Embed Size (px)
Citation preview

ED 034 877
AUTHORTITLE
INSTTTUTIONSPONS AGENCY
BUREAU NOPUB DATECONTRACTNOTE
EDRS PRICEDESCRIPTORS
IDENTIFIERS
ABSTRACT
DOCUMENT RESUME
24 VT 009 931
Colgan, Francis E.; And OthersHealth Occupations Curriculum Development: In Searchof A More Powerful Curriculum.Rocky Mountain Educational Lab., Inc., Greeley, Colo.Office of Education (DHEW) , Washington, D.C. Bureauof Research.BR-6-2828Aug 69OEC-4-7-062828-30-6370n.
EDRS Price MF-$0.50 HC-T3.60Core Curriculum, *Curriculum Development, *EntryWorkers, Grade 11, Health Education, HealthOccupations, *Health Occupations Education,Occupational Information, Occupational Mobility,*Program Development, Questionnaires, Rural Schools,Task AnalysisRMEL, Rocky Mountain Educational Laboratory
The Pocky Mountain Educational Laboratory (PMEL)Health Occupations Curriculum project was initially structured toprovide broad exploratory activities for the total student body, anelective course, orientation to employment, and work entry experiencein the 11th and 12th grades. It was expected that the project wouldprovide a prototype for rural school systems which would betransferable to the urban setting and to other occupational clusters.This paper deals only with the activities and experiences associatedwith the 11th grade health occupations curriculum development, in thehope that other educational agencies might reduce their planningeffort through utilization of the RMEL experience. The appendixincludes a sample questionnaire consisting of performance elements tobe checked in terms of importance and the setting appropriate forteaching of the element by 11th grade teachers, the healthoccupations teacher-coordinator, health services-administrators,supervisors, and job incumbents. (JK)

I
/3 X-6- '2.E" 24'
PA 2P' Y
Pei/64
HEALTH OCCUPATIONS CURRICULUM DEVELOPMENT:
IN SEARCH OF A MORE POWERFUL CURRICULUM
Prepared by .
Dr. Francis E. ColganProgram Specialist
Ocupational EducationRocky Mountain Educational Laboratory
Assisted by
Larry L. HorynaPogram Assistant
Mr. Robert RussellProgram Assistant
Dr. Willard G. JonesExecutive Director
-1,
Prepared pursuant to a contract with the United States Officeof Education, Bureu of Research, H.E.W.Contract No. OEC-4-062828-30-63
August, 1969
ROCKY MOUNTAIN EDUCATIONAL LABORATORY1620 Reservoir Road
Greeley, Colorado 80631
U.S. DEPARTMENT OF HEALTH, EDUCATION & WELFARE
OFFICE OF EDUCATION
THIS DOCUMENT HAS BEEN REPRODUCED EXACTLY AS RECEIVED FROM THE
PERSON OR ORGANIZATION ORIGINATING IT. POINTS OF VIEW OR OPINIONS
STATED DO NOT NECESSARILY REPRESENT OFFICIAL OFFICE OF EDUCATION
POSITION OR POLICY.

bi
PREFACE
The problems associated with delivering health care services are compounded by lack offiscal resources, failure to reach across discipline lines and failure to establish a usefuldialogue among agency personnel to reach a solution to a national problem. Further, theproblem is so obvious and so large that we must abandon inter and intra institutional andagency squabbles regarding licensing and professional standards and get on to thedevelopment of a sound pattern basic to good teaching that will deliver a career initiate whowill only need finishing in the field to be of great value in the Health services industry.Then, instead of neglecting the trainee, the professions, clinics, and health service agencies,in general, just might out-do each other in seeking the product.
The RMEL Health Occupations Curriculum was initially structured to provide total studentbody exposure for 11 th grade students; treatment of special knowledge in an 11th gradeelective course; and orientation to employment in the health services industry throughcooperation with clinical affiliates. The second year of the program included continuing11th grade activities while adding work entry experience for 12th grade students. Theelective classes and the work entry experience would be coordinated by employment of aHealth Occupation s teacher-coordinator. The third year of the project would permit acritical analysis of product, process and change-support systems.
)r It was expected that this project would provide a prototype for the establishment of a highschool level health occupations program for rural school systems and their healthcommunities; and that the program products would be transferrable to the urban setting. Itwas also anticipated that the procedures used in deriving appropriate curricula for healthwould be applicable to other occupational clusters, i.e., mechanical, business, and service.
This paper deals only with the activities and experiences associated with the 1 1 th gradehealth occupations curricieurn development.

ACKNOWLEDGEMENT
Health Occupations Curriculum Development is one of a series of information analysispapers developed and released by the Rocky Mountain Educational Laboratory, Inc.,Greeley, Colorado.
In this paper we are indebted to pioneers in cluster analysis, directors for health occupationsand the numerous educators who have read early drafts and offered constructive criticism.

11
TABLE OF CONTENTS
PREFACE. i
CURRICULUM DEVELOPMENT HEALTH SERVICE OCCUPATIONS - INTRODUCTION. 1
THE NEED TO REVITALIZE VOCATIONAL EDUCATION 6
RATIONALE. 10
RECRUITMENT. 12
OCCUPATIONAL CURRICULUM PRINCIPLES. 13
CURRICULUM STRUCTURE. 13
HEALTH EDUCATION. 14
BASELINE DATA. 18
JOBS, FUNCTIONS AND ASSIGNMENT Or CONTENT 21
SUMMARY 25
CURRICULAR PREVIEW 29
SUGGESTED UNITS OF CONCENTRATION 30
THE ACCIDENT VICTIM (AN EXAMPLE). 31/32
IMPLEMENTATION. 33
SELECTED TOP-PRIORITY SCHOOL SETTINGS 34
PERSONNEL TRAINING. 36
PROGRAM MONITORING AND EVALUATION. 37
PROJECTED COSTS. 39
HEALTH OCCUPATIONS CURRICULUM PROGRAM 39Health Occupations CurriculumFirst year Grade 11. 41
Self - Evaluation. 42
Problems. 42
Surprises. 42
Discoveries. 43

.t r
ILLUSTRATIONS
Figure Page1 Health Occupations Program-Rural Setting 3
2 Opportunties at all Levels of Ability 11
3 An Ecologic Model of Health and Disease 16
4 The Health Grid, Its Axes and Quadrants. 17
5 Training Opportunities Authorized for "Health Occupations" 20
6 Career Mobility within the Health Occupations. 22
7 The Core Program 26
8 Program Description. 40

:I 7
VF/041.P.40711WWP et 63 mem%
CURRICULUM DEVELOPMENTHEALTH SERVICE OCCUPATIONS
Introduction
The purpose of this paper is to report the results of the work of the staff of the RockyMountain Educational Laboratory on the Health Occupation Curriculum project. Thisproject was the second phase of a three phase occupational education project which was oneof two programs of the laboratory.
The demise of the laboratory pit.% ',RAI implementation of the occupational educationproject as planned for Fall, 1969. Much effort was expended during the 1968-69 school yearin formulating the HOC project. Although the project will not be implemented by thelaboratory, the staff of RMEL feels a professional responsibility to report to the educationalcommunity the progress of the project through the planning stage. The results of theresearch, the discussions, the conceptualizing, and the dreaming that occurred during theplanning year are such that educational agencies which might be considering instituting aHealth Occupations program might well benefit from studying them. Furthermore, the stafffeels that the content of this report may reduce the planning effort required by theseagencies since they will not have to conduct their own search for some of the information.
Obviously this report does not offer empirical evidence on the usefulness of the proposedHealth aOccupations Curriculum. An attempt is made, however, to present the evidence thatwas considered in making the planning decisions. The reader may weigh the evidencedifferently and may arrive at different conclusions. Our purpose with this report is not toargue that the evolved plan is the correct plan. Rather our purpose is to present for thereader's consideration the plan and its rationale.
As indicated above the,,Health Occupations Curriculum project was the second phase of athree phase occupational education project of RMEL. The first phase of the project wasimplemented in the fall of 1968. The first phase was concerned with experimenting withprocedures for teaching youngsters of junior high school age methods and techniques forexploring the world of work. This phase, called " I.mage of the World ofWork ", was directedat the often cited problem that youth are not receiving adequate occupational informationand that they hold poor attitudes toward work. The activities were based on the assumptionthat it is more useful to teach youth methods and techniques for studying all occupationsthan to provide information about a limited number of specific occupations.
The second phase..of the occupational education project was intended to be a demonstrationtype activity. The laboratory intended to develop and implement a vocational programbased on the job cluster concept at the secondary level. This report as a presentation of theresults of the planning for the second phase.
The third phase, which was still in a preliminary planning stage, was intended to involveexperimentation with procedures for assisting individuals in the transition from school tothe world of work. The remainder of this report deals only with phase two.

2
Certain decisions were made early in the planning for phase two. First it was decided thatthe activity to be demonstrated would be a bona fide vocational program. That is, it wasdecided that, whatever the content of the program, it would be one such that it wouldprovide the participants with the knowledge, skills, and attitudes necessary for satisfactoryperformance of a job at th3 entry level of a career ladder. Further, it was intended that theprogram would meet requhements of the state plan for vocational education. The rationalefor these decisions was simply that acceptance of the program by the educationalcommunity would be dependent upon whether the program adhered to certain acceptedstandards of the educational community.
A second decision made early in the planning stage was tha t the vocational program wouldbe designed to incorporate some notions of the job cluster concept. Organizing vocationalprograms around job clusters seems to be sound on an intuitive basis. The job clusterapproach, by definition, would be designed to prepare the participant with the prerequisitesfor entering a number of occupations rather than a single occupation, and thus would openup a wider variety of career possibilities. In this time of rapid job change, such a program,ifeffective, would be desirable. Furthermore, a number of investigations have demonstratedon an empirical basis that job clusters which appear to have curricular relevance can beestablished. (See for example Sjogren and Sahl, 1966; Asbell, 1967; Morrison, 1966;Rahmlow and Winchell, 1965; Frautz, 19f 6; Sjogren, Schroeder, and Sahl, 1967; Courtney,1965. These studies are listed in "Empirical Basis for Job Clusters".
Although the cluster approach seems rational, there are some problems with the approachthat were recognized by the staff and which influenced decisions. Sjogren (1969) in a paperdelivered to AERA pointed out that there is no commonly accepted criterion forestablishing job cluster. Thus, with a criterion such as common tasks, the clusters wouldprobably form on the basis of similar jobs across industrial categories. For example, thisapproach would tend to form clusters like clerical or selling across many businesses orindustries. On the other hand, a knowledge criterion might influence the clusters to formwithin industries across job titles. For example, jobs in the health services area would clustertogether on the basis of commoik it,lowledge of terms and practices in the health servicesand clerks, service workers, etc, within the health field would cluster together.
A second problem with the cluster approach is that there is no evidence that a curriculumbased on the cluster approach would in fact be any more "powerful" than a curriculumdesigned to train for a single occupation. Certainly the yearnings from a single occupationcurriculum would be generalizable to other occupath, and it is probably accurate to thinkthat there would not be great observable differences th:zween a cluster curriculum and acurriculum for a single occupation within the cluster. On the other hand, a curriculumplanned on the basis of a cluster would seemingly be designed to optimize commonalitieswhereas the commonalities among skills from a single occupation curriculum wouldprobably occur by chance with little overt attempt to effect the possible transfers.
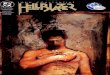
Recognition of problems does not mean solution, and these problems were not solved.However, an attempt was made to accommodate the recognized problems in decisions. Thisis illustrated in Figure 1. With respect to the criterion for clustering question, it was decidedthat no single criterion was optimal for all situations, but that the criterion should beappropriate to the context of and the resources available in the situation. Because thelaboratory was in a predominantly rural region, it was considered important that thedemonstration program be appropriate to schools in rural communities. Employmentpatterns in rural communities are generally such that there are few people employed underany single job title or similar job title. Furthermore, many people perform such a variety oftasks on their job that in a more highly specialized setting their job tasks would beperformed by a number of people with different job titles. For example, a clerk in a small

3
Figure 1
Health Occupations Program-Rural Setting
Limitations of Rural Setting
Limitations of InstructionalResources.Limitations of Student's firsthand experiences with healthoccupations.Limitations of health servicesoccupations instructionalpersonnel.
Strategy Program
Health occupations contextmaterial placed withappropriate 11th gradeteachers.
Health professions teacher-coordinator for elective11th grade course.
Health services facilityresources.
Instructional methodologiesand materials.
Strategies
Design a consortium of specialinterest, consultative andeducational personnel.Build pool of resource personnelfrom health professionalorganizations.Conduct orientation, training andinservice sessions.
Aid, encouragement, information,assistance with instruction-specialprojects, etc.
Identification of additionallearnings for integration andcorrelation.
Observations-experience-advice tomaintain relevance of learnings.
Vicarious clinical experiences.
Assistance with pqpil experiences,individualized actIvity schedulesand work experiences.
Special requirements individualizedinstruction.

4
retail store may sell, take inventory, maintain stocks, and keep the accounts. In a largerstore each of these functions would probably be performed by a different person with adistinct job title. Because of the relatively small number of similar jobs and theaccompanying scarcity of resource persons, it was decided that a vocational program basedon a cluster concept in a school in a rural setting could be established more readily if thecluster were based on a common knowledge criterion, i.e. an industry cluster, than on acommon tasks criterion, i.e. an occupations cluster.
With respect to the second problem cited a hove, it seemed not important whether curriculabased on a single occupation or on clusters appear very different in content. The intent ofthe curricula is important and if the objective that it be generalizable is consideredimportant (we believe it is) then such an objective should be provided for in the curricula. Itwould seem reasonable to assume that curricula based on clusters would be more likely toprovide for fusion of commonality among several occupations.
The next decision faced in the planning of phase two was that of deciding on the content ofthe vocational program. Several factors were considered in arriving at the decision todevelop the program as a Health Occupations Education Program. Among the factors werethe following:
1. The program should prepare participants for job entry into jobs that areavailable both in the immediate geographic area of the school as well asin areas to which the graduate would migrate.
2. The program should provide for jobs at an entry level leading to welldefined career ladders.
3. There should be available agencies in the immediate geographic area tothe schools that are appropriate for and are willing to provide clinical orcooperative work experiences for the participants.
4. Qualified health occupations teacher-coordinators would need to beperpared to guide the program
5. The program should have minimal duplication with existing programs.
6. The program should be in a field in which there are job opportunities atall occupational levels from semi-skilled to professional.
7. The program should provide a guidance function as well as a jobpreparation function.
8. The program should not impose an undue burden on the resources of thecommunity.
The Health Occupations area was adopted on the basis of the following information thatwas accumulated on the factors cited above. First, jobs are available in health occupations atall occupational levels and in rural areas. It has been estimated that 10,000 new jobs areavailable each month in the health services field, and this rate of growth has been projectedthrough 1978, Furthermore, these jobs occur at all levels with about half being at theprofessional and technical level and the other half being jobs of the service worker, clerical,aide, or other skilled and semi-skilled nature. These estimates are based on nationwide data,but a survey of the eight-state RMEL region indicated a situation within these states similarto the national picture.
Secondly, health service agencies of various sorts, hospitals, nursing homes, children'shomes, clinical, etc., are present in rural areas and offer practical possibilities for clinical or

5
cooperative work experience situations. The staff of these agencies constitute a potentialpool of resource persons for the program. Furthermore, there arc jobs at every level in thehealth services so that even though career ladder patterns are not yet well-defined, it is likelythat such definition will not require a great amount of effort. Because of the fact that thereare health occupations that can be quite clearly distinguished by level, it seemed reasonableto conclude that a health occupations program could be designed to serve a guidancefunction as well as a vocational function.
Fourth, a health occupations program would be a unique program at the secondary level.Health occupation education programs at the secondary level are practically non-existentdespite the fact that such occupations exist in nearly all communities and the number ofsuch occupations is increasing. Thus, the proposed program would not duplicate existingprograms.
Finally, on the positive side, a health occupations program would not require large outlaysfor facilities and capital equipment so that it would not be likely to impose an unduefinancial burden on a school system.
There were also some factors that weighed against the health occupations curriculum.Among these was the question of the availability of qualified teachers. Few data areavailable on this point because there are few programs. Furthermore, one should not be toooptimistic about expecting that the establishment of programs will lead to an adequatesupply_of teachers because of the general shortage of health occupations workers. On theother hand, there is a fairly sizable number of married women at home with experience inhealth occupations who could be recruited into teaching in such a program since 300,000trained nurses are, not publicly practicing skills with which they were prepared. Thisexpectation seems reasonable even in rural areas. In general, teacher availability wasregarded as a negative factor with respect to the decision, but also as a problem that couldbe solved.
Another negative factor was the recognition of the rigidity of certain licensing andcertification practices established by legislation or by professional standards. For example,some states set minimum and maximum age limits for entrance into training for certainhealth occupations. The reason for minimum limits has been an attempt to assure maturityand quality of the personnel, while the rationale for the maximum limits has probably beeneconomic in nature. As the health manpower field faces the shortages of personnel andrealizes the dramatic advances made in educational methods, a reevaluation of certainlicensing and certification requirements will 1 ikely occur. Until that happens, however, theeffectiveness of the program may well be hampered by these restrictions. It was intendedthat if the program as it developed were in conflict with licensing or certificationrequirements an attempt would be made to so 1 icit cooperation in relaxing the requirementsfor the experimental or demonstration period. This had not yet been attempted with anyagency, however.
The relatively low rate of pay of many health occupations, especially those at the entrylevel, was another negative factor. The low pay rates in these occupations somewhat n gatesthe argument that there is a shortage of workers. On a purely economic criterion, if therewere a true shortage then the pay rates would rise. The pay rates are so low in manysituations that provision of training is not economical. The payoff to the individual andsociety for the cost of the training will not be justified. Furthermore, there is even a dangerthat training may make the person less employable in the sense that the health serviceagency will not hire the trained person at a higher pay if they can get an untrained person atless pay. It would seem likely, however, that the increased pressure om. health serviceagencies and the accompanying pressures for their operation to be both effective and

:Er
6
efficient, that the agencies cannot operate with their present personnel policies. Theturnover rate in many health occupations is appalling and the reason for this, apparently, isthat the agencies are operating under a false economy. They must necessarily be sacrificing
. efficiency and probably effectiveness in order to effect lower short term dollar costs.Ultimately the health service agencies must realize, as most other segments of economy havealready realized, that investment in human capital is a wise investment. Thus, it is ourexpectation that personnel practices in health service agencies must necessarily change in thenear future, and the change will be such that investment in training will be economicallysound.
Considering all of the indicated factors, it seemed to the staff of RMEL that the decision todevelop a demonstration Health Occupations Education Project for rural secondary schoolsas the second phase of the occupations project was well justified. Accordingly, the staffproceeded to work on planning the curriculum and the procedures for implementing theproject. The remainder of this report describes these activities.
The Need to Revitalize Vocational Education
"America's manpower problems are difficult to solve partly because of the nature ofprojected changes in the labor force, partly because of the level of unemployment and itsuneven distribution in our economy, partly because of the combination of rapid shifts inparts of employment and increasing barriers to labor mobility and partly because of thecomplications of the country's size and its federal, state, and local political structure."(1:10-11) A series of attempts by the federal Congress dating back to the early 1900's havetaken the form of direct appropriations for specific labor force categories through whichstate departments and local vocational educators were to prepare people for employment.Under the Vocational Act of 1963 an extra attempt at evaluating the progress made towardthis important national goal took the form of an Advisory Council on VocationalEducation, which was appointed in 1966, and submitted this report in January of 1968.During the Second Session of the 90th Congress, the General Sub-Committee on Educationconducted twenty-five days of public hearings on amendments to the Vocational Act of1963. In summary, the Advisory Council recommended that the following five tenetsdeserve serious consideration:
1. The dichotomy between academic and vocational education isoutmoded.
2. Developing attitudes, basic educational skills, and habits appropriate forthe world of work are as important as skill training.
_ 3. Pre-vocational orientation is necessary to introduce pupils to the worldof work and provide motivation.
- 4. Multiple career choices are the legitimate concern of vocationaleducation.
5. Vocational programs should be developmental, not terminal, providingmaximum options for students to go on to college, to pursuepost-secondary vocational and technical training or be placed inemployment. (2:203) ,
J

IIM ^
The Advisory Council further recommended that occupational preparation begin in theelementary school by providing a realistic picture of the world of work for those youth. Inthe high school, occupational preparation is recommended and should become more specificand not limited to one , vocation, taking the form of content and structured aroundsignificant families of occupational industries which promise expanding opportunities.(1:2-3)
In a report published in February, 1967, by the Institute for Research in Human Resourcesseveral recommendations are made regarding the role of the secondary school and thepreparation of youth for employment. (3:et al)
In summary, the role of the secondary school as viewed by the Institute is one in whichteachers of the school join as partners in order to reach the goal of full development ofhuman resources. This program as visualized by the Institute would take the form ofattitudinal and occupational information in-puts in the late elementary and early middleschool years; skill development built upon the family of occupations in industries forvocational proficiency development; and finally job placement based upon a consortiaarrangement with business, labor, industry, education and government.
A report by the Task Force on Vocational and Technical Education to the EducationalCommission of the States proposes that the community with all its resources must beinvolved as a context in which learning takes place. Thus the resources of a communityservice area are brought to bear on the opportunity for education which exists for eachindividual in that locale. Cooperation can then be demonstrated which signals thateducation is to be given first priority in the allocation of human and material resources. Theopportunities for pupils will be realized for sensible termination, re-entry, and advancementwill become a viable characteristic of the total educational mechanism. (4:et al)
In order to mobilize the forces for education which the task force recommends, it will benecessary that curriculum reorganization and development occur. The entire program ofstudies of the middle school will evolve into broad avenues of occupational education in thesenior high school. A significant part of the high school instruction may well take the formof basic preparation for clusters of closely related jobs. This part of the curriculum would bederived from analysis of common and basic elements of knowledge, skills, and behaviorsfound among the several jobs in the cluster, as well as the various courses in the curriculum.
In spite of the fact that from 1964 to 1966 total expenditures for vocational educationincreased about two and one-half times, federal grants to the states quadrupuled, and stateand local expenditures doubled, the nation is still faced with a sector of the labor force, agesixteen to nineteen, which seems to be unemployable. During that same period high schoolenrollments in occupational education still fall short of serving the numbers of young peoplewho should benefit from such a program. Only one high school student in four is enrolled invocational programs, although five of six never achieve a full college education. In shortapproximately 60 percent of high school students enter the world of work unprepared tohold a job. (1:2-3)
It is important for school administrators, parents, students, employers and the generalpublic to recognize the size of this group whose members have special needs. The potentialvalue and service which these young people could offer, if not developed, is a waste ofhuman resources. (5:9) Many of these youths have intelligence and interests which makethem capable of mastering the curriculum required to become highly skilled technicians.

10
aA'5
RIM
They appear to have rebelled at mastering the curriculum required to become highly skilledtechnicians. They appear to have rebelled at mastering the scholastic skills. This may be truefor several reasons: late maturity, under-developed interests in organized study, consuminginterest in work, hobbies, or other activities, or lack of opportunity to develop scholasticskills. Many of these students have not studied the required courses in science andmathematics because they did not know they needed them; they did not realize the courseswere important until it was too late to study them in high school; they considered thecourses unusually difficult and avoided them; they did not need them for career objectivesfor which they were preparing in high school; the school they attended did not offer thecourses or offered them for career objectives other than those for which students werepreparing in high school; the school they attended did not offer the courses or offered themin a schedule which made them impossible for the students to take.
Students with underdeveloped scholastic skills are not only unable to enroll in college leveltechnical training programs, but they are also unable to qualify for employment. An entryjob placement program is needed to help these post-high school students develop scholasticskills and offer them the courses they did not study in high school. With these they mayenter the technical or other specialized occupational programs at the college level.
At present only three out of every ten students who enter elementary school later enroll incollegiate programs, and only two of them graduate. Approximately four out of ten highschool graduates considered to be qualified to enter collegiate programs do not do so. (5:9)Many of these students may want to become technicians but have not studied enoughmathematics or science to permit them to enter a high quality technical program in the fieldof their choice, or they may not have had the opportunity to gain an occupationalinformation base which clearly outlines the opportunities available to them in the world ofwork. Thus the sixteen to nineteen year-old needs special consideration. This considerationshould take the form of general administrative policy, availability of federal support, use ofan advisory committee, selection, development and upgrading of required faculty, provisionfor counseling and advisory services to students and parents, required physical facilities suchas classrooms, learning laboratories, and manuals of instruction which cut across the generalcurricula. (5: 18)
From the viewpoint of manpower planning, training programs in occupationaleducation should be designed to serve a number of purposes:
1. They should aim to provide general and special training for theprofessions. Demands in the professions have been rising rapidly in thepast decades and promise to continue to rise.
2. There is a need for training facilities for white-collar occupations withmuch shorter periods of a special training a number of which(stenographer, practical nurse, laboratory technician, draftsman) seem tohave been in relatively short supply of personnel for some years in mostadvanced countries.
3. More adequate and accelerated training for skill-manual or artisan tradesis needed than is currently provided by scholarship schemes, and morework relevant programs are needed to facilitate the transition fromschool to the world of work.
4. Ready access to refresher and retraining programs is necessary to remedyjob obsolescence in an economy of rapidly changing job requirements.

9
5. Training is necessary for the educationally disadvantaged, especially asthey are frequently jobless. Basic education, vocational training,occupational education, each of these serve not only to qualify people.for jobs, but also to raise aspirations and self- respect, to lower barriersto hiring and advancement and to increase the range of a person'semployment possibilities.
6. In-service and/or on-the-job training is needed to adapt individuals tospecial requirements of jobs in particular work places and to preparethem for promotion. (10:154-55)
An obstacle to the reorganization of occupational education is, of course, location and staffof existing training facilities. For instance, rural area vocational training programs in publicschools have been largely or exclusively in agriculture. As a result, one-third of the federallyaided vocational classes in 1963, outside of home economics, were agricultural classes.Because farm employment has declined sharply since World War II and will continue to doso, such a high proportion of trainees for agriculture makes little economic sense, exceptwhere the farm training includes preparation for such employment as gardening,landscaping, farm machinery repair, etc. The movement of population, especially of youngpeople from rural areas to urban centers, has found them largely untrained for theoccupations available in metropolitan areas. Various studies analyzing the employment offormer vocational-agricultural students between 1918 and 1960 show that, at the time thestudies were made, only about one-third were employed in farming and an additionalone-twelfth in farm related occupations. (6:104) The lack of diversified training facilities inrural areas and small towns means that youngsters living in those areas are offered onlynarrow occupational training opportunities and face difficult problems of occupationalchoice and adjustment.
There was a time when sending a child to school for a given number of years was enough toprepare him for the future. This is no longer true.
There was a time when a young person could drop out of school, become employed, andlearn on the job fast enough to have a good future. This is no longer true.
There was a time when this Nation could fill its manpower needs by simple on-the-jobtraining. This is no longer true.
There was a time when "graduation" was thought to be the end of education. This is nolonger true.
There was a time when education did not relate to an individual's self-dignity and life work.This is no longer true.
We have long provided the "vocational" education for doctors, lawyers, engineers, andeducators. We must now recognize the need for an occupational education for everyone. Itis no longer possible or even desirable to separate education, especially education for theworld of work, from the basic problems of one's education for a work life. The VocationalEducation Amendments of 1968 authorize funds for programs that deal with the dilemmasfacing our Nation, its changing world of work, and the new needs of its people. (7:1)
In summary, research activity in the manpower field has previously been directed towardprograms for particular groups and temporary remedies rather than toward solutionsencompassing the nation's total work force. Therefore, the federal govenment in itsactivities in the area should provide the leadership in the coordination of manpower researchand research training.

I0
We do live in a job economy where less than 15 percent of the nation's work force are self-employed. The rest are, as Lester points out, jobholders and job seekers, with paidemployment supplying most of their income and occupying most of their time. Hence,preparing for work, securing employment and moving up the occupational ladder arematters of crucial importance to the American people (1:206-7)
Rationale
In preparing the amendments to the Vocational Act of 1963, the General Sub-Committeeon Education, reporting to the 90th Congress, 2nd Session, indicated that "the dichotomybetween occupational and general education is outmoded." It is then desirable to identifythe common learnings associated with occupations known to be available for entry jobplacement in order to establish a common curricular effort among teachers. It is no longerpossible to rely upon vocational curricula which are specific to a single job, but rather it isnecessary that curricula be designed to prepare a student to enter the world of work throughany one of a number of jobs in an occupational cluster.
As recently as 1966. 31 percent of all the vocational students were enrolled in homeeconomics, 21 percent in trades and industry, 20 percent in office occupations, 15 percentin agriculture, 7 percent in distributive occupations, 4 percent in technical occupations andPh percent in health occupations.
It is reported that 10,000 new jobs per month will be available in the health services fieldthrough 1978. An analysis of these projected entry job placement points reveals that 65percent of them are related to hospital and/or patient care tasks and of this 65 percent, 76percent, or 5,000 new jobs per month, require professional and technical skill and 24percent, or 1,500 new jobs per month, are at the service-aide level. The 10,000 new jobs permonth projected through 1978 do not include the upgrading and on-the-job trainingnecessary for people already employed who must be retreaded with new skills as the newtechnologies and team approach to medicine become a significant new configuration forhealth services. This opportunity for employment is dramatized in Figure 2.
The need for additional personnel in the health manpower field is being generated bypopulation growth, changing age composition, rising educational levels, increased awarenessof the importance , of health care, better financial capability to meet health needs, andwithin medicine itself, a greatly increased capability of medicine at its best for treating andcuring illness.
The fact that the health service industry is now the third largest segment of the total laborforce and is expected to become the largest sector by 1974 suggests a need on the part ofhigh school students for an awareness of the several opportunities for employment as well asthe varying levels of proficiency required for job success in the health occupations field.
The Rocky Mountain Educational Laboratory began to design a program for the ruralschool system that would have among its goals three objectives of high priority:
1. To develop young people's commitments to health careers by way ofrealistic educational experiences in health occupations.
2. To provide students with the guidance, background and education asprerequisites that would facilitate their entry into post-high schooltechnical and professional health programs.
C".

Figure 21 I
Opportunities at
all Levels of Ability

1.
3. To provide students with the knowledge and skills, including humanskills needed to enter the health occupations with an opportunity toascend the health career ladder.
Recruitment
Entrance requirements for health occupation training programs are in effect inventories ofjob entry behavioral characteristics. Existing educational processes are generated to produceterminal behavioral characteristics. The chief concern is, however, with the entry behaviorof students recruited to the educational process. Even when flexible appraisal of entrancerequirements is followed, recruitment of trainees remains difficult. In addition, risingterminal behavior expectations and lowered entry requirements place imponderable burdenson the educational process.
Many of the health occupations have minimum age limits set for entrance into training. Insome states for example, this is established legislatively through licensure and certification.Often professional groups establish minimum ages for entrance to training. The motivationof such groups has been that of assuring maturity and quality of personnel, thoughunfortunately the age requirement is frequently established for entrance into training ratherthan for qualification for certification, concern for patient care, or job entry. The rationalefor age limitation developed during a period when health education lacked sophisticationand when the burden of education fell almost entirely upon the clinical experience. As thehealth manpower field faces the shortages of personnel and realizes the dramatic advancesmade in educational methods outside of the clinical area, a re-evaluation of this rationale forage limitation in the training is dictated.
Throughout the nation, one can observe appalling rates of turnover in job categories listedunder the. health occupations suggesting that many of the people who are trained aredestined to have an extremely limited work experience. Since it is an obligation ofeducational personnel concerned with health to seek creative solutions to the turnoverproblem, an altering of the age limitation to permit earlier entry into the training may havethe effect of prolonging the work experience. The result could be the provision of greatereconomic benefits to the individual in the form of aggregate income and greater benefits tothe health field by reducing to a degree the turnover of personnel.
Another restriction upon recruitment is regulations regarding maximum age for entry intotraining. Today one can find programs which establish an upper age level for candidacy.Rationale for this requirement is questionable. Here, to provide more permanent relief f mturnover, the vast potential reservoir of older candidates suggests an opportunity to insertinto occupations workers who are mature, settled, and in need of the income for longerperiods of time.
There is an intangible aspect of allied health service which deserves consideration. Attentionshould be directed to the concerns other than pay received which are characteristic of jobsatisfaction. The health services are personal services requiring a high degree of humane skill.Personal records may result from the warm, human experiOnce gained through helpingpeople.
An article in Changing Times, the Kiplinger magazine, April, 1969, "Making Your Job PayMore Than Mere Money," provides a resume of research conducted by social scientists
12

13
regarding incentives and gratifications associated with jobs. The rank assigned to each is asfollows: ( I) security, (2) interesting work, (3) opportunity for advancement, (4)recognition, (5) working conditions, (6) wages, (7) supervision, (8) social aspects of the job,(9) opportunity to learn or use ideas, (10) hours, (11) case of job, and (12) fringe' benefits.This list of motivators which has been identified in various studies tends to place wages nearmid-point and places interesting work and opportunity for advancement higher on the list.
Recruitment in a short labor market is further hindered by obstacles dealing with entrancewhich require the applicant to be in the upper half of his class or have a grade average of Cor better. With such standards, recruitment is limited to the area where direct competitionexists for the attention of the college-bound student.
The curriculum which the potential recruit has pursued has tended to escalate. However, ananalysis of health occupations raises the question of whether or not numerous employmentopportunities require a formal one-year course in chemistry, biology or physics.Undoubtedly much of the critical course content could be taught in a health occupationscurriculum. Simply put, how many of the people available on today's labor market can meetor need to meet these prerequisites to become competent in numerous health occupations?Three years of mathematics may be desirable for entrance into some courses but manypupils might learn how to solve routine mathematical problems during their health trainingcourses without the benefit of or need for this, prerequisite.
Occupational Curriculum Principles
Use of the content presently available through local curriculum plus the allied healthmanpower context in each of the classrooms, would pave the way toward achieving thefollowing six principles for human resource development: (11 preparation for useful andgainful, satisfying occupations or employment should be one of the objectives of theeducation of all youth; (2) certain facts, concepts, skills, attitudes, and processes ofvocational-occupational education arc relevant to all education and should be experiencedby pupils at every educational level; (3) education for specific vocational competence shouldprovide for built-in versatility and flexibility to assure that students acquire understandings,knowledge, skills, including humane skills, that are transferable in a changing technology;(5) vocational-occupational education should be considered a part of the entire process ofeducation and therefore should be concerned with all the capacities of an individual:intellectual, manipulative, social, and creative; (6) education in school can at best provideonly part of the total vocational competence of an individual which shortens and makesmore effective pre-job and on-the-job education by the employer. These elements of theeducative process point the way for a reduction in training time necessary for thosepreparing for health occupations careers.
Curriculum Structure
The structure and approach used in a health curriculum must be established whereby themany activities at all levels can be coordinated into high quality learning experiences tomeet the present and projected needs in the health occupations field. With the advent ofMedicare there is now a national commitment to an adequate level of health service forevery American. A single priority factor exists for both rural health care and megalopolishealth care. Each has its place in the overall scheme of better health care for people.

14
An agenda for action on the problems inherent in supplying health workers with qualitytraining and education needs 4o take into account establishment of a structure which makespossible the renewal of the cutting edges of the program and the allowance for addition ofnew activities related to an exploding medical technology. More specifically, the followingare nine characteristics of a modern allied health manpower curriculum: (1) preparatorytraining for health workers should be made a part of the community's responsibility andeducation of allied health workers placed in the mainstream of the educational process inthe secondary school; (2) adequate resources for the support of such training should bemade available through general educational channels: (3) state departments of educationshould establish a department for health occupations at the state level and employcompetent staff in sufficient numbers to give leadership to the development of trainingprograms in health occupations; (4) creation of a dynamic program in cooperation andcoordination should occura communications network system among all elements and"interface groups" to be maintained and used for the training of hrqlth workers; (5)elements in the general education curriculum related to health should be studied,strengthened, and made to serve both as pre-vocational learning for health occupations andas useful knowledge for every boy and girl in maintaining his or her own health; (6) theteachers of the secondary school should become partners in the preparation of boys andgirls in the awareness of opportunities which exist in the health service occupations; (7)teacher training programs both inservice and preservice can be made available for thosefields in which teacher education presently is not offered; (8) encouragement should beshown for the development of integrated instruction for courses which encompass thesecondary school curriculum in order that the general curriculum content may be placed inthe health service occupations context; (9) encouragement should be shown for thepreparation of personnel to meet the demands in the labor force on a general rather than anisolated or singular curriculum training basis in cooperation with post-high school, juniorcollege, and four-year institution programs.
Health Education
Health Education as an academic discipline includes innumerable content areas eachsurrounded by its fair share of controversy. Facts within this discipline are both basic andabundant. Mastery of the facts, however, is not sufficient preparation for healthmaintenance nor for delivering health services within the community. Knowledge, that is,the cognitive domain, has value only to the extent that a person is also able to perform in amanner judged to be adequate by some criterion. Skilled performance based upon correctinformation fails when the manner of service delivery is repulsive to the client. Thus, healtheducation whether for personal maintenance or for performing a service is superior whenknowledge, skill, and attitudes are woven into the fabric of experience for the learner.
Attitudes appear to be the key factor behind any real differences in the performance ofsimilar health services. The phenomenon of attitude as it relates to behavior has beenstudied extensively. The studies tend to demonstrate the elusive and intangible nature of anattitude. Methodology for dealing with those attitudes relevant to health services has beenneglected by the researcher with the result that the discipline relies heavily on adaptingresearch findings from other areas.
Health education continues to rely on the lecture approach which has been the dominatingmethod of instruction since the days of the "seven hygiene lectures" at Harvard in the early
1;

i
15
1800's. The parochial vision of a medical and educational establishment alike has tended toretard achievement of a desirable health education program for the secondary schools. Stillanother problem in health education and health services education is the tendency tosubdivide the study of man into three major areasthe body, primarily the concern of thephysician; the mind, largely the concern of the educator, psychologist, and psychiatrist; andthe spirit, entrusted to the custody of the religious preceptors. Similarly, to the economicand political leaders have been consigned the development and maintenance of man'sphysical, social and economic environment.
This fragmentation of man into areas over which various groups struggle to maintain theirjurisdiction fiirtlpir confuses the purpose of each group which strives for enrichment andfulfillment of a particular segment of man's nature. Special interest groups must realize thatthey do not and cannot have a monopoly over a particular area of the nature of man asharmony is vital to the maintenance of optimal personal health. The delivery of healthservices by necessity requires a meshing of functions to achieve optimal patient care.Harmony can result when the fact is facted that man is a physical, mental and spiritualunitya unity which is constantly undergoing a process of groVvth and adjustment within acontinually changing physical, biological, social and cultural environment. Yet, the commongoals of each appear to provide adequate basis for building dynamic models of healtheducation and thus health services education.
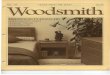
One such model, Figure 3, can be built upon health as personal fitness for full, fruitful,enjoyable living. On such a premise one might establish health as a triangle of physicalfitness, =Mal health and spiritual faith. Applying the three interrelated dimensions it ispossible to view the model of wellness from death to optimal health. Given a dichotomyseveral levels of wellness can be assigned between the extremes. Consideration of well beingas a line representing all stages from optimal health to death. also has the disadvantagesinherent in a dichotomy.
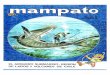
More flexibility can be achieved by conceptualizing relative sickness and wellness as one axisof a "health grid." See Figure 4. The health grid is made up of: (1) the health axis, (2) theenvironmental axis, and (3) the resulting health wellness quadrants. These are: (a) poorhealth in an unfavorable environment, (b) protected poor health in a favorable environment,(c) emergent high-level wellness in an unfavorable environment, and (d) high level wellnessin a favorable environment.
Once the concept of high-level wellness as a health goal has been crystallized and enrichedby many minds contributing to it from their own points of reference, the battle for wellnessin man and society will be joined. There must be many points of engagement if the battle isto be won.
The goal of high-level wellness for man and society can he achieved, though not easily. Theneeds are for a clear-cut concept and dedication to it; for money and research; forunderstanding, courage, and a reassessment of basic values; for a positive orientation towardlife and society; for a program of instruction in the schools which prepares youth tofunction in a cosmopolitan society.
Although many leaders in secondary education have formulated aims for guiding curriculumdevelopment, all lists show a great amount of similarity. the most comprehensive,functional, and influential formulation of objectives was that of, the Commission on the

4
Figure 3
HUMAN INTERACTION
PHYSICAL FITNESPERSONAL I
HEALTHGood Heredity & EnvironmentHealthful, Safe LivingAdequate Medical CareOptimal Nutrition &ExerciseSatisfying Work &
"
RecreationRefreshing Rest & SleepLife Space, Freedom,Privacy MINORChallenges, Risks, ILLNESSCommitments
Poor HeredityPoor EnvironmentLack of Commitments & MAJORValues ILLNESPsychogenic-EmotionalFactorsUnhealthful BehaviorLow-Living Standard CRITICALInadequate Medical Care ILLNESSEndogenous FactorsNeoplasms
DEATH
Personal-Social FulfillmentLove, Hope, Faith, SharingSelf-Regulation &HomeostasisOptimal Growth & Develop-mentHeterosexual AdjustmentResistance to Disease andAgingEmotional MaturityFun, Humor, Enjoyment
Deficiencies & ExcessesDeprivationsNoxious Agents andAllergins
Stressors & Stress
Radiation Hazards
Pathogenic Organisms
Accidents & TraumaticInjuriesPathologic Conditions
Aging & Senescence
An ecologic model of health and disease. Examples of favorableand unfavorable dynamic, interacting hereditary, environmental andpersonal ecologic factors and conditions that are determinants ofthe levels of health and disease on a continuum extending fromzero health (death) to optimal health. Adpated from H.S. Hoyman,
the American School Health Association.
16

ameawmmexamms.........no
.0.'4110411mmi#Aww.A.A1541NWAttr.,4051r4Y44.
/7
,..0,01AW06,0*,41MONMWM11061~10.004aroitk
Figure 4
The Health Grid, Its Axes and Quadrants
Adapted from U.S. Department of Health, Education, and Welfare,Public Service, National Office of Vital Statistics.
PROTECTED POOR HEALTH(in favorable environmenti.e. through social andcultural institutions)
Death 41. Health
VERY FAVORABLEENVIRONMENT
HIGH-LEVEL WELLNESS(in favorable environment)
POOR HEALTH(in unfavorable environment)
PeakAxis Wellness
EMERGENTHIGH-LEVEL WELLNESS
(in unfavorable environment)
*tt
z0.1
c:4
VERY UNFAVORABLEENVIRONMENT

Ili
e la
-111
DIU
f 1.
II.HI
II
II
18
Reorganization of Secondary Education, appointed by the National Education Association.The committee determined the main objectives from an analysis of the activities of theindividual. The seven objectives are : (8:10ff)
1. Health
2. Command of fundamental processes
3. Vocation
4. Worthy home membership
5. Citizenship
6. Worthy use of leisure time
7. Ethical character
Social as well as personal efficiency depends upon health, so health needs should not beneglected in the secondary schools. The school can teach certain facts about health, helppupils form good health habits, and build attitudes that will promote health.The healthobjective should not be attacked as an isolated unit, course, or abstraction, but in relation toother aims and through the medium of all sub /ects of the curriculum. All courses may makesome contribution.
Baseline Data
National manpower reports and baseline data from the eight-state RMEL region wereanalyzed in order to identify; (1) health occupations which have been prepared for at highschool level or do not require high school completion for job entry, (2) health occupationswhich statistics and expert opinion indicated were in short supply, and (3) healthoccupations which were introductory to post-high school technical and ;or professionalpreparation.
Six questions were generated to form the basis for inquiry into the availability of publisheddocuments dealing with health statistics. These are!
1. Are there any statistical data or studies available which show the quantitative orqualitative needs for health services and health manpower in the state or incommunities in this state? Have any statistics been collected by healthdepartments, organizations or health professionals, hospital and nursing homeadministrators or by the state employment (economic security) service? Howmay we get this data?
2. Are there any project proposalsfunded or not fundedwhich offer'evidence ofhealth or health manpower needs on the state or community level? If so, howmay we get copies of the appropiate parts of the proposals?
3. What evidences other than those of a statistical nature are there that state andlocal health needs are not being met because of manpower shortages. Forexample, are the funds available under Medicare and Medicaid not being usedbecause of lack of trained health workers?

19
4. What in your opinion are the critical areas of health manpower needs in yourstate and in communities within the state? On what do you base your opinion?
5. To what degree are the state and its communities planning to meet health needs?What short and long-range plans are underway for developing health servicesthroughout the state? What are the implications of future plans in terms ofhealth manpower? What sort of health manpower skills do you see as being mostproblematic to effective planning?
6. If within the next few years, we are able to produce a significant number ofwell-trained subsidiary paramediem health workers for employment upon highshcool graduation, what sort of workers would be of most value in helping thestate and communties meet their health needs?
The staff examined statements of present employment in the nation and in the RMELregion, projections of employment in the nation and region, statements of projected healthservices facilities in the region, statements of present training programs nationally andstatements of the number of instructors engaged in the several training programs on anational basis.
For example, the extent of training programs nationally and the employment categories forwhich opportunities are authorized for health occupations through MDTA training appearsin Figure 5 . More than fifteen job titles require less than post-high school technicaleducation.
Through resource consultants a list of probable sources for health occupations data wasgenerated.Telephone contact proved to be the most efficient means for gathering more thanforty-two documents from state officials in Arizona, Colorado, Idaho, Kansas, Montana,Nebraska, Utah and Wyoming. Data documents were received from the followingdepartments:
Manpower Coordinating CommitteeLaborResearch Coordinating UnitBoard of NursingPublic InstructionOccupational Research UnitHealth Facilities Planning CouncilHospital and Nursing Division,
Employment SecurityEmploymentPublic Health
Board of Dental ExaminersPlanning Committee for Nursing
Health Services' Education Assoc.Health Career Council
Department of Public HealthDepartment of Public Health
Judging from the sixteen sources which were utilized it appears that extensive datacollection for reporting purposes exists regarding the several dimensions of health care. theavailability of these documents made it unnecessary for RMEL to originate a data gatheringquestionnaire.
It is obvious that there arc serious shortages in the supply of health manpower.of facilities and services adds to the problem of rendering care to every member of society.Attempts have been made toward measuring these shortcomings, but none of the many

Figure 5
Training Opportunities Authorized for "Health Occupations"MDTA Institutional Training Program 1
Cumulative August 1962-June 1968
20
CumulativeAugust 1962
through
CumulativeAugust 1962
throughOccupational Title June 1968 FY 1968 June 1968
Total 83,718 14,875 68,843
Child Care Attendant 197 40 157Chiropractor Assistant 20 - 20Cottage Parent (Med. Serv.) 155 - 155Dental Assistant 967 118 849Dental Hygienist 21 21Dental Laboratory Technician 240 79 161Electrocardigraph Technician 14 - 14Electroencephalograph Technician 24 - 24First Aid Attendant 24 - 24Home Health Aid 1,260 326 934Hospital Admitting Clerk 32 32Hospital Maid 418 20 398Housekeeper/Housecleaner (Med. Serv.) 1,654 - 1,654Inhalation Therapist 265 81 184Medical Assistant 121 46 75Medical Laboratory Assistant 1,044 282 762Medical Records Clerk 257 127 130Medical Secretary/Transcriptionist 207 20 187Miscellaneous Health Occupations 575 320 255Nurse Aid/Orderly 30,039 4,147 25,892Nurse, Licensed Practical 27,493 4,901 22,592Nurse,Professional (Refresher) 12,923 3,612 9,311Occupational Therapy Aid 271 15 256Optician 37 37 -Optometrist 20 - 20Orthopedic Cast Specialist 15 15 -Orthcipetist 78 - 78Psychiatric Aid 3,078 324 2,754Physical Therapist 159 - 159Physical Therapy Attendant 17 - 17Radiation Monitor 40 - 40Radio logic Technologist 207 56 151Surgical Technician 1,243 182 1,061Tray Line Worker 80 80 -Ward Clerk 523 15 508
1 Includes trainees under Section 241 (Redevelopment Areas) and estimates for HealthOccupations in multi-occupational projects.

_ ,...1#11X7411
21
estimates can adequately measure the total need or demand. Even it one could envision theideal staffing for health services for a community, for a state, region or for the nation, thecontinuing development of new technologies, new patterns of service and new methods ofpayment are all constantly changing the needs for both numbers and varieties of healthworkers. In summary, the trend of diversification and specialization may be expected tocharacterize health manpower of the future. Opportunities for entering the health serviceindustry should be based upon curricular strategies which will permit the high school ageyouth to prepare broadly, specialize for job entry and continue ascent during his career.This preparation suggests a ladder of employment which takes into account the trend todiversify and specialize in keeping with new knowledge and techniques as well as newpatterns of service. The ladder of opportunity is illustrated in Figure 6.
Assimilation of the data narrowed the list of potential job entry titles to twenty-three healthoccupation service jobs thought to be appropriate for high school youth. Those healthoccupations were:
Nurse AidePsychiatric AideOrderlyDental AssistantPhysical Therapy AideHome Health AideCentral Supply AideOccupational Therapy AideDietary AideMedical Records ClerkMedical Office AssistantLaboratory Aide
Ward ClerkMental Retardation aide
Rehabilitation AidePharmacy Helper
OrthodontistPediatric Technician
Formula Room WorkerPhysician-Dental Secretary
ReceptionistSocial Service Care Aide
Nursing Unit ClerkAmbulance Emergency Attendant
The search of the data was conducted in the areas of jobs, functions and responsibility forcontent (general curriculum, health occupations elective course, clinical affiliate orientationand experience). A listing of the objectives of the analysis and personnel to whom it wasassigned appears below:
Jobs, Functions and Assignment of Content
Inquiry Resource
1. Determining on the basis of functionaldescriptions of the selected occupations,the functions of each.
2. Analysis of course outlines and coursedescriptions to identify the learningcontributing to each function of eachselected occupation.
3. Evaluation of !earnings by experts as totheir:(a) Relative essentiality to performance
of the function.(b) Whether best taught in the general
education classes, elective classor in clinical affiliate.
Program Staff
Program Staff
1. Supervising HealthProfessionals.
2. Health AgencyAdministrators.
3. General educationteachers
4. Incumbent workers.

Figure 6
22
Experience
Entry Level
Career Mobility within the Health Occupations

23
4. Analysis of preceding evaluation: Program Staff(a) Identification of significant
learning for each function ofeach job.
(b) Identification of commonalitiesof significant learning among jobs.
5. Expert evaluation of essential IL:tuning Curriculum expertsas to relevance and application to existing in Academic andHigh School courses other than healthoccupations elective course.
Vocational Education.
6. Analysis of preceding evaluation, compilationof lists of !earnings applicable toeach content area.
Program Staff
7. Evaluation of appropriateness and Grade 1 1sequential placement of preceding list of Classroom teachers(earnings by classroom teachers inrespective areas.
8. Curriculum construction: Program Staff(a) Curriculum contributed by Consultants(b) Health Occupations core
curriculum(c) Curriculum specific to each
respective occupation.
As a result of strategy meetings the list of twenty-three health service occupations wasreduced to 18 job titles allowing concentration on the study of available courses regardingcurriculum information. The option to expand the list was left open in the event thatunanticipated materials appeared during the search.
A review of literature was conducted to identify those health occupations which couldreadily be studied for course/curriculum content and/or for performance criteria. Minimalnotes concerning first impressions of material of possible value were recorded and revealedan acute shortage of curricular materials as well as a shortage of lists of job performancecriteria. As the search narrowed the decision was reached to limit the collection of materialto those health service occupations for which knowledge, skills, and attitudinal content wasreadily available. Some job performance criteria were available. Those materials listing onlythe course name and number of hours of instruction were judged to be too vague and wereabandoned.
The search was now further narrowed to eleven health service occupations which appearbelow:
Nurse's Aide or OrderlyHome Health AidePsychiatric AideDietary AideFood Service AideDietary Clerk
Medical Records ClerkWard Clerk
Medical Office AssistantDental Assistant
Ambulance and EmergencyAssistant

24
Findings from review of the literature, the shredding of training course materials, andconsultation with resource persons were sorted into three categories: area of knowledge,area of skill, and area of attitude. The category, area of knowledge, was assigned six itemcollection cells:
Hospital management and organizationMaintenance of asepsisStructure and function of the human bodyMeans of communication of ideas, directions and reports (terminology, names, symbols)Function and operation of equipment used in diagnosis and therapyProcedures other than those used in patient care.
Curricular elements, lists of performance criteria, materials and other information pertinentto the area of knowledge in the eleven health service occupations were sorted into theappropriate cells for further consideration.
The category, area of skill, was designed with six cells which formed a depository forstatements, lists, etc., of performance elements for the eleven job entry titles. These were:
Skill in operating equipment and handling instrumentsProcedures used in patient care and treatmentProcedures for maintaining asepsis (cleaning, sterilization and disinfection)Communication skills (reading, transcribing, written and oral reporting)Skill in measurement techniques (counting, reading and interpreting scales)Use of accurate medical terminology.
The general categories listed above while broad and general in nature, provided the necessarynumber of cells for sorting purposes.
Humane skills, the value positions of health service personnel, their attitudes toward thetolerance for service to others are judged to be a crucial attribute in the delivery of healthservices. Five cells were created for storage of clues to required levels of valuation. Thesefive cells were:
Attitude toward maintenance of aseptic environmentAttitude toward mental alertness and competencyAttitude toward unbiased thinking and reportingAttitude toward the responsibilities of the role of members of the health teamSensitivity toward the feelings of others-empathy-including value placed on tactfulness andrecognition of the worth of others .
Course material was collected for these aide level health service occupations through areturn to the literature and a search of the ERIC file. Course material elements weredescribed in the form of performance based upon the following questionS:
1. Is the element significant and appropriate for an educational program?
2. Is there at least one situation where the performance element would contribute tothe overall effectiveness of the job?

25
3.. Is the performance element stated in such a way as to have optimal agreement on itsinterpretation?
The elements were found persistently to fall into more than one category of skill,knowledge or attitude according to the scheme for categorizing essential skills andknowledge, but none fell outside this list of essentials.
The performance elements were considered for all eleven job titles and recorded, analyzedfor knowledge, skill and attitudes, matched with curricular materials, and verified inconversation with those working or teaching in the field. Those that persentedcommonalities were pulled from the group, subjected to reappraisal according to thepreviously stated criteria, duplications eliminated and the core of performance elementsproduced. The performance element categories are: work situation, safety, first aid,terminology, communications, health and hygiene, asepsis, interpersonal relations, and useof equipment. A questionnaire (Appendix A) was developed from this list of performanceelements.
Summary
Health services occupations as projected by the Department of Labor are soon to becomethe largest single sector of the labor force. Challenges confronting trainers of professionaland para-professional health personnel include licensure, certification, shortage ofinstructors and training facilities. In order to prepare human resources for the 10,000 newhealth jobs per month through 1978 and to upgrade people already employed a newconfiguration of training must evolve.
One alternative to present training modes would be to enlist the aid of the entire teachingstaff of a high school in order to emphasize the relevance of their subjects to the 'healthservices occupations as suggested in Figure 7. Armed with knowledge of opportunities in thehealth field through the general curricula the youth could elect a special health servicescourse taught by a health occupations teacher-coordinator. Emphasis on relevant content inthe academic subjects and specialized health services experience provided in part in a clinicalaffiliate will nurture interest and provide unity for the development of human resources forhealth occupations.
Because of the sparse population in its territory, RMEL chose to implement the HealthOccupations Curriculum in rural communities first, since mobility of rural population tourban centers continues. Preparation of these rural people for work which they probablywill seek in the cities should occur in the rural setting. It is highly probable that mechanismsfor training when developed in the rural setting are likely to be transferable to the urbansetting where opportunities for training are more abundant.
The Health Occupations Curriculum system was designed to develop a method for theidentification and assessment of opportunities for entry-level occupations in the field ofhealth services; to identify the necessary knowledge, skills and attitudes required for successin specific jobs in the entry level occupations; to identify clusters of those occupations; tolocate, develop and adapt essential instructional materials which will prepare individuals forthe occupations; to develop programs and materials to be used in the training of instructorsand other personnel in the use of the curriculum; to assess the effectiveness of the program;and to make findings and products of the project available for general use.
J,

----
...4
.-'
"rt
%-:
.;;;'
core
ro r
am
Health Occupations
Clinical
Inquiry
Experience
Knowledge, experieat;v, attitudes
.171
eq CD 1
0

27
It was expected that this project would provide a prtype for the establishment of a highschool level health occupations program in the rural school systems and their healthcommunities; and that the program products would be transferable to the urban setting. Itwas also anticipated that the model used in deriving appropriate and relevant curricula forhealth would be applicable to other occupational clusters, i.e., mechanical, business, andservice.
An organizational strategy for identifying job clusters would] volve: (1) an examination ofa wide variety of jobs, sorting them into groups accord' g to the various tasks, skills,knowledge, aptitudes, work habits, or whatever the job requires for success, (2)incorporation of common job elements into curriculum useful in a number of occupations,(3) assignment of curricular responsibility by function to general class, special class and/orwork affiliate agency for achieving job entry performance criteria.
What advantages could be anticipated from building such a curriculum? There are several:(1) an invaluable aid in demonstrating that the curricula prepare people for real jobrequirements, (2) assistance to students in making effective educational and vocationaldecisions, (3) arming students with flexibility and salient information on which to buildwhen change of job occurs, (4) providing a viable context for experiences leading to masteryof performance criteria, (5) providing the judgmental base for curricular change andmodification (6) and facilitation of administrative functions, e.g, selection of students,employees and assignment of faculty.
At this point in preparing the Health Occupations Curriculum the scope of activitiesbecomes quite clear. The general goal, stated idealistically, is to build a society in which allpeople can function with optimum satisfaction. Translation of the ideal into program plansfor health services career opportunities results in the following objective:
1.0 Conduct a feasibility study.1.1 Build a rationale for establishing a health services careers
program at the secondary school level.1.2 Collect studies of present and projected levels of allied
health manpower.1.3 Collect state plans for hospital and medical facility construction.1.4 Collect descriptions of courses and numbers of persons
being prepared for health services careers.1.5 Collect health curriculum strategy descriptions.1.6 Analyze data to arrive at program alternatives.
2.0 Describe training program.2.1 List the para medical entry jobs for which training is needed.2.2 Build statement of activities describing the entry jobs.2.3 Build the statement of knowledge necessary for job proficiency.2.4 Build the statement of skills required in the function of
the jobs.2.5 Describe the humane skills (attitudes) characteristic of
success in the entry job.2.6 Describe the environment, tools, aids and equipment required
for the clinical affiliates.

-iI-IM
lit
111
3.0 Develop Health services job performance criteria.3.1 Statement of interim standards.3.2 Statement of terminal behavior conditions i.e., classroom,
special experience, clinical affiliate.
4.0 Develop Criterion Test.4.1 Performance test:4.2 Applied knowledge and skills.4.3 Humane and verbal skills.
5.0 Validate Criterion Test.5.1 Pilot tests with job incumbents.5.2 Pilot tests with naive population.5.3 Determine reliability and validity.
6.0 Validate Performance Criteria.6.1 Analyze incumbent and naive sample test data to identify
needless behavioral objectives.6.2 Revise curricular content.
7.0 Develop Learning Sequence.7.1 Use matrix analysis to assign kinds of learnings.7.2 Separate and assign by job function to open classroom,
special class experience and clinical affiliates.7.3 Validate sequence of learnings.7.4 Validate placement of learnings.
8.0 Develop Learning Strategies.8.1 Determine appropriateness for integration, modular format,
isolated unit, etc.8.2 Determine media sources and preview.8.3 Describe alternative methods and suggested materials.
9.0 Develop Individual Lessons.9.1 Develop examples for use by general classroom teacher.9.2 Develop examples for use by special experience teacher.9.3 Develop examples for use by clinical affiliate.
10.0 Validate Individual Lessons.10.1 Field test until 85 percent of successful worker sample accept
criterion.
11.0 Implement and Field Test Curriculum.11.1. Lesson plans.11.2 Teacher training.11.3 Demonstration and curriculum validation.
28
0

12.0 Follow-up Students by Class Year.12.1 Year prior to implementation.12.2 First, year of implementation.12.3 Second year of implementation.12.4. Third year of implementation.12.5 Review employment patterns.
29
13.0 Conduct Normative and Summative Evaluation and Report.
Curricular Preview
Several different presentation methods were considered early in this developmental effort.These included:
specific knowledge and skills addressed to a single job title
general knowledge of occupations which encompass. many career fieldincluding health careers
work-study program with release time
pre-technical course to prepare for post-secondary technical training
The RMEL strategy for presentation of health occupations information, materials andexperiences was to divide the performance elements associated with eleven aide or assistantlevel jobs among the 1 1 th grade teachers, the health occupations teacher- coordinator, andpersonnel of the clinical affiliates. Recruitment and orientation of students for the electivecourse would occur in the spring in general convocation and would build upon conceptspresented, in a health careers brochure. (Appendix 13) Students would be alerted to thegeneral design of the course and the anticipated outcomes; a brief consideration of theopportunities available in the health service industry with emphasis on the opportunity toexplore individually; the patient-centered project method-how it works; the basis forassessing student progress; pitfall of pioneering and the accompanying responsibilities; andfinally, emphasis of the importance of initiative and self- direction in conducting individualprojects.
The general one year course design might be envisioned as composed of eight or morepatient- centered projects. Situations, projects and/or units suggested in this paper are ono-examples to guide this report. Each of the situations is chosen because it is thought tocontain a variety of information about several health occupations. Performance elementsshould not be forced to the surface but should emerge as the natural outgrowth of studentinquiry.
The patient-centered investigation would begin early in the course in order to utilize thecommunication lines previously established. The adaptability and integrity of the healthoccupations teacher-coordinator will reserve to the student the opportunity to makedecisions in keeping with his interests, aptitudes and abilities' as he explores employmentopportunities. The several project periods listed below are assumed to be neither sequentialnor exclusive.

30
Suggested Units of Concentration
Have each student interview someone he knows who has had a recent acute illness andreport to class members his findings regarding the health workers involved, what happenedto the patient, how the patient felt about it, and how the student feels about his findings.
Have each student interview a convalescent patient at home or in a nursing home. Followthe inquiry method suggested above.
Have students examine briefly a group of complex medical problems and decide on one ofthese for in depth exploration of a patient situation, including the patient's care and serviceneeds, and the relationship of the health occupations workers' skill, knowledge andattitudes.
One or more elective surgery situations could be chosen by the students for in depth studyof the components of care and the roles of the variety of health occupations workersinvolved.
Material for the study of an accident victim would be gathered by the instructor. Thesituation components are drawn by the students from their examination of the total recordsof an actual accident situation. This sample unit of the curriculum is included since it wasfelt that the possibilities of this unit can best be demonstrated in a group situation.
Have students discuss a group of handicaps, develop a simulation experience and investigatefurther the needs and feelings of a specific patient with a handicap and the roles of thehealth workers involved.
In a family health unit have the group first discuss the family's responsibility for thepromotion and protection of the health of its members and how differences in familiesaffect the way in which these needs are met. Each student could then investigate one aspectof family health care which is of interest to him.
Have each student plan independently his own experience in a clinical facility. This planwould take him into a situation where he could test his choice of health occupation andobtain more information for entering a specific interest area.
Teachers are known to prefer differing styles of presentation. Though individualized in thelocal setting, at least six distinct planning categories emerge. These are: teacher orientation,statement of objectives, content, materials, student activities and anticipated outcomes.These stages of the planning process have been applied to the suggested unit dealing with theaccident victim to illustrate the importance of pre-planning by the health occupationsteacher-coordinator.

The Accident Victim (An Example
Objectives
Examine emergencycare facilitiesand personnelin relation toone accident.
Examine use ofrecords, reports,observations ofvarious personneland departmentsin relation toone patient/victim,
Add to knowledgeof work elementsand training ofthe healthoccupationsopportunities inthe situation.
Student Activity
Examine all records andlist components of thesituation.
Make decisions forpriority of study,dividing class membersto handle work load,depth of study desiredand possible in eachcomponent.
Practice movingpatients.
Practice skills ofbasic first aid.
Practice monitoringand recording vitalsigns.
Share all findingsconcerning theaccident.
Write a narrativereport, newspaperaccount, poem or useany method to illustratewhat happened in non-technical terms.
Anticipated Outcome
An appreciation for andknowledge of:
Use of records inreporting care, condition,service.
Importance of accuracyin reports.
Procedures concerningpatient identification,safeguarding belongings,release of information.
Terminology involved.Use of a variety ofrecords and reports.
Anatomy and physiologyinvolved.
Skill in first aidprocedures.
Health occupations ofworkers involved, theirfunctions, training,responsibilities, etc.
31

NOW ROPY, JITPSNO
The Accident Victim (An Example) continued
Content
Accident, chosen inview of content andrecords available
(Note: see instructororientation).
Content drawn from .
components as reconstructedfrom records:-police report-hospital records,including:-emergency, admission-doctor's orders & notes-nurse's notes-treatment, X-ray-laboratory, blood service-surgery-insurance-rehabilitation, etc.
Examination of recordsand reports in all areasto consider who and howresponsible as well aswhat was done. Also,safety-accident prevention,functions of all healthworkers involved, firstaid, samaritan laws,decisions concerningpriority of care, bodymechanics for movingpatients, patient identificationemergency admission,patient and family reaction tocrisis, evaluation, observation,vital signs, release ofinformation, safe-guardingbelongings, terminology.
Use of statistics to look atscope of work.
InstructorOrientation
Cooperation of: (1)hospital administrator,(2) attending physician,
(3) police and emergency
personnel, and (4) other
involved authorities,must be obtained andproject scope andpurpose explained priorto attempting to obtainairy records
/111 pertinent recordsmust be obtained, notjust summaries.
All records should bereproduced withpatient/victim andother names blockedout.
Investigate possibilityof Red Cross conductedfirst aid course withcertification of successfulclass members.
Investigate possibilityof individual or smallgroup visits to emergencyfacilities, ambulanceservice, etc.
Materials
All records
Health occupations
information
Medical dictionary
Medical referencetexts
Laboratory manual
Physician's DeskReference
References pertinentto situation.
State laws andlocal ordinancesgoverning records,release ofinformation.
Accident statistics:local, state, andnational.
Books: Red Crossor other FirstAid manual for eachstudent.
32

1
i
33
Much has been written about providing a partnership opportunity for teachers of generalcurricula to expand the occupational knowledge base of pupils. Some examples of contentwhich appear to provide the vehicle for preparing integrated content lessons are:
Agriculture....a means for preserving man's health and well being,regulation of agriculture to prevent diseases.Art....human anatomy, medical illustration.Biology....the human being as a biological organism, inter-relationsbetween man and other organisms.Business and Office....medical record keeping, business and managerialskills used in providing health services.Chemistry and Physics....Chemical and physical reactions and systemsin the body. The use of chemical and physical agents in the treatmentof disease.Classical Languages....Greek and Latin roots basic to medical terminology.Distributive Education....distribution of health products and pharmaceuticals.Eng lish....objective reporting and recording as a basis for medicalnotation.Geography....geography as an epidemiological factor in health anddisease.History....historical perspective of the development of medicine andhealth occupations.Home Economics....role of family members in safeguarding health.Social Studies....role of society in providing services for thepreservation and restoration of health.Trade and Industrial Education....industrial health and safety. Operationand maintenance of diagnostic and therapeutic machinery.
It is anticipated that individual teachers are in the best position to provide the specificsnecessary for integrating course material and health occupation material to provide anappropriate curriculum mix.
Implementation
There are numerous variables which become important as one looks toward implementationof the Health Occupations Curriculum. A topic given considerable attention was thedefinition of a rural school. The National Association of Secondary School Principals chosethree levels of secondary school enrollment on which to gather and report 'data. These are(1) less than 500 students, (2) 500 to 1,000, and (3) more than 1,000 pupils. The programdescribed in this paper was intended for pilot implementation in a school with fewer than500 pupils, grades 9-12.
The extent of formal and informal guidance services appeared to be important. It wasgeneralized that the availability of occupational information and a variety of test data wouldhelp the student understand his opportunities for a career based upon personal attributes.The presence of a school nurse would also add to the potential resource informationavailable to pupils, teachers and the health occupations teacher-coordinator.
r

34
Pupils within the program should be free to probe all manner of jobs specifically in thehealth careers field. Inter-relationships of the program to regional, state and localeducational systems as well as to health agencies is judged to be crucial to success. Theinvolvement of the state director of vocational education and of the state healthoccupations education supervisor would tend to assure that the program can be included forstate and federal reimbursement. The willingness of state education department personnel toengage in an advisory capacity adds to the long range potential of the program.
Community selection for placement of this program can be based on a series of questionsabout the school. A suggested list follows:
Selected Top-Priority School Settings
Question Data to Provide Answer
I . Which educational systems serving I. Location, characteristics
isolated (rural and semi-rural) and attitudes of schoolareas would be willing systems serving isolated
and able to participate in the communities.project?
2. In which of the above systems 2. Proximity of hospitals,are there high schools in nursing homes and otherreasonably close proximity to health agencies to eligibleclinical agencies? schools.
3. Which of the clinically-feasiblehigh schools settings providegreatest assurance for employmentof the high school graduate?
4. Which of the high prioritysettings are offering greatestevidence of project acceptanceby the health community?
3. Evaluation of health agency'sattitude toward employment ofhigh school youth and towardcareer migration within theagency.
4. Evaluation of attitudes oflocal public health officialsand organizations of hospitals,nursing homes, health professionals,etc.
The following program imperatives are representative of those qualities necessarily inherentin the community seeking implementation:
I . The availability of the state supervisor for health occupations to program personnel iscrucial to maintaining a successful program.
2. Cooperation and support of the local board of education, superintendent, buildingprincipal and guidance staff is necessary.
3. Willingness on the part of teachers of general subject matter to place their content intothe health services career context is paramount.

35
4. The proximity of clinical facilities to the school will limit the extent of the studentexperiences.
5. Orientation and training of program staff will occur in a medical setting for theconvenience of special resource personnel and to attain a sense of the clinicalatmosphere.
6. The presence of a school nurse in the high school will affect the program in a positivemanner.
7. An intensive recruitment program will be conducted at the tenth grade level.
8. The health professions organizations in the community will assure a pool of resourcepersonnel.
9. The program will contain job relevance with which both boys and girls can identify.
10. The availability of occupational information and guidance to students in grade nine andten will enhance the program.
11. A patient centered approach to skills, knowledge and attitudes necessary foremployment in the health services career field will assure the relevance of content.
12. Exploration of the health services career field will encourage visitations to clinicalaffiliates by students to gain first hand knowledge of the work of the assistant, thetechnician and the professional.
13. Presentation of media developed by the proprietary-business sector will broaden thestudents perception of the roles of health personnel.
14. A method for updating the nature and needs of the manpower for the health careersfield will be established.
15. A monitoring system to provide guidance, direction and trouble-shooting for the severalprogram parts is necessary.
16. A student follow-up system can provide valuable data for course modification.
17. Ability to communicate in health service parlance is essential to gaining acceptance as amember of the health team.
18. Simulation and other gaming techniques which provide a clinical setting will allow thestudent to project into work-like circumstances.
19. Adoption of a health services career program by urban communities can occur fromdemonstration and pilot efforts conducted in a rural setting.
20. The availability of post high school technical training will make health careerarticulation possible.

.i.,...__.;__. ............
36
Personnel Training
Several levels of personnel training are necessary for implementation of the HealthOccupations Curriculum. These include preparing the Health OccupationsTeacher-Coordinator for certification, building an orientation program for the community,clinical affiliates and staff of the local school, scheduling in-service workshop meetings toassure enroute assessment, reinforcement and modification of program elements andconducting appropriate work sessions to consider the data synthesis, and decision-makingaspects of evaluation.
Specifics of orientation and training will not be detailed in this report. Consultive servicesare allowed for in the proposed budget and assumed to be adequate to fit the needs of aschool with a 9-12 population of 500 pupils.
One of the difficult facets to reconcile in the RMEL Occupational Education Program is theshift from a developmental-reality test focus to report writing regarding what might havebeen. As stated earlier in this paper, 11 th grade pupils, their teachers, administrators andauxilliary' educational personnel were to be exposed to the opportunities for employment inthe health service industry and directly involved in an integrated-content health occupationscurriculum program. Features of this program were the services of a health occupationsteacher-coordinator, patient-centered inquiry for pupils as well as orientation to andexploration of clinical affiliate services, facilities and processes. Objectives for thisinnovative approach for providing high school youth with health service industryinformation and experiences were:
1. To orient high school teachers. to the health occupations curriculumstrategy.
2., To aid 11th grade teachers in adapting health occupations relatedinstruction to selected units of the general curriculum.
3. To update program activities through appropriate in-service training forparticipating teachers.
4. To monitor participating teachers in their presentation of instructionalmaterials.
5. To provide an elective course in health careers for interested students atthe 11th grade level.
6. To establish an extensive orientation experience program in cooperationwith local health service personnel, for all students interested in healthservice careers.
7. To employ a qualified health professional to coordinate the workexperience aspect of the program and teach the elective health careerscourse.
8. To develop guidelines for program improvement and replication.

37
9. To assess program impact through the utilization of both normative andsummative evaluation procedures.
The orientation of teachers to the health occupations curriculum strategy would includeestablishing a summer workshop to be conducted in the medical facility of a Land Grantuniversity. The workshop would have a university summer sessions course number assignedand be offered for credit. Teachers attending the workshop in the environment of themedical facility would have access to each of the job entry types for whom this program isintended. Through workshop activities teachers would build a knowledge base of healthindustry information and explore general education content to identify areas of subjectmatter which could be converted into the health occupations context.
Program Monitoring and :valuation
The function of program monitoring is to provide an ongoing assessment of progress. Ingeneral, monitoring permits early problem identification and keeps the communication linesamong participants both open and clear.
The function of the evaluator is to gather, synthesize, and release information for decisionmaking. Program monitoring and evaluation will be treated as one in the discussion whichfollows.
The Qualitative and Quantitative aspects of the Health Occupations Curriculum focus uponthe student, the teacher, and the intervention process. Concerns of quantitative nature arelisted below as a guide to data gathering for decision making purposes.
Follow up of previous members of the student body, i.e., type of work, posthigh school education, military, marriage, unemployed
Size of elective class(es) in Health Occupations course, grade l l
Registrants for Health Occupations course, second year, grade 1 l
Number of general education teacher days utilizing health occupationinformation
Student mastery of elective course knowledge and general classroomcurriculum content
Students referred by classroom teachers to Health Professions Coordinator
Student mastery of job skills
Student attitudes toward Health Services center
Number of teachers in orientation workshop
Teachers and courses committed to use health context for general subjectmatter

38
Number of revisions and/or modification enroute by classroom teachers
Involvement of Health Services personnel, job titles and kinds of clinicalfacility
Student stations volunteered by clinical affiliates
Health Professionals available on a resource and consulting basis
Students referred from general curriculum to Health Professions Coordinatorfor occupational information
Although the list is long, it is only suggestive of the available data which could add to thedecision making power. The question must always be, How will data gathering add to thesuccess of the program? Product evaluation models generally apply to the quantitative itemscited above.
Qualitative considerations constitute an extremely significant aspect of any program.Antecedent conditions can be recorded and later reassessed to determine the extent ofchange. Change can be accounted for through the use of a change-support model.Qualitative concerns suggested for the Health Occupations Curriculum are:
Extent of teaching staff awareness of and interest in health services careers
Extent of cooperation between school personnel and related health agencies
Student body awareness of health services careers
Extent of age, certification, licensure and other health occupation jobbarriers
Commitment of community to continue program
Receptivity of groups for orientation procedures and materials
Proficiency of teachers for placing course context in health content usingHealth Services Careers information
Extent of presentation of course materials in health occupations context
Response of health services personnel
Effectiveness of Health Professions Coordinator recruited from the latentmanpower supply
Aspiration levels of students seeking health career information
Assessment of enroute changes in program

39
From the context of the local community other concerns may emerge in the form ofquestions about which data should be gathered. Prioritizing the concerns and dividing theminto dependent and independent variables will sharpen the focus of the evaluation activity.A paradigm is illustrated in Figure 8 which focuses upon consistency and congruence asessential aspects of the evaluation and monitoring process.
Projected Costs
The RMEL Health Occupations Curriculum was initially structured to provide total studentbody exposure for 1 1 th grade students, treatment of special knowledge in an 1 1 th gradeelective course, and orientation to employment in the health services industry throughcooperation with clinical affiliates. The second year of the demonstration included repeating1 1 th grade activities while adding work entry experience for 12th grade students. Theelective classes and the work entry experience would be coordinated by employment of aHealth Occupations teacher-coordinator. The third year of demonstration would permit acritical analysis of product, process and change-support systems.
Organizational activities should preceed implementation by as much as six months. Thesequence of activities which appears above in this paper suggest the scope of work to beaccomplished. Recruitment brochure information as shown in Appendix B is included whichwas designed for use with 10th grade students. It is suggested that this activity be completedduring March preceding implementation. Clues to a scope of work for this program appearin the list below:
HEALTH OCCUPATIONS CURRICULUM PROGRAM
July and August
Identify participating teachersSelect Health Occupations CoordinatorOrient health coordinator to program philosophy and strategiesOrient participating teachers to program philosophy and strategiesTrain participating teachers to adapt instructional contentEstablish working relationships with local health personnelDevelop clinical orientation programComplete evaluation designDistribute program materialsDevelop elective course in health careers
September and October
Implement Health Curriculum in grade 11Enroll 1 1 th grade students in health careers courseMonitor presentation of instructionRecycle instructional contentBegin lesson analysis for cognitive, affective, and psychomotor behaviors
td.kaidair ael

-71
,';ft
liAttg
atiW
oto.
-01-
1eat
er.,4
044.
-.ra
IWO
OA
WN
ft-w
-.N
;*A
gl;-
Arr
iwo
PRO
GR
AM
escr
iplio
n
OBSERVED
INPUTS
consistency
OBSERVED
IIM
IN
ratio
nale
TRANSACTIONS
consistency
stan
dard
sOBSERVED
OUTCOMES
congruence
ANTECEDENT
Congruence
CONDITIONS
congruence
INTENDED
INPUTS
consistency
wINTENDED
TRANSACTIONS
consistency
INTENDED
OUTCOMES
I
mpa
riso
nsju
gm
ents
-rot
er,;_
,F.-
fur
ry,
;-
cro K CD 00

41
Conduct first inservice workshop for participating teachersConduct first program advisory committee meetingImplement clinical orientation program for health careers studentsBegin normative and summative evaluation
November and December
Conduct second inservice workshopConduct second advisory committee meetingValidate instructional content
January and February
Orient 10th grade students to health careers programPrepare curricular content proficiency evaluation
March and April
Conduct third inservice workshopConduct third advisory committee meetingReview and update instructional content
May and June
Complete normative evaluationContinue summative evaluationAnalyze dataPrepare report on activities and findingsDisseminate products and findingsConduct fourth inservice workshopPrepare and submit continuation proposalRecycle for second project year
The projected budget for first year activities include early employment of the HealthOccupations Teacher-Coordinator, use of consultants, a follow-up of students and aworksho p stipend for teachers.
Health Occupations CurriculumFirst year Grade 11
Training (20 teachers)
Orientation workshop 5 days @1000. 5000Materials 500Consultants 4 @100 X 3 days 1200Consultants travel and per diem 5 @180 900Inservice meetings 5 @450 2250Inservice Consultants 5 @100 500Consultants travel and per diem 5 @100

42
Services
Data processingMonitoringStudent followup (2 classes)
Personnel
500400500
500
Health Coordinator 15 months salary and benefits 12.500Travel and per diem 340
TOTAL 25,090
Self-Evaluation
The problems, surprises and discoveries encountered in the study of the health curriculumproject have led to a higher level of understanding for the project team. In order that healthcurriculum personnel might benefit from these experiences, the three categories above willbe recounted.
Problems
Any vehicle for change tends to molest the security of present practices with the result thatall sorts of defense mechanisms are mustered to protect the present domain. Questions ariserelating to adding another course to an already crowded curriculum at the high school,responsibility of general education teachers for focusing upon a specific manpower problem,traditional training-entry age requirements for sectors of the health occupations labor force,acceptance of trainees by administration and staff of clinical affiliates, acceptance oftrainees by patients, jurisdictional disputes regarding liscensure and certification,identification of, as well as, pre and in-service training for the health professionscoordinator, release of patient records for educational use, and ability to resist developmentof another terminal-vocational course. These and other problems do not representinsurmountable barriers but challenges which in the final analysis open the door to anurgently needed and satisfying personal service. In short, groups and individuals contacted inthis project have been overwhelmingly cooperative.
Surprises
Apparently no amount of orientation can prepare the curriculum builder for the task ofuntangling alliances. The power structure in medicine as in education is real and foreboding.A new 1,nd often pleasant tone arises, however, from bringing groups together once theyhave identified those attributes which they have in common. By not knowing all the answersthe curriculum builder is able to fit the pieces contributed into place. The process ofgleaning information and establishing the working relationship is paramount since thisprogram reaches into all classrooms, has salient elements dealt with by a health professionaland directly involves the clinical affiliates, patients and community.

-
Discoveries
43
There appears to be a growing sentiment on the part of the community expressed as awillingness to become involved in educational activities. Perhans this willingness toparticipate is only attributable to the dramatic needs for personnel of all abilities in thehealth manpower sector. But, perhaps, these same health community professionals andeducationalists have been seeking ways of increasing the opportunities for youth whileattacking a meaningful national problem. Whatever the case, people will engage in problemsolving across discipline lines and when they do programs of education emerge which arelikely to smack of relevance. It's a matter of listening in order thit you can be heard.

SELECTED REFERENCES
1. Advisory Council on Vocational Education. General Subcommittee for Education. 90thCongress, 2nd session, House of Representatives.
2. Cardinal Principles of Education. Washington: U.S. Office of Education Bulletin No.35., 1918.
3. Educational Commission of the States. "Report of the Ad Hoc Committee onVocational-Technical Education." Denver. Education Commission of the States,1967.
4. Kaufman, et. al. The Role of Secondary Schools in the Preparation of Youth forEmployment. Pennsylvania State University, University Park, Pennsylvania. Instituteof Research in Human Resources. 1967.
5. Lester, Richard A. Manpower Planning. Princeton, New Jersey: Princeton UniversityPress, 1966.
6. "Pre-Technial High School Program." Mimeograph No. 7. Technical Education Program
Series No. 12. Washington, D.C.: United States Government Printing Office, 1967.
7. U.S. Department of Labor. Manpower Report of the President. Washington: U.S.Government Printing Office, 1965.
8. Venn, Grant. "Hotline." Ainerican Association of School Administrators. Vol. 2, No. 1.Washington: American Association of School Administrators, February, 1969.

Empirical Basis for Job Clusters
1. B. Asbell. New Directions in Vocational Education (Washington, D.C.: U.S. GovernmentPrinting Office, 1967).
2. J. K. Coster and E. W. Courtney. "Factors Analyses of Agricultural Competencies andWorkers in Three Selected Occupations." (Purdue University Studies in Education,1965).
3. N. F. Frantz, Jr. "The Cluster Concept as a Program in Vocational Education at theSecondary School Level." Paper presented at a conference on research in vocationaland technical education. (University of Wisconsin, 1966).
4. E. J. Morrison. "General Vocational Skills and the Secondary Curriculum." Paperpresented at a conference on research in vocational and technical education.(University of Wisconsin, 1966).
5. H. F. Rahmlow and L. Winchell. Mathematics Clusters in Selected Areas of VocationalEducation. (Washington State University, 1966).
6. D. D. Sjogren. "A Functional Approach to Curriculum Development." Unpublishedpaper presented at American Educational Research Association, February, 1969,
7. D. D. Sjogren and R. Sahl, Review of Research on Common Job Behaviors. InterimReport, U.S. Office of Education Contract No. 0E-6-85-073, (Fort Collins,Colorado: Colorado State University, 1966).
8. D. D. Sjogren, W. Schroeder and R. Sahi. The Identification of Common BehavioralFactors as Bases for Pre-entry Preparation of Workers for Gqinful Employment. U.S.Office of Education Contract No. 0E-6-85-073. (Fort Collins, Colorado: ColoradoState University, 1967).

!
li
APPENDIX A

I
Intended Purpose and Samples for Performance Elements
The intended use for the questionnaire is to have a large sample (N=500) of 1 1 th gradeteachers identify performance elements which can best be integrated into present localcourse content; to have the health occupations teacher-coordinator identify performanceelement that will become the focus of activities and projects in the elective course(s); and tohave administrators, supervisors and job incumbents (N=500) engaged in delivering healthservices identify those performance elements which should be the responsibility of theorientation experience in the clinical affiliate. A digest of division of responsibility willresult in a high level of accountability for specific performance element and tend to assureinclusion of all performance elements in the 1 lth grade experience.
Questionnaire to Determine Essentialityof Performance Elements
Name of Job:
Your relationship to job: (check)
Worker
Supervisor
Administrator
Directions: This questionnaire consists of a list of performance elements, that is, things thatpeople in certain health jobs are able to do. You are to do two things with each performance
element.
Teacher
Other (describe)
1. Indicate (check) how necessary it is for the job you are rating.
If it is something that everyone in that job must be able to do,check under "required."
If it is something that is helpful in the job but not absolutelynecessary, check under "desirable."
If it is something that is not needed in the job or not related tothe job, check under "not needed."
2. indicate (check) where in your opinion the "required" and "desirable:performance elements are best taught by checking under either"in the classroom" or "on the job." This check is not needed for anyperformance elements which you have already checked as "not needed."

Name of Job:
Performance Element
NecessityLearnedBest
"0CD w or- "t3 o '7
CU .0 CU 0CU CI)Z: .0r V) 4-I
id 4-1 .-(1) 0E;
ELEMENTS REGARDING WORK SITUATION
Has a general appreciation of the activities ofpersonnel in health care institutions.
Develops understanding of the organization of themedical staff in his work situation.
Knows the definition of the majority of presentday health care specialities and the standard titleof a person practicing in those specialities.
Knows how to find the definition of healthspecialities with which he is not familiar.
Can describe the responsibilities of the peoplewith whom he works most closely, the relationshipof hiw work to theirs, and his value in patientcare.
Knows to whom to report work problems.
Refers problems for proper dispostion.
Knows how to report when he must be absent or late.
Knows how to find out about personnel policieswhich affect him in his job.
Knows how to find out about opportunities foradvancement in his chosen field.
Can locate information about services offered byhealth and other service agencies in the communityand state.
Is able to describe some of today's major healthproblems and their contributing factors.
Develops skill in asking questions to determine thescope, responsibilities and limitations of his job.
Knows how to ask for changes in jobresponsibilities.

1
a!
Name of Job:
Performance Element
Necessity
Knows how to resign from his job.
Asks questions to find out what is considered"appropriate" and/or "in good taste" concerningdress, make-up, hair style, jewelry, accessories,etc. for the institution or position.
Can use policy and procedure manuals, referencebooks, workbooks and bulletin boards and keepthem readily available in order.
Plans work considering relative importance oftasks, needs of other health team workers, andneeds of patient and their frjmilies.
Develops increasing ability to assess situationsand determine priority for actions in routine andemergency situations.
Plans work for economy of time, motion andequipment.
Works within limits of delegated and establishedprocedures.
Questions when asked to perform procedures notwithin delegated duties.
Asks for guidance when in doubt about implementinga procedure.
Performs within limits of training and ability.
Demonstrates an understanding of the limitationsof his knowledge, and avoids premature conclusionsand advice.
Maintains the confidential nature of informationrelating to patient care and condition.
Uses established procedures to safeguard patient'sbelongings.
Understands hospital's liability for safe keepingof patients' property.
LearnedBest-.................
.0E 0o r",0S.- 0.1In .0(A 4P
E;cCD

Name of Job:
Performance Element
ELEMENTS REGARDING SAFETY
Is alert to potential environmental hazards.
Places furniture and equipment for convenient andsafe use.
Removes spilled liquids, broken glass and otherobjects from the floor.
Demonstrates understanding of fire prevention andcontrol by:
-keeping stairways and shaft doors closed
- disposing of combustible materials inappropriate containers
-following employee smoking regulations
- removing spark producing equipment ormaterials before beginning proceduresusing oxygen or other explosive gases
Knows how to activate institutional fire alarmsystem.
Knows location of and how to operate fireextinguishers.
Knows location and use of fire exits.
Knows location of equipment and procedures forcarrying out first aid in emergency and/oraccident in the department.
Demonstrates understanding that hospital personnelare responsible under law to carry out the care ofa patient and in a manner that keeps the patientsafe from harm.
Identifies patient accurately and in anappropriate manner.
NecessityLearnedBest

Name of Job:
Performance Element
NecessityLearnedBest
Asks patient to identify himself.
Calls patient by name, not be room or bed number.
Checks identification marker of patient whenmoving, transporting, observing, reporting,recording, when giving personal care, medication,treatment, or diagnostic test, and when trans-ferring responsibility.
Instructs patient as to safety measures in the useand disposal of tobacco and matches.
Knows hospital routine for fire in patirlt areaand follows procedures for closing doors,reassuring and aiding patients.
Follows directions in the application of heat andcold.
Follows established procedures for security ofmedical supplies.
Knows and follows narcotic serwriiv practices.
ELEMENTS REGARDING FIRST AID
Has sufficient knowledge of common medicalconditions and the most common medical emer-gencies to appropriately give first aid.
Has sufficient knowledge of common medicalconditions and the most common medical emer-gencies to obtain and transmit relevantinformation.
Understands and develops skill in use of pressuredressings, manual pressure, and tourniquets, tostop bleeding.
Recognizes local and general, external andinternal, effects of shock and hemorrhage.
r

Name of Job:
Performance Element
NecessityLearnedBest
Knows how to locate and how to contact nearestpoison control center.
Is familiar with emergency care of victims ofpoisoning and of overdosage of drugs.
Understands the importance of maintenance ofrespiratory function, and can check for open air-way, perform mouth to mouth resuscitation, usemechanical resuscitation equipment, and performclosed chest heart massage.
ELEMENTS REGARDING TERMINOLOGY
Knows the common word elements used to formulatemedical terms for the body parts and systems, forthe most common diseases and conditions, diagnoses,and surgical procedures.
Pronounces and interprets medical terms correctly.
Follows directions given in medical phraseology.
Uses a glossary, dictionary or medical dictionaryto check meaning and spelling of terms.
Demonstrates ability to find further informationabout patient care or condition by appropriateuse of: Kardex, charts, procedure books,dictionary, medical dictionary, glossaries,work area reference books, library facilities.
Makes accurate use of pertinent medical term-inology in writing and reading reports and inverbal communication concerning patient care.
Develops ability to recognize the meaning of un-familiar words on the basis of the word rootswhich they contain.
Is able to define medical terminology in laylanguage.
a

Name of Job:
Performance Element
NecessityLearnedBest
MI0) 0
.0) E 0
1:1 1:1 0 P)0) .0 CU 0L ftS 0J L. wI, I. = Vi .0= or- Uf 4-0C7 03CD CD 0 C
CZ CZ = C.) CD
ELEMENTS REGARDING HEALTH AND HYGIENE
Incorporates principles of good health and hygieneand good grooming into personal daily living habits.
Maintains acceptable skin care through bathing,personal cleanliness, use of deodorants, etc.
Maintains a healthy balance of rest and activity.
Is able to relate personal hygiene measures to aknowledge of micro-organisms and body defenses inhealth and disease.
Follows precautionary policies of the institutionor agency, set up to protect health of personneland patients.
Uses good body mechanics to minimize physicalstrain when sitting, standing and walking.
Uses good body mechanics to minimize physicalstrain and/or injury when lifing, pushing, reaching,stooping.
Avoids injury to self and patient by practicinggood body mechanics when moving patients.
Requests assistance to move patients who are heavyor difficult to move.
Handles patient, and equipment used in the care ofpatients, firmly but gently.
Demonstrates ability to position patients withattention to good body alignment.
Can distinguish between food fads and diets whichare based on scientific principles of nutrition.
Can explain how disease may result from an un-balanced diet and from lack of certain foods.

Name of Job:
Performance Element
NecessityTarnerBest
Can relate differences in food needs to differencesin age, development, and activity of individuals.
Shows appreciation of the effect of family customsand personal opinion on the food habits.
Shows appreciation of the differences in foodhabits which are associated with differences innational origin, regional patterns and religiousand socio-economic backgrounds.
Assist in teaching patient hygiene.
Has sufficient knowledge of common medicalconditions and the most common medical emergenciesto be able to assess indication of urgent needfor medical care.
ELEMENTS REGARDING ASEPSIS
Follows handwashing practices according toprocedures set to maintain control of infection.
Washes hands before patient care procedures, orbefore handling clean equipment, linen, food andfood equipment.
Washes hands after handling soiled equipment andsupplies, linen, patient discharges, or aftergiving patient personal care.
Has clean nails, short enough to not interferewith procedures.
Carries out procedures to prevent spread ofinfection from clothing worn by hospitalemployees and visitors.
Keeps hair clean, neat and under control bystyling, arrangement, spray or uses hair net orcap to cover hair where required.
Keeps work areas clean and free of clutter.

I I
Name of Job:
Performance Element
NecessityLearnedBest
.13cu cu E o
8 IWS.. MI Wor 1.. .0
or 11) 4-1CT VI 4-3 RS
CC CS CDre:3O
Has sufficient knowledge of microbiology to under-stand established procedures concerning sterili-zation and aseptic technique.
Recognizes by name bacteria and organisms whichpresent the greatest danger and knows their commonmodes of transmission.
Follows procedures for separate storage of sterileand unsterile supplies and equipment.
Is able to use sterile transfer or pickup forcepswithout contaminating them.
Is able to open containers of sterile supplieswithout contamination of contents-,-or inside ofpack, container or lid.
Understands terms used in sterilization and dis-infection sufficiently well to follow instructionsor follow procedures for cleaning, disinfectionand sterilization.
Follows and helps enforce established proceduresfor aseptic control by restricing unauthorizedpersons to certain areas.
Follows prescribed policies in reporting infectionsand open lesions.
Controls cross infection by following safety pre-cautions in disposal of waste.
Recognizes that all specimen collecting containersare a possible source of infection and handlesthem accordingly.
Correctly uses and disposes of equipment andsupplies used in the care of patients in isolation.
Stores food items in designated place at correcttemperature to prevent spoilage and contamination.
Detects and discards food spoilage.

Name of Job:
Performance Element
Necessity
alCU
10" VICU CUCC C3)
ELEMENTS REGARDING INTERPERSONAL RELATIONS
Is able to recognize and accept emotional reactionscommonly seen in illness and crisis situations.
Is aware of the influence of his conduct andattitudes upon the emotional state and behaviorof others.
Maintains respect for the individual emotionallydistraught patient.
Is able to maintain hit., own emotional control whencarrying out orders to restrain unruly or dis-turbed patients.
Is able to work effectively with persons whosesocial standards of behavior differ from his own.
Demonstrates calmness and objectivity in workingwith uncooperative persons.
Is able to maintain objectivity when criticized.
Is able to maintain a reasonably calm, unhurriedattitude in tense situations.
Seeks guidance from professiondq for help inindividualizing care of patients with specialor severe emotional problems.
Assists in carrying out plans for helping patientsand families adjust to special problems.
Introduces self to patient, and tries to make himfeel at ease.
Appears by posture, conversation and expression tobe interested in patient and/or visitor and/orcoworker.
Makes appropriate referrals of expressed or obvioussocial service, home nursing, emotional or spirit-ual needs of patients.
LearnedBest

Name of Job:
Performance Element
Helps the patient and family to understand andfollow directions of the specialist.
Participates in plans for the patient's rehabili-tation by encouraging the patient to developphysical independence.
Explains the patient's rehabilitation to hisfamily and assists them in participating in theplan.
Makes arrangements for simple types of diversionor recreation of the patient.
Gives patient recognition when progress is made orgoals are reached.
Knows to whom to report patient care problems, andhow to ask for, and offer help.
Develops ability to work cooperatively with theothers in care of patients.
Develops ability to assess and use language thepatient understands in explanations of proceduresand in teaching health care.
Respects patient's needs for privacy in ways suchas: pulling cubicle curtains when giving care,knocking on door before entering, addressingpatient by name before entering curtained cubicle,draping patients adequately during treatment.
Shows awareness of the effects of growth anddevelopment by adapting patient care to thepatient's age and level of development.
Allows patient mental and emotional privacy asneeded in accepting their reactions to pain,tension and embarrasment.
Has sufficient knowledge of common personalitydisorders and common mental disturbances to beable to assess approach to patient care and torecognize gross abnormalities.
learned`"Necessity Best
W'0CUr1
W .0 WI, RI W,.. 1. =Z I-CT VI 4-1CU W 0
C X 0 =
E.000 P-30
S. WVI .0In 44MIGo C0

Name of Job:
Performance Element
NecessityLearneBest
.0(111 cu Er '0 7 "",
CU .0 CU 05 Is (1) L. CUL. z tn= 4.00 WI 4-$cu 0
CC
ELEMENTS REGARDING USE OF EQUIPMENT
Recognizes and identifies commonly used instrumentsand equipment.
Follows procedure books or instructions in deter-mining the equipment and supplies needed for treat-ments or procedures.
Demonstrates good planning by collecting well inadvance of assigned tasks all necessary suppliesand equipment.
Can operate transportation or communication equip-ment used in the departments such as elevator,dumbwaiter, or pneumatic tube.
Follows instructions for reading and reporting ondevices, such as gauges, meters, dials, indicators,numerical counters, at appropriate intervals.
Identifies and stores poisonous and harmfulchemicals, according to procedure, to preventmisuse.
Follows procedures for periodic checks of clean-liness and operation of equipment.
Reports and avoids use of damaged equipment.
Checks inventory and orders unit supplies.
Collects and returns equipment to supply room.
Select appropriate equipment and supplies forcleaning and:other procedures, uses asspecified.

4
Name of Job:
Imo. ~or oticalmOtWas_ ms Was
Performance Element
Necessity
Knows who has the responsibility for completionof the various sections of the medical record.
ELEMENTS REGARDING COMMUNICATIONS
Recognizes and immediately reports deviations fromnormal range in patient's vital signs and signifi-cant changes in patient's condition.
Notes, observes and reports signs which wouldindicate an undesirable reation to medicationor treatment.
Asks for guidance in considering requests ofpatients who are restricted db to diet,activities, fluids, etc.
Reports comments about care and service tosuperiors.
Assists other health team member with patientexamination, diagnostic test treatment or care.
Checks that patient's name and/or identifyingdata is on each page of patient record.
Is conscientious and accurate in reportingpertinent patient's information about the careand condition.
Demonstrates tact in giving and withholdinginformation relative to patient care and theoperation of the hospital.
Is aware of and follows established proceduresrelating to release of information to law enforce-ment officers, insurance representatives, family,patient, and other hospital and health personnel.
Is familiar with authorization and accident reportforms and follows established procedures for theiruse (e.g., autopsy, surgery, diagnostic tests,discharge forms)

Name of Job:
Performance Element
Cooperates in a courteous manner with personnelin other departments.
Knows the names, functions and abbreviations ofother departments or agencies with whom he haswritten or telephone contact.
Is able to complete reporting forms, inter-officeforms, and forms requesting referral to otherinstitutions or departments.
Is able to prepare written communications forordering equipment, and requesting informationor assistance.
Writes reports that are accurate, complete, under-standable and legible.
Uses notes or other reminders to insure accuracyof reports.
Reports malfunctioning equipment and accidenthazards.
Follows directions for summoning and directingaid and reporting medical or other emergencies.
Can follow written and verbal directions incarrying out procedures .
Is able to use the telephone to give and receiveinformation accurately and courteously.
Answers telephone calls promptly.
Allows caller to express himself.
Can use telephone for incoming and outgoing callsand transferring calls in institution or agency.
Demonstrates ability to operate signalling system,paging system, and intercom system in institutionor agency.
Necessity1111r111
LearnedBest

APPENDIX B

-4,,..s...iiiWrisaMETE---...1,..neWligESSMI Irmli'
a
CAREERS Mg HEALTH OCCUPATIONS
An Opportunity for You
What the program is....
Your school will be conducting an experiment in which you will have the opportunity toexamine jobs within the health service career field.
The largest single sector of the work force will soon be in the health service occupations.There are tremendous demands for persons to enter health service jobs.
Not only are there many jobs available at the beginning level for high school graduates andpersons who quit school, but there is also the opportunity for you to climb the career ladderto better jobs in health services.
This is your opportunity to participate with . :,achers, professionals and health facilitiespersonnel in a partnership to secure a promising career future for yourself.
Beginning health service positions....
Nurse's Aide or OrderlyHome Health Aide
Psychiatric AideDietray Aide, Food Service Aide, Dietary Clerk
Medical Records ClerkWard Clerk
Medical Office AssistantDental Assistant
Ambulance and Emergency Assistant
Health service careers are designed for these students....
1. Students who want to explore occupational opportunities inthe health field.
2. Students who plan to prepare for a professional or technicalhealth occupation following high school graduation.
3. Students who are considering quitting school and who wantvocational training in an occupation area of high employmentopportunity.
4. Students who want to learn a saleable skill that will helpthem defray college expenses.

r ....*V.IVIPAMI
5. Students whose occupational goals include a career of socialas well as personal value.
6. Students who want some basic knowledge of health care thatthey can apply to themselves or their families.
This is how it works....
Your school will provide a realistic health service situation to introduce you to healthservice agencies. That will be followed by first hand experiences in actual health facilities.You will have the opportunity to identify the various -"ccupational roles in the health field,to understand their objectives and to plan for entering' a specific job.
If you desire to enter a health service job, you will be assisted in doing so with anindividualized program designed to prepare you for a specific job. Your school will haveguidelines and resources for directing your program and coordinating youi study andexperiences. Your individual program will also be planned cooperatively with healthfacilities, in your community.
Your school has a full time health occupations coordinator who will guide your programstarting in the junior year. He will coordinate the efforts of your teachers and the healthservices in the community in preparing and directing your studies. He will plan clinicalexperiences for you in your junior and senior years.
Test yourself....
Do you have those personal characteristics needed for a successful Health Service career?
1. Are You adaptable, and genuinely ,interested in people? Do you get alongwith'others?
Health services are concerned chiefly with people.
2. Do you have good health, a pleasing personality and a sense of humor?
Health service personnel need enthusiasm and energy. You willneed to be friendly and have good health.
3. Do you enjoy social studies and science?
Health service personnel help other people get the benefits
of modern advances in medical and social sciences. Theseaptitudes will be the foundations upon which you will buildyour career in health services.
4. Can you express yourself effectively in different ways?
Health service personnel make observations and prepare recordinformation vital to the well being of the patient. You willneed to write and speak well to participate as a member of amedical team.

I ;I
5. Are you reliable and accurate?
The patient's care requires a high degree of dependabilityand precise record keeping.
6. Do you have patience, good judgment, and common sense?
You will be called upon to work with many professional people....physicians, nurses, engineers and administrators.
How did you score?
If you can answer yes to the above questions, you may wish to consider further thepossibility of a career in the health services. For additional information, arrange a meetingwith your health occupations counselor.