Embed Size (px)
Citation preview

ONLINE ONLY
Engineered cartilage heals skull defects
Lan Doan, Connor Kelley, Heather Luong, Jeryl English, Hector Gomez, Evan Johnson, Dianna Cody,
and Pauline Jackie Duke
Houston, Tex
Introduction: The purposes of this study were todifferentiate embryonic limb bud cells into cartilage,characterize the nodules produced, and determine theirability to heal a mouse skull defect.
Methods: Aggregated mouse limb bud cells (E12-E12.5), cultured in a bioreactor for 3 weeks, were ana-lyzed by histology or implanted in 6 skull defects. Sixcontrols had no implants. The mice were scanned withmicrocomputed tomography weekly. At 2 and 4 weeks,a mouse from each group was killed, and the defectregion was prepared for histology.
Results: Chondrocytes in nodules were mainly hy-pertrophic. About 90% of the nodules mineralized.BrdU staining showed dividing cells in the perichon-drium. Microcomputed tomography scans showed in-creasing mineral in implanted nodules that completelyfilled the defect by 6 weeks; defects in the controlmice were not healed by then. At 2 and 4 weeks, the con-trol skull sections showed only a thin bony layer overthe defect. At 2 weeks, bone and cartilage filled thedefects with implants, and the implants were wellintegrated with the adjacent cortical bone. At 4 weeks,the implant had turned almost entirely into bone.
Conclusions: Cartilage differentiated in the biore-actor and facilitated healing when implanted into a de-fect. Engineering cartilage to replace bone is analternative to current methods of bone grafting.
Read the full text online at: www.ajodo.org,pages 162.e1-162.e9.
Am J Orthod Dentofacial Orthop 2010;137:162-3
0889-5406/$36.00
Copyright � 2010 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2009.10.001
162
EDITOR’S SUMMARY
Reasons for autogenous bone grafting are now al-most too numerous to mention. In the final stages oftreating cleft lip and palate patients, grafts might beneeded in the cleft area before the placement of im-plants, or to close an oronasal fistula, for proper bonysupport next to the cleft, or even for increased supportfor the alar base. In implant dentistry, ridge augmenta-tion is frequently needed to improve the functionaland esthetic outcome of the implant. In other patients,a deficient alveolar ridge can affect phonetics and es-thetics. I could go on, but why? You would think thisstudy was as important as stem cell research. Well,that’s what it’s all about. This study confirms previousresults showing that engineered bone-forming cartilageis an excellent way to heal even membranous bone.
These authors investigated using in-vitro-differenti-ated cartilage—the bone-forming kind—to facilitate thehealing of skull defects in mice. The aim was to assesshistologically the stage and amount of cartilage pro-duced after 3 weeks of culture. This was evaluatedwith microcomputed tomography scanning and histol-ogy, noting the ability of cartilaginous spheroids usedto heal a defect in a membranous bone. The authors con-cluded that engineering cartilage could be an alternativemethod to repair the defect of a membranous bone.
The details of the study are published online andwill be of special interest to those with a backgroundin histology. Noted the authors, ‘‘Human bone-marrowstem cells will be used next to form cartilage in culture,so that we can proceed toward the goal of providing im-plants to patients constructed from their own stemcells.’’ With this type of basic research in our universi-ties, the future looks a little brighter.

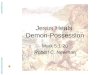
Fig 1. Left, section of cartilage nodule stained with the von Kossa method; right, overlay showinghow the area of mineralization was calculated.
American Journal of Orthodontics and Dentofacial Orthopedics Doan et al 163Volume 137, Number 2
Q & ATurpin: Your approach to tissue engineering hasbeen called ‘‘a change in paradigm.’’ Why?
Doan: The current paradigm for engineering boneis to use bone cells and a scaffold, with addedgrowth factors. We use cartilage cells that maketheir own scaffolding and growth factors, which in-tegrate extremely well into the surrounding boneand are totally replaced during the endochondralprocess.
Turpin: This was the topic of your master’s degreethesis. How do you plan to make use of this researchexperience in the future?
Doan: My part of this project was to show that mes-enchymal cells differentiated into cartilage can healbone. The next step in the laboratory will be to differ-entiate human bone-marrow stem cells into cartilage.The research project will have broad implications;
the ability to repair bony defects in humans with theirown cells will change dentistry.
Turpin: Do you see the use of human stem cellsbecoming commonplace in craniofacial treatmentyears from now?
Doan: With the positive results of our project and thecurrent advances in stem-cell research, the possibil-ity of using them to replace bone in craniofacialfacial defects is promising. And it will not be somany years from now.
Turpin: Is the public cognizant of the varied rolesorthodontists play in the overall care of craniofacialpatients?
Doan: The public, for the most part, is probablyunaware that orthodontists are important membersof craniofacial teams that treat patients with cranio-facial defects.