-
Effect of obesity on total and free insulin-likegrowth factor
(IGF)-1, and their relationship toIGF-binding protein (BP)-1,
IGFBP-2, IGFBP-3,insulin, and growth hormone
SY Nam, EJ Lee, KR Kim, BS Cha, YD Song, SK Lim, HC Lee and KB
Huh
Division of Endocrinology, Department of Internal Medicine, Yong
Dong Severance Hospital, Yonsei University, College of
Medicine,Seoul, Korea
OBJECTIVES: We investigated the effect of obesity on the serum
levels of total and free IGF-1 and their relationship tothe
circulating levels of insulin and IGF binding proteins (IGFBPs) in
age and sex-matched groups.SUBJECTS: The study included 43 obese
subjects (ideal body weight; IBW> 120%) and 45 controls (IBW<
100%). All ofthe subjects were male.MEASUREMENT: Total IGF-1, free
IGF-1, IGFBP-1, IGFBP-2, IGFBP-3, and insulin were measured in
obese subjects andnormal control subjects.RESULTS: No signicant
differences in the circulating levels of total and IGFBP-3 were
observed between the obeseand control groups. In contrast to total
IGF-1, free IGF-1 in obese subjects was signicantly increased
compared tonormal controls (P< 0.05). Serum total and free IGF-1
were inversely correlated with age (r0.42, P 0.001, and0.44, P
0.001). Fasting serum insulin concentrations were elevated in all
the obese subjects (P< 0.05) and positivelycorrelated with IBW
(r 0.57, P 0.001). The levels of serum GH and IGFBP-1 were
suppressed in all the obese subjects(P< 0.05). IGFBP-1 was
inversely correlated with IBW (r0.51, P 0.001) and serum insulin
concentrations(r0.48, P 0.001). The IGFBP-2 concentrations were
also suppressed in obese subjects and inversely related tofree
IGF-1 (r0.48, P 0.001). Using multiple linear regression analysis,
total IGF-1 and insulin concentrations werepositively correlated (r
0.58, P 0.001) and free IGF-1 and IGFBP-1 concentrations were
negatively correlated(r0.57, P 0.001).CONCLUSION: We conrmed that
total IGF-1 and IGFBP-3 concentrations were not signicantly
different between theobese and control groups, despite GH
hyposecretion in obesity. We also found that free IGF-1
concentrations werehigher in obese subjects than in normal
controls. It seems likely that overnutrition and chronic
hyperinsulinaemia inobesity may alter this regulated growth
response by insulin stimulation of IGF-1 production and suppression
ofhepatic IGFBP-1 and IGFBP-2 production, which may inhibit IGF-1
bioactivity.
Keywords: obesity; total IGF-1; free IGF-1; IGFBPs
Introduction
Obesity is associated with the impairment of normalGH (growth
hormone) secretion and bluntedresponses to all stimuli such as
GH-releasing hormone(GHRH), hypoglycaemia, L-dopa, arginine,
glucagon,physical exercise, and sleep.14 Based on the wellknown GH
hyposecretion in obesity, GH-dependentinsulin-like growth factor
(IGF)-1 concentrationswould be expected to be subnormal in obesity.
How-ever, the results have been conflicting,57 due toclinical
differences in age, sex and degree and typeof obesity.
Circulating IGF-1 is predominantly bound in a
ternary 150 kDa complex, consisting of IGF-1, IGF-binding
protein (IGFBP)-3, and an acid-labile sub-unit.8,9 Thus IGFBP-3 and
IGF-1 have relatively longhalf-lives in the circulation,10 and
since they are GHdependent they represent a stable index of
long-termchanges in GH availability and action.11 IGFBP-2 isthe
second most abundant IGF-binding protein inserum. The serum
concentration of IGFBP-2 isknown to be inversely related to GH
secretion,being high in states of GH deficiency and low instates of
GH excess.12 These reports have suggestedthat measurement of
IGFBP-2 might be useful indetecting GH deficiency. In contrast, the
serum con-centrations of IGFBP-1 are lower than those ofIGFBP-3 and
IGFBP-2, and acutely regulated byfood intake and fluctuations in
serum insulin andglucose concentrations.1315 Because of this
uniqueproperty, IGFBP-1 is thought to play an important rolein
acute regulation of IGF-1 availability.16,17 In pre-vious reports,
IGFBP-1 sequestered free IGF-1 and
Correspondence: Dr SY Nam, Division of Endocrinology,Department
of Internal Medicine, Yong Dong SeveranceHospital, Young Dong PO
Box 1217, Seoul, Korea.Received 21 August 1996; revised 3 January
1997; accepted 16January 1997
International Journal of Obesity (1997) 21, 355359 1997 Stockton
Press All rights reserved 03070565/97 $12.00
-
inhibited its metabolic actions.18,19 A small portion
ofcirculating IGF-1 is detected in the free or readilydissociable
state, which is thought to be the metabo-lically active form. The
amount of free/dissociableIGF-1 in serum is dependent on a complex
interplaybetween the production rate and concentrations ofIGF-1 and
IGFBPs.10
In this study, we investigated the effect of obesityon the serum
concentrations of total and free IGF-1and their relationship to the
concentrations of IGF-binding proteins and insulin in age and
sex-matchedgroups.
Subjects and methods
Subjects and protocol
Forty-three obese Korean males aged 2049 y (mean - s.e.m., 34.9
7.9) and 45 normal Korean malesubjects aged 2049 y (33.9 8.3) were
studied. Thenormal control subjects were within 10% of their
idealbody weight (IBW), and the obese subjects weighedmore than
120% of ideal body weight, as determinedby the Fogarty Center
Conference on Obesity. Allsubjects were recruited from subjects
attending themedical-checkup programs at the health-care centre
ofYong Dong Severance Hospital.
An oral glucose tolerance test was performed oneach subject to
screen out impaired glucose toleranceor diabetes mellitus. Apart
from obesity, no abnorm-alities were detected. No subjects had used
anyhormonal preparations or drugs within the 60 d priorto the
study.
The study was approved by the Hospital EthicsCommittee, and
informed consent was obtained fromeach subject.
Blood samples were obtained from each subject byvenepuncture
between 08:00 am and 10:00 am after anovernight fast. Serum was
separated by centrifugation,and stored at 20C until analysis.
Analytical methods
Serum glucose level was measured by the glucose-oxidase method
and insulin level by enzyme-linkedimmunoadsorbent assay (ELISA).
This ELISA usestwo monoclonal antibodies (Novo Nordisk A/S,
Den-mark) directed against human insulin and does notcross-react
with human proinsulin. Serum triglycerideand cholesterol
concentrations were determined in theovernight fasting state with
semi-automated methods(Boehringer, Mannheim, Germany). Serum GH
wasmeasured by an immunoradiometric assay (IRMA)from Daiichi
(Tokyo, Japan); the sensitivity was0.1mg/L and its intra and
interassay coefficients ofvariations were 1.3 and 1.4%,
respectively. SerumIGFBP-1, IGFBP-2, and IGFBP-3 were measured byan
immunoradiometric assay (IRMA) kit (DiagnosticSystem Laboratories,
Inc. Webster, TX); the sensitiv-
ities were 0.01 ng/mL, 0.5 ng/mL, 0.5 ng/mL, respec-tively and
their intra and inter-assay coefficients ofvariations were less
than 10%. Serum total IGF-1 wasmeasured by an IRMA kit (Diagnostic
SystemLaboratories, Inc. Webster, TX); the sensitivity was0.3 mg/L
and its intra and interassay coefficients ofvariations were less
than 10%. Free/dissociable IGF-1concentrations were measured by a
highly sensitivetwo-site IRMA kit (Diagnostic System
Laboratories,Inc. Webster, TX) according to the
manufacturerssuggestions. Assay characteristics have been
reportedpreviously.20 This is a direct detection assay in which100
mL of serum sample are added to tubes containinga dense coating of
high affinity anti-IGF-1 antibody,which binds IGF-1 that is not
bound to or is easilydissociable from IGFBPs. Samples were then
incu-bated for two hours at 28C, washed, and incubatedwith an
125I-labeled anti-IGF-1 antibody directed to asecond epitope of
IGF-1 for two hours at roomtemperature. After decanting and washing
3 times,the tubes were counted in a g-counter. Assay standardswere
recombinant human (rh)IGF1 (0.1320mg/L).The minimal detection limit
was 0.05mg/L or 5 pg/tube. According to the manufacturers
specificationsand previous characterization of the assay, there
wasno cross-reactivity with IGF-II, and no residualIGFBP-1 or
IGFBP-3 was detectable in the assaytube after the first wash.20 The
interassay coefficientsof variations were 7.7, 3.6 and 10.7% at
0.26, 5.52 and13.87 ng/mL, and the intraassay coefficients of
varia-tions were 10.3, 5.1, and 3.3% at 0.29, 6.26, and14.20 ng/mL.
All samples from each subject wereanalyzed in duplicate at the same
time.
Statistical analysis
The results were expressed as the mean s.e.m.Statistical
comparisons were made using the Studentsunpaired t-Test between
obese and control groups.Correlation between different parameters
was calcu-lated by linear regression analysis. Factors related
tototal and free IGF-1 were analyzed using stepwisemultiple
regression. P< 0.05 was accepted as thesignificance level.
Results
Percentage of ideal body weight (138.2 11.7%,mean s.e.m.), BMI
(30.0 2.5 kg/m2), and waist tohip ratio (0.93 0.2) in obese
subjects were signifi-cantly (P< 0.001) higher than those of
normal con-trols (97.6 6.4%, 21.3 1.4 kg/m2, and 0.84 0.0).Fasting
serum glucose (FSG), total cholesterol, trigly-ceride, insulin and
GH concentrations are summarizedin Table 1.
The FSG, triglyceride and insulin concentrations inobese
subjects were significantly greater than those ofnormal controls.
In all obese subjects, fasting GH
IGF-1 and IGFBPs in obesitySY Nam et al
356
-
concentrations were suppressed as compared withcontrol subjects
(P< 0.05).
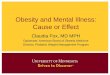
No significant differences in the circulating con-centrations of
the total IGF-1 and IGFBP-3 wereobserved between the control and
obese subjects(Figure 1). Serum total IGF-1 was weakly
correlatedwith IGFBP-3 (r 0.28, P 0.05). The free
IGF-1concentrations were significantly elevated in obesesubjects
(1.46 1.1mg/L vs 0.91 0.9mg/L, P< 0.05;Figure 1). The ratio of
free to total IGF-1 also washigher in obese subjects (0.63% vs
0.39%, P< 0.05;Figure 1).
The IGFBP-1 concentrations were significantlylower in the obese
subjects (Figure 1) and negativelycorrelated with percent of IBW
(r0.51, P 0.001)and serum insulin (r0.48, P 0.001).
The IGFBP-2 concentrations were also suppressedin obese subjects
(P< 0.05; Figure 1) and inverselyrelated to free IGF-1 (r0.48, P
0.001). Addi-tionally, the ratio of IGFBP-2 to IGF-1 was
decreased(1.6 0.5 vs 2.2 1.4, P< 0.005) in obese subjects.
Using multiple linear regression analysis, the totalIGF-1 and
free IGF-1 were analyzed by age, IBW,WHR, fasting serum insulin,
GH, IGFBP-1, IGFBP-2,and IGFBP-3 in all subjects. Of all variables,
age andserum insulin concentrations were associated withserum total
IGF-1. The total IGF-1 was inverselycorrelated with age (r0.42,
P< 0.001) and posi-tively correlated with serum insulin (r
0.58,P< 0.001). The free IGF-1 was negatively correlatedwith age
(r0.44, P< 0.001) and IGFBP-1(r0.57, P< 0.001).
Discussion
Using age and sex matched subjects, we confirmedthat GH levels
were reduced in the obese while GH-dependent total IGF-1 levels
were not significantlydifferent between obese and control subjects.
Similarresults have been reported previously,2123 but
thecontradictory findings of increased or decreasedIGF-1 levels
found by others, although due in partto important clinical
differences in age, sex anddegree of obesity in the different
studies, could beprofoundly influenced by nutritional factors.24,25
Inaddition, the discordant relationship between GH andIGF-1 in
obesity may be also explained by the
hyperinsulinaemia present in obesity:26 insulin mayincrease
hepatic IGF-1 production.27 We found apositive correlation between
the serum total IGF-1and insulin concentrations.
A small portion of circulating IGF-1 is detected inthe free or
readily dissociable state, which is thoughtto be the metabolically
active form.28,29 In the presentstudy, free/dissociable IGF-1 was
assessed by a two-site immunoradiometric assay. The absolute values
forfree/dissociable IGF-1 in both obese and controlgroups were
higher than those reported by Frystyket al30 using RIA after
separation by centrifugalultrafiltration. The difference between
our resultsand theirs are mostly likely due to the ages ofsubjects;
older subjects have lower total and freeIGF-1.30 However, the
ratios of free to total IGF-1in both groups are similar between the
two assaysystems.
The amount of free/dissociable IGF-1 in serum isdependent on a
complex interplay between the pro-duction rate and the
concentrations of IGF-1 andIGFBPs. IGFBP-3 serves as major
stabilizer of thecirculating IGF pool. Circulating IGFBP-3
mightundergo limited proteolysis, which results in smaller
Table 1 Metabolic and hormonal data in control and
obesegroups
Control Obesity
Fasting serum glucose (mmol/L) 5.0 0.5 5.30.6*Total cholesterol
(mg/dL) 185.834.5 191.8 39.1Triglyceride (mg/dL) 114.849.3 176.3
38.1*Insulin (pmol/L) 23.5 12.0 49.2 23.8*GH (ng/mL) 2.0 0.8
0.81.1**P< 0.05 control vs obesity.
Figure 1 Levels of total IGF-1, free IGF-1, ratio of free to
totalIGF-1, IGFBP-1, IGFBP-2, and IGFBP-3 in control (u) and
obesesubjects (j). *P
-
molecular weight IGFBP-3 fragments that have loweraffinity for
IGF-1 than the intact binding protein.Consequently, the levels of
free/dissociable IGF-1are elevated in situations where IGFBP-3
proteolysisis increased.31 Bereket et al32 showed that acute
meal-related hyperinsulinaemia did not increase IGFBP-3proteolysis.
However, it is not known whether IGFBP-3 proteolysis increases in
obese subjects.
In contrast, IGFBP-1 exhibits marked diurnal var-iation in
relation to meals.32 Insulin is the principalregulator of IGFBP-1
and is reported to inhibit hepaticIGFBP-1 synthesis.33 Because of
this property,IGFBP-1 is thought to play an important role in
theregulation of IGF bioactivity. Therefore, the obesity-related
hyperinsulinaemia may decrease circulatingconcentrations of
IGFBP-1, which can result in ele-vated free IGF-1 in obesity. In
our study, circulatingIGFBP-1 concentrations in obese subjects were
lowerthan normal controls. There were also negative corre-lations
between free IGF-1 and IGFBP-1.
IGFBP-2 is the second most abundant IGF-bindingprotein in
serum.34 Several reports have shown thatIGFBP-2 is differentially
regulated by GH and IGF-1.12,34 Administration of GH causes a
reduction inIGFBP-2, while the serum concentration of IGFBP-2is
high in states of GH deficiency.34 In normal adults,the infusion of
IGF-1 results in suppression of GH andan increase in IGFBP-2.38 The
dissociation of theeffect of GH and IGF-1 in regulating IGFBP-2
sug-gests that IGFBP-2 and the ratio of IGFBP-2 to IGF-1may be
useful in detecting GH deficiency. Thus, basedon the well-known GH
hyposecretion in obesity, thelevels of IGFBP-2 and the ratio of
IGFBP-2 to IGF-1would be expected to be high. However, we found
thatIGFBP-2 concentrations and the ratios of IGFBP-2 toIGF-1 were
suppressed in obese subjects. These find-ings indicate that factors
other than GH may beregulating serum IGFBP-2 in obesity. Clemmons
etal34 showed that acute stimulation of insulin did notsuppress
IGFBP-2, but IGFBP-2 concentrations wereelevated after prolonged
fasting. This suggests thatprolonged changes in insulin secretion
may result in asignificant change of IGFBP-2. It appears,
therefore,that the obesity-related chronic hyperinsulinaemiamay
result in suppression of IGFBP-2 in obesity.We also found a
negative correlation betweenIGFBP-2 and free IGF-1 concentrations.
This indi-cates that IGFBP-2 can quantitatively influence
IGF-1transport and may have some role in regulating
IGF-1bioavailability in obesity, because serum IGFBP-2 aremore
abundant than IGFBP-1 in adults.34
Conclusions
We confirmed that GH-dependent IGF-1 andIGFBP-3 concentrations
were not significantly differ-ent between obese and control groups,
despite the GH
hyposecretion in obesity. We also found that free IGF-1
concentrations were increased in obesity comparedto normal
controls. It seems likely that overnutritionand chronic
hyperinsulinaemia in obesity may alterthis regulated growth
response: insulin may stimulateproduction of IGF-1 and suppress
production ofIGFBP-1 and IGFBP-2, which are thought to beinhibitory
IGFBPs.
Acknowledgement
We thank the Ewon Reference Laboratory for themeasurement of
serum IGF-1, IGFBPs, GH and insu-lin. This paper was presented at
the 15th annualmeeting of the Korean Association of
Endocrinologyheld in Seoul 1011th May, 1996.
References1 Barbarino A, De Marinis L, Troncone L. Growth
hormone
response to propranolol and L-dopa in obese subjects.
Meta-bolism 1978; 27: 275278.
2 William T, Berelowitz M, Joffe SN, Thorner MO, Rivier J,Vale
W, Frohman LA. Impaired growth hormone responses togrowth
hormone-releasing factor in obesity. A pituitary defectreversed
with weight reduction. N Engl J Med 1984; 311:14031407.
3 Lee EJ, Kim KR, Lee KM, Lim SK, Lee HC, Lee JH, Lee DJ,Huh KB.
Reduced growth hormone response to L-dopa andpyridostigmine in
obesity. Int J Obes 1984; 18: 465468.
4 Lee EJ, Nam SY, Kim KR, Lee HC, Cho JH, Nam MS, SongYD, Lim
SK, Huh KB. Acipimox potentiates growth hormone(GH) response to
GH-releasing hormone with or withoutpyridostigmine by lowering
serum free fatty acid in normaland obese subjects. J Clin
Endocrinol Metab 1995; 80: 24952498.
5 Rudman D, Kutner MH, Rogers CM, Lubin MF, Fleming GA,Bain RP.
Impaired growth hormone secretion in the popula-tion: Relation to
age and adiposity. J Clin Invest 1981; 67:13611369.
6 Copeland KC, Colletti RB, Devlin JT, McAuliffe TL.
Therelationship between insulin-like growth factor-1, adiposity,and
aging. Metabolism 1990; 39: 584587.
7 Minuto F, Barreca A, Del Monte P, Fortini P, Resentini
M,Morabito F. Spontaneous growth hormone and
somatomedin-C/insulin-like growth factor-1 secretion in obese
subjectsduring puberty. J Endocrinol Invest 1988; 11: 489495.
8 Lamson G, Giudice LC, Rosenfeld RG. Insulin-like growthfactor
binding proteins: structural and molecular relationship.Growth
Factor 1991; 5: 1928.
9 Baxter WF, Martin JL. Characterization of the
acid-labilesubunit of the growth hormone-dependent
insulin-likegrowth factor binding protein complex. J Clin
EndocrinolMetab 1988; 67: 265272.
10 Mohan S, Baylink DJ (Editorial). Insulin-like growth
factor(IGF)-binding proteins in serumDo they have additionalroles
besides modulating the endocrine IGF actions? J ClinEndocrinol
Metab 1996; 81: 38173820.
11 Blum WF, Ranke MB, Kietzmann K, Gauggel E, Zeisel HJ,Bierich
JR. A specific radioimmunoassay for growth hormone(GH)-dependent
somatomedin binding protein: its use fordiagnosis of GH deficiency.
J Clin Endocrinol Metab 1990;70: 12921298.
12 Smith WJ, Nam TJ, Underwood LE, Busby WH, Celnicker
A,Clemmons DR. Use of insulin-like growth factor-bindingprotein-2
(IGFBP-2), IGFBP-3, and IGF-1 for assessinggrowth hormone status in
short children. J Clin EndocrinolMetab 1993; 77: 12941299.
IGF-1 and IGFBPs in obesitySY Nam et al
358
-
13 Suikkari AM, Koivisto VA, Rutanen EM, Yki-Jarvinen H,Karonen
SL, Seppala M. Insulin regulates the serum levels oflow molecular
weight insulin-like growth factor bindingproteins. J Clin
Endocrinol Metab 1988; 66: 266272.
14 Holly JM, Biddlecombe RA, Dunger DB, Edge JA, Amiel SA,Howell
R, Chard T, Rees LH, Wass JA. Circardian variationof GH-independent
IGF-binding protein in diabetes mellitusand its relationship to
insulin. A new role for insulin? ClinEndocrinol (Oxford) 1988; 29:
667675.
15 Busby WH, Snyder DK, Clemmons DR. Radioimmunoassayof a
26,000-dalton plasm an insulin-like growth factor bindingprotein:
control by nutritional factors. J Clin EndocrinolMetab 1988; 67:
12251230.
16 Baxter RC, Cowell CT. Diurnal variation rhythm of
growthhormone independent binding protein for insulin-like
growthfactors in human plasma. J Clin Endocrinol Metab 1987;
65:432440.
17 Conover CA, Lee PD, Kanaley JA, Clarkson JT, Jensen
MD.Insulin regulation of insulin-like growth factor binding
pro-tein-1 in obese and nonobese humans. J Clin EndocrinolMetab
1992; 74: 13551360.
18 Miell JP, Taylor AM, Jones J, Holly JM, Gaillard RC,
PralongFP, Ross RJ, Blum WF. The effect of dexamethasone treat-ment
on immunoreactive and bioactive insulin-like growthfactors (IGFs)
and IGF-binding proteins in normal malevolunteers. J Endocrinol
1993; 136: 525533.
19 Jones JI, Clemmons DR. Insulin-like growth factors and
theirbinding proteins: biological actions. Endocr Rev 1995; 16:
334.
20 Lee PDK, Powell DR, Baker B, Liu F, Belsha CW, BrewerED,
Hintz RL. Characterization of a direct
non-extractionimmunoradiometric assay for free IGF-1 (Abstract
939).Proceedings of the 76th Annual Meeting of the EndocrineSociety
1994.
21 Caufriez A, Golstein J, Lebrun P, Herchuelz A, Fulanetto
R,Copinschi G. Relation between immunoreactive somatome-din-C,
insulin, and T3 patterns during fasting in obese sub-jects. Clin
Endocrinol 1984; 20: 6570.
22 Phillips L, Unterman T. Somatomedin activity in disorder
ofnutrition and metabolism. Clin Endocrinol Metab 1984;
13:145189.
23 Gryzwa M. Serum somatomedin activity and growth-hormonelevel
in obese men: Dependence on degree of obesity andhyperlipidemia.
Exp Clin Endocrinol 1986; 88: 325330.
24 Soliman A, Hassan A, Aref M, Hintz R, Rosenfeld R, RogolA.
Serum IGF-1 and IGF-II concentrations and growth hor-mone and
insulin responses to arginine infusion in children
with protein energy malnutrition before and after
nutritionalrehabilitation. Pediatr Res 1986; 20: 11221130.
25 Clemmons DR, Klibanski A, Underwood LE, McArthur JW,Ridgway
EC, Betins IZ, Van Wyk JJ. Reduction of plasmaimmunoreactive
somatomedin-C during fasting in humans.J Clin Endocrinol Metab
1981; 53: 12471251.
26 DeFronzo RA, Ferrannini E. Insulin resistance. A
multifacetedsyndrome responsible for NIDDM, obesity,
hypertension,dyslipidemia, and athersclerotic cardiovascular
disease. Dia-betes Care 1991; 14: 173194.
27 Froesch ER, Guler HP, Schmid C, Zapf J. Therapeuticpotential
of insulin-like growth factor 1. Trends EndocrinolMetab 1990; 1:
254260.
28 Cascieri MA, Seperatcin R, Hayes NS, Green BG, ChicchiGG,
Applebaum J, Bayne ML. Serum half-life and biologicalactivity of
human insulin-like growth factor I which do notbind to serum
binding proteins. Endocrinology 1988; 123:373381.
29 Lewitt MS. Role of the insulin-like growth factors in
theendocrine control of glucose homeostasis. Diabetes Res ClinPract
1994; 23: 315.
30 Frystyk J, Vestbo E, Skjrbk C, Mogensen CE, rskov H.Free
insulin-like growth factors in human obesity. Metabolism1995; 44:
3744.
31 Binoux M, Lalou C, Lasarre C, Blat C, Hossenlopp P.
Limitedproteolysis of insulin-like growth factor binding
protein-3(IGFBP-3): a physiological mechanism in the regulation
ofIGF bioavailability. Current directions in insulin-like
growthfactor research. Plenum Press: New York. 1994 pp 293300.
32 Bereket A, Wilson TA, Blethen SL, Fan J, Frost RA, GelatoMC,
Lang CH. Effect of short-term fasting on
free/dissociableinsulin-like growth factor 1 concentrations in
normal humanserum. J Clin Endocrinol Metab 1996; 81: 43794384.
33 Brismar K, Fernqvist-Forbes E, Wahren J, Wahren J, Hall
K.Effect of insulin on the hepatic production of insulin-likegrowth
factor binding protein (IGFBP)-I, IGFBP-3 and IGF-Iin insulin
dependent diabetes. J Clin Endocrinol Metab 1994;79: 872878.
34 Clemmons DR, Snyder DK, Busby WH. Variable controllingthe
secretion of insulin-like growth factor binding protein-2 innormal
human subjects. J Clin Endocrinol Metab 1991; 73:727233.
35 Young SCJ, Smith-Banks A, Underwood LE, Clemmons DR.Effects
of recombinant IGF-1 and GH treatment upon serumIGF binding
proteins in calorically restricted adults. J ClinEndocrinol Metab
1992; 75: 603608.
IGF-1 and IGFBPs in obesitySY Nam et al
359