe of all potential confounding influ-ences. Nevertheless, we believe that these conclu-sions will provide strong support for likely causaleffects from teenage drug use and dynamic changesin their drug use patterns over time on varioustypes of mental health functioning in adulthood.
Method
Sample
The sample was initially contacted as 7th-through 9th-grade students in 11 Los Angeles

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 219
TablelDescription of Sample
Variable
Age (years)MRange
Ethnicity (%)BlackHispanicWhiteAsianOther
Education (years)MRange
No. of children (%)NoneOneTwoThree or more
Income for past year (%)Under $5,000$5,000-$15,000$15,000-$30,000Over $30,000
Living situation(%)AloneParentsSpouseCohabitationDormitoryRoommatesOther
Current life activity (%)MilitaryJunior collegeFour-year collegePart-time jobFull-time jobChild rearing/homemakerOther
Men(n = 136)
25.4624-28
81071101
14.6510-18
781561
7284421
9194182
147
3395
7314
Women(n = 351)
25.4924-27
151162111
14.0310-18
6421114
1926469
8194180
1311
0257
67154
Total(N = 487)
25.4824-28
131164111
14.2110-18
681994
16264612
8194181
1310
2266
69114
County schools and was followed for 12 years sothat we could study adolescent and adult growth,development, and drug use. The sample for thisstudy includes 487 participants who provided datain Year 1 (1976), Year 5 (1980), Year 9 (1984), andYear 13 (1988). A description of this sample asadults at Year 13 is given in Table 1. The sample isethnically mixed (about one third non-White), hasa mean age of about 25.5 years, and contains morewomen than men (which has been an unfortunate
feature from Year 1). Most are high school gradu-ates with an average of 2 years of college, morethan two thirds have full-time jobs, and about halfare living with a mate. More complete descriptionsof the sample and the scope of the research projectare reported elsewhere (Newcomb, 1992; New-comb & Bentler, 1988a, 1988b; Stacy, Newcomb, &Rentier, 1991a, 1991b).
Newcomb (1992) provided extensive attritionanalyses across the entire 12 years of this study.

220 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
Overall, these analyses show that gender andethnic composition have been only slightly alteredby attrition. Likewise, there were only minor differ-ences in Year 1 drug use prevalence rates betweendropouts and retained subjects over the 12-yearperiod. Moreover, participants who remained inthe study were quite similar to dropouts on numer-ous drug and personality measures obtained atYear 1.
Measures
Adolescent drug use scales. In Year 1, frequency-of-use scales for 5 classes of drugs were generated:alcohol (beer, wine, and liquor), cigarettes (oneitem), marijuana (cannabis and hashish), cocaine(one item), and hard drugs (including downers,heroin, inhalants, psychedelics, and uppers). Year1 drug use items were rated on 5-point anchoredscales that ranged from never (1) to regularly (5). InYear 5, the same 5 drug use scales were createdfrom identical substances as in Year 1 except forhard drugs, which in Year 5 were expanded toinclude 14 different substances. Year 5 drug itemswere rated on 7-point anchored scales, rangingfrom never (1) to more than once a day (7), for thepast 6 months. All 10 drug use scales were standard-ized, and then the same scales from Year 1 andYear 5 were averaged to produce 5 composite druguse scales reflecting drug use during adolescence.
These five scales of adolescent drug use wereused to reflect a Polydrug Use latent construct thatcaptured the extent of using multiple substancesduring early and late adolescence. In addition, theresidual variables from each of the five scales wereused to capture the specific use of each separatedrug and were tested as predictors. This procedureallowed us to separate the general effects ofpolydrug use, quite prevalent among adolescents(e.g., Clayton & Ritter, 1985), as a latent construct,from the effects of using specific types of drugs, ascaptured in the residual variables of the specificdrug use scales (after prediction from the commonfactor: see Newcomb, in press). This method hasbeen described by Newcomb (1990), with numer-ous examples elsewhere (e.g., Newcomb, 1988;Newcomb & Bentler, 1988a, 1988b). The onedifficulty with this procedure, when used withfirst-order latent factor models, is that systematicand random errors are confounded in the residualvariables (Newcomb, in press). Because of this
limitation, we primarily focus on large effects ofthese specific, residual variables (i.e., Stacy et al.,1991a, 1991b).
Increased drug use. Five young adult drug usescales (Year 9) consisted of the same items andrating scales as in Year 5 and were used to reflect alatent construct of Polydrug Use. For theoreticalpurposes, we wanted to use these drug use mea-sures to construct variables that reflect change indrug use from adolescence to young adulthood. Inother words, we wanted to compare drug usemeasures from adolescence to those in youngadulthood to capture dynamic changes (increased,decreased, or remained the same) of evolving druginvolvement after adolescence to young adulthoodand determine whether these generated changesin psychological functioning and emotional dis-tress into adulthood.
Dynamic changes in drug use can be captured inseveral ways from repeated assessments. Without atime-series design, differences can be representedas change scores. For example, VI - V\ wouldrepresent the change in a variable Kfrom Occasion1 to Occasion 2. In earlier, preliminary work, wetested this typical method to capture these changesin drug use over time as difference scores (New-comb & Bentler, 1989). This quite common methodcreated several difficulties, such as floor and ceil-ing effects, and numerous paradoxical or uninter-pretable results. Because of these difficulties, whichare commonly encountered with change or differ-ence scores (e.g., Cronbach & Furby, 1970; Woody& Costanzo, 1990), we used an alternative proce-dure in the present analyses. Furthermore, differ-ences among observed scores do not adequatelyreflect changes in a latent variable, and even latentvariables created from simple difference scoresmay not adequately reflect the stability of thatlatent construct (e.g., Nesselroade & Bartsch,1977).
J. Cohen and Cohen (1983) suggested an hierar-chical multiple regression approach as an alterna-tive to difference scores with repeated measuredata. However, this approach exaggerates thecross-sectional associations at the follow-up waveof data, which confounds change effects withcontemporaneous correlations. This approach isalso restricted to measured variables and is notextended to latent variables or unmeasured con-structs.
We took J. Cohen and Cohen's (1983) basic

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 221
approach and extended it to resolve both of thesedifficulties and unresolved issues. To deal with thefollow-up confound problems, we needed at leastthree waves of data. Dwyer (1983) pointed out thatto establish causal order between events, morethan two measurement waves are necessary. Werestricted our drug use follow-up measures (Year9) to a data wave earlier than the dependent orconsequence constructs (Year 13) but later thanthe independent variables or baseline measure(Years 1 and 5). Therefore, our change (residual)scores preceded our dependent measures by 4years and did not capitalize on contemporaneousassociations. Furthermore, we took J. Cohen andCohen's approach and applied it to latent con-structs by using the disturbance term of laterPolydrug Use after prediction from earlier Poly-drug Use as a change (residual) score to predictconsequences at a later time. Similarly, we usedmeasured-variable residual variables to simulta-neously capture change in use of specific drugs.
These innovative procedures certainly deviatenecessarily from the inadequate recommendationsof J. Cohen and Cohen (1983). They reflect signifi-cant improvements in method (SEMs), confounds(three waves of data instead of two), and interpre-tation (change precedes effects). Our solution usesresidualized latent- and measured-variable scoresfrom young adulthood to predict changes in men-tal health measures into adulthood. That is, if F2 =B * Fl + D2, where Fl and F2 are the latentvariables F measured at Occasions 1 and 2, and Bis the usual optimal regression weight, D2 repre-sents the part of F2 that is not predictable from Fl(Bentler, 1989). In our models, we evaluate theusual effects of Fl on various subsequent outcomelatent variables (in adulthood), but, in addition, wepermit D2 to be correlated with other factors atTime 1 (Year 9) and evaluate the "causal" effectsof D2 on a variety of other factors measured atTime 3 (Year 13).
In other words, we use residual or disturbanceterms as change variables. These residual variablesreflect that portion of drug use that is not stableover time, capturing whether drug use increased,decreased, or remained the same from one assess-ment to the next. In our structural equationmodels, the residual variables reflect changes ineach of the five types of drugs, as well as changes inpolydrug use as captured by latent constructs.These residual variables are constructed so that
higher values reflect increased drug use and theyare labeled accordingly.
Adolescent psychosocial scales. We includedthree other constructs from late adolescence (Year5) to control for across-time stability and spuriousconfound effects on later psychopathology. A con-struct of Emotional Distress was reflected in threescales: self-derogation (seven items; Kaplan &Pokorny, 1969); (low) self-acceptance (four items;Stein, Newcomb, & Bentler, 1986); and depression(four items; Newcomb, Huba, & Bentler, 1986).This Emotional Distress construct served as ageneral distress measure to control for stability inthe later mental health measures. Support for theuse of a general distress construct is provided byboth Scheier and Newcomb (1993) and Tanakaand Huba (1984).
Deviant or unconventional attitudes and behav-ior are strongly associated with drug use (McGee& Newcomb, 1992). To control for such possibleconfounds, we included a construct of Social Con-formity from adolescence to reflect rejection oradherence to conventional values. This latent fac-tor was reflected in three multiitem scales: lawabidance, (low) liberalism, and religious commit-ment (Newcomb & Bentler, 1988a, 1988b; Stein etal., 1986).
Finally, a latent factor of Social Support duringadolescence was included. This construct was cap-tured by four four-item scales measuring the sup-portiveness of relationships with parents, family,adults, and peers (Newcomb & Bentler, 1988b).Social Support is an important protective factoragainst psychopathology and positive influence onemotional health (e.g., S. Cohen & Wills, 1985;Newcomb & Bentler, 1988b) that must be repre-sented in the present analyses.
Adult Outcome Measures
Adult mental health status was captured by 27measured variables used to reflect nine latentconstructs: Emotional Distress, Self-Derogation,Psychoticism, Depression, Purpose in Life, SuicideIdeation, Anxiety, Hostility, and DisorganizedThinking. The confirmatory factor structure andmore complete description of all items and scalesare presented elsewhere (Scheier & Newcomb,1993).
The adult Emotional Distress construct had twoindicators. These were repeated assessments of

222 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
the same depression and (low) self-acceptancescales used in adolescence. The Self-Derogationscale was also repeated in adulthood but was notused as an indicator of the Emotional Distressconstruct as during adolescence. To gain greatersensitivity and specificity in adult affective function-ing, we created a separate Self-Derogation con-struct with two indicators: one scale each ofpositive and negative self-image (Harlow, New-comb, & Bentler, 1986).
The Magic Ideation (Magid) Scale (Eckblad &Chapman, 1983) was used to create indicators of alatent construct of Psychoticism. The 30 dichoto-mous items assess schizotypy and a predispositionto psychosis. These items were randomly parceledinto three 10-item subscales (Magid 1, 2, and 3;Newcomb & Bentler, 1988a).
A Depression construct was reflected by foursubscales of the 20-item Center for EpidemiologicStudies-Depression Scale (CES-D; Radloff, 1977).The CES-D emphasizes the affective componentof depression. The subscales were derived fromprevious factor analyses and included positiveaffect (the elevated mpod items), negative affect,impaired motivation, and impaired relationships(Harlow et al., 1986).
A construct of Purpose in Life (PIL) was hypoth-esized to reflect three scales created from a slightmodification of the 20-item Crumbaugh and Mahol-ick (1964) measure. Previous exploratory and con-firmatory factor analytic work verified the unidi-mensionality of the measure and the reliability ofthree scales of these 20 seven-point Likert-typeitems as indicators of a latent construct (PIL 1, 2,and 3; Harlow, Newcomb, & Bentler, 1986, 1987).
A Suicide Ideation construct was reflected byfour items: two from the Petrie and Chamberlain(1983) Suicide Behavior Subscale ("I have beenthinking about ways to kill myself and "I have toldsomeone I want to kill myself) and two additionalitems we created ("I have made attempts to killmyself and "I imagine my life will end withsuicide"; Harlow et al., 1986).
Separate constructs of Anxiety and Hostilitywere derived from a modified version of theHopkins Symptom Checklist (Uhlenhuth, Baiter,Mellinger, Cisin, & Clinthorne, 1983). Three itemswith the largest factor loadings from each scalewere chosen as indicators for each construct.
Finally, three four-item scales reflected a con-struct of Disorganized Thinking: thought disorga-
nization, (less) deliberateness, and (less) diligence(Stein et al., 1986).
Results
Descriptive statistics for all adolescent, youngadult, and adult variables are given in Table 2. Theright-hand column presents point-biserial correla-tions of each variable with gender of the respon-dent and reveals several mean differences. Thelargest accounted for less than 4% of the variancebetween men and women. Only a few researchershave found sex differences in psychological conse-quences of alcohol and drug use (e.g., Robbins,1989). The many variables needed in our modelrequire a large sample for stable and reliableresults. Separate analyses by sex would reduce oursample size to unacceptable numbers (e.g., Bentler& Chou, 1987; Marsh, Balla, & McDonald, 1988;Tanaka, 1987). Therefore, we had to combine oursamples of men and women in our SEMs, eventhough this sacrifices our ability to examine gender-specific mental health consequences of drug use.
We now turn to our SEM analyses. Although afew of our variables may be considered quasi-continuous or border on categorical (i.e., drug useitems, not the scales), categorical methods cannotcurrently be practically implemented with such alarge model (Newcomb, 1990). More important,Hays and Huba (1988) demonstrated clearly thatconclusions reached when drug use frequencyitems were analyzed by several different proce-dures all arrived at similar conclusions. Finally, thepresent analyses are based on presumed linearrelationships among the variables and are notdesigned to test for potential curvilinear or othernonlinear patterns, as at least one other study hasnoted may exist between drug use and psychologi-cal variables (Shedler & Block, 1990).
Confirmatory Factor Analyses
Before developing our structural or path model,we conducted a confirmatory factor analysis (CFA)to assess how well the observed measures reflectedthe hypothesized latent constructs. This analysisalso allowed us to examine the correlations amongthe unobserved latent factors. Change in PolydrugUse from adolescence to young adulthood wascaptured as a disturbance term (with higher valuesreflecting Increased Polydrug Use). We accom-

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 223
plished this by allowing the adolescent PolydrugUse construct to predict the young adult PolydrugUse construct, and the residual (or disturbance)variable of this adult latent factor representsIncreased Polydrug Use. Cross-time correlatedresiduals were included a priori for repeatedlymeasured variables. In addition, we correlatedresiduals of cocaine and hard drugs at each time tocapture their unique similarities as measures ofextremely illicit or hard drugs.
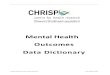
The fit of the model was adequate according toseveral criteria, x2(932, N = 487) = 1,761.01, p <.001, Comparative Fit Index (CFI; Rentier,1990) = .92. The CFI is a sample-size adjustedanalogue to the Normed Fit Index (Bentler &Bonett, 1980) and indicates the amount of covaria-tion in the data accounted for by the hypothesizedmodel. A rule of thumb is not to reject a modelwhen the ratio of the model's chi-square to thedegrees of freedom is less than 2.00 (Bentler, 1980;Bentler & Bonett, 1980). This ratio for the CFAmodel was 1.89, indicating an adequate model fit.Standardized factor loadings and residual vari-ables (variances) of the observed variables for theCFA model are depicted in Figure 1.
As hypothesized, all factor loadings for themeasured variables on the latent factors weresizable and significant (p < .001). The adolescentPolydrug Use construct largely reflected mari-juana, which had the largest loading, followed inmagnitude by alcohol and cigarette use and to alesser extent by cocaine and hard drug use. Simi-larly, marijuana use had nearly the largest factorloading on the young adult Polydrug Use con-struct; however, in this case, cocaine use had alarger loading than alcohol and cigarette use.
Table 3 presents the intercorrelations amongthe 13 latent factors and Increased Polydrug Useresidual variable. For the adolescent latent con-structs, adolescent Polydrug Use was strongly andsignificantly associated with less Social Conformityand moderately correlated with less Social Sup-port, more adolescent Emotional Distress, andmore adult Psychoticism. The stability correlationof adolescent Emotional Distress with adult Emo-tional Distress was of moderate magnitude andlarger than with the other adult constructs. Adoles-cent Emotional Distress was also significantly cor-related with all but one of the other adult mentalhealth constructs (excluding Psychoticism). Thisgenerally supports our use of the adolescent Emo-
tional Distress construct as a broad measure ofadolescent psychological distress and control forstability effects of most adult mental health con-structs.
Adolescent Polydrug Use significantly predictedyoung adult Polydrug Use (p = .74), leaving 45%of residual variance that we interpret as changes(increases or decreases) in Polydrug Use fromadolescence to young adulthood. Increased Poly-drug Use was correlated significantly with adoles-cent Social Conformity and only Psychoticism ofthe adult mental health constructs.
Structural Model Analyses
The same factor structure or measurement por-tion of the CFA model was used as the basis forour initial structural or path model. Correlationsamong all of the adolescent latent factors andIncreased Polydrug Use variable (residual) wereallowed to be estimated freely. We estimatedunidirectional paths from each adolescent con-struct (and Increased Polydrug Use) to every adultconstruct, capturing possible causal relationshipsin a saturated fashion (Newcomb, in press). Thedisturbance terms of all dependent (adult) latentfactors were allowed to intercorrelate freely. Eachof the residual variables from the five specific typesof adolescent drug use was allowed to predict itsanalogous measure in adulthood. The residuals ofeach of these five young adult drug use measuresrepresent increased use of each drug. Finally,within-time correlated residuals for cocaine andhard drugs were retained, and residuals for repeat-edly measured psychosocial variables were corre-lated across time.
As expected, this initial structural model had anidentical fit to the CFA model. This initial struc-tural model only tests standard across-time paths,those between latent constructs (Newcomb, inpress). To capture more detailed, subtle, andcomprehensive patterns in these data, we contin-ued our development of this structural model bytesting for specific or nonstandard paths acrosstime (Newcomb, 1990, in press; Newcomb &Bentler, 1988a, 1988b). Specific nonstandard pathswere added on the basis of empirical importanceand substantive interpretations. Empirical guid-ance was obtained from stepwise Lagrangian mul-tiplier tests (Chou & Bentler, 1990). In some cases,the sign of a parameter estimate was opposite to

224 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
Table 2Summary of Descriptive Statistics
Latent construct/measured variable M
No.of items Range SD Skew Kurtosis
Mean sexdifference3
rpb
Adolescence (Years 1 and 5)Adolescent Drug Use
Alcohol frequencyCigarette frequencyCannabis frequencyCocaine frequencyHard drug frequency
Emotional DistressDepressionSelf-acceptanceSelf-derogation
Social ConformityLiberalnessLaw abidanceReligious commitment
Social SupportRelationships with:ParentsFamilyAdultsPeers
—————
7.6615.892.41
9.9913.1515.44
15.9914.5517.1116.74
6242
19
447
444
4444
-1.33-2.49-0.85-2.22-0.60-3.25-0.30-5.15-0.33-8.74
4-184-200-10
4-194-204-20
6-204-207-206-20
—————
3.253.122.79
2.573.963.98
3.394.142.272.74
0.130.951.733.464.16
0.85-0.67
0.87
0.22-0.21-0.71
-0.78-0.57-0.70-1.08
-0.910.072.67
15.4233.31
-0.490.04
-0.08
0.10-0.70-0.28
-0.09-0.46
0.401.12
-.03.12**.01.06.07
.03-.03
.09*
.03
.13**
.14**
.03-.02
.09*
.04
Young adulthood (Year 9)Young Adult Drug Use
Alcohol useCigarette useCannabis useCocaine useHard drug use
—————
3222
14
-1.62-2.17-0.66-1.79-0.65-3.63-0.60-3.65-0.40-9.12
—————
-0.011.061.461.553.91
-1.04-0.69
1.021.31
21.26
-.09*-.07
.00-.01-.05
Adulthood (Year 13)Emotional Distress
DepressionSelf-acceptance
Self-DerogationPositive self-imageNegative self-image
Purpose in Life (PIL)PIL1PIL 2PIL 3
PsychoticismMagid 1Magid 2Magid 3
Suicide IdeationTold someone kill selfThink about killing selfLife end with suicideTried to kill self
7.2416.06
5.7710.97
11.4210.8411.13
21.6016.2228.78
1.181.251.101.09
44
25
677
101010
1111
4-204-20
4-610-15
4.3-143.6-143.5-14
20-2814-2118-35
1-41-41-41-4
2.992.91
0.551.28
1.681.711.59
1.691.321.91
0.470.540.390.38
1.36-0.94
-2.261.24
-0.97-0.70-0.65
1.200.90
-0.50
2.762.314.355.05
2.250.91
3.950.70
0.870.360.78
1.180.545.68
7.615.56
21.0129.45
.02-.06
-.11*.05
-.06-.06
.03
.07
.05
.03
-.04-.05-.06
.06

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 225
Table 2 (continued)
Latent construct/measured variable
CES-DPositive affectNegative affectImpaired social relationsImpaired cognitions
HostiltyHostility 1Hostility 2Hostility 3
AnxietyAnxiety 1Anxiety 2Anxiety 3
Disorganized ThinkingDeliberatenessDiligenceThought disorganization
M
2.420.500.260.57
2.472.362.00
2.432.562.18
13.4615.808.89
No.of items
Adulthood
4538
111
111
111
Range SD Skew Kurtosis
Mean sexdifference3
rpb
(Year 13) (continued)
0.50-30-2.80-30-2.75
1-51-51-4
1-51-51-5
4-206-204-18
0.600.540.410.44
0.860.800.80
0.870.830.83
3.042.752.89
-1.001.302.290.90
0.250.340.50
0.270.070.60
-0.24-0.60
0.52
0.321.527.521.00
-0.090.20
-0.21
-0.27-0.29
0.40
-0.100.320.00
-.12**.16***.00.10*
.19***
.16***
.16***
.01
.00-.09*
-.06.03.06
Note. Dashes for adolescent drug use indicate standardized scale scores were used averaging over early and late adolescence, anddashes for young adult drug use indicate standardized scale scores were also used. Magid = magic ideation; CES-D = Center forEpidemiologic Studies-Depression Scale.aA positive correlation indicates that women had the larger value.*p < .05. "p < .01. ***p<.001.
the corresponding covariance; these parameterswere regarded as suppressor effects and were notincluded. Specification searches were restricted toonly three types of specific or nonstandard across-time structural paths and were considered in thefollowing sequence: (a) adolescent latent factorsand Increased Polydrug Use variable to measuredvariables in adulthood; (b) measured-variable re-sidual terms in adolescence and those five residu-als reflecting increases in specific types of drug useto adult latent factors; and (c) adolescent mea-sured-variable residuals and five increased specificdrug use residuals to adult measured variables.After paths were added with the Lagrangian test,we made final model adjustments by deletingnonsignificant parameters with the Wald test (Chou& Bentler, 1990). This procedure of additions andthen deletions of model parameters has beenfound to be the best modification strategy tocapture the "true" model (Chou & Bentler, 1990;MacCallum, 1986).
A final structural model was obtained with anadequate fit, x2(856, N = 487) = 1,215.31, p <.001; CFI = .96. Figure 2 depicts the significantpaths between latent factors in this final structural
model. Correlations among adult latent constructresiduals were omitted from the figure for ease ofdepiction but are presented in Table 4.
Adolescent Polydrug Use did not significantlypredict any of the mental health latent constructsin adulthood. On the other hand, Increased Poly-drug Use was significantly associated with in-creased adult Psychoticism and Suicide Ideation.The effect on Psychoticism should be interpretedwith caution, because no comparable baselinemeasure was available to control for its stabilityand adolescent Emotional Distress did not servethis function.
Several nondrug effects between adolescentEmotional Distress and adult latent constructswere also apparent. Adolescent Emotional Dis-tress increased adult Emotional Distress, Self-Derogation, Suicide Ideation, Hostility, Disorga-nized Thinking, and decreased Purpose in Life.Adolescent Social Conformity and Social Supporthad no significant, direct effects on any of the adultlatent constructs.
Table 5 contains a summary of all specific ornonstandard effects reflecting paths from adoles-cent measured-variable residuals and latent fac-

226 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
AD VOUNG ADULTHOOD
Figure 1. Final confirmatory factor analysis model. (Large circles represent latent con-structs, rectangles are measured variables, and small circles with numbers are residualvariables. Factor loadings are standardized and all are significant [p < .001]. Notdepicted in the figure are two-headed arrows [i.e., correlations] joining each possiblepair of factors. Estimates for these correlations are given in Table 3. CES = Center forEpidemiologic Studies; magid = magic ideation; pil = purpose in life.)
tors to the various adult mental health measures(both latent and observed). These paths are allfrom the final structural model and must beconsidered in concert with results from the same
model given in Figure 2 and Table 4. These specificor nonstandard paths provide a detailed picture ofmore specific influences of both drug and nondrugadolescent variables on adult mental health (see

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 227
s!
CM CO CMTf CM CO
I I I
ICL.
W
! V

228 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
ADOLESCENCE
(YEAR 1-5)
YOUNG ADULTHOOD
(YEAH >)
ADULTHOOD
(YEAR 13)
IncreasePolydrug
Uca(.43)

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 229
Table 4Correlations Among the Factor Residuals in Adulthood From theFinal Structural Model
Factor 1
1. EmotionalDistress
2. Psychoticism3. CES-D4. Purpose in Life5. Self-Derogation6. Suicide Ideation7. Hostility8. Anxiety9. Disorganized
Thinking
.00a
.89-.84
.86
.62
.60
.48
.11*
.00a
.11*
.00a
.00a
.00a
.78
.78
.61
.55
.24
—-.70-.63-.60-.51
—.58.61.48
—.39 —.22* .45 —
.78 .00a .43 -.69 .59 .31 .34 .00a —
Note. Unless otherwise noted, all residual correlations are significant at p < .001 level(*p < .01). CES-D = Center for Epidemiologic Studies-Depression Scale."Parameter was nonsignificant and constrained at zero in the final structural model.
Newcomb, in press). Although many of theseeffects are relatively small, they represent partialregression coefficients, indicating unique contribu-tions beyond stability and baseline controls. Table5 is organized into three sections on the basis ofthe content of the predictor variables: adolescentdrug effects, increased drug use effects, and non-drug effects. These effects are numerous, and onlyselected ones are discussed here (all are presentedin Table 5).
By far the largest nonstandard regression effectinvolving drug use was from adolescent PolydrugUse to one indicator of Psychoticism (Magid 1).Among the various adolescent drug use predictorvariables, specific use of alcohol (residual) had fivesignificant across-time effects: higher alcohol usein adolescence decreased later CES-D, impairedcognitions (apparent beneficial effects), and PIL 3and increased one indicator of Suicide Ideation("think about killing self) and one indicator ofAnxiety. Adolescent cigarette use increased adultimpaired cognitions, Magid 3, and thought disorga-nization and decreased PIL 2, positive self-image,and deliberateness. Adolescent cannabis fre-
quency had four significant nonstandard effects:increased CES-D and Magid 3 and decreasedpositive self-image and "tried to kill self." Onlyone effect was noted for adolescent cocaine use: Itincreased one indicator of Psychoticism. Adoles-cent hard drug use increased negative self-image,"told someone kill self," and Magid 2 and de-creased PIL 2.
Increases in Polydrug Use and specific types ofdrug use had a variety of effects on mental healthin adulthood and are presented in the secondsection of Table 5. Increased Polydrug Use exacer-bated impaired relationships and Anxiety 3 andreduced positive affect. Increased consumption ofalcohol into young adulthood had 3 specific effects:improved self-image, reduced impaired relations(apparent beneficial effects), and decreased PIL 1.Increased cigarette use decreased Purpose in Lifeand deliberateness and heightened thoughts aboutkilling self. Increased cannabis use had 10 specificeffects on adult mental health functioning: greaterPsychoticism (and Magid 1), negative affect, Hostil-ity 1, thought disorganization, Emotional Distress,and Self-Derogation. Increased cannabis involve-
Figure 2 (opposite). Final structural model of the across-time effects between latentconstructs. (Large circles represent latent factors, and small circles with numbers reflectresidual variances. Path coefficients are standardized, and significance levels weredetermined by critical ratios on unstandardized coefficients [*p < .05; **p < .01;***p < .001]. Other nonstandard regression effects from this same final model that donot relate latent constructs to one another are given in Table 5. Correlations among theresiduals of adult latent factors are given in Table 4. CES = Center for EpidemiologicStudies.)

230 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
Table 5Nonstandard Effects Not Depicted in Figure 2
Predictors Consequences
Observed
Alcohol freq.Alcohol freq.Alcohol freq.Alcohol freq.Alcohol freq.Cigarette freq.Cigarette freq.Cigarette freq.Cigarette freq.Cigarette freq.Cigarette freq.Cannabis freq.Cannabis freq.Cannabis freq.Cannabis freq.Cocaine freq.Hard drug freq.Hard drug freq.Hard drug freq.Hard drug freq.
Increased alcohol useIncreased alcohol useIncreased alcohol useIncreased cigarette useIncreased cigarette useIncreased cigarette useIncreased cannabis useIncreased cannabis useIncreased cannabis useIncreased cannabis useIncreased cannabis useIncreased cannabis useIncreased cannabis useIncreased cannabis useIncreased cannabis useIncreased cannabis useIncreased cocaine useIncreased cocaine useIncreased cocaine useIncreased hard drug useIncreased hard drug useIncreased hard drug useIncreased hard drug useIncreased hard drug useIncreased hard drug use
Latent Observed Latent
Adolescent drug effectsPolydrug Use Magid 1
CES-DImpaired cognitionsPIL3Think about killing selfAnxiety 3Magid 3Impaired cognitionsPIL2Positive self-imageDeliberatenessThought disorganization
CES-DPositive self-imageTried to kill selfMagid 3Magid 3Magid 2PIL2Negative self-imageTold someone kill self
Increased drug use effectsIncreased Polydrug Use Positive affectIncreased Polydrug Use Impaired relationsIncreased Polydrug Use Anxiety 3
Impaired relationsPIL1Positive self-imageThink about killing selfDeliberateness
Purpose in LifePsychoticism
Magid 1Positive affectNegative affectTried to kill selfHostility 1Thought disorganization
Emotional DistressPurpose in LifeSelf-Derogation
Impaired relationsNegative self-imageTried to kill selfNegative affectImpaired relationsHostility 1Anxiety 2
PsychoticismDisorganized Thinking
Standard-ized
parameterestimate
.25**-.12**-.07*-.08**
.07*
.12**
.10*
.07*-.09**-.08*-.11*
.07*
.17**-.12*-.10*
.11*
.10*
.09*-.06*
.13***
.07*
-.13**.18***.15**
_ 14***-.06**
.09**
.05*-.15**-.06*
.11**
.11*-.17***
.09**-.15**
.09**
.10**
.14***-.14***
.16**
.14**
.06**
.14**-.10**
.08*-.07*
.07*
.14**
.12*

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 231
Table 5 (continued)
Predictors Consequences
Observed
Self-derogationSelf-derogationSelf-derogationSelf-derogationSelf-derogationSelf-derogationSelf-derogationSelf-derogationSelf-derogationSelf-acceptanceSelf-acceptanceSelf-acceptanceSelf-acceptanceSelf-acceptanceSelf-acceptanceSelf-acceptanceSelf-acceptanceSelf-acceptanceSelf-acceptanceSelf-acceptanceDepressionDepressionDepressionDepressionDepressionDepressionDepressionDepressionDepressionDepressionDepressionDepressionDepressionDepressionDepressionDepressionDepression
LiberalnessLiberalnessLaw abidanceLaw abidance
Latent Observed
Nondrug effectsEmotional Distress Impaired relationsEmotional Distress Positive affectEmotional Distress PIL 2Emotional Distress Told someone kill selfEmotional Distress Anxiety 1Emotional Distress Diligence
Negative affectImpaired cognitionsImpaired relationsHostility 2Hostility 3
Magid 3
Negative affectImpaired cognitionsNegative self-imageThink about killing self
Hostility 3
Thought disorganizationMagid 2Magid 3
Negative affectImpaired cognitionsImpaired relationsNegative self-image
PIL1
Anxiety 2Anxiety 3
DeliberatenessThought disorganization
Social Conformity Hostility 2Social Conformity Diligence
Deliberateness
Tried to kill self
Latent
PsychoticismSelf-DerogationAnxietyDisorganized Thinking
CES-D
Hostility
AnxietyDisorganized Thinking
CES-D
Purpose in Life
HostilityAnxiety
Disorganized Thinking
Suicide Ideation
Purpose in Life
Self-Derogation
Standard-ized
parameterestimate
.13**-.25***-.08*
.08*
.07*
.15*
.09**
.14***
.12**
.07*
.11**
.12*
.07*
.13*
.09*
.08*-.13*-.14**-.18***
.10**-.07*-.20***
.06*-.31***
.13*-.15***
.17***
.11**
.15*
.21**
.31***
.14**
.12**-.13**
.13**
.35***
.53***
.21***
.14**
.21**-.15**
.24***
.10*-.07*
.10*-.07*-.08*
.11**
.09*
(table continues)

232 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
Table 5 (continued)
Predictors
Observed
Law abidanceReligious commitmentReligious commitmentReligious commitmentReligious commitment
SocialSocialSocialSocial
Good relations with parentsGood relations with parentsGood relations with parentsGood relations with parentsGood relations with parentsGood relations with parentsGood relations with parentsGood relations with familyGood relations with familyGood relations with familyGood relations with familyGood relations with familyGood relations with adultsGood relations with adultsGood relations with adultsGood relations with peersGood relations with peersGood relations with peersGood relations with peers
Consequences
Latent Observed Latent
Nondrug effects (continued)DiligencePositive self-imageNegative self-imagePIL2Tried to kill self
Support DepressionSupport Negative affectSupport Impaired cognitionsSupport Impaired relations
PsychoticismPurpose in Life
Impaired relationsLife end with suicideTried to kill selfDeliberatenessThought disorganizationPositive self-imageThink about killing selfLife end with suicideTried to kill selfDiligencePositive self-imageHostility 3
AnxietyMagid 2
AnxietyThink about killing selfLife end with suicide
Standard-ized
parameterestimate
.10*
.07*-.06*
.07*
.11"-.05*-.15***-.08*-.11*
.12*
.07*-.12*-.14**-.16*
.19**-.18***
.08*-.10**-.14**-.15**-.10*
.09*-.12**-.09*-.08*-.08*-.07*-.08*
Note. All observed predictors are from the residual of that variable.Studies-Depression Scale; PIL = Purpose in Life.*p < .05. **p < .01. ***p < .001.
Magid = magic ideation; CES-D = Center for Epidemiologic
ment also reduced Purpose in Life, positive affect,and attempts to kill self. Increased cocaine useexacerbated impaired relations, negative self-image, and attempts to kill self. Finally, increasedhard drug use had 6 significant nonstandard effectsrelated to heightened Psychoticism, DisorganizedThinking, impaired relations, and Anxiety 2, and italso reduced negative affect and Hostility 1.
Other specific or nonstandard effects from ado-lescent predictors to adult mental health function-ing were quite numerous and are presented in thethird section of Table 5. For instance, EmotionalDistress increased impaired relations, Anxiety 1,diligence, and "told someone kill self and de-creased positive affect and PIL 2. These results
further confirm our use of a general EmotionalDistress construct to control for adolescent levelsof subsequent mental health measures (Scheier &Newcomb, 1993). The fewest nondrug, specificeffects of adolescent variables were for SocialConformity and its indicators. Both adolescentEmotional Distress and Social Support, in conjunc-tion with their specific indicators, had numeroussignificant effects on adult mental health function-ing. Among some of the larger effects was adoles-cent depression increasing both Hostility and Anxi-ety in adulthood. Social Support and various goodrelations with family and friends as a teenagerameliorated or reduced numerous types of mentalhealth problems as an adult.

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 233
Discussion
Mental health and psychological functioningevolve over time in response to various internaland external forces. To test whether drug useaffects mental health and psychological develop-ment, one must account for the effects of known orlikely influences of these outcomes. In our finalpath model, changes in mental health due to druguse could not be attributed to spurious influencesrelated to conventionality or traditionalism (SocialConformity); parental, peer, or family support(Social Support); or prior levels of EmotionalDistress. All of these likely factors were includedas baseline controls. If drug use and emotional dis-tress are generated by the same underlying causeor vulnerability to psychopathology, this researchdesign would reveal no unique, direct effects fromearlier drug use to later mental health problems(e.g., Garber & Hollon, 1991; Newcomb & Bentler,1988a). Although comorbidity between mentaldisorders and alcohol and drug abuse is quite highin both community and institutional samples (e.g.,Regier et al., 1990), we found that drug use mayprecede or exacerbate mental health problems.
Drug Use Consequences
The Adolescent and Increased Polydrug Useconstructs had unequal influences on adult mentalhealth. Adolescent Polydrug Use had no signifi-cant effects on any adult constructs and only onespecific effect on a measured variable in adulthood(Magid 1). In contrast, Increased Polydrug Usehad five significant long-term negative effects onadult mental health. Those who increased theirpolydrug use from adolescence to young adulthoodexpressed greater Psychoticism and Suicide Ide-ation, as general latent constructs, and specificallymore impaired relations, Anxiety 3, and less posi-tive affect than when they were teenagers. At leastin terms of Polydrug Use (reflecting a high level ofdrug involvement akin to drug abuse—Newcomb,1992; Newcomb & Bentler, 1988b), substance useas a teenager had few long-term detrimental ef-fects on mental health functioning. This is incontrast to the more numerous mental healthadversities associated with increased drug involve-ment from adolescence into adulthood.
Use of specific substances also adversely influ-enced several aspects of mental health, although
many of these effects were small in magnitude.These effects were more prevalent for increases inspecific substances but also included several spe-cific adolescent drug use measures. In our discus-sion, we focus on effects of .10 or higher and giveless attention to smaller, though significant, influ-ences.
Cannabis use had the greatest number of uniqueeffects on the outcome measures. Chronic mari-juana consumption has been associated with an"amotivational syndrome," based on the beliefthat excessive drug consumption leads to emo-tional disenfranchisement (Baumrind & Moselle,1985), perceived parental detachment (Brook, Gor-don, Brook, & Brook, 1989), impairments in cogni-tive functioning (Ferraro, 1980), and deficits inacademic performance (Mellinger, Somers, David-son, & Manheimer, 1976). Others have failed toconfirm that marijuana precipitates declines inmental health or intellectual functioning (e.g.,Ginsberg & Greeley, 1978; Kandel, 1978). Kandelreviewed relevant research and found little evi-dence that teenage marijuana use preceded theproblems associated with amotivation and con-cluded that many of these problems actually pre-ceded marijuana use. Our data indicate that adoles-cent and, particularly, increased cannabis use hadseveral long-term negative mental health conse-quences. Thus, the mental health consequences ofcannabis use may be more pronounced subsequentto adolescence rather than during the teenageyears.
Adolescent cigarette use was related to in-creased Magid 3 and decreased deliberateness andhad four other smaller effects. Increased cigaretteuse was also related to decreased deliberatenessand had two smaller adverse effects. Previously(Newcomb & Bentler, 1988b), we reported thatcigarette use increased emotional distress and alsohad damaging effects on other areas of life function-ing. This earlier study spanned 4 years (in contrastto the present 12-year study) and suggests that thenegative psychosocial consequences of cigaretteuse occur over a relatively short period of time andmay not persist over a greater length of time. Thelong-term major adversity of cigarette smokingmay be largely physical.
Cocaine use has been associated with emotionaldeterioration and psychosocial problems in clinical(e.g., Chitwood, 1985; Kosten et al., 1988) andsurvey populations (Newcomb & Bentler, 1986,

234 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
1987, 1988a, 1988b). Kosten et al. reported moredisturbance on a range of psychosocial outcomesamong addicts who increased their cocaine useover a 2.5-year period while in treatment for opioiddependence. On the other hand, Newcomb andBentler (1986) found no serious short-term conse-quences from cocaine use in their general popula-tion study, although teenagers were followed foronly 1 year and the extent of their cocaine consump-tion was limited. Discussing their findings, New-comb and Bentler (1986) reported, "cocaine use inthis more or less normal adolescent sample, gener-ated no significant increases or decreases in eightmeasures of emotional distress" (p. 272). Negativeeffects may take longer to emerge (e.g., Newcomb& Bentler, 1988a), as is typical with psychiatric dis-turbances (e.g., Lewinsohn, Duncan, Stanton, &Hautzinger, 1986). Contrary to these earlier find-ings from adolescence, we found four specificnegative effects in adulthood associated with ado-lescent and increased cocaine use into youngadulthood. Higher cocaine use during adolescenceincreased one indicator of Psychoticism in adult-hood, whereas increased cocaine use exacerbatedimpaired relations, negative self-image, and at-tempts to kill self. Petronis, Samuels, Moscicki,and Anthony (1990) also found that cocaine usewas associated with risk of making a suicideattempt.
Specific use of hard drugs during adolescencewas associated with increased later negative self-image, one indicator of Psychoticism (Magid 2),thoughts about suicide, and reduced PIL 2; thesegenerally reflect exacerbated personal alienation,self-dislike, and bizarre beliefs. The extreme legalsanctions, psychoactive potency, and social awk-wardness associated with using hard drugs (theiruse is generally not condoned even by peer groups)may contribute to these adverse effects. Equallyalarming, increased hard drug use was moderatelyassociated with increased Psychoticism and Disor-ganized Thinking and had small, but significant,influences on increasing Anxiety 2 and impairedrelationships and reducing hostility (only one indi-cator) and negative affect. We found similar effectsof teenage hard drug use on suicidal ideation overa 4-year period (Newcomb & Bentler, 1988a), andWard and Schuckit (1980) reported that polydrugusers (including hard drugs) had self-destructiveideation. The various potent sympathomimetic,sedating, anesthetic, or euphoriant properties of
these drugs (i.e., hypnotics, stimulants, inhalants,and narcotics) may provide immediate, but tempo-rary relief from psychic distress; however, whenuse is excessive or escalates over prolonged peri-ods of time, hard drugs create several types ofadverse mental health consequences.
There were both adverse and beneficial effectson adult mental health from specific early alcoholuse and increased alcohol use, when other drugeffects were controlled. The adverse consequenceswere related to indicators of Purpose in Life(lower), Anxiety (higher), and Suicide Ideation(higher).
Positive effects from alcohol use may be attrib-uted to the fact that alcohol, for most of society, islegal and does not carry the social, moral, and legalramifications associated with illicit drugs. Currentlaws prohibit alcohol use during adolescence; how-ever, in general, use of alcohol receives fewernegative social sanctions and may be considered bymany as a necessary social link in making thetransition between adolescence and adulthood(e.g., Jessor, 1986). Also, alcohol is generallyconsumed in social situations that may reinforcepositive expectancies in ways unlike other drugs,whose effects are more personal. Therefore, it isnot too surprising that alcohol has some limitedbeneficial effects generally related to affect (re-duced CES-D), social relations (reduced impairedrelations), and self-perception (increased positiveself-image). Similar beneficial effects of alcoholhave been noted in our earlier research (Newcomb& Bentler, 1988a, 1988b) and other studies (e.g.,Kandel et al., 1986).
Nondrug Relationships
Numerous developmental patterns unrelated todrugs were evident in the final SEM. Most of thoseeffects related to adolescent Emotional Distressand its specific measured-variable indicators andreflect synergistic influences over time among vari-ous types of psychopathology or mental health.They also demonstrate how dysphoric affect andpoor self-regard (Emotional Distress in adoles-cence) can have a generalized disruptive influenceon many aspects of adult mental health (emotions,attitudes, and perceptions) and social (impairedrelations) functioning. Emotional Distress alsoincreased diligence, a finding that was unexpected.One possible interpretation is that heightened

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 235
diligence may be an attempt to cope with orcontrol the chaos and helplessness of inner tur-moil. In other words, more diligence may be oneway to impose structure, order, and predictabilityon a life plagued with dissatisfaction and distress.
Various indicators of adolescent Social Confor-mity influenced several aspects of adult psychologi-cal functioning. Adherence to conventionality hadboth positive and negative effects on adult mentalhealth status and may reflect the mixed blessing offollowing social norms (e.g., Shedler & Block,1990). For instance, law abidance increased Self-Derogation and attempts to kill self (as did reli-gious commitment). On the other hand, moreadolescent Social Conformity and law abidanceincreased later diligence, and religious commit-ment enhanced self-image.
Finally, Social Support and many of the indica-tors of the Social Support construct enhancedemotional health and may be protective forces.These variables decreased Anxiety and variousindicators of Suicide Ideation, reduced negativeaffect, and improved social relations. Like Brooket al. (1989), we speculate that early disenfranchise-ment from traditional socialization influences andsupportive interpersonal connections may exacer-bate feelings of alienation and poor self-regardduring this critical developmental period and mayresult in both increases in drug use and increaseddysphoria. The latter finding is reinforced by thehigher levels of depression in adulthood for thoseyouth reporting low Social Support during adoles-cence. The one inconsistent finding to this patternwas that good relations with parents in adoles-cence increased adult Psychoticism. It is possiblethat overinvolvement with parents during adoles-cence may be antithetical to the development tasksof this age, which are to separate and individuatefrom parents and establish one's own intimatesupport network (e.g., Havighurst, 1972). As manyfamily theorists indicate (e.g., Bowen), overinvolve-ment with parents may lead to psychotic condi-tions, as noted in our findings.
Theoretical Implications
Our findings are especially important when weconsider that adolescence is a period of life duringwhich critical emotional, social, and psychologicalskills and competencies are acquired, tested, andrefined (e.g., Erikson, 1968). These involve acquisi-
tion of adult social roles, leaving home, attendingcollege, beginning independent living, employ-ment, marriage, and parenthood, to name just afew. Failure to acquire and master these competen-cies can result in serious emotional deficits andpsychopathology (Havighurst, 1972). Conceivably,drug-abusing or frequent drug-using teenagersmay have insufficient or inadequate socializationexperiences, fail to cope successfully with variousage-related stressors and transitions, and may bealienated from institutions from which many cop-ing skills can be acquired and learned (i.e., familyand schools). These drug-using, disaffected youthmay become depressed and blame themselves fortheir inadequacies, and some may believe thatincreased tension arising from self-doubt and per-sistent thoughts of failure and negative self-imagecan be assuaged through continued or increaseddrug involvement, in the hope of alleviating thisemotional distress. Our findings suggest that disrup-tion to developmental mechanisms through preco-cious, continued, or escalated drug use may causelong-term emotional harm.
Several theoretical explanations have been sug-gested to explain why drug-abusing or heavilydrug-involved youth lack adequate coping skills.Baumrind and Moselle (1985) suggested that ado-lescent drug use creates an hiatus from normaldevelopmental processes, leaving youth withoutthe necessary skills and cognitive abilities to ad-equately meet life's challenges. Alternatively, New-comb (1987; Newcomb & Bender, 1988a, 1988b)suggested that drug-involved youth accelerate theirdevelopment and pass over important developmen-tal experiences needed to acquire critical life skills.One example from our research includes abandon-ment of socially valued educational pursuits (Weng,Newcomb, & Bentler, 1988). Our present data donot directly test these hypotheses, although theyemphasize the importance of the later transitionalyears between adolescence and adulthood, suchthat drug abuse during this critical developmentalperiod may disrupt normal development and cre-ate serious mental health consequences.
Several researchers have suggested that drugabuse does not cause mental illness, but rather,that drug abuse causes unconventional behavior(e.g., Kaplan, Johnson, & Bailey, 1988) that lead todetachment and alienation from important socialinstitutions (i.e., school and family). Over time,such experiences may reduce feelings of purpose in

236 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
life, create social and interpersonal deficits,heighten anxiety and hostility, or even lead tothoughts about suicide. These resulting cognitions,behavior, and affect reflect deficits in emotionalfunctioning (e.g., B. P. Dohrenwend, Shrout, Egri,& Mendelsohn, 1980). This hypothesis is consis-tent with D. P. Dohrenwend's (1961) drift theory,which suggests that mental illness is a cause ofdisorganized social living, ultimately promulgatinga downward socioeconomic and functional spiralof the mentally ill. It is known from studies ofclinical populations that drug-abusing lifestylescan incur severe economic hardships, medicalcomplications, and often serious emotional difficul-ties that may further reinforce a downward drift(Khantzian & Schneider, 1986; Weiss, Mirin, Grif-fin, Michael, & Sollogub, 1986). As more treat-ment alternatives become available to these indi-viduals, including pharmacologic modalities, itbecomes increasingly important to refine andsharpen clinical distinctions between mental healthproblems that are primary and secondary sub-stance abuse disorders (e.g., Meyer, 1986).
One must also pay attention to problems associ-ated with dual diagnosis of substance abuse andother disorders (Ford et al., 1989; Khantzian &Treece, 1985; Regier et al., 1990; Rounsaville &Kleber, 1985). Intervention with drug abusersrequires difficult decisions to be made regardingchoice of treatment and problems associated withcomplicated and interrelated presenting symp-toms. It is possible that the developmental trajec-tory of psychopathology—when not accompaniedwith drug abuse—departs from a similar emotionaldysfunction with substance abuse (e.g., Khantzian& Schneider, 1986). In addition, poor social andcognitive skills of long-term drug abusers mayhinder treatment and recovery and require directremediation over a lengthy period. If early initia-tion and continued use of drugs impair mental andemotional functioning, as we have shown, thisheightens the importance of prevention efforts todelay drug use onset and to provide alternativeaffective coping and social skills (e.g., Hawkins,Lishner, & Catalano, 1985).
Limitations
There are several limitations to this study. First,the data were based on self-report measures andtheir possible biases (e.g., Stacy, Widaman, Hays,
& DiMatteo, 1985). Others have noted that self-report measures of drug use are valid and haveprovided empirical tests to underscore these claims(e.g., Needle, Jou, & Su, 1989). Notwithstanding,error in measurement could be minimized throughuse of collateral and independent reports of druguse, although this information was not availablefor these data.
Second, although youth may confront a numberof important developmental tasks during the tran-sition from adolescence to young adulthood, nego-tiation of other life periods may also produce stressand disequilibrium that could motivate individualsto use or abuse drugs. Even though this studyfocused on one developmental period that repre-sents a considerably long span of the life course,manifestation of the negative effects of drug abusemay not surface until even later in life, into olderadulthood. Certainly, it would be valuable to re-assess these adults further along their develop-mental course to determine whether the patternswe observed continue unabated into their lateradult lives.
Third, and corollary to the previous limitation,the time lag in this study may underestimate thecausal relationships between adolescent measuresand subsequent adult psychological functioning, ifsuch processes occur over a shorter period of time(e.g., Gollob & Reichardt, 1987). On the otherhand, viewed from a life span perspective, our timespan may have limited our ability to make generali-zations regarding the effects of drug use on devel-opmental processes to later and more extendedperiods of development.
Fourth, we did not assess psychiatric impair-ment with standard clinical diagnostic criteria (i.e.,the Diagnostic and Statistical Manual of MentalDisorders, 3rd. ed, rev.; American PsychiatricAssociation, 1987). Rather, we used standard andproven epidemiological assessment tools that havedemonstrated validity and reliability in generalcommunity studies. Although standard diagnosticassessment is most appropriate with clinical popu-lations (e.g. Ford et al., 1989), these categoricaldecision criteria are less appropriate and usefulwith community samples. They are impractical,have little utility with low base-rate pathology, andare cost-prohibitive. Most important, however, isthat they are dichotomous and therefore are re-stricted to only one or a few diagnostic "hits" (dualor triple diagnoses at most) and do not capture the

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 237
true range of psychopathology that is subclinical inextent. Accordingly, the measures used in thisstudy provided a broad, but still limited, assess-ment of psychopathology, as well as capturing thefull range of disturbance in each type of psychopa-thology. A wider selection of assessments alongwith a broader definition of psychopathology maystrengthen the effects observed between drug useand psychopathology.
Fifth, our assessments of drug use representedfrequency of consumption and did not determinedrug abuse, alcoholism, or other criteria of drugdependencies. The associations between use andabuse of drugs appeared to vary on the basis of theparticular substance (Newcomb, 1992), and ourpresent findings were restricted to frequency ofdrug use.
Sixth, because of the necessarily complex natureof our analyses, requiring inclusion and consider-ation of numerous influences to make the stron-gest causal inferences possible, we chose not toprovide simple descriptive statistics regarding howmuch greater risk for a particular type of psychopa-thology is associated with a specific increment indrug use. Although these figures could be pro-vided, they would be erroneous and misleading,because they could not reflect important con-founds, other controls, and shared variance ofcritical constructs. Therefore, the public healthsignificance of our various findings must be in-ferred from the size and significance of the stan-dardized path estimates. In general, the effectswere modest to moderate in magnitude.
Seventh, data for both men and women wereanalyzed together. As with other studies of surveydata (e.g., Johnston, O'Malley, & Bachman, 1988),patterns of drug use may differ between sexes,although we did not find substantial differences indrug use patterns. Previous analyses on this sampleconducted separately by sex have revealed fewsubstantial gender differences in substantive, pro-spective results (Newcomb et al., 1988; Stein,Newcomb, & Bentler, 1987). Conducting analysesseparately by sex would have produced too small ofsamples and compromised the robustness of ourstatistical techniques (e.g., Tanaka, 1987). Notwith-standing, collapsing data across sexes (and otherdemographic characteristics) may have maskedpotential gender differences in linkages betweenadolescent drug use and adult psychological func-tioning.
Finally, several other explanations for declinesin psychological functioning due to drug use couldnot be directly explored. For example, drug usemay alter neurophysiology and thereby impairneuropsychological functioning (e.g., Becker &Kaplan, 1986). Structural brain changes inducedthrough chronic drug use and concomitant neuro-psychological impairment may be synergistic anddifficult to separate. Quite possibly, acute cogni-tive impairment resulting from early drug use maymotivate heightened drug use to relieve distress oravoid the deficits. This may mask further cognitiveimpairment or facilitate misattribution of decre-ments in functioning to drug-induced behavioralchanges. Various biochemical models of addictionneed to be considered (e.g., cocaine and dopaminedepletion), which suggest that drug abuse mayprecipitate neurochemical changes that alone maycontribute to both acute and chronic neuropsycho-logical impairment.
References
Adesso, V. J. (1980). Experimental studies of humandrinking behavior. In H. Rigter & J. C. Crabbe (Eds.),Alcohol tolerance and dependence (pp. 123-155). Am-sterdam: Elsevier.
Adesso, V. J. (1985). Cognitive factors in alcohol anddrug use. In M. Galizio & S. A. Maisto (Eds.),Determinants of substance abuse: Biological, psychologi-cal, and environmental factors (pp. 179-208). NewYork: Plenum Press.
American Psychiatric Association. (1987). Diagnosticand statistical manual of mental disorders (3rd ed.,rev.). Washington, DC: Author.
Barrett, R. J. (1985). Behavioral approaches to individ-ual differences in substance abuse: Drug-taking behav-ior. In M. Galizio & S. A. Maisto (Eds.), Determinantsof substance abuse: Biological, psychological, and envi-ronmental factors (pp. 150-175). New York: PlenumPress.
Baum-Baicker, C. (1985). The psychological benefits ofmoderate alcohol consumption: A review of the litera-ture. Drug and Alcohol Dependence, 15, 305-322.
Baumrind, D., & Moselle, K. A. (1985). A developmen-tal perspective on adolescent drug use. Advances inAlcohol and Substance Use, 5, 41-67.
Becker, J. T., & Kaplan, R. F. (1986). Neurophysiologicaland neuropsychological concomitants of brain dysfunc-tion in alcoholics. In R. E. Meyer (Ed.), Psychopathol-ogy and addictive disorders (pp. 263-292). New York:Guilford Press.

238 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
Beckman, L. (1980). Perceived antecedents and effectsof alcohol consumption in women. Journal of StudiesonAlcohol, 41, 518-530.
Bentler, P. M. (1980). Multivariate analysis with latentvariables: Causal modeling. Annual Review of Psychol-ogy, 31, 419-456.
Bentler, P. M. (1989). EQS structural equations programmanual. Los Angeles: BMDP Statistical Software.
Bentler, P. M. (1990). Comparative fit indexes in struc-tural models. Psychological Bulletin, 107, 238-246.
Bentler, P. M., & Bonett, D. G. (1980). Significance testsand goodness of fit in the analysis of covariancestructures. Psychological Bulletin, 88, 588-606.
Bentler, P. M., & Chou, C.-P. (1987). Practical issues instructural modeling. Sociological Methods & Research,76,78-117.
Bibbs, J. L., & Chambless, D. L. (1986). Alcohol use andabuse among diagnosed agoraphobics. Behavior Re-search and Therapy, 24, 49-58.
Brook, J. S., Gordon, A. S., Brook, A., & Brook, D. W.(1989). The consequences of marijuana use on in-trapersonal and interpersonal functioning in blackand white adolescents. Genetic, Social, and GeneralPsychology Monographs, 115, 351-369.
Bukstein, O. G., Brent, D. A., & Kaminer, Y. (1989).Comorbidity of substance abuse and other psychiatricdisorders in adolescents. American Journal of Psychia-try, 146, 1131-1141.
Chitwood, D. D. (1985). Patterns and consequences ofcocaine use. In N. J. Kozel & E. H. Adams (Eds.),Cocaine use in America: Epidemiologic and clinicalperspectives (pp. 111-129). Rockville, MD: NationalInstitute on Drug Abuse.
Chou, C.-P., & Bentler, P. M. (1990). Model modifica-tion in covariance structure modeling: A comparisonamong likelihood ratio, Lagrange multiplier, and Waldtests. Multivariate Behavioral Research, 25, 115-136.
Clayton, R. R., & Ritter, C. (1985). The epidemiology ofalcohol and drug abuse among adolescents. Advancesin Alcohol and Substance Abuse, 4, 69-97.
Cohen, J., & Cohen, P. (1983). Applied multiple regression Icorrelation for the behavioral sciences (2nd ed.).Hillsdale, NJ: Erlbaum.
Cohen, S., & Wills, T. A. (1985). Stress, social support,and the buffering hypothesis. Psychological Bulletin,98, 310-357.
Cronbach, L. J., & Furby, L. (1970). How we shouldmeasure change—or should we? Psychological Bulle-tin, 74, 68-80.
Crumbaugh, J. C., & Maholick, L. J. (1964). An experi-mental study in existentialism: The psychometric ap-
proach to Frankl's concept of noogenic neurosis.Journal of Clinical Psychology, 20, 200-207.
Dackis, C. A., & Gold, M. S. (1983). Opiate addictionand depression—cause or effect? Drug and AlcoholDependence, 11, 105-109.
Dackis, C. A., & Gold, M. S. (1985). New concepts incocaine addiction: The dopamine depletion hypoth-esis. Neuroscience Behavioral Review, 9, 469-477.
Dohrenwend, B. P., Shrout, P. E., Egri, G., & Mendel-sohn, F. S. (1980). Nonspecific psychological distressand other dimensions of psychopathology. Archives ofGeneral Psychiatry, 37, 1229-1236.
Dohrenwend, D. P. (1961). The social psychological na-ture of stress: A framework for causal inquiry. Journalof Abnormal and Social Psychology, 62, 294-302.
Dorus, W., & Senay, E. C. (1980). Depression, demo-graphic dimensions, and drug abuse. American Journalof Psychiatry, 137, 699-704.
Dwyer, J. H. (1983). Statistical models for the social-andbehavioral sciences. New York: Oxford UniversityPress.
Eckblad, M., & Chapman, L. J. (1983). Magical ideationas an indicator of schizotypy. Journal of Consulting andClinical Psychology, 51, 215-225.
Erikson, E. H. (1968). Identity, youth and crisis. NewYork: Norton.
Ferraro, D. P. (1980). Acute effects of marijuana onhuman memory and cognition. In R. C. Peterson(Ed.), Marijuana research findings: 1980 (pp. 98-119).Rockville, MD: National Institute on Drug Abuse.
Ford, J., Hillard, J. R., Giesler, L. J., Lassen, K. L., &Thomas, H. (1989). Substance abuse/mental illness:Diagnostic issues. American Journal of Drug and Alco-hol Abuse, 15, 297-307.
Garber, J., & Hollon, S. D. (1991). What can specificitydesigns say about causality in psychopathology re-search? Psychological Bulletin, 110, 129-136.
Gawiri, F. H., & Kleber, H. D. (1984). Cocaine abusetreatment: Open pilot study with desipramine andlithium carbonate. Archives of General Psychiatry, 41,903-909.
Gawiri, F. H., & Kleber, H. D. (1985). Neuroendocrinefirtdings in chronic cocaine abusers: A preliminaryreport. British Journal of Psychiatry, 147, 569-573.
Ginsberg, I. J., & Greeley, J. R. (1978). Competingtheories of marijuana use: A longitudinal study. Jour-nal of Health and Social Behavior, 19, 22-34.
Gold, M. S., Washton, A. M., & Dackis, C. A. (1985).Cocaine abuse: Neurochemistry, phenomenology, andtreatment. In N. J. Kozel & E. H. Adams (Eds.),Cocaine use in America: Epidemiologic and clinical

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 239
perspectives (pp. 130-150). Rockville, MD: NationalInstitute on Drug Abuse.
Gollob, H. F., & Reichardt, C. S. (1987). Taking accountof time lags in causal models. Child Development, 58,80-92.
Harlow, L. L., Newcomb, M. D., & Bentler, P. M. (1986).Depression, self-derogation, substance use, and sui-cide ideation: Lack of purpose in life as a mediationalfactor. Journal of Clinical Psychology, 42, 5-21.
Harlow, L. L., Newcomb, M. D., & Bentler, P. M. (1987).Purpose in Life test assessment using latent variable.British Journal of Clinical Psychology, 26, 235-236.
Hartka, E., Johnstone, B. M., Leino, V., Motoyoshi, M.,Temple, M. J, & Fillmore, K. M. (1989, June). Trendsin drinking and depression in several longitudinal samples:An exploratory analysis from the collaborative alcohol-related longitudinal project. Paper presented at themeeting of the Life History Research Society, Mont-real, Quebec, Canada.
Havighurst, R. J. (1972). Developmental tasks and educa-tion (3rd ed.). New York: McKay.
Hawkins, J. D., Lishner, D., & Catalano, R. F. (1985).Childhood predictors and the prevention of adoles-cent substance abuse. In C. L. Jones & R. J. Battjes(Eds.), Etiology of drug abuse: Implications for preven-tion (pp. 75-126). Rockville, MD: National Instituteon Drug Abuse.
Hays, R. D., & Huba, G. (1988). Reliability and validityof drug use items differing in the nature of their re-sponse options. Journal of Primary Prevention, 6, 73-97.
Hesselbrock, M. N., Meyer, R. E., & Keener, J. J.(1985). Psychopathology in hospitalized alcoholics.Archives of General Psychiatry, 42, 1050-1055.
Jessor, R. (1986). Adolescent problem drinking: Psycho-social aspects and developmental outcomes. In R. K.Silbereisen, K. Eyferth, & G. Rudinger (Eds.), Devel-opment as action in context (pp. 241-264). Berlin:Springer-Verlag.
Johnston, L. D., O'Malley, P. M., & Bachman, J. G.(1988). Illicit drug use, smoking, and drinking byAmerica's high school students, college students, andyoung adults: 1975-1987. Rockville, MD: NationalInstitute on Drug Abuse.
Kandel, D. B. (1978). Convergences in prospectivelongitudinal surveys of drug use in normal popula-tions. In D. Kandel (Ed.), Longitudinal research ondrug use: Empirical findings and methodological issues(pp. 3-38). Washington, DC: Hemisphere.
Kandel, D. B. (1984). Marijuana users in young adult-hood. Archives of General Psychiatry, 41, 200-209.
Kandel, D. B., Davies, M., Karus, D., & Yamaguchi, K.
(1986). The consequences in young adulthood ofadolescent drug involvement. Archives of GeneralPsychiatry, 43, 746-754.
Kaplan, H. B., Johnson, R. J., & Bailey, C. A. (1988).Explaining adolescent drug use: An elaboration strat-egy for structural equations modeling. Psychiatry, 51,142-163.
Kaplan, H. B., & Pokorny, A. D. (1969). Self-derogationand psychosocial adjustment. Journal of Nervous andMental Disease, 149, 421^34.
Keykin, E. Y., Levy, J. C., & Wells, V. (1987). Adoles-cent depression, alcohol and drug abuse. AmericanJournal of Public Health, 77, 178-182.
Khantzian, E. J., & Schneider, R. J. (1986). Treatmentimplications of a psychodynamic understanding ofopioid addicts. In R. E. Meyer (Ed.), Psychopathologyand addictive disorders (pp. 323-333). New York:Guilford Press.
Khantzian, E. J., & Treece, C. (1985). DSM-IIIpsychiat-ric diagnosis of narcotic addicts: Recent findings.Archives of General Psychiatry, 42, 1067-1071.
Kleber, H. D., & Gawin, F. H. (1984). Cocaine abuse: Areview of current and experimental treatments. In J.Grabowski (Ed.), Cocaine: Pharmacology, effects, andtreatment of abuse (pp. 111-129). Rockville, MD:National Institute on Drug Abuse.
Kosten, T. R., Rounsaville, B. J., & Kleber, H. D. (1988).Antecedents and consequences of cocaine abuseamong opioid addicts: A 2.5-year follow-up. Journal ofNervous and Mental Disease, 176, 176-181.
Labouvie, E. W. (1986). Alcohol and marijuana use inrelation to adolescent stress. International Journal ofthe Addictions, 21, 333-345.
Lewinsohn, P. M., Duncan, E. M., Stanton, A. K., &Hautzinger, M. (1986). Age at first onset for nonbipo-lar depression (1986). Journal of 'Abnormal Psychology,95, 378-383.
MacCallum, R. (1986). Specification searches in covari-ance structure analyses. Psychological Bulletin, 100,107-120.
Malow, R. M., West, J. A., Williams, J. L., & Sutker,P. B. (1989). Personality disorders classification andsymptoms in cocaine and opioid addicts. Journal ofConsulting and Clinical Psychology, 57, 765-767.
Marlatt, G. A., Baer, J. S., Donovan, D. M., & Kivlahan,D. R. (1988). Addictive behaviors: Etiology and treat-ment. Annual Review of Psychology, 39, 223-252.
Marsh, H. W., Balla, J. R., & McDonald, R. P. (1988).Goodness-of-fit indexes in confirmatory factor analy-sis: The effect of sample size. Psychological Bulletin,103, 391-410.

240 M. NEWCOMB, L. SCHEIER, AND P. BENTLER
McGee, L., & Newcomb, M. D. (1992). General devi-ance syndrome: Expanded hierarchical evaluations atfour ages from early adolescence to adulthood. Jour-nal of Consulting and Clinical Psychology, 60, 766-776.
Mellinger, G. D., Somers, R. H., Davidson, S. T., &Manheimer, D. I. (1976). The amotivational syn-drome and the college student. Annals of the New YorkAcademy of Science, 282, 37-55.
Meyer, R. E. (1986). How to understand the relation-ship between psychopathology and addictive disor-ders: Another example of the chicken and the egg. InR. E. Meyer (Ed.), Psychopathology and addictivedisorders (pp. 3-16). New York: Guilford Press.
Needle, R. H., Jou, S. C, & Su, S. S. (1989). The impactof changing methods of data collection on the reliabil-ity of self-reported drug use of adolescents. AmericanJournal of Drug and Alcohol Abuse, 15, 275-289.
Nesselroade, J. R., & Bartsch, T. W. (1977). Multivari-ate experimental perspectives on the construct valid-ity of the trait-state distinction. In R. B. Cattell &R. M. Dreg^er (Eds.), Handbook of modern personalitytheory (pp. 221-238). New York: Hemisphere.
Newcomb, M. D. (1987). Consequences of teenage druguse: The transition from adolescence to young adult-hood. Drugs and Society, 1, 25-60.
Newcomb, M. D. (1988). Drug use in the workplace: Riskfactors for disruptive substance use among young adults.Dover, MA: Auburn House.
Newcomb, M. D. (1990). What structural modeling tech-niques can tell us about social support. In I. G. Sara-son, B. R. Sarason, & G. R. Pierce (Eds.), Socialsupport: An interactional view (pp. 26-63). New York:Wiley.
Newcomb, M. D. (1992). Understanding the multidimen-sional nature of drug use and abuse: The role ofconsumption, risk factors, and protective factors. InM. D. Glantz & R. Pickens (Eds.), Vulnerability to drugabuse (pp. 255-298). Washington, DC: AmericanPsychological Association.
Newcomb, M. D. (in press). Drug use and intimate rela-tionships among women and men: Separating specificfrom general effects in prospective data using struc-tural equations models. Journal of Consulting andClinical Psychology.
Newcomb, M. D., & Bentler, P. M. (1986). Cocaine useamong adolescents: Longitudinal associations withsocial context, psychopathology, and use of othersubstances. Addictive Behaviors, 11, 263-273.
Newcomb, M. D., & Bentler, P. M. (1987). Cocaine useamong young adults. Advances in Alcohol and Sub-stance Abuse, 6, 73-96.
Newcomb, M. D., & Bentler, P. M. (1988a). Conse-quences of adolescent drug use: Impact on the lives ofyoung adults. Newbury Park, CA: Sage.
Newcomb, M. D., & Bentler, P. M. (1988b). Impact ofadolescent drug use and social support on problems ofyoung adults: A longitudinal study. Journal of Abnor-mal Psychology, 97, 64-75.
Newcomb, M. D., & Bentler, P. M. (1989, September).Effects of specific drug use and cross-time dynamics: Astructural equations approach. Paper presented at theNational Institute on Drug Abuse Technical Review,Longitudinal Studies of Drug Abuse, Rockville, MD.
Newcomb, M. D., Bentler, P. M., & Collins, C. (1986).Alcohol use and dissatisfaction with self and life: Alongitudinal analysis of young adults. Journal of DrugIssues, 16, 479-494.
Newcomb, M. D., Bentler, P. M., & Fahy, B. (1987).Cocaine use and psychopathology: Associations amongyoung adults. International Journal of the Addictions,22, 1167-1188.
Newcomb, M. D., Chou, C.-P., Bentler, P. M., & Huba,G. J. (1988). Cognitive motivations for drug useamong adolescents: Longitudinal tests of gender dif-ferences and predictors of change in drug use. Journalof Counseling Psychology, 35, 426-438.
Newcomb, M. D., Huba, G. J., & Bentler, P. M. (1986).Life change events among adolescents: An empiricalconsideration of some methodological issues. Journalof Nervous and Mental Disease, 174, 280-289.
Petrie, K., & Chamberlain, K. (1983). Hopelessness andsocial desirability as moderating variables in predict-ing suicide behavior. Journal of Consulting and ClinicalPsychology, 51, 485-487.
Petronis, K. R., Samuels, J. F., Moscicki, E. K., &Anthony, J. C. (1990). An epidemiologic investigationof potential risk factors for suicide attempts. SocialPsychiatry and Psychiatric Epidemiology, 25, 193-199.
Radloff, L. S. (1977). The CES-D scales: A self-reportdepression scale for research in the general popula-tion. Applied Psychological Measurement, 1, 385—401.
Regier, D. A., Farmer, M. E., Rae, D. S., Locke, B. Z.,Keith, S. J., Judd, L. L., & Goodwin, F. K. (1990).Comorbidity of mental disorders with alcohol andother drug abuse: Results from the epidemiologiccatchment area (ECA) study. Journal of the AmericanMedical Association, 264, 2511-2518.
Robbins, C. (1989). Sex differences in psychosocialconsequences of alcohol and drug abuse. Journal ofHealth and Social Behavior, 30, 117-130.
Ross, H. E., Glaser, R. B., & Germanson, T. (1988). Theprevalence of psychiatric disorders in patients with

ADOLESCENT DRUG USE AND ADULT MENTAL HEALTH 241
alcohol and other drug problems. Archives of GeneralPsychiatry, 45, 1023-1031.
Rounsaville, B. J., & Kleber, H. D. (1985). Psycho-therapy/counseling for opiate addicts: Strategies foruse in different treatment settings. International Jour-nal of the Addictions, 20, 869-896.
Rounsaville, B. J., Weissman, M. M., Chrits-Christoph,K., Wilber, C., & Kleber, H. (1982). Diagnosis andsymptoms of depression in opiate addicts: Course andrelationship to treatment outcomes. Archives of Gen-eral Psychiatry, 39, 151-156.
Sadava, S. W., Thistle, R., & Forsythe, R. (1978). Stress,escapism, and patterns of alcohol and drug use.Journal of Studies on Alcohol, 39, 725-736.
Scheier, L. M., & Newcomb, M. D. (1993). Multipledimensions of affective and cognitive disturbance:Latent-variable models in a community sample. Psycho-logical Assessment, 5, 230-234.
Shedler, J., & Block, J. (1990). Adolescent drug use andpsychological health: A longitudinal inquiry. AmericanPsychologist, 45, 612-630.
Sher, K. J., & Levenson, R. W. (1982). Risk for alcohol-ism and individual differences in the stress-response-dampening effect of alcohol. Journal of AbnormalPsychology, 91, 350-367.
Shipley, T. C. (1987). Opponent process theory. In H. T.Blane & K. E. Leonard (Eds.), Psychological theoriesof drinking and alcoholism (pp. 346-387). New York:Guildford Press.
Stacy, A. W., Newcomb, M. D., & Bentler, P. M. (1991a).Cognitive motivation and problem drug use: A nine-year longitudinal study. Journal of Abnormal Psychol-ogy, 100, 502-515.
Stacy, A. W., Newcomb, M. D., & Bentler, P. M. (1991b).Personality, problem drinking, and drunk driving:Mediating, moderating, and direct-effect models. Jour-nal of Personality and Social Psychology, 60, 795-811.
Stacy, A. W., Widaman, K. F., Hays, R., & DiMatteo,M. R. (1985). Validity of self-reports of alcohol andother drug use: A multitrait-multimethod assessment.Journal of Personality and Social Psychology, 49, 219-232.
Stein, J. A., Newcomb, M. D., & Bentler, P. M. (1986).Stability and change in personality: A longitudinalstudy from early adolescence to young adulthood.Journal of Research in Personality, 20, 276-291.
Stein, J. A., Newcomb, M. D., & Bentler, P. M. (1987).Personality and drug use: Reciprocal effects acrossfour years. Personality and Individual Differences, 8,419-430.
Tanaka, J. S. (1987). "How big is big enough?": Samplesize and goodness of fit in structural equation modelswith latent variables. Child Development, 58, 134-146.
Tanaka, J. S., & Huba, G. J. (1984). Confirmatoryhierarchical factor analysis of psychological distressmeasures. Journal of Personality and Social Psychology,46, 621-635.
Uhlenhuth, E. H., Baiter, M. B., Mellinger, G. D., Cisin,I. H., & Clinthorne, J. (1983). Symptom checklistsyndromes in the general population: Correlationswith psychotherapeutic drug use. Archives of GeneralPsychiatry, 40, 1167-1173.
Ward, N. G., & Schuckit, M. A. (1980). Factors associ-ated with suicidal behavior in polydrug abusers. Jour-nal of Clinical Psychiatry, 41, 379-385.
Washton, A. M., & Gold, M. S. (1984). Chronic cocaineabuse: Evidence for adverse effects on health andfunctioning. Psychiatric Annals, 14, 733-743.
Weiss, R. D., Mirin, S. M., Griffin, M. L., Michael, J. L.,& Sollogub, A. C. (1986). Psychopathology in chroniccocaine abusers. A merican Journal of Drug and AlcoholAbuse, 12, 17-29.
Weissman, M. M., Wickramaratne, P., Merikangas,K. R., Leckman, J. F., Prusoff, B. A., Caruso, K. A.,Kidd, K. K., & Gammon, D. (1984). Onset of majordepression in early adulthood. Archives of GeneralPsychiatry, 41, 1136-1143.
Weng, L.-J., Newcomb, M. D., & Bentler, P. M. (1988).Factors influencing noncompletion of high school: Acomparison of methodologies. Educational ResearchQuarterly, 12, 8-22.
Wills, T. A. (1985). Stress, coping, and tobacco andalcohol use in early adolescence. In S. Shiffman &T. A. Wills (Eds.), Coping and substance use (pp.67-94). San Diego, CA: Academic Press.
Wise, R. A. (1984). Neural mechanisms of the reinforc-ing action of cocaine. In J. Grabowski (Ed.), Cocaine:Pharmacology, effects, and treatment of abuse (pp.15-33). Rockville, MD: National Institute on DrugAbuse.
Woody, E. Z., & Costanzo, P. R. (1990). Does maritalagony precede marital ecstasy? A comment on Gott-man and Krokoffs "Marital Interaction and Satisfac-tion: A Longitudinal View." Journal of Consulting aridClinical Psychology, 58, 499-501.
Received January 11,1993Revision received May 20,1993
Accepted May 28,1993