Embed Size (px)
Citation preview

European Annals of Otorhinolaryngology, Head and Neck diseases (2013) 130, 95—98
Available online at
www.sciencedirect.com
CASE REPORT
Ectopic pyriform sinus parathyroid adenoma
N. Guevaraa,∗, B. Agopiana, D. Benisvyb, S. Lassallec, J. Santini a,L. Castilloa
a Institut universitaire de la face et du cou, groupement de coopération Sanitaire, centre hospitalier universitaire de Nice,centre Antoine-Lacassagne, 31, avenue de Valombrose, 06107 Nice cedex 2, Franceb Service de médecine nucléaire, centre Antoine-Lacassagne, 33, avenue de Valombrose, 06189 Nice cedex 2, Francec Laboratoire de pathologie clinique et expérimental, hôpital Pasteur, CHU de Nice, 30, avenue de la Voie-Romaine, 06000 Nice,France
KEYWORDSAdenoma;Parathyroid;Pyriform sinus;Ectopic
SummaryObjective: To describe the diagnosis and treatment of ectopic pyriform sinus parathyroid ade-noma.Material and methods: A 44-year-old woman presented with persistent primary hyperparathy-roidism after previous failed cervical exploratory surgery.Results: Diagnosis of ectopic pyriform sinus parathyroid adenoma was suggested by computedtomography and technetium-99 m sestamibi scintigraphy (99mTc-MIBI SPECT/CT). A submucosaltumor was identified under laryngoscopy and resected by endoscopic CO2 laser. Histopathology
confirmed the diagnosis of parathyroid adenoma.Conclusions: Ectopic pyriform sinus locations are rare in parathyroid adenoma. 99mTc-MIBISPECT/CT facilitates diagnosis, especially in case of previous failed neck exploration. Endo-scopic CO2 laser resection is the treatment of choice.© 2012 Elsevier Masson SAS. All rights reserved.bl
asr
Introduction
Ectopic parathyroid adenoma is a significant cause of post-surgical persistent primary hyperparathyroidism (PHPT) [1].
Pre-operative assessment generally allows diagnosis ofthe ectopic gland, but there remains a non-negligible riskof false negatives, as not all parathyroid lesions take up
sestamibi in the same way [2].False positives on this examination are much rarer, oftendue to associated nodular thyroid pathology [3].
∗ Corresponding author. Tel.: +33 04 92 03 17 68.E-mail address: [email protected] (N. Guevara).
C
Aoa
1879-7296/$ – see front matter © 2012 Elsevier Masson SAS. All rights redoi:10.1016/j.anorl.2012.04.008
A pyriform sinus location is quite exceptional; there haseen only one report of management by endoscopic CO2
aser [4].We report the case of a woman presenting with ectopic
denoma of the pyriform sinus, not diagnosed on initialcintigraphy, and treated, after failure of classic neck explo-ation, by endoscopic CO2 laser.
ase report
44-year-old woman was referred for surgical managementf PHPT. Two successive assessments found hypercalcemiand inadequate parathormonemia (ionized calcium and PTH:
served.

96
Figure 1 Weighted subtraction images after planar scintig-raphy (99mTc/99mTc-MIBI). Hyperfixation at right parathyroid P4(black arrow). NB: moderate fixation could be discerned onretrospective re-reading in the inferior part of the left sub-mandibular fovea (white arrow), doubtless corresponding to thepyriform sinus adenoma.
1(mrri
amn
iHp
tssga
o
Cslar
cu
D
Pra
foSftc(essa
riuula
aosrsThis
ilUtei
dbcagdwyta
k[
.48 mmol/L; 56 pg/L (< 38.8), and 1.36 mmol/L; 122.7 ng/L< 51), respectively. Cervical ultrasound found a non-suspectulti-micronodular thyroid with no increase in parathy-
oid volume. 99mTc-MIBI parathyroid scintigraphy suggestedight retrothyroid hyperfunctional parathyroid more or lessn position P4 (Fig. 1).
Cervicotomy with right parathyroid exploration wasssociated to resection of the right P IV, which showedacroscopically increased volume. Histology found slight
odular hyperplasia.Postoperative biological analysis found persistent PHPT:
onized calcium, 1.40 mmol/L; PTH, 93 pg/mL (< 38.8).ormonal assessment for associated multiple endocrine neo-lasia was normal.
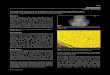
Parathyroid scintigraphy was again performed, coupledo CT (99mTc-MIBI SPECT/CT), 2 months post-surgically. Theestamibi fixation facing the right fossa was unchanged;estamibi fixation as seen at the left pyriform sinus was sug-estive of a hyperfunctional ectopic parathyroid or of andenopathy (Fig. 2).
Flexible endoscopy visualized a submucosal tumefactionf the left pyriform sinus (Fig. 3).
Direct suspension laryngoscopy was performed, withO2 laser lesion resection. Macroscopic examination of thepecimen found a 1.8 × 1 × 1-cm nodular lesion of tissu-ar consistency. Anatomopathologic examination suggesteddenoma, despite the absence of an identifiable residual
ing of normal parathyroid tissue.Postoperatively, blood values returned to normal: ionizedalcium, 1.15 mmol/L; PTH, 10.1 ng/L; at 6 months’ follow-p, there was no recurrence.
ccfb
N. Guevara et al.
iscussion
HPT involving ectopic pyriform sinus adenoma has beenarely reported, and often entails difficulties of diagnosisnd treatment [4,5].
In the present case, initial scintigraphy was false-positiveor right retrothyroid adenoma, showing a subtraction imagef sestamibi fixation with right supralobular projection.cintigraphy generally shows excellent specificity, with thealse-positive risk basically limited to associated nodularhyroid pathology [6], as in the present case. Image fusionoupling single-photon emission CT to conventional CT scanSPECT/CT) easily detects such false positives. It also greatlynhances diagnostic sensitivity to ectopic adenoma [7] andeems indispensable in patients having already undergoneurgical exploration. It is indeed sometimes recommendeds a systematic first-line examination [8].
Thus, retrospectively, on the second scintigraphic explo-ation, the right supralobular projection image could benterpreted as showing micronodular lesions with greaterptake of 99mTc-MIBI than of technetium alone. As theltrasound and peroperative aspects of these micronodularesions were in no way suspect, no surgical treatment waspplied.
It is noteworthy that the first scintigraphic examinationlso failed to diagnose ectopic adenoma. The sensitivityf planar scintigraphy is around 87% to 94% [2,6]. Eveno, on retrospective re-reading of the first results, slightlyeinforced fixation projecting under and inward of the leftubmaxillary gland could be discerned on the planar images.his represented fixation of the ectopic adenoma, which,owever, was overlooked due to the low degree of fixation,ts unexpected location and the apparently more typicalcintigraphic right P4 image.
Cervical ultrasound is indispensable: it also can revealncreased parathyroid volume and enables precise morpho-ogic assessment of the thyroid gland. Thus, associatedS-SPECT-CT performs better than the alternative imagingechniques, raising sensitivity to more than 90% and thusnabling even more precise selection of candidates for min-mally invasive surgery [5,9].
Embryologically the P3 and P4 parathyroids are of endo-ermic origin, deriving respectively from the 3rd and 4thranchial clefts. Two types of ectopia have been reported:ongenital, resulting from pathologic embryonic migration,nd acquired, resulting from secondary migration underravitational force. To these may be added embryonicefects in pharyngeal sac migration, a rare pathology inhich vestigial parathyroid tissue may subsist in the phar-nx. It is rare for adenoma to develop on such vestigialissue; very few cases have previously been reported [10],nd the present case is an addition to these.
Endoscopic CO2 laser resection has, to the best of ournowledge, been described in only one previous report4]. The technical characteristics of CO2 laser enable pre-ise non-hemorrhagic surgery and thus complete excisiononserving the gland. This intra-cavity technique avoidedurther cervicotomy, thus minimizing surgery time and mor-
idity.
Ectopic pyriform sinus parathyroid adenoma 97
Figure 2 Tomoscintigraphy coupled to CT (99mTc-MIBI SPECT/CT). Tissue image with moderate Tc-MIBI fixation localized in theleft pyriform sinus.

98
Fa
C
Enil
D
Tc
R
igure 3 Flexible endoscopy. Submucosal mass in the superiornd posterior part of the left pyriform sinus.
onclusions
ctopic pyriform sinus locations are rare in parathyroid ade-oma. 99mTc-MIBI SPECT/CT facilitates diagnosis, especiallyn case of previous failed neck exploration. Endoscopic CO2
aser resection is the treatment of choice.
[
N. Guevara et al.
isclosure of interest
he authors declare that they have no conflicts of interestoncerning this article.
eferences
[1] Suliburk JW, Sywak MS, Sidhu SB, et al. 1000 minimallyinvasive parathyroidectomies without intra-operative parathy-roid hormone measurement: lessons learned. ANZ J Surg2011;81(5):362—5.
[2] Gallowitsch HJ, Mikosch P, Kresnik E, et al. Compari-son between 99mTc-tetrofosmin/pertechnetate subtractionscintigraphy and 99mTc-tetrofosmin SPECT for preoperativelocalization of parathyroid adenoma in an endemic goiter area.Invest Radiol 2000;35(8):453—9.
[3] Krausz Y, Shiloni E, Bocher M, et al. Diagnostic dilem-mas in parathyroid scintigraphy. Clin Nucl Med 2001;26(12):997—1001.
[4] Stojadinovic A, Shriver CD, Casler JD, et al. Endoscopic laserexcision of ectopic pyriform sinus parathyroid adenoma. ArchSurg 1998;133(1):101—3.
[5] Fraker DL, Harsono H, Lewis R. Minimally invasive parathy-roidectomy: benefits and requirements of localization, diag-nosis, and intraoperative PTH monitoring. Long-term results.World J Surg 2009;33(11):2256—65.
[6] Hindie E, Melliere D, Jeanguillaume C, et al. Parathy-roid imaging using simultaneous double-window recordingof technetium-99m-sestamibi and iodine-123. J Nucl Med1998;39(6):1100—5.
[7] Pata G, Casella C, Besuzio S, et al. Clinical appraisalof 99m technetium-sestamibi SPECT/CT compared to con-ventional SPECT in patients with primary hyperparathy-roidism and concomitant nodular goiter. Thyroid 2010;20(10):1121—7.
[8] Thomas DL, Bartel T, Menda Y, et al. Single photon emissioncomputed tomography (SPECT) should be routinely per-formed for the detection of parathyroid abnormalities utilizingtechnetium-99m sestamibi parathyroid scintigraphy. Clin NuclMed 2009;34(10):651—5.
[9] Patel CN, Salahudeen HM, Lansdown M, et al. Clinicalutility of ultrasound and 99mTc sestamibi SPECT/CT for pre-operative localization of parathyroid adenoma in patientswith primary hyperparathyroidism. Clin Radiol 2010;65(4):278—87.
10] Chan TJ, Libutti SK, McCart JA, et al. Persistent primaryhyperparathyroidism caused by adenomas identified in pha-ryngeal or adjacent structures. World J Surg 2003;27(6):675—9.
![Parathyroid Adenoma/Thymoma Case Reportadenoma and thymoma without mention of sestamibi uptake by the thymoma (whether such imaging was performed or not). Byrne et al. [13] demonstrated](https://img.pdfslide.us/doc/110x75/5e2f040ac0577556e1278f0b/parathyroid-adenomathymoma-case-adenoma-and-thymoma-without-mention-of-sestamibi.jpg)