Embed Size (px)
Citation preview
Contents lists available at ScienceDirect
Current Problems in Surgery
Current Problems in Surgery 51 (2014) 301–331
http://d0011-38(http://c
journal homepage: www.elsevier.com/locate/cpsurg
Effect of negative pressure wound therapy onwound healing
Introduction
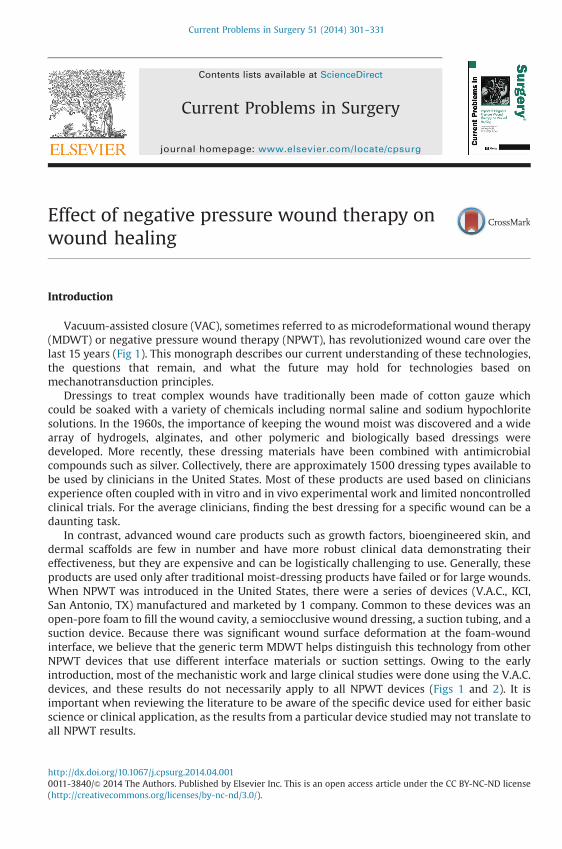
Vacuum-assisted closure (VAC), sometimes referred to as microdeformational wound therapy(MDWT) or negative pressure wound therapy (NPWT), has revolutionized wound care over thelast 15 years (Fig 1). This monograph describes our current understanding of these technologies,the questions that remain, and what the future may hold for technologies based onmechanotransduction principles.
Dressings to treat complex wounds have traditionally been made of cotton gauze whichcould be soaked with a variety of chemicals including normal saline and sodium hypochloritesolutions. In the 1960s, the importance of keeping the wound moist was discovered and a widearray of hydrogels, alginates, and other polymeric and biologically based dressings weredeveloped. More recently, these dressing materials have been combined with antimicrobialcompounds such as silver. Collectively, there are approximately 1500 dressing types available tobe used by clinicians in the United States. Most of these products are used based on cliniciansexperience often coupled with in vitro and in vivo experimental work and limited noncontrolledclinical trials. For the average clinicians, finding the best dressing for a specific wound can be adaunting task.
In contrast, advanced wound care products such as growth factors, bioengineered skin, anddermal scaffolds are few in number and have more robust clinical data demonstrating theireffectiveness, but they are expensive and can be logistically challenging to use. Generally, theseproducts are used only after traditional moist-dressing products have failed or for large wounds.When NPWT was introduced in the United States, there were a series of devices (V.A.C., KCI,San Antonio, TX) manufactured and marketed by 1 company. Common to these devices was anopen-pore foam to fill the wound cavity, a semiocclusive wound dressing, a suction tubing, and asuction device. Because there was significant wound surface deformation at the foam-woundinterface, we believe that the generic term MDWT helps distinguish this technology from otherNPWT devices that use different interface materials or suction settings. Owing to the earlyintroduction, most of the mechanistic work and large clinical studies were done using the V.A.C.devices, and these results do not necessarily apply to all NPWT devices (Figs 1 and 2). It isimportant when reviewing the literature to be aware of the specific device used for either basicscience or clinical application, as the results from a particular device studied may not translate toall NPWT results.
x.doi.org/10.1067/j.cpsurg.2014.04.00140/& 2014 The Authors. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND licensereativecommons.org/licenses/by-nc-nd/3.0/).
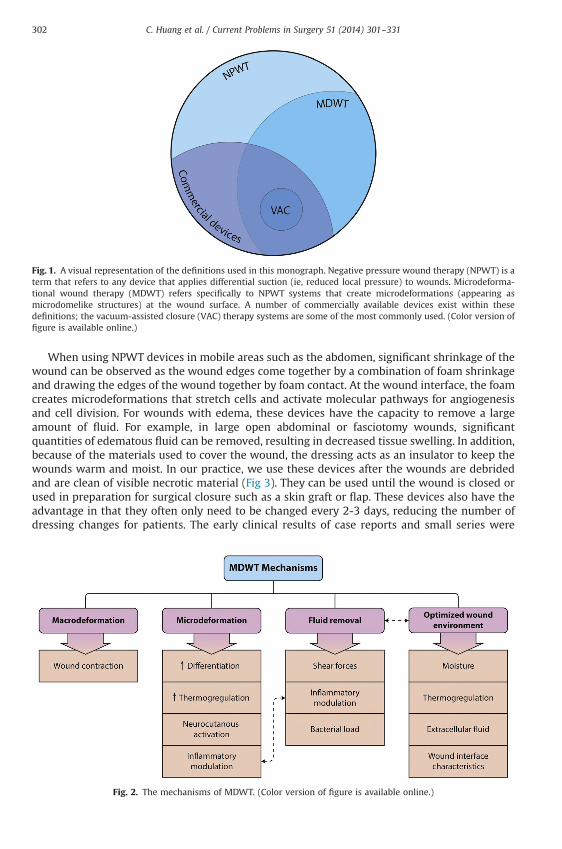
Fig. 1. A visual representation of the definitions used in this monograph. Negative pressure wound therapy (NPWT) is aterm that refers to any device that applies differential suction (ie, reduced local pressure) to wounds. Microdeforma-tional wound therapy (MDWT) refers specifically to NPWT systems that create microdeformations (appearing asmicrodomelike structures) at the wound surface. A number of commercially available devices exist within thesedefinitions; the vacuum-assisted closure (VAC) therapy systems are some of the most commonly used. (Color version offigure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331302
When using NPWT devices in mobile areas such as the abdomen, significant shrinkage of thewound can be observed as the wound edges come together by a combination of foam shrinkageand drawing the edges of the wound together by foam contact. At the wound interface, the foamcreates microdeformations that stretch cells and activate molecular pathways for angiogenesisand cell division. For wounds with edema, these devices have the capacity to remove a largeamount of fluid. For example, in large open abdominal or fasciotomy wounds, significantquantities of edematous fluid can be removed, resulting in decreased tissue swelling. In addition,because of the materials used to cover the wound, the dressing acts as an insulator to keep thewounds warm and moist. In our practice, we use these devices after the wounds are debridedand are clean of visible necrotic material (Fig 3). They can be used until the wound is closed orused in preparation for surgical closure such as a skin graft or flap. These devices also have theadvantage in that they often only need to be changed every 2-3 days, reducing the number ofdressing changes for patients. The early clinical results of case reports and small series were
Fig. 2. The mechanisms of MDWT. (Color version of figure is available online.)
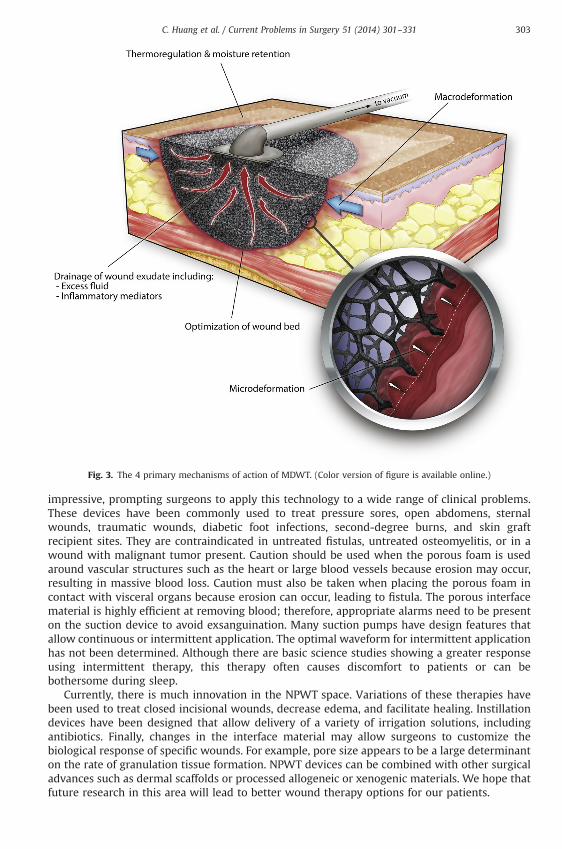
Fig. 3. The 4 primary mechanisms of action of MDWT. (Color version of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 303
impressive, prompting surgeons to apply this technology to a wide range of clinical problems.These devices have been commonly used to treat pressure sores, open abdomens, sternalwounds, traumatic wounds, diabetic foot infections, second-degree burns, and skin graftrecipient sites. They are contraindicated in untreated fistulas, untreated osteomyelitis, or in awound with malignant tumor present. Caution should be used when the porous foam is usedaround vascular structures such as the heart or large blood vessels because erosion may occur,resulting in massive blood loss. Caution must also be taken when placing the porous foam incontact with visceral organs because erosion can occur, leading to fistula. The porous interfacematerial is highly efficient at removing blood; therefore, appropriate alarms need to be presenton the suction device to avoid exsanguination. Many suction pumps have design features thatallow continuous or intermittent application. The optimal waveform for intermittent applicationhas not been determined. Although there are basic science studies showing a greater responseusing intermittent therapy, this therapy often causes discomfort to patients or can bebothersome during sleep.
Currently, there is much innovation in the NPWT space. Variations of these therapies havebeen used to treat closed incisional wounds, decrease edema, and facilitate healing. Instillationdevices have been designed that allow delivery of a variety of irrigation solutions, includingantibiotics. Finally, changes in the interface material may allow surgeons to customize thebiological response of specific wounds. For example, pore size appears to be a large determinanton the rate of granulation tissue formation. NPWT devices can be combined with other surgicaladvances such as dermal scaffolds or processed allogeneic or xenogenic materials. We hope thatfuture research in this area will lead to better wound therapy options for our patients.
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331304
Pressure is defined as force divided by the area to which it is applied. On earth, we live in apressurized atmosphere that allows us to survive. The relationship of pressure and volume canbe approximated using the ideal gas equation: PV ¼ nRT. In this equation, P ¼ pressure, V ¼volume, n ¼ number of moles of gas, R ¼ the universal gas constant, and T ¼ temperature indegrees Kelvin. As such, pressure must always be a positive quantity and “negative pressure” is amisnomer. Gauge pressure, where a pressure is compared with a standard, can be reported as anegative quantity.
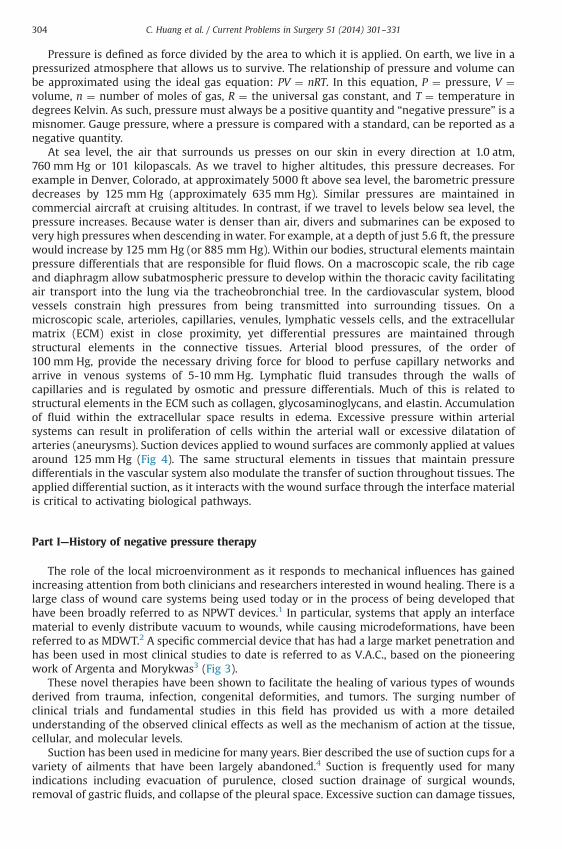
At sea level, the air that surrounds us presses on our skin in every direction at 1.0 atm,760 mm Hg or 101 kilopascals. As we travel to higher altitudes, this pressure decreases. Forexample in Denver, Colorado, at approximately 5000 ft above sea level, the barometric pressuredecreases by 125 mm Hg (approximately 635 mm Hg). Similar pressures are maintained incommercial aircraft at cruising altitudes. In contrast, if we travel to levels below sea level, thepressure increases. Because water is denser than air, divers and submarines can be exposed tovery high pressures when descending inwater. For example, at a depth of just 5.6 ft, the pressurewould increase by 125 mm Hg (or 885 mm Hg). Within our bodies, structural elements maintainpressure differentials that are responsible for fluid flows. On a macroscopic scale, the rib cageand diaphragm allow subatmospheric pressure to develop within the thoracic cavity facilitatingair transport into the lung via the tracheobronchial tree. In the cardiovascular system, bloodvessels constrain high pressures from being transmitted into surrounding tissues. On amicroscopic scale, arterioles, capillaries, venules, lymphatic vessels cells, and the extracellularmatrix (ECM) exist in close proximity, yet differential pressures are maintained throughstructural elements in the connective tissues. Arterial blood pressures, of the order of100 mm Hg, provide the necessary driving force for blood to perfuse capillary networks andarrive in venous systems of 5-10 mm Hg. Lymphatic fluid transudes through the walls ofcapillaries and is regulated by osmotic and pressure differentials. Much of this is related tostructural elements in the ECM such as collagen, glycosaminoglycans, and elastin. Accumulationof fluid within the extracellular space results in edema. Excessive pressure within arterialsystems can result in proliferation of cells within the arterial wall or excessive dilatation ofarteries (aneurysms). Suction devices applied to wound surfaces are commonly applied at valuesaround 125 mm Hg (Fig 4). The same structural elements in tissues that maintain pressuredifferentials in the vascular system also modulate the transfer of suction throughout tissues. Theapplied differential suction, as it interacts with the wound surface through the interface materialis critical to activating biological pathways.
Part I—History of negative pressure therapy
The role of the local microenvironment as it responds to mechanical influences has gainedincreasing attention from both clinicians and researchers interested in wound healing. There is alarge class of wound care systems being used today or in the process of being developed thathave been broadly referred to as NPWT devices.1 In particular, systems that apply an interfacematerial to evenly distribute vacuum to wounds, while causing microdeformations, have beenreferred to as MDWT.2 A specific commercial device that has had a large market penetration andhas been used in most clinical studies to date is referred to as V.A.C., based on the pioneeringwork of Argenta and Morykwas3 (Fig 3).
These novel therapies have been shown to facilitate the healing of various types of woundsderived from trauma, infection, congenital deformities, and tumors. The surging number ofclinical trials and fundamental studies in this field has provided us with a more detailedunderstanding of the observed clinical effects as well as the mechanism of action at the tissue,cellular, and molecular levels.
Suction has been used in medicine for many years. Bier described the use of suction cups for avariety of ailments that have been largely abandoned.4 Suction is frequently used for manyindications including evacuation of purulence, closed suction drainage of surgical wounds,removal of gastric fluids, and collapse of the pleural space. Excessive suction can damage tissues,
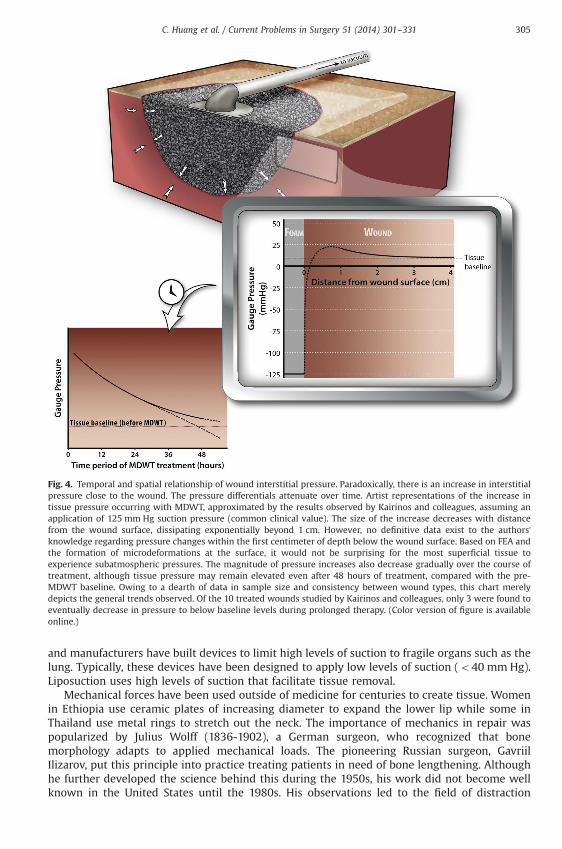
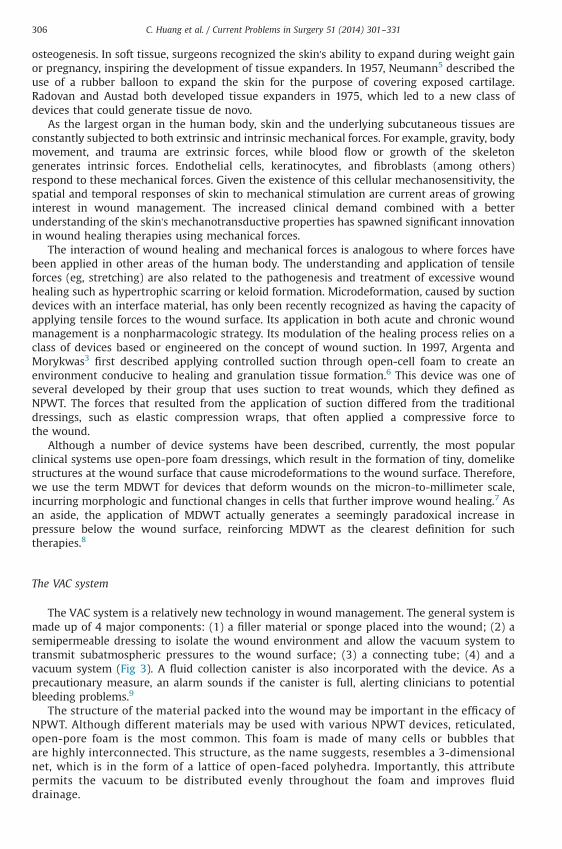
Fig. 4. Temporal and spatial relationship of wound interstitial pressure. Paradoxically, there is an increase in interstitialpressure close to the wound. The pressure differentials attenuate over time. Artist representations of the increase intissue pressure occurring with MDWT, approximated by the results observed by Kairinos and colleagues, assuming anapplication of 125 mm Hg suction pressure (common clinical value). The size of the increase decreases with distancefrom the wound surface, dissipating exponentially beyond 1 cm. However, no definitive data exist to the authors'knowledge regarding pressure changes within the first centimeter of depth below the wound surface. Based on FEA andthe formation of microdeformations at the surface, it would not be surprising for the most superficial tissue toexperience subatmospheric pressures. The magnitude of pressure increases also decrease gradually over the course oftreatment, although tissue pressure may remain elevated even after 48 hours of treatment, compared with the pre-MDWT baseline. Owing to a dearth of data in sample size and consistency between wound types, this chart merelydepicts the general trends observed. Of the 10 treated wounds studied by Kairinos and colleagues, only 3 were found toeventually decrease in pressure to below baseline levels during prolonged therapy. (Color version of figure is availableonline.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 305
and manufacturers have built devices to limit high levels of suction to fragile organs such as thelung. Typically, these devices have been designed to apply low levels of suction (o40 mm Hg).Liposuction uses high levels of suction that facilitate tissue removal.
Mechanical forces have been used outside of medicine for centuries to create tissue. Womenin Ethiopia use ceramic plates of increasing diameter to expand the lower lip while some inThailand use metal rings to stretch out the neck. The importance of mechanics in repair waspopularized by Julius Wolff (1836-1902), a German surgeon, who recognized that bonemorphology adapts to applied mechanical loads. The pioneering Russian surgeon, GavriilIlizarov, put this principle into practice treating patients in need of bone lengthening. Althoughhe further developed the science behind this during the 1950s, his work did not become wellknown in the United States until the 1980s. His observations led to the field of distraction
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331306
osteogenesis. In soft tissue, surgeons recognized the skin's ability to expand during weight gainor pregnancy, inspiring the development of tissue expanders. In 1957, Neumann5 described theuse of a rubber balloon to expand the skin for the purpose of covering exposed cartilage.Radovan and Austad both developed tissue expanders in 1975, which led to a new class ofdevices that could generate tissue de novo.
As the largest organ in the human body, skin and the underlying subcutaneous tissues areconstantly subjected to both extrinsic and intrinsic mechanical forces. For example, gravity, bodymovement, and trauma are extrinsic forces, while blood flow or growth of the skeletongenerates intrinsic forces. Endothelial cells, keratinocytes, and fibroblasts (among others)respond to these mechanical forces. Given the existence of this cellular mechanosensitivity, thespatial and temporal responses of skin to mechanical stimulation are current areas of growinginterest in wound management. The increased clinical demand combined with a betterunderstanding of the skin's mechanotransductive properties has spawned significant innovationin wound healing therapies using mechanical forces.
The interaction of wound healing and mechanical forces is analogous to where forces havebeen applied in other areas of the human body. The understanding and application of tensileforces (eg, stretching) are also related to the pathogenesis and treatment of excessive woundhealing such as hypertrophic scarring or keloid formation. Microdeformation, caused by suctiondevices with an interface material, has only been recently recognized as having the capacity ofapplying tensile forces to the wound surface. Its application in both acute and chronic woundmanagement is a nonpharmacologic strategy. Its modulation of the healing process relies on aclass of devices based or engineered on the concept of wound suction. In 1997, Argenta andMorykwas3 first described applying controlled suction through open-cell foam to create anenvironment conducive to healing and granulation tissue formation.6 This device was one ofseveral developed by their group that uses suction to treat wounds, which they defined asNPWT. The forces that resulted from the application of suction differed from the traditionaldressings, such as elastic compression wraps, that often applied a compressive force tothe wound.
Although a number of device systems have been described, currently, the most popularclinical systems use open-pore foam dressings, which result in the formation of tiny, domelikestructures at the wound surface that cause microdeformations to the wound surface. Therefore,we use the term MDWT for devices that deform wounds on the micron-to-millimeter scale,incurring morphologic and functional changes in cells that further improve wound healing.7 Asan aside, the application of MDWT actually generates a seemingly paradoxical increase inpressure below the wound surface, reinforcing MDWT as the clearest definition for suchtherapies.8
The VAC system
The VAC system is a relatively new technology in wound management. The general system ismade up of 4 major components: (1) a filler material or sponge placed into the wound; (2) asemipermeable dressing to isolate the wound environment and allow the vacuum system totransmit subatmospheric pressures to the wound surface; (3) a connecting tube; (4) and avacuum system (Fig 3). A fluid collection canister is also incorporated with the device. As aprecautionary measure, an alarm sounds if the canister is full, alerting clinicians to potentialbleeding problems.9
The structure of the material packed into the wound may be important in the efficacy ofNPWT. Although different materials may be used with various NPWT devices, reticulated,open-pore foam is the most common. This foam is made of many cells or bubbles thatare highly interconnected. This structure, as the name suggests, resembles a 3-dimensionalnet, which is in the form of a lattice of open-faced polyhedra. Importantly, this attributepermits the vacuum to be distributed evenly throughout the foam and improves fluiddrainage.
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 307
As part of the commercial VAC system, 3 general types of foam are available: blackpolyurethane ether (V.A.C. GranuFoam, KCI), black polyurethane ester (V.A.C. VeraFlow, KCI), andwhite polyvinyl alcohol (V.A.C. WhiteFoam, KCI). Other types of foams are available in othercommercial devices and other types of interface materials continue to be developed. Thetraditional polyurethane ether foam is hydrophobic, whereas the polyvinyl alcohol andpolyurethane ester foams are more hydrophilic. The polyurethane ester devices are designedfor use with instillation therapy. Clinicians have often used the traditional polyurethane etherfoams for wounds with large fluid drainage and for stimulating granulation tissue formation. Incontrast, the polyvinyl alcohol sponges have been used in cases where the wound tunnels orwhen delicate underlying structures, such as tendons or blood vessels, need to be protected.Finally, the increased density and smaller pores of the WhiteFoam help to restrict ingrowth ofgranulation tissue, thereby diminishing pain associated with dressing changes and reducing riskwhen hypergranulation is a concern.10,11
NPWT therapy is most commonly applied to an openwound, accelerating the healing processand bringing the wound margins closer together. Other uses, methods of application, anddifferent patient conditions have been discussed at greater length in the section Clinicalapplications of NPWT, following an explanation of the mechanisms of action. Overall, thehealing of both acute and chronic wounds is improved through the combination of componentsthat include the wound-foam interface, semiocclusive microenvironment, and the mechanicalforces incorporated into NPWT.
Part II—Mechanisms of action
The events underlying the improvement in wound healing observed with MDWT can bebroadly classified as primary mechanisms and their associated secondary effects. Overall, 4primary mechanisms of action have been proposed: (1) wound shrinkage or macrodeformation;(2) microdeformation at the foam-wound surface interface; (3) fluid removal; and (4) stabiliza-tion of the wound environment (Figs 2 and 3).12 There are also several secondary effects likelyinvolved in mechanotransduction pathways that alter the biology of wound healing includingangiogenesis, neurogenesis, granulation tissue formation, cellular proliferation, differentiation,and migration.
Primary mechanisms
MacrodeformationMacrodeformation refers to induced wound shrinkage caused by collapse of the pores and
centripetal forces exerted onto the wound surface by the foam. Polyurethane ether foamsexposed to 125 mm Hg suction can decrease the foam volume by approximately 80%13 and resultin a substantial decrease in wound surface area in a porcine model.14 The extent of contraction islargely dependent on the deformability of the wound. The baseline tension in skin causes woundmargins to naturally pull apart. Because of the inherent tension of the dermis and variableattachment to underlying structures, different wounds contract to different degrees. Forexample, the low elasticity of scalp skin over the rigid calvarium is likely to contract less than alarge abdominal wound in an obese patient.
Interestingly, in both in vivo and in vitro studies, a seemingly paradoxical increase inextracellular pressure is observed in the tissue underlying the wound bed, presumably due totissue compression induced by macrodeformation.8,15 Such a phenomenon may seem moreobvious with circumferential NPWT dressings, for example, in treating large degloving injuriesencompassing a limb. As suction is applied, air is evacuated from the foam and its reduction involume results in the compression of underlying tissue. Increased tissue pressure is also observedwhen NPWT is applied to more cavitary wounds, where the top of the foam is virtually at levelwith the surrounding skin. Logically, one might assume that negative gauge pressures wouldtranslate to lower pressure in adjacent tissues. However, pressure in the underlying tissue
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331308
increases with elevated suction. These extracellular pressure changes also vary with distance fromthe foam-wound interface and the time of treatment (Fig 4).8 Taking these findings intoconsideration can reduce the risks of NPWT in patients with compromised perfusion, potentiallycontraindicating this treatment, especially if circumferential dressings or higher suction pressuresare to be used. Overall, the effects of macrodeformation depend on the type of tissue treated,12 thelevel of suction,14 the volume of the foam,16 the pore volume fraction of the filler material(proportion of sponge occupied by air),17 and the deformability of the surrounding tissues.12
MicrodeformationMicrodeformation refers to the undulated wound surface induced by the porous interface
material when exposed to suction. These physical changes occur on the micron-to-millimeterscale, given common pore diameters are in the range of 400-600 μm, and set in motion a host ofother effects that aid in the healing process. To better understand the micromechanical changesinvolved, models have been designed to mimic tissue stretched by a combination of suction anda counteracting downward force by the sponge struts. In computer simulations of this interfacewith finite element analysis (FEA), our model indicates that at 110 mm Hg, MDWT applicationusing typical foam pore sizes causes an average tissue strain of 5%-20% over most of the woundsurface. Quantitatively, tissue strain corresponds to the percentage increase or decrease inlength of a given material subjected to external forces.18
These mechanical forces appear to be transmitted to individual cells via the ECM. In MDWT,cells are subjected to a variety of mechanical forces, including shear and hydrostatic pressurefrom extracellular fluid, stretch and compression from their surrounding matrix, and theubiquitous pull of gravity.12 These mechanical forces, particularly microstrain, are also highlyvariable across the wound surface (albeit in a repeating pattern between sponge pores). FEA hasdemonstrated that tissue immediately below the foam struts experiences compression, whereastension is found along the wound surface centrally in the pore.18 Overall, the regular yet highlyvariable microenvironment created during this therapy is what causes microdeformation.Microdeformation, in essence, is the morphologic result of these integrated mechanics. Cellshape has been demonstrated to be a determinant of cellular function.19 In addition, cells areknown to adapt to physical stresses.20 Therefore, changes in cellular functions can be initiated bythese dynamic physical inputs. This concept has been discussed in greater detail in thesecondary effects of NPWT action.
Fluid removalFluids in the body have been classically divided among 3 compartments: (1) intravascular,
(2) intracellular, and (3) extracellular. Fluid transport between these compartments is primarilygoverned by the Starling equation, which takes into account the hydrostatic and osmoticpressure differentials across semipermeable membranes. The most variable of these compart-ments is the extracellular space. Excess fluid in this compartment is commonly seen as edema,whereas a lack of fluid in this compartment is a sign of dehydration. The extracellular fluidcompartment is drained by lymphatics, the disruption of which can lead to lymphedema.
Depending on the underlying pathology, chronic wounds and edema are often concomitant,as is the case with lower extremity diabetic ulcers. Excess fluid buildup is commonly accepted asa contravening factor in healing, partly owing to the compressive effect it can exert on local cellsand tissues. Individual cells generate intrinsic tension via their cytoskeleton and interactionswith the ECM, inducing a proliferative response.12 Elevated fluid pressures in the interstitiumdiminish this response by dampening intrinsic tension buildup. Fluids from the extracellularspace appear to communicate with the wound surface. Applying vacuum to this surface resultsin fluid removal from many wounds, including the extracellular space. In our experience,particularly in fasciotomy wounds or in open abdominal wounds, large amounts of fluid can beremoved.21 Fluid removal likely reduces compression of the microvasculature, optimizing tissueperfusion by reducing difference and potentially allowing increased blood flow to the area(Fig 5).3,22 The polyurethane drape is semipermeable, allowing a small amount of air to enter the
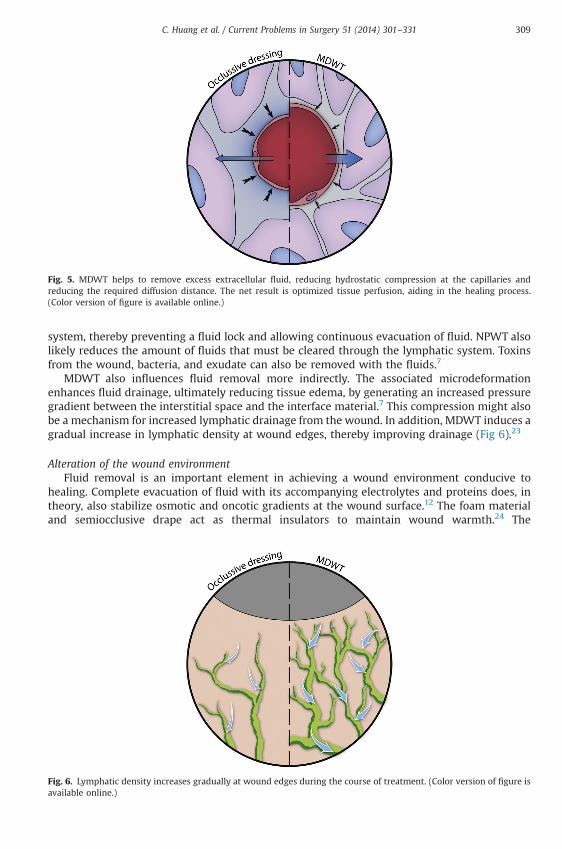
Fig. 5. MDWT helps to remove excess extracellular fluid, reducing hydrostatic compression at the capillaries andreducing the required diffusion distance. The net result is optimized tissue perfusion, aiding in the healing process.(Color version of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 309
system, thereby preventing a fluid lock and allowing continuous evacuation of fluid. NPWT alsolikely reduces the amount of fluids that must be cleared through the lymphatic system. Toxinsfrom the wound, bacteria, and exudate can also be removed with the fluids.7
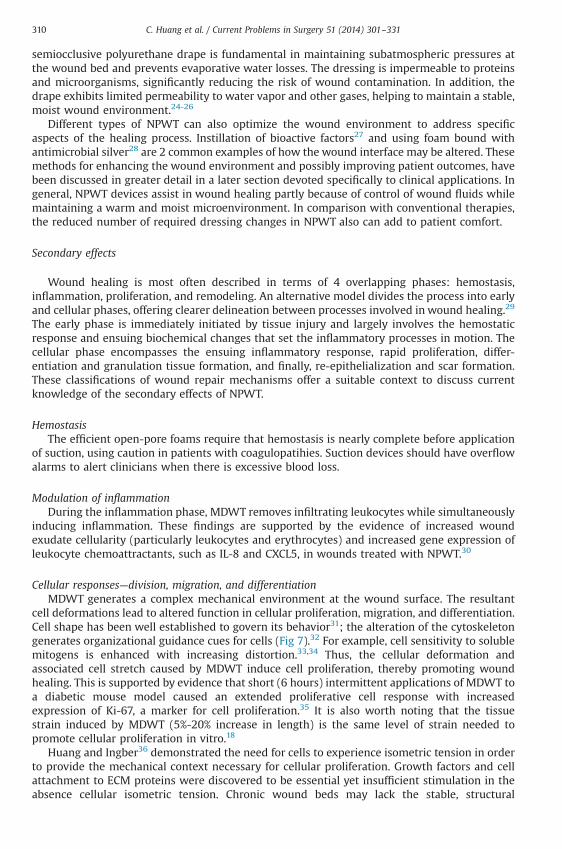
MDWT also influences fluid removal more indirectly. The associated microdeformationenhances fluid drainage, ultimately reducing tissue edema, by generating an increased pressuregradient between the interstitial space and the interface material.7 This compression might alsobe a mechanism for increased lymphatic drainage from the wound. In addition, MDWT induces agradual increase in lymphatic density at wound edges, thereby improving drainage (Fig 6).23
Alteration of the wound environmentFluid removal is an important element in achieving a wound environment conducive to
healing. Complete evacuation of fluid with its accompanying electrolytes and proteins does, intheory, also stabilize osmotic and oncotic gradients at the wound surface.12 The foam materialand semiocclusive drape act as thermal insulators to maintain wound warmth.24 The
Fig. 6. Lymphatic density increases gradually at wound edges during the course of treatment. (Color version of figure isavailable online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331310
semiocclusive polyurethane drape is fundamental in maintaining subatmospheric pressures atthe wound bed and prevents evaporative water losses. The dressing is impermeable to proteinsand microorganisms, significantly reducing the risk of wound contamination. In addition, thedrape exhibits limited permeability to water vapor and other gases, helping to maintain a stable,moist wound environment.24-26
Different types of NPWT can also optimize the wound environment to address specificaspects of the healing process. Instillation of bioactive factors27 and using foam bound withantimicrobial silver28 are 2 common examples of how the wound interface may be altered. Thesemethods for enhancing the wound environment and possibly improving patient outcomes, havebeen discussed in greater detail in a later section devoted specifically to clinical applications. Ingeneral, NPWT devices assist in wound healing partly because of control of wound fluids whilemaintaining a warm and moist microenvironment. In comparison with conventional therapies,the reduced number of required dressing changes in NPWT also can add to patient comfort.
Secondary effects
Wound healing is most often described in terms of 4 overlapping phases: hemostasis,inflammation, proliferation, and remodeling. An alternative model divides the process into earlyand cellular phases, offering clearer delineation between processes involved in wound healing.29
The early phase is immediately initiated by tissue injury and largely involves the hemostaticresponse and ensuing biochemical changes that set the inflammatory processes in motion. Thecellular phase encompasses the ensuing inflammatory response, rapid proliferation, differ-entiation and granulation tissue formation, and finally, re-epithelialization and scar formation.These classifications of wound repair mechanisms offer a suitable context to discuss currentknowledge of the secondary effects of NPWT.
HemostasisThe efficient open-pore foams require that hemostasis is nearly complete before application
of suction, using caution in patients with coagulopatihies. Suction devices should have overflowalarms to alert clinicians when there is excessive blood loss.
Modulation of inflammationDuring the inflammation phase, MDWT removes infiltrating leukocytes while simultaneously
inducing inflammation. These findings are supported by the evidence of increased woundexudate cellularity (particularly leukocytes and erythrocytes) and increased gene expression ofleukocyte chemoattractants, such as IL-8 and CXCL5, in wounds treated with NPWT.30
Cellular responses—division, migration, and differentiationMDWT generates a complex mechanical environment at the wound surface. The resultant
cell deformations lead to altered function in cellular proliferation, migration, and differentiation.Cell shape has been well established to govern its behavior31; the alteration of the cytoskeletongenerates organizational guidance cues for cells (Fig 7).32 For example, cell sensitivity to solublemitogens is enhanced with increasing distortion.33,34 Thus, the cellular deformation andassociated cell stretch caused by MDWT induce cell proliferation, thereby promoting woundhealing. This is supported by evidence that short (6 hours) intermittent applications of MDWT toa diabetic mouse model caused an extended proliferative cell response with increasedexpression of Ki-67, a marker for cell proliferation.35 It is also worth noting that the tissuestrain induced by MDWT (5%-20% increase in length) is the same level of strain needed topromote cellular proliferation in vitro.18
Huang and Ingber36 demonstrated the need for cells to experience isometric tension in orderto provide the mechanical context necessary for cellular proliferation. Growth factors and cellattachment to ECM proteins were discovered to be essential yet insufficient stimulation in theabsence cellular isometric tension. Chronic wound beds may lack the stable, structural
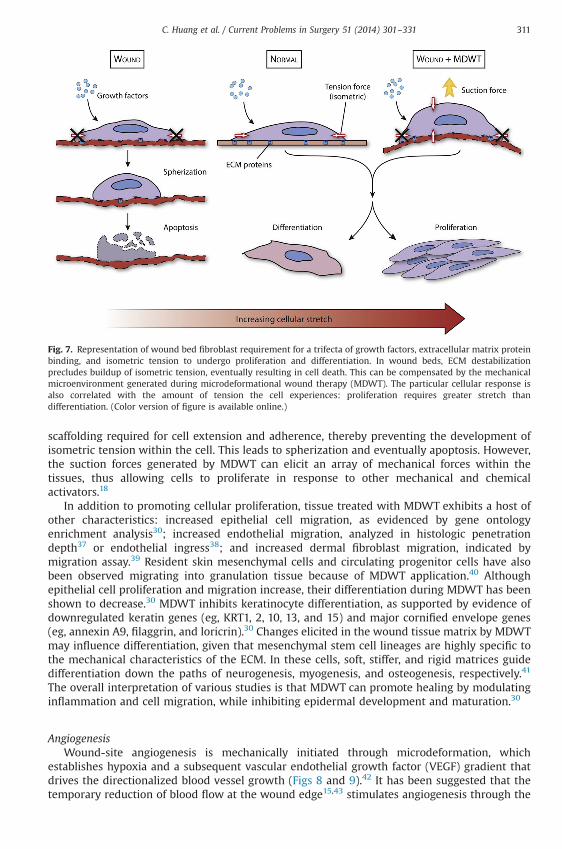
Fig. 7. Representation of wound bed fibroblast requirement for a trifecta of growth factors, extracellular matrix proteinbinding, and isometric tension to undergo proliferation and differentiation. In wound beds, ECM destabilizationprecludes buildup of isometric tension, eventually resulting in cell death. This can be compensated by the mechanicalmicroenvironment generated during microdeformational wound therapy (MDWT). The particular cellular response isalso correlated with the amount of tension the cell experiences: proliferation requires greater stretch thandifferentiation. (Color version of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 311
scaffolding required for cell extension and adherence, thereby preventing the development ofisometric tension within the cell. This leads to spherization and eventually apoptosis. However,the suction forces generated by MDWT can elicit an array of mechanical forces within thetissues, thus allowing cells to proliferate in response to other mechanical and chemicalactivators.18
In addition to promoting cellular proliferation, tissue treated with MDWT exhibits a host ofother characteristics: increased epithelial cell migration, as evidenced by gene ontologyenrichment analysis30; increased endothelial migration, analyzed in histologic penetrationdepth37 or endothelial ingress38; and increased dermal fibroblast migration, indicated bymigration assay.39 Resident skin mesenchymal cells and circulating progenitor cells have alsobeen observed migrating into granulation tissue because of MDWT application.40 Althoughepithelial cell proliferation and migration increase, their differentiation during MDWT has beenshown to decrease.30 MDWT inhibits keratinocyte differentiation, as supported by evidence ofdownregulated keratin genes (eg, KRT1, 2, 10, 13, and 15) and major cornified envelope genes(eg, annexin A9, filaggrin, and loricrin).30 Changes elicited in the wound tissue matrix by MDWTmay influence differentiation, given that mesenchymal stem cell lineages are highly specific tothe mechanical characteristics of the ECM. In these cells, soft, stiffer, and rigid matrices guidedifferentiation down the paths of neurogenesis, myogenesis, and osteogenesis, respectively.41
The overall interpretation of various studies is that MDWT can promote healing by modulatinginflammation and cell migration, while inhibiting epidermal development and maturation.30
AngiogenesisWound-site angiogenesis is mechanically initiated through microdeformation, which
establishes hypoxia and a subsequent vascular endothelial growth factor (VEGF) gradient thatdrives the directionalized blood vessel growth (Figs 8 and 9).42 It has been suggested that thetemporary reduction of blood flow at the wound edge15,43 stimulates angiogenesis through the
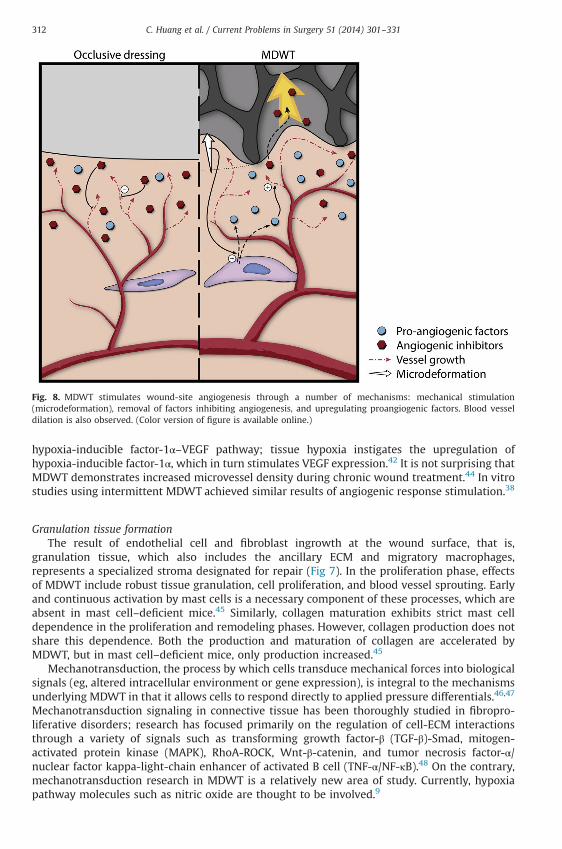
Fig. 8. MDWT stimulates wound-site angiogenesis through a number of mechanisms: mechanical stimulation(microdeformation), removal of factors inhibiting angiogenesis, and upregulating proangiogenic factors. Blood vesseldilation is also observed. (Color version of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331312
hypoxia-inducible factor-1α–VEGF pathway; tissue hypoxia instigates the upregulation ofhypoxia-inducible factor-1α, which in turn stimulates VEGF expression.42 It is not surprising thatMDWT demonstrates increased microvessel density during chronic wound treatment.44 In vitrostudies using intermittent MDWT achieved similar results of angiogenic response stimulation.38
Granulation tissue formationThe result of endothelial cell and fibroblast ingrowth at the wound surface, that is,
granulation tissue, which also includes the ancillary ECM and migratory macrophages,represents a specialized stroma designated for repair (Fig 7). In the proliferation phase, effectsof MDWT include robust tissue granulation, cell proliferation, and blood vessel sprouting. Earlyand continuous activation by mast cells is a necessary component of these processes, which areabsent in mast cell–deficient mice.45 Similarly, collagen maturation exhibits strict mast celldependence in the proliferation and remodeling phases. However, collagen production does notshare this dependence. Both the production and maturation of collagen are accelerated byMDWT, but in mast cell–deficient mice, only production increased.45
Mechanotransduction, the process by which cells transduce mechanical forces into biologicalsignals (eg, altered intracellular environment or gene expression), is integral to the mechanismsunderlying MDWT in that it allows cells to respond directly to applied pressure differentials.46,47
Mechanotransduction signaling in connective tissue has been thoroughly studied in fibropro-liferative disorders; research has focused primarily on the regulation of cell-ECM interactionsthrough a variety of signals such as transforming growth factor-β (TGF-β)-Smad, mitogen-activated protein kinase (MAPK), RhoA-ROCK, Wnt-β-catenin, and tumor necrosis factor-α/nuclear factor kappa-light-chain enhancer of activated B cell (TNF-α/NF-κB).48 On the contrary,mechanotransduction research in MDWT is a relatively new area of study. Currently, hypoxiapathway molecules such as nitric oxide are thought to be involved.9
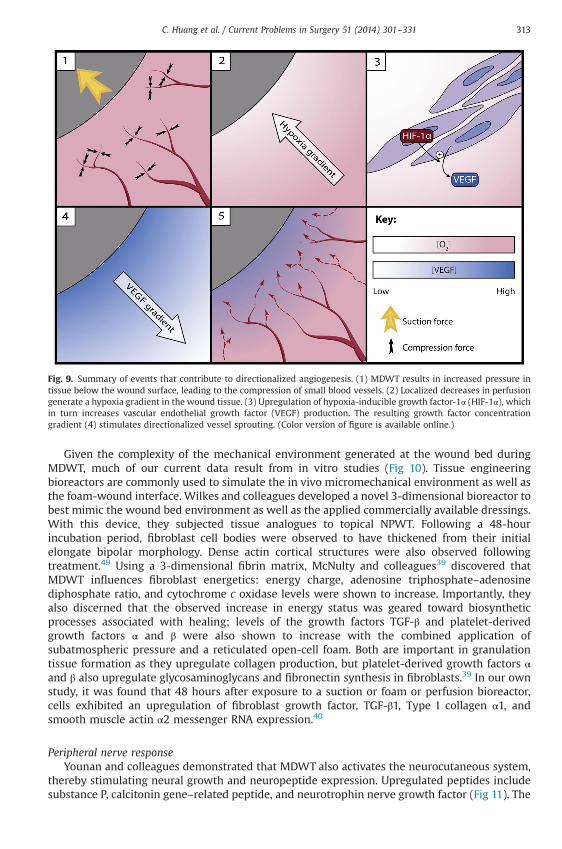
Fig. 9. Summary of events that contribute to directionalized angiogenesis. (1) MDWT results in increased pressure intissue below the wound surface, leading to the compression of small blood vessels. (2) Localized decreases in perfusiongenerate a hypoxia gradient in the wound tissue. (3) Upregulation of hypoxia-inducible growth factor-1α (HIF-1α), whichin turn increases vascular endothelial growth factor (VEGF) production. The resulting growth factor concentrationgradient (4) stimulates directionalized vessel sprouting. (Color version of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 313
Given the complexity of the mechanical environment generated at the wound bed duringMDWT, much of our current data result from in vitro studies (Fig 10). Tissue engineeringbioreactors are commonly used to simulate the in vivo micromechanical environment as well asthe foam-wound interface. Wilkes and colleagues developed a novel 3-dimensional bioreactor tobest mimic the wound bed environment as well as the applied commercially available dressings.With this device, they subjected tissue analogues to topical NPWT. Following a 48-hourincubation period, fibroblast cell bodies were observed to have thickened from their initialelongate bipolar morphology. Dense actin cortical structures were also observed followingtreatment.49 Using a 3-dimensional fibrin matrix, McNulty and colleagues39 discovered thatMDWT influences fibroblast energetics: energy charge, adenosine triphosphate–adenosinediphosphate ratio, and cytochrome c oxidase levels were shown to increase. Importantly, theyalso discerned that the observed increase in energy status was geared toward biosyntheticprocesses associated with healing; levels of the growth factors TGF-β and platelet-derivedgrowth factors α and β were also shown to increase with the combined application ofsubatmospheric pressure and a reticulated open-cell foam. Both are important in granulationtissue formation as they upregulate collagen production, but platelet-derived growth factors αand β also upregulate glycosaminoglycans and fibronectin synthesis in fibroblasts.39 In our ownstudy, it was found that 48 hours after exposure to a suction or foam or perfusion bioreactor,cells exhibited an upregulation of fibroblast growth factor, TGF-β1, Type I collagen α1, andsmooth muscle actin α2 messenger RNA expression.40
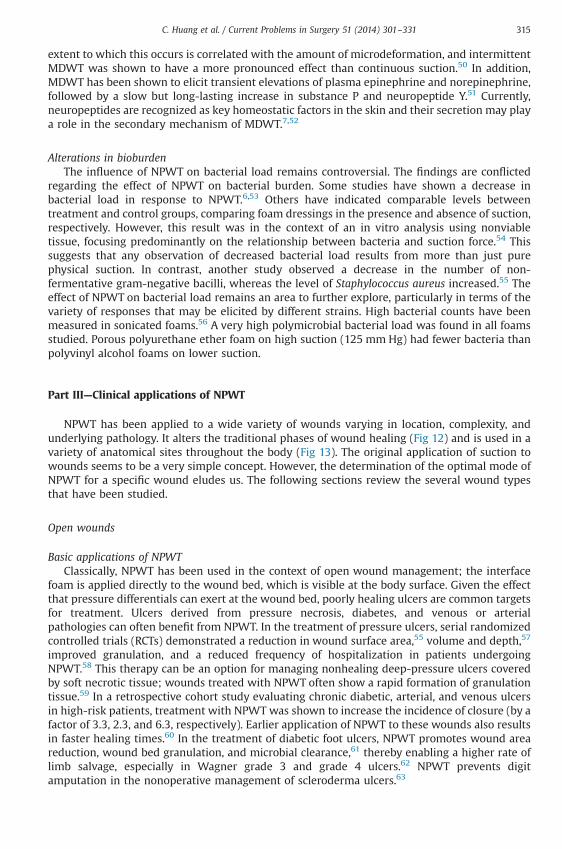
Peripheral nerve responseYounan and colleagues demonstrated that MDWT also activates the neurocutaneous system,
thereby stimulating neural growth and neuropeptide expression. Upregulated peptides includesubstance P, calcitonin gene–related peptide, and neurotrophin nerve growth factor (Fig 11). The
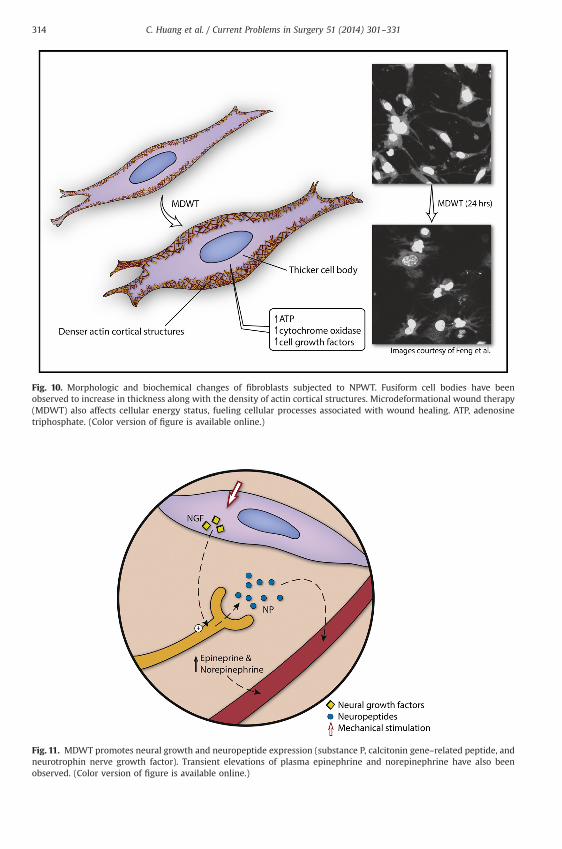
Fig. 11. MDWT promotes neural growth and neuropeptide expression (substance P, calcitonin gene–related peptide, andneurotrophin nerve growth factor). Transient elevations of plasma epinephrine and norepinephrine have also beenobserved. (Color version of figure is available online.)
Fig. 10. Morphologic and biochemical changes of fibroblasts subjected to NPWT. Fusiform cell bodies have beenobserved to increase in thickness along with the density of actin cortical structures. Microdeformational wound therapy(MDWT) also affects cellular energy status, fueling cellular processes associated with wound healing. ATP, adenosinetriphosphate. (Color version of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331314
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 315
extent to which this occurs is correlated with the amount of microdeformation, and intermittentMDWT was shown to have a more pronounced effect than continuous suction.50 In addition,MDWT has been shown to elicit transient elevations of plasma epinephrine and norepinephrine,followed by a slow but long-lasting increase in substance P and neuropeptide Y.51 Currently,neuropeptides are recognized as key homeostatic factors in the skin and their secretion may playa role in the secondary mechanism of MDWT.7,52
Alterations in bioburdenThe influence of NPWT on bacterial load remains controversial. The findings are conflicted
regarding the effect of NPWT on bacterial burden. Some studies have shown a decrease inbacterial load in response to NPWT.6,53 Others have indicated comparable levels betweentreatment and control groups, comparing foam dressings in the presence and absence of suction,respectively. However, this result was in the context of an in vitro analysis using nonviabletissue, focusing predominantly on the relationship between bacteria and suction force.54 Thissuggests that any observation of decreased bacterial load results from more than just purephysical suction. In contrast, another study observed a decrease in the number of non-fermentative gram-negative bacilli, whereas the level of Staphylococcus aureus increased.55 Theeffect of NPWT on bacterial load remains an area to further explore, particularly in terms of thevariety of responses that may be elicited by different strains. High bacterial counts have beenmeasured in sonicated foams.56 A very high polymicrobial bacterial load was found in all foamsstudied. Porous polyurethane ether foam on high suction (125 mm Hg) had fewer bacteria thanpolyvinyl alcohol foams on lower suction.
Part III—Clinical applications of NPWT
NPWT has been applied to a wide variety of wounds varying in location, complexity, andunderlying pathology. It alters the traditional phases of wound healing (Fig 12) and is used in avariety of anatomical sites throughout the body (Fig 13). The original application of suction towounds seems to be a very simple concept. However, the determination of the optimal mode ofNPWT for a specific wound eludes us. The following sections review the several wound typesthat have been studied.
Open wounds
Basic applications of NPWTClassically, NPWT has been used in the context of open wound management; the interface
foam is applied directly to the wound bed, which is visible at the body surface. Given the effectthat pressure differentials can exert at the wound bed, poorly healing ulcers are common targetsfor treatment. Ulcers derived from pressure necrosis, diabetes, and venous or arterialpathologies can often benefit from NPWT. In the treatment of pressure ulcers, serial randomizedcontrolled trials (RCTs) demonstrated a reduction in wound surface area,55 volume and depth,57
improved granulation, and a reduced frequency of hospitalization in patients undergoingNPWT.58 This therapy can be an option for managing nonhealing deep-pressure ulcers coveredby soft necrotic tissue; wounds treated with NPWT often show a rapid formation of granulationtissue.59 In a retrospective cohort study evaluating chronic diabetic, arterial, and venous ulcersin high-risk patients, treatment with NPWT was shown to increase the incidence of closure (by afactor of 3.3, 2.3, and 6.3, respectively). Earlier application of NPWT to these wounds also resultsin faster healing times.60 In the treatment of diabetic foot ulcers, NPWT promotes wound areareduction, wound bed granulation, and microbial clearance,61 thereby enabling a higher rate oflimb salvage, especially in Wagner grade 3 and grade 4 ulcers.62 NPWT prevents digitamputation in the nonoperative management of scleroderma ulcers.63
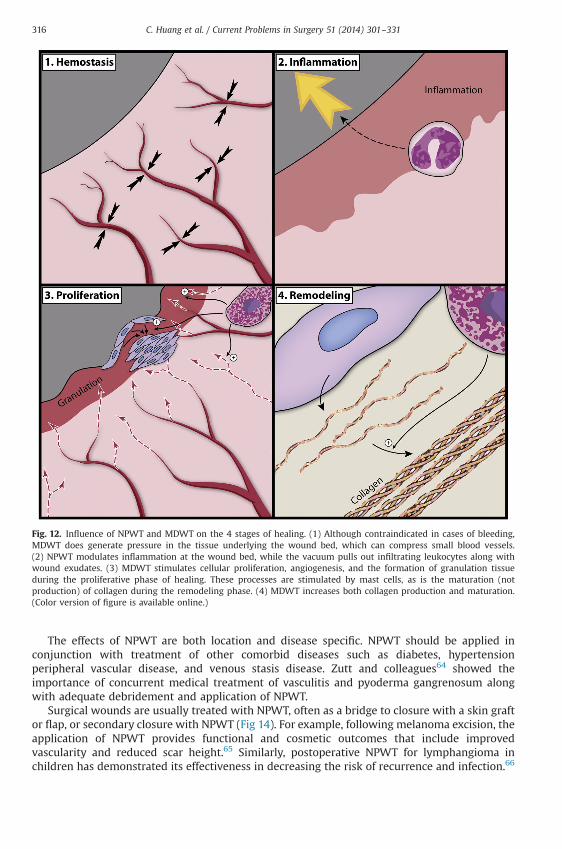
Fig. 12. Influence of NPWT and MDWT on the 4 stages of healing. (1) Although contraindicated in cases of bleeding,MDWT does generate pressure in the tissue underlying the wound bed, which can compress small blood vessels.(2) NPWT modulates inflammation at the wound bed, while the vacuum pulls out infiltrating leukocytes along withwound exudates. (3) MDWT stimulates cellular proliferation, angiogenesis, and the formation of granulation tissueduring the proliferative phase of healing. These processes are stimulated by mast cells, as is the maturation (notproduction) of collagen during the remodeling phase. (4) MDWT increases both collagen production and maturation.(Color version of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331316
The effects of NPWT are both location and disease specific. NPWT should be applied inconjunction with treatment of other comorbid diseases such as diabetes, hypertensionperipheral vascular disease, and venous stasis disease. Zutt and colleagues64 showed theimportance of concurrent medical treatment of vasculitis and pyoderma gangrenosum alongwith adequate debridement and application of NPWT.
Surgical wounds are usually treated with NPWT, often as a bridge to closure with a skin graftor flap, or secondary closure with NPWT (Fig 14). For example, following melanoma excision, theapplication of NPWT provides functional and cosmetic outcomes that include improvedvascularity and reduced scar height.65 Similarly, postoperative NPWT for lymphangioma inchildren has demonstrated its effectiveness in decreasing the risk of recurrence and infection.66
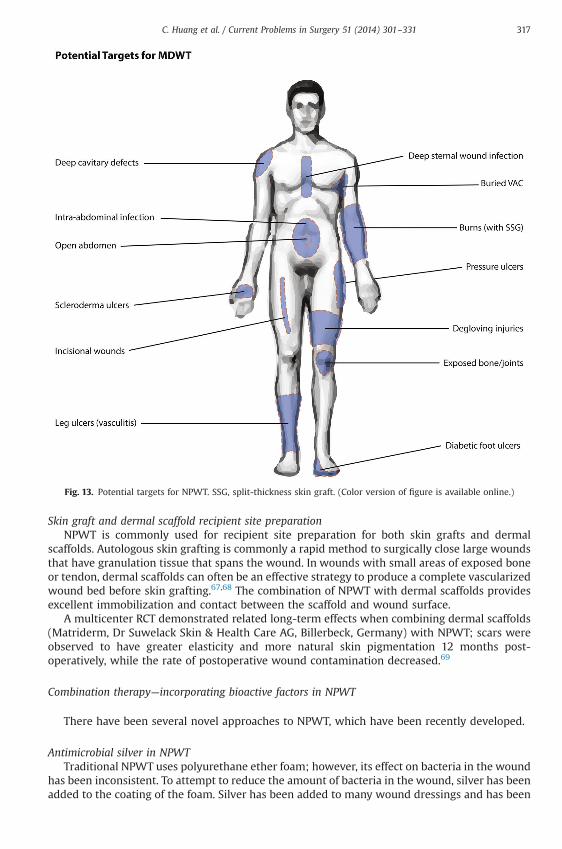
Fig. 13. Potential targets for NPWT. SSG, split-thickness skin graft. (Color version of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 317
Skin graft and dermal scaffold recipient site preparationNPWT is commonly used for recipient site preparation for both skin grafts and dermal
scaffolds. Autologous skin grafting is commonly a rapid method to surgically close large woundsthat have granulation tissue that spans the wound. In wounds with small areas of exposed boneor tendon, dermal scaffolds can often be an effective strategy to produce a complete vascularizedwound bed before skin grafting.67,68 The combination of NPWT with dermal scaffolds providesexcellent immobilization and contact between the scaffold and wound surface.
A multicenter RCT demonstrated related long-term effects when combining dermal scaffolds(Matriderm, Dr Suwelack Skin & Health Care AG, Billerbeck, Germany) with NPWT; scars wereobserved to have greater elasticity and more natural skin pigmentation 12 months post-operatively, while the rate of postoperative wound contamination decreased.69
Combination therapy—incorporating bioactive factors in NPWT
There have been several novel approaches to NPWT, which have been recently developed.
Antimicrobial silver in NPWTTraditional NPWT uses polyurethane ether foam; however, its effect on bacteria in the wound
has been inconsistent. To attempt to reduce the amount of bacteria in the wound, silver has beenadded to the coating of the foam. Silver has been added to many wound dressings and has been
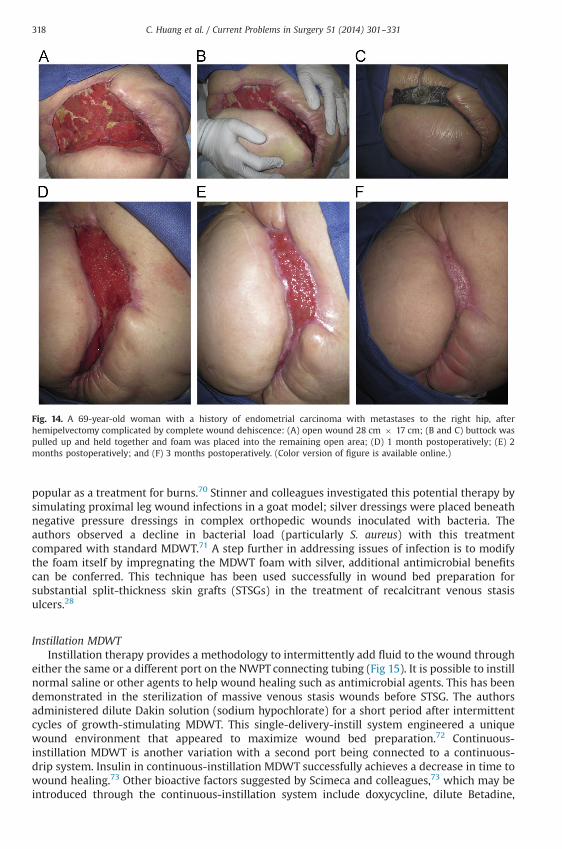
Fig. 14. A 69-year-old woman with a history of endometrial carcinoma with metastases to the right hip, afterhemipelvectomy complicated by complete wound dehiscence: (A) open wound 28 cm � 17 cm; (B and C) buttock waspulled up and held together and foam was placed into the remaining open area; (D) 1 month postoperatively; (E) 2months postoperatively; and (F) 3 months postoperatively. (Color version of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331318
popular as a treatment for burns.70 Stinner and colleagues investigated this potential therapy bysimulating proximal leg wound infections in a goat model; silver dressings were placed beneathnegative pressure dressings in complex orthopedic wounds inoculated with bacteria. Theauthors observed a decline in bacterial load (particularly S. aureus) with this treatmentcompared with standard MDWT.71 A step further in addressing issues of infection is to modifythe foam itself by impregnating the MDWT foam with silver, additional antimicrobial benefitscan be conferred. This technique has been used successfully in wound bed preparation forsubstantial split-thickness skin grafts (STSGs) in the treatment of recalcitrant venous stasisulcers.28
Instillation MDWTInstillation therapy provides a methodology to intermittently add fluid to the wound through
either the same or a different port on the NWPT connecting tubing (Fig 15). It is possible to instillnormal saline or other agents to help wound healing such as antimicrobial agents. This has beendemonstrated in the sterilization of massive venous stasis wounds before STSG. The authorsadministered dilute Dakin solution (sodium hypochlorate) for a short period after intermittentcycles of growth-stimulating MDWT. This single-delivery-instill system engineered a uniquewound environment that appeared to maximize wound bed preparation.72 Continuous-instillation MDWT is another variation with a second port being connected to a continuous-drip system. Insulin in continuous-instillation MDWT successfully achieves a decrease in time towound healing.73 Other bioactive factors suggested by Scimeca and colleagues,73 which may beintroduced through the continuous-instillation system include doxycycline, dilute Betadine,
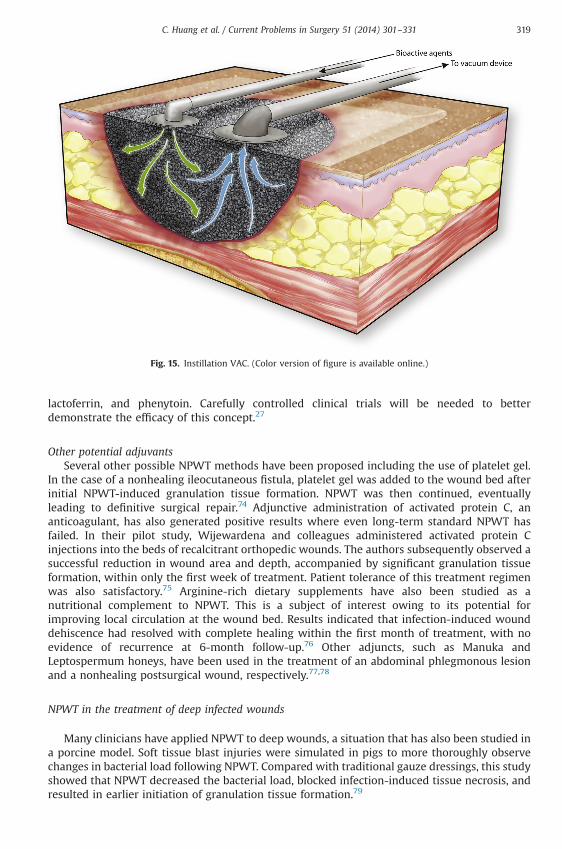
Fig. 15. Instillation VAC. (Color version of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 319
lactoferrin, and phenytoin. Carefully controlled clinical trials will be needed to betterdemonstrate the efficacy of this concept.27
Other potential adjuvantsSeveral other possible NPWT methods have been proposed including the use of platelet gel.
In the case of a nonhealing ileocutaneous fistula, platelet gel was added to the wound bed afterinitial NPWT-induced granulation tissue formation. NPWT was then continued, eventuallyleading to definitive surgical repair.74 Adjunctive administration of activated protein C, ananticoagulant, has also generated positive results where even long-term standard NPWT hasfailed. In their pilot study, Wijewardena and colleagues administered activated protein Cinjections into the beds of recalcitrant orthopedic wounds. The authors subsequently observed asuccessful reduction in wound area and depth, accompanied by significant granulation tissueformation, within only the first week of treatment. Patient tolerance of this treatment regimenwas also satisfactory.75 Arginine-rich dietary supplements have also been studied as anutritional complement to NPWT. This is a subject of interest owing to its potential forimproving local circulation at the wound bed. Results indicated that infection-induced wounddehiscence had resolved with complete healing within the first month of treatment, with noevidence of recurrence at 6-month follow-up.76 Other adjuncts, such as Manuka andLeptospermum honeys, have been used in the treatment of an abdominal phlegmonous lesionand a nonhealing postsurgical wound, respectively.77,78
NPWT in the treatment of deep infected wounds
Many clinicians have applied NPWT to deep wounds, a situation that has also been studied ina porcine model. Soft tissue blast injuries were simulated in pigs to more thoroughly observechanges in bacterial load following NPWT. Compared with traditional gauze dressings, this studyshowed that NPWT decreased the bacterial load, blocked infection-induced tissue necrosis, andresulted in earlier initiation of granulation tissue formation.79
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331320
In humans, NPWT has generally been shown to be effective in the control of woundinfections. This is particularly true of thoracic and abdominal injuries, and deep wounds, whereinfection management is paramount in treatment. Although often useful, dressings infused withsilver are not always indicated80 or even necessary with NPWT. NPWT systems are able to isolatewounds from the external environment with a drainage system that may be superior to standardsurgical drains.
NPWT in cases of exposed bone or joints or bothRecently, open fractures, particularly of the lower extremity, are frequently being treated
with NPWT systems. These systems keep the wound clean from external contamination andkeep it moist and warm. In their retrospective cohort study of open tibial fractures, Blum andcolleagues compared the rate of deep infection between NPWT and conventional dressingtreatment groups (8.4% and 20.6%, respectively). There was nearly 80% reduction in the risk ofdeep tissue infection after adjustment for multivariate analysis.81 Similarly, in a patient with leftknee-joint exposure, the large soft tissue defect was managed by a 20-day course of NPWT.Despite the original severe wound infection (following open reduction and internal fixation of apatellar fracture), a granulated wound bed fully covering the exposed bones and joint wasobserved after negative pressure treatment.82
NPWT systems are sometimes used as an alternative treatment for lower-extremity woundswith exposed bones or joints or both when free-flap transfer is contraindicated.82,83 NPWT canhelp to reduce both the need for flap transfer and the size of the flap, as demonstrated in typeIIIB open tibial fracture treatment. However, it is worth noting that the authors discouraged theapplication of negative pressure for a period lasting longer than 7 days owing to the significantlyhigher rate of infection and the associated risk of amputation.84
Deep sternal wound infectionDeep sternal wound infection (DSWI), also known as mediastinitis, is a devastating
complication of open heart surgery posing severe risks to patients postoperatively. Withoutprompt treatment, the mortality rate from this condition can exceed 50%. Traditional packing ofsternal wounds often resulted in massive bleeding or chronic draining sinus tracts. In a studycohort of patients with DSWIs, NPWT reduced the risk of early reinfections when used as thefirst line of therapy. The data were also suggestive of a decrease in the incidence of late chronicsternal infections and mortality.85 Furthermore, meta-analysis assessing the effect of NPWT onsternal infections found the length of hospital stay to decrease by 1 week.86 In the case ofmethicillin-resistant postcardiotomy DSWIs, MDWT shortened healing time and hospital stayand lowered the recurrence of infection relative to closed mediastinal irrigation withantibiotics.87
Similar to DSWI, poststernotomy osteomyelitis remains a huge concern for patient morbidity,prolonging recovery time, and necessitating surgical reinterventions.88 NPWT does notsubstitute for adequate debridement and antibiotic therapy when osteomyelitis is present.89,90
NPWT as an augmented surgical drainDeep wound infections can often be associated with the buildup of fluid, either in natural
anatomical cavities or in pathologic abscesses. NPWT offers an improved modality for drainingthese infections, partly by providing a greater suction distribution over a larger surface area thanconventional drainage methods. This was shown to help prevent the accumulation of purulentmaterial in the case of a deep neck abscess involving the mediastinum, thereby avoiding theneed for open thoracotomy.91 Similarly, for postoperative or recurrent pleural empyema, NPWTused in conjunctionwith openwindow thoracostomy can help control sepsis, rapidly eradicatingthe local infection in most cases. In addition, NPWT therapy has also been used in complex chestwall wounds that facilitated improved lung expansion and eliminated empyema recurrence.92
Deep cavitary defects, particularly those derived from high-velocity projectiles or blastinjuries, have also appeared to have benefitted from NPWT. These wounds are unique in that the
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 321
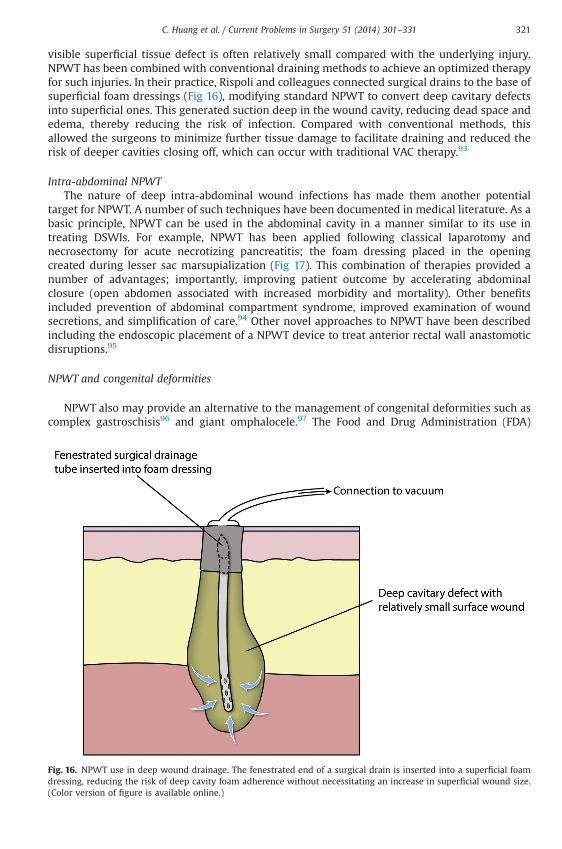
visible superficial tissue defect is often relatively small compared with the underlying injury.NPWT has been combined with conventional draining methods to achieve an optimized therapyfor such injuries. In their practice, Rispoli and colleagues connected surgical drains to the base ofsuperficial foam dressings (Fig 16), modifying standard NPWT to convert deep cavitary defectsinto superficial ones. This generated suction deep in the wound cavity, reducing dead space andedema, thereby reducing the risk of infection. Compared with conventional methods, thisallowed the surgeons to minimize further tissue damage to facilitate draining and reduced therisk of deeper cavities closing off, which can occur with traditional VAC therapy.93
Intra-abdominal NPWTThe nature of deep intra-abdominal wound infections has made them another potential
target for NPWT. A number of such techniques have been documented in medical literature. As abasic principle, NPWT can be used in the abdominal cavity in a manner similar to its use intreating DSWIs. For example, NPWT has been applied following classical laparotomy andnecrosectomy for acute necrotizing pancreatitis; the foam dressing placed in the openingcreated during lesser sac marsupialization (Fig 17). This combination of therapies provided anumber of advantages; importantly, improving patient outcome by accelerating abdominalclosure (open abdomen associated with increased morbidity and mortality). Other benefitsincluded prevention of abdominal compartment syndrome, improved examination of woundsecretions, and simplification of care.94 Other novel approaches to NPWT have been describedincluding the endoscopic placement of a NPWT device to treat anterior rectal wall anastomoticdisruptions.95
NPWT and congenital deformities
NPWT also may provide an alternative to the management of congenital deformities such ascomplex gastroschisis96 and giant omphalocele.97 The Food and Drug Administration (FDA)
Fig. 16. NPWT use in deep wound drainage. The fenestrated end of a surgical drain is inserted into a superficial foamdressing, reducing the risk of deep cavity foam adherence without necessitating an increase in superficial wound size.(Color version of figure is available online.)
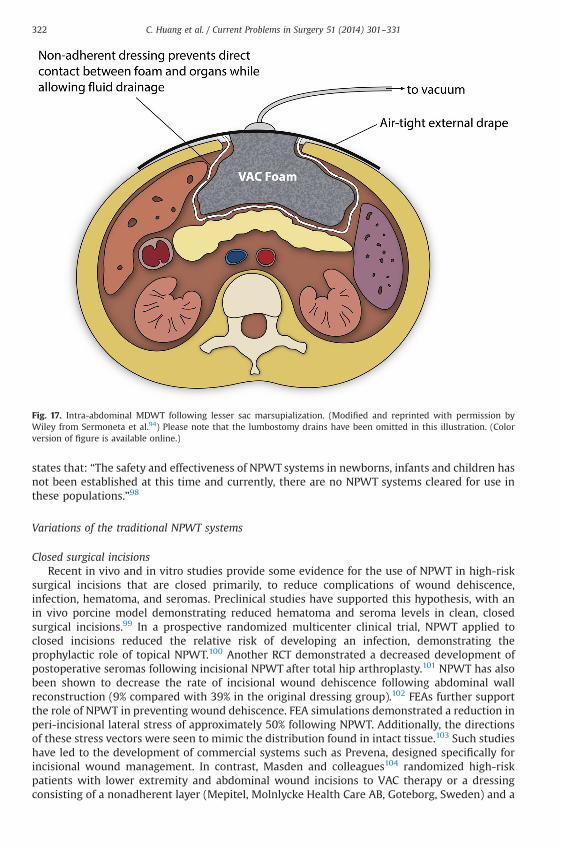
Fig. 17. Intra-abdominal MDWT following lesser sac marsupialization. (Modified and reprinted with permission byWiley from Sermoneta et al.94) Please note that the lumbostomy drains have been omitted in this illustration. (Colorversion of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331322
states that: “The safety and effectiveness of NPWT systems in newborns, infants and children hasnot been established at this time and currently, there are no NPWT systems cleared for use inthese populations.”98
Variations of the traditional NPWT systems
Closed surgical incisionsRecent in vivo and in vitro studies provide some evidence for the use of NPWT in high-risk
surgical incisions that are closed primarily, to reduce complications of wound dehiscence,infection, hematoma, and seromas. Preclinical studies have supported this hypothesis, with anin vivo porcine model demonstrating reduced hematoma and seroma levels in clean, closedsurgical incisions.99 In a prospective randomized multicenter clinical trial, NPWT applied toclosed incisions reduced the relative risk of developing an infection, demonstrating theprophylactic role of topical NPWT.100 Another RCT demonstrated a decreased development ofpostoperative seromas following incisional NPWT after total hip arthroplasty.101 NPWT has alsobeen shown to decrease the rate of incisional wound dehiscence following abdominal wallreconstruction (9% compared with 39% in the original dressing group).102 FEAs further supportthe role of NPWT in preventing wound dehiscence. FEA simulations demonstrated a reduction inperi-incisional lateral stress of approximately 50% following NPWT. Additionally, the directionsof these stress vectors were seen to mimic the distribution found in intact tissue.103 Such studieshave led to the development of commercial systems such as Prevena, designed specifically forincisional wound management. In contrast, Masden and colleagues104 randomized high-riskpatients with lower extremity and abdominal wound incisions to VAC therapy or a dressingconsisting of a nonadherent layer (Mepitel, Molnlycke Health Care AB, Goteborg, Sweden) and a
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 323
silver dressing (Acticoat, Smith & Nephew, Hull, United Kingdom) and found no statisticallysignificant difference in the rates of infection and dehiscence between the 2 groups.
Skin graft immobilizationThe take of STSGs is governed by many factors including the vascularity of the wound surface,
immobilization of the skin graft, and avoidance of infection seroma or hematoma.105 Historically,tie-over bolsters immobilize the graft by applying gentle pressure and are left in place for severaldays. NPWT has been used by several groups instead of a bolster.106,107 The suction applied tothe interface materials stabilizes the graft and eliminates excess fluids.106,107 NPWT improvesthe contact zone for graft integration, aiding in the processes of plasmatic imbibition andvascularization.105 Several prospective randomized clinical trials have shown the effectiveness ofusing NPWT systems for skin graft immobilization.105-108
For congested lower extremity pedicle flaps and free flaps without anastomotic thrombosis,NPWT can improve and resolve tissue edema and venous insufficiency, prevent further flapnecrosis, and promote granulation, thereby avoiding the risk of further surgical re-explorations.109 In random local flaps prone to ischemia and distal necrosis for complex anklewounds, NPWT contributes to their viability by decreasing venous congestion.110 In aretrospective study, NPWT was thought to reduce healing complications of large back donorsites used for free flaps for head and neck reconstruction.111
Degloving injuries involve the shearing of skin and subcutaneous tissue from the underlyingfascia and muscle, including the avulsion of musculocutaneous and fasciocutaneous perfo-rators.112 If left alone, the degloved skin will predictably die. After excising the degloved skin andremoving the fat from the dermis, the skin can then be reapplied to the wound as a full-thickness skin graft. A NPWT device can then be placed on the graft for immobilization.112,113
Combining NPWT with a dermal regeneration template is an additional option and has shownboth excellent functional and esthetic results in treating a subtotal degloving injury of the rightlower limb. In a case study, Dini and colleagues applied NPWT directly to the wound bed for thefirst 10 days, providing temporary wound closure and early granulation tissue development. Adermal regeneration template was then applied directly to the wound bed and covered with aNPWT device. Following an additional 21 days of NPWT with Integra, the cryopreserveddegloved flap was successfully grafted to the wound site with a NPWT device used to immobilizethe graft.114
Part IV—Clinical considerations
A wide array of wound types has been reportedly treated with NPWT. The FDA has approvedNPWT for managing poorly healing wounds. Manufacturer guidelines for the widely usedKCI V.A.C. therapy systems list chronic, acute, traumatic, subacute, and dehisced wounds, partial-thickness burns, ulcers (such as diabetic, pressure, or venous insufficiency), flaps and grafts asindications for use.115
Contraindications
Because inappropriate use of NPWT devices has the potential for patient harm, the clinicianshould carefully weigh the risks, benefits, and alternatives of using NPWT. According to the FDAand KCI guidelines, NPWT is contraindicated in conditions involving (1) necrotic tissue witheschar present, (2) untreated osteomyelitis, (3) nonenteric and unexplored fistulas, (4) malig-nancy in the wound, (5) exposed vasculature, (6) exposed nerves, (7) exposed anastomotic site,and (8) exposed organs.98 In some cases, clinicians have used NPWT despite the establishedcontraindications. For example, some studies have successfully implemented VAC therapy incases of exposed organs,94 exposed anastomotic sites (Fig 18),116 and osteomyelitis.89 The use ofpolyurethane foam under vacuum forces can have detrimental effects when in direct contact
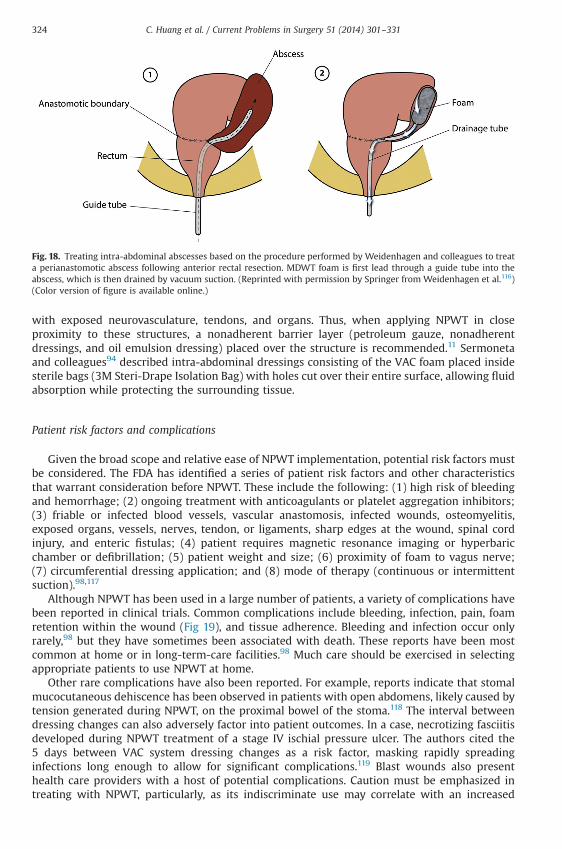
Fig. 18. Treating intra-abdominal abscesses based on the procedure performed by Weidenhagen and colleagues to treata perianastomotic abscess following anterior rectal resection. MDWT foam is first lead through a guide tube into theabscess, which is then drained by vacuum suction. (Reprinted with permission by Springer from Weidenhagen et al.116)(Color version of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331324
with exposed neurovasculature, tendons, and organs. Thus, when applying NPWT in closeproximity to these structures, a nonadherent barrier layer (petroleum gauze, nonadherentdressings, and oil emulsion dressing) placed over the structure is recommended.11 Sermonetaand colleagues94 described intra-abdominal dressings consisting of the VAC foam placed insidesterile bags (3M Steri-Drape Isolation Bag) with holes cut over their entire surface, allowing fluidabsorption while protecting the surrounding tissue.
Patient risk factors and complications
Given the broad scope and relative ease of NPWT implementation, potential risk factors mustbe considered. The FDA has identified a series of patient risk factors and other characteristicsthat warrant consideration before NPWT. These include the following: (1) high risk of bleedingand hemorrhage; (2) ongoing treatment with anticoagulants or platelet aggregation inhibitors;(3) friable or infected blood vessels, vascular anastomosis, infected wounds, osteomyelitis,exposed organs, vessels, nerves, tendon, or ligaments, sharp edges at the wound, spinal cordinjury, and enteric fistulas; (4) patient requires magnetic resonance imaging or hyperbaricchamber or defibrillation; (5) patient weight and size; (6) proximity of foam to vagus nerve;(7) circumferential dressing application; and (8) mode of therapy (continuous or intermittentsuction).98,117
Although NPWT has been used in a large number of patients, a variety of complications havebeen reported in clinical trials. Common complications include bleeding, infection, pain, foamretention within the wound (Fig 19), and tissue adherence. Bleeding and infection occur onlyrarely,98 but they have sometimes been associated with death. These reports have been mostcommon at home or in long-term-care facilities.98 Much care should be exercised in selectingappropriate patients to use NPWT at home.
Other rare complications have also been reported. For example, reports indicate that stomalmucocutaneous dehiscence has been observed in patients with open abdomens, likely caused bytension generated during NPWT, on the proximal bowel of the stoma.118 The interval betweendressing changes can also adversely factor into patient outcomes. In a case, necrotizing fasciitisdeveloped during NPWT treatment of a stage IV ischial pressure ulcer. The authors cited the5 days between VAC system dressing changes as a risk factor, masking rapidly spreadinginfections long enough to allow for significant complications.119 Blast wounds also presenthealth care providers with a host of potential complications. Caution must be emphasized intreating with NPWT, particularly, as its indiscriminate use may correlate with an increased
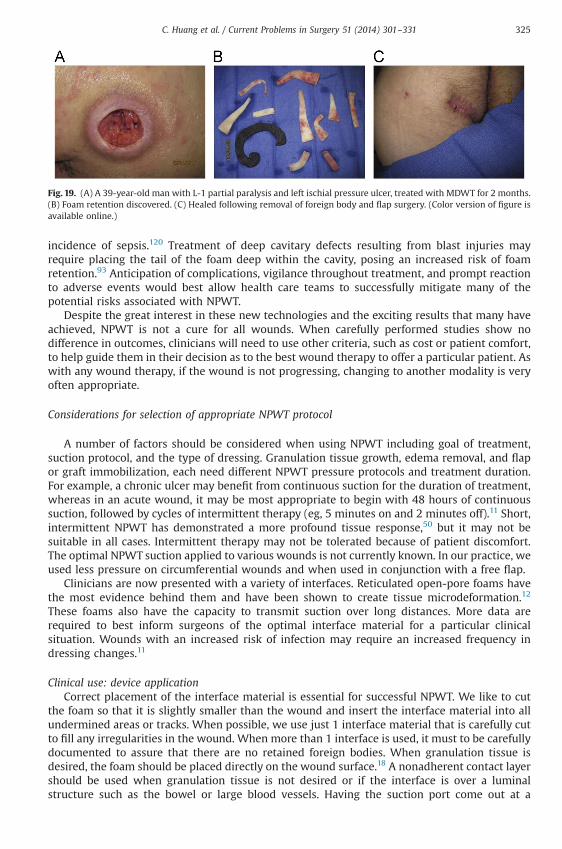
Fig. 19. (A) A 39-year-old man with L-1 partial paralysis and left ischial pressure ulcer, treated with MDWT for 2 months.(B) Foam retention discovered. (C) Healed following removal of foreign body and flap surgery. (Color version of figure isavailable online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 325
incidence of sepsis.120 Treatment of deep cavitary defects resulting from blast injuries mayrequire placing the tail of the foam deep within the cavity, posing an increased risk of foamretention.93 Anticipation of complications, vigilance throughout treatment, and prompt reactionto adverse events would best allow health care teams to successfully mitigate many of thepotential risks associated with NPWT.
Despite the great interest in these new technologies and the exciting results that many haveachieved, NPWT is not a cure for all wounds. When carefully performed studies show nodifference in outcomes, clinicians will need to use other criteria, such as cost or patient comfort,to help guide them in their decision as to the best wound therapy to offer a particular patient. Aswith any wound therapy, if the wound is not progressing, changing to another modality is veryoften appropriate.
Considerations for selection of appropriate NPWT protocol
A number of factors should be considered when using NPWT including goal of treatment,suction protocol, and the type of dressing. Granulation tissue growth, edema removal, and flapor graft immobilization, each need different NPWT pressure protocols and treatment duration.For example, a chronic ulcer may benefit from continuous suction for the duration of treatment,whereas in an acute wound, it may be most appropriate to begin with 48 hours of continuoussuction, followed by cycles of intermittent therapy (eg, 5 minutes on and 2 minutes off).11 Short,intermittent NPWT has demonstrated a more profound tissue response,50 but it may not besuitable in all cases. Intermittent therapy may not be tolerated because of patient discomfort.The optimal NPWT suction applied to various wounds is not currently known. In our practice, weused less pressure on circumferential wounds and when used in conjunction with a free flap.
Clinicians are now presented with a variety of interfaces. Reticulated open-pore foams havethe most evidence behind them and have been shown to create tissue microdeformation.12
These foams also have the capacity to transmit suction over long distances. More data arerequired to best inform surgeons of the optimal interface material for a particular clinicalsituation. Wounds with an increased risk of infection may require an increased frequency indressing changes.11
Clinical use: device applicationCorrect placement of the interface material is essential for successful NPWT. We like to cut
the foam so that it is slightly smaller than the wound and insert the interface material into allundermined areas or tracks. When possible, we use just 1 interface material that is carefully cutto fill any irregularities in the wound. When more than 1 interface is used, it must to be carefullydocumented to assure that there are no retained foreign bodies. When granulation tissue isdesired, the foam should be placed directly on the wound surface.18 A nonadherent contact layershould be used when granulation tissue is not desired or if the interface is over a luminalstructure such as the bowel or large blood vessels. Having the suction port come out at a
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331326
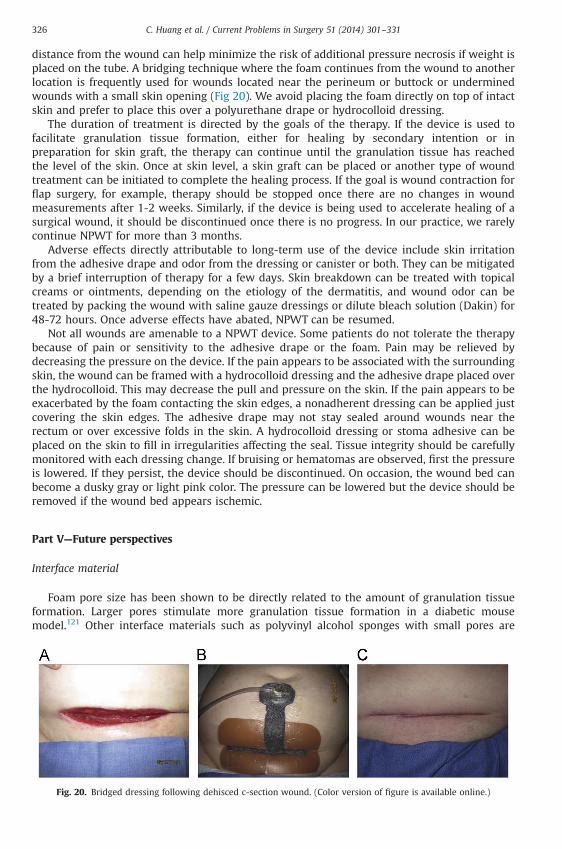
distance from the wound can help minimize the risk of additional pressure necrosis if weight isplaced on the tube. A bridging technique where the foam continues from the wound to anotherlocation is frequently used for wounds located near the perineum or buttock or underminedwounds with a small skin opening (Fig 20). We avoid placing the foam directly on top of intactskin and prefer to place this over a polyurethane drape or hydrocolloid dressing.
The duration of treatment is directed by the goals of the therapy. If the device is used tofacilitate granulation tissue formation, either for healing by secondary intention or inpreparation for skin graft, the therapy can continue until the granulation tissue has reachedthe level of the skin. Once at skin level, a skin graft can be placed or another type of woundtreatment can be initiated to complete the healing process. If the goal is wound contraction forflap surgery, for example, therapy should be stopped once there are no changes in woundmeasurements after 1-2 weeks. Similarly, if the device is being used to accelerate healing of asurgical wound, it should be discontinued once there is no progress. In our practice, we rarelycontinue NPWT for more than 3 months.
Adverse effects directly attributable to long-term use of the device include skin irritationfrom the adhesive drape and odor from the dressing or canister or both. They can be mitigatedby a brief interruption of therapy for a few days. Skin breakdown can be treated with topicalcreams or ointments, depending on the etiology of the dermatitis, and wound odor can betreated by packing the wound with saline gauze dressings or dilute bleach solution (Dakin) for48-72 hours. Once adverse effects have abated, NPWT can be resumed.
Not all wounds are amenable to a NPWT device. Some patients do not tolerate the therapybecause of pain or sensitivity to the adhesive drape or the foam. Pain may be relieved bydecreasing the pressure on the device. If the pain appears to be associated with the surroundingskin, the wound can be framed with a hydrocolloid dressing and the adhesive drape placed overthe hydrocolloid. This may decrease the pull and pressure on the skin. If the pain appears to beexacerbated by the foam contacting the skin edges, a nonadherent dressing can be applied justcovering the skin edges. The adhesive drape may not stay sealed around wounds near therectum or over excessive folds in the skin. A hydrocolloid dressing or stoma adhesive can beplaced on the skin to fill in irregularities affecting the seal. Tissue integrity should be carefullymonitored with each dressing change. If bruising or hematomas are observed, first the pressureis lowered. If they persist, the device should be discontinued. On occasion, the wound bed canbecome a dusky gray or light pink color. The pressure can be lowered but the device should beremoved if the wound bed appears ischemic.
Part V—Future perspectives
Interface material
Foam pore size has been shown to be directly related to the amount of granulation tissueformation. Larger pores stimulate more granulation tissue formation in a diabetic mousemodel.121 Other interface materials such as polyvinyl alcohol sponges with small pores are
Fig. 20. Bridged dressing following dehisced c-section wound. (Color version of figure is available online.)
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 327
nonadherent, with little tissue ingrowth. Several authors have instilled a variety of solutions intothese devices, which may be effective, particularly when treating wounds with high bioburdenof bacteria.27
Optimal cycling
Most biological systems have a more robust response when subjected to variable rather thancontinuous mechanical forces. In a preclinical model, we found that applying NPWT for 4 hoursevery 2 days gave a similar granulation tissue response as continuous therapy. Surprisingly,when faster cycle times were used, there was less granulation tissue formed, suggesting that toofast of a cycle time may damage nascent granulation tissue.35,122,123
Adhesives
Current devices are often limited to obtaining a good seal at the edges of the device, making itdifficult to maintain suction. Advances in adhesive science to allow better adhesion aroundcurved and moist surfaces would make the device more easily applied to difficult wounds.
Summary
The efficacy of NPWT in promoting wound healing has been largely accepted by clinicians,yet the number of high-level clinical studies demonstrating its effectiveness is small and muchmore can be learned about the mechanisms of action. In the future, hopefully we will have thedata to assist clinicians in selecting optimal parameters for specific wounds including interfacematerial, waveform of suction application, and the amount of suction to be applied. Furtherinvestigation into specific interface coatings and instillation therapy are also needed. We believethat advances in mechanobiology, the science of wound healing, the understanding of biofilms,and advances in cell therapy will lead to better care for our patients.
References
1. Schaum KD. A new Medicare part B wound care policy. Adv Skin Wound Care. 2001;14(5):238–240.2. Orgill DP, Bayer L, Neuwalder J, Felter R. Microdeformational Wound Therapy—A New Era in Wound Healing.
Business Briefing: Global Surgery—Future Directions. 2005:1-3.3. Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical
experience. Ann Plast Surg. 1997;38(6):563–576. [discussion 577].4. Meyer W, Schmieden V, Gustav Bier AK. Bier's hyperemic treatment. Surgery, Medicine, and the Specialties: A Manual
of its Practical Application.Philadelphia and London: W.B. Saunders Company; 1908.5. Neumann CG. The expansion of an area of skin by progressive distention of a subcutaneous balloon; use of the
method for securing skin for subtotal reconstruction of the ear. Plast Reconstr Surg (1946). 1957;19(2):124–130.6. Morykwas MJ, Argenta LC, Shelton-Brown EI, McGuirt W. Vacuum-assisted closure: a new method for wound
control and treatment: animal studies and basic foundation. Ann Plast Surg. 1997;38(6):553–562.7. Lancerotto L, Bayer LR, Orgill DP. Mechanisms of action of microdeformational wound therapy. Semin Cell Dev Biol.
2012;23(9):987–992.8. Kairinos N, Solomons M, Hudson DA. Negative pressure wound therapy I: the paradox of negativ-pressure wound
therapy. Plast Reconstr Surg. 2008;123:589–598.9. Saxena V, Orgill D, Kohane I. A set of genes previously implicated in the hypoxia response might be an important
modulator in the rat ear tissue response to mechanical stretch. BMC Genomics. 2007;8:430.10. Frequently asked questions about V.A.C.s Therapy. ⟨http://middleeast.kci-medical.com/ME-ENG/vacfaqs⟩; 2013
[accessed 10.02.2014].11. Mendez-Eastman S. Guidelines for using negative pressure wound therapy. Adv Skin Wound Care. 2001;14(6):
314–322. [quiz 324-315].12. Orgill DP, Manders EK, Sumpio BE, et al. The mechanisms of action of vacuum assisted closure: more to learn.
Surgery. 2009;146(1):40–51.13. Scherer SS, Pietramaggiori G, Mathews JC, Prsa MJ, Huang S, Orgill DP. The mechanism of action of the vacuum-
assisted closure device. Plast Reconstr Surg. 2008;122(3):786–797.14. Borgquist O, Ingemansson R, Malmsjo M. The influence of low and high pressure levels during negative-pressure
wound therapy on wound contraction and fluid evacuation. Plast Reconstr Surg. 2011;127(2):551–559.
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331328
15. Kairinos N, Solomons M, Hudson DA. The paradox of negative pressure wound therapy–in vitro studies. J PlastReconstr Aesthet Surg. 2010;63(1):174–179.
16. Anesater E, Borgquist O, Hedstrom E, Waga J, Ingemansson R, Malmsjo M. The influence of different sizes and typesof wound fillers on wound contraction and tissue pressure during negative pressure wound therapy. Int Wound J.2011;8(4):336–342.
17. Kairinos N, Hudson DA, Solomons M. The influence of different sizes and types of wound fillers on woundcontraction and tissue pressure during negative pressure wound therapy. Int Wound J. 2011;8(6):656–657.
18. Saxena V, Hwang CW, Huang S, Eichbaum Q, Ingber D, Orgill DP. Vacuum-assisted closure: microdeformations ofwounds and cell proliferation. Plast Reconstr Surg. 2004;114(5):1086–1096. [discussion 1097-1088].
19. Ingber DE, Levin M. What lies at the interface of regenerative medicine and developmental biology? Development.2007;134(14):2541–2547.
20. McLeod KJ, Lee RC, Ehrlich HP. Frequency dependence of electric field modulation of fibroblast protein synthesis.Science. 1987;236(4807):1465–1469.
21. Yang CC, Chang DS, Webb LX. Vacuum-assisted closure for fasciotomy wounds following compartment syndromeof the leg. J Surg Orthop Adv. 2006;15(1):19–23.
22. Adamkova M, Tymonova J, Zamecnikova I, Kadlcik M, Klosova H. First experience with the use of vacuum assistedclosure in the treatment of skin defects at the burn center. Acta Chir Plast. 2005;47(1):24–27.
23. Labanaris AP, Polykandriotis E, Horch RE. The effect of vacuum-assisted closure on lymph vessels in chronicwounds. J Plast Reconstr Aesthet Surg. 2009;62(8):1068–1075.
24. Winter GD, Scales JT. Effect of air drying and dressings on the surface of a wound. Nature. 1963;197:91–92.25. Winter GD. Formation of the scab and the rate of epithelization of superficial wounds in the skin of the young
domestic pig. Nature. 1962;193:293–294.26. Hinman CD, Maibach H. Effect of air exposure and occlusion on experimental human skin wounds. Nature.
1963;200:377–378.27. Kim PJ, Attinger CE, Steinberg JS, et al. Negative-pressure wound therapy with instillation: international consensus
guidelines. Plast Reconstr Surg. 2013;132(6):1569–1579.28. Gerry R, Kwei S, Bayer L, Breuing KH. Silver-impregnated vacuum-assisted closure in the treatment of recalcitrant
venous stasis ulcers. Ann Plast Surg. 2007;59(1):58–62.29. Orgill DP, Blanco C. Biomaterials for Treating Skin Loss. Boca Raton, FL: CRC Press; 2009.30. Nuutila K, Siltanen A, Peura M, et al. Gene expression profiling of negative-pressure-treated skin graft donor site
wounds. Burns. 2013;39(4):687–693.31. Ingber DE. The mechanochemical basis of cell and tissue regulation. Mech Chem Biosyst. 2004;1(1):53–68.32. Alford PW, Nesmith AP, Seywerd JN, Grosberg A, Parker KK. Vascular smooth muscle contractility depends on cell
shape. Integr Biol. 2011;3(11):1063–1070.33. Chen CS, Mrksich M, Huang S, Whitesides GM, Ingber DE. Geometric control of cell life and death. Science. 1997;276
(5317):1425–1428.34. Ingber DE. Mechanical control of tissue growth: function follows form. Proc Natl Acad Sci U S A. 2005;102(33):
11571–11572.35. Scherer SS, Pietramaggiori G, Mathews JC, Orgill DP. Short periodic applications of the vacuum-assisted closure
device cause an extended tissue response in the diabetic mouse model. Plast Reconstr Surg. 2009;124(5):1458–1465.
36. Huang S, Ingber DE. The structural and mechanical complexity of cell-growth control. Nat Cell Biol. 1999;1(5):E131–E138.
37. Baldwin C, Potter M, Clayton E, Irvine L, Dye J. Topical negative pressure stimulates endothelial migration andproliferation: a suggested mechanism for improved integration of Integra. Ann Plast Surg. 2009;62(1):92–96.
38. Potter MJ, Banwell P, Baldwin C, et al. In vitro optimisation of topical negative pressure regimens for angiogenesisinto synthetic dermal replacements. Burns. 2008;34(2):164–174.
39. McNulty AK, Schmidt M, Feeley T, Kieswetter K. Effects of negative pressure wound therapy on fibroblast viability,chemotactic signaling, and proliferation in a provisional wound (fibrin) matrix. Wound Repair Regen. 2007;15(6):838–846.
40. Lu F, Ogawa R, Nguyen DT, et al. Microdeformation of three-dimensional cultured fibroblasts induces geneexpression and morphological changes. Ann Plast Surg. 2011;66(3):296–300.
41. Engler AJ, Sen S, Sweeney HL, Discher DE. Matrix elasticity directs stem cell lineage specification. Cell. 2006;126(4):677–689.
42. Erba P, Ogawa R, Ackermann M, et al. Angiogenesis in wounds treated by microdeformational wound therapy.Ann Surg. 2011;253(2):402–409.
43. Wackenfors A, Sjogren J, Gustafsson R, Algotsson L, Ingemansson R, Malmsjo M. Effects of vacuum-assisted closuretherapy on inguinal wound edge microvascular blood flow. Wound Repair Regen. 2004;12(6):600–606.
44. Greene AK, Puder M, Roy R, et al. Microdeformational wound therapy: effects on angiogenesis and matrixmetalloproteinases in chronic wounds of 3 debilitated patients. Ann Plast Surg. 2006;56(4):418–422.
45. Younan GJ, Heit YI, Dastouri P, et al. Mast cells are required in the proliferation and remodeling phases ofmicrodeformational wound therapy. Plast Reconstr Surg. 2011;128(6):649e–658e.
46. Ingber DE. Tensegrity-based mechanosensing from macro to micro. Prog Biophys Mol Biol. 2008;97(2-3):163–179.47. Ingber DE. Mechanobiology and diseases of mechanotransduction. Ann Med. 2003;35(8):564–577.48. Huang C, Ogawa R. Fibroproliferative disorders and their mechanobiology. Connect Tissue Res. 2012;53(3):187–196.49. Wilkes RP, McNulty AK, Feeley TD, Schmidt MA, Kieswetter K. Bioreactor for application of subatmospheric
pressure to three-dimensional cell culture. Tissue Eng. 2007;13(12):3003–3010.50. Younan G, Ogawa R, Ramirez M, Helm D, Dastouri P, Orgill DP. Analysis of nerve and neuropeptide patterns in
vacuum-assisted closure-treated diabetic murine wounds. Plast Reconstr Surg. 2010;126(1):87–96.
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 329
51. Torbrand C, Wackenfors A, Lindstedt S, Ekman R, Ingemansson R, Malmsjo M. Sympathetic and sensory nerveactivation during negative pressure therapy of sternotomy wounds. Interact Cardiovasc Thorac Surg. 2008;7(6):1067–1070.
52. Barker AR, Rosson GD, Dellon AL. Wound healing in denervated tissue. Ann Plast Surg. 2006;57(3):339–342.53. Morykwas MJ, Simpson J, Punger K, Argenta A, Kremers L, Argenta J. Vacuum-assisted closure: state of basic
research and physiologic foundation. Plast Reconstr Surg. 2006;117(suppl 7):121S–126S.54. Assadian O, Assadian A, Stadler M, Diab-Elschahawi M, Kramer A. Bacterial growth kinetic without the influence of
the immune system using vacuum-assisted closure dressing with and without negative pressure in an in vitrowound model. Int Wound J. 2010;7(4):283–289.
55. Moues CM, Vos MC, van den Bemd GJ, Stijnen T, Hovius SE. Bacterial load in relation to vacuum-assisted closurewound therapy: a prospective randomized trial. Wound Repair Regen. 2004;12(1):11–17.
56. Yusuf E, Jordan X, Clauss M, Borens O, Mader M, Trampuz A. High bacterial load in negative pressure woundtherapy (NPWT) foams used in the treatment of chronic wounds. Wound Repair Regen. 2013;21(5):677–681.
57. Joseph E, Hamori CA, Bergman S, Roaf E, Swann NF, Anastasi GW. A prospective, randomized trial of vacuum-assisted closure versus standard therapy of chronic nonhealing wounds. Wounds. 2000;12:60–67.
58. Schwien T, Gilbert J, Lang C. Pressure ulcer prevalence and the role of negative pressure wound therapy in homehealth quality outcomes. Ostomy Wound Manage. 2005;51(9):47–60.
59. Nakayama M. Applying negative pressure therapy to deep pressure ulcers covered by soft necrotic tissue.Int Wound J. 2010;7(3):160–166.
60. Yao M, Fabbi M, Hayashi H, et al. A retrospective cohort study evaluating efficacy in high-risk patients with chroniclower extremity ulcers treated with negative pressure wound therapy. Int Wound J. 2012, doi: 10.1111/j.1742-481X.2012.01113.x.
61. Nather A, Hong NY, Lin WK, Sakharam JA. Effectiveness of bridge V.A.C. dressings in the treatment of diabetic footulcers. Diabet Foot Ankle. 2011;2:5893.
62. Ulusal AE, Sahin MS, Ulusal B, Cakmak G, Tuncay C. Negative pressure wound therapy in patients with diabetic foot.Acta Orthop Traumatol Turc. 2011;45(4):254–260.
63. Patel RM, Nagle DJ. Nonoperative management of scleroderma of the hand with tadalafil and subatmosphericpressure wound therapy: case report. J Hand Surg. 2012;37(4):803–806.
64. Zutt M, Haas E, Kruger U, Distler M, Neumann C. Successful use of vacuum-assisted closure therapy for leg ulcerscaused by occluding vasculopathy and inflammatory vascular diseases—a case series. Dermatology. 2007;214(4):319–324.
65. Oh BH, Lee SH, Nam KA, Lee HB, Chung KY. Comparison of negative pressure wound therapy and secondaryintention healing after excision of acral lentiginous melanoma on the foot. Br J Dermatol. 2013;168(2):333–338.
66. Katz MS, Finck CM, Schwartz MZ, et al. Vacuum-assisted closure in the treatment of extensive lymphangiomas inchildren. J Pediatr Surg. 2012;47(2):367–370.
67. Heit YI, Lancerotto L, Cortes R, et al. Early kinetics of integration of collagen-glycosaminoglycan regenerativescaffolds in a diabetic mouse model. Plast Reconstr Surg. 2013;132(5):767e–776e.
68. Kang GC, Por YC, Tan BK. In vivo tissue engineering over wounds with exposed bone and tendon: autologousdermal grafting and vacuum-assisted closure. Ann Plast Surg. 2010;65(1):70–73.
69. Bloemen MC, van der Wal MB, Verhaegen PD, et al. Clinical effectiveness of dermal substitution in burns by topicalnegative pressure: a multicenter randomized controlled trial. Wound Repair Regen. 2012;20(6):797–805.
70. Khundkar R, Malic C, Burge T. Use of Acticoat dressings in burns: what is the evidence? Burns. 2010;36(6):751–758.71. Stinner DJ, Waterman SM, Masini BD, Wenke JC. Silver dressings augment the ability of negative pressure wound
therapy to reduce bacteria in a contaminated open fracture model. J Trauma. 2011;71(suppl 1):S147–S150.72. Raad W, Lantis 2nd JC, Tyrie L, Gendics C, Todd G. Vacuum-assisted closure instill as a method of sterilizing massive
venous stasis wounds prior to split thickness skin graft placement. Int Wound J. 2010;7(2):81–85.73. Scimeca CL, Bharara M, Fisher TK, Kimbriel H, Mills JL, Armstrong DG. Novel use of insulin in continuous-instillation
negative pressure wound therapy as “wound chemotherapy”. J Diabetes Sci Technol. 2010;4(4):820–824.74. Scala M, Spagnolo F, Trapasso M, Strada P, Moresco L, Santi P. Association of vacuum-assisted closure and platelet
gel for the definitive surgical repair of an enterocutaneous fistula: a case report. In Vivo. 2012;26(1):147–150.75. Wijewardena A, Vandervord E, Lajevardi SS, Vandervord J, Jackson CJ. Combination of activated protein C and
topical negative pressure rapidly regenerates granulation tissue over exposed bone to heal recalcitrant orthopedicwounds. Int J Low Extrem Wounds. 2011;10(3):146–151.
76. Masumoto K, Nagata K, Oka Y, et al. Successful treatment of an infected wound in infants by a combination ofnegative pressure wound therapy and arginine supplementation. Nutrition. 2011;27(11-12):1141–1145.
77. Rudzka-Nowak A, Luczywek P, Gajos MJ, Piechota M. Application of manuka honey and GENADYNE A4 negativepressure wound therapy system in a 55-year-old woman with extensive phlegmonous and necrotic lesions in theabdominal integuments and lumbar region after traumatic rupture of the colon. Med Sci Monit. 2010;16(11):CS138–CS142.
78. Ganacias-Acuna EF. Active Leptospermum honey and negative pressure wound therapy for nonhealing postsurgicalwounds. Ostomy Wound Manage. 2010;56(3):10–12.
79. Li J, Topaz M, Tan H, et al. Treatment of infected soft tissue blast injury in swine by regulated negative pressurewound therapy. Ann Surg. 2013;257(2):335–344.
80. International Concensus. Appropriate use of silver dressings in wounds. An expert working group concensus.London 2012.
81. Blum ML, Esser M, Richardson M, Paul E, Rosenfeldt FL. Negative pressure wound therapy reduces deep infectionrate in open tibial fractures. J Orthop Trauma. 2012;26(9):499–505.
82. Lee SY, Niikura T, Miwa M, et al. Negative pressure wound therapy for the treatment of infected wounds withexposed knee joint after patellar fracture. Orthopedics. 2011;34(6):211.
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331330
83. Barnett TM, Shilt JS. Use of vacuum-assisted closure and a dermal regeneration template as an alternative to flapreconstruction in pediatric grade IIIB open lower-extremity injuries. Am J Orthop. 2009;38(6):301–305.
84. Hou Z, Irgit K, Strohecker KA, et al. Delayed flap reconstruction with vacuum-assisted closure management of theopen IIIB tibial fracture. J Trauma. 2011;71(6):1705–1708.
85. Steingrimsson S, Gottfredsson M, Gudmundsdottir I, Sjogren J, Gudbjartsson T. Negative-pressure wound therapyfor deep sternal wound infections reduces the rate of surgical interventions for early re-infections. InteractCardiovasc Thorac Surg. 2012;15(3):406–410.
86. Damiani G, Pinnarelli L, Sommella L, et al. Vacuum-assisted closure therapy for patients with infected sternalwounds: a meta-analysis of current evidence. J Plast Reconstr Aesthet Surg. 2011;64(9):1119–1123.
87. De Feo M, Vicchio M, Nappi G, Cotrufo M. Role of vacuum in methicillin-resistant deep sternal wound infection.Asian Cardiovasc Thorac Ann. 2010;18(4):360–363.
88. Doss M, Martens S, Wood JP, Wolff JD, Baier C, Moritz A. Vacuum-assisted suction drainage versus conventionaltreatment in the management of poststernotomy osteomyelitis. Eur J Cardiothorac Surg. 2002;22(6):934–938.
89. Tocco MP, Ballardini M, Masala M, Perozzi A. Post-sternotomy chronic osteomyelitis: is sternal resection alwaysnecessary? Eur J Cardiothorac Surg. 2013;43(4):715–721.
90. Tocco MP, Costantino A, Ballardini M, et al. Improved results of the vacuum assisted closure and Nitinol clipssternal closure after postoperative deep sternal wound infection. Eur J Cardiothorac Surg. 2009;35(5):833–838.
91. Gallo O, Deganello A, Meccariello G, Spina R, Peris A. Vacuum-assisted closure for managing neck abscessesinvolving the mediastinum. Laryngoscope. 2012;122(4):785–788.
92. Sziklavari Z, Grosser C, Neu R, et al. Complex pleural empyema can be safely treated with vacuum-assisted closure.J Cardiothorac Surg. 2011;6:130.
93. Rispoli DM, Horne BR, Kryzak TJ, Richardson MW. Description of a technique for vacuum-assisted deep drains inthe management of cavitary defects and deep infections in devastating military and civilian trauma. J Trauma.2010;68(5):1247–1252.
94. Sermoneta D, Di Mugno M, Spada PL, et al. Intra-abdominal vacuum-assisted closure (VAC) after necrosectomy foracute necrotising pancreatitis: preliminary experience. Int Wound J. 2010;7(6):525–530.
95. Bemelman WA. Vacuum assisted closure in coloproctology. Tech Coloproctol. 2009;13(4):261–263.96. Choi WW, McBride CA, Kimble RM. Negative pressure wound therapy in the management of neonates with
complex gastroschisis. Pediatr Surg Int. 2011;27(8):907–911.97. Kilbride KE, Cooney DR, Custer MD. Vacuum-assisted closure: a new method for treating patients with giant
omphalocele. J Pediatr Surg. 2006;41(1):212–215.98. FDA Safety Communication: UPDATE on Serious Complications Associated with Negative Pressure Wound
Therapy Systems [webpage]. ⟨http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm244211.htm⟩; 2011[accessed 25.02.2014].
99. Kilpadi DV, Cunningham MR. Evaluation of closed incision management with negative pressure wound therapy(CIM): hematoma/seroma and involvement of the lymphatic system. Wound Repair Regen. 2011;19(5):588–596.
100. Stannard JP, Volgas DA, McGwin 3rd G, et al. Incisional negative pressure wound therapy after high-risk lowerextremity fractures. J Orthop Trauma. 2012;26(1):37–42.
101. Pachowsky M, Gusinde J, Klein A, et al. Negative pressure wound therapy to prevent seromas and treat surgicalincisions after total hip arthroplasty. Int Orthop. 2012;36(4):719–722.
102. Conde-Green A, Chung TL, Holton 3rd LH, et al. Incisional negative-pressure wound therapy versus conventionaldressings following abdominal wall reconstruction: a comparative study. Ann Plast Surg. 2013;71(4):394–397.
103. Wilkes RP, Kilpad DV, Zhao Y, Kazala R, McNulty A. Closed incision management with negative pressure woundtherapy (CIM): biomechanics. Surg Innov. 2012;19(1):67–75.
104. Masden D, Goldstein J, Endara M, Xu K, Steinberg J, Attinger C. Negative pressure wound therapy for at-risk surgicalclosures in patients with multiple comorbidities: a prospective randomized controlled study. Ann Surg. 2012;255(6):1043–1047.
105. Llanos S, Danilla S, Barraza C, et al. Effectiveness of negative pressure closure in the integration of split thicknessskin grafts: a randomized, double-masked, controlled trial. Ann Surg. 2006;244(5):700–705.
106. Petkar KS, Dhanraj P, Kingsly PM, et al. A prospective randomized controlled trial comparing negative pressuredressing and conventional dressing methods on split-thickness skin grafts in burned patients. Burns. 2011;37(6):925–929.
107. Azzopardi EA, Boyce DE, Dickson WA, et al. Application of topical negative pressure (vacuum-assisted closure) tosplit-thickness skin grafts: a structured evidence-based review. Ann Plast Surg. 2013;70(1):23–29.
108. Moisidis E, Heath T, Boorer C, Ho K, Deva AK. A prospective, blinded, randomized, controlled clinical trial of topicalnegative pressure use in skin grafting. Plast Reconstr Surg. 2004;114(4):917–922.
109. Vaienti L, Gazzola R, Benanti E, et al. Failure by congestion of pedicled and free flaps for reconstruction of lowerlimbs after trauma: the role of negative-pressure wound therapy. J Orthop Traumatol. 2013;14(3):213–217.
110. Goldstein JA, Iorio ML, Brown B, Attinger CE. The use of negative pressure wound therapy for random local flaps atthe ankle region. J Foot Ankle Surg. 2010;49(6):513–516.
111. Schmedes GW, Banks CA, Malin BT, Srinivas PB, Skoner JM. Massive flap donor sites and the role of negativepressure wound therapy. Otolaryngol Head Neck Surg. 2012;147(6):1049–1053.
112. Meara JG, Guo L, Smith JD, Pribaz JJ, Breuing KH, Orgill DP. Vacuum-assisted closure in the treatment of deglovinginjuries. Ann Plast Surg. 1999;42(6):589–594.
113. Morris M, Schreiber MA, Ham B. Novel management of closed degloving injuries. J Trauma. 2009;67(4):E121–E123.114. Dini M, Quercioli F, Mori A, Romano GF, Lee AQ, Agostini T. Vacuum-assisted closure, dermal regeneration template
and degloved cryopreserved skin as useful tools in subtotal degloving of the lower limb. Injury. 2012;43(6):957–959.
115. V.A.C.s Therapy Forms and Brochures. ⟨http://www.kci1.com/KCI1/vactherapyformsandbrochures⟩ [accessed25.02.2014].
C. Huang et al. / Current Problems in Surgery 51 (2014) 301–331 331
116. Weidenhagen R, Gruetzner KU, Wiecken T, Spelsberg F, Jauch KW. Endoscopic vacuum-assisted closure ofanastomotic leakage following anterior resection of the rectum: a new method. Surg Endosc. 2008;22(8):1818–1825.
117. V.A.C. Therapy Indications and Contraindications. ⟨http://kci1.com/KCI1/indicationsandcontraindications⟩ [accessed25.02.2014].
118. Steenvoorde P, den Outer A, Neijenhuis P. Stomal mucocutaneous dehiscence as a complication of topical negativepressure used to treat an open abdomen: a case series. Ostomy Wound Manage. 2009;55(6):44–48.
119. Citak M, Backhaus M, Meindl R, Muhr G, Fehmer T. Rare complication after VAC-therapy in the treatment of deepsore ulcers in a paraplegic patient. Arch Orthop Trauma Surg. 2010;130(12):1511–1514.
120. Marsh DJ, Abu-Sitta G, Patel H. The role of vacuum-assisted wound closure in blast injury. Plast Reconstr Surg.2007;119(6):1978–1979.
121. Heit YI, Dastouri P, Helm DL, et al. Foam pore size is a critical interface parameter of suction-based wound healingdevices. Plast Reconstr Surg. 2012;129(3):589–597.
122. Dastouri P, Helm DL, Scherer SS, Pietramaggiori G, Younan G, Orgill DP. Waveform modulation of negative-pressurewound therapy in the murine model. Plast Reconstr Surg. 2011;127(4):1460–1466.
123. Malmsjo M, Gustafsson L, Lindstedt S, Gesslein B, Ingemansson R. The effects of variable, intermittent, andcontinuous negative pressure wound therapy, using foam or gauze, on wound contraction, granulation tissueformation, and ingrowth into the wound filler. Eplasty. 2012;12:e5.





![Negative pressure wound therapy for skin grafts and ... · [Intervention Review] Negative pressure wound therapy for skin grafts and surgical wounds healing by primary intention Joan](https://img.pdfslide.us/doc/110x75/5eaca82cd857b569f0001932/negative-pressure-wound-therapy-for-skin-grafts-and-intervention-review-negative.jpg)















