-
7/30/2019 efectos 6
1/11
Immediate effects of rapid maxillary expansionwith Haas-type and
hyrax-type expanders:
A randomized clinical trial
Andre Weissheimer,a Luciane Macedo de Menezes,b Mauricio
Mezomo,a Daniela Marchiori Dias,a
Eduardo Martinelli Santayana de Lima,b and Susana Maria Deon
Rizzattoc
Porto Alegre, Rio Grande do Sul, Brazil
Introduction: The purposes of this study were to evaluate and
compare the immediate effects of rapid maxillary
expansion (RME) in the transverse plane with Haas-type and
hyrax-type expanders by using cone-beam
computed tomography. Methods: A sample of 33 subjects (mean age,
10.7 years; range, 7.2-14.5 years)
with transverse maxillary deficiency were randomly divided into
2 groups: Haas (n 5 18) and hyrax (n 5 15).
All patients had RME with an initial activation of 4 quarter
turns followed by 2 quarter turns per day until the
expansion reached 8 mm. Cone-beam computed tomography scans were
taken before expansion and at the
end of the RME phase. Maxillary transversal measurements were
compared by using the mixed analysis of
variance (ANOVA) model and the Tukey-Kramer method. Results: RME
increased all maxillary transverse
dimensions (P\0.0001). There was less expansion at skeletal than
dental levels. The hyrax group had greater
statistically significant orthopedic effects and less tipping
tendency of the maxillary first molars compared with
the Haas group. Conclusions: Both appliances were efficient in
correcting a transverse maxillary deficiency.
The pure skeletal expansion was greater than actual dental
expansion. The hyrax-type expander produced
greater orthopedic effects than did the Haas-type expander, but
this effect was less than 0.5 mm per side and
might not be clinically significant. (Am J Orthod Dentofacial
Orthop 2011;140:366-76)
R
apid maxillary expansion (RME) is an important
method used to correct a transverse maxillary de-ficiency. It
was first described in the literature over
a century ago by Angell,1 and it has been disseminatedand made
widely popular by Haas since 1961.2 In
RME, rigid and fixed expanders are used to produceheavy forces
to obtain the maximum skeletal response
by opening the midpalatal suture, with minimumorthodontic
movement.2-5
Among the appliances used for RME, the tooth-tissueborne
(Haas-type) and the tooth-borne (hyrax-type) expanders are the most
recognized in the literature.The main difference between them is
the acrylic pad that
leans on the lateral walls of the palatal vault (Haas-type)
to reinforce the anchorage for greater orthopedic
response and better force distribution during RME.2,4
In the hyrax-type expander, there is no acrylic pad;
therefore, it is more hygienic and prevents
soft-tissueirritation caused by food impaction under the
acrylicplate.6 Although a cephalometric investigation has
notdemonstrated any differences between Haas-type andhyrax-type
expanders,7 there is no consensus in the lit-erature regarding the
differences in the immediate
RME effects produced by these appliances.Several investigations
have analyzed the effects of
RME through 2-dimensional cephalometric radiographs,which do not
allow accurate identification of dentoske-
letal structures because of the superimposition of manybones in
the different planes of space.2,7-9 To overcomethese limitations,
computed tomography (CT) for theassessment of the transverse
dimensions of themaxilla was introduced by Timms et al10 in
the1980s. However, the use of conventional CT scans inorthodontics
has been limited because of cost and ra-
diation concerns.11 Cone-beam CT (CBCT) has usheredin a new era
in dental diagnostics. This technology wasdesigned for imaging hard
tissues of the maxillofacialregion with minimum distortion at a
lower cost and
with lower radiation emissions compared with
From the Department of Orthodontics, Pontifical Catholic
University of Rio
Grande Do Sul, Porto Alegre, Rio Grande do Sul,
Brazil.aPostgraduate student (Ph.D.).bProfessor.cAssistant
professor.
The authors report no commercial, proprietary, or financial
interest in the prod-
ucts or companies described in this article.
Reprint requests to: Andre Weissheimer, Pontifcia Universidade
Catolica do Rio
Grande do Sul, Faculdade de Odontologia, Predio 6, Avenida
Ipiranga, 6681, sala
209,Porto Alegre, RS, Brazil, CEP 90619-900; e-mail,
[email protected].
Submitted, March 2010; revised and accepted, July 2010.
0889-5406/$36.00
Copyright 2011 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2010.07.025
366
ORIGINAL ARTICLE
mailto:[email protected]:[email protected]
-
7/30/2019 efectos 6
2/11
conventional CT. The high resolution of CBCT imagesis due to the
isotropic voxel (equal in all 3 dimensions),
which produces submillimeter resolutions ranging from0.4 mm to
as low as 0.125 mm.11 Several investigationshave shown the high
accuracy of CBCT images forquantitative and qualitative
analyses.12-15 Its use is
recommended in orthodontics for several purposessuch as
evaluation of impacted teeth,16,17 evaluation
of bone grafts in cleft regions,18 analysis of alveolarbone
before placement of orthodontic temporary an-
chorage devices,19 and evaluation of RME effects onnasomaxillary
structures.20
The purposes of this study were to evaluate and com-pare the
immediate effects of RME on the transverse
plane with Haas-type and hyrax-type expanders byusing
high-resolution CBCT.
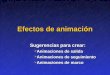
Fig 1. A, Haas-type expander and B, hyrax-type expander at the
end of the active phase of RME.
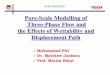
Fig 2. Transverse maxillary posterior region evaluation: A and
B, preexpansion; C and D, atthe end ofthe active phase of
expansion.
Weissheimer et al 367
American Journal of Orthodontics and Dentofacial Orthopedics
September 2011 Vol 140 Issue 3
-
7/30/2019 efectos 6
3/11
MATERIAL AND METHODS
This study was approved by the ethical committee ofthe
Pontifical Catholic University of Rio Grande do Sul in
Brazil. Informed consent was obtained from the parentsof all
patients who agreed to participate in this study. The
sample was selected by examining subjects in need of
or-thodontic treatment at the Department of Orthodonticsof the
School of Dentistry. The inclusion criteria forthis study were
transverse maxillary deficiency, mixeddentition or early permanent
dentition, and no surgicalor other treatment that might affect the
RME effects
during the expansion period. Patients with
congenitalmalformations or periodontal diseases, or above 15
yearsof age were excluded from the study sample.
In this prospective study, the sample comprised 33
healthy white children (11 boys, 22 girls) with a
meanchronologic age of 10.7 years (range, 7.2-14.5 years)
and a mean skeletal age of 10.9 years (range, 6.8-15years).
These patients were randomly divided into 2groups: Haas (n 5 18)
and hyrax (n 5 15). In the Haasgroup, the Haas-type expander, with
4 bands (first perma-
nent molars and first premolars or first deciduous molars)and
buccal and lingual stainless steel bars of 1.0-mmdiameter was used
(Fig 1, A). In the hyrax group, thehyrax-type expander, with 4
bands, buccal and lingualstainless steel bars of 1.0-mm diameter
and a jackscrew
with 1.4-mm stainless steel extensions soldered to the lin-
gual surfaces of each pair of bands, was used (Fig 1, B).Both
appliances had expansion jackscrews with acti-
vations of a quarter turn equivalent to a 0.2-mm expan-sion. All
patients in the Haas and hyrax groups had RME,
with initial activations of 4 quarter turns (0.8 mm)
followed by 2 quarter turns per day (0.4 mm) until theexpansion
screw reached 8 mm.
The i-CAT (Imaging Sciences International, Hatfield,Pa) was used
to obtain CBCT images before RME (T1)and at the end of the active
expansion phase (T2). TheCBCT scans were performed at 120 kV, 8 mA,
scan
time of 40 seconds, and 0.3-mm voxel dimension. Thedata for each
patient were reconstructed with 0.3-mmslice thickness, and the
digital imaging and communica-
tions in medicine (DICOM) images were assessed by us-ing the
EFILM workstation software program (version2.1.2, Merge Healthcare,
Milwaukee, Wis). All linearand angular measurements were made by a
blinded ex-aminer (M.M.), who had no access to the data or the
clin-ical consultations of the patients in this sample.
For transverse maxillary posterior region evaluation,
the DICOMfiles with CBCT images at T1 and T2 were im-ported into
EFILM and visualized as axial imagesarranged side by side. To
obtain standardized axial andcoronal slices and thus allow the
comparisons betweenT1 and T2, the following references were used.
In the
Fig 3. Landmarks used in the evaluation of the maxillary
posterior region.
368 Weissheimer et al
September 2011 Vol 140 Issue 3 American Journal of Orthodontics
and Dentofacial Orthopedics
-
7/30/2019 efectos 6
4/11
axial slices, the images that displayed the root canal in
the most apical region of the palatal root of maxillaryfirst
permanent molars were selected. By using the Mul-tiPlanar
Reformation tool, the MultiPlanar Reformationline was positioned at
the root canal in the most apical
region of the palatal root of the maxillaryfirst perma-nent
molars on the right and left sides. From these ref-erences,
standardized coronal images were produced,and the measurements were
made (Fig 2). The landmarksused for evaluation of the maxillary
posterior region areshown in Figure 3 and described in Table I.
The analyses of the transversal changes in the maxil-lary
anterior region were performed in a similar way tothose of the
posterior region. In the axial slices, imagesat T1 and T2 were
selected with the root canals in the
most apical region of the roots of the maxillary perma-nent
canines visualized. After that, the MultiPlanar
Reformation line was positioned at the root canal inthe most
apical region of the maxillary permanentcanine root on the right
and left sides. From theses ref-erences, standardized coronal
images were produced,
and the measurements were made (Fig 4). The landmarks
used to evaluate the RME effects in the anterior region
ofmaxilla are shown in Figure 5 and described in Table I.
Statistical analysis
Intraexaminer reliability of the measurements wasdetermined by
intraclass correlation coefficients. Double
assessments of each parameter at T1 and T2 (10 daysapart) of 15
randomly selected patients from bothgroups were compared (Table
II). The data obtainedfrom all measurements were processed with SAS
soft-
ware (version 9.0.2, SAS, Cary, NC). Means and standarderrors
for each parameter were calculated, and data at T1
Table I. Landmarks for transverse maxillary evaluation
Skeletal
Line 1-2 Posterior baseline Line formed by the 2 lower points at
the inferior inner contour of the
posterior nasal cavity on the right and left sides,
respectively.
Line 13-14 Anterior baseline Line formed by the 2 lower points
at the inferior inner contour of the anteriornasal cavity on the
right and left sides, respectively.
Distance 5-6 Posterior apical base width Distance between points
5 and 6 (points formed by the intersection of the
line 1-2 with buccal contour of maxilla on the right and left
sides,
respectively).
Distance 11-12 Posterior midpa latal suture width Distance
between points 11 and 12 (lower points at medial limits of
maxillary
palatine processes, on the right and left sides, respectively),
representing
the midpalatal suture.
Distance 15-16 Anterior apical base width (inferior) Distance
between points 15 and 16 (points formed by the intersection of
line
13-14 with buccal contour of maxilla on the right and left
sides,
respectively).
Distance 17-18 Anterior apical base width (superior) Distance
between points 17 and 18 (intersection of the straight line, which
is
parallel and 5 mm superior to line 13-14, with buccal contour of
maxilla
on the right and left sides, respectively).
Distance 21-22 Anterior mid-palatal suture width Distance
between points 21 and 22 (lower points at medial limits of
maxillary
palatine processes, on the right and left sides, respectively),
representingthe midpalatal suture in the anterior region.
Alveolar
Distance 3-4 Posterior width at the alveolar crest level
Distance between points 3 and 4 (coronal-most points of the
maxillary
buccal alveolar processes, on the right and left sides,
respectively).
Distance 19-20 Anterior width at midalveolar level Distance
between points 19 and 20 (intersection of the straight line, which
is
parallel and 5 mm inferior to line 13-14, with buccalcontour of
maxilla on
the right and left sides, respectively).
Dental
Distance 7-8 Intermolar width at occlusal surface Distance
between points 7 and 8 (points formed by the intersection of
a straight line, that superimpose the long axis of the root
canal offirst
permanent molar palatine root, with the occlusal surface on the
right and
left sides, respectively).
Distance 9-10 Intermolar width at palatal root apices Distance
between points 9 and 10 (apices of palatine root of permanent
first
molars, on the right and left sides, respectively).
Angle 1MD Right first molar angulation Angle formed by the
straight line from point 7 and that superimposes the
long axis of the root canal of permanent first molar palatine
root, on the
right side, with line 1-2.
Angle 1ME Left first molar angulation Angle formed by the
straight line from point 8 and that superimposes the
long axis of the root canal of permanent first molar palatine
root, on the
left side, with the line 1-2.
Weissheimer et al 369
American Journal of Orthodontics and Dentofacial Orthopedics
September 2011 Vol 140 Issue 3
-
7/30/2019 efectos 6
5/11
and T2 were compared by using the mixed analysis ofvariance
(ANOVA) model and the Tukey-Kramer method
at a significance level of 5%.
RESULTS
The overall immediate effects of RME on the trans-
verse plane are shown in Table III. There were signifi-cant
increases in maxillary width at the skeletal,alveolar, and dental
levels for both the Haas (TableIV) and the hyrax (Table V) groups
in all parameters
(P\0.05). There was less expansion at the skeletalthan at the
dental level, just as the increase in the max-illary apical base
was smaller in the posterior region(distances 5-6 and 11-12)
compared with the anterior(distances 15-16, 21-22) (Tables III-V).
The hyraxgroup had greater statistically significant increases
in
the maxillary transverse dimensions at the skeletallevel than
did the Haas group in both posterior(distances 5-6 and 11-12) and
anterior (distance 21-22) regions (Table VI). There was no
significant differ-
ence between the groups for the buccal inclination ofthe
maxillary first permanent molars, except for the
linear measure (distance 9-10), which indicated greater
inclination of these teeth in the Haas group than in thehyrax
group (Table VI).
DISCUSSION
After Broadbent21 introduced the cephalostat in
1931, several investigations have analyzed the effectsof RME
through cephalometry in 2-dimensional radio-graphs.3,8,22 The major
problem associated withcephalometry is projection errors, which
have an effect
on linear and angular measurements, caused bymagnification and
distortion and are compounded byincorrect patient positioning.23,24
To overcome theselimitations, we evaluated and compared, using
high-resolution CBCT, the immediate effects of RME on thetransverse
planes with Haas-type and hyrax-type ex-
panders. CBCT was used because it is a suitable exami-nation for
imaging craniofacial areas, with minimumdistortion, at a lower cost
and with lower radiation dos-ages than conventional CT.11,25,26 In
addition, CBCT isan accurate and reliable method for assessing
changesassociated with RME on nasomaxillary structures.20
Fig 4. Transverse maxillary anterior region evaluation: A and B,
preexpansion; C and D, at the end of
the active phase of expansion.
370 Weissheimer et al
September 2011 Vol 140 Issue 3 American Journal of Orthodontics
and Dentofacial Orthopedics
-
7/30/2019 efectos 6
6/11
Regarding previous reports that used CT images toevaluate RME,
our study had an adequate sample size(33 subjects).10,20,27-33
Furthermore, this study designhad some important features: (1) it
was a prospectivestudy; (2) the patients were randomly divided
betweenthe groups; (3) the methodology was highly
standardized in terms of appliance fabrication, and rateand
amount of expansion; and (4) it used high-resolution CBCT. In this
study, since the active expansionphase lasted only 19 days, there
was no need to use
a control group without treatment since normal growthwas not an
influencing factor in this short time. In this
study, the overall effects of RME produced a significantskeletal
increase in the transverse maxillary dimension,confirming previous
reports.2-5,20,28,30,34,35 The skeletal
expansion amounts were greater in the anteriorregion2.82 mm
(distance 17-18), 3.48 mm (distance15-16), and 4 mm (distance
21-22)compared withthe posterior2.64 mm (distance 5-6) and 2.88
mm(distance 11-12) (Table III). In agreement with previous
authors, the expansion pattern was triangular witha wider base
at the anterior portion of maxilla.20,29,35
The greater expansion in the anterior region could be
explained by the resistance of the medial and lateralpterygoid
plates of the sphenoid bone to the maxillarytip movement during the
RME.35 Another feasible expla-nation would be through maxillary
expansion biome-
chanics: ie, the direction of the expansion forceproduced by the
expanders would be located anteriorto the center of resistance of
each maxillary half.36
The hyrax-type expander produced greater skeletalexpansion3.14
mm (distance 11-12) and 4.37 mm(distance 21-22)than did the
Haas-type expander2.62 mm (distance 11-12) and 3.63 mm
(distance21-22) (Table VI). The skeletal gain in the hyrax
groupaccounted for 38.5% to 39.2% (posterior region) and37.5% to
54.7% (anterior region) of the total expansion
(8 mm). In the Haas group, the increases were smaller,ranging
from 27.2% to 32.7% in the posterior region
Fig 5. Landmarks used in the evaluation of the maxillary
anterior region.
Table II. Intraclass correlation coefficients of the
mea-surements
Measurement ICC
Distance 5-6 0.98
Distance 11-12 0.94
Distance 15-16 0.96
Distance 17-18 0.95
Distance 21-22 0.61
Distance 3-4 0.98
Distance 19-20 0.96
Distance 7-8 0.95
Distance 9-10 0.97
Angle 1MD 0.93
Angle 1ME 0.74
Weissheimer et al 371
American Journal of Orthodontics and Dentofacial Orthopedics
September 2011 Vol 140 Issue 3
-
7/30/2019 efectos 6
7/11
and 32.7% to 45.2% in the anterior region. These
comparison results between the appliances differ fromprevious
reports.7,28,37 Siqueira et al7 compared the
Haas-type and hyrax-type expanders through frontalcephalometric
radiographs and found no differences
between them. Garib et al28 also found no differences
between these 2 expanders using spiral CT. This phe-nomenon
could be explained by the small study sample(n 5 8), which reduced
the power of the t test to showstatistically significant
differences. When significantdifferences are demonstrated in such
situations, they
clearly exist and most likely have clinical importance.However,
the absence of significant differences does
not necessarily indicate that they do not exist. In addi-tion,
the RME changes were analyzed 3 months afterthe active expansion
phase, unlike our study, with theimmediate effects of RME on 33
patients evaluated. In
disagreement with the present study, Oliveira et al37
found that the Haas-type expander achieved expansionwith a
greater component of orthopedic movementthan the hyrax-type
expander. However, the comparison
between the 2 kinds of expanders was performed on
study models and anteroposterior cephalograms.The main
difference between Haas-type and hyrax-
type expanders is the acrylic pad close to the palate in
the Haas-type appliance. According to Haas,4 a purpose
of the acrylic pad is to reinforce the anchorage forgreater
orthopedic response during RME. However,the results of our study
did not support this theory,at least regarding the immediate
effects of expansion.
Better results in the immediate skeletal response wereobtained
by the hyrax-type expander vs the Haas-type. This fact can be
explained by differences in appli-ance design: more specifically,
in the connection mech-anism of the jackscrew to the bands of the
anchorageteeth. In the hyrax-type appliance design, the
jackscrew
was directly connected to the bands by a rigid stainlesssteel
framework (1.4 mm), unlike the Haas-type appli-
ance design, where the acrylic was responsible for con-necting
the stainless steel framework (1.0 mm) to the
jackscrew. According to a previous study about the bio-mechanics
of RME, appliance designs that use an
acrylic interface with the teeth are far less stiff thanthose
constructed solely of soldered stainless steel
wire, as in the case of the hyrax-type expander.36 How-ever, the
acrylic pad against the palate would be impor-tant, especially
during the retention period, when it
would prevent the bone from moving through theteeth, thus
averting an orthopedic relapse of the ex-
panded maxilla.4,5,20
Table III. Immediate changes in the maxillary transverse plane
with RME
Variable
T1 T2 Change
PMean SE Mean SE Mean SE
SkeletalDistance 5-6 (mm)
Posterior apical base width 60.29 0.64 62.93 0.64 2.64 0.11
\0.0001*
Distance 11-12 (mm)
Posterior midpalatal suture width 00.00 0.08 02.86 0.08 2.88
0.09 \0.0001*
Distance 15-16 (mm)
Anterior apical base width (inferior) 38.37 0.61 41.85 0.61 3.48
0.23 \0.0001*
Distance 17-18 (mm)
Anterior apical base width (superior) 38.96 0.83 41.78 0.83 2.82
0.23 \0.0001*
Distance 21-22 (mm)
Anterior midpalatal suture width 00.00 0.10 04.00 0.11 4.00 0.13
\0.0001*
Alveolar
Distance 3-4 (mm)
Posterior width at alveolar crest level 51.65 0.51 57.28 0.51
5.63 0.16 \0.0001*
Distance 19-20 (mm)
Anterior width at midalveolar level 40.06 0.58 44.46 0.58 4.40
0.22 \0.0001*
Dental
Distance 7-8 (mm)
Intermolar width at occlusal surface 43.51 0.44 51.31 0.44 7.80
0.15 \0.0001*
Distance 9-10 (mm)
Intermolar width at palatal root apices 29.90 0.52 32.55 0.52
2.65 0.14 \0.0001*
Angle 1MD ()
Right first molar angulation 110.6 1.4 118.1 1.4 7.53 0.74
\0.0001*
Angle 1ME ()
Left first molar angulation 117.7 1.2 123.8 1.2 6.17 0.68
\0.0001*
*Statistically significant (P\0.05).
372 Weissheimer et al
September 2011 Vol 140 Issue 3 American Journal of Orthodontics
and Dentofacial Orthopedics
-
7/30/2019 efectos 6
8/11
In the hyrax group, the transverse expansion at thesuture
gradually decreased from the anterior, by 4.37mm (distance 21-22),
to the posterior, by 3.14 mm
(distance 11-12) (Table V). This sutural orthopedic sep-aration
accounted for 54.7% and 39.2% of the totalexpansion (8 mm) at
distances 21-22 and 11-12,
Table IV. Immediate changes in the maxillary transverse plane
with RME in the Haas group
Variable
T1 T2 Change
PMean (mm) SE (mm) Mean (mm) SE (mm) Mean (mm) SE (mm)
SkeletalDistance 5-6
Posterior apical base width 61.10 0.87 63.29 0.87 2.19 0.15
\0.0001*
Distance 11-12
Posterior midpalatal suture width 00.00 0.11 02.61 0.11 2.62
0.12 \0.0001*
Distance 15-16
Anterior apical base width (inferior) 38.98 0.82 42.28 0.82 3.29
0.30 \0.0001*
Distance 17-18
Anterior apical base width (superior) 39.70 1.12 42.33 1.12 2.62
0.31 \0.0001*
Distance 21-22
Anterior midpalatal suture width 00.00 0.15 03.63 0.15 3.63 0.17
\0.0001*
Alveolar
Distance 3-4
Posterior width at alveolar crest level 51.96 0.69 57.41 0.69
5.44 0.25 \0.0001*
Distance 19-20
Anterior width at midalveolar level 40.56 0.79 44.59 0.79 4.03
0.30 \0.0001*
Dental
Distance 7-8
Intermolar width at occlusal surface 43.42 0.59 51.12 0.59 7.70
0.20 \0.0001*
Distance 9-10
Intermolar width at palatal root apices 30.57 0.71 32.72 0.71
2.15 0.18 \0.0001*
*Statistically significant (P\0.05).
Table V. Immediate changes in the maxillary transverse plane
with RME in the hyrax group
Variable
T1 T2 Change
PMean (mm) SE (mm) Mean (mm) SE (mm) Mean (mm) SE (mm)
Skeletal
Distance 5-6
Posterior apical base width 59.48 0.92 62.58 0.92 3.10 0.17
\0.0001*
Distance 11-12
Posterior midpalatal suture width 00.00 0.12 03.14 0.12 3.14
0.14 \0.0001*
Distance 15-16
Anterior apical base width (inferior) 37.75 0.87 41.42 0.87 3.66
0.34 \0.0001*
Distance 17-18
Anterior apical base width (superior) 38.22 1.19 41.22 1.19 3.00
0.35 \0.0001*
Distance 21-22
Anterior midpalatal suture width 00.00 0.16 04.37 0.16 4.37 0.20
\0.0001*
Alveolar
Distance 3-4
Posterior width at alveolar crest level 51.34 0.73 57.15 0.73
5.80 0.28 \0.0001*
Distance 19-20Anterior width at midalveolar level 39.58 0.83
44.34 0.83 4.76 0.34 \0.0001*
Dental
Distance 7-8
Intermolar width at occlusal surface 43.60 0.62 51.50 0.62 7.90
0.23 \0.0001*
Distance 9-10
Intermolar width at palatal root apices 29.24 0.75 32.38 0.75
3.14 0.21 \0.0001*
*Statistically significant (P\0.05).
Weissheimer et al 373
American Journal of Orthodontics and Dentofacial Orthopedics
September 2011 Vol 140 Issue 3
-
7/30/2019 efectos 6
9/11
respectively. These findings endorse a previous report inwhich,
of the total expansion achieved, the hyrax-typeexpander produced
55% of the suture expansion in theanterior and 38% in the posterior
regions.20 However,
the RME changes were analyzed 3 months after theactive expansion
phase, unlike our study, where the
immediate effects of RME were evaluated.This investigation
showed a more significant skele-
tal response compared with other studies.29,30 Ina study by
Lione et al,29 the RME was performed
with a modified hyrax-type expander (bands on thefirst permanent
molars only), and less sutural expan-sion was obtained in both the
anterior (2.17 mm)and the posterior (1.15 mm) regions. This small
ortho-pedic effect could be explained by (1) the use of a mod-ified
hyrax-type expander, which had less anchorage;
(2) less total expansion (7 mm); and (3) the sutural ex-pansion
evaluated in a more posterior region (posteriornasal spine) than in
our study (in the first molar re-gion). In our investigation, the
amounts of sutural
expansion (2.88 mm in the posterior and 4 mm inthe anterior
regions) were greater than the amounts
reported by Podesser et al30 (1.6 mm in the posteriorand 1.5 mm
in the anterior regions). This differencecould be explained by less
total expansion (7 mm)and the relapse that might have occurred
because of
appliance removal and replacement at the end of theactive phase
of RME for CT scan acquisition in their
study. In our investigations, there was no need to re-move the
appliances before the CBCT examination atT2 because of the lower
level of metal artifacts pro-
duced by CBCT compared with conventional CT.11,38
The greater amounts of expansion at the alveolarlevel (distances
3-4 and 19-20) than the sutural expan-sion (distances 11-12 and
21-22) (Table III) show the
bending of the alveolar processes of the maxilla; this re-sult
agrees with previous reports.20,28,30 The expansionat the alveolar
level (distance 3-4) accounted for 70%
of the total expansion, 36% of which representssutural expansion
and 34% is purely alveolar bendingtoward the buccal aspect.
The great changes in maxillary transverse dimensions
occurred at the dental level, where the expansion ac-counted for
97% (distance 7-8) of the total expansion
Table VI. Comparison between the changes in the maxillary
transverse planes in the groups
Variable
Haas group Hyrax group
P
T2-T1 T2-T1
Mean SE Mean SE
Skeletal
Distance 5-6 (mm)
Posterior apical base width 2.19 0.15 3.10 0.17 0.0002*
Distance 11-12 (mm)
Posterior midpalatal suture width 2.62 0.12 3.14 0.14 0.010*
Distance 15-16 (mm)
Anterior apical base width (inferior) 3.29 0.30 3.66 0.34
0.427
Distance 17-18 (mm)
Anterior apical base width (superior) 2.62 0.31 3.00 0.35
0.438
Distance 21-22 (mm)
Anterior midpalatal suture width 3.63 0.17 4.37 0.20 0.007*
Alveolar
Distance 3-4 (mm)
Posterior width at alveolar crest level 5.44 0.25 5.80 0.28
0.342Distance 19-20 (mm)
Anterior width at midalveolar level 4.03 0.30 4.76 0.34
0.119
Dental
Distance 7-8 (mm)
Intermolar width at occlusal surface 7.70 0.20 7.90 0.23
0.526
Distance 9-10 (mm)
Intermolar width at palatal root apices 2.15 0.18 3.14 0.21
0.0008*
Angle 1MD ()
Right first molar angulation 8.25 0.98 6.80 1.11 0.334
Angle 1ME ()
Left first molar angulation 6.14 0.90 6.19 1.02 0.975
*Statistically significant difference (P\0.05).
374 Weissheimer et al
September 2011 Vol 140 Issue 3 American Journal of Orthodontics
and Dentofacial Orthopedics
-
7/30/2019 efectos 6
10/11
(8 mm) (Table III). This greater expansion at the dental
level compared with the skeletal level agrees with previ-ous
reports.3,4,20,28,30,34,37 However, the actual dentalexpansion can
be found by subtracting the total
expansion at the dental level (distance 7-8) from thesuture and
alveolar expansions (distance 3-4). Thus,from 97% (7.8 mm) of the
total expansion at the
dental level (distance 7-8), only 27% (2.17 mm)represents actual
dental expansion, which was smallercompared with 36% (2.88 mm) of
pure skeletalexpansion (distance 11-12) and with 34% (2.75 mm)
of pure alveolar bending. RME produced significantbuccal tipping
of the first permanent molars,
accounting for 7.53 (angle 1MD) on the right side
and 6.17 (angle 1ME) on the left side (Table III). Therewere no
statistically significant differences between the2 groups in
angular measurements. The amounts of buc-cal tipping of the first
permanent molars for the Haas
group were 8.25 on the right side (angle 1MD) and6.14 on the
left side (angle 1ME), whereas, in the hyraxgroup, the tipping
amounts were 6.80 on the right and6.19 on the left sides. However,
there was a statisticallysignificant difference between the Haas
and hyraxgroups in the linear measurement (distance 9-10),
which
represents the distance between the apices of the palatalroots
of the first permanent molars. The higher values fordistance 9-10
(nearly 8 mm of expansion) reflecteda small buccal tipping of the
first molars. In the hyraxgroup, distance 9-10 increased by 3.14
mm, whereas,
in the Haas group, there was an increase of 2.15 mm,showing
greater tipping of the first permanent molars
with that expander (Table VI). Similar results were re-ported in
other investigations.28-37 In the study ofGarib et al,28 the
Haas-type expander produced greater
buccal tipping of the first permanent molars (3.5)
than did the hyrax-type expander (1.6). Oliveiraet al37 found
that the Haas-type expander produced
greater buccal tipping of the first permanent molars(7.12 right
side, 6.64 left side) compared with the
Hyrax-type expander (6.94 right side, 1.21 left side).However,
these differences were not considered statisti-
cally significant in either study.We assessed the immediate
effects of RME; therefore,
long-term evaluation is necessary for a better under-standing of
the differences between Haas-type andhyrax-type expanders,
especially during the retentionand postretention phases of RME.
CONCLUSIONS
Based on this clinical trial with CBCT to assess theimmediate
effects of RME on the transverse plane with2 kinds of palatal
expanders, the following conclusionscan be drawn:
1. RME produced significant increases in all maxil-lary
transverse dimensions. The expansion pattern
was triangular, with smaller effects at the skeletal
level than at the dental level. However, the pure
skeletal expansion was greater than actual dentalexpansion. The
sutural expansion showed a wedgeshape with the wide base in the
anterior maxilla.
2. The opening of the midpalatal suture accountedfor 50% of the
total expansion (8 mm) in the
anterior region and 36% in the posterior region(there was a
decrease from anterior to posterior).
3. The hyrax-type expander produced greater orthope-dic effects
in 3 of the 5 skeletal points measured
compared with the Haas-type expander. However,the effects were
less than 0.5 mm per side and might
not be clinically significant.
REFERENCES
1. Angell EH. Treatment of irregularities of the permanent or
adult
tooth. Dent Cosmos 1860:540-4, 599-601.
2. Haas AJ.Rapid expansionof themaxillarydentalarch and
nasalcav-
ity by opening the midpalatal suture. Angle Orthod
1961;31:73-90.
3. Haas AJ. The treatment of maxillary deficiency by opening
the
midpalatal suture. Angle Orthod 1965;35:200-17.
4. Haas AJ. Palatal expansion: just the beginning of
dentofacial
orthopedics. Am J Orthod 1970;57:219-55.
5. Haas AJ. Long-term posttreatment evaluation of rapid
maxillary
expansion. Angle Orthod 1980;50:189-217.
6. Biederman W. A hygienic appliance for rapid expansion. J
Clin
Orthod 1968;2:67-70.7. Siqueira D, Almeida R, HenriquesJ.
Frontal cephalometric compar-
ativestudyof dentoskeletal effects producedby three types of
max-
illary expanders. Rev Dent Press Ortodon Ortop Facial
2002;7:
27-47.
8. Chung CH, Font B. Skeletal and dental changes in the
sagittal,
vertical, and transverse dimensions after rapid palatal
expansion.
Am J Orthod Dentofacial Orthop 2004;126:569-75.
9. Sandikciolu M, Hazar S. Skeletal anddental changes after
maxillary
expansion in the mixed dentition. Am J Orthod Dentofacial
Orthop
1997;111:321-7.
10. Timms DJ, Preston CB, Daly PF. A computed tomographic
assess-
ment of maxillary movement induced by rapid expansiona pilot
study. Eur J Orthod 1982;4:123-7.
11. Scarfe WC, Farman AG, Sukovic P. Clinical applications
of
cone-beam computed tomography in dental practice. J Can
DentAssoc 2006;72:75-80.
12. Lagravere MO, Carey J, Toogood RW, Major PW.
Three-dimen-
sional accuracy of measurements made with software on
cone-beam computed tomography images. Am J Orthod Dentofa-
cial Orthop 2008;134:112-6.
13. Mozzo P, Procacci C, Tacconi A, Tinazzi Martini P,
Bergamo
Andreis IA.A newvolumetric CT machine for dental imaging
based
on the cone-beam technique: preliminary results.
EurRadiol1998;
8:1558-64.
14. Hilgers ML, Scarfe WC, Scheetz JP, Farman AG. Accuracy of
linear
temporomandibular joint measurements with cone beam com-
puted tomography and digital cephalometric radiography. Am J
Orthod Dentofacial Orthop 2005;128:803-11.
Weissheimer et al 375
American Journal of Orthodontics and Dentofacial Orthopedics
September 2011 Vol 140 Issue 3
-
7/30/2019 efectos 6
11/11
15. Misch KA, Yi ES, Sarment DP. Accuracy of cone beam
computed
tomography for periodontal defect measurements. J
Periodontol
2006;77:1261-6.
16. Nakajima A, Sameshima GT, Arai Y, Homme Y, Shimizu N,
Dougherty H Sr. Two- and three-dimensional orthodontic
imaging
using limited cone beam-computed tomography. Angle
Orthod2005;75:895-903.
17. Walker L, Enciso R, Mah J. Three-dimensional localization
of
maxillary canines with cone-beam computed tomography. Am J
Orthod Dentofacial Orthop 2005;128:418-23.
18. Hamada Y, Kondoh T, Noguchi K. Application of limited
cone
beam computed tomography to clinical assessment of alveolar
bone grafting: a preliminary report. Cleft Palate Craniofac
J
2005;42:128-37.
19. Poggio PM, Incorvati C, VeloS, Carano A. Safe zones: a guide
for
miniscrew positioning in the maxillary and mandibular arch.
Angle
Orthod 2006;76:191-7.
20. Garrett BJ, Caruso JM, Rungcharassaeng K, Farrage JR, Kim
JS,
Taylor GD. Skeletal effects to the maxilla after rapid
maxillary
expansion assessed with cone-beam computed tomography. Am
J Orthod Dentofacial Orthop 2008;134:8.e1-11.21. Broadbent BH. A
new x-ray technique and its application to ortho-
dontia. Angle Orthod 1931;1:45-66.
22. Sandikciolu M, Hazar S. Skeletal and dental changes after
maxil-
lary expansion in the mixed dentition. Am J Orthod
Dentofacial
Orthop 1997;111:321-7.
23. Ahlqvist J, Eliasson S, Welander U. The effect of projection
errors
on cephalometric length measurements. Eur J Orthod 1986;8:
141-8.
24. Ahlqvist J, Eliasson S, Welander U. The effect of projection
errors
on angular measurements in cephalometry. Eur J Orthod 1988;
10:353-61.
25. Hatcher DC, Aboudara CL. Diagnosis goes digital. Am J
Orthod
Dentofacial Orthop 2004;125:512-5.
26. Ludlow JB,Ivanovic M. Comparative dosimetry of dentalCBCT
de-
vices and 64-slice CT for oral and maxillofacial radiology. Oral
Surg
Oral Med Oral Pathol Oral Radiol Endod 2008;106:106-14.
27. Garib DG, Henriques JF, Janson G, de Freitas MR, Fernandes
AY.
Periodontal effects of rapid maxillary expansion with
tooth-tissue-borne and tooth-borne expanders: a computed
tomography evaluation. Am J Orthod Dentofacial Orthop 2006;
129:749-58.
28. Garib DG, Henriques JFC, Janson G, Freitas MR, Coelho RA.
Rapid
maxillary expansiontooth tissue-borne versus tooth-borne
expanders: a computed tomography evaluation of dentoskeletal
effects. Angle Orthod 2005;75:548-57.29. Lione R, Ballanti F,
Franchi L, Baccetti T, Cozza P. Treatment and
posttreatment skeletal effects of rapid maxillary expansion
studied
with low-dose computed tomography in growing subjects. Am J
Orthod Dentofacial Orthop 2008;134:389-92.
30. Podesser B, Williams S, Crismani AG, Bantleon HP. Evaluation
of
the effects of rapid maxillary expansion in growing children
using
computer tomography scanning: a pilot study. Eur J Orthod
2007;
29:37-44.
31. Habersack K, Karoglan A, Sommer B, Benner KU.
High-resolution
multislice computerized tomography with multiplanar and
3-dimensional reformation imaging in rapid palatal
expansion.
Am J Orthod Dentofacial Orthop 2007;131:776-81.
32. Ballanti F, Lione R, Fanucci E, Franchi L, Baccetti T, Cozza
P. Im-
mediate and post-retention effects of rapid maxillary
expansion
investigated by computed tomography in growing patients.
AngleOrthod 2009;79:24-9.
33. Rungcharassaeng K, Caruso JM, Kan JYK, Kim J, Taylor G.
Factors
affecting buccal bone changes of maxillary posterior teeth
after
rapid maxillary expansion. Am J Orthod Dentofacial Orthop
2007;132:428.e1-8.
34. Lagravere MO, Heo G, Major PW, Flores-Mir C. Meta-analysis
of
immediate changes with rapid maxillary expansion treatment.
J Am Dent Assoc 2006;137:44-53.
35. Bishara SE, Stanley RN. Maxillary expansion: clinical
implications.
Am J Orthod Dentofacial Orthop 1987;91:3-14.
36. Braun S, Bottrel JA,Lee KG,Lunazzi JJ,LeganHL.
Thebiomechan-
ics of rapid maxillary sutural expansion. Am J Orthod
Dentofacial
Orthop 2000;118:257-61.
37. Oliveira NL,Da Silveira AC,Kusnoto B, Viana G.
Three-dimensional
assessment of morphologic changes of the maxilla: a
comparison
of 2 kinds of palatal expanders. Am J Orthod Dentofacial
Orthop
2004;126:354-62.
38. Cohnen M, Kemper J, Mobes O, Pawelzik J, Modder U.
Radiation
dose in dental radiology. Eur Radiol 2002;12:634-7.
376 Weissheimer et al