Embed Size (px)
Citation preview

Effect on Prognosis of Abolition of Exercise-Induced Painless Myocardial
lschemia by Medical Therapy Richard Lim, MRCP, Lorraine Dyke, and Duncan S. Dymond, MD
During exercise radionuclide ventricukgraphy, many patients with coronary artery disease exhib- it painters myocardial ischemia defined as an ab- normal left ventricular ejection fraction response without accompanying angina. To see if complete suppression of such exercise-induced painless ischemia by anti-ischemic medication implies a better prognosis in medically treated coronary ar- tery disease, 34 patients underwent repeat testing at 4 weeks receiving regular conventional therapy that rendered angina no worse than class I. With such therapy, painless ischemia was abolished in 12 patients (group I) and persisted in 22 (6596, group II). Both groups were similar in age, number of diseased vessels, proportion with previous myo- cardial infarction, exercise ejection fraction, and degree of exercise-induced painless ischemia at baseline. At 9 months, adverse events had oc- curred in 11 patients (2 patients with myocardial infarctton, 4 with unstable angina, 2 with angio- plasty and 3 with bypass surgery). Only I of 12 patients (8%) in group I had experienced events compared with 10 of 22 (45%) in group II (chi- square, 5.4, p <0.025,95% confidence interval, 12 to 61%). Thus, the relative risk of adverse events in patients whose painless &hernia was abolished was only 18% of that in patients in whom it was persistent. These results suggest that (1) the abolition of exercise-induced pain- less ischemia by conventional symptom-dictated medical therapy confers a better short-term prog- nosis in medkally treated coronary artery disease, and (2) therapeutic effkacy may need to be as- sessed by tttration against ischemia and not against angina.
(Am J Cardiol1992;69:733-735)
From the Department of Cardiology, St Bartholomew’s Hospital, Lon- don, United Kingdom. This study was supported by a grant from the St Bartholomew’s Hospital Joint Research Board. Manuscript received July 23, 1991; revised manuscript received November 13, 1991, and accepted November 14.
Address for reprints: Richard Lim, MD, Department of Cardiolo- gy, St. Bartholomew’s Hospital, London EClA 7BE, United Kingdom.
vidence E is accumulating that the occurrence of si- lent or painless myocardial ischemia, whether spontaneous’-s or exercise-induced,6-8 is associ-
ated with adverse outcome in various subgroups with coronary artery disease. Recent interest has therefore focused on whether treatment of such ischemia has prognostic implications. 9~10 However, despite numerous reports”-l5 on the effects of antianginal medications on painless ischemia, the question remains: Does treatment or abolition of painless ischemia improve the patient’s prognosis? We have therefore prospectively examined whether eliminating exercise-induced painless ischemia by conventional symptom-dictated antianginal therapy is associated with improved prognosis compared with its persistence despite such therapy.
METHODS S&j&s: After coronary arteriography performed
because of a history of chest pain or a positive postin- farction exercise electrocardiogram, 61 patients were recommended to continue with medical treatment on the basis of minimal angina and arteriographic disease that did not demand early revascularization. However, all had significant coronary artery disease visually de- fined as 150% luminal diameter stenosis in I1 major artery amenable to revascularization. All patients had already been taking antianginal medication chosen by their physician from the usual range of conventional agents. Such medication was interrupted for 4 days for exercise radionuclide ventriculography performed with- in 6 weeks after arteriography. No patient had angina during this temporary period without medication.
At this initial radionuclide ventriculography, 34 sub- jects (29 men, mean age 58 years, range 31 to 71) ex- hibited painless ischemia and thus qualified for further study. Significant narrowing was present in 1 coronary artery in 10 patients, in 2 arteries in 16 patients, and in 3 arteries in 8 patients. None had significant left main stem narrowing, heart failure, left bundle branch block, atria1 fibrillation or valvular disease.
Exercise radienuciii ventricukgraphy: This was performed with the first-pass techniquei using the Scinticor multicrystal gamma camera system (Scinticor Inc, Milwaukee, Wisconsin). Maximal symptom-limited graded upright exercise on a Fitron cycle ergometer was limited by leg fatigue in most patients. Painless isch- emia was defined as a decrease in global left ventricular ejection fraction from rest to exercise in the absence of pain in the upper half of the body. For the purpose of this study in patients with documented coronary artery
MEDICAL TREATMENT OF PAINLESS ISCHEMIA 733

disease, regional ventricular abnormalities were not in- cluded in the analysis.
Anti-ischemic treatment was resumed after the ini- tial radionuclide ventriculography and maintained dur- ing repeat testing at 4 weeks. During this period, no patient had angina worse than Canadian Cardiovascu- lar Society class I or required adjustment of medica- tions. Exercise was performed to the duration and work load previously achieved.
FoNow-up: Telephone contact with all patients was conducted at 3-month intervals until study termination at 9 months, when a 1Zlead electrocardiogram was also recorded to look for new pathologic Q waves. The fol- lowing adverse events constituted study end points: (1) cardiac death or failed sudden death, (2) myocardial infarction, (3) revascularization for significant symp- toms, and (4) unstable angina necessitating hospitaliza- tion. Events were verified by reference to medical rec- ords.
StatMeal analysis: The primary outcome measure was an aggregate of the aforementioned end points and was analyzed according to whether painless ischemia was abolished by medication or persisted despite medi- cation. The relative risk and odds ratio for adverse out- come were calculated. Chi-square and unpaired t testing were performed to compare the groups in which pain- less ischemia was abolished or persistent, with respect to variables previously shown to have independent prog- nostic value. A p value <0.05 was considered statistical- ly significant.
RESULTS During radionuclide ventriculography with patients
taking medication, 12 no longer had painless ischemia (group I) and 22 (65%) continued to have painless isch- emia (group II). Both groups were similar in age, num- ber of significantly narrowed coronary arteries and proportion with a history of myocardial infarction or hypertension. There was also no significant baseline dif- ference between groups I and II in the mean (f stan- dard deviation) exercise ejection fraction (38 f 12% vs
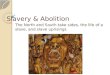
Number of Patients * P <0.025
251 m Advwse Events 10122 l
20 El Event-free
RR = 5.5 15
l/12 *
IO m 3
I I 5
ppleb pplalma
0 l!s&m#h 1iwmf*
Abolished Persistent
FIGURE 1. Reldve ridt (RR) of adverse cudac events ac- khemiawas-byorcam
-tb-PY.
38 f 9%) or degree of painless ischemia induced by exercise (decrease in ejection fraction 8 f 4% vs 11 f 6%).
At g-month follow-up, 11 patients (32%) had experi- enced adverse events comprising 2 cases of acute myo- cardial infarction, 4 of hospital admission for unstable angina, and 5 requiring revascularization (2 percutane- ous angioplasty and 3 bypass surgery) because of signif- icant recurrent angina. No death occurred. Only 1 of 12 patients (8%) in group I had experienced an adverse event compared with 10 of 22 (45%) in group II (chi square, 5.4; p <0.025; 95% confidence interval = 12 to 61%). The odds ratio for adverse events when painless ischemia was not eliminated was 9.2 (95% confidence interval, 1.04 to 79.5). When painless ischemia was controlled with medication, the relative risk of nonfatal adverse cardiac events was only 18% of that when it was persistent despite medication (i.e., an improvement more than fivefold) (Figure 1).
DISCUSSION The control of angina by medication has probably
improved, but the importance of painless ischemia is in- creasingly recognized. However, it is not known wheth- er such painless ischemia, per se, requires treatment or whether it merely reflects potential instability of coro- nary atheromatous lesions and is thus simply a marker of high-risk disease. If the latter is true, mechanical re- vascularization may be necessary to prevent adverse clinical events; if the former is true, anti-ischemic medi- cations may afford adequate protection against isch- emia-related events.
Our study reports on patients already receiving con- ventional symptom-driven anti-ischemic medication. In this small study, we have documented systematically for the first time that complete suppression of exercise-in- duced painless ischemia by such treatment is associated with a better nonfatal short-term outcome. Nearly half of our patients with persistent painless ischemia had ex- perienced an ischemic event within 9 months, compared with a low incidence of <lo% among those who no longer had such ischemia when tested while still taking their regular treatment. Thus, the latter group was 5 times less likely to have an adverse event in the short term. The overall event rate of 32% was partly due to our subjects being highly selected. After coronary arte- riography, they were considered as part of a low-risk group because of minimally symptomatic, noncritical, although significant, anatomic disease, and were there- fore recommended to continue medical treatment. How- ever, all 34 patients subsequently demonstrated induci- ble ischemia during radionuclide ventriculography per- formed without medication specifically for the study.
This suggests that in our practice, up to one third of all patients with coronary artery disease who are recom- mended for medical treatment after arteriography may in fact remain at short-term risk if they have a demon- strable ischemic burden despite minimal angina. We have found that such patients tend to have residual ex- ercise-induced painless ischemia despite clinically ade- quate antianginal therapy. Such persistent ischemia im-
734 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 69 MARCH 15, 1992

plies continuing vulnerability to ischemic events, which appears to be significantly reduced if it can be sup pressed by conventional medical therapy. Our study also provides preliminary nonrandomized evidence to sup- port a strategy of optimizing medical therapy to abolish ischemia and not just angina. However, the hypothesis remains to be proved that painless ischemia which per- sists despite “maximum” medical therapy identities the patients at highest risk. A randomized study is needed to show that additional treatment specifically directed at ischemia that persists despite clinically adequate conventional background medication further improves prognosis.
That subjective symptoms are a poor indicator of myocardial ischemia5J 7,1 8 and thus probably an inade- quate guide to management suggests the need to consid- er objective individualized assessment of the “cardiopro- tective” efficacy of medical treatment. This may be amenable to testing by radionuclide ventriculography, exercise electrocardiography or ambulatory ST-segment monitoring. It is not established that using continuous ambulatory monitoring to guide treatment has any prognostic advantage over the arguably more conve- nient exercise tests, particularly because there is evi- dence that ambulatory ischemia is uncommon when no ischemia is inducible during exercise testing.3J4J9-21 However, it is conceivable that anti-ischemic treatment which fails to suppress painless ischemia induced by maximal exercise may in fact succeed in abolishing spontaneous ischemia. The prognostic implications of complete or partial suppression of ischemia and whether painless ischemia can be stratified for risk merit investi- gation. Finally, because any prognostic test has a time- limited value given the progressive tendency and inher- ent unpredictability of coronary disease, how regularly such testing should occur needs to be defined.
REFERENCES 1. Nademanec. K, Intarachot V, Josephson MA, Rieders D, Mody FV, Singh BN. Prognostic signiticance of silent myocardial ischemia in patients with unstable angina. J Am Co11 Cardiol 1987;10:1-9. 2. Gottlieb SO, Weisfeldt ML, Quyang P, Mellits ED, Gerstenblith G. Silent &hernia predicts infarction and death during 2 year follow-up of unstable angina. J Am CON Cardiol 1987;10:756-760.
3. Tzivoni D, Gavish A, Zin D, Gottlieb S, Moriel M, Keren A, Banai S, Stern S. Prognostic significance of ischemic episodes in patients with previous myocardial infarction. Am J Cardiol 1988;62:661-664. 4. Rocco MB, Nabel EG, Campbell S, Goldman L, Barry J, Mead K, Selwyn AP. Prognostic importance of myocardial ischemia detected by ambulatory monitor- ing in patients with stable coronary artery disease. Circulation 1988;78:877-884. 5. Deedwania PC, Carbajal EV. Silent ischemia during daily life is an indepen- dent predictor of mortality in stable angina. Circulation 1990;81:748-756. 6. Weiner DA, Ryan TJ, McCabe CH, Luk S, Chaitman BR, Sheffield LT. Tristani F, Fisher LD. Signiticance of silent myocardial ischemia during exercise testing in patients with coronary artery disease. Am J Cwdiol 198759725-729, 7. Breitenbucher A, Pfisterer M, Hoffmann A, Burckhardt D. Long-term follow- up of patients with silent ischemia during exercise radionuclide angiography. J Am Co/l Cardiol 1990,15:999-1003. 8. Gasperetti CM, Burwell LR, Belier GA. Prevalence of and variables associated with silent myocardial ischemia on exercise thallium-201 stress testing. JAm Coil Cardiol 1990;16:115-123. 9. Pepine CJ. Is silent ischemia a treatable risk factor in patients with angina pectoris? Circulufion 1990;82 (suppl lI):II-135-11-142. 10. Cohn PF. Should silent ischemia be treated in asymptomatic individuals? Circulofion 1990;82(suppl II):lI-149-D-154. il. Schang SJ Jr, Pepine CJ. Transient asymptomatic S-T segment depression during daily activity. Am J Cardiol 1977;39:396-402. 12. Borer JS, Bacharach SL, Green MV, Kent KM, Johnston GS, Epstein SE. Effect of nitroglycerin on exercise-induced abnormalities of left ventricular re- gional function and ejection fraction in coronary artery disease. Assessment by radionuclide cineangiography in symptomatic and asymptomatic patients. Circu- lation 1978;57:314-320. 13. lmperi GA, Lambert CR, Coy K, Lopez L, Pepine CJ. Effects of titrated beta blockade (metoprolol) on silent myocardial ischemia in ambulatory patients with coronary artery disease. Am J Cordiol 1987;60:519-524. 14. Cohn PF, Vetrovec GW, Nest0 R, Gerber FR. The Nifedipine-Total Isch- emia Awareness Program: a national survey of painful and painless myocardial &hernia including results of antiischemic therapy. Am J Cardiol 1989;63: 534-539. 15. Stone PH. and the ASIS Study Group. Comparison of propranolol, diltiazem, and nifedipine in the treatment of ambulatory ischemia in patients with stable angina. Differential effects on ambulatory &hernia, exercise performance, and angina1 symptoms. Circulation 1990;82:1962-1972. 16. Zaret BL, Berger HJ. First-pass and equilibrium radionuclide angiocardiog- raphy for evaluating ventricular performance. In: Simoons ML, Reiber JHC, eds. Nuclear Imaging in Clinical Cardiology. Boston: Martinus Nijhoff, 1984: 125-151. 17. Deantield JE, Maseri A, Selwyn AP, Ribeiro P, Chierchia S, Krikler S, Morgan M. Myocardial ischaemia during daily life in patients with stable angina: its relation to symptoms and heart rate changes. Lancer 1983;2:753-58. 18. Quyyumi AA, Wright CM, Mockus LJ, Fox KM. How important is a history of cheat pain in determining the degree of ischaemia in patients with angina pectoris? Br Heart J 1985;54:22-26. 19. Campbell S, Barry J, Rocco MB, Nabel EG, Mead-Walters K, Rebecca GS, Selwyn AP. Features of the exercise test that reflect the activity of ischemic heart disease out of hospital. Circulation 1986;74:72-80. 20. Mulcahy D, Keegan J, Sparrow J, Park A, Wright C, Fox K. Ischemia in the ambulatory setting - the total ischemic burden: relation to exercise testing and investigative and therapeutic implications, J Am Co/l Cardiol 1989;14: 1166-l 172. 21. Panra JA, Quyyumi AA, Diodati JG, Callahan TS, Epstein SE. Prediction of the frequency and duration of ambulatory myocardial &hernia in patients with stable coronary artery disease by determination of the ischemic threshold from exercise testing: importance of the exercise protocol, J Am Co11 Cardiol 1991;17:657-663,
MEDICAL TREATMENT OF PAINLESS ISCHEMIA 733